748 A CADEMIC M EDICINE , V OL . 75, N O . 7/J ULY 2000 R ESEARCH R EPORT Stress Management in Medical Education: A Review of the Literature Shauna L. Shapiro, MA, Daniel E. Shapiro, PhD, and Gary E. R. Schwartz, PhD ABSTRACT Purpose. To review systematically clinical studies pro- viding empirical data on stress-management programs in medical training. Method. The authors searched Medline and PSYCHINFO from 1966 to 1999. Studies were included if they evalu- ated stress-management programs for medical trainees (medical students, interns, or residents); reported empir- ical data; and had been conducted at allopathic medical schools. Results. Although the search yielded over 600 articles discussing the importance of addressing the stress of med- ical education, only 24 studies reported intervention pro- grams, and only six of those used rigorous scientific method. Results revealed that medical trainees partici- pating in stress-management programs demonstrated (1) improved immunologic functioning, (2) decreases in de- pression and anxiety, (3) increased spirituality and em- pathy, (4) enhanced knowledge of alternative therapies for future referrals, (5) improved knowledge of the effects of stress, (6) greater use of positive coping skills, and (7) the ability to resolve role conflicts. Despite these prom- ising results, the studies had many limitations. Conclusion. The following considerations should be in- corporated into future research: (1) rigorous study design, including randomization and control (comparison) groups, (2) measurement of moderator variables to deter- mine which intervention works best for whom, (3) spec- ificity of outcome measures, and (4) follow-up assessment, including effectiveness of future patient care. Acad. Med. 2000;75:748–759. Medical education has deleterious con- sequences. Trainees (students, interns, and residents) suffer high levels of stress, which lead to alcohol and drug abuse, 1 interpersonal relationship diffi- culties, 2 depression and anxiety, 3,4 and even suicide. 5 Medical students have mean anxiety scores one standard de- viation above those of non-patients, and their depression levels increase sig- Ms. Shapiro is a doctoral student in clinical psy- chology, University of Arizona, Tucson. Dr. Shapiro is assistant professor, Departments of Psychiatry and Integrative Medicine, University of Arizona College of Medicine. Dr. Schwartz is professor of psychol- ogy, neurology, psychiatry, and medicine, University of Arizona. Correspondence and requests for reprints should be addressed to Ms. Shapiro, University of Arizona De- partment of Psychology, Tucson, AZ 85721; e-mail: ^[email protected]&. nificantly throughout the first year of medical school. 6 Stress may also harm trainees’ professional effectiveness: it decreases attention, 7 reduces concentra- tion, 8 impinges on decision-making skills, 9,10 and reduces trainees’ abilities to establish strong physician–patient relationships. 11 To address these problems, programs have been changed in a variety of ways, including reducing the work week, 12 in- stituting curricular reforms (e.g., smaller classes, less rote memorization), and providing psychological services such as couples counseling, child care services, social activities, support groups, and stress-reduction programs. 13 A decade ago, after a comprehensive literature review of stress in medical ed- ucation, Butterfield concluded that ‘‘the body of literature on effective interven- tions needs to be expanded.’’ 14 Unfor- tunately, this recommendation has not been followed. Despite numerous arti- cles that decry the negative conse- quences of stress and call for interven- tion and change, few have studied the specific effects of stress-management in- terventions in medical education, and even fewer have provided empirical data. Although there is a large literature on stress management in general, its specific application to medical educa- tion has been largely unexplored. To fill this gap, in this article we re- view the literature on stress-manage- ment programs in medical education; specifically, programs providing trainees with coping techniques (such as medi- tation, hypnosis, imagery, and muscle relaxation), education regarding the psychological and physiological effects
Transcript
748 A C A D E M I C M E D I C I N E , V O L . 7 5 , N O . 7 / J U L Y 2 0 0 0
R E S E A R C H R E P O R T
Stress Management in Medical Education:A Review of the Literature
Shauna L. Shapiro, MA, Daniel E. Shapiro, PhD, and Gary E. R. Schwartz, PhD
ABSTRACT
Purpose. To review systematically clinical studies pro-viding empirical data on stress-management programs inmedical training.Method. The authors searched Medline and PSYCHINFO
from 1966 to 1999. Studies were included if they evalu-ated stress-management programs for medical trainees(medical students, interns, or residents); reported empir-ical data; and had been conducted at allopathic medicalschools.Results. Although the search yielded over 600 articlesdiscussing the importance of addressing the stress of med-ical education, only 24 studies reported intervention pro-grams, and only six of those used rigorous scientificmethod. Results revealed that medical trainees partici-pating in stress-management programs demonstrated (1)
improved immunologic functioning, (2) decreases in de-pression and anxiety, (3) increased spirituality and em-pathy, (4) enhanced knowledge of alternative therapiesfor future referrals, (5) improved knowledge of the effectsof stress, (6) greater use of positive coping skills, and (7)the ability to resolve role conflicts. Despite these prom-ising results, the studies had many limitations.Conclusion. The following considerations should be in-corporated into future research: (1) rigorous study design,including randomization and control (comparison)groups, (2) measurement of moderator variables to deter-mine which intervention works best for whom, (3) spec-ificity of outcome measures, and (4) follow-up assessment,including effectiveness of future patient care.Acad. Med. 2000;75:748–759.
Medical education has deleterious con-sequences. Trainees (students, interns,and residents) suffer high levels ofstress, which lead to alcohol and drugabuse,1 interpersonal relationship diffi-culties,2 depression and anxiety,3,4 andeven suicide.5 Medical students havemean anxiety scores one standard de-viation above those of non-patients,and their depression levels increase sig-
Ms. Shapiro is a doctoral student in clinical psy-chology, University of Arizona, Tucson. Dr. Shapirois assistant professor, Departments of Psychiatry andIntegrative Medicine, University of Arizona Collegeof Medicine. Dr. Schwartz is professor of psychol-ogy, neurology, psychiatry, and medicine, Universityof Arizona.
Correspondence and requests for reprints should beaddressed to Ms. Shapiro, University of Arizona De-partment of Psychology, Tucson, AZ 85721; e-mail:^[email protected]&.
nificantly throughout the first year ofmedical school.6 Stress may also harmtrainees’ professional effectiveness: itdecreases attention,7 reduces concentra-tion,8 impinges on decision-makingskills,9,10 and reduces trainees’ abilitiesto establish strong physician–patientrelationships.11
To address these problems, programshave been changed in a variety of ways,including reducing the work week,12 in-stituting curricular reforms (e.g., smallerclasses, less rote memorization), andproviding psychological services such ascouples counseling, child care services,social activities, support groups, andstress-reduction programs.13
A decade ago, after a comprehensiveliterature review of stress in medical ed-ucation, Butterfield concluded that ‘‘thebody of literature on effective interven-
tions needs to be expanded.’’ 14 Unfor-tunately, this recommendation has notbeen followed. Despite numerous arti-cles that decry the negative conse-quences of stress and call for interven-tion and change, few have studied thespecific effects of stress-management in-terventions in medical education, andeven fewer have provided empiricaldata. Although there is a large literatureon stress management in general, itsspecific application to medical educa-tion has been largely unexplored.
To fill this gap, in this article we re-view the literature on stress-manage-ment programs in medical education;specifically, programs providing traineeswith coping techniques (such as medi-tation, hypnosis, imagery, and musclerelaxation), education regarding thepsychological and physiological effects
A C A D E M I C M E D I C I N E , V O L . 7 5 , N O . 7 / J U L Y 2 0 0 0 749
of stress, affiliation with peers and op-portunities for emotional expression(support groups), and intensified rela-tionships with faculty. We then discussimplications for the integration of stressmanagement in medical training andmake suggestions for future research.
LITERATURE REVIEW
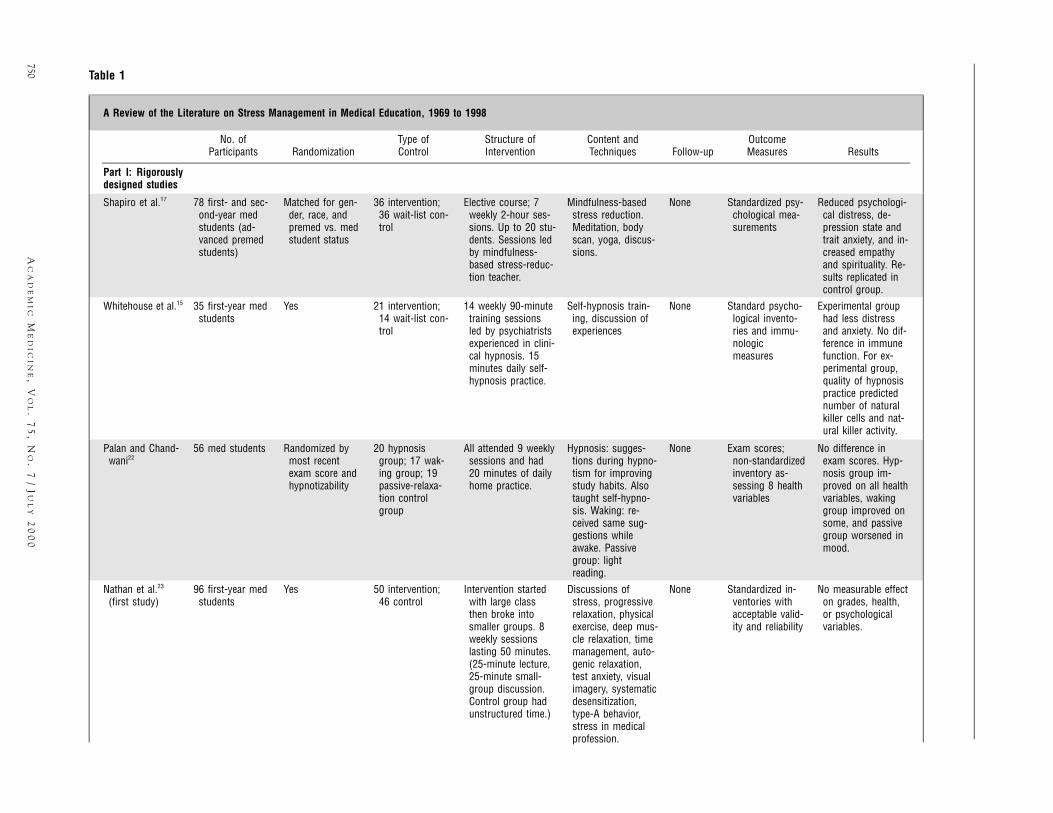
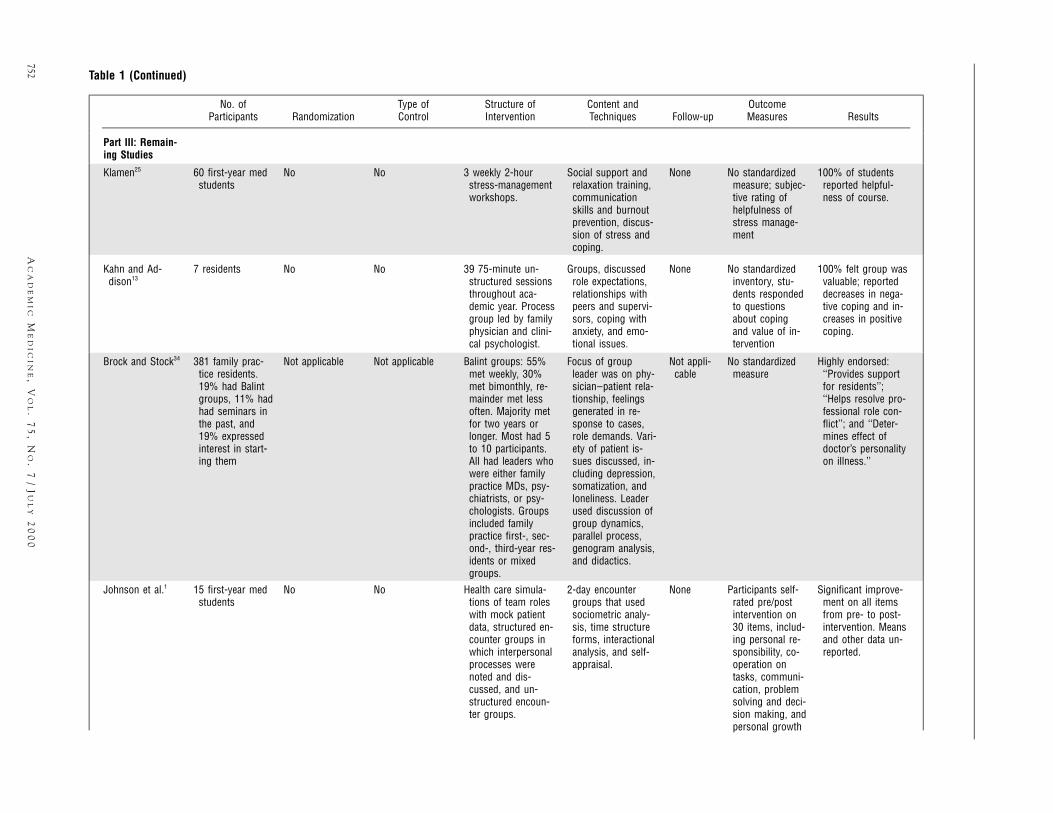
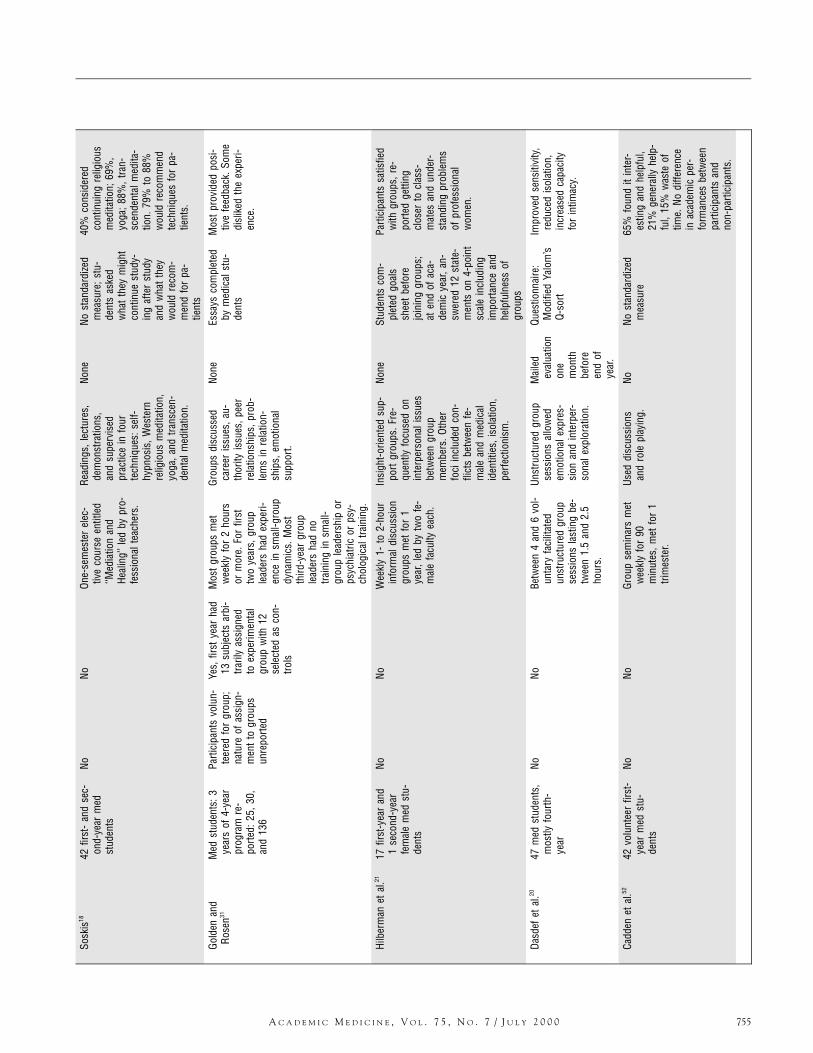
While the literature is replete with pa-pers discussing stress reduction or de-scribing specific programs, we foundonly 24 studies that reported data. Table1 provides a three-part matrix describ-ing these 24 studies across eight cate-gories: participants, randomization, con-trol groups, structure of intervention,content of intervention, follow-up, out-come measures, and results. Part I con-tains the six rigorously designed studies,Part II has the one study that violatedrandomization, and the remaining 18studies comprise Part III.
As can be seen in the table, the stud-ies looked at a heterogeneous group ofprograms that blended a variety of in-terventions and means of delivery. Ofthe 24 studies, only seven used controlgroups or attempted to randomize par-ticipants. This diversity and lack ofconsistent method makes drawing firmconclusions difficult.
Below we discuss each column of thematrix, highlighting key points and is-sues and discussing implications for fu-ture directions. We begin our review ofthe results by addressing the question,‘‘Are stress-management programs inmedical education effective?’’ We thenrefine our analysis by examining threeaspects of the studies: (1) participantsand methods, (2) interventions, and (3)outcome measures.
RESULTS
The 24 studies—the earliest one pub-lished in 1969, the latest in 1998—showed that the stress-managementprograms were helpful psychologicallyand/or physiologically, and virtually all
trainees who responded in all studieswere in favor of the programs’ being of-fered regularly or integrated into thecurriculum. Authors reported that par-ticipating trainees demonstrated im-proved immunologic functioning15,16;decreases in depression and anxiety15,17;increases in spirituality and empa-thy17; enhanced knowledge of alternativetherapies for future referrals18; improvedknowledge about stress19; improvedsensitivity toward themselves,20 theirpeers,20,21 and their patients20; reducedperceptions of isolation20; greater use ofpositive coping skills and less use ofnegative coping skills22; and resolutionof professional role conflicts.21
Only four studies reviewed found nodifference between experimental andcontrol groups on standardized measuresof psychological functioning, immunefunctioning, or health at post-assess-ment.15,19,23,24 However, of these fouronly one conducted any follow-up as-sessment, and this one did find a signif-icant positive change in the interven-tion group compared to the controlgroup. Trainee achievement, as assessedby examination performance, was con-sistently not correlated with participa-tion in stress-reduction programs.
Follow-up
Although all of the studies reported re-sults based on assessments immediatelyafter the interventions, only four20,24–26
assessed trainees beyond the end of theintervention. Of these, three reassessedparticipants a few months later and oneassessed subjects one year later. Whilefollow-ups supported the effectivenessof the interventions, the durations ofstress-management effects for the ma-jority of programs remain unclear.
Participants
Fifteen of the studies focused on medi-cal students, one included both resi-dents and medical students, and the re-maining eight focused on residents. Half
of the studies allowed participants indifferent years of training to participatein the same programs. The other halffocused on single years of training, mostcommonly the first year of medicalschool or residency. Because of the het-erogeneity of the programs described, itis difficult to draw conclusions abouthow these inclusion decisions influ-enced outcomes.
Most of the studies based their con-clusions on small samples. The majorityof the studies had samples under 30; thesmallest had six participants.26 Suchsmall sample sizes made it difficult tofind statistically meaningful results,make generalizations, and rule out typeII errors (incorrectly concluding that anintervention is not effective).
Finally, studies varied in their recruit-ment of participants. Most stress-man-agement programs recruited volunteers,but they may not have reached thosetrainees most in need. As noted by Reu-ben,27 severely impaired residents areleast likely to use support systems suchas groups, mental health counselors, orfaculty mentors. Other stress-manage-ment programs made attendance man-datory.28 This was more common in pro-grams for residents than in programs formedical students. A minority of partic-ipants in the mandatory programs re-sented the requirement; one studyfound that some residents felt that at-tending a support group indicated de-creased competence.28 Future researchshould compare the results of manda-tory and volunteer interventions. In ad-dition, given Reuben’s observation, itmay be particularly important to screenand then target those trainees found tobe most impaired, as they appear to bethe least likely to volunteer.
Randomization
Only seven of the studies15–17,22–24,28 ran-domly assigned participants, and onlyone of those28 used stratified samplingto ensure that equal numbers of differ-ent participants, in that case first-, sec-
750A
CA
DE
MI
CM
ED
IC
IN
E,
VO
L.
75
,N
O.
7/
JU
LY
20
00
Table 1
A Review of the Literature on Stress Management in Medical Education, 1969 to 1998
No. ofParticipants Randomization
Type ofControl
Structure ofIntervention
Content andTechniques Follow-up
OutcomeMeasures Results
Part I: Rigorouslydesigned studies
Shapiro et al.17 78 first- and sec-ond-year medstudents (ad-vanced premedstudents)
Matched for gen-der, race, andpremed vs. medstudent status
36 intervention;36 wait-list con-trol
Elective course; 7weekly 2-hour ses-sions. Up to 20 stu-dents. Sessions ledby mindfulness-based stress-reduc-tion teacher.
Reduced psychologi-cal distress, de-pression state andtrait anxiety, and in-creased empathyand spirituality. Re-sults replicated incontrol group.
Whitehouse et al.15 35 first-year medstudents
Yes 21 intervention;14 wait-list con-trol
14 weekly 90-minutetraining sessionsled by psychiatristsexperienced in clini-cal hypnosis. 15minutes daily self-hypnosis practice.
Self-hypnosis train-ing, discussion ofexperiences
None Standard psycho-logical invento-ries and immu-nologicmeasures
Experimental grouphad less distressand anxiety. No dif-ference in immunefunction. For ex-perimental group,quality of hypnosispractice predictednumber of naturalkiller cells and nat-ural killer activity.
Palan and Chand-wani22
56 med students Randomized bymost recentexam score andhypnotizability
No difference inexam scores. Hyp-nosis group im-proved on all healthvariables, wakinggroup improved onsome, and passivegroup worsened inmood.
Nathan et al.23
(first study)96 first-year med
studentsYes 50 intervention;
46 controlIntervention startedwith large classthen broke intosmaller groups. 8weekly sessionslasting 50 minutes.(25-minute lecture,25-minute small-group discussion.Control group hadunstructured time.)
Discussions ofstress, progressiverelaxation, physicalexercise, deep mus-cle relaxation, timemanagement, auto-genic relaxation,test anxiety, visualimagery, systematicdesensitization,type-A behavior,stress in medicalprofession.
None Standardized in-ventories withacceptable valid-ity and reliability
No measurable effecton grades, health,or psychologicalvariables.
A C A D E M I C M E D I C I N E , V O L . 7 5 , N O . 7 / J U L Y 2 0 0 0 751
Nath
anet
al.23
(sec
ond
stud
y)10
3fir
st-y
ear
med
stud
ents
Yes
49la
rge
grou
p;54
smal
lgro
ups
(7or
8ea
ch)
Com
pare
dla
rge
grou
pw
ithsm
all
grou
ps.A
llha
d8
wee
kly
50-m
inut
esse
ssio
ns(2
5-m
inut
ele
ctur
e,25
-min
ute
disc
ussi
on).
Sam
eas
abov
e.No
neSt
anda
rdize
dIn
-ve
ntor
ies
with
acce
ptab
leva
lid-
ityan
dre
liabi
lity
Nosi
gnifi
cant
diffe
r-en
ce
Kiec
olt-G
lase
ret
al.16
34m
edst
uden
tsYe
s17
inte
rven
tion;
17w
ait
listc
on-
trol
1035
-to
45-m
inut
ese
ssio
nsov
er21 / 2
wee
ks,i
nclu
ding
hypn
osis
and
led
bycl
inic
alps
ycho
lo-
gist
.
Sess
ions
prov
ided
over
view
ofhy
pno-
sis,
self-
hypn
osis
prac
tice,
prog
res-
sive
rela
xatio
n,au
-to
geni
ctra
inin
g,an
dim
ager
yex
er-
cise
s.At
end
ofse
ssio
nsfa
cilit
ator
mad
ehy
pnot
icsu
g-ge
stio
nsfo
rgr
eate
rre
laxa
tion
and
im-
prov
edst
udy
habi
ts.
None
Stan
dard
ized
psy-
chol
ogic
alm
ea-
sure
s,ba
selin
ehe
alth
repo
rt,fre
quen
cyof
re-
laxa
tion
prac
tice
and
imm
unol
ogic
mea
sure
s
Cont
rolg
roup
in-
crea
sed
inan
xiet
y,ob
sess
ive
com
pul-
sive
sym
ptom
s,an
ddi
stre
ss.N
odi
ffer-
ence
inac
adem
icpe
rfor
man
ceor
slee
pqu
ality
.With
inhy
pnos
isgr
oup,
mor
epr
actic
ew
asco
rrel
ated
with
im-
prov
edim
mun
efu
nctio
n.
Holtz
wor
th-M
un-
roe
etal
.2440
first
-an
dse
c-on
d-ye
arm
edst
uden
ts
Yes
20in
terv
entio
n,20
no-tr
eatm
ent
cont
rol
6w
eekl
y1-
hour
ses-
sion
sle
dby
ado
c-to
rals
tude
ntin
clin
-ic
alps
ycho
logy
.
Sess
ions
focu
sed
onte
achi
ngsu
bjec
tsto
chan
gem
alad
aptiv
eco
gniti
ons,
and
topr
actic
em
edita
tion
and
prog
ress
ive
mus
cle
rela
xatio
n.
10w
eeks
post
-in-
terv
entio
n
Este
emor
depr
es-
sion
Inte
rven
tion
grou
pre
porte
din
crea
sed
skill
sin
copi
ngw
ithsc
hool
-rel
ated
stre
ss.
Part
II:On
est
udy
that
viol
ated
rand
omiz
atio
n
Kelly
etal
.1948
:65%
first
-ye
ar;1
2%se
c-on
d-ye
ar;3
%fo
urth
-yea
r;20
%re
side
nts
ornu
rses
Cont
rolg
roup
com
pose
dof
stud
ents
who
calle
daf
ter
inte
r-ve
ntio
ngr
oups
wer
efil
led
14in
terv
entio
n;14
wai
t-lis
tcon
-tro
l
660
-to
90-m
inut
ese
ssio
nsov
er3
wee
ks.S
essi
ons,
coor
dina
ted
bycl
ini-
calp
sych
olog
ista
ndps
ycho
logi
sttra
in-
ees,
had
thre
epa
rts:d
idac
tic,d
is-
cuss
ion,
and
de-
scrip
tions
ofho
me-
wor
kpr
actic
e.
Disc
ussi
onof
stre
ss,
rela
xatio
ntra
inin
g,co
gniti
vem
odifi
ca-
tion
skill
s,tim
em
anag
emen
t,se
lfta
lk.
None
Stan
dard
ized
in-
vent
orie
sw
ithac
cept
ance
valid
-ity
and
relia
bilit
y;on
eno
n-st
an-
dard
inve
ntor
y
Know
ledg
eab
out
stre
ssim
prov
ed.
Nodi
ffere
nce
inst
anda
rdize
dsc
ales
;co
ntro
lgro
upw
ors-
ened
inJe
nkin
sHa
rdDr
ivin
gSc
ale.
Cont
inue
don
next
page
752A
CA
DE
MI
CM
ED
IC
IN
E,
VO
L.
75
,N
O.
7/
JU
LY
20
00
Table 1 (Continued)
No. ofParticipants Randomization
Type ofControl
Structure ofIntervention
Content andTechniques Follow-up
OutcomeMeasures Results
Part III: Remain-ing Studies
Klamen25 60 first-year medstudents
No No 3 weekly 2-hourstress-managementworkshops.
Social support andrelaxation training,communicationskills and burnoutprevention, discus-sion of stress andcoping.
None No standardizedmeasure; subjec-tive rating ofhelpfulness ofstress manage-ment
100% of studentsreported helpful-ness of course.
Kahn and Ad-dison13
7 residents No No 39 75-minute un-structured sessionsthroughout aca-demic year. Processgroup led by familyphysician and clini-cal psychologist.
Groups, discussedrole expectations,relationships withpeers and supervi-sors, coping withanxiety, and emo-tional issues.
None No standardizedinventory, stu-dents respondedto questionsabout copingand value of in-tervention
100% felt group wasvaluable; reporteddecreases in nega-tive coping and in-creases in positivecoping.
Brock and Stock34 381 family prac-tice residents.19% had Balintgroups, 11% hadhad seminars inthe past, and19% expressedinterest in start-ing them
Not applicable Not applicable Balint groups: 55%met weekly, 30%met bimonthly, re-mainder met lessoften. Majority metfor two years orlonger. Most had 5to 10 participants.All had leaders whowere either familypractice MDs, psy-chiatrists, or psy-chologists. Groupsincluded familypractice first-, sec-ond-, third-year res-idents or mixedgroups.
Focus of groupleader was on phy-sician–patient rela-tionship, feelingsgenerated in re-sponse to cases,role demands. Vari-ety of patient is-sues discussed, in-cluding depression,somatization, andloneliness. Leaderused discussion ofgroup dynamics,parallel process,genogram analysis,and didactics.
Not appli-cable
No standardizedmeasure
Highly endorsed:‘‘Provides supportfor residents’’;‘‘Helps resolve pro-fessional role con-flict’’; and ‘‘Deter-mines effect ofdoctor’s personalityon illness.’’
Johnson et al.1 15 first-year medstudents
No No Health care simula-tions of team roleswith mock patientdata, structured en-counter groups inwhich interpersonalprocesses werenoted and dis-cussed, and un-structured encoun-ter groups.
2-day encountergroups that usedsociometric analy-sis, time structureforms, interactionalanalysis, and self-appraisal.
None Participants self-rated pre/postintervention on30 items, includ-ing personal re-sponsibility, co-operation ontasks, communi-cation, problemsolving and deci-sion making, andpersonal growth
Significant improve-ment on all itemsfrom pre- to post-intervention. Meansand other data un-reported.
A C A D E M I C M E D I C I N E , V O L . 7 5 , N O . 7 / J U L Y 2 0 0 0 753
Fran
coet
al.35
150
first
-yea
rm
edst
uden
tsNo
NoIn
form
alsu
ppor
tgr
oups
(7st
uden
tsea
ch)
led
bym
em-
ber
ofde
an’s
staf
f.
Disc
ussi
onof
curr
ic-
ulum
,pro
fess
iona
lid
entit
y,an
dso
cio-
econ
omic
pres
-su
res.
None
Nost
anda
rdize
din
vent
ory;
stu-
dent
san
swer
edqu
estio
n:Sh
ould
prog
ram
beco
n-tin
ued?
80%
felt
the
pro-
gram
shou
ldbe
cont
inue
dth
roug
hth
efir
stye
arof
med
scho
ol.4
2%fe
ltpr
ogra
msh
ould
beco
ntin
ued
thro
ugh
four
thye
ar.
Reub
enet
al.27
Tota
lpro
gram
supp
orte
d25
0re
side
nts
from
vario
usdi
sci-
plin
es;5
4an
-sw
ered
ques
tion-
naire
NoNo
Com
preh
ensi
vesy
s-te
min
itiat
edaf
ter
resi
dent
’ssu
icid
e:(1
)m
ass
com
mun
i-ca
tion
(hos
pita
lne
wsl
ette
rs,g
rand
roun
ds,e
tc.)
vali-
datin
gst
ress
esof
inte
rnsh
ip;(
2)fa
c-ul
tysp
onso
rsy
stem
for
first
-yea
rre
si-
dent
s;(3
)in
divi
dual
coun
selin
gof
resi
-de
nts
byau
thor
s;(4
)ne
twor
kof
men
-ta
lhea
lthpr
ofes
-si
onal
sfo
rin
divi
d-ua
ltre
atm
ent;
and
(5)
wee
kly
supp
ort
mee
tings
.
Artic
lelo
oked
atsu
ppor
tgr
oup
mee
tings
,des
crib
edas
mor
efo
cuse
don
topi
csth
anem
o-tio
ns.C
onte
ntdi
c-ta
ted
byfa
culty
,re
side
nts,
and
oc-
casi
onal
gues
tsp
eake
rs.T
opic
sin
-cl
uded
:ang
erat
na-
ture
oftra
inin
gsy
s-te
m,a
ppro
pria
teem
erge
ncy
care
ofpa
tient
s,m
etho
dsof
com
mun
icat
ing
with
priv
ate
phys
i-ci
ans,
and
prop
os-
als
tore
duce
bur-
den
onon
-cal
lph
ysic
ians
.
None
Unde
scrib
ed,u
n-va
lidat
edqu
es-
tionn
aire
sent
toal
lres
iden
ts;
perc
enta
geof
re-
spon
dent
sto
thos
equ
erie
sno
tre
porte
d
75%
ofre
spon
dent
sfe
ltsy
stem
pro-
vide
dad
equa
teps
y-ch
olog
ical
supp
ort,
80%
had
atte
nded
atle
ast
one
supp
ort
mee
ting,
roug
hly
33%
had
atte
nded
5or
mor
e.1
re-
spon
dent
felt
grou
psno
the
lpfu
l.Of
inte
rns,
67%
had
atte
nded
atle
ast
1m
eetin
gw
ithfa
culty
spon
sor.
Wei
ner48
Inte
rns—
num
ber
not
repo
rted
NoNo
Grou
pm
etw
eekl
yfo
rfre
elu
nch,
led
bycl
inic
alps
ycho
lo-
gist
.
Soci
algr
oup.
None
Anon
ymou
s(n
otpa
ram
etric
)qu
estio
nnai
re
Parti
cipa
nts
en-
dors
edus
eful
ness
ofgr
oup.
Zieg
ler
etal
.49In
tern
s—nu
mbe
rno
tre
porte
dNo
NO36
wee
kly
1-ho
urst
ress
-dis
cuss
ion
grou
psfa
cilit
ated
byM
Ds.M
edia
nnu
m-
ber
ofpa
rtici
pant
sw
as5.
Addr
esse
dst
ress
ex-
perie
nce
due
tohi
ghex
pect
atio
ns,
lack
ofco
ntro
l,an
dde
pend
ence
/inde
-pe
nden
ceis
sues
.
None
Nost
anda
rdize
dm
easu
re;y
ear-
end
ques
tion-
naire
90%
enjo
yed
grou
pse
ssio
ns.5
5%fe
ltgr
oup
help
edth
emde
alw
ithst
ress
.
Cont
inue
don
next
page
754A
CA
DE
MI
CM
ED
IC
IN
E,
VO
L.
75
,N
O.
7/
JU
LY
20
00
Table 1 (Continued)
No. ofParticipants Randomization
Type ofControl
Structure ofIntervention
Content andTechniques Follow-up
OutcomeMeasures Results
Blitch et al.28 30 first-, second-,and third-yearfamily practiceresidents
Yes; stratified toequal numbersof each year ineach group
No 10 residents random-ized to each of 3groups.
Mandatory facilitatedinterpersonalgroups met for 8weekly sessionswith one feedbacksession. Sessionslasted between 1and 2.5 hours dur-ing regular dutytime.
Groups considered avaluable supple-ment to behavioralscience curriculum.
Strahilevitz et al.32 33 pediatrics resi-dents
No No Designed to addresspediatrics residents’feelings of isolation.3 groups met overlunch, facilitated bypediatricians andone psychiatrist.Groups scheduledto last 8 weeks buttwo continued be-yond 8 weeks.
Groups discussedvarious topics, in-cluding frustrationwith residency, pos-itive aspects oftraining, personalissues such as con-flicts between roledemands and pri-vate life, anxietyabout life after resi-dency, and feelingsthat contradict im-ages of profession-alism.
80% felt groupshelped them get toknow peers, realizeothers have similarexperiences, de-velop better work-ing relationships,and express emo-tions. All felt sup-port groups hadplace in training.75% attendancerate.
Webster and Ro-binowitz26
6 second-yearmed students
No No Elective course meet-ing 1 to 1.5 hoursfirst semester, and2 to 2.5 hours dur-ing remainder ofstudy (30 months).Two co-leaders.
4 general themes ofthe group: responseto training experi-ences, identity andcareer decisions,personal and lifecrisis, and genderstereotypes.
10-monthfollow-up
Yalom Inventoryand five otherrating scalesmeasuring gainsfrom group
Interns discussedwork stress andfeelings of depres-sion, anxiety, anger,and helplessness.
None No standardizedmeasure; formsasked whetherstudents valuedthe group
5 returned evalua-tions, all reportingvaluable experience.
A C A D E M I C M E D I C I N E , V O L . 7 5 , N O . 7 / J U L Y 2 0 0 0 755
Sosk
is18
42fir
st-
and
sec-
ond-
year
med
stud
ents
NoNo
One-
sem
este
rel
ec-
tive
cour
seen
title
d‘‘M
edia
tion
and
Heal
ing’
’led
bypr
o-fe
ssio
nalt
each
ers.
Read
ings
,lec
ture
s,de
mon
stra
tions
,an
dsu
perv
ised
prac
tice
info
urte
chni
ques
:sel
f-hy
pnos
is,W
este
rnre
ligio
usm
edita
tion,
yoga
,and
trans
cen-
dent
alm
edita
tion.
None
Nost
anda
rdize
dm
easu
re;s
tu-
dent
sas
ked
wha
tth
eym
ight
cont
inue
stud
y-in
gaf
ter
stud
yan
dw
hat
they
wou
ldre
com
-m
end
for
pa-
tient
s
40%
cons
ider
edco
ntin
uing
relig
ious
med
itatio
n;69
%,
yoga
;88%
,tra
n-sc
ende
ntal
med
ita-
tion.
79%
to88
%w
ould
reco
mm
end
tech
niqu
esfo
rpa
-tie
nts.
Gold
enan
dRo
sen31
Med
stud
ents
:3ye
ars
of4-
year
prog
ram
re-
porte
d:25
,30,
and
136
Parti
cipa
nts
volu
n-te
ered
for
grou
p;na
ture
ofas
sign
-m
ent
togr
oups
unre
porte
d
Yes,
first
year
had
13su
bjec
tsar
bi-
traril
yas
sign
edto
expe
rimen
tal
grou
pw
ith12
sele
cted
asco
n-tro
ls
Mos
tgr
oups
met
wee
kly
for
2ho
urs
orm
ore.
For
first
two
year
s,gr
oup
lead
ers
had
expe
ri-en
cein
smal
l-gro
updy
nam
ics.
Mos
tth
ird-y
ear
grou
ple
ader
sha
dno
train
ing
insm
all-
grou
ple
ader
ship
orps
ychi
atric
orps
y-ch
olog
ical
train
ing.
Grou
psdi
scus
sed
care
eris
sues
,au-
thor
ityis
sues
,pee
rre
latio
nshi
ps,p
rob-
lem
sin
rela
tion-
ship
s,em
otio
nal
supp
ort.
None
Essa
ysco
mpl
eted
bym
edic
alst
u-de
nts
Mos
tpr
ovid
edpo
si-
tive
feed
back
.Som
edi
slik
edth
eex
peri-
ence
.
Hilb
erm
anet
al.21
17fir
st-y
ear
and
1se
cond
-yea
rfe
mal
em
edst
u-de
nts
NoNo
Wee
kly
1-to
2-ho
urin
form
aldi
scus
sion
grou
psm
etfo
r1
year
,led
bytw
ofe
-m
ale
facu
ltyea
ch.
Insi
ght-o
rient
edsu
p-po
rtgr
oups
.Fre
-qu
ently
focu
sed
onin
terp
erso
nali
ssue
sbe
twee
ngr
oup
mem
bers
.Oth
erfo
ciin
clud
edco
n-fli
cts
betw
een
fe-
mal
ean
dm
edic
alid
entit
ies,
isol
atio
n,pe
rfec
tioni
sm.
None
Stud
ents
com
-pl
eted
goal
ssh
eet
befo
rejo
inin
ggr
oups
;at
end
ofac
a-de
mic
year
,an-
swer
ed12
stat
e-m
ents
on4-
poin
tsc
ale
incl
udin
gim
porta
nce
and
help
fuln
ess
ofgr
oups
Parti
cipa
nts
satis
fied
with
grou
ps,r
e-po
rted
getti
ngcl
oser
tocl
ass-
mat
esan
dun
der-
stan
ding
prob
lem
sof
prof
essi
onal
wom
en.
Dasd
efet
al.20
47m
edst
uden
ts,
mos
tlyfo
urth
-ye
ar
NoNo
Betw
een
4an
d6
vol-
unta
ryfa
cilit
ated
unst
ruct
ured
grou
pse
ssio
nsla
stin
gbe
-tw
een
1.5
and
2.5
hour
s.
Unst
ruct
ured
grou
pse
ssio
nsal
low
edem
otio
nale
xpre
s-si
onan
din
terp
er-
sona
lexp
lora
tion.
Mai
led
eval
uatio
non
em
onth
befo
reen
dof
year
.
Ques
tionn
aire
:M
odifi
edYa
lom
’sQ-
sort
Impr
oved
sens
itivi
ty,
redu
ced
isol
atio
n,in
crea
sed
capa
city
for
intim
acy.
Cadd
enet
al.52
42vo
lunt
eer
first
-ye
arm
edst
u-de
nts
NoNo
Grou
pse
min
ars
met
wee
kly
for
90m
inut
es,m
etfo
r1
trim
este
r.
Used
disc
ussi
ons
and
role
play
ing.
NoNo
stan
dard
ized
mea
sure
65%
foun
dit
inte
r-es
ting
and
help
ful,
21%
gene
rally
help
-fu
l,15
%w
aste
oftim
e.No
diffe
renc
ein
acad
emic
per-
form
ance
sbe
twee
npa
rtici
pant
san
dno
n-pa
rtici
pant
s.
756 A C A D E M I C M E D I C I N E , V O L . 7 5 , N O . 7 / J U L Y 2 0 0 0
ond-, and third-year family practice res-idents, would be included in eachgroup. One study19 described a proce-dure that actively violated randomiza-tion: students were recruited on a first-come–first-served basis, with those whocalled earlier being assigned to the ex-perimental group and those who calledlater (who may have been less orga-nized), to the control group. The rest ofthe studies did not describe how partic-ipants were assigned to groups.
Control Groups
With eight exceptions,15–17,19,22–24,29 thestudies reported did not use controlgroups. Most studies used pre/post de-signs, comparing baseline and post-in-tervention ratings. Unfortunately, thereis ample evidence that stress levelsfluctuate considerably during training.Medical students report experiencingconsiderably more stress during exami-nation periods, and interns and resi-dents report varying levels of stress de-pending on assigned rotations, on-callschedules, or time off. Given these fac-tors, it is likely that pre/post designs arevulnerable to these fluctuations. An ex-ample illustrates this problem. Shapiroand colleagues17 reported no change instate anxiety levels (a measure of cur-rent anxiety, as opposed to trait anxiety,which measures characteristics or gen-eral anxiety) for the experimental groupfrom before to after the intervention.However, significant differences in stateanxiety were found between groups (ex-perimental and control) after the inter-vention. The post-intervention assess-ment coincided with the examinationperiod, suggesting that the stress-man-agement intervention had buffered stu-dents against the negative effects of ex-amination stress. If the study had notincluded a control group, the interven-tion would have erroneously appearedineffective.
In some cases not using controlgroups is understandable. Researchershave to balance the value of informa-
tion gleaned from control groupsagainst the possible negative conse-quences for medical trainees enrolled inwait-list controls, inert control groups,or comparison groups suspected to beless effective than the experimentalgroups. Of those who did use controlgroups, five used wait-list controlgroups,15–17,19,29 two compared interven-tions,22,23 and one had a no-treatmentcontrol group.24
Intervention
Structure of the intervention. Themajority of the programs used a groupstructure where trainees met with peersor with leaders. Interventions varied inthe amounts of time required of partic-ipants, from two consecutive intensivedays30 to weekly hour-long meetingsthroughout the academic year.13 Partic-ipants tended to meet from one to twohours.
The optimal duration for interven-tions, both in frequency and duration ofmeetings, is unknown. No study syste-matically examined what length or in-tensity of intervention was most effec-tive. Considering the demands alreadymade on trainees’ time, many of theprograms required only modest addi-tional time commitments. However,this also meant that only a few pro-grams provided long-term support. Con-trolled empirical research needs to de-termine what length of intervention ismost beneficial, considering the train-ees’ rigorous time commitments. Para-doxically, stress-management programsmay initially elicit greater levels ofstress.22 Therefore, a cost–benefit anal-ysis should be performed to determinewhat intensity is most effective bothshort- and long-term.
The facilitators of the interventionsvaried in terms of training, background,and experience level. In selecting groupleaders, one should consider a few is-sues. On the one hand, group leaderswith training experiences similar tothose of the participants will be familiar
with their specific stresses and strug-gles.32 On the other hand, effectivegroup facilitation is not a simple task33
and should be conducted by those withprofessional training, such as socialworkers, psychologists, and psychia-trists.34 Another problem with using fa-cilitators with similar experiences isthat many have dual relationships withthe participants. For example, in somecases the leaders of groups had gradingresponsibility for the participants,35,36 aclear violation of basic support-grouptheory. Further, some stress-manage-ment interventions are based on spe-cialized training and the facilitator mustbe an expert in order to effectivelyteach the stress-management skills (e.g.,hypnosis or meditation). As a result, re-searchers frequently had to choose be-tween selecting facilitators who hadtraining similar to that of the partici-pants, those who had training in groupleadership, or those who had specializedtraining.
Content of the intervention. No‘‘gold standard’’ exists for the content ofstress-reduction programs for medicaltrainees. As in stress-management pro-grams offered in other workplaces,37
content varied considerably. Our reviewrevealed that a wide variety of interven-tions were included under the umbrellaof stress reduction; e.g., directed andnon-directed support groups, relaxationtraining (including meditation and hyp-nosis), time-management and copingskills, mindfulness-based stress reduc-tion, and mentoring programs. Thegroups also varied in the degrees towhich they encouraged emotional ex-pression, incorporated personal as wellas professional issues, and focused ontechnique versus discussion.
Outcome Measures
The most common outcome measureused in the studies was the trainees’evaluations of the stress-managementprograms. The trainees almost univer-sally found the programs helpful and in
A C A D E M I C M E D I C I N E , V O L . 7 5 , N O . 7 / J U L Y 2 0 0 0 757
many cases urged researchers to inte-grate the programs into the curriculum.Most medical schools rely heavily onstudents’ evaluations when makingteaching assignments and rotation se-lections.
Although students’ evaluations arevital as an outcome measure, more ob-jective measures (e.g., behavioral andphysiologic measures) are needed toprovide more comprehensive assess-ment of outcomes. Unfortunately, sys-tematic evaluation of other outcomeswas scarce. Only seven studies usedstandardized measures. Most researchersrelied on non-standardized inventoriesthey had constructed themselves. Theproblems with non-standardized mea-sures are well known to behavioral sci-entists and are not discussed here.
Future researchers might focus on anumber of outcomes that have yet to beexamined. For example, what is the in-fluence of stress-management programson physician–patient communication?How does stress management for phy-sician trainees influence patient out-comes? Do programs with stress-man-agement interventions have less traineedropout?
We believe one unintended and un-fortunate side effect of medical trainingis that it produces physicians who be-lieve that self-denial is valuable andnecessary and that living under stress isnormal. Until physicians recognize thesignificant health impact stress has onthem and the importance of modelinghealthy behaviors (including relativestress-free living) for their patients, it isunlikely that the skills learned in astress-management program will be in-corporated into their professional andpersonal lives.
Stress Assessment
One reason that most of the studies didnot use validated measures is that thereis no ‘‘gold standard’’ for assessment ofstress management. Researchers study-ing stress tend to rely on checklists that
ask respondents to report the number ofsymptoms they are experiencing or theseverity of events they have experi-enced. The most widely employed in-clude the Unpleasant Events Schedule,38
the Hassles Scale,39 the Assessment ofDaily Experiences Questionnaire,40 theInventory of Small Life Events,41 andthe Daily Stress Inventory.42 However,the checklist approach has many limi-tations. Clearly, all self-report instru-ments are open to response biases,social desirability, and unconscious (re-pressive) coping.43 Even more problem-atic, none of these instruments was de-signed to apply to medical trainees, whoexperience not only predictable andgeneral pressures, such as interpersonalstressors, economic problems, fatigue,and confidence deficits,44 but also stress-ors specific to medicine, such as 24-hourschedules and issues of life and death.The particular demands of medicaltraining merit measurement by a toolsensitive and specific to this population.One direction may be to develop amedical education stress inventory.
Although self-report measures ofstress are important, examination ofphysiologic measures of stress shouldsupplement them to validate the effec-tiveness of the stress-management tech-niques. According to Cambell andFiske,45 multi-trait, multi-method as-sessment is the most sophisticated andaccurate research design. The followingare common physiologic measures citedin the literature46,47: electroencephala-gram (EEG), electrocardiogram (EKG),blood pressure (baseline and return tobaseline), cortisol levels, measures ofimmune functioning, finger-pulse tran-sit time (FPTT), ear-pulse transit time(EPTT) (see Cacioppo and Tassinary47
for a more complete description of thesemeasures).
One of the more common criticismsof these forms of assessment is that theymay not generalize outside of the labo-ratory. This important question deservesattention, and measures have been orare being developed (e.g., ambulatory
blood pressure monitor) to address it.Other potential limitations includecost, confounding variables, and time.Despite possible concerns, physiologicmeasures of stress give another relevantpiece of the picture by providing an ob-jective comparison with trainees’ sub-jective self-reports. This is especiallyimportant in light of past studies of re-pression in which physiologic arousalwas objectively measured even thoughparticipants did not self-report arousal.43
Further, these physiologic measures areoften markers of future physiologic pa-thology.
Finally, although the negative con-sequences of stress include decreased at-tention and concentration, poor deci-sion-making ability, alcohol and drugabuse, depression and anxiety, relation-ship difficulties, and even suicide, fewof these variables have been assessed asoutcome measures of stress-manage-ment programs for medical trainees. Fu-ture research must include outcomemeasures that will determine whetherthe stress-management program is ableto buffer against these potential nega-tive consequences of stress.
CONCLUSIONS AND IMPLICATIONS
FOR FUTURE RESEARCH
The purpose of this article is to reviewthe literature on stress management andmedical education. Of the 24 studies re-viewed, the vast majority supported theeffectiveness of interventions designedto reduce the stress of medical ed-ucation and training. In almost allcases (where measured) the participantsfound the programs useful. Unfortu-nately, a lack of careful control in moststudies, few validated outcome mea-sures, and heterogeneous interventionsmake drawing firm conclusions beyondthis premature.
Despite continued calls for researchon stress-management programs in med-ical education, there have been fewcarefully conducted trials. In our search,we found over 600 articles discussing
758 A C A D E M I C M E D I C I N E , V O L . 7 5 , N O . 7 / J U L Y 2 0 0 0
the importance of addressing the stressof medical training. Common themesdescribed by authors of these articlessuggest that the reigning paradigm inmedical education emphasizes perfor-mance under stress, competition, andself-denial. Unfortunately, only 24 ofthese articles reported empirically as-sessed intervention programs, and onlysix of these15–17,22–24 used rigorous sci-entific method.
This discrepancy illustrates that thereis much work to be done. Althoughsome may feel that the obvious conclu-sion is to implement stress-managementprograms immediately without futureresearch, there are still many unan-swered questions. It is unclear whichtypes of stress-management programsare most effective (e.g., meditation ver-sus support group). While it is encour-aging that researchers are exploringmany approaches, it is difficult to makecomparisons among diverse treatments.Interventions have varied in treatmentmodality (e.g., individual versus group),in format (e.g., structured versus un-structured), and in therapeutic tech-niques (e.g., hypnosis versus medita-tion). Further research is needed todisentangle research designs and ex-plore which components of a complexarray of interventions are most effec-tive.
It is also unclear what duration andfrequency are necessary to produce re-sults. Precise comparison of interven-tions of differing durations and frequen-cies must be made to determine themost efficient and effective stress-man-agement programs for medical trainees.Further, although a variety of interven-tions have proven effective, sensitivityto medical trainees in general, and in-dividual differences in particular, is nec-essary. Future research must accuratelydetermine which interventions workbest for whom by assessing moderatorvariables.
Based on our review, the followingconsiderations should be incorporatedinto future research: (1) rigorous design,
including randomization and control(comparison) groups; (2) precise studyof varying durations and frequencies ofinterventions (e.g., two-day interven-tion versus eight-week intervention);(3) measurement of moderator variablesto determine which interventions workbest for whom; (4) specificity of out-come measures; and (5) follow-up as-sessment, including effectiveness of fu-ture patient care.
This review has described the wide-spread interest in stress-managementprograms, the promising start made bythose already implemented, and thegreat unexplored territory that must becharted if these interventions are to ef-ficiently and effectively succeed in thetwin goals of benefiting physicians andtheir patients and establishing a soundscientific base for future research.
The authors acknowledge and thank all of thepioneering researchers who have contributed tothe field of stress management in medical educa-tion. They also thank Benedict Freedman for hisinsightful editorial comments and Heather Ristfor her help in creating Table 1.
REFERENCES
1. Johnson N, Michels P, Thomas J. Screeningtests identify the prevalence of alcohol useamong freshman medical students and amongstudents’ family of origin. J South CarolinaMed Assoc. 1990;86:13–4.
2. Gallegos K, Bettinardi-Angres K, Talbott G.The effect of physician impairment on thefamily. Maryland Med J. 1990;39:1001–7.
3. Pitts FN, Winokur G, Stewart MA. Psychi-atric syndromes, anxiety symptoms and re-sponses to stress in medical students. Am JPsychiatry. 1961;118:333–40.
4. Salt P, Nadelson C, Notman M. Depressionand anxiety among medical students. Paperpresented at APA Annual Meeting, Los An-geles, CA, 1984.
8. Askenasy J, Lewin I. The impact of missilewarfare on self-reported sleep quality. Sleep.1996;19:47–51.
9. Lehner P, Seyed-Solorforough M, O’ConnorM, Sak S, Mullin T. Cognitive biases andtime stress in team decision making. IEEETrans Systems, Man & Cybernetics. 1997;27:698–703.
10. Klein G. The effect of acute stressors on de-cision making. In: Driskell J, Salas E (eds).Stress and Human Performance. Mahwah,NJ: Lawrence Erlbaum, 1996:48–88.
11. Pastore FR, Gambert SR, Plutchik A, Plut-chik R. Empathy training for medical stu-dents. Unpublished manuscript, New YorkMedical College, 1995.
12. Kelly A, Marks F, Westhoff C, Rosen M. Theeffect of the New York State restrictions onresident work hours. Obstet Gynecol. 1991;78:468–73.
13. Kahn NB, Addison RB. Support services forfamily practice residents. J Fam Prac. 1992;34:78–180.
14. Butterfield PS. The stress of residency: a re-view of the literature. Arch Intern Med.1988;148:1428–35.
15. Whitehouse WG, Dinges DF, Orne EC, et al.Psychosocial and immune effects of self-hyp-nosis training for stress management throughthe first semester of medical school. Psycho-som Med. 1996;58:249–63.
16. Kiecolt-Glaser J, Glaser R, Strain E, et al.Modulation of cellular immunity in medicalstudents. J Behav Med. 1986;9:5–21.
17. Shapiro SL, Schwartz GE, Bonner G. Effectsof mindfulness-based stress reduction on med-ical and premedical students. J Behav Med.1998;21:581–99.
18. Soskis DA. Teaching meditation to medicalstudents. J Religion and Health. 1978;17:136–43.
19. Kelly JA, Bradlyn AS, Dubbert PM, St.Lawrence JS. Stress management training inmedical school. J Med Educ. 1982;57:91–9.
20. Dashef SS, Espey WM, Lazarus JA. Time-lim-ited sensitivity groups for medical students.Am J Psychiatry. 1974;131:287–92.
21. Hilberman E, Konanc J, Perez-Reyes M, Hun-ter R, Scagnelli J, Sanders S. Support groupfor women in medical school: a first year pro-gram. J Med Educ. 1975;50:867–75.
22. Palan BM, Chandwani S. Coping with ex-amination stress through hypnosis: an experi-mental study. Am J Clin Hypnosis. 1989;31:173–80.
23. Nathan RG, Nixon FE, Robinson LA, Bairns-father L, Allen JH, Hack M. Effects of a stressmanagement course on grades and health offirst-year students. J Med Educ. 1987;62:514–7.
24. Holtzworth-Munroe A, Munroe MS, Smith
A C A D E M I C M E D I C I N E , V O L . 7 5 , N O . 7 / J U L Y 2 0 0 0 759
RE. Effects of a stress-management trainingprogram on first and second year medical stu-dents. J Med Educ. 1985;60:418–9.
25. Klamen DL. The stress management work-shop for medical students. Acad Psychiatry.1997;21:42–7.
27. Reuben DB, Novack DH, Wachtel TJ, Wart-man SA. A comprehensive support system forreducing house staff distress. Psychosomatics.1984;25:815–20.
28. Blitch JW, Bowman DO, Adams CE, Jett CR,Campbell DC. Promoting the ‘‘whole physi-cian’s’’ well-being: the experience of a supportgroup for family practice residents. Fam PracRes J. 1983;2:231–8.
29. Golden JS, Rosen AC. A group dynamicscourse for medical students. Int J Group Psy-chother. 1975;25:305–14.
31. Kabat-Zinn J, Chapman-Waldrop A. Com-pliance with an outpatient stress reductionprogram. J Behav Med. 1988;11:333–52.
32. Strahilevitz A, Yunker R, Picanick AM,Smith L, Richardson J. Initiating supportgroups for pediatric house officers. Clin Pe-diatr. 1982;21:529–31.
33. Yalom I. Theory and Practice of Group Psy-chotherapy. New York: Basic Books, 1985.
34. Brock CD, Stock RD. A survey of Balintgroup activities in U.S. family practice resi-dency programs. Fam Med. 1990;22:33–7.
35. Franco KS, Tamburrino MB, Carroll BT, So-mani A, Wagner SM. Reducing the stress ofa medical education: two approaches. OhioMed. 1987;October:691–2.
36. Matthews D, Classen D, Willms J, Cotton J.A program to help interns cope with stressesin an internal medicine residency. J MedEduc. 1988;63:539–47.
37. Pelletier KR, Lutz R. Healthy people—healthy business: a critical review of stressmanagement programs in the workplace. AmJ Health Promotion. 1988;winter:5–12, 19.
38. Lewinsohn P, Amenson C. Some relations be-tween pleasant and unpleasant mood-relatedevents and depression. J Abnorm Psychol.1978;87:644–54.
39. Kanner AD, Coyne JC, Schaefer C, LazarusRS. Comparison of two modes of stress man-agement: daily hassles and uplifts versus ma-jor life events. J Behav Med. 1981.
40. Stone A, Neale J. Development of a meth-odology for assessing daily experiences. In:Baum A, Singer J (eds). Advances in Envi-ronmental Psychology: Environment andHealth. Hillsdale, NJ: Lawrence Erlbaum,1982:49–83.
41. Zautra A, Guarnaccia C. Measuring smallevents. Am J Commun Psychol. 1986;14:629–55.
42. Brantley PJ, Waggoner CD, Jones GN, Rap-paport NB. A daily stress inventory: devel-opment, reliability, and validity. J BehavMed. 1987;10:61–74.
43. Schwartz G. Psychobiology of repression and
health: a systems approach. In: Je S (ed). Re-pression and Dissociation: Implications forPersonality Theory, Psychopathology andHealth. Chicago, IL: University of ChicagoPress, 1990:337–87.
44. Rudner H. Stress and Coping Mechanisms ina Group of Family Practice Residents. J MedEduc. 1985;60:565–6.
45. Campbell EG, Louis KS, Blumenthal D.Looking a gift horse in the mouth: corporategifts supporting life sciences research. JAMA.1998;279:995–9.
46. Tyson P. Task-related stress and EEG alphabiofeedback. Biofeedback & Self-Regulation.1987;12:105–19.
47. Liang S, Jemerin JM, Tschann JM, Wara DW,Boyce W. Life events, frontal electroenceph-alogram laterality, and functional immunestatus after acute psychological stressors inadolescents. Psychosomat Med. 1997;59:178–86.
48. Weiner PS. A social–discussion group forfirst-year residents. J Med Educ. 1984;59:137–9.
49. Ziegler JL, Kanas N, Strull WM, Bennet N.A stress discussion group for medical interns.J Med Educ. 1984;59:205–7.
50. Siegel B, Donnelloy JC. Enriching personaland professional development: the experienceof a support group for interns. J Med Educ.1978;53:908–14.
51. Cadden JJ, Flach FF, Blakeslee S, Charlton RJr. Growth in medical students through groupprocess. Am J Psychiatry. 1969;126:862–8.