41
Stroke in the ICU Dr. Mohammad Aljawadi PharmD, Msc, PhD PHCL 478 Clinical Pharmacy Department College of Pharmacy King Saud University APRIL 2015
| Date post: | 22-Dec-2015 |
| Category: |
Documents |
| Upload: | clement-bishop |
| View: | 231 times |
| Download: | 3 times |

Stroke in the ICUDr. Mohammad Aljawadi PharmD, Msc, PhD
PHCL 478Clinical Pharmacy Department
College of Pharmacy King Saud University
APRIL 2015

2
Introduction
One of the top ten diseases that leads to death worldwide1
Can be classified:Acute ischemic stroke (85%)Acute hemorrhagic stroke (15%)
Around 15%-20% ends up treated in the ICU
Transient ischemic attack: Abrupt decrease in cerebral blood flow that does not cause permanent infarction.
1. Lopez AD, Mathers CD, Ezzati M et al (2006) Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet 367:1747–1757. doi: 10.1016/s0140-6736(06)68770-9

3
Definition Abrupt onset of persistent neurologic symptoms caused by inadequate blood flow to a
particular area of the brain or by hemorrhage into the brain, which compresses brain tissue and secondarily compromises perfusion

4
PathophysiologyIschemia due to different reasons will lead to the
creation of two areas: Ischemic core
Penumbral region

5
PathophysiologyThe ischemic core:
Blood flow is too low to maintain electric activity
Multiple events happening simultaneously including: Energy failure
Disruption of ion homeostasis
Glutamate release
Calcium channel dysfunction
Free radical release
Mitochondrial dysfunction
Membrane disruption
Activation of inflammatory cascades
Necrosis and apoptosis
Associated with irreversible damage of neurons
6
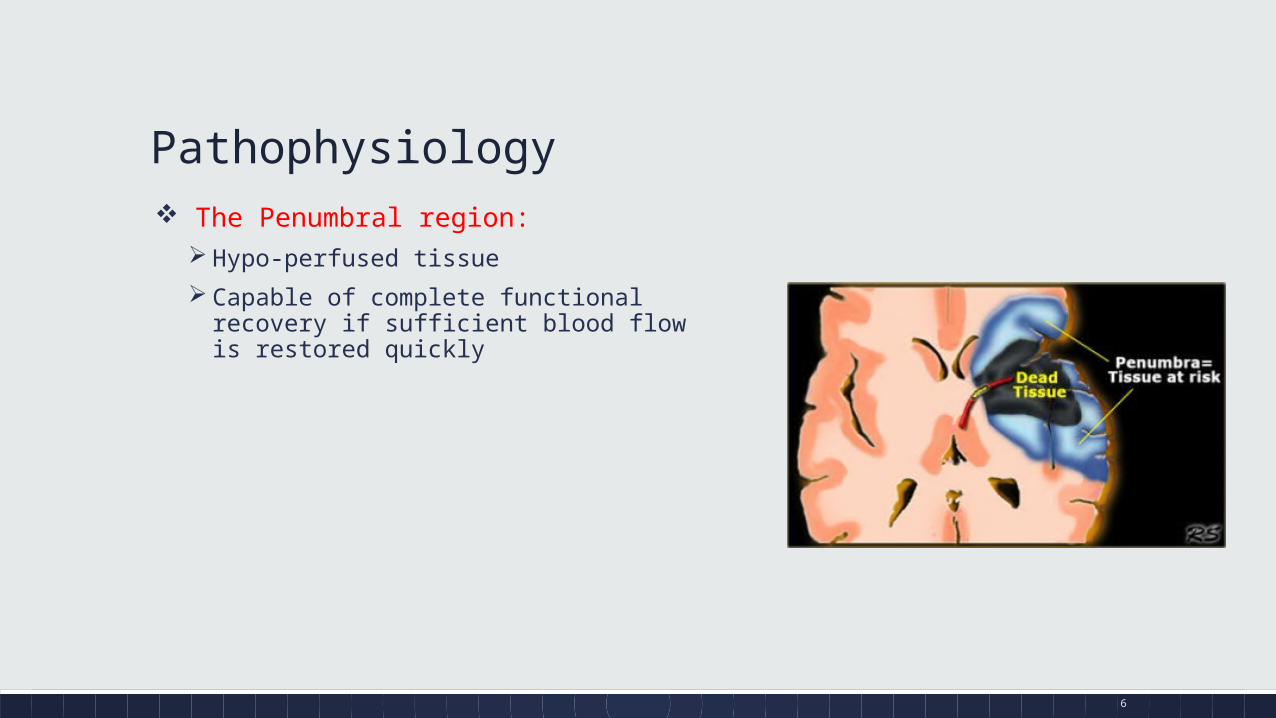
Pathophysiology The Penumbral region:
Hypo-perfused tissue
Capable of complete functional recovery if sufficient blood flow is restored quickly
7
Matching GameWhich one is associated with what? Explain
DVT
Atrial Fibrillation
Stroke
Pulmonary Embolism
You can go in any direction

8
Etiologies of acute ischemic stroke (AIS)Cardio-emobolic mainly due to atrial fibrillation (29%)
Atherosclerosis of cervical or intracranial vessels (16%)
Lacunar disease (16%)
Other: migraine, malignancy, and hypercoagulable states (3%)
Unknown (46%) mostly due to undiagnosed paroxysmal atrial fibrillation
9
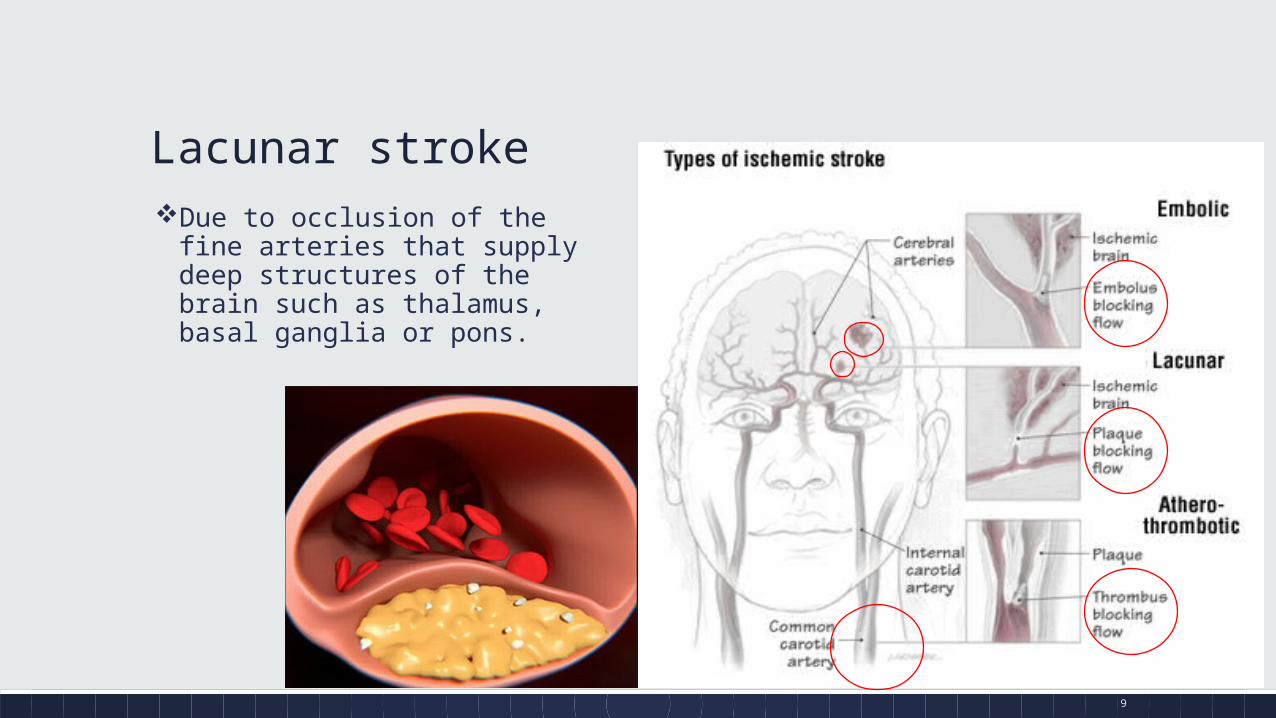
Lacunar strokeDue to occlusion of the fine arteries
that supply deep structures of the brain such as thalamus, basal ganglia or pons.
10
NIH Stroke Scale (FYI) http://www.ninds.nih.gov/doctors/nih_stroke_scale.pdf

11
The Oxford Stroke classification system (FYI)
The classification predicts the extent of the stroke, region affected, underlying etiology, and prognosis.
12
Signs and symptoms (from the patient or his relative)

13
Other S&S:

14
Inside the ICU: ICH=intracerebral hemorrhage
SAH= Subarachnoid hemorrhage

15
Therapy and Treatment recommendations:
1. Aspirin
2. Reperfusion Therapy
3. Stroke Unit
4. Decompressive craniectomy
Supporting Evidence of their benefit
16
1) Aspirin
Aspirin 325 mg within 24-48 hours of stroke onset is associated with prevention of recurrent events
Clopidogrel or dipyridamole: these data do not provide solid evidence about the utility of these antiplatelet agents in the management of patients with acute ischemic stroke.

17
2) Reperfusion Therapy
Reperfusion Therapy
Intravenous thrombolysis
Endovascular therapy
Purpose: To restore impaired blood flow to the ischemic penumbra before irreversible neuronal death occurs.
18
2) Reperfusion Therapy:
Thrombolytics:Intravenous Tissue plasminogen activator (rt-PA):
Alteplase:▪ Should be given within the 4.5 hours of stroke onset
▪ First, rule out hemorrhagic stroke before administration
▪ 3-month favorable outcomes were:
▪ 2·55 (95% CI 1·44–4·52) for 0–90 min
▪ 1·64 (1·12–2·40) for 91–180 min
▪ 1·34 (1·06–1·68) for 181–270 min
▪ 1·22 (0·92–1·61) for 271–360 min in favor of the alteplase group.
19
2) Reperfusion Therapy
Alteplase dosing:0.9 mg/kg (maximum total dose: 90 mg)
Patients ≤100 kg: Load with 0.09 mg/kg (10% of 0.9 mg/kg dose) as an IV bolus over 1 minute, followed by 0.81 mg/kg (90% of 0.9 mg/kg dose) as a continuous infusion over 60 minutes.
Patients >100 kg: Load with 9 mg (10% of 90 mg) as an IV bolus over 1 minute, followed by 81 mg (90% of 90 mg) as a continuous infusion over 60 minutes.
Initiation of anticoagulants (eg, heparin) or antiplatelet agents (eg, aspirin) within 24 hours after starting alteplase is not recommended

20
2) Reperfusion TherapyAlteplase contraindications:
Risk factors for systemic bleeding: Systemic anticoagulation, recent major surgery, recent gastrointestinal or urinary tract hemorrhage,
prior arterial puncture at a non-compressible site within 7 days or evidence of a coagulopathy
Evidence of intracerebral or subarachnoid hemorrhage
BP is elevated (systolic blood pressure [SBP] > 185 mm Hg or diastolic blood pressure [DBP] > 110 mm Hg), as elevated blood pressure can increase the risk of hemorrhagic transformation
Serum glucose is < 50 or > 400 mg/dL as these conditions can cause focal neurologic signs that mimic stroke

21
2) Reperfusion Therapy:Endovascular therapy:
Includes intra-arterial thrombolysis, mechanical embolectomy, and angioplasty/stenting Alternatives for IV rt-PA or patients who fail to improve after rt-PA
Intra-arterial thrombolysis within 6 hours of symptoms onset
Thrombectomy within 8 hours of symptoms onset
No difference between endovascular therapy (alone or with IV rt-PA) and IV rt-PA alone
Following reperfusion: Cranial imaging within 24 hours of reperfusion to detect hemorrhagic transformation
22
Hemorrhagic transformation
Bleeding due to rt-PA useStop rt-PAuse of cryoprecipitate (source of fibrinogen), fresh frozen
plasma, and recombinant factor VII is not supported by robust evidence in this setting.

23
2) Acute Stroke Unit:
Benefit of acute stroke unit1:Improved quality of careFacilitated patient access to thrombolysis and specialized stroke careTimely evaluationImproved early survival across age groupsMore cost-effective than care on other hospital wards/teamsReduced incidence of post-stroke complications, such as urinary tract
infections, pneumonia, and death.
1: http://www.strokeforum.com/acute-stroke-treatment/stroke-units.html

24
2) Acute Stroke Unit:Characteristics of stroke unit:
Care provision by a multidisciplinary team with competencies in the management of stroke and its systemic complications
Coordinated multidisciplinary rehabilitation
Meetings between multidisciplinary team members
Regular educational and training programs
25
2) Acute Stroke Unit:
Team:Neurologists
Nurses
Pharmacists
Neuro-surgeons
Physiotherapists
Occupational therapists
Speech therapists
Social workers
26
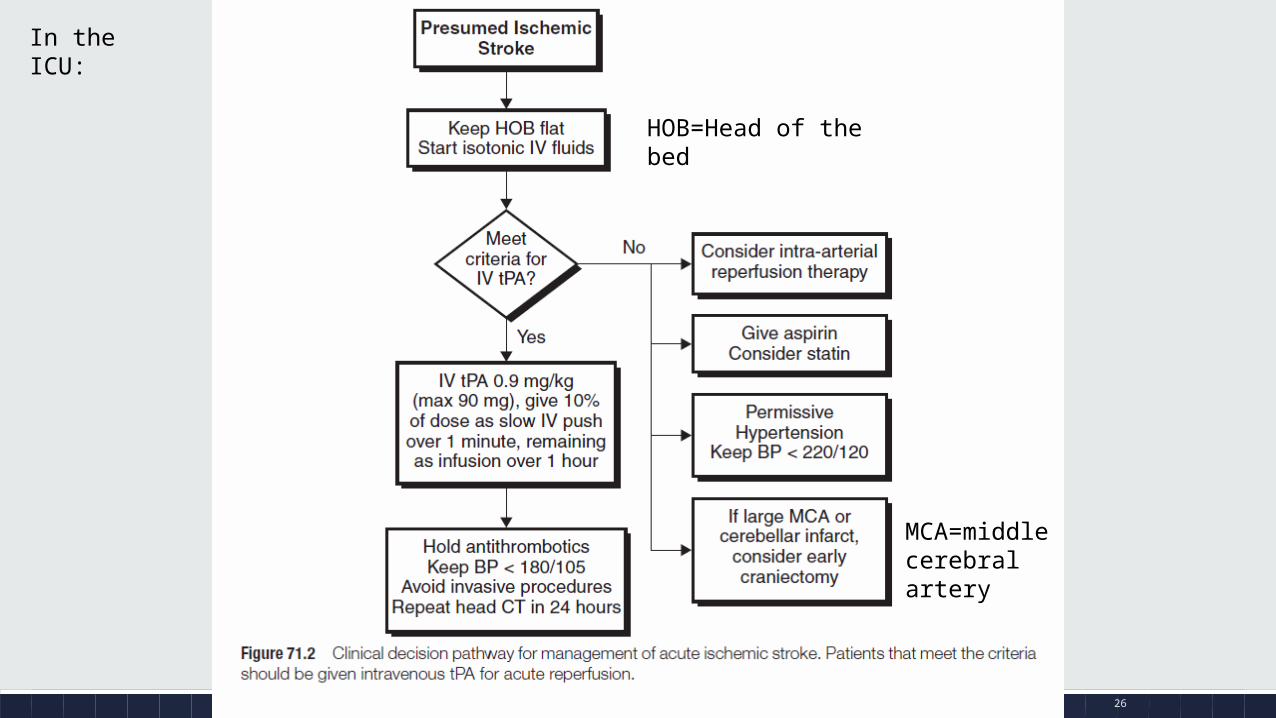
MCA=middle cerebral artery
HOB=Head of the bed
In the ICU:

27
Intensive care management of acute ischemic stroke
▪ Purpose: ▪ Monitoring and optimization
of systemic physiological homeostasis
▪ Monitoring and management of intracranial complications
▪ Includes:▪ Oxygenation
▪ Hemodynamic and fluid management
▪ Myocardial complications
▪ Glycemic control
▪ Fever
▪ Anticoagulation, antiplatelet therapy and thromboprophylaxis
▪ Neuromonitoring
▪ Cerebral edema and hemorrhage
▪ Seizures
▪ End-of-life care

28
Indications for admission after AIS
Universal criteria are:• Decreased conscious level • Need for mechanical ventilation• Intensive hemodynamic management• Invasive neurological and systemic monitoring

29
Oxygenation Continuous monitoring of oxygenation with pulse oximetry for all AIS patients on the
ICU.
Oxygen supplementation should be reserved for those with SpO2 <94 %.
Continuous monitoring of mechanical ventilation with regular arterial blood gas analysis.
Maintain normocapnea—target PaCO2 35–45 mmHg
All patients should undergo a formal swallow assessment

30
Hemodynamics and fluid managementRegular noninvasive BP monitoring in all AIS patients on the ICU
There are no data to guide a specific BP target during the ICU management of AIS
BP lowering is not indicated in those not undergoing thrombolysis except:
220/120 mmHg
In the presence severe cardiac failure, aortic dissection or hypertensive encephalopathy
BP lowering should be cautious, i.e.,15 % in the first 24 h in those not receiving thrombolysis.
BP should be lowered 185/110 mmHg before and for at least 24 h after thrombolysis.

31
Hemodynamics and fluid management Intravenous labetalol and nicardipine are reasonable first-line agents to lower BP.
Labetalol 10 to 20 mg over 1 to 2 minutes
Nicardipine :titrate by 2.5 mg/hour at 5- to 15-minute intervals (maximum dose: 15 mg/hour).
Sublingual nifedipine should be avoided as it can abruptly and inconsistently decrease BP.
If hypotension occurs: Fluid resuscitation
NE if unresponsive to IV fluids

32
Myocardial complications post-AIS:
Include:Dysrhythmias are present in 57% of patients
Elevated cardiac troponins in 17.5%
Left ventricular dysfunction in 12%
Monitoring: ECG, cardiac tropnins

33
Hyperglycemia:Hyperglycemia occurs in more than 40 % of AIS patients
Independently associated with increased mortality and morbidity at 90 days
Key recommendations: Regular blood glucose monitoring is essential.
Although tight glycemic control (72–135 mg/dl) has not been shown to result in deleterious outcomes, there is no evidence of clinical benefit in this population.
Treatment with continuous insulin infusion to maintain serum glucose between 140 and 180 mg/dl (8.0–10.0 mmol/l) is preferred on the ICU.
34
FeverOccurs in almost 50% of patients after AIS
Independently associated with poor outcome
Key recommendations: Avoid pyrexia (T[37.5] Co).
Investigate for, and treat, infectious causes of fever.
Regular paracetamol (acetaminophen) therapy as a first line therapy in those with temperatures > 37.5 Co, the dose administered being dependent on local guidance.
Second-line therapy: IV metamizole, rapid infusion of cold saline (4 Co), and the use of automatic cooling systems.
Ibuprofen does not appear to reliably reduce body temperature after stroke

35
Anticoagulation, antiplatelet therapy and thromboprophylaxis
Use of any anticoagulant is contraindicated in the first 24 h following thrombolysis, but should be considered after this.
Avoid AC in patients with moderate to severe stroke to avoid the development of hemorrhagic stroke
Prophylactic-dose subcutaneous LMWH to prevent DVT and mechanical intermittent calf compression.
36
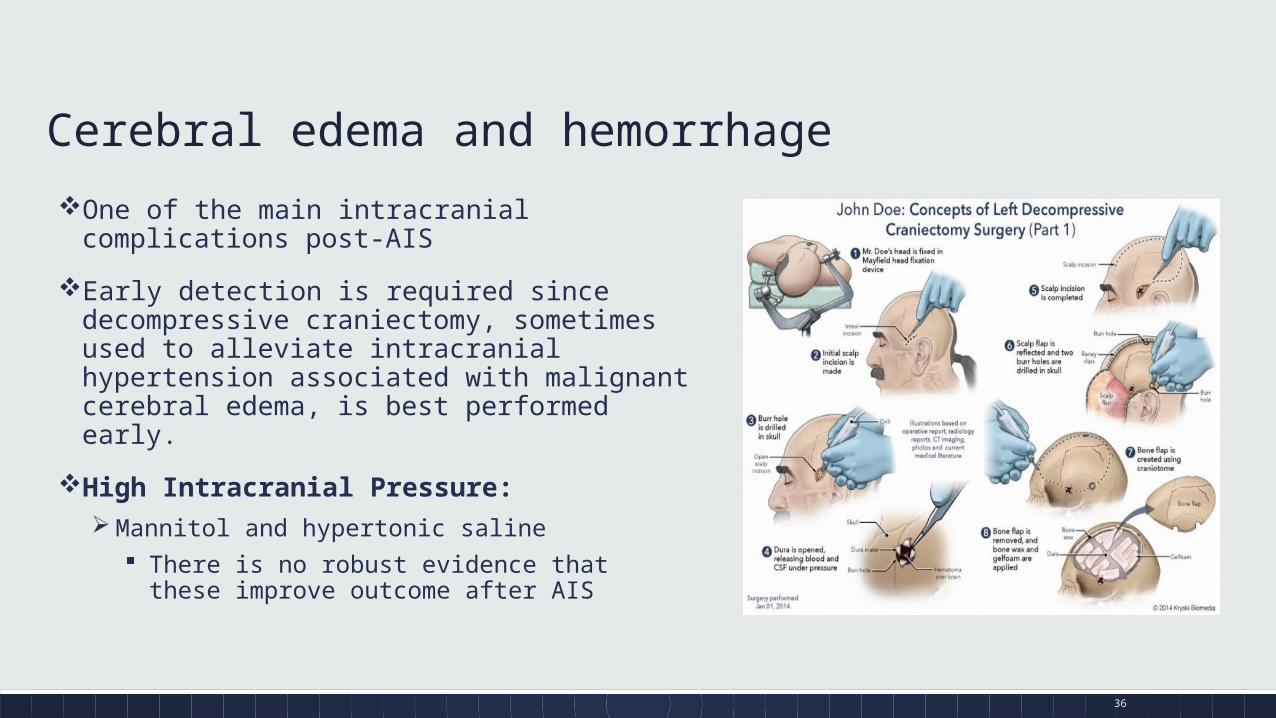
Cerebral edema and hemorrhage
One of the main intracranial complications post-AIS
Early detection is required since decompressive craniectomy, sometimes used to alleviate intracranial hypertension associated with malignant cerebral edema, is best performed early.
High Intracranial Pressure: Mannitol and hypertonic saline
There is no robust evidence that these improve outcome after AIS

37
Others Seizure
Phenytoin has the most evidence
Levetiracetam started to be used in some centers
End of life decision Decision to resuscitate
Advanced directive

38
Neuro-protectants Promising pre-clinical results
Disappointing clinical results due to: Heterogeneity of human stroke
Lack of consistency in methodological design

39
Hemorrhagic Stroke:

40
Questions

41
http://en.wikipedia.org/wiki/Terri_Schiavo_case
http://www.ted.com/talks/jill_bolte_taylor_s_powerful_stroke_of_insight?language=en

















