22
STRUCTURAL POLICY COUNTRY NOTES Indonesia

STRUCTURAL POLICY COUNTRY NOTES
Indonesia

2 SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
Indonesia ASEAN-10Average
Emerging AsiaAverage
2000-07 (average) 2013-17 (average)
IndonesiaGDP growth rates (percentage change)
0 10 000 20 000
OECD Average
Emerging AsiaAverage
ASEAN-10 Average
Indonesia
GDP per capita, 2011 (PPP, current USD)
30 000
Source: Trademap.
Composition of exports in 2011(percentage share of total exports)
Mineral Products38%
Vegetable Products12%Machinery / Electrical
8%
Plastics / Rubber8%
Textiles7%
Others27%
Composition of imports in 2011(percentage share of total imports)
Machinery / Electrical24%
Mineral Products24%
Metals10%
Chemicals &Allied Industries
9%
Transportation7%
Others26%
A. Medium-term economic outlook(forecast, 2013-17 average):GDP growth (percentage change): 6.4Current account balance (% of GDP): -3.7Fiscal balance (% of GDP): -1.2
B. Medium-term planPeriod: 2010-14Theme: Prosperous, democratic and just
C. Basic data (in 2011)Total population: 241 million*Population of Jakarta: 9.6 million (in 2010)GDP per capita at PPP: 4 666 (current USD)
Note: *Total population data for 2011 are an estimate.Sources: OECD Development Centre, MPF-2013, national sources and IMF.
Source: OECD Development Centre, MPF-2013.
0
2
4
6
8
10
Source: IMF and national sources.
Indonesia faces a number of challenges all of which centre on the key question of equality. It must build and upgrade its infrastructure primarily to close the development gap between the urban and rural areas and the west and east of the country. As a vast sprawl of scattered islands, connectivity is a key first step in its infrastructure policy. The same gap – west-east, urban-rural – affects education and, by the same token, human resource development. Generally, education enrolment and attainment levels are lower than in other ASEAN-6 countries, but they are particularly stark when urban and rural areas are compared. As part of its drive to achieve education for all, Indonesia has made significant progress in improving enrolment, particularly at the lower level of education. Decentralisation is key, but local government’s capacity, particularly in staffing and the allocation of funds, is still too limited and there is little accountability.

3SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
Widely available health-care systems need to be established. Indonesia’s expenditure on health care is among the lowest in ASEAN. Health-care provision and facilities are limited and over one-third of the population has no health insurance. The government has undertaken far-reaching social security reform, but much is still to be done to create a sustainable, equitable system.
Indonesia’s medium-term policy challenges and responses
• Narrow the regional divide by enhancing connectivity and the capacity of local government
• Strengthen the capacity of local government to provide education infrastructure • Accelerate health-care reform, focusing on coverage and access to health-care
services
POLICY FOCUS
Narrow the regional divide by enhancing connectivity and the capacity of local government
MP3EI focuses on urban-rural disparities and strengthening connectivity
One of the main pillars of the 2011-25 Master Plan for the Acceleration and Expansion of Indonesia’s Economic Development (MP3EI) is strengthening national connectivity. Under the terms of the plan, the provision of infrastructure will enable connectivity and, by reducing transportation and logistics costs, improve product competitiveness and accelerate economic growth. MP3EI aims to address regional disparities in infrastructure and ensure connectivity among the six economic corridors (Sumatra, Kalimantan, Java, Sulawesi, Bali and Nusa Tenggara, and Papua-Maluku) through an integrated system of national logistics, transportation, and communication and information.
Regional disparities in infrastructure remain a big challenge for Indonesia
Insufficient in quantity and inadequate in quality, transport infrastructure is a serious bottleneck in the economic development of Indonesia (OECD, 2011a). While the total number of vehicles in Indonesia increased threefold between 2001 and 2010, the national road network – which serves more than one-third of vehicle traffic (in vehicle-kilometres) – grew by only a quarter. What is more worrisome is that most of the district and city roads, which account for nearly 80% of the network, are in bad condition (World Bank, 2012a), while the disparities between urban and rural infrastructure pose further challenges.
As for the extent of transport infrastructure, the predominantly rural regions of Kalimantan and Papua-Maluku have substantially less as a proportion of their land area than other regions, especially Sumatra, Java and Sulawesi (Figure 2.2.1).
Disparities also exist between urban and rural regions in the quality of road infrastructure. Over 20% of it is classified as damaged in the Kalimantan and Maluku, while in Papua the proportion of roads classified as good is only 19% of the total.

4 SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
70
60
50
40
30
20
10
0
Population Length of roads Number of vehicles
Figure 2.2.1. Area, population, length of roads and number of vehicles in Indonesia, by region, 2011
(percentage of total)
Source: Ministry of Transportation, Directorate of General Land Transportation, Land Transport in Figures 2011.12 http://dx.doi.org/10.1787/888932774167
Sumatra Java Bali and Nusa Tenggara Kalimantan Sulawesi Papua-Maluku
% Area
Disparities in the quality of infrastructure are corroborated by the results of the 2011 Report on Local Economic Governance (LEG).1 It found that over 55% of respondents perceived the quality of road infrastructure as being “poor” or “very poor” in the provinces of Southeast Sulawesi, Jambi, and North Maluku, while the figure was under 25% for South Kalimantan, Babel and East Java (Figure 2.2.2). The report considered five kinds of infrastructure – roads, street lighting, water supply, electricity, telecommunications. The provinces of Southeast Sulawesi, Maluku and North Maluku came out worst on all five counts.
70
80
60
50
40
30
20
10
0
Averag
ePap
ua
West P
apua
North M
aluku
Maluku
West S
ulawes
i
Centra
l Sula
wesi
Southe
ast S
ulawes
i
Centra
l Kali
mantan
South
Kaliman
tan
West K
aliman
tan
East N
usa T
engg
ara
West N
usa T
engg
ara
East J
ava
Banten
Babel
Lampu
ng
West S
umatr
aJa
mbi
Bengk
ulu
Source: Komite Pemantauan Pelaksanaan Otonomi Daerah (Regional Autonomy Watch [KPPOD]) (2011), Local Economic Governance, A Survey of Business Operators in 245 Districts/Municipalities in Indonesia, www.kppod.org.12 http://dx.doi.org/10.1787/888932774186
Figure 2.2.2. Perceptions of the quality of local road infrastructure in Indonesia, by province, 2011
(percentage of respondents stating “poor” and “very poor”)%
5SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
In general, the report concluded that infrastructure in western Indonesia, the municipalities and main islands is of higher quality than in eastern Indonesia, the regencies, and smaller islands (KPPOD, 2011). It adds that the more densely populated regions score higher on the local infrastructure sub-index – the five types of infrastructure plus four variables: quality of local infrastructure, length of time needed to repair damaged infrastructure, level of generator ownership and frequency of power cuts.
Another reason why developing and improving connectivity is one of the main building blocks of the Master Plan is that the sheer distances between and within Indonesia’s regions make transportation and logistics costs particularly high. Shipping goods in and out as well as within Papua and West Papua is more costly than in other regions of Indonesia.
Decentralisation needs to be reinforced through better co-ordination
In addition to its efforts to improve the funding of infrastructure development, the government’s main policy for narrowing the urban-rural infrastructure gap has been decentralisation. The decentralisation process, which started in 2001, transferred both decision making and financial resources for the delivery of basic services, such as the provision of transport infrastructure, to local governments.2 However, the lack of co-ordination between key stakeholders has dogged the process.
In 2005, as part of a further effort to accelerate the development of infrastructure, the government established the National Committee for the Acceleration of Infrastructure Provision (KKPPI) to better co-ordinate infrastructure development activities among the ministries involved – the Ministry of Finance, the Co-ordinating Ministry for Economic Affairs, and the Ministry of National Development and Planning (Bappenas, 2010). However, KKPPI faces several challenges: it lacks concrete powers to shape policies, make decisions and act independently of the line ministries. For the time being, there is a sizeable gap between urban and rural areas in the number of infrastructure projects that may expect funding through public-private partnership (PPP) schemes (Figure 2.2.3).
In May 2011, as part of MP3EI, the Indonesian government launched 17 new infrastructure projects at numerous locations including Papua (OECD, 2011a), one of the regions lagging behind in terms of transport infrastructure. As the master plan identifies almost 400 infrastructure investment projects – in transport, energy, water and ICT infrastructure – to be completed by 2025, local government capacity to implement such projects needs to be bolstered. The aviation sector in Papua and West Papua, for example, has been underfunded in recent years and there was an acute shortage of high-level technical expertise in a variety of fields. Also in short supply is careful co-ordination between the various components that make up the aviation system and streamlined arrangements for cost sharing between local and central government (World Bank, 2009a).
In December 2011, the Indonesian Parliament passed the long-awaited Land Acquisition Law, which is designed to ease the bottleneck in infrastructure development by improving investment. It empowers the government to appropriate land in return for monetary compensation, the resettlement of occupants, or an ownership share in public projects. A further regulation setting out procedures for land acquisition was signed by the President in August 2012.

6 SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
18
16
14
12
10
8
6
4
2
0
West K
aliman
tanBali
East N
usa T
engg
ara
DI Yog
yaka
rta
Kepula
uan R
iau
Centra
l Kali
mantan
West N
usa T
engg
ara
North
Sumatr
a
West S
umatr
aRiau
Jambi
South
Sumatr
a
Bengk
ulu
Lampu
ng
Banten
DKI Jak
arta
West J
ava
Centra
l Jav
a
East J
ava
South
Kaliman
tan
East K
aliman
tan
North
Sulawes
i
West S
ulawes
i
Centra
l Sula
wesi
South
Sulawes
i
Southe
ast S
ulawes
i
Goronta
lo
Maluku
North
Maluku
West P
apua
Papua
Figure 2.2.3. The number of PPP infrastructure projects in Indonesia, by province
Source: Ministry of National Development Planning and National Development Planning Agency, Republic of Indonesia.12 http://dx.doi.org/10.1787/888932774205
Aceh
Kepu
lauan
Bangk
a Belit
ung
2010 2011 2012
Extra focus needs to be given to local government capacity building
Increasing resources both from public and private sources as well as improving the regulatory environment are essential measures. They are not, however, enough to complete all the infrastructure investment projects identified by the Master Plan. While infrastructure development activities among ministries and across tiers of government need to be better co-ordinated, there is also room for improvement in local government capacity building.
Although decentralisation and multi-level governance mechanisms are necessary parts of the effort to address urban-rural and regional disparities, the interests of Indonesia’s sub-national divisions cannot be effectively represented without local knowledge. Infrastructure development projects may fail or lead to significant waste or corruption in the absence of adequate resources, knowledge and human capital (OECD, 2011b).
In Indonesia, local governments do not necessarily have the capacity to design and implement their assigned infrastructure projects effectively. Central government therefore needs to intervene to build local capacity, by increasing resources, training local government staff, and improving e-government tools (Box 2.2.1).
One of the main challenges Indonesia faces is the quality of its human resources. According to MP3EI 2011-25, around 50% of the workforce in Indonesia have only primary school education, while a mere 8% hold a formal qualification. Moreover, as a result of the apparent development gap between the western and eastern parts of Indonesia and between the urban and rural parts of the country, there are considerable disparities in access to high-quality education.

7SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
Box 2.2.1. Bridging the capacity gap: Examples from OECD countries
Capacity gaps arise when a local government lacks the human, knowledge-related and/or infrastructural resources to carry out development projects. OECD examples of capacity building include involving specialised non-profit organisations and improving the use of e-government tools.
In Greece, as a response to the sovereign debt crisis, a special non-profit organisation was set up to assist small municipalities (with populations of less than 10 000) which lacked the necessary skills for preparing the four-year action plans required to access EU structural funds.
In the United States, at the height of the recent financial crisis in 2009, distressed areas and small towns were less able to apply for relevant programmes and secure funding owing to the rigorous reporting requirements attached to the Recovery Act. Most importantly, they lacked the trained manpower needed to carry out intensive contracting and monitoring processes. The federal government website therefore supplied e-government tools to help recipients of recovery funds meet their quarterly reporting requirements by submitting their project updates online. Moreover, the use of such technology also considerably enhanced the accountability, speed and transparency of the Recovery Act.
Source: OECD (2011b).
POLICY FOCUS
Strengthen the capacity of local government to provide education infrastructure
The improvement of human resources is an important pillar of the implementation strategy outlined in MP3EI. The master plan places a special emphasis on higher education, arguing that in a country that is shifting towards a knowledge-based economy the role of good quality education is paramount. MP3EI aims to tackle the issue of disparities in higher education through supply-side interventions such as establishing community colleges in every district and city. Furthermore, both vocational and academic education programmes are to be aligned with the economic potential of the six economic corridors so that graduates entering the labour market meet their particular needs.
The urban-rural education gap is still a vexed question
Although access to basic education has been steadily improving in Indonesia, as its mounting enrolment rates show (OECD, 2011a), disparities in education are still widespread.
The urban-rural education gap is apparent from literacy, enrolment rates and attainment levels. For instance, while the illiteracy rate among 15-year-olds and over was just 0.9% in the Capital Region of Jakarta in 2010, the comparable rate in Papua was 31.7% (Figure 2.2.4).

8 SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
35
30
25
20
15
10
5
0
Indon
esia
Southe
ast S
ulawes
i
South
Sulawes
i
North
Sulawes
i
Centra
l Kali
mantan
West K
aliman
tan
West P
apua
Papua
North
Maluku
Maluku
West S
ulawes
i
Centra
l Sula
wesi
Goronta
lo
East K
aliman
tan
South
Kaliman
tan
East N
usa T
engg
ara
DKI Jak
arta
West N
usa T
engg
ara Bali
East J
ava
DI Yog
yaka
rta
Centra
l Jav
a
Banten
West J
ava
Lampu
ng
Bengk
ulu
Kep Ban
gka B
elitun
g
South
Sumatr
aJa
mbi
Kepula
uan R
iau Riau
West S
umatr
a
North
Sumatr
aAce
h
Figure 2.2.4. Percentage of illiterate individuals aged 15 years or over in Indonesia, by province, 2010
Source: BPS Statistics Indonesia.12 http://dx.doi.org/10.1787/888932774224
%
Disparities in enrolment rates increase with the level of education. Nearly all provinces boast elementary school enrolment rates of over 90%, the only straggler being the predominantly rural province of Papua with an enrolment rate of 76%. Enrolment gaps are wider at junior and senior high school level (Figure 2.2.5).
100
90
70
60
50
30
20
80
40
10
0
Figure 2.2.5. Net school enrolment rates in Indonesia, by province, 2010
Source: BPS Statistics Indonesia.12 http://dx.doi.org/10.1787/888932774243
%Senior High School Junior High School Elementary School
Indon
esia
Southe
ast S
ulawes
i
South
Sulawes
i
North
Sulawes
i
Centra
l Kali
mantan
West K
aliman
tan
West P
apua
Papua
North
Maluku
Maluku
West S
ulawes
i
Centra
l Sula
wesi
Goronta
lo
East K
aliman
tan
South
Kaliman
tan
East N
usa T
engg
ara
DKI Jak
arta
West N
usa T
engg
ara Bali
East J
ava
DI Yog
yaka
rta
Centra
l Jav
a
Banten
West J
ava
Lampu
ng
Bengk
ulu
Kep Ban
gka B
elitun
g
South
Sumatr
aJa
mbi
Kepula
uan R
iau Riau
West S
umatr
a
North
Sumatr
aAce
h
9SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
Examination by age group of the percentage of the population attending school reveals that the urban-rural gap is already apparent among 5 to 6 year-olds at pre-school level. Indeed it is even wider than among elementary pupils. After elementary school the disparity in enrolment rates increases again, reaching its peak at post-secondary level between the ages of 19 and 24 years old.
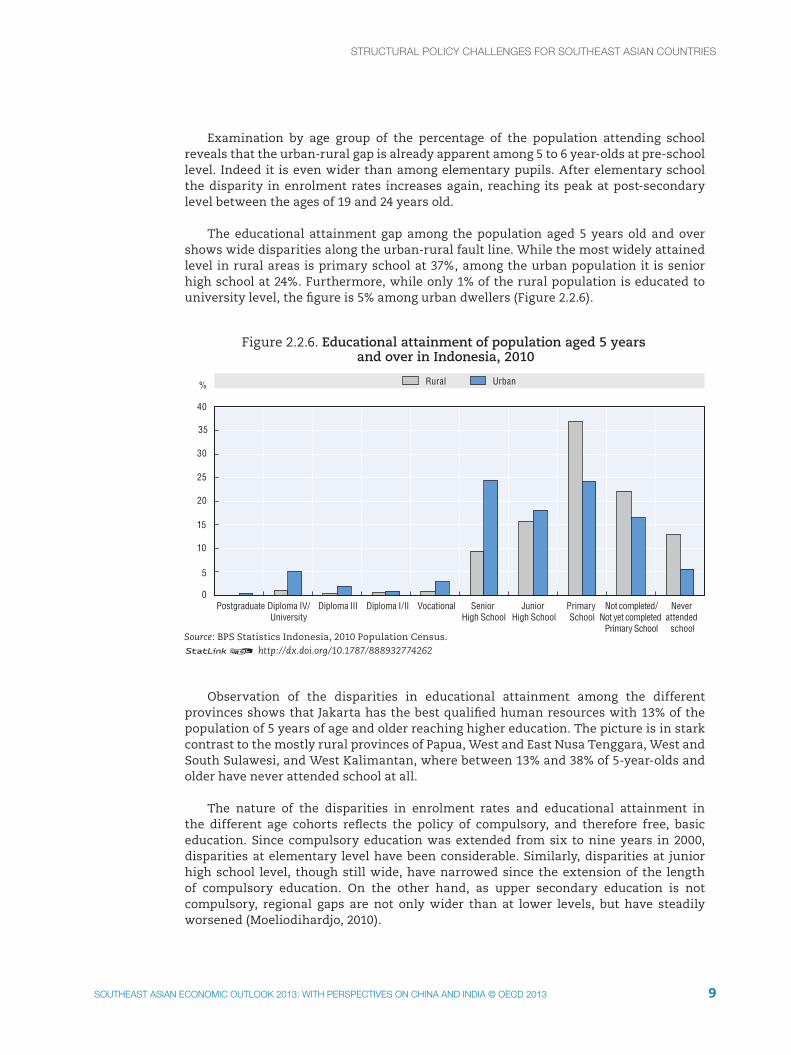
The educational attainment gap among the population aged 5 years old and over shows wide disparities along the urban-rural fault line. While the most widely attained level in rural areas is primary school at 37%, among the urban population it is senior high school at 24%. Furthermore, while only 1% of the rural population is educated to university level, the figure is 5% among urban dwellers (Figure 2.2.6).
40
35
30
25
20
15
10
5
0
Figure 2.2.6. Educational attainment of population aged 5 years and over in Indonesia, 2010
Postgraduate Diploma IV/University
Diploma III Diploma I/II Vocational Senior High School
Junior High School
Primary School
Not completed/Not yet completed
Primary School
Never attended
schoolSource: BPS Statistics Indonesia, 2010 Population Census.12 http://dx.doi.org/10.1787/888932774262
% UrbanRural
Observation of the disparities in educational attainment among the different provinces shows that Jakarta has the best qualified human resources with 13% of the population of 5 years of age and older reaching higher education. The picture is in stark contrast to the mostly rural provinces of Papua, West and East Nusa Tenggara, West and South Sulawesi, and West Kalimantan, where between 13% and 38% of 5-year-olds and older have never attended school at all.
The nature of the disparities in enrolment rates and educational attainment in the different age cohorts reflects the policy of compulsory, and therefore free, basic education. Since compulsory education was extended from six to nine years in 2000, disparities at elementary level have been considerable. Similarly, disparities at junior high school level, though still wide, have narrowed since the extension of the length of compulsory education. On the other hand, as upper secondary education is not compulsory, regional gaps are not only wider than at lower levels, but have steadily worsened (Moeliodihardjo, 2010).

10 SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
Regional disparity in Indonesia is mostly due to the paucity of social and economic infrastructure in the less developed areas (ibid.). The most serious impediments, though, in addition to the great differences in economic development among the provinces, are the shortages of educational infrastructure and quality teachers in disadvantaged areas. The 2005 Teacher Law has helped improve the standard of teaching by introducing incentives and sanctions to ensure that teachers have a minimum level of competency. The law has cut the numbers of teachers holding second jobs, but student learning outcomes do not seem to have improved so far. Nor does the current process of academic upgrading appear to have had anything but limited effects on student learning (World Bank, 2012b).
Although most universities do provide scholarships for students from the less developed provinces, the accumulated lag in education may well prove to be an insurmountable challenge when disadvantaged students take their entry exams to universities. The proportion of students admitted to the top five public universities – all located in Java – and who completed their secondary education outside Java is less than 15% (Moeliodihardjo, 2010).
Local governments need more flexibility to allocate centrally provided education funds
The decentralisation of political and economic powers from central to local governments has also devolved the delivery of education. Consequently, it is the regional governments’ responsibility to maintain schools, pay teachers’ salaries and collect students’ fees. One of the main objectives behind decentralisation was to improve access to and the quality of education – yet it may actually have widened regional differences in educational attainment (Arifin, 2011). Although local governments account for the bulk of spending on education, they have limited autonomy in the allocation of funds transferred to them by central government, as most investment programmes are designed and financed by the central government through grants (OECD, 2010a).
In 2003, as a part of the decentralisation process, the Education Law set out four major directions: i) basic education should be free of all charges; ii) schools should be given the authority to manage their own programmes; iii) community participation in education should be encouraged; and iv) the financing of education should be based on the number of students rather than on the number of schools.
In 2005, the government implemented the School Operational Assistance Programme (BOS) in order to increase enrolment rates. This generally successful scheme (SMERU, 2006) has helped reduce school costs, so easing the burden on Indonesian households, particularly disadvantaged rural ones. Moreover, as part of the 2010-14 Medium-Term Development Plan (RPJN) additional support from the regional government budget (APBD) has extended free education to more and more regions.
In 2007 – and again as part of RPJN – the government started a conditional cash transfer scheme, the Family Hope Programme (PKH), to encourage poor households to send their children to school. The PKH was designed specifically to increase enrolment rates by making the nine-year duration of compulsory basic education a reality.
In the same year, the government launched another conditional cash transfer programme for rural communities, the PNPM Generasi. Under the terms of the programme, community funds (BLM) are allotted to villages, with the amount depending on the number of beneficiaries in a village – namely, pregnant women and children

11SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
under 5 years old or of primary school and junior high school age. How the funds are used is decided by agreement among the villagers, but they must be spent on improving the provision and use of maternal and child health care and basic education services (SMERU, 2011)
Box 2.2.2. Grants for remote, rural and small schools reinforce inequality.
Over half of all provincial and district authorities have attempted to bridge the gap between the School Operational Assistance (BOS) grant that schools receive and their actual operating costs by introducing local school grants (BOSDA). However, BOSDA allocation criteria reinforce patterns of inequality with bigger, better equipped urban schools receiving higher grants than smaller, less well equipped rural schools. Its per-student formula fails to account for differences in operating costs. A school in a remote part of Papua can purchase fewer textbooks and other supplies than a school in Jayapura, the provincial capital, even with the same amount of BOSDA. In addition, electricity usage varies only according to the physical size of the school and the number of classrooms, not the number of students. A per-student formula allocates more to large schools with higher levels of enrolment than smaller schools. Ensuring that smaller schools have enough resources to cover their overheads is a significant issue, because nearly half of all primary schools in Indonesia have fewer than 150 students.
The BOS has recently been decentralised to improve it implementation.
Source: World Bank (2012c).
The 2010-2014 Medium-Term Development Plan also has provision for school infrastructure. Central government has assisted the regional authorities in rehabilitating school buildings built in the 1970s and 1980s and further increasing the total number of classrooms and new schools.
A further measure – the open junior high school system – addresses the lack of school infrastructure and the needs of students who either live in remote locations or simply cannot attend school regularly for economic reasons. Children in poor areas tend to drop out and start working once they have gained basic literacy and numeracy skills, because their parents, who mostly work informally, see their children as workers and place no value in further education (Mukherjee, 2006).
The open junior high school system was created to provide a teaching and learning schedule that is as flexible as possible. Tutors assist in the “learning process” in their neighbourhoods, while students meet every now and then to discuss what they learned and eventually take exams in a “learning place” that may be further away from where they live. No tuition fees are charged in open junior high schools and, although the general curriculum is similar to that of their peers in regular junior high schools, there is more emphasis on life skills as most students do not continue formal education afterwards.
Target funding where needs lie
In addition to increasing public spending on education3 to improve the development of rural school infrastructure, it is also important to balance local autonomy with efficiency and make school funding strategies more responsive to the needs of disadvantaged regions, schools and students. A balance should also be struck between the autonomy delegated to local governments and their accountability. Decentralising the governance

12 SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
of education is not necessarily a way to respond to local needs or address disparities, as local authorities may lack the required capacity. The experience of OECD countries shows that, while the central government should exert control over levels of school funding and performance standards (OECD, 2012a), schools should enjoy autonomy in areas where their knowledge and know-how are relevant – e.g. managing their personnel. Currently personnel management is the responsibility of regional and sub-regional authorities (OECD, 2012b).
As disadvantaged regions and schools may need additional resources (to attract more experienced, better qualified teachers, for example), it is paramount that the right amounts are allocated if disparities are to be effectively addressed. Formula funding – which relies on a mathematical equation incorporating parameters like students’ socio-economic backgrounds and parents’ educational levels – is considered to be a more efficient strategy for ensuring equity (Box 2.2.3) than the current practice of historical budgeting.
Box 2.2.3. Formula funding for equitable and effective resource allocation:Examples from OECD countries
Disadvantaged schools may need additional resources as the challenging socio-economic profiles and varying needs of the students tend to push up teaching costs. The OECD experience is that disadvantaged schools have less experienced, less qualified teachers, even though quality teaching is particularly vital to meeting the learning needs of their students. It is therefore essential that resource allocation should be optimised through an adequate funding scheme in order to improve equity.
Formula funding uses mathematical formulae comprising meaningful parameters to determine school budgets. Formulae contain four main groups of variables used across OECD countries. The variables are based on: i) student numbers and grade levels; ii) needs; iii) curricula or educational programmes; iv) school characteristics. In general, formula funding is considered to be the most efficient, transparent method of school funding that incorporates needs criteria.
In the Netherlands, formula funding that is weighted to meet the needs of disadvantaged students has been in place in all primary schools since 1985. The “weight” of each student is determined by their parents’ educational level, while schools have the freedom to spend the extra resources as efficiently as they can. Formula funding arrangements have apparently succeeded in distributing differentiated resources to schools according to their different needs: primary schools with high proportions of “weighted” students have on average 58% more teachers per student as well as more support staff.
Chile introduced a weighted voucher scheme in 2008 to favour students from low socio-economic backgrounds and schools with high concentrations of disadvantaged students. It replaced a system where all students were weighted equally. Although acceptance of supplementary funds is voluntary, the schools who do accept them are subject to mandatory technical support and a quality assurance system that includes improvement plans and objectives to ensure value for money. Evidence points to the weighted voucher system achieving results and mitigating disparities in education.
Source: OECD (2012a).

13SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
Formula funding weighted to account for disadvantaged students and schools would be a step in the right direction of mitigating educational disparities in Indonesia.
POLICY FOCUS
Accelerate health-care reform, focusing on coverage and access to health-care services
Both the RPJN 2010-2014 and the MP3EI 2011-2025 stress the importance of health care. The RPJN seeks to widen access to health services and sets ambitious numerical targets for increasing life expectancy and reducing infant and maternal mortality rates. Other objectives, it states, are improving the quality of internationally accredited hospitals, standardising pharmaceutical procurement, controlling the prices of branded generic medicines, and gradually expanding the health insurance system to universal coverage by 2014.
The MP3EI reaffirms the importance of improved access to health-care services and proposes to do so through targeted economic assistance to the poor and social insurance for all.
Indonesia’s health-care system remains underdeveloped
Indonesia does not spend enough on health care. Although government health expenditure has increased in recent years, total health expenditure has remained under 3% of GDP (Figure 2.2.7). Among ASEAN countries, only Myanmar spends less on health than Indonesia (Figure 2.2.8).
9
8
7
6
5
4
3
2
1
0
180
160
140
120
100
80
60
40
20
0
Figure 2.2.7. Expenditure on health in Indonesia, 2000-10
Source: WHO Global Health Expenditure Database, http://apps.who.int/nha/database/DataExplorerRegime.aspx.12 http://dx.doi.org/10.1787/888932774281
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
IDR trillion%
General government expenditure on health (RHS)General government health expenditure as % of General government expenditure
Private expenditure on health (RHS)Total expenditure on health as % of GDP

14 SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
8
7
6
5
4
3
2
1
0
Figure 2.2.8. Expenditure on health in Southeast Asia(percentage of GDP)
Source: WHO Global Health Expenditure Database, http://apps.who.int/nha/database/DataExplorerRegime.aspx.12 http://dx.doi.org/10.1787/888932774300
Brunei Cambodia Indonesia Lao PDR Malaysia Myanmar Philippines Singapore Thailand Viet Nam ASEANaverage
%2005 2010
An additional issue of health-care spending is its inefficiency. Although local authorities are responsible for a substantial part of health service delivery, there is a lack of administrative and managerial capacity, while local governments have no incentive to contain costs or increase cost-effectiveness (OECD, 2010a).
The insufficiency and inefficiency of Indonesia’s health expenditure has produced sub-par service provision, as measured by the number of hospitals and the density of medical staff. And even though they have increased slightly (Figure 2.2.9), Indonesia still lags behind its regional peers (Figure 2.2.10). The number of hospital beds per 1 000 people is only 0.6, lower than in Cambodia or Lao PDR. Similarly, there are only 0.3 doctors for every 1 000 inhabitants, while the figure is 0.5 in Myanmar (Figure 2.2.10). The low effective density of medical personnel is due mainly to protective regulations that bar entry into the medical profession as well as to the limited powers of local authorities to sanction absenteeism (OECD, 2010a).
There is room to improve the quality of services on account of the lack of medical appliances and supplies (OECD, 2010a). The result is low confidence in health-care services, with relatively high percentages of the population treating themselves (70%) or using traditional medicine (30%) (Figure 2.2.11).
As a consequence of insufficient, inefficient expenditure and shortages of equipment and medicine, the health status of the population is poor. Figure 2.2.11 shows that when Indonesians are questioned about their health, 31% report they have had complaints in the last month. Furthermore, life expectancy is lower than in any other ASEAN countries except for Cambodia, Lao PDR and Myanmar.

15SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
1 750
1 700
1 650
1 450
1 600
1 550
1 500
1 400
1.0
0.8
0.6
0.4
0.2
0.0
1.2
Figure 2.2.9. Supply of health services in Indonesia
2009 2010 2011Source: Ministry of Health.12 http://dx.doi.org/10.1787/888932774319
Number of hospitals Personnel per 1 000 people
Hospital Nurse (RHS) Midwives (RHS) Doctor (RHS)
7
6
5
4
3
2
1
0
Figure 2.2.10. Supply of health services in Southeast Asia, 2010 or latest year available
Brunei Cambodia Indonesia Lao PDR Malaysia Myanmar Philippines Singapore Thailand Viet Nam ASEANaverage
Source: World Bank.12 http://dx.doi.org/10.1787/888932774338
Per 1 000 people
Hospital beds Physicians Nurses and midwives
Much of the Indonesian society does not have any type of health insurance, either although the share of the population covered by any health insurance programme increased from 43% in 2007 (ILO, 2008) to 65% in 2011 (Figure 2.2.12).

16 SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
%
2005 2006 2007 2008 2009 2010
80
70
60
50
40
30
20
10
0
Figure 2.2.11. Health status and alternative treatment in Indonesia
Source: BPS Statistics Indonesia.12 http://dx.doi.org/10.1787/888932774357
Percentage of population with health complaint during the last month
Percentage of populationwith traditional medicine
Percentage of populationwith self treatment
35%
9%
33%
14%
7%2%
Figure 2.2.12. Health insurance coverage in Indonesia, by programme, 2011
Source: Ministry of Health.12 http://dx.doi.org/10.1787/888932774376
Not insuredJamkesmas Jamkesda Askes Jamsostek Private insurance and others
Despite government efforts to provide coverage for all, the extent of the informal economy – which accounts for about two-thirds of total employment (OECD, 2011a) – and the fragmented nature of the different health insurance schemes leave a considerable proportion of the population without insurance. There is empirical evidence that illness leads to financial risk as people pay for treatment out of their own pockets. This is especially true of the rural population and the poorest quartile of the population where consumption smoothing is imperfect as non-food expenditure is affected by ill health (Sparrow and Van de Poel, 2012).

17SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
The existing publicly managed health insurance programmes differ as to their beneficiaries, benefits, premiums and in the efficiency of their health-care provision and management. The government-financed programmes, Jamkesmas and Jamkesda, for the poor and near-poor cover over 100 million people, or almost 50% of the population. The benefits of Jamkesmas include comprehensive out-patient and in-patient care in public health clinics and third-class hospitals, while those of Jamkesda are provided only in certain provinces and districts and vary in nature from one to the other.
Table 2.2.1. Health insurance programmes in Indonesia
Beneficiaries Premium Benefits Coverage Performance
Jamkesmas - Poor and near-poor population (target population is 93 million people)
- Financed by the government
- Comprehensive out- and in-patient care in public health clinics and third-class hospitals
76 million people - Lack of co-ordination between planning and implementation
(33% of the population)
- Beneficiaries poorly informed about the benefits they are entitled to.
Jamkesda - People who are identified by the local authorities as poor and near-poor but are not covered by Jamkesmas
- Financed by local government
- Benefits are provided only in certain provinces and districts and vary from one to the other.
33 million people - Lack of detailed information about beneficiaries and how they use health care
(14% of the population)
- Beneficiaries of Jamkesda may overlap with those of Jamkesmas
Askes - Civil servants and their dependants
- 2% of basic salary that is matched by the government
- Comprehensive out- and in-patient care, no additional payment needed for prescribed medicine
17 million people - There is no official information either on the exact number of beneficiaries covered or on the amount of benefits paid out
- Mandatory scheme - There is only one state-owned hospital that provides services for Askes card holders in each municipality
(7% of the population)
- The quality of service received varies considerably according to the rank of the civil servant treated
Jamsostek - Formal sector workers and their families who work in private enterprises with at least ten workers and a turnover of at least IDR 1 million
- Either 3% of the salary for single employees and 6% for married employees - Not mandatory (companies can opt out if they offer comparable or better health insurance)
- Generous health care package that includes a wide range of medical services, drugs, and treatment for out-patients and in-patients
6 million people (2% of the population)
- Governance and management are of better quality than in other publicly managed programmes (e.g. Askes), and it is consequently more efficient and transparent
Source: OECD Development Centre’s compilation based on ILO Social Security Department, www.ilo.org/dyn/ilossi/ssimain.schemes?p_lang=en&p_geoaid=360; Widjaja and Simanjuntak (2010); OECD, 2010a.

18 SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
Although Jamkesmas and Jamkesda reach much of their target population, there are serious deficiencies. The poor co-ordination between planning and implementation leads to overlaps, with some people covered by both schemes. Another issue is the lack of detailed information about beneficiaries and how they use health care. There are some, for instance, who are covered but were not originally so – and vice versa – while most people do not know to what services they are entitled.
The two publicly managed but privately financed programmes, Askes and Jamsostek, insure civil servants and their dependents and formal sector workers (and their families). While Askes is a mandatory scheme, employers can opt out of Jamsostek if they offer comparable or better health insurance policies. Although Askes insurance premiums (2% of the salary matched by the government) are more attractive, the benefit package offered by Jamsostek is more generous. The programmes also differ with respect to their performance. Askes provides official information neither on its exact number of beneficiaries nor the amount of benefits it pays out, while its quality of service varies widely according to beneficiaries’ rank in the civil service. Jamsostek, however, is more efficient and transparent in its governance and management practices.
Recent policies address health care and other social security reforms
Since Indonesia began its decentralisation process in 2001, local authorities have had the power to manage public health-care facilities and medical personnel by setting fees and user charges for public health services and allocating the transfers received from central government to finance provision. However, control over medical personnel’s employment and pay conditions and over the health insurance scheme for the poor has remained in the hands of the central government (OECD, 2010a).
In 2004, the National Social Security System (SJSN) Law provided a blueprint for the future shape of the social security system and envisaged a comprehensive system of social protection with universal coverage. In addition to health insurance, the framework included pensions, old-age savings, workers’ compensation, and death benefits – all financed by workers’ contributions, with the exception of provisions for the poor, which are funded by the state. As for informal workers’ contributions, the SJSN Law states that nominal amounts instead of a percentage of wages should be collected. With respect to implementation, it specifies that the health-care programme should be put in place first. The sustainability of the future system was also taken into account, as the law stated explicitly that the programmes had to be affordable for the state budget. In terms of governance, social security administrative bodies (BPJS) would manage the social security funds attached to each programme. A monitoring and research body, the National Social Security Council (DJSN), would be created to formulate policies, synchronise the SJSN system, conduct research into social security, and monitor the social security administrative bodies. However, the law did not address such issues as the amount of benefits, contribution rates, or the exact governance structure of the system (Rachmatarwata and Ginting, 2010).

19SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
In 2011, in a major step towards the actual implementation of the National Social Security System Law, a regulation spelled out the status of the BPJS, BPJS Health and BPJS Employment administering health as well as work accident, old-age, pension and death related programmes. The BPJS are to be managed as trust funds on a non-profit, compulsory-participation basis and are to be externally monitored by the DJSN. When the BPJS’s health programme becomes operational on 1 January 2014, current health insurance schemes will be dissolved and managed by the new administrative body, BPJS Health.
Health-system reforms need to look further ahead
While public spending on health care needs to be increased, the medium- and long-term fiscal sustainability of the reformed health-care system also deserves consideration. Another challenge, in addition to the objective of universal coverage, is that the ageing of Indonesian society will further increase the strain on the system in the long term (Box 2.2.4).
Although the final benefit and contribution levels are still pending, the 2004 BPJS Law was an important step towards creating a financially viable system that is based on compulsory participation and so ensures adequate risk pooling. Nevertheless, further efforts are needed to achieve fiscal sustainability. Cost-effectiveness in treatment procedures as well as the administrative and managerial capacities of local governments need to be enhanced in order to increase spending efficiency.
The issue of fiscal sustainability is closely linked to the balance between the benefit package offered and the level of contribution required. As the different health-care schemes will be dissolved under BPJS Health, it is important to define an adequate but fiscally sustainable basic benefit package that can be supplemented with further private health insurance providing extra services. As regards contributions, there is a need to define the different premiums of employees working in different sectors (i.e. civil servants covered by Askes and private-sector employees by Jamsostek), while the government should continue to fund health insurance for the poor and near-poor. For the informal sector, a tax-based financing scheme or a government-funded one similar to the arrangement for the poor and near-poor could be considered as the administrative and enforcement costs of collecting contributions may be high.
The capacity of the new administrative body, BPJS Health – its funding, its personnel’s technical skills (e.g. actuarial and modelling abilities) and data collection and electronic registration system – needs to be enhanced. On the supply side, physical infrastructure and service provision could be improved to cope with growing demand prompted by coverage for all and – simply – to improve the general quality of services. To ease supply-side constraints, more investment is required in physical infrastructure such as hospitals and medical appliances, especially in rural areas. In terms of service provision, local authorities should be granted greater powers to monitor and sanction staff, e.g. medical personnel for absenteeism (OECD, 2010a).
20 SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
Box 2.2.4. Improving health care under a budget constraint:Examples from OECD countries
In OECD countries, total health-care spending as percentage of GDP has risen significantly from 5% in 1970 to 9.5% in 2007. Total health-care expenditure per capita also increased more than 70% in real terms between 1990 and 2007. In the meantime, public spending on health care, which accounts for 15% of general government expenditure on average in 2007, is projected to increase by 3.5 to 6 percentage points of GDP between 2005 and 2050.
Across OECD countries, but also in Southeast Asian countries, population ageing, rapidly rising health-care prices and costly developments in medical technology are major contributors to upward pressure on health-care budgets.
In order to achieve two competing goals – enhancing the health-care system and maintaining fiscal sustainability – OECD countries use various policy instruments to govern the behaviour of users, providers and payers of health care.
As regards users, many OECD countries try to steer patient demand by restricting their choice (e.g. the requirement to register with a general practitioner and/or limitations on choosing a primary care physician, a specialist and a hospital).
Belgium, Canada, France, Germany, Japan and Switzerland have introduced powerful incentives to encourage them to adjust to demand by relying on fee-for-services and payment per procedure. There is a risk, however, that such provider payment schemes may lead to supply-induced demand owing to information asymmetry between patients and doctors.
As for payers, competition across insurers has been introduced in some countries. In Switzerland, free choice among insurers for basic health-care coverage and open enrolment were introduced in 1996. Overall, OECD countries have relied both on market mechanisms and on regulations, which often play a complementary role.
OECD countries have more specific and practical examples of programmes that can be lessons for Southeast Asian countries. The United Kingdom is implementing a programme of health checks for everyone aged between 40 and 74 to prevent heart disease, stroke, diabetes and kidney disease. According to estimates from the Department of Health, the health check programme will cost GBP 332 million (British pounds) a year, but generate an annual benefit of GBP 3 678 million, save around 650 lives, and prevent 1 600 strokes and heart attacks.
Japan introduced mandatory long-term care insurance system in 2000. It is reviewed or revised every five years, to improve health-care services to elderly people and reduce costs. After the first review in 2005, “hotel costs” (i.e. room and board fees for long-term care residents) were introduced to give people incentives to stay at home and receive community-based services rather than go into more costly long-term care facilities. Japan also expanded the preventative service provision to prevent people from becoming dependent.
Sources: OECD (2010b) and OECD (2011c).

21SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
Notes
1. The LEG study, prepared by KPPOD (Komite Pemantauan Pelaksanaan Otonomi Daerah, or Regional Autonomy Watch) and The Asia Foundation, aims to measure the quality of local economic governance in 245 regencies/municipalities in 19 provinces in Indonesia by surveying business community`s perceptions. Local infrastructure is one of the nine indicators included in- the report. The final LEG Index is the weighted average of the nine sub-indices.
2. See Asia-Pacific page on the World Bank website, http://web.worldbank.org/WBSITE/EXTERNAL/COUNTRIES/EASTASIAPACIFICEXT/0,,contentMDK:23186158~pagePK:146736~piPK:146830~theSitePK:226301,00.html#5.
3. In 2010, public spending on education in Indonesia was only 3% of total GDP.

22 SOUTHEAST ASIAN ECONOMIC OUTLOOK 2013: WITH PERSPECTIVES ON CHINA AND INDIA © OECD 2013
STRUCTURAL POLICy CHALLENgES FOR SOUTHEAST ASIAN COUNTRIES
BibliographyADB (2010), Special Evaluation Study on Asian Development Bank Support for Decentralization in Indonesia, Asian
Development Bank, Manila.
ADB (2007a), Preparatory Studies on National Social Security System in Indonesia, Asian Development Bank, Manila.
Arifin, E.N. (2011), “Regional heterogeneity of the large market and production base”, in A. Ananta et al. (eds.), The Indonesian Economy: Entering a New Era, Institute of Southeast Asian Studies, Singapore.
Bappenas (2012), Public Private Partnerships - Infrastructure Projects Plan in Indonesia 2012, Ministry of National Development Planning Agency of Indonesia, Jakarta.
Bappenas (2010), “Indonesian infrastructure : Condition, problem and policy”, Bappenas Blog, Ministry of National Development Planning Agency of Indonesia, Jakarta.
Bappenas (2009), Medium-term Development Plan (RPJN) 2010-2014, Ministry of National Development Planning Agency of Indonesia, Jakarta.
ILO (2008), Indonesia: Providing Health Insurance for the Poor, International Labour Organization Subregional Office for South East Asia, Bangkok.
KPPOD (Regional Autonomy Watch) (2011), Local Economic Governance, A Survey of Business Operators in 245 Districts/Municipalities in Indonesia, KPPOD, Jakarta.
Moeliodihardjo, B.Y. (2010), “Equity and access in higher education – The case of Indonesia”, draft, March.
Mukherjee, N. (2006), Voices of the Poor: Making Services Work for the Poor in Indonesia, World Bank East Asia and Pacific Region.
OECD (2012a), Equity and Quality in Education – Supporting Disadvantaged Students and Schools, OECD, Paris.
OECD (2012b), Education at a Glance 2012, OECD, Paris.
OECD (2011a), Southeast Asian Economic Outlook 2011/12, OECD, Paris.
OECD (2011b), Making the Most of Public Investment in a Tight Fiscal Environment - Multi-Level Governance Lessons from the Crisis, OECD, Paris.
OECD (2011c), Health Reform: Meeting the Challenge of Ageing and Multiple Morbidities, OECD, Paris.
OECD (2010a), OECD Economic Surveys – Indonesia, OECD, Paris.
OECD (2010b), Health Care Systems: Efficiency and Policy Settings, OECD, Paris.
Pisu, M. (2010), “Tackling the infrastructure challenge in Indonesia”, OECD Economics Department Working Paper, No. 809, OECD Publishing, Paris.
Rachmatarwata, I. and E. Ginting (2010), “Social security reform in Indonesia”, paper presented at the ADB Social Protection Conference, 21 22 April, Manila.
SMERU (2011), “Qualitative impact study for PNPM Generasi and PKH on the provision and the utilization of maternal and child health services and basic education services in the provinces of West Java and East Nusa Tenggara”, SMERU Research Report, Jakarta, January.
SMERU Research Institute (2006), “A rapid appraisal of the PKPS-BBM education sector: School operational assistance (BOS)”, SMERU Research Report, Jakarta, September.
Sparrow, R. and E. Van de Poel (2012), “Financial consequences of ill health and informal coping mechanisms in Indonesia”, SMERU Working Paper, SMERU Research Institute, April.
Widjaja, M. and R.A. Simanjuntak (2010), “Social protection in Indonesia: How far have we reached?”, in M. Asher, S. Oum and F. Parulian (eds.), “Social protection in East Asia – Current state and challenges”, ERIA Research Project Report 2010, No. 9.
World Bank (2012a), Indonesia Economic Quarterly – Rising to Present and Future Challenges, World Bank, Washington DC, July.
World Bank (2012b), Teacher Certification in Indonesia: a Doubling of Pay, or a Way to Improve Learning?, Human Development Sector, World Bank Office Jakarta, Policy Brief, October.
World Bank (2012c), The BOSDA Improvement Program: Enhancing Equity and Performance through Local School Grants, Human Development Sector, World Bank Office Jakarta, Policy Brief, May.
World Bank (2009a), Transport Development Priorities in Papua and West Papua, World Bank, Washington D.C.
World Bank (2009c), Health Financing in Indonesia – A Reform Road Map, World Bank, Washington DC..

















