22
1 / 22 Subarachnoid Bleeds Under the Spider via deepthought
1 / 22
Subarachnoid Bleeds
Under the Spidervia deepthought

2 / 22
SAH: symptoms● “worst headache of my life”
– Sudden-onset– Severe w max intensity in seconds = thunderclap
● Sentinel headache in ~10-40% in aneurysmal– Warning leak ~2-8 wks before overt SAH
● ~1% of all ED headaches● Altered cognition:
– Brief loss of consciousness / encephalopathy (from mild lethargy to coma)
● If convexity-restricted may present w transient focal motor/sensory symptoms similar to seizures
● seizures, nausea/vomiting, meningismus, photophobia● Onset context:
– Most commonly occurs w/o signifcant exertion - ADLs– (may occur during physical/psych stress)
3 / 22
SAH: overview● Bleeding w/i subarachnoid space = between arachnoid & pia
mater (normally flled w CSF)● ~3 to 10% of all USA strokes● Incidence variable depending on region (per 100k adults / yr):
– China 2, US ~14.5, Finland 22.5● Age-associated increase in risk - mean onset 50 yo
– But younger vs. other stroke types● Prognosis
– Mortality range broad: 8 to 65%, ~10-15% prehospital mortality
– ~½ survivors w signifcant impact on quality of life
4 / 22
SAH: etiologies
● Traumatic - most common● spontaneous/non-traumatic● Most aneurysmal ~80%● ~20% non-aneurysmal● ~10% no clear vascular abnormality

5 / 22
SAH: initial diagnosis● Following for those presenting w typical symptoms● Non-contrast head CT:
– Sensitivity decreases from onset as blood diluted by CSF● Approaches 100% if within 6 hrs from bleed onset● False negative approx: < 1.5 in 1000● >90% if w/i 24 hrs of bleed● ~50% days 5-7
● LP if suspicion w normal CT:– “Unequivocal” positive:
● Xanthochromia: spectrophotometry OR visual inspection● Lyzed RBC releasing Hg -> oxyHg (~pink, “hrs”) + BR
(yellow, up to 12 hrs)● Could get false negatives if < 12 hrs from onset
– elevated RBC unchanged tubes 1-4– May also see elevated opening pressure
● If LP equivocal (e.g. no xanthochromia or only 1 tube analyzed)– CTA or conventional angio
● LP confounders– Traumatic taps or sample handling error - false RBC elevation– Spec for xanthochromia may have poor specifcity / high false
positives
Dr. James Heilman via wikipedia

6 / 22
SAH: etiology determination● Angiography - digital subtraction angiography = gold standard
– subtracting pre-contrast image from post-contrast image– Risk of “permanent & transient complications” 1.8% in SAH (3.7% in TIA)– ~15-20% w SAH are w/o vascular lesion on initial 4-vessel angiography
● If initial angio negative -> repeat in 4-14 days re potential false negatives– Up to ~24% negative studies w subsequent aneurysm found– Possible reasons: technical/read error, small aneurysm, obscuration due
to vasospasm, hematoma, or thrombosis in aneurysm● If repeat angio negative: MRI brain/spinal-cord eval source bleed● CTA/MRA
– Lower resolution, can identify aneurysms ~2-5mm– Vs. DSA sensitivity is ~83-98%

7 / 22
SAH: initial angio negative
● Perimesencephalic = majority in some case series (to ~⅔)– Blood isolated to
perimesencephalic cisterns anterior to brainstem -
– Generally benign course● Occult aneurysm - up to 24%● Vascular malformations / AVM -
intracranial or spinal (<10%)● Intracranial arterial dissection -
some studies up to ~4.5%
● Less common:– Sickle cell– Pituitary apoplexy– Cerebral venous thrombosis– Bleeding disorders– Traumatic– Cocaine (aneurysmal & non)– Cerebral amyloid angiopathy– Tumors– Vasculitis– RCVS– Post-endarterectomy
hyperperfusion
8 / 22
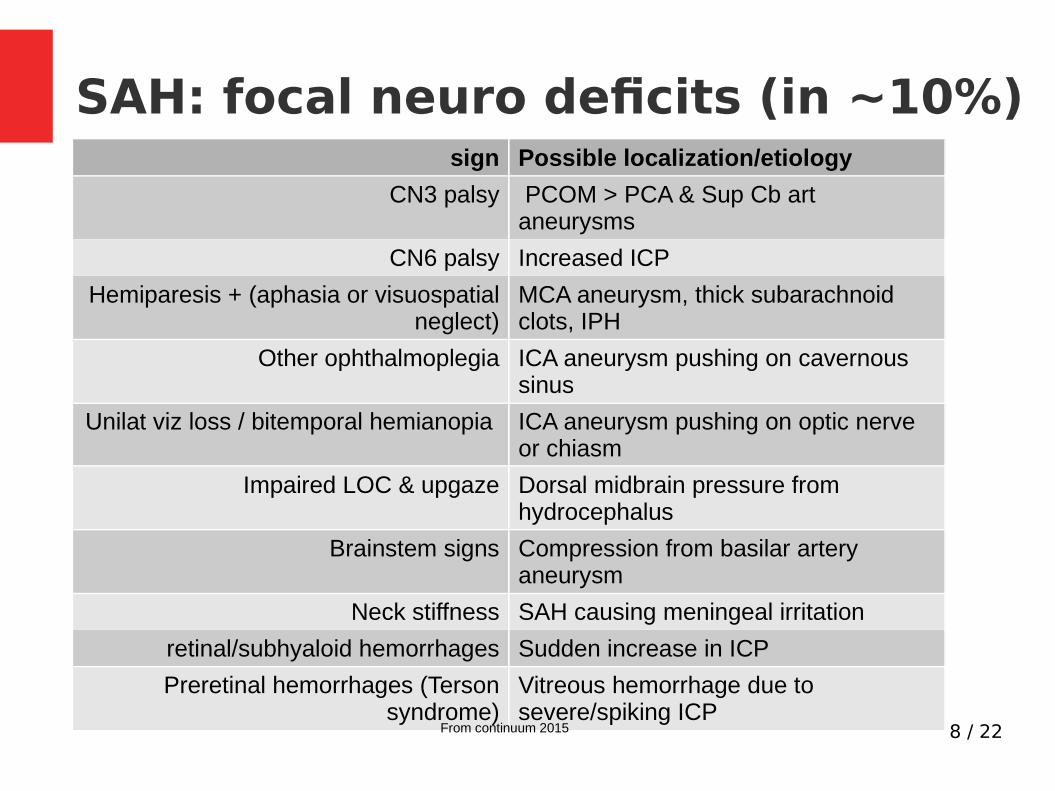
SAH: focal neuro defcits (in ~10%)sign Possible localization/etiology
CN3 palsy PCOM > PCA & Sup Cb art aneurysms
CN6 palsy Increased ICP
Hemiparesis + (aphasia or visuospatial neglect)
MCA aneurysm, thick subarachnoid clots, IPH
Other ophthalmoplegia ICA aneurysm pushing on cavernous sinus
Unilat viz loss / bitemporal hemianopia ICA aneurysm pushing on optic nerve or chiasm
Impaired LOC & upgaze Dorsal midbrain pressure from hydrocephalus
Brainstem signs Compression from basilar artery aneurysm
Neck stiffness SAH causing meningeal irritation
retinal/subhyaloid hemorrhages Sudden increase in ICP
Preretinal hemorrhages (Terson syndrome)
Vitreous hemorrhage due to severe/spiking ICP
From continuum 2015
9 / 22
Aneurysmal SAH● Intracranial aneurysms in 1-2% of population● Types:
– saccular (aka berry) aneurysms - balloon-like vessel wall outpouchings w neck to parent vessel & more fragile dome
● Typically at branch points along intracranial arteries - thought hemodynamic stress weakens wall between branches
– Fusiform aneurysm: dilation of main vessel (less rupture-prone vs. saccular)● Risk factors for aneurysms
– Family history in 1st-degree relatives– Some connective tissue disorders: e.g. Ehlers-Danlos, Marfan’s– Polycystic kidney disease
● Risk for rupture:– Size > 7mm– HTN, current smoking, EtOH abuse, sympathomimetics, labile BP

10 / 22
Aneurysmal SAH: locations
● Acom ~30%● Pcom ~25%
– Arising from ICA may cause painful CN3 palsy● MCA ~20%● Vertebrobasilar ~15%
● Source: Blumenfeld

11 / 22
Aneurysm to symptoms
● Bleeding/rupture● Unruptured large aneurysms may cause
symptoms via mass efect

12 / 22
SAH grading: Hunt-Hess
Grade Neuro status
1 Asymptomatic or mild HA & slight nuchal rigidity
2 Severe HA, stif neck
no neuro defcit except cranial nerve palsy
3 Drowsy or confused, mild focal neuro defcit
4 stuporous, moderate or severe hemiparesis
5 Coma, decerebrate posturing
● Advance +1 for presence of: HTN, DM, severe DM, severe arteriosclerosis, chronic pulmonary disease, or vasospasm on angiography
● Conficting data re utility/prognosis: attempts to grade encephalopathy severity w long-term neurologic outcome

13 / 22
SAH grading: mFisher - vasospasm risk
● Depth:– Thin: < 1mm – Thick: > 1mm
● Fischer scales = index of vasospasm● Not correlated w clinical outcome
Blood appearance on CT vasospam
0 No blood 0%
1 Thin SAH (focal or diffuse) w/o IVH 24%
2 Thin SAH (focal or diffuse) w IVH 33%
3 Thick SAH (focal or diffuse) w/o IVH 33%
4 Thick SAH (focal or diffuse) w IVH 40%
Srcs include: radiopaedia

14 / 22
SAH: complications● Re-bleeding/rupture (mainly 24-48 hrs)● Vasospasm (~70% aneurysmal)● Delayed ischemia (~⅓ of aneurysmal)● Hydrocephalus (“15-85%”) / Increased ICP● Seizures (~20% aneurysmal)
● hypoNa● Cardiac abnormalities● Hypothalamic dysfunction

15 / 22
SAH: further general w/u
● Serologies: CBC, basic chemistries, coags, tox-screen● EKG● If initial-angio negative:
– MRI brain & spinal cord with and without contrast

16 / 22
Aneurysmal SAH: med management
● Nimodipine 60 q4 hrs for 21 days– Ideally w/i 4 days of SAH– Calcium channel blocker– No evidence reduces angiographic or symptomatic vasospasm– Decreases risk of delayed cerebral ischemia through unclear
mechanism– However improves outcomes -> thus standard of care
● decreases odds of “poor outcome” by ~1/3● Decreased odds “defcit, mortality, or both”, infarction rate● Slightly decreased mortality
– NNT to prevent 1 poor outcome: ~13– Treatment efect correlated w severity of SAH– Sfx: hypotension, constipation
● Anti-seizure drugs: routine prophylaxis not recommended despite sz in up to 20%

17 / 22
Aneurysmal SAH: management
● Transcranial doppler ultrasound– Detect vasospasm earlier
● Monitor Na closely● If detect signifcant delayed ischemia w or w/o vasospasm:
– “triple ‘H’” therapy to improve perfusion● Hypervolemia - IVF● Hypertension - alpha-adrenergic agents (safer after clip/coil)● But generally: MAP < 110 & SBP < 160 (& taking into account pre-bleed
BPs)● hemodilution
– May consider cerebral angioplasty and/or selective intraarterial vasodilator therapy
● Hydrocephalus - thought from blood blocking normal outfow of CSF, @ days to wks– If causing encephalopathy - place EVD
● Lumbar drain w reduced vasospasm but contraindications: hydrocephalus + IPH

18 / 22
SAH: ruptured aneurysm● Mortality ~25-50%● Re-rupture risk:
– 1st 24 hrs: 4-15%– 2 weeks ~20%– Elevated for 30 days if untreated
● Prevent re-rupture:– Medical:
● Goal normal: blood volume, temp, glc, lyte balance, ventilation● DVT ppx: SCDs + after 24 hrs unfractionated heparin unless procedures● Maybe antifbrinolytics (can increase DVT & delayed cerebral ischemia)
– procedural: ● Endovascular intervention - e.g. coiling - may be better 1 year
functional outcomes based on ISAT & BRAT trials● Open surgery - clipping w craniotomy (bone replaced) or craniectomy
(not replaced)

19 / 22
Aneurysmal SAH: vasospasm
● Narrowing of imageable vessels post SAH● ~70% of patients● Course (from days post rupture):
– starts ~3-4 days– peak ~7-10 days– Resolves ~14-21 days
20 / 22
SAH: non-aneurysmal management
● Perimesencephalic– Treat as if aneurysmal until followup imaging
(including w nimodipine)● Unclear if nimodipine benefts, but little data
for harm● Hemispheric - do not need to treat with nimodipine● Traumatic:
– vasospasm not usually seen re nimodipine
– If severe TBI: 7 day course of anti-seizure drug recommended (along w consideration of EEG if coma)

21 / 22
SAH: prognosis
● ~25% patients estimated to die pre-hospital● ~50% overall mortality
srcs include: Blumenfeld

22 / 22
sources/refs● UpToDate
– Clinical manifestations and diagnosis of aneurysmal subarachnoid hemorrhage– Nonaneurysmal subarachnoid hemorrhage– Perimesencephalic nonaneurysmal subarachnoid hemorrhage– Subarachnoid hemorrhage grading scales– Treatment of aneurysmal subarachnoid hemorrhage– Management of acute severe traumatic brain injury
● Continuum 2015:– Diagnosis and Management of Subarachnoid Hemorrhage
● Neuroanatomy through Clinical Cases by Hal Blumenfeld, second edition 2010● Other articles:
– NEJM 2017 Subarachnoid hemorrhage article by Lawton & Vates, DOI: 10.1056/NEJMcp1605827
– Sensitivity of Early Brain Computed Tomography to Exclude Aneurysmal Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis. Dubosh et al. Stroke 2016. DOI: 10.1161/STROKEAHA.115.011386
– Avoiding pitfalls in the diagnosis of subarachnoid hemorrhage. Edlow and Caplan. NEJM 2000. DOI: 10.1056/NEJM200001063420106
– Should spectrophotometry be used to identify xanthochromia in the cerebrospinal fuid of alert patients suspected of having subarachnoid hemorrhage? Perry et al. 2006. Stroke. DOI: 10.1161/01.STR.0000240689.15109.47
● SAH image source: https://en.wikipedia.org/wiki/File:SubarachnoidP.png

















