Substrate mapping vs. tachycardia mapping using CARTO in patients with coronary artery disease and ventricular tachycardia: impact on outcome of catheter ablation Marius Volkmer, Feifan Ouyang, Florian Deger, Sabine Ernst, Masahiko Goya, Dietmar Ba ¨nsch, Katharina Berodt, Karl-Heinz Kuck, and Matthias Antz * Department of Cardiology, St Georg Hospital, Hamburg, Germany Received 22 June 2005; accepted after revision 26 July 2006 Aims For ablation of ventricular tachycardia (VT) in patients after myocardial infarction, a three- dimensional mapping system is often used. We report on our overall success rate of VT ablation using CARTO in 47 patients, with a subgroup analysis comparing VT mapping with the results of mapping that had to be performed during sinus rhythm or pacing (substrate mapping). Methods and results A CARTO map was performed and VT ablation attempted using two strategies: Patients in the VT-mapping group had incessant VT (four patients) or inducible stable VT (18 patients) such that the circuit of the clinical VTcould be reconstructed using CARTO. During VT, the critical area of slow conduction was identified using diastolic potentials and conventional concealed entrainment pacing. In contrast, patients in the substrate-mapping group had initially inducible VT. However, a com- plete VT map was not possible because of catheter-induced mechanical block (six patients) or because haemodynamics deteriorated during the ongoing VT (19 patients). Therefore, pathological myocardium was identified by fragmented, late- and/or low-amplitude (,1.5 mV) bipolar potentials during sinus rhythm or pacing, and the ablation site was primarily determined by pace mapping inside or at the border of this pathological myocardium. Acute ablation success in all patients with regard to non- inducibility of the clinical VT or any slower VT was 79% after a single ablation procedure, but increased to 95% after a mean of 1.2 ablation procedures. However, chronic success was 75%, when it was defined as freedom from any ventricular tachyarrhythmia (VT or VF) during a follow-up of 25 + 13 months. In the subgroup analysis, patients in the VT-mapping group were not significantly different from patients in the substrate-mapping group with regard to age (65+7 vs. 65+9 years), ejection fraction (30+7 vs. 30 + 8%), VT cycle length (448 + 81 vs. 429 + 82 ms), number of radiofrequency applications (17+9 vs. 14+6 applications), use of an irrigated tip catheter (23 vs. 32%), and ablation results. Conclusion When using a CARTO-guided approach for VT ablation in patients with coronary artery disease, the freedom from any ventricular arrhythmia is high (75%), but leaves the patient at a 23% risk of developing fast VT/VF during follow-up. Mapping during sinus rhythm or pacing is as successful as mapping during VT. KEYWORDS Catheter ablation; Ventricular tachycardia; Electroanatomical mapping; Internal defibrillator Introduction Catheter ablation in patients with ischaemic ventricular tachycardia (VT) based on conventional mapping techniques is associated with low success rates and is limited to patients with stable VT. 1 However, even these patients can be diffi- cult to treat by ablation if multiple morphologies are induced or if the target VT is mechanically blocked during mapping. Therefore, ,10% of patients with VT and coronary artery disease are suitable for catheter ablation. 2 However, the electroanatomical mapping system CARTO (Haifa, Israel) allows a three-dimensional anatomical reconstruction of the ventricles during sinus rhythm or pacing. This helps to ident- ify the substrate for VT by differentiating scar tissue, ana- tomical and functional barriers, and areas of slow conduction. 3 It has been shown that the application of linear lesions guided by CARTO can reduce VT episodes in patients with non-tolerated VT. 3,4 Combined sinus rhythm mapping and limited mapping during VT demonstrated a significant reduction of internal cardioverter and defibrillator (ICD) interventions in patients in whom the critical isthmus & The European Society of Cardiology 2006. All rights reserved. For Permissions, please e-mail: [email protected]* Corresponding author: II. Med. Abteilung, Asklepios Klinik St Georg, Lohmu ¨hlenstrasse 5, 20099 Hamburg, Germany. Tel: þ49 40 181885 2305; fax: þ49 40 181885 4444. E-mail address: [email protected]Europace (2006) 8, 968–976 doi:10.1093/europace/eul109 Downloaded from https://academic.oup.com/europace/article/8/11/968/573751 by guest on 02 February 2022
Transcript
Substrate mapping vs. tachycardia mapping using CARTOin patients with coronary artery disease and ventriculartachycardia: impact on outcome of catheter ablation
Marius Volkmer, Feifan Ouyang, Florian Deger, Sabine Ernst, Masahiko Goya, Dietmar Bansch,Katharina Berodt, Karl-Heinz Kuck, and Matthias Antz*
Department of Cardiology, St Georg Hospital, Hamburg, Germany
Received 22 June 2005; accepted after revision 26 July 2006
Aims For ablation of ventricular tachycardia (VT) in patients after myocardial infarction, a three-dimensional mapping system is often used. We report on our overall success rate of VT ablation usingCARTO in 47 patients, with a subgroup analysis comparing VT mapping with the results of mappingthat had to be performed during sinus rhythm or pacing (substrate mapping).Methods and results A CARTO map was performed and VT ablation attempted using two strategies:Patients in the VT-mapping group had incessant VT (four patients) or inducible stable VT (18 patients)such that the circuit of the clinical VT could be reconstructed using CARTO. During VT, the critical areaof slow conduction was identified using diastolic potentials and conventional concealed entrainmentpacing. In contrast, patients in the substrate-mapping group had initially inducible VT. However, a com-plete VT map was not possible because of catheter-induced mechanical block (six patients) or becausehaemodynamics deteriorated during the ongoing VT (19 patients). Therefore, pathological myocardiumwas identified by fragmented, late- and/or low-amplitude (,1.5 mV) bipolar potentials during sinusrhythm or pacing, and the ablation site was primarily determined by pace mapping inside or at theborder of this pathological myocardium. Acute ablation success in all patients with regard to non-inducibility of the clinical VT or any slower VTwas 79% after a single ablation procedure, but increasedto 95% after a mean of 1.2 ablation procedures. However, chronic success was 75%, when it was definedas freedom from any ventricular tachyarrhythmia (VTor VF) during a follow-up of 25+ 13 months. In thesubgroup analysis, patients in the VT-mapping group were not significantly different from patients in thesubstrate-mapping group with regard to age (65+7 vs. 65+9 years), ejection fraction (30+7 vs.30+ 8%), VT cycle length (448+ 81 vs. 429+ 82 ms), number of radiofrequency applications (17+9vs. 14+6 applications), use of an irrigated tip catheter (23 vs. 32%), and ablation results.Conclusion When using a CARTO-guided approach for VT ablation in patients with coronary arterydisease, the freedom from any ventricular arrhythmia is high (75%), but leaves the patient at a 23%risk of developing fast VT/VF during follow-up. Mapping during sinus rhythm or pacing is as successfulas mapping during VT.
KEYWORDSCatheter ablation;
Ventricular tachycardia;
Electroanatomical mapping;
Internal defibrillator
Introduction
Catheter ablation in patients with ischaemic ventriculartachycardia (VT) based on conventional mapping techniquesis associated with low success rates and is limited to patientswith stable VT.1 However, even these patients can be diffi-cult to treat by ablation if multiple morphologies areinduced or if the target VT is mechanically blocked duringmapping. Therefore, ,10% of patients with VT and coronary
artery disease are suitable for catheter ablation.2 However,the electroanatomical mapping system CARTO (Haifa, Israel)allows a three-dimensional anatomical reconstruction of theventricles during sinus rhythm or pacing. This helps to ident-ify the substrate for VT by differentiating scar tissue, ana-tomical and functional barriers, and areas of slowconduction.3
It has been shown that the application of linear lesionsguided by CARTO can reduce VT episodes in patients withnon-tolerated VT.3,4 Combined sinus rhythm mapping andlimited mapping during VT demonstrated a significantreduction of internal cardioverter and defibrillator (ICD)interventions in patients in whom the critical isthmus
& The European Society of Cardiology 2006. All rights reserved. For Permissions, please e-mail: [email protected]
ic.oup.com/europace/article/8/11/968/573751 by guest on 02 February 2022
could be identified.5 In many centres, VT ablation usingCARTO is attempted by performing a complete CARTO mapduring VT in all patients. However, this is not possible inthe majority of patients due to mechanical block of the VTby catheter manipulation or haemodynamic deteriorationduring long-lasting VT. We report on our overall successrate on VT ablation using CARTO in 47 patients, with a sub-group analysis comparing VT mapping with the results ofmapping that had to be performed during sinus rhythm orpacing (substrate mapping).
Methods
Patients
Over a period of 3 years, endocardial catheter mapping and radio-frequency (RF) current ablation were performed in 47 consecutivepatients (four females; mean age 65+8 years) with clinically sus-tained, haemodynamically tolerated monomorphic VT remote frommyocardial infarction (.3 months) by use of the electroanatomicalmapping system CARTO (Figure 1). Haemodynamic tolerance wasdefined as preservation of consciousness and no resuscitationrequired during the clinical arrhythmia. However, 22 patients(47%) had previously undergone ICD implantation, resulting in fastarrhythmia termination by the device. The median number of VTepisodes prior to ablation was 7 (range 1–930 episodes) within6 months prior to ablation. The locations of previous myocardialinfarctions were 22 inferior (10 aneurysms), 22 anterior (17 aneur-ysms), and three with both locations (Table 1).
At the time of study inclusion, 43 of 47 patients were onantiarrhythmic drug therapy. They received amiodarone alone(28 patients) or in combination with other antiarrhythmic drugs(seven patients), and eight were treated with sotalol.
Coronary angiography, left ventriculography, and transthoracicechocardiography were performed in all patients prior to the abla-tion. Written informed consent was obtained at least 24 h beforethe procedure.
Electrophysiological study
A conventional computerized electrophysiological (EP) system (EPLaboratory, Quinton Electrophysiology Corporation, Ontario,Canada) and the electroanatomical mapping system CARTO wereused. Patients were continuously monitored throughout the entireEP procedure by invasive systemic and pulmonary arterial pressure,non-invasive oxygen saturation, and urinary flow. The procedureswere performed under deep sedation using continuous pump infu-sion of propofol. For systemic anticoagulation, repeat bolus
injections of heparin based on ACT measurements were given(target value 250–300 s). The standard access to the left ventriclewas retrograde across the aortic valve (35 patients). In six patients,an antegrade transseptal access was used because of severe athero-sclerosis of the aorta or peripheral arteries, and in six furtherpatients, the LV was mapped via combined access because anatom-ical variations did not permit mapping of the entire left ventricle bythe retrograde approach alone.
Right ventricular stimulation
Programmed ventricular stimulation with up to three extrastimuli attwo different sites (right ventricular apex and outflow tract) wasperformed in an attempt to induce the clinical VT and/or anyother non-clinical VT. VT was considered clinical if either the12-lead morphology matched the previously documented VT or ifthe cycle length was within a range of +30 ms of the VT cyclelength documented by the ICD. If the induced VT led to haemo-dynamic deterioration within 2 min in the sedated patient, the VTwas considered unmappable (19 patients).
Mapping
Electroanatomical mappingMapping (and ablation) was performed using 7F steerable catheterswith either a conventional 4 mm tip (NaviStarTM) or a 3.5 mm irri-gated tip electrode (NaviStar ThermoCoolTM, Biosense-WebsterLtd, Diamond Bar, CA, USA). Spatial reference was obtained froma second sensor equipped catheter (RefStarTM, Biosense-WebsterLtd) placed on the patient’s back. Local activation time wasmeasured in relation to a time reference derived from an appropri-ate surface ECG lead. Mapping was performed in a bipolar recordingmode with a filter setting of 30–400 Hz.
Initial CARTO mapAn activation map and voltage map of the entire left ventricle wereperformed during sinus rhythm, atrial or right ventricular pacing inall patients except for those with incessant VT. Although the auto-matic annotation was set to maximum value, each electrogramwas re-annotated to the beginning of the local bipolar potential(reproducible pre-systolic or diastolic potentials were consideredas representing local activation, i.e. localized isolated channels).The voltage map was used in a bipolar mode for the identificationof sites with abnormal signals. Voltages of,1.5 mV were consideredabnormal. Scar tissue was considered at sites with no reproduciblelocal bipolar potential and, if in doubt, failure of bipolar pacingcapture with highest possible output (10 V, 2.9 ms pulse duration).The upper limit of the colour voltage display was set to 1.5 mVsuch that only normal tissue was coloured purple.3
Figure 1 Flow chart demonstrating the distribution of patients into the VT- mapping and substrate-mapping groups.
Substrate vs. CARTO mapping in ischaemic VT 969
Dow
nloaded from https://academ
ic.oup.com/europace/article/8/11/968/573751 by guest on 02 February 2022
Patients were divided into a VT-mapping group (patients withinducible or spontaneous VT, in whom the circuit of the clinical VTcould be reconstructed using CARTO) and a substrate-mappinggroup (patients in whom a complete VT map was not possiblebecause of catheter-induced mechanical block or because theinduced VT was unmappable due to haemodynamic deteriorationduring VT).
VT-mapping groupA complete activation and propagation map during the clinical and/or any other slower VTwas performed, and the setting of the anno-tation window was equal to the VT cycle length. The CARTO VT mapwas combined with conventional entrainment pacing at sites withdiastolic potentials according to the methods for entrainment aspreviously described.6–9
Substrate-mapping groupFollowing the initial map during sinus rhythm or right ventricularpacing, pace mapping in the left ventricle was performed. Siteswhere pace mapping matched the spontaneous VT morphology andwhere the delay between the stimulus and the onset of theQRS-complex was at least 50 ms were classified as potential targetsites within a protected isthmus. However, if the VT morphologywas matched without a delay of the stimulus to QRS interval, thesite was classified as an exit.9
In those patients in whom systematic VT mapping was not poss-ible, because the clinical VT became haemodynamically unstableunder sedation in the EP laboratory, the mapping catheter wasplaced at a potential target site during sinus rhythm or pacing.Then, the VT was induced, entrainment attempted, and RFcurrent applied as soon as diastolic activity was recorded. If theVT terminated within 30 s, the RF current application was
continued; if not, the RF current application was stopped and theVTwas terminated by overdrive pacing or external DC cardioversion.
Ablation strategies
In both the VT-mapping group and the substrate-mapping group,patients were treated with focal ablation (treatment with pointablation in an attempt to ablate a critical channel) and/or linearablation (lines placed inside the infarct or at its border, connectingelectrical barriers, or arranged in a cross-like fashion through theinfarct area).
Ablation settings
RF current (500 kHz) was applied between the distal electrode ofthe mapping catheter and a cutaneous patch electrode.Conventional RF applications were delivered using a temperature-controlled mode (maximum 608C; maximum 180 s; 30–50 W; EPshuttle, Cordis-Stockert Ltd, Freiburg, Germany). For irrigatedtip, RF applications 30–50 W were applied with a temperaturelimit of 458C at a cooling rate of 30 mL/min. The continuous flowduring mapping was 2 mL/min.
Endpoints and success of ablation
The endpoint of focal applications in the VT-mapping group was VTtermination by RF and in the substrate-mapping group, the elimin-ation of isolated potentials. The endpoint for linear ablation (linesor cross-lines) was the completion of the designed lines. Acutesuccess was defined as non-inducibility of the clinical VT and anyVT slower than the clinical VT, either at the end of the ablation pro-cedure (VT-mapping group) or in a repeat EP stimulation studybefore hospital discharge (substrate-mapping group), but allowed
Table 1 Patient characteristics and electrophysiological data
VT group (22 patients) Substrate group (25 patients) P-value
Previous ICD (%) 9 (41) 13 (52) 0.561Previous amiodarone alone or with other AAD (%) 17 (77) 18 (72) 0.747Previous sotalol (%) 4 (18) 4 (16) 1.000
Cycle length of clinical VTa 448+ 81 429+ 82 0.344Additional induced VTs (non-clinical)a 4+ 3 3+ 2 0.268LV volume during SR or pacing (mL)a 249+ 87 257+ 117 0.783Points in CARTO map (SR or pacing)a 173+ 81 217+ 87 0.170Points in CARTO map (VT)a 139+ 77 — —Applied lines, median (range)a 1 (0–5) 2 (0–3) 0.024Total length of lines (mm)a 50+ 35 64+ 36 0.137RF applicationsa 17+ 9 14+ 6 0.330Irrigated RF cathetera (%) 5 (23) 8 (32) 0.530Procedure time (min)a 524+ 150 474+ 124 0.272Fluoroscopy time (min)a 28+ 19 20+ 19 0.835
Follow-up time after hospital discharge (months) 24+ 12 (4–47) 26+ 14 (5–48) 0.696New ICD implanted (%) 8 (36) 6 (24) 0.524Total number of patients with ICD after ablation (%) 17 (77) 19 (76) 1.000Amiodarone alone or with other AAD after ablation (%) 14 (64) 11 (44) 0.244Sotalol after ablation (%) 2 (9) 2 (8) 1.000
AAD, antiarrhythmic drugs; SR, sinus rhythm.aFirst ablation procedure and re-ablations during follow-up.
970 M. Volkmer et al.
Dow
nloaded from https://academ
ic.oup.com/europace/article/8/11/968/573751 by guest on 02 February 2022
induction of fast VT (cycle length .30 ms faster than the clinical VT)or VF. In both groups, chronic success during follow-up was dividedinto freedom from targeted VTs (defined as no recurrence of the clini-cal VT or any VT slower than the clinical VT) and freedom from anyVT/VF (defined as no occurrence of sustained ventricular arrhythmia,including fast VT and ventricular fibrillation).
Management after ablation
Patients were monitored for at least 12 h in the intensive care unit.Continuous infusion of therapeutic heparin for 24 h was followed by100 mg/d aspirin or by oral anticoagulation with phenprocoumon.
A repeat stimulation study was scheduled 2 days (median) afterablation in the substrate-mapping group.
If during the same hospitalization a patient had a VT recurrenceafter the first ablation procedure was performed with a conven-tional 4 mm tip electrode, a repeat ablation was immediatelyperformed aiming at consolidating the initial ablation strategyusing an irrigated tip electrode. Since only limited mapping wasperformed during these repeat procedures, they were not includedinto the procedure-related data analysis (Table 1).
Follow-up
Follow-up started after hospital discharge and was performed every3 months in the ICD-outpatient clinic or by trans-telephonic evalu-ation of events provided by the patient and the referring physician.
Patients who underwent cardiac transplant or died non-arrhythmogenically were considered as having reached the end offollow-up, whereas patients who experienced an arrhythmogenicdeath were rated as an occurrence of VF. If patients died duringthe initial hospitalization, they were not part of the follow-up andtherefore were not considered in the chronic success rates.
Statistical analysis
Data mean+ standard deviation was used to describe continuousvariables with normal distribution; otherwise median and rangewere used. For diagnostic parameters, the absolute and relative fre-quencies were counted. In all cases, the statistics were calculatedusing non-parametric tests (Mann–Whitney, x2) and using Fisher’sexact method because the data set was small. A two-tailed prob-ability of ,0.05 was regarded as significant. The P-values were indi-vidually interpreted as exploratory. Statistics were calculated withSPSS 11.5 (SPSS Inc., Chicago, IL, USA).
Results
Entire patient cohort
In the initial right ventricular stimulation (performed in thepatients who did not have incessant VT), the clinical VTcould be induced in all patients with additional 3+2(range 1–10) non-clinical VT morphologies.In the 47 patients, a total of 61 ablation procedures
was performed (1.2+ 0.5; range one to four procedures).These include 14 repeat procedures due to VT recurrences,performed either during the same hospitalization (fourprocedures; in all of them, a conventional 4 mm tip elec-trode was used in the initial procedure) or during follow-up(10 procedures). An irrigated tip electrode was used in atotal of 17 of 61 (28%) procedures (13 initial procedures(Table 1) and in all four repeat procedures performedduring the same hospitalization).All patients discharged from the hospital completed a
follow-up period of at least 4 months. The mean follow-upperiod of the entire cohort was 25+ 13 months (range4–48 months). Thirty-six patients (77%) finally had an ICD.
Twenty-nine patients (62%) were treated with specific anti-arrhythmic drugs: 25 patients (86%) amiodarone and fourpatients (14%) sotalol.The acute ablation success in all patients with regard
to non-inducibility of the clinical or any slower VT was 79%(34/43) after a single ablation procedure and was unknownin four patients in the substrate-mapping group who didnot undergo repeat stimulation. A total of three patientsdied in hospital. During follow-up of the remaining44 patients, chronic success regarding freedom from theclinical VT or any slower VT was 95% (42/44) after all(1.2+ 0.5) ablation procedures in both groups. However,23% (10/44) of the patients had fast VT or ventricular fibril-lation during follow-up, and one of them (VT-mapping group)underwent successful linear re-ablation. Therefore, chronicsuccess regarding freedom from any sustained ventriculararrhythmia including fast VT and ventricular fibrillationwas 75% (33/44) after all ablation procedures.
VT-mapping group
In the 22 patients of the VT-mapping group, a CARTO map ofthe LV in sinus rhythm or pacing (18 patients; 173+ 81points, diastolic volume 249+ 87 mL) and during VT (22patients; 139+ 77 points) was obtained (Table 1). A criticalzone of slow conduction during VTwas identified in 20 of the22 patients by a combination of CARTO- and conventionalmapping techniques, and the VT was terminated with amedian of two RF pulses1–4 within this area (Figure 2). In16 patients, a median of one additional line (maximumfive lines) was applied to connect scar to scar and/or scarto the mitral annulus, and in three patients, a cross-lineablation was placed through the area with abnormal poten-tials (Figure 3). The mean length of all linear lesions was50+ 35 mm (range 20–158 mm). The mean number of RFpulses in the VT-mapping group was 17+9 (range 5–31).Ablation was acutely successful after the initial procedure
in 17 of 22 patients (77%) (Figure 4). Owing to early VTrecur-rence after the initial ablation with a conventional 4 mm tipelectrode, re-ablation using an irrigated catheter was per-formed at the same sites during the same hospitalizationin three patients, and this increased the acute successrate to 91% (20 of 22 patients). In two patients, the clinicalVT remained inducible at the end of the procedure, and bothwere discharged with an ICD and antiarrhythmic drug treat-ment. In five patients, the previous antiarrhythmic drugtreatment was discontinued and in five modified. Eightpatients received a new ICD after ablation because ofseverely impaired LV function and induction of rapid VTs.During a total follow-up of 24+ 12 months after hospital
discharge in the VT-mapping group (range 4–47 months), thetwo patients in whom the clinical VT remained inducible hadrecurrences of that arrhythmia. However, VTwas frequent inonly one of them requiring linear re-ablation 6 months later,resulting in no more VT during further follow-up of 27months when he died of cancer. Two other patients had aslower VT (compared with the clinical VT) after hospital dis-charge and underwent successful linear re-ablation usingCARTO at 1 month and at 18 months, with no more VT recur-rences during further follow-up. A total of five patients hadfast VT (.30 ms faster than the clinical VT) in hospital (onepatient) or fast VT/VF during follow-up after hospitaldischarge (four patients). The fast VT/VF was controlled
Substrate vs. CARTO mapping in ischaemic VT 971
Dow
nloaded from https://academ
ic.oup.com/europace/article/8/11/968/573751 by guest on 02 February 2022
by the ICD in three patients, and two patients with a stablebut different and faster VT (compared with the clinical VT)underwent a repeat CARTO-guided ablation procedure whilestill in hospital (after 7 days) or during outpatient follow-up(at 11 months).
In the VT-mapping group, there was a total of four deaths.Two patients died in the hospital 2 and 28 days after the pro-cedure: one patient was referred for ablation of an inces-sant VT and septic shock following a massive anterior wallmyocardial infarction, and the ablation procedure was per-formed as a measure of last resort. The VTwas ablated suc-cessfully, but the patient died 2 days afterwards due to thesepsis. The second patient died in the hospital, 28 days afterthe initial procedure, of heart failure and sepsis without VTrecurrence after the second ablation procedure using anirrigated tip catheter. In two patients, late death of non-cardiac cause occurred 26 and 27 months post-ablation.
Substrate-mapping group
In 25 patients, only a CARTO map during sinus rhythm orpacing was performed either because the sedated patientbecame haemodynamically unstable during the ongoing VTin the EP laboratory (19 patients) or a long-lasting mechan-ical block of the target VToccurred (six patients) (Figure 1).A mean of 217+ 87 points were acquired to reconstruct theLV (diastolic volume 257+ 117 mL). Ablation with 14+ 6RF-applications was performed to block protected channelsinside the infarct (,1.5 mV bipolar amplitude) or at itsborder, as well as to connect scar to scar and/or scar tothe mitral annulus. A median of two lines (maximum of
Figure 2 Activation map of the left ventricle during incessant VT (cycle length 420 ms) displayed in a right anterior oblique projection.Colours represent activation time relative to the S-wave in V3. The His-bundle area is marked by an orange dot. Diastolic potentials werefound in the septal area and are marked by pink dots. These potentials span the entire diastole, marked by the red lined box (right).Entrainment pacing confirmed a ‘figure of eight’ re-entry circuit, with a septal area of slow conduction. Ablation at the VT exit site (reddots) successfully eliminated the VT.
Figure 3 Bipolar voltage map of the left ventricle (anteroposteriorprojection). Normal voltages (.1.5 mV) are colour coded in purple,and abnormal low-amplitude potentials are colour coded in blue tored (the latter representing the lowest amplitudes). Scar (no repro-ducible local bipolar potential and failure of bipolar pacing capturewith highest possible output) is grey. Pathological bipolar potentialsand scar are found anterior apical, consistent with a previousanterior myocardial infarction. A cross-line ablation is placedthrough the area with abnormal potentials (red dots).
972 M. Volkmer et al.
Dow
nloaded from https://academ
ic.oup.com/europace/article/8/11/968/573751 by guest on 02 February 2022
three lines) was performed, with a mean length of all linesof 64+ 36 mm (range 25–141 mm).In a total of four patients in the substrate-mapping group,
a non-clinical slow VT was reproducibly induced. In all ofthese patients, a CARTO-VT map was obtained and the VTwas successfully ablated.After the initial procedure, ablation was acutely success-
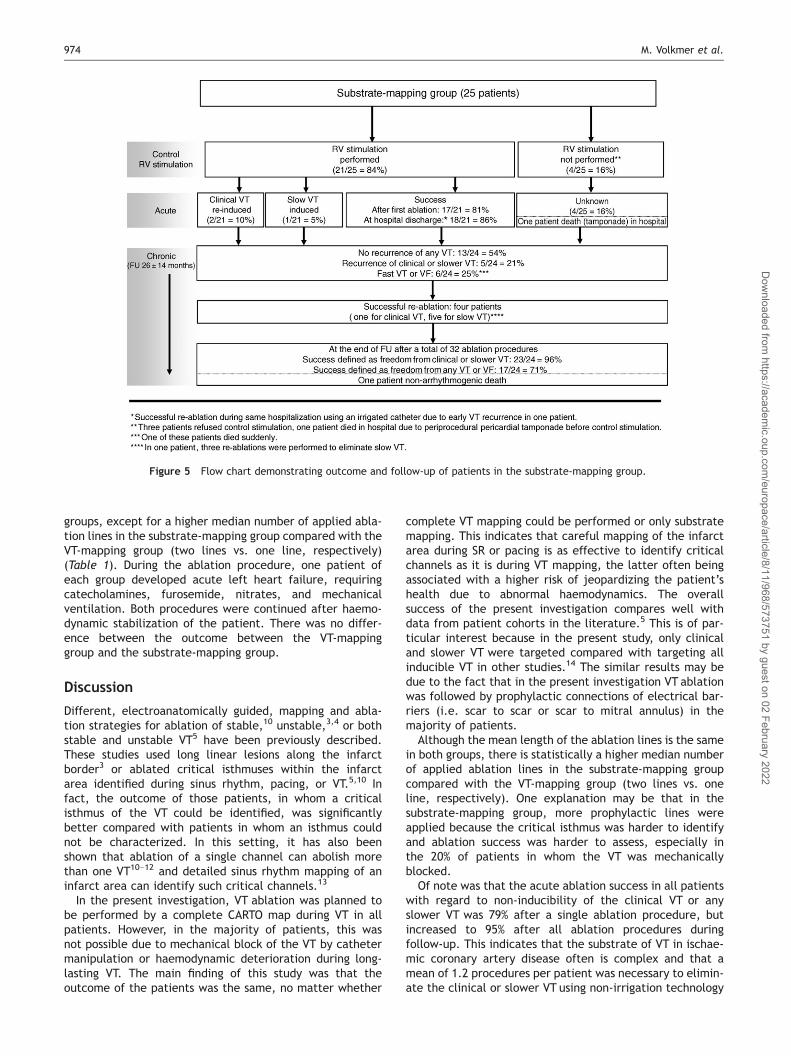
ful in 17/21 patients (81%) who had a repeat EP study (threepatients refused a second RV stimulation, and one patienthad died due to periprocedural pericardial tamponade)(Figure 5). Owing to early VTrecurrence after an initial abla-tion with a conventional 4 mm tip electrode, re-ablationusing an irrigated tip catheter was performed at the samesites during the same hospitalization in one patient, andthis increased the acute success rate to 18/21 patients(86%). In three patients, the clinical VT (two patients) or aslower VT (one patient) was inducible at control stimulation(Figure 5). Previous antiarrhythmic drug therapy was discon-tinued in nine patients and modified in two patients. Sixpatients received an ICD after ablation because of impairedLV function and induction of rapid VT.During a total follow-up after hospital discharge of
26+ 14 months (range 5–48 months) in the substrate-mapping group, one of the two patients with inducible clini-cal VT had no recurrence and the other had a single episodeof VF, successfully terminated by his ICD. Including the latterpatient, a total of six patients in the substrate-mappinggroup had fast VT (.30 ms faster than the clinical VT) orVF during follow-up. Of these patients, five were controlledwith antiarrhythmic drugs and ICD, whereas one femalepatient died unwitnessed (probably suddenly). Duringfollow-up, five other patients had recurrences of the clinical
or slower VT: the patient with the slow VT inducible atrepeat stimulation had recurrences of that VT (underwentthree, finally successful re-ablations of that arrhythmiaduring follow-up). One of the patients who had refusedrepeat stimulation had recurrence of the clinical VT (under-went successful re-ablation during follow-up), and three ofthe acutely successful ablated patients developed a newslow VT that was different from the original clinical VT(two of these patients underwent successful re-ablation,whereas one patient did not, because the VTs were wellmanaged by the antitachycardia pacing of his ICD, and heis listed for heart transplantation because of severe heartfailure).In the substrate-mapping group, one patient underwent
heart transplantation 17 months after ablation without anyVT recurrences, and a total of three patients died: onepatient died in the hospital the night after the procedurefrom electromechanical dissociation after cardiac tampo-nade. Another patient died 17 months after ablation frompump failure after re-infarction without arrhythmias.The above mentioned female patient who died unwitnessedduring sleep 8 months after the procedure was a patientwith an anterior wall infarct, an ejection fraction of40%, and a clinical VT cycle length of 410 ms, which wasnot re-inducible at the control EP study, who refused anICD or antiarrhythmic drugs other than a beta-blocker(metoprolol).
VT-mapping group vs. substrate-mapping group
There were no statistical differences in the comparison ofdemographic data and procedure parameters of the two
Figure 4 Flow chart demonstrating outcome and follow-up of patients in the VT-mapping group.
Substrate vs. CARTO mapping in ischaemic VT 973
Dow
nloaded from https://academ
ic.oup.com/europace/article/8/11/968/573751 by guest on 02 February 2022
groups, except for a higher median number of applied abla-tion lines in the substrate-mapping group compared with theVT-mapping group (two lines vs. one line, respectively)(Table 1). During the ablation procedure, one patient ofeach group developed acute left heart failure, requiringcatecholamines, furosemide, nitrates, and mechanicalventilation. Both procedures were continued after haemo-dynamic stabilization of the patient. There was no differ-ence between the outcome between the VT-mappinggroup and the substrate-mapping group.
Discussion
Different, electroanatomically guided, mapping and abla-tion strategies for ablation of stable,10 unstable,3,4 or bothstable and unstable VT5 have been previously described.These studies used long linear lesions along the infarctborder3 or ablated critical isthmuses within the infarctarea identified during sinus rhythm, pacing, or VT.5,10 Infact, the outcome of those patients, in whom a criticalisthmus of the VT could be identified, was significantlybetter compared with patients in whom an isthmus couldnot be characterized. In this setting, it has also beenshown that ablation of a single channel can abolish morethan one VT10–12 and detailed sinus rhythm mapping of aninfarct area can identify such critical channels.13
In the present investigation, VT ablation was planned tobe performed by a complete CARTO map during VT in allpatients. However, in the majority of patients, this wasnot possible due to mechanical block of the VT by cathetermanipulation or haemodynamic deterioration during long-lasting VT. The main finding of this study was that theoutcome of the patients was the same, no matter whether
complete VT mapping could be performed or only substratemapping. This indicates that careful mapping of the infarctarea during SR or pacing is as effective to identify criticalchannels as it is during VT mapping, the latter often beingassociated with a higher risk of jeopardizing the patient’shealth due to abnormal haemodynamics. The overallsuccess of the present investigation compares well withdata from patient cohorts in the literature.5 This is of par-ticular interest because in the present study, only clinicaland slower VT were targeted compared with targeting allinducible VT in other studies.14 The similar results may bedue to the fact that in the present investigation VT ablationwas followed by prophylactic connections of electrical bar-riers (i.e. scar to scar or scar to mitral annulus) in themajority of patients.
Although the mean length of the ablation lines is the samein both groups, there is statistically a higher median numberof applied ablation lines in the substrate-mapping groupcompared with the VT-mapping group (two lines vs. oneline, respectively). One explanation may be that in thesubstrate-mapping group, more prophylactic lines wereapplied because the critical isthmus was harder to identifyand ablation success was harder to assess, especially inthe 20% of patients in whom the VT was mechanicallyblocked.
Of note was that the acute ablation success in all patientswith regard to non-inducibility of the clinical VT or anyslower VT was 79% after a single ablation procedure, butincreased to 95% after all ablation procedures duringfollow-up. This indicates that the substrate of VT in ischae-mic coronary artery disease often is complex and that amean of 1.2 procedures per patient was necessary to elimin-ate the clinical or slower VT using non-irrigation technology
Figure 5 Flow chart demonstrating outcome and follow-up of patients in the substrate-mapping group.
974 M. Volkmer et al.
Dow
nloaded from https://academ
ic.oup.com/europace/article/8/11/968/573751 by guest on 02 February 2022
in the majority of procedures (72%). In addition, the risk ofclinical occurrence of faster VT remained in 23% of ourpatients after hospital discharge such that additional ICDimplantation may be necessary. This conclusion has alsobeen suggested by Zado et al.15 who found that the riskfor spontaneous rapid VT after successful ablation of stableischaemic VT by use of conventional ablation technologywas 10% in a series of 50 patients.
Limitations
The index arrhythmia was considered a stable VT if thepatient remained conscious and needed no resuscitationduring the clinical arrhythmia. However, 22 patients (47%)had previously undergone ICD implantation, resulting infast arrhythmia termination by the device. As a result, ourpatient cohort may also include some ICD patients withunstable VT, who were terminated by their ICD beforethey could have led to unconsciousness.The present study was not a randomized investigation
comparing prospectively VT-mapping and substratemapping. In most of the patients of both groups, prophylac-tic linear RF ablations were applied for connection of elec-trical barriers, or ablation targeted diastolic potentialsduring sinus rhythm or pacing, suggesting areas of slow con-duction. The identical outcome of both groups may berelated to these additional prophylactic lines.Another limitation may be that irrigated tip ablation
was used in only 28% of procedures, however, to the sameextent in both groups. A higher success rate may beexpected if irrigated technology was used in more patientsbecause this would result in deeper and larger lesions andtherefore a more effective substrate modification andchannel elimination.16,17 In the four patients with an earlyrecurrence during the same hospital stay, all the initialablations had been performed using a conventional 4 mmtip electrode. The use of the irrigated tip catheter duringthe re-ablation procedure at the same sites consolidatedthe previously produced lesions, which were mostlikely smaller and shallower. If the irrigated catheter hadbeen used in the initial ablation, it is very likely that thiswould have prevented early VT recurrence. It, therefore,seems justified to combine both the conventional and theirrigated ablation procedures and rate them as acutesuccess.Our hospital policy to ablate only the clinical or slower VT,
but not faster VT, may have led to a lower success ratecompared with centres which target all induced VT mor-phologies. The rationale for not targeting the faster VTwas that they must have a shorter zone of slow conductionthan the clinical VT and that the ICD could be easily pro-grammed for their effective termination.Since it is sometimes difficult to differentiate between a
focal ablation, an enlarged focal ablation, and a linear abla-tion, we refrained from differentiating between theseapproaches, especially since there was no statistical differ-ence between groups.Comparing VT mapping and substrate mapping may be cri-
ticized because there is some heterogeneity from non-systematic variation in lesion strategy (focal/linear), abla-tion delivery (conventional/cooled-tip), using limited VTinduction and entrainment criteria in the substrate-mappinggroup and not targeting VTs faster than the clinical VT.
However, since focal and linear ablations, as well as irri-gated ablations, were used in both groups to the sameextent with identical endpoints, a subgroup analysis seemspossible. This is especially so since haemodynamic instabilityduring the ongoing VT and mechanical block of the clinicalVT by catheter ablation is clinically relevant. For the treat-ing physician, it is important to realize that even if the VTcannot be mapped with CARTO, the outcome was thesame, which may actually lead to the assumption that acomplete three-dimensional VT map is not necessary inany patient undergoing VT ablation.
Conclusion
When using a CARTO-guided approach for VT ablation inpatients with coronary artery disease, the freedom fromany ventricular arrhythmia is high (75%). However, thepatient has a residual 23% risk of developing fast VT/VFduring follow-up. Mapping during sinus rhythm or pacing isas successful as mapping during VT.
Acknowledgements
The authors would like to thank Sigrid Boczor for the biometriccalculations and Detlef Hennig for technical assistance.
References
1. Della Bella P, De Ponti R, Uriarte JA, Tondo C, Klersy C, Carbucicchio Cet al. Catheter ablation and antiarrhythmic drugs for haemodynamicallytolerated post-infarction ventricular tachycardia; long-term outcome inrelation to acute electrophysiological findings. Eur Heart J 2002;23:414–24.
2. Kim YH, Sosa-Suarez G, Trouton TG, O’Nunain SS, Osswald S,Mc Govern BA et al. Treatment of ventricular tachycardia by trans-catheter radiofrequency ablation in patients with ischemic heartdisease. Circulation 1994;89:1094–102.
3. Marchlinski FE, Callans DJ, Gottlieb CD, Zado E. Linear ablation lesionsfor control of unmappable ventricular tachycardia in patients withischemic and nonischemic cardiomyopathy. Circulation 2000;101:1288–96.
4. Sra J, Bhatia A, Dhala A, Blanck Z, Deshpande S, Cooley R et al.Electroanatomical guided catheter ablation of ventricular tachycardiascausing multiple defibrillator shocks. Pacing Clin Electrophysiol 2001;24:1645–52.
5. Soejima K, Suzuki M, Maisel WH, Brunckhorst CB, Delacretaz E, Blier Let al. Catheter ablation in patients with multiple and unstable ventri-cular tachycardias after myocardial infarction. Circulation 2001;104:664–9.
6. Stevenson WG, Khan H, Sager P, Saxon LA, Middlekauff HR, Natterson PDet al. Identification of reentry circuit sites during catheter mapping andradiofrequency ablation of VT late after myocardial infarction.Circulation 1993;88:1647–70.
7. Stevenson WG, Sager PT, Natterson PD, Saxon LA, Middlekauff HR,Wiener I. Relation of pace mapping QRS configuration and conductiondelay to ventricular tachycardia reentry circuits in human infarct scars.J Am Coll Cardiol 1995;26:481–8.
8. Kuck K-H, Schluter M, Geiger M, Siebels J. Successful catheter ablation ofhuman ventricular tachycardia with radiofrequency current guided by anendocardial map of the area of slow conduction. Pacing ClinElectrophysiol 1991;14:1060–71.
10. Chillou C, Lacroix D, Klug D, Magnin-Poull I, Marquie C, Messier M et al.Isthmus characteristics of reentrant ventricular tachycardia after myo-cardial infarction. Circulation 2002;105:726–31.
11. Wilber DJ, Kopp DE, Glaskock DN, Kinder CA, Kall JG. Catheter ablation ofthe mitral isthmus for ventricular tachycardia associated with inferiorinfarction. Circulation 1995;92:3481–89.
Substrate vs. CARTO mapping in ischaemic VT 975
Dow
nloaded from https://academ
ic.oup.com/europace/article/8/11/968/573751 by guest on 02 February 2022
12. Hadjis TA, Stevenson WG, Harada T, Friedman PL, Sager P, Saxon LA.Preferential locations for critical reentry circuit sites causing ventriculartachycardia after inferior wall myocardial infarction. J CardiovascElectrophysiol 1997;8:363–70.
13. Reddy VY, Neuzil P, Taborsky M, Ruskin JN. Short-term results ofsubstrate mapping and radiofrequency ablation of ischemic ventriculartachycardia using a saline-irrigated catheter. J Am Coll Cardiol 2003;41:2228–36.
14. Borger van der Burg AE, de Groot NM, van Erven L, Bootsma M, van derWall EE, Schalij MJ. Long-term follow-up after radiofrequency catheterablation of ventricular tachycardia: a successful approach? J CardiovascElectrophysiol 2002;13:417–23.
15. Zado ES, Gottlieb CD, Callans DJ, Coyne RF, Man DC, Sarter BH et al.‘Successful’ ventricular tachycardia catheter ablation: an argument forhaving defibrillator backup. (Abstract). Circulation 1997;96:I–319.
16. Watanable I, Masaki R, Min N, Oshikawa N, Okubo K, Sugimura H et al.Cooled-tip ablation results in increased radiofrequency power deliveryand lesion size in canine heart: importance of catheter-tip temperaturemonitoring for prevention of popping and impedance rise. J Interv CardElectrophysiol 2002;6:9–16.
17. Soejima K, Delacretaz E, Suzuki M, Brunckhorst CB, Maisel WH,Friedman PL et al. Saline-cooled versus standard radiofrequency cath-eter ablation for infarct-related ventricular tachycardia. Circulation2001;103:1858–62.
976 M. Volkmer et al.
Dow
nloaded from https://academ
ic.oup.com/europace/article/8/11/968/573751 by guest on 02 February 2022








![Advanced Mapping and Navigation Techniques for ...[14]Spitzer SG, Karolyi L. Ablation of typical atrial flutter with ultrasound 3D RPM mapping (abstract). Europace. 2001; (Suppl B):](https://static.documents.pub/doc/80x56/607c8126d5e0863e9209774b/advanced-mapping-and-navigation-techniques-for-14spitzer-sg-karolyi-l-ablation.jpg)















