81 Case Report Kitasato Med J 2017; 47: 81-86 Received 30 November 2016, accepted 19 December 2016 Correspondence to: Takashi Ishida, Department of Hematology, Kitasato University School of Medicine 1-15-1 Kitasato, Minami-ku, Sagamihara, Kanagawa 252-0374, Japan E-mail: [email protected]Successful treatment with ibrutinib of intractable thrombocytopenia associated with recurrent chronic lymphocytic leukemia Takashi Ishida, 1 Maki Yokoyama, 2 Mikio Danbara, 1 Yusuke Michishita, 1 Ryouichi Horie, 3 Masaaki Higashihara, 1 Koji Miyazaki 4 1 Department of Hematology, Kitasato University School of Medicine 2 Department of Hematology, Kitasato University Graduate School of Medical Science 3 Department of Hematology, Kitasato University School of Allied Health Sciences 4 Department of Transfusion and Cell Transplantation, Kitasato University School of Medicine Chronic lymphocytic leukemia (CLL) is characterized by lymphocytosis with mild progression, although some CLL patients develop fatal cytopenia. This report describes a 69-year-old Japanese man with CD8 + CD19 + CLL presenting with severe thrombocytopenia. Because he showed extreme resistance to various conventional regimens, we administered a novel agent, ibrutinib. Besides a striking reduction in CLL cells, thrombocytes rapidly recovered within 1 to 2 weeks after treatment. This report suggests that ibrutinib may be clinically useful for such patients. Additionally, as CD8 is rarely expressed in B- CLL cells, it is crucial to accumulate such cases for further evaluations. Key words: ibrutinib, thrombocytopenia, chronic lymphocytic leukemia, CD8 Introduction hronic lymphocytic leukemia (CLL) is characterized by the neoplastic proliferation of lymphocytes, with generally slow progression and an asymptomatic history. However, some CLL patients develop severe anemia and thrombocytopenia following repeat disease recurrence, possibly through autoimmune reactions mediated mostly by nonmalignant B cells. 1,2 Severe cytopenia is a serious complication in these patients, with a prevalence of 0.13%. 2 Thus, appropriate and immediate treatment of CLL itself is required to reduce bleeding complications. In contrast, emergency therapeutic options are limited, usually consisting only of transfusions. The present report describes a 69-year-old Japanese man with CD8 + /CD19 + CLL accompanied by intractable thrombocytopenia (platelet count <3,000/ μl), despite transfusions for 25 consecutive days. Because this patient showed extreme resistance to various conventional regimens, we thus administered a novel agent, ibrutinib. Although ibrutinib may provide better outcomes than other salvage treatments, 3,4 its effects in CLL-related cytopenia remain largely unknown. We here report a possible benefit of ibrutinib for such patients. Moreover, we also found that CLL cells in this patient were positive for expression of both CD8 and CD19. Given that the significance of CD8 expression in B-CLL patients remains to be determined, 5 it is therefore important to report such cases for further investigations. Case Report A 69-year-old Japanese man first diagnosed with CLL 14 years earlier was admitted to our hospital for severe thrombocytopenia with CLL progression, characterized by lymphocytosis and lymphadenopathy. This was the sixth such recurrence in this patient's history. Formerly, the patient was treated with fludarabine, cyclophosphamide, rituximab, bendamustine, pulsed methylprednisolone, and ofatumumab. During his previous relapse, he exhibited thrombocytopenia that led to severe hematoma at the dorsal pancreas. He underwent interventional radiology to prevent active bleeding and recurrent bleeding complications were in adequately controlled. Within 2 weeks of starting ofatumumab, he showed marked recovery of platelet counts, to around 110,000/ μ l. Nevertheless, maintenance treatment with ofatumumab became ineffective, with thrombocytopenia (platelet count <10,000/ μ l) becoming evident 6 months later. At the time of admission, his CLL status was C
Transcript
81
Case Report Kitasato Med J 2017; 47: 81-86
Received 30 November 2016, accepted 19 December 2016Correspondence to: Takashi Ishida, Department of Hematology, Kitasato University School of Medicine1-15-1 Kitasato, Minami-ku, Sagamihara, Kanagawa 252-0374, JapanE-mail: [email protected]
Successful treatment with ibrutinib of intractable thrombocytopeniaassociated with recurrent chronic lymphocytic leukemia
Ryouichi Horie,3 Masaaki Higashihara,1 Koji Miyazaki4
1 Department of Hematology, Kitasato University School of Medicine2 Department of Hematology, Kitasato University Graduate School of Medical Science3 Department of Hematology, Kitasato University School of Allied Health Sciences4 Department of Transfusion and Cell Transplantation, Kitasato University School of Medicine
Chronic lymphocytic leukemia (CLL) is characterized by lymphocytosis with mild progression, althoughsome CLL patients develop fatal cytopenia. This report describes a 69-year-old Japanese man withCD8+ CD19+ CLL presenting with severe thrombocytopenia. Because he showed extreme resistanceto various conventional regimens, we administered a novel agent, ibrutinib. Besides a striking reductionin CLL cells, thrombocytes rapidly recovered within 1 to 2 weeks after treatment. This report suggeststhat ibrutinib may be clinically useful for such patients. Additionally, as CD8 is rarely expressed in B-CLL cells, it is crucial to accumulate such cases for further evaluations.
hronic lymphocytic leukemia (CLL) is characterizedby the neoplastic proliferation of lymphocytes, with
generally slow progression and an asymptomatic history.However, some CLL patients develop severe anemia andthrombocytopenia following repeat disease recurrence,possibly through autoimmune reactions mediated mostlyby nonmalignant B cells.1,2 Severe cytopenia is a seriouscomplication in these patients, with a prevalence of0.13%.2 Thus, appropriate and immediate treatment ofCLL itself is required to reduce bleeding complications.In contrast, emergency therapeutic options are limited,usually consisting only of transfusions.
The present report describes a 69-year-old Japaneseman with CD8+/CD19+ CLL accompanied by intractablethrombocytopenia (platelet count <3,000/μl), despitetransfusions for 25 consecutive days. Because this patientshowed extreme resistance to various conventionalregimens, we thus administered a novel agent, ibrutinib.Although ibrutinib may provide better outcomes thanother salvage treatments,3,4 its effects in CLL-relatedcytopenia remain largely unknown. We here report apossible benefit of ibrutinib for such patients. Moreover,we also found that CLL cells in this patient were positive
for expression of both CD8 and CD19. Given that thesignificance of CD8 expression in B-CLL patientsremains to be determined,5 it is therefore important toreport such cases for further investigations.
Case Report
A 69-year-old Japanese man first diagnosed with CLL14 years earlier was admitted to our hospital for severethrombocytopenia with CLL progression, characterizedby lymphocytosis and lymphadenopathy. This was thesixth such recurrence in this patient's history.
Formerly, the patient was treated with fludarabine,cyclophosphamide, rituximab, bendamustine, pulsedmethylprednisolone, and ofatumumab. During hisprevious relapse, he exhibited thrombocytopenia that ledto severe hematoma at the dorsal pancreas. He underwentinterventional radiology to prevent active bleeding andrecurrent bleeding complications were in adequatelycontrolled. Within 2 weeks of starting ofatumumab, heshowed marked recovery of platelet counts, to around110,000/μl. Nevertheless, maintenance treatment withofatumumab became ineffective, with thrombocytopenia(platelet count <10,000/μl) becoming evident 6 monthslater. At the time of admission, his CLL status was
C
82
Ishida T. et al.
Figdure 1. Flow cytometry analysis (A. top, left) of CLL tumor cells and (B. bottom, left) mononuclear cells in thepatient in the present report. Two color graphs were generated: (A. top, right) CD19 (Y-axis) and CD8 (X-axis), and(B. bottom, right) with CD25 (Y-axis) and FOXP3 (X-axis).
Figure 2. Immunofixation electrophoresis upon admission
83
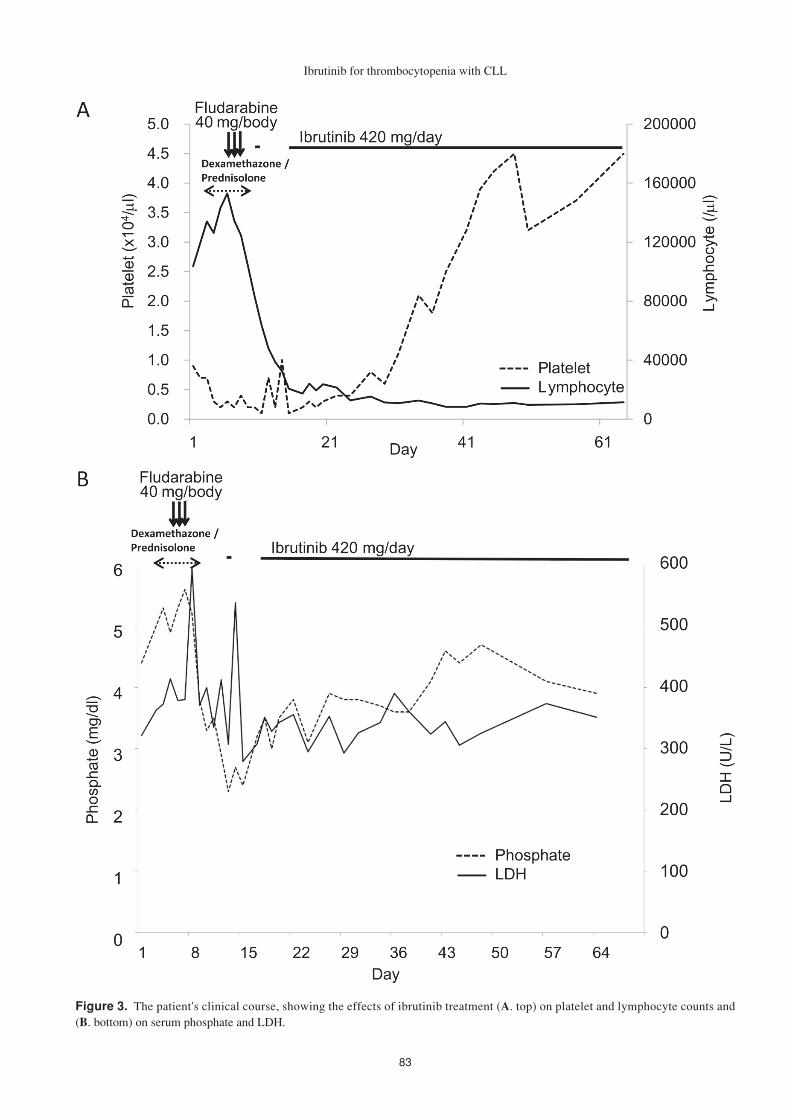
Figure 3. The patient's clinical course, showing the effects of ibrutinib treatment (A. top) on platelet and lymphocyte counts and(B. bottom) on serum phosphate and LDH.
Ibrutinib for thrombocytopenia with CLL
84
Ishida T. et al.
found to be Rai classification IV and Binet classificationC, with factors indicating poor prognosis, in that he wasCD38 positive and had an elevated level of serum β2-microglobulin. A blood test at admission showed amarked increase in lymphocyte count, 108,000/μl(normal range: 1,200−3,690/μl); anemia, 9.9 g/dl(normal range: 11.5−15.0 g/dl), an increased level oflactate dehydrogenase (LDH), 322 U/l (normal range:119−229 U/l); a normal uric acid (UA) level, 6.4 mg/dl(normal range: 2.4−7.0 mg/dl); a slightly elevated serum
phosphate level, 4.4 mg/dl (normal range: 2.5−4.7 mg/dl) and severe thrombocytopenia, 0.9 × 104/μl(normalrange: 16.0−39.0 × 104/μl). These findings suggestedself-destruction of tumor cells due to severe diseaseprogression. Over the next 3 days, he showed furtherprogression of both lymphocytosis (>140,000/μl) andthrombocytopenia (<0.3 × 104/μl). Direct and indirectCoombs tests were both negative, and there were no signsof collagen diseases; elevations of anti-nucleatedantibody, anti-double strand DNA IgG, anti-Sm/SS-A/
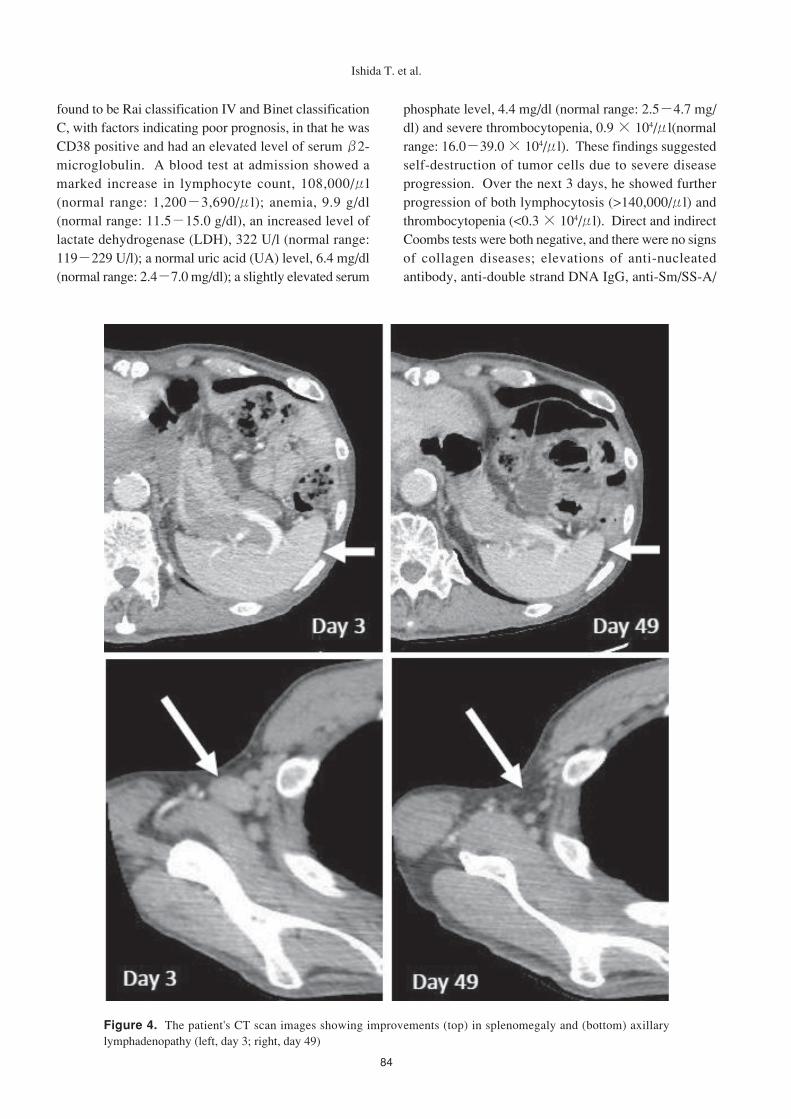
Figure 4. The patient's CT scan images showing improvements (top) in splenomegaly and (bottom) axillarylymphadenopathy (left, day 3; right, day 49)
85
SS-B antibody, lupus anticoagulant, anti-CL β2GPI, orCL-IgG. He also manifested a high fever andmucopercutaneous hemorrhages. Bone marrowaspiration showed a marked increase in lymphocytesexhibiting CLL markers, including CD5+, CD10-, CD19+,CD20-, CD23+, CD38+, and CD52+ phenotype and skewedkappa chain production. Flow cytometry also showedthat these CLL cells were CD8+ B cells (Figure 1A).Immunofixation electrophoresis showed the presence ofM protein, IgM kappa type (Figure 2). Computedtomography (CT) at admission showed cervical,mediastinal, hilar, peritoneal, and retroperitoneallymphadenopathy and splenomegaly. Although weinitially administered dexamethasone 16.5 mg/day for 5days with supportive treatment, including antibiotics,intravenous immunoglobulin, and platelet transfusions;the effects on lymphocytosis and thrombocytopenia wereonly marginal. For the preparation of the treatment withibrutinib, a novel agent that inhibits Bruton's tyrosinekinase (BTK), we administered fludarabine (40 mg/day)for 3 days to reduce absolute lymphocyte numbers.Although fludarabine lowered the total white blood cellcount in this patient, it did not affect the relativelymphocyte ratio, which remained at approximately 95%.Thrombocytopenia (<3,000/μl) also persisted despitecontinuous transfusions. While CD52 was expressed onCLL cells in the present case, the study by Byrd et al.6
reporting that ibrutinib was more effective thanalemtuzumab for refractory CLL patients convinced usto use ibrutinib for the present patient.
Administration of ibrutinib (420 mg/day) resulted inthe rapid disappearance of oral and urinary hemorrhageswithin a few days, prior to a recovery of thrombocytes.Platelet numbers also gradually increased, to 11,000/μlat 2 weeks and 25,000/μl at 3 weeks after starting ibrutinib(Figure 3A). Platelet transfusions were less frequent andwere deemed unnecessary after day 20. The levels ofserum phosphate and LDH had also decreased (Figure3B). No adverse effects of ibrutinib, such as liverdysfunction, arrhythmia, severe cytoreduction, or infectionwere observed. The reduction in malignant CLL cellswas accompanied by a marked recovery of T lymphocytes,reflecting a correction of lymphohematopoiesis. CT scansalso showed marked improvements in systemiclymphadenopathy and splenomegaly (Figure 4).Collectively, these findings indicate that the benefits ofibrutinib included the rapid recovery of CLL mediatedautoimmune thrombocytopenia as well as a decrease inCLL clones.
Discussion
CLL generally progress slowly and does not requireemergency treatment. This report describes a patientwith recurrent CLL who experienced life-threateningthrombocytopenia. Intriguingly, the B-CLL cells in thispatient displayed aberrant expressions of CD8. Thefrequency of CD8+ B cells in CLL patients has beenreported to be less than 1%.7 Although CD8+ B cellshave been reported associated with poor prognosis,7 thisfinding was not supported by the results of another study.5
Thus, to date, it is unclear whether the aberrant expressionof CD8 is an aggressive disease marker for CLL. Indeed,although our patient showed a trend toward aggressivedisease progression, the expression of CD8 on his CLLcells before and after ibrutinib treatment did not differsignificantly, suggesting that CD8 was not indicative ofdisease status or responsiveness to treatment, at least inthis patient.
The underlying mechanisms causing CLL relatedthrombocytopenia have not yet been determined.However, autoimmunity in CLL may be related toprevious treatment with purine analogues and alkylatingagents.1 Fludarabine therapy may mediate the suppressionof regulatory T cells, leading to the production ofautoreactive T cells.8,9 Even though the patient had beentreated with these agents, his peripheral blood regulatoryT cell count did not increase after ibrutinib (Figure 1B).
Several mechanisms of action of ibrutinib in CLLrelated thrombocytopenia have been proposed. Forexample, nonmalignant B cells may produceautoantibodies that target the platelet surface antigens,Ib/IX and IIb/IIIa, resulting in platelet destruction throughopsonization and platelet-dependent cellularcytotoxicity.8,10 Ibrutinib primarily induces apoptosis ofboth malignant and nonmalignant B cells by inhibiting Bcell receptor signaling. BTK, which is expressed on Bcells but not on T cells, plays important roles in B cellsurvival, adhesion, and migration. BTK inhibition byibrutinib would likely reduce the surface expression ofCXCR4, releasing lymphocytes into the blood streamfrom the spleen and lymph nodes, and inhibit their homingcapacities, thereby enhancing the efficiency ofapoptosis.11 Moreover, ibrutinib may inhibit crosstalkbetween CLL cells and immune effecter cells, resultingin a reduction in autoreactive T cells.12 Taken together,these findings suggest that ibrutinib ought to be effectivefor CLL-related thrombocytopenia. Furthermore,modulation of phagocyte signaling is also promising inpatients with immune thrombocytopenic purpura (ITP).The spleen tyrosine kinase (Syk) inhibitor fostamatinib,
Ibrutinib for thrombocytopenia with CLL
86
which blocks Fcγ receptor signaling in phagocytes, maybe effective at ameliorating the destruction of platelets inpatients with ITP.13,14 BTK is responsible for thedownstream signaling of Syk molecules15 and is likelyresponsible for macrophage functions.16
These findings suggest that ibrutinib may potentiallybecome feasible even for the treatment of patients withITP. Although ibrutinib treatment for the patient in thepresent report resulted in the recovery of thrombocytes,his platelet counts did not reach the normal range,remaining at approximately 50,000/μl. This finding isin agreement with the mechanisms of ibrutinib action.Ibrutinib may not immediately "eradicate" CLL cells butrather decrease them and correct their supportingenvironment. We, therefore, continued this patient onmaintenance treatment with ibrutinib, in addition tocareful follow-up.
In conclusion, we encountered a patient withintractable thrombocytopenia associated with severerecurrent CLL who was successfully treated withibrutinib. Although it remains unclear whether ibrutinibis always warranted for such CLL patients, additionalstudies are required, and our findings suggest that ibrutinibought to be considered for the treatment of CLL-associated severe thrombocytopenia. In addition, CLLis less common in Japan than in western countries, andits etiology may show racial and ethnic differences.Therefore, it would be of great importance to evaluateadditional Japanese patients treated with ibrutinib.
References
1. Tandra P, Krishnamurthy J, Bhatt VR, et al.Autoimmune cytopenias in chronic lymphocyticleukemia, facts and myths. Mediterr J Hematol InfectDis 2013; 5: e2013068.
2. Rogers KA, Ruppert AS, Bingman A, et al. Incidenceand description of autoimmune cytopenias duringtreatment with ibrutinib for chronic lymphocyticleukemia. Leukemia 2016; 30: 346-50.
3. Byrd JC, Brown JR, O'Brien S, et al. Ibrutinib versusofatumumab in previously treated chronic lymphoidleukemia. N Engl J Med 2014; 371: 213-23.
4. Eichhorst B, Hallek M, Goede V. New treatmentapproaches in CLL: Challenges and opportunities inthe elderly. J Geriatr Oncol 2016; 7 : 375-82.
5. Islam A, Vladutiu AO, Donahue T, et al. CD8expression on B cells in chronic lymphocyticleukemia: a case report and review of the literature.Arch Pathol Lab Med 2000; 124: 1361-3.
6. Byrd JC, Brown JR, O'Brien S, et al. Ibrutinib versusofatumumab in previously treated chronic lymphoidleukemia. N Engl J Med 2014; 371: 213-23.
7. Ghosh K, Sivakumaran M, Wood JK. Aberrant CD8antigen expression in a patient with B chroniclymphocytic leukaemia showing unusual diseaseprogression. Br J Haematol 1993; 85: 205-6.
8. Semple JW, Provan D, Garvey MB, et al. Recentprogress in understanding the pathogenesis ofimmune thrombocytopenia. Curr Opin Hematol2010; 17: 590-5.
9. Bluestone JA, Tang Q. How do CD4+CD25+regulatory T cells control autoimmunity? Curr OpinImmunol 2005; 17: 638-42.
10. J o h n s e n J . P a t h o g e n e s i s i n i m m u n ethrombocytopenia: new insights. Hematology AmSoc Hematol Educ Program 2012; 2012: 306-12.
11. Chen SS, Chang BY, Chang S, et al. BTK inhibitionresults in impaired CXCR4 chemokine receptorsurface expression, signaling and function in chroniclymphocytic leukemia. Leukemia 2016; 30: 833-43.
12. Lad DP, Varma S, Varma N, et al. Regulatory T-cells in B-cell chronic lymphocytic leukemia: theirrole in disease progression and autoimmunecytopenias. Leuk Lymphoma 2013; 54: 1012-9.
13. Bajpai M. Fostamatinib, a Syk inhibitor prodrug forthe treatment of inflammatory diseases. IDrugs 2009;12: 174-85.
14. Podolanczuk A, Lazarus AH, Crow AR, et al. Ofmice and men: an open-label pilot study for treatmentof immune thrombocytopenic purpura by an inhibitorof Syk. Blood 2009; 113: 3154-60.
15. Qiu Y, Kung HJ. Signaling network of the Btk familykinases. Oncogene 2000; 19: 5651-61.
16. Feng M, Chen JY, Weissman-Tsukamoto R, et al.Macrophages eat cancer cells using their owncalreticulin as a guide: roles of TLR and Btk. ProcNatl Acad Sci U S A 2015; 112: 2145-50.



















![Ibrutinib for treating chronic lymphocytic leukaemia [ID749]](https://static.documents.pub/doc/80x56/61bd033261276e740b0e7527/ibrutinib-for-treating-chronic-lymphocytic-leukaemia-id749.jpg)

