39
Suen PY Department of Surgery PMH 11 February 2012
| Date post: | 15-Dec-2015 |
| Category: |
Documents |
| Upload: | luis-setters |
| View: | 224 times |
| Download: | 0 times |
Suen PYDepartment of Surgery
PMH11 February 2012
Ms Cheung OLF/62
PMH: HT Past Surgical Hx: nil Social Hx: lives with daughter
C/O: abdominal distension and right upper quadrant discomfort for 5 years with increase in severity in recent 6 months
Decrease in appetiteweight loss (5 pounds in recent 1 year)
no jaundice, no pallor, no cervical lymphadenopathy
Abdomen: grossly distended, hepatomegaly with liver span about 25 cm, smooth edge and no shifting dullness
LFT normal (TB 22 umol/L, ALP 64 U/L, ALT 17U/L, albumin 41 g/L)
CEA: 6.1 AFP: 1.89HbsAg: –veHb 12.1g/dL, WBC 4.4x10⁹/L
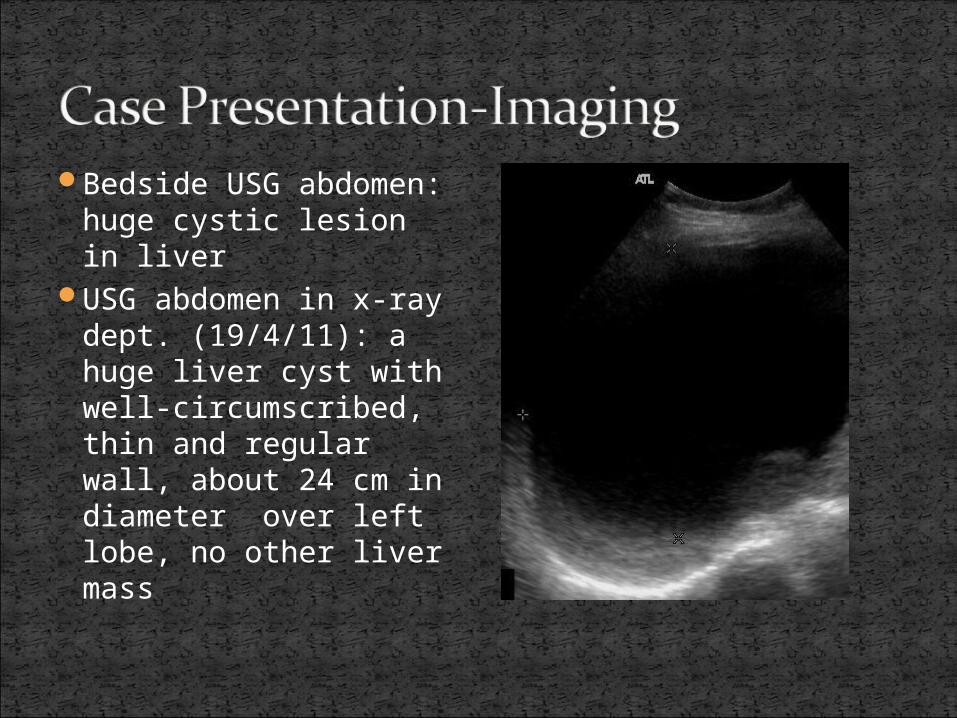
Bedside USG abdomen: huge cystic lesion in liver
USG abdomen in x-ray dept. (19/4/11): a huge liver cyst with well-circumscribed, thin and regular wall, about 24 cm in diameter over left lobe, no other liver mass
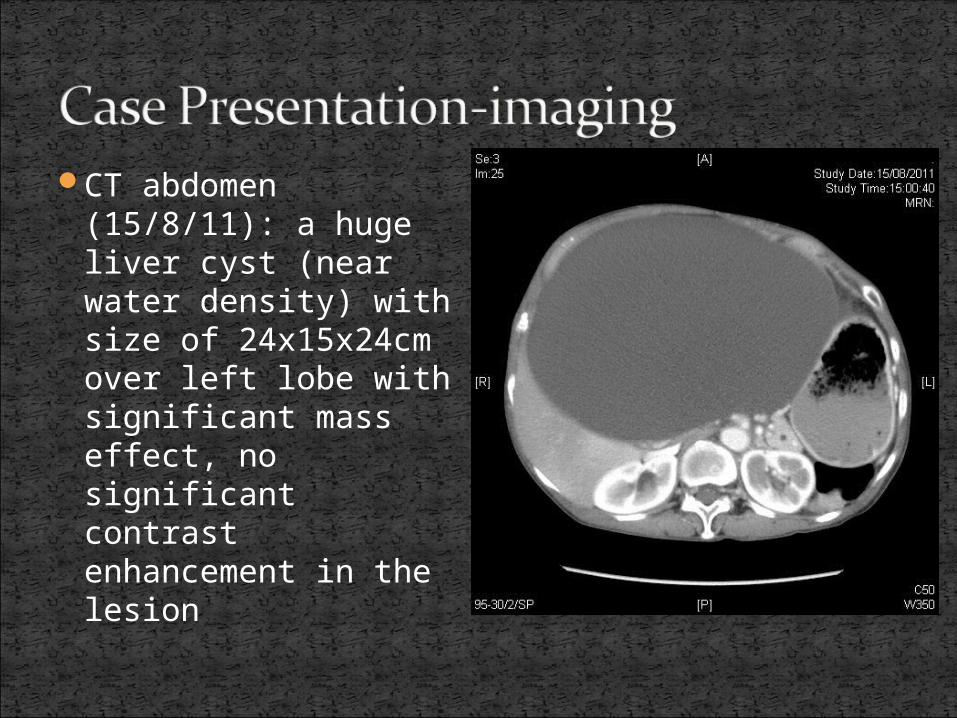
CT abdomen (15/8/11): a huge liver cyst (near water density) with size of 24x15x24cm over left lobe with significant mass effect, no significant contrast enhancement in the lesion
Laparoscopic liver cyst fenestration (marsupialization/unroofing) offerred; patient opted for OT
Operation done on 23/11/11
Findings: a large left hepatic cyst (ab0ut 25 cm in diameter); about 3 litres of serous fluid inside and drained
Sub-umbilical port made under direct vision with pneumoperitoneum created; 10mm epigastric and 5mm right subcostal ports created
Cyst wall punctured and cystic fluid drained
Cyst wall partially excisedInner lining of cyst wall
cauterizedA piece of omentum anchored
into cystic cavity
Post-operatively: uneventfulDischarged on D5
Followed up 1 mouth later:Well, no more abdominal
distension nor discomfortAbdomen: soft and not
distendedWound healedPathology: a single layer of
cuboidal epithelium, suggestive of simple hepatic cyst
Simple hepatic cysts (majority)
polycystic liver disease Neoplastic cysts (benign or malignant)Traumatic cystsParasitic (hydatid) cysts Pyogenic cysts
cystic formations of the liver, containing serous fluid, usually not communicating with biliary system
Most common cystic lesions of the liver2nd most common incidental findings of
benign lesions in the liver after hemangiomaprevalence : 5% 90-95% asymptomatic

For asymptomatic , female to male ratio about 1:1
For symptomatic, female to male ratio 9:1
No malignant potential
About half of patients have a single cyst, whereas the other half have two or more
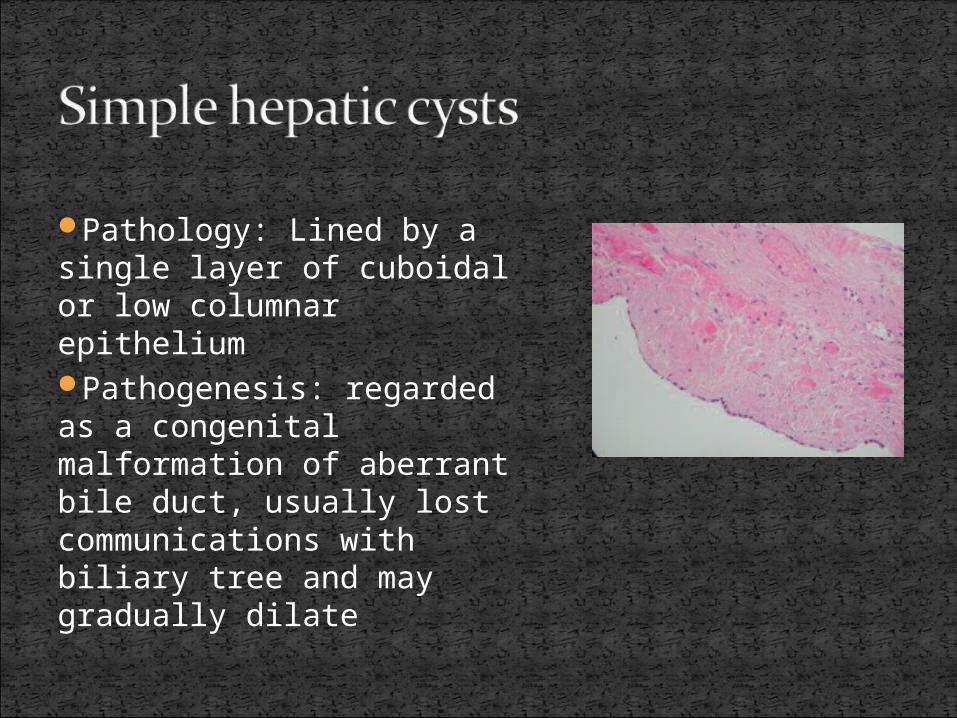
Pathology: Lined by a single layer of cuboidal or low columnar epitheliumPathogenesis: regarded as a congenital malformation of aberrant bile duct, usually lost communications with biliary tree and may gradually dilate
Majority : asymptomatic Commonly discovered as incidental finding
during radiographic studies for unrelated symptoms or for other diseases
Common symptoms: abdominal discomfort, abdominal distension, nausea or vomiting
Rare symptoms: fever, sweating, back or shoulder pain
RareIntra-cystic haemorrhage (most common;
sudden onset of increase in abdominal pain or distension )
Spontaneous ruptureInfectionBiliary compression with obstructive jaundicetorsion
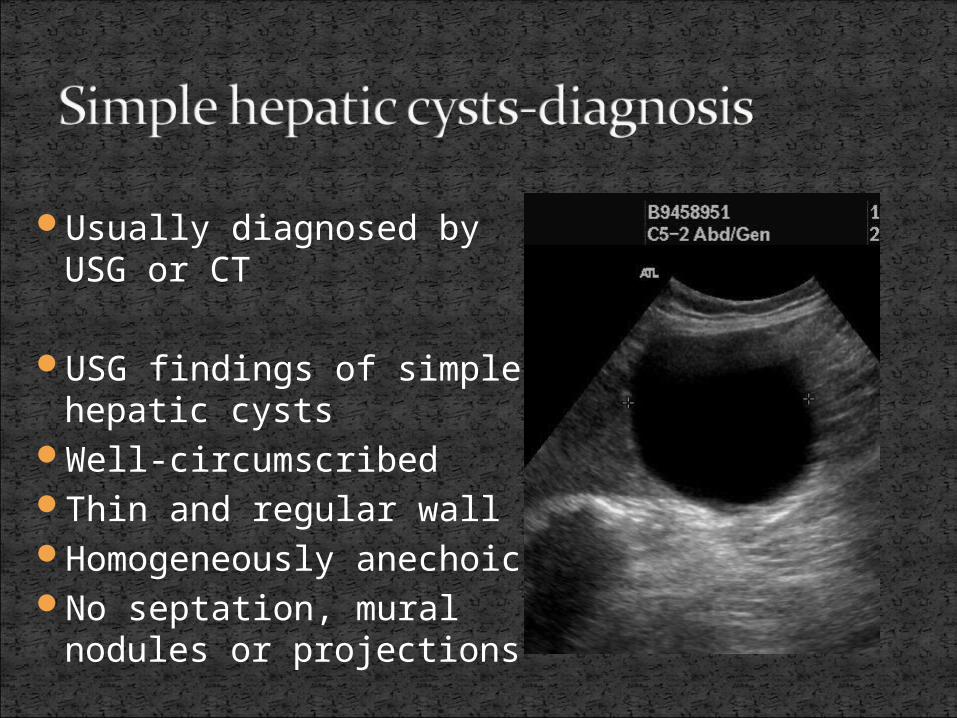
Usually diagnosed by USG or CT
USG findings of simple hepatic cysts
Well-circumscribedThin and regular wallHomogeneously anechoic No septation, mural
nodules or projections
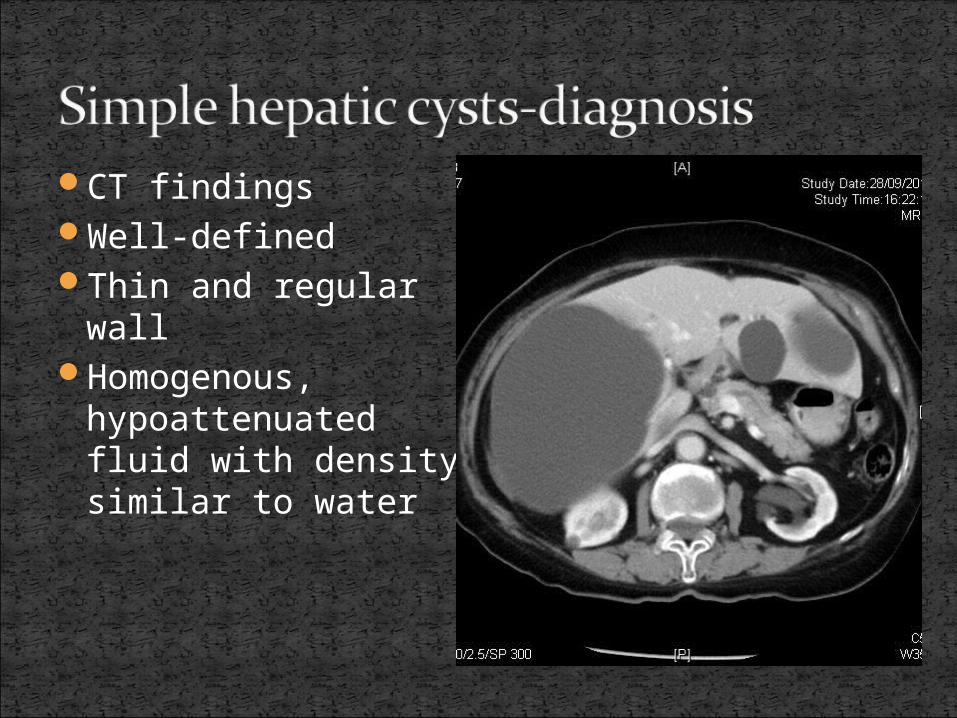
CT findingsWell-definedThin and regular wallHomogenous,
hypoattenuated fluid with density similar to water
MRI may be considered when the diagnosis is equivocal
Well-defined, thin and regular wallFluid signal intensity: low on T1-weighted
images and high on T2-weighted imageNo wall enhancement, nodules or projections;
and no internal signals
Cyst fluid analysis ( percutaneous fluid aspiration for analysis) may also be considered in cases with difficulty in diagnosis
Cytological analysis: acellular fluid and absence of mucin
Chemical analysis: normal CEA, CA19.9 and bilirubin level
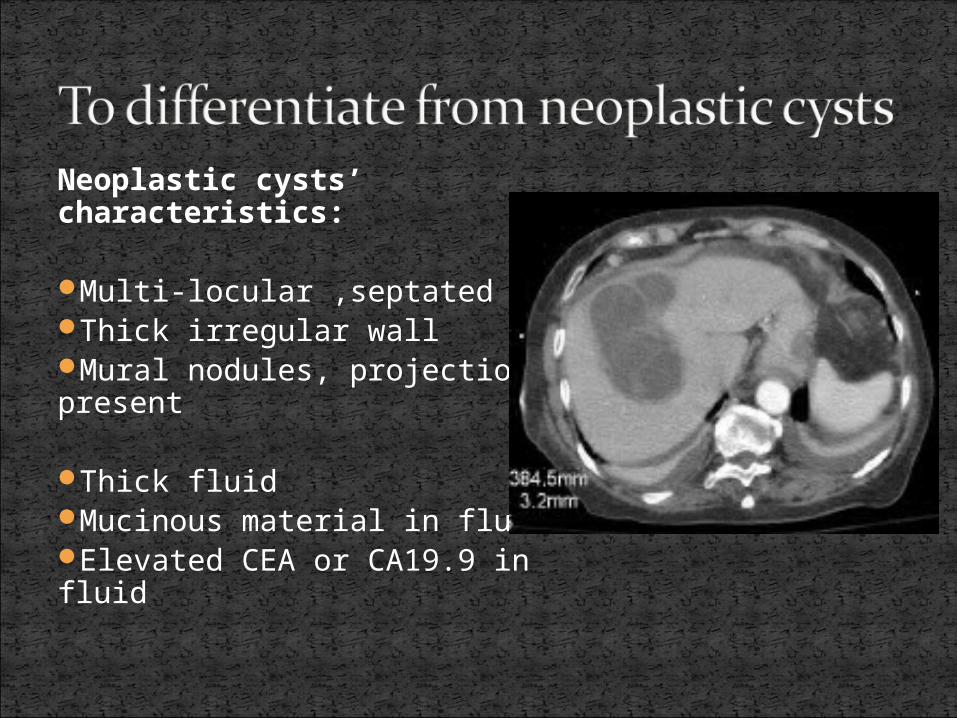
Neoplastic cysts’ characteristics:
Multi-locular ,septatedThick irregular wallMural nodules, projections present
Thick fluidMucinous material in fluidElevated CEA or CA19.9 in fluid
Rare Cystadenomas or cystadenocarcinomaMost are cystadenomas -A benign cystic tumour with potential
malignant transformation to cystadenocarcinoma (very rare)
Radiologically : complex cystic lesions
Majority of patients require no treatment, just for observation
Symptomatic condition (most common)
Intracystic hemorrhageDiagnostic uncertainty
Simple percutaneous aspirationPercutaneous aspiration followed by injection
of a sclerosing agent
Fenestration (unroofing or marsupialization)
Enucleation (rarely applied)
Percutaneous aspiration associated with very high recurrence rate (75-100%)repeated aspiration can result in cyst infectionusually not for definitive treatment
sclerosing agents : ethanol, minocycline hydrochloride, tetracycline hydrochloride
Recurrence rate: 20-30%contraindicated if there is communication
with biliary tractgenerally reserved for patients with high
operative risk
lowest (5 %) recurrence rateShould be considered and offered for most
of symptomatic patientsA laparoscopic approach is favoured (lots
of evidence demonstrates it’s treatment results equivalent to that of an open approach, while it has the advantages of a laparoscopic surgery)

Laparoscopic approach adoptedResection of a portion of the cyst
wall allows drainage into the peritoneal cavity and access to its interior
Ablation of remaining inner lining of cyst wall by cauterization will minimize recurrences and the risk of ascites
A piece of omentum can be anchored into the cavity of cyst to avoid reformation of cyst
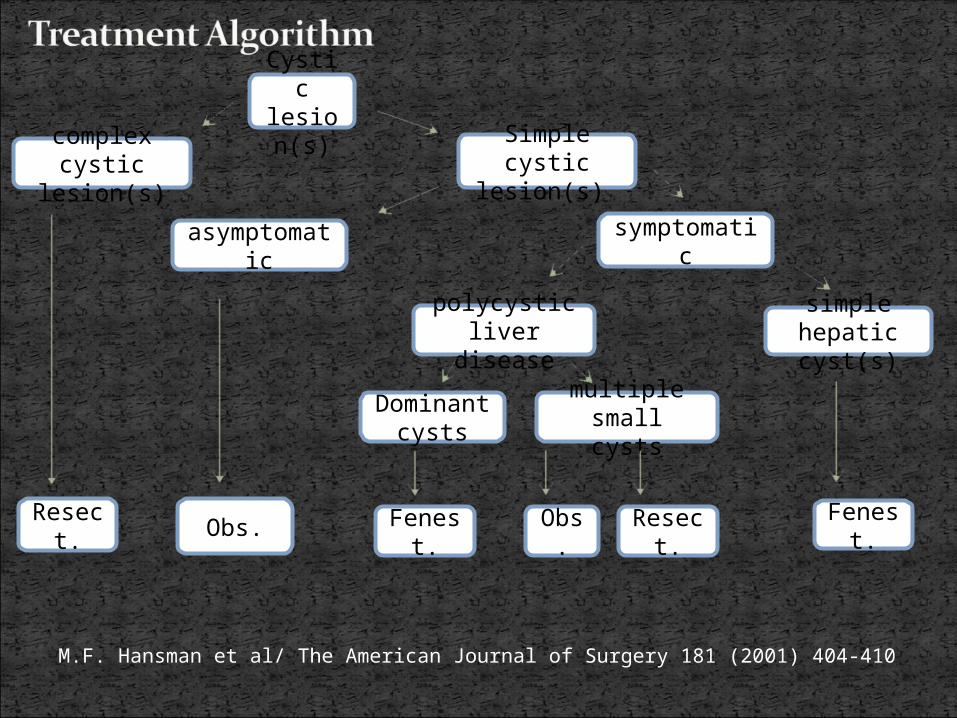
M.F. Hansman et al/ The American Journal of Surgery 181 (2001) 404-410
Cystic lesion(
s) Simple cystic
lesion(s)
symptomatic
simple hepatic cyst(s)
Fenest.
polycystic liver disease
Dominant cysts
multiple small cysts
Fenest.
Resect.
asymptomatic
Obs.
complex cystic
lesion(s)
Obs.Resec
t.
1. Making a definitive diagnosis of the nature of the cystic lesion -DDx: simple hepatic cysts/neoplastic cysts/others -Inx: US/CT +/- MRI or cystic fluid analysis
2. Determining whether the patient’s symptoms are related to the cystic lesion or not -careful history taking -relevant investigations or procedures
3. Deciding whether to intervene or not -assessing the severity of symptoms, occurrence of complications, certainty of the diagnosis, pre-morbid state and the operative risks
4. Deciding the treatment modality -laparoscopic fenestration, percutaneous aspiration followed by injection of a sclerosing agent, simple aspiration or enucleation
Current Surgical Therapy by John L. Cameron, 10th ed.
Surgery of the liver and biliary tract by L.H. Blumgart, 3rd ed.
Hansman MF et al: Management and long-term follow-up of hepatic cysts, Am J Surg 181: 404-410, 2001
Fabiani P et al: long-term outcome after laparoscopic fenestration of symptomatic simple cysts of the liver, Br J Surg 92: 596-597, 2005
Mazza OM et al: Magagement of non-parasitic hepatic cysts, Am J Surg 209: 733-739, 2009
www.medscape. com


















