106
Suits and Cases: Potential Pitfalls in the management of Poisoned Patients John Kashani DO St. Josephs Regional Medical Center New Jersey Poison Center
| Date post: | 25-Dec-2015 |
| Category: |
Documents |
| Upload: | gilbert-mitchell |
| View: | 218 times |
| Download: | 2 times |

Suits and Cases: Potential Pitfalls in the management of
Poisoned Patients
John Kashani DO
St. Josephs Regional Medical Center
New Jersey Poison Center


Case 1
• An 18 year old female, with a past medical history significant for asthma and depression, presents to the ED for shortness of breath
• She has a respiratory rate of 34, is diaphoretic, is actively vomiting and appears confused
Case 1
• Her blood pressure is 90/54, Heart rate is 150 and a rectal temperature is 102
.
farenheit and pulse oximetry is 99% on supplemental oxygen
• Her mother states that this is the worst asthma attack she has ever had
• She is emergently intubated

Case 1
• Shortly after being intubated she seizes and develops ventricular fibrilation
• Despite your best efforts she dies
• An autopsy is requested by the family
• A post mortem salicylate level was 150mg/dL

Introduction
• Salicylates are the most widely used analgesic, anti-pyretic and anti-inflamatory and is the standard for the comparison and evaluation of others
• Because salicylates are so widely available the potential for misuse is often underappreciated

Introduction
• The physician taking care of the salicylate intoxicated patient must be familiar with the pathophysiology, pharmakokinetics, potential pitfalls, and treatment options
Sources of Salicylates
• Found in Willow bark (Salix alba vulgaris)• Available in a multitude of
formulas/preparations– Over-the-counter (pepto-bismol)– Topical preparation (wart removal)– Combinations (excedrin, fiorinal,
percodan)– Other (oil of wintergreen)

Pharmakokinetics
• Peak levels – Regular preparations – Enteric coated– Liquids preparations– Overdose
• Distribution• Metabolism• Excretion

Distribution
• Volume of distribution (Vd)
– Apparent volume the drug is dissolved in
– Measured in Liters or Liters/Kg
• not a real volume

Salicylates: Toxic Dose
• Therapeutic Range: 10–20 mg/kg
• Mild Toxicity: 150 mg/kg
• Moderate Toxicity: 150-300 mg/kg
• Severe Toxicity: > 300 mg/kg

Inflamatory Mediators
• Inhibits cyclooxygenase
– Decrease in prostaglandins
– Increase leukotrienes
• Increases microvascular permeability

acetyl-CoA
oxaloacetate citrate
isocitrate
-ketoglutarate
succinyl-CoAsuccinate
fumarate
malateNAD+
NADH
NAD+
NADH
NAD+
NADH
FAD
FADH2
pyruvate
CO2
CO2
CO2
NAD+
NADH
matrix

Glucose
Pyruvate Lactate
2 ATP
ALT
Muscle
Alanine
Liver
Alanine
Pyruvate
Glucose
NH2
Urea6 ATP
4 ATP
X

Respiration
• Uncouples oxidative phosphorylation– Disrupts hydrogen ion gradient– Unable to generate ATP using electron
transport• Increased oxygen consumption,
increased heat production, increased metabolic rate, decreased ATP production, increased CO2 production

R-COOH
matrix
intermembrane space
H+ H+ H+ H+ H+ H+ H+ H+
H+ H+
H+
R-COOHR-COO-
R-COO-

I
matrix
intermembrane space
II
Q
4H+
4H+
III
4H+
4H+
IV
CytC
O2 H2O
2H+
2H+
succinate
NADH + H+
ATP + H2O
ADP + Pi + H+
3H+
3H+
R-0H
R-0H
R-0- + H+
H+
R-0-
H+
heat

Metabolic
• Increased lipolysis
• Increased production of ketones
– Ketonuria present in almost all overdose patients

Ketone bodies
Acetyl CoA
Fatty Acids

Metabolic
• Hyperglycemia in acute setting
– Glycogenolysis
– May cause glucosuria
• Hypoglycemia may subsequently develop

Metabolic
• Causes a respiratory alkalosis
– Due to respiratory center stimulation
– Increase in respiratory rate and depth

Hematologic
• Platelet dysfunction• Inhibition of Vitamin K dependent
clotting factors• II, VII, IX, X, Protein C, Protein S
• Hypoprothrombinemia

Gastrointestinal Effects
• Nausea
• Vomiting
• Gastritis
• Pylorospasm

Neurologic• Occurs from metabolic derangements and
salicylate CNS levels– Agitation, irritability– Tinnitus
• Occurs at levels of 20-45 mg/dL– Lethargy

Laboratories
• Salicylate Level
– An Level of 100 mg/dL is extremely worrisome (impending doom)
– Chronic Levels of > 30 mg/dL are concerning
• Difficulty in interpretation due to variable Vd
Laboratories
• Levels should be obtained every 1 to 2 hours until downward trend is observed
• Do not rely on a single level• Levels < 20mg/dl and a downward trend
can be medically cleared

Case 2
• A 35 year old male presents to the emergency department for profound weakness, bradycardia and emesis
• An I stat potassium is 8.5mg/dL and an EKG show a sine wave pattern
• IV Calcium chloride is administered and he develops ventricular fibrilitation shortly thereafter

Case 2
• Despite your best efforts he dies
• The wife said he has no medical problems, but was recently doing a “cleansing diet” that included herbal teas

Introduction
• Digitalis and digitalis like cardiac glycosides (DG’s) are found in a variety plants, toads and pharmaceutical agents
• Dried powders and extracts have been used for centuries for medicinal agents and as arrow poisons







Pharmacokinetics
• Peak serum concentrations occur in minutes with IV dosing and 1-2 hours after an oral dose
• The VD is initially small and increases following a two phase compartment model– Higher in infants and neonates and
lower in the elderly

Pharmacokinetics
• Tissue distribution takes 6-12 hours
• Digoxin crosses the placenta with fetal levels approaching that of the mother
• Elimination
– Hepatic metabolism
– Urinary excretion of unchanged drug

Pathophysiology
• Cardiac glycosides inhibit the sodium potassium atp-ase
– Responsible for pumping two sodium ions out of the cell for every two potassium ions in to the cell

3 Na+
2 K+
Na-KATPase Na+
Ca++
SR
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Ca++
Ca++
Ca++Ca++
ATPase
Ca++
myocardium
-90 mv
K+
Na+
Na+
Na+
Ca++
Na+

3 Na+
2 K+
Na-KATPase Na+
Ca++
SR
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Ca++
Ca++
Ca++Ca++
ATPase
Ca++
myocardium
-90 mv
K+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Na+
Na+
Ca++
Na+

3 Na+
2 K+
Na-KATPase Na+
Ca++
SR
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Ca++
Ca++
Ca++Ca++
ATPase
Ca++
myocardium
-90 mv
K+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Na+

3 Na+
2 K+
Na-KATPase Na+
Ca++
SR
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Ca++
Ca++
Ca++Ca++
ATPase
Ca++
myocardium
-90 mv
K+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++Ca++
[Ca++]Ca++
Na+

Inhibition of Na-K-ATPase
[Nai+]
[Cai++]
heart
contractility

3 Na+
2 K+
Na-KATPase Na+
Ca++
SR
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Ca++
Ca++
Ca++Ca++
ATPase
Ca++
muscle
-90 mv
K+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++Ca++
[Ca++]
[K+]
Ca++
Na+

Inhibition of Na-K-ATPase
[Nai+]
[Ko+]
hyperkalemia
[Cai++]
skeletal muscleheart
contractility

3 Na+
2 K+
Na-KATPase Na+
Ca++
SR
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Ca++
Ca++
Ca++Ca++
ATPase
Ca++
myocardium
-90 mv
K+
Na+
Na+
Na+
Ca++
Na+

3 Na+
2 K+
Na-KATPase Na+
Ca++
SR
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Ca++
Ca++
Ca++Ca++
ATPase
Ca++
myocardium
-90 mv
K+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++Ca++
Ca++ Ca++
Ca++
Ca++
Na+

3 Na+
2 K+
Na-KATPase Na+
Ca++
SR
Ca++
Ca++
Ca++
Ca++Ca++
Ca++
Ca++
Ca++
Ca++Ca++
ATPase
Ca++
myocardium
-90 mv
K+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+
Na+Na+
Na+
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++
Ca++Ca++
Ca++ Ca++
Ca++
Ca++
Na+
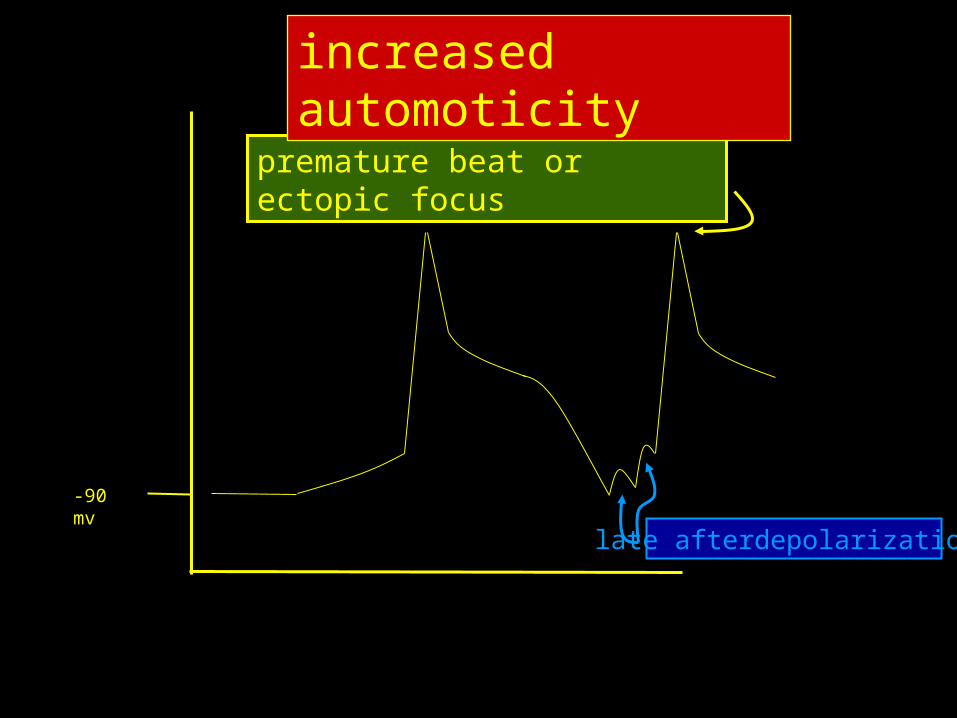
-90 mv
premature beat or ectopic focus
increased automoticity
late afterdepolarizations

Inhibition of Na-K-ATPase
[Nai+]
[Ko+]
hyperkalemia
[Cai++]
skeletal muscleheart
contractility
automoticity
premature beatsescape rhythmsV-tach, V-fib
rise in Nai+
and Cai++
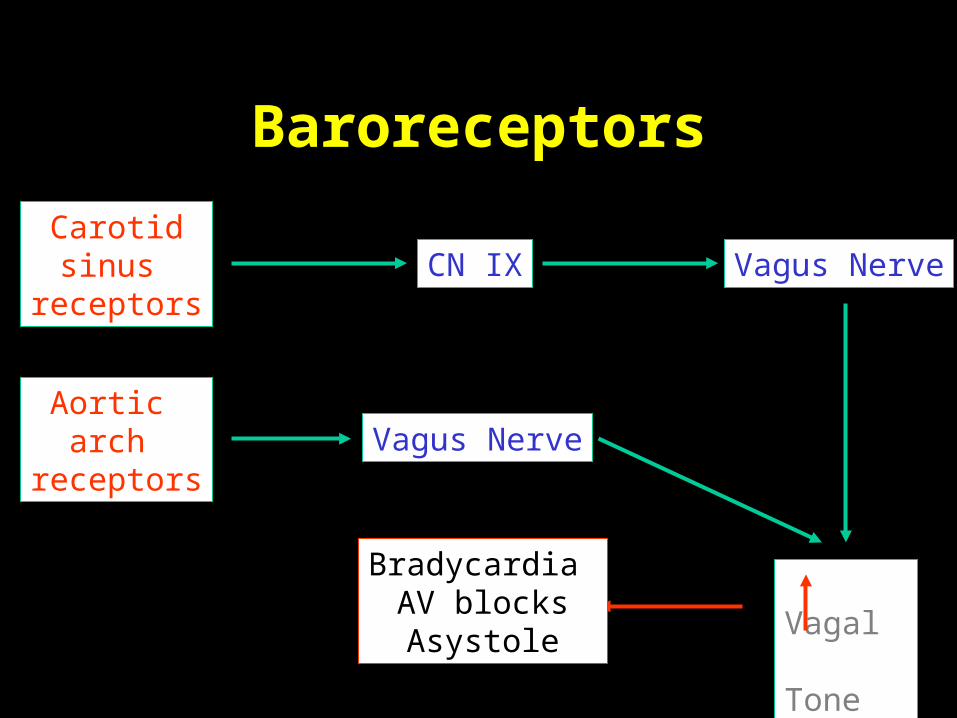
Baroreceptors
Carotidsinus
receptorsCN IX Vagus Nerve
Aortic arch
receptors
Vagal Tone
Bradycardia AV blocksAsystole
Vagus Nerve

Increasedbaroreceptor
firing
CNS
Parasympathetic
Sympathetic
SVRCO
IncreasedArterial
Pressure
(-)(-)
Baroreceptors

Inhibition of Na-K-ATPase
[Nai+]
[Ko+]
hyperkalemia
[Cai++]
skeletal muscleheart
contractility
premature beatsescape rhythmsV-tach, V-fib
firing
baroceptors
vagal tone
bradycardia, AV blocks, asystole
automoticity
rise in Nai+
and Cai++
rise in Nai+
and Cai++

Devils Advocate
• Treatment of Hyperkalemia in a patient with unrecognized digitalis toxicity
– 80 yr old female presents to the ED with AMS, hyperkalemia and bradycardia
– Treated with intravenous pacing and IV calcium chloride
J Toxicol Clin Toxicol. 2003;41(4):373-6
Devils Advocate
• A toxicological Surprise
– A 42 year old man was admitted to a medical service for CP, nausea and vomiting
– Heart rate was 35, EKG showed total AV block
– Potassium was 5.7mmol/L
Lancet. 2000 Oct 21;356(9239):1406.
Devils Advocate
• He was treated for a myocardial infarction
• A transvenous pacer was inserted with an increase in his heart rate to 70 BPM
• A serum digoxin level was 365ng/mL (therapeutic range 10-30)
Lancet. 2000 Oct 21;356(9239):1406.

Digoxin in herbal Supplements
• Digoxin Toxicity in a 26 year-old woman taking a herbal dietary supplement
– Presented to an ED with chest pain
– Initially her heart rate was 70 BPM and BP was 112/59
– Her heart rate dropped to 39 and BP dropped to 59/36J Am Osteopath Assoc. 2001 Aug;101(8):444-6

Digoxin in herbal Supplements
• EKG showed the absence of P waves
• She was given a NS fluid bolus and placed in the trendelenberg position
• Her BP and heart returned to her original baseline
• A digoxin level was 0.9ng/mL
J Am Osteopath Assoc. 2001 Aug;101(8):444-6

Digoxin in herbal Supplements
• She confessed to consuming a tea that contained:
– Skullcap herb, wood betony herb, black cohosh root, hops flowers, valerian root and cayenne pepper fruit
J Am Osteopath Assoc. 2001 Aug;101(8):444-6

Case 3
• A 36 year old female, with a past medical history for depression and chronic back pain, presents to the ED for back pain
• She states that Demerol is the only medication that relieves her pain
• Reluctantly, you write an order for Demerol

Case 3
• Two hours after the administration of Demerol she develops tachycardia, AMS and myoclonus
• You believe that she developed serotonin syndrome
• A NGT is placed in preparation for the administration of cyproheptadine

Case 3
• She has a self limited seizure, vomits and has a decrease in her O2 sat
• She is intubated using etomidate and succinylcholine
• A post intubation x-ray shows a right upper lobe consolidation
• She dies on hospital day 6 from complications of aspiration pneumonia
Serotonin Syndrome
• Drug Induced Disorder• Variable alterations in
– cognition-behavior– neuromuscular activity– autonomic nervous system function
• Increased CNS serotonin neurotransmission at 5-HT1A and 5-HT2A receptors

Serotonin Receptors
• The largest and most diverse of all neurotransmitter systems– 5HT1 – 5HT7
• Each receptor class may contain many subclasses
• 5HT1A - presynaptic and postsynaptic• 5HT1D - presynaptic and postynaptic
5HT2A - postsynaptic

Serotonin Syndrome
• No gender predilection
• Idiosyncratic in nature
• Patients are not more likely to develop SS following an overdose than they are while taking therapeutic doses
• SS is a diagnosis of exclusion

Precipitants
– Addition of second serotonergic drug usually at therapeutic doses
– Increasing primary drug
• Inherited / Acquired
– Reduction in endothelial MAOA activity
– Genetic variation

Serotonergic Agents
• Inhibit 5-HT uptake
• Enhances 5-HT release
• Inhibits 5-HT breakdown
• Metabolized to 5-HT
• 5-HT1A agonist
• Enhances 5-HT receptor response to stimulation

L-tryptophan
5-hydroxytrytophan
5-HT
TPH
AAD
5-HT
5-HT receptors 1-7
MAO
5-HIAA
5-HT1A, D
-
X
X

Inhibit 5-HT Uptake
• Specific SRIs• Non-specific SRIs - clomipramine, trazodone• TCAs• Meperidine• Dextromethorphan• Pentazocine• Tramadol• Dexfenfluramine

Enhance 5-HT Release
• Lithium
• Levodopa, dopamine
• MDMA
• Cocaine
• Amphetamines
• Fenfluramine
• Dexfenfluramine

5-HT1 Agonists
• LSD
• Buspirone
• Sumatriptan
• Dihydroergotamine
Serotonergic Agents
• Inhibits 5-HT breakdown
– MAOIs
• Metabolized to 5-HT
– Tryptophan
• Enhances 5-HT1A receptor response to stimulation
– Lithium

Drug Combinations
• All MAOI combinations• Dextromethorphan and SSRI• Lithium and SSRI• Trazodone and SSRI• Tramadol and SSRI• Trazodone and Buspirone• Selegiline and SSRIs or TCAs• Switching from 1 SSRI to another SSRI

Serotonin Syndrome Associated with Monotherapy
• Clomipramine
• Fluvoxamine
• Venlafaxine
• MDMA
• Sertraline

Clinical Manifestations
• Cognitive and behavioral
– Confusion (54%)
– Agitation (35%)
– Coma (28%)
– Hypomania (15%)
– Seizures (14%)
– Hallucinations (6%)Mills K. Serotonin Syndrome A Clinical Update. Critical Care Clinics, Volume 13:4 Oct 1997
Clinical Manifestations
• Autonomic Dysfunction
– Blood Pressure Lability (47%)
– Hyperthermia (46%)
– Diaphoresis (46%)
– Tachycardia (41%)
– Mydriasis (26%)
– Diarrhea (12%) Mills K. Serotonin Syndrome A Clinical Update. Critical Care Clinics, Volume 13:4 Oct 1997
Clinical Manifestations
• Neuromuscular Abnormalities– Myoclonus (57%) – Hyperreflexia (55%) – Rigidity (49%)– Tremor (49%) – Incoordination (38%) – Shivering (25%) – Nystagmus (13%)– Seizures (14%)
Mills K. Serotonin Syndrome A Clinical Update. Critical Care Clinics, Volume 13:4 Oct 1997

Sternbach’s Suggested Diagnostic Criteria
• Coincidental with the addition of or increase in known serotonergic agents to an established medications regimen - at least 3 of the following– agitation, diaphoresis, diarrhea, fever,
hyperreflexia, incoordination, MS changes, myoclonus, shivering, tremor
• Other etiologies (infections, metabolic, withdrawal) have been ruled out
• A neuroleptic agent has not been started or increased in dosage
Other Criteria
• Hegerl Criteria
• Dursun Criteria
• Randomski Criteria
• Mills Criteria
• Hunters Decision Rules
• MOFO Criteria

Time course
• Usually abrupt
• Occurring within hours after initiation of new serotonergic agent
• 2/3 of cases resolves within 24 hours

Treatment
• Five basic management principles
– Supportive care
– Discontinue serotinergic agents
– Anticipate potential complications
– Administer antiserotinergic agents
– Reassess the need for reinstituting pharmacotherapy

Treatment
• Antipyretics are generally ineffective
• Benzodiazepines are the initial choice for relieving muscle spasm
• No specific antidotes for SS
• Most symptoms resolve in 12 – 24 hours

Cyproheptadiene
• Cyproheptadine (periactin)
– Most consistently effective
– Blocks postsynaptic 5HT1A and 5HT2
receptors
– Only available orally (syrup, tablet)
– Also has antimuscarinic and antihistaminc properties
Case 4
• A 54 year old male presents to the ED with a rash that has been getting progressively worse over that past week and a half
• He also offers complaints of chills, nausea, vomiting and diarrhea
• Past medical history is significant for seizure disorder and hypertension


Case 4
• His medications include phenytoin and lisinopril
• He is febrile with a temperature of 102.c, tachycardic at a ventricular rate of 130, hypotensive with a sys BP of 80, RR 24
• His white count is 28,000 with a left shift, HG: 19, HCT: 45, Platelets 52

Case 4
• Na+ 156, K+ 5.4, Cl- 92, NaHco3- 12,
• BUN: 60, CR 5.2 and glucose is 220
• His LFTS are markedly elevated and he has a creatinine of 3.2
• His phenytoin level 0.5mcg/mL
• He is loaded with IV phenytoin in the ED

Case 4
• One hour after the administration of phenytoin he drops his blood pressure and becomes apneic
• He is subsequently intubated and is transferred to the ICU
• He dies on Hospital day 7 from multi-system organ failure
Introduction
• Anticonvulsant hypersensitivity syndrome (ACHS) is a rare, potentially fatal multisystem disorder that occurs after exposure to phenytoin, carbamazepine, phenobarbital, felbamate and lamotrigine

Signs and Symptoms
• ACHS commonly begins within one to four weeks after starting therapy, but may present as late as three months
• ACHS may occur within hours of a previously sensitized individual
• ACHS is not related to the dose or serum concentration

Signs and Symptoms
• Most commonly ACHS begins with a fever, followed by a rash and variable degrees of lymphadenopathy
• The fever usually ranges from 38 – 40.C
• The Rash may develop concurrently or shortly after the fever

Signs and Symptoms
• The Rash is commonly described as an exanthem with or without pruritus
• The upper extremities, face and trunk are usually first affected
• Periorbital edema, exudative tonsillitis, pharyngitis, oral ulcerations and conjunctivitis may be seen

Signs and Symptoms
• Rarely, more severe skin reactions may occur (SJS, TEN, EM)
– Usually in the setting of repeated exposures or continued use
• Tender lymphadenopathy is commonly seen

Signs and Symptoms
• The Liver is the most common organ involved
• The CNS, heart, lungs, renal system and thyroid gland may be involved– Patients may present with elevated
transaminases, alkaline phosphatase, PT and bilirubin
• The hepatitis is usually mild and anicteric

Signs and Symptoms
• The degree of hepatitis is related to the time between the onset of symptoms and the discontinuation of the offending agent
• Liver biopsies reveal periportal inflammation with or without necrosis
• The majority of patients recover within a few weeks

Signs and Symptoms
• Hematologic abnormalities – Lymphocytosis – Leukocytosis– Eosinophilia– Anemia– Leukopenia – Thrombocytopenia– Aplastic anemia
Pathophysiology
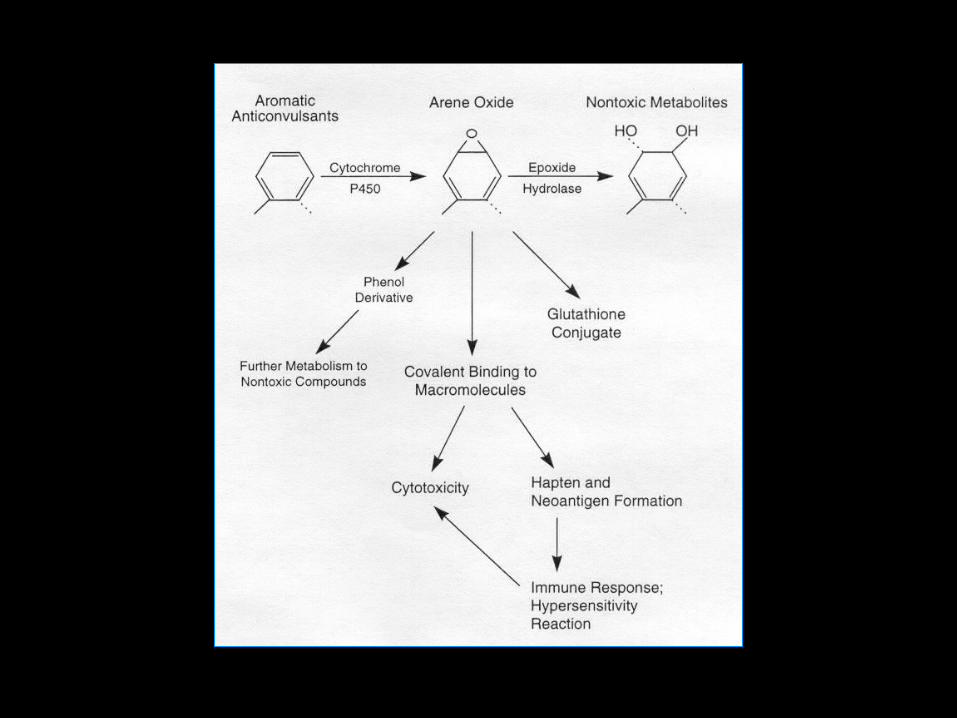
• The anticonvulsants implicated in ACHS all have in common an aromatic benzene ring that is metabolized by cytochrome p450 to an arene oxide
• Arene oxides are highly electrophilic and covalently bind to macromolecules to disrupt cellular function

Pathophysiology
• Arene oxides may also form neoantigens that trigger an immunologic response
• These metabolites are highly unstable and under normal conditions can be detoxified by one of several routes

Diagnosis
• Usually based on history of drug exposure and clinical examination
– Atypical lymphocytes
– Eosinophilia
– Elevated liver enzymes
– hyperbilirubinemia

Treatment
• The mainstay of treatment is discontinuation of the offending agent and supportive care
• Severe skin reactions are best managed in a burn center
• Strict attention must be paid to maintaining fluid and electrolyte balance

Thank You

















