48
SULFONAMIDES • Now largely superceded by antibiotics and trimethoprim- sulfamethoxazole. • They continue to occupy a small place in therapy.
| Date post: | 18-Dec-2015 |
| Category: |
Documents |
| Upload: | brook-tucker |
| View: | 218 times |
| Download: | 1 times |

SULFONAMIDES
• Now largely superceded by antibiotics and trimethoprim-sulfamethoxazole.
• They continue to occupy a small place in therapy.

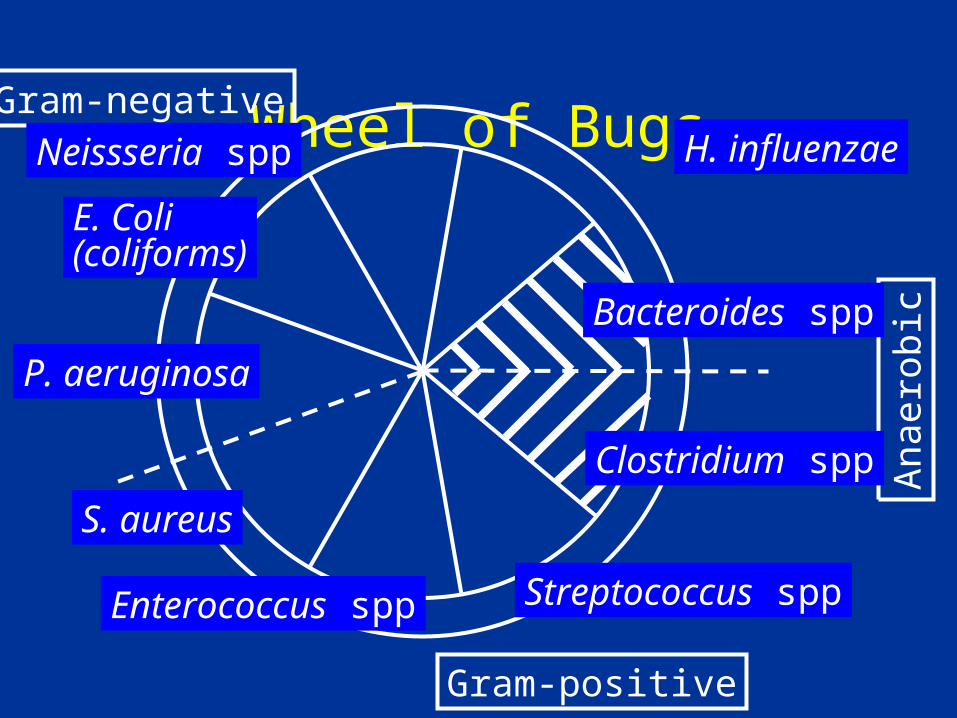
Wheel of BugsGram-negative
Gram-positive
Ana
erob
ic
P. aeruginosa
H. influenzaeNeissseria spp
E. Coli(coliforms)
S. aureus
Streptococcus spp
Bacteroides spp
Clostridium spp
Enterococcus spp

2HN COOH
DIHYDROPTERIDINE
PYROPHOSPHATE DERIVATIVE
DIHYDROPTEROIC ACID
DIHYDROFOLIC ACID
FOLIC ACID BIOSYNTHESIS
Glutamic Acid
2 ATP
2HN SO2NH2
Dihydropteroate
Synthetase

BLOOD
Protein Bound
Metabolites
Free
Oral
X Topical Parenteral
CSF
Body Fluids & Tissues
Kidney
Other-Sweat, Saliva, Prostatic fluid, Stool

KERNICTERUS IN THE NEWBORN
• Displacement of bilirubin from plasma protein binding sites.


SO2N
METABOLISM
Acetylated sulfonamides-inactive, toxic, and less soluble
H
RNC3HC
O

• They are excreted in the urine partly as the parent and partly as the metabolite.
• Some sulfonamides are very insoluble in the acid urine.
EXCRETION

EXCRETION
• Half life of the sulfonamides depends on renal function.
• Dosage should be modified or the sulfonamides should not be used in renal failure.

• Rapidly absorbed and rapidly eliminated (prototype- sulfisoxazole).
• Poorly absorbed sulfonamides (sulfasalazine).
• Topical sulfonamides (sulfacetamide, silver sulfadiazine).
• Long-acting sulfonamides (sulfadoxine)
SULFONAMIDE PREPARATIONS
CONTRAINDICATIONS



DRUG-DRUG INTERACTIONS
• Inhibit metabolism of some drugs.
• Displace certain drugs from plasma albumin.

TRIMETHOPRIM-SULFAMETHOXAZOLE
2HN CH2
OCH3
OCH3
OCH3
80 mg TRIMETHOPRIM
O
2HN SO2NH
N CH3
400 mg SULFAMETHOXAZOLE

COTRIMOXAZOLE
• Optimal ratio of the two drugs is 5:1 sulfa :trimethoprim.

Synergism

• Expanded number of organisms inhibited.
• Bactericidal .
• Decreased resistance.
• Decreased toxicity.
ADVANTAGES

THERAPEUTIC USES


PNEUMOCYSTIS PNEUMONIA (PCP)

PNEUMOCYSTIS PNEUMONIA (PCP)
• The most common opportunistic infection in advanced AIDS (80% of AIDS patients have at least one episode).
• Now considered a fungus (P.jurovecii).
• Multiple infections are often present simultaneously with the PCP.
PROPHYLAXIS
• Routine prophylaxis has been successful in improving survival.
• PCP prophylaxis is indicated if the patient has a CD4 T lymphocyte count lower than 200 cells/mm3, or has oral candidiasis regardless of the CD4 count.

TREATMENT OF PCP
• Early therapy is essential as success of therapy is related to severity of the disease at the time of initiation of therapy.

TMP-SMX
• Treatment of choice.
• Oral form used for mild-moderate cases or after initial response to IV therapy and for prophylaxis.

TMP-SMX
• Excellent tissue penetration.
• Produces a rapid clinical response.

DRUG INTERACTIONS
• Same as with sulfonamides

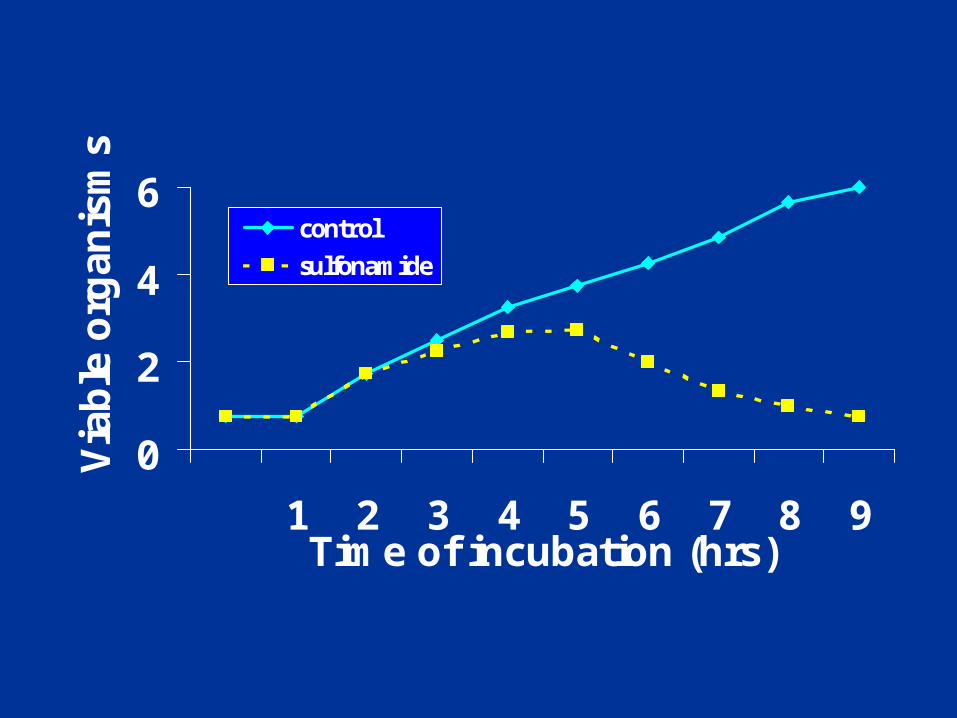
0
2
4
6
1 2 3 4 5 6 7 8 9Time of incubation (hrs)
Via
ble
org
anis
ms
control
sulfonamide

• Results from multiple mechansims.
• Altered dihydropteroate synthetase.
• Cross-resistance among all sulfonamides.
RESISTANCE

PABA
DIHYDROPTEROIC ACID
DIHYROFOLIC ACID
TETRAHYDROFOLIC ACID
+ Pteridine
SULFONAMIDE
TRIMETHOPRIMDihydrofolate Reductase
Dihydrofolate Synthetase
Dihydropteroate Synthetase


• Hypersensitivity reactions -common– allergic rashes– photosensitivity– drug fever– Stevens-Johnson syndrome
ADVERSE EFFECTS








CRYSTALLINE AGGREGATES, HEMATURIA, OBSTRUCTION

ADVERSE EFFECTS
• Headache, nausea, vomiting and diarrhea.
• Hematological effects -anemia, agranulocytosis.


ADVERSE REACTIONS
• Dermatological reactions including skin rashes.
• GI (nausea and vomiting).