Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Rugo HS, Seneviratne L, Beck JT, et al. Prevention of everolimus-related stomatitis in women with hormone receptor-positive, HER2-negative metastatic breast cancer using dexamethasone mouthwash (SWISH): a single-arm, phase 2 trial. Lancet Oncol 2017; published online March 14. http://dx.doi.org/10.1016/S1470- 2045(17)30109-2.
Transcript
Supplementary appendixThis appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors.
Supplement to: Rugo HS, Seneviratne L, Beck JT, et al. Prevention of everolimus-related stomatitis in women with hormone receptor-positive, HER2-negative metastatic breast cancer using dexamethasone mouthwash (SWISH): a single-arm, phase 2 trial. Lancet Oncol 2017; published online March 14. http://dx.doi.org/10.1016/S1470-2045(17)30109-2.
1
Supplementary appendix Supplement to: Rugo HS, Seneviratne L, Beck JT, et al. Prevention of everolimus/exemestane–related stomatitis in women with hormone receptor–positive metastatic breast cancer using dexamethasone mouthwash: results from the phase 2, single-arm SWISH trial.
2
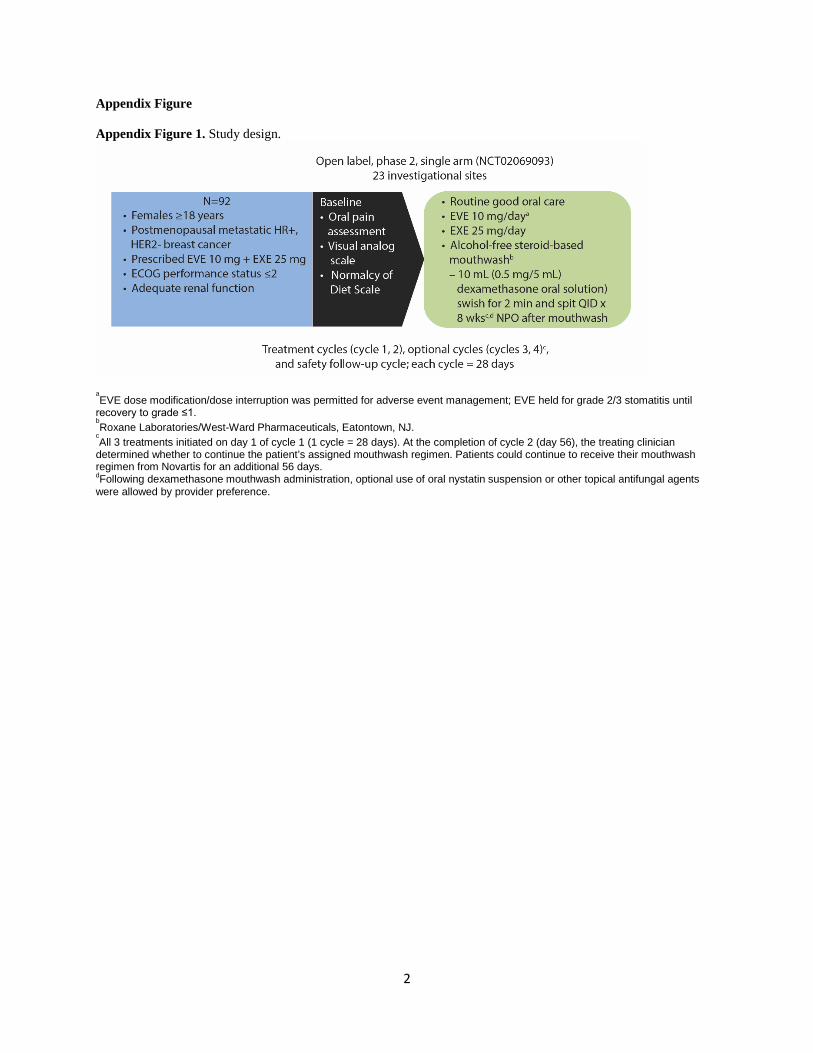
Appendix Figure Appendix Figure 1. Study design.
aEVE dose modification/dose interruption was permitted for adverse event management; EVE held for grade 2/3 stomatitis until
recovery to grade ≤1. bRoxane Laboratories/West-Ward Pharmaceuticals, Eatontown, NJ.
cAll 3 treatments initiated on day 1 of cycle 1 (1 cycle = 28 days). At the completion of cycle 2 (day 56), the treating clinician
determined whether to continue the patient’s assigned mouthwash regimen. Patients could continue to receive their mouthwash regimen from Novartis for an additional 56 days. dFollowing dexamethasone mouthwash administration, optional use of oral nystatin suspension or other topical antifungal agents were allowed by provider preference.
3
Appendix Figure 2. ECOG performance status between baseline and 8 weeks
*11 patients had missing data at 8 weeks. ECOG: Eastern Cooperative Oncology Group
4
Appendix Tables Appendix Table 1. Dose intensity of everolimus and exemestane
Outcomes
Dose intensity, mg Number of mouthwash applications per day*
Median (range) 10 (3–10) 10 (2.8–10) 25 (8–25) 25 (4–25) 3·95 (1.9–4.0) *Analysis of the full analysis set (N=86). †Analysis of the safety set (N=92). SD: standard deviation.
≥ 16 weeks 33 (35·9) 32 (34·8) 18 (20·9) 33 (35·9) aTreatment was optional after week 8. *Full analysis set evaluated by CTCAE 4.0, NDS and VAS through 8 weeks. †Safety set evaluated by CTCAE 4.0.
6
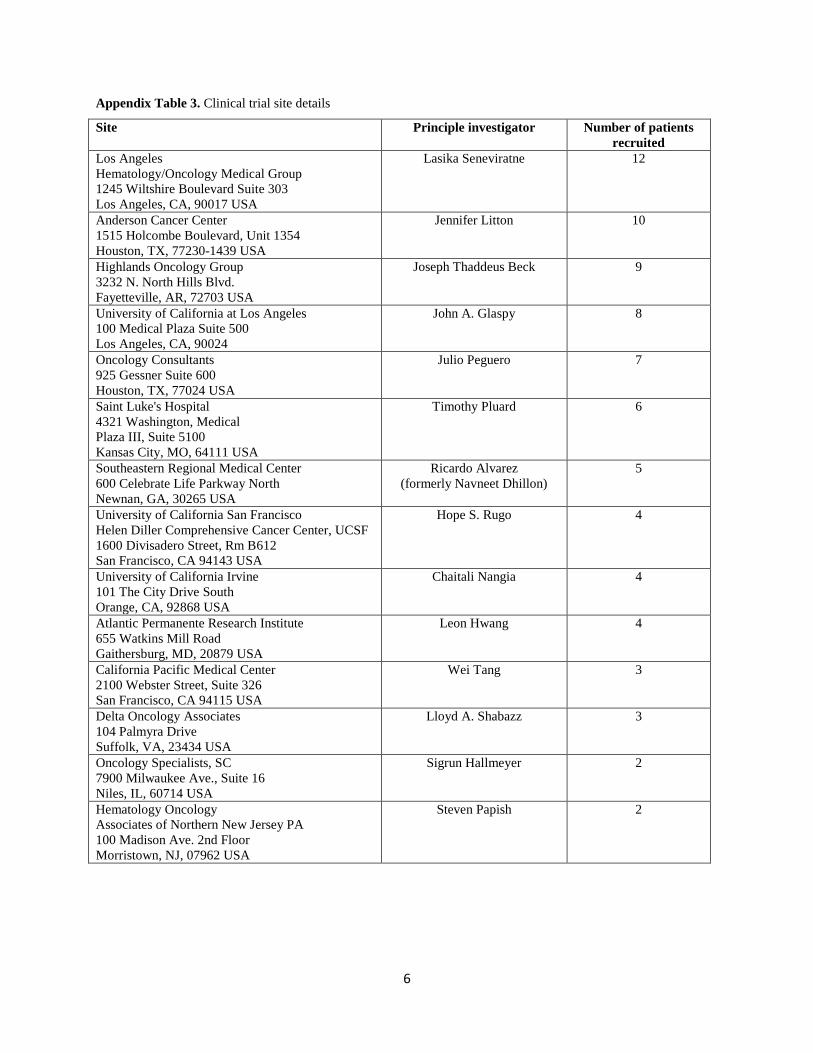
Appendix Table 3. Clinical trial site details
Site Principle investigator Number of patients recruited
Los Angeles Hematology/Oncology Medical Group 1245 Wiltshire Boulevard Suite 303 Los Angeles, CA, 90017 USA
Lasika Seneviratne 12
Anderson Cancer Center 1515 Holcombe Boulevard, Unit 1354 Houston, TX, 77230-1439 USA
Jennifer Litton 10
Highlands Oncology Group 3232 N. North Hills Blvd. Fayetteville, AR, 72703 USA
Joseph Thaddeus Beck 9
University of California at Los Angeles 100 Medical Plaza Suite 500 Los Angeles, CA, 90024
John A. Glaspy 8
Oncology Consultants 925 Gessner Suite 600 Houston, TX, 77024 USA
Julio Peguero 7
Saint Luke's Hospital 4321 Washington, Medical Plaza III, Suite 5100 Kansas City, MO, 64111 USA
Timothy Pluard 6
Southeastern Regional Medical Center 600 Celebrate Life Parkway North Newnan, GA, 30265 USA
Ricardo Alvarez (formerly Navneet Dhillon)
5
University of California San Francisco Helen Diller Comprehensive Cancer Center, UCSF 1600 Divisadero Street, Rm B612 San Francisco, CA 94143 USA
Hope S. Rugo 4
University of California Irvine 101 The City Drive South Orange, CA, 92868 USA
Chaitali Nangia 4
Atlantic Permanente Research Institute 655 Watkins Mill Road Gaithersburg, MD, 20879 USA
Leon Hwang 4
California Pacific Medical Center 2100 Webster Street, Suite 326 San Francisco, CA 94115 USA
Wei Tang 3
Delta Oncology Associates 104 Palmyra Drive Suffolk, VA, 23434 USA
Lloyd A. Shabazz 3
Oncology Specialists, SC 7900 Milwaukee Ave., Suite 16 Niles, IL, 60714 USA
Sigrun Hallmeyer 2
Hematology Oncology Associates of Northern New Jersey PA 100 Madison Ave. 2nd Floor Morristown, NJ, 07962 USA
Steven Papish 2
7
Site Principle investigator Number of patients recruited
Wayne State University/Karmanos Cancer Institute 4100 John R. HW04HO Detroit, MI, 48201 USA
Michael Simon (formerly Sayeh Lavasani)
2
Kaiser Permanente Medical Group 3288 Moanalua St. Honolulu, HI, 96819
Jennifer Carney 2
Northwest Medical Specialties 2920 S. Meridian, Suite 100 Puyallup, WA, 98372 USA
Sibel Blau 2
OnCare Hawaii 98-211 Pali Momi St. Suite 320 Aiea, HI 96701 USA
Arnold K. N. Yee 2
M. Francisco Gonzalez M.D. P.A. Hematology Oncology Center 3 Medical Court Sumter, SC, 29150 USA
M. Francisco Gonzalez 1
Northshore University Health System 2650 Ridge Avenue Evanston, IL, 60201 USA
Douglas Merkel 1
University of Maryland School of Medicine 650 West Baltimore Street, 7N Baltimore, MD, 21201 USA
Timothy Meiller 1
University of Connecticut Health Center 263 Farmington Avenue Farmington, CT, 06030-3940 USA
Rajesh V. Lalla 1
Regional Cancer Care Associates 1930 E. Route 70, Suite V107 Cherry Hill, NJ 08003 USA
Priya Gor 1
8
Appendix Table 4. Exclusion criteria Patients eligible for enrollment in this study must not meet any of the following criteria: 1 Patients currently receiving anticancer therapies (except bisphosphonates, denosumab) 2 Patients who currently have stomatitis/oral mucositis/mouth ulcers 3 Known intolerance or hypersensitivity to everolimus or other rapamycin analogs (e.g. sirolimus,
temsirolimus) 4 Known impairment of GI function or GI disease that may significantly alter the absorption of oral
everolimus 5 Uncontrolled diabetes mellitus as defined by HbA1c > 8% despite adequate therapy. Patients with a known
history of impaired fasting glucose or diabetes mellitus (DM) may be included, however blood glucose and antidiabetic treatment must be monitored closely throughout the trial and adjusted as necessary
6 Patients who have any severe and/or uncontrolled medical conditions such as: •Unstable angina pectoris, symptomatic congestive heart failure, myocardial infarction ≤6 months prior to start of everolimus, serious uncontrolled cardiac arrhythmia, or any other clinically significant cardiac disease •Symptomatic congestive heart failure of New York heart Association Class III or IV •Active (acute or chronic) or uncontrolled severe infection, liver disease such as cirrhosis, decompensated liver disease (except for Hepatitis B and Hepatitis C positive patients) •Known severely impaired lung function (spirometry and DLCO 50% or less of normal and O2 saturation 88% or less at rest on room air) •Active, bleeding diathesis
7 Chronic treatment with corticosteroids or other immunosuppressive agents. Topical or inhaled corticosteroids are allowed
8 Known history of HIV seropositivity 9 Patients who have received live attenuated vaccines within 1 week of start of everolimus and during the
study. Patient should also avoid close contact with others who have received live attenuated vaccines. Examples of live attenuated vaccines include intranasal influenza, measles, mumps, rubella, oral polio, BCG, yellow fever, varicella and TY21a typhoid vaccines
10 Patients who have a history of another primary malignancy, with the exceptions of: non-melanoma skin cancer, and carcinoma in situ of the cervix, uteri, or breast from which the patient has been disease free for ≥3 years
11 Patients with a history of non-compliance to medical regimens or who are considered potentially unreliable or will not be able to complete the entire study or patient diaries
12 Patients who are currently part of any clinical investigation or who has not had resolution of all acute toxic effects of prior anti-cancer therapy to NCI CTCAE version 4.03 Grade 1 (except alopecia or other toxicities not considered a safety risk for the patient at investigator’s discretion).
9
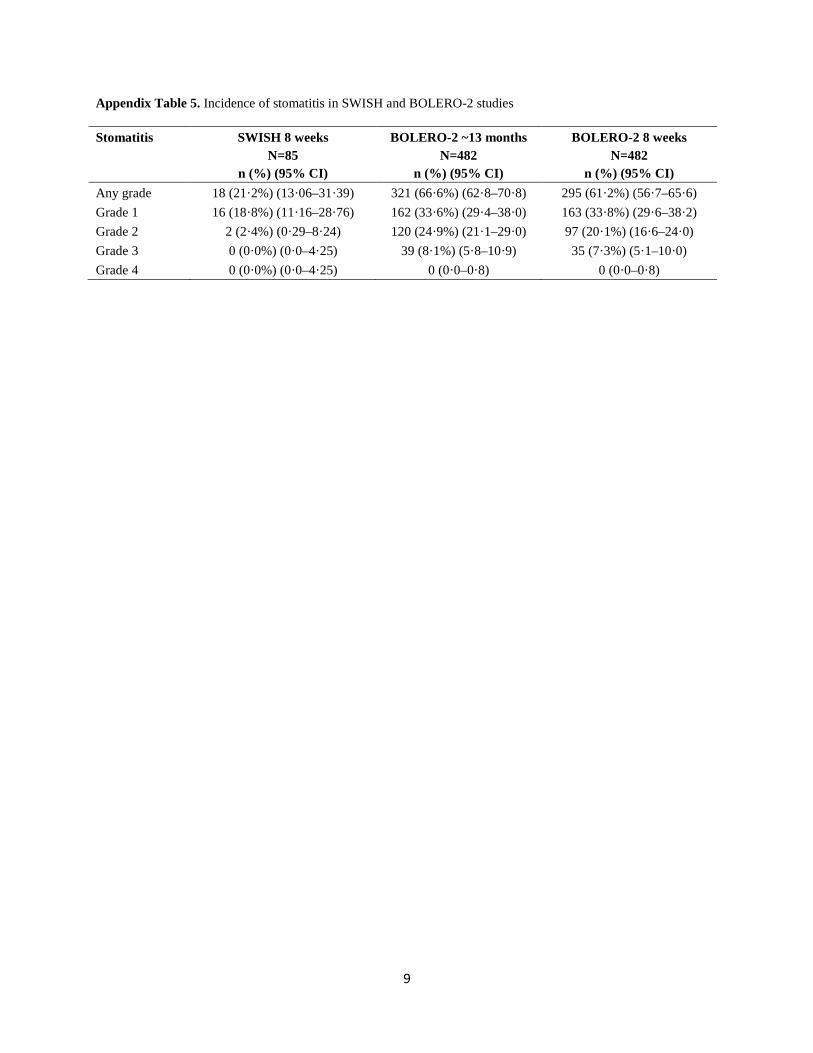
Appendix Table 5. Incidence of stomatitis in SWISH and BOLERO-2 studies Stomatitis SWISH 8 weeks
Other drugs affecting bone structure and mineralization 7 (8·1)
Other immunosuppressants 3 (3·5)
Other therapeutic products 10 (11·6)
Platinum compounds 7 (8·1)
Pyrimidine analogues 24 (27·9)†
Taxanes 49 (57·0)
Vinca alkaloids and analogues 1 (1·2) *49 (57.0%) of patients received cyclophosphamide, and 1 (1.2%) received cyclophosphamide with doxorubicin †13 (15·1%) of patients received capecitabine.