Spring LM, Gupta A, Reynolds KL, et al. Neoadjuvant endocrine therapy for estrogen receptor–positive breast cancer: a systematic review and meta-analysis. JAMA Oncol. Published online June 30, 2016. doi:10.1001/jamaoncol.2016.1897. eMethods. Search Strategy
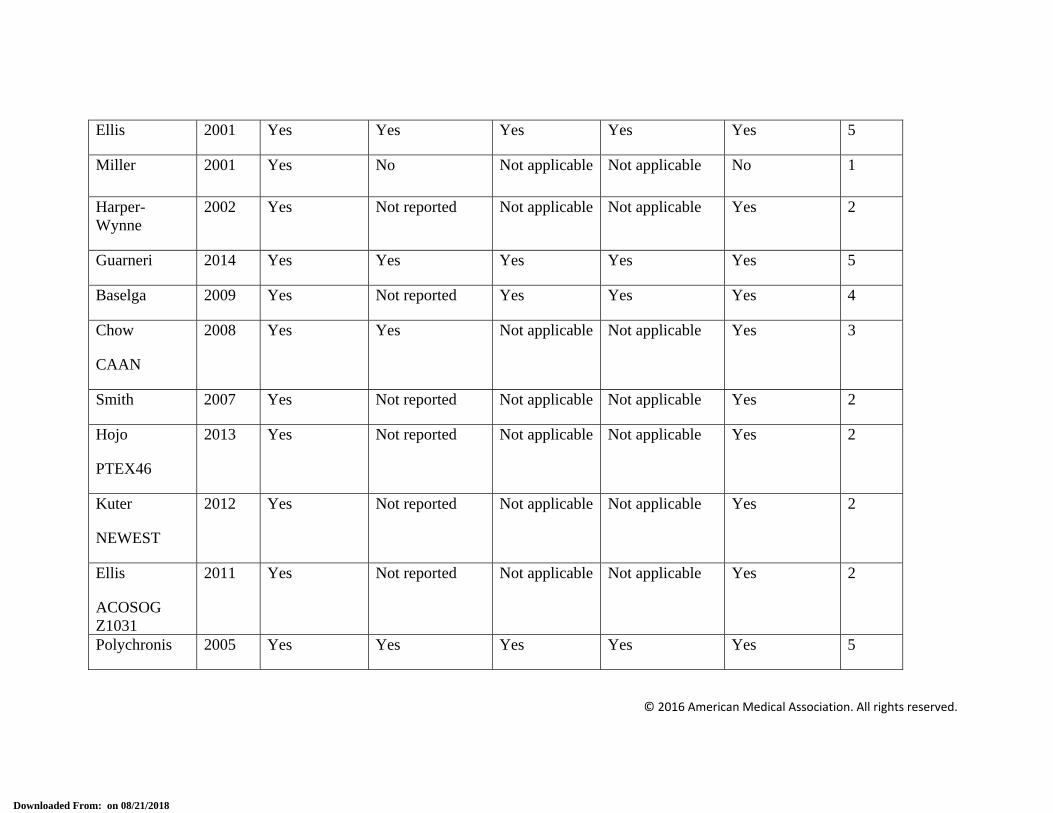
eTable 1. Study Quality of Eligible Trials
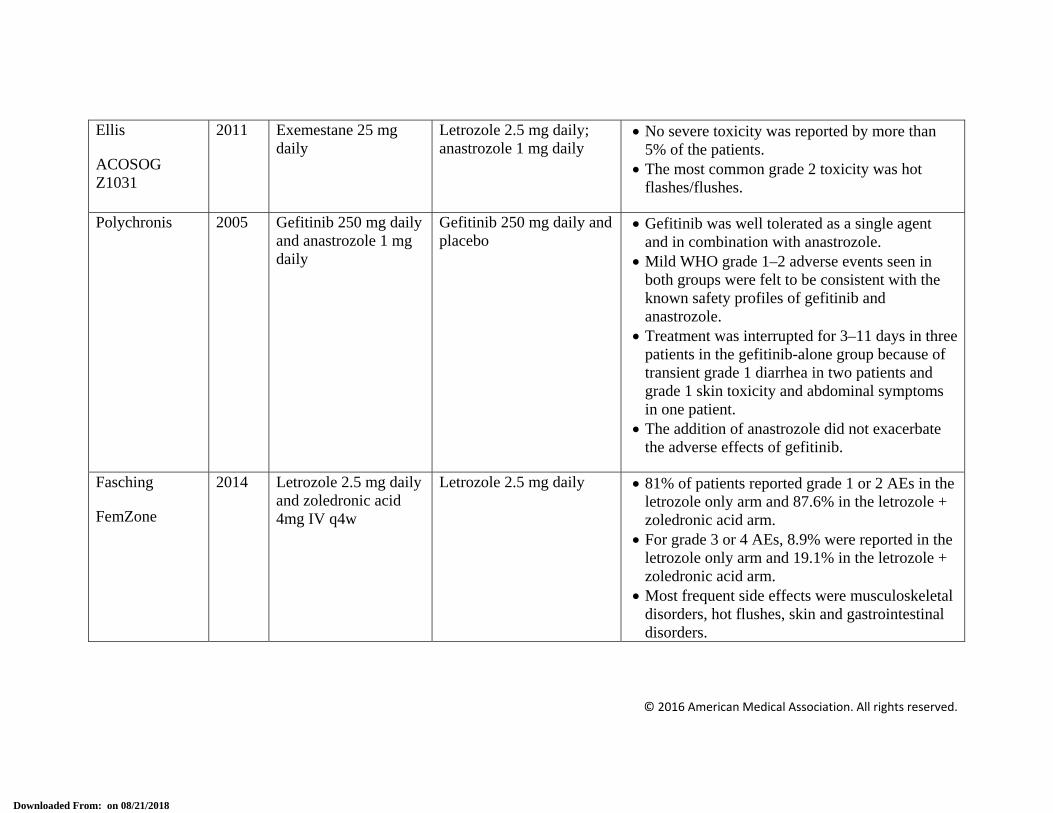
eTable 2. Summary of Toxicities
eFigure 1. Flowchart for Manuscript Selection
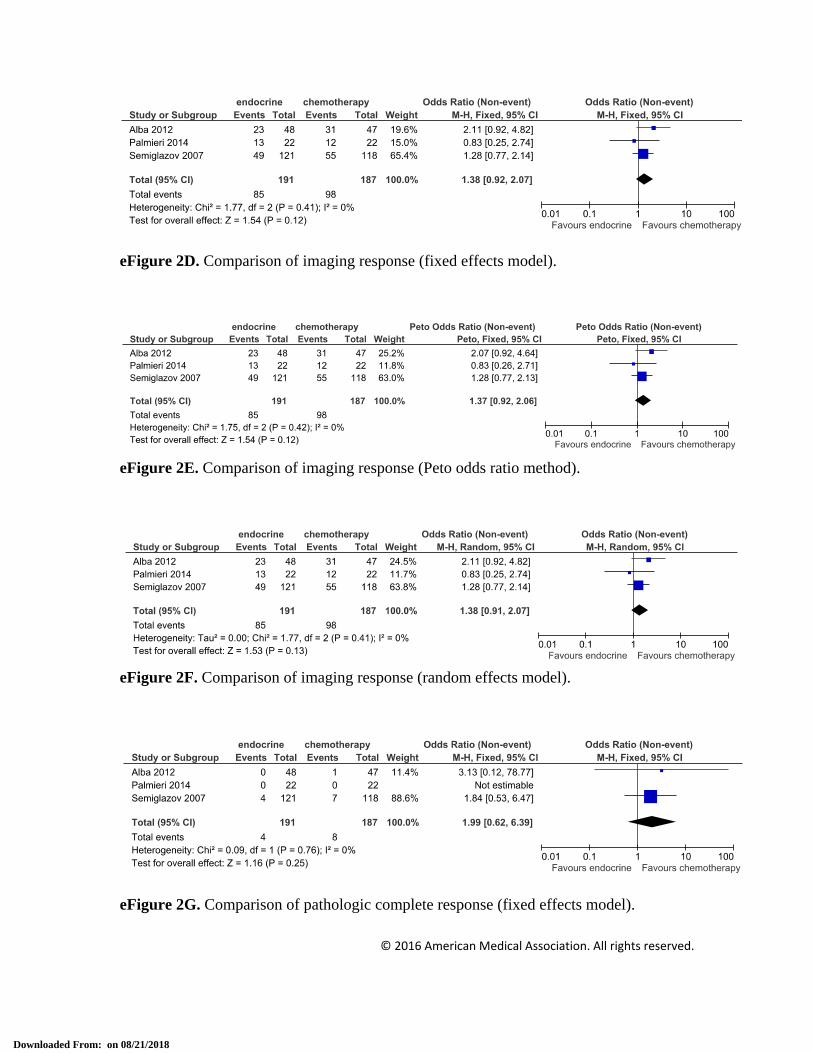
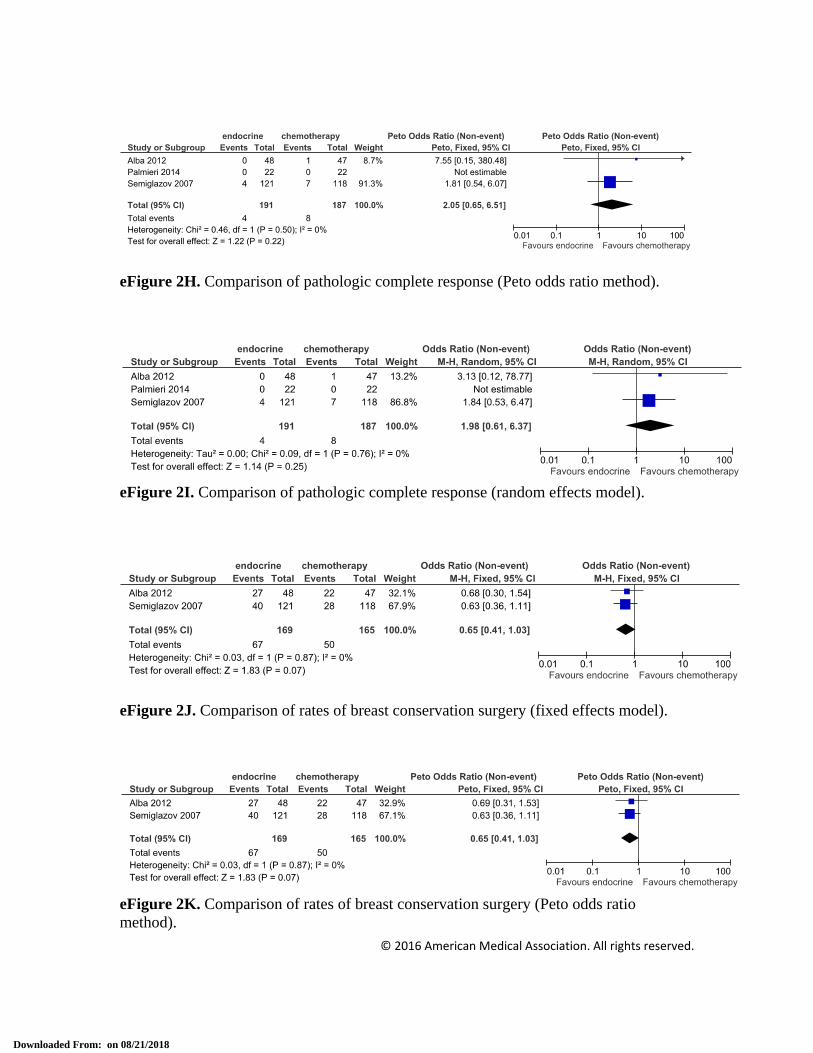
eFigure 2. Neoadjuvant Hormone Therapy vs Neoadjuvant Cytotoxic Chemotherapy
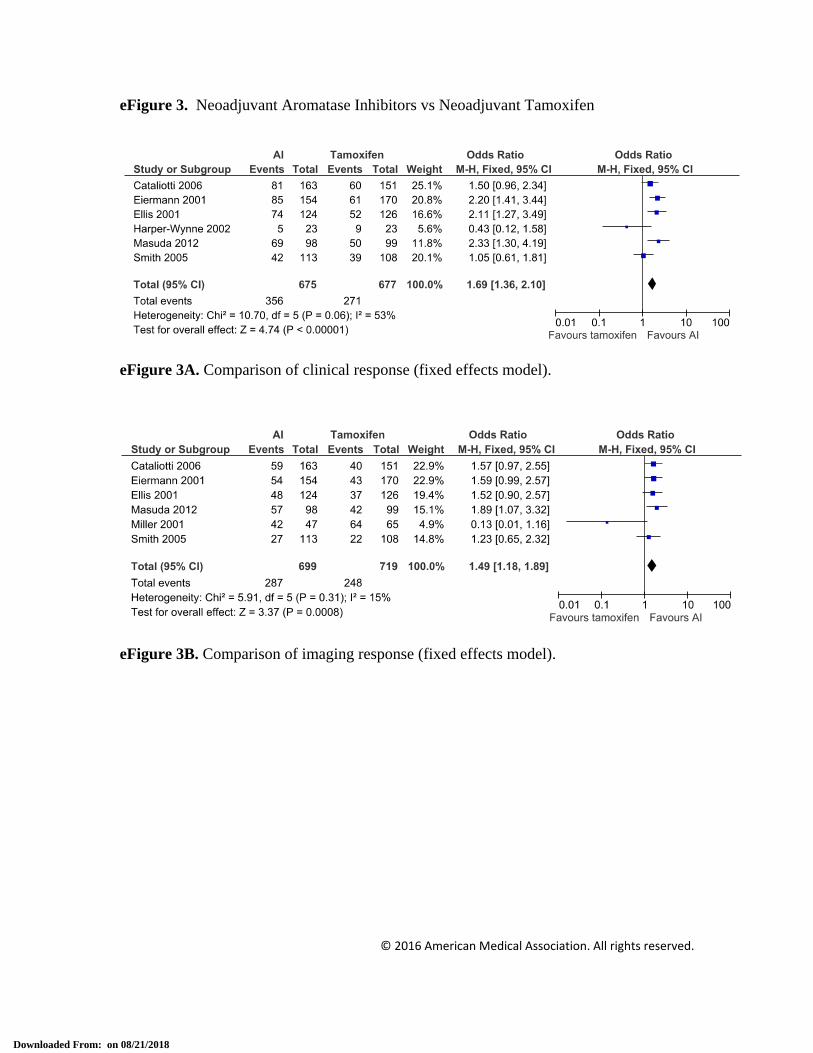
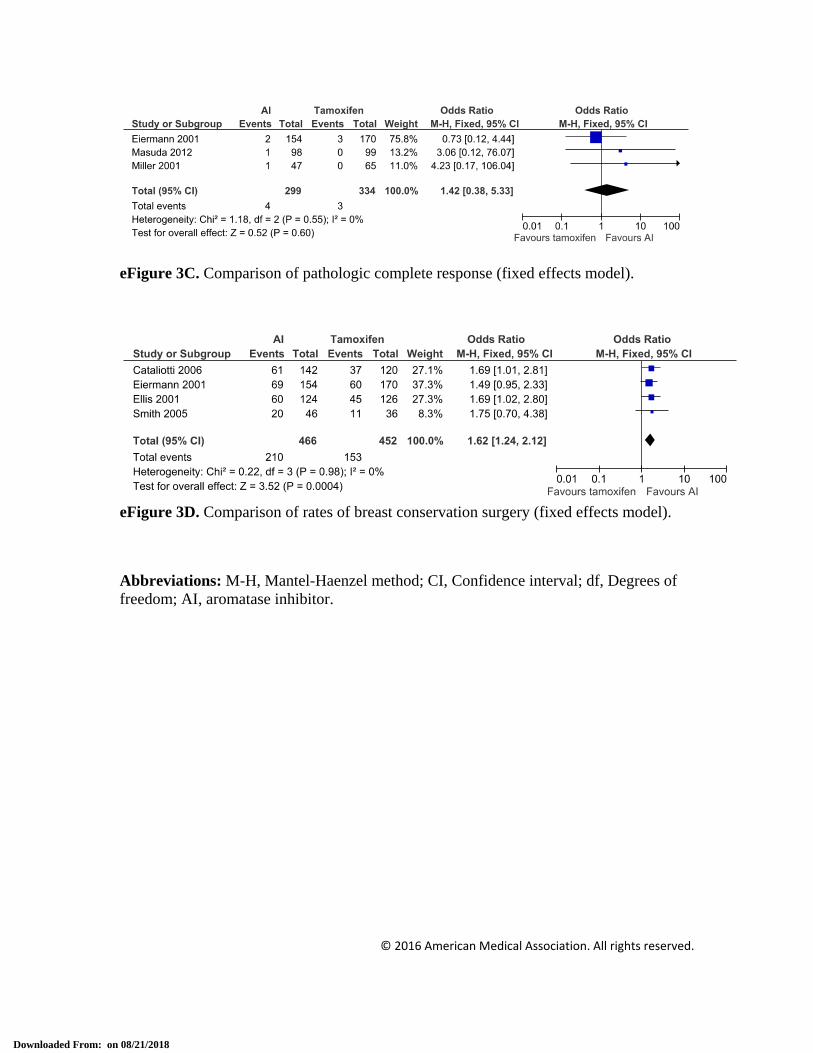
eFigure 3. Neoadjuvant Aromatase Inhibitors vs Neoadjuvant Tamoxifen
eFigure 4. Neoadjuvant Endocrine Therapy vs Dual Therapy
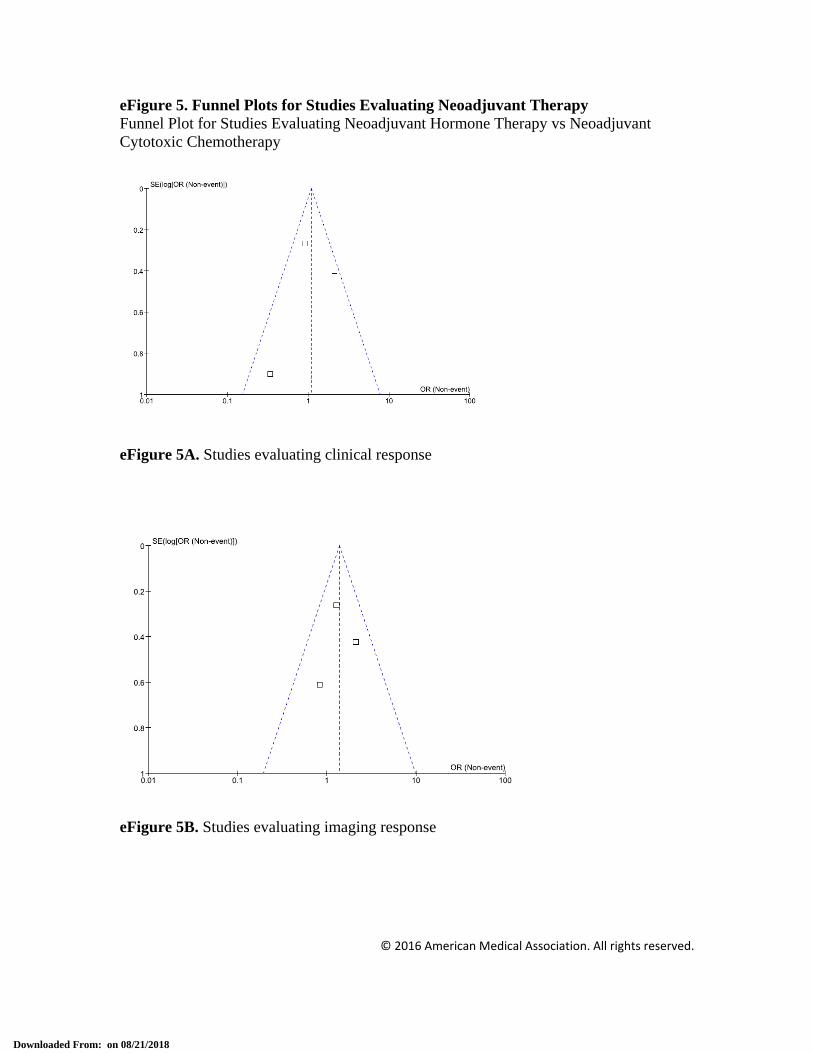
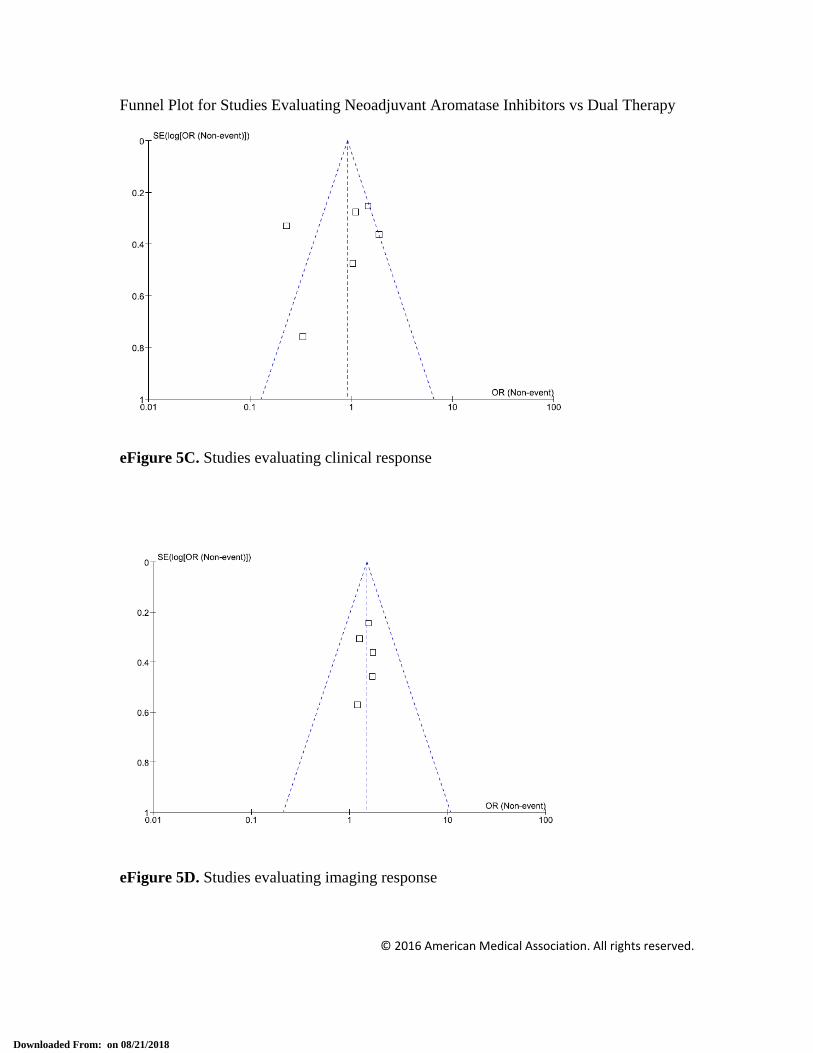
eFigure 5. Funnel Plots for Studies Evaluating Neoadjuvant Therapies
This supplementary material has been provided by the authors to give readers additional information about their work.
((Neoadjuvant Therapy[mesh] OR (neoadjuvant endocrine OR neoendocrine[tiab]) AND (breast cancer[tiab] or breast malignancy*[tiab] or breast tumor*[tiab] or breast tumour*[tiab] or breast neoplasms[mesh] or stage i breast[tiab] or stage ii breast[tiab] or stage iii breast[tiab] or localized breast[tiab] or localised breast[tiab] NOT (metastasis OR metastases OR secondary OR lcis OR dcis)).
47% of patients given CT had grade 3–4 toxicity (excluding amenorrhea) based on NCI-CTCAE 3.0, compared with 9% of patients receiving HT (P < 0.001).
Patients receiving CT experienced more gastrointestinal toxicity, leukopenia, and neutropenia, with a febrile neutropenia rate of 7%.
Palmieri
NEOCENT
2014 Letrozole 2.5 mg daily FEC: 5-fluorouracil 500-600 mg/m2 + epirubicin 75-100 mg/m2 + cyclophosphamide 500-600 mg/m2 x 6 cycles q21d; switched to docetaxel 100 mg/m2 after 3 cycles if SD or PD (N = 11)
Statistically significant differences between treatment groups favoring letrozole were seen in relation to alopecia, nausea, vomiting, stomatitis and anemia.
There were eight serious adverse reactions, all occurring in those who received CT. Six were neutropenia-related.
The incidence of commonly reported adverse events was higher in patients who receiving CT.
No serious adverse events were reported in patients who were receiving HT.
Six patients who were receiving CT experienced febrile neutropenia that led to treatment interruption.
Eiermann
P024
2001 Letrozole 2.5 mg daily Tamoxifen 20 mg daily The nature and frequency of commonly reported AEs was the same for the letrozole and tamoxifen groups (57% in each group).
The most commonly reported AEs related to study treatment were hot flushes and nausea.
Tamoxifen 20 mg daily All treatments were generally well tolerated. The most common adverse event in all groups
was hot flashes, with a nonsignificant trend towards a lower incidence with anastrozole (18%) than with tamoxifen (26%) or the combination (28%).
The only significant difference was in vaginal discharge, which was not reported in any patient on anastrozole (0%) compared with 6% of patients on tamoxifen and 8% of patients on the combination.
Treatment-related AEs were reported by 84% patients in the anastrozole group and 77% patients in the tamoxifen group, with the majority being grade 1 or 2.
50% of patients in the anastrozole group reported musculoskeletal and connect tissue disorder AEs compared to 30% in the tamoxifen group.
Cataliotti 2006
Anastrozole 1 mg daily
Tamoxifen 20 mg daily Both anastrozole and tamoxifen were well tolerated.
AEs considered to be study related were reported in 20.2% of patients in the anastrozole group and 18.1% of patients in the tamoxifen group.
The safety profile was described as consistent with historical results of everolimus monotherapy: grades 3 to 4 AEs occurred in 22.6% of patients who received everolimus and in 3.8% of patients who received placebo.
Dose reduction or interruption as a result of an AE occurred in 52.9% of the everolimus-treated patients versus 7.6% of the placebo-treated patients.
One patient (4%) from the exemestane monotherapy group experienced grade 3 hot flashes.
No other serious and/or severe adverse event was reported in the study.
Smith 2007 Anastrozole 1 mg daily and gefitinib 250 mg daily (combined 2 arms, gefitinib 14 vs. 16 weeks)
Anastrozole 1 mg daily 13% of patients assigned to gefitinib and anastrozole discontinued treatment because of AEs, compared with 2% receiving anastrozole alone.
Hojo
PTEX46
2013 Exemestane 25 mg daily
Exemestane 25 mg daily Not reported
Kuter
NEWEST
2012 Fulvestrant 500 mg/month + 500 mg on day 14 of month 1
Fulvestrant 250 mg/month Both treatments were well tolerated. Treatment-related AEs were experienced by
37.4 and 30.7% of patients and treatment-related serious AEs by 0.9 and 3.0% of patients in the fulvestrant 500 mg and fulvestrant 250 mg groups, respectively.
Gefitinib was well tolerated as a single agent and in combination with anastrozole.
Mild WHO grade 1–2 adverse events seen in both groups were felt to be consistent with the known safety profiles of gefitinib and anastrozole.
Treatment was interrupted for 3–11 days in three patients in the gefitinib-alone group because of transient grade 1 diarrhea in two patients and grade 1 skin toxicity and abdominal symptoms in one patient.
The addition of anastrozole did not exacerbate the adverse effects of gefitinib.
Fasching
FemZone
2014 Letrozole 2.5 mg daily and zoledronic acid 4mg IV q4w
Letrozole 2.5 mg daily 81% of patients reported grade 1 or 2 AEs in the letrozole only arm and 87.6% in the letrozole + zoledronic acid arm.
For grade 3 or 4 AEs, 8.9% were reported in the letrozole only arm and 19.1% in the letrozole + zoledronic acid arm.
Most frequent side effects were musculoskeletal disorders, hot flushes, skin and gastrointestinal disorders.
Common treatment-related side effects such as nausea, vomiting, bone marrow suppression, and mucositis were similar in both groups, but hot flush was more prevalent in the CT/HT arm compared with the CT arm (P = 0.023).
Q21d: every 21 days; q4w: every 4 weeks; CT: chemotherapy; HT: hormone therapy; NCI-CTCAE: National Cancer Institute Common Terminology Criteria for Adverse Events; AEs: adverse events; WHO: World Health Organization.
Excluded (N = 450) based on abstract review Duplications (N = 200) Did not meet criteria (N = 250)
RCTs included (N = 20) CT x HT with AI (N = 3) HT plus CT x CT (N = 1) HT with tamoxifen x HT with AI (N = 6) HT with tamoxifen x HT with AI x HT with tamoxifen/AI (N = 1) HT with AI of differing durations (N = 1) HT with SERD of differing doses (N = 1) HT with 3 different AIs (N = 1) HT and other agents (N = 6)
RCTs excluded (N =7) Duplicate (N = 1) Lack of data (N = 1) Incorrect outcome (N = 5)
eFigure 4G. Comparison of clinical response for neoadjuvant endocrine therapy versus dual therapy with a growth factor pathway inhibitor (fixed effects model).
eFigure 4H. Comparison of clinical response for neoadjuvant endocrine therapy versus dual therapy with a growth factor pathway inhibitor (Peto odds ratio method).
eFigure 4I. Comparison of clinical response for neoadjuvant endocrine therapy versus dual therapy with a growth factor pathway inhibitor (random effects method).
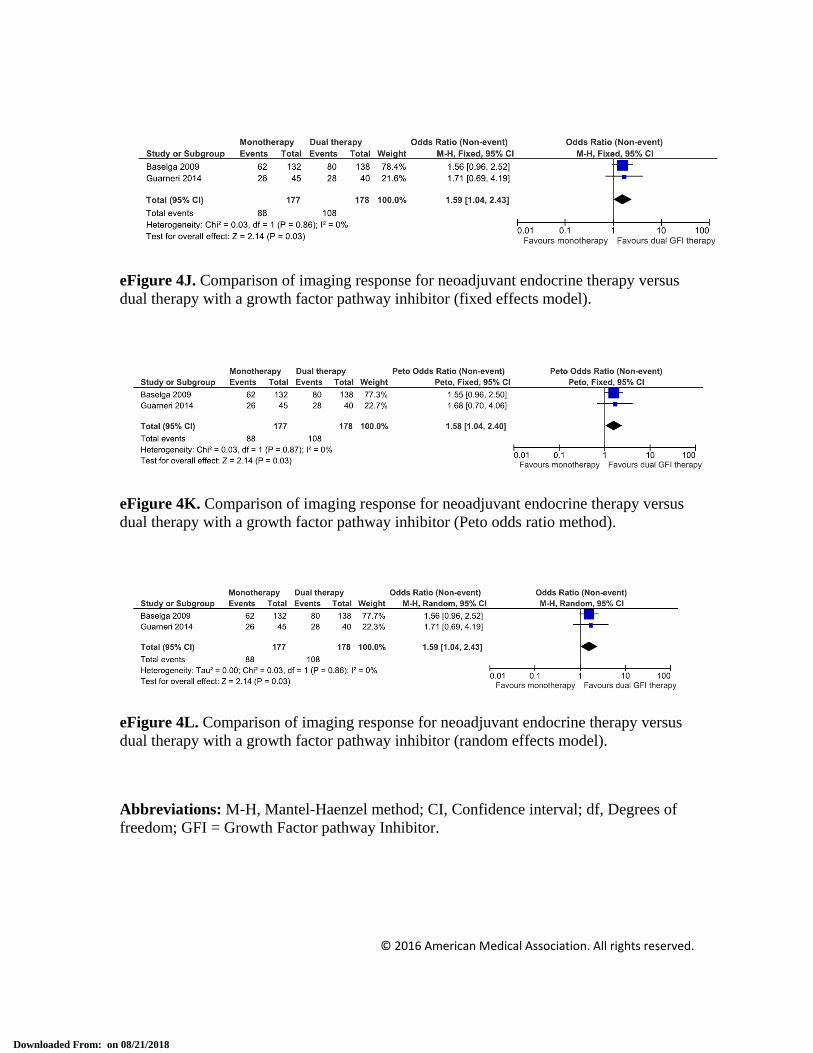
eFigure 4J. Comparison of imaging response for neoadjuvant endocrine therapy versus dual therapy with a growth factor pathway inhibitor (fixed effects model).
eFigure 4K. Comparison of imaging response for neoadjuvant endocrine therapy versus dual therapy with a growth factor pathway inhibitor (Peto odds ratio method).
eFigure 4L. Comparison of imaging response for neoadjuvant endocrine therapy versus dual therapy with a growth factor pathway inhibitor (random effects model).