16
| Date post: | 18-Feb-2016 |
| Category: |
Documents |
| Upload: | thelsjm-ltd |
| View: | 213 times |
| Download: | 0 times |
114 lsjm 30 november 2009 volume 01

115lsjm 30 november 2009 volume 01
EDITORIAL
Welcome to this ‘Innovation’ issue of the London Student Journal of Medicine.
In this section, innovation can be found in everything from revolutionary surgical procedures to the evolution of new working practices for trainee surgeons.
Kavit Amin’s article on face transplant surgery and Anuja Mitra’s discussion of laparoscopic robotic surgery both demonstrate the ethical complexity typical of medical advances. In the case of face transplantation, surgery finds itself amidst the profound challenges faced by patients who have to come to terms with a procedure whose success will most likely cause them crises of identity while leaving them significantly disabled. In contrast, the lower costs, shorter healing times and reduced likelihood of complication offered by laparoscopic robotic surgery appear to present a more straightforward set of gains for the patient and the National Health Service. Similarly promising is the work of Professor Bown at the National Medical Laser Centre in pioneering photodynamic therapy, minimising the invasivenessv common to so many other cancer treatments.
But it is not only in procedures that we can find huge innovation affecting the work of surgeons. Debate of changes to working practice lead Naomi Kaplan and Jarnail Bal to show how entrenched opinion in our profession has become towards the European Working Time Directive. We welcome your contributions to this debate by writing to us: [email protected].
Less contentious, but equally innovative, is the World Health Organisation Surgical Safety Checklist which we featured in our first issue. Building upon this, Carson-Stevens et al. show how student involvement in the initiative will build awareness and hopefully produce a generation of surgeons and healthcare professionals that adhere to a common set of high standards, wherever they practice. The London launch of the Safe Surgery Student Mentor Project was held 22 October 2009 – more information at http://www.safesurg.org/student-mentors.html. Hope can also be found in Nick McNally’s description of the way that Academic Health Science Centres are innovating the way we practice medicine (covered in the last issue) by providing a centre of excellence for research and providing a streamlined path to translational research from bench to bedside.
On matters closer to home, Jonathan Cheah, Associate Editor for the Surgery Section will be stepping down in January to pursue other commitments and we welcome statements of interest from anyone who wishes to find explore the option of joining the LSJM team. For more details, please send any enquires to jonathan.cheah or [email protected]
In summary then, this issue shows us surgery at its most dynamic: innovative, pioneering and revolutionary - facing head on the complexity and controversy generated by ethical and political challenges.
Milan Makwana & Jonathan Cheah
Section Editors Surgery
Illu
stra
tion
: Ella
Bee
se

116 lsjm 30 november 2009 volume 01
NEWS
Robots and Medicine Exhibition A new exhibition at the Hunterian Museum at the Royal College of Surgeons of England explores the history and potential for robots in all areas of Medicine. Sci-Fi Surgery: Medical Robots runs from 8 September – 23 December 2009 and alongside robots in current use today also features robots from the world of science fiction. (For more information see www.rcseng.ac.uk) Prostate Specific Antigen and Screening for Prostate Cancer BMJ 2009;339:b3537 Swedish researchers using a national cohort have sought to evaluate the use of prostate specific antigen (PSA) as a screening tool for prostate cancer. Patients with prostate cancer and their initial PSA levels, taken on average 7 years prior to diagnosis were compared to matched individuals who did not develop prostate cancer. The authors could not identify a cut-off value that had a high enough sensitivity and specificity to validate the use of PSA as a screening marker. However, it appeared that a PSA concentration of below 1ng/mL virtually ruled out a subsequent diagnosis of prostate cancer during the follow-up period of the trial. They concluded that the search for a suitable marker must continue before population based prostate cancer screening can be introduced.
Mild Gestational Diabetes – Treat or Not?N Engl J Med. 2009 Oct 1;361(14):1339-48
A recent large multi-centred trial has sought to elucidate if treating mild gestational diabetes has any effect on pregnancy outcomes. 958 women who were in their 24th-31th week of gestation with a blood glucose concentration of 7.5-11.1mmol/L after a 1 hour 50g oral glucose tolerance test, but a fasting glucose concentration of below 5.3mmol/L, were randomised to treatment or usual ante-natal care. The treatment arm consisted of nutritional counseling, glucose self-monitoring and insulin if required. No significant difference was noted in the composite endpoint, a combination of stillbirth or perinatal death and neonatal complications. However, treatment compared to control was associated with lower mean birth weights (3302g vs. 3408g), lower risk for large-for-gestational-age infants (7% vs. 14%), caesarean deliveries (27% vs. 34%), and preeclampsia or gestational hypertension (9% vs. 14%).
Surgery for Carpal Tunnel Syndrome?Lancet. 2009 Sep 26;374(9695):1074-81
To determine the effectiveness of surgery for patients with carpal tunnel syndrome without denervation, American researchers randomised 116 patients to either surgical or non-surgical treatment including hand exercises and splinting. Hand function and symptoms were measured using the Carpal Tunnel Syndrome Assessment Questionnaire by blinded investigators. Patients in the non-surgical group, if still symptomatic after three months were offered a surgical opinion and as a result substantial crossover did occur. Using intention to treat analysis, 67% of patients had functional improvement of 30% or more at 1 year with surgery, compared to 46% with nonsurgical treatment. However, the authors conclude that although patients in the surgical treatment group fared better and is a useful treatment for carpal tunnel syndrome, the magnitude of the improvement over conservative techniques was of only ‘moderate clinical relevance’.
Hospital Mortality and SurgeryN Engl J Med. 2009 Oct 1;361(14):1368-75
Nearly 85,000 patients enrolled in the American College of Surgeons National Surgical Quality Improvement Program were followed and hospital rates of mortality and post-operative complications studied. Rates of mortality ranged from 3.5% in low-mortality hospitals to 6.9% in high mortality centres. However,
centres, both high-mortality and low-mortality, had similar rates of overall complications (24.6% vs. 26.9%) and major complications (18.2% vs. 16.2%). The rates of mortality after major complications significantly differed. These included myocardial infarction and acute renal failure, which were 21.4% in high-mortality centres vs. 12.5% in low-mortality centres (P<0.001). These findings suggest that although reducing post-operative complications is beneficial, the appropriate management of surgical patients once they suffer complications is also crucial in reducing mortality following surgical procedures.
Surgery Worries for Patients Researching on the InternetAnn R Coll Surg Engl 2009; 91: 460–463
Misleading information found on the internet regarding surgery has been found to cause worry and confusion in 26% of patients who looked for it. Of the 105 patients surveyed at the Chesterfield Royal Hospital one in four found the information they discovered on the internet worrying. Over half of the patients searched the internet using a search engine that could provide results subject to commercial prejudice and populated with inconsistent information. The Royal College of Surgeons has commented that ‘it is vital that patients have access to appropriate, understandable information before and after an operation. Too often information provided online is patchy, unregulated and inconsistent’.
117lsjm 30 november 2009 volume 01
PROFILE
Pict
ure:
Pro
fess
or S
teph
en B
own
Profile of Professor Stephen BownCurrent PostProfessor of Laser Medicine and SurgeryDirector of the National Medical Laser Centre, UCL Division of Surgery and Interventional ScienceHonorary Consultant Gastroenterologist, University College Hospital
Undergraduate trainingBA Physics, Cambridge UniversityMasters in Physics, Harvard UniversityPre-Clinical Medicine, Cambridge UniversityClinical Medicine, University College London
PostgraduateMD, MRCP (UK), FRCP (UK)
What do you do? I run and co-ordinate transitional research projects in the diagnostic and therapeutic use of light and undertake three clinics a week in therapeutic endoscopy.
Why did you get involved in surgery? I am not a surgeon but have always worked closely with surgeons. The attraction of endoscopes is due to the application of physics with practical procedures, interesting instruments and no cutting or stitching!
Describe your typical day On a mixed day of clinical and academic work I am on the wards first thing in the morning giving tutorials to students. I will then go back to the office and have academic meetings about research projects. In the afternoon, I will go back to the hospital to do an endoscopy list. I also do a lot of travelling as I work within a small research field and meet many interest-ing people around the world. I have given invited lectures in 41 countries.
What have been your major achievements? Bringing together scien-tists and clinicians and overcoming the barriers between the clinical world and science. Also, establishing photodynamic therapy as a viable treatment option in many different fields.
What is Photodynamic Therapy (PDT) and what are its applications?PDT is a combination of drug and light. You activate the photosen-sitising drug with light of a wavelength matched to the absorption peak of the drug, thus only having a biological effect where you get drug and light. It is a non-thermal effect so kills living tissues but doesn’t kill collagen or elastin so maintaining mechanical integrity. It is currently used in the treatment of head and neck cancer, all stages of oral cancer, Barrett’s oesophagus and cancers of the skin and bile duct. Exciting new projects in early clinical trials include PDT for treatment of cancers of the pancreas and prostate and the prevention of re-stenosis after balloon angioplasty – three tech-niques pioneered at University College Hospital (UCH).
Amongst all the available minimally-invasive ablative technolo-gies in use, will PDT become the one dominant modality? PDT should be seen as complementary to surgery, radiotherapy and chemotherapy. For many patients, the best option is a combina-
tion of treatments. PDT is particularly attractive for small volume disease close to vital structures and where preservation of functional and mechanical integrity is essential. The side effects are usually less and the recovery time shorter with PDT as it is minimally invasive; however, the treatment must be matched to the extent of disease in each patient.
Where do you see PDT in 20 years time? I see it as one of a variety of minimally invasive treatments; we will have to ask when PDT is the best treatment within the range of alternatives.
How do you balance clinical and academic work and do you have any advice for fu-ture clinical academics? The key to a successful academic career is the motivation of the individual. Most doctors prefer a purely clinical working life, but for those who enjoy the challenge of research, the academic life is rich and rewarding.
What are your ambitions for the future? I am involved in the ‘Killing Cancer’ charity which promotes PDT to the general public and raises funds for research. We are also working on optical diagnosis involving spectral analysis to detect normal or neoplastic tissue using large data banks to correlate optical spectra and histology. This technology won a Medical Futures Innovation Award last year. Who or what has been the greatest influence on your practice? My approach to clinical practice was guided by Professor John Lennard Jones (the consultant on my first firm as a clinical student at UCH), but the greatest influence on my medical career has been my background in physics and lasers and the opportunity to put the two together.
What is the most important thing you learnt as a student? Clinical medicine is an art – you can’t expect everything to fit the textbooks. If something doesn’t fit, look around to find an explanation and sometimes accept that there isn’t one. There is a limit to how far it is worth digging to get clinical answers. And be nice to patients and your colleagues at all levels.
Do you have any advice for future students? Be sure you know what you are letting yourself in for in your career choices and look at all the options, both clinical and academic.
Interviewed by: Helen PickburnIntercalating BSc Medical Student, UCL Medical School and LSJM Panellist
118 lsjm 30 november 2009 volume 01
Arguably, the most important development is the shift of the surgical field from 2-dimensional (2D) to 3-dimensional (3D) visual input. As laparoscopic surgery is entirely dependent on visual stimuli, it is essential that the visual system simulates a natural, high quality image of the surgical field. It was demonstrated that the use of 3D vision in laparoscopic surgery superseded 2D techniques of surgery when performing standard laparoscopic tasks on the da Vinci robot. The 3D vision outclassed in both the time taken to complete the procedure and the number of errors that were performed, proving particularly important for suturing2.
The HistoryPreviously, the use of long, rigid laparoscopic instruments had detrimental effects of amplifying tremor and reducing the range of movement. Currently, these instruments are shorter with tremor abolition filters and motion scaling facilities to eliminate fast movements3.
Robots have been increasingly used in surgery over the last twenty years. In the 1990’s the Probot was the first robot to be used in surgery for the transurethral resection of the prostate to treat benign prostatic hyperplasia4. Perhaps the most renowned and
ARTICLE
IntroductionVideo games have been integrated successfully into modern day culture. The change in demographics of the ‘typical’ gamer has reflected the popularity of this phenomenon. Once held as the purview of school children, the average gamer is now 33 years old with a twelve year history of playing video games1. In 2006, the gaming industry welcomed the release of a highly anticipated new prototype: the Nintendo Wii™. The appeal of this model mainly resided in the fact that the gamer could manipulate objects on the screen using a wireless remote that detected movement in three dimensions. In an age where Minimally Invasive Surgery (MIS) has evolved and we are now looking towards the use of robots in surgery, there have been various anecdotal links suggesting that Video Gaming Experience (VGE) contributes to laparoscopic ability. This article explores the link between VGE and laparoscopic skill and discusses the surgical and societal implications of these findings.
Professor Lord Ara Darzi informs us “The golden age of surgery is waning. The industrial age is being replaced by the information age and laparoscopic surgery provided the wake- up call for the information age”. Laparoscopic surgery is currently held as the gold standard for many surgical procedures, perhaps the most renowned being the laparoscopic cholecystectomy.
Laparoscopic Surgery: Are You Game?Anuja [email protected] 4 Medical Student, Imperial College Londondoi:10.4201/lsjm.surg.007
Sour
ce: w
ww.
intu
itiv
esur
gica
l.com
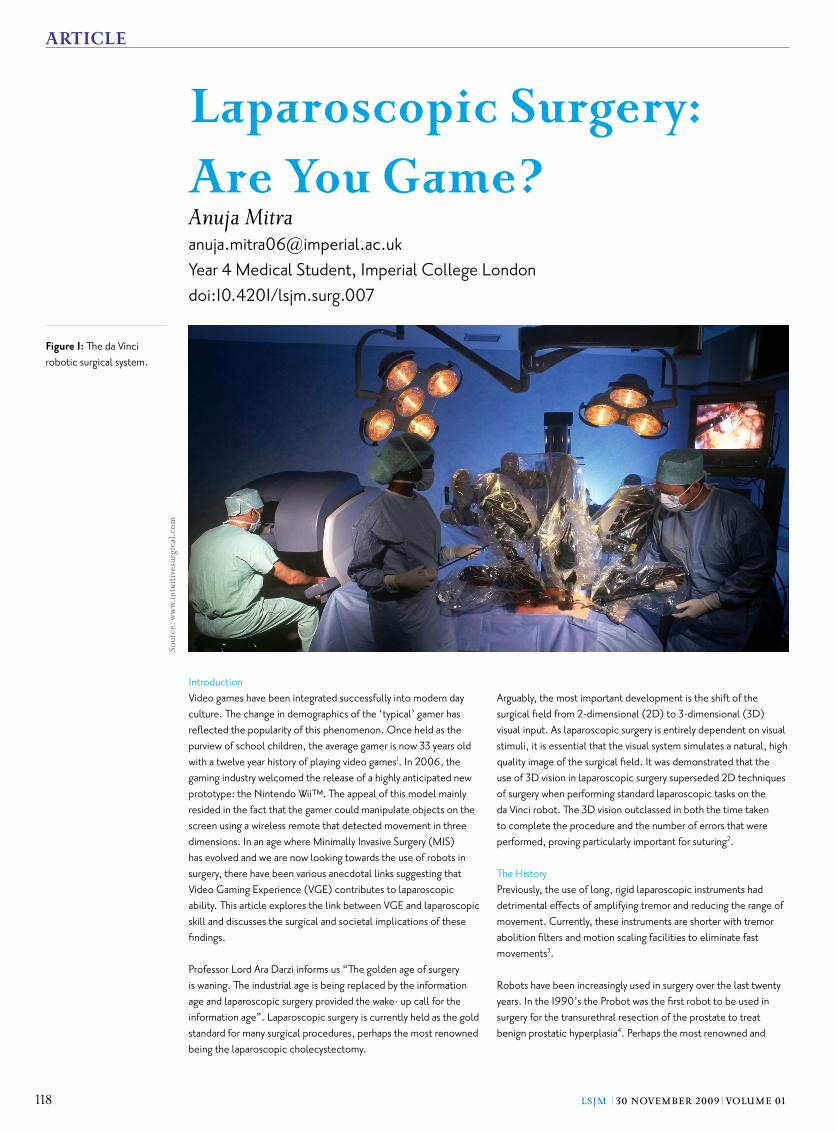
Figure 1: The da Vinci robotic surgical system.
119lsjm 30 november 2009 volume 01
clinically relevant robot up to date is the ‘da Vinci system’ (Figure 1). This was manufactured by an American based company named ‘Intuitive Surgery’ in 2000. It is primarily used for laparoscopic radical prostatectomy and gynaecological surgery, but has been approved for thoracoscopic surgery, laparoscopic and thoracoscopically assisted cardiotomy procedures. The four key components of the da Vinci robot are summarised in Figure 2.5
DiscussionRobotic surgery has its drawbacks, for example longer operative times to execute standard surgical tasks such as capping a hypodermic needle6 and steeper learning curves for basic operations7. However there are some general advantages over open surgery. These are lower morbidity rates, smaller postoperative scars yielding an improved cosmetic result and reduced risk to the patient in terms of intraoperative blood loss and infection rates8.
In laparoscopic surgery, the surgeon has the task of navigating surgical instruments through small incision points on the patient’s body. Operating in a three-dimensional space represented on a viewing screen with minimal tactile feedback constitute basic parallels between laparoscopy and video games9. Surgeons
recognise that laparoscopy has changed the required skill profile
and training needs. It is this new set of skills that have led to anecdotal evidence suggesting VGE is a positive predictive factor for laparoscopic skill10. In particular, professionals believe that the Wii™ has the most potential of any console for trainee surgeons.
The Nintendo Wii™ is a home video gaming system which is the seventh generation console released by Nintendo. Perhaps the most distinguishing feature is the Wii™ remote (Figure 3). The remote is a wireless controller that can be used as a handheld pointing device that allows players to direct on-screen action using a wireless wand. Acceleration is detected in three dimensions11 and the user is able to manipulate and interact with objects on the screen through gesture recognition and pointing.
Video games which require the user to navigate through virtual reality settings such as flying, swimming and racing can lead to the acquisition of complex skills. For instance, depth perception, spatial orientation and visual attention capacity have been shown to develop from a young age12. Accurate hand-eye coordination is a vital skill required in surgery that has been demonstrated to improve with video gaming practice13.
One study explored the relationship between video games and laparoscopic performance by asking participants to perform tasks intended to measure hand–eye coordination, ambidexterity, and depth perception14. The subjects performed three timed laparoscopic tasks on a pelvic trainer. Participants then had 10 minutes of playing on a video game. Finally, subjects repeated the timed laparoscopic tasks. Paired-sample t-tests were used to measure differences between the pre- and post-tests. Results revealed a significant difference between pre and post tests on all three laparoscopic tasks (p = 0.001), (p = 0.008) and (p = 0.000) respectively. The authors concluded that playing video games improved laparoscopic skill and time taken to complete the tasks.
Evidence shows that a brief warm up on a virtual reality simulator ahead of surgery, significantly improves surgical performance by
eliminating the ‘training’ effect15. The use of the Wii™ as a ‘warm up’ tool has been investigated11. A training device called ProMIS which simulates a patient’s body in 3D and tracks the surgeon’s movements as they operate was used in this study. The movements were fed into an algorithm which illustrated Wii™-playing surgeons scored 48% higher on tool control and performance than those without the Wii™ warm-up. It was concluded surgical residents performed better during simulated surgery after playing on the Wii™ console as a warm up to hone their skills.
The advent of MIS poses significantly steeper learning curves and a greater pressure on the individual to master novel skills. A study hypothesised that participants with previous VGE would acquire new surgical skills faster than those with no gaming experience thereby reducing the learning curve. A high VGE was defined as more than 3 hours per week of video game playing. Both groups trained to proficiency on two abstract tasks (Acquire Place and Traversal) on the minimally invasive virtual reality simulator (MIST-VR) and the number of trials required to achieve proficiency were recorded. Results revealed the gamers reached proficiency quicker than the non-gamers (median 0 trials versus 6 trials, p = 0.01) thus it was concluded that previous VGE shortens time to proficiency on two tasks on a validated surgical simulator16.
Figure 2: Key components of the da Vinci robot
Component Advantage
Master console The surgeon is able to manipulate robotic arms by moving dials on the console whilst seated.
Robotic Arms The laparoscopic arms pivot at 1- 2cm operating ports, eliminating the use of the patient’s body for leverage and minimising tissue damage.
Endowrist surgical instruments The instruments enable the surgeon to rotate 360° with 7 degrees of freedom, allowing ambidexterity (2)
3D endoscope visual system Operating images are enhanced, refined and optimized using image synchronizers, high-intensity illuminators and camera control units. The visual system enables a accurate hand- eye relationship to give natural depth perception necessary for precise manipulation of tissue layers
Figure 3: Wii™ remote
ARTICLE

120 lsjm 30 november 2009 volume 01
ARTICLE
Implications on surgical training The success and popularity of laparoscopic surgery poses another dilemma: how shall we train the new generation of surgeons? Surgical training has seen a paradigm shift from traditional training based on apprenticeship to training using a virtual reality (VR) simulator. The MIST- VR training programme is one current curriculum which provides a validated and established approach to assess laparoscopic training on VR simulators17. A study performed with 622 participants showed VR training resulted in a greater reduction in operating time, error and unnecessary movements than standard laparoscopic training18. With VGE being identified as a positive predictive factor for laparoscopic skill, it could have an impact on the current training curriculum. Video games may be used as a practical teaching tool to help train surgeons. In a study performed by Rosser et al on 33 surgical residents, it was shown that video-gamers, past and present were faster, made fewer errors and had higher scores than non-gamers when asked to perform in the Rosser Top Gun Laparoscopic Skills and Suturing Programme10. Therefore training curricula that include video games may help thin the technical interface between surgeons and laparoscopic applications.
However, another study found that although there is a link between VGE and surgical skill, it is not strong enough to warrant changes in the training programme. The relationship between baseline laparoscopic scores and nonsurgical skills were assessed and results showed students who played computer games, typed, utilized chopsticks, or played a musical instrument had better scores and fewer errors than those who did not though this did not reach statistical significance in any comparison19.
Nevertheless, the appeal of video games as an enjoyable, readily available adjunct to VR training is attractive. Software from Nintendo is to be used for the purpose of aiding surgical training by simulating routine procedures11. With the added advantage of vastly cheaper software — the expected price is set to be $250, this is a highly appealing option in comparison to traditional virtual training tools.
Societal implicationsDespite the growing body of evidence showing video gaming to be advantageous in laparoscopic surgery, there are still many unanswered questions and ethical issues which must be addressed before they can be officially incorporated into surgical culture. Video games have been shown to improve laparoscopic skill, however surgical ‘skill’ is one of many important qualities necessary for a successful surgeon. Other qualities such as patient communication, empathy and social interaction have been shown to be hindered by video games. More than 85% of video games contain violence. Research shows that playing violent entertainment games produces aggressive behaviour, affect, and cognition, physiological arousal, desensitisation to real-life violence, and a decrease in pro-social behaviour20. Additionally, the practicalities of introducing video games as an education tool have not been explored yet. What types of video games are optimal for enhancing surgical skill? How often should one play video games? Are there any differences in the types of video games that men and women should use to acquire these skills? The use of video games is an attractive idea but one that has enormous potential for distortion. It is acknowledged that “indiscriminate video game play
is not a panacea”21 and conscientious supervision must be applied to children’s video gaming.
ConclusionWith laparoscopic surgery held as the gold standard for many routine procedures, surgeons must use a different profile of skills to those that were required with open surgery. The immense popularity of video games in modern culture has lead to a suggestion that there is a positive association between VGE and laparoscopic skill. Evidence has demonstrated video games to help in the development and acquisition of a similar set of cognitive skills to what is required in laparoscopic surgery, to act as a warm up prior to surgery to exclude the ‘training’ effect and to reduce the learning curve for novice surgeons. With a change in the training curriculum for laparoscopists which is based on VR simulators, the idea of video games being used as an adjunct seems rational. It is tempting to incorporate this relatively enjoyable, cheap method of training into the curriculum, however a pressing social problem arises with the use of video games. We must make every effort to avoid encouraging a culture of unlimited video gaming with the justification of promoting surgical skills in the generations to follow.
The Nintendo Wii™ has gone on since its launch in 2006 to emphatically outsell its competitors in the market, it seems that time will tell if video games will ever be incorporated formally into the world of surgery. References
Entertainment Software Association. Essential facts about 1. the computer and video game industry. 2006. http://www.theesa.com/archives/files/Essential%20Facts%202006.pdfHubens G, Coveliers H, Balliu L, Ruppert M, Vaneerdeweg W. 2. A performance study comparing manual and robotically assisted laparoscopic surgery using the da Vinci system. Surg Endosc. 2003 Oct;17(10):1595-9. doi:10.1007/s00464-002-9248-1Reynolds RK, Advincula AP. Robot-assisted laparoscopic 3. hysterectomy: technique and initial experience. Am J Surg. 2006 Apr;191(4):555-60. doi:10.1016/j.amjsurg.2006.01.011Davies BL, Hibberd RD, Ng WS, Timoney AG, 4. Wickham JE. The development of a surgeon robot for prostatectomies. Proc Inst Mech Eng H. 1991;205(1):35-8. doi:10.1243/PIME_PROC_1991_205_259_02Intuitive Surgical, Inc. - da Vinci Surgical System.2005. http://5. www.intuitivesurgical.com/ [Last accessed 17 October 2009]Garcia-Ruiz A, Gagner M, Miller JH, Steiner CP, Hahn JF. 6. Manual vs robotically assisted laparoscopic surgery in the performance of basic manipulation and suturing tasks. Arch Surg. 1998 Sep;133(9):957-61. doi:10.1001/archsurg.133.9.957Lenihan JP Jr, Kovanda C, Seshadri-Kreaden U. What is the learning 7. curve for robotic assisted gynecologic surgery? J Minim Invasive Gynecol. 2008;15:589–94. doi:10.1016/j.jmig.2008.06.015Menon M, Tewari A, Baize B, Guillonneau B, Vallancien 8. G. Prospective comparison of radical retropubic prostatectomy and robot-assisted anatomic prostatectomy: the Vattikuti Urology Institute experience. Urology. 2002 Nov;60(5):864-8. doi:10.1016/S0090-4295(02)01881-2Greenfield PM. Technology and Informal Education: 9. What Is Taught, What Is Learned. Science. 2009 Jan 2;323(5910):69-71. doi:10.1126/science.1167190Rosser JC,Jr, Lynch PJ, Cuddihy L, Gentile DA, Klonsky J, Merrell R. 10. The Impact of Video Games on Training Surgeons in the 21st Century. Arch Surg. 2007 Feb;142(2):181-186. doi:10.1001/archsurg.142.2.181
For the full references see thelsjm.co.uk.

121lsjm 30 november 2009 volume 01
ASK THE EXPERT
COMPETITION
Whitehead’s varnish is an antiseptic liquid made from: iodoform 10g, benzoin 10g, prepared storax (a resinous exudate of the Sweetgum tree) 7.5g, Balsam of Tolu 5g (a resin obtained from South American balsam trees) and solvent ether mixed to 100 ml. Whitehead’s varnish has many uses including dressing of skin graft donor sites, packing after exposure of unerupted canine teeth, jaw cavities, and nasal packing.
Whitehead’s varnish remains ‘clean’ and uninfected in contaminated environments like the mouth. The aromatic resins it contains are slowly broken down to produce benzoic acid, which is a potent antiseptic. This, together with its waterproofing capacity makes it more potent than other media. Walter Whitehead was born in 1840 at Halsam Hey, Bury and at the age of 16 he entered his family’s textile business. This is probably when he learned about chemicals and led him to develop his varnish. When he was 19, he was invited by a medical student to observe some operations at the local infirmary. This inspired him
Mystery Object Competition
Can you identify this object from the Hunterian Museum, basedat the Royal College of Surgeons of England?
If so, the Surgery Section has a signed copy of The Knife Man: Blood, Body-Snatching and the Birth of Modern Surgery, a biography of John Hunter, eighteenth-century surgeon by Wendy Moore, to give away. The prize has been kindly supplied by the Hunterian Museum.
to become a doctor. He initially went into general practice, but surgery was his real passion. He became a fellow of the Royal College of Surgeons of Edinburgh in 1866 and at the age of 54 became professor of surgery at the Victoria University, Manchester.
Walter Whitehead was a bold and distinguished surgeon and was known to have said that “the greatest drawback under which a surgeon can suffer is knowledge of anatomy – it makes him timid”.
To enter, e-mail your answer to [email protected] with ‘Mystery Object Competition’ as the subject line along with your name, course and year/place of study by 31 January 2010 . The winner will be the first randomly selected from all the correct entries.
What is Whitehead’s Varnish and who was Walter Whitehead?Luke Cascarini BDS MB BCh FDSRCS FRCS (OMFS) [email protected]
Luke is a Specialist Registrar in Oral and Maxillofacial Surgery at Queen Victoria Hospital East Grinstead, West Sussex and co-author of the surgical text book ‘Principles of Surgery – Everything you need to know but were frightened to ask!’
© The Royal College of Surgeons of England © The Royal College of Surgeons of England
Thank you for your entries from the previous issue. We still haven’t received the winning answer!
122 lsjm 30 november 2009 volume 01
PERSPECTIvE
The European Working Time Directive (EWTD) has met much resistance since coming into effect at European Union level in 19931. Though the British government questioned its legitimacy as health and safety law; it was validated by the European Court of Justice in 19962. The uproar is baffling, considering that this directive was put in place to prevent worker exploitation1, an objective towards which all European countries should be striving. The directive covers a spectrum of employment issues, not limited to: annual leave payment, additional security for night workers as well as appropriate weekly and daily rest periods.3 However the true battle ground remains the 48 hour working week, applicable to doctors in training as of August 1st 20091, that incorporates both overtime3 and on-call time.4 Various points pertaining to the EWTD remain unresolved at the level of European Parliament and Council, most notably the ability of countries to opt out of the directive, in addition to the debate as to whether on-call time can be justified as working time.4 Surgeons in training should not be fighting against an abbreviated work schedule, reduced from the 72 hour weekly timetable accepted in 1991.2 They should instead see this as a much-needed change that will protect their long-term health, safeguard their patients, and provide the necessary impetus to dramatically streamline surgical training.
Importance in Surgery Surgical departments are staffed by surgical trainees according to a schedule of shifts, with surgeons’ hours in the hospital extending well beyond the typical 8 hour working day of many office-based employees. 5 Shift work, which can be divided into night shifts, rotating shifts and ad hoc work hours has the ability to upset both the circadian rhythm and societal integration of those carrying out shifts 5. The health impact of shift work, as opposed to day work, cannot be underestimated. Research has indicated that the risk of coronary heart disease may be higher in women who have undertaken six or more years of shift work.5 The frequency of obesity amongst male and female shift workers is higher than that seen in day workers.6 Metabolic syndrome may be linked to shift work due to the clustering of metabolic risk variables in males and females working shifts.6 Clearly, surgery will never be converted into a nine-to-five job, but any legislation that attempts to normalize hours and incorporate both daily and weekly rest periods must be seen as a valuable attempt at reducing the health threats of shift work. The argument that care should be delivered by the same firm of healthcare personnel throughout a patient’s entire hospital admission 7, and that this is in the best interest of the patient, has been used without much supporting evidence. Surely patients would be more than willing to be seen by a different surgeon if they knew that, when testing their surgical skills on a virtual reality laparoscopic simulator, 20% more errors were made by
surgeons who were awake all night, compared to those who had had a full night’s sleep? 8 Seventeen hours of continuous work, with no sleep, will impair cognitive psychomotor performance to an extent equivalent to a blood alcohol concentration of 0.05%, a level of intoxication which makes driving illegal in twenty-nine countries.9 Similar results showing the detrimental effects of fatigue have been found when workers reach the seventeenth hour of wakefulness between 10:30pm and 12:30am, well before hitting the circadian trough of alertness.10 Healthcare professionals, specifically surgeons in training, are expected to work longer hours than employees in the transportation and nuclear power sectors.11 Many regard it as a badge of honour 10, a display of commitment to a praiseworthy career of saving lives. It goes to show how warped surgical attitudes have become, when in fact the research clearly indicates that fatigue cannot and should not be tolerated in the work environment.
With a reduction in working hours comes the worry that surgical trainees will not be exposed to enough operative cases. This can be prevented by a strong commitment to training and by implementing an effective hospital-specific training curriculum.12 New strategies need to be embraced, for example a shift towards component-based training in the instance of intricate, multi-step procedures such as coronary artery surgery.12 A separation between care-provision and training has been advocated by some as a way to ensure that enough time is allocated for surgical trainees to gain the necessary skills 13, either via artificial tissues, animal models or computer simulation, the latter approach having been successfully employed by the aviation industry for over 40 years.14 Emphasis should be placed on instruction rather than apprentice-like case exposure 15, and early sub-specialization may be a wise approach to handling the new time constraints.14 Surgical training can be carried out on a 48-hour schedule, with a concerted effort by all parties to focus the training regime. Surgical training must fit into the latest timetable, so that as a profession with an elevated reliance on the accuracy and precision of its workers, it can be carried out safely and to the highest standard.
References:Q&A: Working time directive; BBC News [online] 2006 1. http://news.bbc.co.uk/1/hi/world/europe/4536891.stm. [Last accessed Aug 19 2009]. Pickersgill T. The European working time 2. directive for doctors in training. BMJ. 2001 Dec 1; 323(7324):1266. doi:10.1136/bmj.323.7324.1266Working Time Directive; European Commission 3. [online]. c2003 http://ec.europa.eu/social/social/main.jsp?catld=706&langId=en&intPageId-205. European [updated 2008 Dec; Last accessed Aug 19 2009]. No agreement reached on the Working Time Directive; 4. Parliament [online] 2009 http://www.europarl.europa.eu/news/expert/infopress_page/048-54485-117-04-18-908-20090427IPR54484-27-04-2009-2009-false/default_en.htm. [updated 2009; Last accessed Aug 19 2009]. Kawachi I, Colditz GA, Stampfer MJ, Willett WC, Manson 5. JE, Speizer FE Hennekens CH. Prospective study of shift work and risk of coronary heart disease in women. Circulation. 1995 Dec 1;92(11):3178-82. doiKarlsson B, Knutsson A and Lindahl B. Is there an association 6. between shift work and having a metabolic syndrome? Results from a population base study of 27 485 people. Occup Environ Med. 2001; 58: 747-752.doi:10.1136/oem.58.11.747Scott-Coombes D. Reduction in juniors’ hours 7. abolishes concept of continuity of care. BMJ.2002; 324(7339):736. doi:10.1136/bmj.324.7339.736
The European Working Time Directive will be beneficial for Surgeons
Naomi Kaplan BSc (Hons)kaplan.naomi@
googlemail.com
1st Year Clinical StudentUCL Medical School
FOR
For the full references see thelsjm.co.uk.

123lsjm 30 november 2009 volume 01
The European Working Time Directive will be
beneficial for Surgeons
The European Working Time Directive (EWTD) was enacted into United Kingdom (UK) law in 1998, with the intention of improving patient care by reducing doctors’ working hours. From 1 August 2009, all doctors will only be allowed to work a maximum of 48 hours per week.1 This has had a massive effect on the British healthcare system and left many junior doctors and surgical trainees worried about their future careers.
The implementation of the EWTD has not been well thought-out and is unrealistic. It puts patients at risk and has a detrimental effect on surgical training. The working patterns that the EWTD has introduced will not necessarily reduce tiredness and fatigue but may in fact increase it.2
Hospitals must abide by the EWTD and are thus required to design rotas, which work “on paper” but not in reality. As there is now a shortage of cover, there are gaps in rotas, which are filled by doctors who are working over their designated hours but not declaring so, as they are more concerned about their patients’ care than the regulations set by the European Union.
The SiMAP and Jaeger rulings, which state that all hours spent in hospital (whether working or resting) count as work under the EWTD, has exacerbated the effects of the regulation.1 As a result, a significant number of work rotas have moved on to full shift systems, with multiple handovers disrupting continuity of care, to the detriment of both the patient and junior doctors’ training.
The surgical specialities have been particularly affected in terms of their educational opportunities being diminished due to the EWTD. Surgery is a craft dependent on exposure and practise. The introduction of the EWTD may result in surgical trainees devoting their educational time to doing service jobs. Traditionally a consultant would have had around 30,000 hours of training, now the maximum number of hours a trainee could acquire is 18,000 on an 8-year surgical programme.3 Many trainees now feel they are at a disadvantage and will not be as well trained as their predecessors.
With the lack of daytime availability of trainees and the fragmentation induced by disparate shift systems, it is increasingly falling to consultants to undertake tasks, which, in the past, would be performed by their trainees. Ironically, whilst consultants too are subject to the EWTD, the regulations have increased their workload to the point that they themselves may be in breach of the EWTD.
In the face of difficulty in recruiting substantive and locum staff in order to fill the vacancies created by EWTD-compliant rotas, many trusts have resorted to using internal locum shifts in order to make their rotas appear compliant. This has the result of trainees working hours in excess of the EWTD through locum shifts. This is combined with a significant decline in the availability of locum staff, partially exacerbated by recent changes to immigration rules.4, 5
The ‘opt-out’ option is given to all doctors who may voluntarily choose to work up to a maximum of 56 hours. However, this does not necessarily mean that the extra hours will be used for training purposes and may very well be taken up doing service jobs.
A survey by the Association of Surgeons in Training (ASiT) of surgical trainees, covering all surgical specialities, has shown that 80% of trainees would support an individual or speciality ‘opt-out’ of the EWTD to protect their training. Additionally, the same survey showed that 90% of trainees worked over their allocated time every week and 55 % of trainees were pressurised into falsely declaring their actual hours worked 3.
The president of the Royal College of Surgeons (RCS), Mr John Black has been very vocal with his views against the EWTD and its devastating effects on patient care and surgical training. He has stated that surgical training should match trainees’ needs, not the hours that they have worked 6. ASiT have suggested an ‘ideal’ job plan which is fully supported by the RCS. The plan is based on a 65 hour working week and for a typical trainee would consist of; two outpatient clinics, four operating sessions, an endoscopy session and one on-call. This plan fits both patient priorities and teaching requirements. The RCS president suggests a change back to the traditional ‘firm’ with each trainee attached to a team of two consultants for both elective and emergency procedures 3, 6.
The changes implemented by the EWTD significantly hinders the training of surgeons. It does not help, or take into consideration surgical trainees’ professional, educational and personal requirements and makes the process of surgical training almost impossible, ultimately affecting the quality of future service delivered to patients. Surgeons’ training is taken out of their hands and being dictated to them by an external body. Unless the government listens to the views of organisations like ASiT and the RCS and changes their current policies, the quality of surgical training in the UK will take a great blow and patient care will be compromised.
References:European Working Time Directive. Department of Health [online]. 1. 2009 http://www.dh.gov.uk/en/Managingyourorganisation/Humanresourcesandtraining/Modernisingworkforceplanninghome/Europeanworkingtimedirective/DH_415 [Last Accessed 19 August 2009]Bamford N, Bamford D. The effect of a full shift system on 2. doctors. Journal of health organization and management. 2008;22(3):223-37. doi:10.1108/14777260810883512Cresswell B MC, Hawkins W, Harrison E, Fitzgerald E, 3. Roon AV. Optimising Working Hours to Provide Quality in Training and Patient Safety: A Position Statement by The Association of Surgeons in Training. January 2009 http://www.asit.org/assets/documents/ASiT_EWTD_Position_Statement.pdf [Last Accessed 16 August 2009]Immigration rules - NHS Careers [online]. 2009. http://4. www.nhscareers.nhs.uk/explore_oversea_immigration-rules.shtml [Last Accessed 23 September 2009]Immigration change will hurt NHS. BBC NEWS [online]. 5. 2009. http://news.bbc.co.uk/1/hi/health/8048744.stm [Last Accessed 23rd September 2009]
Jarnail Singh Bal BSc (Hons)
Final Year Medical Student The University of Manchester
PERSPECTIvE
AGAINST
AcknowledgementDr Arnab Ghosh (Clinical
Research Fellow, The National Hospital for Neurology and
Neurosurgery) for his help in reviewing this article
For the full references see thelsjm.co.uk.

124 lsjm 30 november 2009 volume 01
ARTICLE
Introduction There are over 250,000 severely disfigured individuals in the United Kingdom (UK) alone, many of them are housebound, unable to face the outside world1. Depression, anxiety and even suicidal intent are some of the consequences of suffering from facial disfigurement. Facial disfigurement can occur as a result of severe infections, burns, and congenital birth defects2. Facial transplantation has more recently become a reconstructive option for these individuals when there have been unsatisfactory outcomes from conventional methods.
In recent times, there has been much debate over facial transplantation, questioning whether it is technically feasible, ethically correct and the psychological impact on individuals receiving the transplant. As we now know it is technically possible, the long-term consequences of immunological therapy and considerable psychological and ethical dilemmas must be considered. Long term immunosuppressive medications are used to maintain graft viability but can shorten life by up to 10 years3. Facial transplantation is not a life-saving operation, rather life-enhancing. This contrasts with established organ transplantation such as that of the heart or kidney, whose principle aim is to prolong life. However, the idea that facial transplantation can improve quality of life makes it a viable prospect.
In 2003, Sir Peter Morris, President of the Royal College of Surgeons of England concluded: ‘We do not feel the time is appropriate to proceed with this experimental procedure. Organ transplantation is to save lives while this is to improve the quality of life’4. The Working Party report highlighted that it would only consider granting ethical approval with further research and emphasis on controlling complications such as immunosuppression. Subsequently, after much deliberation and research by a team in Britain, on 25 October 2006 ethical approval was granted to conduct the world’s first full-facial transplantation. This review aims to explore the surgical, psychological and ethical issues posed by what is still regarded as an experimental procedure.
What has been achieved so far? The world’s first full-facial replant was carried out on a young girl named Sandeep Kaur in 1994. The north-Indian born girl fell victim to a disastrous accident where a thresher caught her braids causing avulsion between the overlying facial tissue and the skull5. Using microsurgical techniques the face was replanted successfully.
The surgical, psychological and ethical barriers to performing the world’s first full facial transplant - are we ready?
Kavit Amin [email protected] 5 Medicine, St. George’s, University of Londondoi:10.4201/lsjm.surg.005
This brought plastic surgeons to further consider the prospect of transplanting facial tissue from deceased individuals. The defining moment for facial transplantation took place in November 2005 when a lady from Lyon in France was given the first partial donor transplant. Professors Dubernard and Devauchelle made history by transplanting a triangular section of nose, mouth and chin from a brain-dead individual. The recipient, 38 year old Isabelle Dinoire, suffered traumatic amputation of her ‘distal nose, upper and lower lips, chin, and adjacent parts of the cheeks’ when she was attacked by her dog6. The results since have been encouraging with some restoration of facial movement and sensation. In China, doctors have also carried out successful facial transplant operations. In April 2006, the cheek, upper lip and nose were transplanted after a man was attacked by a bear. Subsequently he died in December 2008, his death attributed to non-compliance with immunosuppressive medication, although this was never confirmed7. More recently in the United States, Maria Siemionow performed a near total facial transplant that took 22 hours. On 9 December 2008, the 45-year-old underwent what is known to be the fourth facial transplantation to date8.
The surgical challenge In plastic surgery there is a surgical reconstructive ladder. The surgeon starts simple at the bottom rung of the ladder and works up through various surgical techniques depending on the complexity of the task. At the bottom of the ladder is allowing the wound to heal itself (primary intension) or suturing the wound closed (primary closure). Then there is skin grafting. Skin grafts are thin pieces of skin with no intrinsic blood supply. The graft will only survive when blood vessels from the recipient vascular bed grow into it. Higher rungs on the ladder consist of tissue expansion and pedicled flaps, both of which are not indicated in severe facial injuries since they do not cover a sufficient area and do not produce aesthetically pleasing results. The highest, most advanced rung is called a ‘flap’. A flap is a piece of tissue disconnected from its intrinsic blood supply and re-anastomosed to another part of the body using microsurgery. Microsurgery involves operating with a powerful microscope to perform anastomoses of vessels or coaptation of nerves, which are as small as 1mm9. These flaps are known as free flaps or free tissue transfer because they can be moved freely around the body and is known as an auto-transplant10.
For the full references see thelsjm.co.uk.

125lsjm 30 november 2009 volume 01
Facial transplantation utilises a similar concept, but the flap is harvested from another individual as opposed to coming from the patient12. This is known as Composite Tissue Allo-transplantation (CTA). Allo-transplantation refers to the transplant originating from another person, whereas composite indicates it is composed of heterogeneous tissue types. Facial skin grafts and free tissue transfer are often carried out on burns patients, often with mixed results. Patients can be left with unsatisfactory cosmesis and distorted facial expression. Skin grafts can contract over time leaving a hardened, distorted appearance1. Texture and pliability of facial skin is unique, therefore facial transplantation has been proposed only for those patients where multiple skin grafts and free flaps have failed.
The surgeon faces many challenges, which include mal-alignment of the facial graft, aesthetically displeasing surgical scars, but most importantly, graft viability. Graft viability is maintained by effective vascularisation of the donor face by reconnecting the terminal branches of the external carotid artery, superficial temporal artery and internal maxillary artery that will supply the upper third of the face. The facial artery supplies the lower two thirds of the face and is the most essential anastomosis since it supplies most of the graft. Venous drainage will depend upon reconnecting the internal, external and anterior jugular vein. Failure to reconnect any of these vessels or thrombosis at anastomosis sites will result in necrosis of the donor face13. It is important to note that this type of graft failure is a separate process from that of immunological failure. Skin can withstand ischaemia for up to 13 hours, whereas muscle can become ischaemic within 6 hours14. If substantial graft necrosis were to occur, removal of the remaining facial tissue may prove problematic leaving the patient worse off. For this reason, muscle will not be included in the full-facial transplantation, unlike the French partial transplant, but will include skin and subcutaneous tissue6.
As well as immunological matching of donor and recipient, the surgeon must also consider the characteristics of the graft, an essential component for good aesthetic outcome. Sex, ethnicity and age are important to match the degree of similarity in skin texture and composition3. Interestingly there is little literature with regards to donor populations and their attitudes and concerns to donating their facial tissue. In one study, 120 people were questioned (one third doctors, one third nurses and one third lay) about their opinions on facial transplantation. A large proportion stated they would indeed accept a face if they were victim to severe disfigurement. However, none said they would donate their own15.
Rejection, graft vs host and lifelong immunosuppression The majority of the immune system response is mediated by the Major Histocompatibility Complex (MHC), which represents immunological similarity between donor and recipient. Similarity refers to having a high degree of correspondence between MHC which are alleles of a group of genes17. If a foreign graft is introduced it will be attacked unless it is histocompatible, therefore rejection is most likely if the donor and recipient differ in their histocompatibility11. The body’s ability to detect the difference between self and non-self tissues means that transplantation of allografts activates an immune response leading to rejection, a life-threatening complication.
Rejection can be hyper-acute, acute or chronic. Hyper-acute rejection occurs due to B-cell antibodies present in the recipients’ blood stream. This occurs within minutes and can lead to a systemic inflammatory response. ABO blood compatible grafts are therefore required to prevent this problem occurring with cross-matching to enable antibody screening3. Cytotoxic T cells are at the forefront of rejection called the acute phase that can take up to a week. It can even take many years to develop but its effects can be reversed if treated promptly, unlike hyper-acute rejection. The T-cells cause cell lysis and produce cytokines and can be accurately diagnosed on tissue biopsy18. Chronic rejection refers to a complex chronic response that manifests gradually over a longer period of time. It is more concerning in CTA since solid homogenous organ transplants can still survive after partial rejection whilst facial CTA would become functionally impaired. Furthermore, facial CTA will be performed in younger individuals with a higher risk of chronic rejection over time19.
As well as the direct problems with immunosuppression, the combination of organ transplantation and immunosuppression brings about a phenomenon termed graft versus host disease. The donor graft mounts a response against the host. Donor T-cells migrate from the donor organ into the recipients system potentially causing neutropenia. Prophylactic immunosuppressive regimens have decreased graft versus host severity and incidence3. The Royal College of Surgeons of England estimates that the likelihood of acute rejection in the first year may be as high as 10% and that the risk of developing chronic rejection is 30% to 50% between the second and fifth year20. Therefore, accurate donor matching and immunosuppressive medication are at the forefront of transplantation success. However, medications cause many side-effects including hypertension, diabetes and renal toxicity. Even more concerning is the susceptibility to infection by pathogens, which is responsible for a high proportion of post-transplant morbidity. Those with a weakened immune system can become very ill from minor illness necessitating the need for prophylactic antibiotics and antivirals21. Malignancies are another complication and are usually of the skin, colon and lungs. Non-Hodgkin’s lymphoma, Kaposi’s sarcoma and cervical cancer are all virally induced cancers with up to fifty-fold increases in incidence. Immunosuppressive regimens for facial transplants are relatively novel and as yet we are currently unsure about the degree of their safety17.
Graft failure is a serious and relatively known consequence of non-adherence14. Evidence for this comes from Clint Hallam and his hand transplant regimen resulting in hand amputation after 29 months. He developed diabetes initially and later triggered a rejection process due to non-compliance with medication. Several options for overcoming the issue of immunosuppression are currently being explored and initial data is promising. These include biological substitutes through to tissue engineering and adult stem cells.
Psychological and societal concerns The face transmits one’s thoughts, with facial disfigurement greatly hindering our ability to communicate. It is therefore regarded as paramount to human interactions22. Facial movements govern two thirds of our communication, and this in particular has importance for our relationships with others23. Disfigured persons have difficulties accepting their appearance and hide as an adaptive
ARTICLE

126 lsjm 30 november 2009 volume 01
response. Moreover, studies have shown that the degree of disfigurement correlates with the level of psychological distress24. Coping with a new face and the psychological implications to the individual, are extremely important factors for successful facial transplantation, arguably more so than the operation itself. Psychological assessment is vital in selecting persons with realistic expectations to achieve the best outcome for the patient. Individuals that believe they are judged purely upon appearance more prone to unrealistic expectations25. Only those able to cope with intense stressors are likely to be compliant with treatment. Those with higher depressive indices are believed to be less likely to conform to immunosuppressive regimens due to an unstable and fragile psyche26. It is imperative that selected patients have stable families, a strong support network and good understanding of the risks involved. Suitable candidates must be aware of the medical risks, possibility of unsuccessful surgery and media attention15.
There has been concern the transplanted face would resemble that of the donor’s raising significant emotional issues for the deceased’s family and friends. This idea may in part be propagated by the 1997 movie ‘Face/Off’, in which an undercover officer makes use of facial transplantation to take on the physical appearance of a major criminal and infiltrate his organisation27. However, computer generated imaging using laser scanning and photography reveals that despite similarities, the transplanted faces would not be identical. Cadavers have also been used to transfer free facial flaps to assess the degree of similarity between recipient and donor. Both models found the overlying soft tissue moulds to the recipient underlying bone structure resulting in a ‘hybrid’ face28.
Media involvement brings a previously isolated individual to the forefront of society’s attention, a radical change the patient will be ill-prepared for. Isabelle Dinoire claims she is sent many thousands of letters from people saying how ‘well’ she has done and how she should ‘stay strong’. This is a positive facet but with the media coverage assessing graft progress and possibilities of rejection, it is clearly unwarranted and will perhaps create more psychological discomfort in the future29. In view of this, Professor Peter Butler of the Royal Free Hospital, London has stated that for each of his full-facial transplant operations, patients will be kept anonymous and guided through the process using a biopsychosocial approach14. Ethical Debate and Society Previously, surgeons argued ‘should we do it, and how should we go about doing it?’ Ethicists argued ‘just because we are in a position to perform such procedures, does this mean we should?’ However, the debate has since moved on. We are no longer questioning the ethics of performing facial transplantation, but merely the ethics of how30. Supporters of facial transplantation will argue that individuals are hidden in society and resolution of their disfigured features will revive self-esteem and therefore improve their quality of life even though they may not live as long. Since patients are told the potential risks and benefits, patients should have autonomy to make their own decision to proceed31. Conversely, it is argued that when patients are offered a revolutionary new surgical procedure, they will opt for that surgery concentrating on the benefits more closely23. Clark states, ‘if potential patients are desperate for a procedure, the question arises whether it is feasible for them to assess if possible improvements in quality
of life outweigh the potential morbidity and mortality caused by long-term immunosuppression’15. Others argue that consent with regards to facial transplants is counterintuitive. A person with a facial deformity will have hope at the prospect at receiving a new life. The ‘nothing to lose’ approach can be dangerous for these individuals and regulations may need to be enforced to protect these individuals.
The surgeon has a role in informing the patient the risks for the entire process and not giving a biased overview of what may be involved24. A short report by a British plastic surgeon claims that teams from the United States of America, UK and China may be racing for ‘media attention’ rather than the welfare of the patient involved32. Critics argue that all other avenues on the reconstructive ladder should have been explored first for Isabelle Dinoire before attempting the partial facial transplantation33. Conclusion Partial facial transplantation has been carried out to date with some success. We have progressed from successful allograft of a nerve in 1988 to near full-face transplants in 20088. We now know it is technically possible to perform facial transplantation with current microsurgical techniques. Individuals so far have been shown to exhibit a tolerance to the level of toxicity from immunosuppressive medications34. Therefore, we cannot ignore facial transplantation as a reconstructive option. Despite the prospect of such an achievement, there are considerable reasons for concern. Long-term risks may not be apparent to patients, which include rejection, immunosuppression and inadequate post-surgical care. The British Association of Plastic, Reconstructive and Aesthetic Surgeons claims it hoped full-face transplants, long seen as the ‘Holy Grail’ of surgery, would become routine given the right safeguards. There are divided opinions on the psychological well being of these patients post-transplant. Thus the selection process for suitable candidates will be especially important. It is encouraging to see the level of discussion from scientists, ethicists and psychologists, ensuring every aspect of the procedure is considered. We must not lose sight of the fact that our ultimate ambition lies in producing the best outcome for our patients. This will by no means be an overnight process, but will require a dedicated team of individuals attempting to restore an individual’s quality of life.
ReferencesHartman RG. Face value: challenges of transplant 1. technology. Am J Law Med. 2005;31(1):7-46.Van Loey NE, Van Son MJ. Psychopathology and psychological 2. problems in patients with burn scars: epidemiology and management. Am J Clin Dermatol. 2003;4(4):245-72. doi:10.2165/00128071-200304040-00004Hettiaratchy S, Randolph MA, Petit F, Lee WP, Butler PE. Composite 3. tissue allotransplantation--a new era in plastic surgery? Br J Plast Surg. 2004 Jul;57(5):381-91. doi:10.1016/j.bjps.2004.02.012Morris PJ, Bradley JA, Doyal L, Earley M, Hagan P, Milling M, 4. et al. Facial transplantation: a working party report from the Royal College of Surgeons of England. Transplantation. 2004 Feb 15;77(3):330-8. doi:10.1097/01.TP.0000113810.54865.BEInterview: Diana Whybrew. The Guardian [online]. 4 November 5. 2006. http://www.guardian.co.uk/science/2006/nov/04/medicineandhealth.comment [Last accessed 18 October 2009]Devauchelle B, Badet L, Lengele B, Morelon E, Testelin S, Michallet 6. M, et al. First human face allograft: early report. Lancet. 2006 Jul 15;368(9531):203-9. doi:10.1016/S0140-6736(06)68935-6Chenggang Y YH, Xudong Z, Binglun L, Hui Z, Xianjie 7. M, Li Y, et al. Some issues in facial transplantation. Am J Transplant. 2008 Oct 2008;8(10):2169-72.
ARTICLE
127lsjm 30 november 2009 volume 01
BOOK REvIEW
Surgery, An Oxford Core TextEditors: Peter Stonebridge, David Smith, Lesley Duncan and Alastair ThompsonPublisher: Oxford University PressISBN: 0192629905
When facing the prospect of starting clinical medicine, it is not immediately obvious which are the good surgical texts for medical students. Once you start delving into the subject area you become overwhelmed with the choices on offer. Surgery, An Oxford Core Text is a textbook written for the clinical medical student’s first surgical encounter. The lead editor, Peter Stonebridge, a consultant vascular surgeon has compiled a book which is easy to read and explains surgical concepts in a simple and understandable way that does not assume any prior clinical knowledge.
The book is divided into two main sections. The first covers the main general surgical specialties, namely gastro-intestinal, hepato-biliary, vascular, breast and also includes a section on neck lumps and thyroid surgery. The second section contains chapters on peri-operative care and anaesthesia and care of the post-operative patient.
Each chapter begins with a number of patient-based clinical scenarios, which are broken down into a stepwise fashion to promote understanding of the clinical presentation and initial management of these common surgical problems. This is then followed by a more detailed explanation of these conditions, including when necessary, a description of the background scientific theory underpinning the clinical knowledge. The text is supplemented with numerous, well annotated clinical photographs
and stereotypical imaging results for the major surgical conditions. Further, the text is broken up by summary boxes and ‘fast facts’ boxes which help to re-emphasise the key points of the section that has just been read.
Although this book is an excellent introduction to surgery for medical students, it should by no means be seen as a comprehensive manual of everything you need to know about surgery. Firstly, this book lacks chapters on orthopaedics and ear, nose and throat surgery and the section on breast surgery is brief. I also feel that there could be more written about the common operations and basic surgical procedures that we as medical students need to know about. Additionally, this book does not really cover any of the specialist surgical examinations in anywhere near enough detail to be able to perform them, unlike texts such as Browse’s Introduction to Signs and Symptoms of Surgical Disease or even Surgical Talk.
Where Surgery, An Oxford Core Text does excel is with its peri-operative and post-operative chapters and these alone are enough for one to recommend this book as an essential read. The peri-operative section covers areas such as the anaesthetic assessment, post-operative pain management, control of nausea and vomiting, fluid management, nutrition and blood transfusion. The post-operative section covers both common and serious post-operative complications using the universal DRABCDE method. These sections are again centered around clinical cases yet what sets them apart from similar chapters in other books is the fact that the authors explain the scientific theory underlying the rationale for every clinical decision made at each stage of the assessment of a patient. This approach leaves you with a clear understanding of the pre- and post-operative care of a surgical patient and a little less daunted by the prospect of having to deal, for instance, with a patient who has just collapsed on the wards post-operatively. In this respect, not only is this book useful for critical care OSCE stations, but would also be of great help to foundation year doctors on surgical wards.
While this book never becomes overcomplicated in its descriptions, the style it is written in means that it is more suited to being read chapter by chapter than to being dipped in and out of - a point that is underpinned by the editors in the preface. I would not recommend this book as a primary revision tool for surgery as there are other surgical texts that are written specifically with revision for exams in mind. However, I do feel that this would have been the book that I would have liked to read during the weeks in September last year when I first set foot on the surgical wards.
Peter Arthur-Farraj PhD [email protected] 4 Medicine, UCL Medical School

128 lsjm 30 november 2009 volume 01
Surgical safety is an under-recognised public health problem. Estimates show that approximately 234 million operations are performed worldwide each year and that as many as seven million people each year suffer a disabling surgical complication and one million die as a direct result of their surgery.1 In 2006, the World Health Organization (WHO) launched an effort to improve global surgical safety, to reduce surgical mortality and complication rates.2
To achieve this goal, WHO leaders created an evidence-based Surgical Safety Checklist (Figure 1). Components of the Checklist
are designed to address safety issues at three distinct time points for a surgical patient: first, when the patient ‘signs-in’ to the operating theatre, prior to induction of anaesthesia; next, a ‘time-out’ period immediately prior to incision; and finally, a post-operative ‘sign-out’ stage, before the patient leaves the operating room. Each component builds on effective teamwork, keeping all surgical team members aware of the needs of the patient and prepared for any expected complications.3,4 The Checklist has been compared to the detailed flight checks carried out by an airline pilot.
Figure 1: The World Health Organization Surgical Safety Checklist
Surgical Safety Checklist
Has the patient confirmed his/her identity, site, procedure, and consent?
Yes
Is the site marked? Yes Not applicable
Is the anaesthesia machine and medication check complete?
Yes
Is the pulse oximeter on the patient and functioning?
Yes
Does the patient have a:
Known allergy? No Yes
Difficult airway or aspiration risk? No Yes, and equipment/assistance available
Risk of >500ml blood loss (7ml/kg in children)? No Yes, and two IVs/central access and fluids
planned
Confirm all team members have introduced themselves by name and role.
Confirm the patient’s name, procedure, and where the incision will be made.
Has antibiotic prophylaxis been given within the last 60 minutes?
Yes Not applicable
Anticipated Critical Events
To Surgeon: What are the critical or non-routine steps? How long will the case take? What is the anticipated blood loss?
To Anaesthetist: Are there any patient-specific concerns?
To Nursing Team: Has sterility (including indicator results)
been confirmed? Are there equipment issues or any concerns?
Is essential imaging displayed? Yes Not applicable
Nurse Verbally Confirms: The name of the procedure Completion of instrument, sponge and needle
counts Specimen labelling (read specimen labels aloud,
including patient name) Whether there are any equipment problems to be
addressed
To Surgeon, Anaesthetist and Nurse: What are the key concerns for recovery and
management of this patient?
This checklist is not intended to be comprehensive. Additions and modifications to fit local practice are encouraged. Revised 1 / 2009
(with at least nurse and anaesthetist) (with nurse, anaesthetist and surgeon) (with nurse, anaesthetist and surgeon)
© WHO, 2009
Before induction of anaesthesia Before skin incision Before patient leaves operating room
ARTICLE
Sour
ce: W
orld
Hea
lth
Org
aniz
atio
n
Andrew Carson-StevensMB BCh/MPhil student, Cardiff University
Shabnam HafizMD/MPH student, Harvard School of Public Health, Harvard University
Jordan BohnenMD/MPH student, University of California
John Rose Jr.MD/MPH student, University of California, Irvine, CA, USA
Lily GutnikMD student, Ben Gurion University, Beer Sheva, Israel
Daniel HendersonMD student, University of Connecticut School of Medicine
Thomas TsaiMD/MPH student, University of California
Rachel FespermanMD/MPH student, University of North Carolina
Transforming the Culture of Surgical Safety

129lsjm 30 november 2009 volume 01
Between October 2007 and September 2008, the WHO’s Safe Surgery Saves Lives program conducted a pilot-study of the Checklist in eight hospitals in eight cities representing a variety of economic circumstances and diverse patient populations.5 The rate of death was 1.5% before the Checklist was introduced and declined to 0.8% afterward (P = 0.003). Inpatient complications occurred in 11.0% of patients at baseline and in 7.0% after introduction of the Checklist (P<0.001).
A group of likeminded students are collaborating to facilitate the spread of the surgical checklist as part of the patient safety movement. These students represent multiple health professions (e.g. medicine, nursing, healthcare management and public health) from several countries. Together, we clarified a common vision and outlined a strategy for promoting student-led efforts related to the WHO’s Checklist. The vision – “students across the world helping to disseminate the WHO Surgical Safety Checklist and partnering to improve healthcare quality” – reflects our belief that health professions students can play a meaningful role in improving healthcare quality in any setting. In pursuit of this vision, the group’s strategy highlights a number of potential opportunities for student involvement. Specifically, to build awareness about the Checklist, serve as catalysts for its implementation, and collect data regarding its usage to encourage uptake. This collaboration amongst students is known as the Safe Surgery Student Mentor project.
The Safe Surgery Student Mentor project exists to provide support to Student Mentors of the Checklist. Initially, to foster growth and collaboration on campuses, we developed partnerships with surgical and public health faculty, hosted chat sessions, and united with student-oriented quality improvement groups including the Institute for Healthcare Improvement’s (IHI) Open School for Health Professions and the American Medical Student Association’s (AMSA) Surgery Specialty Forum.6-8 Off campus, students are engaging in trials disseminating the Checklist in the U.S, Pakistan, Israel, Uganda, and Wales. Lessons from these efforts, and from additional case studies currently underway, will be used to inform via a guide to improve efficacy in the future. Until that time, the team challenges students worldwide to join the dissemination process by: (1) reading the original research in an article dedicated to the Checklist, (2) visiting the WHO Safe Surgery project website, (3) investigating whether or not the Checklist is currently used at your home institution or facility, and where applicable, (4) considering taking the Checklist on any clinical electives (see Figure 2).
Currently, the Surgical Safety Checklist is endorsed by over 300 organizations worldwide and is actively being implemented in at least 768 sites around the world.9 The Safe Surgery Student Mentor project is currently partnering with over 140 student groups of the
IHI Open School and over 150 chapters of the AMSA and launched the global “Check a box. Save a life” campaign in October 2009 encouraging healthcare student groups to sign up and become partners of the 1st Global Sprint to Improve Healthcare. The WHO Safe Surgery Saves Lives initiative, already in its third year, will benefit greatly from this mobile force of students playing the role of ambassadors for the Surgical Checklist.
Beyond the immediate effects of implementation, which have already been documented to save lives and precious healthcare resources, Student Mentors will set a precedent of patient safety for the next generation of healthcare professionals. The Student Mentor project has also served as a vehicle for students to be engaged in health service delivery and quality improvement research, bridging their clinical experiences with their passion for health reform. This is a call to arms to faculty and senior colleagues to support the enthusiasm of junior colleagues, to assist in developing their ideas for improvement, and aid them in executing this important work. There is an army of enthusiastic students eagerly awaiting new opportunities to improve healthcare quality and patient safety, both domestically and abroad. In this age of grassroots movements and social networks, the Student Mentor project has shown that medical and health professions students are an underutilised resource for translating research into change, policy into practice.
The Safe Surgery Student Mentor project can be reached online via the WHO Safe Surgery campaign’s website, http://www.safesurg.org/student-mentors.html. Students are encouraged to use this forum to share their own experiences with the Checklist in preparation for a more formal launch through IHI and AMSA this autumn.
ReferencesWeiser T, Regenbogen S, Thompson K, Haynes A, Lipsitz 1. S, Berry W, et al. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet. 2008;372(9633):139-44. doi:10.1016/S0140-6736(08)60878-8World Alliance for Patient Safety. Global Patient Safety 2. Challenge 2007-2008: Safe Surgery Saves Lives. Geneva: World Health Organization, 2007. http://www.who.int/patientsafety/safesurgery/en/index.html. [Last accessed 19 June 2009]Allard J, Bleakley A, Hobbs A, Vinnell T. ‘”Who’s on the team today?” 3. The status of briefing amongst operating theatre practitioners in one UK hospital. Journal of Interprofessional Care. 2007;21:2:189–206.Lingard L, Espin S, Whyte S, Regehr G, Baker G R, Reznick 4. R, et al. Communication failures in the operating room: an observational classification of recurrent types and effects. Journal of Quality and. Safety in Health Care. 2004;13:330-334. doi:10.1136/qshc.2003.008425Haynes AB, Weiser TG, Berry WR, Lipsitz SR, Breizat AH, 5. Dellinger EP, et al. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med. 2009;360(5):491–499. doi:10.1056/NEJMsa0810119 IHI Open School for Health Professions. Institute for Healthcare 6. Improvement. Cambridge: IHI, 2008. http://www.ihi.org/IHI/Programs/IHIOpenSchool/. [Last accessed 19 June 2009]. Surgery Specialty Forum. American Medical Student 7. Association. Reston: AMSA, 2009. http://www.amsa.org/surg/. [Last accessed 19 June 2009].Carson-Stevens, A. The IHI Open School: Primum 8. non nocere. The London Student Journal of Medicine {Surgery}. 2009;1(1):46-47. doi:10.4201.lsjm/surg.002Safesurg Project. Safesurg.org: a website for information on how 9. to reduce deaths in surgical care globally. Boston: Safesurg.org, 2009. http://www.safesurg.org./. [Last accessed 19 June 2009].
ARTICLE
Sour
ce: W
orld
Hea
lth
Org
aniz
atio
n
Sour
ce: A
ndre
w C
arso
n-St
even
s
Safe Surgery Student Mentor Challenge(1) Read the article dedicated to Safe Surgery Checklist.(2) Visit the WHO Safe Surgery website and become familiar with available materials (http://www.safesurg.org/student-mentors.html)(3) Investigate your home institution or healthcare facility’s Quality Improvement protocols and see how you can get involved.
(4) Spread awareness by talking to your colleagues about the Checklist.
Figure 2: The Safe Surgery Student Mentor Challenge
AcknowledgementsThe authors would like to
acknowledge the WHO Safe Surgery dissemination team
and the IHI Open School for their ongoing support of the
Safe Surgery Student Mentor project.

















