Page 1/15 Micro- and Macrocirculatory Effects of Landiolol: A Double-Blind, Randomized Study Following Cardiac Surgery Arnaud Ferraris ( [email protected]) Universite Claude Bernard Lyon 1 https://orcid.org/0000-0003-1388-6552 Matthias Jacquet-Lagrèze Hospices Civils de Lyon Laure Cazenave Hospices Civils de Lyon William Fornier Hospices Civils de Lyon Wajma Jalalzai Hospices Civils de Lyon Nicolas Rousseau-Saine Hospices Civils de Lyon Bernard Allaouchiche VetAgro Sup Stephane Junot VetAgro Sup Matteo Pozzi Hospices Civils de Lyon Jean-Luc Fellahi Hospices Civils de Lyon Research Keywords: Cardiac surgery, landiolol, microcirculation, postoperative atrial brillation. Posted Date: April 26th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-444804/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License
Transcript
Page 1/15
Micro- and Macrocirculatory Effects of Landiolol: ADouble-Blind, Randomized Study Following CardiacSurgeryArnaud Ferraris ( [email protected] )
Universite Claude Bernard Lyon 1 https://orcid.org/0000-0003-1388-6552Matthias Jacquet-Lagrèze
AbstractBackground: Postoperative atrial �brillation (POAF) increases morbidity and mortality after cardiacsurgery. Landiolol, a selective ultra-short-acting betablocker has been recently suggested to prevent POAFin the cardiac surgical setting with a good safety pro�le. Micro- and detailed macrocirculatory effects oflandiolol remain however largely unknown in that setting.
Methods: We conducted a prospective, randomized, double-blind study versus placebo in patientsundergoing conventional cardiac surgery. Incremental doses of intravenous landiolol from 0.5 to 10 μg-
1.kg-1.min-1 or placebo were administrated postoperatively. Microcirculatory variables were assessed byboth peripheral near-infrared spectroscopy (NIRS) in combination with a vascular occlusion test andsublingual videomicroscopy. Macrocirculatory variables were obtained from transpulmonarythermodilution and transthoracic echocardiography.
Results: Fifty-nine adult patients were allocated to the landiolol group (n=30) or the placebo group (n=29)from January to November 2019. Heart rate signi�cantly decreased in the landiolol group (P<0.01)whereas mean arterial pressure (P=0.05) and stroke volume (P=0.63) were not signi�cantly modi�edthroughout the study. No modi�cation was found in left and right systolic and diastolic ventricularfunctions except a signi�cant increase in E/A ratio in the landiolol group (P=0.02). No difference wasevidenced between groups in microcirculatory parameters at any landiolol dose. POAF occurred in 9(32%) vs. 5 (17%) patients in placebo and landiolol groups, respectively (P=0.28).
Conclusions: Postoperative incremental doses of landiolol up to 10 μg-1.kg-1.min-1 are e�cacious tocontrol heart rate without signi�cant alterations in both micro- and macrocirculation followingconventional cardiac surgery.
BackgroundPostoperative atrial �brillation (POAF) is a major issue following cardiac surgery with cardiopulmonarybypass (CPB), leading to an increase in both morbidity and mortality [1]. Although not yet recommendedin current guidelines, the use of landiolol, an intravenous ultra-short-acting betablocker recentlyintroduced in Europe, could markedly reduce the incidence of POAF following cardiac surgery [2]. Itshighly selective beta-1 blocker pharmacological properties associating a more selective chronotropic andless negative inotropic and hypotensive effects could be ideal during the perioperative period [3]. Despitea well-documented safety/e�cacy pro�le in Japanese studies [4, 5], the bene�t/risk ratio of landiolol inCaucasian surgical patients has to be further evaluated. Moreover, a better knowledge of both micro- anddetailed macrocirculatory effects of landiolol is required before considering its wider use in routinepractice.
Microcirculatory disorders have been reported following cardiac surgery and in septic shock patients [6–8]. Despite potential negative effects on macrocirculatory variables, bene�cial effects of betablockers onmicrocirculation have been previously suggested both in clinical and experimental studies [9]. The
Page 3/15
assessment of microcirculation is not yet a routine practice in intensive care unit (ICU) [10]. The use ofperipheral near-infrared spectroscopy (NIRS) in combination with a vascular occlusion test (VOT) hasbeen validated to assess regional oxygen saturation (rSO2) and the microcirculatory response to anischemic stress [11]. Besides, sublingual videomicroscopy is considered as the clinical reference methodto analyze microcirculation abnormalities in various hemodynamic scenarios [12].
In this prospective, randomized, double-blind study, we assessed both micro- and detailedmacrocirculatory effects of intravenous landiolol ranging from 0.5 to 10 µg− 1.kg− 1.min− 1 in patientsundergoing conventional cardiac surgery. We hypothesized that landiolol titration would limit or reverseCPB induced-microcirculatory abnormalities compared to placebo without macrocirculatory alterations.
MethodsWe conducted a monocentre, prospective, randomized, placebo-controlled and double-blind study.Patients were enrolled at the University Hospital Louis Pradel (Lyon, France) from January to November2019 after Ethics Committee approval (Comité de protection des personnes Ouest VI, July 17th 2018;Agence Nationale de Sécurité du Médicament, July 10th 2018). The trial was registered withClinicalTrials.gov (NCT03779178) on 12 April 2019. Each patient received appropriate information andwritten informed consent was systematically collected. CONSORT statement was respected in this study.We included adult patients scheduled for conventional cardiac surgery with CPB (coronary artery bypassgrafting, aortic or mitral valve replacement or repair, and combined cardiac surgery). Patients withpreoperative atrial �brillation, contraindications to betablockers, cardiac index < 2.2 L/min,hyperlactatemia > 4 mmol/L, requiring inotropic drugs or norepinephrine > 0.3 µg− 1.kg− 1.min− 1 or majorpostoperative bleeding (> 200 mL/h) were not included into the study.
Patients’ management and data acquisitionPatients were included within 2 hours following postoperative admission to the ICU. They were monitoredwith �ve-lead electrocardiogram, oxygen pulse oximetry, femoral invasive arterial blood pressure andtranspulmonary thermodilution (PiCCO® device, Pulsion Medical systems, Germany). Propofol,vasoactive agents and oxygen intake with mechanical ventilation were kept constant throughout thestudy period.
After rubbing and cleaning the skin with an alcohol swab, a NIRS optode (INVOS oximetry adult sensor®,Medtronic, Minneapolis, MN) was carefully applied to the medial surface of the left or right forearm, 5 cmbelow the elbow. The sensor was attached to the skin of participants with opaque adhesive stickers sothat the angle and position of the optode was kept constant. The sensor was connected to the INVOSoximeter 5100C® device (Medtronic, Minneapolis, MN). All rSO2 values were recorded every 5 seconds.Data were recorded online, transferred to a speci�c software (INVOS analytics 1.2®, Medtronic,Minneapolis, MN) and stored for further analysis. A pneumatic cuff in�ator was positioned at the upperextremity of the ipsilateral upper limb. A rapid arterial occlusion of the upper limb was provoked by
Page 4/15
in�ation of the pneumatic cuff at 50 mmHg above the systolic arterial pressure, until either rSO2 valuesdecreased to 40% or for a maximal period of 10 min, as previously described [7]. The arterial cuff wasthen rapidly de�ated to initiate reperfusion. Recorded NIRS parameters were baseline rSO2, thedesaturation speed during ischemia (baseline rSO2 minus rSO2 min/time of ischemia), the resaturationspeed during reperfusion (rSO2 max minus rSO2 min/time of reperfusion), and the variation in rSO2
during reperfusion (ΔrSO2 = rSO2 max – rSO2 baseline). A regular VOT is depicted in Additional �le 1.
Sublingual videomicroscopy was achieved with a dedicated device MicroScan® and AVA-3 software(Microvision medical, Amsterdam, The Netherlands). The technology uses sidestream dark�eld imagingwhere illumination is achieved by surrounding the tip of the light guide with light-emitting diodes. Werecorded 5 acquisitions of 5 different sites minimum at baseline and at the �nal time point (10 videos perpatient) of 4 seconds minimum. Videomicroscopy records were performed according to currentrecommendations [12] to reach consensus statements in images acquisitions, quality and analysis. Videoanalyses were extracted in a speci�c and validated software [13], namely Capillary Mapper® 1.4.1 onlineversion (https://capillary-mapper.uni-muenster.de), to collect the following data: microvascular �ow index(MFI) quadrant, proportion of perfused vessels (PPV), total vessel density (TVD) and heterogeneity index(HI).
Macrocirculatory variables were derived from the PiCCO® device and assessed on-line after an initialcalibration. A second calibration was performed before the last protocol time point. Heart rate (HR), meanarterial pressure (MAP), stroke volume index (SVi), cardiac index (CI) and pulse pressure variation (PPV)were systematically recorded. The transthoracic echocardiographic analysis (Vivid S6®, General ElectricHealthcare, Boston, MA) was carried out twice : at baseline (T0) and at the �nal time point (T10) by twotrained investigators (MJL and AF). Left ventricular parameters (end-diastolic and end-systolicdimensions and volumes with Simpson’s biplane method, ejection fraction, aortic velocity time integral(VTI), mitral Doppler, and lateral tissular Doppler), right ventricular parameters (tricuspid Doppler, tissularDoppler, tricuspid annular plane systolic excursion (TAPSE), and fractional area changes (FAC)) wererecorded. Echocardiographic SVi (VTI x aortic cross-sectional surface) indexed to body surface wasdetermined as an additional measurement.
Arterial and venous blood gas analyses were sampled twice at baseline and at the �nal study time pointto collect central venous saturation (SvO2) and lactate.
Finally, POAF incidence was estimated from postoperative day 0 in ICU with continuous �ve-leadelectrocardiogram to postoperative day 5 in the surgical ward with daily twelve-lead electrocardiogram.
Study protocolPatients were randomized into a landiolol group and a placebo group according to a 1:1 repartition.Randomization was performed by using MedCalc Statistical Software version 18.11.6 (MedCalc Softwarebvba, Ostend, Belgium; https://www.medcalc.org; 2019). Both landiolol and placebo syringes wereprepared by a Pharmacist as follows: landiolol 50 mg in 50 mL of NaCl 0.9%, and placebo 50 mL of NaCl
Page 5/15
0.9%. The treatment distribution and perfusion was blinded both to the patient and the investigator. Acomplete set of measurements was carried out in all patients at six experimental time points: baseline(T0), landiolol 0.5 (T0.5), 1 (T1), 2 (T2), 5 (T5) and 10 (T10) µg− 1.kg− 1.min− 1 converted into 0.03, 0.06,0.12, 0.3 and 0.6 mL− 1.kg− 1.h− 1 respectively, according to landiolol dilution (1mg/mL). A stabilizationperiod of 20 min (5 half-lives) was respected at each step. The treatment was stopped if MAP wasinferior to 65 mmHg and/or HR decreased below 60/min, otherwise it was maintained at maximal doseup to oral betablocker resumption for a maximal period of 12 hours. The whole study protocol is depictedin Additional �le 2.
EndpointsThe primary endpoint of the study was the assessment of the resaturation speed measured by NIRScombined to a VOT during incremental doses of landiolol. Secondary endpoints were: 1) The effects ofincremental doses of landiolol on other microcirculatory variables given by NIRS and sublingualvideomicroscopy; 2) The effects of incremental doses of landiolol on macrocirculatory variables given bytranspulmonary thermodilution and transthoracic echocardiography; 3) The effects of incremental dosesof landiolol on metabolic parameters.
Statistical analysisThe sample size was based on a previous study by our group using postoperative esmolol in the cardiacsurgical setting and showing that resaturation speed grew up from 0.53%/min before esmolol to0.82%/min at the highest esmolol dose [6]. Considering that microcirculatory abnormalities would becomparable, we determined that the enrollment of 58 patients assigned in a 1:1 ratio would give 90%power to detect a difference between both groups with an alpha risk of 0.05. Continuous variables wereanalyzed with a linear mixed effect model using landiolol doses as a variable with a �xed effectaccording time points (T0.5 to T10), and patient as a variable with a random effect for intercepts andslopes. Visual inspection of residual plots was performed to assess the absence of deviations fromhomoscedasticity or normality [14]. Data are expressed as mean ± SD, or median [interquartile range], ornumber (%), according to their nature and distribution (Shapiro-Wilkinson test). We compared data byusing a Wilcoxon test and/or a paired Student’s t-test, as appropriate. All tests were two-tailed, and a Pvalue less than 0.05 was considered statistically signi�cant. Statistical analyses were performed using Rsoftware version 3.4.3 (R-project, GNU GPL).
ResultsFifty-nine adult patients were randomized into a landiolol group (n = 30) and a placebo group (n = 29)from January to November 2019. One patient was excluded from the analysis because ofvideomicroscopy technical problems. The �ow chart of the study is depicted in Fig. 1. The maindemographic and clinical characteristics of the whole cohort of patients are reported in Table 1. Nosigni�cant difference was found between groups. Two patients did not receive the full dose regimen
Page 6/15
because of MAP < 65mmHg in one case and HR < 60/min in the other case. Nine (32%) patients inplacebo group vs. 5 (17%) in landiolol group experienced POAF between day 0 and day 5 (P = 0.285).
Page 7/15
Table 1Patients’ demographic and clinical characteristics (n = 59)
Placebo Landiolol
n = 29 n = 30 P value
Age, years 64 ± 10 63 ± 11 0.51
Male, n 21 (72) 23 (77) 1.0
Weight, kg 79 ± 19 77 ± 12 0.64
BMI, kg/m² 27.4 ± 5.4 26.1 ± 3.2 0.24
Chronic heart failure, n 1 (3) 1 (3) 1.0
Diabetes mellitus, n 3 (10) 5 (17) 0.74
Hypertension, n 20 (69) 16 (53.3) 0.34
Chronic renal failure, n 4 (14) 5 (17) 1.0
COPD, n 0 (0) 3 (10) 0.25
Peripheral arterial disease, n 3 (10) 2 (7) 0.97
Chronic medications
Beta-blockers 4 (14%) 4 (13%) 0.96
ACE inhibitors/ARB 14 (48%) 13 (43%) 0.52
Diuretics 4 (14%) 7 (23%) 0.37
Statins 13 (45%) 14 (47%) 0.89
Platelet inhibitors 15 (52%) 12 (40%) 0.37
Type of surgery
Valvular replacement or repair 21 (73%) 15 (50%) 0.08
Data are mean ± SD or median [25th -75th ] or number (%).
BMI: body mass index; COPD: chronic obstructive pulmonary disease; LVEF: left ventricular ejectionfraction; ACE: Angiotensin converting enzyme; ARB: Angiotensin II receptor antagonist.
Page 8/15
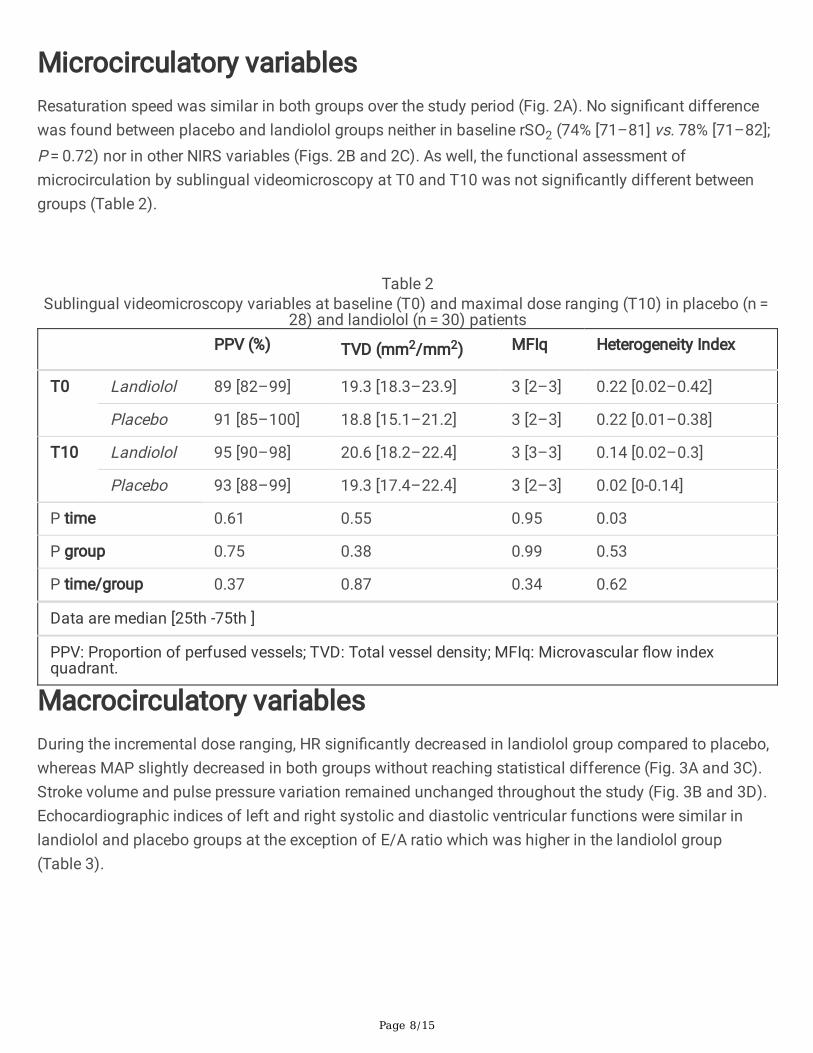
Microcirculatory variablesResaturation speed was similar in both groups over the study period (Fig. 2A). No signi�cant differencewas found between placebo and landiolol groups neither in baseline rSO2 (74% [71–81] vs. 78% [71–82];P = 0.72) nor in other NIRS variables (Figs. 2B and 2C). As well, the functional assessment ofmicrocirculation by sublingual videomicroscopy at T0 and T10 was not signi�cantly different betweengroups (Table 2).
Table 2Sublingual videomicroscopy variables at baseline (T0) and maximal dose ranging (T10) in placebo (n =
PPV: Proportion of perfused vessels; TVD: Total vessel density; MFIq: Microvascular �ow indexquadrant.
Macrocirculatory variablesDuring the incremental dose ranging, HR signi�cantly decreased in landiolol group compared to placebo,whereas MAP slightly decreased in both groups without reaching statistical difference (Fig. 3A and 3C).Stroke volume and pulse pressure variation remained unchanged throughout the study (Fig. 3B and 3D).Echocardiographic indices of left and right systolic and diastolic ventricular functions were similar inlandiolol and placebo groups at the exception of E/A ratio which was higher in the landiolol group(Table 3).
Page 9/15
Table 3Echocardiographic variables at baseline (T0) and maximal dose ranging (T10) in placebo (n = 28) and
landiolol (n = 30) patients
T 0 T 10 Ptime
Pgroup
Ptime/group
Landiolol Placebo Landiolol Placebo
Left ventricular function
LVEF (%) 50 [43–56]
49 [40–63]
50 [42–59] 48 [44–58] 0.72 0.84 0.63
VTI (cm) 19 [15–22]
18 [15–23]
17 [14–22] 18 [16–24] 0.57 0.73 0.44
SVi 44 [36–61]
47 [30–57]
54 [39–58] 53 [42–58] 0.43 0.98 0.05
E/A 1 [0.8–1.2]
0.9 [0.8–1.1]
1.2 [0.9–1.4]
0.9 [0.7–1.1]
0.59 0.82 0.02
E/e’ 9.3 [7.4–14.5]
13.4[9.7–18]
10.5 [7.8–14.9]
13.6 [10.1–15.1]
0.85 0.02 0.62
Right ventricular function
TAPSE (mm) 13 [12–16]
13 [12–19]
12 [9–14] 14 [11–15] 0.17 0.31 0.37
FAC (%) 40 [34–44]
35 [25–41]
33 [30–36] 39 [29–40] 0.62 0.97 0.25
S tricuspid(cm/s)
8 [7–9] 9 [7–11] 7 [6–8] 9 [7–11] 0.43 0.36 0.34
E/A tricuspid 1 [0.8–1.2]
1.1 [0.8–1.2]
0.8 [0.7-1.0]
0.9 [0.8–1.2]
0.19 0.21 0.58
E/e’ tricuspid 5.3 [4.7–6.5]
6.4 [5.3–7.5]
4.9 [4.3–6.1]
6.2 [4.7–7.1]
0.16 0.09 0.35
Data are median [25th -75th ]
LVEF: Left ventricular ejection fraction; VTI: Velocity-time integral; SVi: stroke volume measured as VTIx aortic surface x corporeal surface; E/A: Mitral E and A waves velocities ratio; E/e’: Mitral E wavevelocity and annular e’ wave velocity ratio; TAPSE: Tricuspid annular plane systolic excursion; FAC:right ventricular fractional area change; S tricuspid: tricuspid systolic annular velocity; E/A tricuspid:Tricuspid E and A waves velocities ratio; E/e’ tricuspid: Tricuspid E wave velocity and annular e’ wavevelocity ratio.
Metabolic variablesNo signi�cant difference was found on SvO2 between landiolol and placebo 65% [60–71] vs. 64% [60–69] respectively (P = 0.19), but a time-effect was observed 74% [68–79] vs. 65% [60–71] (P < 0.01).
Page 10/15
Lactate was similar in landiolol and placebo groups: 1.7 [1.4–2.2] vs. 1.9 [1.4–2.3] at T0, and 2.0 [1.7–2.4] vs. 1.4 [1.2–2.2] at T10 (P value time/group = 0.25), respectively.
DiscussionThe main results of the present randomized study are that a dose regimen of intravenous landiolol from0.5 to 10 µg− 1.kg− 1.min− 1 following conventional cardiac surgery: 1) is not associated withhemodynamic microcirculatory effects, either bene�cial or detrimental; 2) is responsible for a decrease inHR without changes in arterial pressure, stroke volume, and right and left systolic and diastolic ventricularperformances; 3) is not associated with metabolic disturbances. Taken together, those results suggestthat postoperative use of low-dose landiolol is e�cacious to control heart rate with a good detailedhemodynamic safety pro�le.
While expected postoperative microcirculatory abnormalities were observed in both groups, no differencewas found between landiolol and placebo groups. NIRS parameters were similar, including resaturationspeed, a parameter assessing microvascular reactivity. In addition, no difference was detected insublingual videomicroscopy analysis. Even if it is not yet a routine technology, an expert consensus fordaily practical use and interpretation has been recently published [12]. We are in accordance with thatconsensus statement about images acquisitions and analyses. Video analysis was performed on-line in afree-of-charge software, namely Capillary Mapper (https://capillary-mapper.uni-muenster.de). Thiswebsite was successfully validated for manual analysis of microcirculation videos against the goldstandard analyzer software AVA 3 [13]. Thus, our results suggest that landiolol has neither bene�cial nordetrimental effect on microcirculation according current monitoring of the study. Microcirculatorydisorders have been mainly reported in sepsis, including heterogeneity in perfusion and obstructedcapillaries [15]. Similar alterations could occur following cardiac surgery with cardiopulmonary bypass asmicrocirculation is known for being highly responsive to in�ammatory mediators [16]. Suchmicrocirculatory abnormalities can be independent from systemic hemodynamic alterations [15] andassociated with adverse outcomes [17]. Previous studies reported potential bene�cial effects of esmololon microcirculation in both experimental and clinical settings [6, 9], the reason why we hypothesizedlandiolol could be bene�cial as well. However, as there was no control group in our previous study [6], wemight actually have only observed a time-related improvement in microcirculation, similar to currentresults.
As expected, we found a signi�cant dose-dependent reduction in heart rate with landiolol. Besides, arterialpressure, stroke volume and metabolic parameters remained unchanged, suggesting the use of low doselandiolol to control postoperative heart rate was safe. Further, echocardiographic systolic and diastolicindices of right and left ventricular function were not affected by landiolol, the E/A ratio being evenslightly improved. To the best of our knowledge, no detailed cardiac effects of landiolol had beenpreviously reported. Overall, our results are in favor of a valuable safety pro�le of landiolol in that speci�ccardiac surgical setting.
Page 11/15
If several strengths of the present study can be outlined (detailed and multimodal micro-andmacrocirculatory approaches of landiolol hemodynamic effects, presence of a control group todifferentiate a time-effect from a drug-effect, robust methodology), some comments are mandatoryregarding its limitations. First, patients were strictly selected: normal cardiac function, sinus mode,elective conventional cardiac surgery. Subsequently, our results could not be extrapolated to more severepatients and/or surgical procedures. Second, we used peripheral NIRS in combination with a VOT, aspreviously described. We acknowledge physiological and technical limits of this method which cannotcapture all the subtleties of the microcirculation. However, the simultaneous use of sublingualvideomicroscopy reinforces the absence of signi�cant microcirculatory effects of landiolol. Additionaltools as capillary re�ll time could also be assessed in future issues. Finally, although not signi�cant, onecan argue that right ventricular echocardiographic parameters were slightly altered in the landiolol group.Thus, further studies should speci�cally focus on potential effects of landiolol on the right ventricle,especially in patients with right ventricular dysfunction.
ConclusionsIn conclusion, the MMELPOAF study is the �rst randomized controlled trial describing the effects of adose ranging of landiolol following cardiac surgery on both micro- and macrocirculation. No signi�cantalterations were found, suggesting a good hemodynamic safety pro�le in that speci�c surgical setting.
DeclarationsDetails of authors’ contribution
AF participated in the design of the study, patients inclusions and manuscript redaction. MJL participatedin the design of the study, patients inclusions, statistical analysis and manuscript redaction. LCparticipated in patients inclusions. WF participated in the design of the study and patients inclusions. WJparticipated in patients inclusions. NRS participated in the design of the study. BA, SJ and MPparticipated in coordination and helped to draft the manuscript. JLF participated in the design of thestudy, coordination and helped to draft the manuscript.
All authors read and approved the �nal manuscript.
Acknowledgments: Not applicable
Con�icts of interest:
-Arnaud Ferraris received lecture fees from Amomed Pharma France
-Jean-Luc Fellahi is member of the Scienti�c Advisory Board Amomed Pharma France and receivedconsulting and lecture fees.
-The other authors have no con�icts of interest to declare
Page 12/15
Funding statement: Support was provided by the ARCOTHOVA Group (Grant: 10,000 €) and AmomedPharma France (20,000 €)
Acknowledgments : Not applicable
Availability of data : On demand to the corresponding author
Ethics Committee approval : Comité de protection des personnes Ouest VI, July 17th 2018; AgenceNationale de Sécurité du Médicament, July 10th 2018. Each patient received appropriate information andwritten informed consent was systematically collected.
Consent for publication : Not applicable
References1. Maesen B, Nijs J, Maessen J, Allessie M, Schotten U. Post-operative atrial �brillation: a maze of
mechanisms. Europace. 2012;14:159–74.
2. Fellahi J-L, Heringlake M, Knotzer J, Fornier W, Cazenave L, Guarracino F. Landiolol for managingatrial �brillation in post-cardiac surgery. Eur Heart J Suppl. 2018;20:A4–9.
3. Mio Y. [New ultra-short-acting beta-blockers: landiolol and esmolol–the effects on cardiovascularsystem]. Masui. 2006;55:841–8.
4. Li L, Ai Q, Lin L, Ge P, Yang C, Zhang L. E�cacy and safety of landiolol for prevention of atrial�brillation after cardiac surgery: a meta-analysis of randomized controlled trials. Int J Clin Exp Med.2015;8:10265–73.
5. Shibata SC, Uchiyama A, Ohta N, Fujino Y. E�cacy and Safety of Landiolol Compared to Amiodaronefor the Management of Postoperative Atrial Fibrillation in Intensive Care Patients. J CardiothoracVasc Anesth. 2016;30:418–22.
�. Fornier W, Jacquet-Lagrèze M, Collenot T, Teixeira P, Portran P, Schweizer R, et al. Microvasculareffects of intravenous esmolol in patients with normal cardiac function undergoing postoperativeatrial �brillation: a prospective pilot study in cardiothoracic surgery. Crit Care Lond Engl.2017;21:302.
7. Monthé-Sagan K, Fischer M-O, Saplacan V, Gerard J, Hanouz J-L, Fellahi J-L. Near-infraredspectroscopy to assess microvascular dysfunction: A prospective pilot study in cardiac surgerypatients. J Crit Care. 2016;31:264–8.
�. Creteur J, Carollo T, Soldati G, Buchele G, De Backer D, Vincent J-L. The prognostic value of muscleStO2 in septic patients. Intensive Care Med. 2007;33:1549–56.
9. Jacquet-Lagrèze M, Allaouchiche B, Restagno D, Paquet C, Ayoub J-Y, Etienne J, et al. Gut andsublingual microvascular effect of esmolol during septic shock in a porcine model. Crit Care LondEngl. 2015;19:241.
Page 13/15
10. De Backer D, Ospina-Tascon G, Salgado D, Favory R, Creteur J, Vincent J-L. Monitoring themicrocirculation in the critically ill patient: current methods and future approaches. Intensive CareMed. 2010;36:1813–25.
11. Ferraris A, Jacquet-Lagrèze M, Fellahi J-L. Four-wavelength near-infrared peripheral oximetry incardiac surgery patients: a comparison between EQUANOX and O3. J Clin Monit Comput. 2017.
12. Ince C, Boerma EC, Cecconi M, De Backer D, Shapiro NI, Duranteau J, et al. Second consensus on theassessment of sublingual microcirculation in critically ill patients: results from a task force of theEuropean Society of Intensive Care Medicine. Intensive Care Med. 2018;44:281–99.
13. Hessler M, Arnemann P-H, Zamit F, Seidel L, Kampmeier T-G, Kathöfer U, et al. A new complimentaryweb-based tool for manual analysis of microcirculation videos: Validation of the Capillary Mapperagainst the current gold standard AVA 3.2. Microcirc N Y N 1994. 2018;25:e12505.
14. version) JP (S. to 2007) DB (up, to 2002) SD (up, to 2005) DS (up, authors (src/rs.f) E, sigma) SH(Author �xed, et al. nlme: Linear and Nonlinear Mixed Effects Models [Internet]. 2018 [cited 2019 Mar14]. Available from: https://CRAN.R-project.org/package=nlme.
15. De Backer D, Donadello K, Sakr Y, Ospina-Tascon G, Salgado D, Scolletta S, et al. Microcirculatoryalterations in patients with severe sepsis: impact of time of assessment and relationship withoutcome. Crit Care Med. 2013;41:791–9.
1�. Backer DD, Dubois M-J, Schmartz D, Koch M, Ducart A, Barvais L, et al. Microcirculatory Alterations inCardiac Surgery: Effects of Cardiopulmonary Bypass and Anesthesia. Ann Thorac Surg.2009;88:1396–403.
17. Vellinga NAR, Boerma EC, Koopmans M, Donati A, Dubin A, Shapiro NI, et al. International study onmicrocirculatory shock occurrence in acutely ill patients. Crit Care Med. 2015;43:48–56.
Figures
Page 14/15
Figure 1
Flow-chart of the study
Page 15/15
Figure 2
Near-infrared spectroscopy variables combined with a vascular occlusion test at six different time pointsin placebo (n=28) and landiolol (n=30) patients. A: Resaturation speed (%/sec); B: Desaturation time(sec); C: Delta rSO2 (%). rSO2: regional oxygen saturation (%).
Figure 3
Macrocirculatory hemodynamic variables at six different time points in placebo (n=28) and landiolol(n=30) patients. A: Heart rate (HR, min-1); B: Indexed stroke volume (Svi, mL/m2); C: Mean arterialpressure (MAP, mmHg); D: Pulse pressure variation (PPV, %).
Supplementary Files
This is a list of supplementary �les associated with this preprint. Click to download.