18
Steven Joniau, MD, PhD University Hospitals Leuven Leuven Belgium Surgery for localized, locally advanced and high risk prostate cancer
| Date post: | 14-Apr-2017 |
| Category: |
Health & Medicine |
| Upload: | europa-uomo-epad |
| View: | 740 times |
| Download: | 1 times |

Steven Joniau, MD, PhD
University Hospitals Leuven
Leuven
Belgium
Surgery for localized, locally advanced and
high risk prostate cancer
117,328 patients with prostate cancer
26,410 low risk (22.5%)
cT1-T2, PSA <10 ng/ml AND Gleason 2-6
26,611 intermediate risk (22.7%)
cT1-T2 AND PSA 10 - <20 OR Gleason 7
30,159 high risk (25.7%)
cT3 or PSA 20-50 or Gleason 8-10
Non-curatively treated
Rider JR et al. Eur Urol 2012 2
Who dies of PCa? Natural evolution of non-curatively treated PCa
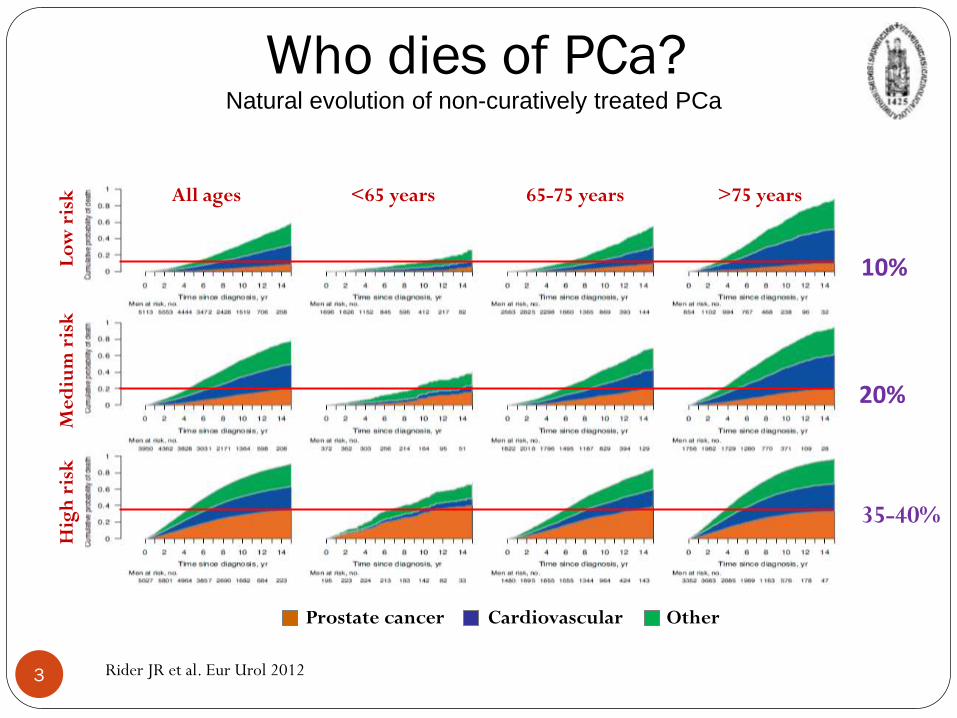
10%
20%
35-40%
Rider JR et al. Eur Urol 2012
All ages <65 years 65-75 years >75 years
Prostate cancer Cardiovascular Other
Lo
w r
isk
M
ed
ium
ris
k
Hig
h r
isk
Who dies of PCa?
Natural evolution of non-curatively treated PCa
3

Complete removal of the prostate, seminal vesicles, and pelvic lymph nodes (when necessary)
• With minimal perioperative morbidity, no blood transfusions, and early return to normal activities
• No positive surgical margins
• No long-term loss of continence or potency
Goals of modern radical prostatectomy (RP)
4

PIVOT Trial
PSA detected
RP vs observation for localised PCa
RP did not significantly reduce all-cause or PCa-specific mortality as compared
with observation
Wilt TJ et al. N Engl J Med 2012;367:203-13
PCa-specific mortality
5

Low-risk PCa
PCa specific mortality
6
Overall mortality
Wilt TJ et al. N Engl J Med 2012;367:203-13

PCa specific mortality
7
Overall mortality
Intermediate risk PCa
Wilt TJ et al. N Engl J Med 2012;367:203-13

PCa-specific survival
~45%
~17%
P= 0.05
High risk PCa
8 Wilt TJ et al. N Engl J Med 2012;367:203-13

Briganti A, Spahn M, Joniau S et al. for EMPaCT Eur Urol 2013
Only men ≤ 59 years old had higher risk of PCa-related
death than death-related to other causes
10%
<10%
Prostate cancer Other
MORTALITY RATES FOR SURGICALLY TREATED
HIGH-RISK PCa

Cooperberg M, et al. AUA 2015 – Data from CAPSURE
Which treatment for which cancer?
Up untill 2007, Low-risk PCa was too often actively treated,
while high-risk PCa was too often undertreated 10

Cooperberg M, et al. AUA 2015 – Data from CAPSURE 11
After 2007, Low-risk PCa was more often treated with AS/WW,
while high-risk PCa was more often actively treated!!!
Which treatment for which cancer?

Cumulative incidence function estimates of cancer
specific and other cause mortality survival curves
(n=34 515), stratified according to treatment type.
Sooriakumaran P et al. BMJ 2014;348:bmj.g1502
M+ or N+ or T4 or
PSA>50 Low Intermediate High
RP
RT
12

Sooriakumaran P et al. BMJ 2014;348:bmj.g1502
13
Cumulative incidence function estimates of cancer
specific and other cause mortality survival curves
(n=34 515), stratified according to treatment type.

Cooperberg M, et al. AUA 2015 – Data from CAPSURE 14
HIGH-RISK 15-Y
EA
R C
AN
CE
R M
OR
TA
LIT
Y

- Retrospective analysis of data from the Norwegian Prostate Cancer Registry, 2004-2005
- 3486 patients, RP (n = 895), EBRT +/- ADT (n = 1339), or no local treatment (n = 1252)
- Clinical stage T1-T3, PSA ≤100 ng/ml, D’Amico risk group stratification
- Comparison of active local treatment (RP, RAD) versus no active local treatment (NoLocTrt)
PCa mortality
Other cause mortality
15
HIGH-RISK

Big surgeon, big incision…?

• NO difference in positive surgical margins
• NO difference in incontinence
• SMALL difference in erectile dysfunction in favor of RALP

The changing role of surgery
• Properly performed, RP is a highly effective treatment
for high-risk prostate cancer in men with a sufficiently long life expectancy to justify the risks
• Outcomes of RP – cancer control, peri-op complications, and long-term urinary and sexual function – are directly related to the skill and experience of the surgeon, but not to the technology used (open v. robot-assisted)
18

















