272
| Date post: | 10-Mar-2016 |
| Category: |
Documents |
| Upload: | hospital-em-foco |
| View: | 306 times |
| Download: | 25 times |

Surgery for Low Back Pain

Marek SzpalskiRobert GunzburgBjörn L. RydevikJean-Charles Le HuecH. Michael Mayer (Eds.)
Surgery for Low Back Pain

ISBN: 978-3-642-04546-2 e-ISBN: 978-3-642-04547-9
DOI: 10.1007/978-3-642-04547-9
Springer Heidelberg Dordrecht London New York
Library of Congress Control Number: 2009938032
© Springer-Verlag Berlin Heidelberg 2010
This work is subject to copyright. All rights are reserved, whether the whole or part of the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfilm or in any other way, and storage in data banks. Duplication of this publication or parts thereof is permitted only under the provisions of the German Copyright Law of September 9, 1965, in its current version, and permission for use must always be obtained from Springer. Violations are liable to prosecution under the German Copyright Law.
The use of general descriptive names, registered names, trademarks, etc. in this publication does not imply, even in the absence of a specific statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use.
Product liability: The publishers cannot guarantee the accuracy of any information about dosage and appli-cation contained in this book. In every individual case the user must check such information by consulting the relevant literature.
Cover design: eStudio Calamar, Figueres/Berlin
Printed on acid-free paper
Springer is part of Springer Science+Business Media (www.springer.com)
Marek Szpalski, MDDepartment of Orthopedic SurgeryHôpitaux Iris SudUniversité Libre de Bruxelles142 rue Marconi1190 Brussels, Belgium
Department of OrthopedicsNew York UniversityNew York, [email protected]
Robert Gunzburg, MDEeuwfeestkliniekAlgemeen Ziekenhuis MonicaHarmoniestraat 682018 [email protected]
Björn L. Rydevik, MD, PhDSahlgrenska University Hospital/SahlgrenskaDepartment Orthopaedic Surgery413 45 Gö[email protected]
Jean-Charles Le Huec, MDCHU Bordeaux Hôpital PellegrinService d’Orthopédie TraumatologiePlace Amalie Raba Leon33076 Bordeaux [email protected]
H. Michael Mayer, MD, PhDOrthopädische KlinikMünchen-HarlachingWirbelsäulenzentrumHarlachinger Str. 5181243 Mü[email protected]

v
Low back pain is one of the most common conditions encountered in clinical prac-tice; however, its definition itself is subject to debate and precise knowledge about it is conflicting. It can be attributed to a great number of different origins although, often, the true cause of nociception cannot be precisely defined. Furthermore, psy-chosocial variables have an important influence on the reporting back pain symp-toms. Nevertheless, low back pain and the pathologies believed to be its cause are the main indication for spine surgery in most area of the world while true evidence about indications remains elusive and there is much discussion about the very different techniques used.
The goal of this book is to shed some light on this complex subject. The indispens-able bases of biology and biomechanics of spinal structures are covered as well as the important psychosocial determinants associated with back complaints. Diagnosis is now enhanced by new magnetic resonance techniques described thoroughly.
Conservative treatment is still the base of low back pain handling, and natural his-tory of the condition as well as the main conservative therapeutic options are described in detail. Medications, rehabilitation, back schools, manipulative therapies, and orthoses are the subject of fully documented chapters.
Surgical techniques abound for the treatment of lumbar spine disorders and this book tries to clarify their indications and results. For many years fusion was the most used technique and became the “de facto” gold standard. The role of pelvic girdle pain and facet syndrome is subject to debate and the possible surgical treatment is discussed in those conditions. Chapters will cover different technique as well as the possible drawbacks like blood loss and adjacent level degeneration. The latter has led to the development of “nonfusion” technologies like artificial disks, semirigid fixa-tion techniques, or interspinous implants. Indications, counter indications, techniques, and complications of those different techniques are presented and lead to discussion about what evidence we have for their effectiveness.
Outcome assessment is paramount to finding evidence for treatments of low back pain. The principles of outcome assessment in back pain as well as the review of actual available evidence ends the book.
This book is intended for clinicians as well as researchers in many fields of spinal disorders. It is of use to orthopedic and neurosurgeons, rheumatologists, neurologists, physiatrists, physical therapists, as well as psychologists and social security and insurance specialists.
Brussels, Belgium Marek SzpalskiAntwerp, Belgium Robert Gunzburg
Preface

vii
Contents
Part I Basics. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1.1 The Biology of Intervertebral Disc Degeneration . . . . . . . . . . . . . . . . 3Cornelia Neidlinger-Wilke and Hans-Joachim Wilke
1.2 Low Back Pain: Where Does the Pain Come From? . . . . . . . . . . . . . 11Helena Brisby
1.3 The Role of Cytokines in the Degenerative Spine . . . . . . . . . . . . . . . . 17Björn Rydevik and Helena Brisby
1.4 Psychosocial Aspects of Low Back Pain. . . . . . . . . . . . . . . . . . . . . . . . 23Christine Cedraschi and Valérie Piguet
1.5 Instability and Low Back Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Tommy Hansson
Part II Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
2.1 Dynamic MRI of the Spine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39J. J. Abitbol, Soon-Woo Hong, Sana Khan, and Jeffrey C. Wang
2.2 Assessment of Status of End Plate and Diffusion in Degenerative Disc Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47S. Rajasekaran
2.3 The Role of Physician Extenders in a Low Back Pain Practice. . . . . 57Michael R. Zindrick, Michael N. Tzermiadianos, Cary R. Templin, and Raymond E. Hines III
Part III Conservative Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
3.1 Natural Evolution of Nonspecific Low-Back Pain . . . . . . . . . . . . . . . 65Michel Benoist and Thibaut Lenoir
3.2 Prescribing Conservative Treatment for Low Back Pain. . . . . . . . . . 73F. Balagué and J. Dudler

viii Contents
3.3 Comprehensive Rehabilitation for Low back Pain and Back Schools . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79Margareta Nordin
3.4 The Place of Chiropractic Care in the Treatment of Low Back Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85Christopher J. Colloca
3.5 Efficacy of IDET and PIRFT for the Treatment of Discogenic Low Back Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95Brian J. C. Freeman
3.6 Lumbar Orthoses to Prevent and Treat Low-Back Pain . . . . . . . . . . 101Michel Benoist and Thibaut Lenoir
Part IV Surgical Treatment: Fusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 107
4.1 Indication for Lumbar Spinal Fusion . . . . . . . . . . . . . . . . . . . . . . . . . 109Max Aebi
4.2 Evidence for Efficacy of Pedicle-Based Systems . . . . . . . . . . . . . . . . . 123Jeremy Fairbank
4.3 Low Back Pain Is Not an Indication for Stabilisation in Patients Operated for Lumbar Spinal Stenosis . . . . . . . . . . . . . . . 127E. Munting
4.4 Hybrid Construct for DDD in the Lumbar Spine: The Compromise Between Fusion and Nonfusion . . . . . . . . . . . . . . . 131J. C. Le. Huec, R. Meyrat, F. Debusscher and S. Aunoble
4.5 The Management of Spondylolysis and Spondylolisthesis . . . . . . . . . 137Brian J. C. Freeman and Ujjwal K. Debnath
4.6 Transpedicular-Transdiscal-Transcorporal (TPDC)-Fixation. . . . . . 147Max Aebi
4.7 Facet Problems: A Surgical Indication? . . . . . . . . . . . . . . . . . . . . . . . 155F. Pellisé
4.8 Adjacent Level Disease: “Myth” or “Fact” . . . . . . . . . . . . . . . . . . . . . 159David A. Wong and Katherine E. Wong
4.9 Pelvic Girdle Pain: Indication for Surgery? . . . . . . . . . . . . . . . . . . . . 165Bengt Sturesson
4.10 Blood Loss Management in Major Spine Surgery . . . . . . . . . . . . . . . 169Serena S. Hu and Jeremy A. Lieberman

Contents ix
Part V Surgical Treatment: Other Technologies . . . . . . . . . . . . . . . . . . . . 175
5.1 How Disc Replacement Fits in the Treatment Algorithm for Degenerative Disc Disease: Refining Indications for Disc Replacement . . . . . . . . . . . . . . . . . . . . . 177Richard D. Guyer and Donna D. Ohnmeiss
5.2 Clinical Factors that May Affect Outcome in Lumbar Total Disc Replacement. What Is the Evidence? . . . . . . . 183Michael R. Zindrick, Mark Lorenz, Leonard I. Voronov, Michael N. Tzermiadianos, and Alexander Hadjipavlou
5.3 A Prospective Randomized Comparison of Two Lumbar Total Disk Replacements . . . . . . . . . . . . . . . . . . . . . . 193Richard D. Guyer and Donna D. Ohnmeiss
5.4 Limitations of Lumbar Disk Arthroplasty . . . . . . . . . . . . . . . . . . . . . 199Serena S. Hu
5.5 Is Posterior Dynamic Stabilization an Option to Avoid Adjacent Segment Decompensation? . . . . . . . . . . . . . . . . . . 207Missoum Moumene and Jürgen Harms
5.6 Immediate Biomechanical Effects of Lumbar Posterior Dynamic Stabilisation . . . . . . . . . . . . . . . . . . . . 213Brian J. C. Freeman and Caspar E. W. Aylott
5.7 Overview of Pedicle Screw-Based Posterior Dynamic Stabilization Systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 221Richard D. Guyer, Donna D. Ohnmeiss, and Kevin R. Strauss
5.8 Semirigid Fixation System for the Lumbar Spine . . . . . . . . . . . . . . . 227Dieter Grob, Andrea Luca, and Anne F. Mannion
5.9 Nonrigid Stabilization of the Spine – Problems Observed: Screw Loosening/Breakage/Implant Failure/Adjacent Segment Degeneration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 233Paul F. Heini
5.10 Interspinous Implants: State of the Art and Research of Evidence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 241Marek Szpalski, Robert Gunzburg, Christopher J. Colloca, and Robert J. Moore
5.11 NuBac Disc Arthroplasty System: Rationale and Clinical Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 249Massimo Balsano, Domagoj Coric, and Margreet Derks

x Contents
Part VI Outcomes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 257
6.1 Outcome Assessment for Cost-Utility Evaluations: SF-6D vs. EQ-5D . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 259Rikke Søgaard, Terkel Christiansen, and Finn Bjarke Christensen
6.2 Review of the Medical Evidence Regarding the Surgical Treatment of Low Back Pain . . . . . . . . . . . . . . . . . . . . . . 267Andrew P. White, Justin G. Brothers, and Alexander R. Vaccaro
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 279

xi
J.J. Abitbol California Spine Group, 5395 Ruffin Road Suite 103, San Diego, CA 92123, USA [email protected]
Max Aebi Center for Orthopaedic Research, University of Bern, Stauffenbachstrasse 78, 3014, Bern, Switzerland [email protected]
S. Aunoble Spine Unit, Bordeaux University Hôpital, CHU Bordeaux, 33076 Bordeaux, France
Caspar E. W. Aylott Department of Spinal Surgery, Level 3, Theatre Block, Royal Adelaide Hospital, North Terrace, Adelaide, SA 5000, Australia
Federico Balagué Service de Rhumatologie, Médicine Physique et Réhabilitation, HFR- Hospital Cantonal, Case postale, 1708 Fribourg, Switzerland [email protected]
Massimo Balsano Spinal Regional Department, ULSS 4, Schio, Vicenza, Italy [email protected]
Michel Benoist University of Paris VII, Hôpital Beaujon, 100 Bd. du Gl. Leclerc 92110 Clichy, France [email protected]
Helena Brisby Department of Orthopaedics, Sahlgrenska University Hospital, 413 45, Gothenburg, Sweden [email protected]
Justin G. Brothers Thomas Jefferson University, Philadelphia, PA, USA [email protected]
Christine Cedraschi Division of Internal Medicine for Rehabilitation, Geneva University Hospitals, Rue Gabrielle Perret-Gentil 4, 1211 Geneva 14, Switzerland [email protected]
Finn Bjarke Christensen Health Economics Unit, Institute of Public Health, University of Southern Denmark, J.B. Winsløws Vej 9, 5000 Odense C, Denmark
Terkel Christiansen Health Economics Unit, Institute of Public Health, University of Southern Denmark, J.B. Winsløws Vej 9, 5000 Odense C, Denmark [email protected]
Contributors

xii Contributors
Christopher J. Colloca Department of Kinesiology, Arizona State University, 101 South Roosevelt Avenue, Chandler, AZ 85226, USA [email protected]
Domagoj Coric Carolina Neurosurgery and Spine Associates, 225 Baldwin Avenue, Charlotte, NC 28207, USA, [email protected]
Ujjwal K. Debnath Department of Orthopaedic Surgery, Letterkenny General Hospital, Donegal, Ireland
F. Debusscher Spine Unit, Bordeaux University Hospital, CHU Bordeaux, 33076 Bordeaux, France
Margreet Derks Pioneer Surgical Technology BV, Princenhof Park 10, 3972 NG Driebergen, The Netherlands, [email protected]
Jean Dudler Service de Rhumatologie, Médecine Physique et Réhabilitation, CHUV Hôpital Orthopédique, Avenue Pierre-Decker 4, 1011 Lausanne, Switzerland, [email protected]
Jeremy Fairbank Nuffield Orthopaedic Centre, Oxford OX3 7LD, UK [email protected]
Brian J.C. Freeman Department of Spinal Surgery, Level 3, Theatre Block, Royal Adelaide Hospital, North Terrace, Adelaide, SA 5000, Australia [email protected]
Dieter Grob Spine Center, Schulthess Klinik, Lengghalde 2, 8008 Zürich, Switzerland [email protected]
Robert Gunzburg Eeuwfeestkliniek, Algemeen Ziekenhuis Monica, Harmoniestraat 68, 2018 Antwerpen, Belgium [email protected]
Richard D. Guyer Texas Back Institute, 6020 West Parker Rd. 200, Plano, TX 75093, USA, [email protected]
Alexander Hadjipavlou University of Crete, Heraklion, 71110 Crete, Greece [email protected]
Tommy Hansson Department of Orthopaedics, Sahlgrenska Academy, 413 45 Göteborg, Sweden, [email protected]
Jürgen Harms Department of Orthopaedic Traumatology I, Spine Surgery, Klinikum Karlsbad-Langensteinbach, 76307 Karlsbad, Germany [email protected]
Paul F. Heini Spine & Ortho center, Klinik Sonnenhof 3006 Bern, Switzerland, [email protected]
Raymond E. Hines III Hinsdale Orthopedic Associates, Hinsdale, IL 60521, USA
Soon-Woo Hong California Spine Group, 5395 Ruffin Road, Suite 103, San Diego, CA 92123, USA

Contributors xiii
Serena S. Hu Department of Orthopedic Surgery, 500 Parnassus Avenue, Room MU320 West, San Francisco, CA 94143, USA, [email protected]
J.C. Le Huec Spine Unit, Bordeaux University Hospital, CHU Bordeaux, 33076 Bordeaux, France, [email protected]
Sana Khan California Spine Group, 5395 Ruffin Road, Suite 103, San Diego, CA 92123, USA
Thibaut Lenoir Department of Orthopaedic Surgery, Hôpital Beaujon, 100 Bd. du Gl. Leclerc, 92110 Clichy, France, [email protected]
Mark Lorenz Hinsdale Orthopaedic Associates, SC, Hinsdale, IL 60521, USA [email protected]
Andrea Luca Spine Center, Schulthess Klinik, Lengghalde 2, 8008 Zürich, Switzerland
Anne F. Mannion Spine Center, Schulthess Klinik, Lengghalde 2, 8008 Zürich, Switzerland, [email protected]
R. Meyrat Spine Unit, Bordeaux University Hospital, CHU Bordeaux, 33076 Bordeaux, France
Robert J. Moore The Adelaide Centre for Spinal Research, Institute of Medical and Veterinary Science, Adelaide, SA, Australia, [email protected]
Missoum Moumene Department of Research and Development, DePuy Spine Inc., Raynham, MA, USA, [email protected]
E. Munting Clinique Saint Pierre, 1340 Ottignies Louvain-la-Neuve, Belgium, [email protected]
Cornelia Neidlinger-Wilke Institute of Orthopaedic Research and Biomechanics, Centre of Musculoskeletal Research, University of Ulm, Helmholtzstraße 14, 89081 Ulm, Germany, [email protected]
Margareta Nordin Occupational and Industrial Orthopaedic Center (OIOC), Graduate Program of Ergonomics and Biomechanics, New York University (NYU) Hospital for Joint Diseases, NYU Langone Medical Center, CDC/NIOSH Education and Research Center (ERC), New York University, New York, NY, USA [email protected]
Donna D. Ohnmeiss Texas Back Institute Research Foundation, 6020 West Parker Rd. 200, Plano, TX 75093, USA, [email protected]
F. Pellisé Unitat de Cirugia del Raquis Vall d’Hebron, Hospital Vall d’Hebron, Barcelona, Vall d’Hebron 119-129, 08035 Barcelona, Spain [email protected]
Valérie Piguet Multidisciplinary Pain Centre, Division of Clinical Pharmacology and Toxicology, Geneva University Hospitals, Rue Gabrielle Perret-Gentil 4, 1211 Geneva 14, Switzerland, [email protected]

xiv Contributors
S. Rajasekaran Department of Orthopaedic and Spine Surgery, Ganga Hospital, 313 Mettupalayam Road, Coimbatore, 641043 Tamil Nadu, India [email protected]
Björn Rydevik Department of Orthopaedics, Sahlgrenska University Hospital, 413 45, Gothenburg, Sweden, [email protected]
Rikke Søgaard CAST–Centre for Applied Health Services Research and Technology Assesment, University of Southern Denmark, J.B. Winsløws Vej 9, 5000 Odense C, Denmark, [email protected]
Kevin R. Strauss K2M, Inc., Leesburg, VA, USA
Bengt Sturesson Department of Orthopaedics, Ängelholm Hospital, 262 81 Ängelholm, Sweden, [email protected]
Marek Szpalski Department of Orthopedic Surgery, Hôpitaux Iris Sud, Université Libre de Bruxelles, 142 rue Marconi, 1190 Brussels, Belgium Department of Orthopedics, New York University New York, USA [email protected]
Cary R. Templin Hinsdale Orthopedic Associates, Hinsdale, IL 60521, USA
Michael N. Tzermiadianos Hinsdale Orthopedic Associates, Hinsdale, IL 60521, USA 45, Eleftheria Square (Electra BLD, 1st floor) 71201 Heraklion, Crete, Greece [email protected]
Alexander R. Vaccaro Department of Orthopaedic Surgery and Neurosurgery, Rothman Institute at Jefferson University Hospital, Thomas Jefferson University, Philadelphia, PA, USA, [email protected]
Leonard I. Voronov Loyola University Medical Center, Maywood, IL, USA
Jeffrey C. Wang Department of Orthopaedic Surgery, Santa Monica – UCLA Medical Center and Orthopaedic Hospital, 1250 16th Street, 7th Tower, No. 745, Santa Monica, CA 90404, USA
Jeremy A. Lieberman Spine Anesthesia Service Department of Anesthesia and Perioperative Care, University of California, San Francisco, 521 Parnassus Ave., Box 0648, Room L-008, San Francisco, CA, [email protected]
Andrew P. White Carl J. Shapiro Department of Orthopaedics - Stoneman 10, Harvard Medical School, Beth Israel Deaconess Medical Center, 330 Brookline Ave, Boston, MA 02215, USA, [email protected]
Hans-Joachim Wilke Institute of Orthopaedic Research and Biomechanics, Centre of Musculoskeletal Research, University of Ulm, Helmholtzstraße 14, 89081 Ulm, Germany, [email protected]
David A. Wong Advanced Center for Spinal Microsurgery, Presbyterian St. Luke’s Medical Center, Denver, CO 80218, USA, [email protected]
Katherine E. Wong Denver Spine, Advanced Center for Spinal Microsurgery, Presbyterian St. Luke’s Medical Center, Denver, CO 80111, USA
Michael R. Zindrick Hinsdale Orthopedic Associates, Hinsdale, IL 60521, USA [email protected]
Part
BasicsI

3M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_1.1, © Springer-Verlag Berlin Heidelberg 2010
Introduction: The Normal Intervertebral Disc
Intervertebral discs act as the joints of the spinal col-umn and provide it with mobility and flexibility. The predominant mechanical functions of intervertebral discs are to transmit the compressive loads through the spine and to allow it to bend and twist. These complex mechanical functions depend on the structural and bio-chemical composition of the disc matrix: the disc cells that are responsible for the synthesis and maintenance of these matrix molecules.
Morphologically, intervertebral discs consist of a cen-tral nucleus pulposus surrounded by the fibrous annulus lamellae. The discs are enclosed axially by the cartilagi-nous endplates, which form the interface between the disc and the adjacent vertebrae. The major components of the disc matrix are water, collagen and proteoglycans, mainly aggrecan. There is a gradient in the proportion of these three matrix constituents throughout the disc; the outer annulus has the highest collagen concentration and the lowest aggrecan and water content, while aggrecan and water concentration increase towards the central nucleus, with a decrease in collagen content.
Although disc cells occupy only one percent of the whole tissue, the annulus and nucleus cells produce and maintain all of the matrix molecules so that each disc cell is responsible for a large volume of matrix. As discs are avascular, oxygen and other nutrients must diffuse from these blood vessels across the endplate
and through the matrix to reach the cells of the disc, and products of metabolism must be removed by the reverse route. In addition, since the discs are subjected to mechanical loading at all times, disc cells are also exposed to multiple physical stimuli including tension, compression and also fluid flow (because discs lose and regain about 25% of their fluid during a diurnal cycle). The consequence of hydration and dehydration of the disc is a change in the physicochemical environ-ment of the disc cells since concentrations of matrix molecules, ions and hence, osmolarity are influenced by fluid loss and regain. All these factors are thought to affect the activity of disc cells and play an important role in the maintenance of a balance between the matrix forming and degrading processes.
Recent studies suggest that all these environmental factors and their complex interactions influence disc physiology. Changes in these factors, either as a cause or a consequence of degenerative changes in the disc tissue, are thought to influence disc matrix turnover. Besides these external factors, a strong familial predis-position for disc degeneration has been noted, suggest-ing that genetic effects are the highest risk factor for disc degeneration. The present review summarizes recent knowledge on the biology of disc degeneration and the open questions that remain to be investigated.
Biology of Disc Degeneration
Intervertebral disc degeneration is one of the main rea-sons for back pain and a very common burden for the affected patient as well as the society because of the high costs for the health system [28]. Though it is not known how much the degenerated disc itself contrib-utes to chronic back pain, it can be estimated that more
The Biology of Intervertebral Disc Degeneration
Cornelia Neidlinger-Wilke and Hans-Joachim Wilke
C. Neidlinger-Wilke (*) Institute of Orthopaedic Research and Biomechanics, Centre of Musculoskeletal Research, University of Ulm, Helmholtzstraße 14, 89081 Ulm, Germany e-mail: [email protected]
1.1

4 C. Neidlinger-Wilke and H.-J. Wilke
than 90% of all surgical spine treatments are performed as a consequence of disc degeneration.
There was very little research activity in the disc field for a long time, but during the last few years a number of studies investigating epidemiological [6, 7], biological [49, 50] and biomechanical aspects [1, 47] of disc degeneration have been published.
Histological Findings and Biomechanical Effects of Disc Degeneration
From a biomechanical point of view, the disc is a fas-cinating structure. The nucleus of the disc in the early life or in only slightly degenerated discs acts like a gelatinous mass. A compressive load decreases disc height and can increase the hydrostatic pressure up to a considerable magnitude [52], which pushes the sur-rounding structures in all directions away from the centre of the nucleus. This leads to a bulging of the endplates of the vertebrae and of the outer annulus, which leads to an almost equal stress distribution throughout the disc [13]. In flexion, extension or lat-eral bending, the inner and middle annulus is also compressed but the outer annulus has to resist more strain. During the day, load reduces the disc height mainly because of water being squeezed out, and also due to creep of the viscoelastic collagen fibres of the annulus. Both effects are reversible in healthy discs when unloading the spine, e.g. during a night’s bed rest [52]. The longer the load acts on the spine, the more the annulus bulges and the more the facet joints are loaded. Degenerated discs alter their structure and function [2, 53]. Finite element studies showed that the risk of prolapses is highest in the posterior and poste-rolateral annulus under load combinations, especially in a non- and mildly degenerated disc [42, 43]. Moderate or strongly degenerated discs have a lower risk for a prolapse.
The histomorphological alterations of the disc tis-sue are complex as recently reviewed [38]. The central nucleus, which has a very high water-binding capacity in young age, gets more and more dry and the gelati-nous structure changes into a more fibro-cartilaginous tissue. Cleft formation with fissures is often observed. In the nucleus of degenerated discs, the formation of cell clusters and an increased level of cell senescence
has been reported [39]. The finding of an increased number of senescent cells predominantly in the nucleus of herniated discs suggests that cell senescence plays an important role in disc degeneration. Also the annu-lus structure changes during degeneration. The annu-lus lamellae become more irregular with a more disorganized collagen and elastin network. Annular tear formation is considered as a morphological sign of degeneration in many discs [32]. These enormous structural changes result in a decreased flexibility and a reduced water-binding capacity of degenerated disc with the consequence that the discs have impaired load-bearing properties.
Epidemiology and Diagnosis of Disc Degeneration
For an epidemiological investigation of disc degenera-tion, these structural changes can be diagnosed by magnetic resonance imaging (MRI). Low disc signal intensity is considered as a sensitive sign of disc degen-eration. It, together with the determination of other important disc features (such as disc height, annulus fibrosus contours, tears in the annulus, fissures in the nucleus, end-plate morphology), is the basis of scoring the degree of disc degeneration [37, 50]. Twin studies using this technique have shown the high influence of genetic factors. However, recent MRI techniques also have limitations because of their poor specificity in the evaluation of significant disc degenerative changes. Measurements of intervertebral disc water (through determination of diffusion coefficients) might provide better means of determining impaired disc integrity and degrees of degeneration. In the future, quantitative dynamic MR imaging of patients during exposure to physiological loads could be a promising tool for a bet-ter diagnosis of disc degeneration.
Aetiology of Disc Degeneration
Disc degeneration is a complex problem with multiple factors contributing to this phenomenon. Mechanical loads, genetic predisposition, and alterations of the phys-icochemical environment of the disc are all discussed

51.1 The Biology of Intervertebral Disc Degeneration
to be contributors to degenerative pathways; it is not known, however, exactly how these different aspects interact and influence each other.
Influence of Mechanical Loading
Though it was thought for a long time that disc degen-eration is mainly caused by abnormal loading, no direct evidence for mechanical load-induced disc degeneration has yet been found possibly because its interactions with occupational and psychosocial fac-tors make a clear separation of mechanical from other factors difficult.
In animal experiments the direct influence of mechanical loading has found that discs exposed to abnormal compressive or vibration forces showed signs of degenerative changes [16, 23, 25, 26]. On the other hand, other well-controlled studies found no adverse effects on the disc after long-term compression or intense exercise [15, 36]. In a treadmill training study with young beagle dogs, measurements of disc collagen and proteoglycans supported the hypothesis that an adaptation of the tissue to enhanced motion and stress is possible. In vitro studies using human-disc cells taken from discs removed at surgery suggest that mechanical loads could influence gene expression of matrix-form-ing proteins or matrix-degrading enzymes [29, 30]. However, the effects of load were quite low and showed high variability between different patients. Effects on animal cells differ between studies. Physiological ranges of intermittent hydrostatic pressure applied to canine disc cells in alginate beads increased proteoglycan bio-synthesis [14]. On the other hand, high frequencies (around 5 Hz) of dynamic hydrostatic loading disrupted protein metabolism of pig intervertebral disc cells [20]. Thus, in vitro studies using disc cells suggest that mechanical loads can influence disc matrix turnover via alteration of gene expression or biosynthesis of disc matrix proteins or matrix degrading enzymes. In sum-mary, the results of most animal studies suggest that at least certain forms of mechanical loads can contribute to the induction of disc degeneration, while clinical studies failed to prove a strong causal link between occupa-tional exposures and disc degeneration. These results suggest that while mechanical factors have some influ-ence, other factors also contribute to the complex aetiol-ogy of disc degeneration.
Genetic Predisposition
Evaluations of questionnaires helped to identify envi-ronmental risk factors for disc degeneration like ciga-rette smoking, repetitive mechanical loading and lifting of heavy loads; relatively recent studies suggest, how-ever, that genetic influences might be the highest risk factor, and that environmental factors have only modest effects. Based on the results of many studies, genetic inheritance is now considered to be the highest risk fac-tor for disc degeneration [6].
From the findings of twin studies, genetic factors are estimated to contribute 60–70% to disc degenera-tion [7, 27, 41]. DNA-genotyping of blood samples of patients with disc degeneration and age-matched con-trols have led to the identification of a number of varia-tions (single nucleotide polymorphism) in individual genes associated with disc degeneration. Polymorphisms in genes encoding for aggrecan, collagen I, II, and IX have been correlated with degeneration-associated alterations of the disc matrix. Also variations in non-collagenous matrix proteins like CILP (cartilage inter-mediate layer protein) or in genes encoding for inflammation factors (interleukins (IL1, IL6) have been reported. Polymorphisms in genes encoding for matrix degrading enzymes like MMPs and in the vita-min D receptor genes have been found to accelerate degenerative changes though the exact mechanism is often unknown.
Initiation of Disc Degeneration: Alterations of the Physicochemical Environment
In normal intervertebral discs, the maintenance and turnover of the disc matrix are in a balanced state, which means that matrix formation and matrix degra-dation compensate each other (Fig. 1.1.1). Disc degen-eration starts when the catabolic processes prevail and exceed the synthesis of matrix-forming proteins. The changes of the disc tissue during degeneration have been recently reviewed [50].
The most striking biochemical alteration of disc matrix during degeneration is a degradation of aggre-can, the predominant disc matrix proteoglycan. These huge macromolecule aggregates with their high density

6 C. Neidlinger-Wilke and H.-J. Wilke
of fixed negative charges are responsible for the unusual high osmotic pressure, and thus, the high water-binding capacity of the disc tissue. Shorter molecules of aggre-can and a lower concentration explain the decreased hydration capacity of degenerated discs.
Impaired Nutrient Supply
Many environmental factors that are believed to contrib-ute to the initiation of these degenerative changes are discussed whereas decreased nutrition is assumed to be a key contributor [51]. Normal discs are avascular, and nutrient supply and removal of metabolic degradation products occur predominantly via diffusion from the blood vessels at the cartilaginous endplate. A reduction of this nutrient supply is assumed to be one – if not the major – reason for disc degeneration. Calcification of the cartilaginous endplates leads to a decreased permeability for nutrients and metabolites. In vivo measurements with microelectrodes have shown that the nutrient supply in the centre of many degenerated discs is low [5].
Disc cells are very sensitive to alterations of these environmental conditions. In vitro experiments have shown that the disc cells need critical concentrations of glucose, a suitable pH and oxygen supply to stay viable
and metabolic active [8, 9]. The cells are particularly sensitive to the accumulation of lactic acid, which decreases the pH [5]. In vitro studies have shown that an acidic pH decreases proteoglycan biosynthesis of disc cells, but does not decrease the activity of matrix-degrading enzymes. All of these alterations in the nutritional environment may result in adverse effects on disc cell function, and thus, contribute to degenera-tive changes of intervertebral discs [31].
Intervertebral disc cells exist in an unusual high osmotic environment compared to cells in other connec-tive tissues [48]. Due to reversible hydration and dehydra-tion of the disc, the osmotic environment is not constant, but underlies diurnal variation, with the highest value at the end of a working day when almost 25% of the disc fluid is extruded from the disc tissue, and the lowest val-ues in the morning after water imbibition, which occurs during the night when the axial load is very low [46].
Degeneration results in alterations to the osmotic environment: degradation of disc proteoglycans leads to a fall in osmolarity in the disc tissue. In vitro experi-ments with disc cells [54] and full-organ cultures of intervertebral discs [12] have shown that osmolarity can directly influence matrix formation and degradation as the expression of genes that are responsible for these anabolic or catabolic processes can be up- or down-reg-ulated by osmotic conditions [54]. Both diurnal changes
Fig. 1.1.1 Scheme of a normal disc. Annulus and nucleus cells produce matrix proteins (collagens and proteoglycans) and matrix degrading enzymes. Both processes are in balance. There is no
vascularization and innervation of the disc. It is suggested that intact aggrecan macromolecules have an inhibitory influence (…) on disc vascularization and innervation
disc cells produce- matrix proteins:
collagens
balance
- matrix degrading enzymes:
MMPs, TIMPs
normal disc
nerves
blood vessels
anulus cells
nucleus cells
proteoglycans (aggrecan)

71.1 The Biology of Intervertebral Disc Degeneration
and long-term alterations of the disc osmolarity as caused by degeneration may alter disc cell responses to mechanical loading.
Innervation and Vascularization
In degenerated discs, ingrowth of blood vessels and pain fibres is observed [11, 18]. Both processes are associated, and therefore may play a direct role in the development of discogenic back pain. It has been sug-gested that there is a causal relationship between the decreased proteoglycan and pressure and an increased vascularization and innervation of degenerated discs (Fig. 1.1.2). A possible role of angiogenic and neu-rotrophic growth factors in the regulation of disc neo-vascularization and innervation is supported by a recent immunohistological study [17]. An increased level of inflammatory mediators and matrix fragments in degenerated disc tissue is discussed to be responsi-ble for a progression of the degeneration process [3, 39]. As an association of degeneration with poly-morphisms of pro-inflammatory genes (IL-1, IL-6, COX-2) has been demonstrated, these inflammation
factors might play a role in the disc degradation path-way. There are an increasing number of studies inves-tigating the role of mediators, growth factors and inflammation molecules in disc pathogenesis.
Molecular Aspects of Disc Degeneration
For an explanation of the mechanism of disc degenera-tion, it is important to know how all the above mentioned factors, which may contribute to degenerative processes, directly influence disc cell function as the disc cells, though they occupy less than 1% of the disc tissue, are responsible for disc matrix turnover and maintenance.
Alterations of the discs’ physical and biochemical environment could be transduced into cellular res-ponses via proteins and receptors in the cell membrane, ion channels and receptors. A high number of signal-ling transduction pathways is reported and both mechanical loads and alterations of the metabolic envi-ronment can initiate via specific pathways intracellular mechanisms that finally lead to an up- or down-regula-tion of genes for matrix forming proteins or matrix degrading enzymes.
Fig. 1.1.2 Scheme of tissue alterations that are discussed to con-tribute to disc degeneration. There is an imbalance between matrix formation and degradation, whereas degradation exceeds biosynthesis. Impaired disc nutrition leads to cell senescence and apoptosis. Cell death is observed in degenerated discs. The pre-dominant disc proteoglycan aggrecan is degraded. Therefore, degenerated discs have a reduced water binding capacity.
Moreover, it is suggested that degraded aggrecan macromolecules reduce their inhibitory influence on disc vascularization and innervation, and nerves and blood vessels can invade into the disc tissue. Recent studies suggest that these disc matrix alterations are regulated by angiogenic and neurotrophic factors, inflamma-tion factors and mechanical influences. Their exact role in the pathogenesis of disc degeneration remains to be investigated
less biosythesis,more degradation: MMPs, TIMPs, Cathepsins
degenerated disc
Pleiotrophin
VEGF
nerves
aggrecan degradationcell deathimpairednutrition
blood vessels

8 C. Neidlinger-Wilke and H.-J. Wilke
Degradation and disorganization of the disc matrix is a visible sign of the degeneration process.
Matrixmetalloproteinases (MMPs) are a well-char-acterized group of enzymes which are known to play a crucial role in the degenerative pathways, though the mechanisms are still unknown. Their activity is modu-lated by the tissue inhibitors of metalloproteinases (TIMPs) [22, 44]. Under normal conditions, MMPs and TIMPs are in balance, but an imbalance between MMPs and TIMPs can increase MMP activity and degradation.
In the literature, there are reports that several MMPs (MMP-1, -2, -3, -7, -9, and -13) are increased during disc degeneration [24, 40]. Many disc matrix collagens and other macromolecules are possible substrates for these enzymes. The fact that degradation products that result from MMP-activity might also have regulatory functions indicates the high complexity of this aspect of matrix breakdown. Moreover, the possible role of aggre-can degrading enzymes (ADAMTs) in disc breakdown is also discussed in the literature [45].
Another group of matrix-degrading enzymes, the cathepsins, might also play a role in disc matrix degra-dation. As these enzymes show their optimum activity in a more acidic environment, these enzymes could play a role in later steps of matrix degradation when an accumulation of lactic acid has already decreased the pH of the disc matrix [33].
The role of inflammatory mediators in interverte-bral disc degeneration has been recently reviewed [35]. A number of mediators including nitric oxide, inter-leukins, PGE2, TNF-alpha and other cytokines have been implicated in the degeneration of intervertebral discs (reviewed by Paesold et al. [33]). However, though these studies show that disc cells have the potential to produce inflammatory mediators and cytokines, the exact mechanisms of their role in the degenerative pathway and their possible contribution to discogenic back pain remain to be investigated.
In degeneration matrix, breakdown predominates over synthesis. Upregulation of the responsible proteases such as MMPs and ADAMTs (a disintegrin and metalloprotei-nase-1 with thrombospondin motifs) by cytokines includ-ing IL-1, IL-6 and TNF-alpha, which were all found in degenerated [34] and herniated discs [4], could play an important role in the progression of disc degeneration. As these cytokines are all produced by both disc cells [19] and by inflammatory cells like mast cells and macrophages [21], the source of these cytokines (disc cells or blood cells) is still unclear. Thus, disc vascularization might
play an important role in the initiation of degradative pathways regulated by inflammation factors. However, as disc cells have the potential to produce the inflammatory cytokines that are necessary to mediate an inflammation reaction [33], the role of the disc itself in the initiation of these processes remains to be investigated.
Summary
In summary, though the present results suggest that disc degeneration might be genetic in origin, the identi-fication of these genes alone will not provide clinical solutions for an understanding of pathogenesis path-ways of disc degeneration. Our knowledge of the biol-ogy of disc degeneration has increased during the past years, but there are many unanswered questions that remain to be investigated: There is still no clear diagno-sis in approximately 85% of disc degeneration related disorders and no clinical consensus on indications of methods and treatment. Functional genetic strategies will be necessary to identify those genes involved in disc-degeneration linked pathologies, which can act as targets for the development of diagnostic and repair strategies. These techniques have to be based on the knowledge of disc physiology, cell biology and biome-chanics to prevent inappropriate or very expensive treatments of disc degeneration-related disorders.
Acknowledgement The authors thank Dr. Jill Urban, Department of Physiology, Anatomy and Geneticsy, Oxford University, UK, for reviewing this manuscript.
References
1. Adams MA, Roughley PJ (2006) What is intervertebral disc degeneration, and what causes it? Spine 31:2151–2161
2. Adams MA, McNally DS, Dolan P (1996) ‘Stress’ distribu-tions inside intervertebral discs. The effects of age and degeneration. J Bone Joint Surg Br 78:965–972
3. Aota Y, An HS, Homandberg G, Thonar EJ, Andersson GB, Pichika R, Masuda K (2005) Differential effects of fibronec-tin fragment on proteoglycan metabolism by intervertebral disc cells: a comparison with articular chondrocytes. Spine 30:722–728
4. Aydin MV, Sen O, Kayaselcuk F, Bolat F, Tufan K, Caner H, Altinors N (2005) Analysis and prevalence of inflammatory cells in subtypes of lumbar disc herniations under cyclooxy-genase-2 inhibitor therapy. Neurol Res 27:609–612

91.1 The Biology of Intervertebral Disc Degeneration
5. Bartels EM, Fairbank JC, Winlove CP, Urban JP (1998) Oxygen and lactate concentrations measured in vivo in the intervertebral discs of patients with scoliosis and back pain. Spine 23:1–7; discussion 8
6. Battie MC, Videman T (2006) Lumbar disc degeneration: epi-demiology and genetics. J Bone Joint Surg Am 88(suppl 2): 3–9
7. Battie MC, Videman T, Gibbons L, Fisher L, Manninen H, Gill K (1995) 1995 Volvo Award in clinical sciences. Determinants of lumbar disc degeneration. A study relating lifetime exposures and magnetic resonance imaging findings in identical twins. Spine 15:2601–2612
8. Bibby SR, Urban JP (2004) Effect of nutrient deprivation on the viability of intervertebral disc cells. Eur Spine J 13: 695–701
9. Bibby SRS, Jones DA, Ripley RM, Urban JPG (2005) Metabolism of the intervertebral disc: effects of low levels of oxygen, glucose and pH on rates of energy metabolism of bovine nucleus pulposus cells. Spine 30:487–496
10. Freemont AJ (2009) The cellular pathobiology of the degener-ate intervertebral disc and discogenic back pain. Rheumatology (Oxford, England) 48:5–10. DOI ken396 [pii] 10.1093/rheu-matology/ken396
11. Freemont AJ, Peacock TE, Goupille P, Hoyland JA, O’Brien J, Jayson MI (1997) Nerve ingrowth into diseased interver-tebral disc in chronic back pain. Lancet 350:178–181
12. Haschtmann D, Stoyanov JV, Ferguson SJ (2006) Influence of diurnal hyperosmotic loading on the metabolism and matrix gene expression of a whole-organ intervertebral disc model. J Orthop Res 24:1957–1966
13. Heuer F, Schmidt H, Wilke HJ (2008) The relation between intervertebral disc bulging and annular fiber associated strains for simple and complex loading. J Biomech 41: 1086–1094
14. Hutton WC, Elmer WA, Bryce LM, Kozlowska EE, Boden SD, Kozlowski M (2001) Do the intervertebral disc cells respond to different levels of hydrostatic pressure? Clin Biomech (Bristol, Avon) 16:728–734
15. Hutton WC, Ganey TM, Elmer WA, Kozlowska E, Ugbo JL, Doh ES, Whitesides TE Jr (2000) Does long-term compres-sive loading on the intervertebral disc cause degeneration? Spine 25:2993–3004
16. Iatridis JC, Mente PL, Stokes IA, Aronsson DD, Alini M (1999) Compression-induced changes in intervertebral disc properties in a rat tail model. Spine 24:996–1002
17. Johnson WE, Patterson AM, Eisenstein SM, Roberts S (2007) The presence of pleiotrophin in the human interverte-bral disc is associated with increased vascularization: an immunohistologic study. Spine 32:1295–1302
18. Johnson WE, Caterson B, Eisenstein SM, Hynds DL, Snow DM, Roberts S (2002) Human intervertebral disc aggrecan inhibits nerve growth in vitro. Arthritis Rheum 46: 2658–2664
19. Kang JD, Georgescu HI, McIntyre-Larkin L, Stefanovic-Racic M, Donaldson WF 3rd, Evans CH (1996) Herniated lumbar intervertebral discs spontaneously produce matrix metalloproteinases, nitric oxide, interleukin-6, and prosta-glandin E2. Spine 21:271–277
20. Kasra M, Merryman WD, Loveless KN, Goel VK, Martin JD, Buckwalter JA (2006) Frequency response of pig inter-
vertebral disc cells subjected to dynamic hydrostatic pres-sure. J Orthop Res 24:1967–1973
21. Kato T, Haro H, Komori H, Shinomiya K (2004) Sequential dynamics of inflammatory cytokine, angiogenesis inducing factor and matrix degrading enzymes during spontaneous resorption of the herniated disc. J Orthop Res 22:895–900
22. Kozaci LD, Guner A, Oktay G, Guner G (2005) Alterations in biochemical components of extracellular matrix in inter-vertebral disc herniation: role of MMP-2 and TIMP-2 in type II collagen loss. Cell Biochem Funct 24:431–436
23. Kroeber MW, Unglaub F, Wang H, Schmid C, Thomsen M, Nerlich A, Richter W (2002) New in vivo animal model to create intervertebral disc degeneration and to investigate the effects of therapeutic strategies to stimulate disc regenera-tion. Spine 27:2684–2690
24. Le Maitre CL, Freemont AJ, Hoyland JA (2006) Human disc degeneration is associated with increased MMP 7 expres-sion. Biotech Histochem 81:125–131
25. Lotz JC, Chin JR (2000) Intervertebral disc cell death is dependent on the magnitude and duration of spinal loading. Spine 25:1477–1483
26. Lotz JC, Colliou OK, Chin JR, Duncan NA, Liebenberg E (1998) Compression-induced degeneration of the interverte-bral disc: an in vivo mouse model and finite-element study. Spine 23:2493–2506
27. MacGregor AJ, Andrew T, Sambrook PN, Spector TD (2004) Structural, psychological, and genetic influences on low back and neck pain: a study of adult female twins. Arthritis Rheum 51:160–167
28. Maniadakis N, Gray A (2000) The economic burden of back pain in the UK. Pain 84:95–103
29. Neidlinger-Wilke C, Wurtz K, Liedert A, Schmidt C, Borm W, Ignatius A, Wilke HJ, Claes L (2005) A three-dimen-sional collagen matrix as a suitable culture system for the comparison of cyclic strain and hydrostatic pressure effects on intervertebral disc cells. J Neurosurg Spine 2:457–465
30. Neidlinger-Wilke C, Wurtz K, Urban JP, Borm W, Arand M, Ignatius A, Wilke HJ, Claes LE (2006) Regulation of gene expression in intervertebral disc cells by low and high hydro-static pressure. Eur Spine J 15:372–378
31. Ohshima H, Urban JP (1992) The effect of lactate and pH on proteoglycan and protein synthesis rates in the intervertebral disc. Spine 17:1079–1082
32. Osti OL, Vernon-Roberts B, Moore R, Fraser RD (1992) Annular tears and disc degeneration in the lumbar spine. A post-mortem study of 135 discs. J Bone Joint Surg Br 74: 678–682
33. Paesold G, Nerlich AG, Boos N (2007) Biological treatment strategies for disc degeneration: potentials and shortcom-ings. Eur Spine J 16:447–468
34. Peng B, Hao J, Hou S, Wu W, Jiang D, Fu X, Yang Y (2006) Possible pathogenesis of painful intervertebral disc degen-eration. Spine 31:560–566
35. Podichetty VK (2007) The aging spine: the role of inflam-matory mediators in intervertebral disc degeneration. Cell Mol Biol (Noisy-le-Grand, France) 53:4–18
36. Puustjarvi K, Lammi M, Helminen H, Inkinen R, Tammi M (1994) Proteoglycans in the intervertebral disc of young dogs following strenuous running exercise. Connect Tissue Res 30:225–240

10 C. Neidlinger-Wilke and H.-J. Wilke
37. Rajasekaran S, Naresh-Babu J, Murugan S (2007) Review of postcontrast MRI studies on diffusion of human lumbar discs. J Magn Reson Imaging 25:410–418
38. Roberts S, Evans H, Trivedi J, Menage J (2006) Histology and pathology of the human intervertebral disc. J Bone Joint Surg Am 88(suppl 2):10–14
39. Roberts S, Evans EH, Kletsas D, Jaffray DC, Eisenstein SM (2006) Senescence in human intervertebral discs. Eur Spine J 15(suppl 3):S312–S316
40. Roberts S, Caterson B, Menage J, Evans EH, Jaffray DC, Eisenstein SM (2000) Matrix metalloproteinases and aggre-canase: their role in disorders of the human intervertebral disc. Spine 25:3005–3013
41. Sambrook PN, MacGregor AJ, Spector TD (1999) Genetic influences on cervical and lumbar disc degeneration: a mag-netic resonance imaging study in twins. Arthritis Rheum 42:366–372
42. Schmidt H, Heuer F, Wilke HJ (2008) Interaction between finite helical axes and facet joint forces under combined load-ing. Spine 33:2741–2748. doi:10.1097/BRS.0b013e31817c4319 00007632-200812010-00008 [pii]
43. Schmidt H, Kettler A, Rohlmann A, Claes L, Wilke HJ (2007) The risk of disc prolapses with complex loading in different degrees of disc degeneration – a finite element anal-ysis. Clin Biomech (Bristol, Avon) 22:988–998. DOI S0268-0033(07)00138-6 [pii] 10.1016/j.clinbiomech.2007.07.008
44. Seguin CA, Pilliar RM, Roughley PJ, Kandel RA (2005) Tumor necrosis factor-alpha modulates matrix production and catabolism in nucleus pulposus tissue. Spine 30:1940–1948
45. Seguin CA, Bojarski M, Pilliar RM, Roughley PJ, Kandel RA (2006) Differential regulation of matrix degrading
enzymes in a TNFalpha-induced model of nucleus pulposus tissue degeneration. Matrix Biol 25:409–418
46. Sivan S, Neidlinger-Wilke C, Wurtz K, Maroudas A, Urban JP (2006) Diurnal fluid expression and activity of interverte-bral disc cells. Biorheology 43:283–291
47. Stokes IA, Iatridis JC (2004) Mechanical conditions that accelerate intervertebral disc degeneration: overload versus immobilization. Spine 29:2724–2732
48. Urban JP (2002) The role of the physicochemical environ-ment in determining disc cell behaviour. Biochem Soc Trans 30:858–864
49. Urban JP, Roberts S (2003) Degeneration of the interverte-bral disc. Arthritis Res Ther 5:120–130
50. Urban JP, Winlove CP (2007) Pathophysiology of the inter-vertebral disc and the challenges for MRI. J Magn Reson Imaging 25:419–432
51. Urban JP, Smith S, Fairbank JC (2004) Nutrition of the inter-vertebral disc. Spine 29:2700–2709
52. Wilke HJ, Neef P, Caimi M, Hoogland T, Claes LE (1999) New in vivo measurements of pressures in the intervertebral disc in daily life. Spine 24:755–762
53. Wilke HJ, Rohlmann F, Neidlinger-Wilke C, Werner K, Claes L, Kettler A (2006) Validity and interobserver agree-ment of a new radiographic grading system for intervertebral disc degeneration: Part I. Lumbar spine. Eur Spine J 15:720–730
54. Wuertz K, Urban JP, Klasen J, Ignatius A, Wilke HJ, Claes L, Neidlinger-Wilke C (2007) Influence of extracellular osmolarity and mechanical stimulation on gene expres-sion of intervertebral disc cells. J Orthop Res 25: 1513–1522

11M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_1.2, © Springer-Verlag Berlin Heidelberg 2010
Introduction
Patients with low back pain constitute a common patient group and can be divided into the acute group where the pain may be severe but short standing, and the group where the pain continues for a longer time and often influences many aspects of life. Patients with persisting low back pain, lasting longer than 3 months, are usually referred to as chronic [4], but perhaps a bet-ter expression for the condition is long-lasting low back pain (LLBP). One reason for using long-lasting instead of chronic is that in low back pain, as in conditions known to follow the patient for the rest of his/her life, a well-defined test does not set a precise diagnosis (com-pare with classic chronic diseases such as diabetes, heart failure and rheumatoid arthritis). Patients with LLBP suffer from more or less well-defined conditions that involve different anatomical structures and path-ways in the pain system, and only 10–15% of patients with low back pain get a specific diagnosis [17].
There is a rapid ongoing development in surgical implants and surgical techniques, as well as suggested non-surgical treatment methods, for patients with low back pain. However, the lack of instruments to set a precise diagnose and/or identify the pain foci in many of these patients still remains. There are probably mul-tiple reasons for the somewhat slow development of diagnostics compared to the rapid development in the treatment area. One reason for this might be the anat-omy of the spinal structures with multiple flexible
parts; another, the complexity of the nervous system where pain may arise from a direct influence of the peripheral and/or central nervous system as well as the stimulation of nociceptors located in different spinal structures. Hence, the slow development of diagnostic tools may also be caused by the fact that research in the area of diagnostics for lumbar pain is not only difficult and time consuming, but also not economically sup-ported to the same extent as new treatment methods, where the economical potential can be defined more easily in a business perspective.
In this article possible pain sources for acute and chronic low back pain, as well as existing diagnostic tools to support or reject possible pain foci, are described. Further, the nervous system response and modulation mechanisms in response to long-standing pain, as well as psychological/personality factors influ-encing pain experiences, are discussed.
Intervertebral Discs
Intervertebral discs are today considered as the main pain foci in patients with long-standing or chronic low back pain. The disc is the largest mobile part of the three-joint system building a motion segment in the spine (one motion segment defined as two vertebrates with connecting disc and bilateral facet joints). The highest shear and fibre strains of the disc have been demonstrated to occur posterolaterally in response to combined movements [37]. It is, therefore, not surpris-ing that disc deterioration often is seen at the posterior part of the disc as a posterolateral or central disc her-niation, a disc bulging, or by an increased fluid content at the posterior border of the disc in MRI (high inten-sity zone, HIZ).
Low Back Pain: Where Does the Pain Come From?
Helena Brisby
H. Brisby Department of Orthopaedics, Sahlgrenska University Hospital, 413 45, Gothenburg, Sweden e-mail: [email protected]
1.2

12 H. Brisby
Patients with disc herniations often report preced-ing low back pain before the onset of sciatic pain. This pain experience is suggested to be caused by stimula-tion of nerve endings in the annulus fibrosus due to the annular tear.
In parallel with investigations on mechanical prob-lems in the spine, different inflammatory and sig-nalling substances have been suggested to be of importance in the development and persistence of back pain. A number of experimental studies have demonstrated negative effects of disc tissue, and in particular, nucleus pulposus (NP) on nerve roots. NP can reduce spinal nerve root conduction velocity [32], induce nerve fibre degeneration, increase nerve fibre discharges [40], attract inflammatory cells [31] and induce increased intraneural capillary permeability [12]. Pro-inflammatory factors, which include cytok-ines (e.g. TNF and various interleukins), have been demonstrated to be present in disc herniation tissue [2]. High levels of pro-inflammatory mediators (IL-6 and IL-8) have also been found in disc tissue from patients considered to have discogenic low back pain undergoing fusion surgery [11].
In non-degenerated discs the presence of nerve fibres are detected in the absolute outer layers of the annulus fibrosus [33, 36]. These nerve fibres have been demon-strated to be both substance P-, calcitonin-gene-related peptide- (CGRP-) and vasoactive intestinal polypep-tide- (VIP)- immunoreactive [25]. Nerve impulses sig-nalling sensory information from the intervertebral disc have in animal studies been demonstrated to be con-ducted through the sinuvertebral nerve into rami com-municantes to sensory neurons in more cranially located dorsal root ganglia.
In degenerated discs nerve endings have been found to extend into deeper layers of the annulus fibrosus [15, 27] and even into the NP [34]. The nerve fibres have been detected both in the anterior and the poste-rior parts of disc specimens following vascularized granulation tissue [25, 34]. The stimulation of these nerve endings may correlate with the dull chronic ache, exacerbated by the mechanical load of the spine, that is experienced by chronic low back pain patients and is often referred to as discogenic pain.
The main diagnostic tool today to detect disc degen-eration is magnetic resonance imaging (MRI) where a number of signs as a decrease in water content, decreased disc height, disc bulging and/or indirect signs as vertebrae oedema can be detected. However,
disc degeneration changes seen by MRI investigations can also be seen at high frequency in asymptomatic individuals [6, 7, 21].
Another tool that is widely used and debated is dis-cography. The mechanism of discography involves the theory of increasing the intradiscal pressure for stimu-lation of mechanical nociceptors in the annulus fibro-sus. Based on this assumption, discography has been suggested to be a tool for evaluating pain characteris-tics and the precise level of pain generation. However, concordant pain during a discography is not always combined with a fissured and ruptured disc on discog-raphy/CT discography [28] and discography has not conclusively been demonstrated to be helpful to increase the result of spinal fusions in chronic low back patients [13, 14].
Another way to use discography is to look at the decrease in pain after local anaesthetics are injected; however, studies in this field are not conclusive.
Facet Joints
In the normal capsule of the facet joint both sensory and autonomic nerve fibres have been detected, and thus, the facet joint capsule has a structural basis for pain perception [38]. As in all joints, osteoarthrosis of the facet joint may occur and is more common in patients with disc degeneration. An inflammatory reac-tion is common in joints with osteoarthrosis and may stimulate nociceptors. Also mechanosensors may be influenced if the joint destruction leads to changes in the mobility of the joint such as in degenerative spon-dylolisthesis. Facet joint injections are sometimes used in elderly patients with facet joint osteoarthrosis to decrease low back pain with a minimal procedure. Measurement of nitric oxide has been performed in other osteoarthritic joints such as the knee joint and temporomandibular joint, and a relationship between NO and osteoarthrosis, as well as pain, has been observed [23, 39]. Recently, increased concentration of NO in, or in close relation to, the facet joints was also demonstrated in patients with facet joint osteoar-thritis and low back pain [8].
If measurement of inflammatory markers or pain markers can be used as diagnostic tools to diagnose pain originating from the facet joints or some other part of a painful spinal segment is not yet clear.

131.2 Low Back Pain: Where Does the Pain Come From?
Muscles
Most muscles are well innervated and changes in their normal function may contribute to the pain experience both in acute and long-standing low back pain.
In acute low back pain the muscle spasm is often extensive and has been suggested to be the main reason for the, often quite severe, pain that may hold back these patients from almost all movements the first day(s). However, if the muscle response in acute low back pain is a primary or a secondary event remains unclear.
The activation patterns for the trunk muscles (both abdominal and lumbar) have been demonstrated to be changed in patients with chronic low back pain in both experimental and clinical studies [16, 22]. If this, in concordance with the spasm in acute pain, is a response aiming to stabilize a degenerated spinal segment by decreasing movement and pain (pain- adaptation model) or if the changed muscle function contributes to the pain (pain-spasm-pain model) is, however, unclear [41].
Ligaments
Nerve fibres have been detected in the posterior- longitudinal ligament (PLL) [25], but not in some of the other ligaments such as the ligamentum flavum. The disc and the PLL have a close anatomical relation-ship, and it is reasonable to believe that a gradual loss of disc height causing bulging of the posterior part of the disc will influence the PLL and thus initiate stimu-lation of nociceptors in the PLL. This may be caused by stretching or by chemical factors released from the disc. However, little is known of the role of PLL and other ligaments in pain signalling and no diagnostic tools to look at these structures in vivo in regard to pain signalling exist.
Vertebraes
Nociceptors have been demonstrated to be present in bone structures also. Compression fractures in the spine are a common cause of pain in the spine in older and/or osteoporotic patients. These can occur without
trauma and can be visualized with x-ray, CT or MR scans.
In patients with low back pain and disc degeneration, changes in the vertebrae are also often noticed in MRI. Signal changes in the bone marrow of the vertebral body adjacent to a degenerated disc are called Modic changes and are suggested to be oedema caused by micro fractures or inflammatory changes [3]. Exactly how this influence nociceptors is unclear; however, some correlations between Modic changes and pain symptoms have been described [24, 26].
Nervous System Involvement and Adaptation
Free nerve endings present in various spine struc-tures respond to mechanical pressure/deformation and chemical stimuli just as in other organs. The pain impulses are conducted through myelinated A delta and unmyelinated C fibres to the dorsal root ganglion and continues via the spinothalamic tract to the thal-amus and gives rise to the pain experience when reaching the somatosensory cortex.
Inflammatory substances from a deteriorated disc or from facet joint arthrosis may influence nerve roots and DRG, as well as nociceptors in different surround-ing structures. Biochemical and mechanical factors may also act together to increase direct negative effects on nerve roots. Nerve tissue damage may also by itself increase inflammation by stimulation of macrophage infiltration and increasing the number of activated T cells, which may add to the pain [1, 29]. Several bio-markers associated to pain and/or neurotransmission have been studied in CSF and serum in patients with chronic low back pain and also in patients with sciatica [5, 9, 10, 18]. However, no clear diagnostic help has been demonstrated by the use of biomarkers in patients with low back pain.
When handling pain patients, one always has to bear in mind that pain perception is a subjective expe-rience. The function of pain perception is primarily the detection of tissue damage, a mechanism extremely important for the survival of the individual, but may also cause major clinical problems. In response to stimulation of free nerve endings, the somatosen-sory system may increase its sensitivity resulting in a

14 H. Brisby
non-functional way to respond – normally innocuous stimuli result in an amplified response (peripheral sensitization).
Pain impulses may also be modulated at higher cen-tres, both at the spinal and the supraspinal level (cen-tral hyperexcitibiability). The first possible level for impulse modulation is the DRG. The changed magni-tude of perceived pain is often referred to as neural plasticity and is considered to play a critical role in the evolution of chronic pain.
Upregulation of chemokines within the nervous system, which can be released by astrocytes or micro-glia, may also contribute to pain modulation and the development of chronic pain [1]. Augmented central pain processing has been demonstrated in chronic low back pain patients with fMRI [19]. Hyperalgesia and increased neural activity measured by fMRI after thumbnail pressure were seen in this patient group when compared to controls. Chronic low back pain patients have also been demonstrated to have brain chemistry alterations demonstrated by proton mag-netic resonance spectroscopy. A reduction of N-acetyl aspartate and glucose has been found in dorsolateral prefrontal cortex in these patients [20].
The way people “think” about chronic low back pain has also been suggested to influence move-ments, and it has been demonstrated that pain physi-ology education can markedly alter brain activity, registered by fMRI, during performance of a specific task [30].
The Psychosocial Aspects of Chronic Pain
Since pain is a subjective experience, it can, as with most experiences, be affected by psychosocial fac-tors. Low back pain patients with certain psycholog-ical characteristics such as pain-related anxiety and low acceptance of pain have been demonstrated to be less sensitive to treatment [35]. On the other hand, long-standing severe pain may also affect a person psychologically and it is, therefore, difficult to ascer-tain the role psychological factors play in the devel-opment of chronic pain. However, most authors agree that psychosocial factors contribute to the indi-vidual perception of long-standing pain and coping with it.
Summary
In summary, many structures in the spine can theoreti-cally contribute to acute low back pain as well as long-standing low back pain. The intervertebral disc, the facet joints and the muscle are the most likely local actors for initiation and maintenance of low back pain (both acute and long-standing).
There are mechanical as well as biological ratio-nales behind the theory that the disc is a tissue of major interest in low back pain. However, when it comes to diagnostics, investigations/test(s) to detect disc degen-eration do exist, but are still inconclusive in pointing out a certain disc as the pain foci. As for the facet joints, ligaments and the vertebras, still less is known regarding their role in low back pain patients. In patients with low back pain, changed activity of the muscles localized around the spine is common; how-ever, whether this is a secondary response or not is less clear. When the complexity of the nervous system and psychological factors is added, the need for more research and better diagnostic tools in this patient group becomes obvious.
References
1. Abbadie C (2005) Chemokines, chemokine receptors and pain. Trends Immunol 26:529–534
2. Ahn SH, Cho YW, Ahn MW et al (2002) mRNA expression of cytokines and chemokines in herniated lumbar interverte-bral discs. Spine 27:911–917
3. Albert HB, Kjaer P, Jensen TS et al (2008) Modic changes, possible causes and relation to low back pain. Med Hypotheses 70:361–368
4. Allan DB, Waddell G (1989) An historical perspective on low back pain and disability. Acta Orthop Scand Suppl 234:1–23
5. Balague F, Nordin M, Schafer D et al (2006) The potential value of blood biomarkers of intervertebral disk metabolism in the follow-up of patients with sciatica. Eur Spine J 15:627–633
6. Boden SD, Davis DO, Dina TS et al (1990) Abnormal magnetic-resonance scans of the lumbar spine in asymptom-atic subjects. A prospective investigation. J Bone Joint Surg Am 72:403–408
7. Borenstein DG, O’Mara JW Jr, Boden SD et al (2001) The value of magnetic resonance imaging of the lumbar spine to predict low-back pain in asymptomatic subjects: a seven-year follow-up study. J Bone Joint Surg Am 83-A:1306–1311
8. Brisby H, Ashley H, Diwan AD (2007) In vivo measurement of facet joint nitric oxide in patients with chronic low back pain. Spine 32:1488–1492

151.2 Low Back Pain: Where Does the Pain Come From?
9. Brisby H, Olmarker K, Larsson K et al (2002) Proinflammatory cytokines in cerebrospinal fluid and serum in patients with disc herniation and sciatica. Eur Spine J 11:62–66
10. Brisby H, Olmarker K, Rosengren L et al (1999) Markers of nerve tissue injury in the cerebrospinal fluid in patients with lumbar disc herniation and sciatica. Spine 24:742–746
11. Burke JG, GW RW, Conhyea D et al (2003) Human nucleus pulposis can respond to a pro-inflammatory stimulus. Spine 28:2685–2693
12. Byrod G, Otani K, Brisby H et al (2000) Methylprednisolone reduces the early vascular permeability increase in spinal nerve roots induced by epidural nucleus pulposus applica-tion. J Orthop Res 18:983–987
13. Carragee EJ, Lincoln T, Parmar VS et al (2006) A gold stan-dard evaluation of the “discogenic pain” diagnosis as deter-mined by provocative discography. Spine 31:2115–2123
14. Cohen SP, Hurley RW (2007) The ability of diagnostic spi-nal injections to predict surgical outcomes. Anesth Analg 105:1756-1775, table of contents
15. Coppes MH, Marani E, Thomeer RT et al (1997) Innervation of “painful” lumbar discs. Spine 22:2342–2349; discussion 2349–2350
16. Dankaerts W, O’Sullivan P, Burnett A et al (2006) Altered patterns of superficial trunk muscle activation during sitting in nonspecific chronic low back pain patients: importance of subclassification. Spine 31:2017–2023
17. Deyo RA, Weinstein JN (2001) Low back pain. N Engl J Med 344:363–370
18. Gebhardt K, Brenner H, Sturmer T et al (2006) The course of high-sensitive C-reactive protein in correlation with pain and clinical function in patients with acute lumbosciatic pain and chronic low back pain – a 6 months prospective longitu-dinal study. Eur J Pain 10:711–719
19. Giesecke T, Gracely RH, Grant MA et al (2004) Evidence of augmented central pain processing in idiopathic chronic low back pain. Arthritis Rheum 50:613–623
20. Grachev ID, Fredrickson BE, Apkarian AV (2002) Brain chemistry reflects dual states of pain and anxiety in chronic low back pain. J Neural Transm 109:1309–1334
21. Jensen MC, Brant-Zawadzki MN, Obuchowski N et al (1994) Magnetic resonance imaging of the lumbar spine in people without back pain. N Engl J Med 331:69–73
22. Kaigle AM, Wessberg P, Hansson TH (1998) Muscular and kinematic behavior of the lumbar spine during flexion-extension. J Spinal Disord 11:163–174
23. Karan A, Karan MA, Vural P et al (2003) Synovial fluid nitric oxide levels in patients with knee osteoarthritis. Clin Rheumatol 22:397–399
24. Kjaer P, Korsholm L, Bendix T et al (2006) Modic changes and their associations with clinical findings. Eur Spine J 15:1312–1319
25. Konttinen YT, Gronblad M, Antti-Poika I et al (1990) Neuroimmunohistochemical analysis of peridiscal nocicep-tive neural elements. Spine 15:383–386
26. Kuisma M, Karppinen J, Niinimaki J et al (2007) Modic changes in endplates of lumbar vertebral bodies: prevalence and association with low back and sciatic pain among middle-aged male workers. Spine 32:1116–1122
27. Le Maitre CL, Hoyland JA, Freemont AJ (2007) Interleukin-1 receptor antagonist delivered directly and by gene therapy inhibits matrix degradation in the intact degenerate human intervertebral disc: an in situ zymographic and gene therapy study. Arthritis Res Ther 9:R83
28. Lim CH, Jee WH, Son BC et al (2005) Discogenic lumbar pain: association with MR imaging and CT discography. Eur J Radiol 54:431–437
29. Moalem G, Tracey DJ (2006) Immune and inflammatory mechanisms in neuropathic pain. Brain Res Rev 51:240–264
30. Moseley GL (2005) Widespread brain activity during an abdominal task markedly reduced after pain physiology edu-cation: fMRI evaluation of a single patient with chronic low back pain. Aust J Physiother 51:49–52
31. Olmarker K, Blomquist J, Stromberg J et al (1995) Inflam-matogenic properties of nucleus pulposus. Spine 20:665–669
32. Olmarker K, Rydevik B, Nordborg C (1993) Autologous nucleus pulposus induces neurophysiologic and histologic changes in porcine cauda equina nerve roots. Spine 18:1425–1432
33. Palmgren T, Gronblad M, Virri J et al (1999) An immunohis-tochemical study of nerve structures in the anulus fibrosus of human normal lumbar intervertebral discs. Spine 24: 2075–2079
34. Peng B, Wu W, Hou S et al (2005) The pathogenesis of dis-cogenic low back pain. J Bone Joint Surg Br 87:62–67
35. Riipinen M, Niemisto L, Lindgren KA et al (2005) Psycho-social differences as predictors for recovery from chronic low back pain following manipulation, stabilizing exercises and physician consultation or physician consultation alone. J Rehabil Med 37:152–158
36. Roberts S, Eisenstein SM, Menage J et al (1995) Mechano-receptors in intervertebral discs. Morphology, distribution, and neuropeptides. Spine 20:2645–2651
37. Schmidt H, Kettler A, Heuer F et al (2007) Intradiscal pres-sure, shear strain, and fiber strain in the intervertebral disc under combined loading. Spine 32:748–755
38. Sommer C, Lindenlaub T, Teuteberg P et al (2001) Anti-TNF-neutralizing antibodies reduce pain-related behavior in two different mouse models of painful mononeuropathy. Brain Res 913:86–89
39. Suenaga S, Abeyama K, Hamasaki A et al (2001) Tempo-romandibular disorders: relationship between joint pain and effusion and nitric oxide concentration in the joint fluid. Dentomaxillofac Radiol 30:214–218
40. Takebayashi T, Cavanaugh JM, Cuneyt Ozaktay A et al (2001) Effect of nucleus pulposus on the neural activity of dorsal root ganglion. Spine 26:940–945
41. van Dieen JH, Selen LP, Cholewicki J (2003) Trunk muscle activation in low-back pain patients, an analysis of the litera-ture. J Electromyogr Kinesiol 13:333–351

17M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_1.3, © Springer-Verlag Berlin Heidelberg 2010
Introduction
The intervertebral disc has traditionally been regarded as a biomechanically important structure in the spine, with characteristic biomechanical properties related to both the annulus fibrosus and the nucleus pulposus. However, research performed during the last 15 years has revealed that the intervertebral disc is also biologi-cally active, and the disc cells have been demonstrated to produce different pro-inflammatory cytokines, for example, TNF and various interleukins [7, 18, 22, 24]. These different factors have been shown, in a number of studies, to play important roles in the pathophysiol-ogy of disc degeneration and disc herniation. This chapter provides an overview of the role of cytokines in degenerative disorders of the spine.
Cytokines
Cytokines constitute a group of small trophic regulatory proteins and can be divided into, for example, growth factors, interleukins and interferones. Cytokines are produced by a large number of different cells through-out the body and participate in inflammatory responses, but also take part in other processes such as immuno-reactions, pain regulation and hematopoesis [37].
Cytokines act by binding to specific membrane receptors and influence cells in their close surrounding also at low concentrations. The increased expression
of one cytokine often initiates a cascade of other cytok-ines, which may lead to synergistic effects, for exam-ple, an active inflammatory reaction. Some cytokines, however, may also act as antagonists and have, e.g. anti-inflammatory effects. The actions of cytokines are also often closely related to other inflammatory sub-stances, for example, nitric oxide (NO).
One of the most well-known pro-inflammatory cytokines is tumour necrosis factor alpha (TNF-alpha), often referred to nowadays as just Tumour Necrosis Factor, TNF. TNF has been demonstrated to play a major role in severe inflammatory events such as sep-sis and joint destruction in rheumatoid arthritis patients [12–14, 25, 37].
TNF and Disc Herniation
The observations by Mixter and Barr in 1934 indicated that sciatica due to lumbar disc herniation was mainly a mechanical problem related to compression of the nerve root by the herniated part of the disc [23]. However, during the last 15 years an alternative concept has grad-ually evolved pointing out that biological factors related to various components of the intervertebral disc also are of major importance in the pathophysiology of sci-atic pain [27]. Olmarker and co-workers demonstrated for the first time that autologous nucleus pulposus in a pig model can induce structural nerve fibre damage as well as decreased spinal nerve conduction velocity [30]. In that study the effects of autologous nucleus pulposus were compared to the effects of autologous retroperitoneal fat in a blinded experimental set-up. These original observations have subsequently been reproduced by other non-related research groups [2, 14, 17, 34]. A series of experimental investigations
The Role of Cytokines in the Degenerative Spine
Björn Rydevik and Helena Brisby
B. Rydevik (*) Department of Orthopaedics, Sahlgrenska University Hospital, 413 45, Gothenburg, Sweden e-mail: [email protected]
1.3

18 B. Rydevik and H. Brisby
have shown that TNF seems to be an important compo-nent of the nucleus pulposus in causing the nerve root irritation which renders the nerve root sensitive to mechanic compression, leading to nerve root pain [26, 29, 31]. These pronounced biologic effects of nucleus pulposus are related to the cells of the nucleus pulpo-sus [20]. Local application of exogenous TNF on nerve roots mimics nucleus pulposus induced nerve injury [17]. In a series of investigations it has also been dem-onstrated that local application of nucleus pulposus or constriction of nerve roots, together with experimental treatment of the animal with anti-TNF substances such as etanercept (a soluble receptor) of infliximab (a chi-meric monoclonal antibody), can prevent the nerve root injury effects [29, 32, 39]. Moreover, it has been shown that local application of autologous nucleus pulposus on spinal nerve roots in rats can induce pain behavioural changes and that such pain behavioural changes can be prevented by anti-TNF treatment [28]. Further, in a neurophysiological experimental set-up, nucleus pulposus application onto the dorsal root gan-glion has been demonstrated to increase afferent fibre evoked responses in the thalamus within a few min-utes, suggesting that nucleus pulposus itself can affect sensory transmitting pathways [5].
Other Cytokines and Disc Herniation
In a disc herniation rabbit model, intervertebral disc cells in the created disc herniation have been demon-strated to produce not only tumour necrosis factor, but interleukin-1beta as well, at day 1 after the disc injury [38]. mRNA expressions of different cytokines have also been investigated in human herniated disc speci-mens from patients undergoing surgery [1]. IL-8, TNF-alpha, TGF-beta and IL-1alpha were the most frequently expressed cytokines of those investigated in this study, and were found in 70%, 65%, 50% and 39%, respectively, of the specimens. IL-8 mRNA expression was associated with short symptom dura-tion (average 3.8 weeks) and also associated with provocation of the radiating pain by back extension. The expression of IL-1alpha was found more fre-quently in transligamentous herniations than in sub-ligamentous herniations.
Further, patients with lumbar disc herniation and sciatica of short duration have been shown to have
increased concentration of IL-8 in the cerebrospinal fluid [3, 6]. These findings support the concept that several inflammatory substances are involved when a disc herniation occurs (see Fig. 1.3.1).
Cytokines and Intervertebral Disc and Facet Joint Degeneration
The cells of the intervertebral disc are biologically active, as well as responsive, and increase their pro-duction of interleukin-6, prostaglandin E2 and matrix metalloproteinases when stimulated with interleu-kin-1 [22]. These findings are of particular interest in view of the increased levels of interleukin-1 found in degenerated intervertebral discs [22]. Disc specimens from patients with discogenic low back pain have fur-ther been shown to express increased levels of inter-leukin-6, interleukin-8 and TNF compared to controls [7, 36]. Recently the concentration of TNF in blood samples also was demonstrated to be increased in patients with chronic low back pain compared to con-trols [35].
Regarding facet joints it has been shown in a rat model that experimentally induced lumbar facet joint inflammation causes mechanical allodynia in the ipsilateral limb and that the number of TNF-alpha
Cytokines
Nerve rootdysfunction
Ab
Pain
NPcell
Compression
CSF
serum TNF
IL-8Macrophages
Fig. 1.3.1 Schematic presentation of various events regarding nerve root involvement in conjunction with disc herniation. Nerve root compression and application of nucleus pulposus cause nerve root dysfunction and pain (sciatica). There is evi-dence for involvement of inflammatory components and activa-tion of the immune system in this process. Biomarkers for inflammation, e.g. IL-8 in CSF and TNF in serum, can be detected. Adapted from Brisby 2000 [3]

191.3 The Role of Cytokines in the Degenerative Spine
immunoreactive cells in the epidural space was significantly increased compared to controls [33]. Clinical studies have shown increased levels of interleukin-1b in human facet joint tissue from patients undergoing surgery for lumbar spinal steno-sis and disc herniation [16]. These studies also dem-onstrated that the concentrations of interleukin-1b correlated with leg pain, and the authors suggested that interleukin-1b may leak from facet joints to the nerve roots, and thus induce radiating sciatic pain. Another inflammatory substance that is closely related to the presence of cytokines, NO, has recently been demonstrated to be elevated in facet joints in patients with chronic low back pain and facet joint arthrosis when compared to healthy controls [4]. Interestingly, chronic low back pain patients who responded to facet corticosteroid injection with a temporary pain reduction, had higher concentrations of NO in their facet joints than patients who did not respond positively.
Clinical Studies on Anti-TNF Treatment for Disc Herniation Induced Sciatica
Based on the basic science research studies regarding the pathophysiology of sciatic pain related to cytokine activation, for example, TNF, clinical research has been conducted investigating these novel therapeutic strategies. The first study to evaluate the use of Infliximab (a TNF-alpha monoclonal antibody) to treat sciatica was published by Karppinen et al. in 2003 [19]. In this study the authors evaluated the effects in 10 patients with severe sciatic pain due to lumbar disc herniation, confirmed by MRI, who were on the waiting list for surgical treatment of the disc herniation. The results were compared to historical controls and comprised 62 patients who received saline in a randomized controlled trial of periradicu-lar infiltration for sciatica. In this study, Karppinen and co-workers showed a statistically significant improvement of leg pain as well as significantly decreased disability up to 12 weeks after treatment. Furthermore, they showed that in the study group there were significantly more patients who were pain free, defined as more than 75% decrease of leg pain from baseline, compared to the controls. Also at four weeks, all of the four patients who were off work in
the treated group had returned to work, while in the control group about 40% of the patients were still off work. Genevay and co-workers evaluated the efficacy of etanercept in the treatment of acute severe sciatica in a pilot study in which ten patients received three subcutaneous injections of etanercept (25 mg) every three days [11]. The results were compared to ten historical control patients who received intravenous methylprednisolone for treatment of the same condi-tion. Visual Analogue Scale for leg pain and back pain was evaluated at ten days and 6 weeks. The authors conclude that leg and back pain decrease sig-nificantly more with anti-TNF treatment than with intravenous cortisone. Korhonen et al. performed a randomized controlled trial with 1-year follow-up of the treatment effects using infliximab for manage-ment of disc herniation induced sciatica [21]. In this study no positive effect was seen when comparing the two groups. However, the authors concluded that “Although the long-term results of this randomized trial do not support the use of infliximab compared to placebo for lumbar radicular pain in patients with disc herniation induced sciatica, further study in a sub-group of patients appears to be warranted”. In particular, the authors noted that at 2 weeks, 33% of the infliximab treated patients reported more than 75% reduction in leg pain by VAS, while only 17% of the control patients reported such reduction in leg pain. Thus, initial clinical studies indicate a possible role of anti-TNF treatment in disc herniation, but clinical studies have provided contradictory results. A recent study by Cohen and co-workers [9] evalutated the effects of epidural etanercept for the treatment of sciatica in a RCT in 24 patients. The study showed positive results of epidural etanercept over a 6 month follow-up period as compared to placebo control (saline).
Cytokines and Spine Surgery
It has been shown that patients undergoing micro endo-scopic surgery for lumbar disc herniation had less sys-temic cytokine response as compared to patients who underwent open discectomy [8, 15]. Serum levels of TNF-alpha, IL-1beta, IL-6, IL-8 and CRP were mea-sured before surgery and up to 24 h post-operatively

20 B. Rydevik and H. Brisby
[15]. Serum IL-6 and CRP increased less significantly following microendoscopic surgery than after open discectomy. The authors conclude that microsurgical approaches are less traumatic to the patients than open discectomy. However, both surgical techniques lead to good clinical results.
Conclusions
Experimental and clinical research performed mainly during the last 15 years has provided evidence that cytokines such as TNF and interleukins are involved in the pathophysiology of various spinal pain conditions and that these substances may also be activated by spi-nal surgery. Moreover, a research-based concept that the intervertebral disc is biologically active and not merely a biomechanically important structure in the spine has gradually evolved during the same period of time. These developments may lead to a better understand-ing of back pain pathogenesis as well as provide a plat-form for the development of novel treatment approaches for certain subgroups of patients with back pain.
Acknowledgements This review is partly based on research supported by the Swedish Research Council, Project number K2008-53X-20627-01-3, and Marianne and Marcus Wallenberg’s Foundation.
References
1. Ahn SH, Cho YW, Ahn MW et al (2002) mRNA expression of cytokines and chemokines in herniated lumbar interverte-bral discs. Spine 27:911–917
2. Anzai H, Hamba M, Onda A et al (2002) Epidural applica-tion of nucleus pulposus enhances nociresponses of rat dor-sal horn neurons. Spine 27:E50–E55
3. Brisby H (2000) Nerve tissue injury markers, inflammatory mechanisms and immunologic factors in lumbar disc hernia-tion. Clinical and experimental studies: Thesis, Gothenburg University; ISBN 91-628-4380-X
4. Brisby H, Ashley H, Diwan AD (2007) In vivo measurement of facet joint nitric oxide in patients with chronic low back pain. Spine 32:1488–1492
5. Brisby H, Hammar I (2007) Thalamic activation in a disc herniation model. Spine 32:2846–2852
6. Brisby H, Olmarker K, Larsson K et al (2002) Proinflammatory cytokines in cerebrospinal fluid and serum in patients with disc herniation and sciatica. Eur Spine J 11:62–66
7. Burke JG, GW RW, Conhyea D et al (2003) Human nucleus pulposus can respond to a pro-inflammatory stimulus. Spine 28:2685–2693
8. Chao Z, Yue Z, Tong-wei C et al (2007) Microendoscopic discectomy, a less traumatic procedure for lumbar disk her-niation. Chin J Traumatol 10:311–314
9. Cohen SP, Bogduk N, Dragovic A et al (2009) Randomized, double-blind, placebo-controlled dose-response, and pre-clinical safety study of transforaminal etanercept for the treatment of sciatica. Anaesthesiology 110(5):1116–1126
10. Cuellar JM, Montesano PX, Antognini JF et al (2005) Application of nucleus pulposus to L5 dorsal root ganglion in rats enhances nociceptive dorsal horn neuronal windup. J Neurophysiol 94:35–48
11. Genevay S, Guerne PA, Gabay C (2004) Efficacy of tumor necrosis factor-alpha blockade for severe sciatica? Rev Med Suisse Romande 124:543–545
12. Goldring SR (2002) Bone and joint destruction in rheuma-toid arthritis: what is really happening? J Rheumatol Suppl 65:44–48
13. Hehlgans T, Pfeffer K (2005) The intriguing biology of the tumour necrosis factor/tumour necrosis factor receptor super-family: players, rules and the games. Immunology 115:1–20
14. Hotchkiss RS, Karl IE (2003) The pathophysiology and treatment of sepsis. N Engl J Med 348:138–150
15. Huang TJ, Hsu RW, Li YY et al (2005) Less systemic cytokine response in patients following microendoscopic versus open lumbar discectomy. J Orthop Res 23:406–411
16. Igarashi A, Kikuchi S, Konno S (2007) Correlation between inflammatory cytokines released from the lumbar facet joint tissue and symptoms in degenerative lumbar spinal disor-ders. J Orthop Sci 12:154–160
17. Igarashi T, Kikuchi S, Shubayev V et al (2000) 2000 Volvo Award winner in basic science studies: Exogenous tumor necrosis factor-alpha mimics nucleus pulposus-induced neu-ropathology. Molecular, histologic, and behavioral compari-sons in rats. Spine 25:2975–2980
18. Kang JD, Georgescu HI, McIntyre-Larkin L et al (1996) Herniated lumbar intervertebral discs spontaneously pro-duce matrix metalloproteinases, nitric oxide, interleukin-6, and prostaglandin E2. Spine 21:271–277
19. Karppinen J, Korhonen T, Malmivaara A et al (2003) Tumor necrosis factor-alpha monoclonal antibody, infliximab, used to manage severe sciatica. Spine 28:750–753; discussion 753–754
20. Kayama S, Olmarker K, Larsson K et al (1998) Cultured, autologous nucleus pulposus cells induce functional changes in spinal nerve roots. Spine 23:2155–2158
21. Korhonen T, Karppinen J, Paimela L et al (2005) The treat-ment of disc herniation-induced sciatica with infliximab: results of a randomized, controlled, 3-month follow-up study. Spine 30:2724–2728
22. Le Maitre CL, Hoyland JA, Freemont AJ (2007) Interleukin-1 receptor antagonist delivered directly and by gene therapy inhibits matrix degradation in the intact degenerate human intervertebral disc: an in situ zymographic and gene therapy study. Arthritis Res Ther 9:R83
23. BJ MWJ (1934) Rupture of the intervertebral disc with involve-ment of the spinal canal. New Engl J Med 211:210–215

211.3 The Role of Cytokines in the Degenerative Spine
24. Murata Y, Nannmark U, Rydevik B et al (2006) Nucleus pulposus-induced apoptosis in dorsal root ganglion follow-ing experimental disc herniation in rats. Spine 31:382–390
25. Okamoto H, Hoshi D, Kiire A et al (2008) Molecular targets of rheumatoid arthritis. Inflamm Allergy Drug Targets 7:53–66
26. Olmarker K, Larsson K (1998) Tumor necrosis factor alpha and nucleus-pulposus-induced nerve root injury. Spine 23: 2538–2544
27. Olmarker K, Myers R, Rydevik B et al (2004) Pathophysiology of nerve root pain in disc herniation and spinal stenosis. In: Wiesel SW et al (eds) The lumbar spine. Lippincott William and Wilkins, Philadelphia, pp 25-39
28. Olmarker K, Nutu M, Storkson R (2003) Changes in sponta-neous behavior in rats exposed to experimental disc hernia-tion are blocked by selective TNF-alpha inhibition. Spine 28:1635–1641; discussion 1642
29. Olmarker K, Rydevik B (2001) Selective inhibition of tumor necrosis factor-alpha prevents nucleus pulposus-induced thrombus formation, intraneural edema, and reduction of nerve conduction velocity: possible implications for future pharmacologic treatment strategies of sciatica. Spine 26: 863–869
30. Olmarker K, Rydevik B, Nordborg C (1993) Autologous nucleus pulposus induces neurophysiologic and histologic changes in porcine cauda equina nerve roots. Spine 18: 1425–1432
31. Park MS, Lee HM, Hahn SB et al (2007) The association of the activation-inducible tumor necrosis factor receptor and ligand with lumbar disc herniation. Yonsei Med J 48:839–846
32. Sommer C, Schafers M, Marziniak M et al (2001) Etanercept reduces hyperalgesia in experimental painful neuropathy. J Peripher Nerv Syst 6:67–72
33. Tachihara H, Kikuchi S, Konno S et al (2007) Does facet joint inflammation induce radiculopathy?: an investigation using a rat model of lumbar facet joint inflammation. Spine 32:406–412
34. Takebayashi T, Cavanaugh JM, Cuneyt Ozaktay A et al (2001) Effect of nucleus pulposus on the neural activity of dorsal root ganglion. Spine 26:940–945
35. Wang H, Schiltenwolf M, Buchner M (2008) The role of TNF-alpha in patients with chronic low back pain-a prospec-tive comparative longitudinal study. Clin J Pain 24:273–278
36. Weiler C, Nerlich AG, Bachmeier BE et al (2005) Expression and distribution of tumor necrosis factor alpha in human lumbar intervertebral discs: a study in surgical specimen and autopsy controls. Spine 30:44–53; discussion 54
37. Vilcek J (1998) The cytokines: an overview. In: Thomson A (ed) The cytokine handbook, 3rd edn, Chapter 1. Academic Press, San Deigo, pp 1–20
38. Yoshida M, Nakamura T, Sei A et al (2005) Intervertebral disc cells produce tumor necrosis factor alpha, interleukin-1beta, and monocyte chemoattractant protein-1 immediately after herniation: an experimental study using a new hernia model. Spine 30:55–61
39. Zanella JM, Burright EN, Hildebrand K et al (2008) Effect of etanercept, a tumor necrosis factor-alpha inhibitor, on neuropathic pain in the rat chronic constriction injury model. Spine 33:227–234

23M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_1.4, © Springer-Verlag Berlin Heidelberg 2010
Psychosocial factors have been largely investigated as outcome predictors of surgical interventions and numerous studies have examined the consequences of surgery on psychological variables. These issues have been explored in the context of various surgical proce-dures: e.g. the need to address the psychosocial profile of the candidates for fusion surgery; or the influence of psychosocial factors in the poor outcomes of lumbar discectomy when morphological problems have been adequately managed by surgery.
Psychological distress and depression; pain beliefs, expectations, pain behaviours, and coping strategies; and social factors are reviewed in this chapter with a focus on the role of these aspects in the outcomes of surgery.
Psychological Distress and Depression
Psychological distress and depression have received a considerable amount of attention. Results regarding the association between these factors and surgical outcomes are, however, not univocal. Various studies have pointed to the association between depression and poor outcomes of spine surgery (e.g. [30, 40]). A prospective study of psychological predictors of surgery outcome (mostly fusion) showed that lower levels of distress before sur-gery were associated with work resumption, improved back and leg pain, and functional gains in activities of
daily living at follow-up, 1 year after surgery [38]. Similarly, emotional health as assessed by the mental component score of the SF-36 was a significant predictor of pain and function outcomes up to 2 years after fusion surgery [39]. Depression was also found to be a signifi-cant predictor in terms of pain relief and function [20, 33], as well as of return to work after controlling for pre-operative pain and disability in patients undergoing lum-bar discectomy [33]. Depression was found to be a consistent predictor of the outcome of surgery as assessed by a composite core index measure for low back pain (LBP) [9] encompassing pain, back-specific function, generic health status, work disability and patient satisfac-tion [24]. Depression was also a highly influential comor-bidity in a large observational study exploring the influence of medical and psychosocial comorbidities on perceived health and disability in patients undergoing lumbar spine surgery [34].
A review of biopsychosocial risk factors for an unfavourable outcome after disc surgery found posi-tive evidence for anxiety and somatisation, but not for depression [7]. The report from the Swedish Lumbar Spine Study comparing the importance of predictors of functional and work status outcome in surgical and non-surgical treatment [16] did not evidence any sig-nificant association between depressive symptoms and surgical outcome. The results showed, however, that pre-treatment depressive symptoms predicted improve-ment in the non-surgical group. Besides, self-rated improvement was associated with a decrease of depres-sive symptoms in both groups. Similarly, pre-operative psychological distress was not a predictor of the func-tional status after surgical treatment in Tandon et al.’s study [36], but patients reporting improvement after surgery also showed reduced distress. It has been con-cluded that depressive symptoms or distress are no obvious contraindications to surgery [24].
Psychosocial Aspects of Low Back Pain
Christine Cedraschi and Valérie Piguet
C. Cedraschi (*) Division of Internal Medicine for Rehabilitation, Geneva University Hospitals, Rue Gabrielle Perret-Gentil 4, 1211 Geneva 14, Switzerland e-mail: [email protected]
1.4

24 C. Cedraschi and V. Piguet
The association between depression or psychologi-cal distress and surgical outcome is still an area open for debate. Many LBP patients do not suffer clinical depression and display self-denigratory views and feelings. Clinical depression should therefore be dis-tinguished from depressed mood, which may not fit into a psychopathological model.
Divergences in the results regarding the role of psy-chological distress and depression may be related to various factors such as the diagnosis, the time frame (acute or chronic pain) and also the duration of pain before the intervention with treatment delays increas-ing the likelihood of poor functional outcome. Data from the literature point to the importance of the abil-ity to rapidly relieve pain which may limit the adverse effects of psychological distress: indeed, no corre-lation was found between emotional distress, even severe, and poor surgical outcomes in patients suffer-ing acute and subacute sciatica from disc herniation undergoing early surgery [6]. In these patients with a very high chance of dramatic and lasting improvement after surgery, psychological screening failed to predict outcomes, whereas the same psychometric profile pre-dicted worse outcomes in patients with chronic sciatica pain and disability [6].
Beliefs, Behaviours, and Coping Strategies
Beliefs are assumptions about reality which serve as a lens through which events are interpreted. As such, they shape the individual’s understanding of his/her environ-ment [21]. Coping includes cognitive, but also behav-ioural aspects and has been defined as the individual’s endeavour to deal with external and/or internal demands that are appraised as taxing or exceeding the resources of the person [21]. Beliefs about pain, illness and treat-ment, and coping strategies exist before pain onset, but they are developed when back pain occurs and may be modified by pain persistence or recurrence.
Patients’ views and patient-oriented outcomes are increasingly acknowledged, including beliefs about pain and illness, and expectations of treatment. Patients’ expectations have been shown to influence treatment outcomes so that patients with higher expectations of surgery had better outcomes than those with lower expectations [18, 22]. High expectations for physical
function have been associated with improved function and satisfaction with physical function, but high expec-tations for pain relief have been associated with greater report of pain and decreased satisfaction with pain relief, suggesting that these expectations should be addressed differently in pre-operative discussions [18]. Similarly, positive expectations for return to work have been asso-ciated with higher post-surgical work resumption and increased physical function [32]. However, how far patient expectations predict or influence outcomes is not yet clear, and other data have shown that patients with very high, frequently unrealistic, expectations of recov-ery, particularly in terms of pain and function, reported less satisfactory outcomes of surgery [25].
Clinically, when it comes to allowing the patient to develop realistic expectations, it is important to pro-vide him/her with information about the treatment and its course, what can reasonably be expected in his/her case, as well as with advice and reassurance about resuming daily activities [26, 27].
Pain behaviours refer to physical or verbal attempts to communicate suffering and disability. In the acute stage, they can be seen as appropriate and adaptive in order to avoid further injury, whereas they have no therapeutic value in the chronic stage. Instead, they perpetuate the patient’s adoption of the sick role and are, therefore, maladaptive. The Swedish Lumbar Spine Study showed no association between pain behaviours and patient global assessment of treatment effects or work status after surgery [16]. Contradictory findings have been reported regarding the predictive value of coping strategies such as “general avoidance” and “search for social support” on the functional status after surgery [17, 19].
As functional outcomes may partly rely on patient self-management and active participation in the recovery process, the identification of cognitive and behavioural factors amenable to change and of treatment strategies favouring these changes is of considerable interest. A ran-domized trial compared the effectiveness of behavioural graded activity vs usual care provided by physiotherapists following first-time lumbar disc surgery in mostly chronic LBP patients [29]. It was expected that behavioural graded activity would alter fear of movement and pain catastrophising, and thus lead to improved functional sta-tus and higher rates of recovery. However, the results did not meet these expectations. Neither fear of movement nor pain catastrophising seemed to be affected by the treatment programmes. Furthermore, no between-group

251.4 Psychosocial Aspects of Low Back Pain
differences were observed regarding functional status, pain, general health, social functioning and return to work. A study investigating the prognosis of multi-facto-rial outcome in lumbar discectomy showed no significant contribution of pre-operative cognitive reactions to pain and coping strategies to prediction of outcome 6 months post-surgery [20]. Another trial comparing the effective-ness of lumbar fusion surgery associated with post- operative physiotherapy vs a cognitive intervention associated with exercises in patients with chronic LBP showed a decrease of fear-avoidance beliefs in the cogni-tive intervention group and equal improvements in both groups regarding back pain, use of analgesics, emotional distress, life satisfaction and return to work at 1-year fol-low-up [5]. Fear-avoidance beliefs before surgery also significantly predicted work loss 6 months post-surgery in a large trial including patients undergoing surgery for various diagnoses [35]. A large prospective cohort study indicated that higher levels of fear of movement and pas-sive pain coping predicted more severe pain and more disability 6 months after surgery [8]. These studies are based on the body of evidence regarding pain-related fear and its mediating role in the initiation and maintenance of chronic disability in musculoskeletal pain, which empha-sizes the importance of fear-avoidance and its conse-quences [41]. Whether and how fear avoidance is associated with outcomes of surgery is unclear. A recent systematic review on fear avoidance and prognosis in prospective inception cohorts of acute LBP patients con-cluded that while there is some evidence that fear of pain may play a role in chronic LBP, there is little evidence to link fear of pain with poor prognosis at early stages of LBP [31]. The authors contend that emotional process-ing through fear or catastrophising is not necessary for the outcome of reduced activity. Positive reinforcement from significant others for expressed beliefs and avoid-ance behaviour would suffice to increase the likelihood of such behaviour without fear [31]. Addressing the role of these aspects in surgical candidates, as well as in post-operative interventions, clearly warrants further investigation.
Social Factors
The evaluation of social factors includes variables that originate outside the individual. The measure of these factors may rely on patient self-reports and be coloured
by subjective perception, thereby blurring the distinction between psychological and social factors.
Among the social factors that might contribute to the outcomes of surgery, studies point to the role of spouses or significant others and indicate that rein-forcement of pain behaviours by the spouse can reduce spine surgery benefits [12, 33], when the spouse and the family are overprotective and encourage passivity in the patient. However, social support has also been associated with recreational activities, which may con-tribute to help reducing disability [33].
Job satisfaction has been associated with LBP dis-ability. Similarly, psychological aspects of work, i.e. occupational mental stress, general job satisfaction and job-related resignation, were shown to be related to post-operative pain relief and disability [33].
Various studies have shown the duration of pre-oper-ative work incapacity to be a negative predictor of out-come [11, 16, 19, 38]. A prospective observational study of work status as a predictor of outcome from fusion in patients with discogenic back pain has shown that patients working at the time of surgery had a more than ten times greater likelihood of working at follow-up [1].
Compensation status has often been implicated in the development of chronic LBP. Studies evaluating the role of compensation status on various outcomes of surgery display contradictory results. Pre-operative compensation payments and the presence of a com-pensation claim were found to be negatively associated with pain relief and physical activity after surgery [14, 37, 39]. However, a 10-year follow-up study indi-cated that the negative effects of compensation on sat-isfaction and disability scores results seem to dissipate with time [30]. An intervention study conducted in a social security sickness fund on mandatorily insured patients emphasized the importance of post-operative rehabilitation. This study showed increased return to work rates after lumbar disc surgery when medical advisers applied a rehabilitation programme focused on early mobilization and return to work, rather than the usual claim-based practice [11].
The results of another trial in operatively and non-operatively managed patients with sciatica showed that patients who had been receiving workers’ compensa-tion at baseline were more likely to be receiving dis-ability benefits and to report less relief from symptoms and improvement in quality of life at the time of follow-up [2]. However, they were only slightly less likely to be working at the time of follow-up. The

26 C. Cedraschi and V. Piguet
results also showed that patients who had been receiv-ing workers’ compensation at baseline were more likely to be young, male, less educated and involved in physically demanding jobs. These findings parallel those of other studies regarding the association between formal education, back-related disability level and back-related continued disability.
Various factors may account for this association between work status and outcomes of treatment. It has been suggested that job characteristics need to be con-sidered (e.g. occupational category and strength requirement of the job, as well as lack of job auton-omy or decision latitude, or difficulty in obtaining lighter duties during a back pain episode), and also along with patients’ expectations: patients’ expecta-tion of continued pain was found to be significantly associated with education on the one hand and with continued disability on the other [10]. Similarly, it has been shown that manual workers, especially when unskilled, are less likely to remain in work than those in non-manual occupations if they have a limiting ill-ness. This is all the more so when unemployment rates are high [4]. Hence, work status may be related to fac-tors originating outside the patient or the treatment, such as job characteristics, but also local socio-eco-nomic context or sickness and invalidity legislation. Compensation is dependent on the specificities of each health care system [13, 15] and these specificities may account for part of divergences in the results.
Conclusions
This overview hints at contradictory findings and also raises comparability issues in terms of type of patients, surgery, time frame, duration of follow-up or outcome measures. Besides, as it is likely that many of these psy-chological and social variables share predictive vari-ance, their impact can only be determined in multi-causal models. In a recent review, Mannion and Elfering [23] underlined that in view of the evidence it would be inju-dicious to recommend that patients with a surgically remediable pathology be denied surgery merely on the basis of their presurgical psychological screening.
When it comes to clinical considerations, reassur-ance provided by the physician, personal interest, providing medical information and careful listening are important components in a situation of stress and
vulnerability, which may in turn be associated with dis-tress. It has indeed been suggested that the patient–physician relationship plays an essential role in the patient’s recovery, encouraging self-care attitudes in the patient rather than reliance on medical intervention only. These characteristics of the clinical situation have been further stressed in the development of an evi-dence-based booklet for patients undergoing lumbar discectomy and un-instrumented decompression. This booklet aimed to help in removing uncertainty amongst surgeons and patients about post-operative restrictions, reactivation and return to work. It strongly emphasized key messages highlighting the reduction of uncertainty; promotion of positive beliefs; provision of practical advice on self-managemen, and encouraging early reactivation [26]. The patient–physician relationship is of foremost importance to help sort out patients’ per-ceptions and interpretations of symptoms, which may influence expectations – realistic or unrealistic – and contribute to shape the definition of what a meaningful or acceptable outcome might be [3]. This is even more so when surgical indications remain ill defined (e.g. chronic non-specific lower-back pain) [28]. These out-comes should be mutually acceptable and negotiated with the patient within the framework of a stepwise active approach where patient and clinician discuss goals, treatment outcomes, as well as possible obsta-cles to recovery.
References
1. Anderson PA, Schwaegler PE, Cisek D, Leverson G (2006) Work status as a predictor of surgical outcome of discogenic low back pain. Spine 31:2510–2515
2. Atlas SJ, Chang Y, Kamman E et al (2000) Long-term dis-ability and return to work among patients who have a herni-ated lumbar disc: the effect of disability compensation. J Bone Joint Surg 82:4–15
3. Balagué F, Mannion AF, Pellisé F, Cedraschi C (2007) Clinical update: low back pain. Lancet 369:726–728
4. Bartley M, Owen C (1996) Relation between socioeconomic status, employment, and health during economic change, 1973–93. BMJ 313:445–449
5. Brox JI, Sorensen R, Friis A et al (2003) Randomized clini-cal trial of lumbar instrumented fusion and cognitive inter-vention and exercises in patients with chronic low back pain and disc degeneration. Spine 28:1913–1921
6. Carragee EJ (2001) Psychological screening in the surgical treatment of lumbar disc herniation. Clin J Pain 17: 215–219
7. den Boer JJ, Oostendorp RAB, Beems T et al (2006) A systematic review of bio-psychosocial risk factors for an

271.4 Psychosocial Aspects of Low Back Pain
unfavourable outcome after lumbar disc surgery. Eur Spine J 15:527–536
8. den Boer JJ, Oostendorp RAB, Beems T, Munneke M, Evers AVM (2006) Continued disability and pain after lumbar disc surgery: the role of cognitive-behavioral factors. Pain 123: 45–62
9. Deyo RA, Battie M, Beurskens AJHM et al (1998) Outcomes measures for low back pain research. A proposal for stan-dardized use. Spine 23:1003–1013
10. Dionne C, Koepsell TD, Von Korff M et al (1995) Formal education and back-related disability. In search of an expla-nation. Spine 20:2721–2730
11. Donceel P, Du Bois M, Lahaye D (1999) Return to work after surgery for lumbar disc herniation. Spine 24:872–876
12. Epker J, Block AR (2001) Presurgical psychological screen-ing in back pain patients: a review. Clin J Pain 17:200–205
13. Fordyce WE (ed) (1995) Back pain in the workplace. Management of disability in nonspecific conditions. International Association of the Study of Pain (IASP) Press, Seattle
14. Greenough CG, Peterson MD, Fraser RD (1998) Instrumented posterolateral lumbar fusion. Results and comparison with anterior interbody fusion. Spine 23:479–486
15. Hadler NM (1989) Disabling backache in France, Switzerland, and the Netherlands: contrasting sociopolitical constraints on clinical judgment. J Occup Med 31:823–831
16. Hägg O, Fritzell P, Ekselius L, Nordwall A (2003) Predictors of outcome in fusion surgery for chronic low back pain. Eur Spine J 12:22–33
17. Hasenbring M, Marienfeld G, Kuhlendahl D, Soyka D (1994) Risk factors of chronicity in lumbar disc patients. Spine 19:2759–2765
18. Iversen MD, Daltroy LH, Fossel AH, Katz JN (1998) The prognostic importance of patient pre-operative expectations of surgery for lumbar spinal stenosis. Patient Educ Counsel 34:169–178
19. Junge A, Fröhlich M, Ahrens S et al (1996) Predictors of bad and good outcome of lumbar spine surgery. Spine 21: 1056–1064
20. Kohlboeck G, Greimel KV, Piotrowski WP et al (2004) Prognosis of multifactorial outcome in lumbar discectomy. Clin J Pain 20:455–461
21. Lazarus RS, Folkman S (1984) Stress, appraisal, and coping. Springer, New York
22. Lutz GK, Butzlaff ME, Atlas SJ et al (1999) The relationship between expectations and outcomes in surgery for sciatica. J Gen Intern Med 14:740–744
23. Mannion AF, Elfering A (2006) Predictors of surgical out-come and their assessement. Eur Spine J 15:S93–S108
24. Mannion A, Elfering A, Staerkle R et al (2007) Predictors of multidimensional outcome after spinal surgery. Eur Spine J 16:777–786
25. McGregor AH, Hughes SPF (2002) The evaluation of the surgical management of nerve root compression in patients with low back pain. Part 2: patient expectations and satisfac-tion. Spine 27:1471–1477
26. McGregor AH, Burton AK, Sell P, Waddell G (2007) The development of an evidence-based patient booklet for patients undergoing lumbar discectomy and un-instrumented decompression. Eur Spine J 16:339–346
27. Nordin M, Cedraschi C, Skovron ML (1998) Patient-health care provider relationship in patients with non-specific low back pain: a review of some problem situations. Bailliere’s Clin Rheumatol 12(1):75–92
28. Nordin M, Balagué F, Cedraschi C (2006) Non-specific lower back pain: surgical vs non-surgical management. Clin Orthop Relat Res 443:156–167
29. Ostelo RWJG, de Vet HCW, Vlaeyen JWS et al (2003) Behavioral graded activity following first-time lumbar disc surgery. 1-year results of a randomized clinical trial. Spine 28:1757–1765
30. Penta M, Fraser RD (1997) Anterior lumbar interbody fusion. A minimum 10-year follow-up. Spine 22: 2429–2434
31. Pincus T, Vogel S, Burton AK, Santos R, Field AP (2006) Fear avoidance and prognosis in back pain. A systematic review and synthesis of current evidence. Arthritis Rheum 54:3999–4010
32. Rönnberg K, Lind B, Zoëga B et al (2007) Patients’ satisfac-tion with provided care/information on clinical outcome after lumbar disc herniation. Spine 32:256–261
33. Schade V, Semmer N, Main CJ, Hora J, Boos N (1999) The impact of clinical, morphological, psychosocial and work-related factors on the outcome of lumbar discectomy. Pain 80:239–249
34. Slover J, Abdu WA, Hanscom B, Weinstein JN (2006) The impact of comorbidities on the change in Short Form 36 and Oswestry scores following lumbar spine surgery. Spine 31:1974–1980
35. Staerkle R, Mannion AF, Elfering A et al (2004) Longitudinal validation of the fear-avoidance beliefs (FABQ) in a Swiss-German sample of low back pain patients. Eur Spine J 13: 332–340
36. Tandon V, Campbell F, Ross ERS (1999) Posterior lumbar interbody fusion. Association between disability and psy-chological disturbance in non-compensation patients. Spine 24:1833–1838
37. Taylor VM, Deyo RA, Ciol M et al (2000) Patient-oriented outcomes from low back surgery. A community-based study. Spine 25:2445–2452
38. Trief PM, Grant W, Frederickson B (2000) A prospective study of psychological predictors of lumbar surgery out-come. Spine 25:2616–2621
39. Trief PM, Ploutz-Snyder R, Fredrikson BE (2006) Emotional health predicts pain and function after fusion: a prospective multicenter study. Spine 31:823–830
40. Van Susante J, Van de Schaaf D, Pavlov P (1998) Psychological distress deteriorates the subjective outcome of lumbosacral fusion. A prospective study. Acta Orthop Belg 64:371–377
41. Vlaeyen JW, Linton SJ (2000) Fear-avoidance and its conse-quences in chronic musculoskeletal pain: a state of the art. Pain 85:317–332

29M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_1.5, © Springer-Verlag Berlin Heidelberg 2010
Instability of the spine has been defined as an abnormal movement in the motion segment as a response to applied loads. The abnormal motion occur due to dam-age to the motion restraining structures, passive or active such as ligaments, joint capsules, discs and mus-cles that will alter their ability to withstand otherwise normal loadings. Biomechanical studies of the spine have demonstrated the role of different structures and their ability to provide stability of the motion segments of the spine. Comparison of the normal and unstable vertebral motion segment in vivo as well as in vitro have revealed an insight into intriguing interactions between active and passive providers of stability. The role of the normal neuromuscular control system of the spine and this system’s reactions to injuries influencing upon the stability have attracted more and more interest [5]. Kinematic studies have also indicated that the neutral zone seemed to be a more sensitive parameter than the ROM in documenting instability and destabilization and even restabilization by progressive disc degeneration with osteophyte formation, tendency to fusion or muscle stabilization [14]. A development in three stages of spi-nal instability in relation to intervertebral joint degen-eration was proposed already by Kirkaldy-Willis and Farfan [12]. The proposal of three clinical and biome-chanical stages was actually meant for degenerative spondylolisthesis and the stages represented:
Temporary dysfunction•Unstable phase•Stabilization•
The degenerative changes were disc degeneration, facet joints osteoarthritis, ligamentous degeneration, and muscle alterations. The duration of each stage var-ied greatly, and there were no clear-cut clinical signs or symptoms to distinguish one stage from the next.
The first phase, defined as the temporary dysfunc-•tion phase, was associated with slight reversible anatomic changes.The second, or unstable, phase was characterized •by disc height reduction, ligament and joint capsule laxity, and facet joint degeneration.In the third, or stabilization, phase, osteophytes and •marked disc space narrowing lead to stabilization of the motion segment with a reduction (partial or complete) in its ROM, sometimes after spondylolis-thesis had already occurred.
On the basis of this model, the radiologic observation in at least degenerative spondylolisthesis does not nec-essarily indicate that intervertebral instability is still present at the time of imaging because a new stabiliza-tion may have already occurred. Depending on the actual stage it is reasonable to assume that, if present, the pain mechanisms vary and that the relation between pain and instability will vary as well.
Segmental instability of the spine since long has been discussed as one of rather few specific causes of low back pain. Although segmental instability has been extensively studied, discussed and proposed its relation to back pain remain controversial. Certain pathological conditions in the human lumbar spine manifest them-selves as abnormal motion between the separate verte-brae. For long it has been assumed that this abnormal motion can be, detected and measured using radiographic techniques [17, 18]. An excessive antero-posterior translation in the sagittal plane predominantly seen on
Instability and Low Back Pain
Tommy Hansson
T. Hansson Department of Orthopaedics, Sahlgrenska Academy, 413 45 Göteborg, Sweden e-mail: [email protected]
1.5

30 T. Hansson
flexion-extension radiographs has been sought and often taken as a proof of instability.
Studies using functional radiography have revealed that around half of the subjects with visible, slight degenerative changes of the intervertebral joint had hyper-mobility noted as retrolisthesis or anterolisthesis. Both entities occurred at the same frequency in the studied population. Among those without visible degen-erative changes 2/3 had hyper-mobility and once again with a similar proportion between retro- or anterolisthe-sis. Radiating sensations down one or both leg also was equally frequent irrespective of type of slip between the vertebrae. A frequent EMG finding was signs of dam-age to the innervations of the multifidus muscles [16].
Even in a condition like spondylolisthesis, degen-erative or isthmic and with it’s A-P-slip it is uncertain whether instability per se is involved in the generation of pain. In other words, despite the fact that definitions as well as detailed explanatory patho-mechanical mod-els have been proposed there seem to remain many more questions than answers in the ongoing “instabil-ity” debate.
Radiography and Instability
Because of its simplicity, low expense, and wide avail-ability radiography and particularly, functional flexion-extension radiography is the most thoroughly studied and the most widely used method in the imaging diag-nosis of lumbar intervertebral instability [13].
Certain radiographic findings have been proposed as indicators of vertebral instability are:
Degenerative changes of the intervertebral joint •especially of the disc itself are, although still ques-tioned, the radiological finding most commonly related to back pain. The presence of moderate disc degeneration with only slight disc space narrowing and osteosclerosis has been regarded to be a require-ment for instability. A marked disc space narrowing on the other hand has been considered to be indica-tive of the late stabilization phase described by Kirkaldy-Willis and Farfan [12].The so called vacuum phenomenon was early sug-•gested as a sign of instability. Excessive intervertebral distraction of the unstable disc was believed to cause a negative intradiskal pressure turning interstitial
nitrogen into gaseous nitrogen gathering in the turn-ing interstitial nitrogen in the surrounding tissues to become gaseous filling free spaces within the degen-erated nucleus pulposus and annulus fibrosus.Traction spurs that is the osteophytes located few •millimetres from the endplates and oriented horizon-tally have also been regarded a signs of instability. Tensile stresses exerted by traction in the fibres attaching the anterior longitudinal ligament to the vertebral body are believed to generate this type of osteophyte. While the traction spur is caused by ten-sile stresses the claw osteophyte is more likely to be caused by compression. This type is associated with restoration of stabilization rather than instability. It is not uncommon to see both types in the same spine.
Even the value of provocation in diagnosing lumbar instability has been questioned. When the reliability of provocation radiography during traction-compression combined with flexion-extension was tested in more than 300 patients with suspected instability the find-ings were inconclusive [15].
In other words in spite of its frequent use no one conclusively has been able to relate radiographically abnormal motion to a specific back problem. There are several explanations for this;
There is a lack of accurate and standardized mea-•surement techniques,There is no adequate definition of normal motion,•There are large variations in motion between differ-•ent subjects and different spinal levels,Radiography is a static measurement device except •when used as cine.
This means that plain X-ray technique only can reveal abnormal motions occurring at the end points of for example a flexion-extension motion.
Movements like flexion-extension in the lumbar spine are directed by an intrinsic neuromuscular sys-tem that involves passive structures like the interverte-bral disc, ligaments, bone and active structures like muscles and their tendons inclusive. A disorder or injury is likely to disturb the neuromuscular balance and cause dysfunction and/or pain [4]. In back-healthy subjects flexion-extension is a pain-free movement. It is accomplished by appropriately timed excitation of all the involved muscles.
During the deeper part of flexion of the lumbar spine several studies have shown that there is a spontaneous

311.5 Instability and Low Back Pain
reduction in electric activity of the erector spinae mus-cles [2].
This reduction in myoelectric activity was referred to as a “flexion-relaxation” phenomenon. It was suggested that the muscular activity was shut off by signals from receptors in the spinal ligaments stimulated through stretching of them during deep trunk flexion [17].
More recent studies in our group have made this explanation the most plausible for the decreased muscu-lar activity during deep flexion of the lumbar spine [11].
One of many structures stretched during deep flex-ion is the facet joint capsule known to contain proprio-ceptors [2].
Experimental studies on our pig model also have demonstrated that stretching of the facet joint capsules illicit inhibitory responses in the lumbar paraspinal muscles [7].
It is likely that structures like the disc, posterior ligaments, fascia as well as stretched but electrically silent muscles provide stability during “the flexion-relaxation” period [2]. Also it has been shown that the more lateral lumbar muscles, the quadratus lumborum and the iliocaostalis were activated whereas the more medial muscles (multifidus) were inactivated during deep and progressive flexion [1]. In other words, the spine is not only guarded by passive structures during deep flexion but by muscles as well, however more lat-erally located than previously thought of.
It is a reasonable assumption that the normal prop-erties of the structures, passive or active making up the intervertebral joint have been changed through injury or degeneration to permit the abnormal motion which defines segmental instability.
Since the intervertebral disc and above all the changes caused in the disc by degeneration are key-stones to pathological motions in the intervertebral joint this chapter aims at presenting results from kine-matic studies but also studies of properties of the inter-vertebral disc at different grades of degeneration in vitro and in vivo.
Dynamic Loading of the Intervertebral Joint In Vivo
As normal as possible rheological conditions are essential in all kinds of biomechanical testing. For that reason the in vivo dynamic stiffness was studied in
intact and injured intervertebral discs of lumbar motion segments subjected to vibratory loading [3, 8]. A por-cine model was used that allowed application of a min-iaturized servo-hydraulic testing apparatus designed for applying controlled force or displacement in the spine of the anaesthetized animal [8]. The design of the device is based upon two shanks, a mobile and a stationary one, located on the thrust bar [6] (Fig. 1.5.1). The compression induced by this device is an arch-type movement rather than a pure axial compression movement. The difference between those two move-ments is negligible when small movements (<5 mm) as in this experiment were used. No other coupled forces are induced by the device leaving the vertebrae free to rotate axially, bend laterally, and shear anteroposteri-orly and laterally. Force or displacement is applied via the actuator and can be computed acting at the geomet-ric centre of the disc [6].
Animals weighing between 80 and 95 kg were used and the testing occurred at the L2–L3 level. The ani-mals were grouped into three groups; A. consisted of 12 animals with intact (uninjured) disc, B. 6 animals with an acutely injured disc and C. 6 animals with a degenerated (chronic lesion) disc. During testing each animal was placed prone on the operation table. All animals were operated upon at the decided level. The testing device was rigidly fixed to the spine through intra-pedicular screws (Fig. 1.5.1) inserted bilaterally at the L2 and L3 vertebrae.
Group A. was sinusoidal compressed from 0.05 to 25 Hz and at a peak load of either 100 or 200 N.
Group B. with the acutely injured disc (injured through a 15-mm deep antero-lateral scalpel stab
Fig. 1.5.1 The miniaturized servo-hydraulic testing apparatus designed for applying controlled force or displacement in the spine of the anaesthetized animal

32 T. Hansson
injury in the annulus parallel to the endplates of the adjacent vertebrae) was subjected to a peak load set of 200 N.
Group C. with a degenerated disc at the L2–L3 the same loading protocol as in group b. was used. The disc degeneration was created after a similar injury as in group B. In this experiment the animals were recu-perated after the surgical procedures and monitored daily for 3 months.
The results showed that there were no significant differences in dynamic stiffness between the intact and acutely injured discs. For the degenerated disc group a significant increase in stiffness was found when com-pared with the intact disc group. Qualitatively there were no distinct alterations in the shape of the fre-quency response compared with the intact disc.
It was concluded that the in vivo dynamic axial stiffness of the intervertebral joint is dependent upon excitation frequency, load magnitude and load history and that the biomechanical properties of the disc were significantly affected by the degenerative changes of the disc but not by the acute injury
Kinematics of the Intervertebral Joint
In order to better understand the mechanisms of seg-mental instability, its kinematics and potential rela-tions to pain we developed techniques to be used both clinically and experimentally, invasive as well as non-invasive.
To measure the motion in the intervertebral joint a special device was developed called IMD (interverte-bral motion device) (Fig. 1.5.2). This device is rigidly fixed to the vertebrae through K-wires inserted around 20 mm into the spinous processes of two adjacent ver-tebrae [10]. IMD consists of a linkage transducer sys-tem that allows for the dynamic measurement of the sagittal plane. The system is highly repeatable and has accuracy (root mean square (RMS) error) of 0.4 and 0.14 mm for rotatory and translatory movements respectively.
Three displacement transducers detect the motion, which occurs between the pins during flexion-exten-sion (Fig. 1.5.3).
When the IMD is used for measuring motions in a human spinal segment a goniometer measuring the total trunk flexion-extension usually is used simultaneously.
Fig. 1.5.3 The IMD device including the strain gauges fixed to the spinous processes of L3 and L4 in a patient
Fig. 1.5.2 A schematic drawing of the IMD (intervertebral motion device) used for measurement of the kinematics between separate vertebrae in vivo. The device is rigidly fixed to the ver-tebrae through K-wires drilled and secured into the bone of the spinous processes
ROT
AX
SH
Ga GcGb
P1
P0

331.5 Instability and Low Back Pain
Intervertebral Patterns of Motion
Pilot studies with the IMD in back patients with assumed segmental instability indicated that the total flexion-extension motion in the tested intervertebral joint usually was very small e.g. axial translation was much greater and discriminative. Interestingly and shown in the dynamic test reported above disc degen-eration predominantly influenced the discs’ axial stiffness. That made us believe that the pattern of motion was of greater interest than just determining the achieved angle at the end of a motion.
The Pattern of Motion After Experimental Injuries to the Intervertebral Joint
To better understand the pattern of motion we detected in healthy subjects or patients with suspected segmen-tal instability we applied an experimental model which simulated the alterations in segmental kinematics which we had detected in the degenerated human inter-vertebral joint [11].
Once again the pig model was used. With the ani-mal lying prone one of the following type injuries were created to the L3–L4 disc or facet joints.
(A) Disc Anulus Lesion. Using a left-sided retroperito-neal approach, an approximately 12 mm stab incision
was made with a scalpel blade into the mid-part of the anterior anulus fibrosus, without penetration into the nucleus.
(B) Disc nucleus lesion. A 15-mm stab incision was made through the mid-part of the anterior annulus of the disc, parallel to the end plates, penetrating into the nucleus pulposus.
(C) Facet capsule lesion. Using a dorsal approach, bilateral central incisions were made through the collagen capsule of the facet joints into the syn-ovial joint.
(D) Facet joint slit lesion. Bilateral 2 mm wide slits were made along the facet joints, removing on both sides the cartilage that covers the surfaces of the articular processes.
(E) Facet joint wedge lesion. Portions of the superior and inferior articular processes were removed bilaterally, creating a wedge gap approximately 3–4 mm wide across the joint.
(F) Sham lesion. The animals in the sham group (n = 10) underwent the same standard surgical pro-cedures as the other animals but with no injuries to the L3–L4 intervertebral joint [9].
Three months after injury, the animals once again were anaesthetized and placed on a special table allowing flexion-extension motions of the spinal levels studied (Fig. 1.5.4). The IMD (Fig. 1.5.2) was also applied over the L3–L4 level for determination of the POM. The effects of muscular contraction were also examined
Fig. 1.5.4 The anaesthetized animal placed on a special table to allow flexion-extension motions of the spinal levels studied
Forcetransducer
Motor
Support
Pediclescrews
Stimulatingelectrodes
Motion sensors
Support
Pressurecatheter
Caudal displacement
Rostral displacement
10 mm
L4 L3
L4 L3
L4 L3z
y
x
b c
a
10 mm

34 T. Hansson
through bipolar electrodes placed bilaterally around the multifidus and longissimus thoracis at the L2 and L5 vertebral levels. An intense contraction along the paraspinal muscles was achieved by stimulating repet-itive pulses with square voltage [9].
Depending on the type of injury the degenerative changes in the disc and facet joints varied. The kinematic behaviour differed between the injury types but showed a high degree of repeatability within each group.
These studies showed that degenerative changes in the lumbar spine similar to those seen in humans develop within 3 months after a disc injury has been created. Injury-typical POM could be seen when a dynamic measuring technique (IMD) was used. It was also evident that the maximum ROM was a more sen-sitive parameter in detecting alterations in segmental kinematics than is the end ROM. Axial translation and not as supposed sagittal rotation or shear translation was the translatory direction which showed the most change after creation of experimental injuries and disc degeneration. The disc annulus lesion (A), the facet joint wedge lesion (C) and the facet capsule lesion (E) were in order those injuries that most influenced upon the axial translation. The paraspinal muscles ability to provide stability in a chronically changed motion seg-ment was seriously reduced [9].
The Pattern of Motion in Patients with Clinically Suspected Segmental Instability
The POM, the muscular activity and the overall trunk motion were determined during dynamic flexion-exten-sion in seven patients with chronic low back pain. Their pain was supposedly caused by changes that might affect the stability of at least one intervertebral joint in the lumbar spine. Their supposed segmental instability diagnosis was on pain history, clinical findings and pro-nounced radiographic changes, in at least one of the L2–L3, L3–L4, L4–L5 or L5–S1 intervertebral joints. The pain history included sudden stabbing pain epi-sodes especially during certain movements of the spine and typically when the spine was not “guarded”. The patients also had difficulties in flexing the lumbar spine or when rising from a flexed position. All the patients had at least two of the four following radiographic cri-teria on the suspected level.
1. Anterior–posterior translation >3 mm on lateral view static standing radiographs.
2. Angulatory disc space collapse accompanied by trans-lation of the affected vertebra on flexion-extension radiographs
3. Pronounced disc space narrowing (>50% lowering of disc height compared to the nearest disc of nor-mal height).
4. Apparent traction spurs on both sides of the disc.
In all but one patient there was just one supposed unstable intervertebral joint. One patient had two pos-sible unstable segments. Both levels were studied in this patient [11].
The suspected levels were; three L2–L3, two L3–L4 and three L4–L5. Two adjacent motion segments were studied in half of the controls.
Using continuous measuring techniques, the mus-cular behaviour could be precisely defined in relation to the segmental motion throughout the flexion-extension movement the subjects performed (Fig. 1.5.5). An identical protocol was used in six volunteers, the control group, without any recent (>3 months) back problems.
The patient group consisted o four men and three women (mean age 51.4, range 46–56 years). The con-trol group was made up of three men and three women with a mean age of 40.5, range 38–48 years [11].
IMD in Humans
K-wires (2.6 mm diameter) were rigidly fixed under surgical conditions to the neighbouring spinous pro-cesses on the actual vertebral level. The IMD was then secured to the pins (Fig. 1.5.2). In subjects in whom two segments were tested the caudal motion segment was first tested [11].
The trunk flexion-extension angle was simultane-ously measured during the flexion-extension protocol using an electronic goniometer attached to the side of the upper right arm of the subject.
During testing the subject was instructed to hold the arms and hands firmly against the chest and to main-tain a constant position during the flexion-extension. Testing was first performed without and any external loads and then repeated while the subjects held 5 kg weight in the hands against the chest (Fig. 1.5.5).

351.5 Instability and Low Back Pain
EMG Recording
The electromyographic EMG activity of the lumbar erector spinae muscles was recorded during the flex-ion-extension from two sets of surface electrodes placed bilaterally to the L3–L4 inter space and 3 cm lateral to the spinous process recording signals from the lumbar part of the longissimus thoracis´lumbar fibres.
Flexion-Extension Movement
When performing the flexion-extension protocol the subjects were asked to maintain sagittal plane symme-try of the body. Beginning from an erect standing pos-ture the subject bent forward as deep as possible after
which the direction of the movement was reversed passing through the neutral position and continued until maximum extension was reached and then returned to the neutral position.
Kinematics in the Experimental Clinical Study
For all three kinematic variables, sagittal rotation, axial translation and shear translation, the ranges of motion were significantly less, at least 50%, among the patients than among the controls. The controls also flexed and extended their trunks more than the patients. As in the animal models the maximum ROM did not necessarily occur at the endpoints, why the maximum range not always was equal to the end ROM. This was especially pronounced for the axial translation and here more for the patients than for the controls.
There were many differences in the POM between patients and controls. Overall it was found that the patients displayed less intervertebral motion than the controls and especially so in flexion. Even the axial translation motion was less in the patients [11].
EMG Behaviour
For the controls under forward flexion the EMG activ-ity increased to a maximal value. After that max value a progressive decrease in myolelectric activity occurred to full trunk flexion i.e. flexion-relaxation phenome-non. From full flexion the EMG activity increased dra-matically to a maximal value, and therefore decreased to practically no activity in full extension.
In the patients the EMG activity increased but not as much or to a peak value as in the controls. This meant that there was no flexion-relaxation. From full flexion the pattern in the patients were relatively simi-lar to that in the controls.
This study showed that intervertebral motion was significantly less, by at least 50% in the patients with chronic low back pain and supposedly due to seg-mental instability. Trunk flexion and extension were also significantly reduced in the patients. In the con-trol group flexion-relaxtion was demonstrated by a 78% increase in EMG activity. Most of the patients
Fig. 1.5.5 The IMD fixed to two lumbar spinous processes while the patient is extending the spine (fixed pelvis) with 5 kg weight in the hands

36 T. Hansson
demonstrated on the other hand absolutely no flex-ion-relaxation. Flexion-relaxation in the controls occurred in those where intervertebral rotation had reached a stage of completion before maximum trunk flexion was achieved [11].
Conclusions
These studies of experimental and clinical segmental instability have given several not expected results.
Disc degeneration changed the dynamic biomechan-•ical properties of the intervertebral disc significantly. The axial stiffness showed the greatest differences between degenerated and non-degenerated discs suggesting the possibilities of an axial instability.Dynamic measurements of the intervertebral joint •demonstrated that the POM revealed more and other motions than what have been found with static tech-niques. Changes in the axial direction had the great-est magnitude.Specific experimental injuries to the intervertebral •joint, mimicking among others severe disc degen-eration created specific POM.Patients with clinical segmental instability demon-•strated less motion in all directions of the suspected intervertebral joint than back-healthy controls.The patients with chronic low back pain supposedly •due to segmental instability showed no flexion-relaxtion phenomenon.Our results suggested that a “protective” long-standing •back muscle activity rather than an increased motion per se is the most likely pain mechanism in “seg-mental instability”.
References
1. Andersson EA, Oddsson LI, Grundstrom H, Nilsson J, Thorstensson A (1996) EMG activities of the quadratus lum-borum and erector spinae muscles during flexion-relaxation and other motor tasks. Clin Biomech (Bristol, Avon) 11:392–400. DOI 0268003396000332 [pii]
2. Cavanaugh JM, Ozaktay AC, Yamashita HT, King AI (1996) Lumbar facet pain: biomechanics, neuroanatomy and neuro-physiology. J Biomech 29:1117–1129. doi:0021929096000231 [pii]
3. Ekstrom L, Kaigle A, Hult E, Holm S, Rostedt M, Hansson T (1996) Intervertebral disc response to cyclic loading–an ani-mal model. Proc Inst Mech Eng [H] 210:249–258
4. Hodges P, Holm AK, Hansson T, Holm S (2006) Rapid atro-phy of the lumbar multifidus follows experimental disc or nerve root injury. Spine 31:2926–2933. doi:10.1097/01.brs.0000248453.51165.0b00007632-200612010-00008 [pii]
5. Hodges P, Kaigle Holm A, Holm S, Ekstrom L, Cresswell A, Hansson T, Thorstensson A (2003) Intervertebral stiffness of the spine is increased by evoked contraction of transversus abdominis and the diaphragm: in vivo porcine studies. Spine 28:2594–2601. doi:10.1097/01.BRS.0000096676.14323.25
6. Hult E, Ekstrom L, Kaigle A, Holm S, Hansson T (1995) In vivo measurement of spinal column viscoelasticity–an ani-mal model. Proc Inst Mech Eng [H] 209:105–110; discus-sion 135
7. Indahl A, Kaigle AM, Reikeras O, Holm SH (1997) Interaction between the porcine lumbar intervertebral disc, zygapophysial joints, and paraspinal muscles. Spine 22: 2834–2840
8. Kaigle A, Ekstrom L, Holm S, Rostedt M, Hansson T (1998) In vivo dynamic stiffness of the porcine lumbar spine exposed to cyclic loading: influence of load and degenera-tion. J Spinal Disord 11:65–70
9. Kaigle AM, Holm SH, Hansson TH (1997) 1997 Volvo Award winner in biomechanical studies. Kinematic behavior of the porcine lumbar spine: a chronic lesion model. Spine 22:2796–2806
10. Kaigle AM, Pope MH, Fleming BC, Hansson T (1992) A method for the intravital measurement of interspinous kine-matics. J Biomech 25:451–456
11. Kaigle AM, Wessberg P, Hansson TH (1998) Muscular and kinematic behavior of the lumbar spine during flexion-extension. J Spinal Disord 11:163–174
12. Kirkaldy-Willis WH, Farfan HF (1982) Instability of the lumbar spine. Clin Orthop Relat Res 165:110–123
13. Leone A, Guglielmi G, Cassar-Pullicino VN, Bonomo L (2007) Lumbar intervertebral instability: a review. Radiology 245:62–77. doi:245/1/62 [pii] 10.1148/radiol.2451051359
14. Panjabi MM (2003) Clinical spinal instability and low back pain. J Electromyogr Kinesiol 13:371–379. doi:S1050641103000440 [pii]
15. Pitkanen M, Manninen HI, Lindgrer KA, Turunen M, Airaksinen O (1997) Limited usefulness of traction-com-pression films in the radiographic diagnosis of lumbar spinal instability. Comparison with flexion-extension films. Spine 22:193–197
16. Sihvonen T, Lindgren KA, Airaksinen O, Manninen H (1997) Movement disturbances of the lumbar spine and abnormal back muscle electromyographic findings in recur-rent low back pain. Spine 22:289–295
17. Sihvonen T, Partanen J, Hanninen O, Soimakallio S (1991) Electric behavior of low back muscles during lumbar pelvic rhythm in low back pain patients and healthy controls. Arch Phys Med Rehabil 72:1080–1087
18. Soini J, Antti-Poika I, Tallroth K, Konttinen YT, Honkanen V, Santavirta S (1991) Disc degeneration and angular move-ment of the lumbar spine: comparative study using plain and flexion-extension radiography and discography. J Spinal Disord 4:183–187

Part
DiagnosisII

39M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_2.1, © Springer-Verlag Berlin Heidelberg 2010
Introduction
Spinal imaging is one of the most important diagnostic tools for assessing spine pathologies. The advent of Magnetic Resonance Imaging (MRI) allowed much more detailed evaluation of musculoskeletal injuries including the spine. However, because of the structural limitations of MRI equipment, patient scanning has been limited to supine or prone positions without weight-bearing, which renders static images in fixed positions. Specifically, dynamic evaluation of the spine with functional loading has not been possible.
Dynamic imaging with positional changes in a closed MRI has been attempted to evaluate structures in the functional spinal unit [1–4]. Using a closed MRI, Muhle et al. [2] reported an increase in the rate of detecting spinal stenosis in the extension position. In addition, other studies have demonstrated significant anatomical variation between neutral, flexion, or exten-sion positions. Axial loaded images, with positional change, can precisely assess pathology by simulating daily functional states allowing symptom-specific patient positioning while scanning.
The recent introduction of a front-open Kinetic MRI (kMRI) system eliminates the limitations of closed, static, single-position MRI. Changing patient positioning frequently affects spinal symptoms and pathology. Increased symptom(s) severity may present only when the patient is in a specific position and may disappear upon position change. Spinal nerve compro-mise, spinal cord compression, or cauda equina can
affect structures in the functional unit such as the facet joints or musculature. Kinetic MRI provides physi-cians with information according to the patient’s posi-tion and can reveal pathology previously not identified by conventional MRI.
A variety of methods have been employed to evalu-ate spinal kinematics. Imaging modalities include plain radiographs, fluoroscopy, CT scan, and MRI – all of which are frequently utilized for kinematic evaluation of the functional unit. Currently, the most precise and reliable method involves a cadaveric model. Kinetic MRI provides images of positional changes combined with loading and is the best method for evaluating in vivo biomechanics.
Contents
Technical Aspects
Kinetic MRI consists of two vertically-oriented doughnut-shaped magnetic coils with a gap. The machine is a mid-field 0.6 T Magnet. A mid-field scan-ner is optimal for positional imaging since the high-field system is more susceptible to motion artifact and may increase scan time. The front-open design of the kinetic MRI affords varied patient positioning during imaging. To maintain patient positioning during longer imaging, assistive devices or equipments are utilized.
Except for serial changes in the frontal plane, both sagittal and axial planes can be imaged. This allows flexion-distraction or axial rotation. Such positional changes allow spinal loading if the patient is not supine. Axial and sagittal image cuts can be acquired as with conventional static MRI. Although processing
Dynamic MRI of the Spine
J. J. Abitbol, Soon-Woo Hong, Sana Khan, and Jeffrey C. Wang
J. J. Abitbol (*) California Spine Group, 5395 Ruffin Road, Suite 103, San Diego, CA 92123, USA e-mail: [email protected]
2.1

40 J. J. Abitbol et al.
time is longer (currently), in some settings, collected data can be displayed 3-dimensionally, thereby repre-senting the patient’s anatomy and movement.
Diagnostic Aspects
Weight-Bearing
The spine’s weight-bearing capacity, such as during standing and sitting, is an important function to evalu-ate. Many symptoms occur and/or are aggravated dur-ing weight-bearing. Conventional supine MRI imaging may not reveal the pathology related to one or more symptoms. Utilizing kinetic MRI provides more reli-able and suitable information to accurately diagnose musculoskeletal disorders affected by weight-bearing.
Flexion and Extension
Diagnostic evaluation of motion in the axial and sagit-tal planes is important, as symptoms may be influenced or aggravated upon positional change. Unlike kinetic MRI, other imaging methods are limited in demon-strating motion-related abnormalities.
Disk Morphology
Disk degeneration accompanies aging and some spinal disorders. Age-dependent changes in disk morphology are closely correlated with progressive disk degeneration [5]. Signal changes in the nucleus pulposus using T2-weighted imaging is well-known in the evaluation of disk degeneration. While several grading systems have been developed to assess the severity of disk degenera-tion, the histological grading system using MRI images is considered to be the most accurate. Kinetic MRI can be used to assess disk degeneration, as well as examine related morphologic and kinematic changes. While dis-cography is useful to evaluate symptomatic disk degen-eration, patients are exposed to radiation and a needle-invasive procedure. During discography, position change or axial loading can induce pain. Kinetic MRI can produce similar evaluative results noninvasively.
Kinetic MRI can evaluate morphological change(s) caused by progressive disk degeneration. Karadimas et al.
[6] reported that posterior disk height decreased with weight-bearing in advanced grade 3 and 4 disk degen-eration. This means disk degeneration is more sensi-tive to change in disk height during axial loading and corresponds to size change of the neural foramen. In addition, seated position with axial loading increased intradiscal pressure. Therefore, disk instability sec-ondary to degeneration may lead to greater posterior protrusion and pain. Diagnosis of disk herniation could be better evaluated if the patient assumes a full flexion-extension position. Zamani et al. [7] found annular bulging in 27% of disks in the erect extended position with the presence of disk degeneration that increased to 40%.
Disk herniation is understood to be a common cause of nerve root compression. In a clinical scenario, local-izing pain can be difficult, especially in cases of multi-level involvement. Gilbert et al. [8] demonstrated that underestimating the level of disk involvement may mask a major lesion site.
Spinal Canal and Intervertebral Foramen
Spinal canal diameter is closely associated with spi-nal stenosis and myelopathy. Symptoms of these dis-orders are relatively sensitive to positional change(s). Vitaz et al. [9] suggested that kinetic MRI is suit-able for evaluating degenerative cervical myelopathy. Muhle et al. [1] reported a correlation between the degenerative stage and cervical myelopathy through kinetic MRI imaging. That study demonstrated that functional cord impingement at extension also increased with advanced degeneration. Studies of spinal canal diameter during flexion-extension, while utilizing kinetic MRI, showed statistically significant difference in both cervical [9] and lumbar [10] regions.
With advancing age, spinal stenosis increases and frequently presents at multiple levels. An appropri-ate treatment plan is dependent on precise diagnosis of the level(s) affected by spinal stenosis. Although static MRI may obtain information about multilevel stenosis, many surgeons defer to myelography for accurate preoperative planning. Myelography pro-vides well-localized imaging of dural compression, which may be comparable to intraoperative findings [11]. In a report comparing kinetic MRI to myelogra-phy, in the diagnosis of lumbar spinal stenosis, both imaging modalities were closely correlated. However,

412.1 Dynamic MRI of the Spine
kinetic MRI is preferred for patients since it is less painful, noninvasive, and has considerable lower risk for complications.
Cross-sectional analysis of the disk level is another assessment method. In vitro studies using CT showed a significant reduction of the cross-sectional area of the spinal canal at extension when compared with flexion [12, 13], or at axial loading [14]. However, CT does not demonstrate any difference in ligamentum flavum thick-ness. Schmid et al. [15] demonstrated the measurement of the cross-sectional area in asymptomatic volunteers showed significant differences during flexion and exten-sion using kinetic MRI. This study quantitatively proved that the thickness of the ligamentum flavum increased at extension with statistical significance. In a study using kinetic MRI, Weishaupt et al. [16] postulated that the cross-sectional area uniformly decreased at exten-sion regardless of the extent of disk herniation.
Foraminal neural compression can be predicted by measuring the cross-sectional area of the neural foram-ina. Positional changes proved to significantly affect measurement of the neural foramina in a pattern simi-lar to the central canal area, which showed increase at flexion and decrease at extension [13, 15, 17, 18]. A morphometric cadaver study by Mayoux-Benhamou et al. [19] postulated that such reduction of neural foraminal size at extension can result from three ana-tomical changes: reduction of vertical height with pedicles closer, decreased width of the upper foramen by separation and ascent of the upper extremity of the inferior articular facet with bulging of the capsule and ligamentum flavum, and decreased width of the lower foramen by the associated disk bulge. Compared with supine imaging, nerve root contact, without deviation, increases in frequency during loaded flexion and exten-sion views in kinetic MRI. This means that kinetic MRI may provide additional information in select patients with equivocal findings of nerve root compro-mise on supine MRI, or upon strong suspicion of dynamic nerve root compromise in the upright extended position [16, 20].
Paraspinal Muscles
The role of the paraspinal muscles in relation to low back pain remains unclear. However, atrophy of the paraspinal muscles may accompany pathologies such as disk herniation, spinal stenosis, and spondylolisthesis.
Electromyography, ultrasonography, histopathology, and static MRI have been used to study the paraspinal muscles. However, dynamic MRI can provide more information in relation to morphology and biomechan-ics. Jorgensen et al. [21] reported that the cross-sectional area of the back muscles at L4–L5 and L5-S1 decreased by different percentages as the torso moved from neu-tral to 45° of flexion in the sagittal plane. This suggests that the lumbar back muscles may not be uniformly lengthening during torso flexion.
Ligaments
Thickness of the ligamentum flavum has been fre-quently evaluated in relation to spinal stenosis [13, 15, 18]. However, in acute traumatic conditions, other liga-ments may be important. Ignelzi [22] reported four cases where kinetic MRI was used to assess acute cer-vical trauma. Though fractures demonstrated on plain X-ray or CT alone may not be indicative of spinal insta-bility, that information, combined with MRI demon-strating ligamentous injury, provided a high index for instability, which was important for clinical decisions.
Facet Joints
The function spinal unit consists of three joint com-plexes, one intervertebral disk and two facet joints. Facet joints play an important role in segmental stability and biomechanics and are best visualized on axial images. In a study comparing normal volunteers to patients with disk herniation, it was demonstrated that the facet angle in patients is uniformly decreased in the lower lumbar spine, such as L3-L4, L4-L5, and L5-S1 [23].
Bony structures, such as the facet joints, are better visualized using CT, rather than MRI. However, recent advances in MRI demonstrated images acceptable to accurately assess degenerative facet joint change(s) when compared with CT [24].
Biomechanical Aspects and Intraoperative and Postoperative Evaluation
The definition of instability remains unclear and may be due to unknowns related to biomechanics of the functional spinal unit in vivo. Kinetic MRI’s positional

42 J. J. Abitbol et al.
imaging capability is a significant advancement in ana-lyzing in vivo biomechanics.
Translational Motion
For instability assessment, translation and angular motion are considered to be important parameters. Segmental motion in the sagittal plane in relation to instability has frequently been studied using flexion-extension radiographs and fluoroscopy. However, high radiation exposure and low accuracy may limit the use of radiography and fluoroscopy. When kinetic MRI is employed, these parameters are measurable without radiation and render soft tissue structures in great detail.
In some patients with spondylolisthesis, a supine static MRI may miss the diagnosis, although the spon-dylolisthesis is demonstrated on plain standing radio-graphs. In a study of healthy subjects, McGregor et al. [25] reported reliable and repeatable translation motion using kinetic MRI. They demonstrated that anterolis-thesis occurs in flexion and retrolisthesis in extension. Using kinetic MRI, dynamic instability has been detected with the same criteria as in simple radio-graphs. However, kinetic MRI also allowed simultane-ous analysis of soft tissue relationships, such as spinal cord compression, with the instability [9].
Disk degeneration and segmental motion have been studied using simple radiographs, discograms [26], MRI images [27–29], and cadaveric studies [30–32]. In these studies, no statistically significant correlation between translational motion and disk degeneration has been found [27, 29, 33, 34]. In a report where kinetic MRI was utilized, no significant difference in translational motion among normal subjects and patients with spondylolisthesis was shown [35].
Angular Motion
Using kinetic MRI, Harvey et al. [36] demonstrated that lordosis and flexion in the lumbosacral spine had linear correlation with age in healthy subjects. McGregor et al. [25] reported that segmental angular motion had the greatest value in the lower lumbar lev-els, specifically L4-L5 and L5-S1. The least amount of motion occurred at the L1-L2 junction. These results were similar to a study using 3-dimensional radiogra-phy [37].
Vitzthum et al. [24] reported dynamic examination of the lumbar spine comparing normal volunteers and patients with disk herniation using kinetic MRI. Segmental angular motion was found to decrease when disk herniation appeared in the lower lumbar levels. Karadimas et al. [6] demonstrated that segmental angular motion decreased with increased disk degen-eration in patients with chronic low back pain using kinetic MRI. This result was in accord with a study wherein flexion-extension radiographs and static MRI was conducted by Murata et al. [29]. Their lumbar lor-dosis study did not show a significant difference between conventional and kinetic MRI.
Axial Rotation
Axial rotation can be examined using kinetic MRI. Many reports where cadavers were used describe axial rotation. However, few studies exist using kinetic MRI. In an in vitro study by Fujiwara et al. [38], static MRI and flexion-extension radiographs demonstrated axial rotation increased to grade 4 with disk degeneration. However, axial rotation decreased where disk degenera-tion was grade 5, a worse grade level. The study using kinetic MRI, conducted by Vitzthum et al. [24], demon-strated that segmental axial rotation increased in the disk herniation group as compared to the normal group.
Lateral Bending
The study of lateral bending, using kinetic MRI, is limited and may be due to technical difficulties and lower clinical usability.
Study Effects of Dynamic Stabilization
Dynamic stabilization of the functional unit is a cur-rent trend in spine surgery. Motion-preserving surger-ies, such as arthroplasty and dynamic fixation, are popular. Kinetic MRI is capable of evaluating motion characteristics in patients. Exact evaluation before and after motion-preserving surgery is still unclear and may be resolved in the future to some extent by using kinetic MRI.
Postoperatively, the spine may best be analyzed using kinetic MRI in patients who have previously undergone

432.1 Dynamic MRI of the Spine
an instrumented or uninstrumented intersegmental fusion. Using kinetic MRI, Jinkins et al. [39] demon-strated that hypermobile intersegmental spinal instabil-ity may occur adjacent to levels of a stable fusion.
Siddiqui et al. [40, 41] reported changes in the cross-sectional area of the spinal canal and interverte-bral foramen before and after X-STOP® (Kyphon Inc., Sunnyvale, CA USA) in vivo implantation and con-firmed adequate nerve decompression using this device. In a postoperative biomechanical study related to X-STOP® and Dynesys® (Zimmer, Inc., Warsaw, IN USA) implantation, where kinetic MRI [42, 43] was utilized, segmental motion decreased and posterior disk height increased at the device level.
Intraoperatively, open MRI allows direct surgical access to the stationary patient during imaging. It pro-vides all of the advantages of conventional MR imaging, including multiplanar acquisition and excellent defini-tion of soft anatomy. Woodard et al. [44] reported that intraoperative MRI provided accurate and rapid localiza-tion and confirmed the adequacy of decompression in the majority of the 12 spine surgery cases studied. Verheyden et al. [45] employed open MRI during surgery and dem-onstrated that positioning of screws into the pedicle was secure and the degree of indirect reduction of the verte-bral posterior wall could be immediately imaged.
Limitations
Although open kinetic MRI provides excellent imag-ing during motion in the sagittal and axial planes, dynamic imaging of the coronal plane is limited. It is difficult to obtain sufficient information when severely deformed patients, such as those with scoliosis, are imaged.
Kinetic MRI’s mid-range magnetic field may be another limiting factor. The magnetic field is 0.6 T and some soft tissue structures are better visualized using high-field 1.5 T static MRI. Therefore, surgical plan-ning based on open kinetic MRI should be carefully decided based on the pathology being addressed (e.g., brain tumor resection vs. discectomy) [46].
To obtain precise information using kinetic MRI, it may require positioning patients to induce or aggravate symptoms. Since it takes longer to produce images using kinetic MRI, patient discomfort and blurred images (when movement occurs during imaging) can occur.
Conclusions
Although conventional static MRI, with the patient positioned supine, remains a useful imaging method to assess degenerative spinal diseases, it can miss an occult herniated disk, stenosis, or instability visualized using kinetic MRI. Therefore, kinetic MRI can be per-formed in patients with equivocal findings on conven-tional MRI, or those whose symptoms alter with positional change. Kinetic MRI has the potential to evaluate in vivo biomechanical changes both preopera-tively and postoperatively. With continued advance-ment in understanding the utilization of positional imaging, kinetic MRI may become a more meaningful imaging modality for various other conditions.
References
1. Muhle C, Metzner J, Weinert D et al (1998) Classification system based on kinematic MR imaging in cervical spon-dylitic myelopathy. ANJR Am J Neuroradiol 19:1763–1771
2. Muhle C, Weinert D, Falliner A et al (1998) Dynamic changes of the spinal canal in patients with cervical spondy-losis at flexion and extension using magnetic resonance imaging. Invest Radiol 33:444–449
3. Chung SS, Lee CS, Kim SH et al (2000) Effects of low back posture on the morphology of the spinal canal. Skeletal Radiol 29:217–223
4. Chen CJ, Hsu HL, Niu CC et al (2003) Cervical degenera-tive disease at flexion-extension MR imaging: prediction criteria. Radiology 227:136–142
5. Boden SD, Davis DO, Dina TA et al (1990) Abnormal magnetic-resonance scans of the lumbar spine in asymptom-atic subjects. A prospective investigation. J Bone Joint Surg Am 72:403–408
6. Karadimas EJ, Siddiqui M, Smith FW et al (2006) Positional MRI changes in supine versus sitting postures in patients with degenerative lumbar spine. J Spinal Disord Tech 19: 495–500
7. Zamani AA, Moriarty T, Hsu L et al (1998) Functional MRI of the lumbar spine in erect position in a superconducting open-configuration MR system; preliminary results. J Magn Reson Imaging 8:1329–1333
8. Gilbert JW, Wheeler GR, Lingreen RA et al (2006) Open stand-up MRI: a new instrument for positional neuroimag-ing. J Spinal Disord Tech 19:151–154
9. Vitaz TW, Shields CB, Raque GH et al (2004) Dynamic weight-bearing cervical magnetic resonance imaging: techni-cal review and preliminary results. South Med J 97: 456–461
10. Wildermuth S, Zanetti M, Duewell D et al (1998) Lumbar spine: quantitative and qualitative assessment of positional (upright flexion and extension) MR imaging and myelogra-phy. Radiology 207:391–398

44 J. J. Abitbol et al.
11. Bell GR, Ross JS (1992) Diagnosis of nerve root compres-sion. Myelography, computed tomography, and MRI. Orthop Clin North Am 23:405–419
12. Schonstrom N, Lindahl S, Willen J et al (1989) Dynamic changes in the dimensions of the lumbar spinal canal: an experimental study in vitro. J Orthop Res 7:115–121
13. Inufusa A, An HS, Lim TH et al (1996) Anatomic changes of the spinal canal and intervertebral foramen associated with flexion-extension movement. Spine 21:2410–2412
14. Nowicki BH, Yu S, Reinartz J et al (1990) Effect of axial loading on neural foramina and nerve roots in the lumbar spine. Radiology 176:433–437
15. Schmid MR, Stucki G, Duewell S et al (1999) Changes in cross-sectional measurements of the spinal canal and inter-vertebral foramina as a function of body position: in vivo studies on an open-configuration MR system. AJR Am J Roentgenol 172:1095–1102
16. Weishaupt D, Schmid MR, Zanetti M et al (2000) Positional MR imaging of the lumbar spine: does it demonstrate nerve root compression not visible at conventional MR imaging? Radiology 215:247–253
17. Nowicki BH, Haughton VM, Schmidt TA et al (1996) Occult lumbar lateral spinal stenosis in neural foramina subjected to physiologic loading. AJNR Am J Neuroradiol 17: 1605–1614
18. Fujiwara A, An HS, Lim TH et al (2001) Morphologic changes in the lumbar intervertebral foramen due to flexion-extension, lateral bending, and axial rotation: an in vitro ana-tomic and biomechanical study. Spine 26:876–882
19. Mayoux-Benhamou MA, Revel M, Aaron C et al (1989) A morphometric study of the lumbar foramen. Influence of flexion-extension movements and of isolated disc collapse. Surg Radiol Anat 11:97–102
20. Weishaupt D, Boxheimer L (2003) Magnetic resonance imaging of the weight-bearing spine. Semin Musculoskelet Radiol 7:277–286
21. Jorgensen MJ, Marras WS, Gupta P (2003) Cross-sectional area of the lumbar back muscles as a function of torso flex-ion. Clin Biomech (Bristol, Avon) 18:280–286
22. Ignelzi RJ (1993) The potential role of low field MR with open design in assessing ligamentous injury in acute cervical trauma. Surg Neurol 39:519–529
23. Vitzthum HE, Konig A, Seifert V (2000) Dynamic examina-tion of the lumbar spine by using vertical, open magnetic resonance imaging. J Neurosurg 93:58–64
24. Weishaupt D, Zanetti M, Boos N et al (1999) MR imaging and CT in osteoarthritis of the lumber facet joints. Skeletal Radiol 28:215–219
25. McGregor AH, Anderton L, Gedroyc WM et al (2004) Assessment of spinal kinematics using open interventional magnetic resonance imaging. Clin Orthop Relat Res (392): 341–348
26. Soini J, Antti-Poika I, Tallroth K et al (1991) Disc degenera-tion and angular movement of the lumbar spine: comparative study using plain and flexion-extension radiography and dis-cography. J Spinal Disord 4:183–187
27. Paajanen H, Erkintalo M, Dahlstrom S et al (1989) Disc degeneration and lumbar instability. Magnetic resonance examination of 16 patients. Acta Orthop Scand 60:375–378
28. Burton AK, Battie MC, Gibbons L et al (1996) Lumbar disc degeneration and sagittal flexibility. J Spinal Disord 9: 418–424
29. Murata M, Morio Y, Kuranobu K (1994) Lumbar disc degen-eration and segmental instability: a comparison of magnetic resonance images and plain radiographs of patients with low back pain. Arch Orthop Trauma Surg 113:297–301
30. Nachemson AL, Schultz AB, Berkson MH (1979) Mechanical properties of human lumbar spine motion seg-ments. Influence of age, sex, disc level, and degeneration. Spine 4:1
31. Mimura M, Panjabi MM, Oland TR et al (1994) Disc degen-eration affects the multidirectional flexibility of the lumbar spine. Spine 19:1371–1380
32. Tanaka N, An HS, Lim TH et al (2001) The relationship between disc degeneration and flexibility of the lumbar spine. Spine J 1:47–56
33. Pitkanen MT, Manninen HI, Lindren KA et al (2002) Segmental lumbar spine instability at flexion-extension radi-ography can be predicted by conventional radiography. Clin Radiol 57:632–639
34. Axelsson P, Karlsson BS (2004) Invertebral mobility in the progressive degenerative process. A radiostereometric anal-ysis. Eur Spine J 13:567–572
35. McGregor AH, Anderton L, Gedroyc WM et al (2002) The use of interventional open MRI to assess the kinematics of the lumbar spine in patients with spondylolisthesis. Spine 27:1582–1586
36. Harvey SB, Smith FW, Hukins DW (1998) Measurement of lumbar spine flexion-extension using a low-field open-mag-netic resonance scanner. Invest Radiol 33:439–443
37. Pearcy M, Portek I, Shepherd J (1984) Three-dimensional X-ray analysis of normal movement in the lumbar spine. Spine 9:294–297
38. Fujiwara A, Tamai K, An HS et al (2000) The relationship between disc degeneration, facet joint osteoarthritis, and sta-bility of the degenerative lumbar spine. J Spinal Disord 13:444–450
39. Jinkins JR, Dworkin JS, Damadian RV (2005) Upright, weight-bearing, dynamic-kinetic MRI of the spine: initial results. Eur Radiol 15:1815–1825
40. Siddiqui M, Nicol M, Karadimas E et al (2005) The posi-tional magnetic resonance imaging changes in the lumbar spine following insertion of a novel interspinous process dis-traction device. Spine 30:2677–2682
41. Siddiqui M, Karadimas E, Nicol M et al (2006) Influence of X-STOP on neural foramina and spinal canal area in spinal stenosis. Spine 31:2958–2962
42. Siddiqui M, Karadimas E, Nicol M et al (2006) Effects of X-STOP device on sagittal lumbar spine kinetic in spinal stenosis. J Spinal Disord Tech 19:328–333
43. Beastall J, Karadimas E, Siddiqui M et al (2007) The Dynesys lumbar spinal stabilization system: a preliminary report on positional magnetic resonance imaging findings. Spine 32:685–690
44. Woodard EJ, Leon SP, Moriarty TM et al (2001) Initial expe-rience with intraoperative magnetic resonance imaging in spine surgery. Spine 26:410–417

452.1 Dynamic MRI of the Spine
45. Verheyden P, Katscher S, Schulz T et al (1999) Open MR imaging in spine surgery: experimental investigations and first clinical experiences. Eur Spine J 8:346–353
46. McCulloch JA (2001) Low-field-strength (open) MRI does not delivery the information needed to plan lumbar micro-discectomy and/or microdecompression. Spine J 1:160
47. Cargill SC, Pearcy M, Barry MD (2007) Three-dimensional lumbar spine postures measured by magnetic resonance imaging reconstruction. Spine 32:1242–1248
48. Thompson JP, Pearce RH, Schechter MT et al (1990) Preliminary evaluation of a scheme for grading the gross morphology of the human intervertebral disc. Spine 15: 411–415
49. Pfirrmann CW, Metzdorf A, Zanetti M et al (2001) Magnetic resonance classification of lumber intervertebral disc degen-eration. Spine 26:1873–1878

47M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_2.2, © Springer-Verlag Berlin Heidelberg 2010
Evaluation of Nutrition to the Disc
Although multi-factorial, alterations in nutrition are considered to be the “final common pathway” for DDD [24]. Along with intact nutritional pathways, a stable mechanical environment that will maintain the normal hydrostatic pressure is also important to maintain the health of the disc. The end plate (EP) plays a crucial role in maintaining the mechanical environment and the intact nutritional pathways and thus, plays a crucial role in both the health and disease of the lumbar discs. However, it is reduced to a thin layer of cartilaginous tissue early in life and is susceptible to mechanical failure [25]. Autopsy studies have demonstrated micro-cracks and progressive failure of the EP even in the first decade of life. Corresponding physiological changes in diffusion have also been demonstrated by serial post-contrast magnetic resonance imaging (MRI) studies [26, 27]. These damages increase in frequency and severity over the age, but the healing potential of the EP is not clear. EP damage can precipitate DDD in a variety of ways including altered nutrition [28], leak-age of protein macro-molecules and loss of hydrostatic pressure, altered matrix synthesis [21–23, 29, 30], sec-ondary annular damage and vascularization of the nucleus pulposus without auto immune changes [31, 32]. It is now well accepted that structural failure of the EP may be the crucial factor in initiating the prog-ress of DDD [11, 21, 26, 30, 33, 34].
Biological treatment methods such as the use of recombinant proteins, cytokines and growth factors [35–38], molecular therapy [39–43], gene transfer techniques [44–46] and stem cell therapy [47–50] are now viewed as attractive options to halt or even reverse DDD. However, the success of these therapies will depend on the nutritional status of the discs, which in turn depends on the status of the EP. A normal EP will allow normal diffusion and ensure adequate nutrition for implanted cells. In contrast, these therapies will fail when performed in a degenerated disc that has dam-aged EPs, which do not allow any nutrition. The “soil” is as important as the “seed” and any biological ther-apy is doomed to fail when employed in an inappropri-ate setting of poor nutritional supply. It becomes important that the functional status of the EP and the nutrition to the disc is properly assessed before any treatment decision is performed [51].
Assessment of the Structure and Function of End Plate in Vivo
There is a volume of literature on the EP and its role in DDD [21–23, 26, 30, 32, 52–55].However, most of them are based on laboratory studies [56, 57], animal studies [58–61] or cadaveric studies [25]. MRI is a commonly performed investigation and has proved successful in evaluating the status of the discs. It would be helpful to have a MRI-based assessment of the EP status and damage.
A clear understanding of MRI appearance of the EP is necessary. Modic et al. described three types of changes in the EP region (Fig. 2.2.1), which are now popularly termed as “EP changes” [62]. However, these are changes in the vertebral marrow and subchondral
Assessment of Status of End Plate and Diffusion in Degenerative Disc Disease
S. Rajasekaran
S. Rajasekaran Department of Orthopaedic and Spine Surgery, Ganga Hospital, 313 Mettupalayam Road, Coimbatore, 641043 Tamil Nadu, India e-mail: [email protected]
2.2

48 S. Rajasekaran
bone and do not represent the actual EP. Uniform hypo-intense bands that separate the nucleus pulposus and the subchondral bone and clearly seen in T1 and T2 weighted images have been reported to functionally represent the EP in the MRI. Subsequent detailed stud-ies of 365 lumbar discs have also confirmed that the status of the EP and severity of damage can be identi-fied by studying the hypo-intense bands [51].
Rajasekaran et al. assessed the status of 730 EPs of 365 discs from 73 individuals (26 healthy human vol-unteers and 47 patients) in T1 weighted images and
described six types according to the severity of damage (Fig. 2.2.2) [51]. Type I EP had no damage and was seen as a uniformly symmetrical concave hypo-intense band without EP breaks or associated Modic changes. Type II EP had focal thinning either at the centre or periphery, but without any EP break or Modic changes. Type III EP demonstrated focal disc marrow contact regions without alteration in the contour of the EP. Modic changes were absent. Type IV EP damage resembles a typical schmorl’s node occupying up to 25% of the EP area with typical depression. Subchondral
Fig. 2.2.1 The existing phrase “end plate (EP) changes”, which has already found wide usage and acceptance in the literature, causes confusion of the exact representation of EP in literature. The magnetic resonance imaging (MRI) frequently shows signal intensity (SI) changes of the subchondral bone (grey arrows), which have been termed “EP changes”. The three types of changes that have been described actually represent the MRI appearance of the changes in the vertebral bone marrow. (b–d) The changes frequently extend into the body and are not those of the EP. In the normal T1 MRI picture, there is a hypointense
zone between the subchondral bone and the nucleus pulposus (white arrows), which probably represents the EP rather than the hyperintense zone of the bone margins (a). The zone is anatomi-cally distinct and functionally represents the EP, as it is sharply demarcated from the bone and the nucleus pulposus by being hypointense by at least 60–100 U. The time–intensity curve of this zone is also distinct from the neighbouring bone and nucleus pulposus. Anatomic alterations of this zone seen in MRI were seen to effect substantial changes in the diffusion pattern of the disc

492.2 Assessment of Status of End Plate and Diffusion in Degenerative Disc Disease
changes were usually present. Type V EP involves more extensive damage occupying up to 50% of the EP area and was always associated with sub-chondral changes. Type VI EP represented complete EP damage with gross irregularity or sclerosis. Depending on the severity of EPD, an EP score was given to denote the extent of damage of each EP (Fig. 2.2.2) and a “Total End Plate Damage Score (TEPS)” was derived for each disc by adding up the score of both end plates (EPs).
The TEPS has a good correlation to the incidence of DDD (Fig. 2.2.3) [51]. The incidence of DDD was only 12% when the TEPS was below 4 and progres-sively increased to 90% when the TEPS was 11 (Trend Chi square, p < 0.001). TEPS had an overriding influ-ence on degeneration with significant correlation at 1% level irrespective of the level of the disc or the age of the patient. Irrespective of age, discs were healthy when the EPs were intact, and were degenerated when
EPs were damaged. This explains the frequent obser-vation of elderly patients having “young discs” and vice versa.
The correlation between TEPS and incidence of DDD was not linear, but was found to fit into a logistic curve pattern (Fig. 2.2.3). The incidence of DDD was low till a score of six was achieved, but then rapidly increased for each unit increase in TEPS with most of the disc being degenerated when a score of nine was achieved. The findings indicate that the risk of DDD was low in the presence of a normal EP (Type 1), thin-ning of EP (Type II) or only focal disc marrow contacts (Type III). Focal disc marrow contacts produce only patchy changes adjacent to the marrow contact zones with no major alteration in the matrix or the diffusion pattern of the disc (Fig. 2.2.4). DDD increased sub-stantially when the EP showed macrobreaks (Type IV, V and VI).
Fig. 2.2.2 This figure shows six varieties of end plates (EPs) according to severity of damage. Type I is a normal EP and is seen as an uninterrupted hypo-intense band and symmetrically concave. Type II is an EP with areas of thinning either in the centre or periphery; no obvious break is visualized. Type III is an EP that shows focal defects with established disc marrow contact. The contour of the EP is maintained and there is no sub-chondral bone (SCB) change. Type IV EPs have breaks less than 25% with sub-chondral depression. Modic changes are usually present around the node. Type V are larger EP defects occupying up to 50% of the EP with associated modic changes. Type VI EPs have extensive damage involving almost the entire EP

50 S. Rajasekaran
Diffusion and Nutrition
The intervertebral discs are the largest avascular struc-tures in the body and depend entirely on diffusion from blood vessels at the periphery for supply of essential nutrients for cellular activity and removal of metabolic wastes. EP plays an important role not only in control-ling diffusion but also in preventing osmotically active proteoglycans (which are essential for hydration of the discs) from leaving the discs. Small solutes, such as oxygen, glucose and sulphate, are also transported into the discs chiefly by diffusion [63] and their concentra-tion is maximal in the periphery and gradually decreases towards the centre.
Diffusion of discs was initially studied by measuring hydrogen wash out [64], using radioactive [65–67] or fluorescent tracers [68] and measuring intra disc nitrous oxide administered during anaesthesia by inserting the microelectrodes into the disc during surgery [70]. The paucity of methods to assess the status of the EP in vivo by a non-intervention method was one of the serious handicaps limiting our understanding of the physiology of nutrition in health and its alteration in disease. In recent years, post-contrast MRI has been widely used as a non-invasive means of studying transport into the discs in animals and humans in vivo [26, 27, 51]. An increase in signal intensity (SI) in the discs following intravenous injection of a non-ionic contrast (gadodi-amide) can be used to measure the amount of diffusion. The non-invasive nature of this technique and the pos-sibility of calculating enhancement in various regions of interest of the spine over different periods of time allowed interesting opportunities to study disc diffusion
Fig. 2.2.3 Logistic curve was constructed to infer the influence of total end plate damage score (TEPS) on degenerative disc disease (DDD) over the various values of TEPS. The curve had a good fit with correlation coefficient of R > 0.9 and the curve formula show-ing the association was y > a/(1 + b*exp(−cx)); Coefficient data: (a > 5.187; b > 189.391; c > 0.859). It is seen that the incidence of DDD was negligible in patients with a TEPS score of less than four and then slowly rising till six. The curve showed a steep response till the score of nine after which there was an asymptote indicating that most discs were degenerated by the time the score was nine. The curve indicated that the critical TEPS score was six beyond which the incidence of DDD was very high
3.9 5.0 6.1 7.3 8.4 9.5 10.7
DD
D (
as P
firr
man
Gra
din
g)
Logistic Curve For Influence of TEPS on DDD
TEPS
R = 0.9
5.40
4.60
3.80
3.00
2.20
1.40
0.60
Fig. 2.2.4 The integrity of the end plate is important for the health of lumbar discs. However, minor disruptions with only focal disc marrow contacts do not result in major alterations in diffusion or disc degeneration. Here, there is a focal end plate damage in the superior end plate of L4 (a). Immediately after
the dye injection, there is an increase with intensity highlighting the disc marrow contact at the region of the end plate damage (b). At two hours (c), six hours (d) and twelve hours (e) the alteration in diffusion is found to be restricted to the area of end plate damage with normal diffusion in the remaining areas
Precontrast 10 min 2 Hrs 6 Hrs 12 Hrs
L4 L4 L4 L4 L4
a b c d e

512.2 Assessment of Status of End Plate and Diffusion in Degenerative Disc Disease
in detail. Following a intravenous injection of gadodi-amide (0.3 mmol/kg), the vertebral body (VB) and sub-chondral bone (SCB) attained peak enhancement at 10 min, and the EP attained peak enhancement at 2 h subsequently by the Peripheral Nucleous Pulposus (PNP) at 6 h and Central Nucleous Pulposus at 6–12 h.
This phenomenon was termed as “diffusion march” and was found to be an important characteristic of a normal disc with an intact EP. The EP zone achieved enhancement only after a delay at 2 h (EP delay). Frequently, the increase in intensity was seen visually from 2 h as bright bands of enhancement parallel to the EP, which gradually widened towards the centre. The findings allowed identification of the EP breaks in vivo. Rajasekaran et al. [51] reported that diffusion in an intact EP is characterized by maintenance of the diffu-sion march, the presence of EP delay and the absence of enhancement spikes in the areas of PNP. In contrast, minor break in the zone is characterized by the pres-ence of enhancement spikes in the PNP even in the 10 min sequence.
Several alterations in diffusion pattern have been identified depending upon the severity of damage to the EPs (Fig. 2.2.5 and Table 2.2.1). The diffusion pat-tern was normal (Pattern A) if uninterrupted smooth diffusion bands parallel to the EP were noticed at 2 h and slowly progressing to the central nucleus pulposus (CNP). Measurement of SI at various zones also con-firmed the presence of “diffusion march” phenomenon and “EP delay” [51]. Pattern B diffusion had diffusion spikes across the EP, enhancing the disc marrow con-tact zones. The PNP at the site of the break showed enhancement even at 10 min, but diffusion band over the other areas was intact and there was no pooling inside the matrix. Pattern C diffusion was associated with defects with subchondral bone depression in the EP and had pooling restricted to the area of defect. The diffusion bands were maintained at other areas and there was no pooling in the CNP. Pattern D diffusion had more extensive defects where the pooling of the dye extended from the subchondral defect to the PNP and areas of the CNP. Patchy areas of normal diffusion
pattern were still seen. Pattern E diffusion had a com-plete loss of normal diffusion and there was complete pooling occupying the entire CNP.
Pooling of the dye in the nucleus pulposus results from the leak of the contrast through large disc marrow contact channels and vascularization of the disc matrix. This represents a pathological state and must not be confused with increased nutrition. Vascularization of the disc has been found to be associated with autoim-mune reactions, accumulation of immunoglobulins and destruction of NP [31, 69]. Pooling of the dye in NP also strongly indicates a destroyed matrix and can be considered as a critical radiological sign to confirm irreversible degeneration. It also probably indicates an altered milieu interior with altered nutritional path-ways which will not support biological treatment. Patients chosen for biological therapies must be care-fully selected on the basis of the status of the EP and the nutrition. Discs with a TEPS of six and above and discs showing gross pooling of the dye in the NP may not be suitable for biological or regenerative therapies (Fig. 2.2.6).
Conclusions
Damage to the EP appears to be the initiating factor for DDD both by altering the mechanical environment and affecting the nutritional pathways. The EP score that assesses the damage to the EPs in plain MRI studies has been shown to have a good correlation in DDD, irrespective of the level or age of the patient [51]. A total EP score of six appears to be critical, beyond which there is a high incidence of degeneration. Similarly, the post-contrast MRI studies offer the pos-sibility of assessing the status of diffusion, which in turn reflects the status of the nutritional pathways. A TEPS of more than six and “gross pooling of dye” in the NP represents structural failure and altered nutri-tion and may indicate an environment unsuitable for biological treatment and regenerative therapies.

52 S. Rajasekaran
Diffusion Patterns in Serial Post - Contrast MRI
Pre-contrast
Pattern A
Pattern B
Pattern C
Pattern D
Pattern E
2 hours 6 hours 12 hours

532.2 Assessment of Status of End Plate and Diffusion in Degenerative Disc Disease
Table 2.2.1 Various patterns of diffusion in post-contrast MRI
Patterns Diffusion characteristics Status of EP
A Uninterrupted uniform band of diffusion EP delay and diffusion march presentNo enhancement spikes or pooling
Normal
B Areas of disc marrow contact Normal diffusion band maintained in other areasNo gross changes in the diffusion pattern
Focal breaks
C Focal pooling in PNP at site of defect Diffusion band is affected at defect level onlyNo pooling inside CNP
Minimal EP damage
D Focal pooling within the defect and extending into the CNPEP delay and diffusion march is altered
Moderate EP damage
E Totally abnormal diffusion pattern with gross pooling in CNPNo diffusion bands visualized Total EP damage
PNP peripheral nucleus pulposus; CNP central nucleus pulposus
• TEPS 7 and above• Diffusion pattern D or E
• TEPS 6 and below• Diffusion pattern A or B
FusionArthroplasty
Motion preservation
Biological treatment
Physical therapy
Fig. 2.2.6 The spectrum of treatment available for symptomatic DDD. Biological treatment and regenerative medicine therapies would be suitable for discs with a TEPS score less than six and with a diffusion pattern of A and B, which indicate good nutritional status. Motion preservation techniques with distraction and unloading the disc have also showed good results. The above therapy would probably fail in discs with established degeneration or in discs with a TEPS of seven and more or a diffusion pattern of (C, D) or E. They would probably require arthroplasty or fusion
Fig. 2.2.5 Five visually distinguishable diffusion patterns were observed in serial post contrast MRI. Pattern A represented nor-mal diffusion pattern observed in healthy discs with intact end plates. The diffusion bands were uninterrupted and parallel to the end plates and slowly progressed to the central nucleus pul-posus. No abnormal disc marrow contacts were seen. Pattern B was seen in discs with focal end plate defects with patent disc marrow contacts which became very prominent in 2 h post con-trast pictures. The typical diffusion bands were seen in the rest of the areas and there was no abnormal pooling of the dye.
Pattern C was seen in defects with involvement of the sub-chondral bone and large disc marrow contacts. Here there was pooling of the dye at the region of the defect but the diffusion bands were maintained in the other areas. There was no leakage of the dye to the centre of the nucleus pulposus. Pattern D was associated with pooling of the dye in the peripheral nucleus pulposus by 2 h extending into small areas of the central nucleus pulposus subsequently. Pattern E indicated a total disruption of the disc and the entire disc space was filled with the dye even by 10 min

54 S. Rajasekaran
References
1. Kauppila LI (1997) Prevalence of stenotic changes in arter-ies supplying the lumbar spine. A postmortem angiographic study on 140 subjects. Ann Rheum Dis 56:591–595
2. Kurunlahti M, Tervonen O, Vanharanta H et al (1999) Association of atherosclerosis with low back pain and the degree of disc degeneration. Spine 24:2080–2084
3. Kawaguchi Y, Osada R, Kanamori M et al (1999) Association between an aggrecan gene polymorphism and lumbar disc degeneration. Spine 24:2456–2460
4. Roughley PJ, Alini M, Antoniou J (2002) The role of proteo-glycans in ageing, degeneration and repair of the interverte-bral disc. Biochem Soc Trans 30:869–874
5. Annunen S, Paassilta P, Lohiniva J et al (1999) An allele of COL9A2 associated with intervertebral disc disease. Science 285:409–412
6. Takahashi M, Haro H, Wakabayashi Y et al (2001) The asso-ciation of degeneration of the intervertebral disc with 5a/6a polymorphism in the promoter of the human matrix metal-loproteinase-3 gene. J Bone Joint Surg Br 83:491–495
7. Ishihara H, McNally DS, Urban JPG et al (1996) Effects of hydrostatic pressure on matrix synthesis in different regions of the intervertebral disk. J Appl Physiol 80:839–846
8. Lotz JC, Chin JR (2000) Intervertebral disc cell death is dependent on the magnitude and duration of spinal loading. Spine 25:1477–1482
9. Lotz JC, Hsieh AH, Walsh AL et al (2002) Mechanobiology of the intervertebral disc. Biochem Soc Trans 30:853–858
10. MacLean JJ, Lee CR, Grad S et al (2003) Effects of immo-bilization and dynamic compression on intervertebral disc cell gene expression in vivo. Spine 28:973–981
11. Adams MA, Freeman BJC, Morrison HP, Nelson IW, Dolan P (2000) Mechanical initiation of intervertebral disc degeneration. Spine 25:1625–1636
12. Hutton WC, Elmer WA, Boden SD et al (1999) The effect of hydrostatic pressure on intervertebral disc metabolism. Spine 24:1507–1515
13. Hutton WC, Toribatake Y, Elmer WA et al (1998) The effect of compressive force applied to the intervertebral disc in vivo: a study of proteoglycans and collagen. Spine 23: 2524–2537
14. Hutton WC, Yoon ST, Elmer WA et al (2002) Effect of tail suspension (or simulated weightlessness) on the lumbar intervertebral disc: study of proteoglycans and collagen. Spine 27:1286–1290
15. Sauerland K, Raiss RX, Steinmeyer J (2003) Proteoglycan metabolism and viability of articular cartilage explants as modulated by the frequency of intermittent loading. Osteoarthritis Cartilage 11:343–350
16. Walsh AJ, Lotz JC (2004) Biological response of the inter-vertebral disc to dynamic loading. J Biomech 37:329–337
17. Goel VK, Monroe BT, Gilbertson LG et al (1995) Interlaminar shear stresses and laminae separation in a disc. Spine 20:689–698
18. Lu YM, Hutton WC, Gharpuray VM (1996) Do bending, twisting, and diurnal fluid changes in the disc affect the pro-pensity to prolapse? A viscoelastic finite element model. Spine 21:2570–2579
19. Natarajan RN, Andersson GBJ (1999) The influence of lum-bar disc height and cross-sectional area on the mechanical response of the disc to physiologic loading. Spine 24: 1873–1881
20. Kim Y (2000) Prediction of peripheral tears in the annulus of the intervertebral disc. Spine 25:1771–1774
21. Antoniou J, Goudsouzian NM, Heathfield TF et al (1996) The human lumbar endplate: evidence of changes in biosyn-thesis and denaturation of the extra-cellular matrix with growth, maturation, ageing, and degeneration. Spine 21: 1153–1161
22. Buckwalter JA (1982) Fine structural studies of the human intervertebral disc. In: White AA, Gorden SL (eds) Idiopathic low back pain. CV Mosby, St. Louis, pp 108–143
23. Eyre DR (1988) Collagens of the disc. In: Ghosh P (ed) The biology of the intervertebral disc, Vol. I. CRC, Boca Raton, FL, pp 171–188
24. Adams MA, Roughley PJ (2006) What is Intervertebral Disc Degeneration, and What Causes It? Spine 31:2151–2161
25. Boos N, Weissbach S, Rohrbach H, Weiler C, Spratt KF, Nerlich AG (2002) Classification of age-related changes in lumbar intervertebral discs. Spine 27:2631–2644
26. Rajasekaran S, Naresh Babu J, Arun R et al (2004) ISSLS prize winner. A study of diffusion in human lumbar discs. Spine 29:2654–2667
27. Rajasekaran S, Naresh-Babu J, Murugan S (2007) Review of postcontrast MRI studies on diffusion of human lumbar discs. J Magn Reson Imaging 25(2):410–418. Review
28. Videman T, Sarna S, Battie MC et al (1995) The long-term effect of physical loading and exercise lifestyles on back-related symptoms, disability and spine pathology among men. Spine 20:699–709
29. Roberts S, Caterson B, Evans H et al (1994) Proteoglycan components of the intervertebral disc and cartilage endplate: an immunolocalisation study of animal and human tissues. Histochem J 26:402–411
30. Tanaka M, Nakahara S, Inoue H (1993) A pathologic study of discs in the elderly. Separation between the cartilaginous endplate and the vertebral body. Spine 18:1456–1462
31. Satoh K, Konno S, Nishiyama K et al (1999) Presence and distribution of antigen-antibody complexes in the herniated nucleus pulposus. Spine 24:1980–1984
32. Gruber HE, Hanley EN Jr (2003) Recent advances in disc cell biology. Spine 28:186–193
33. Moore RJ, Vernon-Roberts B, Fraser RD et al (1996) The origin and fate of herniated lumbar intervertebral disc tissue. Spine 21:2149–2155
34. Vernon-Roberts B (1992) Age-related and degenerative pathology of intervertebral discs and apophyseal joints. In: Jayson MIV (ed) The lumbar spine and back pain, 4th edn. Edinburgh, Churchill Livingstone, pp 17–41
35. Crean JK, Roberts S, Jaffray DC et al (1997) Matrix metal-loproteinases in the human intervertebral disc: role in disc degeneration and scoliosis. Spine 722:2877–2884
36. Goupille P, Jayson MI, Valat JP, Freemont AJ (1998) Matrix metalloproteinases: the clue to intervertebral disc degenera-tion? Spine 23:612–626
37. Roberts S, Caterson B, Menage J et al (2000) Matrix metal-loproteinases and aggrecanase: their role in disorders of the human intervertebral disc. Spine 25:3005–3013

552.2 Assessment of Status of End Plate and Diffusion in Degenerative Disc Disease
38. Weiler C, Nerlich AG, Zipperer J et al (2002) SSE Award Competition in Basic Sciences: expression of major matrix metalloproteinases is associated with interverte-bral disc degeneration and resorption. Eur Spine J 11: 308–320
39. Yoon ST, Park JS, Kim KS et al (2004) ISSLS prize winner: LMP-1 upregulates intervertebral disc cell production of proteoglycans and BMPs in vitro and in vivo. Spine 29:2603–2611
40. Takegami K, An HS, Kumano F et al (2005) Osteogenic protein-1 is most effective in stimulating nucleus pulposus and annulus fibrosus cells to repair their matrix after chon-droitinase ABC-induced in vitro chemonucleolysis. Spine J 5:231–238
41. Li X, Leo BM, Beck G et al (2004) Collagen and proteogly-can abnormalities in the GDF-5-deficient mice and molecu-lar changes when treating disk cells with recombinant growth factor. Spine 29:2229–2234
42. Kang JD, Stefanovic-Racic M, McIntyre LA et al (1997) Toward a biochemical understanding of human interverte-bral disc degeneration and herniation. Contributions of nitric oxide, interleukins, prostaglandin E2 and matrix metallopro-teinases. Spine 22:1065–1073
43. An HS, Takegami K, Kamada H et al (2005) Intradiscal administration of osteogenic protein-1 increases interverte-bral disc height and proteoglycan content in the nucleus pul-posus in normal adolescent rabbits. Spine 30:25–31; discussion-2
44. Nishida K, Kang JD, Gilbertson LG et al (1999) Modulation of the biologic activity of the rabbit intervertebral disc by gene therapy: an in vivo study of adenovirus-mediated transfer of the human transforming growth factor beta 1 encoding gene. Spine 24:2419–2425
45. Paul R, Haydon RC, Cheng H et al (2003) Potential use of Sox9 gene therapy for intervertebral degenerative disc dis-ease. Spine 28:755–763
46. Wallach CJ, Sobajima S, Watanabe Y et al (2003) Gene transfer of the catabolic inhibitor TIMP-1 increases mea-sured proteoglycans in cells from degenerated human inter-vertebral discs. Spine 28:2331–2337
47. Zhang YG, Guo X, Xu P et al (2005) Bone mesenchymal stem cells transplanted into rabbit intervertebral discs can increase proteoglycans. Clin Orthop 430:219–226
48. Sakai D, Mochida J, Yamamoto Y et al (2003) Transplantation of mesenchymal stem cells embedded in Atelocollagen gel to the intervertebral disc: a potential therapeutic model for disc degeneration. Biomaterials 24:3531–3541
49. Sakai D, Mochida J, Iwashina T et al (2005) Differentiation of mesenchymal stem cells transplanted to a rabbit degener-ative disc model: potential and limitations for stem cell ther-apy in disc regeneration. Spine 30:2379–2387
50. Cheung KM, Ho G, Leung VY et al (2005) The effect of severity of disc degeneration on mesenchymal stem cells’ ability to regenerate the intervertebral disc: a rabbit model. Eur Cell Mater 10(Suppl 3):45
51. Rajasekaran S, Venkatadass K, Naresh Babu J, Ganesh K, Shetty AP (2008) Pharmacological enhancement of disc dif-fusion and differentiation of healthy, ageing and degenerated disc; results from invivo serial post contrast MRI studies in 365 human lumbar disc. Eur Spine J 17:626–643
52. Buckwalter JA (1995) Spine update: ageing and degenera-tion of the human intervertebral disc. Spine 20:1307–1314
53. Martin MD, Boxell CM, Malone DG (2002) Pathophysiology of lumbar disc degeneration: a review of the literature. Neurosurg Focus 13:1–6
54. Nachemson AL (1992) Newest knowledge of low back pain: a critical look. Clin Orthop 279:8–20
55. Natarajan RN, Ke JH, Andersson GBJ (1994) A model to study the disc degeneration process. Spine 19:259–265
56. Stairman JW, Holm S, Urban JPG (1991) Factors influenc-ing oxygen concentration gradients in the intervertebral disk: a theoretical analysis. Spine 16:444–449
57. Urban JPG, Maroudas A (1979) Measurement of fixed charge density and partition coefficients in the intervertebral disc. Biochim Biophys Acta 586:166–178
58. Ibrahim MA, Haughton VM, Hyde JS (1995) Effect of disk maturation on diffusion of low molecular weight gadolinium complexes:An experimental study in rabbits. Am J Neuroradiol 16:1307–1311
59. Ibrahim MA, Jesmanowicz A, Hyde JS et al (1994) Contrast enhancement of normal intervertebral disks: time and dose dependance. Am J Neuroradiol 15:419–423
60. Nguyen CM, Haughton VM, Papke RA, An H, Censky SC (1998) Measuring diffusion of solutes into intervertebral disks with MR imaging and paramagnetic contrast medium. Am J Neuroradiol 19:1781–1784
61. Roberts S, Menage J, Urban JP (1989) Biochemical and structural properties of the cartilage end-plate and its rela-tion to the intervertebral disc. Spine 14:166–174
62. Modic MT, Steinberg PM, Ross JS et al (1988) Degenerative disk disease: assessment of changes in vertebral body mar-row with MR imaging. Radiology 166:193–199
63. Ishihara H, Urban JP (1999) Effects of low oxygen concen-trations and metabolic inhibitors on proteoglycan and pro-tein synthesis rates in the intervertebral disc. J Orthop Res 17:829–835
64. Ogata K, Whiteside LA (1981) 1980 Volvo Award Winner in Basic Science Nutritional pathways of the intervertebral disc. An experimental study using hydrogen washout tech-nique. Spine 6:211–216
65. Urban JP, Holm S, Maroudas A (1978) Diffusion of small solutes into the intervertebral disc: as in vivo study. Biorheology 15:203–221
66. Adams MA, Hutton WC (1986) The effect of posture on diffusion into lumbar intervertebral discs. J Anat 147: 121–134
67. Katz MM, Hargens AR, Garfin SR (1986) Intervertebral disc nutrition diffusion versus convection. Clin Orthop Relat Res 210:243–245
68. Roberts S, Urban JPG, Evans H et al (1996) Transport prop-erties of the human cartilage endplate in relation to its com-position and calcification. Spine 21:415–420
69. Palmgren T, Gronblad M, Virri J et al (1999) An immunohis-tochemical study of nerve structures in the annulus fibrosus of human normal lumbar intervertebral discs. Spine 24: 2075–2079
70. Urban MR, Fairbank JC, Etherington PJ, Loh FRCA L (2001) Electrochemical measurement of transport into scoli-otic intervertebral discs in vivo using nitrous oxide as a tracer. Spine 26:984–990

57M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_2.3, © Springer-Verlag Berlin Heidelberg 2010
Introduction
The vast majority of patients presenting to physicians with low back pain complaints are treated successfully in a nonoperative fashion. The medical care and treat-ment of the low back pain patient population are labor intensive with a low patient visit to surgery ratio. A successful and efficient spine surgery practice requires screening a large volume of patients before a surgical case is identified. The spine surgeon is often over-whelmed by a large quantity of referrals, leading to the task of having to actively manage both large numbers of nonoperatively and surgically treated low back patients. These patients generate large numbers of phone calls, follow-up visits, prescription refills, dis-ability forms for Worker’s Compensation, and personal injury claims, representing a significant expenditure of physician and staff time. In this environment, skilled physician extenders including physician assistants (PAs), physical therapists (PTs), and advanced nurse practitioners (APNs) are extremely effective in helping to successfully meet the increased requirements of low back patient management. This team approach frees up physician time and aid in the reduction of the wait-ing periods for specialized spine care. Furthermore, the additional attention that patients receive, as opposed to care delivered only by a single physician, is posi-tively perceived by patients as comprehensive and thorough, high-quality healthcare.
There are several allied health professional catego-ries. Some of them are properly trained and certified to
perform, under supervision, many of the routine ser-vices that physicians would otherwise have to provide directly. They can substantially add to physician pro-ductivity, especially in a practice that sees a lot of man-aged care patients, and therefore, can function as physician extenders. Physician extenders include reg-istered nurses, advanced nurse practitioners, physician assistants, physical therapists, and athletic trainers. How each of these healthcare professionals can function at a low back practice is dictated by state and local licen-sure and credentialing statutes. While all can function in the clinic, assisting in surgery is primarily limited to physician’s assistants and certified surgical assistants. Whether their services can be reimbursed by insurance varies both within insurance policies and state medi-ated reimbursement policy. This discussion will focus on the role of nurses, physician assistants, and physio-therapists, assessing their function in the clinical and surgical environment of a spine surgery practice.
Allied Healthcare Professionals
Nursing
The oldest sense of “nursing” in the English language can be traced back to the fourteenth century and referred to a woman employed to suckle and care for a younger child. By the fifteenth century, nursing had evolved into the act of looking after another, not necessarily meaning a woman looking after a child [1]. Prior to the founda-tion of modern nursing, nuns and the military often pro-vided nursing-like services [2]. Florence Nightingale, working to improve conditions of soldiers in the Crimean War, laid the foundation for professional
The Role of Physician Extenders in a Low Back Pain Practice
Michael R. Zindrick, Michael N. Tzermiadianos, Cary R. Templin, and Raymond E. Hines III
M. R. Zindrick (*) Hinsdale Orthopedic Associates, Hinsdale, IL 60521, USA e-mail: [email protected]
2.3

58 M. R. Zindrick et al.
nursing as we know it today [3]. Nursing has grown to be one of the most critical aspects of patient care and has become a government regulated profession, requiring appropriate licensure and credentialing. New Zealand was the first country to regulate nurses nationally in 1901. In the United States (US), North Carolina was the first state to pass a nursing licensure law in 1903.
Nurses are often placed in key management roles within health services and hold research posts at uni-versities. The modern era has seen the development of several types of nursing degrees. With additional train-ing, advance degrees to the nursing are available including nurse clinician and nurse practitioner cate-gories. Each degree allows for more extensive clinical responsibilities, even approaching those of the primary care physician.
Physician Assistants
The shortage and uneven distribution of primary care physicians in the United States during the mid-1960s led to the creation of the first class of PAs in 1965. That class put together selected navy corpsmen who had received considerable medical training during their military service and during the war in Vietnam but had no comparable civilian employment. The curriculum of the PA program was based in part on the experience of the fast-track training of doctors during World War II [4, 5].
Physician Assistants are healthcare professionals licensed to practice medicine in the United States, under physician supervision. They are trained in inten-sive education programs accredited by the Commission on Accreditation of Allied Health Education Pro-grams (previously the American Medical Association’s Committee on Allied Health Education and Accredi-tation). Common services provided by a PA include taking medical histories and performing physical examinations, ordering and interpreting lab tests, diag-nosing and treating illnesses, assisting in surgery, pre-scribing and/or dispensing medication, and counseling patients regarding diagnosis and treatment options. Physician Assistants can prescribe medications in forty-nine states [6].
In the United States, the PA model has proven to be a cost-effective way to train quality primary care pro-viders with a high degree of acceptance of the PA role
by patients and other healthcare providers. Several countries including the United Kingdom, Scotland, Canada, the Netherlands, Taiwan, South Africa, and Ghana are exploring the concept of the physician assis-tant as a way to quickly and efficiently train and employ autonomous and flexible health workers to address their nation’s healthcare needs [7].
Because of their close working relationship with physicians, PAs are educated in the medical model designed to complement physician training. Upon grad-uation, physician assistants take a national certification examination developed by the National Commission on Certification of PAs in conjunction with the National Board of Medical Examiners. To maintain their national certification, PAs must log 100 h of continuing medi-cal education every 2 years and sit for a recertification every 6 years. Graduation from an accredited physi-cian assistant program and passage of the national cer-tifying exam are required for state licensure.
Physician assistants can function to assist in patient care in both the clinic based and surgical environment. Almost universally their services are reimbursed ade-quately to cover the cost of their salaries and benefit packages.
Physiotherapists
The use of physiotherapists to see orthopedic outpa-tients was first described in 1989 [8]. In 1994, Hourigan and Weatherley reported a system to triage back pain by physiotherapists that eventually became widespread in United Kingdom and other countries [9]. According to this system, acute back pain outpatients are seen initially by a trained physiotherapist. The physiotherapist takes a careful history, performs a physical and radiological examination, and refers on to the spine surgeon only prob-lematic cases and those potentially in need of surgery. Initially, all cases were discussed in resume with the con-sultant surgeon. However, as the physiotherapists became more experienced, the surgeon, in most cases, found that he/she was only sanctioning what has been proposed.
Certified Athletic Trainers
Certified athletic trainers help move patients faster through the appointment and treatment process, thereby

592.3 The Role of Physician Extenders in a Low Back Pain Practice
increasing physician productivity and efficiency and allowing the office to treat more patients in the same amount of time. They can reduce re-injury rates through patient instruction, reduce recovery time from nonsur-gical injuries, and aid in the rehabilitate musculoskel-etal injuries. Athletic training services are reimbursable by many insurance companies, and services are either directly billed or billed incident to physician services.
Physician Extenders’ Tasks
Assisting in the Office
In an ideal setting, the low back pain patient/physician encounter would be limited to reviewing the pertinent medical history, the pertinent physical examination, the pertinent radiographic and medical tests, and spending the majority of time discussing with the patient the medical problem at hand and potential treatment modalities. The time requirements necessary to obtain and interpret the patient’s pertinent medical history, physical examination, radiographic findings and medical tests are significant and can be over-whelming to daily practice patterns. Obtaining this information from the patient and organizing it prior to the physician’s visit with the patient is one of the most valuable functions that a physician extender can pro-vide in spine practice. By identifying pertinent find-ings which require further study (MRI, discogram, etc.), the practice efficiency is enhanced.
Physician extenders can also be used for telephone triage and assistance with the scheduling of patients’ appointments. In busy practices with high telephone traffic, the PAs and NPs can assess the patient’s prob-lem and determine the urgency for the visit.
Initial Evaluation
History: The physician extender can facilitate the patient filling out intake forms while obtaining and reviewing a thorough past medical history. Important points of this process include determining associated diseases, medications, prior surgeries or interventions (such as physical therapy or injection therapy), and all pertinent information regarding patient’s current chief complaints and organizing this for the physician in a
standard fashion. The use of standard entry forms that include all of this information including a pain draw-ing is the basic requirement for the practice, and the physician extender can help to streamline this process for the patient and the physician.
Physical examination: Qualified physician extend-ers are skilled and competent to perform a thorough neurological and musculoskeletal physical examina-tion. With pertinent physical findings provided by the assistant at the initial encounter, the physician is able to focus his or her time on the physical examination as it related to the patient’s specific complaints. Again, a standardized office form that encompasses the com-plete examination highlighting positive findings is par-amount for increasing efficiency.
Follow-Up Visits
Physician extenders can be effectively used in the clin-ical practice to see patients for follow-up clinic visits. Included in these visit categories are initial postopera-tive visits and follow-ups during ongoing nonoperative management. Follow-up visits to review test results (MRI, discogram, etc.) and outline treatment plans that may include surgical intervention are best handled by the physician, although the assistant can help to further explain the physician’s discussion with the patient if the patient has extensive questions.
In Hospital Tasks
Most hospitals in the United States will credential nurses and physician assistants to function within the hospital environment. The assistant’s interaction with the patient may include acute inpatient care and assis-tance in surgical procedures.
Physician extenders can assist in rounds on a daily basis, i.e., seeing patients and reviewing laboratory and radiographic data, while being legally and clini-cally qualified to write chart notes and orders. Most institutions require, however, close physician supervi-sion of these functions, including daily cosigning of all orders and notes. To work effectively, open and timely communication must exist between the physician and the assistant. It is imperative that the physician main-tains communication with the patient in order that the

60 M. R. Zindrick et al.
patient does not perceive the assistant’s presence as physician’s neglect.
Hospital Medical Records
Credentialed, qualified physician extenders are capa-ble, under physician supervision, to prepare most of the hospital required medical reports. These include histories and physicals, consultations, and discharge summaries. Most institutions will allow these to be dictated by credentialed health care professional such as APNs and PAs, while close physician supervision and cosigning of these documents are required.
Back Pain Clinics and Triage for Back Pain
The realization that one of the key factors that encour-ages acute back pain to become chronic is being off work led to the development of back pain screening clinics, as a system of triage, to reduce long waiting times for diagnosis and treatment. Triage is the medical model of diagnosis used to exclude serious pathology. As triage directs the management pathway, its role is to place the patients into groups at an early stage, iden-tifying those who might benefit from surgery, and fast tracking them, identifying those who will benefit from conservative management and tracking them accord-ingly. Triage deals with identifying “red flags” denot-ing serious spinal pathology and “yellow flags” denoting the psychosocial factors, nerve root pain, cauda equina, and inflammatory disorders. Triage in low back pain clinics is traditionally performed by trained physiotherapists [10]. The introduction of these services, initially in the United Kingdom and subse-quently in other countries, resulted in a reduction in the waiting periods for the specialized spine clinic, and a clinical and economical improvement in the care of those suffering from acute low back pain [11]. A potential disadvantage of this approach is that physio-therapists are less reliable than surgeons when con-ducting physical examination [12, 13].
Assistance in Surgical Procedures
Most institutions in the US require that surgical assis-tants be either other physicians, physician’s assis-tants, or credentialed surgical assistants. The educational
curriculum of PAs includes training in surgical assisting skills, which is recognized by most institutions and cre-dentialing bodies. Nurses, however, are generally not allowed to function in this capacity unless they partici-pate in extra training and are credentialed specifically as surgical assistants. Assistance in surgical procedures is beyond the basic training of registered nurses, nurse clinicians, or nurse practitioners. Physician’s assistants and nurses, once credentialed as surgical assistants, may bill for their services and are recognized by most third-party payers. In this time of shrinking physician reimbursements, income received assisting in the oper-ating room can be substantial and either partially offset or fully cover the costs associated with employing a physician extender. It is this financial incentive that supports the physician’s assistant as a most desirable adjunct member of a health care team managing low back surgical practice in United States.
Other Clinical Tasks
In today’s medical environment, there exists a multitude of patient contact tasks required in providing healthcare. These include dictating and completing the medical record for initial and follow-up office visits, effectively communicating with referring physicians and third-party payers, sorting through and evaluating test results includ-ing laboratory and radiographic studies, returning patient phone calls, coding and submitting physician charges for surgery, hospital consultations and prescription refills. In addition, the paperwork generated by disabil-ity and workers compensation claims is overwhelming, and the physician extender can be instrumental in effi-ciently managing this load.
Though crucial in providing quality healthcare, many of these tasks can be effectively delegated to qualified physician extenders, thereby freeing the phy-sician to perform more of those tasks that he or she is uniquely qualified to perform.
Conclusions
Providing all of the necessary services required in the modern, tightly regulated, healthcare environment, can stretch physician time beyond that which is available.

612.3 The Role of Physician Extenders in a Low Back Pain Practice
Performing all required tasks leaves limited time for direct patient contact. Using a physician extender in a low back practice frees up the physician’s time to focus his/her attention and skills on those patients who require a higher level of care and allow the practice to treat more patients daily. This shortens waiting period for specialized low back pain quality care, enables effi-cient and higher quality physician -patient contact, and possibly affects treatment outcomes. Furthermore, the additional attention the patients receive, when being treated by a medical team as opposed to a single physi-cian, is positively perceived as thorough, comprehen-sive, quality healthcare.
References
1. “Nurse” (1989) The Oxford English Dictionary, 2nd edn. Oxford University, p 603–604
2. Marjie Bloy (2002) Florence Nightingale (1820–1910) available at: http://www.victorianweb.org/history/crimea/florrie.html
3. Nightingale F (1860) Notes on Nursing. What it is and what it is not. New York D. Appleton and Company. Available at: http://digital.library.upenn.edu/women/nightingale/nursing/nursing.html#III
4. American Academy of Physician Assistants. Information about PAs and the PA profession. Available at: www.aapa.org/geninfo1.html
5. American Academy of Physician Assistants 2007–2008 Policy Manual. Alexandra Va
6. The Pew Heath Professions Commission. Charting a course for the twenty first century. Physician Assistants and Managed care. San Francisco UCSF Center for Health Professionals 1998
7. Legler CF, Cawley JF, Fenn WH (2007) Physician assistants: education, practice and global interest. Med Teach 29(1): e22–e25
8. Byles SE, Ling RSM (1989) Orthopaedic out-patients -A fresh approach. Physiotherapy 75:433–437
9. Hourigan PG, Weatherley CR (1994) Initial assessment and follow up by a physiotherapist of patients with back pain referred to a spinal clinic. J R Soc Med 87:213–214
10. Weatherley CR, Hourigan PG (1988) Triage of back pain by physiotherapists in orthopaedic clinics. J R Soc Med 91: 377–379
11. Mofidi A, Sedhom M, O’Shea K, Cassells M, Curley A, Fogarty E, Dowling F (2003) Screening of lower back pain, low back pain clinic. The clinical experience. Ir Med J 96(9): 270–273
12. McCombe PF, Fairbank JC, Cockersole BC et al (1989) 1989 Volvo Award in clinical sciences: reproducibility of physical signs in low-back pain. Spine 14:908–918
13. McCarthy CJ, Gittins M, Roberts C, Oldham JA (2007) The reliability of the clinical tests and questions recommended in international guidelines for low back pain. Spine 32(8): 921–926

Part
Conservative TreatmentIII

65M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_3.1, © Springer-Verlag Berlin Heidelberg 2010
Abbreviations
HRqOl Health related quality of lifelBP low-back painMRI Magnetic resonance imagingNSN Nociceptive spinal neuronRDq Roland disability questionnaireSF36 Short from 36VAS Visual analog scale
low-back pain (lBP) is a frequent problem in the adults of western societies. It affects approximately 80% of the population at some time in life [2] with a point prevalence of 20%. It is also the most frequent diagnosis for work incapacity and disability benefits [16]. Moreover, chronic lBP is responsible for huge medical and compensation expenses. Prevention mea-sures have been developed to modify this unfavorable evolution. However, despite appropriate prevention, the prognosis remains less favorable in a subset of patients who develop a chronic problem with intermit-tent exacerbations.
The purpose of this chapter is:
1. To summarize the natural evolution of nonspecific lBP.
2. To overview the various factors influencing the con-dition to become chronic and evaluate the therapeu-tic strategies capable of hastening the resolution of pain and disability.
Definition
Nonspecific lBP can be defined as any type of lBP after exclusion of serious conditions such as tumors, infections, or spondylo-arthropathies, as well as lBP of nonspinal origin. Unfortunately, this large group is not uniform. Classification into subgroups depends on the conceptualization and management of the condition. Traditionally, the natural course of lBP is considered as a medical biomechanical problem. More recently, the influence of psychologic and social factors has led to the development of a psycho-social model of chronic disease. Finally, a biopsychosocial analysis has been proposed as a paradigm for management [43, 44].
Natural history is an important issue. It can be con-sidered as the gold standard for evaluation of the vari-ous treatment strategies. Its knowledge is also valuable to evaluate correctly the risk factors of passage to chro-nicity and to give the patient appropriate information on prognosis.
Database
Information on natural history is provided by a huge number of epidemiologic studies. For example, in an extensive literature search, Pengel et al. [29] retrieved over 4,000 articles. However, caution is recommended in interpreting the data considering the varied quality of the studies, the wide variety of study designs, and the choice of cohort. As emphasized by Hestbalk et al. [23], the lack of distinction between outcome parameters is another important source of confusion. Results of ques-tionnaires used in the outcome assessments may be biased by erroneous symptoms recall or non response.
Natural Evolution of Nonspecific Low-Back Pain
Michel Benoist and Thibaut Lenoir
M. Benoist (*) University of Paris VII, Hôpital Beaujon, 100 Bd. du Gl. leclerc 92110 Clichy, France e-mail: [email protected]
3.1

66 M. Benoist and T. Lenoir
Moreover and most importantly, there are major cultural, political, and socio-economic differences across coun-tries. Generalization from one country to another is dif-ficult. In summary, while interpreting the data one must keep in mind the limitations of assessing evolution of pain, and of its severity. Therefore and as stated by Anderson [1], “validity and reliability of the data on lBP are uncertain and should be considered approximate.”
Classification as a Function of Time
lBP can be measured as the length of time the patient has experienced pain [27]. It is now generally admitted to distinguish three types of lBP: acute if the pain is shorter than 4 weeks, chronic if the pain lasts more than 3 months, and subacute for pain lasting between 4 weeks and 3 months. This classification is obviously a simplification of reality, but is useful in research and clinical practice. It is also now admitted that pain trans-mission involves four main levels: the nociceptive input coming from the peripheral tissues, the cord, the brain, and the descending inhibitory pathways. Classification as a function of time is based on the neuro-physiologic mechanisms of pain.
Acute nonspecific lBP has a direct relationship with peripheral stimuli. Nociceptive nerve fibers located in the degenerated disk and in other structures of the motion segments (facets, ligaments, and muscles) are physically stimulated through mechanical instability, and chemically by neurogenic and inflammatory medi-ators and by cytokines [14, 31, 35]. Figure 3.1.1 pres-ents a hypothetical and rough sketch of the biologic events leading to the sensitization of nerve terminals
and generation of lBP. Chronic lBP (over 3 months) is, at least in part, dissociated from the peripheral stim-uli. Prolonged pain leads to central sensitization of the central nervous system defined by an increase of the nociceptive spinal neurons excitability (Fig. 3.1.2). There is now evidence that central sensitization of the cord can enable persistent pain states independent of a primary afferent drive. There is also increasing evi-dence that in addition to the spinal cord, the higher cor-tical centers play a role in the CNS central sensitization. Results of functional MRI studies of the brain per-formed in a group of chronic lBP patients have shown on brain mapping an augmentation of central nocicep-tive activity [18]. Subacute nonspecific lBP (between 1 and 3 months) is an important phase, as during this period biopsychosocial impairments begin to develop in relation to the onset of the CNS sensitization due to the prolonged period of peripheral nociceptive activity. Persistence of pain during this period calls for careful interviews and validated questionnaires to identify other problems, psychosocial or work-related [27].
Prognosis of Acute and Subacute Low-Back Pain
Von Korff and Saunders recommended summarizing the available data on short-term course during the first 3 months after the index consultation period
CHRONIC
PAINCentral
sensitization of CNS
permits development
andamplification of
painfulperception
Brain
NSNNociceptor
A delta, C
Corticalnociceptivehyperactivity
Increase ofspinal neurons
excitability
Cord
Fig. 3.1.2 Central sensitization of the central nervous system
Acute non-specific L.B.P
Robotsganglion
Physical stimulation instability
Cytokines
PGE2Bradykin
Small fibers
Substance P
Substance P
Sensitize
Excite
Fig. 3.1.1 Peripheral stimulation of the nerve terminals in acute nonspecific low-back pain (lBP)

673.1 Natural Evolution of Nonspecific Low-Back Pain
corresponding to the acute and subacute phases according to the traditional classification [41].
It was originally considered that 90% of patients with acute lBP recover within 6 weeks irrespective of the type of treatment or without treatment [43]. Such high recovery rates are disclosed in truly acute incident cases. For example, in the study by Coste et al. [11] using an inception cohort design and including 113 patients with less than 72 h pain duration and no lBP in the past, the mean duration of the episode was 8 days and 87% of the patients had recovered by day 30. Only six patients (5%) had not recovered by 3 months. Interestingly, lower SF36 and higher RDq scores were associated with delayed recovery, highlighting the key role of work-related factors and the initial HRqOl in identifying the patients at risk of chronicity very early after the onset of the episode. Pengel et al. [29] have selected 15 studies of prospective design for a system-atic review of lBP prognosis. The inception cohort of participants had lBP for less than 3 weeks. The fol-low-up period was at least 3 months with reports on symptoms, health quality of life, disability, or return to work. Most studies reported that pain and disability decreased rapidly within 1 month of initial levels, fol-lowed by a slow decrease until about 3 months. The pooled mean pain level was 22 at 1 month and 15 at 3 months on a 100 point score with similar numbers for the disability score. Most patients off work with lBP had returned to work within 3 months after which pain and disability remained constant in the two studies with a follow-up beyond 3 months.
Cross-sectional or longitudinal studies including mixed cohorts of patients with primary acute lBP, recent exacerbations of chronic lBP, and sometimes sciatica, which are different conditions, report less favorable outcomes. In a review paper, Von Korff and Saunders [41] summarized the data from five high-quality studies including over 1,000 patients at different stages of the disease during the first 3 months after the index consultation. The percentage of pain-free patients at 1 month was approximately 50%, 30% with mild to moderate pain intensity and 15–20% with severe pain. There was a modest improvement between 1 and 3 months (the subacute period). At 3 months, approxi-mately 60% were pain-free, 20–25% had moderate to severe disability usually accompanied by high intensity pain, and 20–25% had a mild moderate pain intensity.
More pessimistic findings can be disclosed in other studies examining the clinical course of mixed cohorts
of care seeking patients. As an example, in the study by Thomas et al. [36], 48% of the 113 patients were still experiencing disabling lBP evaluated on VAS and Hanover score at 3 months after the initial consultation. In a prospective cohort study of patients seen in pri-mary care, Cherkin et al. [10] used symptom satisfac-tion measures based on patients’ own criteria to assess the clinical course. They found that at 7 weeks, only 67% of patients reported good outcome after the index consultation. In the study reported by Van den Hoogen et al. [38], 15 general practitioners from Amsterdam studied consecutive patients with an acute lPB of recent onset or of exacerbation of chronic back pain. Thirty-five percentage of the 269 patients still experi-enced lBP after 3 months.
This brief summary of a few selected studies exam-ining the natural history of lBP at short-term course indicates a high variability of outcomes ranging from 5 [11] to 48% [36] of patients with persistent lBP. However, it should be noted that most studies indicate a modest improvement between 1 and 3 months. As stated by Roland and Morris [32], the variability of the symptoms between patients, as well as the frequency of the recurrences, complicates the ability to accurately summarize the natural evolution of lBP. In addition, as emphasized above, the choice of cohort and the dif-ferent outcome measures are the main factors explain-ing the variability of prognostic estimates.
As carefully discussed by Van Korff and Saunders [41], there is a hierarchical relation between pain inten-sity, back functioning, disability, and sick leave. Mild recurrent back pain may have little impact on HRqOl, and patient functioning. Patients are occasionally exam-ined with moderate or even high intensity levels of pain with no significant activity limitations. However, mod-erate to severe activity limitations are usually accompa-nied by high-intensity pain levels and reduced work ability.
Prognosis at Long-Term Course: Chronic LBP
Most studies indicate that once established, chronic lBP is persistent in many patients [12]. Chronic lBP can be permanent and is defined as pain present most of the days within a given time frame and/or recurrent with episodic flare-ups of varying duration, frequency, and

68 M. Benoist and T. Lenoir
severity. Obviously, chronic lBP is not a static but a fluc-tuating condition. Intermittent increases can markedly affect affect disability and health-related quality of life.
A recent study of good methodological quality [3] has evaluated for 6 months the evolution of acute lBP of less than 6 weeks duration, and with no back pain in the previous 12 months, in an inception cohort of 100 patients. At 6 months follow-up, 40% had fully recov-ered before 3 months, and 60% had persistent lPP, either continuous (14%) or with recurrent episodes (46%).
Good quality studies have shown that disabling lBP may persist largely over 6 months. In the Manchester study [36] based upon a cross-sectional analysis of 180 patients, disabling lBP persisted in 73% at 1 week, 48% at 3 months, and 42% at 12 months. About a third of the participants were classified as having chronic disabling lBP with related disability at each of the three consultations. In an effort to evaluate the long-term course of primary care patients, Von Korff and Saunders [41] analyzed the results of four studies including their own [4, 28, 30, 42]. long-term extend-ing pain, number, and duration of recurrences, as well as pain intensity and disability, were addressed. The summary of long-term outcomes at 1–2 years follow-up was as follows: Approximately 33% of primary care patients experienced lBP of moderate intensity; 15% reported severe-intensity pain and 20–25% reported substantial activity limitations.
Other studies report different and sometimes more pessimistic outcomes. For example, in the retrospec-tive study of Van Tulder et al. [37] based upon 524 patients, the median duration of symptoms was more than 4 years. A cohort of 1,246 patients with acute lBP generated from 208 community practitioners was followed regularly over 22 months by Carey et al. using valid reliable measures [8]. Ninety six patients had chronic continuous symptoms for 3 months, form-ing the inception cohort of chronic lBP. Two-thirds of patients with chronic lBP at 3 months had disabling chronic symptoms at 22 months.
Hestbalk et al. [23] have reviewed and analyzed 36 studies of long-term course of lBP. Twenty-eight stud-ies were observational, and eight were randomized. Because of the lack of homogeneity of the reviewed studies, meta-analysis was not possible. Results are expressed as ranges of study estimates to evaluate the extent of persistent or recurring symptoms. The overall findings of this review were as follows: between 42 and 75% of subjects still experienced pain after 12
months. Between 3 and 40% were still sick-listed 6 months after inclusion in a study, with relapses of work absence ranging between 26 and 37%. The point prev-alence rates of lBP in persons with previous episodes of lBP range from 14 to 93%, whereas the correspond-ing rates for those without a prior history of lBP range from 7 to 39%, the risk of lBP being twice as high for those with a history of lBP.
Overall, one can summarize very schematically the evolution of chronic lBP at long term as follows: at 12 months, lBP persists in two out of three cases (not always with activity limitations). Relapses occur in over half of the patients, with a new sick listing in approximately one case out of three. Patients must be informed of this possible evolution in order to diminish fear-avoidance and its consequences.
Sick Listing and Return to Work
Absence of work and sick listing have a deleterious effect on natural evolution. Prolonged absence from work makes return to work less likely. Spitzer et al. [34] have shown that approximately half of the patients absent from work more than 6 months return to work; the rate of return to work is even lower for those sick-listed for more than 1 year. Studies have demonstrated that compensation influences prolonged work inca-pacity [19, 26]. Other factors including job satisfac-tion, socioeconomic or psychosocial factors have a decisive influence on return to work. In a 1-year study, Hansson and Hansson [21] have compared work resumption in cohorts of employed patients of six nationalities, sick listed for chronic lBP for at least 3 months. The frequencies of work resumption varied between countries, ranging within the first year from 73% in the Netherlands to 32% in Denmark. Work resumption was principally dependent on psychoso-cial and work-related factors. It was also shown that EUROqOl, a quality of life instrument, was the most powerful predictor of return to work or no return to work, indicating that self-rated health with psycho-logical distress is an important predictor of persistent disability and that work incapacity should not be regarded solely as a biological medical problem [22]. Persistent chronic lBP and sick listing are not lim-ited to employed workers. For example, in a subset of self employed dentists, physicians, and veterinarians,

693.1 Natural Evolution of Nonspecific Low-Back Pain
chronic lBP developed in 23% with insurance claims lasting over 6 months [39].
Who Develops Chronic Back Pain?
Measures of lBP show that chronic nonspecific lBP can be a persistent disabling condition in a substantial proportion of patients. This group, the so-called “tertiary group,” consumes most of the resources.
Heavy physical jobs including lifting, twisting, vibration exposure, or repetitive tasks are associated with acute lBP and tissue injuries. However, the influ-ence of occupational factors on the development of chronicity has not been clearly demonstrated. In the Boeing study [5] it was found that perceptions of work, perceptions of safety and other psycho-social factors played a greater role than all physical measures. Similarly in the expert model developed by Frymoyer and Cats-Baril [17], work environment, psychosocial factors and duration of the current episode were the main predictors of long-term disability. These findings clearly call for a broader approach of the multifaceted aspects of chronic lBP.
Several psychosocial risk factors have been linked to the patient’s persistent pain [2, 5, 9, 25, 44]. These aspects, as well as their clinical relevance and their impact on therapeutic considerations, will be discussed in another chapter. However, these factors do not fully explain the patient’s symptoms in a significant num-ber of individuals. Thomas et al. [36] have developed an interesting model of adverse prognostic factors. They were able to dissociate premorbid factors from episode-specific factors of chronicity. Premorbid fac-tors included history of lBP, dissatisfaction with work, and high psychological distress, confirming the role of psychological and work-related factors. The episode- specific factors included sex (women), radiating leg pain, and widespread pain. This latter factor is impor-tant to consider. Widespread pain is the cardinal feature of fibromyalgia, probably related to an augmentation of central nociceptive activity as shown on brain mapping. Similar findings have been shown on chronic lBP patients without psychosocial problems [18]. A recent study [33] has sought to determine whether recurrent lBP has a different symptomatology in two occupa-tional groups: nurses and administrative workers, and whether in the two occupational groups different
factors are associated with the presence of lBP. Interestingly, in the two groups, occurrence of recur-rent lBP was strongly associated with the presence of complaints in other body regions pointing out of the clinical importance of widespread pain associated with chronic lBP. These findings, discussed in another chapter, suggest the crucial role of the central nervous system in the development of chronicity. They also suggest the existence of a subgroup of chronic lBP patients with central sensitization different from those with a depressive symptomatology.
On the other hand, chronicity could also be linked to the structural pathology of the lower back and to the persistence of the nociceptive input emanating from the degenerative spinal unit. Indications of fusion or non-fusion procedures are based on this assumption. Unfortunately, unlike osteoarthritis of the hip or knee, discal degeneration does not necessarily mean pain. The relation between imaging abnormalities and lBP are discussed in a special chapter. Recently, high-quality studies [7, 13, 15] have shown that a substantial pro-portion of well-selected chronic lBP patients can be successfully treated by surgery. It was also demon-strated that others obtain satisfactory results with an appropriate conservative therapy including an inten-sive multidisciplinary rehabilitation program [20].
As shown in Fig. 3.1.3, while examining a disabled chronic lBP patient, the problem is to differentiate those patients with a dominant influence of central sensitization, whether psycho-social or fibromyalgia-like, from patients for whom persistence of the periph-eral nociceptive input is the principal source of the pain. Structured questionnaires, interviews with care-ful listening, and a good patient–physician relationship
Psycho social Fibromyalgia like
Chronic L.B.P.
Peripheral sensitization persistence of nociceptive input
Central sensitization
Fig. 3.1.3 The decision to operate or not is based on a careful assessment of the various clinical and radiological parameters

70 M. Benoist and T. Lenoir
often enable to detect patients with psychosocial prob-lems who should be directed to rehabilitation. Hopefully, development of biologic methods or imaging strate-gies will be able to identify patients with central sensi-tization without major psycho or social abnormalities or imaging features of hyperstimulation of the periph-eral nerve terminals. As already mentioned, functional MRI of the brain has shown an augmented cerebral pain processing in this category of patients. On the other hand, development of sensitive specific imaging signs or other methods to ascertain the discogenic ori-gin of the pain is mandatory. Prevalence and clinical relevance of endplates changes of Modic I type have been reported and discussed [6, 24, 40, 45]. At present, the decision to operate or not is based on a careful overall clinical assessment of the patient, comprehend-ing the various parameters involved in chronic pain.
Conclusions
Methodological variations including choice of cohort, study designs, outcome measures, as well as the lack of precision in the definition of nonspecific lBP, explain the difficulty in accurately assessing the natu-ral course of lBP. However, a few conclusions and suggestions can be reached as follows:
The course of nonspecific lBP at short and long •term is not as favorable as originally claimed.The relation between pain, back functioning, and •disability is complex. Healthy subjects with moder-ate or even severe pain intensity may have no func-tional limitations, and do not necessarily seek care.All studies confirm the existence of a subset of •chronically disabled sick-listed patients (15–20%) who consume most of the economic resources.General health, individual physical work related, and •various psychosocial factors influence the persis-tence and recurrence of multifaceted chronic lBP.Although no biologic mechanisms have been found •to relate the psychosocial factors to the develop-ment and maintenance of chronic lBP, the role of the central nervous system at the cord and brain lev-els appears crucial.Further studies are needed to validate the existence of •a subgroup of patients without psychosocial or work-related factors, who develop central sensitization similar to that observed in fibromyalgia patients.
Persistence of the peripheral nociceptive input ema-•nating from the degenerated spinal units can also explain continuation of the pain.The difficult therapeutic challenge is to differenti-•ate the different categories of patients.
References
1. Anderson GBJ (1997) The epidemiology of spinal disorders. In: Frymoyer JW (ed) The adult Spine. lippincott-Raven, Philadelphia
2. Anderson GBJ (1999) Epidemiological features of chronic low-back pain. lancet 354:581–585
3. Bakker E, Verhagen A, lucas C et al (2007) Spinal mechani-cal load: a predictor of persistent low-back pain? A prospec-tive cohort study. Eur Spine J 16:933–941
4. Bergquist-Ulmann M, larson U (1977) Acute low-back pain in industry. A controlled prospective study with special ref-erence to therapy and confounding factors. Acta Orthop Scand 170:11–17
5. Bigos SJ, Battie MC, Spengler DM et al (1991) A prospec-tive study of work perception and psychosocial factors affecting the report of back injury. Spine 16:1–6
6. Braithwaite J, White J, Salfuddin A et al (1998) Vertebral endplate changes on lumbar spine MRI. Correlation with pain reproduction on lumbar discography. Eur Spine J 7:363–368
7. Brox JI, Sorensen R, Friis A et al (2003) Randomized con-trol trial of lumbar instrumented fusion and cognitive inter-vention and exercises in patients with chronic low-back pain and disc degeneration. Spine 28:1913–1921
8. Carey J, Garrett J, Jackman A (2000) Beyond the good prog-nosis. Examination of an inception cohort of patients with chronic low-back pain. Spine 25:115–120
9. Carragee EJ (2001) Psychological and functional profiles in select subjects with low-back pain. Spine J 1:198–204
10. Cherkin D, Deyo R, Street J et al (1996) Predicting outcomes for back pain seen in primary care using patients’ own crite-ria. Spine 21:2900–2907
11. Coste J, lefrancois G, Guillemin F et al (2004) Prognosis and quality of life in patients with acute low-back pain: insights from a comprehensive inception cohort study. Arthritis Rheum 51:168–176
12. Croft PR, Macfarlane GJ, Papageorgiou AC et al (1998) Outcome of low-back pain in general practice: a prospective study. BMJ 316(7141):1356–1359
13. Fairbank J, Frost H, Wilson-Mac Donald J et al (2005) Randomised controlled trial to compare surgical stabiliza-tion of the lumbar spine with an intensive rehabilitation pro-gram for patients with chronic low-back pain: the MRC spine stabilization trial. BMJ 330:485–492
14. Freemont A, Peack TE, Goupille P et al (1997) Nerve ingrowth into diseased intervertebral disc in chronic back pain. lancet 350:178–181
15. Fritzell P, Haag O, Wessberg P et al (2001) llumbar fusion versus non surgical treatment for chronic low-back pain: a multicenter randomized controlled trial from the sweedish lumbar spine study group. Spine 26:2521–2532

713.1 Natural Evolution of Nonspecific Low-Back Pain
16. Frymoyer JW (1988) Back pain and sciatica. N Engl J Med 318:291–300
17. Frymoyer JW, Cats-Baril W (1987) Predictors of low-back pain disability. Clin Orthop 221:89–98
18. Gieseke T, Gracely RH, Masilo AH et al (2004) Evidence of augmented central pain processing in idiopathic chronic low-back pain. Arthritis Rheum 50:613–623
19. Greenough CC (1993) Recovery from low-back pain 1–5 year follow-up of 287 injury related cases. Acta Orthop Scand 64(Suppl 254):1–64
20. Guzman J, Esmail R, Karjalainen K et al (2001) Multi-disciplinary rehabilitation for chronic low-back pain. Systematic review. BMJ 322:1511–1516
21. Hansson TH, Hansson EK (2000) The effects of common medical interventions on pain, back function and work resumption in patients with chronic low-back pain. Spine 25:3055–3064
22. Hansson EK, Hansson TH, Jonsson R (2006) Predictors for work ability and disability in men and women with low-back or neck problems. Eur Spine J 15:780–793
23. Hestback l, leboeuf-YDE C, Manniche C (2003) low back-pain what is the long-term course? A review of studies of general patient populations. Eur Spine J 13:149–165
24. Ilharreborde B, Olivier E, Rillardon l et al (2005) Efficiency of total disc replacement arthroplasty in the treatment of chronic low-back pain. Presented at the Issls annual meet-ing. May 10–14, New York, USA
25. Klenerman l, Slade PD, Stanley M et al (1995) Predicting long term functional limitations among back pain patients in a general practice setting. Spine 20:478–484
26. leavitt F (1992) The physical exertion factor in compens-able work injuries. A hidden flaw in previous research. Spine 17:307–310
27. Nachemson A (2004) The evidence base for treatment of not degenerative disc disease but back pain. In: Gunzburg R, Spaslski M, Anderson GBJ (eds) Degenerative disc disease. lippincott Williams and Wilkins, Philadelphia
28. Pedersen PA (1981) Prognostic indicators in low-back pain. JR Coll Gen Pract 31:209–216
29. Pengel l, Herbert R, Maher C et al (2003) Acute low-back pain: systematic review of its prognosis. BMJ 327(7410): 323–327
30. Philips H, Grant l (1991) Acute back pain. A psychological analysis. Behav Res Ther 29:429–434
31. Roberts S, Eisenstein SM, Menage Y (1995) Mechano-receptors in intervertebral discs. Morphology, distribution and neuropeptides. Spine 20:2645–2651
32. Roland M, Morris R (1983) A study of the natural history of low-back pain part II: development of guidelines for trials of treatment in primary care. Spine 8:145–150
33. Shenk P, lanblit HJ et al (2007) Symptomatology of recur-rent low back pain in nursing and administrative professions. Eur Spine J 16:1789–1898
34. Spitzer WO, leblanc FE, Dupuis M et al (1987) Scientific approach to the assessment and management of activity-related spinal disorders: a monograph for clinicians. Report of the quebec Task force on spinal disorders. Spine 12:51–559
35. Takahashi H, Suguro T, Okazima Y et al (1996) Inflammatory cytokines in the herniated disc of the lumbar spine. Spine 21:218–224
36. Thomas E, Silman AJ, Croft P et al (1999) Predicting who develops chronic low-back pain in primary care: a prospec-tive study. BMJ 318:1662–1667
37. Tulder MW VAN, Koew BM, Bouter lM (1997) Management of chronic non specific low back pain in primary care: a descriptive study. Spine 22:76–82
38. van den Hoogen H, Koes B, Deville W et al (1997) The progno-sis of low-back pain in general practice. Spine 22:1515–1521
39. Van Doorn T (1995) low back disability among self employed dentists, veterinarians, physicians and physical therapists in The Netherlands. Acta Orthop Scand 66(Suppl 263):1–64
40. Vital JM, Gille O, Pointillart V et al (2003) Course of Modic I, 6 months after lumbar posterior osteosynthesis. Spine 28:715–720
41. Von Korff M, Saunders K (1996) The course of back pain in primary care. Spine 21:2833–2837
42. Von Korff M, Deyo RA, Cherkin D (1993) Back pain in pri-mary care. Outcomes at 1 year. Spine 18:855–862
43. Waddell G (1987) A new clinical model for the treatment of low back pain. Spine 12:632–644
44. Waddell G (1992) Biopsychosocial analysis of low-back pain. Baillere Clin Rheumatol 6:523–557
45. Werhaupt O, Zanetti M, Hodler J (2001) Relevance of end-plates abnormalities at MRI imaging. Radiology 218:420–427

73M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_3.2, © Springer-Verlag Berlin Heidelberg 2010
Introduction
As clinicians, prescribing conservative treatment is an essential part of our daily activity. Prescriptions are based on knowledge, and evidences are available for the different therapies in LBP. However, evidence is just a measure of the generalizability, or external valid-ity, of the efficacy of a given treatment. In other terms, how well some form of treatment performs for an “average patient” or a group of patients, a measure usually defined within the frame of a scientific study. In an era of limited healthcare resources, all our patients would be ideally “average,” and treatments would be evidence-based. Only treatments demon-strated to be effective would be considered and used for LBP, as for any other condition.
However, the decisions made by clinicians for indi-vidual patients are multifactorial and do not rely solely on scientific evidence as already highlighted by Sackett [35]. The adherence of practitioners to the recommen-dations of guidelines, a peer reviewed condensate of scientific evidences, is far from being perfect [14]. An impressive study from the US including more than ten million ambulatory visits during a 6-year period has shown that the AHRQ clinical practice guidelines for the management of acute LBP had a more than modest impact on physician behavior. Worst, there was no evi-dence of a trend toward improved compliance with guidelines over time [16].
In this chapter, we are going to concentrate on the variables that play a role in individual decision mak-ing. What makes a doctor prescribe or not a given treatment to the unique individual patient sitting in front of him? Different categories of factors play a role in such procedure that might be classified into several categories from patients-related factors, doctor’s pre-vious experiences with treatments, or even to societal factors (Fig. 3.2.1).
Treatment-Related Factors
We prescribe a treatment because we know or we believe it to be effective. However, all treatments come with a cost, in terms of price, risk, or cumbersomeness, a factor we implicitly integrate in our decision making. None hesitates to prescribe borderline efficient but safe treatments; however, we all would be reluctant to use a highly effective treatment for LBP if treatment-related mortality is an issue.
There are plenty of articles summarizing the avail-able evidence more or less strongly supporting the therapies available for LBP [1, 5, 7–9, 22, 25, 41], and
Prescribing Conservative Treatment for Low Back Pain
F. Balagué and J. Dudler
F. Balagué (*) Service de Rhumatologie, Médicine Physique et Réhabilitation, HFR-Hospital Cantonal, Case postale, 1708 Fribourg, Switzerland e-mail: [email protected]
3.2
Psychological Cultural
Individual patient
Biological Socio-economic
Physician
Treatment
SocietyPrescription
Fig. 3.2.1 Schematic description of the variables in place during the process of prescription

74 F. Balagué and J. Dudler
some are presented in this book. However, it has also been recently highlighted that there is insufficient evi-dence regarding the effectiveness of many of the avail-able therapies used for chronic LBP [19]. For example, opioids are frequently prescribed in western countries, despite a recent review showing limited evidence sup-porting their utilization in chronic LBP sufferers [11]. And in his review, Joines conclude that good quality randomized controlled trials are still needed to clarify the role of various treatments [19].
Another problem with treatment effectiveness is that for a treatment to be effective, at least two things have to be present. The treatment must have an active ingredient that is likely to have a positive effect on the symptom or disease being treated, and the patient must also adhere to the treatment regime [40], a fact taking for granted but probably far from the truth. Based on their review of literature, Oleske et al. highlight that dropout rates are higher in intervention studies of LBP when participants are allocated to groups requiring the most effort (dynamic exercise over physiotherapy or over rest) [30].
Finally, we gullibly assume that proof of efficiency in one dimension of LBP will directly apply to all other aspects of the syndrome. In their recent review, Krismer and van Tulder recommended that the goals of treat-ment should be defined according to the international classification of functioning, disability and health (ICF) of the WHO. Reduction of pain, prevention of disability, and maintenance of work capacity are all goals of treatment in patients with nonspecific low back pain [22]. However, most treatments do not dem-onstrate the same efficacy in all these domains, and we all know patients with good symptomatic response who never return to work.
Patient-Related Factors
Individual patients’ response, which is the outcome clinicians are dealing with in daily practice, does not necessarily match the results of a scientific study. Patients come in different sizes and colors, and no patient is average. Many dimensions influence the response to treatment: biological (age, gender, comor-bidities), psychological (preferences, comorbidities), cultural (beliefs, attitudes), or socioeconomic. Not only can they influence the biologic response to a given
treatment but most of these variables can also likely influence patients’ compliance with treatment.
Even with a perfect compliance, individual biologi-cal characteristics may play a role. For example, genetic background (e.g., CYP2C9, CYP2D6) has been shown to explain different responses to analge-sics or antiinflammatory drugs [18, 21, 39]. The clini-cian, however, is not aware of the individual patient’s genotype and an unexpected response to analgesics might be erroneously attributed to lack of compliance or to psychological factors. Furthermore, patients with LBP have been shown to present significantly more comorbidities than the general population [38]. These associations may of course interfere with the treatment that the physician would like to prescribe for LBP. Age is another relevant biologic variable and specific rec-ommendations concerning the conservative treatment of LBP in older patients have been published recently [10]. The challenge with medication is to find the dos-age that maximizes pain relief and minimizes side effects [40].
If biological variables are significant, the work from Pulliam et al. demonstrates that psychological and cul-tural factors are as important to understand the efficiency of our prescription. They analyzed the difficulties encoun-tered in the implementation of a secondary prevention program in acute LBP patients. Several groups of prob-lems were identified apart from biological factors, i.e., personality factors, satisfaction, comprehension, side effects, financial issues, length of treatment, type of regi-men, social issues, and patient beliefs. The authors made some useful suggestions to improve patients’ adherence to prophylactic interventions, e.g., financial incentives, involvement of the referring physician, good communi-cation, involvement of family members, case manage-ment services, and avoiding too lengthy or complicated interventions [33].
Patient’s own preferences and expectations are also important. The patient’s preferences may influence the outcome. Manca et al.’s study compared a brief physio-therapy intervention with usual physiotherapy for neck pain. Patients preferring and allocated to the brief inter-vention showed better health outcomes and lower costs with a better cost-effectiveness than patients without that particular preference [26]. Expectations are equally relevant to define the goals of treatment and, thus, the prescription. Zelman et al. studied a group of chronic pain patients (including almost 40% of chronic LBP) and reported on the patients’ point of view on their goals

753.2 Prescribing Conservative Treatment for Low Back Pain
for the management of persistent pain and particularly what can be considered “tolerable” or “unacceptable” days [42]. According to this study, chronic LBP patients show reasonable expectations and identified five key components of what can be considered “a day of desir-able pain management,” i.e., taking the edge off the pain, some functional capacity, social engagement desirable, night time rest, and reduced negative affect [42].
Finally, if patient-related factors are certainly impor-tant, understanding patients’ preferences is a challeng-ing task. In a study of 314 patients, a majority of patients preferred to see their general internist for a potential LBP and agreed/strongly agreed that it was important for them to see the same doctor for a back pain as for any other medical problems, despite 72% of them thinking that specialists were better able to pre-scribe medication for back pain. At the same time, they wanted unrestricted access to specialists to supplement care provided by general internists. Interestingly, their understanding of the job of an internist showed amaz-ing gaps (e.g., 22% thought that an internist delivers babies, 51% that she/he does minor surgery, and 11% that she/he does major surgery) [24]. Nevertheless, patient’s decisions appear more logical and compre-hensible when they actually suffer from LBP, when “only” 58% agreed/strongly agreed that it was impor-tant to see the same doctor for their actual back pain as for any other medical problems [24].
Physician-Related Factors
As previously mentioned, we prescribe treatments because we judge it to be effective. We like to believe that most of our prescriptions are evidence-based, even if we should probably admit they are heavily tinted by our previous experiences. Also, we should never forget that evidences regarding the effectiveness of many of the available therapies used for chronic LBP are still lacking [19]. Referring to published literature does not solve all our problems as shown by Furlan et al. in their critical review of reviews on the treatment of chronic LBP. They highlighted two important points that the clinician should bear in mind. Reviews of bet-ter quality tended to have more uncertain or negative conclusions, and when two or more reviews examine the same intervention, conflicting conclusions about effectiveness were very likely [15].
Moreover, when evidences are available, they do not directly translate into adequate use. A study including 30 primary care physicians has shown that many of the physicians report reluctance to regularly consult algo-rithms when treating chronic pain [17]. Doctor seems more prone to prescribe following her/his beliefs with regard to the origin of pain than any evidence-based recommendations. If a doctor thinks that she/he has identified the anatomic origin of pain, it seems logical that the treatment will be guided by her/his hypothesis [20], rather than to the effectiveness/acceptability of guidelines. Adherence of Irish general practitioners to published guidelines was rather low in a recent pro-spective study [14].
Patient-Physician Interaction-Related Factors
The literature shows that many reasons exist for a doc-tor to make decisions unsupported by the available sci-entific evidence [2]. A fair amount of them are related to the therapeutic relationship or the interaction between patient and physician. A review of some prob-lem situations in that relationship was published a few years ago by Nordin et al., and suggestions displayed remain perfectly adapted in 2010 [29].
It is impossible to analyze or describe all possible flaws in the patient-physician interaction, which could play a role in the act of prescription, but some examples would help to understand this complexity. General prac-titioners’ interpretations of patients’ preferences, rather than the actual patient’s expectations, can be a major reason for nonadherence to the guidelines recommenda-tions as shown by a recent qualitative study [36, 37]. Physicians’ fear of losing patients is another factor that may contribute to inadequate prescription with treat-ments that not only lack scientific evidences, but also may be dangerous. One of the examples is the use of intramuscular NSAIDs instead of using oral forms, a flaw which can be perhaps corrected by the use of patient information leaflet as recently demonstrated [34].
If physician’s fear and interpretation can mislead the prescription process, patients also endorse their respon-sibilities. In a recent study in the US, 63% (and possibly 72%) of the 831 adults subjects who saw both a medical doctor and a complementary and alternative therapy (CAM) provider did not disclose at least one of their

76 F. Balagué and J. Dudler
CAM therapies to their doctor [12]. Patients failed to report their therapy, even if they judged CAM therapies to be more helpful than conventional medical care for the treatment of neck and back conditions, among other pathologies. This lack of communication was not due to a selection bias as the same patients judged conventional care to be more helpful than CAM therapy for treatment of hypertension and less than 50% of them judged that CAM providers were better listeners and did a better job of explaining their medical conditions. The authors con-clude that many patients view medical doctors as mem-bers of a larger, patient-selected healthcare team [12], and it certainly appears that the doctor is not the unique reference for the patient, as we like to believe. Other aspects of the limitations of the information provided by patients during a clinical encounter have been high-lighted in recent studies [6, 28].
The relationship between patient and physician can influence not only the prescription, but also its evalua-tion, which in turn may subsequently influence the pre-scription. Evaluating compliance in daily practice is not an easy task, and is not regularly performed by cli-nicians. A recent American study has evaluated the predictors of missed visits and dropouts in an occupa-tional health longitudinal study for work-related low back troubles [30]. Most predictors, either of dropout, early vs. late dropout, or number of missed visits, were variables unrelated to medical care. Dropout was related to age and poor self-reported health status, while greater body fat percentage was associated to early dropout. Finally, patients with back pain longer than 2 weeks and arthritis missed more than three vis-its [30]. Evaluation of the outcome is another area where patient’s and healthcare provider’s perception may differ. Recently, Perreault and Dionne published a study including 78 patient-physiotherapist dyads where the perception by the therapists of patients’ pain using a numerical rating scale and their functional capacity by means of the Roland and Morris disability questionnaire was on the average a third lower than when self-reported by patients. Interestingly, if a majority of studies quoted demonstrated a detrimental effect of higher discrepancies between patients and professionals, a favorable effect was observed in this case [31].
Patient and doctor relationships are not so trivial, and we can ask what makes our consultation a “good back-consultation” for the patient? Laerum et al. recently published the results of a combined qualitative
and quantitative study of chronic LBP patients and summarized what patients consider a “good back-consultation.” The main aspects were to be taken seri-ously (be seen, heard, and believed), to be given an understandable explanation of what is wrong, to have patient-centered communication (seeking patients’ perspectives/preferences), to receive reassurance, to be given, if possible, a favorable prognosis, and to be told what can be done (by the patient him- or herself and by the care provider) [23]. The authors made some useful suggestions to improve our daily practice with LBP patients, i.e., “deal more with psychosocial issues and particularly how LBP affect various roles of daily life. This is also important because psychosocial fac-tors are important predictors of prognoses and clinical course of LBP and chronic LBP almost consistently has important psychosocial consequences; use more open-ended questions, not least when dealing with psychosocial and complex emotional issues; improve the structuring of the consultation with more distinct opening, intersectional/management and closing phase of the consultation, not least with pre-announcing and declaring what is coming next in the encounter. This has been shown to give better patient satisfaction, compliance and recall; make more use of summarizing and repetition of what has happened during the consul-tation.” This reminded us that management of chronic LBP patients is more than “just” prescribing [3].
Societal-Related Factors
Healthcare system characteristics and regulations vary from country to country, and without doubt influence the prescription habits. This fact is certainly not sim-ply and directly related to the domestic national gross product as a recent comparison between Australia, New Zealand, and the US has shown. Despite the fact that many aspects of the clinical practice are remark-ably similar between these three countries, the average American receives much less exposure to primary care physicians for musculoskeletal-related health prob-lems than patients living in the other two countries (29.7 min/year vs. 55.5 min/year in NZ and 83 min/year in Australia) [4]. However, economical aspects also play an important role in many decisions. For instance, in Switzerland not all spinal surgeons are allowed (i.e., reimbursed) by the insurance companies

773.2 Prescribing Conservative Treatment for Low Back Pain
to implant disk prosthesis. In the same country, radiof-requency facet joints denervation are not reimbursed anymore. Similarly, the role of insurance coverage has been suggested to explain differences between the US and the European literature in terms of dropouts (higher in the US) in intervention studies of low back pain [30].
Influences of those societal-related factors on indi-vidual prescription will appear obvious, nevertheless their influences on the external validity of some evi-dences presented to promote a treatment strategy will be much more subtle. A group of British authors has analyzed the cost-effectiveness of two physiotherapy strategies for back and neck pain patients. A brief phys-iotherapy pain management approach using cognitive-behavioral principles was cheaper than a traditional McKenzie approach, but the latter offers the greatest health outcome (in QUALYs) and was the most cost-effective in their trial [27], a result not necessarily applicable to different socioeconomic environments.
Conclusions
The practice of clinical medicine remains an art with a scientific background. When the clinician makes deci-sions for an individual patient, she/he takes into account many factors, either consciously or unconsciously. Treatment cannot be based solely on “hard” evidences, because they are not always available or adequate for the given patient. Tailoring of individual treatments is necessary and is in agreement with the principles of EBM. However, the scientific evidences must be kept in mind and we should not rely only on our experience. In a study where 9% of diagnostic testing or surgeries were refused, based on recommendations and against the treating physician’s opinion and experience, 85% of these patients improved with simple conservative management over a follow-up period of 1 year [13]. Furthermore, this approach was reported to be highly “cost-effective” [13].
For a good practice, or rather an always improving practice, the clinician must keep in mind the influence of subjective factors when his decisions are not fully in agreement with the recommendations of existing guide-lines. He should be particularly concerned about totally subjective factors related to the patient or his personal experiences. He must also evaluate the effect of his
treatment with valid tools on a regular basis to confirm the efficacy and adequacy of his decisions, being always ready to change therapeutic prescriptions/recommen-dations if lack of efficacy becomes evident.
Finally, if a regular application of these principles can certainly improve our medical practice, it appears from the nonmedical point of view that most doctors do a fair job in their daily practice: “If doctors prac-ticed medicine like many companies practice manage-ment, there would be more unnecessarily sick or death patients and many more doctors in jail or suffering other penalties for malpractice” [32].
References
1. Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, Mannion AF, Reis S, Staal J, Ursin H, Zanoli G; COST B13 Working Group on Guidelines for Chronic Low Back Pain (2006) Chapter 4. European guide-lines for the management of chronic nonspecific low back pain. Eur Spine J 15:S192–S300
2. Balagué F, Cedraschi C (2006) Radiological examination in low back pain patients: anxiety of the patient? Anxiety of the therapist? Joint Bone Spine 73:508–513
3. Balagué F, Mannion AF, Pellisé F, Cedraschi C (2007) Clinical update: low back pain. The Lancet 369:726–728
4. Bindman AB, Forrest CB, Britt H, Crampton P, Majeed A (2007) Diagnostic scope of and exposure to primary care physicians in Australia, New Zealand, and the United States: cross sectional analysis of results from three national sur-veys. BMJ 334:1261
5. Burton AK, Balague F, Cardon G, Eriksen HR, Henrotin Y, Lahad A, Leclerc A, Muller G, van der Beek AJ; Pain CBWGoGfPiLB (2006) Chapter 2. European guidelines for prevention in low back pain. Eur Spine J 15:S136–S168
6. Carragee E (2007) Validity of self-reported history in patients with acute back or neck pain after motor vehicle accidents. Spine J 8(2):311–319
7. Chou R, Qaseem A, Snow V, Casey D, Cross T, Shekelle P, Owens DK (2007) Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American college of physicians and the American pain society. Ann Intern Med 147:478–491
8. Chou R, Hoyt Huffman L (2007) Nonpharmacologic thera-pies for acute and chronic low back pain: a review of the evidence for an American pain society/American college of physicians clinical practice guideline. Ann Intern Med 147:492–504
9. Chou R, Hoyt Huffman L (2007) Medications for acute and chronic low back pain: a review of the evidence for an American pain society/American college of physicians clini-cal practice guideline. Ann Intern Med 147:505–514
10. Cohen RI, Chopra P, Upshur C (2001) Low back pain, part 2. Guide to conservative, medical, and procedural therapies. Geriatrics 56:38–47
78 F. Balagué and J. Dudler
11. Deshpande A, Furlan A, Mailis-Gagnon A, Atlas S, Turk D (2007) Opioids for chronic low-back pain. Cochrane Database Syst Rev (3):CD004959
12. Eisenberg DM, Kessler RC, Van Rompay MI, Kaptchuk TJ, Wilkey SA, Appel S, Davis RB (2001) Perceptions about complementary therapies relative to conventional therapies among adults who use both: results from a national survey. Ann Intern Med 135:344–351
13. Friedlieb OP (1994) The impact of managed care on the diagnosis and treatment of low back pain: a preliminary report. Am J Med Qual 9:24–29
14. Fullen BM, Maher T, Bury G, Tynan A, Daly LE, Hurley DA (2007) Adherence of Irish general practitioners to European guidelines for acute low back pain: a prospective pilot study. Eur J Pain 11:614–623
15. Furlan A, Clarke J, Esmail R, Sinclair S, Irvin E, Bombardier C (2001) A critical review of reviews on the treatment of chronic low back pain. Spine 26:E155–E162
16. Jackson JL, Browning R (2005) Impact of national low back pain guidelines on clinical practice. South Med J 98: 139–143
17. Jamison RN, Gintner L, Rogers JF, Fairchild DG (2002) Disease management for chronic pain: barriers of program implementation with primary care physicians. Pain Med 3: 92–101
18. Janicki P, Schuler G, Francis D, Bohr A, Gordin V, Jarzembowski T, Ruiz-Velasco V, Mets B (2006) A genetic association study of the functional A118G polymorphism of the human mu-opioid receptor gene in patients with acute and chronic pain. Anesth Analg 103:1011–1017
19. Joines JD (2006) Chronic low back pain: progress in therapy. Curr Pain Headache Rep 10:421–425
20. Kent P, Keating J (2004) Do primary-care clinicians think that nonspecific low back pain is one condition? Spine 29:1022–1031
21. Kirchheiner J, Brockmöller J (2005) Clinical consequences of cytochrome P450 2C9 polymorphisms. Clin Pharmacol Ther 77:1–16
22. Krismer M, van Tulder M (2007) Low back pain (non-spe-cific). Best Pract Res Clin Rheumatol 21:77–91
23. Laerum E, Indahl A, Skouen JS (2006) What is “the good back-consultation”? A combined qualitative and quantitative study of chronic low back pain patients’ interaction with and perceptions of consultations with specialists. J Rehabil Med 38:255–262
24. Lewis CL, Wickstrom GC, Kolar MM, Keyserling TC, Bognar BA, DuPre CT, Hayden J (2000) Patients prefer-ences for care by general internists and specialists in the ambulatory setting. J Gen Intern Med 15:75–83
25. Main CJ, Sullivan MJL, Watson PJ Edinburgh (2008) Pain management. Practical applications of the biopsychosocial perspective in clinical and occupational settings, 2nd edn. Churchill Livingstone Elsevier, Edinburgh
26. Manca A, Epstein DM, Torgerson DJ, Klaber Moffett JA, Coulton S, Farrin AJ, Hahn S, Jackson DA, Richmond SJ (2006) Randomized trial of a brief physiotherapy interven-tion compared with usual physiotherapy for neck pain patients: cost-effectiveness analysis. Intl J Technol Assess Health Care 22:67–75
27. Manca A, Dumville JC, Torgerson DJ, Klaber Moffett JA, Mooney MP, Jackson DA, Eaton S (2007) Randomized trial of two physiotherapy interventions for primary care back and neck pain patients: cost-effectiveness analysis. Rheumatology 46:1495–1501
28. McCarthy C, Gittins M, Roberts C, Oldham J (2007) The reli-ability of the clinical tests and questions recommended in international guidelines for low back pain. Spine 32: 921–926
29. Nordin M, Cedraschi C, Skovorn ML (1998) Patient-health care provider relationship in patients with non-specific low back pain: a review of some problem situations. Baillière’s Clin Rheumatol 12:75–92
30. Oleske DM, Morrissey Kwasny M, Lavender SA, Andersson GBJ (2007) Participation in occupational health longitudinal studies: predictors of missed visits and dropouts. Ann Epidemiol 17:9–18
31. Perreault K, Dionne CE (2006) Does patient-physiotherapist agreement influence the outcome of low back pain? A pro-spective cohort study. BMC Musculoskeletal Disord Sep 20;7:76
32. Pfeffer J, Sutton RI (2006) Evidence-based management. Harv Bus Rev 84:62–74, 133
33. Pulliam C, Gatchel RJ, Robinson RC (2003) Challenges to early prevention and intervention: personal experiences with adherence. Clin J Pain 19:114–120
34. Rosemann T, Joos S, Koerner T, Heiderhoff M, Laux G, Szecsenyi J (2006) Use of a patient information leaflet to influence patient decisions regarding mode of administration of NSAID medications in case of acute low back pain. Eur Spine J 15:1737–1741
35. Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS (1996) EBM: what it is and what it isn’t. BMJ 312:71–72
36. Schers H, Braspenning J, Drijver R, Wensing M, Grol R (2000) Low back pain in general practice: reported manage-ment and reasons for not adhering to guidelines in The Netherlands. Br J Gen Pract 50:640–644
37. Schers H, Wensing M, Huijsmans Z, van Tulder M, Grol R (2001) Implementation barriers for general practice guide-lines on low back pain. Spine 26:E348–E353
38. Schneider S, Mohnen S, Schiltenwolf M, Rau C (2007) Comorbidity of low back pain: representative outcomes of a national health study in the Federal Republic of Germany. Eur J Pain 11:387–397
39. Stamer U, Stüber F (2007) The pharmacogenetics of analge-sia. Expert Opin Pharmacother 8:2235–2245
40. Turk DC, Dworkin RH (2004) What should be the core out-comes in chronic pain clinical trials? Arthritis Res Ther 6:151–154
41. van Tulder M, Becker A, Bekkering T, Breen A, del Real MT, Hutchinson A, Koes B, Laerum E, Malmivaara A; Care CBWGoGftMoALBPiP (2006) Chapter 3. European guide-lines for the management of acute nonspecific low back pain in primary care. Eur Spine J 15:S169–S191
42. Zelman D, Smith M, Hoffman D, Edwards L, Reed P, Levine E, Siefeldin R, Dukes E (2004) Acceptable, manageable, and tolerable days: patient daily goals for medication man-agement of persistent pain. J Pain Symptom Manage 28: 474–487

79M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_3.3, © Springer-Verlag Berlin Heidelberg 2010
Introduction
A group at McMaster University in Canada first for-mulated evidence-based medicine (EBM) as a term in 1992 by Gordon Guyatt. The concept of EBM was to rely on the best available evidence and clinical expe-rience in medical decision making. The concept can be traced back to the twentieth century in its current form and includes the best available evidence from well-designed studies, clinical expertise, patient’s values, and cost for the society. EBM and methodol-ogy have greatly developed during the last two decades. There are now explicit criteria of evaluation for the domains of risk, prognosis, assessment, treat-ment, and economic studies. Evidence summaries are provided by literature review using best evidence syn-thesis (BES) or some rating system, for example, by Taskforces, Cochran, or Rand.
Systematic reviews and large taskforces have sum-marized the evidence for comprehensive rehabilitation for lower back pain and back schools. These reviews have led to changes in the clinical management of patients with lower back pain over the last decade. These two topics are discussed in this chapter, which focusses on treatment studies and gives some exam-ples of strong evidence for education of the patient and comprehensive rehabilitation to avoid chronic disability.
Level of Evidence
Treatment studies and levels of evidence of efficacy are usually divided into five levels (one being the strongest evidence and five the weakest evidence [1]. The levels are described as follows:
Level 1 evidence – randomized control trials of high quality and systematic reviews
Level 2 evidence – lesser quality randomized con-trol trials, prospective comparative studies, and sys-tematic reviews with inconsistent results
Level 3 evidence – case control studies, retrospec-tive comparable studies
Level 4 evidence – case seriesLevel 5 evidence – expert opinionIf a treatment has showed good efficacy in several
Level 1 studies, the treatment is usually well accepted by clinicians and implemented in clinical care.
Back Schools
The evidence for efficacy from Cochrane reviews and The European Guidelines state:
“There is moderate evidence suggesting that back schools, in an occupational setting, reduce pain, and improve func-tion and return-to-work status, in the short and intermediate-term, compared to exercises, manipulation, myofascial therapy, advice, placebo or waiting list controls, for patients with chronic and recurrent LBP. However, future trials should improve methodological quality and clinical relevance and evaluate the cost-effectiveness of back schools” [2],
and
“Back schools based on traditional biomedical/biome-chanical information, advice and instruction are not
Comprehensive Rehabilitation for Low back Pain and Back Schools
Margareta Nordin
M. Nordin Occupational and Industrial Orthopaedic Center (OIOC), Graduate Program of Ergonomics and Biomechanics, New York University (NYU), Hospital for Joint Diseases, NYU Langone Medical Center, CDC/NIOSH Education and Research Center (ERC), New York University, New York, NY, USA e-mail: [email protected]
3.3

80 M. Nordin
recommended for prevention in LBP (strong evidence). High intensity programs, which comprise both an educa-tional/skills program and exercises, can be recommended for patients with recurrent and persistent back pain (mod-erate evidence)” [2].
The European Guidelines articulated the following evidence for Back Schools and the working population:
“Back schools based on traditional biomedical/biome-chanical information, advice and instruction are not rec-ommended for prevention in LBP (strong evidence). There is insufficient evidence to recommend for or against psychosocial information delivered at the work-site (weak evidence), but information oriented toward promoting activity and improving coping may promote a positive shift in beliefs (weak evidence)” [3].
These recommendations give clear guidelines for cli-nicians; if the patient seeks care education is important however the more classic education including biomed-ical/biomechanical content may not be efficient instead the education should focus on reducing fear for the condition, coping skills as well as keeping active, later publications favor individualized education once the patient is in treatment for chronic back pain.
Back schools were believed to be the panacea 20 years ago; the back school concept was later reviewed and thoroughly criticized 10 years ago, and in the new millennium, a more knowledgeable informed approach is being used. Information to the patient is important, but all patients may not need the same information; the school concept has been modified within a framework of “schooling” with individualized education and more participation from the patients’ side. In fact, a recent review recommends brief education for the reduction of sick leave [4].
Information to the Individual Seeking Care in the Acute Stage of Low Back Pain
Once the clinician has ascertained that the individual seeking care has benign low back (no Red Flags), i.e., nonspecific low back pain (NSLBP), the patient needs the reassurance that the condition will resolve most of the time. The information given must be unambiguous and positive and should contain the following items:
NSLBP is common and usually resolves within a •couple of weeks; however, recurrence is high and a few individuals about 6–10% has chronic low back pain of unknown origin.
Keeping as active as possible (including working) •is important for recovery and bed rest for a long time is detrimental for the skeletal system as well as for the spine.Over the counter medication is helpful, but so is a •warm shower or an ice pack on back when the pain is difficult to bear the first days.If you need help for your recovery we can help to •get you back to activity, but the condition usually resolves.
No treatment today has shown to be superior to the natural history of low back pain in the acute stage and the choice of treatment is vast ranging from injec-tions, massage, manipulation, mobilization, acupunc-ture, physiotherapy, and others. In fact, adequate information, positive reinforcement, maintaining activ-ity as much as possible for the first 2–4 weeks is cur-rently the best evidence for early treatment for acute low back pain. This message may even do better if reinforced with pamphlet or brochure with the same advice. A follow up visit is important to verify progres-sive well being and prevention of long-term disability.
If at follow-up visit the patient has not progressed in well being, the clinician has a variety of options to consider for treatment. The most important choice is between active and passive treatment. Active treat-ment is superior to passive treatment to regain activity and work. Passive treatment may give short relief of pain, but may also pacify the patient in not taking responsibility in their own recovery. Active treatment (exercise) and education, individually or in the form of back school (grouping patients together), are supe-rior for regaining desired functional level. Education only without an exercise component is less effective. Patients not recovering the first month may exhibit “Yellow Flags,” i.e., psychosocial factors predicting pain distress and disability. Screening for “Yellow Flags” is crucial before the choice of treatment as it will affect the outcome of treatment [5–7].
Back Schools (Group Education) vs. Individual Education
The typical back school in health care is a program delivered over 2–4 visits in a group setting of patients with subacute or chronic NSLBP. The participants in the traditional back school learn about epidemiology,

813.3 Comprehensive Rehabilitation for Low back Pain and Back Schools
the spine structures, recovery, activity, lifting, and other items of choice of the clinician teaching. The school is usually performed in a didactic fashion; how-ever, some schools also have practical and functional teaching, for example, lifting. Pamphlet and reading material are usually distributed, and discussion is com-mon. The information delivered was successful in that it did change the participants’ knowledge but did not change significantly the participants’ functional level or reduce the pain, which is the main goal of the back school [2]. Back schools have lost popularity over the years and the educational component is now much more individualized to the patients’ needs.
Education Individualized or in Group
Education of the patient is important for any disorder that has high recurrence or may become chronic. The goal of the education should be to empower the patient to be able to manage the condition and, if necessary, get help when needed. People with back pain have dif-ferent worries leading to different questions. In our clinic we are asking the patients what their questions are and what do they want to know. Education of the patient is integrated in the evaluation and treatment of the low back pain. Patients have access to a physician, physical therapist, pain manager (psychologist), or/and ergonomist. Some patients do not want to be in a group and some patients enjoy a group interaction. The delivery of education is informal and individualized to each patient and is based on the questions asked. The goal of the education is how the clinician can empower the patient to manage the back pain and become active and self-sufficient in their daily life [8].
Comprehensive Rehabilitation
The components of comprehensive rehabilitation include a careful evaluation for a specific goal (for example, return to work), and treatments based on best evidence are exercise, cognitive behavioral treatment (CBT), education, and others. Few systematic reviews have been carried out, as the field is still relatively new in combination treatment. The Cochrane Review con-cludes “that there is moderate evidence of positive
effectiveness of multidisciplinary rehabilitation for sub-acute low back pain and that a workplace visit increases the effectiveness. But because this evidence is based on trials that had some methodological shortcomings, and several expensive multidisciplinary rehabilitation programs are commonly used for uncomplicated/non-specific sub-acute low back problems, there is an obvi-ous need for high quality trials in this field” [9]. We can cautiously interpret these findings as multidisci-plinary treatment in a subacute phase and chronic of low back pain gives a better result than mono disciplin-ary care; the strongest components of such care seem to be exercise, CBT, education, and work site visit. Each of the components above will be briefly reviewed and the main outcome for this review is return to work and stay at work.
When Do A Patient Need Multimodal or Multidisciplinary Care for NSLBP?
Patients with NSLBP who do not progressively recover may need a combination treatment based on signs and symptoms at revisit to prevent chronicity. A screening is appropriate at this stage. The “Red Flags” are to be screened again to ascertain that the medical diagnosis has not changed and remains NSLBP. In addition, the patient is screened for “Yellow Flags,” i.e., psychoso-cial factors that are best treated with CBT. Patients who have remained on passive treatment for 2–4 weeks may need an active exercise program, and if that does not work, combined with CBT. Each of these treatment exercises and CBT treatments has moderate to good evidence of efficacy; however, for the patient not pro-gressing with one of the therapies, the combination of the two yields a better result for regaining an active lifestyle and work. The combination treatment should start within 2–3 weeks of unimodal treatment.
Exercise Treatment
Exercise has shown moderate effect or moderate to excellent effect on chronic and recurrent NSLBP [10–14]. There are many different types of exercise to choose from, but as of today, no one specific exercise regimen seems to be superior to any other exercise

82 M. Nordin
regimen; the most important seems to get the patient adopting a regular exercise regimen that the patient seems comfortable with and will continue doing.
When a patient starts an exercise regimen it should be at 50% of capacity and progressively more demand-ing including strengthening, stretching, endurance, and aerobic exercise. Supervised exercise has better results than unsupervised in the beginning of the regi-men. To get results, three visits a week is better than once a week to start an exercise regimen. Discussions with the patients regarding how to maintain a regimen during their daily life are crucial, otherwise effects of an exercise regimen may quickly fade in a couple of months. Some patients want to return to a sports activ-ity, specific training for the chosen sports activity has to be trained and learned.
Change of lifestyle and including an exercise regi-men may be challenging to the patient and many patients drop out (about 50%) or do not complete treat-ment. It is, therefore, important to individualize the regimen to the patient’s need [15].
Cognitive Behavioral Treatment
Cognitive Behavioral Therapy (CBT) is based on mod-ifying cognitions, assumptions, beliefs, and behaviors. Patients having NSLBP with a longer duration has a pain localized to the lower back without detectable lesion or cause for the pain [16]. Pain itself can lead to catastrophizing, anxiety, fear avoidance, passivity, depression, and other symptoms. There is a strong rec-ognition nowadays that psychological and psychosocial factors are predictors of disability and nonrecovery in patient with low back pain. CBT has proven to be very successful as a therapeutic choice for these patients. The particular therapeutic techniques vary according to the need of the patient, but commonly include keeping a diary of significant events and associated feelings, thoughts, and behaviors; questioning and testing cogni-tions, assumptions, evaluations, and beliefs that might be unhelpful and unrealistic; gradually facing activities that might have been avoided; and trying out new ways of behaving and reacting. Relaxation and distraction techniques are also commonly included.
CBT is usually given by a clinical psychologist; patients exhibiting “Yellow Flags” are referred and the patient is subjected to an in-depth evaluation consisting of a 1 h interview. If the patient is an appropriate
candidate for CBT, usually two to six encounters are necessary.
The utility of CBT is well supported by randomized trials, systematic reviews, and in clinical practice both in subacute and chronic NSLBP patients. CBT inter-ventions include creative visualization, imagery, pro-gressive muscle relaxation techniques, problem solving techniques, and others. The goal is to have the patient understand, accept, and gain control over the back pain problem and its possibly deleterious consequences by helping the patient develop adaptive coping behaviors and strategies. There is moderate-to-strong evidence that CBT should be used early if bio-psychosocial signs or symptoms are present, and there is strong evi-dence that CBT should be used in patients with chronic NSLBP [17, 18]. The European Guidelines recom-mended cognitive-behavioral treatment for patients with chronic LBP based on “conclusive evidence that there are no differences in effectiveness between the various types of behavioral therapy and that behavioral treatment is more effective for pain, functional status and behavioral outcomes than placebo/no-treatment/waiting-list control” [3].
Multimodal Programs for Chronic Low back Pain
Multimodal programs usually consist of a progressive exercise regimen, CBT, education, and/or possibly a worksite visit if the goal is to return the patient to work. This combination of modalities has been very success-ful in highly structured positive environment in occu-pational settings or workers compensation patients to reduce workloss [19–21]. However, the findings have to be interpreted with caution because there were some flaws in the methods of the few studies reviewed and the results need to be confirmed [22]. These highly structured programs warrant more research in nonoc-cupational settings and where the goal may be differ-ent from work loss [23].
Conclusions
Persistent NSLBP for more than 4 weeks responds well to an exercise regimen, if no progress is made, CBT adds additional success. Throughout the treatment patient

833.3 Comprehensive Rehabilitation for Low back Pain and Back Schools
education should focus on how to manage possible recurrence and/or bouts of pain. The goal of the treat-ment should be to empower the patient to manage the condition. Staying active, active exercise regimens, and CBT are significantly more successful than pas-sive treatment regimens for return to activity and dis-ability (work loss), while more passive treatments such as manipulation and/or medication still have an effect on pain reduction but not necessarily return to activity including work.
References
1. Watters WC, Duszinsky B (2007) Evidence-based medicine: helping at an individual and organizational level. NASS Spineline 8–12
2. Heymans MW, van Tulder MW, Esmail R, Bombardier C, Koes BW (2005) Back schools for nonspecific low back pain: a systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine 30(19):2153–2163
3. Airaksinen O, Brox JI, Cedraschi C et al (2006) Chapter 4. European guidelines for the management of chronic nonspe-cific low back pain. Eur Spine J 15(Suppl 2):S192–S300
4. Brox JI, Storheim K, Grotle M, Tveito TH, Indahl A, Eriksen HR (2008) Evidence-informed management of chronic low back pain with back schools, brief education, and fear-avoid-ance training. Spine J 8(1):28–39
5. Kendall NAS, Linton SJ, Main CJ (1997) Guide to assessing psychosocial yellow flags in acute low back pain: risk factors for long term disability and work loss. Accident Rehabilitation and Compensation Insurance Corporation of New Zealand and the National Health Committee, Wellington
6. Linton SJ, Boersma K (2003) Early identification of patients at risk of developing a persistent back problem: the predictive validity of the Orebro Musculoskeletal Pain Questionnaire. Clin J Pain 19(2):80–86
7. Weiser S, Rossignol M (2006) Triage for nonspecific lower-back pain. Clin Orthop Relat Res 443:147–155
8. Nordin M, Welser S, Campello MA, Pietrek M (2002) Self-care techniques for acute episodes of low back pain. Best Pract Res Clin Rheumatol 16(1):89–104
9. Guzman J, Esmail R, Karjalainen K, Malmivaara A, Irvin E, Bombardier C (2002) Multidisciplinary bio-psycho-social
rehabilitation for chronic low back pain. Cochrane Database Syst Rev (1):CD000963
10. Abenhaim L, Rossignol M, Valat JP et al (2000) The role of activity in the therapeutic management of back pain. Report of the international Paris task force on back pain. Spine 25(Suppl 4):1S–33S
11. van Tulder MW, Malmivaara A, Esmail R, Koes BW (2000) Exercise therapy for low back pain. Cochrane Database Syst Rev (2):CD000335
12. Chou R, Qaseem A, Snow V et al (2007) Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American college of physicians and the American pain society. Ann Intern Med 147(7):478–491
13. Mayer J, Mooney V, Dagenais S (2008) Evidence-informed management of chronic low back pain with lumbar extensor strengthening exercises. Spine J 8(1):96–113
14. Standaert CJ, Weinstein SM, Rumpeltes J (2008) Evidence-informed management of chronic low back pain with lumbar stabilization exercises. Spine J 8(1):114–120
15. Alexandre NM, Nordin M, Hiebert R, Campello M (2002) Predictors of compliance with short-term treatment among patients with back pain. Rev Panam Salud Publica 12(2): 86–94
16. Pither C (2007) Optimizing non-operative care. Curr Orthop 21:1–8
17. Nordin M, Balague F, Cedraschi C (2006) Nonspecific lower-back pain: surgical versus nonsurgical treatment. Clin Orthop Relat Res 443:156–167
18. Ostelo RW, van Tulder MW, Vlaeyen JW, Linton SJ, Morley SJ, Assendelft WJ (2005) Behavioural treatment for chronic low-back pain. Cochrane Database Syst Rev (1):CD002014
19. Steenstra IA, Anema JR, Bongers PM, de Vet HC, Knol DL, van Mechelen W (2006) The effectiveness of graded activity for low back pain in occupational healthcare. Occup Environ Med 63(11):718–725
20. Campello MA, Weiser SR, Nordin M, Hiebert R (2006) Work retention and nonspecific low back pain. Spine 31(16): 1850–1857
21. Loisel P, Abenhaim L, Durand P et al (1997) A population-based, randomized clinical trial on back pain management. Spine 22(24):2911–2918
22. Karjalainen K, Malmivaara A, van Tulder M, et al (2003) Multidisciplinary biopsychosocial rehabilitation for sub-acute low back pain among working age adults. Cochrane Database Syst Rev (2):CD002193
23. Campello M, Weiser S, van Doorn JW, Nordin M (1998) Approaches to improve the outcome of patients with delayed recovery. Baillieres Clin Rheumatol 12(1):93–113

85M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_3.4, © Springer-Verlag Berlin Heidelberg 2010
Introduction
Indeed, the societal burden of musculoskeletal disorders transcends countries and cultures [17] and has paved the way for cooperative multidisciplinary efforts in the utilization of healthcare resources in search of the best management. To this extent, low back pain (LBP) is one of the most common musculoskeletal conditions in western society [80]. In the United States, $25 bil-lion is spent annually on medical care services for back problems and another $50 billion is spent on lost pro-ductivity and disability payments [1]. Despite the high prevalence of LBP and the numerous conventional medical treatments used for this condition, few treat-ments are supported by strong scientific evidence [79]. The limited effectiveness and high costs of conven-tional medical treatments have contributed to a high level of utilization of complementary and alternative medical (CAM) therapies both in the United States and around the world [3, 33]. In fact, studies suggest that between 30 and 50% of the adult population in indus-trialized nations use some form of CAM to prevent or treat a variety of health-related problems [3].
Spinal manipulation, performed mostly by chiro-practors in the United States [72], is the most popular CAM therapy for back pain [7]. In just over 100 years since its inception, chiropractic has risen to become the largest profession practicing outside traditional mainstream medicine in the United States and many countries internationally [58]. Categorized under the umbrella of Complementary and Alternative Medicine,
chiropractic has made the largest progression into pri-vate and public healthcare financing systems, mainly due to consumer demand and patient satisfaction [58]. These factors, together with scientific inquiry, have increasingly influenced chiropractic to be viewed as an effective specialty by many within the medical profes-sion [3].
Chiropractic Education, Training, and Practice
Born in the United States, there are currently approxi-mately 60,000 chiropractors practicing in the U.S. and an additional 90,000 chiropractors throughout the world [58]. Chiropractic has been licensed in all 50 United States since 1974 and is covered by most insur-ance plans in the U.S. [63, 74]. Additionally, the prac-tice is licensed or recognized by government health authorities in all Canadian provinces and in over 30 countries worldwide, including Australia, New Zealand, Denmark, England, Germany, the Netherlands, Japan, Saudi Arabia, South Africa, Mexico, and the Russian Federation [14, 54, 68].
Just as it does for other healthcare professionals, each of the 50 states in the U.S. has its own scope of practice statutes and regulations and licensing requirements for chiropractic doctors [16]. Typically, the scope of prac-tice of chiropractors in the different states includes broad diagnostic authority including radiography and laboratory analysis, although some states limit the use of invasive procedures, such as needle electromyo-graphic (EMG) or phlebotomy, in diagnostic testing. All states authorize chiropractors to use spinal manipulation as a primary intervention, and the majority of states per-mit the practice of physiological therapeutics under the
The Place of Chiropractic Care in the Treatment of Low Back Pain
Christopher J. Colloca
C. J. Colloca Department of Kinesiology, Arizona State University, 101 South Roosevelt Avenue, Chandler, AZ 85226, USA e-mail: [email protected]
3.4

86 C. J. Colloca
scope of chiropractic practice. Chiropractors in the US are not allowed to prescribe drugs or perform major sur-gery from chiropractic practice. However, some states authorize certain minor surgeries [54].
Chiropractic Education and Training
Since 1974, standards for chiropractic education have been established and monitored by the Council on Chiropractic Education (CCE). Recognized by the U.S. Department of Education as the specialized accredit-ing agency for chiropractic education, the CCE sets and monitors standards for the curriculum, faculty and staff, facilities, patient care, and research [16]. A chi-ropractic education program consists of four academic years of professional education averaging a total of
4,822 h, and ranging from 4,400 to 5,220 h in the 16 colleges [45]. Table 3.4.1 provides a review of course-work in a typical chiropractic educational program.
The program of study at all chiropractic schools is divided into Basic and Clinical Sciences with an overwhelming emphasis on clinical training (70% of the curriculum). Basic sciences education includes an average of 570 h of anatomy (40% of all basic science hours), 305 h of physiology (21%), 205 h of pathol-ogy (14%), 150 h of biochemistry (11%), 120 h of microbiology (8%), and 70 h of public health (5%) [16]. Table 3.4.2 provides a glance of specific clinical subjects taught in chiropractic college and the aver-age total contact hours in chiropractic education. This includes an average of 1,975 h in clinical sciences and 1,405 h of clinical training.
A recent study comparing chiropractic and medi-cal education collected data on all chiropractic and
Table 3.4.1 Subjects taught in a typical trimester-based chiropractic program, by year and numbers of contact hours (From [16])
Year 1 Year 2 Year 3 Year 4
General anatomy (210)a Pharmacotoxicology (30) Integrated chiropractic clinical application (90)
Clinical internship (450)
Functional anatomy and biomechanics (210)
Clinical microbiology (90) Physiological therapeutics (30)
Histology (90) Pathology (135) Chiropractic principles (75)
Human biochem. (105) Chiropr. principles (60) Practice management (75)
Chiropr. principles (90) Chiropr. procedures (300) Imaging interpretation (90)
Clinical chiropractic (60) Physics and clinical imaging (90) Radiological position and technique (30)
Palpation (120) Clinical orthopedics and neurology (180)
Differential diagnosis (90)
Neuroscience (120) Nutritional assessment (60) Clinical application of manual procedures (60)
Normal radiological anatomy (90)
Community health (60) Clinical internship (390)
Human physiology (135) Physiological therapeutics (105) Dermatology (15)
Fundamentals of nutrition (60) Clinical nutrition (60) Clinical psychology (15)
Introduction to physical examination skills (120)
Research methods (30) Obstetrics/gynecology (15)
Chiropractic procedures (105) Practice management (30) Pediatrics (15)
Imaging interpretation (75) Geriatrics (15)
Differential diagnosis (90) Clinical laboratory clerkship (15)
Clinical chiropr. applied (90)
Total hours: 1,515 Total HRS: 1,485 Total HRS: 1,410 Total: 450aNumber of contact hours is noted in parentheses

873.4 The Place of Chiropractic Care in the Treatment of Low Back Pain
medical schools in North America and performed an in-depth analysis of three chiropractic and three medi-cal schools [29]. The chiropractic programs’ 4 years of undergraduate education totaling approximately 4,800 contact hours was similar to medical programs (4 undergraduate years, with approximately the same number of contact hours (4,667)), but typically with an additional 3-year residency to meet the requirements for practice. Basic science comprises 25–30% of the total contact hours in both the chiropractic and medi-cal programs and the two programs have roughly simi-lar contact hours in biochemistry, microbiology, and pathology. Chiropractors receive substantially more hours in anatomy education and physiology, but fewer in public health.
The contrast between the two programs is dramatic in the area of clinical clerkships, which averaged 3,467 h in medicine vs. 1,405 h in chiropractic. In medicine,
this comprises, on average, 74% of the total contact hours, while in chiropractic training, it comprises only 29%. Some of the difference may be explained by the manner in which chiropractic and medical programs are structured. In chiropractic, 41% of the program (averag-ing 1,975 h) is allocated to chiropractic clinical sci-ences, which consists of extensive laboratory and hands-on training in manual procedures and has no equivalent in medicine. Combining the chiropractic clinical sciences with the clinical clerkships, the per-centage of a chiropractic program devoted to clinical education is 70% compared to medicine’s 74%. The major difference, therefore, is in didactic teaching and clinical experience [16]. Thus, on average, medical stu-dents receive twice the number of hours in clinical experience, but receive over 1,000 fewer hours in lec-tures and laboratory education. If the medical residency is included, the total number of hours of clinical experi-ence for medicine increases to 6,413 [29].
Chiropractic Practice
One indicator of chiropractic mainstreaming into health-care is the steadily increasing use by patients in the United States and around the world. Studies suggest that between 30 and 50% of the adult population in industri-alized nations use some form of CAM to prevent or treat a variety of health-related problems [3]. Today, it is esti-mated that CAM is responsible for 629 million visits per year to practitioners of CAM, thereby exceeding total visits to all U.S. primary care physicians [33]. The Journal of the American Medical Association [33] reports that estimated expenditures for CAM professional ser-vices are conservatively estimated at $21.2 billion, with at least $12.2 billion paid out-of-pocket. This exceeds the 1997 out-of-pocket expenditures for all U.S. hospitaliza-tions. Clearly, efficacy and patient satisfaction are driv-ing these trends of public demand and utilization.
Of all the so-called CAM professions, chiropractic has made the largest inroads into private and public healthcare financing systems and is increasingly viewed as an effec-tive specialty by many in the medical profession. In fact, large numbers of physicians are either referring to or prac-ticing themselves some of the more prominent and well-known forms of CAM and many physicians believe that these therapies are useful or efficacious [3]. Another recent study of physicians’ attitudes toward CAM determined
Table 3.4.2 Average total contact hours in specific clinical subjects taught in 16 chiropractic colleges including lecture and laboratory (From [16])
Clinical subject Hours Percentage of Total
Adjustive technique/spinal analysis
555 22
Physical/clinical/laboratory diagnosis
410 17
Diagnostic imaging, radiology 305 12
Principles of chiropractic 245 10
Orthopedics 135 6
Physiologic therapeutics 120 5
Nutrition/dietetics 90 4
Professional practice and ethics 65 3
Biomechanics 65 3
Gynecology/obstetrics 55 2
Psychology 55 2
Research methods 50 2
Clinical pediatrics and geriatrics 50 2
First aid and emergency 45 2
Dermatology 30 1
Otolaryngology 25 1
Other 160 7
Total hours of clinical training 2,460 100

88 C. J. Colloca
that over half of providers had referred a patient for bio-feedback or chiropractic care [67].
In 1998, Astin et al. [3] published the results of their comprehensive literature search that identified 25 sur-veys that examined the practices and beliefs of conven-tional physicians with regard to five of the more prominent CAM therapies: acupuncture, chiropractic, homeopathy, herbal medicine, and massage. Across surveys, chiropractic had the highest rate of physician referral (40%) among the five CAM therapies. Approximately half of the surveyed physicians believed in the efficacy of chiropractic (53%), while fewer believed in the value of homeopathy (26%) and herbal approaches (13%). This review suggests that large numbers of physicians are either referring to or utiliz-ing some of the more prominent and well-known forms of CAM, and specifically chiropractic. Indeed, coop-erative care between doctors of chiropractic and other medical physicians is an important factor in the place of chiropractic care in the treatment of LBP.
Chiropractors play a significant role in healthcare delivery for patients. A recent study estimated that approximately 7% of U.S. adults had received chiroprac-tic treatment in the past year [32, 33]. A substantial num-ber of patients seeking care for back pain in the U.S. (25–42%) utilize chiropractic care. An analysis of the 1974–1982 RAND Health Insurance Experiment data found that chiropractors were the first healthcare provid-ers seen for 38% of episodes of back pain and that chiro-practors were the “primary” provider (i.e., the provider type that delivered the majority of care) for 40% of LBP episodes [72]. Furthermore, this study determined that chiropractors were retained as primary provider for 92% of their patients who had a second episode of back pain, compared to 75% retention for general medical practitio-ners. Thus, many back pain patients have used chiroprac-tors as first contact primary providers of care for at least this specific problem.
A recent study by Wolsko et al. [82] found that of those reporting back or neck pain in the last 12 months, 37% had seen a conventional provider and 54% had used com-plementary therapies to treat their condition. Chiropractic, massage, and relaxation techniques were the most com-monly used complementary treatments for back or neck pain (20, 14, and 12%, respectively, of those with back or neck pain). Chiropractic, massage, and relaxation tech-niques were rated as “very helpful” for back or neck pain among users (61, 65, and 43%, respectively), whereas conventional providers were rated as “very helpful” by 27% of users. It is estimated that nearly one-third of all complementary provider visits in 1997 (203 million of
629 million) were made specifically for the treatment of back or neck pain [82]. A brief review of the chiropractic patient encounter will assist in understanding the role of chiropractic care in this patient population.
The Chiropractic Patient Encounter
The majority of patients visiting doctors of chiropractic suffer musculoskeletal complaints, namely LBP, while the remainder seeks care for head, neck, or extremity pain [48]. Like in medicine, the chiropractic patient encounter begins with a detailed health history, followed by consultation, physical examination, and clinical deci-sion making to form a diagnostic impression. Chiropractic doctors are licensed to perform and interpret plain film radiography, and are less likely than medical physicians to utilize advanced diagnostic imaging [31]. Using stan-dard historical, diagnostic, and assessment procedures, chiropractors attempt to differentiate problems of mechanical vs. visceral origin [16]. Such information is critical to clinical decision making including a chiro-practic referral to the patient’s primary care physician. Some mechanical assessment strategies are common to orthopedic and physical medicine procedures [20, 28] and others are unique to chiropractic [70].
Four kinds of measurements provide relevant infor-mation about patient clinical status and/or response to treatment in chiropractic practice. In general, they are: (1) perceptual measurements (i.e., reports of pain severity and pain tolerance), (2) structural measure-ments (i.e., anomalies, pathology, or posture), (3) functional measurements (i.e., range of motion, strength, stiffness, activities of daily living), and (4) physiologic measurements (i.e., neurologic assess-ment, laboratory examinations) (Fig. 3.4.1). The chiro-practic literature is also paying increased attention to the role pain behavior and psychosocial issues play in conditions such as back pain and to the evaluation and management strategies in these areas [10].
Typical chiropractic care plans are similar to those in physical therapy, with recurring visit frequency until treatment goals are obtained or re-evaluated. Outcome measures, including pain indices, functional disabilities, perceived health status, range of motion, posture, and muscle strength, are among variables to assess patient progress. Both qualitative and quantita-tive clinical assessments are used for diagnostic and outcome assessment purposes in chiropractic practice (Table 3.4.3) [20].

893.4 The Place of Chiropractic Care in the Treatment of Low Back Pain
Chiropractic Treatment: Spinal Manipulation
The main intervention among chiropractic practitioners is spinal manipulation, also known as the chiropractic adjustment, a term preferred by many chiropractors to better characterize the perceived therapeutic effect of targeting spinal joint abnormalities [45]. There are over one-hundred distinct chiropractic, osteopathic, and physical therapy manipulation techniques, a large array of highly specialized adjusting tables and equip-ment, and a great deal of variation in the specific tech-niques used by individual practitioners [45]. Estimates have indicated that approximately 96% of SMT is per-formed by chiropractors [71].
There are four terms with distinct definitions that are frequently used to characterize manual manipulative
Posture
Anomaly
Pathology
Structural
Pain Threshold
Health Status
Outcomes
Assessment TestingMuscle
Thermography
Neurological Testing
PhysiologicalSpine
Range of Motion
Proprioception
EnduranceStiffness
Strength
Fu
nct
ion
al
Percep
tual
Fig. 3.4.1 Categorization of spine instrument measures (per-ceptual, structural, functional, and physiological) and the associ-ated tests in each category
Table 3.4.3 Qualitative clinical assessments and their quantitative counterparts examined in chiropractic practice (From [20])
Test Qualitative (findings) Quantitative (units of measurement)
Perceived pain, disability, and/or functional status
Patients’ subjective description (patient demeanor)
Outcome assessment instruments (numerical score compared to normative values)
Pain threshold or pain tolerance
Palpation for pain (tenderness, grading of trigger points)
Pressure algometry (psi, kg/cm2, or Pa)
Posture Visual postural analysis (i.e., head tilt, high shoulder, etc.)
Postural grid photographySurface topographical measures
Computer assisted digitizationDiagnostic imaging (X-ray, MRI, CT) (millimeters or
degrees)
Range of motion Visual estimation (restricted mobility, pain production or reproduction)
Inclinometric measurement Goniometric measurement (degrees)
Intersegmental range of motion
Motion palpation (articular fixation, pain)
Spinal stiffness assessments Static/quasi-static (N/m)Dynamic (Kg−1, Kg, m/Ns, Ns/m, m/N)Instantaneous axis of rotation (degrees)Instantaneous helical axis (radians)
Muscle strength Muscle testing (grading 0–5) Dynamometric measurement (kg or lbs.)Computerized and digital equipment (kg or lbs.)
Load cell or strain gauge typesB200 (kg or lbs.)EMG (mV)
Muscle endurance Muscle testing (grading 0–5) Biering-Sorensen test (time duration, sec., of task performance) EMG (median frequency analysis) (Hz)
Muscle spasm Palpatory myospasm assessment Surface electromyography (mV)
Nerve function Orthopedic/neurologic exam (i.e., mechanical tests, stretch tests, deep tendon reflex, dermatomal sensation)
Nerve conduction velocity (ms)Needle electromyography (mV)
H-Reflex (mV)Somatosensory evoked potentials (mV)Current perception threshold (mV)Thermography (degrees C or F)
Pathology History, inspection, palpation Diagnostic imaging Laboratory analysis

90 C. J. Colloca
methods: specific contact thrust procedures (i.e., high velocity, low amplitude [HVLA] thrusts), nonspecific contact thrust procedures (i.e., mobilization), manual force, mechanically-assisted procedures (i.e., drop tables or flexion-distraction tables), and mechanical force, manually-assisted procedures (i.e., stationary or hand-held instruments) [45]. The general umbrella term of spinal manipulative therapy is often used to encompass all types of manual techniques regardless of their precise anatomic and physiologic focus or their discipline of origin.
Mobilization is defined as passive movement of a joint within its physiologic range of motion. This roughly equates to the range of motion a joint can typically be taken through by its intrinsic musculature. Manipulation is passive joint movement, which takes the joint beyond its physiologic range into the paraphysiologic space. When a joint is moved into this “para-physiologic” range, cavitation can occur, which, in a synovial joint, is typified by an audible release or “pop.” The audible joint cavitation is not a necessary element of spinal manipula-tion, although its occurrence is commonplace. Studies have identified that the audible release has not been found to be associated with the neuromuscular reflex responses [21, 24] (Fig. 3.4.2) thought to be related to the mechanisms of spinal manipulation or clinical out-comes [7, 34, 35]. In contrast, although poorly under-stood, the speed of the spinal manipulative thrust has been reported to be of prime importance to the mecha-nisms of treatment [24–26, 46, 75].
Both mobilization and manipulation are used to facilitate joint motion. When applied in manual medi-cine and physical therapy, assessment and manipulative treatment tend to focus exclusively on joint pain and restriction. Chiropractors typically consider the nature and mode of condition onset, muscle spasm, pain radiation patterns, static and dynamic postures, and/or gaits as well as joint pain in determining whether or not a mechanical intervention should be applied [16]. For instance, the spinal areas manipulated using typi-cal manual medicine and physical therapy assessment approaches are often based on which joints or regions have restricted motion. In contrast to physical therapy or manual medicine, the decision as to which area to manipulate using various chiropractic techniques may be based upon pain radiation patterns, which paraspinal muscle regions are taut and how they are innervated, the biomechanical function of affected joints compared to that of adjacent areas, and the mechanics involved in
initial onset [27, 39, 40]. Thus, the regions manipulated by chiropractors may not directly correspond to the symptomatic region or to the area that a nonchiroprac-tor may feel is the site of the manipulable lesion.
Mechanisms of Spinal Manipulation
Recognizing the enormous impact of LBP to health-care, research has been conducted to elucidate the role of somatic structures as sources of LBP. In recent years, neurophysiologic and neuroanatomic investigations have been conducted to identify and characterize somatosen-sory units located within the tissues of the lumbar spine to clarify their role in LBP. Devices such as glass rods, metal probes, nylon threads, and electrical impulses have been used to mechanically stimulate somatic structures and afferent units [4, 11, 60, 86]. Mechanosensitive and nociceptive afferents have been identified in the lumbar intervertebral disks [5, 12, 61, 66], zygapophyseal joints [13, 55, 56, 86], spinal ligaments [11, 49, 50, 85], and the paraspinal musculature [6, 87] in both animal and human studies. This research, and that of others [53], has identified these tissues as probable sources of LBP and somatic referred pain [6, 30, 39, 59]. Spinal nerve roots and dorsal root ganglia have also been shown to be the
Fig. 3.4.2 Dynamic spinal stiffness assessment is performed with a hand-held electromechanical device equipped with an impedance head (Impulse iQ® Adjusting Instrument, Neuro-mechanical Innovations, Chandler, AZ, U.S.A.), while simulta-neous electromyographic (EMG) measurement is obtained from the adjacent erector spinae muscles. In this manner the muscular contributions to spinal stiffness can be taken into consideration during the neuromechanical assessment

913.4 The Place of Chiropractic Care in the Treatment of Low Back Pain
source of radicular pain [15, 38]. Beneficial effects of SMT have been thought to be associated with mechano-sensitive afferent stimulation and presynaptic inhibition of nociceptive afferent transmission in the modulation of pain [81, 83], inhibition of hypertonic muscles [76], and improvement of functional ability [57, 71, 77].
While the mechanisms of spinal manipulation remain poorly understood, its beneficial clinical effects are thought to be related to mechanical, neurophysiologic, and reflexogenic mechanisms [47]. Mechanical models have evolved with the theory that spinal manipulation produces realignment and improved function of mis-aligned and dysfunctional functional spinal units (FSUs) resultant from the spinal manipulative treatment, thus referred to as chiropractic adjustment [78]. Recent evi-dence has demonstrated that significant FSU move-ments are produced by spinal manipulation in selected treatments applied to animal models [24, 25, 36, 73] and in human studies [37, 51, 52, 62]. Neurophysiologic models theorize that spinal manipulation may also stim-ulate or modulate the somatosensory system and subse-quently may evoke neuromuscular reflexes [19, 21–23, 26, 47, 65, 84]. Such mechanical and neurophysiologic studies suggest that joint manipulation may have both direct and indirect clinical benefits. Research efforts have further measured neuromuscular and neurophysi-ological responses of spinal manipulation thought to be associated with nociceptive inhibition [41–44, 64]. The heterogeneity of spinal pain, along with the lack of definitive diagnoses, highlights the need to better under-stand the underlying physiologic and psychological mechanisms of pain and disability and the role chiro-practic care plays in patient care.
Clinical Outcomes of Spinal Manipulation for Low Back Pain
Spinal manipulation is one of the most widely studied conservative treatments for spinal pain. To date, over 100 randomized controlled clinical trials (RCTs) on some form of spinal manipulation have appeared in the literature [58]. Nearly half of the RCTs have studied the effects of spinal manipulation on acute, subacute, and chronic LBP. Although the results are controversial, over half of these studies favored spinal manipulation over the comparison treatments in at least a subgroup of patients. Subsequent systematic reviews have reported
that there was moderately strong evidence of a short-term benefit of manipulation for both acute and chronic back pain, but insufficient evidence for or against the effectiveness of manipulation for sciatica.
In a 2003 metaanalysis of the effectiveness of spinal manipulative therapy for LBP relative to other therapies, Assendelft and co-workers’ [2] spinal manipulative therapy was found to have similar outcome effective-ness when compared to general practitioner care, anal-gesics, physical therapy, exercises, or back school. In this work, spinal manipulative therapy had clinically and statistically significant benefits only when it was compared with either sham manipulation or the group of therapies judged to be ineffective or even harmful.
Despite the many published randomized clinical tri-als (RCTs), a substantial number of reviews, and sev-eral national clinical guidelines, much controversy still remains regarding the evidence for or against efficacy of spinal manipulation for LBP. An extensive system-atic review and best evidence synthesis was conducted by Bronfort and colleagues in 2004 [9] to reassess the efficacy of spinal manipulative therapy and mobiliza-tion for the management of LBP, with special attention to applying more stringent criteria for study admissibil-ity into evidence and for isolating the effect of manipu-lation and/or mobilization. In this report, 69 RCTs met the study selection criteria and were reviewed and assigned validity scores varying from 6 to 81 on a scale of 0–100. Forty-three RCTs met the admissibility crite-ria for evidence. The following conclusions were made for acute and chronic LBP and their mix [9]:
• Acute LBP: There is moderate evidence that spinal manipulation provides more short-term pain relief than mobilization and detuned diathermy, and lim-ited evidence of faster recovery than a commonly used physical therapy treatment strategy.
• Chronic LBP: There is moderate evidence that manipulation has an effect similar to an efficacious prescription nonsteroidal antiinflammatory drug; manipulation/mobilization is effective in the short term when compared with placebo and general practitioner care, and in the long term compared to physical therapy. There is limited to moderate evi-dence that spinal manipulation is better than physi-cal therapy and home back exercise in both the short and long term. There is limited evidence that spinal manipulation is superior to sham manipulation in the short term and superior to chemonucleolysis for

92 C. J. Colloca
disk herniation in the short term. However, there is also limited evidence that mobilization is inferior to back exercise after disk herniation surgery.
• Mix of Acute and Chronic LBP: Spinal manipula-tion/mobilization provides either similar or better pain outcomes in the short and long term when compared with placebo and with other treatments, such as McKenzie therapy, medical care, manage-ment by physical therapists, soft tissue treatment, and back school.
The positive reports for the clinical effectiveness of spi-nal manipulation have recently paved way for the inclu-sion of spinal manipulation into well-established clinical guidelines, as recently been published in the American Pain Society/American College of Physicians Clinical Practice Guideline [18]. Chou et al. [18] assessed the benefits and harms of a number of interventions includ-ing spinal manipulation for acute and chronic LBP (with and without leg pain). The authors recommended, “for patients who do not improve with self-care options, clinicians should consider the addition of nonharmco-logic therapy with proven benefits – for acute, chronic or subacute LBP, spinal manipulation …” among other established interventions. Further research is necessary to better understand which patients respond best to chiropractic interventions. Moreover, while preliminary evidences for spinal manipulation in patients with disk protrusion and sciatica are encouraging [8, 69], continued investigations will assist in better understand-ing the effects of chiropractic care in this patient population.
Conclusions
The chiropractic profession has evolved in its educa-tion and training and research status to be an accepted healthcare provider for patients with many musculosk-eletal conditions including LBP. In the past few decades, chiropractic has strengthened its educational system; initiated research that has validated spinal manipulation; increased its market share of satisfied patients; initiated collaborations with other disciplines in practice, research, and professional settings; and effectively used political, legislative, and legal mea-sures to secure a role [58]. Continued progress toward multidisciplinary cooperative efforts will assist patients who benefit from the care of chiropractic providers.
References
1. Asche CV, Kirkness CS, dam-Marx C, Fritz JM (2007) The societal costs of low back pain: data published between 2001 and 2007. J Pain Palliat Care Pharmacother 21:25–33
2. Assendelft WJ, Morton SC, Yu EI, Suttorp MJ, Shekelle PG (2003) Spinal manipulative therapy for low back pain. A meta-analysis of effectiveness relative to other therapies. Ann Intern Med 138:871–881
3. Astin JA, Marie A, Pelletier KR, Hansen E, Haskell WL (1998) A review of the incorporation of complementary and alternative medicine by mainstream physicians. Arch Intern Med 158:2303–2310
4. Avramov AI, Cavanaugh JM, Ozaktay CA, Getchell TV, King AI (1992) The effects of controlled mechanical loading on group-II, III, and IV afferent units from the lumbar facet joint and surrounding tissue. An in vitro study. J Bone Joint Surg Am 74:1464–1471
5. Bogduk N (1983) The innervation of the lumbar spine. Spine 8:286–293
6. Bogduk N, Twomey LT (1991) Clinical anatomy of the lum-bar spine, 2nd edn. Churchill Livingstone, Edinburgh
7. Brodeur R (1995) The audible release associated with joint manipulation. J Manipulative Physiol Ther 18:155–164
8. Bronfort G, Evans RL, Anderson AV, Schellhas KP, Garvey TA, Marks RA, Bittell S (2000) Nonoperative treatments for sciatica: a pilot study for a randomized clinical trial. J Manipulative Physiol Ther 23:536–544
9. Bronfort G, Haas M, Evans RL, Bouter LM (2004) Efficacy of spinal manipulation and mobilization for low back pain and neck pain: a systematic review and best evidence syn-thesis. Spine J 4:335–356
10. Cauffield JS (2000) The psychosocial aspects of comple-mentary and alternative medicine. Pharmacotherapy 20: 1289–1294
11. Cavanaugh JM, el-Bohy A, Hardy WN, Getchell TV, Getchell ML, King AI (1989) Sensory innervation of soft tissues of the lumbar spine in the rat. J Orthop Res 7: 378–388
12. Cavanaugh JM, Kallakuri S, Ozaktay AC (1995) Innervation of the rabbit lumbar intervertebral disc and posterior longitu-dinal ligament. Spine 20:2080–2085
13. Cavanaugh JM, Ozaktay AC, Yamashita HT, King AI (1996) Lumbar facet pain: biomechanics, neuroanatomy and neuro-physiology. J Biomech 29:1117–1129
14. Chapman-Smith DA (1997) Legislative approaches to the regulation of the chiropractic profession. Med Law 16: 437–449
15. Chatani K, Kawakami M, Weinstein JN, Meller ST, Gebhart GF (1995) Characterization of thermal hyperalgesia, c-fos expression, and alterations in neuropeptides after mechani-cal irritation of the dorsal root ganglion. Spine 20:277–289
16. Cherkin DC, Mootz RD (1997) Chiropractic in the United States: training, practice, and research. Research Summary. AHCPR Publication No. 98-N002
17. Cherkin DC, Deyo RA, Loeser JD, Bush T, Waddell G (1994) An international comparison of back surgery rates. Spine 19:1201–1206
18. Chou R, Huffman LH (2007) Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American pain society/American college of physicians clinical practice guideline. Ann Intern Med 147:492–504

933.4 The Place of Chiropractic Care in the Treatment of Low Back Pain
19. Colloca CJ (1997) Articular neurology, altered biomechan-ics, and subluxation pathology. In: Fuhr A, Colloca CJ, Green JR, Kellar TS (eds) Activator methods chiropractic technique. Mosby, St. Louis, pp 19–64
20. Colloca CJ, Keller TS, Lehman GJ, Harrison DD (2005) The use of measurement instruments in chiropractic practice, In: Principles and Practice of Chiropractic, 3rd edn. pp 629–659
21. Colloca CJ, Keller TS (2001) Electromyographic reflex response to mechanical force, manually-assisted spinal manipulative therapy. Spine 26:1117–1124
22. Colloca CJ, Keller TS, Gunzburg R, Vandeputte K, Fuhr AW (2000) Neurophysiologic response to intraoperative lum-bosacral spinal manipulation. J Manipulative Physiol Ther 23:447–457
23. Colloca CJ, Keller TS, Gunzburg R (2003) Neuromechanical characterization of in vivo lumbar spinal manipulation. Part II. Neurophysiological response. J Manipulative Physiol Ther 26:579–591
24. Colloca CJ, Keller TS, Harrison DE, Moore RJ, Gunzburg R, Harrison DD (2006) Spinal manipulation force and dura-tion affect vertebral movement and neuromuscular responses. Clin Biomech, 21:254–262
25. Colloca CJ, Keller TS, Moore RJ, Gunzburg R, Harrison DE (2007) Intervertebral disc degeneration reduces vertebral motion responses. Spine 32:E544–E550
26. Colloca CJ, Keller TS, Moore RJ, Gunzburg R, Harrison DE (2008) Effects of disc degeneration on neurophysiological responses during dorsoventral mechanical excitation of the ovine lumbar spine. J Electromyogr Kinesiol 18(5): 829–837
27. Cooperstein R, Perle SM, Gatterman MI, Lantz C, Schneider MJ (2001) Chiropractic technique procedures for specific low back conditions: characterizing the literature. J Mani-pulative Physiol Ther 24:407–424
28. Coulehan JL (1985) Chiropractic and the clinical art. Soc Sci Med 21:383–390
29. Coulter ID, Hurwitz EL, Adams AH, Genovese BJ, Hays R, Shekelle PG (2002) Patients using chiropractors in North America: who are they, and why are they in chiropractic care? Spine 27:291–298
30. Cramer GD, Darby SA (1995) Basic and clinical anatomy of the spine, spinal cord, and ANS
31. de Zoete A, Assendelft WJ, Algra PR, Oberman WR, Vanderschueren GM, Bezemer PD (2002) Reliability and validity of lumbosacral spine radiograph reading by chiro-practors, chiropractic radiologists, and medical radiologists. Spine 27:1926–1933
32. Eisenberg DM, Kessler RC, Foster C, Norlock FE, Calkins DR, Delbanco TL (1993) Unconventional medicine in the United States. Prevalence, costs, and patterns of use. N Engl J Med 328:246–252
33. Eisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S, Van Rompay M, Kessler RC (1998) Trends in alternative medicine use in the United States, 1990–1997: results of a follow-up national survey. JAMA 280:1569–1575
34. Flynn TW, Fritz JM, Wainner RS, Whitman JM (2003) The audible pop is not necessary for successful spinal high-velocity thrust manipulation in individuals with low back pain. Arch Phys Med Rehabil 84:1057–1060
35. Flynn TW, Childs JD, Fritz JM (2006) The audible pop from high-velocity thrust manipulation and outcome in individu-als with low back pain. J Manipulative Physiol Ther 29: 40–45
36. Fuhr AW, Smith DB (1986) Accuracy of piezoelectric accel-erometers measuring displacement of a spinal adjusting instrument. J Manipulative Physiol Ther 9:15–21
37. Gal J, Herzog W, Kawchuk G, Conway PJ, Zhang YT (1997) Movements of vertebrae during manipulative thrusts to unembalmed human cadavers. J Manipulative Physiol Ther 20:30–40
38. Garfin SR, Rydevik B, Lind B, Massie J (1995) Spinal nerve root compression. Spine 20:1810–1820
39. Gatterman MI (1995) Foundations of chiropractic: sublux-ation. Mosby, St. Louis
40. Gatterman MI, Cooperstein R, Lantz C, Perle SM, Schneider MJ (2001) Rating specific chiropractic technique procedures for common low back conditions. J Manipulative Physiol Ther 24:449–456
41. Gillette RG (1986) Potential antinocieptive effects of high level somatic stimulation – chiropractic manipulation ther-apy may coactivate both tonic and phasic analgesic systems. Some recent evidence. Trans Pac Consortium Res 1:A4 (1)–A4(9)
42. Gillette RG (1987) A speculative argument for the coactiva-tion of diverse somatic receptor populations by forceful chi-ropractic adjustments. A review of the neurophysiologic literature. Man Med 3:1–14
43. Gillette RG, Kramis RC, Roberts WJ (1994) Sympathetic activation of cat spinal neurons responsive to noxious stimu-lation of deep tissues in the low back. Pain 56:31–42
44. Gillette RG, Kramis RC, Roberts WJ (1998) Suppression of activity in spinal nocireceptive ‘low back’ neurons by paraver-tebral somatic stimuli in the cat. Neurosci Lett 241: 45–48
45. Haldeman S, Chapman-Smith D, Petersen DM (1993) Guidelines for chiropractic quality assurance and practice parameters. Aspen, Gaithersburg, MD
46. Herzog W (1996) On sounds and reflexes. J Manipulative Physiol Ther 19:216–218
47. Herzog W, Scheele D, Conway PJ (1999) Electromyographic responses of back and limb muscles associated with spinal manipulative therapy. Spine 24:146–152
48. Hurwitz EL, Coulter ID, Adams AH, Genovese BJ, Shekelle PG (1998) Use of chiropractic services from 1985 through 1991 in the United States and Canada. Am J Public Health 88:771–776
49. Imai S, Hukuda S, Maeda T (1995) Dually innervating noci-ceptive networks in the rat lumbar posterior longitudinal ligaments. Spine 20:2086–2092
50. Jiang H, Russell G, Raso VJ, Moreau MJ, Hill DL, Bagnall KM (1995) The nature and distribution of the innervation of human supraspinal and interspinal ligaments. Spine 20: 869–876
51. Keller TS, Colloca CJ, Gunzburg R (2003) Neuromechanical characterization of in vivo lumbar spinal manipulation. Part I. Vertebral motion. J Manipulative Physiol Ther 26:567–578
52. Keller TS, Colloca CJ, Moore RJ, Gunzburg R, Harrison DE, Harrison DD (2006) Three-dimensional vertebral motions produced by mechanical force spinal manipulation. J Manipulative Physiol Ther 29:425–436
53. Kuslich SD, Ulstrom CL, Michael CJ (1991) The tissue ori-gin of low back pain and sciatica: a report of pain response to tissue stimulation during operations on the lumbar spine using local anesthesia. Orthop Clin North Am 22:181–187
54. Lamm LC, Wegner E, Collord D (1995) Chiropractic scope of practice: what the law allows–update 1993. J Manipulative Physiol Ther 18:16–20

94 C. J. Colloca
55. Li QH, Cavanaugh JM, Ozaktay AC, King AI (1995) The relationship between local facet load and nerve discharge in the lumbar facet and surrounding tissue. Trans Orthop Res Soc 20:303
56. McLain RF, Pickar JG (1998) Mechanoreceptor endings in human thoracic and lumbar facet joints. Spine 23:168–173
57. Meade TW, Dyer S, Browne W, Frank AO (1995) Randomised comparison of chiropractic and hospital outpa-tient management for low back pain: results from extended follow up. BMJ 311:349–351
58. Meeker WC, Haldeman S (2002) Chiropractic: a profession at the crossroads of mainstream and alternative medicine. Ann Intern Med 136:216–227
59. Milette PC, Fontaine S, Lepanto L, Breton G (1995) Radiating pain to the lower extremities caused by lumbar disk rupture without spinal nerve root involvement [see comments]. AJNR Am J Neuroradiol 16:1605–1613
60. Minaki Y (1996) An electrophysiological study on the mechanoreceptors in the lumbar spine and adjacent tissues. Neuro-Orthopedics 20:23–35
61. Nakamura S, Takahashi K, Takahashi Y, Morinaga T, Shimada Y, Moriya H (1996) Origin of nerves supplying the posterior portion of lumbar intervertebral discs in rats. Spine 21:917–924
62. Nathan M, Keller TS (1994) Measurement and analysis of the in vivo posteroanterior impulse response of the human thoracolumbar spine: a feasibility study. J Manipulative Physiol Ther 17:431–441
63. Pelletier KR, Astin JA (2002) Integration and reimburse-ment of complementary and alternative medicine by man-aged care and insurance providers: 2000 update and cohort analysis. Altern Ther Health Med 8:38–9, 42, 44
64. Pickar JG (2002) Neurophysiological effects of spinal manipulation. Spine J 2:357–371
65. Pickar JG, McLain RF (1995) Responses of mechanosensi-tive afferents to manipulation of the lumbar facet in the cat. Spine 20:2379–2385
66. Roberts S, Eisenstein SM, Menage J, Evans EH, Ashton IK (1995) Mechanoreceptors in intervertebral discs. Morphology, distribution, and neuropeptides. Spine 20: 2645–2651
67. Rooney B, Fiocco G, Hughes P, Halter S (2001) Provider attitudes and use of alternative medicine in a midwestern medical practice in 2001. WMJ 100:27–31
68. Rupert RL, Manello D, Sandefur R (2000) Maintenance care: health promotion services administered to US chiro-practic patients aged 65 and older, part II. J Manipulative Physiol Ther 23:10–19
69. Santilli V, Beghi E, Finucci S (2006) Chiropractic manipula-tion in the treatment of acute back pain and sciatica with disc protrusion: a randomized double-blind clinical trial of active and simulated spinal manipulations. Spine J 6:131–137
70. Schaefer RC, Faye LJ (1990) Motion palpation and chiro-practic technique, 2nd edn. Motion Palpation Institute, Huntington Beach, CA
71. Shekelle PG (1994) Spinal manipulation. Spine 19: 858–861
72. Shekelle PG, Adams AH, Chassin MR, Hurwitz EL, Brook RH (1992) Spinal manipulation for low-back pain. Ann Intern Med 117:590–598
73. Smith DB, Fuhr AW, Davis BP (1989) Skin accelerometer displacement and relative bone movement of adjacent verte-brae in response to chiropractic percussion thrusts. J Manipulative Physiol Ther 12:26–37
74. Stano M, Smith M (1996) Chiropractic and medical costs of low back care. Med Care 34:191–204
75. Suter E, Herzog W, Conway PJ, Zhang YT (1994) Reflex response associated with manipulative treatment of the tho-racic spine. J Neuromusculoskeletal Syst 2:124–130
76. Thabe H (1986) Electromyography as a tool to document diagnostic findings and therapeutic results associated with somatic dysfunctions in the upper cervical spinal joints and sacroiliac joints. Man Med 2:53–58
77. Triano JJ, McGregor M, Hondras MA, Brennan PC (1995) Manipulative therapy versus education programs in chronic low back pain. Spine 20:948–955
78. Troyanovich SJ, Harrison DE, Harrison DD (1998) Structural rehabilitation of the spine and posture: rationale for treat-ment beyond the resolution of symptoms. J Manipulative Physiol Ther 21:37–50
79. van Tulder MW, Koes BW, Bouter LM (1997) Conservative treatment of acute and chronic nonspecific low back pain. A systematic review of randomized controlled trials of the most common interventions. Spine 22:2128–2156
80. Waddell G (1996) Low back pain: a twentieth century health care enigma. Spine 21:2820–2825
81. Willis W, Coggeshall R (1991) Sensory mechanisms of the spinal cord, 2nd edn. Plenum, New York
82. Wolsko PM, Eisenberg DM, Davis RB, Kessler R, Phillips RS (2003) Patterns and perceptions of care for treatment of back and neck pain: results of a national survey. Spine 28:292–297
83. Wyke B (1980) Articular neurology and manipulative ther-apy. Lincoln Institute of Health Sciences, Carlton, Victoria, pp 67–72
84. Wyke B (1985) Articular neurology and manipulative ther-apy. In: Glasgow E, Twomey L, Scull E, Kleynhans A, Idczak R (eds) Aspects of manipulative therapy. Churchill-Livingstone, New York, pp 72–77
85. Yahia LH, Newman N, Rivard CH (1988) Neurohistology of lumbar spine ligaments. Acta Orthop Scand 59:508–512
86. Yamashita T, Cavanaugh JM, el-Bohy AA, Getchell TV, King AI (1990) Mechanosensitive afferent units in the lum-bar facet joint. J Bone Joint Surg [Am] 72:865–870
87. Yamashita T, Minaki Y, Oota I, Yokogushi K, Ishii S (1993) Mechanosensitive afferent units in the lumbar intervertebral disc and adjacent muscle. Spine 18:2252–2256

95M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_3.5, © Springer-Verlag Berlin Heidelberg 2010
Percutaneous intradiscal thermocoagulation techniques were introduced in 2000 by Saal et al. [1] as a mini-mally invasive treatment option for patients with dis-cogenic low back pain (LBP). Controlled thermal energy is delivered to the intervertebral disc via a per-cutaneous intradiscal catheter inserted under radio-logical guidance. There are two different techniques depending on whether the heat is generated by a ther-mal resistive coil (Intra-Discal Electrothermal Therapy [IDET]) or radiofrequency (Percutaneous Intradiscal Radio-Frequency Thermocoagulation [PIRFT]). The objective of both techniques is to shrink collagen fibrils and thermocoagulate inflammatory and neural tissues within the disc. This chapter reviews the current litera-ture and assesses the safety and efficacy of both proce-dures in the treatment of discogenic LBP.
Intra-Discal Electrothermal Therapy (IDET)
The IDET technique involves placement of a navigable intradiscal catheter (Fig. 3.5.1) (Smith and Nephew Inc, Andover, Massachusetts, USA) with a tempera-ture-controlled thermal resistive heating coil to a final position at the inner posterior annulus (Fig. 3.5.2a, b). The standard heating protocol raises the catheter tip temperature from 65 to 90°C over 12.5 min. The tem-perature is maintained at 90°C for 4 min. According to Saal et al., this creates annular temperatures between
60 and 65°C [1]. The authors proposed the mechanism of action of IDET to be a combination of thermo-coag-ulation of native nociceptors and in-grown un-myeli-nated nerve fibres plus annular collagen shrinkage stabilizing annular fissures.
There followed a number of prospective cohort stud-ies reporting favourable outcomes following IDET [1–6] and some less favourable [7, 8]. Saal et al. reported on the 24 month outcome in a cohort of 62 patients [6]. The mean visual analogue score (VAS) dropped from 6.57 to 3.41. The average sitting time increased by 52.7 min. Eighty-one percent of patients showed at least a 7.0 point improvement in physical function and 78% at least a 7.0 point improvement in bodily pain, as measured by the Short-Form 36 (SF-36) questionnaire. Derby et al. reported 32 consecutive cases of IDET
Efficacy of IDET and PIRFT for the Treatment of Discogenic Low Back Pain
Brian J. C. Freeman
B. J. C. Freeman Department of Spinal Surgery, Level 3, Theatre Block, Royal Adelaide Hospital, North Terrace, Adelaide, SA 5000, Australia e-mail: [email protected]
3.5
Fig. 3.5.1 Patient in the prone position. Introducer needles have been positioned in both the L4/5 and the L5/S1 discs using a pos-tero-lateral approach. IDET catheters have been positioned to cover the posterior annulus and the L4/5 IDET catheter has been connected to the generator (from Freeman [32], with permission)

96 B. J. C. Freeman
treating both discrete annular fissures and global disc degeneration [2]. The mean VAS improved by 1.84 (Standard Deviation [SD] ± 2.38) and the mean Roland Morris score improved by 4.03 (SD ± 4.82). No signifi-cant difference was noted in the outcome measures reported at 6 months and 12 months. Overall, 62.5% had a favourable outcome, 25% no change and 12.5% had a non-favourable outcome. One patient underwent a spine fusion due to persistent discogenic LBP.
A number of low quality retrospective studies were reported in the literature, some positive [10] and some negative [9, 11, 12]. Webster et al. investigated the out-come of workers’ compensation claimants following IDET [13]. The authors identified 142 cases treated by 97 different healthcare providers. The mean follow-up was 22 months. Ninety-six (68%) of the cases did not meet one or more of the published inclusion criteria. Fifty-three of one hundred and forty-two cases (37%) had at least one lumbar injection and 32 of 142 cases (23%) had lumbar surgery after IDET. The procedure appeared to be less effective when performed by a variety of providers, compared to the original series performed by single providers.
In a prospective quasi-controlled study, Karasek reported on 53 patients who were offered IDET for treatment of LBP due to internal disc disruption [14]. Authority to undergo IDET was sought from the patient’s insurance carriers. Authority was obtained in 36, but denied in 17. The 36 patients constituted the treatment group and underwent IDET. The 17 patients constituted the “control” group and underwent a reha-bilitation programme. The control group was followed for 3 months: the median VAS was 8 (range 5–8) before rehabilitation and 8 (range 7–8) at 3 months. The IDET
group had a median VAS of 8 (range 7–9) before treat-ment reducing to 3 (range 1–7) at 12 months. The authors concluded that IDET relieved discogenic pain, had a success rate between 20 and 60% and was supe-rior to physical rehabilitation. Bogduk subsequently reported the 24 month outcome in the IDET group [15]. Fifty-four percent of patients reduced their pain by half, with one in five patients achieving complete relief of pain. This study has a number of methodolog-ical flaws and its conclusions are at best speculative.
Pauza et al. reported a randomized placebo-controlled trial of IDET for the treatment of chronic discogenic LBP [16]. Under light sedation, the 17-guage introducer needle was inserted down to the outer aspect of the annu-lus fibrosus. At this point, the randomization schedule was revealed to the principle investigator. Randomization employed a 3:2 ratio (3 IDET: 2 sham). For those ran-domized to active treatment, the intra-discal catheter was inserted and appropriately positioned, followed by the standard heating protocol. For those randomized to sham treatment, the introducer needle remained in position, but no catheter was inserted. The patient was exposed to a fluoroscope monitor showing passage of an intra-discal catheter and manufactured generator noises for 16.5 min to mimic an active treatment. Outcomes including VAS, SF-36 and Oswestry Disability Index (ODI) were assessed prior to treatment and after 6 months. Publicizing the study attracted enquiries from 4,253 people. From 1,360 individuals prepared to submit to randomization, 260 (19.1%) were found poten-tially eligible after clinical examination and 64 became eligible after lumbar discography (4.7%). Thirty-seven were allocated to IDET and 27 to sham treatment. After treatment, eight patients (12.5%) violated the study
baFig. 3.5.2 (a) Antero-posterior and (b). Lateral radiograph showing optimal position of IDET catheter in the L4/5 disc (from Freeman [32], with permission)

973.5 Efficacy of IDET and PIRFT for the Treatment of Discogenic Low Back Pain
protocol mandating rejection from the analysis, leaving a total of 56 patients: 32 from the IDET group and 24 from the sham group. Both groups exhibited signifi-cant improvement in the VAS, but improvements in the IDET group were greater than the sham group (p > 0.045). For patients in the IDET group, the mean VAS dropped from 6.6 to 4.2, (SD 2.3) and the mean ODI dropped 31 to 20 (SD 11). For patients in the sham group, the mean VAS dropped from 6.5 to 5.4 (SD 2.6) and the mean ODI dropped from 33 to 28 (SD 12). Taking this into context, the “advantage” for IDET patients over sham patients was 1.3 points on the VAS (p > 0.045) and seven points on the ODI (p > 0.05). There were no significant differences in the SF-36 sub-sets bodily pain or physical function between groups. IDET was not a universally successful treatment; 50% of patients did not experience any appreciable benefit and 40% of patients achieved greater than 50% relief of their pain.
Freeman et al. conducted a prospective, random-ized, double-blind, placebo-controlled trial with cross-over offered to the placebo subjects when un-blinding occurred at 6 months [17]. A total of 57 subjects were enrolled without inducement, according to strict inclu-sion and exclusion criteria. All subjects had chronic discogenic LBP, marked functional disability, degen-erative disc disease as evidenced by magnetic reso-nance scan, failed conservative management and one or two-level symptomatic disc degeneration as determined by provocative lumbar discography followed by post-discography computed tomography. The study adopted a 2:1 (IDET: Placebo) randomization schedule. From 57 subjects, 38 were randomized to IDET and 19 to sham treatment. Under light neuroleptic anaesthesia, the 17-gauge introducer needle was inserted followed by successful deployment of the IDET catheter in all cases. The catheter lead was passed to an independent technician. This technician then opened a sealed enve-lope to ascertain the randomization schedule and covertly either connected the catheter to the generator (active IDET group) or did not (sham group). Both sur-geon and subject were blinded to this step. The stan-dard heating protocol was followed. Subjects were reviewed at 6 weeks and 6 months by an independent observer. Outcome measures recorded at baseline and 6 months included the VAS (back pain), the LBP out-come score (LBOS), the ODI, the SF-36 (Australian version), the Zung Depression Index (ZDI), the Modified Somatic Perception Questionnaire (MSPQ),
sitting tolerance, work tolerance, medication and the presence of any neurological deficit. Successful out-come was defined as one demonstrating all of the following: No neurological deficit resulting from the procedure, an improvement in the LBOS of seven or more points and an improvement in the SF-36 sub-scales bodily pain and physical functioning of greater than one SD from the mean. The 2:1 (IDET: Placebo) randomization produced two groups with well-matched baseline outcome scores. Two subjects (both from IDET group) from 57 (3.5%) withdrew from the study and subsequently went on to have spinal fusion. No subject in either treatment arm met the joint criteria for “success”. The specified primary analysis showed no difference between the treatments. Secondary out-comes were compared at baseline and 6 months. These included comparisons of change in LBOS, ODI, Zung Depression Inventory, MSPQ and SF-36 scores. There were no significant changes in any of the aforemen-tioned outcome measures. No fewer than eight sub-group analyzes were undertaken to search for any significant differences between groups. No statistically significant or clinically important differences were noted. There were no serious adverse events in either group. Transient radiculopathy (<6 weeks) was reported in four subjects who underwent IDET and in one sub-ject who underwent the sham procedure.
Pauza et al. concluded that IDET is “an effective treatment for discogenic LBP”; however, there was modest overall benefit and some patients did not ben-efit at all [16]. Freeman et al. showed no significant benefit from IDET over placebo [17]. These two ran-domized controlled trials (RCTs) report inconsistent results. There are important differences between the two studies such as the inclusion criteria, severity of patient disease, how the sham procedures were per-formed, the blinding procedure, and how success and the mean clinically important differences were defined. These differences are highlighted in Table 3.5.1. Whilst Pauza et al. appear to show statistically significant dif-ferences between the groups, others have argued the effect size is clinically irrelevant [18].
Safety Issues
Complications following IDET reported in the litera-ture include dural puncture, headaches [9], catheter

98 B. J. C. Freeman
breakage [19, 20], nerve root injury, disc herniation [21], cauda equina syndrome [22–24], vertebral body osteonecrosis [25, 26] and discitis [11].
Percutaneous Intradiscal Radio-Frequency Thermocoagulation (PIRFT)
Barendse reported on a variation of percutaneous intra-discal thermocoagulation using heat generated by radiofrequency in 2001 [27]. The “lesion” was made in the centre of the disc using a radiofrequency probe (Radionics, Burlington, MA, USA). It has been specu-lated that the anti-nociceptive effect of PIRFT is caused by a temperature increase of the free nerve endings in the outer annulus fibrosus. Barendse et al. conducted a randomized controlled trial (RCT) of PIRFT for
chronic discogenic LBP [27]. Thirteen patients were randomized to receive a 90-s 70°C lesion and 15 were allocated to the sham group. Eight weeks following treatment there were two treatment successes in the “sham group” and one in the “lesion group”. No sig-nificant differences were observed in the pre and post-VAS, global perceived effect or ODI in either group. The authors concluded that PIRFT was not effective in reducing chronic discogenic LBP.
Ercelen conducted a RCT comparing two different modalities of PIRFT [28]. The radiofrequency probe was heated to 80°C and either held for 120 or 360 s. Pain and disability were assessed at 6 months. As com-pared with baseline values, pain and disability improved by 1 month in both groups, but this effect disappeared from the second month. The final outcome measures at 6 months were similar to those measured at the begin-ning of the study. Finch et al. reported on the use
Table 3.5.1 Comparison of the two randomized controlled trials (RCTs) assessing efficacy of IDET vs. placebo
Study Freeman et al. [20] Pauza et al. [4]
Start date of trial November 1999 September 2000
Study total (N) 57 64
Withdrawn or loss to follow up 2 (3.5%) 8 (12.5%)
Mean age (years) IDET 37.5 IDET 42Placebo 40.2 Placebo 40
Disc height Up to 50% loss Up to 20% loss
Disc morphology Discrete annular tear or global degeneration
Posterior annular tear only
Worker compensation (% in each group) IDET 55.3 Excluded from studyPlacebo 57.9
Duration of symptoms (months) IDET 41 IDET 78% over 24Placebo 66 Placebo 74% over 24
ODI baseline IDET 41.4 IDET 32Placebo 40.7 Placebo 33
SF-36 PF baseline IDET 41.8 IDET 54Placebo 35.0 Placebo 48
SF-36 BP baseline IDET 33.1 IDET 35Placebo 24.4 Placebo 35
Definition of success No neurological deficit Comparison of mean categorical outcomesLBOS > 7.0SF-36 PF > 1 SD
SF-36 BP > 1 SD
ODI oswestry disability index: higher score indicates greater disability; PF physical function sub-set of SF-36: higher score indi-cates better physical function; BP bodily pain sub-set of SF-36: higher score indicates lower levels of pain
Adapted from Freeman et al. [17], with permission

993.5 Efficacy of IDET and PIRFT for the Treatment of Discogenic Low Back Pain
of a flexible radiofrequency electrode (discTRODE, Valleylab, Boulder, Colorado, USA) in a prospective case-control study to determine the efficacy of radiof-requency heating of painful annular tears [29]. Thirty-one patients underwent the procedure. A further 15 patients were unable to obtain funding for the proce-dure and served as the “control” group. Pain and dis-ability decreased significantly over 12 months in the radiofrequency group, but remained unchanged in the untreated “control” subjects.
PIRFT vs. IDET
Karpural et al. carried out a small non-randomized comparison of IDET with intradiscal radio-frequency ablation (RFA) [30]. The authors reported the 12 month outcome for each cohort (21 patients in each group). For the IDET group, the mean VAS dropped from 7.9 to 1.4 compared to 6.6 to 4.4 for the RFA group. Larger improvements in the pain disability index were noted in the IDET group.
Conclusions
Initial reports from the originators of IDET were posi-tive [1, 5, 6]. Further retrospective and prospective studies carried out at beta sites were much less impres-sive. Two RCTs addressing the effectiveness of IDET provided inconsistent evidence [16, 17]. One RCT demonstrated a positive effect on pain severity only [16], whilst the other study demonstrated no substan-tial benefit from the procedure [17].
Results from RCTs show that PIRFT is not effective in the treatment of discogenic LBP [27, 28]. The avail-able evidence does not support the continued use of IDET or PIRFT for the treatment of discogenic LBP.
These procedures have been associated with poten-tially serious side effects. Despite this, more than 75,000 IDET procedures have been performed in the United States alone since 1998 [31]. One can only assume that the minimally invasive nature of this inter-vention encourages clinicians to have a low threshold to offer such treatment to patients, even though such treatment is ineffective in the majority of cases. For ethical, clinical and legal reasons, this behaviour
appears inappropriate. Clinicians treating patients with LBP should refrain from using new technologies based on promising results derived from case reports or non-randomized trials.
References
1. Saal JS, Saal JA (2000) Management of chronic discogenic low back pain with a thermal intradiscal catheter: a prelimi-nary report. Spine 25:382–388
2. Derby R, Eek B, Chen Y et al (2000) Intradiscal electrother-mal annuloplasty (IDET): a novel approach for treating chronic discogenic back pain. Neuromodulation 3:82–88
3. Gerszten PC, Welch WC, McGrath PM et al (2002) A pro-spective outcomes study of patients undergoing intradiscal electrothermy (IDET) for chronic low back pain. Pain Phys 5:360–364
4. Lutz C, Lutz GE, Cooke PM (2003) Treatment of chronic lumbar diskogenic pain with intradiskal electrothermal ther-apy: a prospective outcome study. Arch Phys Med and Rehab 84:23–28
5. Saal JA, Saal JS (2000) Intradiscal electrothermal treatment for chronic discogenic low back pain. A prospective outcome study with a minimum 1-year follow-up. Spine 25:2622–2627
6. Saal JA, Saal JS (2002) Intradiscal electrothermal treatment for chronic discogenic low back pain. A prospective out-come study with a minimum 2-year follow-up. Spine 27: 966–973
7. Park SY, Mood SH, Park MS et al (2005) Intradiscal electro-thermal treatment for chronic lower back pain patients with internal disc disruption. Yonsei Med J 46:539–545
8. Spruit M, Jacobs WCH (2002) Pain and function after intra-discal electrothermal treatment (IDET) for symptomatic lumbar disc degeneration. Eur Spine J 11:589–593
9. Cohen SP, Larkin T, Abdi S (2003) Risk factors for failure and complications of intradiscal electrothermal therapy: a pilot study. Spine 28:1142–1147
10. Lee MS, Cooper G, Lutz GE et al (2003) Intradiscal electro-thermal therapy (IDET) for treatment of chronic lumbar dis-cogenic pain: a minimum 2-year clinical outcome study. Pain Phys 6:443–448
11. Davis TT, Delamarter RB, Sra P et al (2004) The IDET pro-cedure for chronic discogenic low back pain. Spine 29: 752–756
12. Freedman BA, Cohen SP, Kuklo TR et al (2003) Intradiscal electrothermal therapy (IDET) for chronic low back pain in active-duty soldiers: 2-year follow-up. Spine J 3:502–509
13. Webster BS, Verma S, Pransky GS (2004) Outcomes of workers’ compensation claimants with low back pain under-going intradiscal electrothermal therapy. Spine 29:435–441
14. Karasek M, Bogduk N (2000) Twelve-month follow-up of a controlled trial of intradiscal thermal anuloplasty for back pain due to internal disruption. Spine 25:2601–2607
15. Bogduk N, Karasek M (2002) Two-year follow-up of a con-trolled trial of intradiscal electrothermal anuloplasty for chronic low back pain resulting from internal disc disrup-tion. Spine J 2:343–350

100 B. J. C. Freeman
16. Pauza KJ, Howell S, Dreyfuss P et al (2004) A randomised, placebo-controlled trial of intradiscal electrothermal therapy for the treatment of discogenic low back pain. Spine J 4:27–35
17. Freeman BJC, Fraser RD, Cain CMJ et al (2005) A ran-domised double blind controlled trial: intra-discal electro-thermal therapy versus placebo for the treatment of chronic discogenic low back pain. Spine 30:2369–2377
18. Urrutia G, Kovacs F, Nishishinya MB et al (2007) Percutaneous thermocoagulation intradiscal techniques for discogenic low back pain. Spine 32:1146–1154
19. Eckel TS, Ortiz AO (2002) Intradiscal electrothermal ther-apy in the treatment of discogenic low back pain. Tech Vasc Interv Radiol 5:217–222
20. Orr RD, Thomas S (2005) Intradural migration of broken IDET catheter causing a radiculopathy. J Spinal Disord Techn 18:185–187
21. Cohen SP, Larkin T, Polly DW Jr (2002) A giant herniated disc following intradiscal electrothermal therapy. J Spinal Disord Tech 15:537–541
22. Ackerman WE III (2002) Cauda equina syndrome after intradiscal electrothermal therapy. Reg Anaesth Pain Med 27:622
23. Hsia AW, Isaac K, Katz JS (2000) Cauda equina syn-drome from intradiscal electrothermal therapy. Neurology 55:320
24. Wetzel FT (2001) Cauda equina syndrome from intradiscal electrothermal therapy. Neurology 56:1607
25. Djurasovic M, Glassman SD, Dimar JR et al (2002) Vertebral osteonecrosis associated with the use of intradiscal electrothermal therapy. A case report. Spine 27: E325–E328
26. Scholl BM, Theiss SM, Lopez-Ben R et al (2003) Vertebral osteonecrosis related to intradiscal electrothermal therapy: a case report. Spine 28:E161–E164
27. Barendse GAM, Van den berg SGM, Kessels AHF et al (2001) Randomised controlled trial of percutaneous intradis-cal radio-frequency thermo-coagulation for chronic disco-genic back pain. Lack of effect from a 90-second 70°C lesion. Spine 26:287–292
28. Ercelen O, Bulutcu E, Oktenoglu T et al (2003) Radiofrequency lesioning using two different time modalities for the treatment of lumbar discogenic low back pain: a randomized trial. Spine 28:1922–1927
29. Finch PM, Price LM, Drummond PD (2005) Radiofrequency heating of painful annular disruptions; one year outcomes. J Spinal Disord Tech 18:6–13
30. Kapural L, Hayek S, Malak O et al (2005) Intradiscal ther-mal annuloplasty versus intradiscal radiofrequency ablation for the treatment of discogenic pain: a prospective matched control trial. Pain Med 6:425–431
31. Smith and Nephew. IDET: For physicians: about the proce-dure. Available at http://www.idetprocedure.com/2000_pro-fessional/2100_about.html Accessed 23 July 2009.
32. Freeman BJC (2006) IDET: a critical appraisal of the evi-dence. Eur Spine J 15(Suppl.3):S448–S457

101M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_3.6, © Springer-Verlag Berlin Heidelberg 2010
Introduction
Orthotic devices with various concepts and designs have been used since the Middle Ages to correct defor-mities and keep the spine straight. Various materials have been used over the years for orthotic fabrication. In the last century, thermoplastic composites replaced leather and plaster of Paris. Numerous types of lumbar supports have been developed worldwide for the treat-ment of spinal disorders [2, 7, 8]. This book is devoted to nonrigid stabilization systems, the goals of which are (1) to stabilize the motion segment by restricting but not suppressing motion; (2) to protect the adjacent level and create the best conditions for healing and hopefully regenerating the discal tissue; and (3) by so doing to obtain pain relief by lowering the nociceptive physical and mechanical input. The biomechanical goals of lumbar orthoses are, as suggested many years ago by Nachemson [21], to correct deformity, limit spinal motion, stabilize part of the spine, and reduce the loads on the trunk structures. Lumbar supports and nonrigid stabilization operative techniques have more or less similar mechanical goals. In a sense, lumbar orthoses could be considered as “external nonrigid sta-bilization systems.” Lumbar supports are used as part of the conservative treatment before surgery. In this chapter, we will first summarize the mechanical effec-tiveness of lumbar orthoses, taking into account the kinematics of the lumbar spine, and second, their
clinical effectiveness in preventing and treating non-specific low-back pain.
Kinematics
The functional unit of the motion segment consists of two vertebrae and their intervening soft tissues. The unit is divided into two portions: the anterior portion consisting of the vertebral bodies separated by the disk and sur-rounded by the longitudinal ligaments and the posterior portion formed by the arch, facets, transverse and spinous process, and various ligaments. The functional units (FSU) do not move independently, and motion of the lumbar spine implies the combined action of several FSU. Each FSU has 6° of freedom: rotation about and transla-tion along a transverse, a sagittal, and a longitudinal axis [35]. Radiographic measurements in vivo have shown that the range of motion of individual motion segments is small. Values of segmental motion documented by White and Panjabi [23, 35] show a cephalocaudal increase of motion in flexion-extension, ranging from approximately 4° in the upper thoracic region to 12° at the thoraco-lum-bar level and to about 20° at the lumbo-sacral level.
The functional range of motion varies among indi-viduals and decreases with age. Lumbar motion is maxi-mum in the sagittal flexion-extension plane. The first 50–60° of trunk flexion comes from the lumbar spine. Forward tilting of the pelvis provides the additional 20–30° [6]. Schematically, there is more range of motion in flexion than in axial rotation, the latter being limited by the facet joints [14]. Functional trunk movements involve not only the combined motion of different parts of the spine but also pelvic motion, which increases the functional range of the trunk.
Lumbar Orthoses to Prevent and Treat Low-Back Pain
Michel Benoist and Thibaut Lenoir
M. Benoist (*) University of Paris VII, Hôpital Beaujon, 100 Bd. du Gl. Leclerc, 92110 Clichy, France e-mail: [email protected]
3.6

102 M. Benoist and T. Lenoir
Rationale for Orthoses in “Degenerative Disk Disease”
Two clinical syndromes are associated with degenera-tive conditions. The first is primary radicular pain with usually some component of low-back pain. The second is pure primary low-back pain with no radicular pain caused by nerve-root irritation. In the case of radicular pain caused, for example, by a discal herniation, the nerve root is the nociceptive receptor responsible for transmitting the pain message. In the case of pure LBP, the nerve fibers located in the disks, the facets, or other innervated structures of the functional spinal unit rel-evant to pain sensation comprise the receptor unit.
The nerve terminals are sensitized by inflammatory and signaling substances found in degenerate, painful disks such as neuropeptides and various inflammatory cytokines [4]. Diminution of the disk height, as well as tears and clefts that are the mechanical hallmarks of degeneration, leads to abnormal motions and loading, causing physical stimulation of the sensitized nerve endings. The fact that mechanical stimulation can gen-erate pain is supported by the common observation that low-back pain is strongly influenced by posture and movements of the patient. In clinical practice, most chronic LBP patients have no obvious radiologic signs of instability. It is possible, as stated by Kirkaldy Willis and Farfan [11], that very subtle displacements and lack of smoothness in the normal range of motion may cause pain where sensitized nerve terminals are gently stimu-lated. The rationale for orthosis is to avoid and restrict painful movements and to stabilize and immobilize the sensitized spinal unit in the hope of healing the inflamed discal tissues. Limiting the mechanical constraints is therefore a logical objective. It remains to be seen whether the mechanical effectiveness of orthoses is able to reach this objective and whether they are able to prevent and treat low-back pain in clinical practice.
Mechanical Effectiveness of Lumbar Orthoses
In order to diminish or suppress mechanical stimulation of the innervated, sensitized structures of the lumbar spine, bracing can be effective in two principal ways: immobilization or restriction of lumbo-sacral range of motion and reduction of back muscle force. The
immobilizing efficacy can be related to restriction of the intersegmental motion and of gross body motion.
All of the supports tested by Fidler and Plasmans [7] in a cohort of healthy volunteers reduced the seg-mental angular movements evaluated on X-ray films in maximum flexion extension. An approximate 40° reduction in sagittal angular motion amplitude was observed. There were considerable variations among individuals. Effectiveness in reducing movements at each level varied according to the support used. For example, canvas corsets reduced the mean angular movement to two-thirds of normal at each level. Raney and baycast jackets reduced the values to one-third of normal in the middle of the lumbar spine.
Nachemson et al. [20, 21] assumed that gross motion restriction is more important than reduction in the intersegmental motion. When the upper spine is in flexion, extension, or lateral bending, heavy loads are applied to the trunk. Any orthoses limiting upper body gross motion are expected to be effective. Numerous studies of varying methological quality have attempted to determine whether the use of a support reduces gross body motion, obstructs extreme movements, and improves the body posture through a reminder func-tion due to a tactil feedback. Most studies of the litera-ture have found a significant restriction of gross body motion of varying importance according to the support used [13]. It has also been shown that to immobilize the lumbo-sacral junction thoroughly, it is imperative to include at least one thigh in the lumbar support [22]. Similarly, lumbo-sacral rotation needs thigh inclusion in order to be effectively decreased [14]. A high-qual-ity systematic review and metaanalysis of studies on the putative mechanisms of action was carried out by Van Poppel et al. [31]. In spite of conflicting results, these authors were able to draw conclusions from the results of the meta-analysis. The literature search iden-tified 33 controlled studies. The criteria used by the authors for the methodologic assessment were in keep-ing with the usual checklists used to assess the quality of randomized controlled trials [18]. Thirteen of the selected studies focused on trunk motion. Most inves-tigators reported on maximal range of motion, others on angular movement of spinal disks, or range of motion during specified tasks. In all the studies a design was used in which the same subjects were tested with and without lumbar orthoses. Meta-analysis of these studies provided evidence that lumbar orthoses restrict trunk motion. A statistically significant overall

1033.6 Lumbar Orthoses to Prevent and Treat Low-Back Pain
effect was found in flexion-extension and lateral bend-ing. However, this effect was not significant on rota-tion. The results were statistically homogenous for flexion-extension, but heterogeneous for lateral bend-ing and rotation. This heterogeneity, according to sub-sequent analysis performed by the authors, was related to the type of lumbar support and outcome measure.
Another mechanism for orthoses to decrease the risk of low-back pain relates to a reduction of back muscle force. This could theoretically be obtained by an increase of abdominal pressure without a concomi-tant augmentation of abdominal muscle activity. The raised abdominal pressure tends to extend and elon-gate the spine. By doing so, the lumbar lordosis is straightened and the force required in extensor muscu-lature is reduced, thus relieving the compressive loads off the spine [3]. Several studies have investigated the effects of lumbar orthoses on intraabdominal pressure and muscular activity by electromyogram of the paras-pinous and abdominal musculature. Most of these studies report contradictory or conflicting results. For example, Walter and Morris [34] studying the electri-cal activity of muscles of the trunk when wearing spi-nal supports found a decrease of abdominal muscle activity, but an increase of paraspinous muscle activity during ambulation. In contrast, Morris and Lucas [19], as well as Nachemson [20], have shown that lumbar supports worn during lifting do not affect the activity of the erector spinae. The same conflicting results are observed in the measurements of intraabdominal pres-sure. The most precise and extensive information comes from the systematic review provided by Van Poppel et al. [31], as mentioned above. Twelve studies reporting on electromyogram measurements and 11 studies on intraabdominal pressure-measures were selected. In most electromyographic studies, measure-ments of IAP were not performed simultaneously. Reports of the reviewed studies yielded inconsistent and conflicting results. Separate meta-analyses for studies on electromyogram of back muscles and on IAP were performed. Only three studies on electro-myogram and seven on IAP could be included in the meta-analysis. No statistically overall effect of lumbar support was observed on electromyogram or on IAP. The overall conclusion of the authors was that there was no evidence in the literature that lumbar orthoses influence back muscle EMG and IAP. Previous reviews of the literature [2, 17, 25] had concluded that because of the inconsistent results of the available studies, no
conclusive statement could be made. The conclusions of Van Poppel’s systematic review are supported by a study by Szpalski et al. [28]. The influence of a lumbar belt was tested on an isoinertial dynamometric device on 20 healthy volunteers with and without the lumbar brace. The conclusion of the study was that orthoses had an effect on the amplitude of motion, but all other characteristics of trunk motion, static or dynamic, remained unaltered.
Clinical Effectiveness of Lumbar Orthoses
Currently, lumbar supports are provided as treatment to patients with LBP and sciatica, or for prevention, either primary with the aim of preventing onset of LBP, or secondary with the aim of preventing recurrent epi-sodes. There are numerous studies investigating the clinical effectiveness of lumbar supports. Unfortunately, most of these studies are of poor methodologic quality owing to inadequate randomization, absence of assess-ment of cointerventions, or of compliance. Moreover, these studies often yielded contradictory results. In a state of the art review published in 1987, Nachemson [20] stated that slightly more than 50% of the patients estimated that orthotic devices helped them. Since then a few reviews have summarized the published studies and reached the conclusion that effectiveness of orthoses was controversial [5, 10, 24, 29]. A more recent systematic review [9] is particularly important as it evaluates the literature using the methodology recommended by the Cochrane Collaboration Review Group [32]. We will briefly analyze the results of this high-quality review which provides, in these authors’ opinion, the best and most useful information.
Seven studies on prevention (five RCTs and two CCTs) and six studies on treatment (six RCTs) were identified out of 153 relevant articles. Because of the heterogeneity in study populations, interventions and in outcomes, meta-analysis could not be performed. The results were evaluated qualitatively, using the rat-ing system based on four levels of evidence depending on the design, the quality, and outcome of the studies [32]. This system is summarized as follows:
Level A: Strong evidence: findings concur in sev-eral high-quality RCTs.

104 M. Benoist and T. Lenoir
Level B: Moderate evidence: findings concur in one high-quality RCT and one or more RCTs of low qual-ity, or findings concur in several studies of low quality.
Level C: Limited evidence: based on findings of one RCT (of high or low quality), or generally consis-tent findings in CCTs; or contradictory findings in sev-eral studies.
Level D: No evidence: no RCT or other types of studies of satisfactory scientific quality.
Results of the data analysis, using this rating system and concerning the effect of lumbar orthosis on pre-vention, are as follows:
1. There is moderate evidence (Level B) that lumbar orthoses compared with no orthoses do not prevent LBP.
2. There is also moderate evidence (Level B) that lum-bar supports are not more effective than other types of intervention.
3. There is limited evidence that lumbar support added to another type of intervention such as back school is not more effective than back school alone.
However, two reviews [30, 33] have investigated the effects of lumbar orthoses in secondary prevention. The authors have analyzed subgroups of workers with a history of LBP. Results indicate that this category of workers may be at a reduced risk for recurrent episodes if wearing a support. Further studies are needed to con-firm this possibility.
Is there evidence in the literature to support the use of orthoses for the treatment of low-back pain? As men-tioned above, six trials for treatment were selected in Jellema’s study [9]. All were RCTs (one high-quality and five low-quality). Only one study [16] included patients with chronic LBP, the other studies included patients with unspecified duration of complaints or with varying duration of pain (acute, subacute, and chronic). The conclusions of the systematic review are as follows:
1. There is limited evidence (Level C) that lumbar supports provide pain relief in patients with LBP, when compared with patients without support.
2. There is moderate evidence (Level B) that lumbar orthoses are not more effective than other types of treatment.
3. There is conflicting evidence as to whether patients wearing a support go back to work more rapidly than those without a support.
The conclusions of Jellema’s review were quite similar to those of a previous systematic review by Koes and Van Den Hoogen [12] who stated that effectiveness of orthoses was controversial, and that it remained unclear whether they were better than other interventions. Guidelines for the management of low-back pain are based on the results of these studies. Wearing a support was not recommended for prevention or for treatment of nonspecific low-back pain by the European Guidelines Committee of the Cost B13 Project, 2006.
Comparison of Different Types of Lumbar Orthoses
Numerous types of lumbar supports are now available [27]. The type of orthosis should be prescribed individ-ually according to the pathology, the posture, and the physical characteristics of any given patient. The mate-rial used and the height and rigidity of the support depend on the level of control needed and, more specifi-cally, on the planes of motion to be restricted. For exam-ple, a cloth lumbosacral orthosis SLO will reduce the normal flexion-extension by 30%, the lateral flexion by 10%, and the rotation by 0%. A rigid plastic SLO will reduce the flexion-extension by 60%, the lateral flexion by 40%, and the rotation by 20%. A rigid TSLO will reduce the flexion-extension by 60%, the lateral flexion by 50%, and the rotation by 30%. As already mentioned, a rigid TSLO including one thigh is necessary to immo-bilize the lumbar spine, including the rotation [21, 26]. Posture should also be considered. A delordosing brace for low-back pain and sciatica is recommended by some authors [15, 36]. According to them, the flexed posture tightens the posterior longitudinal ligament, thereby diminishing posterior disk bulge.
The important issue is whether some types of lumbar supports are more clinically effective in the prevention or treatment of nonspecific low-back pain. As empha-sized by Jellema et al. [9], no scientific conclusion can be formulated from the literature. Many studies do not describe the type of support they have used, as well as the compliance. Therefore, the specific clinical effects of the various types of braces remain unclear. There is, however, one high-quality RCT [33] which compared two different types of support, one with a rigid stay in the back, and one without. Patients with the rigid stay had a more global improvement on a subjective index.

1053.6 Lumbar Orthoses to Prevent and Treat Low-Back Pain
Conclusions
The authors believe that there is no hard scientific evi-dence of the effectiveness of lumbar supports for pre-vention and for treatment of nonspecific low-back pain. However, in clinical practice there is a subgroup of patients who think that orthotic devices help them [20]. As the use of orthoses seems to be questionable on biomechanical grounds, it may be that other effects such as massage, heat, antivibratory, or placebo explain the clinical benefit observed in some patients. As pointed out by Balagué [1], “the practice of medicine remains an art with a scientific background.” Although evidence-based guidelines must be kept in mind, other clinical, psychological, cultural, or societal factors need to be considered at the individual level in the con-servative treatment of nonspecific LBP. This remark can be applied to the use of orthoses as a treatment of low-back pain.
References
1. Balagué F, Dudler J (2007) Conservative treatment for low-back pain. XIV Brussels International Symposium, November 16 and 17. Brussels, Belgium
2. Barron BA, Feurstein M (1991) Industrial back belts and low-back pain: mechanisms and outcomes. J Occup Rehab 4:125–139
3. Bartelink DL (1957) The role of the abdominal pressure in relieving the pressure on the lumbar intervertebral discs. J Bone Joint Surg 39:718–725
4. Benoist M, Boulu P (2004) Disc degeneration and low-back pain. In: Gunzburg R, Szpalski M, Anderson GBJ (eds) Degenerative disc disease. Lippincott Williams and Willkins, Philadelphia, pp 111–121
5. Dillingham TR (1998) Lumbar supports for prevention of low-back pain in the work place. JAMA 279:1826–1828
6. Farfan HF (1975) Muscular mechanism of the lumbar spine and the position of power and efficiency. Orthop Clin North Am 6:135–146
7. Fidler MW, Plasmans CMT (1983) The effect of four types of support on the segmental mobility of the lombosacral spine. J bone Joint Surg 65:943–947
8. Hodgson EA (1996) Occupational back belt use: a literature review. Am Assoc Occup Health Nurs 44:438–443
9. Jellema P, Van Tulder MW, Van Poppel MNM et al (2001) Lumbar supports for prevention and treatment of low-back pain. A systematic review within the framework of the Cochrane Back Review Group. Spine 26:377–386
10. Karas BE, Conrad KM (1996) Back injury prevention inter-ventions in the work place. Am Assoc Occup Health Nurs 44:189–196
11. Kirkaldy-Willis WH, Farfan HF (1982) Instability of the lumbar spine. Clin Orthop 165:110–123
12. Koes BW, Van den Hoogen HMM (1994) Efficacy of bed rest and orthoses for low-back pain. Eur J Phys Med Rehabil 4:86–93
13. Lanz SA, Schultz AB (1986) Lumbar spine orthoses wear-ing: restriction of gross body motion. Spine 11:830–842
14. Lumsden RM, Morris JM (1960) An in vivo study of axial rotation and immobilization at the lumbosacral joint. J Bone Joint Surg 50:1591–1602
15. MacNab I (1981) Backache. Williams and Wilkins, Baltimore/London, p 154
16. Million R, Nilsen KH, Jayson MIV et al (1981) Evaluation of low-back pain and assessment of lumbar corsets with and without back supports. Ann Rheum Dis 40:449–454
17. Minor SD (1996) Use of back belts in occupational settings. Phys Ther 76:403–408
18. Moher D, Jadad AR, Nichol G et al (1995) Assessing the quality of randomized controlled trials: an annoted bibliogra-phy of scales and checklists. Control Clin Trials 16:63–75
19. Morris JM, Lucas BD (1964) Biomechanics of spinal brac-ing. Ariz Med 21:170–176
20. Nachemson A (1987) Orthotic treatment for injuries and dis-eases of the vertebral column. Phys Med Rehab State Art Rev 1:11–24
21. Nachemson A, Schultz A, Anderson GBJ (1983) Mechanical effectiveness studies of lumbar spine orthoses. Scand J Rehab Med 9(Suppl):139–149
22. Norton PL, Brown T (1957) The immobilizing efficiency of back braces. J Bone Joint Surg 39:111–138
23. Panjabi MM, White A, Brand RA (1974) A note in defining body parts configurations. J Biomech 7:305
24. Penrose KW, Chook K, Stump JL (1991) Acute and chronic effects of pneumatic lumbar support on muscular strength, flexibility and functional impairment. Sports Train Med Rehabil 2:121–129
25. Perkins MS, Bloswick DS (1995) The use of back belts to increase intraabdominal pressure as a means of preventing low-back injuries. A survey of the literature. Int J Occup Environ Health 1:326–335
26. Petersen BP, Panjabi MM, White AA (1999) A user’s guide to lumbar orthoses: theoretical, scientific, and clinical rationale. In: Szpalski M, Gunzburg R, Pope MH (eds) Lumbar segmen-tal instability. Lippincott Williams and Wilkins, Philadelphia
27. Pope MH, Magnusson M, Sandler AJ et al (1997) Orthoses for treatment of cervical and low-back disorders. In: Frymoyer JW (ed) The adult spine: principles and practice, 2nd edn. Lippincott-Raven, Philadelphia
28. Szpalski M, Gunzburg R, Michel F, Hayez JP (1997) Influence of lumbar braces, isometric or dynamic character-istics of trunk function. Presented at International Society for the Study of the Lumbar Spine annual meeting. June 2–6, Singapore
29. Van Poppel MNM, Koes BW, Smid T et al (1997) A system-atic review of controlled clinical trials on the prevention of back pain in industry. Occup Environ Med 54:841–847
30. Van Poppel MNM, Koes BW, Van der Ploeg T et al (1998) Lumbar supports and education for the prevention of low-back pain in industry: a randomized controlled trial. JAMA 279:1789–1794

106 M. Benoist and T. Lenoir
31. Van Poppel MNM, de Looze MP, Koes BM et al (2000) Mechanisms of action of lumbar supports. A systematic review. Spine 25:2103–2113
32. VanTulder MW, Assendelft WJJ, Koes BW et al (1997) Editorial board of the cochrane collaboration back review group for spinal disorders. Spine 22:2323–2330
33. Walsh NE, Schwartz RK (1990) The influence of prophylac-tic orthoses on abdominal strength and low-back injury in the workplace. Am J Phys Med Rehabil 69:245–250
34. Walters RL, Morris JM (1970) Effect of spinal supports on the electrical activity of muscles of the trunk. J Bone Joint Surg 52:51–59
35. White AA, Panjabi MM (1990) Clinical biomechanics of the spine, 2nd edn. J.B.Lippincott, Philadelphia
36. Wilner S (1985) Effect of a rigid brace on back pain. Acta Orthop Scand 56:40–42

Part
Surgical Treatment: FusionIV

109M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_4.1, © Springer-Verlag Berlin Heidelberg 2010
Introduction
Recent studies have demonstrated a steady increase in the number of lumbar fusions from 1992 to 2003 when considering the US average rate of discharges per thousand Medicare enrolled, equaling more than 4 times the number of fusions within this time period. At the same time, the number of discectomies and lumbar laminectomies has not increased accordingly, when compared with earlier times. [1]. Also, the number of nonlumbar fusions has doubled in this time, whereas that of the nonlumbar discectomy and laminectomy surgery has stayed almost the same dur-ing this time. As demonstrated in the comparative magnitude of variability of orthopedic procedures in the Dartmouth small area analysis, lumbar fusions have purely defined indications compared to, for instance, hip fracture treatment or hip replacement [2]. One of the major areas of indication for lumbar fusions is the degenerated disk disease as well as the postdiscectomy syndrome. If this pathology is com-pared to low back pain (LBP) in pediatric spondylolis-thesis as well as high slip spondylolisthesis treated by lumbar fusion, it is only the pediatric spondylolisthe-sis and the high slip spondylolisthesis, which are l till after 5 years significantly more pain-free than patients who had surgery for degenerative disease and post-discectomy syndrome. This indicates that there are
pathomorphologies, which may also profit in a long-term follow-up from lumbar fusion, whereas other surgical indications, specifically for LBP in degener-ated disk disease or in postdiscectomy syndromes, the profit of surgery is less obvious [3]. Most of random-ized prospective trials suggest that any advantage of surgery over nonsurgical care is modest [4], although recent studies report a relevant long-term profit from a surgical treatment in chronic LBP in more than 70% [5]. In addition, there is pretty good evidence that the fusion technique does not alter the outcome in patients with chronic LBP [6]; however, it increases the com-plication rate with increasing technical sophistication of the procedure [7].
This also demonstrates that LBP is not a diagnosis but a very unspecific symptom for which there is no surgical treatment except when it is combined with precise diagnostic entities with a history, which corre-lates with a distinct pathomorphology, clinical picture, and often a conclusive invasive pain evaluation. There is a whole list of these disorders which go along with LBP, and each of these pathologies may have a specific outcome when treated by surgery (Table 4.1.1). Today’s debate about surgery in LBP is mostly centered on the axial back pain with disk degeneration or internal disk disruption, a frequent radiological entity, but not regu-larly combined with LBP. A surgical indication for fusion in LBP necessitates a meticulous history and clinical evaluation combined with imaging, which should correlate clearly with the clinical picture.
In this overview we will neither include LBP in the context of osteoporosis and osteoporotic compression fractures, nor will we refer to back pain in the context of spinals tumors and trauma.
Indication for Lumbar Spinal Fusion
Max Aebi
M. Aebi Center for Orthopaedic Research, University of Bern, Stauffenbachstrasse 78, 3014, Bern, Switzerland e-mail: [email protected]
4.1

110 M. Aebi
Clinical Evaluation
The corner stone of clinical evaluation is the patient history, specifically the pain history. All the ele-ments and sources of possible pain need to be addressed with the patient to design a clear picture of the underlying pathology. A clinical assessment of the spine (balance!) and a precise neurological assessment are important, but often not conclusive. Only after an extensive history and clinical examina-tion the choice of imaging of the spine is made. Although we have sophisticated imaging technol-ogy available, like MRI, CT-scan, or a combination of CT-myelogram, a conventional X-ray in standing position, ap, lateral (usually a whole spine image) and oblique is helpful to understand the alignment and “the architecture” of the lumbar spine, and when combined with flexion-extension films in supine position, the imaging may give some impression about the stability of the motion segments [8, 9]. This noninvasive imaging technology may be expanded by facet blocks, discograms, extraforaminal root blocks, and epidural blocks to clarify the pain source. Each of these examinations is isolated per se not a conclusive procedure [10, 11]; however, in combina-tion with the history, the clinical findings, and the imaging, it may be a further mosaic stone in the whole picture in justifying a surgical or nonsurgical indication.
Spinal Disorders Which Go Along with Low Back Pain and Which May Constitute an Indication for Fusion Surgery
Dysplastic Spondylolisthesis and Spondylolysis
Unstable spondylolysis as well as spondylolisthesis is a frequent diagnosis and it occurs in more than 5% of the Caucasians. In the Inuit population the incidence is more than 20%. Many of these findings are irrelevant when not combined with a distinct clinical picture. However, specifically in adolescents and young adults, a spondylolysis and spondylolisthesis even of low grade may be an indication for lumbar fusion of all the nonsurgical treatments are ineffective. It is recom-mended not to treat these patients nonsurgically for many years when the patient has really invalidating pain. In such a case patients are conditioned to their pain. The experience shows, also not supported by evi-dence-based studies, that patients operated for spon-dylolysis and spondylolisthesis in younger years, meaning before their thirties, generally do very well and rarely return for further surgery [12]. The lumbar fusion for spondylolysis and spondylolisthesis L5/S1 can be a posterior surgery with fusion alone or com-bined with posterior instrumentation (pedicle screws) or a combination of posterior fixation with an interbody fusion, be it a PLIF or a TLIF. An ALIF may be equally as successful and goes along with a significantly smaller surgical trauma due to less muscle stripping than poste-rior surgery. Studies from Finland and others demon-strate that the type of fusion does not necessarily go along with better outcome [13, 14]. However, the non-instrumented fusions do have a higher incidence of nonunions and loss of correction [13]. We recently have developed systematically a posterior instrumenta-tion using the pedicle screw in the sacrum as so-called transpedicular-transdiscal-transcorporal screw from S1 into the body of L5, either in combination with a poste-rior pedicle screw-rod-system or as isolated sacral lumbar screws (see Chapter 4.6, p. 145). The isolated screws may be helpful in younger patients as a minimally invasive instrumented posterior fusion of L5/S1. A number of potential complications are, how-ever, to be considered when this surgical technique is
Table 4.1.1 Pathomorphological correlates to low back pain (LBP) other than unspecific LBP
Lumbar disk herniation
Internal disk rupture, black disk (axial back pain)
Facet joint arthritis, facet joint syndrome
Spondylolysis and spondylolistheis (dysplastic)
Degenerative spondylolisthesis
True instability (degenerative, posttraumatic)
Adjacent segment syndrome
Postdiscectomy syndrome
Transitional lumbosacral anomaly
Spinal stenosis
Degenerative scoliosis

1114.1 Indication for Lumbar Spinal Fusion
chosen. A recent study of a Swedish group came to the conclusion that the outcome of posterior lumbar inter-body fusion vs. posterolateral fusion in adult isthmic spondylolisthesis was almost identical in the two groups at a 2-years follow-up [15]. High-grade spon-dylolisthesis (grade III–V) are only safely treated with a circumferential fusion (anterior column support) and have a high incidence of implant failure when operated by a posterior instrumentation only [16–19].
Degenerative Spondylolisthesis
This is a frequent problem in middle-aged and elderly patients, mostly going along with spinal stenosis and finally necessitating a decompression. Whether the fusion is indicated or whether the decompression alone is sufficient is an ongoing debate [20–22]. The 1997 Volvo Award winning paper in clinical category by Fishgrund et al. demonstrated almost identical results in the instrumented and noninstrumented fusions for degenerative spondylolisthesis. However, there was a significant difference in terms of successful arthrodesis in so far that instrumented fusion reached 83% of suc-cessful fusion, whereas noninstrumented fusion reached only 45% [23]. The pseudarthrosis rate was
18% for instrumented fusion and 55% for uninstru-mented fusion. However, in a reassessment of the same patients after 5 years, it seemed that the fused patients did definitively better than those with a persistent non-union [24]. Similar figures could be identified in the Swedish Lumbar Spine Study [25–27].
True Instability (Posttraumatic, Degenerative)
The posttraumatic instability is the best understood form of lumbar instability and usually warrants surgical treatment since these patients may go along with sig-nificant LBP. However, a degenerative instability may not necessarily go along with LBP, although the patho-logical movement may be quite significant [28, 29]. The degenerative process with the destruction of the disk may lead to an unstable segment, which can be recog-nized in the functional X-rays, specifically in supine position with flexion-extension and usually by air inclu-sion in the disk [8, 9, 30] (Fig. 4.1.1). Degenerative instability may, however, be difficult to prove other than with a specific history and indirect imaging signs. It may be more appropriate, however, to talk about “dys-mobility” in the degenerative lumbar spine than about
ba
Fig. 4.1.1 Degenerative instability: (a) Functional lateral X-ray in flexion (supine), (b) Instrumented posterior and anterior interbody fusion with a peek cage

112 M. Aebi
instability. Pope et al. defined segmental instability as a loss of stiffness of a motion segment, which causes pain and has the potential to result in progressive deformity and will finally place neurogenic structures at risk [29] (Fig. 4.1.2). If the morphologically demonstrated insta-bility goes along with LBP, as it may be proven by facet joint infiltration and immobilization, this degenerative instability is a surgical indication. Unfortunately, there
are no specific studies available with prospective anal-ysis of the development of instability. To some degree the de novo occurring degenerative scoliosis may be interpreted as a degenerative instability, which is expressed in a chronic global instability of a spinal area as well as measurable segmental instabilities, either in the sagittal as well as in the frontal plain or as a combination as a three-dimensional instability.
Fig. 4.1.2 Degenerated disk disease with a more “global instability” which leads to a degenerative scoliosis: (a) female patient with 57 years with narrowed disk space L2–3; (b) two years later with now severe damage of the disk L2–3 as well as L3–4 and progressive pain; (c) postoperative image with posterior instrumented fusion combined with TLIF- cages at L2–3 and L3–4 and good sagittal as well as frontal alignment
L2
L2
2 yrs later……
b
a

1134.1 Indication for Lumbar Spinal Fusion
Adult Degenerative Scoliosis
The most complex lumbar spinal disorder that goes along with LBP is the degenerative scoliosis, which may also be called a de novo scoliosis. This latter, how-ever, represents only one form of degenerative scolio-sis. It seems that this form of scoliosis is developing on the ground of an asymmetrical degeneration of one or more disks with secondary translation and rotational dislocation within one or several motion segments over time. Asymmetric loading may be the reason for asym-metric degeneration and a consecutive deformity. There are other forms of degenerative scoliosis, like a regular secondary degenerated lumbar counter- curve to the classical idiopathic thoracic curve. Or a primar-ily idiopathic lumbar scoliosis can become secondarily degenerated and also become symptomatic with LBP [31]. These lumbar degenerative curves may become painful with a progression of the curve and accompa-nying neurological deficits or symptoms, and finally be a surgical indication. There is very little pros pective literature available that compares different surgical procedures, e.g., minimal invasive against maximal invasive reconstructive surgery or surgical against non-surgical treatment, which would demonstrate the supe-riority of one over the other procedure [32–34].
Spinal Stenosis
Spinal Stenosis is classically accompanied by a clau-dication symptomatology. However, the claudication may also be in combination with LBP due to signifi-cant degenerated facet joints and disks and/or seg-mental instability [35]. Very rarely patients complain about significant back pain, which is dependent or arises with an increasing walking distance, but with-out having typical claudication-type of pain in the legs. Often these patients have a constitutional narrow canal with accompanying facet joint and disk arthritis. These patients may profit from a decompression. If the spinal stenosis goes along with a significant facet joint arthritis and degenerative spondylolisthesis or a secondary degenerative scoliosis and/or kyphoscolio-sis, the decompression may be followed by an instru-mented fusion to avoid further progression of the deformity or secondary instability. Recent RCTs dem-onstrated superiority of the surgical treatment over the nonsurgical therapy for lumbar spinal stenosis [33]; however, the best surgical treatment is still under debate [36, 37]. The attempts to treat these patients with a multisegmental dynamic fixation have failed so far (Fig. 4.1.3).
Adjacent Segment Problem
This is an increasingly frequent problem observed in degenerative disk disease in patients who develop a degenerated segment adjacent to an operated or fused spinal segment [38]. Usually the adjacent segment disease can be associated with instability, spinal steno-sis, and significant facet joint arthritis and impinge-ment. The adjacent segment disease is a heavily disputed topic in today’s spine surgery and there is only little evidence that this disorder is only related to spinal fusion as it can be equally seen in patients with rigid degenerated spinal segments, and it may be that the mechanically changed loading conditions express a genetic predisposition. It has also been discussed that an adjacent segment disease may be associated with a malalignment of the spine in the sagittal plain [11, 39–41].
Fig. 4.1.2 (continued)

114 M. Aebi
constitutional narrow canal L2-3 status postdecompression elsewhere
a
FlexionExtension
b
Fig. 4.1.3 Sixty-eight-years-old male patient with a multilevel constitutional spinal stenosis with a condition after isolated decompression L2–3: (a) preoperative imaging (MRI) and postop imaging with dynamic fixation; (b) persistent severe back as well
as claudication pain, still stenosis; (c) after revision, large decom-pression and reversion into a stable multilevel fusion. Immediately asymptomatic

1154.1 Indication for Lumbar Spinal Fusion
Postdiscectomy Syndrome
A segment that has been operated several years ago for disk degeneration and/or herniation may become pain-ful over time due to a significant osteochondrosis of the originally operated segment with narrowing of the disk space with consequent bone-to-bone contact, sub-chondral oedema, later sclerosis, osteophytes, and incongruent facet joints (Fig. 4.1.4). Stabilization of such a segment may reduce the LBP significantly, since the painful segment is immobilized by the fusion. Here it is worth, however, to do some invasive pain evaluations, like discograms and facet joint infiltra-tions, to get a handle on etiology of the pain.
Transitional Anomalies at the Lumbosacral Spine
Although considered by most radiologists as an acci-dental finding, transitional anomalies are frequent and usually lead to overmobility at the superior adjacent segment, in most cases of L4/5. This segment then shows an early degeneration with disk space narrow-ing, subchondral oedema and sclerosis, osteophyte
formation, and finally, foraminal stenosis (Fig. 4.1.5). The disk that is included in the transitional anomaly is usually intact. There is a wide range of variations of transitional anomalies with hemisacralization or hemi-lumbalization, either with or without nearthrotic joints [42–45]. Most of these lesions can be identified as painful with direct infiltration of the anomaly itself or the adjacent degenerated segment. If the pain is perma-nent and improves with infiltration and is persistent with proper conservative treatment, a surgical indica-tion may be given. Surgery may consist in a resection of a unilateral large transverse process, which is in a nearthrotic relationship with the massa lateralis of S1 or in a fusion of the adjacent segment to the transi-tional anomaly.
Facet Joint Arthritis (Spondylarthritis)
In case of significant arthritic changes of the facet joints with hypertrophy of the capsule, hypertrophied facet osteophytes, incomplete spontaneous fusion of the facet joints, and air inclusion, the patients may profit from a facet joint infiltration. If a temporary pain release can be reached, a direct fusion or screw fixation
* *“Pseudolysis”dueto ciment enhancement
*Large decompression
c
Fig. 4.1.3 (continued)
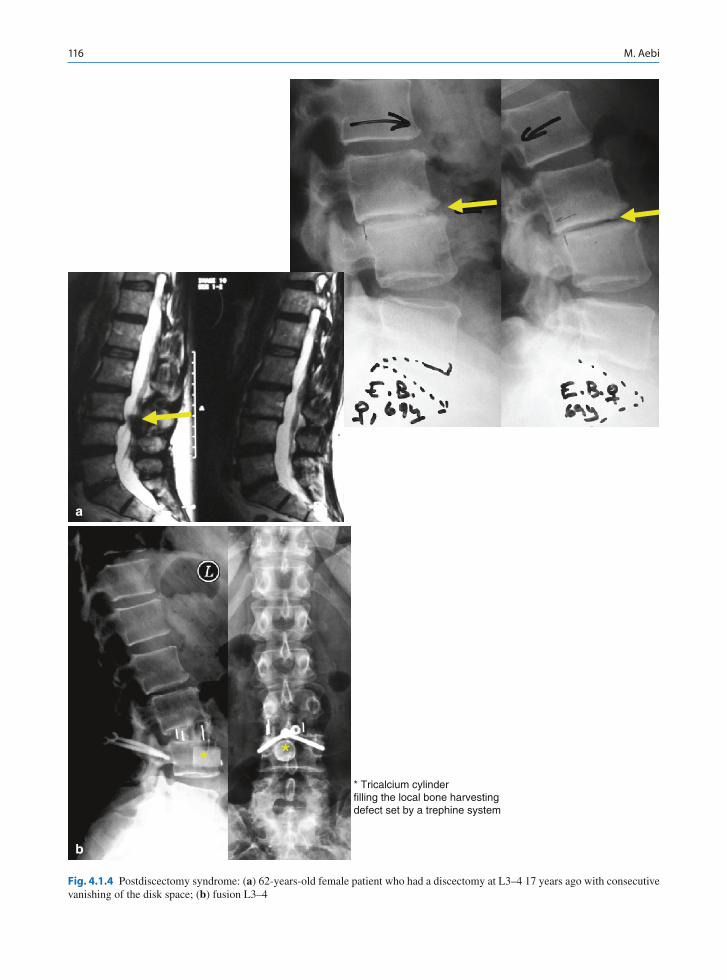
116 M. Aebi
* Tricalcium cylinderfilling the local bone harvestingdefect set by a trephine system
* *
a
b
Fig. 4.1.4 Postdiscectomy syndrome: (a) 62-years-old female patient who had a discectomy at L3–4 17 years ago with consecutive vanishing of the disk space; (b) fusion L3–4

1174.1 Indication for Lumbar Spinal Fusion
Fig. 4.1.5 Transitional anomaly: 71-years-old biologically clearly younger patient with a severe back pain history for many years with a transitional anomaly L5-S1 (with a relatively good disk) and a consecutive degenerated disk with severe
osteochondrosis L4–5: (a) preop imaging, (b) postop imaging after stand-alone interbody fusion with cage at L4–5 followed by rapid improvement of the pain situation
a
Postop.
b

118 M. Aebi
of the arthritic joint may be quite helpful. The so-called “facet joint syndrome” which is radiologically difficult to identify, even with MRI, is a diagnosis which rarely goes along with long-lasting periods of pain relief after surgical treatment. Even if the facet joint infiltration may be suggestive for a facet joint syndrome, the pain relief through fusion may only be temporarily.
In a recent study it has been demonstrated that cases where there is fluid in the lumbar facet joints, detected on MRI, as well as instability in flexion lumbar radio-graphs, in patients with L4/5 degenerative disease, pain correlates well with the morphological findings. Therefore, fluid on MRI in the facet joints should raise suspicion of lumbar instability and qualifies for fusion surgery [46].
The X-rays, respectively the MRI, of significant facet arthritis should be done supine as well as standing to demonstrate the fluid in the joint. When standing, the fluid is pressed out and the facet joints are almost locked. When the patient is supine, the joints may open and air inclusion can be demonstrated on the conven-tional X-rays as well as fluid in the joints. These patients often indicate typical pain in the night when turning in bed which wakes them up and pain in the morning while getting up until the facet joints have “settled” under the axial load. True facet joint arthritis, as the relevant pain source, can usually be stabilized with simple translaminar or transfacetal screws. In case of a still significantly good disk, a combination with an anterior interbody fusion through a TLIF or PLIF may be mandatory to get the patient pain-free (Fig. 4.1.6).
Axial Back Pain: Internal Disk Disruption
This is the most frequent problem considered as syn-onym for LBP. Axial back pain in younger patients with significant recurrence rate and unresponsiveness for conservative treatment may be considered for fusion surgery or since recently for disk arthroplasty (Fig. 4.1.7). Many of these patients already have black disks or definitively changed disks in the MRI, some-times combined with a hypodense Modic sign in the annulus. These suspicious disks may be tested with a discogram where concordant and memory pain may be proven together with a pathological discogram. Although a positive discography was not highly pre-dictive in identifying bone fide isolated intradiscal
lesions, primarily causing LBP illness, it can be con-sidered as a good standard evaluation of the discogenic pain diagnosis as determined by provocative discogra-phy [10, 47, 48]. However, it needs to be noted that despite removal of the pain generator (disk), as diag-nosed by discography, approximately half of the patients continued with significant pain and impair-ment. Therefore, the usefulness of discography still remains to be proved. Physical job characteristics and psychological aspects of work were more powerful than magnetic resonance imaging identified disk abnormalities in predicting the need for LBP-related medical consultation and the resultant work capacity, as demonstrated in a recent paper analyzing natural history of individuals with asymptomatic disk abnor-malities in magnetic resonance imaging, to investigate predictors of LBP-related medical consultation and work incapacity [49].
Discussion
The question when and whether surgery should be done in patients with so-called LBP remains contro-versial [3]. As there is very little strong evidence-based research in combination with anterior or posterior lum-bar fusion, many of the decisions are based on narra-tive-based medicine, meaning experience [50–55]. However, it should be emphasized that LBP is not a diagnosis, but a symptom, and therefore, only the cause of back pain may be addressed by surgery.
Lumbar fusion surgery can be subdivided in cases where
1. Surgery should be done on a relatively acute basis (combined with neurological deficit).
2. Cases where surgery should be planned without major delay in order to avoid further degeneration, progression, and/or chronification.
3. Cases where it is preferable to wait until the patient makes the indication himself for quality of life.
4. Cases where surgery should be avoided whenever possible, even when there is pathomorphology on imaging present.
Also, which technique is best for which indication remains controversial and depends on a lot of variables of clinical evaluation. In recent years, it became more and more obvious that circumferential fusion in axial

1194.1 Indication for Lumbar Spinal Fusion
Extension
a
b
Fig. 4.1.6 Male patient with a significant facet joint syndrome: (a) preop imaging with a repetitive improvement of the pain after facet joint injections. Black disk negative on discogram; postop imaging after translaminar screw fixation and fusion L5-S1

120 M. Aebi
57yrs old female
60yrs old female:28m p.o.
a
b
Fig. 4.1.7 Fifty-seven-years-old female patient with incapacitating axial back pain since several years; (a) preop imaging with severe osteochondrosis and black disk L5-S1; (b) 1 year postop after anterior stand-alone intervertebal fusion with cage: patient asymptomatic

1214.1 Indication for Lumbar Spinal Fusion
LBP is generally superior to posterolateral fusion in a long-term perspective, specifically also in cost-utility evaluation of randomized controlled trials for severe, chronic LBP [5, 56]. They demonstrated that circum-ferential fusion is dominant over instrumented postero-lateral fusion, i.e., both being significantly cheaper and significantly better in a long-term societal prospective. Results were extremely robust to comprehensive sensi-tivity analyses. Those findings represent a robust exter-nal validity to western specialized centers for spine surgery.
Furthermore, however, it has been demonstrated that a higher proportion of fusion procedures and the introduction of new spinal implants between 1993 and 1997 did not reduce reoperation rates. It has been shown that the cumulative incidence of a second lum-bar spine operation has been increased in spite of more sophisticated surgical techniques [49].
References
1. Weinstein JN (2006) United States’ trends and regional vari-ations in lumbar spine surgery: 1992–2003. Spine 31(23): 2707–2714
2. Wenneberg JE, Weinstein JM (2000) Atlas of musculoskel-etal health care. Chicago, AHA
3. Mirza SK, Deyo RA (2007) Systematic review of random-ized trials comparing lumbar fusion surgery to nonoperative care for treatment of chronic back pain [Literature Review]. Spine 32(7):816–823
4. Fritzell P (2005) Fusion as treatment for chronic low back pain – existing evidence, the scientific frontier and research strategies. Eur Spine J 14(5):519–520
5. Christensen FB (2004) Lumbar spinal fusion. Outcome in relation to surgical methods, choice of implant and postoper-ative rehabilitation. Acta Orthop Scand Suppl 75(313):2–43
6. Fritzell P, Hägg O, Wessberg P, Nordwall A; Swedish Lumbar Spine Study Group (2004) Chronic low back pain and fusion: a comparison of three surgical techniques: a pro-spective multicenter randomized study from the Swedish lumbar spine study group. Spine 27(11):1131–1412
7. Fritzell P, Hägg O, Nordwall A; Swedish Lumbar Spine Study Group (2003) Complications in lumbar fusion surgery for chronic low back pain: comparison of three surgical tech-niques used in a prospective randomized study. A report from the Swedish Lumbar Spine Study Group. Eur Spine J 12(2):178–189
8. Leone A, Guglielmi G, Cassar-Pullicino VN, Bonomo L (2007) Lumbar intervertebral instability: a review. Radiology 245(1):62–77
9. Fritz JM, Piva SR, Childs JD (2005) Accuracy of the clinical examination to predict radiographic instability of the lumbar spine. Eur Spine J 14(8):743–750
10. Carragee EJ, Lincoln T, Parmar VS, Alamin T (2006) A gold standard evaluation of the “discogenic pain” diagnosis as deter-mined by provocative discography. Spine 31(18):2115–2123
11. Willems PC, Elmans L, Anderson PG, van der Schaaf DB, de Kleuver M (2007) Provocative discography and lumbar fusion: is preoperative assessment of adjacent discs useful? Spine 32(10):1094–1099; discussion 1100
12. Ekman P, Möller H, Tullberg T, Neumann P, Hedlund R (2007) Posterior lumbar interbody fusion versus posterolateral fusion in adult isthmic spondylolisthesis. Spine 32(20):2178–2183
13. Seitsalo S, Osterman K, Hyvarinen H, Schlenzka D, Poussa M (1990) Severe spondylolisthesis in children and adolescents. A long-term review of fusion in situ. J Bone JoinSurg Br 72(2):254–265
14. Lee SH, Choi WG, Lim SR, Kang HY, Shin SW (2004) Minimally invasive anterior lumbar interbody fusion fol-lowed by percutaneous pedicle screw fixation for isthmic spondylolisthesis. Spine J 4(6):644–649
15. Ekman P, Möller H, Tycho T, Neumann P, Hedlund R (2007) Posterior lumbar interbody fusion versus posterolateral fusion in adult isthmic spondylolisthesis. Spine 32(20):2178–2183
16. Boos N, Marchesi D, Zuber K, Aebi M (1993) Treatment of severe spondylolisthesis by reduction and pedicular fixation. A 4-6-year follow-up study. Spine 18(12):1655–1661
17. Laursen M, Thomsen K, Eiskjaer SP, Hansen ES, Bunger CE (1999) Functional outcome after partial reduction and 360 degree fusion in grade III-V spondylolisthesis in adolescent and adult patients. J Spinal Disord 12(4):300–306
18. Smith JA, Deviren V, Berven S, Kleinstueck F, Bradford DS (2001) Clinical outcome of trans-sacral interbody fusion after partial reduction for high-grade L5–S1 spondylolisthe-sis. Spine 26(20):2227–2234
19. Fabris DA, Costantini S, Nena U (1996) Surgical treatment of severe L5–S1 spondylolisthesis in children and adoles-cents: results of intraoperative reduction, posterior interbody fusion, and segmental pedicle fixation. Spine 21(6):728–733
20. Sengupta DK, Herkowitz HN (2005) Degenerative spon-dylolisthesis: review of current trends and controversies. Spine 30(Suppl 6):S71–S81
21. Weinstein JN, Lurie JD, Tosteson TD, Hanscom B, Tosteson AN, Blood EA, Birkmeyer NJ, Hilibrand AS, Herkowitz H, Cammisa FP, Albert TJ, Emery SE, Lenke LG, Abdu WA, Longley M, Errico TJ, Hu SS (2007) Surgical versus nonsurgical treatment for lumbar degenerative spon-dylolisthesis. N Engl J Med 356(22):2257–2270
22. McLain RF (2004) Instrumented fusion for degenerative spondylolisthesis: is it necessary? Spine 29(2):170
23. Fischgrund JS, Mackay M, Herkowitz HN, Brower R, Montgomery DM, Kurz LT (1997) 1997 Volvo Award winner in clinical studies. Degenerative lumbar spondylolisthesis with spinal stenosis: a prospective, randomized study com-paring decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 22(24):2807–2812
24. Fischgrund JS (2004) The argument for instrumented decompressive posterolateral fusion for patients with degen-erative spondylolisthesis and spinal stenosis. Spine 29(2): 173–174
25. Brox JI, Sörensen R, Friis A et al (2003) Randomized clini-cal trial of lumbar instrumented fusion and cognitive inter-vention and exercises in patients with chronic low back pain and disc degeneration. Spine 28:1913–1921

122 M. Aebi
26. Hägg O, Fritzell P, Nordwall A; Swedish Lumbar Spine Study Group (2002) Characteristics of patients with chronic low back pain selected for surgery: a comparison with the general population reported from the Swedish lumbar spine study. Spine 27(11):1223–1231
27. Fritzell P, Hägg O, Jonsson D, Nordwall A; Swedish Lumbar Spine Study Group (2004) Cost-effectiveness of lumbar fusion and nonsurgical treatment for chronic low back pain in the Swedish lumbar spine study: a multicenter, random-ized, controlled trial from the Swedish Lumbar Spine Study Group. Spine 29(4):421–434; discussion Z3
28. Hayes MA, Howard TC, Gruel CR, Kopta JA (1989) Roentgenographic evaluation of lumbar spine flexion-exten-sion in asymptomatic individuals. Spine 14(3):327–331
29. Pope MH, Frymoyer JW, Krag MH (1992) Diagnosing insta-bility. Clin Orthop Relat Res 60–7. Review
30. Axelsson P, Karlsson BS (2004) Intervertebral mobility in the progressive degenerative process. A radiostereometric analysis. Eur Spine J 13(6):567–572
31. Aebi M (2005) The adult scoliosis. Eur Spine J 14(10): 925–948
32. Akbarnia BA, Ogilvie JW, Hammerberg KW (2006) Debate: degenerative scoliosis: to operate or not to operate. Spine 31(Suppl 19):S195–S201
33. Shapiro GS, Taira G, Boachie-Adjei O (2003) Results of sur-gical treatment of adult idiopathic scoliosis with low back pain and spinal stenosis: a study of long-term clinical radio-graphic outcomes [clinical case series]. Spine 28(4):358–363
34. Takahashi S, Delécrin J, Passuti N (2002) Surgical treatment of idiopathic scoliosis in adults: an age-related analysis of outcome [deformity]. Spine 27(16):1742–1748
35. Katz JN, Harris MB (2008) Clinical practice. Lumbar spinal stenosis. N Engl J Med 358(8):818–825
36. Weinstein JN, Tosteson TD, Lurie JD, Tosteson AN, Blood E, Hanscom B, Herkowitz H, Cammisa F, Albert T, Boden SD, Hilibrand A, Goldberg H, Berven S, An H; SPORT Investigators (2008) Surgical versus nonsurgical therapy for lumbar spinal stenosis. N Engl J Med 358(8):794–810
37. Spratt KF, Keller TS, Szpalski M, Vandeputte K, Gunzburg R (2004) A predictive model for outcome after conservative decompression surgery for lumbar spinal stenosis. Eur Spine J 13(1):14–21
38. Park P, Garton H, Gala VC, Hoff JT, McGillicuddy JE (2004) Adjacent segment disease after lumbar or lumbosacral fusion: reviews of the literature. Spine 29(17):1938–1944
39. Chen WJ, Lai PL, Niu CC, Chen LH, Fu TS, Wong CB (2001) Surgical treatment of adjacent instability after lum-bar spine fusion. Spine 26(22):E519–E524
40. Penta M, Fraser RD (1997) Anterior lumbar interbody fusion: a minimum 10-year follow-up. Spine 22(20):2429–2434
41. Cheh G, Bridwell KG, Lenke LG, Buchowski JM, Daubs MD, Kim Y, Baldus C (2007) Adjacent segment disease following lumbar/thoracolumbar fusion with pedicle screw instrumenta-tion: a minimum 5-year follow-up. Spine 32(20):2253–2257
42. Taskaynatan MA, Izci Y, Ozgul A, Hazneci B, Dursun H, Kalyon TA (2005) Clinical significance of congenital lum-bosacral malformations in young male population with pro-longed low back pain. Spine 30(8):E210–E213
43. Luoma K, Vehmas T, Raininko R, Luukkonen R, Riihimaki H (2004) Lumbosacral transitional vertebra: relation to disc degeneration and low back pain. Spine 29(2):200–205
44. Brault JS, Smith J, Currier BL (2001) Partial lumbosacral transitional vertebra resection for contralateral facetogenic pain. Spine 26(2):226–229
45. Luoma K, Vehmas T, Raininko R, Luukkonen R, Riihimäki H (2004) Lumbosacral transitional vertebra: relation to disc degeneration and low back pain. Spine 29(2):200–205
46. Chaput C, Padon D, Rush J, Lenehan E, Rahm M (2007) The significance of increased fluid signal on magnetic resonance imaging in lumbar facets in relationship to degenerative spondylolisthesis. Spine 32(17):1883–1887
47. Buttermann GR, Garvey TA, Hunt AF, Transfeldt EE, Bradford DS, Boachie-Adjei O, Ogilvie JW (1998) Lumbar fusion results related to diagnosis. Spine 23(1):116–127
48. Steven ID, Fraser RD (1996) Clinical practice guidelines. Particular reference to the management of pain in the lum-bosacral spine. Spine 21(13):1593–1596
49. Boos N, Semmer N, Elfering A et al (2002) Natural history individuals with asymptomatic disc abnormalities in mag-neticresonance imaging: predictors of low back parin-related medical consultation and work incapacity. Spine 25(12): 1484–1492
50. Bono CM, Lee CK (2004) Critical analysis of trends in fusion for degenerative disc disease over the past 20 years: influence of technique on fusion rate and clinical outcome. Spine 29(4):455–463
51. Moore KR, Pinto MR, Butler LM (2002) Degenerative disc disease treated with combined anterior and posterior arthrodesis and posterior instrumentation. Spine 27(15): 1680–1686
52. Herkowitz HN, Abraham DJ, Albert TJ (1999) Management of degenerative disc disease above an L5–S1 segment requir-ing arthrodesis. Spine 24(12):1268
53. van Tulder M, Becker A, Bekkering T, Breen A, del Real MT, Hutchinson A, Koes B, Laerum E, Malmivaara A; COST B13 Working Group on Guidelines for the Management of Acute Low Back Pain in Primary Care (2006) Chapter 3 European guidelines for the management of acute nonspe-cific low back pain in primary care. Eur Spine J 15(Suppl 2):S169–S191
54. Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, Mannion AF, Reis S, Staal JB, Ursin H, Zanoli G; COST B13 Working Group on Guidelines for Chronic Low Back Pain (2006) Chapter 4 European guide-lines for the management of chronic nonspecific low back pain. Eur. Spine J 15(Suppl 2):S192–S300
55. Schafer J, O’Connor D, Feinglass S, Salive M (2007) Medicare evidence development and coverage advisory committee meeting on lumbar fusion surgery for treatment of chronic back pain from degenerative disc disease [Editorial]. Spine 32(22):2403–2404
56. Søgaard R, Bünger CE, Laurberg I, Christensen FB (2007) Cost-effectiveness evaluation of an RCT in rehabilitation after lumbar spinal fusion: a low-cost, behavioural approach is cost-effective over individual exercise therapy. Eur Spine J 17(2):262–271

123M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_4.2, © Springer-Verlag Berlin Heidelberg 2010
History
Roy-Camille is widely attributed as the originator of pedicle screws. They became both popular and contro-versial in North America through the implant develop-ments led by Art Steffee. Since then, many have contributed to implant and screw design, methods of connecting the screw heads to plates and rods and facil-itating insertion and removal. From the inception of these devices there have been concerns about accuracy of insertion and methods of improving or perfecting implant insertion. Bioengineers have been involved in this process throughout, particularly in developing and testing robust designs that are easy to insert and use. This article is not offering a review of this work, which while perhaps incomplete, does give a clear message that pedicle screws are biomechanically sound. A recent article on pedicle screw in flexible fixation will allow access to the literature [1]. In contrast, the clini-cal evidence of efficacy is less clear-cut – this is what I shall explore in this chapter.
Indications
Trauma
The evidence base for fixation of spinal fractures is largely based on anecdote. One systematic review is Verlaan, 2004 [2]. Their conclusion, which is based on
a review of 132 reports (mainly retrospective case-series) of a total of 5,748 patients, is that in general, surgical treatment of traumatic spine fractures is safe and effective. Surgical techniques can only be com-pared using randomized controlled trials. There is nothing specific about pedicle screws.
Deformity
Pedicle screws have transformed spinal deformity sur-gery and are widely used. Using pedicle screws throughout the spine was pioneered by Suk in Korea [3]. Biomechanical evidence suggests that screws are better than alternative methods of attachment to the spine and this is the basis for the evidence base. This probably means that the spine will end up straighter [4]. Whether or not this provides a better clinical out-come is another question not addressed by the avail-able literature [5].
Degenerative
The important complications associated with pedicle screws are misplacement, pseudoarthrosis and revi-sion. I am not discussing misplacement but the other two complications are important elements of success.
Here the evidence base is more complex because the focus is on pain rather than deformity. It would seem that pedicle screws may increase the fusion rate, but not improve the clinical results. This area is made more complex because the indications for surgery for chronic back pain have a poor evidence base. First let us look at outcomes.
Evidence for Efficacy of Pedicle-Based Systems
Jeremy Fairbank
J. Fairbank Nuffield Orthopaedic Centre, Oxford OX3 7LD, UK e-mail: [email protected]
4.2

124 J. Fairbank
Fifteen years ago, Zdeblick [6] published one of the earliest trials in spine surgery where degenerative spondylolisthesis in 124 patients was widely decom-pressed and fused either with or without pedicle screws. Sixty-four percent was fused in the non-instrumented arm compared with 88% in the instrumented arm. There were no differences in the clinical outcome. There were methodological problems with this study, but in the view of a review group, not withstanding these problems, the overall conclusion was valid [7]. However, if you look at the clinical outcome, there is nothing to choose between the groups.
Fischgrund et al. reported a 2-year follow up of 76 patients with degenerative spondylolisthesis [8]. They were randomized to posterolateral fusion with or with-out instrumentation. Clinical outcome was excellent or good in 76% with instrumentation and 85% without instrumentation. Successful arthrodesis occurred in 82% with instrumentation and 45% without instru-mentation. Overall, successful fusion did not influence patient outcome.
The same patients were followed 5–14 years follow-ing surgery (Av f/u 7 year 8 months) [9]. Only 47 patients could be found (62%). They found the clinical outcome was excellent to good in 86% of patients with a solid arthrodesis, and only in 56% of the patients with a pseudoarthrosis. There were significant differences in residual back and lower limb pain, even though the pre-operative back and lower limb pain was similar in these groups. The “solid fusion” group had better symptom severity and physical function. In spite of this, they found similar “patient satisfaction” status in each group. This was a prospective study, but with a high dropout, which should temper the interpretation of this result.
France et al. prospectively randomized 71 fusion cases to pedicle fixation or no fixation. At 2 years, there was no difference in clinical outcome and a slight and non-significant increase in fusion rates [10].
In a Danish study, 129 patients were randomized by Christensen et al. to posterolateral fusion and decom-pression, with or without pedicle screws. At 5 years, 93% were followed up. Of those randomized to pedicle screws, a quarter (24%) required revision surgery com-pared with 14% of non-instrumented patients. There was no difference in work capacity (51%) or functional outcome between groups. Patient satisfaction was 70% in the uninstrumented group and 67% in the instru-mented group.
The Swedish spine study randomized 294 patients to fusion by three different methods (and a fourth group to non-operative care) [11]. For the purposes of this chapter we shall look at the 222 patients random-ized to posterolateral fusion alone (73 patients), poste-rior lateral fusion with instrumentation (mainly pedicle screws) (74 patients) and interbody fusion with instru-mentation (75 patients). There were no clinical differ-ences in outcome, but the early complication rates in each group were 6, 16 and 31%, respectively. However, the fusion rates were 72, 87 and 91%, respectively.
In Norway [12, 13], 64 patients were randomized to posterior fusion with pedicle screws (1 or 2 levels) or cognitive interventional exercises. In the surgery group, the mean ODI was reduced from 41 to 26, and in the CBT group, ODI fell from 42 to 30. This reflects no clinical difference between groups.
In the UK, we did the MRC Spine Stabilization Trial, for which we recruited 349 patients [14]. Patients were randomized to an intensive non-operative functional res-toration programme or to spinal fusion of the surgeons’ choice. We have just published a report of the outcomes in the surgical arm of the study. In 176 patients, 3 groups of operations were chosen by the treating surgeons: 24 patients with flexible fixation (Graf/Global ligament), 56 patients with posterolateral fusion (96% fixed by pedicle screws) and 57 patients with interbody fusion with posterior fixation. At 2 years, revision surgery was needed in 8, 2 and 14% of each group, respectively. The economic cost of each group of operations in pounds sterling (mean and 95% confidence intervals) was £6927 (£6349–£7505), £6164 (£5565–£6763) and £9264 (£8594–£9933). This makes posterolateral fusion even with pedicle screws, cheaper than the other two options.
Conclusions
Meta-analysis supports the conclusion that instrumen-tation increases fusion rates (Odds Ratio 2.3 (95% CI 1.1–4.8)), but not clinical outcome [15].
My conclusion would be that using posterior instru-mentation for degenerative disorders (and that means pedicles screws) will increase the length of surgery, the complication rate, the revision rate, and hence, the cost of surgery over an uninstrumented fusion. If we look down the line at the clinical outcome, there seems little to favour instrumentation over non-instrumented fusion.

1254.2 Evidence for Efficacy of Pedicle-Based Systems
This article is not here to ask if you should be doing fusions in the first place, but if you must, the first choice should be uninstrumented fusion. Deformity is another matter, and certainly better corrections can be obtained. There are still questions around the quality of the out-come. Spinal fractures are mainly managed successfully using pedicle screws, although again there are arguments for non-operative treatment of some fracture patterns.
References
1. Wilke H-J, Drumm J, Häussler K, Mack C, Steudel W-I, Kettler A (2008) Biomechanical effect of different lumbar interspinous implants on flexibility and intradiscal pressure. Eur Spine J 17(8):1049–1056
2. Verlaan J, Diekerhof C, Buskens E, van der Tweel I, Verbout A, Dhert W et al (2004) Surgical treatment of traumatic frac-tures of the thoracic and lumbar spine: a systematic review of the literature on techniques, complications, and outcome. Spine 29(7):803–814
3. Suk S, Lee C, Kim W, Chung Y, Park Y (1995) Segmental pedicle screw fixation in the treatment of thoracic idiopathic scoliosis. Spine 20(12):1399–1405
4. Lehman R, Lenke L, Keeler K, Kim Y, Buchowski J, Cheh G et al (2008) Operative treatment of adolescent idiopathic scoliosis with posterior pedicle screw-only constructs: mini-mum three-year follow-up of one hundred fourteen cases. Spine 33(14):1598–1604
5. Winter R, Lonstein J, Denis F (2007) How much correction is enough? Spine 32(24):2641–2643
6. Zdeblick TA (1993) A prospective, randomized study of lumbar fusion. Preliminary results. Spine 18(8):983–991
7. Angevine P, Dickman C, McCormick P (2007) Lumbar fusion with and without pedicle screw fixation: comments on a prospective, randomized study. Spine 32(13):1466–1471
8. Fischgrund J, Mackay M, Herkowitz H, Brower R, Montgomery D, Kurz L (1997) Degenerative lumbar spon-dylolisthesis with spinal stenosis: a prospective randomized study comparing decompressive laminectomy and arthrode-sis with or without spinal instrumentation. Spine 22: 2807–2812
9. Kornblum M, Fischgrund J, Herkowitz H, Abraham D, Berkower D, Ditkoff J (2004) Degenerative lumbar spon-dylolisthesis with spinal stenosis: a prospective long-term study comparing fusion and pseudarthrosis. Spine 29(7): 726–733
10. France JC, Michael J, Lauerman WC, Cain JE, Glover JM, Lawson KJ, Coe JD et al (1999) A randomized prospective study of posterolateral lumbar fusion: outcomes with and without pedicle screw instrumentation. Spine 24(6): 553–560
11. Fritzell P, Hagg O, Wessburg P, Nordwall A, Group SLSS (2002) Chronic back pain and fusion: a comparison of three surgical techniques: a prospective multicentre randomized study from the Swedish Lumbar Spine Study Group. Spine 27:1131–1141
12. Brox J, Sørensen R, Friis A, Nygaard Ø, Indahl A, Keller A et al (2003) Randomized clinical trial of lumbar instru-mented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 28(17):1913–1921
13. Brox J, Reikerås O, Nygaard Ø, Sørensen R, Indahl A, Holm I et al (2006) Lumbar instrumented fusion compared with cognitive intervention and exercises in patients with chronic back pain after previous surgery for disc herniation: a pro-spective randomized controlled study. Pain 122(1–2): 145–155
14. Wilson-MacDonald J, Fairbank J, Frost H, Yu L-M, Barker K, Collins R et al (2008) The MRC spine stabilization trial: sur-gical methods, outcomes, costs, and complications of surgi-cal stabilization. Spine 33(21):2334–2340
15. Gibson J, Waddell G (2005) Surgery for degenerative lum-bar spondylosis: updated cochrane review. Spine 30(20): 2312–2320

127M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_4.3, © Springer-Verlag Berlin Heidelberg 2010
Introduction
According to text books and the princeps paper of Verbiest, the typical complaints of patients presenting with lumbar spinal stenosis (LSS) are neurogenic clau-dication, radicular pain and neurological impairment like motor deficit or sensory disturbance [1]. In daily clinical practise, it appears that the symptoms associ-ated with LSS range from none to one or several of the following: neurogenic claudication, radicular pain, motor deficit, sensory alterations or deficit and low back pain (LBP). The latter is often the major symp-tom that leads the patient to seek treatment. LBP is significant in up to 75% of the patients with LSS.
While it is agreed upon that the surgical decompres-sion of the compromised neural structures will cure or relieve peripheral symptoms in a significant number of cases, the therapeutic attitude regarding LBP remains a subject of controversy [2, 3]. Indications for fusion, with or without instrumentation, or stabilisation by some non-rigid means are still not well-defined. The presence of LBP, disc degeneration, spondylolysthesis, instability on dynamic radiographs or iatrogenic instability induced by facetectomy or discectomy are among the arguments invoked to carry out some type of stabilisation. However, the indication for instrumentation must be discussed in view of the demonstrated increase of morbidity associ-ated to it and a series of contraindications for stabilisa-tion often observed in the same group of patients: osteoporosis, obesity, multi-level hyper-mobility, risk factors for infection like diabetes, cortisone therapy, etc.
Finally, the true contribution of stabilisation to the improvement of outcome in the treatment of spinal stenosis vs. selective decompression alone is not known, except in cases of major, focal instability where fusion is mandatory. The picture is even more confused because of the large variety of procedures that are used regarding decompression as well as stabilisation.
Decompression can be obtained by total laminec-tomy with or without facet resection or limited lamino-tomy by fenestrations between lamina, sparing the facet joints as initially described by Senegas [4]. This can even be improved by preserving the spinous pro-cess and the supraspinous ligament allowing for rein-sertion of the lumbar fascia by the end of the procedure. When comparing the local anatomy after completion of a laminectomy vs. the fenestration technique, it is obvious that a difference in spine function may result. With the conservative procedure, after healing, strong adherences are formed between the soft tissues and the posterior elements, providing better stability and pos-sibly better functionality to the vertebral column. A recent prospective study by Fu et al. does indicate a better outcome of the fenestration technique as com-pared to laminectomy in particular regarding LBP [5]. This is in accordance with the work of Postacchini et al. who already showed a better outcome regarding LBP in patients treated by partial laminotomy com-pared to classic laminectomy [6].
The same confusion exists regarding stabilisation. Stabilisation can be obtained by fusion with or without instrumentation or only by instrumentation without fusion including systems with pedicular anchoring united by polymeric strands, claiming to present less rigidity, or even more recently, interspinous devices intended to open up the spinal canal. Some peer reviewed studies do not substantiate the initial enthusi-asm for these procedures [7]. Besides the different
Low Back Pain Is Not an Indication for Stabilisation in Patients Operated for Lumbar Spinal Stenosis
E. Munting
E. Munting Clinique Saint Pierre, 1340 Ottignies Louvain-la-Neuve, Belgium e-mail: [email protected]
4.3

128 E. Munting
techniques, the indication for any type of stabilisation is not better defined.
This study will not bring an answer to these ques-tions. However, in our daily practise, we did see a lot of patients with spinal stenosis of which major complaint was LBP, associated to some extent to neurogenic clau-dication and/or nerve root pain. Quite often, after decom-pressive laminotomy sparing the posterior elements and without any kind of stabilising device, the patients reported the disappearance or significant improvement of their LBP. Therefore, we decided to assess more spe-cifically the outcome of LBP in LSS patients after decompression by minimal laminotomy, sparing the facet joints, the spinous processes and the supraspinous ligaments. Stabilisation was only carried out when major instability was demonstrated peroperatively.
Materials and Methods
Hundred and thirty six patients operated for LSS with a minimum 1-year follow-up were reviewed. A grade 1 degenerative spondylolysthesis was observed in 40 of these patients. Patients were assessed pre- and post-operatively by Dallas questionnaire or by grading their LBP as severe, significant, minor or absent. The same was asked for leg/buttock pain and walking capacity.
The decompression procedure also called “calibra-tion” involves flavoligamentectomy, undercutting of the lamina, the facet joints and the neuroforamina as needed, according to the preoperative MRI and/or CT-scan (Fig. 4.3.1). In case of disc protrusion, discec-tomy and/or disc osteophytes resection is carried out if the canal calibration is not sufficient to decompress the
a b
c d
Fig. 4.3.1 a–d: Pre- and post-operative aspect of the spinal canal treated by the fenestration technique

1294.3 Low Back Pain Is Not an Indication for Stabilisation in Patients Operated for Lumbar Spinal Stenosis
neural structures. The caudal half of the lamina, the spinous processes and the supra-spinous ligament are preserved. After decompression, the lumbar fascia is carefully re-attached to the spinous process and the supra-spinous ligament. The patient is encouraged to walk the day after surgery. No brace is prescribed.
Results
Laminotomy was associated with some type of stabili-sation in 18/136 of the cases (13%), because of major instability (over 5 mm antero-posterior mobility) and independently of the presence of degenerative spon-dylolysthesis. Instrumented arthrodesis was preferred in case of focal instability (11 cases: 8%) and Dynesisr (Zimmer, Warsaw) in case of multilevel instability (7 cases: 5%).
Five cases with laminotomy only were lost to fol-low-up. Overall results were good or excellent in 84 (74%) of isolated laminotomies, in 11/11 laminotomies with arthrodesis and in 2/7 laminotomies with Dynesisr. Out of 113 patients presenting severe or significant LBP preoperatively and undergoing only laminotomy, 74% were significantly improved regarding LBP. Seven patients had to be re-operated for some reason, of which two because of symptomatic instability with LBP requiring instrumented fusion and one after stabilisa-tion with a Dynesisr that became loose after some months. The patient’s LBP was cured by simple removal of the hardware. Radicular symptoms resolved or were significantly improved in 87% and walking distance was increased in 90% of the patients. Incidental duro-tomy had no adverse effect except in one case where a re-operation was needed for dural tear repair.
Discussion
In LSS, Grob et al. [8] did not find any difference in out-come of decompression with or without arthrodesis in the absence of obvious instability. When LBP is a major symptom in patients with LSS, significant improvement by decompression alone can be obtained if severe insta-bility is not demonstrated prior or at the time of surgery. When associated with LSS, disabling LBP should be
considered as a distinct entity in which, a priori, the treat-ment should be selective decompression and not arthrod-esis. A recent paper by Visuri et al. shows, with an MRI study, that LSS predicts chronic LBP more accurately than intervertebral disc degeneration may support the idea of a specific link between LSS and LBP [9].
Minimal laminotomy sparing the spinous processes and the supraspinous ligament obviously allows fixa-tion of the paraspinal muscles and lumbar fascia to the vertebrae. The healing process and the unavoidable fibrosis associated with it, provides a very strong and “dynamic” stabilisation means that may partially explain the high frequency of significant improvement of LBP in patients undergoing only laminotomy with-out stabilisation. The avoidance of direct adhesion of the muscles to the dural sac – as observed in classic laminectomy – is also theoretically favourable.
Whatever the reasons for improvement or cure of LBP observed only after decompression , the facts are that the incidence of these favourable results, are simi-lar to what is observed for arthrodesis indicated for LBP.
Obviously, all the potential complications specifi-cally related to instrumented fusion or stabilisation are avoided while performing decompression only. The incidence of relative contraindications for stabilisation is quite elevated in LSS patients. Osteoporosis affects 55% of the people of age 50 and older in the United States [10]. Diabetes, obesity, smoking, long-term ste-roid use are also conditions often found in elderly patients that increase the risk for infection, non-union or hardware loosening in case of non-fusion techniques.
Multi-level involvement of spinal stenosis and degenerative alterations is another fact that renders dif-ficult the definition of the levels to be treated. The more levels to be instrumented, the higher the risk for complications.
Conclusions
Demonstrated, biomechanical instability is an excel-lent indication for fusion in patients with LSS.
In patients with spinal stenosis in the absence of obvious instability, decompression by serial fenestra-tions without fixation improves LBP significantly in 74% of the patients. The symptom “LBP” is not an

130 E. Munting
indication for fusion or stabilisation in the absence of instability. This is advantageous in terms of lesser risk for complications and economically by avoiding the significant costs of spinal instrumentation. The indica-tions for some type of stabilisation should be restricted to well-defined cases of severe and focal instability that can be demonstrated during surgery.
The preservation of the spinous processes and the supraspinous ligament and the reinsertion of the lum-bar fascia to these structures contribute to the long-term stability of the spine.
References
1. Verbiest H (1954) Aradicular syndromefrom developmental narrowing of the lubar vertebral canal. J Bone Joint Surg 36B:230–237
2. Keller AS, RB WuYA, Deyo RA, Singer DE (2005) Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the Maine lumbar spine study. Spine 15:936–943
3. Weinstein JN, Lurie JD, Tosteson TD, Hanscom B, Tosteson AN, Blood EA, Birkmeyer NJ, Hilibrand AS, Herkowitz H, Cammisa FP, Albert TJ, Emery SE, Lenke LG, Abdu WA,
Longley M, Errico TJ, Hu SS (2007) Surgical versus non-surgical treatment for lumbar degenerative spondylolisthe-sis. N Engl J Med 356(22):2257–2270
4. Senegas J, Etchevers JP, Vital JM, Baulny D, Grenier F (1988) Recalibration of the lumbar canal, an alternative to laminectomy in the treatment of lumbar canal stenosis. Rev Chir Orthop Rep Appar Mot 74:15–22
5. Fu YS, Zeng BF, Xu JG (2008) Long-term outcomes of two different decompressive techniques for lumbar spinal steno-sis. Spine 33:514–518
6. Postacchini F, Cinotti G, Perugia D, Gumina S (1993) The surgical treatment of central lumbar stenosis. Multiple lami-notomy compared with total laminectomy. J Bone Joint Surg Br 75(3):386–392
7. Verhoof OJ, Bron JL, Wapstra FH, van Royen BJ (2008) High failure rate of the interspinous distraction device (X-Stop) for the treatment of lumbar spinal stenosis caused by degenerative spondylolisthesis. Eur Spine J 17(2): 188–192
8. Grob D, Humke T, Dvorak J (1995) Degenerative lumbar spinal stenosis. Decompression with and without arthrode-sis. J Bone Joint Surg Am 77(7):1036–1041
9. Visuri T et al (2005) Narrowing of lumbar spinal canal pre-dicts chronic low back pain more accurately than interverte-bral disc degeneration: a magnetic resonance imaging study in young finnish male conscripts. Mil Med 170(11): 926–930
10. National Osteoporosis Foundation. America’s bone health: The state of osteoporosis and low bone mass in our nation. February 2002
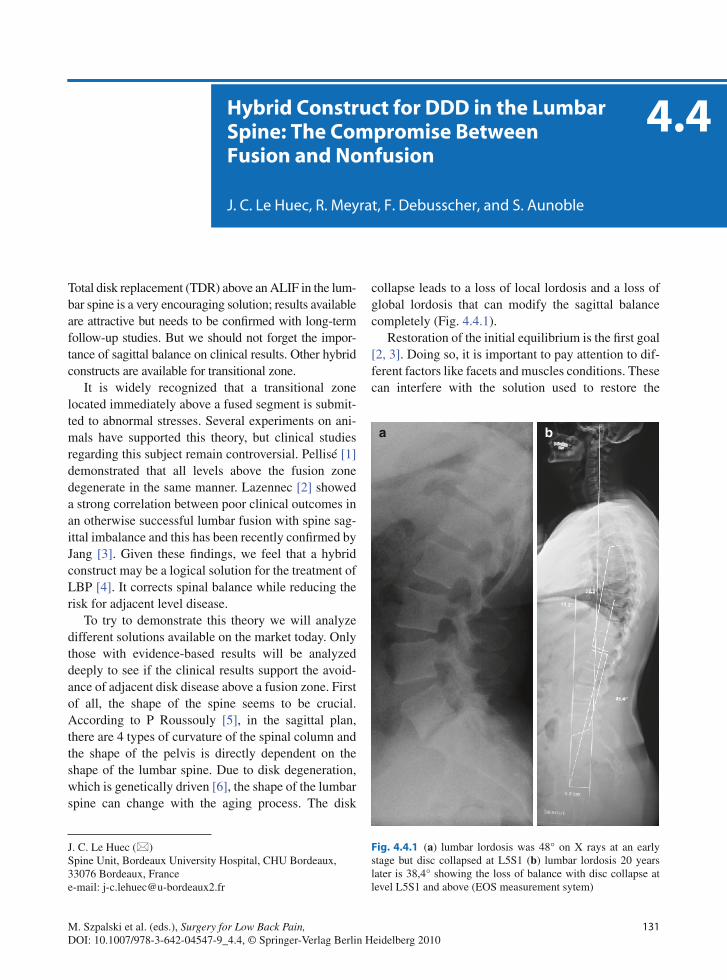
131M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_4.4, © Springer-Verlag Berlin Heidelberg 2010
Total disk replacement (TDR) above an ALIF in the lum-bar spine is a very encouraging solution; results available are attractive but needs to be confirmed with long-term follow-up studies. But we should not forget the impor-tance of sagittal balance on clinical results. Other hybrid constructs are available for transitional zone.
It is widely recognized that a transitional zone located immediately above a fused segment is submit-ted to abnormal stresses. Several experiments on ani-mals have supported this theory, but clinical studies regarding this subject remain controversial. Pellisé [1] demonstrated that all levels above the fusion zone degenerate in the same manner. Lazennec [2] showed a strong correlation between poor clinical outcomes in an otherwise successful lumbar fusion with spine sag-ittal imbalance and this has been recently confirmed by Jang [3]. Given these findings, we feel that a hybrid construct may be a logical solution for the treatment of LBP [4]. It corrects spinal balance while reducing the risk for adjacent level disease.
To try to demonstrate this theory we will analyze different solutions available on the market today. Only those with evidence-based results will be analyzed deeply to see if the clinical results support the avoid-ance of adjacent disk disease above a fusion zone. First of all, the shape of the spine seems to be crucial. According to P Roussouly [5], in the sagittal plan, there are 4 types of curvature of the spinal column and the shape of the pelvis is directly dependent on the shape of the lumbar spine. Due to disk degeneration, which is genetically driven [6], the shape of the lumbar spine can change with the aging process. The disk
collapse leads to a loss of local lordosis and a loss of global lordosis that can modify the sagittal balance completely (Fig. 4.4.1).
Restoration of the initial equilibrium is the first goal [2, 3]. Doing so, it is important to pay attention to dif-ferent factors like facets and muscles conditions. These can interfere with the solution used to restore the
Hybrid Construct for DDD in the Lumbar Spine: The Compromise Between Fusion and Nonfusion
J. C. Le Huec, R. Meyrat, F. Debusscher, and S. Aunoble
J. C. Le Huec (*) Spine Unit, Bordeaux University Hospital, CHU Bordeaux, 33076 Bordeaux, France e-mail: [email protected]
4.4
a b
Fig. 4.4.1 (a) lumbar lordosis was 48° on X rays at an early stage but disc collapsed at L5S1 (b) lumbar lordosis 20 years later is 38,4° showing the loss of balance with disc collapse at level L5S1 and above (EOS measurement sytem)

132 J. C. Le Huec et al.
balance. Restoration of lordosis with facet arthritis is a bad concept, and keeping motion on a segment with bad muscles is not appropriate [7].
The transitional zone adjacent to a fusion can be treated through either an anterior and/or posterior approach.
Two techniques are available for the anterior approach: nucleus replacement and TDR. Among all the nucleus replacement devices, only PDN Raymedica [8, 9] has a long follow-up. However, long-term outcome seems to be disappointing [8]. Recently the DASCOR [10] presented a 3-year follow-up with promising results (Fig. 4.4.2). However, more extensive studies need to be done before any conclusion can be arrived at. The sec-ond anterior approach technique, using TDR, has become very popular in recent years. In the presence of good posterior paraspinous muscles and in the absence of facet problems, TDR is a very elegant technique that allows the patient to contour his spine and restore bal-ance [11, 12]. According to Le Huec [13], TDR can decrease the stress on the adjacent level by decreasing the lordosis at the adjacent level (Fig. 4.4.3).
TDR above an ALIF in the lumbar spine seems to be a good compromise [14–16], particularly at level L4–5 since it is the most important level involved in restoring the lumbar lordosis and overall balance [17]. The recent IDE study (2-years follow-up) using Maverick demon-strated statistical superiority of the TDR compared to fusion ALIF (anterior lumbar interbody fusion) in the treatment of discogenic back pain [18]. This is very encouraging, but needs to be confirmed on a long-term follow-up at 5 years to demonstrate the efficacy of the prevention of adjacent disk disease.
Since the posterior approach is the most common approach for the treatment of DDD and LBP, its effects on the transitional zone after a fusion need to be evalu-ated. The posterior approach requires detachment of the posterior paraspinal muscles and leads to fatty degenera-tion and loss of function [7, 19]. Compromise of the paraspinal muscles reduces support of the transitional zone. A weakened transitional zone in a spine with sagit-tal imbalance can lead to further decompensation and further instability. Several dynamic stabilization systems have been developed aimed at the transitional zone [20].
Fig. 4.4.2 (a) principle of balloon DASCOR technology (Disc Dynamic, Minneapolis, USA). Once in the disc the balloon is insufflated with polymer to obtain a mechanical support between the endplates (b) post operative MRI showing the device in good position
a
b

1334.4 Hybrid Construct for DDD in the Lumbar Spine: The Compromise Between Fusion and Nonfusion
Interspinous devices often used for the treatment of stenosis are not designed to reduce the stresses at the transitional zone. They increase the local kyphosis, limit extension, and increase the load on the anterior part of the disk. Today, the efficacy of interspinous devices to prevent adjacent pathologies has not been demonstrated [21].
Pedicular-based systems initially reported by Dubois have brought forth the concept of disk neutralization [22, 23]. Clinical experience using this technology extends beyond 10 years. The Dynesis system is one such system where a flexible rod system allows con-trolled flexion and extension [24]. However, Dynesis is very stiff when compared with titanium rods, and according to Grob D [25], (Fig. 4.4.4) demonstrates little advantage over fusion. In contrast, Putzier M has demonstrated a significant decrease in postdiscectomy LBP using Dynesis in a prospective randomized trial [26]. The Aladin system developed by Perrin has showed some promising results on midterm follow-up, but there was no balance analysis report. More recent technologies (N spine, Penjabi system, Cosmic, etc.) that display more physiological flexibility and force distribution have been implanted. Only short-term fol-low-ups are available. Longer follow-ups are needed to confirm efficacy. The objective of all dynamic systems is to limit flexion and the resulting kyphosis above the fused level and to allow some controlled extension [20].
Theoretically, it prevents or slows degeneration of a normal or near-normal disk at the transitional zone. In cases of a collapsed disk the advantage of these systems is less meaningful because the disk is stiff [22]. Since fusion is not the goal, there is a risk for instrumentation fatigue, and eventually, instrumentation failure (screw loosening, breakage, etc.). Pedicular-based system implanted with high disk leads to a risk of implant fail-ure after disk collapse due to overstress on the screws.
In addition to the posterior-based stabilization sys-tem, in case of presence of a disk height able to main-tain some motion, it seems that to support the nucleus may solve the problem related to the disk collapse leading to pedicular screw failure. This is a new hybrid concept that needs to be evaluated. 360° function res-toration is the new challenge. Anyway, the advantage of motion preservation must be in balance with a good fusion in good position as recommended by par Jang and Lazennec [2, 3].
Conclusions
Hybrid construct is an interesting solution to prevent overstress at adjacent level than a fusion [27]. Keeping mobility on the adjacent fusion level seems to be effec-tive for the prevention of adjacent disk disease.
a b
Fig. 4.4.3 (a, b) TDR can decrease the stress on the adjacent level by decreasing the lordosis at the adjacent level

134 J. C. Le Huec et al.
Different devices are available for the surgeon; some need anterior approach and others posterior approach. Long-term outcomes are not yet well known for these techniques, but some display better results already.
TDR above an ALIF in the lumbar spine is a very encouraging solution; results available are attractive but needs to be confirmed with long-term follow-up studies. But do not forget the importance of the sagittal balance on surgical results.
References
1. Pellisé F, Hernández A, Vidal X, Minguell J, Martínez C, Villanueva C (2007) Radiologic assessment of all unfused lumbar segments 7.5 years after instrumented posterior spi-nal fusion. Spine 32(5):574–579
2. Lazennec JY, Ramaré S, Arafati N, Laudet CG, Gorin M, Roger B, Hansen S, Saillant G, Maurs L, Trabelsi R (2000) Sagittal alignment in lumbosacral fusion: relations between radiological parameters and pain. Eur Spine J 9(1):47–55
3. Jang JS, Lee SH, Min JH, Kim SK, Han KM, Maeng DH (2007) Surgical treatment of failed back surgery syndrome due to sagittal imbalance. Spine 32(26):3081–3087
4. Bertagnoli R, Tropiano P, Zigler J, Karg A, Voigt S (2005) Hybrid constructs. Orthop Clin North Am 36(3):379–388
5. Roussouly P, Berthonnaud E, Dimnet J (2003) Geometrical and mechanical analysis of lumbar lordosis in an asymptom-atic population: proposed classification. Rev Chir Orthop Reparatrice Appar Mot 89(7):632–639
6. Battié MC, Videman T (2006) Lumbar disc degeneration: epi-demiology and genetics. J Bone Joint Surg Am 88(Suppl 2): 3–9
7. Suwa H, Hanakita J, Ohshita N, Gotoh K, Matsuoka N, Morizane A (2000) Postoperative changes in paraspinal mus-cle thickness after various lumbar back surgery procedures. Neurol Med Chir 40(3):151–154; discussion 154–155
8. Bertagnoli R, Karg A, Voigt S (2005) Lumbar partial disc replacement. Orthop Clin North Am 36(3):341–347
9. Ray CD (2002) The PDN prosthetic disc-nucleus device. Eur Spine J 11(Suppl 2):S137–S142
10. Yuan HA, Hudging G, Bao QB, Bowman B (2003) Early experience with a new and novel approach to disc nucleus arthroplasty. Presented at the third annual meeting of the spine Arthroplasty society, Phoenix Arizona, May 1–4
11. Panjabi M, Henderson G, Abjornson C, Yue J (2007) Multidirectional testing of one- and two-level ProDisc-L versus simulated fusions. Spine 32(12):1311–1319
12. Tournier C, Aunoble S, Le Huec JC, Lemaire JP, Tropiano P, Lafage V, Skalli W (2007) Total disc arthroplasty: conse-quences for sagittal balance and lumbar spine movement. Eur Spine J 16(3):411–421
13. Le Huec J, Basso Y, Mathews H, Mehbod A, Aunoble S, Friesem T, Zdeblick T (2005) The effect of single-level, total disc arthroplasty on sagittal balance parameters: a prospec-tive study. Eur Spine J 14(5):480–486
14. Goel VK, Grauer JN, Patel TCh, Biyani A, Sairyo K, Vishnubhotla S, Matyas A, Cowgill I, Shaw M, Long R, Dick D, Panjabi MM, Serhan H (2005) Effects of charité artificial disc on the implanted and adjacent spinal segments mechanics using a hybrid testing protocol. Spine 30(24): 2755–2764
15. Grauer JN, Biyani A, Faizan A, Kiapour A, Sairyo K, Ivanov A, Ebraheim NA, Patel TCh, Goel VK (2006) Biomechanics of two-level Charité artificial disc placement in comparison to fusion plus single-level disc placement combination. Spine 6(6):659–666
16. Panjabi M, Malcolmson G, Teng E, Tominaga Y, Henderson G, Serhan H (2007) Hybrid testing of lumbar CHARITE discs versus fusions. Spine 32(9):959–966; dis-cussion 967
Fig. 4.4.4 Dynesis (Zimmer spine, Warsaw, USA) is a posterior pedicle based system used to prevent overstress on the top of fused segment

1354.4 Hybrid Construct for DDD in the Lumbar Spine: The Compromise Between Fusion and Nonfusion
17. Siepe CJ, Mayer HM, Heinz-Leisenheimer M, Korge A (2007) Total lumbar disc replacement: different results for different levels. Spine 32(7):782–790
18. Gornet MF, Burkus JK, Mathews HH et al (2007) MAVERICK total disc replacement vs. anterior lumbar interbody fusion with the infuse bone graft/LT-CAGE device: a prospective, randomized, controlled, multicenter trial. Presented at the 22nd annual North American Spine Society, Austin, Texas, Oct. 23–27
19. Gille O, Jolivet E, Dousset V, Degrise C, Obeid I, Vital JM, Skalli W (2007) Erector spinae muscle changes on magnetic resonance imaging following lumbar surgery through a pos-terior approach. Spine 32(11):1236–1241
20. Zander T, Rohlmann A, Burra NK, Bergmann G (2006) Effect of a posterior dynamic implant adjacent to a rigid spi-nal fixator. Clin Biomech 21(8):767–774
21. Gillet P (2007) Comment on “Long-term actuarial survivor-ship analysis of an interspinous stabilization system.” Eur Spine J 16(8):1289–1290. Epub 2007 Mar 30
22. Schwarzenbach O, Berlemann U, Stoll TM, Dubois G (2005) Posterior dynamic stabilization systems: DYNESYS. Orthop Clin North Am 36(3):363–372
23. Stoll TM, Dubois G, Schwarzenbach O (2002) The dynamic neutralization system for the spine: a multi-center study of a novel non-fusion system. Eur Spine J 11(Suppl 2):S170–S178. Epub 2002 Sep 10
24. Schmoelz W, Huber JF, Nydegger T et al (2003) Dynamic stabi-lization of the lumbar spine and its effect on adjacent segments: an in vitro experiment. J Spinal Disord Tech 16:418–423
25. Grob D, Benini A, Junge A, Mannion AF (2005) Clinical experience with the Dynesys semirigid fixation system for the lumbar spine: surgical and patient-oriented out-come in 50 cases after an average of 2 years. Spine 30(3): 324–331
26. Putzier M, Schneider SV, Funk JF, Tohtz SW, Perka C (2005) The surgical treatment of the lumbar disc prolapse: nucleot-omy with additional transpedicular dynamic stabilization versus nucleotomy alone. Spine 30(5):E109–E114
27. Cheng BC, Gordon J, Cheng J, Welch WC (2007) Immediate biomechanical effects of lumbar posterior dynamic stabilization above a circumferential fusion. Spine 32(23):2551–2557

137M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_4.5, © Springer-Verlag Berlin Heidelberg 2010
Spondylolysis
Spondylolysis is defined as a defect in the pars interar-ticularis (PI) and is unique to humans by virtue of their upright posture [1–3]. The foetal incidence of spon-dylolysis has conclusively been shown to be zero. By 6 years of age, the incidence has been reported at 4.4% and by adulthood at 6% [4]. Defects of the PI are twice as common in boys compared to girls. The incidence in the young athletic population is also much higher, and varies between 15 and 47% [5–8].
Ciullo et al. suggest that heredity plays a significant role in the clinical manifestation of this condition [9]. Repetitive loading in an individual with such genetic susceptibility ultimately leads to a stress fracture of the PI. Interestingly, neural arch defects have not been dem-onstrated in other primates. Alaskan Eskimos have an unusually high incidence between 20 and 50% [10]. The relative frequency of spondylolysis in Canadian Eskimos doubles between adolescence and early adulthood [11].
During embryological development, two factors may contribute to developmental dysplasia of the PI. First, ossification does not progress uniformly in the lower lumbar segments. Second, there appears to be a transi-tion in density between trabecular bone in the pars and the inferior articulating facet and the less dense trabe-cular bone at the base of the pedicle. If this differential ossification in tissue type and density persists into child-hood, a potential area of weakness may exist [12]. With further mechanical stress, fatigue fracture may occur.
Clinical Presentation
Typically, patients present with aching low back pain (LBP) “along the belt line”. Pain may radiate to the posterior aspect of the thighs. It may be unilateral or bilateral and is often exacerbated by hyper-extension and twisting. Radicular involvement is rare. The stand-ing one-leg lumbar extension manoeuvre typically accentuates pain. More symptomatic patients may have lumbar paraspinal muscle spasm and pain throughout the full range of lumbar motion.
Athletes have a higher incidence and prevalence of symptomatic lesions which develop at a different age compared to those observed in the asymptomatic pop-ulation [13]. The sports-active individual may present with earlier and more painful LBP, compared to those in the general population. In addition, the sports-active individual with a PI defect appears to suffer from greater loss of function compared to when a PI defect exists in the general population.
Natural history studies show unilateral pars defects not to be associated with the development of spon-dylolisthesis or significant disability [4]. Bilateral pars defects in the general population developed symptom-atic progression in only a small percentage of subjects over the long term [4]. The prognosis for a 6-year-old child with a pars defect in terms of disability and pain appears to follow that of the general population [14]. Periods of most rapid and likely slippage occur between 9 and 15 years [9]. Progressive slippage after the com-pletion of vertebral growth (circa 18–21 years) is rare.
There has been much speculation regarding the source of pain in spondylolysis. Soft tissue obtained from the pars defect at the time of surgery has been shown, by immunolocalization techniques, to contain neuropeptides associated with sensory or nociceptive transmission, possibly implicating the “spondylolysis
The Management of Spondylolysis and Spondylolisthesis
Brian J. C. Freeman and Ujjwal K. Debnath
B. J. C. Freeman (*) Department of Spinal Surgery, Level 3, Theatre Block, Royal Adelaide Hospital, North Terrace, Adelaide, SA 5000, Australia e-mail: [email protected]
4.5

138 B. J. C. Freeman and U. K. Debnath
ligament” as a source of pain [15]. In another study, con-nective and scar tissue harvested from the pars defect of symptomatic patients contained a high density of neural tissue, also implicating the pars as a potential pain source [16]. Ciullo et al. postulated two possible sources of pain; first from the acute stress fracture, and second from the segmental instability that may follow [9]. While some authors contest the fact that segmental instability leads to pain [17], others have more clearly implicated the inter-vertebral disc or facet joint as a source of pain [18]. To complicate matters further, pars defects are not universally painful. In one survey of 32,600 asymptom-atic individuals, a pars defect was noted in 7.2% [19].
Investigations
Plain lateral radiographs often may not reveal a pars defect, particularly if the defect is unilateral. The sen-sitivity may be increased if oblique radiographs are
utilized to check for the “Scottie dog sign”. However, the use of oblique radiographs incurs an excessive radiation dose for the patient and should be avoided.
Both planar bone scintigraphy and single-photon-emission computed tomography (SPECT) are more sen-sitive than plain radiographs in detecting pars lesions. They may also be able to distinguish between radio-graphic lesions that are active and those that are inactive (and presumably asymptomatic) [20–25]. SPECT offers a more sensitive indication of low intensity metabolic bone activity and bony remodelling, especially in early subtle stress reactions, than planar bone scintigraphy [20]. As the spondylolysis becomes chronic, SPECT reverts to normal, even though the spondylolysis has not completely healed [20, 22, 24–26].
Computerized tomography (CT) is applied using the reverse gantry technique, ensuring that the plane of the scan is perpendicular to that of the defect, and in thin section. In this format, CT is the most spe-cific investigation for demonstrating a spondyloly-sis (Fig. 4.5.1a). It is the investigation of choice for
cb
a
Fig. 4.5.1 (a) Reverse-gantry computed tomography through L5 showing bilateral pars defects (from Debnath et al. [44] with permission). (b) Antero-posterior radiograph following Modified Buck’s repair of L5 spondylol-ysis (from Debnath et al. [44] with permission). (c) Lateral radiograph following Modified Buck’s repair of L5 spondylol-ysis (from Debnath et al. [44] with permission)

1394.5 The Management of Spondylolysis and Spondylolisthesis
identifying radiographically occult lesions [24]. Combined SPECT and CT increases the probability of diagnosis of a pars defect [27]. Preoperative evalua-tion with CT scan is essential in planning for operative fixation. It gives valuable information regarding the morphology of the defect particularly in terms of its site, width, orientation and gapping [28, 29].
Magnetic resonance imaging (MRI) offers reduced radiation exposures and is gaining popularity for the investigation of patients with suspected injuries of the PI. Short T1 inversion recovery images can reveal changes within the PI, as well as oedema within the pedicles, thus providing greater sensitivity when com-pared to other imaging modalities [30]. Hollenberg et al. described a new MRI classification system which defines five grades of pars defect (Table 4.5.1) and dem-onstrated high intra- and inter-observer reliability [31].
Treatment
Conservative Treatment
Treatment depends on the severity of symptoms, age of the patient and level of sporting activity. Conservative options include: avoidance of sporting activity, trunk stability, strength training and analgesic medication or brace treatment. The aim of managing painful lesions
in young active individuals is to achieve bony union (or at least a fibrous union) of the pars defect in order to eliminate movement across the defect. The basic components of conservative treatment can be split into four areas.
1. Reduction of activity level that causes the pain and relative immobilization.
2. Stretching the hamstrings and glutei.3. Abdominal strengthening exercises and back exten-
sors, including core stability and functional stabi-lizing programmes.
4. Graded return to provocative exercise when symp-toms subside to allow comfortable exercise.
Conservative treatment in the form of bracing and avoidance of sports for at least 3–6 months has been recommended. Steiner and Micheli treated symptom-atic patients with a modified Boston brace worn for 23 h per day for 6 months, followed by a weaning period [32]. Participation in sports was permitted, pro-vided the brace was worn and the activity did not pro-duce symptoms.
Appropriate physical therapy includes hamstring and lumbo-sacral stretching, along with abdominal core strengthening [33]. Criteria for return to sports are dominated by symptom-led decisions and rarely based on the natural history of the lesion in terms of healing. The healing potential for a symptomatic unilateral pars defect is higher than bilateral spondylolytic defects. This has been established by Sys et al. who followed up 11 athletes with unilateral spondylolysis demonstrating healing rates of 100% [34]. Fuji et al. suggested that the stage of the defect at diagnosis was the most important predictor of successful union [35]. Non-operative management for 6–12 months has been declared the gold standard for managing patients with either unilateral or bilateral spondylolysis [36, 37].
Surgical Treatment
A small percentage of patients need surgery. The inci-dence of disabling LBP due to a pars defect in the young competitive athlete is low. However, there are some individuals who experience disabling symptoms that are unresponsive to conservative treatment and preclude them from participating in their sport. Historically, postero-lateral fusion with or without excision of the posterior elements had been the
Table 4.5.1 Magnetic resonance imaging (MRI) classification of lumbar PI defects from Hollenberg et al. [31] (with permission)
Grade Description of MRI Findings
0 Normal, no signal abnormalities of PI
1 T2 signal abnormalities of PI with or without signal changes of adjacent pedicle or articular process, but no spondylolysis
2 T2 signal abnormalities and thinning, fragmentation or irregularity of the PI visible on T1 and T2-weighted images
3 Visible complete unilateral or bilateral spondylolysis with associated abnormal T2 signal
4 Complete spondylolysis without abnormal T2 signal (old united fractures)
PI pars interarticularis

140 B. J. C. Freeman and U. K. Debnath
recommended surgical treatment. Loss of motion and increased load on the adjacent segment have however made this an unpopular treatment.
Removal of the fibrous non-union, insertion of autogenous bone graft and direct repair of the PI defect eliminates the main locus of pain and preserves motion in that motion segment. Injection of the pars defect with local anaesthetic has been advocated to confirm the source of pain prior to surgical intervention [11, 38]. Several techniques have been developed to stabilize a spondylolytic defect in the lumbar spine. Commonly used methods include the direct repair described by Buck [39] (Fig. 4.5.1b, c), the Morscher hook screw [40, 41], the Scott wiring technique [42] and other screw-hook combinations [43]. Several authors have analyzed the effectiveness of various systems with successful outcomes reported in 72–95% of patients [39–47].
Biomechanical studies on fresh frozen calf lumbar spines with artificially-induced bilateral pars defects confirmed increased inter-vertebral mobility, not only at the involved level, but also at the level adjacent to the defect [48]. This hyper-mobility of both segments was significantly reduced by a “Buck’s repair” of the spondylolytic segment. Deguchi et al. carried out a biomechanical comparison of four spondylolysis fixa-tion techniques [49]. The screw-rod-hook system of Morscher and Buck’s technique allowed the least motion across the pars defect, when tested in flexion [49]. Similarly, Kip et al. concluded that these two techniques provided the strongest and stiffest construct [50].
Predictors of successful surgical outcome include; age less than 25 years, spondylolysis of less than 4 mm, absence of disc degeneration at the target level, posi-tive response to a pars block, method of surgical repair and psychological motivation of the individual under-going surgery [38, 39, 44, 51]. Ivanic et al. reported a pseudarthrosis rate of 8.6% for patients less than 20 years, compared to 35% in patients over the age of 20 years [40].
Should an additional source of pain, such as the inter-vertebral disc, be confirmed on lumbar discogra-phy, most authors would proceed with an instrumented fusion of the affected motion segment if the patient was sufficiently disabled. Others have strived to retain motion, performing a direct repair of the pars defect in
conjunction with a total disc replacement for such indi-viduals [52].
Summary
Lumbar spondylolysis is a common condition with an adult incidence of 6%, many of whom remain asymp-tomatic. The incidence is much higher in sports-active individuals ranging from 15 to 47%. Unilateral pars defects are not associated with significant disability or the development of spondylolisthesis in the long term. Bilateral pars defects in the general population develop symptomatic progression in only a small percentage of subjects over the long term. MRI is gaining popularity as the investigation of choice in patients with suspected injuries of the PI. Conservative treatment is effective in the majority of instances, particularly for unilateral defects. Direct repair of the PI defect maybe indicated if conservative measures fail. Under such circum-stances, successful outcome has been reported in 72–95% of patients.
Spondylolisthesis
Spondylolisthesis is defined as the forward displace-ment of one vertebra with reference to the vertebra below. It was first described in 1792 by Herbinaux, a Belgian obstetrician who noted that occasionally a bony prominence was present in front of the sacrum and this was potentially implicated in problems with delivery [53]. Spondylolisthesis is reported with an incidence between 2 and 3% in Caucasian females and 6% in Caucasian males.
Wiltse et al. proposed an anatomic classification of spondylolisthesis consisting of six types [3, 54, 55] (Table 4.5.2). Isthmic spondylolisthesis (Type II) was further subdivided into three subtypes: (A) Lytic type associated with a stress fracture of the pars; (B) Elongated type with an intact pars; (C) Associated with an acute fracture of the PI resulting from a major trauma.
Marchetti and Bartolozzi subsequently developed a classification based on aetiology that differentiates between the various pathologic processes leading to

1414.5 The Management of Spondylolysis and Spondylolisthesis
spondylolisthesis [56]. Two main categories are defined (Table 4.5.3). The first category is defined by primary developmental deficiencies at the lumbo-sacral junction resulting in various degrees of dysplasia. The second cat-egory, acquired spondylolisthesis, is as a result of trau-matic, post-surgical, pathologic or degenerative causes.
The acute traumatic, post-surgical, pathologic and degenerative types of spondylolisthesis are usually recognized as inherently different from the acquired types and treated accordingly. Unfortunately, devel-opmental and spondylolytic (isthmic) spondylolisthe-sis in adolescents and young adults have often been grouped together. As a consequence, the natural his-tories of these processes have been obscured, resulting in confusion over the most appropriate treatment. The two pathologies share a similar initial radiographic
deformity, but the aetiologies and natural histories are clearly different, warranting different clinical expec-tation and subsequent treatment. For example, the natural history of highly dysplastic developmental spondylolisthesis is much more progressive than the acquired spondylolytic variety. A growth deficiency of the antero-superior sacrum may be an important factor in the progression of dysplastic spondylolistheisis.
Clinical Presentation
Most adults with isthmic spondylolisthesis are asymp-tomatic; indeed for patients past the third decade of life, it is unusual for spondylolisthesis to produce pain. Adolescent patients typically present with mechanical LBP with or without radiculopathy. Typically, the L5 nerve root is affected with pain on the outer aspect of the calf, and in extreme cases, with motor weakness of extensor hallucis longus. In the adolescent patient, there are often postural changes with hamstring tight-ness. In extreme cases, patients may present with a cauda equina syndrome.
Spondylolytic spondylolisthesis is almost never associated with central spinal stenosis; in fact, the true antero-posterior diameter of the spinal canal is wid-ened as the posterior elements remain behind [55]. True herniation of the disc at the level of the spon-dylolisthesis is rare. The neural foramen is narrowed by forward shift of L5 on S1, and the reduction in disc height leads to a so-called up-down stenosis.
Degenerative spondylolisthesis is defined as an anterior displacement of one vertebral body on another in the presence of an intact neural arch. This condition may produce LBP as well as radicular or referred pain, and often produces symptoms of neurogenic claudica-tion. The condition is 5–6 times more frequent in women and usually occurs after the age of 40 years. The L4–5 interspace is 6–10 times more frequently involved compared to adjacent levels. The intact neu-ral arch results in spinal stenosis of the central canal. Hypertrophic changes of the facet joints and the disc are common. Degenerative changes in the superior articular process lead to nerve root canal stenosis, whereas those in the inferior articular process lead to central canal stenosis. The dural sac follows the slipped vertebra as it is held tightly by Hofmann’s ligaments.
Table 4.5.2 Wiltse anatomic classification of spondylolisthesis from Wiltse [54] (with permission)
Type Subtypes
I Dysplastic
II Isthmic IIA stress fracture of the parsIIB elongated but intact parsIIC acute fracture of the pars
III Degenerative
IV Post-surgical
V Post-traumatic
VI Pathologic
Table 4.5.3 Marchetti-Bartolozzi etiologic classification of spondylolisthesis from Marchetti et al. [56] (with permission)
Acquired Developmental
Traumatic Acute fractureStress fracture
High dysplastic With lysisWith elongation
Post-surgical DirectIndirect
Low dysplastic With lysisWith elongation
Pathological LocalSystemic
DegenerativePrimarySecondary

142 B. J. C. Freeman and U. K. Debnath
Investigations
Standing antero-posterior and lateral radiographs of the lumbar spine are useful. The role of flexion/exten-sion radiographs remains uncertain. MRI is very use-ful for assessing the degree of neural compromise and the adjacent inter-vertebral discs. Further studies including provocative lumbar discography, selective nerve root blocks, facet blocks and pars blocks may be useful in assessing the sources of pain.
Radiographic Measurements
Meyerding proposed a grading system to describe the amount of forward translation of one vertebra on another [57]. For example, with an L5/S1 spondylolis-thesis, translation of L5 is described relative to the superior surface of S1 as observed on a weight-bearing lateral radiograph of the lumbo-sacral junction. Grade 1 refers to a forward slippage between 1 and 25% (Fig. 4.5.2a), Grade 2 between 26 and 50%, Grade 3 between 51 and 75% and Grade 4 between 76 and 100%. Slippage greater than 100% is called spondy-loptosis. Slips of Grade 1 and 2 are regarded as low-grade slips and slips of Grade 3 or higher are regarded as high-grade slips.
Sacral slope is defined as the angle between the sacral end-plate and the horizontal line and is normally between 40 and 60°. The inter-segmental angulation between L5 and S1 is lordotic with a lumbo-sacral angle ranging from −20 to −30°. The term pelvic inci-dence was introduced by Duval-Beaupére in 1992 [58].
Pelvic incidence is defined as the angle subtended by a line drawn from the centre of the femoral head to the mid-point of the sacral end-plate and a line perpendicu-lar to the centre of the sacral end-plate. The mean value in adults is 53° (range from 34 to 77°). Pelvic tilt is defined as the angle subtended by a vertical reference line originating from the centre of the femoral head and a line drawn from the centre of the femoral head to the mid-point of the sacral end-plate. There is a mathemati-cal relationship between the pelvic incidence, sacral slope and pelvic tilt, in which the pelvic incidence will equal the sum of the sacral slope and pelvic tilt.
A high pelvic incidence results in high shear forces at the lumbo-sacral junction and is associated with a higher degree of slippage. Labelle et al. suggest that pelvic morphology and spino-pelvic balance are abnor-mal in developmental spondylolisthesis and that these abnormalities should be quantified on lateral standing radiographs of the spine and pelvis as they have impor-tant implications for the evaluation and treatment of this pathological condition [59].
The posterior elements clearly play a key role in resisting the high shear forces at the lumbo-sacral junction. The loss of posterior restraint can result in spondylolisthesis. Whilst Hammerberg recognizes that spino-pelvic relationships have a role in the develop-ment and progression of spondylolisthesis, the exact nature is not yet clearly defined [60].
Treatment
Conservative management includes trunk stability, strength training, analgesic medication, epidural steroid
baFig. 4.5.2 (a) Lateral radiograph showing low-grade spondylolytic spondylolisthesis L4/L5 (Meyerding grade I) (From Freeman [65], with permission). (b) Lateral radiograph following instrumented postero-lateral fusion L4/5 combined with decompression. Note incidental partial reduction of slippage (From Freeman [65], with permission)
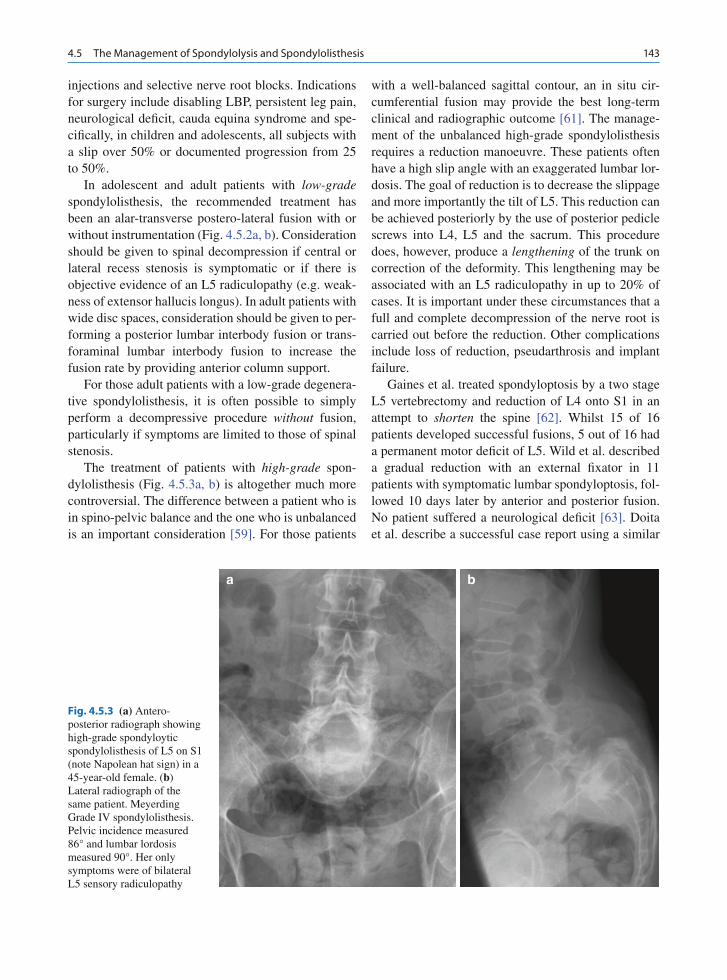
1434.5 The Management of Spondylolysis and Spondylolisthesis
injections and selective nerve root blocks. Indications for surgery include disabling LBP, persistent leg pain, neurological deficit, cauda equina syndrome and spe-cifically, in children and adolescents, all subjects with a slip over 50% or documented progression from 25 to 50%.
In adolescent and adult patients with low-grade spondylolisthesis, the recommended treatment has been an alar-transverse postero-lateral fusion with or without instrumentation (Fig. 4.5.2a, b). Consideration should be given to spinal decompression if central or lateral recess stenosis is symptomatic or if there is objective evidence of an L5 radiculopathy (e.g. weak-ness of extensor hallucis longus). In adult patients with wide disc spaces, consideration should be given to per-forming a posterior lumbar interbody fusion or trans-foraminal lumbar interbody fusion to increase the fusion rate by providing anterior column support.
For those adult patients with a low-grade degenera-tive spondylolisthesis, it is often possible to simply perform a decompressive procedure without fusion, particularly if symptoms are limited to those of spinal stenosis.
The treatment of patients with high-grade spon-dylolisthesis (Fig. 4.5.3a, b) is altogether much more controversial. The difference between a patient who is in spino-pelvic balance and the one who is unbalanced is an important consideration [59]. For those patients
with a well-balanced sagittal contour, an in situ cir-cumferential fusion may provide the best long-term clinical and radiographic outcome [61]. The manage-ment of the unbalanced high-grade spondylolisthesis requires a reduction manoeuvre. These patients often have a high slip angle with an exaggerated lumbar lor-dosis. The goal of reduction is to decrease the slippage and more importantly the tilt of L5. This reduction can be achieved posteriorly by the use of posterior pedicle screws into L4, L5 and the sacrum. This procedure does, however, produce a lengthening of the trunk on correction of the deformity. This lengthening may be associated with an L5 radiculopathy in up to 20% of cases. It is important under these circumstances that a full and complete decompression of the nerve root is carried out before the reduction. Other complications include loss of reduction, pseudarthrosis and implant failure.
Gaines et al. treated spondyloptosis by a two stage L5 vertebrectomy and reduction of L4 onto S1 in an attempt to shorten the spine [62]. Whilst 15 of 16 patients developed successful fusions, 5 out of 16 had a permanent motor deficit of L5. Wild et al. described a gradual reduction with an external fixator in 11 patients with symptomatic lumbar spondyloptosis, fol-lowed 10 days later by anterior and posterior fusion. No patient suffered a neurological deficit [63]. Doita et al. describe a successful case report using a similar
ba
Fig. 4.5.3 (a) Antero-posterior radiograph showing high-grade spondyloytic spondylolisthesis of L5 on S1 (note Napolean hat sign) in a 45-year-old female. (b) Lateral radiograph of the same patient. Meyerding Grade IV spondylolisthesis. Pelvic incidence measured 86° and lumbar lordosis measured 90°. Her only symptoms were of bilateral L5 sensory radiculopathy

144 B. J. C. Freeman and U. K. Debnath
approach with decompression, slow reduction using an Ilizarov external fixator and subsequent interbody fusion, for a patient with lumbo-sacral spondyloptosis [64].
Summary
Spondylolisthesis is a common low back condition with an incidence as high as 6% in Caucasian males. Spondylolisthesis has both developmental and acquired types and occurs as a consequence of the forward cur-vature of the lumbar segments coupled with the disso-ciation of the posterior elements and the vertebral body due to a defect in the PI. A large majority of patients remain asymptomatic. For those patients who become symptomatic with low-grade spondylolisthesis, surgi-cal treatment commonly involves a decompression plus an instrumented postero-lateral fusion in situ. For those patients with high-grade spondylolisthesis, con-troversy surrounds surgical treatment, in particular, whether the deformity should be reduced or not? An assessment of the spino-pelvic balance should assist in this decision making.
References
1. Pedersen AK, Hagen R (1988) Spondylolysis and spon-dylolisthesis: treatment by internal fixation and bone graft-ing of the defect. J Bone Joint Surg [Am] 70:15–24
2. Standaert CJ, Herring SA (2000) Spondylolysis: a critical review. Br J Sports Med 34:415–422
3. Wiltse LL, Widell EH Jr, Jackson DW (1975) Fatigue frac-ture: the basic lesion in isthmic spondylo-listhesis. J Bone Joint Surg [Am] 57:17–22
4. Beutler WJ, Fredrickson BE, Murtland A, Sweeney CA, Grant WD, Baker D (2003) The natural history of spondylol-ysis and spondylolisthesis: 45-year follow-up evaluation. Spine 28:1027–1035
5. Blanda J, Bethem D, Moats W et al (1993) Defects of pars interarticularis in the athlete: a protocol for non-operative treatment. J Spinal Disord 6:406–411
6. Micheli LJ, Wood R (1995) Back pain in young athlete: sig-nificant differences from adults in causes and patterns. Arch Pediatr Adolesc Med 149:15–18
7. Rossi F, Dragoni S (1990) Lumbar spondylolysis: occur-rence in competitive athletes. Updated achievements in a series of 390 cases. J Sports Med Phys Fitness 30:450–452
8. Soler T, Calderon C (2000) The prevalence of spondylolysis in the Spanish elite athlete. Am J Sports Med 28:57–62
9. Ciullo JV, Jackson DW (1985) Pars interarticularis stress reaction, spondylolysis, and spondylolisthesis in gymnasts. Clin Sports Med 4:95–110
10. Kettlekamp DB, Wright DG (1971) Spondylolysis in Alaskan Eskimo. J Bone Joint Surg [Am] 53:563–566
11. Merbs CF (2002) Asymmetrical spondylolysis. Am J Phys Anthropol 119:156–174
12. Sagi HC, Jarviss JG, Uhthoff HK (1998) Histomorphic anal-ysis of the development of the pars interarticularis and its association with isthmic spondylolysis. Spine 1(23): 1635–1639
13. Stinson JT (1993) Spondylolysis and spondylolisthesis in the athlete. Clin Sports Med 12:517–528
14. Fredrickson BE, Baker D, McHolick WJ, Yuan HA, Lubicky JP (1984) The natural history of spondylolysis and spondylolis-thesis. J Bone Joint Surg [Am] 66:699–707
15. Eisenstein SM, Ashton IK, Darby RS, AJ KP, Menage J, Evans H (1994) Innervation of the spondylolysis “ligament”. Spine 15:912–916
16. Schneiderman GA, McLain RF, Hambly MF, Nielsen SL (1995) The pars defect as a pain source. A histologic study. Spine 15:1761–1764
17. Bogduk N (1995) The anatomical basis for spinal pain syn-dromes. J Manipulative Physiol Ther 18:603–605
18. Peng B, Wu W, Hou S, Li P, Zhang C, Yang Y (2005) The pathogenesis of disogenic low back pain. J Bone Joint Surg [Br] 87B:62–67
19. Moreton RD (1966) Spondylolysis. JAMA 195:671–67420. Bellah RD, Summerville DA, Treves ST, Micheli LJ (1991)
Low-back pain in adolescent athletes: detection of stress injury to the pars interarticularis with SPECT. Radiology 180:509–512
21. Collier BD, Johnson RP, Carrera GF, Meyer GA, Schwab JP, Flatley TJ, Isitman AT, Hellman RS, Zielonka JS, Knobel J (1985) Painful spondylolysis or spondylolisthesis studied by radiography and single-photon emission computed tomogra-phy. Radiology 154:207–211
22. Dutton JA, Hughes SP, Peters AM (2000) SPECT in the management of patients with back pain and spondylolysis. Clin Nucl Med 25:93–96
23. Elliott BC (2000) Back injuries and the fast bowler in cricket. J Sports Sci 18:983–991
24. Harvey CJ, Richenberg JL, Saifuddin A, Wolman RL (1998) The radiological investigation of lumbar spondylolysis. Clin Radiol 53:723–728. Review
25. Lusins JO, Elting JJ, Cicoria AD, Goldsmith SJ (1994) SPECT evaluation of lumbar spondylolysis and spondylolis-thesis. Spine 19:608–612
26. Debnath UK, Freeman BJC, Dodaran MS, Kerslake RW, Webb JK (2003) When should SPECT imaging be performed in symptomatic posterior element lumbar stress injuries? Oral presentation British Orthopaedic Association Annual Meeting 2002, Published J Bone Joint Surg [Br] 85-B(Suppl II):168–169
27. Gregory PL, Batt ME, Kerslake RW, Scammell BE, Webb JK (2004) The value of combining SPECT and CT in the inves-tigation of spondylolysis. Eur Spine J 13:503–509
28. Campbell RS, Grainger AJ, Hide IG, Papastefanou S, Greenough CG (2005) Juvenile spondylolysis: a compara-tive analysis of CT, SPECT and MRI. Skeletal Radiol 34: 63–73

1454.5 The Management of Spondylolysis and Spondylolisthesis
29. Saifuddin A, White J, Tucker S, Taylor BA (1998) Orientation of lumbar pars defects: implications for radiological detection and surgical management. J Bone Joint Surg [Br] 80:208–211
30. Udeshi UL, Reeves D (1999) Routine thin slice MRI effec-tively demonstrates the lumbar pars interarticularis. Clin Radiol 54:615–619
31. Hollenberg GM, Beattie PF, Meyers SP, Weinberg EP, Adams MJ (2002) Stress reactions of the lumbar pars inter-articularis: the development of a new MRI classification sys-tem. Spine 27:181–186
32. Steiner ME, Micheli LJ (1985) Treatment of symptomatic spondylolysis and spondylolisthesis with the modified Boston brace. Spine 10:937–943
33. McCleary MD, Congeni JA (2007) Current concepts in the diagnosis and treatment of spondylolysis in young athletes. Curr Sports Med Rep 6:62–66. Review
34. Sys J, Michielsen J, Bracke P, Martens M, Verstreken J (2001) Non-operative treatment of active spondylolysis in elite ath-letes with normal X-ray findings: literature review and results of conservative treatment. Eur Spine J 10:498–504
35. Fuji K, Katoh S, Sairyo K, Ikata T, Yasui N (2004) Union of defects in the pars interarticularis of the lumbar spine in chil-dren and adolescents: the radiological outcome after conser-vative treatment. J Bone Joint Surg [Br] 86:225–231
36. Debnath UK, Freeman BJ, Grevitt MP, Sithole J, Scammell BE, Webb JK (2007) Clinical outcome of symptomatic unilateral stress injuries of the lumbar pars interarticularis. Spine 32:995–1000
37. Standaert CJ, Herring SA (2007) Expert opinion and contro-versies in sports and musculoskeletal medicine: the diagno-sis and treatment of spondylolysis in adolescent athletes. Arch Phys Med Rehabil 88:537–540
38. Suh PB, Esses SI, Kostuik JP (1991) Repair of pars interar-ticularis defect. The prognostic value of pars infiltration. Spine 16:S445–S448
39. Buck JE (1970) Direct repair of the defect in spondylolisthesis – preliminary report. J Bone Joint Surg [Br] 52:432–438
40. Ivanic GM, Pink TP, Achatz W et al (2003) Direct stabiliza-tion of lumbar spondylolysis with a hook-screw. Mean 11-year follow-up period for 113 patients. Spine 28: 255–259
41. Morscher E, Gerber B, Fasel J (1984) Surgical treatment of spondylolisthesis by bone grafting and direct stabilization of spondylolysis by means of a hook screw. Arch Orthop Trauma Surg 103:175–178
42. Nicol RO, Scott JH (1986) Lytic spondylolysis. Repair by wiring. Spine 11(10):1027–1030
43. Gillet P, Petit M (1999) Direct repair of spondylolysis with-out spondylolisthesis, using a rod-screw construct and bone grafting of the pars defect. Spine 24:1252–1256
44. Debnath UK, Freeman BJC, Gregory P, de la Harpe D, Kerslake RW, Webb JK (2003) Clinical outcome and return to sport after the surgical treatment of spondylolysis in young athlete. J Bone Joint Surg [Br] 85:244–249
45. Hardcastle PH (1993) Repair of spondylolysis in young fast bowlers. J Bone Joint Surg [Br] 75:398–402
46. Kakiuchi M (1997) Repair of the defect in spondylolysis. Durable fixation with pedicle screws and laminar hooks. J Bone Joint Surg [Am] 79:818–825
47. Tokuhashi Y, Matsuzaki H (1996) Repair of defects in spon-dylolysis by segmental pedicular screw hook fixation. A pre-liminary report. Spine 21:2041–2045
48. Mihara H, Onari K, Cheung BC (2003) The biomechanical effects of spondylolysis and its treatment. Spine 28: 235–238
49. Deguchi M, Rapoff AJ, Zdeblick TA (1999) Biomechanical comparison of spondylolysis fixation techniques. Spine 24:328–333
50. Kip PC, Esses SI, Doherty BI, Alexander JW, Crawford MJ (1994) Biomechanical testing of pars defect repairs. Spine 19:2692–2697
51. Wu SS, Lee CH, Chen PQ (1999) Operative repair of symp-tomatic spondylolysis following a positive response to diag-nostic pars injection. J Spinal Disord 12:10–16
52. Marnay T (2004) Montpellier, France, Personal communi-cation
53. Herbinaux G (1792) Traite sur divers accouchement laborieux et sur les polypes de la matrice. Bruxells de Boubers
54. Wiltse LL (1962) Etiology of spondylolisthesis. J Bone Joint Surg [A] 44:539–559
55. Wiltse LL (1969) Spondylolisthesis: Classification and Etiology in: Symposium on the spine, The American Academy of Orthopaedic Surgeons The C.V. Mosby Co, St. Louis, pp 143–168
56. Marchetti PG, Bartolozzi P (1997) Classification of Spondylolisthesis as a guideline for Treatment. In: Bridwell K.H and Dewald R.L (Eds) The Textbook of Spinal Surgery, 2nd Edn. Lippincott-Raven, Philadelphia, pp 1211–1254
57. Meyerding HW (1931) Spondylolisthesis. J Bone Joint Surg 13:39–43
58. Duval-Beaupére G, Schmidt C, Cosson P (1992) A barycen-tremetric study of the sagittal shape of the spine and pelvis: the conditions required for an economic standing position. Ann Biomed Eng 20:451–462
59. Labelle H, Roussouly P, Bérthonnaud E et al (2005) The importance of spino-pelvic balance in L5–S1 developmental spondylolisthesis: a review of pertinent radiologic measure-ments. Spine 30:S27–S34
60. Hammerberg KW (2005) New concepts on the pathogenesis and classification of spondylolisthesis. Spine 30:S4–S11
61. Helenius I, Lamberg T, Österman K (2006) Postero-lateral, anterior or circumferential fusion in situ for high-grade spon-dylolisthesis in young patients: a long-term evaluation using the Scoliosis Research Society questionnaire. Spine 31:190–196
62. Gaines R, Nichols W (1985) Treatment of spondyloptosis by two-stage L5 vertebrectomy and reduction of L4 onto S1. Spine 10:680–686
63. Wild A, Jäger M, Webb JK (2001) Staged reposition and fusion with external fixator in spondyloptosis. Z Orthop Ihre Grenzgeb 139:152–156
64. Doita M, Uno K, Maeno K et al (2008) Two-stage decom-pression, reduction and interbody fusion for lumbo-sacral spondyloptosis through a posterior approach using Ilizarov external fixation. J Neurosurg (Spine) 8:186–192
65. Freeman BJC (2005) The spine and spinal cord. In: Burnand KG (ed) The New Aird’s Companion in Surgical Studies, 3rd edn. Elsevier–Churchill Livingstone, China, pp 1014–1029

147M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_4.6, © Springer-Verlag Berlin Heidelberg 2010
Introduction
Transsacral-transcorporal fixation has long been estab-lished mostly as anterior procedure with a fibular strut or direct screw fixation. René Louis in France and Marchetti in Italy have used this technique mostly in spondylolisthesis of L5/S1 [1, 2]. Either by a primarily posterior approach or by an anterior approach alone, they reduced the spondylolisthesis and fixed the lum-bosacral junction with one or two screws, which are introduced in the midline from the anterior superior border of L5, obliquely down through the vertebral body of L5 and the disk space L5/S1, into the body of S1. The disk space L5/S1 has been fused with a tricor-tical bone graft. As an alternative, this technique has been used also together with a fibular strut. In this case, a K-wire has been positioned in the direction as described for the screw above, and a cannulated, large drill has been used to create a drill-hole, which could accept a fibular strut. Henry Bohlman and others have used the same principle of lumbosacral fixation, but through a posterior approach [3–8]. They prepared the midline of the spinal canal at the sacral level and drilled a hole from there obliquely up through the body of S1 through the disk space of L5/S1 into the body of L5, where a fibular strut could be positioned. There is obvi-ously the risk that this strut can move back and would in this case compress the dural sac at the sacral level.
As for the anterior approach, transabdominal as well as retroperitoneal approaches have been used with the established risks of injuries to the abdominal content or
the big vessels in the area of the bifurcation of the aorta as well as the vena cava. Very few are known about possible complications by introducing a screw, respec-tively a K-wire, from the front in the neighborhood of the peritoneum as well as the big vessels, which may get into conflict with a screw or a K-wire.
Several authors in the last years have presented fixation techniques at the lumbosacral junction by a posterior approach, while using the pedicle for the transfixation of the lumbosacral junction. Grob has published a series of cases with a direct screw fixation through the pedicles of S1, the disk space, and the ver-tebral body of L5 for spondylolysis or spondylolis-thesis [9]. Bradford, Bartoluzzi, and others have used this transpedical-transdiscal-transcorporal fixation for pedicle screws in the context of major fixation con-structs for the lumbosacral junction, inclusive of defor-mities of the lumbar and thoracic spine [3, 4, 8, 10].
The pedicle has long been used and understood as an access to the anterior vertebral body, and the idea that there is just one direction of positioning a screw in a pedicle has long been challenged by other tech-nologies like transpedicular biopsies, transpedicular treatment of infections with irrigation systems, trans-pedicular bone grafting, as well as the whole concept of the vertebroplasty [11–22]. A pedicle screw cannot only vary its direction in the horizontal plane, meaning the screw can be more medialized or more lateralized, but the screw can also be varied in the direction of the sagittal plane, meaning that the screw can be guided upward cranially or downward caudally. Specifically, when the screw is introduced in the sagittal plane with an oblique upward direction, in case of a spondylolis-thesis with a gliding of the superior vertebral body relative to the body below, a screw can easily traverse the intervertebral space and find good fixation in the vertebral body above, guaranteeing a sufficient fixation
Transpedicular-Transdiscal-Transcorporal (TPDC)-Fixation
Max Aebi
M. Aebi Center for Orthopaedic Research, University of Bern, Stauffenbachstrasse 78, 3014, Bern, Switzerland e-mail: [email protected]
4.6

148 M. Aebi
in situ of the lumbosacral junction. Equally, this tech-nique can be applied in mostly degenerative spon-dylolisthesis of L4 over L5 or L3 over L4 in case there is a clear gliding of the superior vis-à-vis the inferior vertebral body, which guarantees that the screw enters into the superior vertebral body, once traversed the intervertebral space, not just in the anterior part of the vertebral body, but basically in the center allowing a sufficiently long path in the superior vertebral body.
It also needs to be mentioned that Marchetti has used not only one screw from the front to fix the lum-bosacral junction, but two parallel screws, thereby positioning a screw each in the left and the right half of the vertebral body [2].
We have used a transpedicular-transdiscal-transcor-poral fixation-technique for the lumbosacral junction since the midnineties. We used this technique first in combination with a posterior pedicle fixation from L5 to S1 or from L4 to S1. In these cases, we put regular screws in the pedicle L5 and/or L4 and used the pedicle screw S1 as a transpedicular-transdiscal-transcorporal screw. In case of a pedicle fixation of the pedicle L5 as well as S1, we called this construct a delta-fixation (Fig. 4.6.1). Later, we started to use transpedicular-transdiscal-transcorporal screws alone without a rod-pedicle-screw-construct in cases where a purely in situ fixation of a spondylolisthesis was indicated and where specifically the disk space was narrowed (Fig. 4.6.2). For this case, we introduced cannulated 7.3 mm tita-nium cancellous short threaded screws, which were introduced over primarily set K-wires.
Indication and Surgical Techniques
The indication for a screw fixation only through a transpedicular-transdiscal-transcorporal fixation is a spondylolisthesis of at least grade I with a preferen-tially mostly collapsed intervertebral disk at the level of L5/S1. However, also L4/5 and L3/4 in degenerative spondylolisthesis can be approached in this way. The primary purpose of this fixation is an in situ-fixation and it is not the goal to reduce the spondylolisthesis, since if this is done, the screw fixation will not work. The path that is created in the transcorporal portion of the screw fixation is too short in a case where there is not at least a listhesis of grade I. In most adult patients with longstanding spondylolisthesis and a secondarily degenerated disk at this level, a reduction is not neces-sary. This surgery technique is an alternative to a more complex and more expensive technique, when using a posterior pedicle system in combination with a reduc-tion and intervertebral cages to maintain or restore the intervertebral height at the lumbosacral junction. Such procedures may allow the restoration of the anatomical constellation at the lumbosacral junction. However, the outcome has not been proven to be better than a simple in situ-fusion, which has been practiced for many decades without internal fixation [23]. To put two transpedicular-transdiscal-transcorporal screws adds additional stability in a simple procedure to an in situ-fusion.
The procedure can be done with a minimal expo-sure, including the opening of the spinal canal at the
Fig. 4.6.1 Delta fixation

1494.6 Transpedicular-Transdiscal-Transcorporal (TPDC)-Fixation
respective level to decompress the neurostructures, specifically in spondylolisthesis combined with spon-dylolysis and secondary hypertrophic nonunion and capsule tissue compromising the exit of the nerve roots in the foramen L5/S1 in case of a lumbosacral spon-dylolisthesis. This fixation is like a so-called “circum-ferential fixation,” since the transdiscal/transcorporal screws stabilize the anterior column and the trans-pedicular portion of the screw has its beginning in the posterior elements adding posterolateral fusion. In case of a significant instability at the level of the fixation, an additional stabilization, specifically if reduction is
done, can be achieved with a pedicle screw-rod- fixation as a frame (delta fixation) (Fig. 4.6.1).
In case the disk space is completely destroyed and the vertebral body is basically sitting on the vertebral body or the sacrum below without any relevant disk material in between and with even some destructions of the end-plate, the screws may also act as compres-sion-screws (short threaded cancellous screws). Care has to be taken, however, when adding compression, not to obstruct the foraminal exit for the roots, since compression leads to shortening, and therefore, sagit-tal decrease of the foraminal diameter.
Fig. 4.6.2 Thirty-nine–years-old female patient, back and root pain: Decompression and fixation and fusion

150 M. Aebi
Fig. 4.6.3 Secondarily degenerated spondylolisthesis L5/S1 and spondylodesis (a) preop-imaging (b) CT - myelogram showing displacement of the tools S1 + L5 (c) postop-imaging
a
b
c

1514.6 Transpedicular-Transdiscal-Transcorporal (TPDC)-Fixation
The following are the two surgical techniques which can be used:
1. Screw-only fixation, either with two screws or three screws (Fig. 4.6.3 and 4.6.4):
The two-screw-fixation is a purely transpedicular-trans-discal-transcorporal fixation by introducing the screws over a K-wire into the pedicle S1, slightly oblique, upward and directed toward the midline (Fig. 4.6.2). The screws in a spondylolisthesis and in the usually present hypolordotic position can be introduced almost perpen-dicular to the table, what will end in an oblique tra-verse of the disk space. If the patient is in prone position and the lumbar spine is maintained in a more or less physiological alignment for this specific patient, the disk space L5/S1 or L4/5 is usually directed obliquely from cranial posterior to caudal anterior in relation to a perpendicular line to the table. This means that if a screw is positioned in a perpendicular line or slightly upward toward the head, this screw will traverse the disk space in an oblique fashion.
Together with these two pedicle screws, an addi-tional third screw can be introduced through the midline of the sacrum obliquely upward, identical as the pedicle screws (Fig. 4.6.4). For this purpose, the dural sac of the sacrum at the level of S1 needs to be uncovered and mobilized to the side, so the midline of the spinal canal in the sacrum anteriorly can be identified and a drill-hole prepared to take up a screw starting at the posterior wall of the sacrum in the sacral spinal canal. This may add additional stability to the lumbosacral fixation.
2. The so-called delta-fixation:
The delta-fixation is a transpedicular-transdiscal-trans corporal screw-fixation where this screw is part
of a pedicular rod-system. The transpedicular- transdiscal-transcorporal screw is used as the inferior anchorage of a construct, linking a transpedicular screw in L5 and/or L4 with a rod (Fig. 4.6.1). This is a very strong fixation that has been tested under experi-mental conditions in the laboratory [24]. From these tests, it could be assumed that a simple screw fixation through the pedicles is sufficient in low instability segments and in converting posteriorly the concept of the anterior transpedicular-transdiscal-transcorporal fixation, which has been practiced in many hundred cases and does not use the pedicle as a fixation-path, but the cancellous bone of the vertebral bodies, which adds more stability to a screw. There have also been constructs proposed, where a regular pedicle fixation in the sacrum and in the above lying vertebral bodies has been used and connected by rods, and in addition to this frame-type-fixation, a transsacral-transdiscal-transcorporal fixation from the back has been added.
For the regular screw fixation with screws only, we have used in the past the cannulated 7.3 mm short threaded cancellous titanium screws (Synthes), which are introduced over a preset K-wire (Fig. 4.6.5). These screws are self-cutting; however, if the subchondral bone at the end plate, specifically of S1 but also at L5, is sclerosized, it is recommended to drill with the can-nulated drill over the K-wire, at least through both end plates. If the bone, specifically of the L5 subchondral area, is very hard, the self-cutting screw may push the vertebral body anteriorly and increase the interverte-bral space, which had naturally collapsed before through the degeneration of the disk. This distraction of the degenerated disk space is not wanted, since it creates a much higher stress on the screws if there is no anterior column support in the intervertebral space.
Fig. 4.6.4 Thirty-three-years-old female patient with previous posterior decom-pression and posterior fixation with VAS and consecutive screw breakage and nonunion

152 M. Aebi
Ideally, the fixation must be an in-situ-fixation. Once the K-wire is positioned in a good direction, it is easy to introduce the cannulated screws, which can be used with or without the washer to resist sinking of the heads over the pedicle of S1 or the vertebrae above (see Fig. 4.6.4).
The utilization of the K-wire bares some risks. It can perforate the anterior wall of the vertebral body and injure the vessels in front of it. The perforation can happen while drilling the K-wire into the verte-bral body of L5 or when introducing the screw, which may push the K-wire forward. Therefore, the intro-duction of the K-wire is achieved with continuous control through a lateral view of an image intensifier. The a/p-projection of the image intensifier is usually not used because most tables available do not allow a good quality image when images are done through the patient and the table. Furthermore, there are more precise ways to control the direction of the K-wire, respectively the screw, in the frontal and hor-izontal plane. For this purpose, in the context of the decompressive surgery, the pedicle S1 or the respec-tive pedicle is identified precisely in its whole con-tour from the inner side, and the K-wire is angulated from the outside toward the inside into this visible pedicle, guaranteeing that the screw is heading toward the midline of the spine. At the same time, the pedi-cle can also be observed that it is not perforated cra-nially, which means that the screw or the K-wire is exiting too early and using space of the foramen L5/S1. The introduction of the K-wire, respectively the screw, under the vision of the pedicle in which the
screw or K-wire is introduced, is more precise than an insufficient X-ray.
Once the screw fixation is done, a regular posterolat-eral spondylodesis of L5/S1, respectively of the fixed segment, is achieved. We do that usually with the bone, which has been removed through the decompression and has been milled in small corticocancellous chips, which are combined with tricalciumphosphate granula (Chronos®) to enhance the fusion mass.
Results
We have used this technique until the end of 2005 in more than thirty-six patients. Screws only have been used in twenty-four patients. Out of these twenty-four, in three patients we used three screws, meaning two transpedicular screws plus a screw in the median posi-tion. In twelve patients, we have used a delta-fixation, where the transpedicular-transdiscal screw has been combined with a rod-pedicle-system for the body(s) above. We have used transpedicular-transdiscal-transcorporal screws 29 times at the level of L5/S1, 5 times at the level of L4/5, and twice at the level of L3/4. The average age of our patients was 44 years (13–67). The ratio between male and female patients was 21/15. There were complications, which were related directly to the screw, respectively K-wire intro-duction and more general complications. There was one deep femoral vein thrombosis in one case. There was one early infection after disconnection of the Hemovac-drain, which was unrecognized. Due to an image intensifier failure, there was one death because of a K-wire, which perforated the anterior L3 vertebral body wall unobserved in a fixation of a degenerative spondylolisthesis case at the level of L3/4 and dam-aged the vena cava with a consecutive rapid massive retroperitoneal noncontrolled bleeding.
The infection has been controlled with wound deb-ridement, irrigation, and antibiotics, and has healed without any residual consequences. There was one screw-breakage with a proven nonunion and there was another screw-breakage in a patient, who was pain-free. In one case, there was a L4 root-weakness, which was not due to an irritation through the screw or K-wire, but possibly through a narrowing of the foramen by the compressive effect of the cancellous short-threaded screws. There were sensory disturbances in the S1 root
Fig. 4.6.5 Cannulated 7.3 mm titanium cancellous short thread screws

1534.6 Transpedicular-Transdiscal-Transcorporal (TPDC)-Fixation
in a case, where a third median screw had been inserted. This screw has been removed and the sensory distur-bances have almost completely recovered. Another patient had a L5-sensory disturbance with hyperes-thetic sensations. There was no intraspinal or intrafo-raminal reason for this L5-root-symptomatology; however, the screw perforated the lateral wall of L5, although in the CT there was no direct contact between screw and the root. The screw has been removed and repositioned and the patient has gradually recovered from this sensory disturbance. The reason for this sen-sory disturbance is unexplained and may be due to irri-tation of some sympathetic or parasympathetic nerve fibers extravertebral.
The overall satisfaction of the patients was more than 80% and the functional status allowed 28 patients to go back to their work or school. One patient is retired and five patients are on workman’s compensation. Out of them, three were patients with a delta-fixation. Concerning pain, at least 1 year postoperatively, one patient was unchanged and twenty-two patients had a significant better VAS. Twenty-one patients who have been treated with screws only and eight out of twelve patients with a delta fixation had a significantly better VAS than preoperatively.
Discussion
The transpedicular-transdiscal-transcorporal screw fixation is an alternative stabilization technique for a uniseg-mental fusion in cases with a spondylolisthesis of at least grade I, when the purpose is basically fixation in situ, but also in combination with a unisegmental or longer pedicle screw-rod fixation. Through the transla-tion anteriorly, the path of a screw through the disk space from the vertebra below to the vertebra above is lengthened, thereby allowing sufficient anchorage of the screw in the vertebra below and the vertebra above. In opposite to the anterior screw fixation of a spon-dylolisthesis or a fixation with a fibular strut, the anchor-age of the fixation is partially in the pedicle, which is a better bed for a screw fixation, therefore undoubtedly enhancing stability. This fixation-technique is not appropriate in a highly unstable spondylolisthesis, but in patients where an in-situ-fixation may enhance fusion. In more unstable conditions, it is recommended to combine this screw-fixation with a classical posterior
rod-screw-fixation. Nevertheless, the screw, which tra-verses the discal space, allows an anterior column fixa-tion. The experience up to now has demonstrated essentially four issues, which need to be considered carefully while doing this surgery.
1. Disk space distraction must be avoided while insert-ing the screws over the K wires. The end plates may be sclerosized to a degree that even the self-cutting screw may push the vertebral body in front of the tip instead of biting through. Therefore, it is recom-mended to drill the end plates of the two adjacent vertebraes. The K-wire as guide for the screw has two inherent risks. The insertion of the screw over the K-wire may push it anteriorly, if there is a small angulation between the K-wire and the cannulated screws. The K-wire may perforate in front and injure a vessel. Also, the insertion of the K-wire has the risk to perforate the anterior cortex and injure the adjacent, specifically veins with fatal consequences, as demonstrated in one case. The danger is that the K-wire may wrap the vessel, when inserted with a drill. To minimize this risk, we recommend that while using a K-wire, it should be tapped carefully once it is in the vertebral body and has passed the end-plates. Due to the fatal complication in one case, we try whenever possible not to use a K-wire any-more, but to open the pedicle as usual with an awl and to perforate the end-plates equally with the awl.
2. The image intensifier needs to be used in the lateral projection. However, the a/p-projection can better be controlled by identifying under direct vision the medial wall of the pedicle S1 in case of a S1/L5 screw fixation with an instrument and angulating the direction of the awl or K-wire at least 15° toward the midline. Through the identification of the pedi-cle, we make sure that the screw does not perforate the pedicle medially or cranially and yet converges to the midline.
3. The screw may break, specifically if the disk space is wide and there is a relevant bending moment on the screw. The screw has the tendency to break close to the transition from the threaded part to the shaft of the screw. To avoid this problem, regular 7 mm pedicle screws out of the pedicle system can be used equally and since they are fully threaded, they avoid compression between the two vertebral bodies.
4. The compression of two vertebral bodies against each other through a compression-screw-concept

154 M. Aebi
(short threaded cancellous screw) may lead to a nar-rowing of the root canal or the foraminal exit in the sagittal plain with secondary irritation of the root L5 in case of a fixation of S1/L5. When a screw fixation has been achieved, it is recommended to explore the foramen with an appropriate instrument to make sure that the space is sufficient for the root.
This technique offers, in most cases, a sufficient fixa-tion to enhance fusion in situ in case of spondylolisthe-sis, but for significantly less costs than a regular pedicular system with rod connections.
References
1. Louis R, Maresca C (1976) Les arthrodèses stables de la charnière lombosacrée (70 cas). Rev Chir Orthop (Suppl 2): 70–79
2. Marchetti PG, Binazzi R, Briccoli A, Vaccari V, Borelli P, De Zerbi M, Manca A, Landi S (1994) The surgical treat-ment of spondylolisthesis. Chir Organi Mov 79(1):85–91
3. Bartolozzi P, Sandri A, Cassini M, Ricci M (2003) One-stage posterior decompression-stabilization and trans-sacral Interbody fusion after partial reduction for severe L5–S1 spondylolisthesis. Spine 28(11):1135–1141
4. Boachi-Adjei O, Do T, Rawlins BA (2002) Partial lum-bosacral kyphosis, reduction, decompression and posterior lumbosacral transfixation in high grade isthmic spondylolis-thesis: clinical and radiographic results in six patients. Spine 27(6):E161–E168
5. Bohlmann HH, Cook SS (1982) One-stage decompression and posterolateral and interbody fusion for lumbosacral spondyloptosis through a posterior approach. Report on two cases. J Bone Joint Surg Am 64:415–418
6. Hanson DS, Bridwell KH, Rhee JM, Lenke LG (2002) Dowel fibular strut grafts for high-grade dysplastic isthmic spondylosisthesis. Spine 27(18):1982–1988
7. Smith MD, Bohlmann HH (1990) Spondylolisthesis treated by a single-stage operation combining decompression with in situ posterolateral and anterior fusion. An analysis of eleven patients who had long-term follow-up. J. Bone Joint Surg Am 72(3):415–421
8. Smith JA, Deviren V, Berven S, Kleinstueck F, Bradford DS (2001) Clinical outcome of trans-sacral interbody fusion after partial reduction for high grade L5/S1 spondylolisthe-sis. Spine 26(20):227–2234
9. Grob D, Humke T, Dvorak J (1996) Direct pediculo-body fixation in cases of spondylolisthesis with advanced inter-vertebral disc degeneration. Eur Spine J 5(4):281–285
10. Hu SS, Bradford DS, Transfeldt EE, Cohen M (1996) Reduction of high-grade spondylolisthesis using Edwards instrumentation. Spine 21(3):367–371
11. Crow WN, Borowski AM, Hadjipavlou AG, Walser EM et al (1998) Percutaneous transpedicular automated nucleotomy for debridement of infected discs. J Vasc Interv Radiol 9:161–165
12. Daniaux H, Seykora P, Genelin A, Lang T, Kathrein A (1991) Application of posterior plating and modifications in thoracolumbar spine injuries. Indication, techniques and results. Spine 16(Suppl 3):S125–S133
13. Hadjipavlou AG, Arya S, Crow WN et al (1996) Percutaneous transpedicular biopsy of the spine. J Interv Radiol 11: 103–108
14. Hadjipavlou AG, Crow WN, Borowski A, Mader JP, Adesokan A, Jensen RE (1998) Percutaneous transpedicular discectomy and drainage in pyogenic spondylodiscitis. Am J Orth 27:188–197
15. Hadjipavlou AG, Katonis PK, Gaitanis IN, Muffoletto AJ, Tzermiadianos MN, Crow W (2004) Percutaneous trans-pedicular discectomy and drainage in pyogenic spondylodis-citis. Eur Spine J 13:707–713
16. Heini PF, Orler R (2004) Kyphoplasty for treatment of osteoporotic vertebral fractures. Eur Spine J 13(3):184–192
17. Jelinek JS, Kransdorf MJ, Gray R et al (1996) Percutaneous transpedicular biopsy of vertebral body lesions. Spine 21(17): 2035–2040
18. Kaya RA, Aydin Y (2004) Modified transpedicular approach for the surgical treatment of severe thoracolumbar or lumbar burst fractures. Spine J 4(2):208–217
19. Leferink VJM, Zimmermann KW, Veldhuis EFM, tenVerg-ert EM, tenDuis HJ (2001) Thoracolumbar spinal fractures: radiological results of transpedicular fixation combined with transpedicular cancellous bone graft and posterior fusion in 183 patients. Eur Spine J 10(6):517–523
20. Murrey DB, Brigham CD, Kiebzak GM, Finger F, Chewning SJ (2002) Transpedicular decompression and pedicle subtraction osteotomy (eggshell procedure): a retro-spective review of 59 patients. Spine 27(21):2338–2345
21. Stringham DR, Hadjipavlou A, Dzioba RB, Lander P (1994) Percutaneous transpedicular biopsy of the spine. Spine 19: 1985–1991
22. Ward JC, Jeanneret B, Oehlschlegel C, Magerl F (1996) The value of percutaneous transpedicular vertebral bone biopsies for histologic examination. Results of an experimental histo-pathologic study comparing two biopsy needles. Spine 21(21):2484–2490
23. Kuntz KM, Snider RK, Weinstein JN, Pope MH, Katz JN (2000) Cost-effectiveness of fusion with and without instru-mentation for patients with degenerative spondylolisthesis and spinal stenosis. Spine 24(9):1132–1139
24. Steffen T (2004) Unpublished Data from the Orthopaedic Research Lab, McGill University, Montreal, Canada: Personal Communication
155M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_4.7, © Springer-Verlag Berlin Heidelberg 2010
The apophyseal facet joints are diarthrodial joints located in the posterior aspect of the functional spinal unit. Together with the intervertebral disc, they consti-tute a three-joint complex providing motion, stability and protection to the neural structures. Facet problems are often a surgical indication, mainly after acute trauma with facet dislocation. However, in the absence of “red flags”, the surgical indications are less clear [1]. Historically, degenerated lumbar facet joints have been implicated in low back pain (LBP) syndromes [3, 4].
Facet Joint Degeneration
As occurs with any other synovial joint, facets undergo degenerative changes that are characteristic of osteo-arthritis [12]. According to Kirkaldy-Willis, these changes appear simultaneously in the facets and inter-vertebral disc, progressively modifying the morphol-ogy of the functional spine unit [14]. However, the degenerative process is not necessarily a pathological process, since degeneration of the spine is almost uni-versal in the asymptomatic adult population [5]. The morphological changes occurring at the zygapophy-seal lumbar facet joints during degeneration have been described using various imaging techniques, such as plain radiography, computed tomography (CT) and magnetic resonance imaging (MRI). In addition, many systems to grade lumbar facet joint degeneration are accessible from the MEDLINE database. A recent
review of existing grading systems concludes that morphological changes occurring during the degenera-tion of the lumbar facet joints are better evaluated and graded with CT and MRI [12]. Among more than 12 reported grading systems, only three met acceptable criteria for reliability that was recommended. The Weishaupt system provides the best intra- and inter-observer reliability [12]. Although the clinical signifi-cance of facet joint degeneration is still under debate, facets are often related to back pain and radicular symptoms.
Low Back Pain
A large part of the adult population will have LBP at some stage in life. In a great majority of cases, the pain source cannot be identified [1].
Diagnosis
For some authors, lumbar facet joint deterioration is a significant contributor to LBP [18]. The prevalence of facet joint pain varies considerably according to the diagnostic procedure used. Its prevalence as a cause of LBP has been reported to range from 7.7 to 75% using single facet joint diagnostic anaesthesia, and from 15 to 40% using double facet joint anaesthesia and saline injections as control [18]. Jackson et al (1988 Volvo Award in Clinical Sciences) evaluated 454 patients with facet joint injections [11]. All had the chief com-plaint of LBP, normal neurological examinations and no signs of root tension. Three hundred and ninety completed the protocol, which included lumbar motion
Facet Problems: A Surgical Indication?
F. Pellisé
F. Pellisé Unitat de Cirugia del Raquis Vall d’Hebron, Hospital Vall d’Hebron, Barcelona, Vall d’Hebron 119–129, 08035 Barcelona, Spain e-mail: [email protected]
4.7

156 F. Pellisé
pain assessment before and after facet injection. A total of 127 variables were studied. There were 229 males and 161 females with a median age of 38. Facet joint arthrograms were performed prior to intra-articular injection of a local anaesthetic and cortisone. Initial mean pain relief was only 29%. Variables correlating significantly with greater post-injection pain relief were older age, prior history of LBP, normal gait, maximum pain on extension following forward flexion in the standing position, an absence of leg pain, muscle spasm and aggravation of pain on Valsalva. The greatest pain relief immediately after injection was seen with lumbar extension and rotation, movements reported to stress the facet joints or aggravate pain of facet joint origin. Patients with greater pain on lumbar extension and rotation as a group, however, did not experience more pain relief. From the results of this study, the authors were not able to identify clinical facet joint syndromes or predict patients responding better to this procedure. They concluded that the facet joints were not com-monly the single or primary source of LBP in the great majority (more than 90%) of patients studied [11].
Diagnosis based on double anaesthesia and saline control injections is an expensive and time-consuming procedure. However, there is no single clinical param-eter indicating that LBP results from facet joints. To determine clinical criteria that could identify patients with painful facet joints, Revel et al designed a pro-spective randomized study to compare the efficacy of facet joint injection with lidocaine or saline in two groups of patients with LBP, with and without clinical criteria that were determined in a previous study to implicate the facet joint as the primary source of pain [18]. A group of 43 patients with LBP who met at least five criteria were compared with 37 patients who met fewer criteria. Patients randomly received an injection of either lidocaine or saline into the lower facet joints. The result was considered positive if more than 75% pain relief was determined by a visual analogue scale. The patient, the radiologist and the investigator were blinded. There was a significant interaction between clinical group and injection effect (p > 0.003). The presence of five of seven variables (age greater than 65 years and pain that is not exacerbated by coughing, hyperextension, forward flexion, rising from flexion or extension-rotation and well-relieved by recumbence), always including the last item, distinguished 92% of patients responding to lidocaine injection and 80% of non-responders in the lidocaine group [18].
In a recent study, Hancock et al carried out a system-atic review of tests to identify the disc, sacroiliac joint or facet joint as the source of LBP [10]. The authors retrieved eight studies of moderate quality dealing with diagnostic testing for facet joint pain. The index tests were considered informative when positive likelihood ratios were >2 and/or negative likelihood ratios <0.5, and confidence intervals did not include one. The authors concluded that the two studies by Revel et al found informative positive likelihood ratios and negative like-lihood ratios for Revel’s criteria. However, two other studies failed to find informative positive likelihood ratios or negative likelihood ratios. None of the seven individual items that make up Revel’s criteria were found to have informative positive likelihood ratios by more than one study [10]. In fact, none of the diagnos-tic tests for the facet joint appear to be informative.
Facet Joint Denervation
When the concept of facet joint block as a diagnostic test was developed, the natural progression was to explore facet joint denervation procedures in the hope of providing longer-lasting and perhaps permanent relief of facet joint pain [8]. Since the first article on radiofrequency denervation in 1975 [19], the technique has been increasingly used and popularized as the treat-ment of choice for LBP of facet origin. The rationale for neurotomy is based on the premise that cutting the nerve supply to a painful structure may alleviate pain and permit a return of function. The major afferent nerve supply to the facet joint is provided by the medial branch of the posterior primary ramus. Following a “dual innervation” pattern, the medial branch supplies its adjacent facet and the joint immediately below. There is agreement throughout the literature that the medial branch of the posterior primary ramus is con-stant and is fixed adjacent to the bone in the region of the mamillo-accessory ligament. There is no evidence of nerve fibres crossing the midline; hence, the facet joints on each side have unilateral innervation [9].
There are two pre-requisites for the success of this therapy. First, the structure responsible for the pain at or near the articular facet joints must be identified by using a diagnostic block. Second, the precise location and section of the nerve supply to that joint must be identi-fied [15]. Many non-controlled observational studies of

1574.7 Facet Problems: A Surgical Indication?
patients whose LBP was treated with facet joint radiof-requency denervation have reported improvement, as assessed subjectively by the patient or physician. Improvement of 60–80% has been reported in studies excluding patients with previous back surgery and approximately 40% in studies including these patients. Facet nerve blocks have been shown to have a very high placebo effect. A recent Cochrane systematic review assessed the effectiveness of radiofrequency denerva-tion for the treatment of musculoskeletal pain disorders [17]. Of seven relevant randomized controlled trials, three examined lumbar zygapophyseal joint pain; two were considered to be high-quality [15, 20] and one low-quality [7]. All studies had short follow-up (2, 3 and 6 months). Radiofrequency denervation had a posi-tive short-term effect in one high-quality study, but a neutral effect in the other high-quality study. The results of the low-quality study remained unclear because the authors did not include an intention-to-treat analysis. Therefore, the reviewers concluded that the evidence of a short-term effect was conflictive [17]. However, for those favouring the technique, the greatest design flaw of these trials is the weakness of the diagnostic and inclusion criteria [6].
Radicular Pain
The close proximity of facet joints to the nerve root canal makes their degeneration, which leads to facet enlargement or malalignment, an important factor con-tributing to spinal stenosis.
Lumbar Spinal Stenosis and Degenerative Spondylolisthesis
According to non-randomized studies, patients with nar-rowing of the lumbar vertebral canal and concurrent neurogenic claudication with persistent severe pain and progressive neural dysfunction benefit from decompres-sive surgery, but may experiment slow deterioration over time [2]. The first randomized control trial assessing the effectiveness of surgery as compared to conservative treatment involved 94 patients from four university hos-pitals in Finland [16]. The study showed better outcomes after surgical treatment. Patients were randomized into a
surgical (50 patients) or non-surgical (44 patients) group. Surgery consisted of segmental decompression and an undercutting facetectomy of the affected area. The pres-ence or risk of lumbar instability was, at the surgeon’s discretion, treated by fusion augmented by transpedicu-lar instrumentation when necessary. Lumbar fusion, in all cases augmented with instrumentation, was added in ten patients. In the non-operative group, the patient was prescribed non- steroidal anti-inflammatory drugs and referred to a physiotherapist. Both treatment groups showed improvement during follow-up. At 1 year, the mean difference in favour of surgery was 11.3 in dis-ability (ODI), 1.7 in leg pain (0–10 NRS) and 2.3 in back pain (0–10 NRS). At the 2-year follow-up, the mean differences were slightly smaller: 7.8 in disability, 1.5 in leg pain and 2.1 in back pain. Walking ability, either reported or measured, did not differ between the two treatment options. As pointed out by the authors, longer follow-up is needed to determine if these differ-ences favouring surgery persist over time [16].
Degenerative spondylolisthesis is the slipping for-ward of one vertebra on another, with an intact neural arch. In degenerative spondylolisthesis the zygapophy-seal facet joints are at the origin of the problem and lose normal alignment. Due to facet subluxation, there might be a narrowing of the spinal canal with encroachment on the neural structures. When radicular symptoms or neurogenic claudication persist, surgery provides better outcomes than conservative treatment, as was shown in the SPORT trial [21]. The study included 304 patients in a randomized cohort and 303 in an observational cohort. Surgery consisted of standard posterior decom-pressive laminectomy with or without bilateral single-level fusion (iliac crest bone grafting with or without posterior pedicle-screw instrumentation. The non-surgical protocol was standard care, recommended to include at least active physical therapy, education or counsel-ling, including instructions for exercising at home, and non-steroidal anti-inflammatory agents, if tolerated. The 1-year crossover rates were very high in the ran-domized cohort (40% in each direction), but moderate in the observational cohort. The intention-to-treat analysis for the randomized cohort did not show statis-tically significant effects for the primary outcomes (SF-36 bodily and physical function scales, modified ODI). However, the as-treated analysis for both cohorts combined showed a significant advantage for surgery at three months that increased at 1 year and diminished only slightly at 2 years.

158 F. Pellisé
Synovial Cysts
Facet joint enlargement due to a synovial cyst with or without haemorrhage may be asymptomatic and found incidentally, or cause symptomatic compression of the neural structures and be the origin of radicular symp-toms [13]. Most patients with lumbar synovial cysts tend to be in their sixth decade of life, with a slight female predominance. The incidence of lumbar syn-ovial cyst is thought to be less than 0.5% of the general symptomatic population. The cysts are commonly found at the L4–L5 segment and may be bilateral or unilateral. The aetiology is unclear, but underlying spi-nal instability, facet joint arthropathy and degenerative spondylolisthesis have a strong association with wors-ening symptoms and cyst formation. Khan and Girardi recently concluded in a very comprehensive review paper that resection and decompression with or with-out fusion remains an appropriate treatment option in patients with persistent radicular symptoms, despite appropriate conservative treatment [13].
Conclusions
Chronic LBP of facet origin is very difficult to •define. There is conflicting evidence that invasive treatment modalities are more effective than pla-cebo to improve LBP of supposed facet origin.Symptomatic neural compression due to facet joint •enlargement with or without spinal stenosis or degenerative spondylolisthesis is a good surgical indication when symptoms persist, despite adequate conservative treatment.
References
1. Airaksinen O, Brox I, Cedraschi C et al (2006) European guidelines for the management of chronic non-specific low back pain. Eur Spine J 15(Suppl 2):S192–S299
2. Atlas SJ, Keller RB, Robson D et al (2000) Surgical and nonsurgical management of lumbar spinal stenosis: four years outcomes from the Maine Lumbar Spine Study. Spine 25:556–562
3. Ayers CE (1935) Further case studies of lumbo-sacral pathology with consideration of involvement of interverte-bral discs and articular facets. N Engl J Med 213:716–721
4. Badgley CE (1941) The articular facets in relation to low-back pain and sciatic radiation. J Bone Joint Surg 23: 481–496
5. Boden SD, Davis DO, Dina TS, Patronas NJ, Wiesel SW (1990) Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation. J Bone Joint Surg Am 72(3):403–408
6. Dreyfuss P, Halbrook B, Pauza K, Joshi A, McLarty J, Bogduk N (2000) Efficacy and validity of radiofrequency neurotomy for chronic lumbar zygapophysial joint pain. Spine 25(10):1270–1277
7. Gallagher J, Petriccione di Vadi PL, Wedley JR (1994) Radiofrequency facet joint denervation in the treatment of low back pain: a prospective controlled double-blind study to assess its efficacy. Pain Clin 7:193–198
8. Geurts JW, van Wijk RM, Stolker RJ et al (2001) Efficacy of radiofrequency procedures for the treatment of spinal pain: a systematic review of randomized clinical trials. Reg Anesth Pain Med 26(5):394–400
9. Hall DJ (2004) Facet joint denervation: a minimally invasive treatment for low back pain in selected patients. The Lumbar spine, 3rd edn. Lippincott Williams and Wilkins, philadel-phia, New York
10. Hancock MJ, Maher CG, Latimer J, Spindler MF, McAuley JH, Laslett M, Bogduk N (2007) Systematic review of tests to identify the disc, SIJ or facet joint as the source of low back pain. Eur Spine J 16:1539–1550
11. Jackson RP, Jacobs RR, Montesano PX (1988) 1988 Volvo award in clinical sciences. Facet joint injection in low-back pain. A prospective statistical study. Spine 13(9):966–971
12. Kettler A, Wilke HJ (2006) Review of existing grading sys-tems for cervical and lumbar facet joint degeneration. Eur Spine J 15:705–718
13. Khan AM, Girardi F (2006) Spinal lumbar synovial cysts. Diagnosis and management challenge. Eur Spine J 15: 1176–1182
14. Kirkaldy-Willis WH, Wedge JH, Yong-Hing K, Reilly J (1978) Pathology and pathogenesis of lumbar spondylosis and stenosis. Spine 3:319–328
15. Leclaire R, Fortin L, Lambert R, Bergeron YM, Rossignol M (2001) Radiofrequency facet joint denervation in the treat-ment of low back pain. A placebo-controlled clinical trial to assess efficacy. Spine 26(13):1411–1417
16. Malmivaara A, Slätis P, Heliövaara M et al (2007) Surgical or nonoperative treatment for lumbar spinal stenosis? A ran-domized controlled trial. Spine 32:1–8
17. Niemistö L, Kalso E, Malmivaara A et al (2003) Radiofrequency denervation for neck and back pain: a sys-tematic review within the framework of the Cochrane Collaboration Back Review Group. Spine 28:1877–1888
18. Revel M, Poiraudeau S, Auleley GR, Payan C, Denke A, Nguyen M, Chevrot A, Fermanian J (1998) Capacity of the clinical picture to characterize low back pain relieved by facet joint anesthesia: proposed criteria to identify patients with painful facet joints. Spine 23(18):1972–1976
19. Shealy CN (1975) Percutaneous radiofrequency denervation of spinal facets. Treatment for chronic back pain and sciat-ica. J Neurosurg 43:448–451
20. van Kleef M, Barendse GA, Kessels A, Voets HM, Weber WEJ, de Lange S (1999) Randomized trial of radiofrequency lumbar facet denervation for chronic low back pain. Spine 24(18):1937–1942
21. Weinstein JN, Lurie JD, Tosteson TD et al (2007) Surgical versus nonsurgical treatment for lumbar degenerative spon-dylolisthesis. N Engl J Med 356(22):2257–2270

159M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_4.8, © Springer-Verlag Berlin Heidelberg 2010
One of the potential allures of nonrigid stabilization of the spine compared to traditional fusion is the possibil-ity that adjacent level disease can be eliminated or reduced [1]. Negative effects on the shoulder levels above and/or below a fused segment have been a rec-ognized downside to fusion in both the lumbar [2–4] and cervical spine [5, 6]. Occurrence of adjacent level disease has sometimes been referred to as the “topping off” process. We will explore whether this prospect is “myth” or “fact” by reviewing the relevant literature concerning adjacent level kinematics/biomechanics and clinically observed “topping off” phenomenon.
The two issues that are of primary interest in com-paring adjacent level disease in fusion vs. nonfusion stabilizing technology are the frequency of occurrence and the timing of pathologic development. One could argue that the use of nonfusion stabilization technol-ogy would be of benefit both if the frequency/incidence of adjacent level disease could be reduced, and if the time frames to observed occurrence could be extended (particularly if the time frames were in the order of years to decades).
Some interesting hybrid approaches using nonfu-sion stabilization technology have been employed in an effort to avoid adjacent level disease. A novel tactic to influence the biomechanics has been the use of bio-degradable instrumentation. While such interventions are still in the early stages of evaluation, they will be discussed as a possible future surgical option.
Spinal Fusion: Background on “TheGold Standard”
For spinal fusion, it is generally recognized that there is a definite risk of adjacent level clinically significant degeneration. Studies have primarily concentrated on evaluation of the cervical and lumbar spine. These are the most common anatomic regions for surgical inter-vention. As they also represent the mobile areas of the spine, the neck and the low back also constitute the segments most influenced by biomechanical forces.
“Topping off” syndrome, or adjacent level degen-eration, has been considered a general consequence of cervical fusion [5]. In the cervical spine, there have been studies of discetomy with and without anterior fusion [7, 8]. This provides an opportunity to establish the occurrence of postfusion adjacent level disease relative to natural history. In his study of 253 patients undergoing anterior discectomy, Lunsford [7] found 8% of fused patients and 5.5% of nonfused patients developed clinically significant adjacent level disease at a follow-up of 12–72 months. In contrast, radio-graphic (not necessarily symptomatic) adjacent level disease was found less commonly (41%) in patients having posterior laminotomy/foraminotomy vs. ante-rior cervical discectomy and fusion for a soft disk her-niation in a review by Herkowitz [8].
There have been isolated reports of adjacent level degeneration even in posterior laminaplasty/nonfusion operative techniques [9].
The level of the index surgery has been found to be a risk factor in the development of adjacent level symp-tomatic degeneration. Hilibrand [10] found a higher incidence in patients with their original fusion at C5–6 or C6–7. The study also concluded that a single level fusion at the index surgery was a significant risk factor
Adjacent Level Disease: “Myth” or “Fact”
David A. Wong and Katherine E. Wong
D. A. Wong (*) Advanced Center for Spinal Microsurgery, Presbyterian St. Luke’s Medical Center, Denver, CO 80218, USA e-mail: [email protected]
4.8
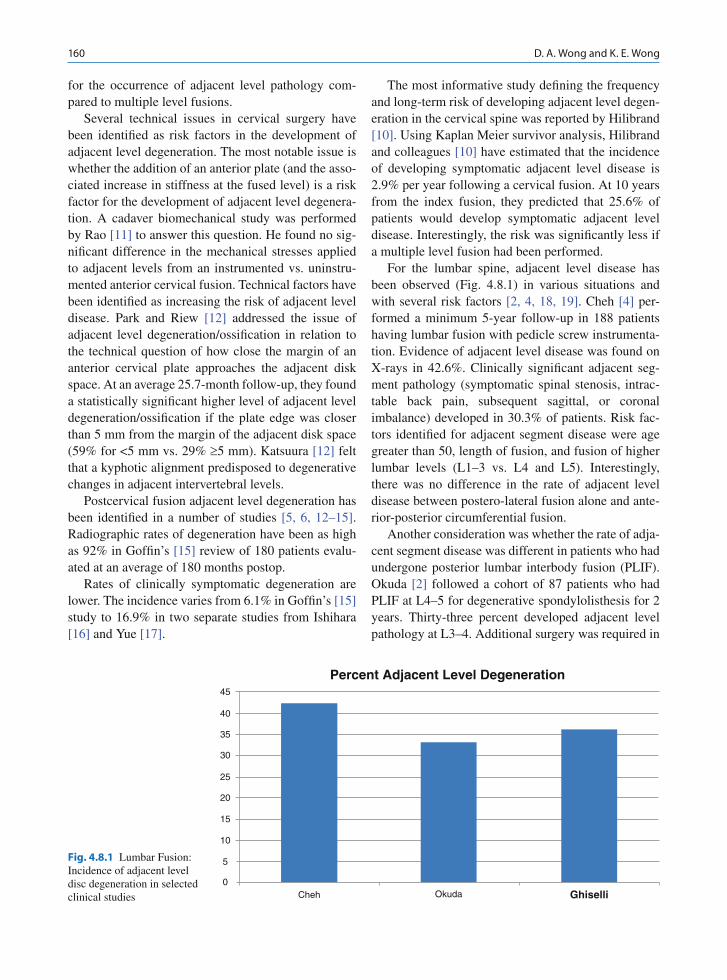
160 D. A. Wong and K. E. Wong
for the occurrence of adjacent level pathology com-pared to multiple level fusions.
Several technical issues in cervical surgery have been identified as risk factors in the development of adjacent level degeneration. The most notable issue is whether the addition of an anterior plate (and the asso-ciated increase in stiffness at the fused level) is a risk factor for the development of adjacent level degenera-tion. A cadaver biomechanical study was performed by Rao [11] to answer this question. He found no sig-nificant difference in the mechanical stresses applied to adjacent levels from an instrumented vs. uninstru-mented anterior cervical fusion. Technical factors have been identified as increasing the risk of adjacent level disease. Park and Riew [12] addressed the issue of adjacent level degeneration/ossification in relation to the technical question of how close the margin of an anterior cervical plate approaches the adjacent disk space. At an average 25.7-month follow-up, they found a statistically significant higher level of adjacent level degeneration/ossification if the plate edge was closer than 5 mm from the margin of the adjacent disk space (59% for <5 mm vs. 29% ³5 mm). Katsuura [12] felt that a kyphotic alignment predisposed to degenerative changes in adjacent intervertebral levels.
Postcervical fusion adjacent level degeneration has been identified in a number of studies [5, 6, 12–15]. Radiographic rates of degeneration have been as high as 92% in Goffin’s [15] review of 180 patients evalu-ated at an average of 180 months postop.
Rates of clinically symptomatic degeneration are lower. The incidence varies from 6.1% in Goffin’s [15] study to 16.9% in two separate studies from Ishihara [16] and Yue [17].
The most informative study defining the frequency and long-term risk of developing adjacent level degen-eration in the cervical spine was reported by Hilibrand [10]. Using Kaplan Meier survivor analysis, Hilibrand and colleagues [10] have estimated that the incidence of developing symptomatic adjacent level disease is 2.9% per year following a cervical fusion. At 10 years from the index fusion, they predicted that 25.6% of patients would develop symptomatic adjacent level disease. Interestingly, the risk was significantly less if a multiple level fusion had been performed.
For the lumbar spine, adjacent level disease has been observed (Fig. 4.8.1) in various situations and with several risk factors [2, 4, 18, 19]. Cheh [4] per-formed a minimum 5-year follow-up in 188 patients having lumbar fusion with pedicle screw instrumenta-tion. Evidence of adjacent level disease was found on X-rays in 42.6%. Clinically significant adjacent seg-ment pathology (symptomatic spinal stenosis, intrac-table back pain, subsequent sagittal, or coronal imbalance) developed in 30.3% of patients. Risk fac-tors identified for adjacent segment disease were age greater than 50, length of fusion, and fusion of higher lumbar levels (L1–3 vs. L4 and L5). Interestingly, there was no difference in the rate of adjacent level disease between postero-lateral fusion alone and ante-rior-posterior circumferential fusion.
Another consideration was whether the rate of adja-cent segment disease was different in patients who had undergone posterior lumbar interbody fusion (PLIF). Okuda [2] followed a cohort of 87 patients who had PLIF at L4–5 for degenerative spondylolisthesis for 2 years. Thirty-three percent developed adjacent level pathology at L3–4. Additional surgery was required in
Fig. 4.8.1 Lumbar Fusion: Incidence of adjacent level disc degeneration in selected clinical studies
45
40
35
30
25
20
15
10
5
0Cheh Okuda Ghiselli
Percent Adjacent Level Degeneration

1614.8 Adjacent Level Disease: “Myth” or “Fact”
the 2-year follow-up period in 4% (generally for neu-rologic deterioration). Age was not felt to be a risk fac-tor. There was an increased incidence of facet tropism and horizontalization of the lamina of L3 in the 4% requiring additional surgery.
Wai and Fraser’s [20] long-term study of patients having anterior lumbar interbody fusion was the one report reviewed, which concluded that the adjacent level disease seen was not likely to be influenced by an associated fusion. They looked at MRI scans and outcomes in 39 out of an original cohort of 64 patients having ALIF between 1980 and 1983 (25/64 > 39% lost to follow-up). In the 39 patients reviewed, MRI evidence of degeneration at nonfused levels was 74.3% (29 patients). There was no degeneration at the segment adjacent to the fusion in 17.9% (seven patients). Degeneration was isolated to the segment adjacent in 23.1% (nine patients). Breaking down the data, overall 56.4% (22/39 patients – nine isolated to adjacent level, 13 including diffuse degeneration) had some evidence of adjacent level degeneration. Considering this rate of 56.4% of adjacent level pathology, their conclusion is somewhat at odds with studies cited previously such as Okuda [2] (33% adja-cent degeneration) and Cheh [4] (42.6% adjacent level X-ray changes), where the authors felt that there was a relation between fusion and development of adjacent level pathology.
Ghiselli et al. [19] used a Kaplan Meier survivor analysis methodology (similar to the Hilibrand cervi-cal study) to look at the adjacent segment problem fol-lowing lumbar fusion. They have estimated that the rate of surgery for adjacent level disease was 3.9% per year following a primary lumbar fusion. Thus, at 10 years, the survivorship analysis predicted that 36.1% of lumbar fusion patients would have further operative intervention. Interestingly, their study also showed that the risk of adjacent level degeneration was signifi-cantly less for a multiple level fusion compared to a single segment arthrodesis. This is the most definitive study indicating both the incidence and the expected time frames for onset of degenerative changes in the adjacent levels after a lumbar fusion.
The Hilibrand (cervical) and Ghiselli (lumbar) sur-vivor analyzes [10, 19] are very informative in terms of defining the risk and likely time frames for the devel-opment of clinically significant adjacent level degen-eration following cervical and lumbar fusion (Fig. 4.8.2). The incidence appears to be a little higher in the lumbar spine (3.9% patients reoperated per year, 36.1% at 10 years) than the cervical spine (2.9% per year, 25.6% at 10 years). Adjacent level degeneration following spinal fusion can be considered a “fact,” not a myth. The survivor analysis [10, 19], in particular, helps define the parameters against which nonfusion technologies must be compared.
Fig. 4.8.2 Kaplan Meier Survival Analysis for Cervical Fusion (Hilibrand) and Lumbar Fusion (Ghiselli). Percent development of Adjacent level disease per year and predicted survivorship at 10 years
40
35
15
10
0
Cervical Lumbar
Per year 10 years
5
20
25
30

162 D. A. Wong and K. E. Wong
Interspinous Implants
Although the initial clinical indication for interspinous devices was treatment of neurogenic claudication from spinal stenosis [21, 22], some devices have been con-sidered for an indication of nonfusion stabilization [1]. Because of the consideration for stabilization, kine-matic and biomechanical studies have been performed which also give data on the adjacent levels [23]. Cadaver biomechanical studies of interspinous implants have suggested that the mechanical pressures in the disk at the index operated segment are reduced (20% reduction in neutral, 41% in extension) [24]. Of more import to the present discussion is the finding that the pressures at adjacent levels were not signifi-cantly affected. Other cadaver studies have looked at the biomechanics of the facets. Investigation suggests that the facet pressure can be reduced 39% at the oper-ated level, again without a significant pressure change at the adjacent levels [25]. Limited in vivo studies of kinematics after implantation of an X-Stop device have shown a similar lack of effect on adjacent levels [26]. Some authors have considered that the biomechanical properties suggest that an indication for interspinous devices would be correction of sagittal plane instabil-ity and avoidance of adjacent level pathology [27].
The literature lacks any long-term studies that would more definitively answer whether interspinous implants have an effect on the incidence and timing of adjacent level degeneration. In these circumstances, any positive influence of interspinous implants must be considered a “myth.”
Pedicle Screw-Based Nonfusion Systems
In patients having implanted pedicle screw-based non-fusion systems, there have been limited reports on the effects to adjacent levels. Using a positional magnetic resonance imaging methodology, Beastall [28] observed an intended degree of motion at the stabilized level, but no significant hypermobility at the shoulder levels above or below. Korovessis [28] followed a cohort of patients with dynamic instrumentation of the lumbar spine. Although a few cases of screw loosening were observed, no significant adjacent level disease was seen in the follow-up period which averaged almost 4 years.
As the studies to date are limited, we must still con-sider adjacent level degeneration in the situation of pedicle screw-based nonfusion systems as a “myth.”
Hybrid/Novel Approaches
Wardlaw [29] has used Dynesis instrumentation in a hybrid situation primarily at L5-S1 trying to avoid adjacent segment degeneration at L4–5. At the fusion level, a slightly long plastic spacer is compressed, leading to a more rigid construct to help enhance fusion. At L4–5, a standard nonfusion stabilization is performed. Nonrigid stabilization of the adjacent level holds some theoretical hope of reducing transfer of mechanical stress and decreasing adjacent level degen-eration. Patients involved in the preliminary technical report have not been followed for a sufficient time to confirm or deny the theoretical usage.
The addition of a metal plate to an anterior cervical fusion increases the rigidity of the fused segment and theoretically increases the mechanical forces transmit-ted to the shoulder levels above and below. In an effort to avoid this long-term stress shift, there have been limited applications of biodegradable plate technology [30]. Preliminary reports only have been published with insufficient data to form a conclusion concerning the effects of biodegradable implants.
The limited numbers involved in these hybrid or novel methodologies render any positive effect on adjacent levels in the realm of “myth.”
Disk Arthroplasty
While not generally considered as a primary stabiliz-ing intervention, we must consider disk arthroplasty as a form of nonfusion stabilizing technology. Several authors have addressed the influence of disk arthro-plasty on adjacent levels. Cunningham [31] looked at the biomechanics of lumbar TDA and found that the normal centrode of rotation was relatively maintained with TDA. In terms of motion, this would give TDA a favorable mechanical profile compared to fusion regarding shifting mechanical stresses to adjacent lev-els. Chang [32] performed disk pressure studies of adjacent levels in the cervical spine comparing disk

1634.8 Adjacent Level Disease: “Myth” or “Fact”
arthroplasty and fusion. Pressures were slightly lower at adjacent levels compared to fusion, except in flexion where pressures were higher with ProDisc–C.
Longer-term follow-up is more available for lumbar TDA. Lemaire [33] has an 8.7-year follow-up of ProDisc. David [34] has reported a 13.2-year follow-up of Charite. Rates of symptomatic ASD were low and varied between 1.9 and 2.8%, respectively. However, other studies have shown higher rates of adjacent level degeneration. Putzier [35] reported on a 17.3-year fol-low-up of 53 Charite cases with a 17.0% rate of radio-logic and symptomatic adjacent level disease. Huang [36] reviewed 42 semiconstrained prostheses and found a 23.8% rate of adjacent level degeneration.
Given rates of adjacent level degeneration as high as 23.8%, we should consider adjacent level degenera-tion with the presently available arthroplasties as a “fact.” Future design changes incorporating advanced shock absorption characteristics, in addition to motion technology, hold out the possibility that this “fact” can be altered for the benefit of future patients.
Conclusions
A preponderance of spinal fusion literature definitely substantiates an association with the development of adjacent level disease subsequent to surgery. Thus, in the context of spinal fusion, adjacent level degenera-tion should be considered a recognized “fact.”
The two papers using Kaplan Meier survivor analy-sis methodology (Hilibrand cervical [10], Ghiselli lumbar [19]) give us a baseline incidence of adjacent level degeneration for fusion (Fig. 4.8.2). These stud-ies set the parameters for any comparative investiga-tion of adjacent level degeneration using nonfusion technology.
In consideration of nonfusion stabilization proce-dures as a whole, kinematic studies give us hope that a similar connection to adjacent level pathology might be circumvented compared to fusion. However, the weight of clinical evidence currently available to fac-tually resolve the question is limited. These circum-stances dictate that, at least for the present, the concept of avoiding adjacent level pathology by the use of interspinous devices, pedicle screw-based stabilization technology, hybrid surgeries, biodegradable instru-mentation, or disk arthroplasty must be considered in
the category of “myth.” Future investigations with larger patient enrollment and longer-term follow-up can be expected to give us a more definitive answer as to the effects of nonfusion stabilization technology on adjacent level degeneration.
References
1. Kim DH, Albert TJ (2007) Interspinous process spacers. J Am Acad Orthop Surg 15(4):200–207
2. Okuda S, Iwasaki M, Miyauchi A, Aono H, Morita M, Yamamoto T (2004) Risk factors for adjacent segment degeneration after PLIF. Spine 29(14):1535–1540
3. Park P, Garton HJ, Gala VC, Hoff JT, McGillicuddy JE (2004) Adjacent segment disease after lumbar or lumbosacral fusion: review of the literature. Spine 29(17):1938–1944
4. Cheh G, Bridwell KH, Lenke LG, Buchowski JM, Daubs MD, Kim Y, Baldus C (2007) Adjacent segment disease following lumbar/thoracolumbar fusion with pedicle screw instrumenta-tion: a minimum 5-year follow-up. Spine 32(20):2253–2257
5. Bartolomei JC, Theodore N, Sonntag VK (2005) Adjacent level degeneration after anterior cervical fusion: a clinical review. Neurosurg Clin N Am 16(4):575–587
6. Hilibrand A, Robbins M (2004) Adjacent segment degenera-tion and adjacent segment disease: the consequences of spi-nal fusion? Spine J 4(6S):190S–194S
7. Lunsford LD, Bissonette DJ, Jannetta PJ et al (1980) Anterior surgery for cervical disease. Part I: treatment of lateral cervi-cal disc herniation in 253 cases. J Neurosurg 53:1–11
8. Herkowitz HN, Kurz LT, Overholt DP (1990) Surgical man-agement of cervical soft disc herniation. A comparison between the anterior and posterior approach. Spine 15:1026–1030
9. Wang MY, Green BA, Vitarbo E, Levi AD (2003) Adjacent Segment disease: an uncommon complication after cervical expansile laminoplasty:a case report. Neurosurgery 53(3): 770–772
10. Hilibrand A, Carlson GD, Palumbo MA, Jones PK, Bohlman HH (1999) Radiculopathy and myelopathy at seg-ments adjacent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am 81:519–528
11. Rao RD, Wang M, McGrady LM, Perlewitz TJ, David KS (2005) Does anterior plating of the cervical spine predispose to adjacent segment changes? Spine 30(24):2788–2792
12. Katsuura A, Huduka S, Saruhashi Y et al (2001) Kyphotic malalignment after anterior cervical fusion is one of the fac-tors promoting the degenerative process in adjacent interver-tebral levels. Eur Spine J 10:320–324
13. Kulkarni V, Rajshekhar V, Raghuram L (2004) Accelerated spondylotic changes adjacent to the fused segment following central cervical corpectomy: magnetic resonance imaging study evidence. J Neurosurg 100:2–6
14. Teramoto T, Ohmori K, Takatsu T et al (1994) Long term results of the anterior cervical spondylodesis. Neurosurgery 35:64–68
15. Goffin J, Geusens E, Vantomme N et al (2004) Long term follow up after interbody fusion of the cervical spine. J Spinal Disord Tech 17:79–85

164 D. A. Wong and K. E. Wong
16. Ishihara H, Kanamori M, Kawaguchi Y et al (2004) Adjacent segment disease after anterior cervical interbody fusion. Spine J 4:624–628
17. Yue WM, Brodner W, Highland TR (2005) Long term results after anterior cervical discectomy and fusion with allograft and plating: a 5-11 year radiographic and clinical follow up study. Spine 30:2138–2144
18. Ghiselli G, Wang JC, Hsu WK, Dawson EG (2003) L5-S1 segment survivorship and clinical outcome analysis after L4-L5 isolated fusion. Spine 28(12):1275–1280
19. Ghiselli G, Wang JC, Bhatia NN, Hsu WK, Dawson EG (2004) Adjacent segment degeneration in the lumbar spine. J Bone Joint Surg Am 86:1497–1503
20. Wai E, Santos E, Morcom R, Fraser R (2006) Magnetic reso-nance imaging 20 years after anterior lumbar interbody fusion. Spine 31(17):1952–1956
21. Zucherman JF, Hsu KY, Hartjen CA et al (2004) A prospec-tive randomized multi-center study for the treatment of lum-bar spinal stenosis with the X Stop interspinous implant: 1 year results. Eur Spine J b13:22–31
22. Zucherman JF, Hsu KY, Hartjen CA et al (2005) A multi-center prospective randomized trial evaluating the X STOP interspinous process decompression system for the treat-ment of neurogenic intermittent claudication: two year fol-low-up results. Spine 30:1351–1358
23. Lindsey D, Swanson K, Fuchs P, Hsu K, Zucherman J, Yerby S (2003) The effects of an interspinous implant on the kinematics of the instrumented and adjacent levels in the lumbar spine. Spine 28(19):2192–2197
24. Swanson KE, Lindsey DP, Hsu KY, Zucherman JF, Yerby SA (2003) The effects of an interspinous implant on interverte-bral disc pressures. Spine 28:26–32
25. Wiseman CM, Lindsey DP, Frederick AD, Yerby SA (2005) The effect of an interspinous process implant on facet load-ing during extension. Spine 30:903–907
26. Siddiqui M, Karadimas E, Nicol M, Smith FW, Wardlaw D (2006) Effects of X-Stop device on sagittal lumbar spine kine-matics in spinal stenosis. J Spinal Disord Tech 19(5):328–323
27. Minns RJ, Walsh WK (1997) Preliminary design and experi-mental studies of a novel soft implant for correcting sagittal plane instability in the lumbar spine. Spine 22:1819–1825
28. Beastall J, Karadimas E, Siddiqui M, Nicol M, Hughes J, Smith F, Wardlaw D (2007) The dynesis lumbar stabilization system: a preliminary report on positional magnetic reso-nance imaging findings. Spine 32(6):685–690
29. Wardlaw D. Personal communication. Manuscript submitted for peer review
30. Vaccaro AR, Robbins MM, Madigan L, Albert TJ, Smith W, Hilibrand AS (2004) Early findings in a pilot study of ante-rior cervical fusion in which bioabsorbable interbody spac-ers were used in the treatment of cervical degenerative disease. Neurosurg Focus 16(3):E7
31. Cunningham BW (2004) Basic scientific considerations in total disc arthroplasty. Spine J 4(6S):219S–230S
32. Chang UK, Kim DH, Lee MC et al (2007) Changes in adjacent-level disc pressure and facet joint force after cer-vical arthroplasty compared with cervical discectomy and fusion. J Neurosurg Spine 7:33–39
33. Lemaire JP, Carrier H. Sariali el H et al (2005) Clinical and radiological outcomes with the Charite artificial disc: a 10 year minimum follow up. J Spinal Disord Tech 18:353–359
34. David T (2007) Long term results of one level lumbar arthro-plasty: minimum 10 year follow up of the CHARITE artifi-cial disc in 106 patients. Spine 32:661–666
35. Funk PM, JF SSV et al (2006) Charite total disc replacement – clinical and radiographical results after an average follow up of 17 years. Eur Spine J 15:183–195
36. Huang RC, Tropiano P, Marnay T et al (2006) Range of motion and adjacent level degeneration after lumbar total disc replacement. Spine J 6:242–247

165M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_4.9, © Springer-Verlag Berlin Heidelberg 2010
PGP generally arises in relation to pregnancy, trauma, arthritis and osteoarthritis. Pain is experienced between the posterior iliac crest and the gluteal fold, particularly in the vicinity of the SIJs. The pain may radiate in the posterior thigh and can also occur in conjunction with/or separately in the symphysis. The endurance capac-ity for standing, walking and sitting is diminished.
The diagnosis of PGP can be reached after exclu-sion of lumbar causes. The pain or functional distur-bances in relation to PGP must be reproducible by specific clinical tests [1].
The cause of PGP is multi-factorial, and PGP may be related to different conditions. Only a few factors are proven to have an impact on the development of the condition. Most studies have included women in rela-tion to pregnancy because the vast majority of patients with PGP are women. A large number of patients have been collected during routine pregnancy controls. In these latter cases, there is no disease or trauma to initiate the condition, as there is in, for example, ankylosing spondylitis or after trauma. Consequently, there is no obvious explanation for the onset of most cases of PGP.
Fusion of the SIJs is described in ten cohort studies [3, 4, 6–9, 12, 13, 19, 25, 29], the first by Smith-Peterson and Rogers in 1926. External fixation to eval-uate patients for surgery was previously used by Slätis [17, 18] and Walheim [30]. The effect of external fixa-tion on the movements of the SIJs was studied by Sturesson et al. [24]. They showed that the movements in the SIJs were reduced from 1.2 to 0.6° around the
x-axis as well as the helical axis. When the external fixator was tightened, sacrum rotated anteriorly (nuta-tion) to a more stable position. This movement pattern proved the hypothesis proposed by Vleeming and Snijders [26, 27].
This study is a preliminary report based on patient files and telephone interviews with the patients. All patients operated with a fusion of the SIJs are reported.
Material
Among the patients referred to the hospitals in Malmö (3) and Ängelholm (50) because of intolerable PGP between 1989 and 2007, 52 patients, 41 women and 11 men, were selected for the evaluation of sacroiliac fusion. Typical symptoms were intolerable pain in the sacroiliac area and reduced ability to sit, stand and walk. All patients underwent a 3 weeks test period with the external fix-ator. If their posterior pelvic pain was markedly reduced, the test was judged as positive. Forty-five patients, 36 women and 9 men, were accepted for a sacroiliac fusion. The age of the patients was between 22 and 59 years at the time of the operation. The pain duration before surgery was between 2 and 12 years. In 21 patients the indication for surgery was post-preg-nancy PGP, in 14 patients post-traumatic pain, in two patients reactive arthritis, in one patient extrofi of the symphysis, in one patient pain after bone harvesting and in six patients the reason for PGP was unknown. All patients had undergone a longstanding individually tailored physiotherapy before surgery. Seven patients, two men and five women, had no positive effect with the external fixator test, and thus, not fulfilled the cri-teria for surgery.
Pelvic Girdle Pain: Indication for Surgery?
Bengt Sturesson
B. Sturesson Department of Orthopaedics, Ängelholm Hospital, 262 81, Ängelholm, Sweden e-mail: [email protected]
4.9

166 B. Sturesson
Methods
Several manual diagnostic tests are proposed for diag-nosing PGP. The test used in this study was initially the P4 test [14], Menell’s test and Sacral Springing Test. When the ASLR test [11] and long ligament tests [28] were defined, they were included in the test protocol.
After a clinical examination the diagnostic proce-dure continued with a SIJ block to the affected joint(s) [10, 16]. Patients who experienced a significant pain relief by the SIJ block were offered to be operated on with an external Hoffman-Slätis frame. The frame was tightened until the pain in the posterior part of the pel-vis was relieved and the ability to walk was restored. The patients were then sent home and told to do nor-mal exercises to test whether the frame could relieve the PGP or not. The patients were fully aware that fusion surgery was depended on the effect of the fix-ator. Of the 52 patients tested with the external fixator, 45 patients, 36 women and 9 men, were accepted for a sacroiliac fusion. The fusion was performed with the technique described by Smith-Peterson and Rogers [19] with the difference that the patient was allowed to ambulate. Twenty-five patients were operated bilater-ally and had the external fixator during the healing process. Thirteen were operated unilaterally with an external frame as fixator. Five were operated onwith a unilateral screw fixation to the S1 vertebral body. Two patients were operated unilaterally on both sides with screw fixation with one respectively 2 years intervals between the operations. The fusion was considered successful if the patient was pain free or if the function to sit, stand and walk was restored. Generally, radiog-raphy was performed after 4 and 12 months. If the patient showed no relief in symptoms, a computed tomography was performed to evaluate the healing more accurately.
Results
The patients were followed up with a telephone inter-view 6 months to 18 years after surgery. Twenty-four patients judged the operation as a success and the life and pain situation was considerably changed. Thirteen patients considered improved result and improved function after surgery. Three patients were unchanged,
two patients had a too short follow-up (6 months) and three patients from Hong Kong (2) and Canada (1) were impossible to reach for a telephone follow-up. Five of the patients were re-operated because of pseudarthrosis. All healed after re-operation with revision of the fusion area and new bone transplanta-tion and internal fixation with ileosacral screw fixa-tion. Additionally, two patients were re-operated, but the primary operation was performed at another hos-pital. One patient had a nerve injury to the L5 nerve after a screw fixation. The screw was replaced but the nerve injury persisted. Two years later, she was oper-ated on the opposite side, and after 10 years on sick leave she has now returned to work 1 year after the last operation.
No patient deteriorated after surgery. Only one patient would hesitate to redo the operation if similar symptoms should return. Forty patients were sick-listed before surgery and 22 patients are now in full-time work and three in part-time work. One is retired because of age and 16 are still on sick leave or disabled.
Discussion
Why some women develop persisting PGP after preg-nancy is unknown? About 1% [2] have persisting pain 2 years after delivery, but the pain is intolerable only in very few. Most patients with PGP can be treated with stabilizing physiotherapy [21–23]. The dominating physiotherapy treatment consists of stabilizing exer-cises where the transverse and oblique abdominal as well as the large gluteal muscles are trained. The rea-son why not all patients can stabilize the pelvis can have different explanations. One possible explanation is that there is a neuromuscular malfunction in the affected muscles, and independent on how much the patient is exercising, there will be no training effect. Another possible explanation is that low virulent anaerobic bacteria can infect the joint.
Among patients with a trauma, the cartilage is most likely injured with a secondary arthritis as a cause of pain. Histology [5] reveals that the degenerative pro-cess starts already in the third decade. There are, how-ever, no evidence that degenerative findings can be correlated to pain. On the other hand, it is well-known that knee arthritis is not necessary painful, even if radi-ography reveals arthritis [15].

1674.9 Pelvic Girdle Pain: Indication for Surgery?
In most cases with PGP after pregnancy, roentgeno-grams reveal no positive findings. In this study the patients were accepted for surgery only if the test with the external Hoffman-Slätis fixator showed total or marked relief of symptoms. Seven patients had posi-tive SIJ blocks, but no effect of the external fixator. Different explanations for the lack of effect were pos-sible. One is that the external fixator is ineffective in reducing the pain, which for example would be the case in an acute infection. This cannot be the case with these patients. Another explanation can be that these patients had a low lumbar cause of pain. Innervation to the posterior part of the SIJ is derived from L5 to S2 [20] and an injection with local anaesthesia to this part of the joint can reduce pain coming from, for example, the L5-S1 facet joints.
The diagnostic procedure, before surgery can be offered, is long and complicated. If a sacroiliac fusion is considered, a pre-operative test with external Hoffman-Slätis fixator is recommended. Pain around the SIJ is a target area for referred pain innervated of the L4, L5 and S1 nerves. There is a considerable risk that patients can be operated on with wrong indication. This was probably the case when two patients assessed by a senior surgeon had a sacroiliac fusion. They were assessed to be completely clear candidates for a sacro-iliac fusion after positive results of sacroiliac blocks. These patients were not included in the study because they had no external fixator prior to surgery. Neither of them had improvement after surgery.
The pain pattern among patients with severe PGP has many similarities with patients with nerve entrap-ment. Before the diagnosis of disc hernia, probably many patients were diagnosed having sacroiliac pain. The main difference is, however, that when a disc her-nia usually resolves, the patient with severe PGP are deteriorating. Despite the long history of pain and dis-ability, it is striking that about 50% of the patients in the present study are totally restored. It seems that the previous studies have better or equal results [3, 4, 6–9, 12, 13, 19, 25, 29]. Thus, the success rate can be com-pared with patients operated for back pain.
The present study is only a preliminary report based on files and telephone interviews. However, taking into consideration the pain duration and the high degree of disability before surgery, the high rate of successful out-come after surgery is rewarding for both patient and sur-geon. Sacroiliac fusion can be recommended in selected cases, but has to be studied within a research protocol.
References
1. COST B13:WG4 European Guidelines for the diagnosis and treatment of pelvic girdle pain, personal communication
2. Albert H, Godskesen M, Westergaard J (2001) Prognosis in four syndromes of pregnancy-related pelvic pain. Acta Obstet Gynecol Scand 80:505–510
3. Belanger TA, Dall BE (2001) Sacroiliac arthrodesis using a posterior midline fascial splitting approach and pedicle screw instrumentation: a new technique. J Spinal Disord 14: 118–124
4. Berthelot JM, Gouin F, Glemarec J, Maugars Y, Prost A (2001) Possible use of arthrodesis for intractable sacroiliitis in spon-dylarthropathy: report of two cases. Spine 26:2297–2299
5. Bowen V, Cassidy JD (1981) Macroscopic and microscopic anatomy of the sacroiliac joints from embryonic life until the eighth decade. Spine 6:620–628
6. Buchowski JM, Kebaish KM, Sinkov V, Cohen DB, Sieber AN, Kostuik JP (2005) Functional and radiographic outcome of sacroiliac arthrodesis for the disorders of the sacroiliac joint. Spine J 5:520–528
7. Gaenslen FJ (1927) Sacro-iliac arthrodesis. J Am Med Assoc 89:2031–2035
8. Giannikas KA, Khan AM, Karski MT, Maxwell HA (2004) Sacroiliac joint fusion for chronic pain: a simple technique avoiding the use of metalwork. Eur Spine J 13:253–256
9. Keating JG, Avillar MD, Price M (1997) Sacroiliac joint arthrodesis in selected patients with low back pain. In: Movement, stability and low back pain. Churchill Livingstone, pp 573–586
10. Maigne JY, Aivaliklis A, Pfefer F (1996) Results of sacroiliac joint double block and value of sacroiliac pain provocation tests in 54 patients with low back pain. Spine 21:1889–1892
11. Mens JM, Vleeming A, Snijders CJ, Stam HJ, Ginai AZ (1999) The active straight leg raising test and mobility of the pelvic joints. Eur Spine J 8:468–473
12. Moore MR (1997) Surgical treatment of chronic painful sacroiliac joint dysfunction. In: Vleeming A et al (eds) Movement, stability and low back pain. Churchill Living-stone, pp 563–572
13. Olerud S, Walheim GG (1984) Symphysiodesis with a new compression plate. Acta Orthop Scand 55:315–313
14. Östgaard HC, Zetherström G, Roos-Hansen E, Svanberg G (1994) The posterior pelvic pain provocation test I pregnant women. Eur Spine J 3:258–260
15. Paradowski PT, Englund M, Roos EM (2004) Lohmander LS (2004)Similar group mean scores, but large individual varia-tions, in patient-relevant outcomes over 2 years in meniscec-tomized subjects with and without radiographic knee osteoarthritis. Health Qual Life Outcomes 2:38
16. Schwarzer AC, Aprill CN, Bogduk N (1995) The sacroiliac joint in chronic low back pain. Spine 20:31–37
17. Slätis P, Eskola A (1989) External fixation of the pelvic gir-dle as a test for assessing instability of the sacro-iliac joint. Ann Med 21:369–372
18. Slätis P, Karaharju EO (1975) External fixation of the pelvic girdle with a trapezoid compression frame. Injury 7:53–56
19. Smith-Petersen MN, Rogers WA (1926) End-result study of arthrodesis of the sacroiliac joint for arthritis – traumatic and nontraumatic. J Bone Joint Surg 8:118–136

168 B. Sturesson
20. Solonen KA (1957) The Sacroiliac joint in the light of ana-tomical, roentgenological and clinical studies. Acta Orthop Scand Suppl 27:1–127
21. Stuge B, Hilde G, Vollestad N (2003) Physical therapy for pregnancy-related low back and pelvic pain: a systematic review. Acta Obstetet Gynecol Scand 82:983–990
22. Stuge B, Lærum E, Kirkesola G, Vøllestad N (2004) The efficacy of a treatment program focusing on specific stabiliz-ing exercises for pelvic girdle pain after pregnancy. A ran-domized controlled trial. Spine 29:351–359
23. Stuge B, Veierød MB, Lærum E, Vøllestad N (2004) The effi-cacy of a treatment program focusing on specific stabilizing exercises for pelvic girdle pain after pregnancy. A two-year follow-up of a randomized clinical trial. Spine 29:E197–E203
24. Sturesson B, Udén A, Önsten I (1999) Can an external frame fixation reduce the movements of the sacroiliac joint? A radiostereometric analysis. Acta Orthop Scand 70:37–41
25. van Zwienen CM, van den Bosch EW, Snijders CJ, van Vugt AB (2004) Triple pelvic ring fixation in patients with
severe pregnancy-related low back and pelvic pain. Spine 29:478–484
26. Vleeming A, Stoeckart R, Volkers ACW, Snijders CJ (1990) Relation between form and function in the sac-roiliac joint. 1. Clinical anatomical aspects. Spine 15: 130–132
27. Vleeming A, Volkers ACW, Snijders CJ, Stoeckart R (1990) Relation between form and function in the sacroiliac joint. 2. Biomechanical aspects. Spine 15:133–136
28. Vleeming A, Pool-Goudzwaard A, Hammudoghlu D, Stoeckart R, Snijders CJ, Mens JM (1996) The function of the long dorsal sacroiliac ligament: its implication for under-standing low back pain. Spine 21:556–562
29. Waisbrod H, Krainick JU, Gerbershagen HU (1987) Sacroiliac joint arthrodesis for chronic lower back pain. Arch Orthop Trauma Surg 106:238–240
30. Walheim GG (1984) Stabilization of the pelvis with the Hoffman frame. An aid in diagnosing pelvic instability. Acta Orthop Scand 55:319–324

169M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_4.10, © Springer-Verlag Berlin Heidelberg 2010
With the increasing rate of spine surgery being performed worldwide, the complexity of these surgeries is also increasing. This chapter reviews the types of procedures most at risk for significant blood loss and covers various options, surgical and anesthetic, which can be implemented to decrease that blood loss.
The consequences of high blood loss cases are numerous. The increased stress to the cardiac system and the major perfusion needs, including cerebral, car-diac, and renal, are well-known. Transfusion reactions can range from mild itching or fevers to major reac-tions. Exposure to allogenic blood transfusion can also increase the risk of bacterial infections, ranging from wound infection to pneumonia or bacteremia [1], although this relative risk can be reduced by reducing the white blood cells in the transfused blood [2]. More recently, transfusion related acute lung injury (TRALI), which includes dyspnea, hypoxemia, hypotension, bilateral pulmonary edema, and fever, has been recog-nized as linked to transfusion of any blood product, which may contain even small amounts of plasma [3]. Certainly, increased transfusion needs appear to be correlated with longer intensive care and hospital length of stay [4, 5]. Large volume blood loss during posterior procedures is also associated with the devel-opment of postoperative visual loss (POVL) [6].
Certainly, any spine surgeon is well aware of the potential for bleeding during posterior spinal surgery, where the muscles stripped from the spine have numer-ous potential bleeding points, and any intracanal work has the potential to cause epidural bleeding. For the former, patients with neuromuscular conditions have
greater risk of bleeding during the surgery. Osteoporotic patients have greater bleeding channels from their porotic bone. Anterior spine exposures are also affected by osteoporotic bone, particularly since the vertebral bodies themselves are generally more severely affected than the posterior elements. Of course, the anterior vasculature has great potential for extensive bleeding; experience with anterior exposures by the spine sur-geon or vascular surgeon is critical for minimizing this risk. Revision surgery is usually associated with higher blood loss, with the potential for critical blood loss being greatest for revision anterior spinal surgery if the major vessels are injured.
There are a number of types of spinal procedures that are more likely to lead to greater surgical blood loss than others. These include neuromuscular spinal deformities, revision surgery, more extensive fusions (>10 levels) such as those for scoliosis or kyphosis, surgery of longer duration (>6 h), and tumor resec-tions. In addition, multiple osteotomies, pedicle sub-traction osteotomy, eggshell, or other types of resections expose extensive cancellous bony surface areas and have potential for significant bleeding.
It is worth noting that pediatric spine cases differ from adult spine cases. Pediatric periosteum strips smoothly from the bone at the time of surgery. Pediatric patients have more flexible curves, which may allow shorter fusions. Adults have stiffer curves which may require inclusion of longer segments, including compen-satory curves. These stiffer curves may require anterior release and fusion and/or multiple osteotomies to enable curve correction; Adult bones may be more osteoporotic and have increased bleeding from their surfaces. Because adult patients are more likely to have spinal stenosis as a component of their indication for surgery, they often require spinal decompression with the potential for epi-dural bleeding. Pseudoarthrosis is more unusual in
Blood Loss Management in Major Spine Surgery
Serena S. Hu and Jeremy A. Lieberman
S. S. Hu (*) Department of Orthopedic Surgery, 500 Parnassus Avenue, Room MU320 West, San Francisco, CA 94143, USA e-mail: [email protected]
4.10

170 S. S. Hu and J. A. Lieberman
pediatric patients, except those with neurofibromatosis, connective tissue conditions, and neuromuscular condi-tions such as meningomyelocele. The fusion rate is lower in adults, thus it is more common to require revision sur-gery which has greater potential for blood loss.
While not actually reducing surgical bleeding, blood conservation methods, such as cell salvage and preoperative erythropoietin, can decrease the need for homologous blood transfusions [7–9]. Predonation of autologous blood combined with intraoperative use of cell saver may not both be necessary unless significant blood loss (>2,000 mL) occurs [10, 11].
During surgery, there are several options that the surgeon and the anesthesiologist can use to decrease the potential for blood loss. These can be divided into local methods, which can be utilized by the surgeon, and systemic methods, such as hemodilution, con-trolled hypotension, proper use of blood products, and antifibrinolytics.
Clearly, the surgeon should always perform careful hemostasis, use the proper tissue planes for exposure, and apply cautery judiciously, either monopolar or bipo-lar as appropriate. Local agents such as gelfoam, surgi-cal, and oxycel, essentially different formulations of cellulose or gelatin, can be used to improve local hemo-stasis when applied to bleeding surfaces such as muscle or bone, which is not easily cauterized. Oftentimes, these substances are mixed with thrombin, a component of the clotting cascade, for additional efficacy. Application of these substances combined with direct pressure, i.e., packing off of that area of the surgical field, can decrease local oozing. Bone wax can be applied to specific bony bleeding sites. However, this may interfere with bone healing and should be used in limited areas.
There are occasions where it may be appropriate to complete a major operation at a second stage. There may be a threshold beyond which the patient may not tolerate additional blood loss, or where a patient who is a Jehovah’s witness and will not accept blood trans-fusion will become significantly compromised. If the rate of bleeding is increasing steadily, suggesting a developing or progressive coagulopathy, particularly if the surgeon anticipates more than 1–2 h of additional surgery, it may be safer to complete the surgery at a later date. This may expose the patient to a potentially higher risk of infection or longer hospitalization, but massive blood loss due to a coagulopathy or even dis-seminated intravascular coagulation, carries with it potentially greater risks as has been noted above.
Controlled hypotension has been used successfully to decrease blood loss during spine surgery [9]. It has been demonstrated that decreasing the venous pressure will result in a decrease of the intraosseous pressure, which will decrease the surgical bleeding [12]. A vari-ety of agents have been used to induce hypotension, including anesthetics or vasoactive agents. Many appear to be effective in reducing bleeding, and selection may be based on other effects of these drugs. Its use is lim-ited if the patient has vascular disease, cardiac disease, or poorly managed hypertension. It may be risky in patients who have a compromised spinal cord, either with a spinal cord injury or myelopathy, since spinal cord perfusion could be compromised with hypoten-sion. Where appropriate, nitroglycerin is more effective than halothane for inducing controlled hypotension. It is worth noting that Tsuji and colleagues (2001) studied patients undergoing cervical laminaplasty for myelopa-thy and found that the use of PGE1 for inducing hypotension appeared to improve the pulsatility index, as a measure of blood flow to the anterior spinal artery.
Isovolemic hemodilution is the drawing off of a pint or two of blood with subsequent maintenance of intra-vascular volume with colloid and crystalloid. While not reducing blood loss, the intraoperative bleeding will be of more dilute blood, decreasing the need for intraoperative blood transfusion [9, 13]. Some concern was raised that hemodilution might lead to early coag-ulopathy, however, no effect on global coagulation fac-tors could be measured in one carefully designed study to examine this concern [14].
It is essential that appropriate monitoring of the hematocrit and clotting function occurs in the operating room. Dilution coagulopathy may result from the loss of clotting factors, platelets, or fibrinogen. Judicious use of laboratory studies of clotting factor levels is essential during periods of significant blood loss. Anticipation of blood products needs is important, as there may be a delay in thawing frozen plasma or pool-ing platelets.
There are several antifibrinolytics that stabilize the initial fibrin clot, which have been used with some suc-cess in orthopedic and spine patients. These include Aprotinin, transexamic acid (TXA), and e-aminocap-roic acid.
Aprotinin, a serine protease inhibitor that acts as an antifibrinolytic as well as a platelet membrane stabilizer, has been shown in several prospective studies, including some randomized and blinded, to decrease blood loss in

1714.10 Blood Loss Management in Major Spine Surgery
spine surgery as well as other orthopedic cases in which high blood loss can be expected (tumor surgery, revi-sion joint replacement) [15–18]. Despite the risk of ana-phylaxis, if the patient has had a repeat exposure [19], its effectiveness in Level I trials seemed clear enough that it was recommended for use in complex cases in a Current Concepts review in the Journal of Bone and Joint Surgery [20]. Recently, extensive safety concerns have been raised, both for cardiac cases [21] as well as a recent study [22], where renal failure occurred in sev-eral patients who received Aprotinin during their spine surgery. This prospective, randomized trial found four patients receiving Aprotinin developed renal failure requiring dialysis, compared to only one patient in the control group, whose renal failure probably was due to an overdose of gentamycin . These concerns led to a safety review by the FDA [23], begun in Oct 2007, with the manufacturing company agreeing to stop marketing the drug at the FDA’s request shortly thereafter.e-aminocaproic acid, or amicar, was used in adult
deformity patients [18]. This study compared amicar and Aprotinin in adult deformity patients who were undergoing combined anterior and posterior spinal fusion. Decreased blood loss was found in the Aprotinin and amicar groups compared to controls.
TXA, a synthesized form of lysine, prevents enzymes from breaking down blood clots and has been studied in spine surgery [24]. This study found that TXA decreased the blood loss and transfusion requirements in spinal fusions for patients with Duchenne’s muscular dystro-phy, a patient population which often has extensive sur-gical blood loss [25]. TXA can reduce the transfusion needs for PSF in adolescent idiopathic scoliosis patients. Although not studied specifically in spine cases, it has also been shown that topical TXA may decrease the surgical EBL by up to 50%, apparently by increasing the D-dimer and PAP locally where it is applied [26], Buffery [27] published a meta-analysis looking at the use of these antifibrinolytics in orthopedic and spine surgeries. The majority of the studies were in total hip replacement and total knee replacement surgeries. Their analysis resulted in favor of TXA and Aprotinin as compared to controls. There were too few studies using amicar to be conclusive of its efficacy. They found no difference for any of these agents in the incidence of thromboembolic events vs. controls.
Recombinant activated factor VII, a component of the coagulation cascade used originally for hemophiliac patients, is finding more recent application in other
situations where control of bleeding is of concern. This includes trauma patients, those with intracerebral bleed-ing and potentially high blood loss surgeries. A feasi-bility and safety study in spine surgery patients was recently published [28]. This involved patients in whom significant blood loss was anticipated [29] (greater than three level fusions), and in whom there were no risk factors for thrombosis. A unique study design was uti-lized. Patients were randomized to receive the study drug or placebo once a blood loss trigger of 10% of the patient’s blood volume was reached and an additional 10% or more blood loss was anticipated. The lowest dose, at 30 mg/kg, was tested first for safety, with the higher doses of 60 and 90 mg not tested until safety was established at the prior dose. Although there was no dif-ference between blood loss in the different treatment groups, when adjusting for the a priori factors of the patient’s blood volume and the number of segments of fusion, use of rFVIIa resulted in a significant difference in mean blood loss and total transfusion. The lowest dose of 30 mg was as effective as the other doses. Adverse effects were similar between the study and control groups; there was one patient who received the study drug who suffered a fatal stroke and MI. This patient had risk factors, including a long smoking his-tory and hypertension, as well as periods of intraopera-tive hypotension, the former of which should have excluded him from entry into the study.
Weighing of risk-benefit ratios for the use of these drugs and techniques should always be considered when using any of these options described. Cost ben-efit ratios are increasingly coming to the attention and responsibility of the surgeons and anesthesiologists caring for patients (Table 4.10.1).
This must be balanced by the cost of blood prod-ucts: packed cells (leuko reduced) $247, plateletphere-sis (leuko reduced) $603, fresh frozen plasma ($74), cryoprecipitate $74 each, and $370 for pooled crypt,
Table 4.10.1 Summarizes the cost for a typical dosing of the agents discussed at one institution
Dosage Cost
Aprotinin 1 m KIU + 0.25 m KIU/h × 6 h surgery
$475.01
Tranexemic acid
10 mg/kg 70 kg patient, + 10 mg/kg-h
$185.20
Amicar 5 g + 15 mg/kg-h $1.90
rfVIIa 30 mcg × 70 kg × 3 doses $ 6,912

172 S. S. Hu and J. A. Lieberman
which does not include the anesthesia or nursing costs. It is also important to consider the cost of treating patients who have a transfusion reaction, develop TRALI, or adult respiratory distress syndrome (ARDS), or may have a higher infection risk as a result of receiv-ing blood products.
Clearly, major spine surgery can incur significant intra-operative blood loss. Surgeons and anesthesiologists can work together using a variety of techniques and agents to decrease this blood loss. The safety and efficacy pro-file of antifibrinolytics, plus rfVIIa, is promising for use in spine patients, although requires continued study and reporting. Decreasing blood loss and transfusion require-ments during major spine surgery should help reduce the overall complication rate in these patients.
References
1. Carson JL, Altman DG, Duff A, Noveck H, Weinsstein MP, Sonnerberg FA, Hudson JI, Provenzano G (1999) Transfusion complications: risk of bacterial infection associated with allogenic blood transfusion among patients undergoing hip fracture repair. Transfusion 39:694–701
2. Innerhofer P, Wallexzek L, Luz G, Hobisch-Hagen P, Benzer A, Stockl B, Hessenberger G, Nussbaumer W, Schoberberger W (1999) Transfusion complications: transfusion of Buffy coat-depleted blood components and risk of postoperative infection in orthopedic patients. Transfusion 39:625–631
3. Kopko PM, Marshall CS, Mackenzie MR, Holland PV, Popovsky MA (2002) Transfusion- related acute lung injury: report of a clinical look back investigation report of a clini-cal look- back investigation. J Am Med Assoc 287:15
4. Nahtomi-Shick O, Kostuik J, Winters B, Breder C, Sieber A, Sieber F (2001) Does intraoperative fluid management in spine surgery predict intensive care unit length of stay. J Clin Anesth 13:208–212
5. Zheng F, Cammisa F, Sandhu H, Girardi F, Khan S (2002) Factors predicting hospital stay, operative time, blood loss, and transfusion in patients undergoing revision posterior lumbar spine decompression fusion and segmental instru-mentation. Spine 27(8):818–824
6. Lee LA, Roth S, Posner KL, Cheney FW, Caplan RA, Newman NJ, Domino KB (2006) The American society of anesthesiologist postoperative visual loss registry. Anesthesi-ology 105:652–659
7. Goodnough LT, Rudnick S, Price T, Ballas S, Collins M, Crowley J, Kosmin M, Kruskall M, Lenes B, Menitove J, Silberstein L, Smith K, Wallas C, Abels R, Von Tress M (1989) Increase preoperative collection of autologous blood with recombinant human erythropoietin therapy. N Engl J Med 321(17):1163–1168
8. Goodnough LT, Marcus RE (1992) Effect of autological blood donation in patient undergoing elective spine surgery. Spine 17(2):172–174
9. Hur S, Huizenga B, Major M (1992) Acute normovolemic hemodilution combined with hypotensive anesthesia and other. Spine 17(8):867–873
10. Siller T, Dickson J, Erwin W (1996) Efficacy and cost con-sideration of intraoperative autologous transfusion in spina fusion for idiopathic scoliosis with pre-deposited blood. Spine 21(7):848–852
11. Simpson M, Georgopoulos G, Eilert R (1993) Intraoperative blood salvage in children and young adults undergoing spi-nal surgery with pre-deposited autologous blood: efficacy and cost effectiveness. J Pediatr Orthop 13:777–780
12. Kakiuchi M (2002) Intraoperative blood loss during cervical laminoplasty correlates with the vertebral intraosseous pres-sure. J Bone Joint Surg (BR) 84-B(4):518–520
13. Copley LA, Stephens RB, Safavi FZ, Newton PO (1999) Hemodilution as a method to reduce transfusion require-ments in adolescent spine fusion surgery. Spine 24(3): 219–222
14. Hobish-Hagen P, Wirletner B, Mair J, Luz G, Innerhofer P, Frischhut B, Ulmer H, Schobersberger W (1999) Conse-quences of acute normovolaemic hemodilution on hemosta-sis during major orthopaedic surgery. Br J Anesth 82(4):503–509
15. Cole J, Murray D, Snider R, Bassett G, Bridwell K, Lenke L (2003) Aprotinin reduced blood loss during spinal surgery in children. Spine 28(21):2482–2485
16. Murkin JM, Shannon NA, Bourne RB, Rorabeck CH, Cruickshank M, Wylie G (1995) Anesth Analg 80:343–348
17. Samama CM (2004) Aprotinin and major orthopedic sur-gery. Eur Spine J 13-S(1):S56–S61
18. Urban M, Beckman J, Gordon M, Urquhart B, Boachie-Adjei O (2001) The efficacy of antifibrinolytic in the reduc-tion of blood loss during complex adult reconstructive spine surgery. Spine 26(10):1152–1157
19. Dietrich W, Spath P, Zuhisdorf M, Dailchau H, Kirchhoff PG, Kuppe H, Preiss D, Mayer G (2001) Anaphylactic reactions to aprotinin re-exposure in cardiac surgery. Anesthesiology 95:64–71
20. Kokoszka A, Kuflik P, Bitan F, Casden A, Neuwirth M (2005) Evidence based review of the role of aprotinin in blood conservation during orthopaedic surgery. J Bone Joint Surg 87:1129–1136
21. Royston D, Van Haaften N, De Vooght P (2007) Aprotinin; friend or foe? A review of recent medical literature. Eur J Anaesthesiol 24:6–14
22. Okubadejo GO, Bridwell K, Lenke L, Buchowski JM, Fang D, Baldus C, Nielson C, Lee C (2007) Aprotinin may decrease blood loss in complex adult spinal deformity sur-gery but it may also increase the risk of acute renal failure. Spine 32(20):2265–2271
23. Food and Drug Administration, Regulatory administration November 26, 2007 http://www.fda.gov/bbs/topics/NEWS/2007/NEW01738.html. Aprotinin: FDA Informs of Ongoing Safety Review FDA Website 2007
24. Shapiro F, Zurakoski D, Sethna N (2007) Tranexamic acid diminishes intraoperative blood loss and transfusion in spi-nal fusion for duchenne muscular dystrophy scoliosis. Spine 32(20):2278–2283
25. Neilipovitz DT, Murto K, Hall L, Barrowman NJ, Splinter WM (2001) A randomized trial of tranexamic acid to reduce blood transfusion for scoliosis surgery. Anesth Analg 93: 82–87

1734.10 Blood Loss Management in Major Spine Surgery
26. Krohn CD, Sorensen R, Lange JE, Riise R, Bjornsen S, Brosstd F (2003) Tranexamic acid given into the wound reduces postoperative blood loss by half in major orthopae-dic surgery. Eur J Surg Suppl 588:57–61
27. Zufferey P, Merquiol F, Laporte S, Decousus H, Mismette P, Auboyer C, Samama CM, Molliex S (2006) Do antifibrinolytics reduce allogenic blood transfusion in orthopedic surgery? Anesthesiology 105(5):1034–1046
28. Saches B, Delacy D, Green J, Graham S, Ramsay J, Kreisler N, Kruse P, Khutoryansky N, Hu S (2007) Recombinant activated factor VII in spinal surgery a multi-center, randomized, double blind, placebo controlled dose escalation trial. Spine 32(21):2285–2293
29. Johnson R, Murphy M, Miller M (1989) Fusion and transfu-sion: an analysis of blood loss and autogous replacement during lumbar fusion. Spine 14(4):358–362

Part
Surgical Treatment: Other TechnologiesV

177M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_5.1, © Springer-Verlag Berlin Heidelberg 2010
Introduction
Today, we have many surgical options for treating symp-tomatic degenerative disc disease for those patients who fail adequate non-operative treatment. Though many of these technologies are new, they need to pass the test of time with positive objective outcome measures.
We know from the Kirkaldy-Willis’ degenerative cascade that there are many stages of degenerative disc disease. These range from the earliest stages of annular tears to the full-blown end stage degenerative disc dis-ease with marked disc space collapse. So where does disc replacement fit in the treat algorithm? Along with the gross physical changes of the disc described in the degenerative cascade, in recent years, a greater knowl-edge of the physiological changes within the disc and related pain mechanisms has continued to develop. At the same time, the number of treatment options is esca-lating. Years ago, the treatment for degenerative disc pain was limited to discectomy, anterior fusion with iliac crest autograft or allograft, posterior fusion typi-cally performed with autograft, and about the only option was with or without pedicle screw system. Now the number of options and techniques is much greater. While the new technologies are exciting, they also bring new challenges. Each has to be evaluated according to rigorous protocol to determine its effectiveness. This may be particularly true of “add-on” devices such as anterior lumbar plates, image-guided surgery, nucleus
replacements or disc implants following routine dis-cectomy. The real key to optimizing spine care likely lies in determining in which subgroups of patients are specific devices beneficial, or not, based on a firm understanding of the individual patient’s problem. Total disc replacement has a place in this continuum of painful disc degeneration and surgical options.
As with any non-emergent spinal problem, non-operative therapy should be the first line of treatment. This includes exercise, medication, physical therapy and patient education. If satisfactory pain relief is not achieved using these interventions, the next phase of care is based on more extensive diagnostic evaluation, typically MRI. Based on the results of physical exami-nation and imaging studies, the next step in the contin-uum of care is typically injections. In the future, at this point in the degenerative cascade, therapies based on tissue engineering may have a role. Such therapies may involve the injection of agents targeted to revitalize the water imbibing properties of a normal disc. While such interventions are under development, it will likely be years before they are commonly available.
In the absence of therapies based on tissue engi-neering, more direct manipulation of disc tissue may be pursued currently. There are multiple therapies available based on percutaneous approaches. There is no general consensus on the exact indications for these interventions to optimize outcome.
There has been some discussion on the role of interspinous devices in the treatment of symptomatic disc degeneration by unloading the disc. To date, the use of these devices for pain arising from the disc, rather than from stenosis, has not been investigated and the potential role of such implants remains unknown for painful disc degeneration.
How Disc Replacement Fits in the Treatment Algorithm for Degenerative Disc Disease: Refining Indications for Disc Replacement
Richard D. Guyer and Donna D. Ohnmeiss
R. D. Guyer (*) Texas Back Institute, 6020 West Parker Rd. 200, Plano, TX 75093, USA e-mail: [email protected]
5.1

178 R. D. Guyer and D. D. Ohnmeiss
Perhaps one of the most widely accepted spinal sur-geries is discectomy for the treatment of herniated disc. This pathology alone typically does not merit fusion or total disc replacement. More severe disc problems, pri-marily painful disc degeneration that is beyond simple disc herniation, is the phase of the degenerative con-tinuum that has traditionally been treated with lumbar fusion. This is likely the phase optimally treated with TDR. There has been two decades of experience with TDR in Europe, with good results generally reported, even in studies with more than 10-year follow-up [8, 12, 16]. Randomized trials in the United States have provided a direct comparison to fusion with TDR and found TDR to be as effective as fusion, or more effec-tive on some parameters [7, 18]. As with many surgical procedure, indications for these devices have been continually refined; a process that remains ongoing. Specific indications and contra-indications for TDR are discussed below in detail.
Indications
The ideal TDR candidate should have painful disc degen-eration at one or two lumbar segments. Discography is the method of choice to confirm the painful motion segment prior to intervention. The facet joints should be normal or have only mild degenerative changes. The build of the ideal candidate should be thin. This makes accessing the disc space for implantation much easier.
If a surgeon is not well-experienced with anterior lumbar spine surgery, it is suggested that the first cases selected for TDR should be performed at the L5-S1 level. Considering the vascular anatomy, this level is more eas-ily accessed than cephalad levels. After experience is gained at this level, higher levels may be addressed.
Contra-Indications
Osteoporosis
One of the most important contra-indications for TDR that must be respected is osteoporosis. At the very least, bone mineral density scanning for females more than 40 years of age and males more that 50 is advisable. A DEXA T-sore of less than −1.0 should exclude a patient from receiving a total disc replacement. Earlier, lower T-scores were allowed, but there has been an
increased awareness of the importance of ruling out patients who may have an increased risk of vertebral body fracture due to osteoporosis or osteopenia.
Spinal Deformity
To date, there is not much information available provid-ing firm criteria for TDR in patients with lumbar sco-liosis. In the Charité trial, curvature of 11° or more was used as an exclusion criteria [7]. The exact curvature that may be successfully treated with TDR is not known. However, one must be aware that the curvature may alter the loading and function of an artificial disc. Scoliosis of multiple levels may pose a particular challenge in trying to realign the spine with the devices. One possible appli-cation in scoliosis patients may be the use of TDR at the L5–S1 level in patients with previous multiple-level deformity correction above this segment, which has now become painful. This application of TDR has not been rigorously investigated. Spinal deformity due to tumour, trauma or fracture should not be treated with TDR due to potential biomechanical weakening of the bony structures of the segment(s) to be implanted.
Obesity
Obesity is an exclusion criterion for TDR. Body mass index (BMI) has been used to set limits for obesity. There is no data suggesting that heavy body weight compromises the function or safety of TDR. Actual weight or BMI may not really be the issue. The item of importance is the depth of the patient’s abdomen, i.e., the distance from the skin to the spine. There may be difficulty with device placement or a much larger inci-sion may be required to properly position the implant into the disc space. Certainly a large patient should not be included in a surgeon’s first few cases and very large patients should be avoided all together.
Disc Space Collapse
Disc space collapse is another issue to consider. Some collapse of the disc space is frequently associated with symptomatic disc degeneration and may be even more prevalent among patients with a previous discectomy. In fact, the ideal patient has some disc space narrowing, but there should be no bone-on-bone contact. The exact measurement of the disc space height that is ideal is not

1795.1 How Disc Replacement Fits in the Treatment Algorithm for Degenerative Disc Disease
defined. Bertagnoli et al. suggested a disc space height of at least 4 mm to be a good TDR candidate [2]. However, no basis for this particular value was provided. One reason for concern with severely collapsed disc spaces is that severe disc degeneration may be associ-ated with significant changes of the facet joints. This was not a concern with fusion since the operated seg-ment was to be rendered immobile, including the facets. However, with TDR, the facets will be mobile and if they are potentially a source of pain prior to TDR, they may be symptomatic following the procedure, compro-mising the overall treatment result. In patients with minimal facet changes, facet injections may be used pre-operatively to evaluate the joint as a possible pain generator. If the joint is painful, TDR is not indicated.
Psychological and Behavioural Issues
As with any spine surgery procedure, psychological factors may have a significant impact on TDR outcome. Ideally, TDR candidates should undergo pre-operative psychosocial screening conducted by a psychologist familiar with chronic back pain patients [6]. Part of the screening process is helpful in determining if the patient has realistic expectations for outcome. One other item, possibly related to behavioural characteristics, is the role of work status at the time of surgery. Anderson et al. reported that in a group of patients undergoing fusion for symptomatic disc degeneration, working at the time of surgery was related to a significantly improved outcome [1]. In our experience of comparing factors related to outcome in our clinic’s 20 best and 20 worst outcome of TDR, the only factor that signifi-cantly differed between the two groups was the length of time off work prior to surgery [15]. In an additional study, we have found that TDR or fusion patients oper-ated for symptomatic disc degeneration patients off work for more than 13 weeks improved from their pre-operative condition, but did not improve as much as patients off work for a shorter duration [14]. The differ-ence in outcome could not be attributed to having greater pain or disability prior to surgery. It may be that patients off work for a longer duration have a greater behavioural component to their symptoms.
Approach Considerations
TDRs are designed for implantation using an anterior to the disc space. As with any anterior spine surgery,
patients with prior abdominal surgery in the vicinity of the disc to be operated may not be good candidates for TDR due to the increased risk of vascular injury. Evaluation by the approach surgeon may be beneficial. Also, patients with calcification of the vessels may be ruled out as candidates for TDR due to the risk of vas-cular complications.
Anatomical Considerations
While not necessarily a strict contra-indication for TDR, one should assess the shape of the vertebral bod-ies and endplates. As discussed by Yue, there are sev-eral distinct endplate shapes [17]. Those with a “hook” on the posterior margin may pose difficulty in getting the TDR implanted as deeply posterior as desired. Also, this shape may be prone to fracture if the spike is “chipped” off during prosthetic implantation.
The shape of the vertebral body may make the selection of implant size more difficult. Vertebrae with a bevelled edge (Fig. 5.1.1), also referred to as “con-vex” by Yue [17], may require a smaller implant than
Fig. 5.1.1 The bevelled anterior edges of the vertebral bodies must be taken into account when determining the size of the implant to avoid compromised bone-implant contact area

180 R. D. Guyer and D. D. Ohnmeiss
what would typically be used for the size of the verte-bral body due to the lack of being able to get the implant seated firmly on the bevel.
The presence of deep Schmorl’s nodes should be assessed carefully. These may compromise optimal device placement as well as possibly compromise the structural integrity of the vertebral body, leading to bony fracture.
Who Not to Exclude from TDR
As more studies are performed, multiple variables have been investigated to determine their possible impact on the results of TDR. While severe facet joint changes should be a contra-indication for TDR, minor facet joint abnormalities do not appear to negatively influ-ence results [9, 11].
There had been some concern expressed over using TDR in patients with a previous discectomy. However, when comparing results of 24-month follow-up in patients with and without a history of previous discec-tomy, there was no difference in results [10]. The only added consideration in such patients is to check that there was no significant removal of the posterior ele-ments in the previous surgery to render the segment unstable, which is a contra-indication for TDR.
The US IDE trials limited the upper bound on age to 60 years. However, Bertagnoli et al. found that TDR resulted in significant improvement in pain and func-tion scores in patients more than 60 years of age [5]. However, in older patients special precautions should be rigorously adhered to. These include DEXA scan-ning for osteoporosis, careful evaluation to rule out stenosis and careful assessment of the anterior vessels so that the spine can be approached safely.
Smoking has generally been found to have a nega-tive impact on the results of lumbar fusion surgery, par-ticularly in patients who smoke more than a pack a day. However, in a study comparing results of TDR in smok-ers and non-smokers, both groups improved signifi-cantly with no significant differences between these two groups [4]. The authors did caution to be more aware of vascular problems. Also, it may be advisable to be more aggressive in screening smokers for osteoporosis.
Although excluded in the IDE trials, the use of TDR adjacent to a fusion does not appear to be problematic. Bertagnoli reported on a series of patients in whom
TDR was used to treat adjacent segment deterioration next to a previously fused segment [3]. The authors did emphasize the importance of ruling out pain arising from the facet, instrumentation or pseudoarthrosis prior to considering TDR. Another application of TDR in the treatment of two-level painful disc degeneration is using TDR at one level and a fusion at the other. Good results have been reported for this hybrid procedure [13].
Conditions for Which Fusion Should Be Considered Rather than TDR
While TDR does have a place in the continuum of care for painful disc degeneration, there are patients in the continuum who are beyond the point of being good TDR candidates. These patients may be fusion candi-dates. The conditions present in such patients include greater than Grade I spondylolisthesis, significant facet joint arthrosis or stenosis, scoliosis, fracture, facet joint pain, or instability following a laminectomy or other decompressive procedure.
Discussion
In the future there may be less invasive treatments, par-ticularly those related to tissue engineering, which may be indicated for the early stages of disc degeneration or disc disruption. Already we are seeing trials evaluat-ing nucleus replacements and post-discectomy repair implants. For discs that are degenerated beyond where these interventions may be applicable, TDR will likely remain a viable treatment option. At the more severe end of the degenerative spectrum, there are patients whose conditions are not amenable to TDR and in whom fusion remains the treatment of choice after non-operative interventions have failed. As with all of the emerging technologies, including TDR, interspinous spacers, tissue engineering, facet joint replacements and various other forms of posterior dynamic stabiliza-tion, there will be many iterations of ongoing studies refining the indications for the various implants.
In the ideal world where economics was not an issue, the surgeon would have many more options to offer their patients with advancing technology. For the earliest stages of symptomatic disc degeneration, other motion

1815.1 How Disc Replacement Fits in the Treatment Algorithm for Degenerative Disc Disease
preservation surgeries will suffice, but for the more advanced degeneration, TDR with the ensuing first gen-eration and now second generation will offer our patients more options instead of the traditional fusion. I believe, with newer designs of TDR and in combination with posterior reconstruction, fusion for painful disc degen-eration will be restricted to fewer and fewer patients.
References
1. Anderson PA, Schwaegler PE, Cizek D et al (2006) Work status as a predictor of surgical outcome of discogenic low back pain. Spine 31:2510–2515
2. Bertagnoli R, Kumar S (2002) Indications for full prosthetic disc arthroplasty: a correlation of clinical outcome against a variety of indications. Eur Spine J 11(suppl 2):S131–S136
3. Bertagnoli R, Yue JJ, Fenk-Mayer A et al (2006) Treatment of symptomatic adjacent-segment degeneration after lumbar fusion with total disc arthroplasty by using the prodisc pros-thesis: a prospective study with 2-year minimum follow up. J Neurosurg Spine 4:91–97
4. Bertagnoli R, Yue JJ, Kershaw T et al (2006) Lumbar total disc arthroplasty utilizing the ProDisc prosthesis in smokers versus nonsmokers: a prospective study with 2-year mini-mum follow-up. Spine 31:992–997
5. Bertagnoli R, Yue JJ, Nanieva R et al (2006) Lumbar total disc arthroplasty in patients older than 60 years of age: a prospective study of the ProDisc prosthesis with 2-year min-imum follow-up period. J Neurosurg Spine 4:85–90
6. Block AR, Gatchel RJ, Deardorff WW et al (2003) The psy-chology of spine surgery. American Psychological Association, Washington DC
7. Blumenthal S, McAfee PC, Guyer RD et al (2005) A prospec-tive, randomized, multicenter Food and Drug Administration investigational device exemptions study of lumbar total disc replacement with the CHARITE artificial disc versus lumbar fusion: part I: evaluation of clinical outcomes. Spine 30: 1565–1575
8. David T (2007) Long-term results of one-level lumbar arthroplasty: minimum 10-year follow-up of the CHARITE artificial disc in 106 patients. Spine 32:661–666
9. Elders GJ, Blumenthal SL, Guyer RD et al (2005) Effect of facet joint arthrosis on outcome after artificial disc replace-ment. Spine Arthroplasty Society, New York, NY
10. Leahy M, Zigler JE, Ohnmeiss DD et al (2008) Comparison of results of total disc replacement in post-discectomy patients versus patients with no previous lumbar surgery. Spine 33:1690–1693
11. Le Huec JC, Basso Y, Aunoble S et al (2005) Influence of facet and posterior muscle degeneration on clinical results of lumbar total disc replacement: two-year follow-up. J Spinal Disord Tech 18:219–223
12. Lemaire JP, Carrier H, Sariali el H et al (2005) Clinical and radiological outcomes with the Charite artificial disc: a 10-year minimum follow-up. J Spinal Disord Tech 18:353–359
13. Lhamby J, Guyer R, Zigler J et al (2006) Patients undergo-ing total disc replacement with spinal fusion at different lumbar levels. International Society for the Study of the Lumbar Spine, Bergen, Norway
14. Rohan MX, Ohnmeiss DD, Guyer RD et al (2007) Relationship between the length of time off work pre-operatively and clini-cal outcome at 24-month follow-up. North American Spine Society, Austin, Texas
15. Siddiqui S, Guyer R, Zigler J et al (2006) Factors related to the 20 best and 20 worst 24-month outcomes of total disc replacement in prospective FDA-regulated trials. Spine Arthroplasty Society, Montreal, Canada
16. Tropiano P, Huang RC, Girardi FP et al (2005) Lumbar total disc replacement. Seven to eleven-year follow-up. J Bone Joint Surg Am 87:490–496
17. Yue J, Bertagnoli R, Oetgen M et al (2007) Does vertebral endplate morphology influence clinical and radiographic outcomes in lumbar disc arthroplasty? An initial assessment of a novel classification system of lumbar endplate morphol-ogy. Spine Arthroplasty Society, Berlin, Germany
18. Zigler J, Delamarter R, Spivak JM et al (2007) Results of the prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of the ProDisc-L total disc replacement versus circumferential fusion for the treatment of 1-level degenerative disc disease. Spine 32:1155–1162

183M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_5.2, © Springer-Verlag Berlin Heidelberg 2010
Evaluating the scientific merit of a new technology early in its life cycle is important for a clinician considering incorporating these techniques into practice. The distinc-tion between marketing hype and true scientific support-ing evidence is sometimes blurred. Understanding the strength and quality of evidence that a new technique may have over older tried and established methods is paramount and understand the clinical value and risk ben-efit ratio of new techniques and the value such techniques may or may not give to one’s practice and to patients.
The goal of evidence-based medicine is to apprize and use clinical research findings to aid making deci-sions about the care of individual patients. Evidence-based medicine (EBM) combines the physician’s clinical experience, with the best available evidence, and patient values [1, 2]. The process of EBM involves translation of a specified problem into an answerable question and systematic retrieval of best evidence available [3]. Clinical findings are raked based on the strength of scientific methodology employed in per-forming research and developing conclusions. Using the EBM approach, clinicians can choose the best available evidence when making clinical decisions. Armed with this knowledge, the medical practitioner and the patient can make a well-informed decision.
In the ideal EBM model, the best available evidence from the literature is combined with clinical experi-ence and patients’ values. When dealing with new technology, there is, however, a lack of physician expe-rience. Patient values may be artificially manipulated and overly optimistic due to marketing and advertising,
leading to the misconception that “newest means best”. Under such circumstances, it becomes even more imperative for a clinician embarking on the use of new technology, to fully understand what “best evidence” exists for newer techniques. This distortion of the related values of the EBM tripod, physician’s experi-ence, best evidence, and patient values, is obvious in the early introduction of motion technology. Few physi-cians have little if any experience with these techniques or devices. Patients have been bombarded by the lay press and manufacturers representations that artificial discs and other parts replacement of the spine will be the answer to their misery and disability. In an attempt to determine the level of the best existing evidence for several factors that may affect outcomes, the authors undertook this study. Understanding the strengths and weaknesses of the available literature can better allow the medical practitioner and the patient to make well-informed decisions regarding treatment options.
In an attempt to get to the heart of the existing evi-dence about a variety of clinical factors that might affect the outcomes of artificial disc replacement for the lum-bar spine, we posed eleven questions and undertook a systematic review of the existing literature [4]. Those questions were grouped in three main categories: (a) patient selection issues, (b) surgical technique issues, and (c) motion technology issues. Sorting through med-ical literature to obtain answers can often be difficult. Research studies are susceptible to invalid conclusions resulting from bias, confounding or chance. With the introduction of evidence-based medicine techniques, however, the medical literature can be sorted into levels of evidence based on scientific merit. Higher level studies minimize bias, confounding and chance mak-ing their conclusions more likely reliable. By the very nature of their design, lower level studies do not address
Clinical Factors that May Affect Outcome in Lumbar Total Disc Replacement. What Is the Evidence?
Michael R. Zindrick, Mark Lorenz, Leonard I. Voronov, Michael N. Tzermiadianos, and Alexander Hadjipavlou
M. N. Tzermiadianos (*) 45, Eleftherias Square (Electra BLD, 1st floor), 71201 Heraklion, Crete, Greece e-mail: [email protected]
5.2

184 M. R. Zindrick et al.
bias, confounding and chance making their results more prone to error. Higher level studies, however, may also have unavoidable methodological flaws. In the ADR literature, the Food and Drug Administration (FDA) Investigational Device Exemption (IDE) studies represent the highest quality evidence available [5, 6]. Those studies are randomized, controlled, and use vali-dated outcome measures with a minimum of 2 year follow-up. Entry criteria and patient randomization for the studies is generally good. Lacking in all studies, however, is blinding. The reason for lack of blinding can be easily understood; nonetheless, this exerts a bias on outcome and should be considered when weighing their conclusions.
We performed a thorough review of the clinical litera-ture between January 1990 and May 2007 on peer
reviewed literature in English language [4]. Data that were only in abstract form was not used. Duplicate reports were eliminated if there were prior studies that presented the same group of patients and the most current report was used. If the authors reported a subset of a multi- centre study, the largest multi-centre series data available were used. Only studies including data addressing the above framed questions were included in this review.
We retrieved and reviewed 76 papers; 49 of them were excluded from our study as they did not include relevant information, or were duplicates [4]. The remain-ing 27 papers were ranked into appropriate evidence lev-els using the modification of Sackett grading system provided in the J Bone Joint Surg Am, January 2003 [7]. Briefly summarized, Level I studies are randomized, controlled clinical trials. Level II studies are pro spective
Table 5.2.1 The articles included in this review were ranked by level of evidence, study design, follow-up, and outcome measures
Author Level No pts
Study design
F.U. Lost at F.U. (%)
Outcome measures
Charité
Tortolani 2007 [8] I Prognostic 276 Prosp 2 years Heterotopic ossificationTrouillier 2006 [9] I Prognostic 13 Prosp 6 months Facet subchondral bone densityMcAfee 2005 [10] I Therapeutic 205– 99 Prosp 2 years 8.5 ODI, SF36Shim 2007 [11] III Therapeutic 61 Retro 3 years 6.5 ODIDavid 2007 [12] IV Therapeutic 108 Retro 13.2 year 2 Non-validatedPutzier 2006 [13] IV Therapeutic 71 Retro 17 years 25 ODIRegan 2005 [14] IV Therapeutic 100 Prosp 6–24 months ODILemaire 2005 [15] IV Therapeutic 107 Retro 11.3 years 7 Non-validatedVan Ooij 2003 [16] IV Therapeutic 27 Retro 7.5 years Non-validatedScott 2000 [17] IV Therapeutic 14 Retro 18–68 months 28.50 Non-validatedZeegers 1999 [18] IV Therapeutic 50 Prosp 2 years 8 Non-validatedLemaire 1997 [19] IV Therapeutic 105 Retro 4 years Non-validatedCinotti 1996 [20] IV Therapeutic 46 Retro 3.2 years Non-validated
ProDisc
Patel 2006 [21] I Prognostic 52 Prosp 2 years ODI, CT scanHuang 2006 [22] III Prognostic 64 Retro 8.7 years 34 Radiographic reviewHuang 2005 [23] III Prognostic 64 Retro 8.6 years 41 Stauffer-Coventry score, ODISiepe 2007 [24] IV Therapeutic 99 Prosp 2 years ODISiepe 2006 [25] IV Therapeutic 94 Prosp 3 years 2 ODI, SF36Chung 2006 [26] IV Therapeutic 38 Prosp 37 months 5 ODIBertagnoli 2006 [27] IV Therapeutic 22 Prosp 2 years 0 ODIBertagnoli 2005 [28] IV Therapeutic 118 Prosp 2 years 12 ODIBertagnoli 2005 [29] IV Therapeutic 29 Prosp 2 years 14 ODITropiano 2005 [30] IV Therapeutic 64 Retro 8.7 years 14 Non-validatedTropiano 2003 [31] IV Therapeutic 53 Prosp 1.4 years ODIBertagnoli 2002 [32] IV Therapeutic 108 Prosp 3months–2 years ODIMayer 2002 [33] IV Therapeutic 34 Prosp 1 year 23.5 ODI
Maverick
Le Huec 2005 [34] IV Therapeutic 64 Prosp 2 years 0 ODI
ODI oswestry disability index; Prosp prospective study; Retro retrospective study; CT Computed Tomography; FU Follow-up; pts Patients

1855.2 Clinical Factors that May Affect Outcome in Lumbar Total Disc Replacement. What Is the Evidence?
non-randomized comparative studies. Level III studies are retrospective comparative studies or case-controlled studies. Level IV includes case series, with no compari-son group. Level V evidence, which refers to expert opinions, was not included in the present study. Previous reviews on ADR were also not included. Articles were graded according to the type of study (therapeutic, prognostic, etc) and the level of evidence (I–IV) by two independent reviewers. We also listed other variables that may affect study quality, especially in level IV studies, such as the study design, follow-up period, per-centage of patients lost at follow-up, and the use of validated outcome measures (Table 5.2.1).
Patient Selection Issues
(a) Is the outcome after single segment implantation similar to multi-segmental implantation? Ten level IV studies were found (Table 5.2.2). Three studies [20, 24, 26] report inferior results with multi-segmental implan-tations , while six studies [15, 18, 28–31, 33] report similar results . Therefore, available studies evaluating the question of single vs. multilevel surgery provide conflicting results.
(b) Does spinal level of ADR affect outcome? Two pro-spective, level IV studies were found. Regan et al. [13] in a study of 100 patients implanted with Charité, report no statistical difference in outcome when L4-L5 was com-pared to L5-S1 at 6–24 months of follow-up [14]. Siepe et al. [24] in a study of 99 patients with ProDisc II with a mean 2 year follow-up reported a trend towards better outcomes at L4-L5 when compared to L5-S1 [24].(c) Does patients’ age affect outcome? Eight level IV studies were found (Table 5.2.3). Younger age was a favourable predictive factor in three studies [18, 25, 34], while was a negative factor in one study [30]. Patient age did not affect outcome in four studies [17, 26, 27, 31]. Some authors report higher complication rates in older patients, as lordosis enhancement after implanta-tion can exacerbate spinal stenosis, and compromised bone quality can increase the risk of subsidence [27]. In conclusion, the role of patients’ age remains unclear; however, the possibility of higher complications and the morbidity of additional surgical interventions in older patients should be considered in decision making.(d) Does prior surgery affect outcome? Twelve level IV studies were found (Table 5.2.4). Prior surgery had a negative effect on outcome in six studies [12, 20, 29–31, 34], while it had no effect on outcome in five studies [19, 25, 26, 28, 33]. In one study, prior surgery
Table 5.2.2 Effect of number of levels implanted in clinical outcomes
Author Level Study design FU No pts Effect of multi-segmental implantation on outcome
Charité
Cinotti 1996 [20] IV Retro 3.2 years 1 level: 36 Inferior results2 levels: 10
Lemaire 2005 [15] IV Retro >10 years 1 level: 54 No difference2 level: 45
Zeegers 1999 [18] IV Prosp 2 years 1 level: 29 No difference2 level: 18
ProDisc
Siepe 2007 [24] IV Prosp 2 years 1 level: 79 Inferior results2 level: 20
Chung 2006 [26] IV Prosp 2 years 1 level: 25 Inferior results2 level: 11
Bertagnoli 2005 [28] IV Prosp 2 years 1 level: 106 No differenceBertagnoli 2005 [29] IV Prosp 2 years ³ 2 levels: 25Tropiano 2005 [30] IV Prosp 8.7 years 1 level: 35 No difference
³ 2 levels: 20Tropiano 2003 [31] IV Prosp 1–2 years 1 level: 40 No difference
³ 2 levels: 13Mayer 2002 [33] IV Prosp 1 year 1 level: 31 No difference
³ 2 level: 3

186 M. R. Zindrick et al.
Table 5.2.4 Effect of prior surgery on patients’ outcome
Author Level Study design
FU No pts with (+) or without (−) previous surgery
Effect of previous surgery on outcome
Charité
Cinotti 1996 [20] IV Retro 3.2 years (+) : 24 Negative effect(−): 22
David 2007 [12] IV Retro 13.2 years (+): 44 Negative effect in patients with > 2 previous surgeries(−): 62
Zeegers 1999 [18] IV Prosp 2 years (+): 27 Negative effect at 1 year(−): 33 No effect at 2 years
Lemaire 1997 [19] IV Retro 4 years (+) : 55 No effect(−): 50
ProDisc
Bertagnoli 2005 [29] IV Prosp 2 years (+): 17 Negative effect(−): 12
Tropiano 2005 [30] IV Prosp 8.7 years (+): 28 Negative effect(−): 27
Tropiano 2003 [31] IV Prosp 1.4 years (+): 11 90% satisfactory results(−): 33 97% satisfactory result
Mayer 2002 [33] IV Prosp 1 year (+): 9 No effect(−): 25
Bertagnoli 2005 [28] IV Prosp 2 years (+): 60 No effect(−): 46
Siepe 2006 [25] IV Prosp 3 years (+): 17 No effect(−): 75
Chung 2006 [26] IV Prosp 2 years (+):7 No effect(−):29
Maverick
Le Huec 2005 [34] IV Prosp 2 years 64 Negative effect
Table 5.2.3 Effect of patients’ age on clinical outcomes
Author Level Study design FU No pts Effect of age on outcome
Charité
Zeegers 1999 [18] IV Prosp 2 years 46 Patients < 45 years had better outcomeScott 2000 [17] IV Retro 4 years 14 Age > 45 did not affect outcome
ProDisc
Siepe 2006 [25] IV Prosp 3 years 92 Patients < 40 years had better outcomeTropiano 2005 [30] IV Prosp 8.7 years 55 Patients > 45 years had better outcomeChung 2006 [26] IV Prosp 2 years 36 Age did not affect outcomeBertagnoli 2006 [27] IV Prosp 2 years 22 Age did not affect outcomeTropiano 2003 [31] IV Prosp 1.4 years 53 Age > 50 did not affect outcome
Maverick
Le Huec 2005 [34] IV Prosp 2 years 64 Young patients had better outcome

1875.2 Clinical Factors that May Affect Outcome in Lumbar Total Disc Replacement. What Is the Evidence?
had a negative effect on outcome at 1 year and no effect at 2 years follow-up [18]. Most of the studies used non-validated outcome measures [12, 18–20, 30].(e) Does preoperative facet degeneration affect out-come? Only one level IV study was found. Le Huec et al. [34] in a prospective study of 64 Maverick ADR reported that mild or moderate facet osteoarthritis (grade 1 or 2, on the 0–3 Fujiwara scale), did not influence outcome at 2 years follow-up. Patients with severe facet arthrosis had worse outcome, but their number was small to reach conclusive evidence. Therefore, the role of pre-exist-ing facet arthrosis is still obscure. Pre-existing facet arthrosis is currently a contraindication to ADR; how-ever, one study suggests that mild to moderate facet degeneration does not influence ADR outcomes [34]. Clinically significant facet arthrosis is reported to be present in 66% of patients undergoing fusion surgery [35]. Nevertheless, the extent of facet degeneration that can be accepted in motion preservation surgery remains to be evaluated, as most of the candidates for this surgery are expected to have some degree of facet arthrosis.
Surgical Technique Issues
(a) Does prosthesis positioning affect ROM or outcome? One level I study and seven level IV studies were found (Table 5.2.5). There is level I evidence that accuracy of placement affects both clinical outcome and range of motion after ADR [10]. Data from level IV studies are conflicting; three studies reported that placement can affect long-term outcome leading to the development of symptomatic facet arthrosis [12, 15] or decreased ROM [20], while four studies showed no effect [18, 21, 26, 34]. Therefore, higher level studies appear to support the importance of surgical precision upon clinical outcome.
Motion Technology Issues
(a) Does ROM of the implanted segment affect out-come? One level III and two Level IV studies were found (Table 5.2.6). A level III prognostic study reports
Table 5.2.6 Effect of range of motion after implantation on clinical outcome
Study Level design FU No pts ROM Effect of ROM on outcome
Charité
Putzier 2006 [13] IV Therapeutic Retro 17 year 53 Functional–mobile implants: 17%
Patients with functional implants were less satisfied
ProDisc
Huang 2005 [23] III Prognostic Retro 8.6 year 39 ROM>5°: 28% Better outcomes with ROM >5°Chung 2006 [26] IV Therapeutic Prosp 3 year 36 Better outcomes with higher ROM
Table 5.2.5 Effect of implant positioning on Range of motion (ROM) and clinical outcome
Author Level Study design FU No pts Effect of placement
Charité
McAfee 2005 [10] I Prosp 2 years 276 Affects both outcomes and ROMDavid 2007 [12] IV Retro 13.2 years 106 Anterior placement is correlated with the
development of symptomatic facet arthrosisLemaire 2005 [15] IV Retro 10 years 100 All patients that developed facet arthrosis had
non-ideal placementZeegers 1999 [18] IV Prosp 2 years 50 No effectCinotti 1996 [20] IV Retro 3.2 years 46 Affects ROM
ProDisc
Patel 2006 [21] IV Prosp 2 years 52 No effectChung 2006 [26] IV Prosp >2 years 36 No effect
Maverick
Le Huec 2005 [34] IV Prosp 2 years 64 No effect if implant was between 0 and 7 mm from the posterior wall
ROM (Range of motion)
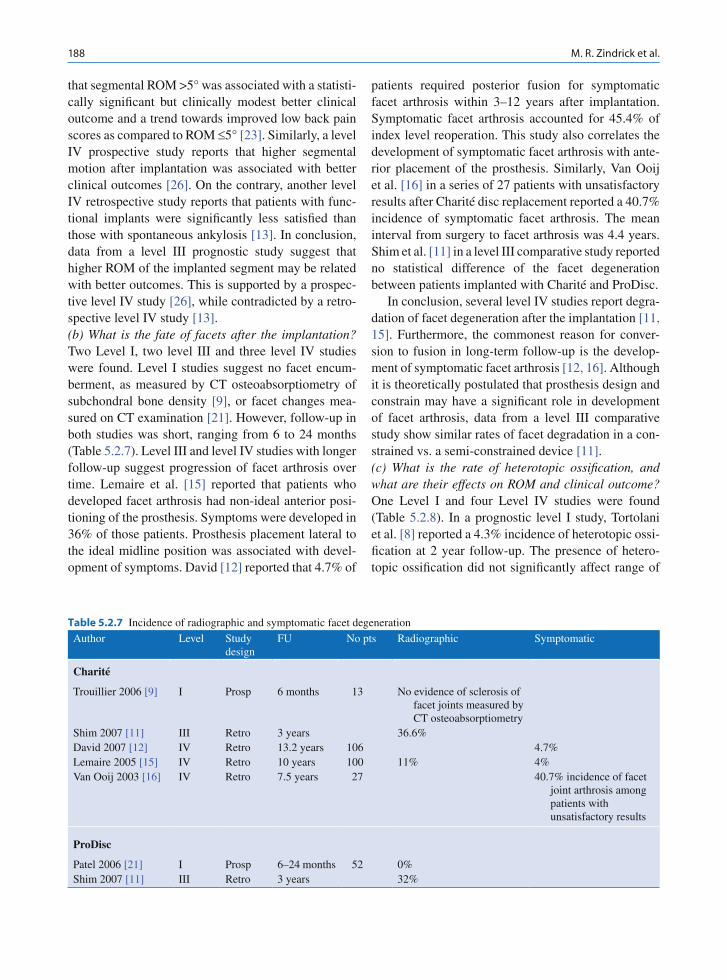
188 M. R. Zindrick et al.
that segmental ROM >5° was associated with a statisti-cally significant but clinically modest better clinical outcome and a trend towards improved low back pain scores as compared to ROM £5° [23]. Similarly, a level IV prospective study reports that higher segmental motion after implantation was associated with better clinical outcomes [26]. On the contrary, another level IV retrospective study reports that patients with func-tional implants were significantly less satisfied than those with spontaneous ankylosis [13]. In conclusion, data from a level III prognostic study suggest that higher ROM of the implanted segment may be related with better outcomes. This is supported by a prospec-tive level IV study [26], while contradicted by a retro-spective level IV study [13].(b) What is the fate of facets after the implantation? Two Level I, two level III and three level IV studies were found. Level I studies suggest no facet encum-berment, as measured by CT osteoabsorptiometry of subchondral bone density [9], or facet changes mea-sured on CT examination [21]. However, follow-up in both studies was short, ranging from 6 to 24 months (Table 5.2.7). Level III and level IV studies with longer follow-up suggest progression of facet arthrosis over time. Lemaire et al. [15] reported that patients who developed facet arthrosis had non-ideal anterior posi-tioning of the prosthesis. Symptoms were developed in 36% of those patients. Prosthesis placement lateral to the ideal midline position was associated with devel-opment of symptoms. David [12] reported that 4.7% of
patients required posterior fusion for symptomatic facet arthrosis within 3–12 years after implantation. Symptomatic facet arthrosis accounted for 45.4% of index level reoperation. This study also correlates the development of symptomatic facet arthrosis with ante-rior placement of the prosthesis. Similarly, Van Ooij et al. [16] in a series of 27 patients with unsatisfactory results after Charité disc replacement reported a 40.7% incidence of symptomatic facet arthrosis. The mean interval from surgery to facet arthrosis was 4.4 years. Shim et al. [11] in a level III comparative study reported no statistical difference of the facet degeneration between patients implanted with Charité and ProDisc.
In conclusion, several level IV studies report degra-dation of facet degeneration after the implantation [11, 15]. Furthermore, the commonest reason for conver-sion to fusion in long-term follow-up is the develop-ment of symptomatic facet arthrosis [12, 16]. Although it is theoretically postulated that prosthesis design and constrain may have a significant role in development of facet arthrosis, data from a level III comparative study show similar rates of facet degradation in a con-strained vs. a semi-constrained device [11].(c) What is the rate of heterotopic ossification, and what are their effects on ROM and clinical outcome? One Level I and four Level IV studies were found (Table 5.2.8). In a prognostic level I study, Tortolani et al. [8] reported a 4.3% incidence of heterotopic ossi-fication at 2 year follow-up. The presence of hetero-topic ossification did not significantly affect range of
Table 5.2.7 Incidence of radiographic and symptomatic facet degeneration
Author Level Study design
FU No pts Radiographic Symptomatic
Charité
Trouillier 2006 [9] I Prosp 6 months 13 No evidence of sclerosis of facet joints measured by CT osteoabsorptiometry
Shim 2007 [11] III Retro 3 years 36.6%David 2007 [12] IV Retro 13.2 years 106 4.7%Lemaire 2005 [15] IV Retro 10 years 100 11% 4%Van Ooij 2003 [16] IV Retro 7.5 years 27 40.7% incidence of facet
joint arthrosis among patients with unsatisfactory results
ProDisc
Patel 2006 [21] I Prosp 6–24 months 52 0%Shim 2007 [11] III Retro 3 years 32%

1895.2 Clinical Factors that May Affect Outcome in Lumbar Total Disc Replacement. What Is the Evidence?
motion or clinical outcome. Five level IV studies were also found. Cinotti et al. [20] reported a 15.2% inci-dence of periannular ossifications; and 57% of patients with ossifications had spontaneous interbody fusion. However, periannular ossifications did not affect clini-cal outcome. David [10] reported partial ossification in 3.8% of patients and complete ossification with spontaneous fusion in 2.8% of patients. Ossifications occurred only in patients treated with postoperative brace and activities restriction, while it was not noted in patients who had early active physiotherapy [12]. Putzier et al. [13] reported that 60% of patients had spontaneous fusion and another 13% had signs of pos-sible or likely motion impairment. Patients with func-tional implants without signs of heterotopic ossification were less satisfied than those with spontaneous anky-losis. Lemaire et al. [15] reported a 3% incidence of heterotopic ossification, without any cases of sponta-neous arthrodesis. However, 9% of patients in that study had ROM <2°, which is beyond the measure-ment error accepted by the FDA.(d) What is the incidence of adjacent level degenera-tion after ADR? Two level III and six level IV studies
were found (Table 5.2.9). Cinotti et al. [20] reported a 0% incidence in 3.2 years of follow-up based on MRIs performed on 10 patients out of the 46 included in the authors’ series. However, no selection criteria for the 10 patients were provided. Other studies with more than 3 years of follow-up, report that the incidence of ALD ranges between 17 [13] and 28.6% [11]. Additional surgery was required in 2–3% of patients in two series [12, 15].(e) What is the effect of motion preservation on adja-cent level degeneration? Only two level IV studies were found (Table 5.2.10). Data suggest that preserva-tion of motion after ADR may reduce the risk for adja-cent level degeneration [13, 22].
One of the main theoretical advantages of disc arthroplasty over spinal fusion is the prevention of the accelerated degeneration of the adjacent segments. The surprisingly high incidence of adjacent level degenera-tion reported in these studies suggests that disc arthro-plasty may not have a protective effect on the adjacent segments as initially thought. In contrast, two level IV studies with long follow-up suggest that preservation of motion may have a prophylactic effect on adjacent discs
Table 5.2.9 Reported rate of adjacent level degeneration (ALD) after ADR
Author Level Study design
FU No pts Radiographic ALD (%)
Surgery for ALD (%)
Charité
Shim 2007 [11] III Retro 3 years 33 19.4David 2007 [12] IV Retro 13.2 years 106 2.8Lemaire 2005 [15] IV Retro 11.3 years 100 2Putzier 2006 [13] IV Retro 17 years 53 17Cinotti 1996 [20] IV Retro 3.2 years 10/46 0
ProDisc
Shim 2007 [11] III Retro 3 years 24 28.6Huang 2006 [22] IV Retro 8.7 years 42 24Bertagnoli 2002 [32] IV Prosp 3 months–2 years 108 9.2
Table 5.2.8 Incidence of heterotopic ossification (HO) and its effect on range of motion (ROM) and clinical outcome
Author Level Study design
FU No pts H.O. (%) Effect on ROM Effect on outcome
Charité
Tortolani 2007 [8] I Prosp 2 years 276 4.3 No effect No effectDavid 2007 [12] IV Retro 13.2 years 106 6.6 NegativePutzier 2006 [13] IV Retro 17 years 53 73 Negative NegativeLemaire 2005 [15] IV Retro 11.3 years 100 3Cinotti 1996 [20] IV Retro 3.2 years 46 15.2 Negative No effect

190 M. R. Zindrick et al.
[13, 23]. Huang et al. [23] suggested that ROM ³5° is a plausible crucial threshold to prevent adjacent level degeneration. The motion data provided to FDA from the IDE of Charité show that at 24 months after implan-tation 33% of patients had less than 5° of ROM [36]. Since it may take more than a decade for symptomatic junctional degeneration to develop, longer follow-up period is necessary to shed more light on the effect of ADR vs. fusion in randomized prospective trials.
Conclusions
Not surprisingly, the majority of the experimental stud-ies were level IV, with only limited higher level stud-ies. This reflects the difficulties in performing a randomized controlled trial, as well as the reluctance among clinicians and patients to deviate from their concepts of what the optimum treatment should be. In the absence of higher level studies, most of the best evidence concerning ADR comes from level IV stud-ies (Table 5.2.1). Therefore, existing evidence does not allow drawing definite conclusions in the majority of the clinical questions regarding indications and factors that may affect outcomes. Where feasible, conclusions are mainly drawn from lower level, least reliable evi-dence. Highest quality data are short term and longer term data are of lower quality and in many instances conflicting. This lower level data, however, are plenti-ful and often quoted.
The clinician must understand when taking impor-tant clinical decisions that the scientific ground on which he/she is treading may not be as solid, as one would wish. There exist no long-term studies of high level scientific merit that demonstrate long-term effi-cacy of motion preservation technology over traditional techniques. Additionally, there exist limited data to
suggest or support that junctional breakdown above fusions is clinically altered or is different from the nor-mal degenerative process expected over ensuing period of time. There are limited data to suggest that motion technologies prevent the natural progression of degen-eration, either at the index level or at adjacent segments, at this time. However, it is important to clarify that lack of evidence is not synonymous to lack of benefit. High-level studies with long-term follow-up are necessary to shed further light on important clinical issues.
References
1. Straus S, Richardson W, Glasziou P, Haynes B (2005) Evidence based medicine, 3rd edn. Elsevier, Churchill Livingstone, London
2. Sackett DL, Straus S, Richardson W et al (2000) Evidence-based medicine. How to practice and teach EBM. Churchill Livingstone, New York
3. Dawes M, Summerskill W, Glasziou P et al (2005) Sicily statement on evidence-based practice. BMC Med Educ 5:1
4. Zindrick MR, Tzermiadianos MN, Voronov LI et al (2008) An evidence-based medicine approach in determining fac-tors that may affect outcome in lumbar total disc replace-ment. Spine 33(11):1262–1269
5. Blumenthal S, McAfee PC, Guyer RD et al (2005) A prospec-tive, randomized, multicenter Food and Drug Administration investigational device exemptions study of lumbar total disc replacement with the CHARITÉ artificial disc versus lumbar fusion: part I: evaluation of clinical outcomes. Spine 30: 1565–1575
6. Zigler J, Delamarter R, Spivak JM et al (2007) Results of the prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of the ProDisc-L total disc replacement versus circumferential fusion for the treatment of 1-level degenerative disc disease. Spine 32:1155–1163
7. Wright JG, Swiontkowski MF, Heckman JD (2003) Introducing levels of evidence to the journal. J Bone Joint Surg Am 85:1–3
8. Tortolani PJ, Cunningham BW, Eng M et al (2007) Prevalence of heterotopic ossification following total disc replacement.
Table 5.2.10 Effect of motion preservation on the incidence of adjacent level degeneration (ALD)
Author Level Study design FU No pts Radiographic ALD
Charité
Putzier 2006 [13] IV Retro 17 years 53 20% in patients with spontaneous fusion0% in patients with ROM >3°
ProDisc
Huang 2006 [22] IV Retro 8.7 years 42 34% in patients with ROM <5°0% in patients with ROM >5°
1915.2 Clinical Factors that May Affect Outcome in Lumbar Total Disc Replacement. What Is the Evidence?
A prospective, randomized study of two hundred and sev-enty-six patients. J Bone Joint Surg Am 89(1):82
9. Trouillier H, Kern P, Refior HJ, Muller-Gerbl M (2006) A prospective morphological study of facet joint integrity following intervertebral disc replacement with the CHARITÉ artificial disc. Eur Spine J 15:174–182
10. McAfee PC, Cunningham B, Holsapple G, Adams K et al (2005) A prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of lumbar total disc replacement with the CHARITÉ artifi-cial disc versus lumbar fusion: part II: evaluation of radio-graphic outcomes and correlation of surgical technique accuracy with clinical outcomes. Spine 30:1576–1583
11. Shim CS, Lee SH, Shin HD et al (2007) Charité versus ProDisc: a comparative study of a minimum 3-year follow-up. Spine 32:1012–1018
12. David T (2007) Long-term results of one-level lumbar arthroplasty: minimum 10-year follow-up of the CHARITÉ artificial disc in 106 patients. Spine 32(6):661–666
13. Putzier M, Funk JF, Schneider SV, Gross C et al (2006) Charité total disc replacement-clinical and radiographical results after an average follow-up of 17 years. Eur Spine J 15:183–195
14. Regan JJ (2005) Clinical results of Charité lumbar total disc replacement. Orthop Clin North Am 36:323–340
15. Lemaire JP, Carrier H, Ali el-HS et al (2005) Clinical and radiological outcomes with the charitetrade mark artificial disc: A 10-year minimum follow-up. J Spinal Disord Tech 18:353–359
16. van Ooij A, Oner FC, Verbout AJ (2003) Complications of artificial disc replacement: a report of 27 patients with the SB Charité disc. J Spinal Disord Tech 16:369–383
17. Sott AH, Harrison DJ (2000) Increasing age does not affect good outcome after lumbar disc replacement. Int Orthop 24:50–53
18. Zeegers WS, Bohnen LM, Laaper M, Verhaegen MJ (1999) Artificial disc replacement with the modular type SB Charité III: 2-year results in 50 prospectively studied patients. Eur Spine J 8:210–217
19. Lemaire JP, Skalli W, Lavaste F et al (1997) Intervertebral disc prosthesis. Results and prospects for the year 2000. Clin Orthop Relat Res 337:64–76
20. Cinotti G, David T, Postacchini F (1996) Results of disc pros-thesis after a minimum follow-up period of 2 years. Spine 21:995–1000
21. Patel VV, Andrews C, Pradhan BB et al (2006) Computed tomography assessment of the accuracy of in vivo place-ment of artificial discs in the lumbar spine including radio-graphic and clinical consequences. Spine 31:948–953
22. Huang RC, Tropiano P, Marnay T et al (2006) Range of motion and adjacent level degeneration after lumbar total disc replacement. Spine J 6:242–247
23. Huang RC, Girardi FP, Cammisa FP Jr et al (2005) Correlation between range of motion and outcome after lumbar total disc replacement: 8.6-year follow-up. Spine 30: 1407–1411
24. Siepe CJ, Mayer HM, Heinz-Leisenheimer M, Korge A (2007) Total lumbar disc replacement: different results for different levels. Spine 32:782–790
25. Siepe CJ, Mayer HM, Wiechert K, Korge A (2006) Clinical results of total lumbar disc replacement with ProDisc II: three-year results for different indications. Spine 31: 1923–1932
26. Chung SS, Lee CS, Kang CS (2006) Lumbar total disc replace-ment using ProDisc II: a prospective study with a 2-year mini-mum follow-up. J Spinal Disord Tech 19:411–415
27. Bertagnoli R, Yue JJ, Nanieva R et al (2006) Lumbar total disc arthroplasty in patients older than 60 years of age: a prospective study of the ProDisc prosthesis with 2-year min-imum follow-up period. J Neurosurg Spine 4:85–90
28. Bertagnoli R, Yue JJ, Shah RV et al (2005) The treatment of disabling single-level lumbar discogenic low back pain with total disc arthroplasty utilizing the Prodisc prosthesis: a pro-spective study with 2-year minimum follow-up. Spine 30: 2230–2236
29. Bertagnoli R, Yue JJ, Shah RV et al (2005) The treatment of disabling multilevel lumbar discogenic low back pain with total disc arthroplasty utilizing the ProDisc prosthesis: a pro-spective study with 2-year minimum follow-up. Spine 30: 2192–2199
30. Tropiano P, Huang RC, Girardi FP et al (2005) Lumbar total disc replacement. Seven to eleven-year follow-up. J Bone Joint Surg Am 87:490–496
31. Tropiano P, Huang RC, Girardi FP, Marnay T (2003) Lumbar disc replacement: preliminary results with ProDisc II after a minimum follow-up period of 1 year. J Spinal Disord Tech 16:362–368
32. Bertagnoli R, Kumar S (2002) Indications for full prosthetic disc arthroplasty: a correlation of clinical outcome against a variety of indications. Eur Spine J 11(suppl 2):S131–S136
33. Mayer HM, Wiechert K, Korge A, Qose I (2002) Minimally invasive total disc replacement: surgical technique and preliminary clinical results. Eur Spine J 11(suppl 2): S124–S130
34. Le Huec JC, Basso Y, Aunoble S et al (2005) Influence of facet and posterior muscle degeneration on clinical results of lumbar total disc replacement: two-year follow-up. J Spinal Disord Tech 18:219–223
35. Huang RC, Lim MR, Girardi FP, Cammisa FP Jr (2004) The prevalence of contraindications to total disc replacement in a cohort of lumbar surgical patients. Spine 29:2538–2541
36. Mirza SK (2005) Point of view: commentary on the research reports that led to Food and Drug Administration approval of an artificial disc. Spine 30:1561–1564

193M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_5.3, © Springer-Verlag Berlin Heidelberg 2010
Introduction
Total disk replacement (TDR) was developed in Europe and has been available there for many years with good results reported [1–6]. Favorable results for TDR have been reported more recently from other regions as well [7, 8]. After the completion of the FDA-regulated trials, these implants are gaining acceptance in the United States [9, 10]. In these ran-domized studies, TDR was compared to anterior lum-bar interbody fusion or combined anterior/posterior instrumented fusion. The TDR results were as good as fusion, and better on some outcome measures. There is little information comparing TDRs. In a relatively small retrospective study of 61 patients, it was reported that the results of Charité and ProDisc were similar [8]. To date, there has not been a prospective, randomized study comparing two TDR devices. The purpose of the current, ongoing study was to compare the results of TDR using Kineflex to Charité.
Materials and Methods
Kineflex is a three-piece metal on metal, semicon-strained lumbar artificial disk consisting of two cobalt chrome molybdenum (CCM) end plates and a fully articulating CCM core (Fig. 5.3.1a). It has been used
clinically since 2002, with over 1,500 disks implanted worldwide. Kineflex is being investigated under an IDE clinical study in the United States that began in the summer of 2005 and completed enrollment in the December of 2006. The Charité Artificial consists of two end plates manufactured from CoCrMo alloy and a UHMWPE sliding core (Fig. 5.3.1b). It has been used clinically since the 1980s and has been approved for use in the United States since 2004.
A total of 85 patients from two centers participating in the FDA-regulated trial were randomized in a 1:1 ratio to receive the Kineflex or Charité TDR. All patients were treated for single-level symptomatic disk degeneration at either the L4-5 or L5-1 level. The majority of the surgeries were performed at L5-1. Data reported for this include peri-operative data and 12-month clinical follow-up. Peri-operative data were collected including estimated blood loss, operative time, and the length of hospitalization. Clinical results were based on visual analog scales assessing pain (VAS) and the Oswestry Disability Index. Radiographic data through the 6-month follow-up were available at the time of this writing. All radiographs were sent to a central independent center to be measured. Radiographic assessment included disk space height and range of motion determined from flexion/extension films.
Patient Selection Criteria
Appropriate patient selection is important for achiev-ing optimal clinical outcomes. A summary of patient selection criteria from the Kineflex IDE clinical study are as follows:
A Prospective Randomized Comparison of Two Lumbar Total Disk Replacements
Richard D. Guyer and Donna D. Ohnmeiss
R. D. Guyer (*) Texas Back Institute, 6020 West Parker Rd. 200, Plano, TX 75093, USA e-mail: [email protected]
5.3

194 R. D. Guyer and D. D. Ohnmeiss
Inclusion Criteria Overview
Between 18 and 60 years of age•Evidence of degenerative disk disease (DDD) at •either L4/L5 or L5/S1 with radiographic evidence of one or more of the following:
Mild to moderate osteophyte formation of the −vertebral endplatesLoss of disk height of at least 2 mm when com- −pared to adjacent levelHerniated nucleus pulposus −Loss of water content on MRI −
History of back and/or radicular pain which is •severe, ongoing, and recurrentHave at least 6 months of prior conservative treat-•ment for discogenic back painHave a visual analog score (VAS) of at least 40 on a •100-mm scale
Exclusion Criteria Overview
Any back or leg pain of unknown origin•Degenerative spondylolisthesis with greater than •3 mm slippage at study level
Disk space height less than 3 mm at study level•Scoliosis of the lumbar spine with greater than 11° •coronal deformityLess than 2° of motion at index level•Metabolic bone disease (e.g., osteopenia, gout, •osteomalacia, Paget’s disease)Morbid obesity (body mass index greater than 40 or •more than 100 pounds overweight)
There were 44 patients randomized to the Kineflex group and 41 were assigned to the Charité group. The mean age was 40.6 years, ranging from 20 to 60 years. TDR was performed at the L4-5 level in 22.4% of patients and at L5-1 in the remaining 77.6%.
Biomechanical Testing
A substantial body of preclinical mechanical testing has been performed on the Kineflex Spinal System including static testing, monoaxial fatigue testing, and wear testing. These tests were performed to sim-ulate the load and movement to which the disks would be exposed under in vivo conditions, and to
Fig. 5.3.1 The Kineflex (a) and Charité (b) devices
a b
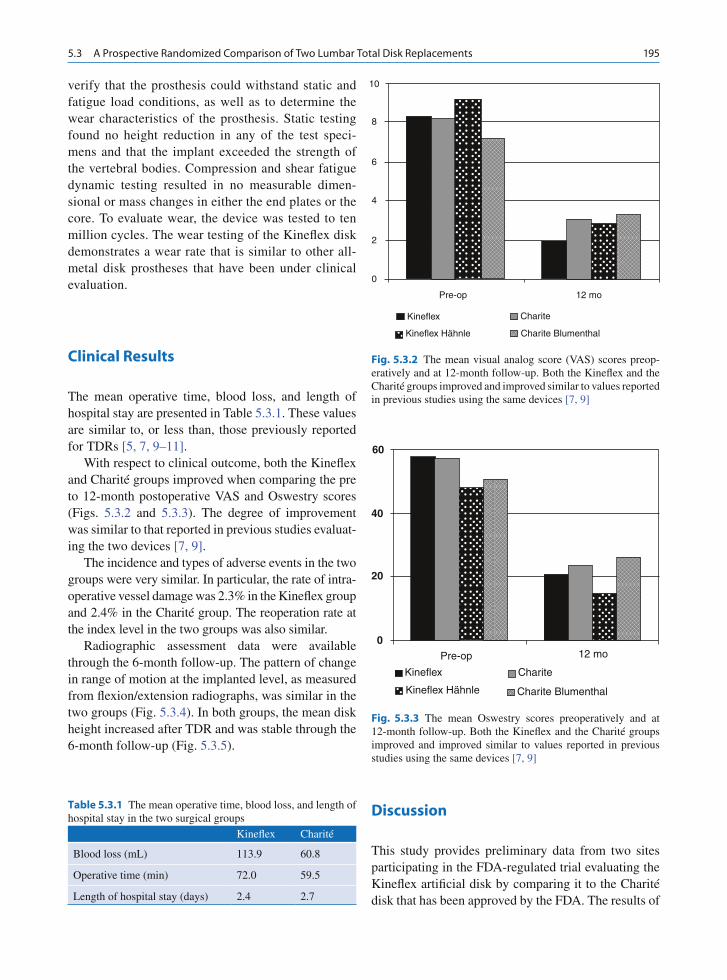
1955.3 A Prospective Randomized Comparison of Two Lumbar Total Disk Replacements
verify that the prosthesis could withstand static and fatigue load conditions, as well as to determine the wear characteristics of the prosthesis. Static testing found no height reduction in any of the test speci-mens and that the implant exceeded the strength of the vertebral bodies. Compression and shear fatigue dynamic testing resulted in no measurable dimen-sional or mass changes in either the end plates or the core. To evaluate wear, the device was tested to ten million cycles. The wear testing of the Kineflex disk demonstrates a wear rate that is similar to other all-metal disk prostheses that have been under clinical evaluation.
Clinical Results
The mean operative time, blood loss, and length of hospital stay are presented in Table 5.3.1. These values are similar to, or less than, those previously reported for TDRs [5, 7, 9–11].
With respect to clinical outcome, both the Kineflex and Charité groups improved when comparing the pre to 12-month postoperative VAS and Oswestry scores (Figs. 5.3.2 and 5.3.3). The degree of improvement was similar to that reported in previous studies evaluat-ing the two devices [7, 9].
The incidence and types of adverse events in the two groups were very similar. In particular, the rate of intra-operative vessel damage was 2.3% in the Kineflex group and 2.4% in the Charité group. The reoperation rate at the index level in the two groups was also similar.
Radiographic assessment data were available through the 6-month follow-up. The pattern of change in range of motion at the implanted level, as measured from flexion/extension radiographs, was similar in the two groups (Fig. 5.3.4). In both groups, the mean disk height increased after TDR and was stable through the 6-month follow-up (Fig. 5.3.5).
Discussion
This study provides preliminary data from two sites participating in the FDA-regulated trial evaluating the Kineflex artificial disk by comparing it to the Charité disk that has been approved by the FDA. The results of
Table 5.3.1 The mean operative time, blood loss, and length of hospital stay in the two surgical groups
Kineflex Charité
Blood loss (mL) 113.9 60.8
Operative time (min) 72.0 59.5
Length of hospital stay (days) 2.4 2.7
Fig. 5.3.2 The mean visual analog score (VAS) scores preop-eratively and at 12-month follow-up. Both the Kineflex and the Charité groups improved and improved similar to values reported in previous studies using the same devices [7, 9]
10
8
6
4
2
0
Pre-op
Kineflex
Kineflex Hähnle Charite Blumenthal
Charite
12 mo
Fig. 5.3.3 The mean Oswestry scores preoperatively and at 12-month follow-up. Both the Kineflex and the Charité groups improved and improved similar to values reported in previous studies using the same devices [7, 9]
60
20
0
40
Kineflex Hähnle Charite Blumenthal
Charite
12 moPre-op
Kineflex
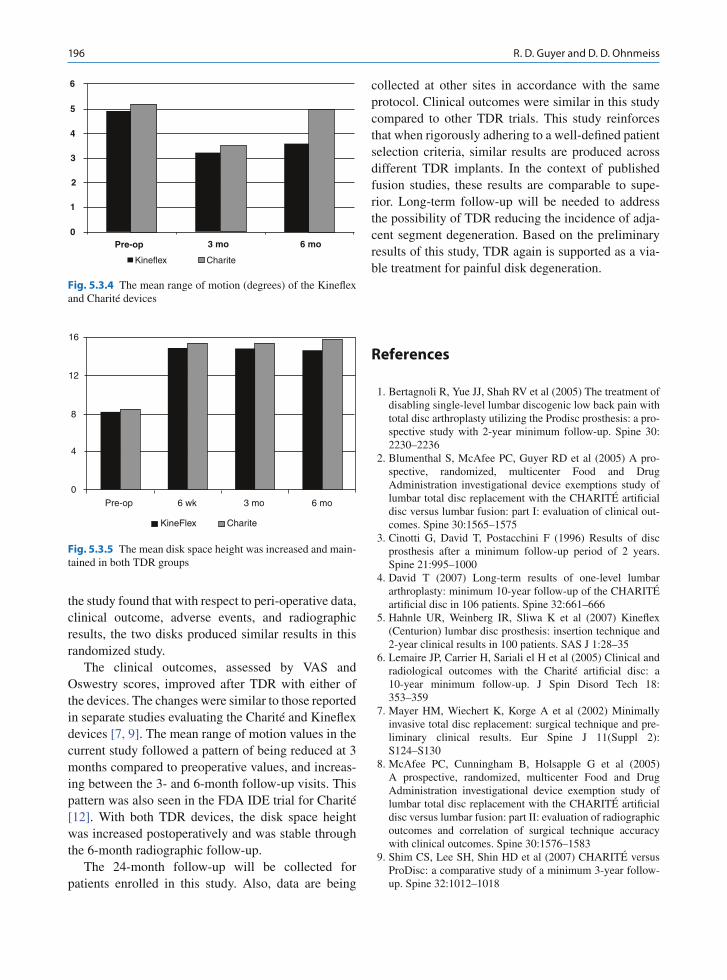
196 R. D. Guyer and D. D. Ohnmeiss
the study found that with respect to peri-operative data, clinical outcome, adverse events, and radiographic results, the two disks produced similar results in this randomized study.
The clinical outcomes, assessed by VAS and Oswestry scores, improved after TDR with either of the devices. The changes were similar to those reported in separate studies evaluating the Charité and Kineflex devices [7, 9]. The mean range of motion values in the current study followed a pattern of being reduced at 3 months compared to preoperative values, and increas-ing between the 3- and 6-month follow-up visits. This pattern was also seen in the FDA IDE trial for Charité [12]. With both TDR devices, the disk space height was increased postoperatively and was stable through the 6-month radiographic follow-up.
The 24-month follow-up will be collected for patients enrolled in this study. Also, data are being
collected at other sites in accordance with the same protocol. Clinical outcomes were similar in this study compared to other TDR trials. This study reinforces that when rigorously adhering to a well-defined patient selection criteria, similar results are produced across different TDR implants. In the context of published fusion studies, these results are comparable to supe-rior. Long-term follow-up will be needed to address the possibility of TDR reducing the incidence of adja-cent segment degeneration. Based on the preliminary results of this study, TDR again is supported as a via-ble treatment for painful disk degeneration.
References
1. Bertagnoli R, Yue JJ, Shah RV et al (2005) The treatment of disabling single-level lumbar discogenic low back pain with total disc arthroplasty utilizing the Prodisc prosthesis: a pro-spective study with 2-year minimum follow-up. Spine 30: 2230–2236
2. Blumenthal S, McAfee PC, Guyer RD et al (2005) A pro-spective, randomized, multicenter Food and Drug Administration investigational device exemptions study of lumbar total disc replacement with the CHARITÉ artificial disc versus lumbar fusion: part I: evaluation of clinical out-comes. Spine 30:1565–1575
3. Cinotti G, David T, Postacchini F (1996) Results of disc prosthesis after a minimum follow-up period of 2 years. Spine 21:995–1000
4. David T (2007) Long-term results of one-level lumbar arthroplasty: minimum 10-year follow-up of the CHARITÉ artificial disc in 106 patients. Spine 32:661–666
5. Hahnle UR, Weinberg IR, Sliwa K et al (2007) Kineflex (Centurion) lumbar disc prosthesis: insertion technique and 2-year clinical results in 100 patients. SAS J 1:28–35
6. Lemaire JP, Carrier H, Sariali el H et al (2005) Clinical and radiological outcomes with the Charité artificial disc: a 10-year minimum follow-up. J Spin Disord Tech 18: 353–359
7. Mayer HM, Wiechert K, Korge A et al (2002) Minimally invasive total disc replacement: surgical technique and pre-liminary clinical results. Eur Spine J 11(Suppl 2): S124–S130
8. McAfee PC, Cunningham B, Holsapple G et al (2005) A prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of lumbar total disc replacement with the CHARITÉ artificial disc versus lumbar fusion: part II: evaluation of radiographic outcomes and correlation of surgical technique accuracy with clinical outcomes. Spine 30:1576–1583
9. Shim CS, Lee SH, Shin HD et al (2007) CHARITÉ versus ProDisc: a comparative study of a minimum 3-year follow-up. Spine 32:1012–1018
Fig. 5.3.4 The mean range of motion (degrees) of the Kineflex and Charité devices
6
5
2
3 mo 6 moPre-op0
1
3
4
Kineflex Charite
Fig. 5.3.5 The mean disk space height was increased and main-tained in both TDR groups
4
0
ChariteKineFlex
6 mo3 mo6 wkPre-op
8
12
16

1975.3 A Prospective Randomized Comparison of Two Lumbar Total Disk Replacements
10. Siepe CJ, Mayer HM, Wiechert K et al (2006) Clinical results of total lumbar disc replacement with ProDisc II: three-year results for different indications. Spine 31:1923–1932
11. Tropiano P, Huang RC, Girardi FP et al (2005) Lumbar total disc replacement. Seven to eleven-year follow-up. J Bone Joint Surg Am 87:490–496
12. Zigler J, Delamarter R, Spivak JM et al (2007) Results of the prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of the ProDisc-L total disc replacement versus circumferential fusion for the treatment of 1-level degenerative disc disease. Spine 32:1155–1162

199M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_5.4, © Springer-Verlag Berlin Heidelberg 2010
Motion-sparing procedures that can address back pain, such as disk replacements and dynamic stabilization, have caught the enthusiasm of surgeons and patients alike. While these innovations are exciting and have significant promise, it is important to also keep in mind the limitations of what this new technology can offer.
These procedures, for the most part, are considered to be alternatives to fusions for low back pain. But all fusions for low back pain are not the same. When the indication for surgery is spondylolisthesis, scoliosis, or fracture, the successful relief of back pain can be upward of 80%. However, fusion for discogenic low back pain, or degenerative disk disease, has histori-cally had success rates of 50–70%.
One of the problems with the diagnosis of degen-erative disk disease is the difficulty in clarifying the difference between physiologic aging and pathologic degeneration. Back pain is ubiquitous in the upright human spine; however, disability due to back pain dif-fers widely among cultures. The majority of back pain is self-limited, with only a small percentage of people with back pain developing “chronic” low back pain for longer than 3 months. Boden [1] found that Magnetic Resonance Imaging (MRI) performed in asymptom-atic individuals under age 60, 20% showed HNP.
In addition, a test used by many surgeons to demon-strate that a specific disk or disks is/are the source of the pain, the discogram, can be unreliable in chronic pain patients [2, 3]. Arguably, many patients who have low back pain become chronic pain patients; our cur-rent diagnostic testing does not allow us to sort those in
whom “chronic pain behavior” is reversible. These studies found that occupational factors, neurophysio-logical factors, and psychometric factors were more predictive of the development of back pain than abnor-mal MRI or positive discography [3].
They also studied patients who underwent lumbar fusion for discogenic back pain (positive single-level concordant discogram with negative control level) compared to those who had lumbar fusions for unstable spondylolisthesis (2007). The discogenic back pain group had a 43% rate of “minimal acceptable outcome” compared to 91% in the spondylolisthesis group; for “highly effective success criteria,” the rates were 27% and 72%, respectively.
Certainly, TDR has a limited or no role in patients who have isthmic spondylolisthesis, spinal stenosis, and the majority of degenerative spondylolisthesis cases. Several authors have reviewed their lumbar spine surgical practices [4–6] and found that many of their typical surgical patients had contraindications to TDR, most commonly stenosis, spondylolysis, or spondylolis-thesis, scoliosis, HNP, osteoporosis, pseudoarthrosis, or insufficient posterior elements. In fact, only 5% of the lumbar surgery patients were felt to be appropriate TDR candidates. The degree of facet arthrosis for which TDR may still be effective is not yet determined, but may not be a major contraindication for TDR in at least one review of lumbar fusion patients [7].
Prior advances of the management of degenerative disk disease have been heralded as potentially revolu-tionizing its treatment: these include BAK (screw in cages), IDET (intradiscal electrothermal treatment), nucleoplasty, use of bone dowels with bone morphoge-netic protein, as well as nuclear replacements, dynamic stabilization, and facet replacement, which are on the horizon. BAK cages, inserted through an anterior approach, were thought to avoid damage to the
Limitations of Lumbar Disk Arthroplasty
Serena S. Hu
S. S. Hu Department of Orthopedic Surgery, 500 Parnassus Avenue, Room MU320 West, San Francisco, CA 94143, USA e-mail: [email protected]
5.4

200 S. S. Hu
posterior musculature and the consequent “fusion dis-ease” [8]. However, with longer than the initial 2-year follow-up by other surgeons, the technique proved to have an unacceptably high pseudoarthrosis rate [9–11] (Fig. 5.4.1) and technically posed significant risk to the adjacent neurovascular structures, especially when working through the recommended tube. IDET and nucleoplasty procedures, although minimally invasive, proved to be highly technique and placement depen-dent, and the practitioners have narrowed their indica-tions considerably [12–14, 33, 35]. The area of heating was demonstrated to be quite limited, >60°C, sufficient for collagen denaturation, and potentially collagen shrinkage occurred only within 1–2 mm of the catheter surface, while development of temperature adequate to ablate nerves was difficult to achieve in clinically relevant regions [15].
The design of the recent lumbar disk replacements has been refined to the point of their having a reasonable ability to restore normal disk kinematics within the limi-tations of material properties [16–21]. Although wear debris and osteolysis has been problematic in the hip and knee, it appears less concerning in the spine, both clinically as well as in biomechanical testing [22, 23], although clinical data are only midterm in duration.
Another concern about lumbar fusions was the risk of accelerated degeneration at the adjacent segment. This was classically analyzed in the cervical spine by Hilibrand (1999) but has also been studied in the lum-bar spine by Ghiselli [24]. The latter study reviewed 215 patients at an average follow-up of 6.7 years and
found 27.5% to have required decompression or decompression and fusion at an adjacent level. This translated to a rate of symptomatic degeneration of 16.5% at 5 years and 36.1% at 10 years (Fig. 5.4.2). This rate did not appear to increase if more levels were initially fused. These are retrospective studies and it is not clear whether adjacent segment disease is truly accelerated by the fusion or whether it is a continuation of the natural history. It has been observed that ASD occurs more frequently with circumferential fusion and with instrumented fusions, which may imply these stiffer constructs may lead to have ASD, however, the commonly used pedicle screws and their linkage to the longitudinal rod are generally in immediate proximity to the facet above and may cause damage.
At this point in time, the data available comparing lumbar fusion to TDR with regard to adjacent segment disease are too early to demonstrate whether preserving motion will be protective or avoid accelerating ASD [34, 36]. The early Prodisc cases performed by the inventor surgeon have been analyzed, and it has been found that 24% of the 42 patients reviewed had radio-graphic evidence of ASF (loss of disk space height, anterior osteophyte formation, or dynamic instability at an average of 8.7 years after TDR) [25, 37]. They found that patients with motion of 5° at the level of the TDR had no ASD compared to 34% of patients whose TDR had less than 5°, although there was no difference in clinical outcomes. Although suggestive, comparative data for a 10 year or similar time frame, such as will be available in the US FDA studies for Charite, Prodisc,
Fig. 5.4.1 Patient with failed fusion with BAK cages

2015.4 Limitations of Lumbar Disk Arthroplasty
Fig. 5.4.2 (a and b) Radiographs from healthy 46-year-old female, with degenerative spondylolisthesis refractory to conser-vative treatment; (c) lateral MRI, T2 weighed image, demonstrat-ing spinal stenosis; (d, e) radiographs postop, showing radiographic
fusion. Patient has returned to full activities, including sports; (f) radiographs 11 years postop show advanced degeneration at adjacent L3–4 level; (g) radiographs after successful revision with proximal decompression and proximal extension of fusion
a
fed
cb

202 S. S. Hu
and others, will be needed to demonstrate whether or not use of TDR will affect the incidence of ASD.
Published series from Europe are favorable although nonrandomized, with up to 90% of patients reporting good to excellent results, including some patients fol-lowed for at least 10 years [26].
Although most surgeons who have experience with TDR have a significant number of patients who feel the surgery improves their symptoms significantly, it is important to review the data from the US FDA studies critically. The defined criteria for “success” included at least 25% improvement of the Oswestry score com-pared to preoperative scores, no device failures, no neurologic loss, which had a 57% success rate among the Charité patients completing the study, compared to
47% of controls [27]. Likewise, for Prodisc, overall success was 53% for Prodisc patients compared to 41% of the control patients [28].
Even if one simply looks at functional improvement as measured by Oswestry Disability score, which may be the most important thing for a patient, the results were 64% of the Charité patients achieved 25% improvement compared to 50% of the controls. Among the Charité patients, 71% of them were satisfied at 2 years, compared to 59% of the control patients [27], which approached but did not reach statistical signifi-cance. The results from the Prodisc study are similar with 77% of the Prodisc patients achieving at least the prescribed 15% improvement compared to 63% of controls [28].
Given McAfee’s recent determination of the rota-tional instability of the lumbar disk arthroplasty [29], a surgeon certainly needs to be cautious about addressing multiple level disease. His study was sparked by the referral of an “alarming number of cases” in whom iatrogenic lumbar rotational instabil-ity developed (Fig. 5.4.3). In addition, its potential role in treating cases with even mild to moderate scoliosis may be questionable.
Why are the results so variable for this patient pop-ulation? Some patients are clearly benefited by this surgery (Fig. 5.4.4), while others see minimal to no benefit. The indications for surgery in the FDA studies were clearly as strict as our current knowledge allows, which suggests that we do not understand what factors are different in those who had poor outcomes. Research continues in an effort to improve our understanding of painful degenerative disk disease. Alamin et al are working with Functional Anesthetic Discography. We and others have looked with specialized imaging tech-niques combined with biochemical and histologic analysis to better understand this condition.
g
Fig. 5.4.2 (continued)

2035.4 Limitations of Lumbar Disk Arthroplasty
a b
c d
Fig. 5.4.3 (a) Preoperative AP radiographs of patient with dis-cogenic back pain. Minimal coronal deformity noted. (b) Six weeks after 2-level Charité, performed in Europe, clear rota-tional and lateral deformity has developed. She had moderate improvement of back pain for several weeks after her index surgery. Note relative posterior placement of L5-S1 device. (c) Patient returned to her surgeon in Europe, who performed L4–5 Dynesys. Patient had minimal improvement of back and
leg pain (d) with worsening leg and back pain, patient under-went revision. Posterior exploration was performed first, with exposure and neurolysis of inferior end plate from thecal sac, placement of pedicle screws. Anterior removal of L5-S1 Charité was then performed with interbody allograft plus BMP fusion. Posterior rod placement and fusion completed the surgery. Patient has had 75% relief of leg pain and about 50% relief of back pain

204 S. S. Hu
References
1. Boden SD, Davis DO, Dina TS et al (1990) Abnormal mag-netic-resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation. J Bone Joint Surg Am 72(3):403–408
2. Carragee EJ (2000) Is lumbar discography a determinate of discogenic low back pain: provocative discography recon-sidered. Curr Rev Pain 4(4):301–308
3. Carragee EJ, Alamin TF, Miller JL et al (2005) Discographic, MRI and psychosocial determinants of low back pain dis-ability and remission: a prospective study in subjects with benign persistent back pain. Spine J 5(1):24–35
4. Chin KR (2007) Epidemiology of indications and contrain-dications to total disc replacement in an academic practice. Spine J 7(4):392–398
5. Fras CI, Auerbach JD (2008) Prevalence of lumbar total disc replacement candidates in a community-based spinal sur-gery practice. J Spinal Disord Tech 21(2):126–129
a
b
Fig. 5.4.4 (a) 35-year-old male with 2-year history of LBP refractory to conserva-tive care. Radiographs show narrowing of L5-S1 disk space. MRI shows L5-S1 degeneration with Modic changes. Discography (not shown) concordant at L5-S1, with negative control level. (b) Patient underwent L5-S1 Prodisc placement, with 90% relief of his back pain

2055.4 Limitations of Lumbar Disk Arthroplasty
6. Huang RC, Lim MR, Girardi FP et al (2004) The prevalence of contraindications to total disc replacement in a cohort of lumbar surgical patients. Spine 29(22):2538–2541
7. Wong DA, Annesser B, Birney T et al (2007) Incidence of contraindications to total disc arthroplasty: a retrospective review of 100 consecutive fusion patients with a specific analysis of facet arthrosis. Spine J 7(1):5–11
8. Kuslich SD, Danielson G, Dowdle JD et al (2000) Four-year follow-up results of lumbar spine arthrodesis using the Bagby and Kuslich lumbar fusion cage. Spine 25(20): 2656–2662
9. Button G, Gupta M, Barrett C et al (2005) Three- to six-year follow-up of stand-alone BAK cages implanted by a single surgeon. Spine J 5(2):155–160
10. McAfee PC, Cunningham BW, Lee GA et al (1999) Revision strategies for salvaging or improving failed cylindrical cages. Spine 24(20):2147–2153
11. McAfee PC, Lee GA, Fedder IL et al (2002) Anterior BAK instrumentation and fusion: complete versus partial discec-tomy. Clin Orthop Relat Res 394:55–63
12. Cohen SP, Williams S, Kurihara C et al (2005) Nucleoplasty with or without intradiscal electrothermal therapy (IDET) as a treatment for lumbar herniated disc. J Spinal Disord Tech 18(Suppl):S119–S124
13. Freeman BJ (2006) IDET: a critical appraisal of the evi-dence. Eur Spine J 15(Suppl 3):S448–S457
14. Maurer P, Block JE, Squillante D (2008) Intradiscal electro-thermal therapy (IDET) provides effective symptom relief in patients with discogenic low back pain. J Spinal Disord Tech 21(1):55–62
15. Kleinstueck FS, Diederich CJ, Nau WH et al (2003) Temperature and thermal dose distributions during intradis-cal electrothermal therapy in the cadaveric lumbar spine. Spine 28(15):1700–1708; discussion 1709
16. Auerbach JD, Wills BP, McIntosh TC et al (2007) Evaluation of spinal kinematics following lumbar total disc replacement and circumferential fusion using in vivo fluoroscopy. Spine 32(5):527–536
17. Cunningham BW, Gordon JD, Dmitriev AE et al (2003) Biomechanical evaluation of total disc replacement arthro-plasty: an in vitro human cadaveric model. Spine 28(20): S110–S117
18. Cunningham BW, McAfee PC, Geisler FH et al (2008) Distribution of in vivo and in vitro range of motion follow-ing 1-level arthroplasty with the CHARITE artificial disc compared with fusion. J Neurosurg Spine 8(1):7–12
19. O’Leary P, Nicolakis M, Lorenz MA et al (2005) Response of Charité total disc replacement under physiologic loads: pros-thesis component motion patterns. Spine J 5(6):590–599
20. Rohlmann A, Zander T, Bergmann G (2005) Effect of total disc replacement with ProDisc on intersegmental rotation of the lumbar spine. Spine 30(7):738–743
21. Rousseau MA, Bradford DS, Bertagnoli R et al (2006) Disc arthroplasty design influences intervertebral kinematics and facet forces. Spine J 6(3):258–266
22. Cunningham BW (2004) Basic scientific considerations in total disc arthroplasty. Spine J 4(6 Suppl):219S–230S
23. Rawlinson JJ, Punga KP, Gunsallus KL et al (2007) Wear sim-ulation of the ProDisc-L disc replacement using adaptive finite element analysis. J Neurosurg Spine 7(2):165–173
24. Ghiselli G, Wang JC, Bhatia NN et al (2004) Adjacent seg-ment degeneration in the lumbar spine. J Bone Joint Surg Am 86-A(7):1497–1503
25. Huang RC, Tropiano P, Marnay T et al (2006) Range of motion and adjacent level degeneration after lumbar total disc replacement. Spine J 6(3):242–247
26. Lemaire JP, Carrier H, Sariali W et al (2005) Clinical and radiological outcomes with the Charité artificial disc: a 10-year minimum follow-up. J Spinal Disord Tech 18(4): 353–359
27. Blumenthal S, McAfee PC, Guyer RD et al (2005) A pro-spective, randomized, multicenter Food and Drug Admin-istration investigational device exemptions study of lumbar total disc replacement with the CHARITE artificial disc ver-sus lumbar fusion: part I: evaluation of clinical outcomes. Spine 30(14):1565–1575; discussion E387
28. Zigler J, Delamarter R, Spivak JM et al (2007) Results of the prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of the ProDisc-L total disc replacement versus circumferential fusion for the treatment of 1-level degenerative disc disease. Spine 32(11):155–162; discussion 1163
29. McAfee PC, Cunningham BW, Hayes V et al (2006) Biomechanical analysis of rotational motions after disc arthroplasty: implications for patients with adult deformi-ties. Spine 31(19 Suppl):S152–S160
30. Carragee EJ, Alamin TF, Miller J et al (2002) Provocative discography in volunteer subjects with mild persistent low back pain. Spine J 2(1):25–34
31. Carragee EJ, Lincoln T, Parmar VS et al (2006) A gold standard evaluation of the “discogenic pain” diagnosis as determined by provocative discography. Spine 31(18): 2115–2123
32. Davis TT, Delamarter RB, Sra P et al (2004) The IDET pro-cedure for chronic discogenic low back pain. Spine 29(7): 752–756
33. Freeman BJ, Fraser RD, Cain CM et al (2005) A random-ized, double-blind, controlled trial: intradiscal electrother-mal therapy versus placebo for the treatment of chronic discogenic low back pain. Spine 30(21):2369–2377; discus-sion 2378
34. McAfee PC, Cunningham B, Holsapple G, et al (2005) A prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of lumbar total disc replacement with the CHARITE artificial disc versus lumbar fusion: part II: evaluation of radiographic outcomes and correlation of surgical technique accuracy with clinical outcomes. Spine 30(14):1576–1583; discus-sion E388
35. Saal JA, Saal JS (2002) Intradiscal electrothermal treatment for chronic discogenic low back pain: prospective outcome study with a minimum 2-year follow-up. Spine 27(9):966–973; discussion 973
36. Siepe CJ, Mayer HM, Wiechert K et al (2006) Clinical results of total lumbar disc replacement with ProDisc II: three-year results for different indications. Spine 31(17):1923–1932
37. Thierry D (2007) Long-term results of one-level lumbar arthroplasty: minimum 10-year follow-up of the CHARITE artificial disc in 106 patients. Spine 32(6):661–666

207M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_5.5, © Springer-Verlag Berlin Heidelberg 2010
Introduction
Degenerative disk disease (DDD) at the level adjacent to an immobilized (fused) spinal segment is a well-recognized condition [1–4] which is believed to result from the supraphysiological biomechanical stress and increased range of motion (ROM) created at that level by the fusion [1]. This may be caused by the patient’s postoperative attempt to achieve similar ROM as before surgery [5]. It is therefore hypothesized that topping a fusion with a posterior dynamic stabilization (PDS) system at the level adjacent to a fusion may diminish these increased stress and ROM, and subsequently, reduce the incidence of adjacent-level disk disease.
The overall concept of PDS is viewed as potentially beneficial not only for topping off a fusion, but also as an alternative to fusion for patients with specific back problems, such as stenosis, facet pain, and DDD [6]. However, no research has been conducted to date to determine the desirable degree of motion control and disk/facet unloading needed to achieve meaningful clinical results. Despite this limitation, a wide variety of PDS systems are currently in various stages of development and clinical investigation.
Similar to an internal brace, the PDS is intended to work in parallel with the segmental structural element, transferring the load from one vertebra to the other. We hypothesized that a PDS system with a stiffness equiv-alent to that of an intact spinal segment would effec-tively share the load with the disk and the facet joints,
while maintaining 50% of the intact segment motion at the operated level. In this study, the residual ROM of a spinal segment instrumented with the Dynarod PDS system was evaluated and compared to that of a spinal segment instrumented with Dynesys, Nflex, and PEEK rods. In addition, the residual ROM of a Dynarod-stabilized spinal segment after discectomy or bilateral facetectomy was also evaluated.
Hypotheses
1. A PDS with a stiffness equivalent to that of an intact spinal segment would reduce the ROM of an instru-mented spinal level to 50% of that observed in an intact spine and share 50% of the load with the structural element.
2. A PDS with a stiffness equivalent to that of an intact spinal segment might be sufficient to stabilize a spi-nal motion segment.
3. Topping off a fusion with a PDS may provide some protection against fusion-induced adjacent-level degeneration.
Study Objectives
1. To create and validate a three-dimensional finite element model (FE-Model) of the human osseo-ligamentous lumbar spine.
2. To use the validated FE-Model to investigate the impact of PDS instrumentation in stabilizing the spine and protecting levels adjacent to a fusion.
Is Posterior Dynamic Stabilization an Option to Avoid Adjacent Segment Decompensation?
Missoum Moumene and Jürgen Harms
M. Moumene (*) Department of Research and Development, DePuy Spine Inc., Raynham, MA, USA e-mail: [email protected]
5.5

208 M. Moumene and J. Harms
Materials and Methods
The validity of load sharing and ROM calculations as related to PDS’ biomechanical function depends on the precision of the FE-Model utilized for the analyses. In this study, we used two FE-Models as follows:
L4–L5 FE-Model
This model was used to optimize an appropriate design for PDS and investigate other PDS currently in clinical trials, using Load control.
L1-S1 FE-Model
This model was used to evaluate the biomechanical effect of a PDS topping off fusion using displacement control (Hybrid test method)
FE-Models
The 3D nonlinear FE-Model of the intact ligamentous L4–L5 motion segment validated in all six degrees of freedom (DOF) was used for PDS design optimization [7]. The model was expanded to an L1-S1 FE-Model for the biomechanical study of a PDS topping off fusion. The 3D geometry of L1, L2, L3 was adapted from the model of L4 using vertebrae’s three-dimensional anat-omy [8]. The facet joint morphologies, a critical artic-ulation, were derived from studies by Panjabi et al. [9] and Grobler et al. [10]. The curvature of the lumbar lordosis was created based on Bogduk [11] using Hypermesh (Altair Engineering Inc.) to position each vertebra. The intervertebral disks were created between vertebrae using the adjacent superior and inferior sur-faces of the vertebral bodies. A finite element package (ANSYS, version 11; Swanson Analysis System) was used to formulate the FE-Model.
The finite element model (FEM) included all the critical components of the spine: cortical and cancel-lous bone; endplates; annulus fibrosus and nucleus pulposus of the intervertebral disks; articular cartilage; synovial fluid of the facet joints; anterior longitudinal ligament; posterior longitudinal ligament; intertrans-verse ligament; ligament flavum; capsular ligament;
supraspinous ligament; and interspinous ligament. Mate rial properties of these various tissues were selected from the literature and are summarized elsewhere [7].
Implanted Model Formulation
An intact L4–L5 model, as well as L4–L5 models instrumented with Dynarod, Dynesys, and Nflex, was used in this study (Fig. 5.5.1). Three-dimensional models of each device were built and included in the FE analyses. The Dynarod, made of an alloy of nickel and titanium (Nitinol), was designed to mimic the stiffness of an intact spinal segment. This was achieved by optimizing the cross-section of the nitinol rod to achieve these desired biomechanical properties. The stiffness of the Dynesys and Nflex was modeled based on the manufacturers’ specifications. A 5.5-mm PEEK rod was used in this study. Nflex, Dynarod, and PEEK rods were placed along the functional spinal unit (FSU) without distraction. For the Dynesys system, a distraction of 2 mm was applied using a spacer. The cord was tightened to 300 N bringing the FSU to its preinstrumentation position. All pedicle screws were rigidly fixed to the vertebrae. A 7.5 Nm moment was applied to the intact and instrumented spinal models in
Fig. 5.5.1 FE-Models of intact and instrumented L4–L5 seg-ments with Dynarod, Dynesys, and Nflex
Intact Dynarod
Dynesys Nflex
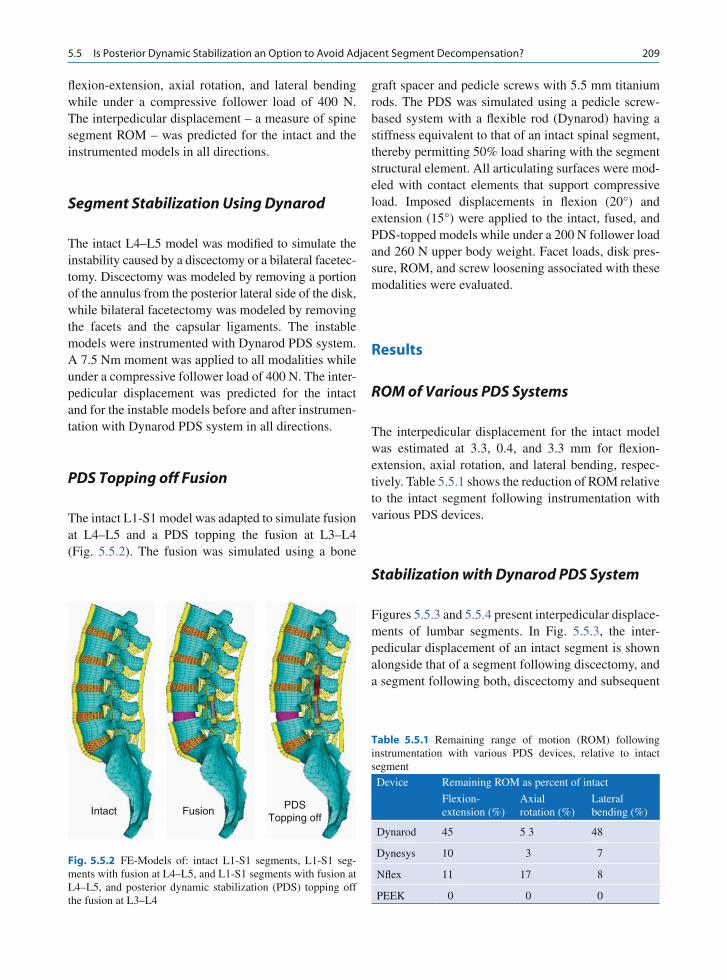
2095.5 Is Posterior Dynamic Stabilization an Option to Avoid Adjacent Segment Decompensation?
flexion-extension, axial rotation, and lateral bending while under a compressive follower load of 400 N. The interpedicular displacement – a measure of spine segment ROM – was predicted for the intact and the instrumented models in all directions.
Segment Stabilization Using Dynarod
The intact L4–L5 model was modified to simulate the instability caused by a discectomy or a bilateral facetec-tomy. Discectomy was modeled by removing a portion of the annulus from the posterior lateral side of the disk, while bilateral facetectomy was modeled by removing the facets and the capsular ligaments. The instable models were instrumented with Dynarod PDS system. A 7.5 Nm moment was applied to all modalities while under a compressive follower load of 400 N. The inter-pedicular displacement was predicted for the intact and for the instable models before and after instrumen-tation with Dynarod PDS system in all directions.
PDS Topping off Fusion
The intact L1-S1 model was adapted to simulate fusion at L4–L5 and a PDS topping the fusion at L3–L4 (Fig. 5.5.2). The fusion was simulated using a bone
graft spacer and pedicle screws with 5.5 mm titanium rods. The PDS was simulated using a pedicle screw-based system with a flexible rod (Dynarod) having a stiffness equivalent to that of an intact spinal segment, thereby permitting 50% load sharing with the segment structural element. All articulating surfaces were mod-eled with contact elements that support compressive load. Imposed displacements in flexion (20°) and extension (15°) were applied to the intact, fused, and PDS-topped models while under a 200 N follower load and 260 N upper body weight. Facet loads, disk pres-sure, ROM, and screw loosening associated with these modalities were evaluated.
Results
ROM of Various PDS Systems
The interpedicular displacement for the intact model was estimated at 3.3, 0.4, and 3.3 mm for flexion-extension, axial rotation, and lateral bending, respec-tively. Table 5.5.1 shows the reduction of ROM relative to the intact segment following instrumentation with various PDS devices.
Stabilization with Dynarod PDS System
Figures 5.5.3 and 5.5.4 present interpedicular displace-ments of lumbar segments. In Fig. 5.5.3, the inter-pedicular displacement of an intact segment is shown alongside that of a segment following discectomy, and a segment following both, discectomy and subsequent
Table 5.5.1 Remaining range of motion (ROM) following instrumentation with various PDS devices, relative to intact segment
Device Remaining ROM as percent of intact
Flexion-extension (%)
Axial rotation (%)
Lateral bending (%)
Dynarod 45 5 3 48
Dynesys 10 3 7
Nflex 11 17 8
PEEK 0 0 0
Fig. 5.5.2 FE-Models of: intact L1-S1 segments, L1-S1 seg-ments with fusion at L4–L5, and L1-S1 segments with fusion at L4–L5, and posterior dynamic stabilization (PDS) topping off the fusion at L3–L4
Intact Fusion PDSTopping off

210 M. Moumene and J. Harms
instrumentation with PDS. Figure 5.5.4 shows the interpedicular displacement of an intact segment, a segment following bilateral facetectomy, as well as a segment following bilateral facetectomy and subse-quent instrumentation with PDS.
After discectomy, extension ROM increased by 30%. Stabilization of the segment with Dynarod controlled the ROM to 70% vs. that of an intact segment (i.e.; non-discectomized). Bilateral facetectomy increased ROM predominantly in extension and axial rotation by 135 and 450%, respectively. Adding Dynarod, the corre-sponding ROM was reduced to 79 and 140% vs. that of an intact segment.
PDS Topping off a Fusion
The interpedicular displacement at L4–L5 in the intact model was estimated at 4.0, 3.7, and 2.1 mm for flex-ion-extension, axial rotation, and lateral bending, respectively. The corresponding interpedicular dis-placement at L3–L4 was estimated at 4.7, 2.0, and 2.6 mm.
Following a fusion at L4–L5, the motion at the adja-cent level (L3–L4) was increased by 18% (see Table 5.5.2). Instrumentation of this level with a Dynarod PDS decreased that motion by 54% vs. that observed in a segment adjacent to a normal (nonfusion) segment. The results for axial rotation and lateral bend-ing followed similar patterns, as shown in Table 5.5.2.
Facet loading was also evaluated to determine the potential impact of PDS on long-term adjacent-level degeneration. For this analysis, facet loads were nor-malized against those observed in a normal spine, without fusion and/or PDS instrumentation. Following a fusion at L4–L5, facet loading at the adjacent (L3–L4) level increased by 45% in extension vs. facet loads observed adjacent to normal, nonfused segments (see Table 5.5.3). Adding a Dynarod PDS to the L3–L4 segment reduced that facet loading by 26% vs. that of the normal spine. Similar trends were observed in axial rotation and lateral bending, as shown in Table 5.5.3. In both cases, a PDS topping off a fusion reduced facet loads at adjacent levels.
1.92
2.5
3
Inte
rped
icu
lar
Dis
pl.
(mm
)
1.5
1
0.5
0Flex Ext AR LB
2.0
0.8
1.3
3.1
1.11.2
0.2 0.3
1.7 1.7
0.8
Facetectomy
Intact
PDS
Fig. 5.5.4 Interpedicle displacement of: (1) an intact segment; (2) a segment following bilateral facetectomy; and (3) a segment following bilateral facetectomy and subsequent instrumentation with a Dynarod PDS
1.92
Inte
r-P
edic
le D
isp
l. (m
m)
1.5
1
0.5
0Flex
DiscectomyIntact PDS
Ext AR LB
2.1
0.7
1.3
1.7
0.9
0.2 0.20.1
1.7
1.9
0.8
Fig. 5.5.3 Interpedicle displacement of: (1) an intact segment; (2) a segment following discectomy; and (3) a segment following dis-cectomy and subsequent instrumentation with a Dynarod PDS
Table 5.5.3 Relative facet loading (%) at the level adjacent to a fusion, as compared to facet loading in normal spinal segments (without fusion or PDS instrumentation)
Procedure Flexion Extension Axial rotation
Lateral bending
Fusion only 0 +45 +13 +24
PDS topping off fusion
0 −26 −27 −53
Table 5.5.2 Relative ROM (%) at the level adjacent to a fusion, as compared to the ROM observed in a normal spinal segment (without fusion and without PDS instrumentation)
Procedure Flexion-extension
Axial rotation
Lateral bending
Fusion only +18 +31 +8
PDS topping off fusion
−54 −44 −50

2115.5 Is Posterior Dynamic Stabilization an Option to Avoid Adjacent Segment Decompensation?
Finally, intradiscal pressure at levels adjacent to a fusion (L3–L4) was also analyzed using: (1) a normal segment, (2) a segment with a L4–L5 fusion, as well as (3) a segment with a L4–L5 fusion and a L3–L4 PDS instrumentation (Table 5.5.4).
In the fusion model, a 10% increase in adjacent-level intradiscal pressure vs. normal was observed in flexion. With the PDS, this intradiscal pressure decreased such that the final pressure at L3–L4 was only 5% greater than that observed in a normal case. The decreases in intradiscal pressure following PDS instrumentation were much greater in extension (50% reduction), axial rotation (14% reduction), and lateral bending (10% reduction), as shown in Fig. 5.5.4.
With regard to bone screw loading, the PDS system reduced the screw bending load by 40%, as compared to that observed using a rigid titanium rod.
Conclusions
Various PDS systems are being introduced to the spi-nal community at increasing rates, yet this is the first research done to date to try to determine the adequate biomechanics of a PDS design to achieve meaningful clinical results. The most important rationales for the development of these devices are:
1. Stabilizing the spinal motion segment, without fus-ing the segment.
2. Preventing the long-term adverse effect of fusion, namely the accelerated adjacent-level degeneration.
A pedicle screw-based PDS system with a stiffness equivalent to that of an intact spinal segment was shown to be sufficient to stabilize the spine while pre-serving 50% of the intact ROM, consequently reduc-ing the load on its structural element. The Dynesys,
Nflex, and PEEK rods, on the other hand, reduced nearly all of the ROM at the instrumented level, thereby acting as fusion devices, not as PDS systems.
In this hybrid test model, topping off a fusion with a PDS system that has a stiffness equivalent to that of an intact spine segment was shown to relieve facet loading and reduce intradiscal pressure on adjacent segments. Assuming that these loads contribute to adjacent-level disk disease, these data indicate that PDS topping of a fusion may provide some protection against fusion-induced adjacent-level degeneration. In addition, reduced bone screw interface loading further suggests that PDS may be an option to avoid adjacent segment decompensation.
Limitations of this study are those of the displace-ment control test method. This method, being a finite element study, does not and cannot simulate the effect of adaptation that may occur over many years after implantation of a device in a patient.
References
1. Eck JC, Humphreys SC, Hodges SD (1999) Adjacent-segment degeneration after lumbar fusion: a review of clinical, biome-chanical, and radiologic studies. Am J Orthop 28(6):336–340
2. Ghiselli G et al (2004) Adjacent segment degeneration in the lumbar spine. J Bone Joint Surg Am 86-A(7):1497–1503
3. Lee CK (1988) Accelerated degeneration of the segment adjacent to a lumbar fusion. Spine 13(3):375–377
4. Park P et al (2004) Adjacent segment disease after lumbar or lumbosacral fusion: review of the literature. Spine 29(17): 1938–1944
5. Panjabi MM (2007) Hybrid multidirectional test method to evaluate spinal adjacent-level effects. Clin Biomech (Bristol, Avon) 22(3):257–265
6. Sengupta DK (2004) Dynamic stabilization devices in the treat-ment of low back pain. Orthop Clin North Am 35(1):43–56
7. Moumene M, Geisler FH (2007) Comparison of biomechan-ical function at ideal and varied surgical placement for two lumbar artificial disc implant designs: mobile-core versus fixed-core. Spine 32(17):1840–1851
8. Panjabi MM et al (1992) Human lumbar vertebrae. Quantitative three-dimensional anatomy. Spine 17(3):299–306
9. Panjabi MM et al (1993) Articular facets of the human spine. Quantitative three-dimensional anatomy. Spine 18(10): 1298–1310
10. Grobler LJ et al (1993) Etiology of spondylolisthesis. Assessment of the role played by lumbar facet joint mor-phology. Spine 18(1):80–91
11. Bogduk N (1999) Clinical anatomy of the lumbar spine and scrum 3rd edn. Churchill Livingstone, Edinburgh London New York Philadelphia Toronto, pp 55–59
Table 5.5.4 Relative intradiscal pressure (%) at the level adjacent to a fusion, as compared to the intradiscal pressure in normal spinal segments (without fusion or PDS instrumentation)
Procedure Flexion Extension Axial rotation
Lateral bending
Fusion only +10 +5 −1 −4
PDS topping off fusion
+5 −50 −14 −10

213M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_5.6, © Springer-Verlag Berlin Heidelberg 2010
Introduction
The current premise, on which spinal fusion is offered to patients with a painful lumbar motion segment, is that the pain arises secondary to abnormal motion or “instability”. By the elimination of this motion, one hopes to eliminate the pain. However, results follow-ing spinal fusion are far from predictable, with reported satisfactory clinical results ranging from 46 to 82% [1, 2]. Furthermore, many patients complain of postural or positional pain occurring without motion, suggesting that low back pain may have aetiologies relating to abnormal load transmission rather than abnormal kinematics.
The normal intervertebral disc is isotropic, i.e. behaving as a fluid-filled bag, transmitting load uni-formly across the surface of the disc to the end plate [3]. The degenerate intervertebral disc, however, becomes anisotropic or non-homogenous with areas of frag-mented and condensed collagen, fluid and gas [4]. Load transmission across the end plate of a degenerate disc therefore becomes uneven. The loads across the disc space are now highly dependent on position. McNally et al. correlated changes in the pattern of loading in vivo across a degenerate intervertebral disc with pain on provocative lumbar discography [5]. Mulholland et al. proposed the concept of the “stone in the shoe”, where pain in a specific posture arises from a degenerate disc largely due to abnormal load transmission [6]. Altering this posture may result in the “stone in the shoe”
moving to a point of less load transmission and there-fore less pain.
It has been well documented that abnormal load transmission may result in degenerative changes in synovial joints such as the hip and the knee. An appro-priately placed osteotomy that reduces point loading is often successful in alleviating such pain [7]. It would seem reasonable to assume therefore that altering load transmission across a degenerate disc may similarly result in the alleviation of such pain. Furthermore, these changes could be accomplished without the loss of movement in the motion segment. This type of argu-ment has been used to promote the use of dynamic stabilisation devices. Such devices may offload the intervertebral disc by a process of load sharing and limiting abnormal motion, so that painful positions are not experienced [8]. In addition by preserving motion, dynamic stabilisation may, in some way, protect the adjacent level intervertebral disc.
Clinical Results
The Dynesys posterior dynamic stabilisation device (Zimmer Spine, Minneapolis, Minnesota) was devel-oped by Gilles Dubois and first implanted in 1994 [9] (Fig. 5.6.1a, b). The system consists of pedicle screws, polycarbonate urethane spacers and a polyethylene-terephthalate cord. Posterior dynamic stabilisation seeks to allow some movement across the symptom-atic motion segment but to restrict abnormal motion.
Stoll et al. in a prospective multi-centre study evalu-ated safety and efficacy of Dynesys for the treatment of lumbar instability conditions in a consecutive series of 83 patients [9]. Indications included unstable segmental
Immediate Biomechanical Effects of Lumbar Posterior Dynamic Stabilisation
Brian J. C. Freeman and Caspar E. W. Aylott
B. J. C. Freeman (*) Department of Spinal Surgery, Level 3, Theatre Block, Royal Adelaide Hospital, North Terrace, Adelaide, SA 5000, Australia e-mail: [email protected]
5.6

214 B. J. C. Freeman and C. E. W. Aylott
conditions, mainly combined with spinal stenosis (60.2%), degenerative discopathy (24.1%), disc herni-ation (8.4%) and revision surgery (6.0%). Thirty-nine of the 83 patients had a degenerative spondylolisthesis and 30 patients had undergone some form of previous lumbar surgery. In 56 of these 83 patients, dynamic stabilisation was combined with direct spinal decom-pression. A mean follow-up period of 38.1 months was achieved (range 11.2–79.1 months). The mean visual analogue score (VAS) for low back pain improved from 7.4 to 3.1, the mean VAS for leg pain improved from 6.9 to 2.4 and the mean Oswestry disability index (ODI) improved from 55.4 to 22.9. Nine of eight-three patients suffered complications unrelated to the implant including incidental durotomy (2), infection (1), motor weakness (1), dysaesthesia (1), seroma (1), neuroma (1), cardiovascular (1) and thromboembolic complica-tions (1). Complications relating to the implant included two screw misplacements (one requiring re-position) and eight screw loosenings evident on radiographs. A further 11 of 83 required subsequent additional surgery including implant removal, extension of Dynesys, decompression of adjacent segment and laminectomy of the index segment.
Grob et al. studied 31 patients who underwent dynamic stabilisation [10]. The primary indications included spinal stenosis, spondylosis, disc degenera-tion, failed back surgery and degenerative spondylolis-thesis. Forty-two percent of this cohort underwent
decompression surgery, in addition to Dynesys instru-mentation. With an average follow-up of 2.8 years (2–3.6 years), the mean VAS for back pain reduced from 7.0 (SD 2.1) to 4.7 (SD 3.2). The mean VAS for leg pain reduced from 6.6 (SD 2.4) to 3.8 (SD 3.6). When assessing global outcome, 29% of patients said that the procedure had “helped a lot”, 23% stated it had “helped”, 10% said the procedure “only helped a little”, 35% stated the procedure “didn’t help” and 3% claimed to be worse. Overall, approximately two-thirds of patients reported some improvement in their leg/back pain; however, only 40% reported an improvement in their ability to perform physical activity, and just 50% reported an improvement in quality of life. Six of thirty-one (19%) required re-intervention or were being investigated with a view to re-intervention within 2 years. Grob et al. commented that the overall results following dynamic stabilisation were poorer compared to historical controls that had undergone fusion for similar indications. He concluded stating there was still insufficient evidence to suggest that semi-rigid fixation of the lumbar spine resulted in better patient-oriented outcomes when compared to spinal fusion.
Welch et al. reported the 1-year preliminary results in clinical outcomes following insertion of the Dynesys dynamic neutralisation system in 106 patients [11]. This study forms part of a multi-centre randomised prospective Food and Drug Administration (FDA) investigational device exemption (IDE) clinical study.
Fig. 5.6.1 (a) Antero-posterior; and (b) lateral radiographs showing Dynesys stabilisation between L3 and S1. The polyethylene-terephthalate cord and spacer are radiolucent, and therefore, not seen on the radiographs. This patient had intractable low back pain, disc degenera-tion in the lower three lumbar discs on MRI, with positive lumbar discography of the lower three lumbar discs. The L2-3 discogram (control) was negative
a b

2155.6 Immediate Biomechanical Effects of Lumbar Posterior Dynamic Stabilisation
To date, 101 patients from six IDE sites underwent dynamic stabilisation of the lumbo-sacral spine with the Dynesys construct. Indications for surgery included degen erative spondylolisthesis or retrolisthesis (Grade I), lateral or central spinal stenosis and their physicians’ determination that the patient required decompression and instrumented fusion for one or two contiguous spinal levels between L1 and S1.
Clinical outcomes were measured using a tradi-tional VAS for low back and leg pain, and ODI and general health were assessed with the Short Form 12 questionnaire (SF-12). Preliminary results reported for the 101 patient cohort, mean age of 56.3 (range 27–79 years), demonstrated a reduction in the VAS for leg pain from 80.3 to 25.5, a reduction in the VAS for low back pain from 54 to 29.4 and a reduction in the ODI from 55.6 to 26.3 at 12 months. While these results are encouraging, it should be noted that no results are pre-sented for those patients undergoing fusion within this multi-centre randomised prospective trial and, in addi-tion, the follow-up is extremely short at 12 months. One looks forward to the study being completed and the full results being reported.
It appears that outcome following dynamic stabili-sation remains highly variable. Clearly, authors are reporting different indications for surgery. The num-ber of patients having combined decompression and dynamic stabilisation also varies. These confounding factors make direct comparison of different studies very difficult.
Based on promising preliminary findings, dynamic stabilisation now enjoys wide clinical application in Europe, despite the fact that its mechanism of action is still far from clear. This paper seeks to explore the bio-mechanical effects of lumbar posterior dynamic stabi-lisation by literature review. In doing so, it may provide further insight into mechanisms of action and perhaps define technical details that may result in superior out-come for some patients.
Biomechanical Effects of Lumbar Posterior Dynamic Stabilisation
Schmoelz et al. in a cadaveric study compared inter-segmental motions of the intact specimen with those of the dynamic stabilisation system and those of an inter-nal fixator specifically to investigate the effects of both
stabilisation methods on the adjacent segment [12]. Six fresh frozen lumbar spines were used for testing. The soft tissues were dissected and the lumbar spine from L2-L5 was fixed in polymethyl-methacrylate cement in such a manner that the L3-L4 disc was in the horizontal plane. The specimens were placed in the spine tester and loaded with pure moments of ±10 Nm in all the three principle motion planes (flexion/exten-sion, lateral bending and axial rotation). Moments were applied continuously with a constant rate of 1°/s. The specimens were not constrained in any way and motion was recorded using a 3-dimensional ultra-sound-based motion analysis system. Four situations were studied as follows:-
1. The intact spine.2. The de-stabilised spine (a controlled defect was
created at the L3-L4 segment).3. Subsequent stabilisation of the defect at L3-L4 with
the dynamic stabilisation system.4. Stabilisation of the defect in L3-L4 with an internal
fixator.
The range of motion (ROM) and the neutral zone (NZ) for both the bridged and the adjacent segments were determined.
Regarding the bridged segment, for all three planes of motion, the de-stabilised spine showed an increase in the ROM in the NZ compared with the intact spine. Both the Dynesys and the internal fixator reduced the ROM and NZ below that of the intact spine for lateral bend and flexion. In extension, the ROM for the Dynesys was in the range of the intact spine, while the internal fixator showed a decrease in the ROM. In axial rotation, the internal fixator stabilised the segment to a ROM below the magnitude of the intact spine, whereas the Dynesys stabilised the defect, but showed an increased ROM compared with the intact spine.
With regard to the adjacent segment, in general, the ROM in the NZ of the adjacent segments was not affected by the instrumentation of the bridged seg-ment. The results appear to suggest that the dynamic neutralisation system is capable of stabilising an unsta-ble segment sufficiently, but allows more motion in the bridged segment compared to the internal fixator. The adjacent segment does not seem to be influenced by the stiffness of the fixation procedure, under the described loading conditions.
Niosi et al. carried out a 3-dimensional kinematic evaluation of the Dynesys system and specifically

216 B. J. C. Freeman and C. E. W. Aylott
looked at the influence of spacer length on the kine-matic behaviour at the implanted level [13]. The authors used ten fresh frozen cadaveric lumbar spine segments from L2-L5. The L2 and L5 vertebrae were potted in dental stone, such that the L3-L4 disc space remained horizontal. Three-dimensional flexibility tests were conducted on each of the specimens under five different conditions as follows:-
1. Intact spine.2. Injured spine at L3-4 (partial facetectomy. Resection
of supraspinous and interspinous ligament and pos-tero-lateral nucleotomy).
3. Dynesys implant at L3-L4 (standard length spacer).4. Dynesys implant at L3-L4 (long spacer).5. Dynesys implant at L3-L4 (short spacer).
The spine testing machine applied a maximum pure moment of ±7.5 Nm to the top vertebra, while the specimen was allowed to move in an unconstrained 3-dimensional fashion. This continuous moment was applied at a rate of approximately 1.3°/s in all the three primary directions of loading, namely flexion/exten-sion, lateral bending and axial rotation. All tests were conducted with and without the presence of a com-pressive follower load of 600 N to simulate physiologic compressive loading in an in vitro spine study.
The length of the polycarbonate urethane spacer was determined so that a neutral position of the spine was maintained. Spacer lengths 2 mm longer and 2 mm shorter than this standard length were investigated. During flexibility testing, the position of each vertebra was monitored by rigidly attaching four infrared light emitting diodes to each vertebral body. An opto-elec-tronic camera system was used to measure the three -dimensional coordinates of the markers. For the L3-4 segment, the authors calculated the NZ and ROM around the primary axis of rotation and the helical axis of motion (HAM) for the L3-4 segment over the entire motion.
The ROM with the standard length Dynesys spacer was significantly less than the intact and injury condi-tions in all directions of loading. The injury typically increased the NZ, and implantation of the Dynesys gen-erally reduced the NZ to a magnitude below that of the intact spine. The injury did not cause a significant dif-ference in the position or orientation of the HAM com-pared to the intact condition. In all loading conditions there was generally an increase in ROM with a long spacer and a reduction in the ROM with a short spacer,
when compared to the kinematics of the standard length spacer. The NZ was typically greatest with the long spacer and least with the short spacer. There were no significant differences in orientation or location of the HAM between the three spacer lengths. Interestingly, even though ROM was substantially reduced with the implanted Dynesys, a long spacer produced kinematic behaviour that was more similar to that of the intact spine, compared to the other spacer lengths tested.
In summary, the magnitude of ROM in all the load-ing directions with the Dynesys system was signifi-cantly lower than that of the intact and injured specimens. Injury typically increased the NZ, but implantation of the Dynesys restored the NZ to a mag-nitude less than that of the intact spine. Spacer length of the Dynesys did affect the kinematic behaviour. ROM was affected most significantly followed by HAM, and finally, NZ in which no significant differ-ences were observed between the three spacer lengths.
Aylott et al. used stress profilometry to assess the influence of Dynesys on both bridged and adjacent intervertebral discs [14]. Twelve cadaveric segments (L3-L5) were dissected and Dynesys instrumentation was inserted in the lower motion segment (L4/5). The specimen was then mounted in Wood’s metal and placed in the materials testing machine (Fig. 5.6.2). A
Fig. 5.6.2 Posterior view L3-L5 cadaveric specimen mounted on the material testing machine. Note Dynesys instrumentation bridging across the L4-L5 interspace

2175.6 Immediate Biomechanical Effects of Lumbar Posterior Dynamic Stabilisation
preliminary creep cycle was performed. Specimens were compressed to 1 kN in 4° of extension, neutral and 6° of flexion. The stress distribution in the mid-sagittal and antero-posterolateral (oblique) diameter of both the bridged and the adjacent disc was measured, by withdrawing a miniature pressure transducer across the intervertebral disc (Fig. 5.6.3). Compressive stresses were measured in both vertical and horizontal directions. Testing was conducted without instrumen-tation and with three different spacer sizes (+2 mm, neutral and −2 mm). Stress profiles were obtained across the disc with instrumentation removed, to check reproducibility of measurement with prolonged test-ing. The specimen was then subjected to a degenera-tion load and the above sequence repeated. For each stress profile, peak stress in the anterior annulus, peak stress in the nuclear region, peak stress in the posterior annulus and width of the functional nucleus were mea-sured (Fig. 5.6.4).
In the absence of instrumentation, stress peaks in the anterior annulus increased significantly when the load angle was set to 6° of flexion. In extension, stress peaks increased in the posterior annulus. When Dynesys instrumentation was added to the motion segment across L4-5, stress peaks in the anterior annulus were reduced. This was observed in both the flexed and extended pos-tures and was most significant with the −2 mm spacer. The reduction in anterior stress peaks seemed to come at the expense of the posterior annulus, with increased
posterior peaks in neutral and flexed postures. This was most significant with a −2 mm spacer.
Regarding the adjacent level, Dynesys instrumenta-tion had little effect (for all loading angles) on either the posterior annulus or the nucleus pulposus. However, stress in the anterior annulus decreased significantly in extension and increased significantly in flexion. Considering the effect of spacer size, the −2 mm spacer increased posterior annulus stresses both in extension and flexion. The +2 mm spacer did not result in large peak stresses in the posterior annulus. In summary, Dynesys instrumentation demonstrated potential to relieve stress peaks in the anterior annulus of the bridged segment, particularly in positions of flexion. Stress distribution through the adjacent disc remained relatively normal when the inferior motion segment was instrumented, suggesting that the adjacent seg-ment was not biomechanically prejudiced following the application of Dynesys.
Schmoelz et al. similarly studied the influence of dynamic stabilisation on load bearing of a bridged disc by measuring intra-discal pressure [15]. The aim was to investigate the load transfer through discs bridged with a dynamic or rigid stabilisation system and to evaluate the effect of the stabilisation on the intra-dis-cal pressure of the adjacent segments. Six fresh frozen human lumbar spines (L2-L5) were used. All soft tis-sues were dissected with the specimens embedded in polymethylmethacrylate cement and subsequently
Fig. 5.6.4 Example of a stress profile obtained from a non-degenerate intervertebral disc loaded in the neutral position (0°). Note the peak stress in the posterior annulus, nucleus and ante-rior annulus
Peak sress posterior annulus (PA)(horizontal component)
Width of functional nucleus (FN)Peak nuclear stress (NP)
Peak stress anteriorannulus (AA)(horizontal component)
00 10 20 30 40 50 60 70 80 90 100
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
Str
ess
/ M P
a
Position / mm
verticalhorizontal
Fig. 5.6.3 L3-L5 cadaveric specimen mounted on the materials testing machine. Note Dynesys instrumentation across the infe-rior segment (right of picture) with intra-discal pressure trans-ducer in the superior adjacent disc (left of picture)

218 B. J. C. Freeman and C. E. W. Aylott
mounted on a materials testing machine. Care was taken to align the L3-4 disc in the horizontal plane. A flexible pressure transducer with a 1.2 mm diameter was used to measure intra-discal pressures. The speci-mens were loaded with pure moments of ±10 Nm in each of the three principle motion planes (flexion/extension, lateral bend and axial rotation), while the remaining 5° of freedom were allowed to move freely. Four situations were studied as follows:-
1. Intact spine.2. De-stabilised spine (controlled defect created at L3-4).3. Stabilisation of this controlled defect at L3-4 with
internal fixation.4. Stabilisation of this controlled defect at L3-4 with
modified Dynesys.
In general, compared to the intact spine, stabilising the surgical defect with either the Dynesys instrumenta-tion or the internal fixator resulted in unloading of the bridged disc, both in flexion and extension. There was no substantial difference in the intra-discal pressure of the bridged disc when stabilised by the internal fixator or by the Dynesys instrumentation. With regard to the adjacent disc and under the moment-controlled load protocol used in this study, the effects of stabilisation (either internal fixator or Dynesys instrumentation) on the intra-discal pressure of the adjacent discs were negligible.
Cheng et al. studied the immediate biomechanical effects of dynamic stabilisation compared to the tradi-tional rigid rod fixation [16]. Twelve fresh frozen human cadaveric lumbar spines (L1-L5) were acquired for biomechanical testing. Six of the specimens were ran-domised to the dynamic stabilisation group and six were randomised to the traditional rigid rod fixation group. Spines were mounted on a materials testing machine and tested in flexion/extension bending, lateral bending and axial rotation. Each specimen was subjected to the following sequential treatments ordered from the least invasive to the most invasive treatments for the proposed dynamic stabilisation or traditional rigid rod fixation:-
1. Intact.2. De-stabilised (L3-4 discectomy and partial face-
tectomy).3. Posterior instrumentation at the index level (L3-L4).4. Posterior instrumentation extended superiorly
(L2-L3 and L3-L4).5. Posterior instrumentation at the index level (L3-L4)
and cage at L3-L4.
6. Posterior instrumentation extended superiorly (L2-L3) and L3-L4 with cage at L3-L4 – hybrid construct.
The spines were aligned in the simulator and ±6 Nm was applied in flexion/extension, axial rotation and lat-eral bending. The testing was performed at 1°/s with no follower load.
For the instrumented segment (L3-L4), flexion/extension bending and lateral bending were not statis-tically different between those specimens stabilised with dynamic stabilisation and those stabilised with rigid internal fixation. However, axial rotation for those stabilised with Dynesys demonstrated significantly more rotation compared to those specimens stabilised with rigid internal fixation.
For the “adjacent” segment (L2-L3), dynamic sta-bilisation reduced the ROM by 64% of the intact specimen in flexion/extension bending, compared to 91% reduction of the intact specimen ROM for the traditional pedicle screw system. In lateral bending, dynamic stabilisation reduced motion by 50% com-pared to 81% for the traditional pedicle screw sys-tem. In axial rotation, dynamic stabilisation reduced motion by 10% of intact specimen compared to 49% in those specimens stabilised by posterior pedicle screw system. In each mode of loading, the rigid rod fixation reduced motion in the adjacent segment more than the dynamic posterior stabilisation device for treatment six.
For this study, Dynesys appears biomechanically no different compared with rigid rod fixation at the index level under the testing parameters described. What Cheng et al. have demonstrated is that extension of the dynamic stabilisation system to the level above (i.e. L2-3) a circumferential fusion at L3-L4 may help to stabilise the level without excessive rigidity seen with traditional pedicle screw systems.
Schulte et al. investigated the effects of dynamic semi-rigid implants on the ROM of lumbar motion segments after decompression using 21 fresh frozen human lumbar spine motion segments [17]. ROM and the NZ were measured in flexion/extension, lateral bending and axial rotation under four conditions via application of a pure-moment load (−5 to +5 Nm). The four conditions investigated were:-
1. Intact specimen.2. Decompression (transection of supra and infra-
spinous ligament, ligamentum flavum, partial laminectomies, partial facetectomies).

2195.6 Immediate Biomechanical Effects of Lumbar Posterior Dynamic Stabilisation
3. Decompression plus implantation of Wallis instrumentation.
4. Decompression plus implantation of Dynesys instrumentation.
Following decompression, a significant increase in the ROM was observed for flexion/extension, lateral bend-ing and axial rotation. Following insertion of the semi-rigid devices, a restriction in the ROM in all planes was observed for both the Wallis and Dynesys instrumenta-tion. These biomechanical studies would tend to sup-port the hypothesis that the semi-rigid implants provide a primary stabilising function. Whether they can improve the clinical outcome must be verified by a prospective clinical study.
It would be interesting to look at a less aggressive decompression, for example, one carried out using a spinous process osteotomy where the interspinous and supra-spinous ligaments are preserved along with the remnants of the spinous processes, thereby preserving the posterior tension band.
Conclusions
Hypotheses regarding the source of low back pain in degenerative disc disease have advanced the theory that abnormal load transmission across the degener-ated intervertebral disc may be responsible. Posterior dynamic stabilisation systems may provide benefit comparable to fusion techniques but without the need to eliminate motion. Perceived advantages of dynamic stabilisation include preservation of motion within the bridged segment and also the adjacent segment. In addi-tion, as bone graft is not harvested for dynamic stabili-sation of the spine, the morbidity of surgery is reduced.
Early clinical studies with Dynesys have reported promising results; however, many investigators have included a broad range of pathology and combined dynamic stabilisation with spinal decompression. Furthermore, considerable variation exists in the pre-cise surgical technique of dynamic stabilisation; in par-ticular the most appropriate spacer length has not yet been described. Other studies have reported much less favourable results following dynamic stabilisation. A well-defined randomised controlled study comparing dynamic stabilisation to spinal fusion for one and two-level degenerative spondylolisthesis combined with
spinal stenosis has commenced. The longer-term results are eagerly awaited.
This paper has sought to explore the biomechanical effects of lumbar posterior dynamic stabilisation by literature review. In doing so, it has hopefully provided further insight into the possible mechanisms of action and effectiveness of posterior dynamic stabilisation devices.
Studies assessing the ROM and NZ in cadaveric specimens have provided biomechanical evidence that posterior dynamic stabilisation of the lumbar spine allows continued inter-segmental motion within the bridged segment. However, this motion is significantly reduced compared to an intact motion segment, and in some studies, not statistically significantly different from that described to the inter-segmental motion observed following a posterior pedicle screw stabilisa-tion. Spacer length is important, with a longer spacer (+2 mm) allowing a greater range of inter-segmental motion within the bridged segment.
Regarding the adjacent segment, there is evidence, particularly above a circumferential fusion model as part of a hybrid construct, that Dynesys allows more physiological movement in the adjacent segment when compared to a posterior pedicle screw construct. In a surgically-created decompression model, it has been shown that Dynesys instrumentation leads to a restric-tion in the ROM, thereby offering a primary stabilising function.
Studies assessing intra-discal pressure and stress profilometry in both the bridged and adjacent segment have confirmed that dynamic stabilisation off loads the bridged disc and has the potential to relieve stress peaks in both the anterior and posterior annulus, pro-vided the appropriate spacer length is chosen. Dynamic stabilisation may provide pain relief by altering the transmission of abnormal load across the degenerate intervertebral disc. The intervertebral disc of the adja-cent segment appears not to be biomechanically prej-udiced (as it may be following a posterior pedicle screw construct), following the application of poste-rior dynamic stabilisation.
Observing immediate biomechanical effects of lumbar posterior dynamic stabilisation is only part of the answer. Further study is required to determine the optimal implant design, particularly attention should be focused on spacer length. Careful patient selection with well-defined indications and clearly documented adjuvant procedures (such as spinal decompression)

220 B. J. C. Freeman and C. E. W. Aylott
will allow appropriate comparison of clinical studies. It is likely that long-term studies with at least 5–10-year follow-up will be required to show any clear advantage of dynamic stabilisation over and above that observed following spinal fusion.
References
1. Wetzel FT, LaRocca SH, Lowery GL (1994) The treatment of lumbar spinal pain syndromes diagnosed by discography: lumbar arthrodesis. Spine 19:792–800
2. Thomsen K, Christensen FB, Eiskjaer SP et al (1997) 1997 Volvo Award Winner in clinical studies. The effect of pedicle screw insertion on functional outcome and fusion rates in postero-lateral lumbar spinal fusion: a prospective ran-domised clinical study. Spine 22:2813–2822
3. McNally DS, Adams MA (1992) Internal intervertebral disc mechanics as revealed by stress profilometry. Spine 17: 66–73
4. Moore RJ, Vernon-Roberts B, Fraser RD et al (1996) The origin and fate of herniated lumbar intervertebral disc tissue. Spine 21:2149–2155
5. McNally DS, Shackleford IM, Goodship AE et al (1996) In vivo stress measurement can predict pain on discography. Spine 21:2580–2587
6. Mulholland RC, Sengupta DK (2002) Rationale, principles and experimental evaluation of the concept of soft stabilisa-tion. Eur Spine J 11(Suppl 2):198–205
7. Troum OM, Crues JV III (2004) The young adult with hip pain: diagnosis and medical treatment, circa 2004. Clin Orthop 418:9–17
8. Nockels RP (2005) Dynamic stabilisation in the surgical management of painful lumbar spinal disorders. Spine 30(Suppl 16):S68–S72
9. Stoll TM, Dubois G, Schwarzenbach O (2002) The dynamic neutralisation system for the spine: a multi-centre study of a novel non-fusion system. Eur Spine J 11(Suppl 2):S170–S178
10. Grob D, Benini A, Junge A, Mannion AF (2005) Clinical experience with the Dynesys semi-rigid fixation system for the lumbar spine. Surgical and patient-oriented outcome in 50 cases after an average of 2 years. Spine 30(3):324–331
11. Welch WC, Cheng BC, Awad TE et al (2007) Clinical out-comes of the Dynesys dynamic neutralisation system: one-year preliminary results. Neurosurg Focus 22(1):E8:1–8
12. Schmoelz W, Huber JF, Nydegger T et al (2003) Dynamic stabilisation of the lumbar spine and its effects on adjacent segments. J Spinal Disord Tech 16(4):418–423
13. Niosi CA, Zhu QA, Wilson DC et al (2006) Biomechanical characterisation of the three-dimensional kinematic behav-iour of the Dynesys dynamic stabilisation system: an in-vitro study. Eur Spine J 15:913–922
14. Aylott CEW, McKinlay KG, Freeman BJC et al (2005) Dynesys (dynamic neutralisation system for the spine): acute biomechanical effects on the human cadaveric lumbar spine. J Bone Joint Surg 87B Orthop Proc Suppl III:234
15. Schmoelz W, Huber JF, Nydegger T et al (2006) Influence of a dynamic stabilisation system on load-bearing of a bridged disc: an in-vitro study of intra-discal pressure. Eur Spine J 15:1276–1285
16. Cheng BC, Gordon J, Cheng J, Welch WC (2007) Immediate biomechanical effects of lumbar posterior dynamic stabilisa-tion above a circumferential fusion. Spine 32(23):2551–2557
17. Schulte TL, Hurschler C, Haversath M et al (2008) The effect of dynamic, semi-rigid implants on the range of motion of lumbar motion segments after decompression. Eur Spine J 17:1057–1065

221M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_5.7, © Springer-Verlag Berlin Heidelberg 2010
Introduction
Spinal fusion has long been used to treat various painful spinal conditions. Although the results have often been good, intuitively eliminating motion of an organ that was physiologically designed to move is undesirable. With this in mind, we are entering an age of rethinking implant design, ie, moving away from rigid internal fixation devices to those that allow motion. While lumbar total disk replacement (TDR) has been in use for more than 20 years, posterior dynamic devices are much newer. Unfortunately, there are not as many studies available describing their biomechanics, indica-tions/contraindications, and outcomes. In this chapter, we will provide an overview of lumbar pedicle-based dynamic stabilization systems.
Adjacent Segment Degeneration
One of the first authors to publish on the potential of accelerated degeneration next to a fused segment was Casey Lee [1, 2]. He described how fusion added stresses on the adjacent unfused segment, particularly the facet joints. Since that time, there have been numerous publications on the fate of adjacent seg-ments after fusion. The results of these studies have not been consistent. In a recent prospective random-ized study comparing fusion with nonoperative treatment, it was reported that adjacent segment degeneration was more prevalent following fusion [3].
In only the more degenerated segments were the changes found to be related to clinical outcome. The question arises whether motion preserving technology can have a protective effect on the adjacent segment. Studies have supported that maintaining motion through the use of total disk replacements (TDRs) has a protective effect on the segments adjacent to an oper-ated degenerative segment [4, 5].
History of Dynamic Posterior Stabilization
Perhaps one of the earliest dynamic stabilization sys-tems was a spring held in place by hooks, first used in 1963 [6]. Although this was primarily designed to hold bone graft in place, the authors appreciated the semi-rigid immobilization the springs provided. Such early attempts of internal fixation to stabilize the spine gave way to pedicle screw rod systems. A plethora of biome-chanical papers soon followed comparing the stiffness of the various pedicle screw and rod constructs. While it could be shown one construct was stiffer than another, one big question loomed that could not be answered – what is the ideal stiffness? Relatively early after the introduction of pedicle screws, questions arose concern-ing the stress on the adjacent segments following fusion and even the impact of internal fixation on the bone density of adjacent vertebral bodies [7, 8]. In general, the concept of a device being “too stiff” with respect to spinal implants gained acceptance. Unfortunately, the questions remain as to what is the ideal stiffness, do dif-ferent applications ideally require different stiffnesses, and what is the best method to design less stiff or non-rigid devices. This last item is being addressed by the many designs of dynamic stabilization we see today.
Overview of Pedicle Screw-Based Posterior Dynamic Stabilization Systems
Richard D. Guyer, Donna D. Ohnmeiss, and Kevin R. Strauss
R. D. Guyer (*) Texas Back Institute, 6020 West Parker Rd. 200, Plano, TX 75093, USA e-mail: [email protected]
5.7

222 R. D. Guyer et al.
There are fabric rods, flexible rods, jointed rods, spiral cut rods, rods with curves or spirals, and other designs. There tends to be a general consensus among the designs that it is desirable to attach the devices to the spine via pedicle screws. This is one of the attractions of many of the new posterior dynamic stabilization systems. Pedicle screws became commonly used in the 1980s and practi-cally every spine surgeon is trained to use these devices. Originally, these constructs were used to stabilize the spine while bony incorporation of the fusion bone graft occurred. It was almost a natural transition to design future devices based on this familiar technology. Now, there are many options for devices that are all built upon this early pedicle screw concept. While the open place-ment of the screws has not significantly changed, the variety of implants available to attach to them has changed dramatically. Still, the authors are unaware of any significant study proving the efficacy for any of these devices.
As the interest in motion preserving technology has increased for spine, we are now seeing a wide array of flexible, or semirigid, rods as well as facet joint replace-ments that are designed to be implanted using screws or other anchoring devices placed into the pedicles. The purpose of this chapter is to provide an overview of the general design concepts for the many dynamic systems currently available.
Cord-Type Systems
Rather than using rigid metal, one of the earliest designs of a dynamic stabilization system used cords affixed to metallic pedicle screws. The first of these was the Graf ligament, which was made of nylon. The results reported for this device have been mixed [9–15]. Most of the studies suffer from small sample sizes.
Years later, the Dynesys (Zimmer, Inc.) was intro-duced that also used a polyethylene-terephalate cord attached to pedicle screws, and it incorporated poly-carbonate urethane bumpers over the cord to limit extension. The surgical technique for Dynesys requires a 300 N pretension on the cord, thereby placing the plastic bumper in compression and creating a fairly stiff construct at the time of the procedure. The results from studies on this device have also varied with favor-able [16–18] and unfavorable outcomes including
reports of screw loosening, screw malposition, or adja-cent segmental degeneration in 17–19% of patients [19–21]. None of these studies were prospective ran-domized trials. Results from the multicenter FDA IDE Dynesys trial were presented recently comparing dynamic stabilization to posterior fusion in the treat-ment of stenosis, degenerative spondylolisthesis, or retrolisthesis [22]. Both groups improved significantly and the authors indicated that the dynamic group improved significantly more than the fusion group on the outcome measures of back and leg pain.
Semirigid/Flexible Rods
Semirigid, or flexible, rods are designed to provide sta-bility to the spine, but to have some flexibility to reduce stresses on the adjacent segments. Some of the rods are similar to the metal rods of the past but are made of polyetheretherketone (PEEK) [23] or other materials with a modulus of elasticity more similar to bone. How beneficial this characteristic is in posterior dynamic stabilization has yet to be investigated. These types of devices typically provide flexibility along the entire implant length and are attached to metal screws.
A similar metal device called Potomac (K2M, Inc.; Leesburg, VA) provides bending motion about its long axis. The device is made from Nickel-Titanium (NiTi, Nitinol) alloy, also known as Shape Memory Alloy. It is more flexible than a titanium rod, but not signifi-cantly different with respect to load sharing capacity [24]. There are no clinical data available on the use of this device.
While there are many designs of flexible rods avail-able, there are little data from which to determine if they offer benefit over traditional stiffer rods or not using any posterior stabilization at all, particularly when an interbody fusion has been performed.
Curved and Spiral Designs
One means by which to make a metal rod less rigid is to incorporate the concept of spirals or curves into the rod. These designs concentrate the motion in the regions of the curves. One such implant is the (Dynamic Stabilization System; Spinal Concepts, Austin, TX) [25],

2235.7 Overview of Pedicle Screw-Based Posterior Dynamic Stabilization Systems
which consists of a loop of Ø4.0 mm spring grade tita-nium attached to two pedicle screws. Two other systems (BioFlex System; Bio-Spine and the Nitinol Memory loop) incorporate curves into the design of rods made of Nitinol, a shape memory alloy metal [26]. Kim et al. reported favorable results associated with the use of the Nitinol devices at fused and adjacent segments [26].
Jointed Rods
Another design of rods are those that have one or more joints and provide flexibility at only one or a few discrete points along the implant as opposed to semi-rigid or flexible rods that allow motion along the length of the device. Among these designs is the Isobar (Scient’X). This device allows for 2° of bend-ing motion about the long axis of the device as well as axial rotation about its long axis. But, as previously stated, the exact amount and type of motion required are unknown.
Other Means of Providing Motion
One version of a flexible rod is Accuflex (Globus Medical). It provides motion through a spiral cut made into the rod [27]. The degree of flexibility is dependent upon the pitch, width of the cut, and the number of times the spiral cut wraps around the rod. The Accuflex device was offered as Ø6.5 mm rod [27] and approved for single-level fusion. The device has not been sold or marketed for several years. The N Fix (N Spine) has a rod made of titanium and an elastomeric material, which acts as a damper in translational motion. This device is similar to the Agile (Medtronic) device except that it provides translational motion, while the Agile provides only bending motion. Both devices are provided as Ø6.0 mm for connection to pedicle screws and reduce to approximately Ø3.0 mm diameter in the dynamic segment. It is well-known in the industry that the Agile system was removed from the market 2 weeks after it was launched due to failures of the device. One metallic design of pedicle screw-based system allows for changes in the interpedicular distance (Axient; IST, Boston, MA). This device was designed to address a concern that during flexion, the interpedicular distance changes.
This was not a concern when trying to fuse a segment, but potentially is an issue when designing implants for motion. However, there have been no reports published supporting benefits of this design feature.
Total Facet Joint Replacement
Several types of facet joint replacements have been introduced that use a pedicle-based anchoring system. All of these devices are designed for single-level use above the L5-S1 level and primarily for the treatment of spinal stenosis. Unlike the dynamic rods discussed earlier which typically achieve US regulatory approval by claiming substantial equivalence to fusion con-structs, all of these devices will be evaluated in multi-center prospective randomized FDA-regulated trials. One total facet replacement system is the TFAS (Archus Orthopedics; Redmond, WA). This is an all-metal system that has plugs rather than actual screws put into the pedicles and is anchored with PMMA. Preliminary results of the FDA IDE trial were recently presented and were favorable [28].
The TOPS system (Impliant) is designed as a sin-gle-level posterior device requiring four pedicle screws for fixation. It provides 3° of rotational freedom and this flexural assemble is housed within an elastomeric boot. Early results reported were promising [29, 30]. However, the FDA IDE trial in the Unites States was temporarily put on hold due to a device failure. After a redesign, enrollment was reinitiated.
The ACADIA (Facet Solutions) is an all-metal implant whose design incorporates the interface of flat sliding surfaces similar to the anatomy of the facet joint. Six-month follow-up results from a 20 patient IDE pilot study showed a 78% reduction in Oswestry scores and 80% reduction in leg pain scores. (Presented by Regan, North American Spine Society precourse; October, 2008)
Other Devices
The Stabilimax NZ (Applied Spine Technologies) was designed based on the concept of the neutral zone and does not require removal of the facets. The device has springs attached between pedicle screws that allow

224 R. D. Guyer et al.
controlled motion. The FDA IDE trial was temporarily put on hold but has resumed after a device modifica-tion was made.
Devices Designed for Combined Posterior Stabilization and Total Disk Replacement
The use of TDR is limited by the contraindications of facet joint problems or other posterior spinal problems or instability. This gave rise early on to the possibility of combining TDR with dynamic posterior stabiliza-tion or total facet replacement. To date, the authors are aware of only one system being designed for this com-bined intervention. The device is designed to incorpo-rate a two-piece (left and right) TDR (TruDiscPL; Disk Motion Technologies, Boca Raton, Florida) to be implanted using a posterior approach and then supple-mented with dynamic posterior stabilization. The sys-tem has undergone biomechanical testing [31]. No published data on clinical outcome with this device were found.
Indications for Posterior Dynamic Devices
Specific indications for semirigid, or flexible, rods have not been investigated to any degree of rigor in clinical series. The indications described for these sys-tems tend to fall into one or more of several categories: replacement of rigid screw and rod constructs for fusion, as a replacement for fusion altogether (particu-larly in combination with decompression), TDR sal-vage, adjunct to disk decompression, treatment of disk degeneration, and to be combined with TDRs to create a circumferential dynamic replacement. Whether some semirigid implants are better suited for particular indi-cations remains to be determined.
In a letter to the Editor, Gardner et al. described indications for the Graf systems as chronic low back pain unresponsive to nonoperative management with a well-defined source of pain, particularly mild to mod-erate disk degeneration, instability related to decom-pression, no more than grade I spondylolisthesis, and pseudoarthrosis repair to serve as a tension band for interbody procedures [32]. They suggested contraindi-cations to be severe disk degeneration and more than
grade I spondylolisthesis. Their overall statement was that soft stabilization is for soft tissue problems and fusion is for bony problems. Schnake et al. reported on the use of Dynesys as an adjunct to decompression and a replacement for fusion [17]. The authors thought this produced results similar to decompression and fusion with stenosis and spondylolisthesis. Highsmith et al. described three general indications for use of a PEEK rod [23]. These included instability that is treated with a fusion, but there is a desire to put less stress on the adjacent segments – the treatment of a degenerated adjacent segment above a previous fusion, and possible use as a tension band to provide stability even when a solid fusion may not be the goal.
Scott-Young described the use of dynamic posterior fixation as a salvage procedure for problematic TDRs [33]. He discussed that in some patients dynamic sta-bilization could be used to stabilize a TDR segment without sacrificing the benefit of motion at the seg-ment. He also discussed the planned combination of TDR and dynamic stabilization.
Another possibility in using semirigid rods is in “topping off” a fusion. That is, the instrumentation is used to provide stability for bony incorporation to occur at the level of a posterior fusion and the device is extended to the level above to reduce instability. This type of application may be useful in patients undergo-ing decompression at a level above a decompression and fusion. With respect to the suggestion of using semirigid rods for the treatment of painful disk degen-eration, there are little, if any, data to support their use for this application.
Indications for dynamic total facet replacements have been more clearly defined. These devices are designed primarily for patients with stenosis with facet arthropathy as a major component. To date, none of these devices are designed for implantation at the L5-S1 level. Some do include the indications of facet replacement at one level with decompression at adja-cent levels.
Summary
An appreciation for adjacent segment breakdown aris-ing from stiff spinal fusions gave rise to the desire to stabilize the spine, but to do so with less rigid implants. A natural progression seemed to be from using pedicle

2255.7 Overview of Pedicle Screw-Based Posterior Dynamic Stabilization Systems
screws with which most spine surgeons are very famil-iar, and replacing the stiff metallic rods of the past with less rigid implants.
Unfortunately, almost all of the semirigid implants were approved through the 510(k) process in the United States whereby mechanical test data for fusion devices were the predicate. Therefore, no rigorous controlled trials were undertaken for these implants to provide evaluation of these devices for nonfusion applications, as described in the previous section con-cerning indications for use. The only rod-like device to initiate a formal clinical trial as a dynamic stabilization device was the Dynesys. Interestingly, the manufac-turer had received approval for this device as a fusion implant first.
The next step was the development of total facet replacements for the treatment of stenotic patients. While these technologies are exciting, time and data are needed to determine their results.
The concept of dynamic posterior stabilization is appealing. However, a series of clinical trials needs to be initiated to help define the most appropriate indica-tions and contraindications for these implants. Insight may also be gained through the use of national regis-tries to accumulate data for a large number of patients.
References
1. Lee CK (1988) Accelerated degeneration of the segment adjacent to a lumbar fusion. Spine 13:375–377
2. Lee CK, Langrana NA (1984) Lumbosacral spinal fusion. A biomechanical study. Spine 9:574–581
3. Ekman P, Moller H, Shalabi A, Yu YX, Hedlund R (2008) A prospective randomized study on the long-term effect of lumbar fusion on adjacent disc degeneration. North American Spine Society, Toronto, Canada
4. Harrop JS, Youssef JA, Maltenfort M, Vorwald P, Jabbour P, Bono CM et al (2008) Lumbar adjacent segment degenera-tion and disease after arthrodesis and total disc arthroplasty. Spine 33:1701–1707
5. Huang RC, Tropiano P, Marnay T, Girardi FP, Lim MR, Cammisa FP Jr (2006) Range of motion and adjacent level degeneration after lumbar total disc replacement. Spine J 6:242–247
6. Attenborough CG, Reynolds MT (1975) Lumbo-sacral fusion with spring fixation. J Bone Joint Surg Br 57:283–288
7. McAfee PC, Farey ID, Sutterlin CE, Gurr KR, Warden KE, Cunningham BW (1989) 1989 Volvo Award in basic sci-ence. Device-related osteoporosis with spinal instrumenta-tion. Spine 14:919–926
8. McAfee PC, Farey ID, Sutterlin CE, Gurr KR, Warden KE, Cunningham BW (1991) The effect of spinal implant rigidity
on vertebral bone density. A canine model. Spine 16: S190–S197
9. Grevitt MP, Gardner AD, Spilsbury J, Shackleford IM, Baskerville R, Pursell LM et al (1995) The Graf stabilisation system: early results in 50 patients. Eur Spine J 4:169–175
10. Brechbuhler D, Markwalder TM, Braun M (1998) Surgical results after soft system stabilization of the lumbar spine in degenerative disc disease–long-term results. Acta Neurochir (Wien) 140:521–525
11. Madan S, Boeree NR (2003) Outcome of the Graf ligamen-toplasty procedure compared with anterior lumbar interbody fusion with the Hartshill horseshoe cage. Eur Spine J 12: 361–368
12. Konno S, Kikuchi S (2000) Prospective study of surgical treatment of degenerative spondylolisthesis: comparison between decompression alone and decompression with graf system stabilization. Spine 25:1533–1537
13. Hadlow SV, Fagan AB, Hillier TM, Fraser RD (1998) The Graf ligamentoplasty procedure. Comparison with postero-lateral fusion in the management of low back pain. Spine 23:1172–1179
14. Guigui P (1994) Chopin D [Assessment of the use of the Graf ligamentoplasty in the surgical treatment of lumbar spi-nal stenosis. Apropos of a series of 26 patients]. Rev Chir Orthop Reparatrice Appar Mot 80:681–688
15. Kanayama M, Hashimoto T, Shigenobu K, Harada M, Oha F, Ohkoshi Y et al (2001) Adjacent-segment morbidity after Graf ligamentoplasty compared with posterolateral lumbar fusion. J Neurosurg 95:5–10
16. Stoll TM, Dubois G, Schwarzenbach O (2002) The dynamic neutralization system for the spine: a multi-center study of a novel non-fusion system. Eur Spine J 11(Suppl 2):S170–S178
17. Schnake KJ, Schaeren S, Jeanneret B (2006) Dynamic stabi-lization in addition to decompression for lumbar spinal steno-sis with degenerative spondylolisthesis. Spine 31:442–449
18. Putzier M, Schneider SV, Funk JF, Tohtz SW, Perka C (2005) The surgical treatment of the lumbar disc prolapse: nucleot-omy with additional transpedicular dynamic stabilization versus nucleotomy alone. Spine 30:E109–E114
19. Grob D, Benini A, Junge A, Mannion AF (2005) Clinical experience with the Dynesys semirigid fixation system for the lumbar spine: surgical and patient-oriented outcome in 50 cases after an average of 2 years. Spine 30:324–331
20. Wurgler-Hauri CC, Kalbarczyk A, Wiesli M, Landolt H, Fandino J (2008) Dynamic neutralization of the lumbar spine after microsurgical decompression in acquired lumbar spinal stenosis and segmental instability. Spine 33:E66–E72
21. Lee SE, Park SB, Jahng TA, Chung CK, Kim HJ (2008) Clinical experience of the dynamic stabilization system for the degen-erative spine disease. J Korean Neurosurg Soc 43:221–226
22. Davis R, Delamarter R, Wingate J, Sherman J, Maxwell J, Welch W (2008) Twenty-four month results from a prospec-tive randomized controlled IDE study of the Dynesys dynamic stabilization system. North American Spine Society, Toronto, Canada
23. Highsmith JM, Tumialan LM, Rodts GE Jr (2007) Flexible rods and the case for dynamic stabilization. Neurosurg Focus 22:E11
24. Donald G, Cammisa F, Nunley P, Strauss K, Cunningham B, Miz G (2008) In vitro biomechanical analysis of the spine using pedicle screws and rods: Ti-6Al-4V vs. NiTi (Nitinol). Spine Arthroplasty Society, Miami, Florida

226 R. D. Guyer et al.
25. Sengupta DK (2005) Dynamic stabilization devices in the treatment of low back pain. Neurol India 53:466–474
26. Kim YS, Zhang HY, Moon BJ, Park KW, Ji KY, Lee WC et al (2007) Nitinol spring rod dynamic stabilization system and Nitinol memory loops in surgical treatment for lumbar disc disorders: short-term follow up. Neurosurg Focus 22:E10
27. Mandigo CE, Sampath P, Kaiser MG (2007) Posterior dynamic stabilization of the lumbar spine: pedicle based stabilization with the AccuFlex rod system. Neurosurg Focus 22:E9
28. Sachs B, Webb S, Brown C, Wiles D, Castellvi A, Wingo C et al (2008) The Total Facet Arthroplasty System® (TFAS®) in the treatment of degenerative lumbar spinal stenosis: mid-term results of US IDE trial with longest follow-up of 24-months. North American Spine Society, Toronto, Canada
29. McAfee P, Khoo LT, Pimenta L, Capuccino A, Sengoz A, Coric D et al (2007) Treatment of lumbar spinal stenosis with a total posterior arthroplasty prosthesis: implant
description, surgical technique, and a prospective report on 29 patients. Neurosurg Focus 22:E13
30. Guyer RD (2007) Impliant TOPS: total posterior element replacement. In: Szpalski M, Gunzburg R, Le Huec JC, Brayda-Bruno M (eds) Nonfusion technologies in spine surgery. Lippincott Williams and Wilkins, Philadelphia, pp 221–224
31. Goel VK, Kiapour A, Faizan A, Krishna M, Friesem T (2007) Finite element study of matched paired posterior disc implant and dynamic stabilizer (360° motion preservation system). SAS J 1:55–62
32. Gardner A, Declerck GM, Hardcastle P, Markwalder TM, Moon MS, Salanova C et al (2000) Re: The Graf ligamento-plasty procedure. Comparison with posterolateral fusion in the management of low-back pain. Spine 25:273–276
33. Scott-Young M (2007) Posterior dynamic stabilization devices in the coming age of lumbar disc replacement. Neurosurg Focus 22:E14

227M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_5.8, © Springer-Verlag Berlin Heidelberg 2010
The concept of spinal fusion originally arose from the notion that a degenerated motion segment is often “unstable” or shows “movement abnormalities,” and that accordingly, the elimination of motion in the affected segment would prevent it from undertaking the movements associated with the generation of pain. Recent thinking, however, suggests that the prevention of movement per se may not be the most important factor accounting for the success of fusion. For a long time, solid fusion was thought to be a requirement for a successful outcome; however, the results of many recent studies have challenged this concept by show-ing that patients’ self-rated improvements in pain and function after surgery are not directly related to the attainment of solid fusion [1–6].
It is now well accepted that degeneration of the spine is often associated with pain. It has been noted that back pain is primarily related to position or posture, rather than movement of the lumbar spine, and it has, thus, been hypothesized that it is the abnormal pattern of loading associated with degeneration, rather than the abnormal movement itself, which accounts for disk degeneration causing back pain in some patients [7].
The dynamic neutralization system for the spine (Dynesys) is a nonfusion pedicle screw stabilization system that was developed 14 years ago [8]. In view of the arguments presented above and the suggestion that prevention of all movements within fused seg-ments may not only be detrimental to sagittal balance and overall function but may also elicit acceler-ated degenerative changes in neighboring segments,
“soft stabilization” was developed with subsequent optimistic reports [8, 9] of clinical results superior to those of fusion.
Although the system has now been in clinical use for more than a decade, there are few studies in the literature that report on patient-oriented outcome after Dynesys implantation. A report from the originators of the system showed marked reductions in average pain and disability in a group of 73 patients, approximately 3 years after Dynesys instrumentation [8]. However, neither the proportion of patients declaring a success-ful global outcome nor the proportion attaining a clini-cally relevant change in pain or Oswestry disability was reported. Furthermore, the complications reported with the 3-year period were quite considerable.
The aim of the present study was to examine patient-oriented outcomes in a group of 50 patients in whom the Dynesys system had been implanted. This Dynesys group was compared to a larger patient population that underwent instrumented fusion for similar indications.
Materials and Methods
Patients
A total of 50 consecutive patients who had undergone semirigid fixation of the lumbar spine with the Dynesys system took part in the study. Three surgeons were involved. The mean age of the patients at operation was 50 years (SD, 12 years; range, 30–80 years); there were 30 women and 20 men. Comparative data were obtained from 311 patients in our in-house registry who had undergone fusion of the lumbar spine for degenerative conditions.
Semirigid Fixation System for the Lumbar Spine
Dieter Grob, Andrea Luca, and Anne F. Mannion
D. Grob (*) Spine Center, Schulthess Klinik, Lengghalde 2, 8008 Zürich, Switzerland e-mail: [email protected]
5.8

228 D. Grob et al.
The indication for surgery for both groups was degen-erative disease (disk/stenosis/spondylosis) resulting in some form of instability associated with neurogenic or radicular pain, and/or chronic back pain. For 30 of 50 (60%) Dynesys patients and 67% of the fusion patients, the procedure was their first spinal operation. Twenty of fifty (40%) in the Dynesys group and 33% in the fusion group had previously undergone decompression of the same or neighboring segments, and/or fusion of neighboring segments (Table 5.8.1).
Preoperative Evaluation
Preoperative evaluation of the Dynesys group included patient history, imaging, and clinical and neurologic evaluation by the treating surgeon. The data were entered into the hospital’s computerized patient records system.
All the patients in the Dynesys group were contacted by letter and invited to complete a short questionnaire (to be returned in the post) regarding their perceptions of the outcome of surgery. The questionnaire enquired about: pain intensity (0–10 VAS); changes in overall back symptoms and leg symptoms as a result of the operation (categorized in each case as “much improved,” “improved,” “no change,” “worse”); reoperations under-gone since the Dynesys implantation (number and nature of operation); removal of the Dynesys system (yes, no, don’t know); change in work status, quality of life, and ability to perform free-time/sporting activities as a result of the operation (in each case, “much improved,” “improved,” “same,” “worse”); global outcome after surgery (categorized as “helped a lot,” “helped,” “helped
a little,” “no change,” “made things worse”); and whether, in hindsight, the same decision would be made to undergo surgery (yes, no). For the data of the fusion group, the Spine Society of Europe Spine Tango register (www.eurospine.com) was used. Patient-orientated out-come measures, 2 years after surgery, were evaluated using an in-house register comprising the Core Outcome Measures Index (COMI) [10] and questions on global outcome. Since the COMI was not available at the time of the Dynesys evaluation, only the questions that were comparable in both evaluations are presented in this study (pain intensity and global outcome).
Results
There were 5/50 (10%) intraoperative/immediate-postoperative complications in the Dynesys group. In the fusion group, 1.9% (6/311) patients suffered from surgical-related complications.
Examination of the first postoperative radiographs in relation to positioning of the Dynesys screws revealed six cases of “technical error”: in two cases, the screws were positioned extrapedicularly; in two cases, too far laterally (in both these cases, computer assistance had been used); in one case, just one screw had been used, and in one more case, the screws on the right-hand side showed loosening.
None of these technical errors per se caused signifi-cant symptoms or necessitated reintervention. No spe-cific data are available regarding the “technical error” rate of complications of the fusion group.
A total of 8 of 50 (16%) Dynesys patients either required reintervention in the 2-year follow-up or were undergoing further investigative tests with a view to reoperation in the near future. Three patients required revision surgery at the same spinal level with removal of the Dynesys system: in two of these, a rigid fusion was carried out due to implant loosening (after 6 months and 18 months); and in the third, the Dynesys instru-mentation was removed on one side due to infection (after 8 months). One patient required decompression and revision due to radicular pain (after 3 months) and another required a morphine pump, 12 months after the Dynesys instrumentation. One patient underwent metal removal in connection with a spondylodesis carried out 2 years earlier, at the level below that instrumented with Dynesys (12 months after the Dynesys operation). At the time of the present follow-up study, a further two
Table 5.8.1 Demographic and basic clinical data of the two groups, Dynesys and fusion
Dynesys N > 50 Fusion N > 311
Age (mean ± SD; range, y)
50 ± 12 (30–80) 61 ± 13 (21–87)
Gender (% men) 40 31
Previously operated (%)
40 33
Levels operated
1 level (%) 28 372–3 levels (%) 70 634 levels (%) 2 –

2295.8 Semirigid Fixation System for the Lumbar Spine
patients with signs of screw loosening were undergoing consultation, with a view to possible revision; both underwent reoperation shortly after (Dynesys removal and fusion). In the fusion group, 9% of the patients had required reoperations by the 24-months follow-up.
A total of 49 of 50 (98%) Dynesys patients com-pleted and returned the patient-oriented follow-up questionnaire. The remaining patient from whom no questionnaire was received was contacted by telephone to obtain the most basic outcome data. The average questionnaire follow-up duration was 2.1 (SD 1.1) years (range, 0.3–3.6 years; median, 2.3 years).
The patients’ mean (SD) preoperative pain inten-sity, as documented on the preoperative clinical evalu-ation form during the initial consultation, was 7.2 (1.9) for back pain and 6.0 (2.7) for leg pain. At follow-up, the mean (SD) patient self-rated pain intensity was 5.2 (3.2) for back pain and 3.6 (3.6) for leg pain.
In the follow-up questionnaire, the proportions of patients who declared that their back symptoms had resolved, improved, were unchanged, or were worse were 12, 50, 25, and 13%, respectively; the corre-sponding figures for self-rated leg symptoms were 36, 34, 17, and 13%, respectively.
At the time of follow-up, the patients’ self-rated ability to carry out physical activities (sport/hobbies) had “improved” as a result of the operation in 33% patients, was “unchanged” in 40%, and was “worse” in 27%. Overall quality of life had “improved” in 47%, was “unchanged” in 37%, and was “worse” in 16%.
In response to a question enquiring as to whether the patients were in the same job now as before the operation, the following replies were recorded: 20% were in the exact same job as before; 20% were in the same job but only able to work part-time; 4% had changed jobs for personal reasons or due to changes in the job market; 10% had retired on the grounds of age; 25% had gone onto a disability pension due to back problems; and 21% had a different employment status for other reasons.
The patients’ overall self-rating of the global out-come is shown in Table 5.8.2. In hindsight, 68% would make the same decision to undergo surgery, while the remaining 32% reported that they would not.
Approximately, 40% patients underwent decom-pression in addition to the Dynesys instrumentation, making it somewhat difficult to separate out the rela-tive effects of the decompression and those of the sta-bilization on the patients’ self-ratings of pain, disability, quality of life, etc. measured at follow-up. Thus, the various outcome variables were compared between the patients who received Dynesys instrumentation only (D) and those who received Dynesys in addition to decompression (DDec).
There was an overall trend for poorer results in the D group compared with the DDec group, with the dif-ferences for some of the variables (change in quality of life after the operation; and “would you, in hindsight, make the same decision again to undergo the opera-tion?”) approaching statistical significance, even with the small numbers involved. When these same catego-ries were applied to the fusion group, there was no notable difference in favor of the decompression group (Table 5.8.3).
Table 5.8.2 Pain levels and global outcome at the 2-year follow-up in Dynesys and fusion groups
Dynesys N > 50
Fusion N > 311
VAS leg pain at 2 year follow-up (mean ± SD)
3.6 ± 3.6 3.3 ± 3.0
VAS back pain at 2 year follow-up (mean ± SD)
5.2 ± 3.2 3.7 ± 2.8
Global outcome
Helped a lot (%) 28 43Helped (%) 20 32Helped only little (%) 18 14Didn’t help (%) 26 9Made things worse (%) 8 2
Table 5.8.3 Difference in outcome between patients receiving only Dynesys (or only fusion) and those receiving these in addition to decompression
Dynesys (N > 50) Fusion (N > 311)
No decompression (%)
Decompression (%)
No decompression (%)
Decompression (%)
Helped/helped a lot Good 40 60 75 76
Helped only a little Fair 30 0 17 13
Didn’t help made things worse Bad 30 40 8 11

230 D. Grob et al.
Discussion
Fusion is generally considered to be the treatment of choice for painful degenerative conditions of the lum-bar spine that have proven unresponsive to nonopera-tive therapy. The results reported in the literature for the outcome after fusion vary according to patient selection and indication; satisfactory results have been reported to range from 16 to 95%, with an average of about 68% [1]. More recent, large-scale studies con-firm these figures (57% good/excellent [11]; 63% patients “better” or “much better” [5]). For a long time, good results were thought to be dependent on radio-logically confirmed solid fusion, although recent stud-ies in which patients with pseudarthrosis showed the same clinical outcome as patients with solid fusion [2, 6, 11, 12] have challenged this notion. It might, there-fore, be hypothesized that it is the reduction in (rather than the elimination of) segmental motion – brought about by partial fusion, or perhaps even simply by an alteration of the structure of the spinal tissues, induced by the surgery itself – that results in the alleviation of pain. It was on this basis that “nonfusion” concepts for treating painful degenerative disorders of the lumbar spine were developed.
Clinical use of the Dynesys semirigid instrumentation began in 1994. Since then, various individual case studies have been presented, showing restoration of disk height and improvements in Modic changes after Dynesys [9, 13–17] associated with significant pain relief.
In the present study, approximately two-thirds of the patients reported some improvement in their leg/back pain. However, only one-third reported an improvement in their ability to perform physical activ-ities and just under half, an improvement in their qual-ity of life. Less than half declared that the operation had helped or helped a lot. In an analysis of the results of the group of 311 patients who had undergone fusion in our hospital, for the same indication, and by the same surgeons using the same infrastructure, 75% declared that the operation had helped/helped a lot. Naturally, randomized controlled trials would be nec-essary to investigate this with the scientific rigor required to make definitive statements about the rela-tive merits of the two techniques.
In the present study, when the patients who under-went decompression in addition to Dynesys were com-pared with those who only received Dynesys, the
results were generally more favorable for the former group. In the face of such potential confounding fac-tors, caution must be exercised in attributing the results to the Dynesys per se.
Although the group results presented here for Dynesys are not very favorable, there are some patients who clearly benefited from the surgery. No previous studies have identified predictors of success for the Dynesys implant system, either in relation to the surgi-cal indication or to other baseline factors (such as age, gender, diagnostics used, previous operations, baseline pain levels, etc.). The sample size in the present study was not large enough to carry out meaningful multivari-ate analyses to accurately identify predictor variables.
Examination of the purported mechanism of action of the Dynesys system may also shed some light on the issue of the varying individual responses to its implan-tation. When Dynesys first appeared on the market, it was promoted as a device that would allow motion to be “preserved” and “modulated,” i.e., movement would be retained, but at a moderate level in relation to the otherwise unphysiologic, hypermobility displayed by the degenerated segment(s) [18]. However, two biome-chanical studies have shown that, at least in vitro, the range of intersegmental motion after Dynesys instru-mentation is much lower than expected [19, 20]. Independently, both these studies showed that for flex-ion/extension and lateral bending, almost identical ranges of motion were observed for Dynesys instru-mentation and a rigid internal fixator. Only in axial rotation did the Dynesys allow a significantly greater range of motion compared with rigid fixation.
At present, based on our experience, there is no overwhelming evidence to suggest that the Dynesys system performs better than traditional fusion with indications in the degenerative lumbar spine. This statement seems to be confirmed in more recent litera-ture [15, 16, 21, 22]. Ultimately, the elimination of donor site morbidity seems to be the only proven advantage of the Dynesys system.
References
1. Turner JA, Ersek M, Herron L et al (1992) Patient outcomes after lumbar spinal fusions. JAMA 268:907–911
2. Agazzi S, Reverdin A, May D (1999) Posterior lumbar inter-body fusion with cages: an independent review of 71 cases. J Neurosurg 91(Suppl 2):186–192

2315.8 Semirigid Fixation System for the Lumbar Spine
3. Christensen BF, Hansen ES, Laursen M et al (2002) Long-term functional outcome of pedicle screw instrumentation as a support for posterolateral spinal fusion: randomized clini-cal study with a 5-year follow-up. Spine 27:1269–1277
4. Fischgrund JS, Mackay M, Herkowitz HN et al (1997) 1997 Volvo Award winner in clinical studies. Degenerative lum-bar spondylolisthesis with spinal stenosis: a prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 22:2807–2812
5. Fritzell P, Hagg O, Wessbert P et al (2001) 2001 Volvo Award winner in clinical studies: lumbar fusion versus nonsurgical treatment for chronic low back pain. Spine 26:2521–2534
6. Fritzell P, Hagg O, Wessberg P et al (2002) Chronic low back pain and fusion: a comparison of three surgical tech-niques: a prospective multicenter randomised study from the Swedish lumbar spine study group. Spine 27:1131–1141
7. Mulholland RC, Sengupta DK (2002) Rationale, principles and experimental evaluation of the concept of soft stabiliza-tion. Eur Spine J 11(Suppl 2):198–201
8. Stoll TM, Dubois G, Schwarzenbach O (2002) The dynamic neutralisation system for the spine: a multi-center study of a novel non-fusion system. Eur Spine J 11(Suppl 2):170–178
9. Welch WC, Cheng BC, Awad TE, Davis R, Maxwell JH, Delamarter R, Wingate JK, Sherman J, Macenski MM (2007) Clinical outcomes of the Dynesys dynamic neutralization sys-tem: 1-year preliminary results. Neurosurg Focus 22(1):E8
10. Mannion AF, Elfering A, Staerkle R, Junge A, Grob D, Semmer NK, Jacobshagen N, Dvorak J, Boos N (2005) Outcome assessment in low back pain: how low can you go? Eur Spine J 14(10):1014–1026. Epub 2005 Jun
11. France JC, Yaszemski MJ, Lauerman WC et al (1999) A ran-domized prospective study of posterolateral lumbar fusion: outcomes with and without pedicle screw instrumentation. Spine 24:553–560
12. Andersen T, Christensen FB, Hansen ES et al (2003) Pain 5 years after instrumented and non-instrumented posterolat-eral lumbar spinal fusion. Eur Spine J 12:393–399
13. Huber JF (2003) Clinical experience with Dynesys: Synos (Stiftung Förderung der orthopädischen Chirurgie) work-shop: motion preserving instrumentation of the lumbar spine, August 22. Schulthess Klink, Zürich, Switzerland
14. Leu HJ (2003) Clinical experience with Dynesys: Synos (Stiftung Förderung der orthopädischen Chirurgie) work-shop: motion preserving instrumentation of the lumbar spine, August 22. Schulthess Klink, Zürich, Switzerland
15. Schnake KJ, Scharen S, Jeanneret B (2006) Dynamic stabili-zation in addition to decompression for lumbar spinal stenosis with degenerative spondylolisthesis. Spine 31(4):442–449
16. Bothmann M, Kast E, Boldt GJ, Oberle J (2008) Dynesys fixation for lumbar spine degeneration. Neurosurg Rev 31(2): 189–196
17. Schwarzenbach O, Berlemann U, Stoll TM, Dubois G (2005) Posterior dynamic stabilization system: Dynesys. Orthop Clin North Am 36(3):363–372
18. Baumgartner W (2003) Die Synos (Stiftung Förderung der orthopädischen Chirurgie) workshop: motion preserving instrumentation of the lumbar spine, August 22. Schulthess Klink, Zürich, Switzerland
19. Oxland T (2003) In vitro studies of the biomechanics of the Dynesys system: Synos (Stiftung Fo¨ rderung der orthopa¨dischen Chirurgie) workshop: motion preserving instrumentation of the lumbar spine, August 22. Schulthess Klink, Zürich, Switzerland
20. Schmoelz W, Huber JF, Nydegger T et al (2003) Dynamic stabilisation of the lumbar spine and its effects on adjacent segments: an in vitro experiment. J Spinal Disord Tech 16:418–423
21. Scharen S, Broger I, Jeanneret B (2008) Minimum four-year follow up of spinal stenosis with degenerative spondylolis-thesis treated with decompression and dynamic stabilization. Spine. 33(18):E636–E642
22. Grob D, Benini A, Junge A, Mannion A (2005) Clinical experience with the Dynesys semirigid fixation system for the lumbar spine. Surgical and patient-oriented outcome in 50 cases after an average of 2 years. Spine 3:324–331

233M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_5.9, © Springer-Verlag Berlin Heidelberg 2010
Introduction
Stabilization procedures of spinal motion segments in certain situations of segmental “instabilities” are widely used and generally accepted. Until recently, the classic intervention at the lumbar spine consisted in a postero-lateral fusion procedure with or without instrumenta-tion. The need of bone graft or bone graft substitutes on one hand and of nonunion on the other hand needs to be mentioned. Although spinal stabilization and fusion have shown to be efficient in many spine pathologies, there is an ambiguous reputation for spinal fusions for low back pain due to degenerative problems [1, 2]. Independent of the problem addressed, one of the main restraints of spi-nal fusion remains the problem of adjacent level degen-eration, the so-called fusion disease [3, 4]. Therefore, nonfusion devices are promoted in order to prevent adjacent level problems, and furthermore, to facilitate the surgical procedure by avoiding bone harvesting and bone grafting. Besides disk arthroplasty, posterior pedicle-based systems are used for this purpose.
Although many of them have been available for more than 10 years, there is only limited information available regarding indication and long-term outcome, especially when the issue of adjacent level degenera-tion is addressed.
Based on a series of patients treated with dynamic stabilization and the observed technical failures, some fundamental questions do arise:
1. What loads are acting at the each individual motion segment (disk and facet joints)?
2. How can we interfere and to what extent do we need to change the loading pattern acting on the spine with a dynamic implant?
3. Can we apply a prophylactic dynamic stabilization in order to stop the degenerative cascade?
Today, we have to say that the loads acting on the lum-bar spine are not exactly clear. The available data are mainly based on few in vivo measurements that have been performed by telemetric measurements with instrumented implants in patients treated for degenera-tive and traumatic spine instabilities [5, 6] and in vivo intradiscal pressure measurements [7–9, 10]. Models with FE have been developed for many different vari-ables; however, the real mechanical situation in a spi-nal motion segment seems far more complex than the actual models are able to predict [11, 12]. In conse-quence, there is a lack of knowledge regarding the amount of force that is needed to provide sufficient sta-bility in order to do the job required (stabilize the patho-logic motion segment, but prevent adjacent segment degeneration) on one hand. Therefore, on the other hand, it is not really known which mechanical require-ments need to be fulfilled by a dynamic system in order to withstand the occurring loads (which in turn are not really clear). This paradox may be the reason that the indications for these implants remain obscure, and fur-thermore, it might be the explanation that even after extensive in vitro mechanical testing some of these sta-bilization systems did fail during the first clinical trials.
Engineers are able to give very precise information about the mechanical performance of individual implant components; however, one critical aspect represents the load transfer from the implant to the bone: Focusing on
Nonrigid Stabilization of the Spine – Problems Observed: Screw Loosening/Breakage/Implant Failure/Adjacent Segment Degeneration
Paul F. Heini
P. F. Heini Spine & Ortho Center, Klinik Sonnenhof, 3006 Bern, Switzerland e-mail: [email protected]
5.9

234 P. F. Heini
pedicle screw-based systems, the critical area represents the bone – screw interface. From rigid fixation systems we have learned that either screw or rod breakage or screw loosening is observed if no fusion is achieved. So why should this not happen with a dynamic system? The flexibility of the implant should prevent implant failure. But how about the screw-bone interface?
Observed Failures of Different Dynamic Fixation Systems
Dynesis
A case series of failed fixations with the Dynesis sys-tem shows screw loosening/screw migration and screw breakage.
In about 25% of cases (28/120 patients treated over a time period of 5 years), usually within 6 months after the index operation, treatment failure did occur. Loosening was observed most often in younger patients with higher physical activity (16/28). Patients did pres-ent with recurrent pain. Screw loosening was observed with sometimes very extensive bone resorption around the screw (Fig. 5.9.1), otherwise simple screw migra-tion did occur (Fig. 5.9.2). Screw breakage was observed in two cases with a crack about 1 cm from the screw tip. Obviously, the screw tip with its deep flanges at the tap achieved bony ingrowth, whereas the shaft of the screw started to swing in the pedicle (Fig. 5.9.3). Adjacent segment degeneration was an issue for treat-ment failure in ten patients. This was observed within 18 months in average after the index operation (Fig. 5.9.4).
We did not observe failures of the connection of the screw head and the cord or failures of the PCU damper.
Fig. 5.9.1 Screw migration in L4: the postoperative standing film shows correct screw placement in a 34 years old male patient with improved back and leg pain who was operated for a postdiscectomy problem (a, c). Six months after this stabilization the patient started to complain about recurrent pain and at the 1 year FU X-ray, one can find a screw migration (b) and loosening (d). Sometimes screw loosening is not easy to recognize and X-rays have to be assessed very carefully
a b
c d

2355.9 Nonrigid Stabilization of the Spine – Problems Observed
Fig. 5.9.2 Typical failure of bone-screw interface with wide bone resorption around the screws (arrows). Example in a 73 year old man operated for a spinal stenosis due to a degenerative slip at L3–L4. The X-rays were taken 1 year after the index
surgery, the patient was in recurrent pain 6 months after the intervention. The screw motion in the flexion-extension view appears important (dashed and dotted lines)
Fig. 5.9.3 Broken screw removed at S1 only 4 months after a two-level stabilization. The screw breakage occurs typically about 1.5 cm from its tip. Obviously, the deep flanges of the tap promote a bone ingrowth, whereas the shaft of the screw can swing. The breakage occurs at the point of highest stress (dashed line)

236 P. F. Heini
Fig. 5.9.5 Failed dynamic stabilization with a Cosmic system. This patient experienced recurrent leg pain 3 weeks after a decompression and stabiliza-tion. This system shows a monoaxial mobility which does not prevent the so-called wiper effect. In this case the sliding of L3 over L4 is progressing because the facet joints have no frontal orientation. Furthermore, screw loosening was observed at revision probably as a consequence of the rigid rod connection
Fig. 5.9.4 Problem of adjacent segment failure: 72-year old female after decompression and dynamic stabilization (stenosis due to severe osteoarthritis) (a). 3.5 years after the intervention, the patient presents with recurrent symptoms with severe claudication due to a severe degeneration of the adjacent segment stenosis (b)

2375.9 Nonrigid Stabilization of the Spine – Problems Observed
Cosmic
Cosmic is a nonfusion device with a rigid rod but mono-axial mobility (Cosmic) at the screw head, and is used to provide segmental stability without a fusion (Fig. 5.9.5). Among others, the indications include instabilities after decompression (laminotomy, laminectomy, facetec-tomy) [13]. A small series of patients who did need early revision surgery after this type stabilization has been analyzed: all patients underwent a decompression and stabilization for degenerative grade I slippage at L4–L5. Due to a fundamental problem related to this implant by the monoaxial mobility, a translational motion is still possible, which in turn allows a further shift of the vertebrae. Furthermore, the rigid rod is provoking high peak loads at the bone-screw interface, which in turn is the reason for screw loosening in these cases.
Other
In a pilot clinical series, the use of a newly engineered elastic fixation system (SOFI) did fail due to the dis-connection of the metallic part and the PCU damper
unit. Obviously, the loads during flexion of the spine were not anticipated correctly, which in turn led to the early implant failure. The use of the implant was, therefore, discontinued (Fig. 5.9.6).
Review of the Literature
Looking at technical aspects of dynamic stabilization systems reveals a rather high complication rate. For the Dynesis system, Stoll reports the results on 73 patients operated by three spine surgeons – the overall reopera-tion rate after 2 years in this series was 20%, of which 10% were due to implant loosening and implant fail-ure. The radiological rate of loosening is reported as high as 10% [14]. Grob reported a 19% reoperation rate in a series of 31 points and the rate of screw loosening was 16% [15]. Schnake reports on a series of 26 pts with degenerative spondylolisthesis and spinal steno-sis. Over a FU period of 2 years, a 17% rate of screw loosening was observed, however without further clini-cal consequences [16]. This series was followed further with persisting satisfactory outcome after 4 years; espe-cially no further implant failure was observed in com-parison to the 2 year FU [17]. In a prospective case
Fig. 5.9.6 This young female patient is suffering from a Ehlers-Danlos syndrome and underwent a 360° fusion at L4–L5, together with an interspinous stabilization with the Wallis sys-tem 1 year ago (a). A newly designed dynamic stabilization
system was finally implanted due to ongoing pain problems (b), which failed within 2 months due to the underestimation of forces occurring during flexion (c)

238 P. F. Heini
series of 37 patients with spinal stenosis and “dysfunc-tional segmental motion,” Würgler et al. reported a 19% reoperation rate during the first year after the index operation. Screw breakage was observed in four patients; screw loosening was not assessed. The overall outcome was dissatisfactory in 32% of cases assessed by the Stauffer Coventry Scale [18].
Beastall reports on the in vivo MR measurements on 24 patients before and after a dynamic stabilization of the lumbar spine. There were eight single-level stabili-zations, ten double-level, five with three-levels, and one four-level fixations. The motion of the whole lumbar spine was significantly decreased, and in the area of sta-bilization, the range of motion decreased below 5°. This value is often used as the threshold for the definition of a fusion! In other words, the dynamic stabilization sys-tem does reduce the mobility close to a fused motion segment. The anterior disk height over the observed time period did show a significant decrease [19].
Welch et al. provide a summary of a 1-year FU of the investigational device exemption (IDE) study of the FDA for the Dynesis system. Only patients with spinal stenosis were included in this study. The clinical results after 1 year are quoted to be similar as in a stan-dard decompression and fusion procedure. The radio-logical outcome is not mentioned in their report. The 1 year overall reoperation rate was 15% [20]. Kim is reporting a case series of stabilizations with a pedicle screw-based nitinol spring (Nitinol Bio Flex). Hundred and three out of hundred and sixty-five patients have been assessed with a minimum FU of 6 months. Forty-six patients got a monosegmental stabilization, and 57 patients had a hybrid construct with a fusion and an adjacent segment stabilization. One broken screw is reported, and in three levels a halo around the screws was observed [21]. Mandingo reports the use of a flex-ible rod (AccuFlex); however, they did always com-bine the fixation with an interbody fusion. Although the name is making us believe that the system is dynamic, the authors state that “it is not intended as a nonfusion stabilization device” [22].
Conclusions
There is need for nonfusion devices that are able to sta-bilize the spine as much as necessary but preserve motion as much as possible. The problem we have to
face today is that we do not know how much stability is necessary, and technically, how one should trans-form the loads most reliably. None of the available sys-tems stand the proof of prevention of adjacent segment degeneration; the failure rate is definitely higher in comparison to fusion surgery [23]. One should approach the problem stepwise: (a) mono- and bisegmental stabi-lization; and (b) hybrid fixation with fusion and an pro-tective stabilization of the next segment in order to stop fixations, for instance, at L1 or T12, finally get a sys-tem that can be used in a minimally invasive manner that allows to address progressive lumbar spinal defor-mities and hold the viscous circle of degeneration and deformity progression.
References
1. Buttermann GR, Garvey TA, Hunt AF, Transfeldt EE, Bradford DS, Boachie-Adjei O, Ogilvie JW (1998) Lumbar fusion results related to diagnosis. Spine 23:116–127
2. Fritzell P, Hagg O, Wessberg P, Nordwall A (2001) 2001 Volvo Award winner in clinical studies: lumbar fusion versus nonsurgical treatment for chronic low back pain: a multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group. Spine 26:2521–2532; discussion 2532–2524
3. Okuda S, Iwasaki M, Miyauchi A, Aono H, Morita M, Yamamoto T (2004) Risk factors for adjacent segment degeneration after PLIF. Spine 29:1535–1540
4. Penta M, Sandhu A, Fraser RD (1995) Magnetic resonance imaging assessment of disc degeneration 10 years after ante-rior lumbar interbody fusion. Spine 20:743–747
5. Rohlmann A, Bergmann G, Graichen F, Mayer HM (1995) Telemeterized load measurement using instrumented spinal internal fixators in a patient with degenerative instability. Spine 20:2683–2689
6. Rohlmann A, Graichen F, Kayser R, Bender A, Bergmann G (2008) Loads on a telemeterized vertebral body replacement measured in two patients. Spine 33:1170–1179
7. Nachemson A, Morris JM (1964) In vivo measurements of intradiscal pressure. Discometry, a method for the determi-nation of pressure in the lower lumbar discs. J Bone Joint Surg Am 46:1077–1092
8. Sato K, Kikuchi S, Yonezawa T (1999) In vivo intradiscal pressure measurement in healthy individuals and in patients with ongoing back problems. Spine 24:2468–2474
9. Wilke HJ, Neef P, Caimi M, Hoogland T, Claes LE (1999) New in vivo measurements of pressures in the intervertebral disc in daily life. Spine 24:755–762
10. Lee KK, Teo EC, Qiu TX, Yang K (2004) Effect of facetec-tomy on lumbar spinal stability under sagittal plane load-ings. Spine 29:1624–1631
11. Polikeit A, Ferguson SJ, Nolte LP, Orr TE (2003) Factors influencing stresses in the lumbar spine after the insertion of intervertebral cages: finite element analysis. Eur Spine J 12: 413–420

2395.9 Nonrigid Stabilization of the Spine – Problems Observed
12. Rohlmann A, Burra NK, Zander T, Bergmann G (2007) Comparison of the effects of bilateral posterior dynamic and rigid fixation devices on the loads in the lumbar spine: a finite element analysis. Eur Spine J 16:1223–1231
13. Strempel A, Stoos C, Moosmann D, Martin A (2006) Non-fusion stabilization of the lumbar spine in the case of degen-erative diseases with a dynamic pedicle screw rod. Columna 5:27–34
14. Stoll TM, Dubois G, Schwarzenbach O (2002) The dynamic neutralization system for the spine: a multi-center study of a novel non-fusion system. Eur Spine J 11(Suppl 2):S170–S178
15. Grob D, Peyer JV, Dvorak J (2001) The use of plate fixation in anterior surgery of the degenerative cervical spine: a com-parative prospective clinical study. Eur Spine J 10:408–413
16. Schnake KJ, Schaeren S, Jeanneret B (2006) Dynamic stabi-lization in addition to decompression for lumbar spinal steno-sis with degenerative spondylolisthesis. Spine 31:442–449
17. Schaeren S, Broger I, Jeanneret B (2008) Minimum four-year follow-up of spinal stenosis with degenerative spon-dylolisthesis treated with decompression and dynamic stabilization. Spine 33:E636–E642
18. Wurgler-Hauri CC, Kalbarczyk A, Wiesli M, Landolt H, Fandino J (2008) Dynamic neutralization of the lumbar spine
after microsurgical decompression in acquired lumbar spinal stenosis and segmental instability. Spine 33:E66–E72
19. Beastall J, Karadimas E, Siddiqui M, Nicol M, Hughes J, Smith F, Wardlaw D (2007) The Dynesys lumbar spinal sta-bilization system: a preliminary report on positional mag-netic resonance imaging findings. Spine 32:685–690
20. Welch WC, Cheng BC, Awad TE, Davis R, Maxwell JH, Delamarter R, Wingate JK, Sherman J, Macenski MM (2007) Clinical outcomes of the Dynesys dynamic neutralization system: 1-year preliminary results. Neurosurg Focus 22:E8
21. Kim YS, Zhang HY, Moon BJ, Park KW, Ji KY, Lee WC, Oh KS, Ryu GU, Kim DH (2007) Nitinol spring rod dynamic stabilization system and Nitinol memory loops in surgical treatment for lumbar disc disorders: short-term follow up. Neurosurg Focus 22:E10
22. Mandigo CE, Sampath P, Kaiser MG (2007) Posterior dynamic stabilization of the lumbar spine: pedicle based stabilization with the AccuFlex rod system. Neurosurg Focus 22:E9
23. Fritzell P, Hagg O, Nordwall A (2003) Complications in lumbar fusion surgery for chronic low back pain: compari-son of three surgical techniques used in a prospective ran-domized study. A report from the Swedish Lumbar Spine Study Group. Eur Spine J 12:178–189

241M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_5.10, © Springer-Verlag Berlin Heidelberg 2010
Introduction
Lumbar spinal stenosis (LSS) is a common condition in elderly patients and also one of the most common rea-sons to perform spinal surgery at an advanced age [1].
Even though stenosis and claudication have been described as early as 1883 [2], the modern description of this pathology was performed by Verbiest in the fif-ties [3].
Spinal stenosis leading to radiculopathy or neuro-genic claudication can be caused by different factors, of which a number are related to degenerative pro-cesses. The real participation of the so-called congeni-tal stenosis is still a subject of debate.
Some definitions need to be clarified. The classic symptom characterizing spinal stenosis is neurogenic claudication. The pathophysiology of this phenome-non is not entirely understood. However, Porter has proposed an elegant theory [4, 5]. In this explanation, claudication is caused by the venous pooling, induced by the stenotic impairment of venous drainage at root level, and will only occur if stenosis (central and/or lateral) is present at two adjacent levels. This situation is, however, not the rule, and many stenotic patients do not present with true neurogenic claudication. Often complaints linked to stenosis are sciatic pain due to the direct compression of neural structures.
Identification of stenotic images in the mid and exit zones of the foramen has been made possible by MRI studies, and it was found that stenosis could be found in up to 80% of subjects over seventy [6].
Dynamic Nature of Lumbar Stenosis
LSS is characterized by a narrowing of the spinal canal with encroachment of the neural structures from degenerated or hypertrophied osteoligamentous struc-tures. Decreased disk height, bulging of the posterior annulus, and buckling of the ligamenta flava are among the most common viscoelastic structures contributing to LSS, while hypertrophic facet joints and laminar thickening are among the major osteogenic contribu-tors to the narrowing of the spinal canal and neurofo-ramina. It is well established that the diameter of the spinal canal decreases during extension [7], which in turn amplifies stenotic conditions in the presence of degenerative changes.
The functional status of the spine has also been studied in relation to stenosis and the worsening of symptoms during extension. It has been shown that subjects with stenotis changes inducing a have abnor-mal patterns motion in sagittal extension [8]. This sug-gests a sort of proprioceptive protective behavior in case of potentially stenotic movements.
Classical Treatment
When standardized conservative treatment fails in LSS patients, the standard of care consists of surgical decom-pression. Of concern in decompressive lumbar spinal surgery is the creation of instability as a consequence of the degenerative nature of LSS [9]. Segmental instabil-ity is often considered a cause for low back pain mostly related to degenerative processes. Subsequently, more invasive methods have been developed including rigid stabilization and fusion systems with pedicle screw fixa-tion [10].
Interspinous Implants: State of the Art and Research of Evidence
Marek Szpalski, Robert Gunzburg, Christopher J. Colloca, and Robert J. Moore
M. Szpalski (*) Department of Orthopedic Surgery, Hôpitaux Iris Sud, Université Libre de Bruxelles, 142 rue Marconi, 1190 Brussels, Belgium e-mail: [email protected]
5.10

242 M. Szpalski et al.
Accelerated adjacent segment disk degeneration from abnormal load sharing is also a concern with implantation of rigid systems [11]. As a result, dynamic stabilization systems have been developed to prevent overloading of adjacent spinal segments.
Some of these involve implants secured to the spine by pedicle screw fixation such as the Graf [9] and Dynesis [12] systems. In spite of encouraging early results of pedicle screw systems for flexible interver-tebral stabilization [13, 14], some long-term results were less optimistic [15, 16]. Increased lumbar lordo-sis, stretching of the Dacron parts, mal-positioning, and/or loosening of pedicle screws have been reported as reasons for failure.
Interspinous Processes Implants
Due to the dynamic nature of spinal stenosis and neu-rogenic claudication, it appeared logical to prevent the harmful extension motion of affected segment(s) by fitting some kind of device between adjacent spinous processes.
However, the first interspinous implant, the Wallis (Abbott Spine), was not proposed as a treatment for stenosis, but as an alternative to fusion in disk degenera-tion and instability, and was used with a tension band around the spinous processes [17]. This implant uses Polyetheretherketone (PEEK), is fixed to the spine by two bands looped, and tensioned around the adjacent spinous processes [18].
It was hypothesized that, combined with a tension band, stabilization could also be obtained in flexion, thereby avoiding the need for pedicle screw fixation [18]. Little biomechanical data exist to support these notions.
Later, different interspinous implants have been developed to assist in providing dynamic spinal stabi-lization in order to avoid or supplement LSS decom-pression. The principle of all these systems consists of inserting the spacer between the spinous processes at the stenotic level in order to increase the intervertebral space and stretch the ligamenta flava and posterior annular fibers, thereby enlarging both the central canal and neuroforamina [19, 20]. Little is known, however, about how these interspinous implants influence the in vivo range of motion (ROM) of the lumbar spine.
Moreover, they offer the advantage of being much less invasive than pedicular systems, some even being
implanted percutaneously. The procedure is fast and without major difficulty and not linked to any major complications. If needed, it can even be performed in lateral prone and under local anesthesia.
Several such experimental implants have been developed, some connecting spinous processes and laminae [21], others placed between two adjacent spinous processes with a spring [22], one with a sili-cone implant [23].
A number of devices are in commercial use and that number grows rapidly.
The X-stop Interspinous Process Distraction System (Medtronic) is the first device having been proposed specifically for spinal stenosis and has been the subject of a multicenter prospective-controlled study which, despite some methodological flaws, gave the first evi-dence supporting use of an interspinous device. It compared the device with nonoperative treatment with a Zurich Claudication Questionnaire [24], and quality of life as measured with SF-36 also appears improved [25]. Clinical results seem to be maintained at 4 years [26]. Cadaveric studies show that X-Stop appears to decrease intradiscal pressure [27] and unload the facet joints [28], while not modifying adjacent level kine-matics [20].
The Coflex (Paradigm Spine) is a U-shaped tita-nium device attached to the adjacent processes. The shape allows for a certain degree of elasticity and appears to restore a degree of stability in destabilized cadaveric spines mostly in extension [29]. A nonran-domized study comparing Coflex with PLIF and decompression in patients with stenosis and instability showed similar clinical results, but less hypermobility at adjacent segments in the Coflex group. A modified version with more rigid attachment to the processes appears too efficient to restore a certain degree of sta-bility in motions other than extension in destabilized cadaver spines and could be used as an adjunct fixation for fusion surgery [30].
The Diam (Medtronic) is a polyester-encased sili-cone implant secured with a band to the spinous pro-cess. Contrarily to the two previous devices, it allows for unilateral insertion. A cadaveric study showed that the device can restore the increased motion observed after discectomy [31]. The safety of the device was assessed at 1 year compared to similar surgery without implantation. There were no differences in clinical results measured by VAS and MacNab outcome or disk height, but some processes fractures and a slight

2435.10 Interspinous Implants: State of the Art and Research of Evidence
kyphosis. [32]. A retrospective study showed good results, but was methodologically flawed [33].
Other devices are becoming available in increasing number, but without much data. Some are to be used percutaneously like the Aprius (Medtronic) or the Inspine (Synthes). While an appealing solution, percu-taneous insertion may be challenging in the presence of marked facet hypertrophy, often present in elderly degenerative patients.
While some surgeons (and companies) try to stretch the indications of interspinous implant beyond spinal stenosis, like instability, or associated with discectomy, there is no evidence in those domains, and failures have been reported when used to prevent recurrent disk herniations [34] or in presence of degenerative spon-dylolisthesis [35].
Although rare, some complications have also been reported including foreign body responses to polyeth-ylene wear [36].
A recent biomechanical study compared the behav-ior of Coflex, Diam, Wallis, and X-Stop on intra-discal pressure and restabilization of destabilized spinal segments. The four implants strongly stabi-lized and reduced intradiscal pressure in sagittal exten-sion but had almost no effect in the other planes of motion [28].
Evidence About the Effect of an Added Tension Band
The InSwing® (Orthofix Spinal Implants) is a novel device allowing unilateral insertion with self-locking and self-positioning, thanks to a self-opening wing system (Fig. 5.10.1). Once open, the vertical pressure of the adjacent spinal processes keeps the wings locked in open position. The instrumentation allows for a uni-lateral insertion (Fig. 5.10.2) by means of mirrored hook-shaped tension band inserters who are passed blindly around the adjoining spinous processes, allow-ing to stay close to the bone without involving the erector spinae muscle on the other side. It also differs from other devices in that it can be used alone or with a tension band around the adjacent processes. Cadaveric studies showed that a calculated tensioning torque of the band has a direct effect on stabilization and open-ing of disk and foramens [37].
An in vivo animal study demonstrated the important stabilizing effect of the banding during flexion [38]. Ten adolescent Merino lambs (24–30 kg) were used for the study. A destabilization procedure was performed at the level of L1–L2 on both sides, thereby simulating an instability resembling stenotic degenerative spon-dylolisthesis. Following general anesthesia, the animal
Fig. 5.10.1 (a) Insertion of the InSwing® interspinous device is accomplished via a unilateral approach. (b) Following insertion, the wings of the device automatically open (c) on the contralateral side thus securing the implant between the spinous processes. (d) Following insertion, longitudinal pressure cranially and caudally insure its placement

244 M. Szpalski et al.
Fig. 5.10.2 Insertion of the 8-mm InSwing® interspinous device demonstrating (a) the self-pivotating (opening) L-shaped wings allowing for unilateral insertion. (b) Once inserted through the interspinous space, the wings automatically open on the contralateral side securing the implant between the spinous processes
Fig. 5.10.4 Sagittal plane radiographs of the ovine lumbar spine demonstrating the Cobb method of lumbar analysis of L1–L2 of the initial condition (a) and with the InSwing® device in place (b)
was placed in a side-lying posture and lateral radio-graphs were taken in full flexion and extension of the trunk. Each radiograph was centered at the level of L1–L2. The same radiographic protocol was repeated following the insertion of an 8-mm InSwing® inters-pinous device at L1–L2. This insertion required only a minimal dissection of the paraspinal muscles on the left side. The supraspinous ligament remained intact as did the paraspinal muscles on the contralateral side. Finally, a tension band (Fig. 5.10.3) was passed in the implant and around the L1 and L2 spinous processes and tight-ened to 1 N/m, another new set of flexion–extension radiographs were acquired. The tension was obtained with a proprietary dynamometric band tightening device provided by the implant manufacturer and enforced by securing the band with metal clips. Intersegmental ROM was assessed in each of the conditions and com-pared using Cobb’s method at the superior endplate of L1 relative to the inferior endplate of L2 (Fig. 5.10.4).
Fig. 5.10.3 The tension band is looped through prefabricated holes in the InSwing® interspinous device and subsequently secured around the adjacent spinous processes of L1 and L2 and then tightened to a tension of 1 N/m and fixed with metal clips

2455.10 Interspinous Implants: State of the Art and Research of Evidence
Following the first test condition, the L1–L2 destabili-zation procedure, the mean total sagittal plane interseg-mental ROM was 6.3 ± 2.7°. After instrumentation with the InSwing® interspinous implant, the mean total sag-ittal plane ROM was reduced by 15.9% to 5.3 ± 2.7°. The addition of the tension band, the third test condi-tion, resulted in a 42.9% reduction in total sagittal plane ROM to 3.6 ± 1.9°, as compared to the initial ROM results following the destabilization procedure. These reductions in total sagittal plane ROM, as a result of the implant itself (p > 0.47) and then the addition of the ten-sion band (p > 0.06), were not statistically significant. The mean observed lumbar flexion ROM following the destabilization procedure was 14.3 ± 1.8°. The addition of the interspinous implant without the tension band resulted in an insignificant (p > 0.74) 1.4% reduction in lumbar flexion. In contrast, a 15.4% reduction in lum-bar flexion ROM was observed when comparing mean results following the destabilization procedure (14.3 ± 1.8°), to readings made after instrumenting with the InSwing® interspinous implant and securing with the tension band (12.1 ± 3.0°). This reduction in lumbar flexion ROM with the addition of the implant and ten-sion band was statistically significant (p > 0.01). Figure 5.10.5 summarizes the mean changes in lumbar extension, flexion, and ROM from the initial condition, preimplant, to those measurements obtained following
implantation with the interspinous device, and those with the addition of the tension band to the interspinous device.
Additionally, this in vivo animal study was used to determine the effect of the interspinous implant on lum-bar spine stiffness during exposure to acute dorsoven-tral (DV) loading. The same lambs were mechanically tested in vivo using a validated computer-controlled force application apparatus designed to quantify DV stiffness [39]. The anesthetized sheep were placed prone on a stainless steel operating table, which included a rigid (wood) support beneath the abdomen (just caudal to the ribcage). The support was designed to orient the long axis of the sheep spine parallel to the operating table and perpendicular to the load actuator and second-arily to stabilize the trunk. Foam blocks were also placed on either side of the sheep abdomen to further stabilize the trunk along the medial–lateral axis (Fig. 5.10.6). Oscillatory (2 Hz) loads (~5% of body weight) were applied to the L2 spinous process using the stylus of the actuator under load control and with the animals lying prone on an operating table. Load and displacement at L2 were collected at a sampling rate 2,500 Hz. DV stiffness (load/deformation, N/mm) was determined over six trials of 20 cycles of loading, and averaged. Four spinal conditions were examined: the initial intact condition (A), following a destabilization procedure at the L1–L2 level simulating a stenotic degenerative spondylolisthesis (B), following the insertion of an 8 mm InSwing® interspinous device at L1–L2 (C), and again with the implant secured by means of a tension band tightened to 1 N/m around the interspinous processes of L1 and L2.(D). Stiffness comparisons for each condition were performed using a one-way balanced analysis of variance (ANOVA). To specifically identify which pairs of means (i.e., which conditions) were different, if any, a Tukey’s honestly significant difference (hsd) multiple comparison test was employed at a significance level of a > 0.05.
The mean stiffness (± standard deviation) for the intact (A), destabilization (B), InSwing® (C), and InSwing® with tension band (D) conditions were 4.99 ± 0.89, 4.89 ± 0.82, 4.82 ± 0.92, and 5.00 ± 1.20 N/mm, respec-tively. Results from the one-way ANOVA confirmed that significant differences (p < 0.0001) exist in the mean stiff-ness between the following conditions: (A) and (B), (A) and (C), (B) and (D), and (C) and (D). In contrast, there were no significant differences in mean stiffness between conditions (A) and (D), and (B) and (C).
Fig. 5.10.5 Mean changes in lumbar extension, flexion, and range of motion (ROM) from the initial preimplant condition to those measurements obtained following the implantation of the interspinous device and with the addition of the tension band. Error bars represent the standard deviations of the mean. The asterisk denotes a significant difference (p < 0.05)
Pre Implant0
2
4
6
8
10
12
14
16
18
20
Deg
rees
With Implant No Band With Implant With Band
Extension
Flexion
ROM

246 M. Szpalski et al.
The InSwing® interspinous device, with the addi-tion of the tension band, restored spinal stiffness back to the intact condition.
The importance of the tension band is confirmed in our findings showing that the addition of the tension band significantly reduced lumbar flexion ROM, pro-viding increased stability to the lumbar spine.
Only a few other studies have investigated inters-pinous implants secured with tension bands. Floman et al. [34] used the Wallis device after primary disk excision in the hope of reducing recurrent disk hernia-tion. In their nonrandomized study, they found the implant to probably be incapable of reducing the inci-dence of recurrent herniation. In a literature review by Christie et al. [40], the mechanisms of action and effectiveness of interspinous distraction devices were investigated. They [40] report dynamic stabilization as a system that favorably alters the movement and load transmission of a spinal motion segment, without the intention of fusion of the segment. In other words, such a system would restrict motion in the direction or plane that produces pain, or painful motion, but would other-wise allow a full ROM. The authors of that study report that, despite some variation in their proposed indica-tions, interspinous implants share the mechanism of limiting extension of the lumbar spine and, as a result, appear to improve clinical symptoms [40].
Degenerative spondylolisthesis, however, often causes segmental instability leading to segmental spi-nal stenosis resulting from the anterior slip of the cephalad vertebra. In the current study, an appreciable linear decrease in intersegmental ROM was observed following the introduction of the InSwing® interspinous
device, which was further accentuated with the addi-tion of the tension band. These findings therefore pro-mote the indication for the use of such implants to increase spinal stability, at least in the sagittal plane. Indeed, we believe that the observed reduction of flex-ion in this study corresponds with a decrease of ante-rior slippage in degenerative spondylolisthesis. To which extent, a 15% limitation of flexion as observed in the current study would equate to a similar reduction in the human cannot be ascertained from these data. Further in vivo in human studies will assist in under-standing the clinical utility of the InSwing®.
In related work, Kim et al. [32] researched the effects of the DIAM by looking at disk height 1 year after surgery. The study did not, however, include an evaluation of the kinematic stabilization effects of the implant. Phillips et al. [31] performed an in vitro study similar to the current study using the DIAM. In their work, these researchers investigated changes in motion of the lumbar spine with the DIAM device, after par-tial facetectomy and discectomy, in flexion–extension, lateral bending, and axial rotation. Their specimens were tested under the following conditions: [19] intact, [37] after unilateral hemifacetectomy at L4–L5, [40] #2 and discectomy, and [7] #3 with DIAM. Angular motion values at the operated and adjacent segments were assessed. Their findings suggest that insertion of the DIAM device after discectomy restored the angu-lar motion to below the level of the intact segment in flexion–extension [31]. The authors concluded that the DIAM device is effective in stabilizing the unstable segment, reducing the increased segmental flexion–extension, and lateral bending motions observed after
Fig. 5.10.6 Schematic diagram of the computer-controlled mechanical testing apparatus positioned over the ovine L3 spinous process of the prone-lying sheep. The apparatus consisted of an actuator assembly comprised a voice coil actuator, linear variable differential transformer, load cell, and stainless steel indenter. The actuator assembly was attached to a stainless steel and aluminum load frame that was rigidly mounted on the stainless steel operating table. Wood and foam supports were used to position and stabilize the sheep trunk and abdomen during the application of dorsoventral (DV) forces Foam Neck support Operating table surface
Indenter
Wood support
Operating table clamp (×2)
Stainless steel tubingcross–supports (×2)
Stainless steel uprightsupports (×4)
Aluminum supportframe (×2)
Foam abdomenSupports (×2)
Computer–controlledvoice coil actuator
Actuator clamp
Belts

2475.10 Interspinous Implants: State of the Art and Research of Evidence
discectomy. Their study neither investigated the use of the implant with or without the tension band, nor gave any indication as to the amount of tension applied on the band.
The interspinous device investigated tended to reduce the total sagittal ROM at the level of the implant; however, the results were not significant. The addition of a tension band was found to significantly stabilize the spine in flexion. To our knowledge, this is the first in vivo study radiographically showing the advantage of using an interspinous device (InSwing®) to stabilize the spine in flexion. These results are particularly important in light of the nonfusion devices currently proposed for patients with clinical symptoms of insta-ble degenerative spondylolisthesis.
Results of a prospective study at 1 year showed marked clinical improvement as measured by ODI and VAS, as well as increase of the foramen surfaces (Fig. 5.10.7) [41].
Conclusions
Interspinous implants represent a logical treatment for spinal stenoisis and, indeed, there is acceptable evidence to support that indication. There are many products on the market, but we feel that a unilateral approach and total preservation of the supraspinous ligament are para-mount characteristics. The latter ligament plays a non-negligible role in the stability of the spine in flexion.
Care must be taken not to extend the indications without further evidence to avoid too wide a use which will result in inevitable failures.
References
1. Szpalski M, Gunzburg R (1998) The role of surgery in the management of low back pain. Baillieres Clin Rheumatol 12(1):141–159
2. Lane WA (1893) Case of spondylolisthesis associated with progressive paraplegia: laminectomy. Lancet 1:991
3. Verbiest H (1954) A radicular symptom from developmental narrowing of the lumbar vertebral canal. J Bone Joint Surg 36B:230–237
4. Porter RW, Ward D (1992) Cauda equina dysfunction: the significance of multiple level pathology. Spone 17:9–15, 23
5. Porter RW (2000) Vascular compression theory. In: Gunzburg R, Szpalski M (eds) Lumbar spinal stenosis. Lippincott Williams and Wilkins, Philadelphia, pp 159–162
6. Sasaki K (1995) Magnetic resonance imaging findings of the lumbar nerve root pathway in patients over 50 years old. Eur Spine J 4:71–76
7. Dai LY, Xu YK, Zhang WM, Zhou ZH (1989) The effect of flexion-extension motion of the lumbar spine on the capacity of the spinal canal. An experimental study. Spine 14:523–525
8. Szpalski M, Michel F, Hayez JP (1996) Determination of trunk motion patterns associated with permanent or transient stenosis of the lumbar spine. Eur Spine J 5:332–337
9. Fujiwara A, Tamai K, An HS, Kurihashi T, Lim TH, Yoshida H, Saotome K (2000) The relationship between disc degeneration, facet joint osteoarthritis, and stability of the degenerative lumbar spine. J Spinal Disord 13:444–450
10. Resnick DK, Choudhri TF, Dailey AT, Groff MW, Khoo L, Matz PG, Mummaneni P, Watters WC III, Wang J, Walters BC, Hadley MN (2005) Guidelines for the perfor-mance of fusion procedures for degenerative disease of the lumbar spine. Part 9: fusion in patients with stenosis and spondylolisthesis. J Neurosurg Spine 2:679–685
11. Levin DA, Hale JJ, Bendo JA (2007) Adjacent segment degeneration following spinal fusion for degenerative disc disease. Bull NYU Hosp Jt Dis 65:29–36
12. Stoll TM, Dubois G, Schwarzenbach O (2002) The dynamic neutralization system for the spine: a multi-center study of a novel non-fusion system. Eur Spine J 11(Suppl 2):S170–S178
13. Freudiger S, Dubois G, Lorrain M (1999) Dynamic neu-tralisation of the lumbar spine confirmed on a new lumbar
Fig. 5.10.7 Implantation of InSwing® at L4 and L5 level. Although the implant is made of Polyetheretherketone (PEEK), the titanium markers enable to verify positioning. Note the pres-ervation of adequate lordosis

248 M. Szpalski et al.
spine simulator in vitro. Arch Orthop Trauma Surg 119: 127–132
14. Grevitt MP, Gardner AD, Spilsbury J, Shackleford IM, Baskerville R, Pursell LM, Hassaan A, Mulholland RC (1995) The Graf stabilisation system: early results in 50 patients. Eur Spine J 4:169–175
15. Grob D, Benini A, Junge A, Mannion AF (2005) Clinical experience with the Dynesys semi-rigid fixation system for the lumbar spine: surgical and patient-oriented outcome in 50 cases after an average of 2 years. Spine 30:324–331
16. Rigby MC, Selmon GP, Foy MA, Fogg AJ (2001) Graf liga-ment stabilisation: mid- to long-term follow-up. Eur Spine J 10:234–236
17. Senegas J (1991) Surgery of the intervertebral ligaments, alternative to arthrodesis in the treatment of degenerative instabilities. Acta Orthop Belg 57S:221–6
18. Senegas J (2002) Mechanical supplementation by non-rigid fixation in degenerative intervertebral lumbar segments: the Wallis system. Eur Spine J 11(Suppl 2):S164–S169
19. Bono CM, Vaccaro AR (2007) Interspinous process devices in the lumbar spine. J Spinal Disord Tech 20:255–261
20. Lindsey DP, Swanson KE, Fuchs P, Hsu KY, Zucherman JF, Yerby SA (2003) The effects of an interspinous implant on the kinematics of the instrumented and adjacent levels in the lumbar spine. Spine 28:2192–2197
21. Leahy JC, Mathias KJ, Heaton A, Shepherd DE, Hukins DW, Deans WF, Brian MW, Wardlaw D (2000) Design of spinous process hooks for flexible fixation of the lumbar spine. Proc Inst Mech Eng [H] 214:479–487
22. Laudet CG, Elberg J-F, Robine D (1993) Comportement biomécanique d’un ressort inter-apophysaire vertébral pos-térieur analyse expérimentale du comportement discal en compression et en flexion/extension. Rachis 5
23. Minns RJ, Walsh WK (1997) Preliminary design and experi-mental studies of a novel soft implant for correcting sagittal plane instability in the lumbar spine. Spine 22:1819–1825
24. Zucherman JF, Hsu KY, Hartjen CA, Mehalic TF, Implicito DA, Martin MJ, Johnson DR, Skidmore GA, Vessa PP, Dwyer JW, Puccio ST, Cauthen JC, Ozuna RM (2005) A multicenter, prospective, randomized trial evaluat-ing the X STOP interspinous process decompression system for the treatment of neurogenic intermittent claudication: two-year follow-up results. Spine 30:1351–1358
25. Hsu KY, Zucherman JF, Hartjen CA, Mehalic TF, Implicito DA, Martin MJ, Johnson DR 2nd, Skidmore GA, Vessa PP, Dwyer JW, Cauthen JC, Ozuna RM (2006) Quality of life of lumbar stenosis-treated patients in whom the X STOP interspinous device was implanted. J Neurosurg Spine 5(6):500–507
26. Kondrashov DG, Hannibal M, Hsu KY, Zucherman JF (2006) Interspinous process decompression with the X-STOP device for lumbar spinal stenosis: a 4-year follow-up study. J Spinal Disord Tech 19(5):323–327
27. Swanson KE, Lindsey DP, Hsu KY, Zucherman JF, Yerby SA (2003) The effects of an interspinous implant on inter-vertebral disc pressures. Spine 28:26–32
28. Wilke HJ, Drumm J, Häussler K, Mack C, Steudel WI (2008) Kettler A Biomechanical effect of different lumbar inters-pinous implants on flexibility and intradiscal pressure. Eur Spine J 17(8):1049–1056
29. Tsai KJ, Murakami H, Lowery GL, Hutton WC (2006) A biomechanical evaluation of an interspinous device (Coflex)
used to stabilize the lumbar spine. J Surg Orthop Adv 15: 167–172
30. Kettler A, Drumm J, Heuer F, Haeussler K, Mack C, Claes L, Wilke HJ (2008) Can a modified interspinous spacer prevent instability in axial rotation and lateral bending? A biome-chanical in vitro study resulting in a new idea. Clin Biomech (Bristol, Avon) 23:242–247
31. Phillips FM, Voronov LI, Gaitanis IN, Carandang G, Havey RM, Patwardhan AG (2006) Biomechanics of posterior dynamic stabilizing device (DIAM) after facetectomy and discec-tomy. Spine J 6(6):714–722
32. Kim KA, McDonald M, Pik JH, Khoueir P, Wang MY (2007) Dynamic intraspinous spacer technology for posterior stabi-lization: case-control study on the safety, sagittal angulation, and pain outcome at 1-year follow-up evaluation. Neurosurg Focus 22(1):E7
33. Taylor J, Pupin P, Delajoux S, Palmer S (2007) Device for intervertebral assisted motion: technique and initial results. Neurosurg Focus 22(1):E6
34. Floman Y, Millgram MA, Smorgick Y, Rand N, Ashkenazi E (2007) Failure of the Wallis interspinous implant to lower the incidence of recurrent lumbar disc herniations in patients undergoing primary disc excision. Reported. J Spinal Disord Tech 20(5):337–341
35. Verhoof OJ, Bron JL, Wapstra FH, van Royen BJ (2008) High failure rate of the interspinous distraction device (X-Stop) for the treatment of lumbar spinal stenosis caused by degenera-tive spondylolisthesis. Eur Spine J 17(2):188–192
36. Jerosch J, Moursi MG (2008) Foreign body reaction due to polyethylene’s wear after implantation of an interspinal seg-ment. Arch Orthop Trauma Surg 128(1):1–4
37. Ciupik L, Cecek I, Gunzburg R, Kierzkowska A, Szpalski M (2006) Biomechanical evaluation of corrective-stabilizing function of polymeric-polyester interspinous stabilizer. Inzynieria Biomaterialow (Enginnering of Biomaterials) 58–60:32–34
38. Gunzburg R, Szpalski M, Callary SA, Colloca CJ, Kosmopoulos V, Harrison D, Moore RJ (2009) Effect of a novel interspinous implant on lumbar spinal range of motion. Eur Spine J 18:696–703
39. Keller TS, Colloca CJ, Harrison DE, Moore RJ, Gunzburg R (2007) Muscular contributions to dynamic dorsoventral lum-bar spine stiffness. Eur Spine J 16:245–254
40. Christie SD, Song JK, Fessler RG (2005) Dynamic inters-pinous process technology. Spine 30:S73–S78
41. Szpalski M, Pienazek J, Gunzburg R, Ciupik L (2008) One year follow up after insertion of a minimally invasive self-locking interspinous implant. Results at one year and CT measurements of foramen sizes. Spineweek, Geneva, May 26–30, 2008
42. Humke T, Grob D, Grauer W, Sandler A, Dvorak J (1996) Foraminal changes with distraction and compression of the L4/5 and L5/S1 segments. Eur Spine J 5:183–186
43. Kong DS, Kim ES, Eoh W (2007) One-year outcome evaluation after interspinous implantation for degenerative spinal stenosis with segmental instability. J Korean Med Sci 22:330–335
44. Siddiqui M, Smith FW, Wardlaw D (2007) One-year results of X Stop interspinous implant for the treatment of lumbar spinal stenosis. Spine 32:1345–1348
45. Wiseman CM, Lindsey DP, Fredrick AD, Yerby SA (2005) The effect of an interspinous process implant on facet load-ing during extension. Spine 30:903–907

249M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_5.11, © Springer-Verlag Berlin Heidelberg 2010
Introduction
During common ageing, intervertebral discs change in chemical composition and biomechanical properties. The process of disc degeneration can be described in three stages: dysfunction, instabilization and stabiliza-tion. During dysfunction, dehydration of the nucleus of the disc and tearing of annulus layers can be observed, while clinically manifested by episodic low back pain (LBP) [1]. The tearing can subsequently lead to multi-ple annular tears and delamination of the annulus fibro-sis, vertebral instability and further loss of hydration of the nucleus and loss of disc height: the instabilization. This phase is commonly manifested by frequent, more intense episodes of LBP. The final phase, stabilization, is marked by further disc height decrease and formation of osteophytes. Although LBP may be less distinctive, complaints caused by stenosis may be more evident.
Most of the patients suffering from discogenic LBP benefit from non-surgical treatment [2, 3], but if no satisfactory results are obtained, surgical intervention might be considered as the next treatment step.
During the intervention, the complete diseased disc is removed followed by either fusion or total disc arthroplasty (TDA). For long time, fusion was consid-ered as the gold standard of surgical intervention, but concerns about the loss of function of the motion segment and the stress to the adjacent levels [4–6] as well as clinical results have assured the acceptance of disc arthroplasty as the treatment option. The disc arthroplasty system aims at restoration of function and
flexibility, while reducing the chance of developing adjacent level disease [7, 8].
Both fusion and total disc replacement are based on the removal of the total diseased disc, whereas the described degeneration process starts with the interver-tebral nucleus. The degenerating disc nucleus becomes stiffer, resulting in a shift of load-bearing characteristics from the intervertebral disc to posterior spine elements, e.g. facet joints [9]. This change in biomechanical load-ing may stimulate the nerve endings present at the facet joints, ligaments and muscles resulting in LBP and may accelerate further disc degeneration. Disc degenera-tion may also lead to release of cytokines and free radi-cals that irritate nerve endings resulting in LBP [10].
As both the biomechanical and the chemical changes occur in the intervertebral disc, and primarily affect the nucleus [10, 11], development of treatment options involving mainly the disc nucleus are emerging. Patients who are in the dysfunction and instability phase are typical candidates for surgical intervention that only removes the diseased nucleus which is replaced with a device for restoring the function of a healthy nucleus.
NuBac Disc Arthroplasty System (Fig. 5.11.1) is a newly developed device that is intended to treat patients
NuBac Disc Arthroplasty System: Rationale and Clinical Results
Massimo Balsano, Domagoj Coric, and Margreet Derks
M. Balsano (*) Spinal Regional Department, ULSS 4, Schio, Vicenza, Italy e-mail: [email protected]
5.11
Fig. 5.11.1 NuBac™ Disc Arthroplasty System

250 M. Balsano et al.
at an early phase by restoring function, while protect-ing levels and relief of pain. This chapter will discuss the design rationale of the NuBac and the pre-clinical and clinical results obtained with the system.
Design Rationale
Different devices have been developed to replace the nucleus. The designs and materials for nucleus replace-ments vary from different hydrogel or non-hydrogel elastomers, which are either preformed or formed in situ, to non-elastomeric materials such as metal, poly-methylmethacrylate (PMMA) and pyrolytic carbon. Most of these devices had complications like subsid-ence, extrusion and reactive endplate changes. This could be explained by the fact that most of these devices are either too soft with risk for extrusion or use rigid non-articulating constructs that do not allow for uniform load distribution resulting in subsidence, extrusion and end plate changes.
One of the earliest reported experiences with nucleus implants is a stainless steel ball, the Fernström ball. Fernström believed that a ball-formed nucleus device would best restore the articulation of the adjacent verte-brae while preventing anterior or posterior slippage of neighbouring vertebrae. Retrospective, non-randomized, controlled studies showed excellent and good results after short-term [12] and long-term follow-up. After an aver-age follow-up time of 17 years, results for herniated disc patients and discogenic back pain patients were graded excellent and good in 83 and 75%, respectively [13].
The clinical results obtained with the Fernström ball indicate a non-elastic device that allows motion of the indexed level and is able to relieve discogenic back pain over a long period. Based on the shape of the Fernström ball and its small or nearly pointed contact area subsidence was to be expected. Results showed that the device was subsiding in 88% of the patients and that subsidence stopped after 1–3 mm per end plate [12]. It is commonly assumed that subsidence is stopped after reaching a balance between the contact stress of the Fernström ball on the end plates and the strength of the end plates, i.e. subsidence increases the contact area of the device resulting in less contact stress on the end plates.
Newly developed nucleus devices should include the principle of motion-preserving, while preventing
subsidence of the device. The NuBac Disc Arthroplasty is designed to mimic natural kinematics of an intact disc. Free motion is maintained by the two-piece design with an inner ball-and-socket articulation, whereby this motion is constrained by preserving the surrounding annulus and ligaments.
To prevent subsidence, the NuBac is developed with large contact area; for the smallest NuBac implant, the contact area is 2.2 times the contact area of a 12-mm Fernström after 3 mm subsidence (Fig. 5.11.2). For a medium NuBac implant with a contact area of 191 mm2 the average contact stress under 400 N is 2.1 MPa. Reported end plate strengths vary from 2.7 MPa [14] to 20 MPa [15] which are larger than the average con-tact stress for the smallest NuBac device, thus theoreti-cally preventing subsidence of the device.
Choice of Material
The NuBac is manufactured from polyetheretherke-tone (PEEK Optima, Invibio, Greenville, NC, USA), a new bearing material for articulating spine devices where historically metal-on-ultra high molecular weight polyethylene (UHMWPE) is the most used followed by metal-on-metal. PEEK is a thermoplastic with an elastic modulus close to that of bone and is radiolu-cent. Previously, biocompatibility and biodurability testing showed no significant material changes after ageing and no cytotoxic and histopathologic responses or other inflammatory responses [16].
Four groups of 6 PEEK devices were investigated to determine the wear rate for different motion profiles, e.g. unidirectional, multi-directional, multi- directional with frequency shifting and multi-directional with accelerated ageing [17]. All samples were pre-soaked in saline solution at 37 ± 2°C for approximately 28 weeks. For the multi-directional testing, the condi-tions of ISO 18192-1 for TDA were followed with adjustment of the dynamic compressive magnitude to reflect the load sharing mechanism of the device with the annulus. The single-directional testing was contin-ued until 40 million cycles.
A wear-in period up to one million cycles was observed for both the multi-directional tested group and the group tested with frequency shifting, while no in-wear period was observed for the single-directional
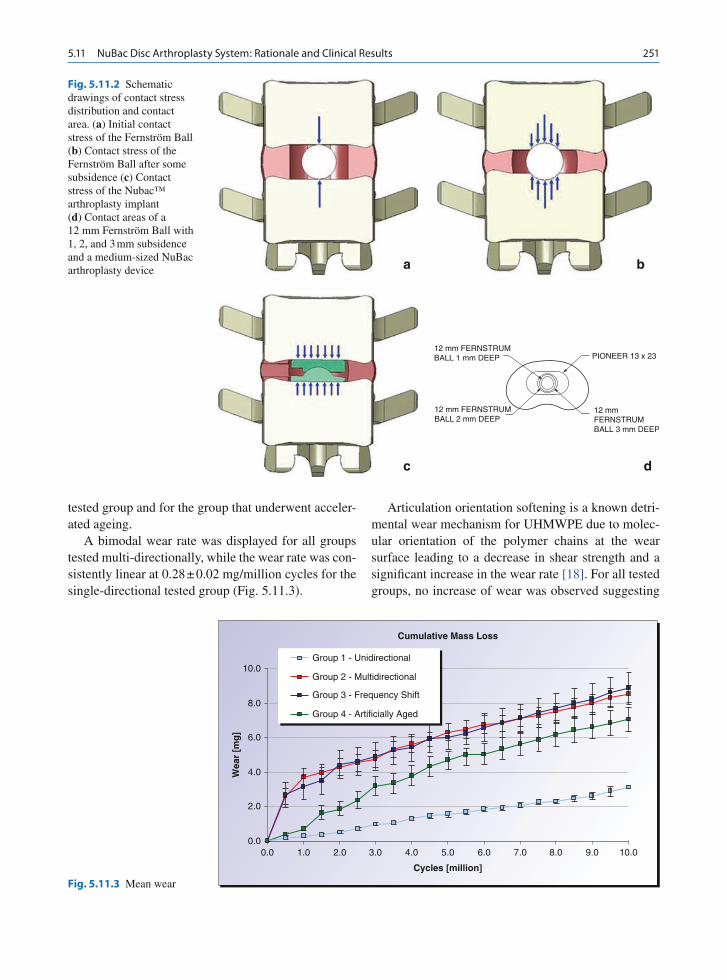
2515.11 NuBac Disc Arthroplasty System: Rationale and Clinical Results
tested group and for the group that underwent acceler-ated ageing.
A bimodal wear rate was displayed for all groups tested multi-directionally, while the wear rate was con-sistently linear at 0.28 ± 0.02 mg/million cycles for the single-directional tested group (Fig. 5.11.3).
Articulation orientation softening is a known detri-mental wear mechanism for UHMWPE due to molec-ular orientation of the polymer chains at the wear surface leading to a decrease in shear strength and a significant increase in the wear rate [18]. For all tested groups, no increase of wear was observed suggesting
Fig. 5.11.2 Schematic drawings of contact stress distribution and contact area. (a) Initial contact stress of the Fernström Ball (b) Contact stress of the Fernström Ball after some subsidence (c) Contact stress of the Nubac™ arthroplasty implant (d) Contact areas of a 12 mm Fernström Ball with 1, 2, and 3 mm subsidence and a medium-sized NuBac arthroplasty device a b
c d
12 mm FERNSTRUMBALL 1 mm DEEP
12 mm FERNSTRUMBALL 2 mm DEEP
12 mmFERNSTRUMBALL 3 mm DEEP
PIONEER 13 x 23
Fig. 5.11.3 Mean wear
0.00.0
2.0
4.0
6.0
8.0
10.0
Wea
r [m
g]
1.0 2.0 3.0 4.0 6.0 7.0 9.08.0 10.05.0
Cycles [million]
Cumulative Mass Loss
Group 1 - Unidirectional
Group 2 - Multidirectional
Group 3 - Frequency Shift
Group 4 - Artificially Aged

252 M. Balsano et al.
that PEEK does not undergo orientation softening at the wear surface.
Also for UHMWPE, exposure to radiation and oxi-dation lead to accelerated wear rates, susceptible to bond cleavage during irradiation [19]. For the accelerated-aged test group for PEEK, no wear-in period was observed suggesting that a thin cross-linked layer was developed during the ageing process. In con-trary to UHMWPE, the wear rate decreased signifi-cantly at 5–10 million cycles and was not significantly different from the other test groups suggesting that an oxidative layer was formed that is removed over time.
For metal-on-UHMWPE articulation, it has been shown that frequency shifting can increase the wear rate by several orders of magnitude. A small but sig-nificant increase in the wear rate was observed as com-pared to the uni- and multi-directional testing due to the frequency shifting.
The small variation in the wear rate suggests that PEEK is a consistent material with relatively low long-term wear properties and not subject to known major wear increasing factors of UHMWPE.
Reducing Risk for Expulsion and Subsidence
Unlike TDA nucleus, implants are not fixed to the verte-bral bodies that challenge migration and expulsion of the implant. Although only one extrusion is reported for the Fernström ball, for the PDN device (Raymedica, Inc., Minneapolis, MN, USA) extrusion rates between 8 and 36% have been reported [20, 21]. This expulsion rate might be explained by the bulky properties of the device and the inability to adapt its shape to the changed angulation during bending. These characteristics can result in an uneven load distribution pattern during bend-ing with increased forces at the side of bending and decreased forces at the opposite side, pushing the implant to the opposite side. This might result in expulsion, especially when the implantation window of the annu-lus is at that specific place or if the annulus is, undesir-able, in degenerative poor condition (Fig. 5.11.4).
The articulating properties of the NuBac device facilitate an even load distribution irrespective of the
Fig. 5.11.4 Schematic drawings of stress distribution under compression and bending. (a) Bulk polymer nucleus implant under compression (b) Bulk polymer nucleus implant under
bending (c) Partial extrusion of bulk polymer nucleus implant under bending (d) Nubac arthroplasty device under compression (e) NuBac arthroplasty device under bending
a b c
d e
Shear Force

2535.11 NuBac Disc Arthroplasty System: Rationale and Clinical Results
spinal position, e.g. flexion-extension, lateral bending and axial rotation. This feature may reduce the risk of implant extrusion during any condition. In addition, an even load distribution of the implant maintains an even load distribution on the end plates, while uneven load distribution may cause oedema and fracture of the end plates resulting in subsidence.
To investigate the articulating characteristics of the device on expulsion risk, six adjacent pairs of human cadaver FSUs (L3–5) were tested. L3–4 served as intact control, and after nucleotomy the device was inserted via a right lateral approach at L4–5. Axial rotation, lateral bending and flexion/extension was tested by 100,000 cycles of unilateral left bending ranging from 2.5 to 7.5 Nm at 2 Hz with the compres-sive load ranging from 205 to 750 N. No expulsion occurred for any of the samples.
There are no clinically validated standards for accessing the expulsion risk. The used scenario was worst case scenario as bending to the opposite side will open the annular window and might facilitate expul-sion. The results demonstrated that the expulsion risk is low. This can be explained by the inner-articulating design that allows the upper and lower plate of the device to move along with the movement of the seg-ment resulting in keeping both plates of the device in full contact with the endplates. In addition, the height of the implant will be less at the bending side and higher at the opposite (window) side which will also make it harder to expulse.
Multi-Directional ROM and Load-to-Failure: An In Vitro Cadaveric Model
Multi-directional range of motion (ROM) and neutral zone were examined by Cunningham (Union Memorial Hospital, Baltimore) [22]. Eight human cadaveric spines (L2–3 and L4–5 segments) were evaluated with unconstrained intact movements of ±7.5 Nm for axial rotation, flexion-extension and lateral bending testing. ROM and neutral zone at the operated level were quan-tified for the intact spine, spine with nucleotomy and spine with NUBAC implant.
After nucleotomy, multi-directional flexibility test-ing indicates significant increase in the segmental ROM and neutral zone (ANOVA, p < 0.05). In
addition, both ROM and neutral zone for the device reconstructed level returned to levels not statistically different from the intact condition (Fig. 5.11.5) indi-cating that the device was able to re-establish the kine-matics to the intact condition. The centre-of-rotation is in the middle of the device, unlike for bulky devices where it is on the side of the device, facilitating both normal kinematics and preventing subsidence.
After reconstruction, load-to-failure was investigated by axial compression. For seven specimens, the observed failure mechanism was fracture of the adjacent verte-bral body without significant damage of the end plates. Observed mean failure load was 3,340 ± 2,029 N which is comparable to the compressive failure load to that of an intact lumbar segment [23, 24].
Clinical Results
A prospective, longitudinal, multi-centre study to investigate safety and efficacy was initiated. Main patient inclusion criterion was symptomatic single- or double-level discogenic back pain. Depending on sur-geon preferences and patient pathologies, anterolateral, lateral or posterior approach was used for implantation. Function was measured with ODI and pain was mea-sured with VAS. These self-administered patient ques-tionnaires were collected pre-operatively and at 6 weeks, 3, 6, 12 and 24 months post-operatively.
The first patient was included in December 2004 and over 250 NUBAC implants were implanted since then. Hundred and forty-four patients returned at least one patient questionnaire and were included in the study. The device has been implanted at L2-S1 with 2.0% at L2–3, 4.7% at L3–4, 52.7% at L4–5 and 40.5% at L5-S1. The mean operative time was 98 ± 49 min. The mean estimated blood loss was 60 ± 90 mL. The average ODI improved from 55 pre-operatively to 30, 24, 22, 21 and 16 respectively at 6 weeks, 3, 6, 12 and 24 months post-operatively (Fig. 5.11.6). The average VAS decreased from 78 pre-operatively to 33, 29, 25, 29 and 27 respectively at 6 weeks, 3, 6, 12, and 24 months post-operatively (Fig. 5.11.7).
No major intra-operative and post-operative vascu-lar and neurological complications have been reported.
The main indication for the NUBAC device is disco-genic back pain secondary to DDD and is similar to the indication for interbody fusion and TDA devices. It has
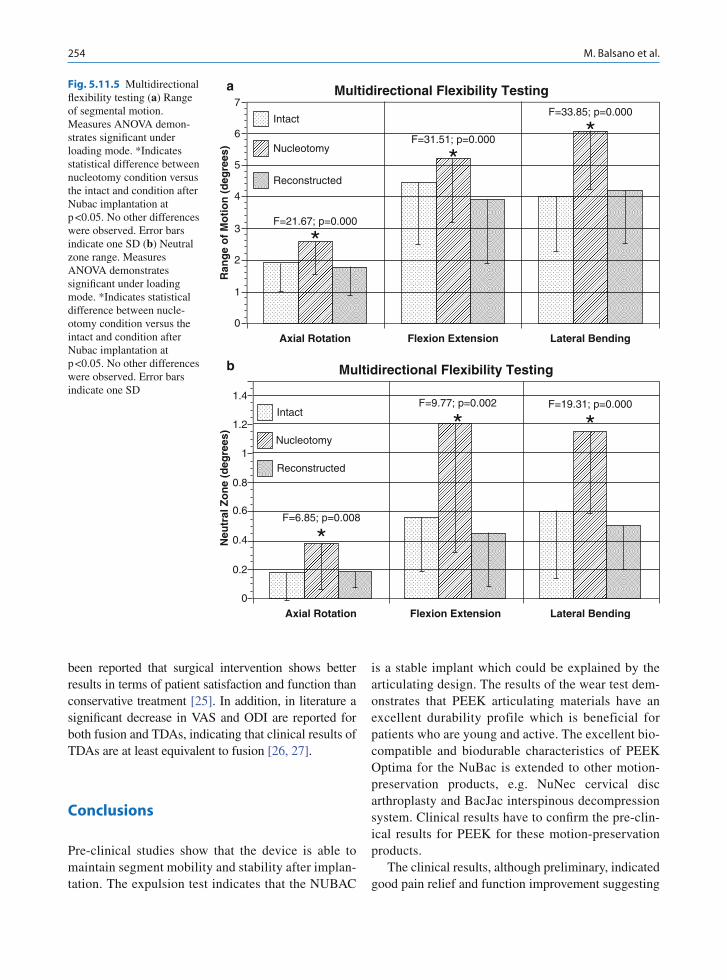
254 M. Balsano et al.
been reported that surgical intervention shows better results in terms of patient satisfaction and function than conservative treatment [25]. In addition, in literature a significant decrease in VAS and ODI are reported for both fusion and TDAs, indicating that clinical results of TDAs are at least equivalent to fusion [26, 27].
Conclusions
Pre-clinical studies show that the device is able to maintain segment mobility and stability after implan-tation. The expulsion test indicates that the NUBAC
is a stable implant which could be explained by the articulating design. The results of the wear test dem-onstrates that PEEK articulating materials have an excellent durability profile which is beneficial for patients who are young and active. The excellent bio-compatible and biodurable characteristics of PEEK Optima for the NuBac is extended to other motion-preservation products, e.g. NuNec cervical disc arthroplasty and BacJac interspinous decompression system. Clinical results have to confirm the pre-clin-ical results for PEEK for these motion-preservation products.
The clinical results, although preliminary, indicated good pain relief and function improvement suggesting
Fig. 5.11.5 Multidirectional flexibility testing (a) Range of segmental motion. Measures ANOVA demon-strates significant under loading mode. *Indicates statistical difference between nucleotomy condition versus the intact and condition after Nubac implantation at p <0.05. No other differences were observed. Error bars indicate one SD (b) Neutral zone range. Measures ANOVA demonstrates significant under loading mode. *Indicates statistical difference between nucle-otomy condition versus the intact and condition after Nubac implantation at p <0.05. No other differences were observed. Error bars indicate one SD
a Multidirectional Flexibility Testing
Intact
7
Ran
ge
of
Mo
tio
n (
deg
rees
)
6
5
4
3
2
1
0
Nucleotomy
Reconstructed
F=21.67; p=0.000
*
Axial Rotation Flexion Extension Lateral Bending
F=31.51; p=0.000
*
F=33.85; p=0.000
*
b
1.4
1.2
1
Neu
tral
Zo
ne
(deg
rees
)
0.8
0.6
0.4
0.2
0
Axial Rotation Flexion Extension Lateral Bending
Multidirectional Flexibility Testing
Intact
Nucleotomy
Reconstructed
F=6.85; p=0.008
*
F=9.77; p=0.002
*F=19.31; p=0.000
*

2555.11 NuBac Disc Arthroplasty System: Rationale and Clinical Results
that the NUBAC device is a feasible alternative for treatment of LBP caused by DDD.
Acknowledgements Umberto Agrillo, MD, Ospedale Sandro Pertini, Rome, ItalyQi-Bin Bao, PhD, Pioneer Surgical Technology, Marquette, Mich, USAAlfredo Bucciero, MD, Clinica Pineta Grande, Castel Volturno (CE), ItalyKenneth Davenport, MD, Orthopaedic Surgery Association of Marquette, Marquette, USALuis Pimenta, MD, PhD, Santa Rita Hospital, Sao Paulo, BrazilAlejandro Reyes-Sanchez, MD, Instituto de Ortopedia, Mexico City, Mexico
Matthew Songer, MD, Orthopaedic Surgery Association of Marquette, Marquette, USADieter Werner, MD, Arkade Privatklinik Niederschmalkalden, Breitungen, GermanyHansen Yuan, MD, SUNY Upstate Medical University, Syracuse, USA
References
1. Kirdaldy-Willis WH et al (1978) Pathology and pathogene-sis of lumbar spondylosis and stenosis. Spine 3(4):319–328
Fig. 5.11.6 ODI Scores
pre
0
10
20
30
40
50
60
70
6 weeks
OD
I Sco
re (
%)
6 months3 months 12 months 24 months
Follow-up time
ODI (function) NuBac
ProDisc-L
Charité
Fig. 5.11.7 VAS Scores
pre
0
10
20
30
40
50
60
70
80
90
6 weeks
VA
S S
core
6 months3 months 12 months 24 months
Follow-up time
VAS (pain) NuBac
ProDisc-L
Charité

256 M. Balsano et al.
2. Resnick DK et al (2005) Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 7: intractable low-back pain without stenosis or spondylolisthesis. J Neurosurg Spine 2(6):670–672
3. Resnick DK et al (2005) Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 13: injection therapies, low-back pain and lumbar fusion. J Neurosurg Spine 2(6):707–715
4. Eck JC et al (1999) Adjacent-segment degeneration after lumbar fusion: a review of clinical, biomechanical, and radiologic studies. Am J Orthop 28(6):336–340
5. Lee CK (1988) Accelerated degeneration of the segment adjacent to a lumbar fusion. Spine 13(3):375–377
6. Schlegel JD et al (1996) Lumbar motion segment patholo-gies adjacent to thoracolumbar, lumbar and lumbosacral fusions. Spine 21(8):970–981
7. Huang RC et al (2006) Range of motion and adjacent level degeneration after lumbar total disc replacement. Spine J 6(3):242–247
8. Moumene M et al (2007) Comparison of biomechanical function at ideal and varied surgical placement for two lum-bar artificial disc implant designs: mobile-core versus fixed-core. Spine 32(17):1840–1851
9. Setton LA et al (2006) Mechanobiology of the intervertebral disc and relevance to disc degeneration. J Bone Joint Surg Am 88(Suppl 2):52–57
10. Buckwalter JA et al (2000) Intervertebral disk structure, composition, and mechanical function. In: Buckwalter JA et al (eds) Orthopaedic basic science biology and biome-chanics for the musculoskeletal system, 2nd edn. Ameri-can academy of orthopaedic surgeons, Rosemont, IL, p 558
11. Niosi CA et al (2004) Degenerative mechanics of the lumbar Spine. Spine J 4(6 Suppl):202S–208S
12. Fernström U (1966) Arthroplasty with intercorporal endo-prothesis in herniated disc and in painful disc. Acta Chir Scand Suppl 357:154–159
13. McKenzie AH (1995) Fernström intervertebral disc arthro-plasty: a long-term evaluation. Ortho Int Ed 3:313–324
14. Tan JS et al (2005) Interbody device shape and size are important to strengthen the vertebra-implant interface. Spine 30(6):638–644
15. Lowe TG et al (2004) A biomechanical study of regional endplate strength and cage morphology as it relates to struc-tural interbody support. Spine 29(21):2389–2394
16. Cartwright K et al (2005) Investigation in the effect of gamma sterilization (200kGy) and accelerated aging on the properties of PEEK-Optima. Invibio Technical Report
17. Brown T et al A comprehensive wear assessment of PEEK-OPTIMA for disc arthroplasty applications. WBC2008, poster 125
18. Wang A (2001) A unified theory of wear for ultra-high molecular weight polyethylene in multi-directional sliding. Wear 248(1–2):38–47
19. Jahan MS et al (1991) Combined chemical and mechanical effects on free radicals in UHMWPE joints during implanta-tion. J Biomed Mater Res 25(8):1005–1017
20. Klara PM et al (2002) Artificial nucleus replacement: clini-cal experience. Spine 27(12):1374–1377
21. Shim CS et al (2003) Partial disc replacement with the PDN prosthetic disc nucleus device: early clinical results. J Spinal Disord Tech 16(4):324–330
22. Bao QB et al (2006) Pioneer surgical technology: NUBAC artificial nucleus. In: Kim DH et al (eds) Dynamic recon-struction of the spine, 1st edn. Thieme Medical, pp 128–136
23. Bell GH et al (1967) Variations in strength of vertebrae with age and their relation to osteoporosis. Calcif Tissue Res 1(1):75–86
24. Perry O (1957) Fracture of the vertebral end-plate in the lumbar spine. Acta Orthop Scand 25(Suppl):34–39
25. Weinstein JN, Tosteson TD, Lurie JD et al (2006) Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT): a random-ized trial. JAMA 296(20):2441–2450
26. Zigler J et al (2007) Results of the prospective, randomized, multicenter food and drug administration investigational device exemption study of the ProDisc-L total disc replacement ver-sus circumferential fusion for the treatment of 1-level degen-erative disease. Spine 32(11):1155–1162; discussion 1163
27. Blumenthal S et al (2005) A prospective, randomized, mul-ticenter Food and Drug Administration investigational device exemptions study of lumbar total disc replacement with the CHARITE artificial disc versus lumbar fusion: part I: evaluation of clinical outcomes. Spine 15;30(14):1565–1575; discussion E387–E391

Part
OutcomesVI

259M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_6.1, © Springer-Verlag Berlin Heidelberg 2010
Economic Evaluation
Until recently, medicine was fairly straightforward. The doctor had limited therapeutic options, patients did as they were told, and mortality was an unequivocal outcome. Now medicine has become health care, an amalgam of psychology, physiology, anthropology, epidemiology, edu-cation, management theory, and politics. Economics has been the latest candidate for the melting pot, on the back of a simple message: when resources are limited, relating the cost of an intervention to its benefits can facilitate the difficult choices that have to be made between competing options [1].
The discipline of relating the cost of an intervention to its benefits is denoted as economic evaluation. The standard textbook definition is that two or more alter-natives are being compared and both costs and benefits are assessed [2]. Although evaluations are increasingly conducted using meta-analysis and mathematical mod-eling, the classical approach of stochastic evaluation is the main focus of this chapter. Stochastic refers to the fact of evaluations being conducted alongside clinical trials at the patient-level, i.e., parameters of costs and benefits are stochastic across patients.
So, if economic evaluation is conducted alongside clinical trials, do clinicians measure outcomes and health economists measure costs? The answer is no. Clinicians do measure clinical outcomes but these are most often different from what is required for economic evaluation. Health economists do measure costs but their magnitude has no intrinsic interest; the real interest is in the ratio of
incremental costs to incremental benefits, which can inform priority-setting under the objective of maximiz-ing population health. Given this objective, it becomes imperative to capture, exhaustively, all the differences between the outcomes of interventions and not just selected dimensions of pain or functional disability, say e.g., pain and functional ability.
Historically, cost-effectiveness evaluation has been the most frequent type of evaluation possibly because of the readily available outcomes data, as clinical effect measures can be directly adapted as benefit measures. Accordingly, the main caveat of cost-effectiveness eval-uations is a restricted use of results both in terms of the chosen dimension of effect and in terms of the instru-ment chosen to quantify it. For example, if an evaluation is based on the Oswestry Disability Index, producing a single-index of reduction in functional disability, the resulting ratio of incremental costs to incremental bene-fits can inform priority-setting between the interventions evaluated using the Oswestry Disability Index only, because construct and scaling are instrument-specific.
In recent years, cost-utility evaluation has become the preferred type of analysis [3]. The outcome param-eter in a cost-utility evaluation is, principally, of exclu-sive interest to the health economic perspective in being a preference-based index of health, also referred to as utility. The notion of preference-based usually refers to the fact that the general population’s preferences are used to weigh the patient-reported health status. Individual gains of utility over time across trial partici-pants are typically summed and reported as quality-adjusted life-years (QALYs), a fact that opens for priority-setting across specialties, in principle, is unre-stricted with respect to the instrument used to measure outcomes.
The QALY has become an established generic mea-sure, which in the perception of most decision-makers,
Outcome Assessment for Cost-Utility Evaluations: SF-6D vs. EQ-5D
Rikke Søgaard, Terkel Christiansen, and Finn Bjarke Christensen
R. Søgaard (*) CAST–Centre for Applied Health Services Research and Technology Assessment, University of Southern Denmark, J.B. Winsløws Vej 9, 5000 Odense C, Denmark e-mail: [email protected]
6.1

260 R. Søgaard et al.
represents a standard unit although there are alternative ways of estimating it. The choice of methodology for estimation typically lies in the hands of the trialist. Ceteris paribus, the trialist is concerned with adapting a measure that is first of all valid, and furthermore, is sensitive enough to capture relevant differences between groups. Low back pain may be a special case and the fact that instruments perform well in other populations provides no guarantee that they will perform well in populations suffering low back pain.
The objective of this chapter is to inform the choice of instrument to assess generic, preference-based out-come in clinical trials conducted in low back pain. The chapter proceeds as follows: the first section presents the general history of preference-based measures and the rationale for limiting the choice of instrument between the SF-6D and the EQ-5D; the second section presents selected evidence of the performance of the instruments in low back pain; the third section presents an empirical head-to-head comparison of the two mea-sures’ performance in low back pain; and the final sec-tion attempts a conclusion about the optimal choice of instrument for researchers conducting clinical trials in low back pain.
The History of Preference-Based Measures
The scope of a perference-based measure is to con-dence the multidimensional construct of health into a single-index score anchored at zero (dead) and one (perfect health). This is traditionally approached as a two-step procedure by means of an instrument for the description of health status and an ancillary scoring algorithm for the assignment of a preference-value. The former component usually takes the form of a questionnaire aimed at study participants in a clinical trial setting, while the latter component is usually a scoring model derived from a survey of the general population’s preferences.
In the 1970s, some early preference-based measures of the Index of Well-Being (later termed the Quality of Well-Being Index) and the Rosser Classification were proposed in the United States and in the United Kingdom, respectively [4, 5]. The Rosser Classification characterized individuals into as few as 29 health states; hence its sensitivity was somewhat restricted. During the 1980s, these early measures were refined and new instruments emerged: the 12D (later termed the 15D)
and the health utility index (HUI), among others [6, 7]. The most recent measures came about in the 1990s with the EQ-5D and the Australian Assessment of Quality of Life being two of the most influential devel-opments [8, 9].
In 1999, Brazier et al. reported a systematic review of the use of health status measures for economic evalu-ation [10]. They identified five preference-based, generic measures: the Rosser Classification, the Quality of Well-Being Index, the HUI, the 15D, and the EQ-5D. Arguing that conventional psychometric tests of valid-ity were inappropriate to assess economic validity of measures, the authors instead assessed the instruments’ ability to describe health as well as their scoring modles’ theoretical and empirical validity. On grounds of lim-ited ability to describe health, the Rosser Classification was found inferior to the others. The Quality of Well-Being Index and the 15D were also found inferior because their scoring models were not anchored on a sound economical theoretical foundation. The remain-der measures, the HUI and the EQ-5D, were found to hold test–retest reliability as well as practicality on top of the assessed issues of validity.
Since the review of Brazier et al., a further measure has evolved. The SF-6D was derived from the, perhaps, most widely used instrument clinically, the SF-36 [11]. This was an interesting proposition for at least two rea-sons: if the extensive amount of validation studies car-ried out for the SF-36 would be directly transferable to the SF-6D, the measure holds a major potential for the discipline of economic evaluation, and furthermore, there is an enormous amount of both historic and con-current SF-36 data, which has now become usable for economic evaluation.
Following the recommendations of Brazier et al. and the addition of the most recent development, the SF-6D, the choice of measure for generic preference-based outcome assessment essentially stands between the HUI, the EQ-5D, and the SF-6D. The current rec-ommendations of the UK National Institute for Health and Clinical Excellence (NICE) are, however, limited to a choice between the EQ-5D and the SF-6D [3]. This may be due to the fact that the HUI offers no UK-based preference weights of the (adult) normal population. For these reasons, the focus of the present chapter is restricted to a comparison of the SF-6D and the EQ-5D.
The SF-6D came about in its first version in 1998 as a result of Brazier and colleagues’ conceptual restruc-turing of the SF-36 into some ranked levels of selected dimensions: physical functioning, role limitations, social

2616.1 Outcome Assessment for Cost-Utility Evaluations: SF-6D vs. EQ-5D
functioning, pain, mental health, and vitality [12]. In 2002, a revised version, which was valued using the so-called standard gamble technique in a representa-tive sample of the UK general population was reported [13]. The revised version included the same dimen-sions as the first (although the item-mix was different) and presented with four to six levels of function in each dimension, producing a total of 18,000 health states. The resulting scoring model of the 2002 sur-vey contained some logical inconsistencies, and there-fore, a consistent model became available on request from the research group led by Brazier (University of Sheffield, UK).
The EQ-5D was developed in a large multidisci-plinary group, the EuroQol group, which proposed the first version of the instrument in 1990 [14]. The first version contained six dimensions, selected upon review of other generic health status measures, which were labeled mobility, self-care, main activity, social rela-tionships, pain, and mood [15]. These were shortly modified into the current version including only five dimensions: mobility, self-care, usual activity, pain/discomfort, and anxiety/depression, each with three levels of function and thus producing a total of 243 health states (245, when added for completeness, unconscious and immediate death). Several scoring models have been published, many of them based on the protocol of the most influential survey; the study conducted by the Measurement and Valuation of Health Group at York, applying the so-called time-trade-off technique in a representative sample of the UK general population [16, 17]. The scoring models currently available for the EQ-5D have recently been published in an easily accessible and nontechnical user guide by the EuroQol group [18].
Table 6.1.1 presents the dimensions and the number of levels for the two measures. It is clear that they are not measuring the same construct. First, the SF-6D includes one dimension, vitality, which is not covered in the EQ-5D. Second, the weighting of dimensions varies between instruments, for example, physical functioning is addressed by two of five dimensions in the EQ-5D, whereas only one of six dimensions in the SF-6D relates to that. The inverse is the case for psy-chosocial functioning, which is addressed by three of six dimensions in the SF-6D and only one of five in the EQ-5D. The pain dimension is covered in a similar manner for the two instruments, although the SF-6D focuses on disability associated with pain, whereas the EQ-5D focuses on pain and discomfort per se.
Another noteworthy issue is that measures address different levels of severity. For example, the worst function level in dimensions relating to physical func-tioning is described by limits you in the SF-6D, whereas the wording in the EQ-5D is unable or confined to bed. This may enable a floor effect of the former relative to the latter. In contrast, a general ceiling effect of the EQ-5D can be suspected as the limited number of lev-els in each dimension may not facilitate discrimination between, for example, states of perfect and good health.
SF-6D and EQ-5D in Low Back Pain
Conventional studies of psychometric validity have been conducted specifically in low back pain for both the SF-6D and the EQ-5D. The first version of the SF-6D was compared to a disease-specific measure, the modified Roland scale, in a population of 379 patients with low back pain [19]. Comparing single-index val-ues with the levels of disease severities, the SF-6D was found to hold construct validity. A similar study for the EQ-5D was conducted in 326 patients suffering chronic low back pain [20]. Here, the EQ-5D was compared to the Oswestry Disability Index and found to hold con-struct validity and matching properties of responsive-ness. These findings are in agreement with results from the previous acute low back pain [21].
Another approach to examining discriminative abil-ities is to look at the number of health states contained in an instrument. The numbers of 18,000 for the SF-6D and 243 for the EQ-5D are theoretical health states, which are not the same as plausible health states likely to ever come into use. This was illustrated in a study by McDonough et al. [22], where the two instruments were applied preoperatively in a sample of 2,097 patients with disk herniation (51%), spinal stenosis (26%), or degenerative spondylolisthesis (23%). The total num-ber of unique health states assigned using the SF-6D was 1,012 and the corresponding number for the EQ-5D was 72. It is implied that the number of unique health states may refer to the degree of homogeneity of the sample as well as discriminative abilities of the instrument.
Another important factor is the magnitude of a mini-mally important difference (MID) as it has limited interest to pick up differences that are not relevant to decision-making. In a recent study, Walters et al.

262 R. Søgaard et al.
Table 6.1.1 Dimensions and number of levels in the SF-6D and the EQ-5D
SF-6D EQ-5D
Physical functioning Mobility
Your health does not limit you in vigorous activities (1) No problems walking about (1)Your health limits you a little in vigorous activities (2) Some problems walking about (2)Your health limits you a little in moderate activities (3) Confined to bed (3)Your health limits you a lot in moderate activities (4) Self-careYour health limits you a little in bathing and dressing (5) No problems with self-care (1)Your health limits you a lot in bathing and dressing (6) Some problems washing or dressing myself (2)
Unable to wash or dress self (3)
Role limitations Usual activities
You have no problems with your work or other regular daily activities as a result of your physical health or any emotional problems
(1) No problems with performing usual activities (e.g., work, study, housework, family, or leisure activities)
(1)
You are limited in the kind of work or other activities as a result of your physical health
(2) Some problems with performing usual activities
(2)
You accomplish less than you would like as a result of emotional problems
(3) Unable to perform usual activities (3)
You are limited in the kind of work or other activities as a result of your physical health and accomplish less than you would like as a result of emotional problems
(4)
Social functioning
Your health limits your social activities none of the time (1)Your health limits your social activities a little of the time (2)Your health limits your social activities some of the time (3)Your health limits your social activities most of the time (4)Your health limits your social activities all of the time (5)
Pain Pain/discomfort
You have no pain (1) No pain or discomfort (1)You have pain, but it does not interfere with your normal
work (both outside the home and housework)(2) Moderate pain or discomfort (2)
You have pain that interferes with your normal work (both outside the home and housework) a little bit
(3) Extreme pain or discomfort (3)
You have pain that interferes with your normal work (both outside the home and housework) moderately
(4)
You have pain that interferes with your normal work (both outside the home and housework) quite a bit
(5)
You have pain that interferes with your normal work (both outside the home and housework) extremely
(6)
Mental health Emotions
You feel tense or downhearted and low none of the time (1) Not anxious or depressed (1)You feel tense or downhearted and low a little of the time (2) Moderately anxious or depressed (2)You feel tense or downhearted and low some of the time (3) Extremely anxious or depressed (3)You feel tense or downhearted and low most of the time (4)You feel tense or downhearted and low all of the time (5)
Vitality
You have a lot of energy all of the time (1)You have a lot of energy most of the time (2)You have a lot of energy some of the time (3)You have a lot of energy a little of the time (4)You have a lot of energy none of the time (5)
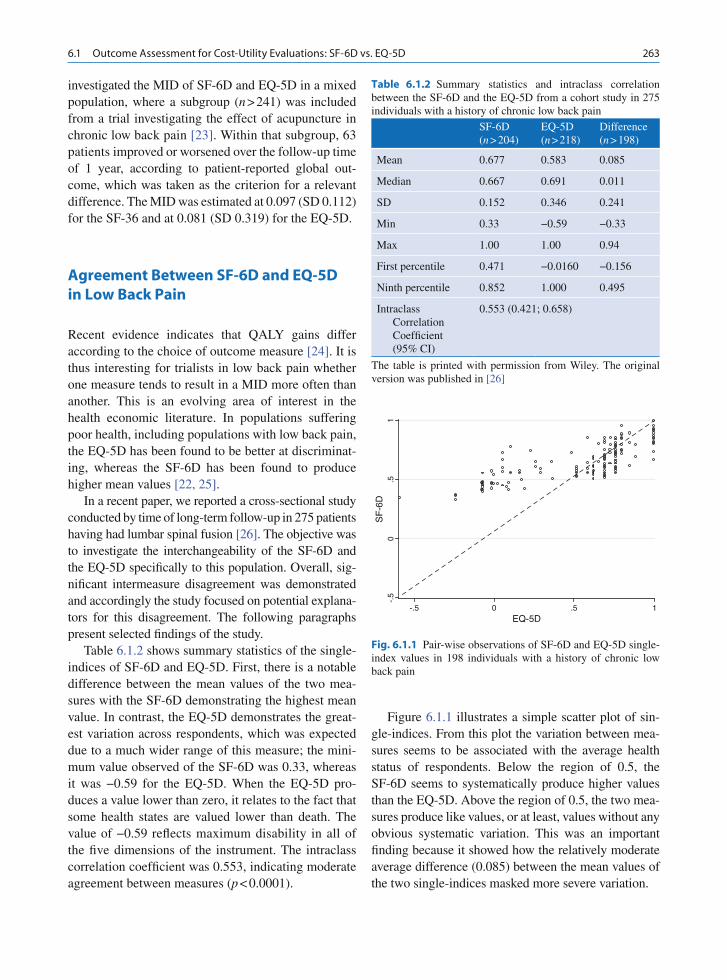
2636.1 Outcome Assessment for Cost-Utility Evaluations: SF-6D vs. EQ-5D
investigated the MID of SF-6D and EQ-5D in a mixed population, where a subgroup (n > 241) was included from a trial investigating the effect of acupuncture in chronic low back pain [23]. Within that subgroup, 63 patients improved or worsened over the follow-up time of 1 year, according to patient-reported global out-come, which was taken as the criterion for a relevant difference. The MID was estimated at 0.097 (SD 0.112) for the SF-36 and at 0.081 (SD 0.319) for the EQ-5D.
Agreement Between SF-6D and EQ-5D in Low Back Pain
Recent evidence indicates that QALY gains differ according to the choice of outcome measure [24]. It is thus interesting for trialists in low back pain whether one measure tends to result in a MID more often than another. This is an evolving area of interest in the health economic literature. In populations suffering poor health, including populations with low back pain, the EQ-5D has been found to be better at discriminat-ing, whereas the SF-6D has been found to produce higher mean values [22, 25].
In a recent paper, we reported a cross-sectional study conducted by time of long-term follow-up in 275 patients having had lumbar spinal fusion [26]. The objective was to investigate the interchangeability of the SF-6D and the EQ-5D specifically to this population. Overall, sig-nificant intermeasure disagreement was demonstrated and accordingly the study focused on potential explana-tors for this disagreement. The following paragraphs present selected findings of the study.
Table 6.1.2 shows summary statistics of the single-indices of SF-6D and EQ-5D. First, there is a notable difference between the mean values of the two mea-sures with the SF-6D demonstrating the highest mean value. In contrast, the EQ-5D demonstrates the great-est variation across respondents, which was expected due to a much wider range of this measure; the mini-mum value observed of the SF-6D was 0.33, whereas it was −0.59 for the EQ-5D. When the EQ-5D pro-duces a value lower than zero, it relates to the fact that some health states are valued lower than death. The value of −0.59 reflects maximum disability in all of the five dimensions of the instrument. The intraclass correlation coefficient was 0.553, indicating moderate agreement between measures (p < 0.0001).
Figure 6.1.1 illustrates a simple scatter plot of sin-gle-indices. From this plot the variation between mea-sures seems to be associated with the average health status of respondents. Below the region of 0.5, the SF-6D seems to systematically produce higher values than the EQ-5D. Above the region of 0.5, the two mea-sures produce like values, or at least, values without any obvious systematic variation. This was an important finding because it showed how the relatively moderate average difference (0.085) between the mean values of the two single- indices masked more severe variation.
-.5
0.5
1S
F-6
D
-.5 0 .5 1EQ-5D
Fig. 6.1.1 Pair-wise observations of SF-6D and EQ-5D single-index values in 198 individuals with a history of chronic low back pain
Table 6.1.2 Summary statistics and intraclass correlation between the SF-6D and the EQ-5D from a cohort study in 275 individuals with a history of chronic low back pain
SF-6D (n > 204)
EQ-5D (n > 218)
Difference (n > 198)
Mean 0.677 0.583 0.085
Median 0.667 0.691 0.011
SD 0.152 0.346 0.241
Min 0.33 −0.59 −0.33
Max 1.00 1.00 0.94
First percentile 0.471 −0.0160 −0.156
Ninth percentile 0.852 1.000 0.495
Intraclass Correlation Coefficient (95% CI)
0.553 (0.421; 0.658)
The table is printed with permission from Wiley. The original version was published in [26]

264 R. Søgaard et al.
Figure 6.1.2 illustrates the agreement between single -indices using a Bland and Altman plot with regression-adjusted limits of agreement. The limits of agreement (mean difference ± 1.96 SD) represent the expected variation between the measures for any true value of the average. The pragmatic way to interpret the limits of agreement in the present context is that if the range between the limits is not important to deci-sion-makers, then the two measures can be used inter-changeably. The adjusted limits of agreement ranged from −0.188 to 0.358 for a mean difference of 0.085, which is equal to an expected variation between the SF-6D and the EQ-5D measures of 0.546 for any true pair of future observations.
The above-mentioned study has one important limi-tation in not being a longitudinal study. We can there-fore only pose hypotheses about the relationship between SF-6D and EQ-5D over time: if the identified differ-ences carry over into the estimation of QALY gain, divergent conclusions on whether an intervention is worthwhile is a realistic consequence. This is because change scores are negatively correlated with baseline scores, meaning that any procedure that lowers the scores of poor health states will potentially increase the change scores [27].
There is a few examples of longitudinal studies in the literature although not specifically related to low back pain. Conner-Spady and Suarez-Almazor exam-ined the relationship in a cohort of 161 patients
visiting a rheumatologic clinic that was followed for 12 months [28]. They reported an effect size (health gain in units of standard deviations) of 0.42 for the SF-6D and 0.52 for the EQ-5D, which is equivalent to mean improvements of 0.05 and 0.15, respectively. The same study was reported, in another article by Conner-Spady and Suarez-Almazor, with particular emphasis on the impact on the incremental QALY gain [24]. Using retrospective ratings by patients on whether they were in better, the same, or poorer health, QALY differ-ences between better and poorer health were 0.09 for the SF-6D and 0.23 for the EQ-5D. An intuitive inter-pretation of these results would be that for the compari-son of an effective and an ineffective intervention, choosing the EQ-5D over the SF-6D would, ceteris paribus, upscale the resulting QALY gain by a factor 3 (0.23/0.09»3).
Level of Health-Related Quality of Life: Low Back Pain vs. Cancer
Patients suffering chronic low back pain generally score health-related quality of life in the same region as patients with life-threatening cancer although, to the best of our knowledge, there is no single survey exam-ining the level of the quality of life in low back pain. Values can, however, be drawn from the limited num-ber of intervention studies that have applied either the SF-6D or the EQ-5D.
In subacute low back pain, Brazier et al. reported single-indices from a trial in general practice investi-gating the cost-effectiveness of alternative conserva-tive treatments [25]. The SF-6D score was 0.66 (SD 0.14) and the EQ-5D score was 0.64 (SD 0.27).
In chronic low back pain, McDonough et al. reported single-indices from the SPORT trial [22]. In their population of mixed diagnoses (disk herniation, spinal stenosis, and degenerative spondylolisthesis), the SF-6D score was 0.57 (SD 0.12) and the EQ-5D score was 0.39 (SD 0.33). Riviero-Arias et al. reported EQ-5D score of 0.35 (95% confidence inter-val 0.30; 0.40) in their surgical arm and 0.41 (95% confidence interval 0.36; 0.46) in their conservative arm of a randomized controlled trial in 349 patients eligible for surgery [29]. The validation study of the EQ-5D by Solberg et al. was conducted in 326 patients having low back surgery due to degenerative
-.5
0.5
1
Diff
eren
ce (
SF
-6D
- E
Q-5
D)
0 1Average
Fig. 6.1.2 Agreement between SF-6D and EQ-5D single- indices in 198 individuals with a history of chronic low back pain: regression-adjusted limits of agreement (mean differ-ence ± 1.96 SD) showing an expected variation of 0.546 between measures. The figure is printed with permission from Wiley. The original version was published in [26]

2656.1 Outcome Assessment for Cost-Utility Evaluations: SF-6D vs. EQ-5D
disorders [20]. They reported a baseline score as low as 0.23 (95% confidence interval 0.19; 0.27). The general endpoint scores of low back pain studies lie in the region of 0.65.
It is clear from the above, that chronic low back pain patients score extremely low levels of quality of life prior to surgery, especially when based on the EQ-5D instrument. In a recent review of EQ-5D-based quality of life scores in different cancer diagnoses (prostate cancer, breast cancer, cancers of the digestive system, Hodgkin’s/non-Hodgkin’s lymphoma, and nonspecific cancer), only one of 34 studies reported values as low as those observed in chronic low back pain [30]. The lowest score identified by the review was estimated at baseline in 25 patients suffering from nonspecific cancer.
Concluding Remarks
To satisfy the requirements of decision-makers operat-ing under an overall objective of maximizing popula-tion health and a premise of scarce resources, cost-utility evaluations, providing a cost per QALY for different choices, have become popular. If cost-utility evaluations are to be run alongside clinical trials, the tri-alist has to append an instrument for the measurement of generic, preference-based outcomes. The objective of this chapter was to inform the choice of instrument to assess generic, preference-based outcomes in clinical trials conducted in low back pain.
There is a range of alternative measures, but this work looked into the performance of only two with ref-erence to the recommendations of a comprehensive review and the guidelines of NICE in the UK. The SF-6D and the EQ-5D have both been found to be prac-tical, and overall, psychometrically valid in low back pain. Yet, the literature represents several studies dem-onstrating that the two measures cannot be used interchangeably.
The entity of low back pain is a heterogenous dis-ease category and different recommendations may be appropriate for different subgroups. The differential in mean values between SF-6D and EQ-5D is most signifi-cant in populations suffering relatively poor health – for example, chronic low back pain – whereas, the two measures seem almost interchangeable in near-perfect health. However, as the average patient improves over
time, trialists have to consider both baseline and expected endpoint scores. For example, assuming that patients demonstrate values below the region of 0.5 at baseline and reach values above 0.5 at follow-up, the choice of measure will have significant impact on the QALY gain with the EQ-5D most likely producing the highest gain.
In conclusion, the SF-6D and the EQ-5D are, indi-vidually, psychometrically valid instruments for out-comes assessment in low back pain, but they cannot be used interchangeably to estimate QALY gains. Nevertheless, there is no gold standard on how to mea-sure generic health, and for that reason, the recommen-dation for researchers in low back pain is to choose the preferred measure and discuss the impact of alterna-tive choices with respect to relative QALY gains.
References
1. Kernick DP (1998) Has health economics lost its way? BMJ 317(7152):197–199
2. Drummond M, Sculpher M, Torrance G, O’Brien B, Stoddard G (2005) Methods for the economic evaluation of health care programmes, 3rd edn. Oxford University, Oxford
3. National Institute for Clinical Excellence (2004) Guide to the methods of technology appraisal. NICE, London
4. Fanshel S, Bush J (1970) A health status index and its appli-cation to health service outcomes. Oper Res 18:1021–1066
5. Rosser RM, Watts VC (1972) The measurement of hospital output. Int J Epidemiol 1(4):361–368
6. Torrance GW, Boyle MH, Horwood SP (1982) Application of multi-attribute utility theory to measure social preferences for health states. Oper Res 30(6):1043–1069
7. Sintonen H (1981) An approach to measuring and valuing health states. Soc Sci Med [Med Econ] 15(2):55–65
8. Hawthorne G, Richardson J, Osborne R, McNiel H (1997) The Australian Quality of Life (AQoL) instrument. Monash University Working Paper
9. The EuroQol Group (1990) EuroQol – a new facility for the measurement of health-related quality of life. Health Policy 16:199–208
10. Brazier J, Deverill M, Green C (1999) A review of the use of health status measures in economic evaluation. J Health Serv Res Policy 4(3):174–184
11. Ware JE (1993) SF-36 health survey: manual and interpreta-tion guide. Nimrod, Boston
12. Brazier J, Usherwood T, Harper R, Thomas K (1998) Deriving a preference-based single index from the UK SF-36 Health Survey. J Clin Epidemiol 51(11):1115–1128
13. Brazier J, Roberts J, Deverill M (2002) The estimation of a preference-based measure of health from the SF-36. J Health Econ 21(2):271–292

266 R. Søgaard et al.
14. EuroQol group (1990) EuroQol – a new facility for the mea-surement of health-related quality of life. Health Policy 16(3):199–208
15. Kind P (1996) The EuroQol instrument: an index of health-related quality of life. In: Spiker B (ed) Quality of life and pharmacoeconomics in clinical trials, 2nd edn. Lippincott-Raven, Philidelphia, pp 191–201
16. Dolan P, Gudex C, Kind P, Williams A (1996) The time trade-off method: results from a general population study. Health Econ 5(2):141–154
17. The MVH group (1995) The measurement and valuation of health: final report on the modelling of valuation tariffs. University of York, York
18. EQ-5D Value Sets: Inventory, Comparative Review and User Guide. Springer; 2007
19. Hollingworth W, Deyo RA, Sullivan SD, Emerson SS, Gray DT, Jarvik JG (2002) The practicality and validity of directly elicited and SF-36 derived health state preferences in patients with low back pain. Health Econ 11(1):71–85
20. Solberg TK, Olsen JA, Ingebrigtsen T, Hofoss D, Nygaard OP (2005) Health-related quality of life assessment by the EuroQol-5D can provide cost-utility data in the field of low-back surgery. Eur Spine J 14(10):1000–1007
21. Suarez-Almazor ME, Kendall C, Johnson JA, Skeith K, Vincent D (2000) Use of health status measures in patients with low back pain in clinical settings. Comparison of spe-cific, generic and preference-based instruments. Rheumatology (Oxford) 39(7):783–790
22. McDonough CM, Grove MR, Tosteson TD, Lurie JD, Hilibrand AS, Tosteson AN (2005) Comparison of EQ-5D, HUI, and SF-36-derived societal health state values among
spine patient outcomes research trial (SPORT) participants. Qual Life Res 14(5):1321–1332
23. Walters SJ, Brazier JE (2005) Comparison of the mini-mally important difference for two health state utility measures: EQ-5D and SF-6D. Qual Life Res 14(6): 1523–1532
24. Conner-Spady B, Suarez-Almazor ME (2003) Variation in the estimation of quality-adjusted life-years by different preference-based instruments. Med Care 41(7):791–801
25. Brazier J, Roberts J, Tsuchiya A, Busschbach J (2004) A comparison of the EQ-5D and SF-6D across seven patient groups. Health Econ 13(9):873–884
26. Søgaard R, Christensen F, Bünger C, Videbæk T, Christiansen T (2009) Interchangeability of the EQ-5D and the SF-6D in long-lasting low back pain. Value Health 12(4):606–612
27. Cronbach L, Furby L (1970) How we should measure “change” – or should we? Psychol Bull 74(1):68–80
28. Conner-Spady B, Suarez-Almazor ME (2001) A comparison of preference-based health status tools in patients with muscoloskeletal disease. In: Norinder A, Pedersen KM, Roos P (eds) Proceedings of the 18th Plenary Meeting of the EuroQol Group. IHE, Lund, pp 235–243
29. Rivero-Arias O, Campbell H, Gray A, Fairbank J, Frost H, Wilson-MacDonald J (2005) Surgical stabilisation of the spine compared with a programme of intensive rehabilita-tion for the management of patients with chronic low back pain: cost utility analysis based on a randomised controlled trial. BMJ 330(7502):1239–1245
30. Pickard AS, Wilke CT, Lin HW, Lloyd A (2007) Health utili-ties using the EQ-5D in studies of cancer. Pharmacoeconomics 25(5):365–384

267M. Szpalski et al. (eds.), Surgery for Low Back Pain, DOI: 10.1007/978-3-642-04547-9_6.2, © Springer-Verlag Berlin Heidelberg 2010
Introduction
Low back pain (LBP), defined as pain, stiffness, or ten-sion between the costal margin and the inferior gluteal folds, affects approximately 60% of adults at some point in their lives [41]. The annual incidence is 15% and the point prevalence is estimated to be 30% [5]. Quantifying the impact of this disorder, it was esti-mated that in 1986 alone, LBP treatment cost United States healthcare systems $11.1 billion [43].
Although LBP syndromes may have a definitive rec-ognized pathological mechanism, 90% of all LBP patients have pain of a nonspecific variety. Patients in this majority segment may be particularly difficult to treat. Furthermore, modern studies have reported that the distinction between acute and chronic back pain may not be as clear as originally thought [12]. A recur-rent and fluctuating course appears to occur more often than single episodes or constant unalleviated pain [26].
Further revealing the difficulties with accurate diag-nosis, several studies have shown a poor correlation between LBP and positive diagnosis from a wide vari-ety of imaging studies [14, 15, 29, 47]. For this reason, in part, many studies have been performed to identify reliable diagnostic techniques in concert with investiga-tions to establish the most effective treatments for LBP.
The majority of patients with degenerative disk dis-ease are treated nonoperatively. If conservative treat-ment fails, surgical intervention may be considered for the appropriate patient. Arthrodesis is an accepted
surgical option, and is commonly performed for back pain attributable to disk degeneration. While success-ful fusion eliminates motion at a potentially painful level and offers the ability to restore intervertebral height and alignment, it does have significant limita-tions. Intervertebral disk arthroplasty is evolving as a surgical alternative [9].
Arthroplasty has developed as an alternative to spinal fusion secondary to the real and perceived shortcomings of spinal fusion. The problems of adja-cent segment disease, pseudarthrosis, and the signifi-cant morbidity of harvesting autologous bone graft have limited the success of lumbar fusion surgery. And, importantly, there is a poor correlation between successful fusion and good clinical outcome; despite achieving a high rate of spinal fusion by modern techniques (>90–95%), clinical outcomes of the same magnitude have not been achieved [46]. Inappropriate indications, imprecise diagnoses, and psychosocial factors each have been blamed for the high degree of variability in LBP reduction following spinal arthrodesis.
This review will assess the published medical evi-dence that relates to surgery directed toward the treat-ment of LBP. Categorically, these include studies investigating lumbar fusion and nonfusion technolo-gies. For each treatment, the quality of the medical evi-dence will be reviewed, such that rational conclusions and recommendations may be made.
Pathophysiology of Low Back Pain
Our comprehension of the etiology and mechanisms associated with LBP is in evolution. It is anticipated that an improved and more detailed understanding may
Review of the Medical Evidence Regarding the Surgical Treatment of Low Back Pain
Andrew P. White, Justin G. Brothers, and Alexander R. Vaccaro
A. P. White (*) Carl J. Shapiro Department of Orthopaedics - Stoneman 10, Harvard Medical School, Beth Israel Deaconess Medical Center, 330 Brookline Ave, Boston, MA 02215, USA e-mail: [email protected]
6.2

268 A. P. White et al.
help guide treatment. Categorizing patients as to the cause of their pain is currently challenging. Findings on diagnostic imaging consistent with lumbar disk degeneration can be found in 34% of asymptomatic people between 20 and 39 years of age, 59% of asymp-tomatic people between 40 and 59 years of age, and 93% of asymptomatic people between 60 and 80 years of age [7]. It is critical to recognise that disk degenera-tion is not ubiquitously associated with LBP. Similarly, LBP is not always associated with subjective findings of degeneration.
With normal physiologic aging, the nucleus pulpo-sus desiccates, causing the typical “dark disk” phe-nomenon commonly seen on T2-weighted MR sequences. This loss of water and nucleus pulposus volume is associated with buckling of the annulus fibrosus. The balance in the breakdown and anabolic repair of trivalent pyridinoline cross-links, responsi-ble for tissue cohesiveness, is subsequently upset. This leads to apoptosis and degeneration of arterioles supplying both the disk and the vertebral endplates. Resultant loss of nutrient and oxygen supply causes excessive lactic acid production, more apoptosis, and further degeneration. Posttranslational protein modifi-cation and cell senescence also affect the mechanical characteristics and the recovery capabilities of the involved disk. Analogous degeneration occurs at the end plates, with thinning and fissure formation. This increases permeability and allows disproportionate load bearing that may be related to disk degeneration findings [5].
While physiologic aging and disk degeneration are commonly thought to be associated with LBP, nerve sensitization and proliferation are more directly and more commonly related to the syndrome. A recent nerve sensitization investigation compared 19 disks excised from patients with discogenic LBP to 12 non-painful but degenerated disks. Ten nondegenerated disks were also studied as a control. Histological immu-nostaining showed that the painful disks contained increased numbers of nerve fibers sensitive to neurofila-ment 200 (NF), substance P (SP), and vasoactive-intes-tinal peptide (VIP) [34]. These inflammatory mediators are established chemical messengers for pain. Nerve sensitization is likely to be one factor to explain why similarly degenerated disks may be associated with dra-matically dissimilar clinical presentations of LBP.
Excessive nerve growth with subsequent nerve sensitization may be caused by disk degeneration and
may be a origin of LBP for many patients [34]. Nerve ingrowth occurs primarily within vascularized granu-lation tissue, extending from the nucleus pulposus to the outer annulus, along tears likely resulting from disk degeneration. During compression and move-ment, fluid may leak from these fissures causing irri-tation. Release of inflammatory cytokines such as prostaglandin E
2 (PGE
2) and Interleukins 6 and 8 (IL-
6, IL-8) may be responsible for nerve sensitization in the painful disk. Nitric oxide (NO) and phospholi-pase A
2 (PLA
2) have also been detected in the granu-
lation tissue [34]. Using similar pathways, these mediators have been linked to hyperalgesia in animal studies [1, 31].
Matrix metalloproteinases (MMPs) have also been implicated in LBP. They are a family of zinc-utilizing enzymes that are suspected to be active in disk hernia-tion and posterior longitudinal ligament rupture. Inflammatory mediators upregulate MMP action and are therefore found densely within the granulation tis-sue. It is speculated that the wide array of MMP actions such as neovascularization and macrophage infiltration may be responsible for spontaneous disk resorption after herniation [5].
These data concerning the degenerative mecha-nisms that may be related to LBP have prompted the development of treatments aimed at the chemical source. Antibodies and receptor antagonists to the pain-causing agents such as TNF-a, MMPs, and IL-1 are in early clinical trials and show promising results [27, 31].
Is Chronic Low Back Pain Treatable with Surgery?
Many surgeons and investigators continue to debate whether or not discogenic chronic LBP should be treated with surgery. A handful of recently reported prospective randomized trials have addressed this question from varied perspectives. Some have consid-ered fusion, while others have considered total disk arthroplasty as surgical treatment for LBP. Many other studies, while they may not represent level one evi-dence, (Table 6.2.1) do offer important contributions to the issue of whether and how discogenic LBP might be surgically treated [3, 9, 10, 13, 19, 21, 23, 33].

2696.2 Review of the Medical Evidence Regarding the Surgical Treatment of Low Back Pain
Table 6.2.1 Levels of evidence
Types of studies
Therapeutic studies – investigating the results of treatment
Prognostic studies – investigating the effect of a patient characteristic on the outcome of disease
Diagnostic studies – investigating a diagnostic test
Economic and decision analyses – developing an economic or decision model
Level I High-quality randomized controlled trial with statistically significant difference or no statistically significant difference, but narrow confidence intervals
Systematic reviewa of level-I randomized controlled trials (and study results were homogeneousb)
High-quality prospective studyc (all patients were enrolled at the same point in their disease with ³80% follow-up of enrolled patients)
Systematic reviewa of level-I studies
Testing of previously developed diagnostic criteria in series of consecutive patients (with universally applied reference “gold” standard)
Systematic reviewa of level-I studies
Sensible costs and alternatives; values obtained from many studies; multiway sensitivity analyses
Systematic reviewa of level-I studies
Level II Lesser-quality randomized controlled trial (e.g., <80% follow-up, no blinding, or improper randomization)
Prospectivec comparative studyd
Systematic reviewa of level-II studies or level-I studies with inconsistent results
Retrospectivee studyUntreated controls from a
randomized controlled trial
Lesser-quality prospective study (e.g., patients enrolled at different points in their disease or <80% follow-up)
Systematic reviewa of level-II studies
Development of diagnostic criteria on the basis of consecu-tive patients (with universally applied reference “gold” standard)
Systematic reviewa of level-II studies
Sensible costs and alternatives; values obtained from limited studies; multiway sensitivity analyses
Systematic reviewa of level-II studies
Level III Case-control studyf
Retrospectivee comparative studyd
Systematic reviewa of level-III studies
Case-control study Study of nonconsecutive patients (without consistently applied reference “gold” standard)
Systematic reviewa of level-III studies
Analyses based on limited alternatives and costs; poor estimates
Systematic reviewa of level-III studies
Level IV Case seriesg Case series Case-control studyPoor reference standard
No sensitivity analyses
Level V Expert opinion Expert opinion Expert opinion Expert opinionaA combination of results from two or more prior studiesbStudies provided consistent resultscStudy was started before the first patient enrolleddPatients treated one way (e.g., with cemented hip arthroplasty) compared with patients treated another way (e.g., with cementless hip arthroplasty) at the same institutioneStudy was started after the first patient enrolledfPatients identified for the study on the basis of their outcome (e.g., failed total hip arthroplasty), called “cases,” are compared with those who did not have the outcome (e.g., had a successful total hip arthroplasty), called “controls”gPatients treated one way with no comparison with group of patients treated another wayhA complete assessment of the quality of individual studies requires critical appraisal of all aspects of the study design

270 A. P. White et al.
Treatment of LBP with Spinal Fusion
In 2001, The Swedish Lumbar Spine Study compared outcomes for 310 subjects who underwent spinal fusion or nonsurgical treatment for treatment of degenerative, disabling LBP [21]. While the surgical treatment was any of three fusions, the nonsurgical treatment was more structured. The program included physical therapy, infor mative sessions, coping strategies, cognitive train-ing, as well as other pain relief procedures such as acupuncture and injections. When compared to the non-surgical treatment group, the fusion patients enjoyed improved resolution of back pain (32% as compared to 6.8%) and leg pain (20.5 vs. 17.8%), as well as supe-rior satisfaction (62.6 vs. 29% patients reporting “Much Better” and “Better”) and an increased rate of returning to work (39 vs. 23%). Excellent consistency of surgical results was maintained; there were no significant dif-ferences found between the first 100 and last 100 patients enrolled in the study. One significant limita-tion of this study was that there was a relatively high degree of crossover between assigned patient groups. The fact that many patients ultimately received treat-ment that they were not originally randomized to receive limited the power of the “intention to treat” analysis. As such, the study relied on an “as treated” analysis to report the statistical results. A second criti-cism of the study is that the heterogeneity of the non-surgical treatment group was not analyzed.
The following year, The Swedish Lumbar Spine Study reported the efficacy of three spinal fusion tech-niques for the treatment of degenerative, disabling LBP [22]. Patients were randomized to groups for postero-lateral fusion (PLF) without internal fixation, PLF with variable screw placement (VSP), and interbody fusion (anterior or posterior – depending on surgeon prefer-ence). Each technique demonstrated significantly reduced pain, disability, and signs of depression at 2 years follow-up. There was some difference found among fusion rates with 72% fusion in the PLF without internal fixation, 87% in the PLF with VSP, and 91% in the interbody treatment group. Despite this discrepancy, there was very little difference in patient outcomes.
In 2003 and 2006, Brox and colleagues attempted to repeat the Swedish Lumbar Spine Study by comparing PLF with VSP to nonsurgical treatment. This was done, in part, related to the criticism received for heterogeneous nonsurgical treatment group and high rate of crossover between assigned groups. These studies made use of
cognitive interventions such as informative sessions on pain receptors in the disks, facet joints, and muscles, as well as patients instructed to use their backs without cau-tion as they could not further injure them. Furthermore, the rehabilitation emphasized exercise to strengthen deep abdominal and core muscles of the erector spinae. It is notable that most patients were falsely of the opinion that use of their backs would worsen their situation. In both studies, the primary outcome of the Oswestry Disability Index (ODI) showed no significant difference in treatment between the posterior lumbar instrumented fusion and cognitive intervention with exercises. The nonsurgical group did demonstrate, however, significantly improved scores on the fear-avoidance assessments when compared to the surgical group. This may suggest continued success via self-initiated exercises and stretching. Both of these studies have been criticized, however, because of their surprisingly small number of patients (61 in 2003 and 57 in 2006) in each study [10, 11].
Fairbank and colleagues published a related ran-domized prospective study in 2005. Three hundred forty-nine patients were randomized to surgical (fusion) or nonsurgical treatment. The fusion tech-nique was determined by the surgeon. The nonsurgical group followed an intensive 3 week, 5 day per week rehabilitation program. This program emphasized stretching, stabilization exercises, and cardiovascular endurance exercises along with cognitive behavioral therapy to identify and overcome unhelpful beliefs about back pain. Although the surgical group experi-enced a more favorable Oswestry outcome (p > 0.045), the nonsurgical group also showed marked improve-ment from baseline. Also, other primary outcomes such as the shuttle walking test did not differ between groups. Due to the marginal improvement in the Oswestry Index only, it was concluded that this inten-sive rehabilitation plan could be as effective as surgery. More importantly, rehabilitation avoided the compli-cations that arose in 10.8% of the surgical cases. It was acknowledged, however, that such a program was unlikely to be available to the average patient [19].
While there may be a statistical benefit to fusion over typical nonsurgical treatments, surgical complications and associated psychological stressors must be consid-ered. The required recovery and risk associated with sur-gery can be used to guide the treatment of each individual patient. For example, patients who want the most rapid return to work may prefer the potential quick fix of sur-gery despite its risk [13].

2716.2 Review of the Medical Evidence Regarding the Surgical Treatment of Low Back Pain
Patient Selection for Spinal Fusion
There has been a great deal of difficulty in determining precise surgical indications for treating LBP. To this end, attempts have been made to classify physical as well as imaging findings. Another approach has been made to examine psychosocial factors. Trief and col-leagues recently reported the preoperative psychologi-cal evaluations and postoperative outcomes of 102 fusion patients. At 1-year follow-up, patients who expe-rienced considerable preoperative anxiety as defined by the Modified Somatic Perception Questionnaire were less likely to return to work (p < 0.001), less likely to report decrease in pain (p < 0.01), and less likely to report increase in function (p < 0.01). The authors also found that depression (as defined by the Zung Depression Scale) was predictive of poor outcomes, but with lower statistical certainty at p < 0.01, p < 0.058, and p < 0.05, respectively. Preoperative hostility defined by the Cook-Medely Hostility Scale, however, was not predictive of postoperative outcomes [39]. Furthermore, Schofferman et al. found that of 86 patients undergoing lumbar spine surgery, those with serious childhood psychological trauma had an 85% chance of an unsuccessful surgical result [37].
Certain psychosocial factors that may predict sur-gical outcomes were also investigated by Hagg and colleagues. A total of 264 patients (201 surgical) were evaluated for depression, personality traits, personal-ity disorders, as well as other behaviors. This study considered whether the patient was “improved” or not using the ODI and also considered whether or not they returned to full-time work. Age (p > 0.001), current amount of sick leave (p < 0.0001), and a Neurotic per-sonality trait (p > 0.02) were found to be significantly predictive of outcome. The authors concluded that “neurotic” patients, defined as having muscular ten-sion, somatic anxiety, psychathenia, and guilt, should not be offered surgical (fusion) treatment [28].
Evaluations of Fusion Techniques
Many surgeons have the impression that the manner in which the fusion procedure was performed has bearing on the success of the procedure. One of the potential problems with a posterior approach for lumbar fusion is the substantial tissue damage caused during
operation. This may compound the initial LBP and impair short-term clinical outcomes [3, 36].
Single-level anterior and posterior lumbar fusion techniques were retrospectively compared in a group of 122 patients with LBP by Pradhan and collegues [35]. Most patients had degenerative disk disease, although a few had spondylolisthesis with instability. Anterior lumbar interbody fusion (ALIF) with BAK cage implant was performed for 58 of 122 patients (48%), while the other 64 (52%) received a PLF with bilateral pedicle screw fixation. Both techniques uti-lized iliac crest autograft for fusion. Only 77 (63%) of the procedures were primary fusions, while 45 (37%) patients were treated with a revision of a previous fusion. Perio peratively, the ALIF procedure was asso-ciated with significantly less blood loss than the PLF (p < 0.01) and also required less time (p < 0.01). Hospital stay was also shorter for patients in the ante-rior approach group by an average of 1.6 days (p < 0.01). Revision subgroups showed no difference in hospital stay or blood loss compared to primary fusion patients. Complications occurred in 6 of 58 (10.3%) of the ALIF patients and in 8 of 64 (12.5%) of the PLF patients; this difference was not statistically signifi-cant. Radiographically confirmed fusion rates were very similar at 95% for the ALIF and 92% for the PLF. Primary outcomes were defined by the “Clinical Rating,” which was assigned by qualifying several criteria including patient satisfaction, pain relief, physical limitations, and use of analgesics. Clinical outcomes demonstrated little difference between ante-rior and posterior revision subgroups. When compar-ing primary fusion with revision subgroups, however, the primary fusion subgroup was superior in Clinical Rating when compared to the revision for both approaches (p < 0.01). Overall, this study found that the anterior interbody approach experiences favorable perioperative conditions, but shows little difference in long-term clinical outcomes [35].
The relative benefit of circumferential fusion vs. posterior (alone) fusion was recently reported, as well [42]. PLF or PLF with ALIF was performed for 148 patients with severe, chronic LBP. Success was ana-lyzed using the Dallas Pain Questionnaire (DPQ) and the Low Back Pain Rating Scale (LBPR). At 5–9 years follow-up, the circumferential fused patients were sig-nificantly better in all areas of the DPQ including daily activities (p > 0.002), work/leisure (p > 0.005), anxiety/depression (p > 0.017), and social concerns (p > 0.019).

272 A. P. White et al.
While the LBPR scale showed no difference between the two treatment groups for leg pain, it did demon-strate that the circumferential group experienced sig-nificantly less back pain (p < 0.05). Furthermore, the circumferential fusion provided higher fusion rates at 2 years follow-up than the PLF (92 vs. 80%) [16]. Recalling that Pradhan did not demonstrate a signifi-cant long-term clinical difference between ALIF alone and PLF alone, it may be the case that supplemental instrumented posterior fusion is a benefit to anterior interbody fusion [30, 35].
Total Disk Arthroplasty for LBP Treatment
To date, only two lumbar total disk arthroplasty devices have been Food and Drug Administration (FDA) approved with Investigational Device Exemption (IDE) investigation results reported in the literature. These are the Charité (DePuy Spine, Raynham MA) and the ProDisc (Synthes Spine, Paoli PA) devices.
The results of the FDA regulated IDE study com-paring the Charité artificial disk to ALIF were reported with level 1 evidence in two recent publications. One detailed the clinical outcomes with 24-month mini-mum follow-up [6], while the other evaluated the potential association between the technical accuracy of the surgery and subsequent clinical and radiographic outcomes [32]. In total, 304 patients with symptom-atic, single-level degenerative disk disease at L4-L5 or L5-S1 were enrolled in the study. They were random-ized to receive either Charité arthroplasty or a stand-alone BAK cage instrumented ALIF. The ALIF procedure was chosen over a circumferential or poste-rior fusion in order to realistically compare intraopera-tive statistics and clinical outcomes without skewing by neurological complications.
Clinical outcome was assessed primarily via the ODI, the Visual Analog Scale (VAS), and the SF-36 Health Survey at 6 weeks, 3 months, 6 months, 12 months, and 24 months follow-up. At 2 years follow-up, the Charité group showed statistically greater overall success (p < 0.0001) and ODI score (p < 0.0038) when compared to the ALIF group. Furthermore, patient satisfaction 2 years after surgery was 73.7% in the Charité group as compared to 53.1% in the control
(p< 0.0550). Significantly more (p < 0.0062) investi-gational patients (69.9%) reported that they would have the same procedure again as compared to the control ALIF patients (50%). Also, it should be noted that the changes in ODI and VAS scores for the Charité group at 6 months follow-up (p < 0.0017) were more statistically significant than the control at the 2-year mark (p < 0.267). This may indicate that the Charité group experienced a rapid postoperative improvement with diminished continuing long-term gains [6].
Postoperative radiographs of the 304 Charité IDE patients were later evaluated to assess the association between the accuracy of Charité device placement and dynamic radiographic findings including range of motion, disk space height restoration, and subsidence. At 2 years follow-up, the patients who underwent total disk replacement showed a mean 13.6% increase in ROM, while the fusion group showed an 82.5% decrease. It was found that the Charité group had statistically sig-nificant increases in disk space height (p > 0.05) and less subsidence (p > 0.02). Based on PA and lateral radio-graphs, device placement was categorized. Patients with an “ideally” placed device (within 3 mm of exact central placement in coronal and midsagittal planes) (81.1% of the study patients) showed improved disk height restora-tion compared to “suboptimal” placement (3–5 mm from exact central placement in at least one plane) (12.2%) and “poor” placement (>5 mm from exact central place-ment in at least one plane) (6.7%). Also, the poorly placed disks had significantly less flexion and extension ROM compared to the other two. The ideal and subopti-mal groups experienced 7.12° and 7.47° of flexion/extension ROM, respectively, while the poor group experienced only 3.15° (p > 0.003.) The authors con-cluded that the accuracy of implantation was critical in order to achieve the goals of the procedure, particularly restoration of height and postoperative motion [32].
In 2007, the results of the ProDisc-L Total Disk Replacement FDA IDE study were reported. The FDA directed inclusion and exclusion criteria were similar to that of the Charité IDE study, but the permitted treatment levels and the control group were different. The experi-mental ProDisc device was implanted between L3 and S1 and was compared to a circumferential fusion as a control. The circumferential fusion procedure consisted of an ALIF with interbody allograft and a PLF with pedi-cle screw instrumentation. In total, 286 patients were enrolled. Patients were randomized 2:1 (experimental to

2736.2 Review of the Medical Evidence Regarding the Surgical Treatment of Low Back Pain
control) with 161 undergoing ProDisc arthroplasty and 75 patients undergoing a circumferential fusion. The authors presented multiple outcomes measures to dem-onstrate superiority of ProDisc treatment compared to fusion at 2 years follow-up. ODI scores were signifi-cantly higher in the ProDisc group (p < 0.0449), as were neurological relief (p < 0.0341) and maintenance of disk height (p < 0.0029). The reported fusion rate in the con-trol arm was 97% based on radiographic analysis. Also, Arthroplasty device motion was maintained at 2 years in 94% of patients, averaging 7.7° per segment [4, 48].
While these two well-designed, prospective, ran-domized FDA IDE studies do represent level 1 evidence, it is important to recognize that the minimum follow-up in each investigation is only 2 years. Since there are both theoretical and observed long-term shortcomings of total disk replacement, investigators have great interest in analyzing long-term results. One recent report con-sidered 106 patients who were treated with single-level lumbar Charité total disk arthroplasty in France between 1989 and 1995, representing a minimum follow-up of 10 years [17]. At the 10-year evaluation, 82.1% of patients reported either good or excellent outcome with 87 of 96 (89.6%) working patients returning to work. Radiographic analysis demonstrated that 90.6% of the implants were still mobile. The author concluded that these total disk replacement patients represented evi-dence of safe and effective long-term results.
Another longer-term follow-up analysis was recently reported in the literature. In this series, 33 patients underwent Charité TDR with 41-month mean follow-up and 24 patients underwent ProDisc TDR with 38-month follow-up [38]. The investigators evaluated clinical and radiographic outcomes, but were also inter-ested in evaluating the pre and postoperative status of the adjacent intervertebral disks and in the facet joints at the treated levels. For this reason, patients were evalu-ated with MR imaging as well. They mean ODI improvement was found to be similar to the IDE studies (78.9% for Charité and 75.8% for ProDisc). Maintenance of motion was good, with a change in ROM of 2.4° at L4-L5 and 2.4° at L5-S1 for Charité and 5.4° and 2.1° for ProDisc, which are values similar to both the IDE FDA studies and the 10-year follow-up of Charité pre-viously discussed. Adjacent disk degeneration as evalu-ated by the Pfirrmann scale using T2-weighted MRI, however, was concerning. The authors reported that 6/31 (19%) of the Charité and 6/21 (28%) of the ProDisc had degenerated. While there was not a statistically
significant difference between implants, concern was raised as to whether both devices were accelerating the rate of adjacent segment degeneration. The authors also evaluated the degeneration of the same segment facet joints using the Fujiwara grading system. They reported that 12/33 (36%) of the Charité and 8/25 (32%) of the ProDisc had demonstrated significant degenerative change of the facet joints by the 41 and 38 month mean evaluation, respectively. The authors questioned if the arthroplasty devices may have accelerated the wear of the same segment facet joints [38].
Complications of Surgery for Low Back Pain
The Swedish Lumbar Spine Study Group performed an analysis to assess complications and reoperation rates in a homogenous population with chronic LBP. This multicenter study included 74 patients in the control group and over 200 patients in the surgical groups. Group 1 patients received a PLF without internal fixa-tion, group 2 patients received a PLF with VSP, and group 3 patients received PLF with VSP and an anterior interbody fusion, constituting a traditional circumfer-ential fusion. Overall, 52/211 (24.6%) patients experi-enced a complication. The rate of early (within 2 weeks of surgery) complications in groups 1, 2, and 3 was 6, 18, and 31% (p > 0.001), respectively. The total rate of complications in the same groups was 12, 22, and 40% (p > 0.0003). An analysis of preoperative conditions showed that the preoperative risks were not different between patient groups. The authors attributed the observed differences in complication rates to the surgi-cal techniques. Despite this significant difference in complications, however, a clinical outcomes analysis showed no significant difference between the tech-niques. Furthermore, there were no significant differ-ences in outcomes between subgroups of patients with complications and those without.
Revision surgery was required in 31/211 (15.0%) patients. This included four in the noninstrumented group for pseudarthrosis and 14 in the instrumented groups requiring hardware removal. There was no dif-ference found in clinical outcomes between patients with hardware and those who had it removed at 2 years follow-up. This study demonstrated that complication rates increased with more complex and invasive surgical

274 A. P. White et al.
technique. The clinical outcomes at 2 years, however, were not impacted by the presence of complications or requirement for revision surgery [8, 20].
A study reporting complications following total disk replacement included only 27 patients. All patients had previous Charité implants and presented with persisting back and leg pain. The cause of this pain seemed to be degeneration of adjacent joints (51.9%) with facet joint arthrosis predominating. Additionally, subsidence (59.3%) and anterior migration of the implant (7.4%) was observed in some cases with hyperlordosis seen in some cases [40]. It was hypothesized that facet joint arthrosis may appear several years after implantation as seen in 40.7% of (11 of 27) patients with complications. This may be due to excessive joint loading secondary to abnormal motion dictated by implant kinematics. Additionally, the shock absorbing function of the inter-vertebral disk is not replicated by the polyethylene core of the Charité (and most other) devices. As such, motion in the compression distraction loading modes is lost. End plate fixation is an additional focus for concern. Current implants are built for good initial bone fixation, but have questionable long-term integration. The ante-rior, retroperitoneal approach for proper positioning can also be a complicated working area in close prox-imity to the great vessels, potentially leading to throm-bosis. For males, there is a risk of permanent retrograde ejaculation between 2 and 7% and occurred in 7.4% (2 of 27) patients in this study. The main problem, how-ever, is revision. In the case of failure, these implants are very difficult to remove without damaging neigh-boring vessels and nerve roots. Often the solution is an additional PLF over the implant (29.6%), but histori-cally this has shown very little clinical improvement.
Cochrane Studies
The most comprehensive review of surgical treatment for LBP is represented by the Cochrane Review. In 1999, this study compiled 26 randomized controlled trials involving surgery for lumbar disk prolapse. It revisited this subject in 2005 with 31 randomized con-trolled trials reporting with level 1 evidence. In addi-tion, 14 randomized controlled trials were used in the metaanalysis of degenerative lumbar spondylosis.
The efficacy of discectomy was evaluated in nine trials. Discectomy was compared to another surgical
technique and to conservative treatment. Metaanalysis of patient and observer outcome ratings showed dis-cectomy was significantly superior to conservative treatment after 1 year. At 4 and 10-year follow-up, however, there was no statistically significant differ-ence found between the two groups with regained motor function, but residual sensory deficits using var-ious patient-centered pain and function analysis. Microdiscectomy experienced longer intraoperative time, but without any other difference from the stan-dard procedure. Using different types of interposition membrane did not statistically change scarring or clin-ical outcomes.
The analysis of degenerative lumbar spondylosis was aided by splitting the trials into two groups. One group included all techniques for stenosis with nerve compression, while the other included all fusions. No randomized controlled trials were identified studying the efficacy of surgical decompression for stenosis. A few studies examining the influence of PLF in addition to decompression vs. a control decompression showed little difference between the two groups. Instrumentation in fusion improves fusion rates (93% with pedicle screws vs. 86% without pedicle screws), but does not improve clinical outcome (86 vs. 90%) when com-pared to noninstrumented fusion.
Several of these studies had methodological errors in randomization, blinding, or even inconsistent rat-ings of clinical outcome. Although there were uni-formly good follow-up rates, most of the studies only had data for 2 years and there was considerable patient cross-over. Furthermore, several studies included fewer than 50 patients with heterogeneous pathologies.
Unfortunately, due to these issues, the authors were unable to draw any statistically significant conclusions about the relative effectiveness of three different fusion approaches. Also, due to the small number of trials for disk arthroplasty, no firm conclusions about this sub-ject could be made [24, 25].
SPORT Trials
In 2006 and 2007, results of two large studies represent-ing Level 1 evidence on the treatment of common spinal disorders were published. The Spine Patient Outcomes Research Trial (SPORT) utilized 11 centers across the United States to compare clinical outcomes for surgical

2756.2 Review of the Medical Evidence Regarding the Surgical Treatment of Low Back Pain
vs. nonsurgical treatment for several diagnoses at various follow-up times. The study examining lumbar disk her-niation enrolled 743 patients with symptoms and confir-matory signs of lumbar radiculopathy with a disk herniation at the corresponding level validated by imag-ing. Of these, 528 received surgical treatment of a stan-dard open discectomy with examination of nerve root and 191 received nonsurgical treatment such as physical therapy, education and counseling, home exercises, and NSAIDs. At 3 months follow-up as defined by the SF-36 pain survey, the surgical group (40.9) experienced sig-nificantly better bodily pain measures compared to the nonsurgical group (26.0). The ODI scores were also in favor of the operative group at 3 months (mean change: −36.1 vs. −20.9). At 2 years follow-up, however, this sig-nificant margin tapered off. Bodily pain reported by the surgical group showed only moderate continued improve-ment to 42.6, while the nonsurgical group showed steady pain reduction to a score of 32.4. Finally, the ODI scores at 2 years also followed this trend with the nonoperative group (−24.2) gaining more ground than the surgical group (−37.6) [45]. The authors concluded that although both treatments helped to resolve back pain and sciatica at 2 years follow-up, those who received surgery experi-enced a greater improvement and more immediate ame-lioration of pain.
The study examining spondylolisthesis randomized 304 patients with neurogenic claudication or radicular leg pain with associated neurologic signs, spinal steno-sis, or degenerative spondylolisthesis confirmed by lat-eral radiograph. One hundred fifty-nine received surgical treatment of a standard posterior decompressive laminectomy with or without bilateral single-level fusion using iliac crest autograft, while 145 received similar conservative as treatment detailed above. At 3 months follow-up using the same outcomes measures, the sur-gical group (28.1) experienced significantly better bodily pain measures compared to the nonsurgical group (10.3). The ODI scores were also in favor of the operative group at 3 months (mean change: −20.8 vs. −6.2). At 2 years follow-up, this trend persisted. Bodily pain reported by the surgical group (29.9) was still greater than the nonsurgical group (11.7). Similarly, the surgi-cal group experienced better ODI scores at 2 years fol-low-up than the nonsurgical group (−24.2 vs. −7.5). Clearly, the conclusion drawn was that for patients with spondylolisthesis and spinal stenosis, surgical treatment is considerably superior to nonsurgical treatment after 2 years [8, 18, 44, 45].
In 2008, another study using the SPORT design and resources examined intervertebral disk herniation (IDH) and back pain with focus on location and mor-phology of the herniation. This study included 1,191 patients with sciatica and confirmatory imaging study demonstrating IDH. Hernias were classified by loca-tion (central, posterolateral, foraminal, and far lateral) and morphology (protrusion, extrusion, and sequestra-tion). As with the prior trials, standard open discec-tomy with nerve root decompression was compared to nonoperative therapy including physical therapy, edu-cation, and medication. Of the eligible patients, 775 operative therapy within 2 years and 416 remained nonoperative. This study used a 0–6 pain scale to eval-uate how “bothersome” their back pain and leg pain was at baseline, 3 months, 1 year, and 2 years follow-up. They found surgical intervention provided greater improvement in both back and leg pain than nonopera-tive therapy at each follow-up period (p < 0.001). Surgery provided greater relief in leg pain than back pain at 3 months follow-up (−1.4 vs. −0.9 p < 0.001), but not at 1 year and 2 years [2, 44, 45].
Surgery for all herniation subgroups resulted in sig-nificantly greater improvement in back pain from base-line at each follow-up. Central herniations were present in only 131 (11%) patients and were associated with younger age greater back than leg symptoms. Those receiving surgical intervention experienced significant reductions in pain when compared to conservative treatment at 3 months (p < 0.028) and 1 year (p < 0.041), but not at 2 years (p < 0.056). Due to a limited number of patients with foraminal and far lateral lesions, these two subgroups were incorporated with the posterolat-eral lesions into a lateral subgroup. These patients experienced significant reductions in pain with surgery at every follow-up period (p < 0.001). Protrusion mor-phology herniations experienced significant reductions in pain when compared to conservative treatment at 3 months (p < 0.001) and 2 years (p < 0.0016), but not at 1 year (p < 0.15). A limited number of sequestrations were combined with the extrusions for statistical anal-ysis. This subgroup experienced significant reductions in pain when compared to conservative treatment at 3 months and 1 year (p < 0.001), but not at 2 years (p < 0.15) [2].
The largest limitation of this study was nonadher-ence of patients to their randomized treatment cohort. In the first 2 years of follow-up, 40% of patients assigned to surgery did not have surgery, while 45%

276 A. P. White et al.
assigned to nonoperative care did have surgery [2]. This potential bias was accounted for by statistical analysis using an as-treated method. The authors stress the lack of significant difference is baseline back pain scores or treatment effect of surgery between the ran-domized and as-treated groups.
Conclusions
While there is some convincing evidence that surgical treatment for LBP may be reasonable for many condi-tions, the medical evidence discussed is lacking to sup-port this categorically. Successful LBP relief with surgery intervention occurs most frequently in patients with a definitive source to their pain. The poor predict-ability of pain relief seen in many cases may be related to our incomplete understanding of the etiology of LBP and our relatively poor ability to identify a cause. More research is needed to elucidate these uncertain-ties before decisive conclusions can be met.
References
1. Ahmed M, Bjurholm A, Kreicbergs A et al (1993) Neuropeptide Y, tyrosine hydroxylase and vasoactive intes-tinal polypeptide-immunoreactive nerve fibers in the verte-bral bodies, discs, dura mater, and spinal ligaments of the rat lumbar spine. Spine 18:268–273
2. Am P, Blood EA, Frymoyer JW et al (2008) SPORT lumbar intervertebral disk herniation and back pain: does treatment, location or morphology matter? Spine 33(4):428–435
3. Bentsen SB, Wahl AK, Hanestad BR et al (2007) Outcomes for patients with chronic low back pain treated using instru-mented fusion. Scand J Caring Sci 21:71–78
4. Bertagnoli R, Yue JJ, Shah RV et al (2005) The treatment of disabling single-level lumbar discogenic low back pain with total disc arthroplasty utilizing the ProDisc prosthesis. Spine 30:2230–2236
5. Biyani A, Andersson GBJ (2004) Low back pain: pathophys-iology and management. J Am Acad Orthop Surg 12: 106–115
6. Blumenthal S, McAfee PC, Guyer RD et al (2005) A pro-spective, randomized, multicenter food and drug administra-tion investigational device exemptions study of lumbar total disc replacement with the CHARITETM artificial disc versus lumbar fusion; Part I. Spine 30:1565–1575
7. Boden SD, Davis DO, Dina ST et al (1990) Abnormal mag-netic-resonance scans of the lumbar spine in asymptomatic subjects. J Bone Joint Surg Am 72:403–408
8. Boden SD, Kang J, Sandhu H et al (2002) Use of recombinant human bone morphogenetic protein-2 to achieve posterolat-eral lumbar spine fusion in humans. Spine 27: 2662–2673
9. Brodke DS, Ritter SM (2004) Nonoperative management of low back pain and lumbar disc degeneration. J Bone Joint Surg Am 86:1810–1818
10. Brox JI, Sorensen R, Friis A et al (2003) Randomized clini-cal trial of lumbar instrumented fusion and cognitive inter-vention and exercises in patients with chronic low back pain and disc degeneration. Spine 28:1913–1921
11. Brox JI, Reikeras O, Nygaard O et al (2006) Lumbar instru-mented fusion compared with cognitive intervention and exercise in patients with chronic back pain after previous surgery for disc herniation: a prospective randomized con-trolled study. Pain 122:145–155
12. Carragee EJ (2005) Persistent low back pain. N Engl J Med 352:1891–1898
13. Carragee EJ (2006) Surgical treatment of lumbar disc disor-ders. JAMA 296:2485–2487
14. Carragee EJ, Tanner CM, Yang B et al (1999) False-positive findings on lumbar discography. Spine 24:2542–2547
15. Carragee EJ, Lincoln T, Parmar VS et al (2006) A gold stan-dard evaluation of the “Discogenic Pain” diagnosis as deter-mined by provocative discography. Spine 31:2115–2123
16. Christensen FB, Hansen ES, Eiskjaer SP et al (2002) Circumferential lumbar spinal fusion with Brantigan cage versus posterolateral fusion with titanium Cotrel-Dubousset instrumentation: a prospective, randomized clinical study of 146 patients. Spine 27:2674–2683
17. David T (2007) Long term results of one-level lumbar arthroplasty. Spine 32:661–666
18. Dimar JR, Glassman SD, Burkus KJ et al (2006) Clinical outcomes and fusion success at 2 years of single-level instru-mented posterolateral fusions with recombinant human bone morphogenetic protein-2/compression resistant matrix ver-sus iliac crest bone graft. Spine 31:2534–2539
19. Fairbank J, Frost H, Wilson-MacDonald J et al (2005) Randomised controlled trial to compare surgical stabilisa-tion of the lumbar spine with an intensive rehabilitation pro-gramme for patients with chronic low back pain: the MRC spine stabilisation trial. BMJ 330:1233
20. Fritzel P, Hagg O, Nordwall A (2004) Complications in lum-bar fusion surgery for chronic low back pain: a comparison of three surgical techniques used in a prospective random-ized study. A report from the Swedish Lumbar Spine Study Group. Eur Spine J 12:178–189
21. Fritzell P, Hagg O, Wessberg P et al (2001) 2001 Volvo Award winner in clinical studies: lumbar fusion versus non-surgical treatment for chronic low back pain. Spine 26: 2521–2534
22. Fritzell P, Hagg O, Wessberg P et al (2002) Chronic low back pain and fusion: a comparison of three surgical tech-niques. Spine 27:1131–1141
23. German JW, Fole KT (2005) Disc arthroplasty in the man-agement of the painful lumbar motion segment. Spine 30:S60–S67
24. Gibson JNA, Waddell G (2005) Surgery for degenerative lumbar spondylosis: update Cochrane Review. Spine 30:2312–2320
25. Gibson JNA, Grant IC, Waddell G (1999) The Cochrane Review of surgery for lumbar disc prolapse and degenerative lumbar spondylosis. Spine 24:1820–1832

2776.2 Review of the Medical Evidence Regarding the Surgical Treatment of Low Back Pain
26. Grotle M, Brox JI, Veierod MB et al (2005) Clinical course and prognostic factors in acute low back pain. Spine 30:976–982
27. Gruber HE, Norton HJ, Hanley EN Jr (2000) Anti-apoptotic effects of IGF-1 and PDGF on human intervertebral disc cells in vitro. Spine 25:2153–2157
28. Hagg O, Fritzell P, Ekselius L et al (2003) Predictors of out-come in fusion surgery for chronic low back pain. A report from the Swedish Lumbar Spine Study. Eur Spine J 12:22–33
29. Jensen MC, Brant-Zawadzki MN, Obuchowski N et al (1994) Magnetic resonance imaging of the lumbar spine in people without back pain. N Engl J Med 331:69–73
30. Kim KT, Lee SH, Lee YH et al (2006) Clinical outcomes of 3 fusion methods through the posterior approach in the lum-bar spine. Spine 31:1351–1357
31. Korhonen T, Karppinen J, Malmivaara A et al (2000) Abstract: treatment of sciatica with infliximab, a monoclonal humanised chimaeric antibody against TNF-a. 29th Annual Meeting Proceedings. International Society for the Study of the Lumbar Spine, Toronto, Canada, p 14
32. McAfee PC, Cunningham B, Holsapple G et al (2005) A prospective, randomized, multicenter Food And Drug Administration investigational device exemption study of lumbar total disc replacement with CHARITE artificial disc versus lumbar fusion; part II. Spine 30:1576–1583
33. Mirza SK, Deyo RA (2007) Systematic review of random-ized trials comparing lumbar fusion surgery to nonoperative care for treatment of chronic back pain. Spine 32:816–823
34. Peng B, Wu W, Hou S et al (2005) The pathogenesis of dis-cogenic low back pain. J Bone Joint Surg (Br) 87B:62–67
35. Pradhan BB, Nassar JA, Delamarter RB et al (2002) Single-level lumbar spine fusion: a comparison of anterior and pos-terior approaches. J Spinal Disord Tech 15:355–361
36. Sasso RC, Kitchel SH, Dawson EG (2004) A prospective, randomized controlled clinical trial of anterior lumbar inter-body fusion using a titanium cylindrical threaded fusion device. Spine 29:113–122
37. Schofferman J, Anderson D, Hines R et al (1992) Childhood psychological trauma correlates with unsuccessful lumbar spine surgery. Spine 17(Suppl):S138–S144
38. Shim CS, Lee SH, Shin HD et al (2007) CHARITE versus ProDisc. Spine 32:1012–1018
39. Trief PM, Grant W, Fredrickson B (2000) A prospective study of psychological predictors of lumbar surgery out-come. Spine 25:2616–2621
40. Van Ooij A, Oner FC, Verbout AJ (2003) Complications of artificial disc replacement. J Spinal Disord Tech 16:369–383
41. Van Tulder M, Koes B, Bombardier C (2002) Low back pain. Best Pract Res Clin Rheumatol 16:761–775
42. Videbaek TS, Christensen FB, Soegaard R et al (2006) Circumferential fusion improves outcome in comparison with instrumented posterolateral fusion: long term results of a randomized clinical trial. Spine 31:2875–2880
43. Webster BS, Snook SH (1990) The cost of compensable low back pain. J Occup Med 32:13–15
44. Weinstein JN, Lurie JD, Tosteson TD et al (2006) Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT) observa-tional cohort. JAMA 296:2451–2459
45. Weinstein JN, Lurie JD, Tosteson TD et al (2007) Surgical versus nonsurgical treatment for lumbar degenerative spon-dylolisthesis. N Eng J Med 356:2257–2270
46. West JL III, Bradford DS, Ogilvy JW (1991) Results of spi-nal arthrodesis with pedicle screw-plate fixation. J Bone Joint Surg (Am) 73:1179–1184
47. Willems PC, Elmans L, Anderson PG et al (2007) Provocative discography and lumbar fusion. Spine 32:1094–1099
48. Zigler J, Delamarter R, Spivak JM et al (2007) Results of the prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of the ProDisc-L Total Disc Replacement versus circumferen-tial fusion for the treatment of 1-level degenerative disc dis-ease. Spine 32:1155–1162

279
Index
AAccuflex device, 223Adjacent level degeneration (ALD)
incidence of, 189interspinous implants, 162motion preservation, effect of, 189, 190postcervical fusion, 160
Adjacent level diseasedisc arthroplasty, 162–163hybrid/novel approaches, 162interspinous implants, 162pedicle screw-based nonfusion systems, 162spinal fusion, 159–161
index surgery, 159Kaplan Meier survival analysis, 161lumbar fusion, 160
Adjacent segment decompensation. See Posterior dynamic stabilization (PDS)
Adjacent segment failure, 113–115. See also Nonrigid stabilization
Adult degenerative scoliosis, 113Aetiology, disc degeneration
genetic predisposition, 5impaired nutrient supply, 6–7mechanical loading, influence of, 5physicochemical environment, 5–6
ALD. See Adjacent level degenerationALIF. See Anterior lumbar interbody fusione-Aminocaproic acid, 171Anterior lumbar interbody fusion (ALIF), 271, 272Aprotinin, 171Arthroplasty, 267. See also Total disc arthroplastyAxial back pain. See Internal disc disruption
BBack schools
acute stage, 80evidence, 79–80group education vs. individual education, 80–81patient education, 81
Biomechanical effects. See Lumbar posterior dynamic stabilization
Blood loss managementantifibrinolytics, 170–171dosage and cost, 171, 172spine surgery
systemic and local methods, 170types, 169
TRALI, 169
CCAM. See Complementary and alternative medical therapyCBT. See Cognitive behavioral therapyCentral nervous system, sensitization, 66Charité, TDR device
disc space height, 196Oswestry scores, 195range of motion, 196VAS, 195
Chiropractic treatmentclinical subjects, 86–87education and training, 86mobilization and manipulation, 90patient encounter
clinical assessments and encounterparts, 88–89spine instrumental measures, 88–89
practice, 87–88spinal manipulation, 85–86 (see also Spinal manipulation)
Classification, function of timeacute and subacute, 66–67chronic, 67–68
Clinical and biomechanical stagesradiologic observation, 29–30stabilization, 29temporary dysfunction, 29unstable phase, 29
Cochrane review, 81, 274Coflex device, 242Cognitive behavioral therapy (CBT), 81, 82Complementary and alternative medical therapy (CAM)
healthcare delivery, 88patient-physician interaction-related factors, 75–76practice, 87–88therapies and techniques, 88
Comprehensive rehabilitationback schools
acute stage, 80group education vs. individual education, 80–81patient education, 81
CBT, 81European guidelines
back schools and working population, 80

280 Index
efficacy, 79–80evidence-based medicine (EBM), 79exercise treatment, 81–82level of evidence, 79multidisciplinary treatment, 81multimodal programs, 82
Conservative treatmentchiropractic treatment (see Chiropractic treatment)IDET
mechanism, 95Oswestry disability index (ODI), 96, 97vs. PIRFT, 99vs. placebo, 97–98posterior annulus, 95–96prone position, 95randomized placebo-controlled trial, 96safety issues, 97–98VAS, SF-36, 96, 97
lumbar orthosesclinical effectiveness, 103–104degenerative disc disease, 102kinematics, 101mechanical effectiveness, 102–103types comparison, 104
natural evolution, NSLBPabsence of work and sick listing, 68–69acute and subacute, 66–67chronic, 67–68database, 65–66definition, 65methodological variations, 70
patient physician-related interactionCAM, 75–76evaluation, 76psychosocial factors, 76
patient-related factorsbiological and psychological, 74prescribe medication, 75
physician, 75PIRFT
vs. IDET, 99radiofrequency probe, 98RCT, 98
societal-related factors, 76–77treatment
assumption, 74effectiveness, 74mortality, 73
Cord-type systems, 222Core outcome measures index (COMI), 228Cosmic systems, 237Cost-utility evaluations. See SF-6D vs. EQ-5DCytokines role
anti-TNF treatment, 19interleukin and disc herniation, 18intervertebral disc and facet joint degeneration, 18–19and spine surgery, 19–20TNF and disc herniation, 17–18
DDASCOR technology, 132Degenerative disc disease (DDD). See also Disc degeneration
advantages, 180contra-indications
anatomical considerations, 179–180approach considerations, 179disc space collapse, 178–179obesity, 178osteoporosis, 178psychological and behavioural issues, 179spinal deformity, 178
diffusion and nutrition, 50–53end plate, structure and function of, 47–50fusion, 180indications, 178lumbar orthoses, 101–105nutrition evaluation, 47
Degenerative instability, 111–113Degenerative processes, disc, 7–8Degenerative spine
anti-TNF treatment, 19cytokines, 17 (see also Cytokines role)
and disc herniation, 18intervertebral disc and facet joint degeneration, 18–19and spine surgery, 19–20
TNF and disc herniation, 17–18Degenerative spondylolisthesis, 111Delta fixation, 151, 152Diagnosis
disc degenerationdiffusion and nutrition, 50–53end plate structure and function, in vivo, 47–50nutrition evaluation, 47
dynamic MRI, spine (see also Dynamic MRI, spine)diagnostic aspects, 40–43limitations, 43technical aspects, 39–40
physician extender roleallied healthcare professionals, 57–59clinical tasks, 60hospital tasks, 59–60office tasks, 59
Disc arthroplasty, 162–163Disc degeneration
aetiology ofgenetic predisposition, 5impaired nutrient supply, 6–7mechanical loading, influence of, 5physicochemical environment, 5–6
biology of, 3–4biomechanical effects, 4diffusion and nutrition
signal intensity (SI), 50treatment, 51, 53various patterns, post-contrast MRI, 51–53
end plate structure and function, in vivodamage type, severity of, 48–49logistic curve pattern, 49–50lumbar discs, 49–50region types, 47–48
epidemiology and diagnosis, 4histological findings and biomechanical effects, 4innervation and vascularization, 7molecular aspects of, 7–8

Index 281
morphology, normal disc, 3nutrition evaluation, 47
Disc herniationinterleukin, 18sciatica, anti-TNF treatment, 19tumour necrosis factor alpha, 17–18
Disc space collapse, 178–179Dynamic MRI, spine
diagnostic aspectsangular motion, 42axial rotation, 42biomechanical aspects, 41–42disc morphology, 40dynamic stabilization, effects of, 42–43facet joints, 41flexion and extension, 40lateral bending, 42ligaments, 41paraspinal muscles, 41spinal canal and intervertebral foramen, 40–41translational motion, 42weight-bearing, 40
limitations, 43technical aspects, 39–40
Dynamic stabilization systems. See Pedicle-based dynamic stabilization systems
Dynarod PDS system, 209Dynesys device, 234–236.
See also Lumbar posterior dynamic stabilisationDysplastic spondylolisthesis, 110–111
EElectromyographic activity, instability
behaviour, 35–36recording, 35
End plate (EP)degenerative disc disease, 47structure and function, assessment
classification and score, 48–49damage type, severity of, 48–49logistic curve pattern, 49–50lumbar discs, 49–50region types, 47–48
FFacet joints, 12
arthritis, 115, 118degeneration, 155denervation, 156–157
Finite element model (FE-model), 207, 208Flexion-extension motion
IMD device, 32, 33pattern of motion, 33–34protocol, 34, 35radiography and instability, 30–31
Fusion vs. nonfusion. See Hybrid construct, DDD
GGenetic predisposition, 5
HHealth related quality of life (HRQOL), 67Health utility index (HUI), 260Helical axis of motion (HAM), 216Heterotopic ossification (HO), 188–189Hoffman–Slätis fixator, 167HRQOL. See Health related quality of lifeHUI. See Health utility indexHybrid construct, DDD
anterior approach, 132Dynesis system, 133, 134lumbar lordosis, 131pedicular-based systems, 133posterior approach, 132
IIDET. See Intra-discal electrothermal therapyIMD. See Intervertebral patterns of motionImplanted model formulation, 208–209Implant failure. See Nonrigid stabilizationInfluencing factors, chronic back pain
fibromyalgia, 69HRQOL, 67occupational, 69physical, 69psychosocial, 68
Initiation, disc degeneration, 5–6Instability. See Segmental instabilityInSwing® (Orthofix spinal implants), 243Internal disc disruption, 118Interspinous implants, 162. See also Lumbar
spinal stenosis (LSS)Intervertebral disc and facet joint degeneration, 18–19Intervertebral disc degeneration. See Disc degenerationIntervertebral instability. See also Segmental instability
dynamic loading, in vivo, 31–32experimental injuries, 33–34kinematics of, 32patterns of motion, 33and radiography, 30–31
Intervertebral patterns of motion (IMD)flexion-extension motion, 33in humans, 34–35
Intra-discal electrothermal therapy (IDET)mechanism, 95Oswestry disability index (ODI), 96, 97vs. PIRFT, 99vs. placebo, 97–98posterior annulus, 95–96prone position, 95randomized placebo-controlled trial, 96safety issues, 97–98VAS, SF-36, 96, 97
In vitro cadaveric model, 253
KKaplan Meier survival analysis, 161Kineflex, TDR device
disc space height, 196exclusion and inclusion criteria, 194

282 Index
Oswestry scores, 195range of motion, 196visual analog score (VAS), 195
LLaminotomy, 129Ligaments, 13LSS. See Lumbar spinal stenosisLumbar disc arthroplasty
BAK cages, 199–200degenerative spondylolisthesis, 200, 201iatrogenic lumbar rotational instability, 202, 203limitations, 199, 200
Lumbar lordosis, 131Lumbar orthoses
clinical effectivenesslevels, 103–104prevention effect, 104
degenerative disc disease, 102kinematics, 101mechanical effectiveness
back muscle force reduction of, 103immobilization and restriction, 102
types comparison, 104Lumbar posterior dynamic stabilization
biomechanical effectscontinued inter-segmental motion, 2193-dimensional kinematic evaluation, 215–216helical axis of motion (HAM), 216L3-L5 cadaveric specimen, 216–217range of motion (ROM) and neutral zone (NZ), 215stress profile, 217traditional rigid rod fixation, 218
Dynesys device, 213–215intervertebral disc, 213
Lumbar spinal fusionadjacent segment problem, 113–115adult degenerative scoliosis, 113clinical evaluation, 110degenerative spondylolisthesis, 111dysplastic spondylolisthesis, 110–111facet joint arthritis, 115, 118internal disc disruption, 118pathomorphological correlations, 109, 110postdiscectomy syndrome, 115, 116spinal stenosis, 113spondylolysis, 110–111surgery, subdivisions, 118transitional anomalies, 115, 117true instability, 111–113
Lumbar spinal stenosis (LSS)added tension band
DIAM device, 246dorsoventral (DV) loading, 245InSwing® (Orthofix spinal implants), 243sagittal plane radiographs, 244
decompression, 129definitions of, 241dynamic nature, 241interspinous processes implants, 242–243laminectomy vs. fenestration technique, 127
laminotomy, 129pre and post-operative aspect, 128–129treatment, 241–242
Lumbar spine, 227–230. See also Semirigid fixation systemLumbar total disc replacement
clinical literatures, 184effect of
adjacent level degeneration (ALD), 190implant positioning, 187number of levels, clinical outcomes, 185patient’s age, clinical outcomes, 186prior surgery, 186range of motion (ROM), 187
evidence-based medicine (EBM), 183incidence of
vs. adjacent level degeneration (ALD), 189heterotopic ossification (HO), 189radiographic and symptomatic facet degeneration, 188
motion technology issues, 187–190patient selection issues, 185–187surgical technique issues, 187
MMagnetic resonance imaging (MRI), 39. See also Dynamic
MRI, spinedisc degeneration, 4lumbar PI defects classification, 139
Marchetti–Bartolozzi classification, spondylolisthesis, 140, 141Matrix formation and degradation, 5–6Matrix metalloproteinases (MMPs), 5, 8, 268Minimally important difference (MID), 261, 263MMPs. See MatrixmetalloproteinasesMuscle spasm, 13Myoelectric activity reduction, 31
NNonrigid stabilization
dynamic fixation system, failuresCosmic, 237Dynesis, 234–236
literature review, 237–238Nonspecific low back pain (NSLBP)
back schoolsacute stage, 80group education vs. individual education, 80–81patient education, 81
comprehensive rehabilitationCBT, 82exercise treatment, 81–82multimodal multidisciplinary, 81
natural evolution (see also Conservative treatment)absence of work and sick listing, 68–69acute and subacute, 66–67chronic, 67–68database, 65–66definition, 65methodological variations, 70
NuBac disc arthroplasty systemclinical results, 253–254design rationale, 250device model, 249

Index 283
expulsion and subsidence, 252–253in vitro cadaveric model, 253material choice, 250–252multidirectional flexibility testing, 254ODI scores, 255VAS scores, 255
Nucleus pulposus (NP), 12
OObesity, 178ODI. See Oswestry disability index scoresOsteoporosis, 178Oswestry disability index (ODI) scores, 195, 255
PPain behaviours, 24–25Pain beliefs, 24Pain coping strategies, 24Pain sources and factors
facet joints, 12intervertebral discs, 11–12ligaments, 13muscles, 13nervous system involvement and adaptation, 13–14psychosocial aspects, chronic pain, 14vertebraes, 13
Pathophysiology, 267–268Patient encounter
clinical assessments and encounterparts, 88–89measurements and types, 88, 89
Patient-physician interaction-related factors, prescribe, 75–76Patient-related factors, prescribe, 74–75PDS. See Posterior dynamic stabilizationPedicle-based dynamic stabilization systems
accuflex device, 223adjacent segment degeneration, 221cord-type systems, 222curved and spiral designs, 222–223history, 221–222indications, 224jointed rods, 223semirigid/flexible rods, 222Stabilimax NZ, 223–224and total disc replacement, combined, 224total facet joint replacement, 223
Pedicle screwsdeformity, 123degenerative, 123–124history, 123trauma, 123
Pelvic girdle pain (PGP)causes and diagnosis, 165Hoffman–Slätis fixator, 167materials, 165method, 166
Percutaneous intradiscal radio-frequency thermocoagulation (PIRFT)
vs. IDET, 99radiofrequency probe, 98randomized controlled trial (RCT), 98
Peripheral stimulation, nerve terminals, 66
PGP. See Pelvic girdle painPhysician extender role
allied healthcare professionalscertified athletic trainers, 58–59nursing, 57–58physician assistants, 58physiotherapists, 58
clinical tasks, 60hospital tasks
clinics and triage, 60hospital medical records, 59–60surgical procedures, assistance, 60
office tasksfollow-up visits, 59history and physical examination, 59
PIRFT. See Percutaneous intradiscal radio-frequency thermocoagulation
PLF. See Posterolateral fusionPostdiscectomy syndrome, 115, 116Posterior dynamic stabilization (PDS)
development principles, 211Dynarod PDS system, 209facet loading, 210FE-models, 208hypotheses, 207implanted model formulation, 208–209interpedicle displacement, 210intradiscal pressure, 211L4–L5 FE-model, 208L1-S1 FE-model, 208objectives, 207range of motion (ROM), 209, 210topping off fusion, 209–211
Posteriorlongitudinal ligament (PLL). See LigamentsPosterolateral fusion (PLF), 270Posttraumatic instability, 111–113Potomac device, 222Prescribing conservative treatment. See Conservative treatmentPrescription process of, 73Psychosocial aspects
beliefs, 24chronic pain, 14coping, 24distress and depression, 23–24pain behaviours, 24–25patient–physician relationship, 25social factors
compensation status, 25job characteristics, 26job satisfaction, 25patient self-reports, 25
QQuality adjusted life-years (QALYs), 259, 263
RRadicular pain
lumbar spinal stenosis and degenerative spondylolisthesis, 157
synovial cysts, 158Randomized controlled clinical trials (RCTs)

284 Index
conservative treatment, 98PIRFT, 98spinal manipulation, 91
Range of motion (ROM), 187
SScrew loosening/breakage. See Nonrigid stabilizationScrew-only fixation, 151Segmental instability
clinical and biomechanical stages, 29–30EMG
behaviour, 35–36recording, 35
flexion-extension movement, 35IMD
in humans, 34–35total flexion-extension motion, 33
intervertebral joint dynamic loading, in vivominiaturized servo-hydraulic testing apparatus, 31stiffness, 32
kinematics ofexperimental clinical study, 35IMD, 32
pattern of motion, 33–34clinically suspected segment, 34experimental injuries, 33–34
and radiographytraction-compression and flexion-extension, 30–31vertebral, indicators of, 30
results, 36Semirigid fixation system
demographic and basic clinical data, 228dynamic neutralization system, 227Dynesys decompression, 228pain levels and global outcome, 229patients, 227–228preoperative evaluation, 228
SF-6D vs. EQ-5Ddimensions and number of levels, 262economic evaluation, 259–260low back pain vs. cancer, 264–265pair-wise observations, 263preference-based measures, 260–261regression-adjusted limits, 264statistics and intraclass correlation, 263
Social factor evaluationcompensation status, 25job characteristics, 26job satisfaction, 25patient self-reports, 25
Societal-related factors, prescribe, 76–77Spinal fusion
evaluation, 271–272index surgery, 159Kaplan Meier survival analysis, 161lumbar fusion, 160patient selection, 271PLF with VSP, 270
Spinal manipulationchiropractic treatment, 91
mobilization and manipulation, 90stiffness assessment, 90therapeutic effect, 89
clinical outcomes, 91–92acute LBP, 91chronic LBP, 91–92RCTs, 91
mechanisms, 90–91Spinal stenosis, 113Spine patient outcomes research trial (SPORT), 274–276Spine surgery, 19–20. See also Degenerative spine
complications, 273–274level one evidences, 268–269systemic and local methods, 170types, 169
Spondylarthritis. See Facet jointsSpondylolisthesis
clinical presentation, 141definition, 140investigations, 142Marchetti–Bartolozzi etiologic classification, 140, 141radiographic measurements, 142treatment, 142–144Wiltse anatomic classification, 140, 141
Spondylolysis, 110–111clinical presentation, 137–138conservative treatment, 139definition, 137investigations, 138–139surgical treatment, 139–140
SPORT. See Spine patient outcomes research trialStabilimax NZ, 223–224Synovial cysts, 158
TTIMPs. See Tissue inhibitors of metalloproteinasesTissue inhibitors of metalloproteinases (TIMPs), 8Topping off syndrome. See Adjacent level diseaseTotal disc arthroplasty, 272–273Total disc replacements (TDRs)
biomechanical testing, 194–195Charité, 195–196disc space height, 196Kineflex, 194–196Oswestry scores, 195patient selection criteria, 193–194range of motion, 196VAS, 195
Total facet joint replacement, 223TPDC-fixation. See Transpedicular-transdiscal-transcorporal
fixationTransexamic acid (TXA), 171Transfusion related acute lung injury (TRALI), 169Transitional anomalies, 115, 117Transpedicular-transdiscal-transcorporal (TPDC)-fixation
delta fixation, 151, 152K-wire, 147limitations, 153pedicle screws, 147, 148screw-only fixation, 151

Index 285
Treatment-related factors, prescribe, 73–74Two lumbar total disc replacements. See Total disc
replacements (TDRs)
VVariable screw placement (VSP), 270VAS. See Visual analog scoreVascularization and innervation, 7Vertebraes, 13
Visual analog score (VAS), 195, 255VSP. See Variable screw placement
WWiltse anatomic classification, spondylolisthesis, 140, 141
XX-stop interspinous process distraction system, 242

















