24
Patient Safety Priorities 2016/17 Surgical Division

Patient Safety Priorities 2016/17 Surgical Division
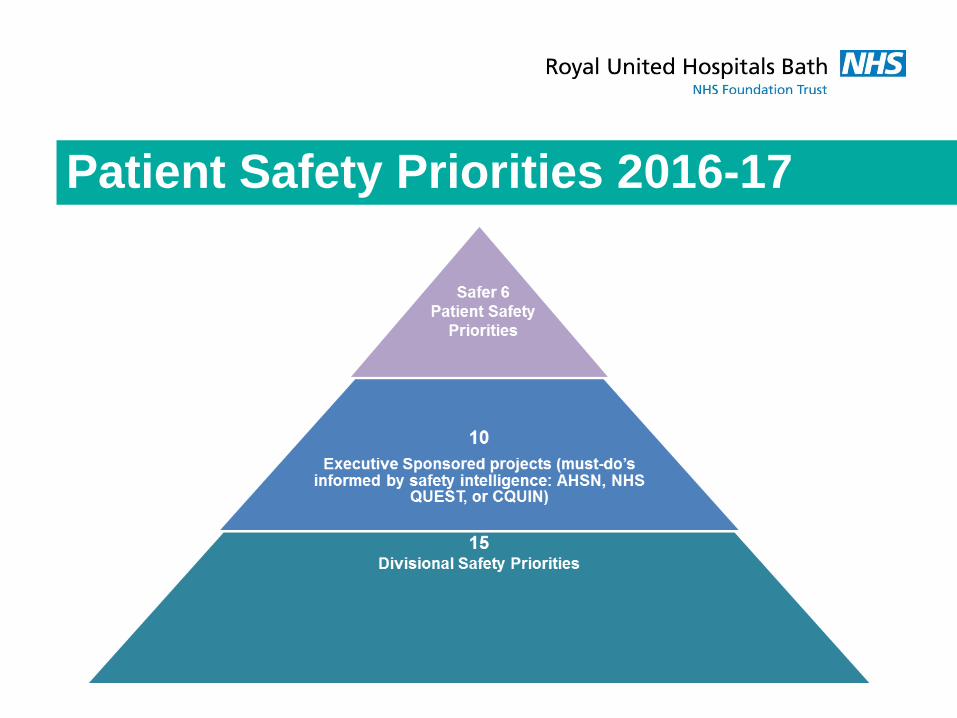
Acute Kidney Injury
(AKI), NEWS, Sepsis, Clostridium difficile (inc
AMR), Movement of patients location,
Improving Insulin safety,
Medicine Safer nurse staffing
Stroke (SSNAP) Ambulatory Care
Patients with a LOS >20 days
Women & Children’s Glucose Tolerance Testing
Stillbirth Jaundice Management
Paediatric “safe” programme Learning from incidents
Patient Safety Priorities 2016-17
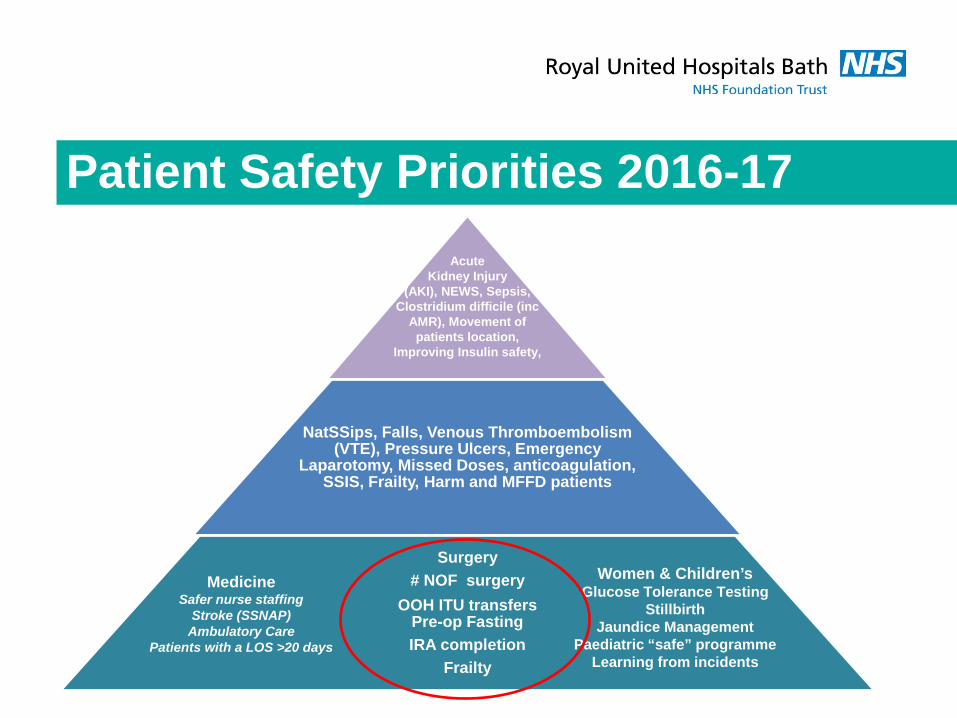
NatSSips, Falls, Venous Thromboembolism (VTE), Pressure Ulcers, Emergency
Laparotomy, Missed Doses, anticoagulation, SSIS, Frailty, Harm and MFFD patients
Surgery # NOF surgery
OOH ITU transfers Pre-op Fasting IRA completion
Frailty
Acute Kidney Injury
(AKI), NEWS, Sepsis, Clostridium difficile (inc
AMR), Movement of patients location,
Improving Insulin safety,
Medicine Safer nurse staffing
Stroke (SSNAP) Ambulatory Care
Patients with a LOS >20 days
Women & Children’s Glucose Tolerance Testing
Stillbirth Jaundice Management
Paediatric “safe” programme Learning from incidents
Patient Safety Priorities 2016-17
Fractured neck of femur Hip fracture carries a mortality of 30-35% Early surgery (within 48hrs)
Reduces pain, duration of immobility, pressure ulcers
Reduces morbidity and mortality Reduces LOS Increased return to independent living
BPT introduced 2011 Surgery within 36hr Joint care ortho/geriatrician. MDT input. Prevention (falls/bone health)
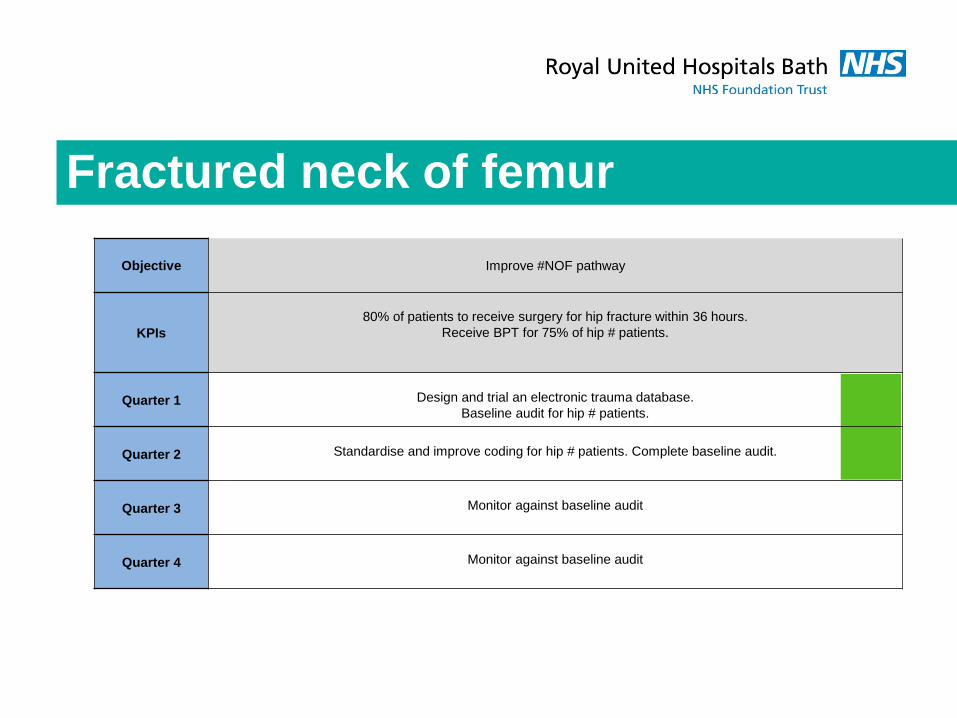
Fractured neck of femur Objective Improve #NOF pathway
KPIs
80% of patients to receive surgery for hip fracture within 36 hours.
Receive BPT for 75% of hip # patients.
Quarter 1
Design and trial an electronic trauma database. Baseline audit for hip # patients.
Quarter 2
Standardise and improve coding for hip # patients. Complete baseline audit.
Quarter 3
Monitor against baseline audit
Quarter 4
Monitor against baseline audit
Fractured neck of femur Database designed, implementation delayed
(FirstNet). Paper based system in place Audit completed
No further delays for NOAC Capacity issues
Ongoing monthly review of patients not achieving 36hr target to identify further learning
Coding reviewed. Recording of osteoporotic fractures agreed with NHSE. Ongoing review of coding

Baseline
OOH ITU discharges OOH ITU discharge is any transfer between
2200 and 0700 ICNARC data shows OOH transfers significantly
increase both morbidity and mortality

OOH ITU discharges
Objective Eliminate overnight transfer out of ITU
KPIs Eliminate OOH ITU transfers
Quarter 1 Baseline audit of current practice Identify themes and devise an action plan
Quarter 2 Formation of a task & finish group with key stakeholders
Quarter 3 Improvements from baseline
Quarter 4 Improvements from baseline
OOH ITU discharges Part of larger project CQUIN group chaired by Claire Damen
Increased staff awareness Work with site team to achieve daytime transfers Datix all OOH discharges Analysis of all OOH discharges Monthly monitoring and reporting
Apr May Jun Jul Aug Sept OOH discharges 10 3 6 3 5 (4) 6 (3) Datix reports 3 3 5 1 3 3
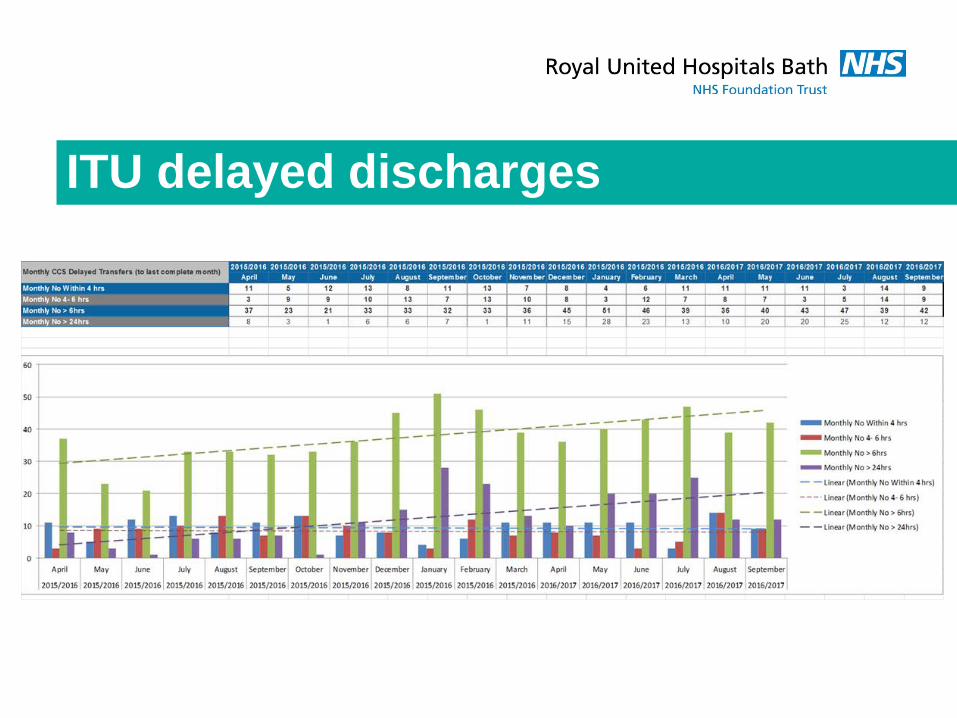
ITU delayed discharges
Pre-operative fasting Fasting is utilised to prevent pulmonary
aspiration of stomach contents during induction of anaesthesia
Incidence is 1:10000, predominantly emergency cases, causing serious morbidity and death
Prolonged fasting causes harm Dehydration Hypovolaemia Hypoglycaemia Delayed recovery from anaesthesia → Poor clinical outcomes

Pre-operative fasting
Objective Minimise pre-op fasting (non-elective)
KPIs Reduction in pre-op fasting time
Quarter 1 Maximise theatre 1 efficiency Baseline audit of unnecessary fasting
Quarter 2 Launch 12 hour stop
Quarter 3 Action planning
Quarter 4 Monitor fasting times

Theatre 1 scheduling 8am SAU MDT
meeting Triage of cases Traffic light system,
12 hour stop
4pm meeting

Wait times for theatre 1
Category A (within 1 hour) Category D (elective)
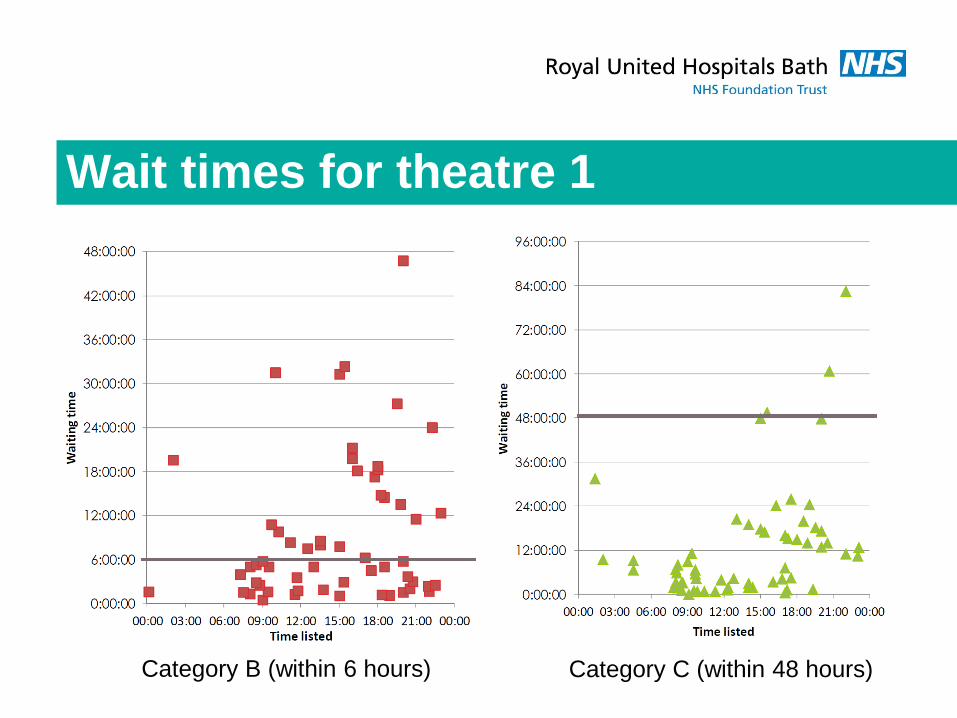
Wait times for theatre 1
Category B (within 6 hours)
Category C (within 48 hours)
IRA completion Up to 10% inpatients experience a safety-related
incident Approx 50% of these are preventable Risk assessment on admission identifies
vulnerable patients allowing steps to be taken to reduce risk
IRA completion
Objective Timely IRA completion
KPIs 95% completion of initial risk assessments (IRA) on all surgical wards
Quarter 1 Baseline Audit of current practice.
Identify barriers preventing timely completion and devise action plan
Quarter 2 Re-launch IRA standard
Quarter 3 Demonstrate improvement from Q2
Quarter 4 Demonstrate improvement from Q3

IRA completion Baseline audit complete Barriers/problems identified Relaunch planned for November
Meeting with Surg Sisters/wards Inclusion in handover Monitoring tools Review pre-assessment pathway

Frailty recognition Frail patients have little physiological reserve
and decompensate rapidly in hospital Increased complications Delayed recovery Prolonged LOS Limited recovery of pre-morbid state
Early recognition and specialist MDT input mitigates this

Frailty
Objective Early identification of frailty in Surgical patients
KPIs 95% completion of the frailtiy assessment on admission
Quarter 1 Agree criteria and devise frailty assessment tool for surgical patients
Quarter 2 Launch new assessment tool and baseline measures
Quarter 3 Demonstrate improvement from Q2
Quarter 4 Demonstrate improvement from Q3
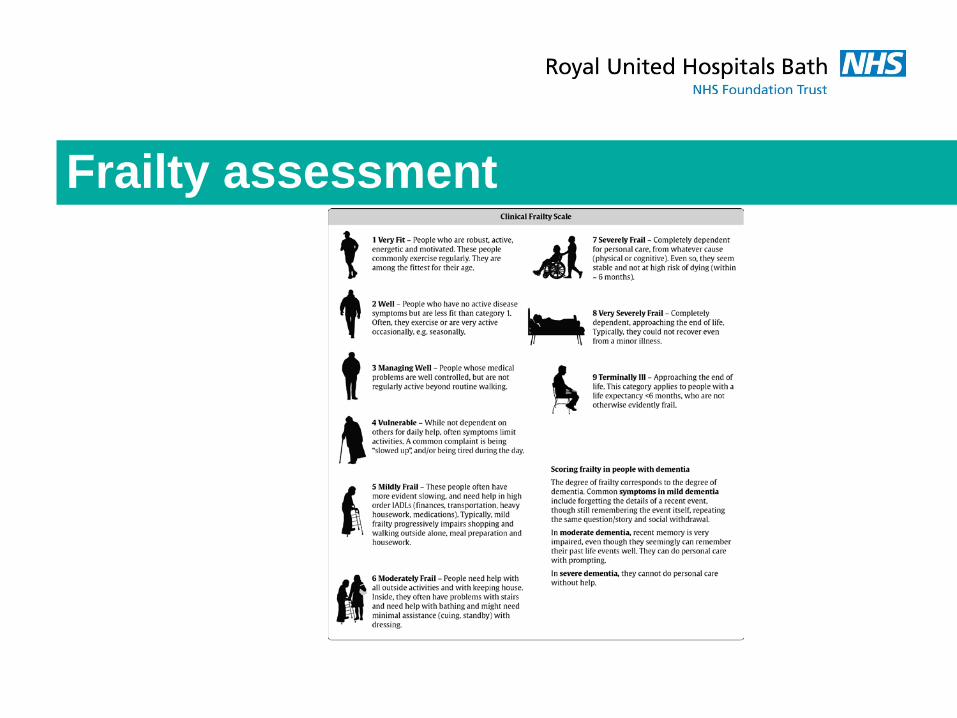
Frailty assessment

Frailty in laparotomy patients “Orthogeriatrics” success story Pilot of similar approach in elderly Gen Surgery
patients undergoing laparotomy QI project started May 2016, running to end
November 3 sessions/wk geriatician time Patients >70 yr eligible for NELA Data input behind schedule (no research nurse) Results early 2017

















![Fasting and Power [Draft]imranhosein.org/inhmedia/books/fasting&power-new.pdf · Fasting in Islam – its basic objective 21 Fasting and internal spiritual power 26 Religion and the](https://static.documents.pub/doc/80x56/5ed9610cf59b0f56f45f61bd/fasting-and-power-draft-amppower-newpdf-fasting-in-islam-a-its-basic-objective.jpg)