Page 1
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Steven J Morgan, MDMOTUS
Swedish Medical CenterDenver Colorado
Tibial Plateau Fractures Reduction Tips and Implant Selection
We have discovered: good judgement comes from experience and experience comes from BAD judgement
Surgical Timing ?
Page 2
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Surgical Timing ?
Special Equipment
C-Arm Radiolucent Table
Reduction ToolsPositioning Aids or Bumps
Page 3
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Redution ToolsFemoral Distracto or Ex Fix
Reduction ToolsTraction
Reduction ToolsClamps
Page 4
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Distraction and Clamp Combination
Reduction ToolsSpecialized Bone Tamps
Elevation of Depressed Segments
Open
Arthroscopic
Percutaneous C-Arm
Page 5
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Arthroscopic Reduction ToolsACL Guide
Elevate the depressed central fragment from below.
Page 6
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
ButtressPlate as a Reduction Tool
Surgical Exposures
Surgical Exposures
Anterolateral Exposure
Page 7
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Page 8
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Coronal FxPosteromedial Fragment
Sagittal Fx Separates Entire Medial Plateau
The Medial Plateau
Page 9
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Direct Posterior Approach
1 Galla and Lobenhoffer, Unfallchirurg 2003, 106:241-7. 2 Fakler et al., J. Orthop. Trauma 2007, 21:330-6.
Fakler et al., J. Orthop. Trauma 2007, 21:330-6.
Page 10
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
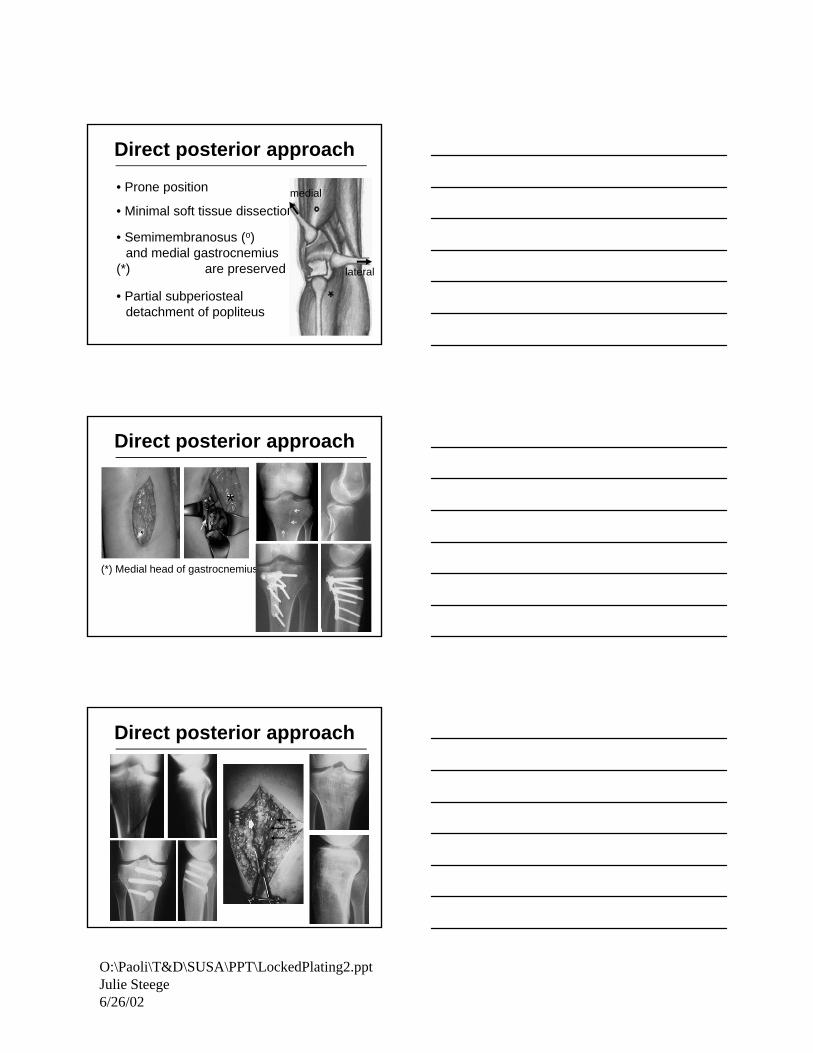
Direct posterior approach
• Prone position
• Semimembranosus (o) and medial gastrocnemius
(*) are preserved
• Minimal soft tissue dissection
lateral
medial
• Partial subperiosteal detachment of popliteus
Direct posterior approach
(*) Medial head of gastrocnemius
*
Direct posterior approach
Page 11
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Direct posterior approach
Arthroscopic Assisted Reduction
Tibial Plateau– Numerous reports
– Successful
– Specific patterns
Page 12
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
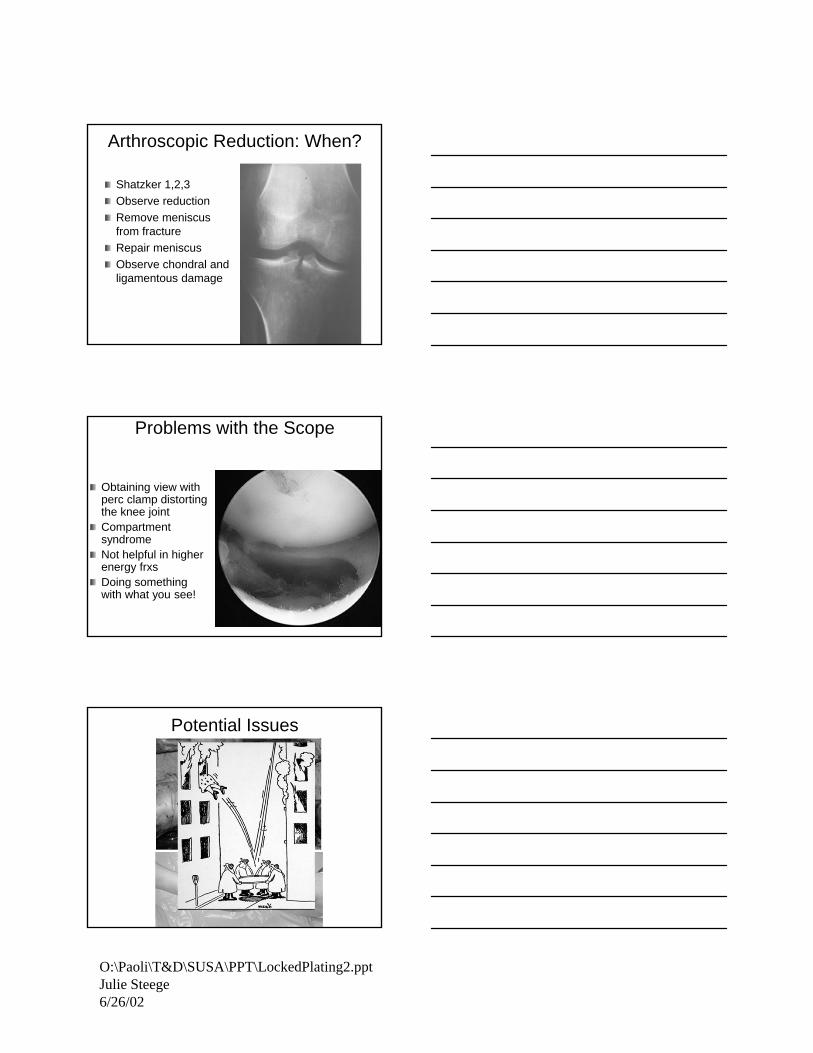
Arthroscopic Reduction: When?
Shatzker 1,2,3
Observe reduction
Remove meniscus from fracture
Repair meniscus
Observe chondral and ligamentous damage
Problems with the Scope
Obtaining view with perc clamp distorting the knee jointCompartment syndromeNot helpful in higher energy frxsDoing something with what you see!
Potential Issues
Page 13
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Flouroscopic Reduction
Allows multiplanar view
Familiar landmarks
Your hands are not required
We know what we are seeing (usually)
Problems with Flouro
Overestimating the reduction Don’t See The MeniscusDoing something with what you see!
Type 1 – Split Fractures
Techniques– Ligamentotaxis– Arthroscopy for Joint Reduction– Flouroscopy
Fixation– Screws
Large or Small
– Buttress Plates
–No Locked Plates
Page 14
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Type 1 – Split Fractures
Think Meniscus–Widely Displaced Splits–Widening of the Condyle–Incomplete Reduction
Type I
Type I
Page 15
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Split Fractures of the Lateral Plataeu– 3 x 6.5 mm cancellous screws
– 2 x 6.5 mm cancellous screws + 4.5 screw with washer as an antiglide
– 6 hole L buttress plate
– NO difference in stabilityKoval, J Orthop Trauma, 1996
Type II
Techniques– Ligamentotaxis For Split– Elevation for Depressed Segment ?– Arthroscopy for Joint Reduction– Flouroscopy / Percutaneous
Fixation– Screws
SmallRaft Screws
– Buttress Plates
–No Locked Plates
42 y.o male - closed injury
Split depression
Work through split
Bone graft or sub.
Page 16
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Meniscus !
Raft plate / periarticular plate
concept – not an implant!
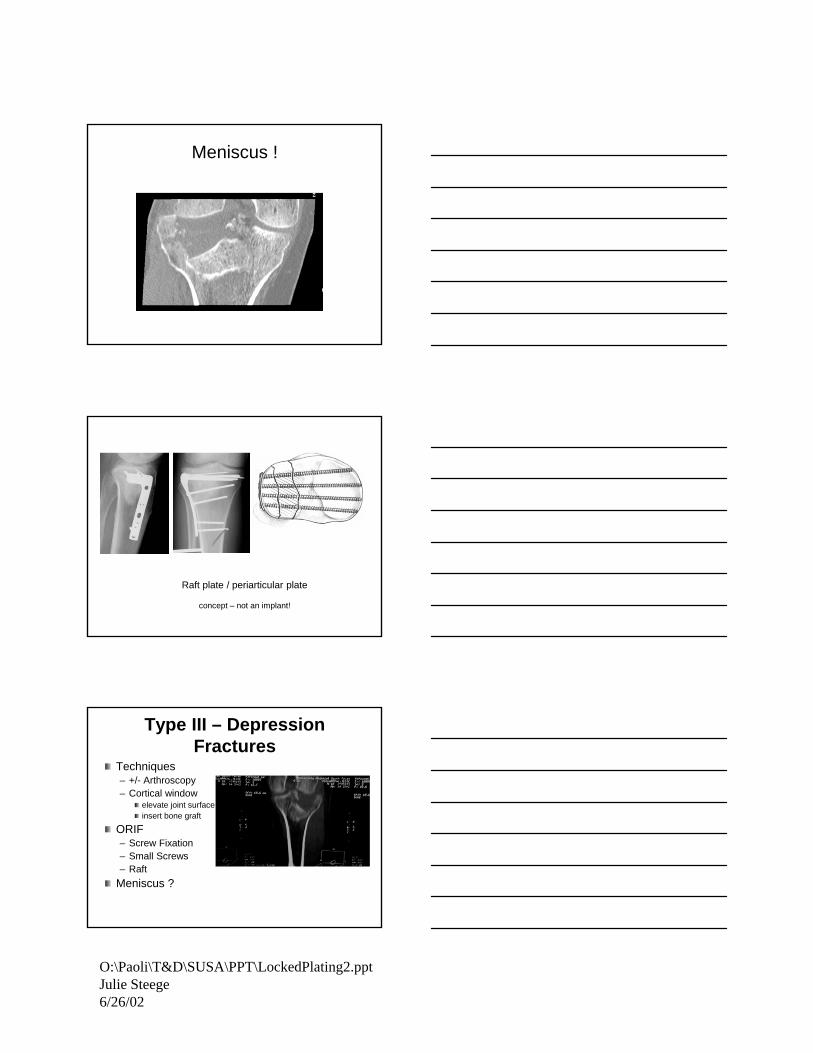
Type III – Depression Fractures
Techniques– +/- Arthroscopy– Cortical window
elevate joint surface insert bone graft
ORIF– Screw Fixation – Small Screws– Raft
Meniscus ?
Page 17
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Type III
Type III
Type III
Page 18
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Type IV – Medial Plateau Fx
High Energy– Neurovascular Injury– Ligamentous (LCL) (ACL)– Poor Soft Tussues– Compartment Syndrome
Techniques– Ligamentotaxis
Distractor/Fixator
– Post Medial Approach– Buttress plate – Avoid Varus
Will This Work ?
6 weeksImmediate post op 3 month
How Not To Do IT !
Lateral Locked Plate ?
Page 19
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Medial plateau
Low profile non-locked plate
Type V & VI Bicondylar Fractures
Techniques– Soft Tissue Assessment !!!
– +/- Temporary Bridging ExFix
– Must Support both sides With FixationTwo Plates
Lateral Locked Plate
– DO NOT approach through midline incision
– Two surgical approaches has less morbidity
High load to the implant !
Page 20
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
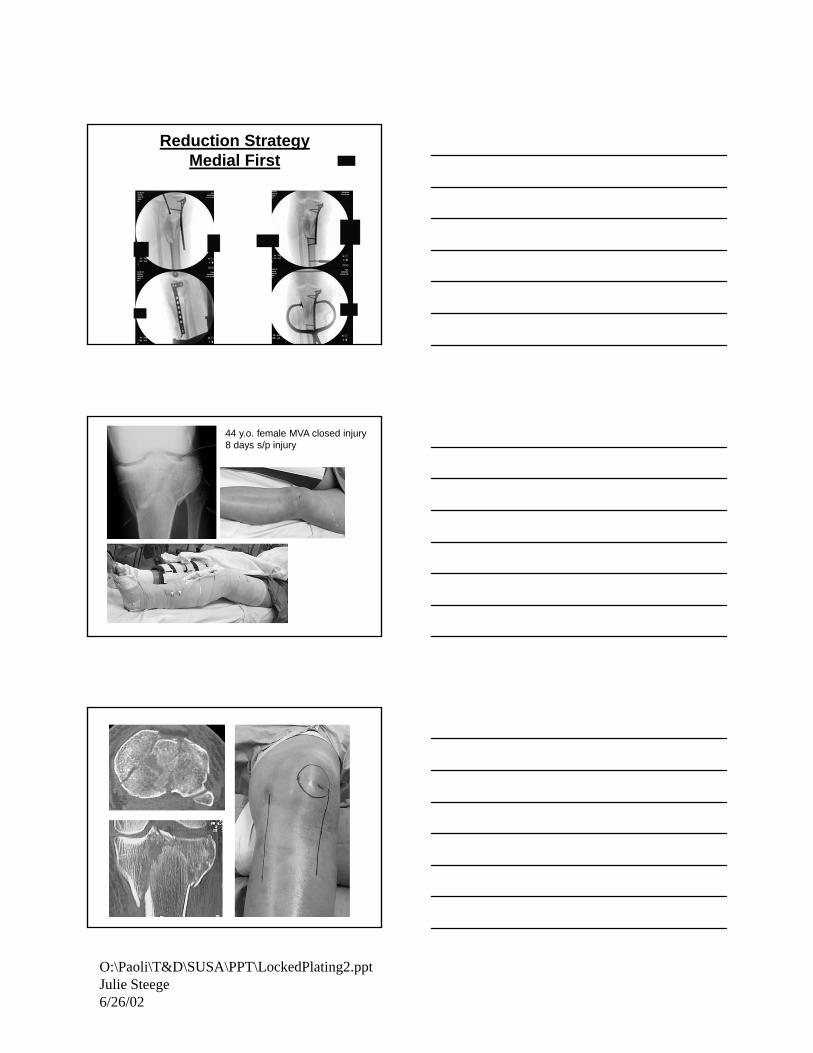
Reduction StrategyMedial First
44 y.o. female MVA closed injury8 days s/p injury
lateral side•correct flex/ext•reduce saggital split•buttress lateral side
Reduction strategy:
medial side first•close coronal split•buttress medial side
Page 21
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
3.5 mm LCDCP
Page 22
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
3.5 mm periarticular plate
No intervening stripping
Case Example
Page 23
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
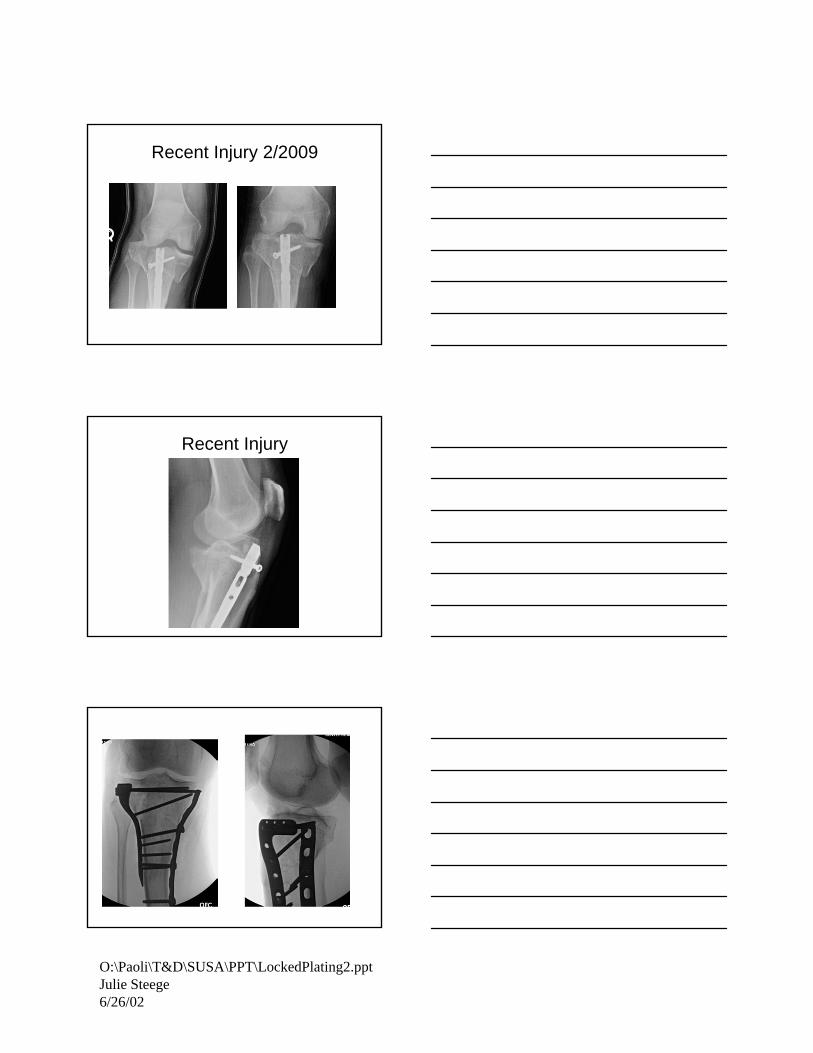
Recent Injury 2/2009
Recent Injury
Page 24
O:\Paoli\T&D\SUSA\PPT\LockedPlating2.pptJulie Steege6/26/02
Keep Trying To Improve
Gracias !