Surgical Treatment of the Low (Distal Third) Rectal Cancer Feza H. Remzi FACS, FASCRS, FTSS Feza H. Remzi FACS, FASCRS, FTSS ( Hon ) ( Hon ) Chairman Chairman Department of Colorectal Surgery Department of Colorectal Surgery Professor of Surgery Professor of Surgery Rupert B Turnbull Jr,. MD Chair Rupert B Turnbull Jr,. MD Chair Digestive Disease Institute Digestive Disease Institute Cleveland Clinic, Cleveland, OH Cleveland Clinic, Cleveland, OH
Transcript
Surgical Treatment of theLow (Distal Third) Rectal Cancer
Feza H. Remzi FACS, FASCRS, FTSS ( Hon )Feza H. Remzi FACS, FASCRS, FTSS ( Hon ) Chairman Chairman
Department of Colorectal SurgeryDepartment of Colorectal SurgeryProfessor of SurgeryProfessor of Surgery
Rupert B Turnbull Jr,. MD Chair Rupert B Turnbull Jr,. MD Chair Digestive Disease InstituteDigestive Disease Institute
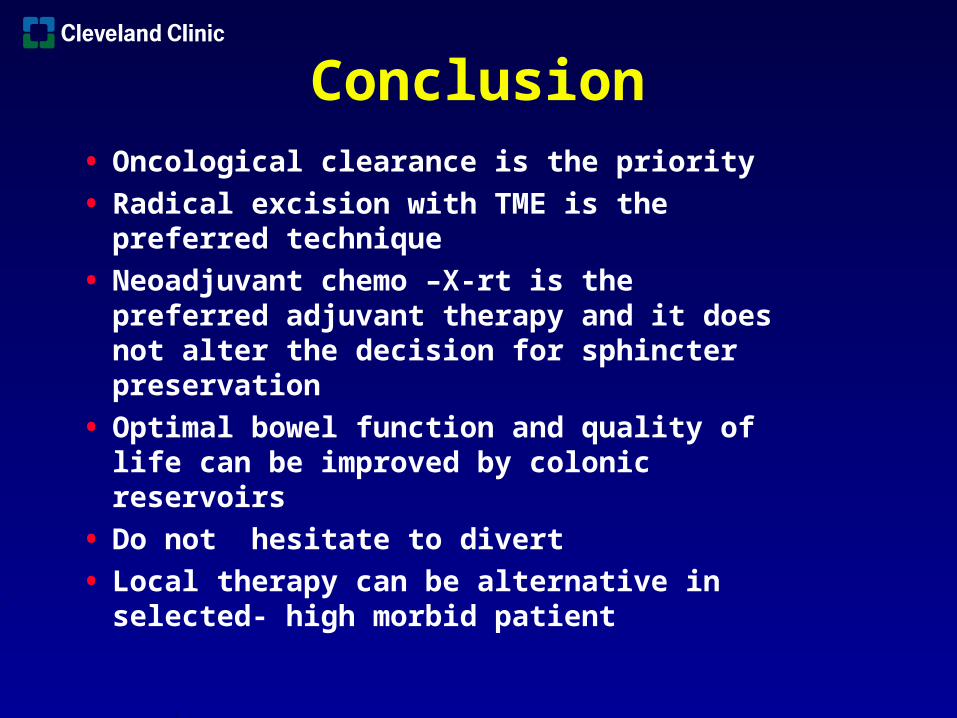
• Radical excision with TME is the preferred technique
• Neoadjuvant chemo –X-rt is the preferred adjuvant therapy and it does not alter the decision for sphincter preservation
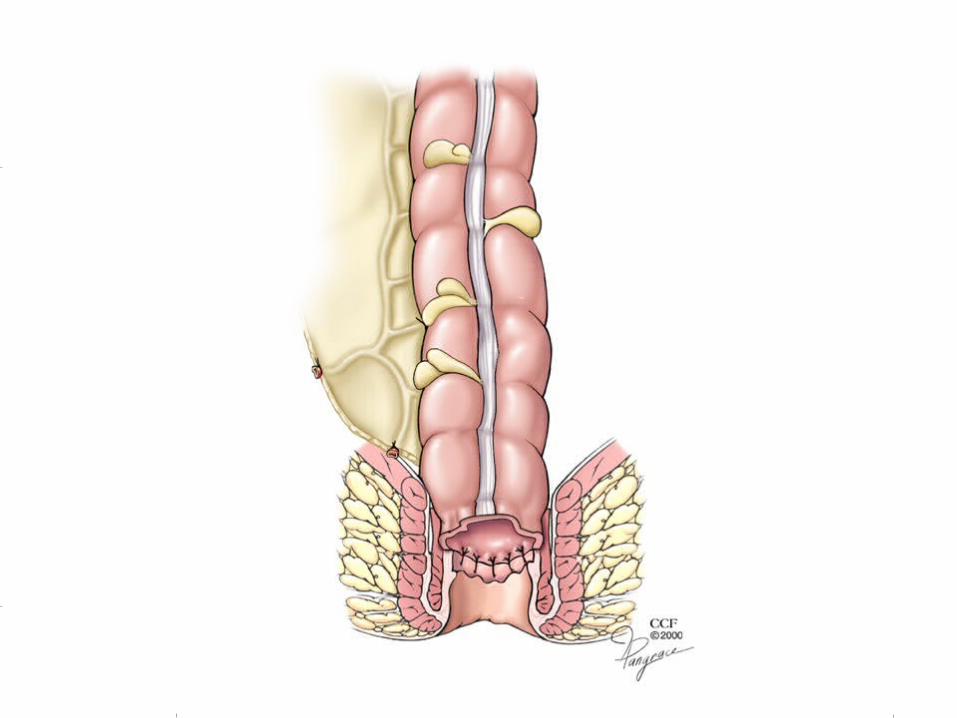
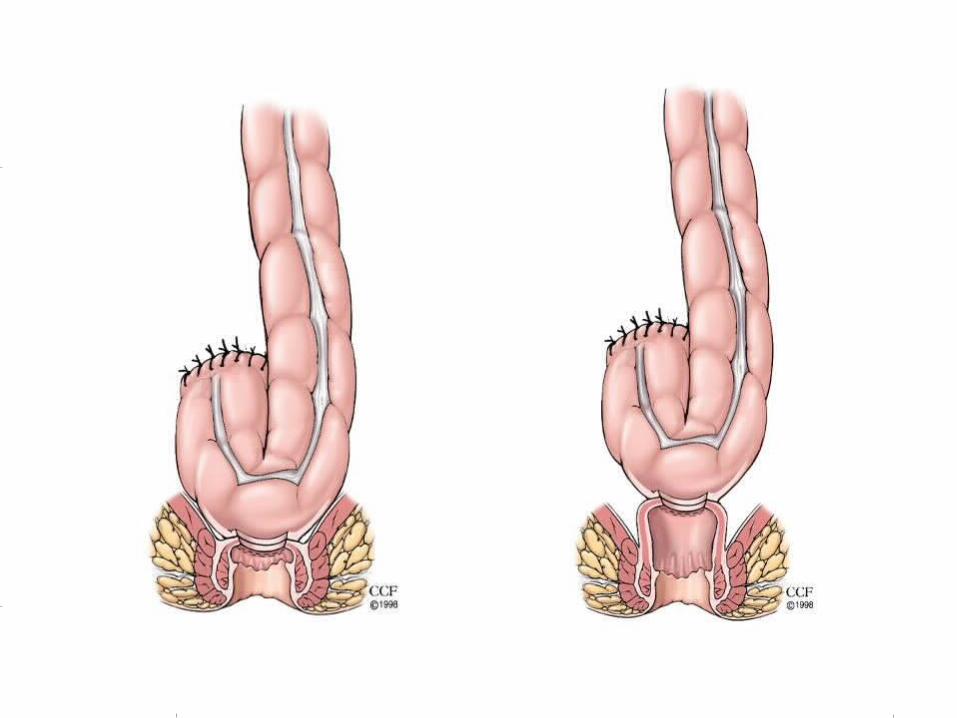
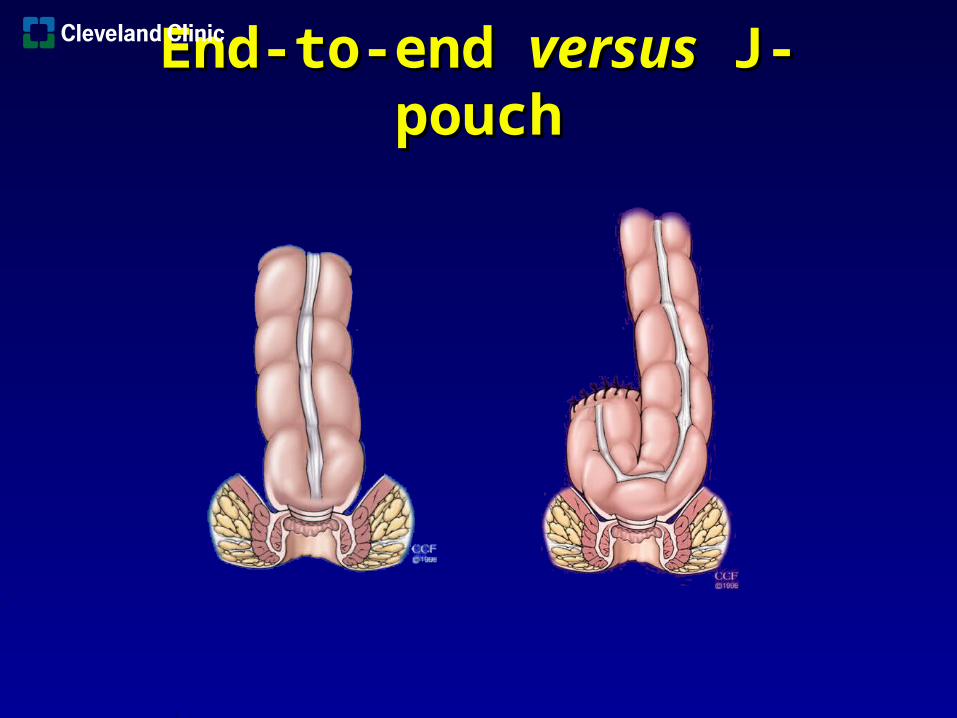
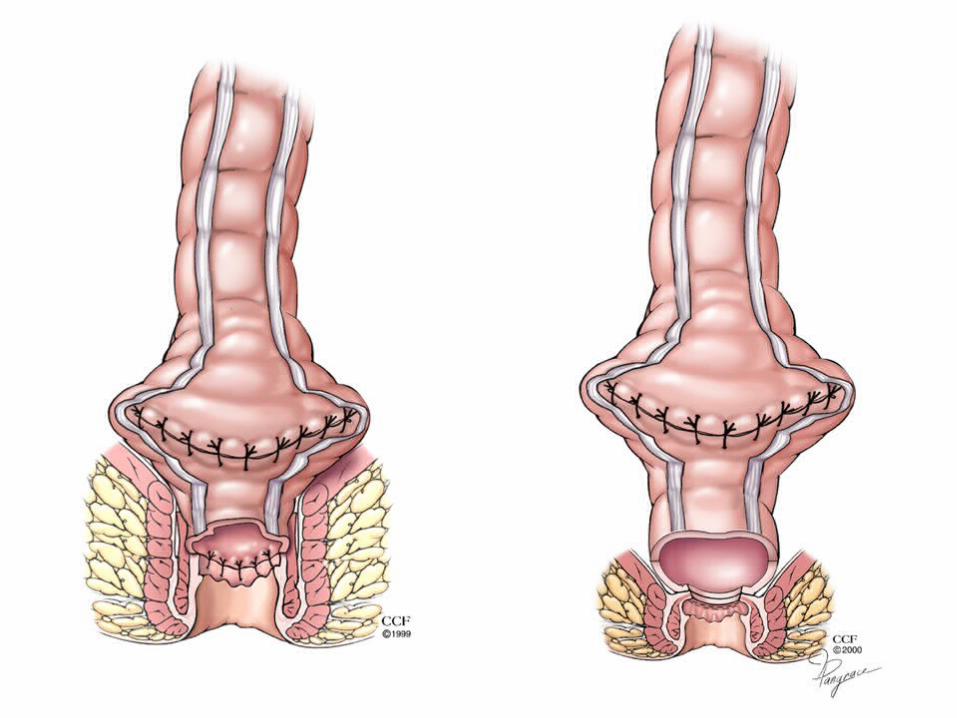
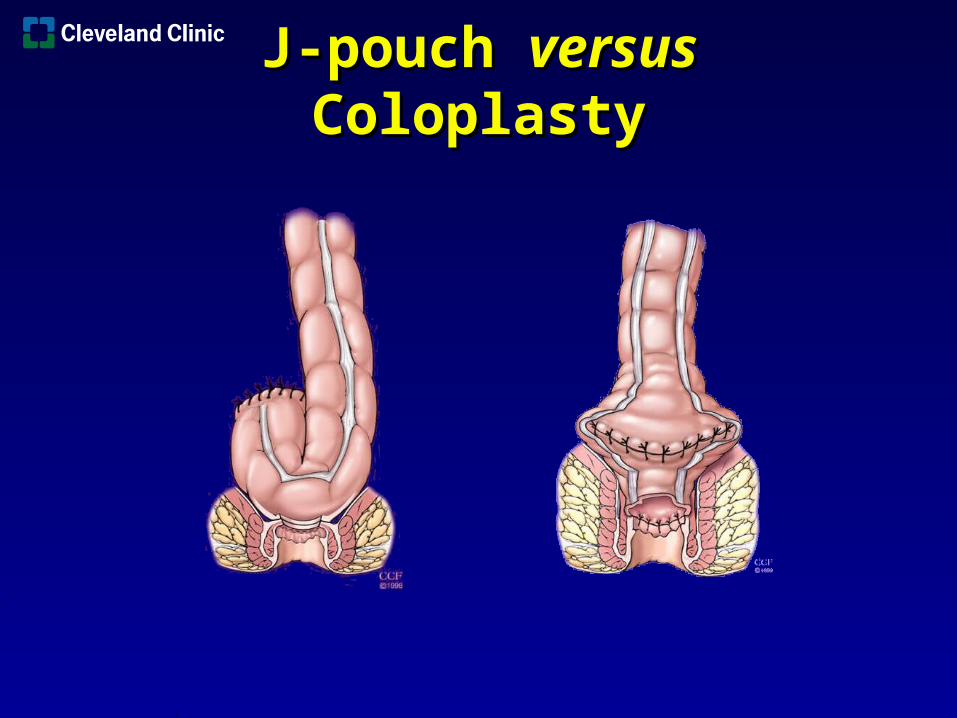
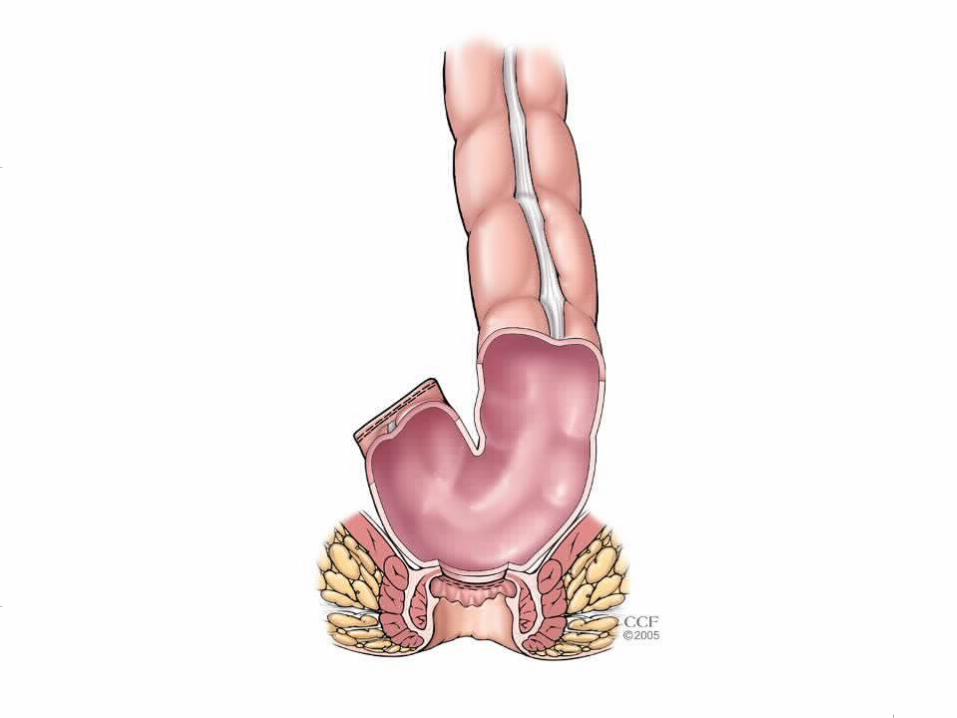
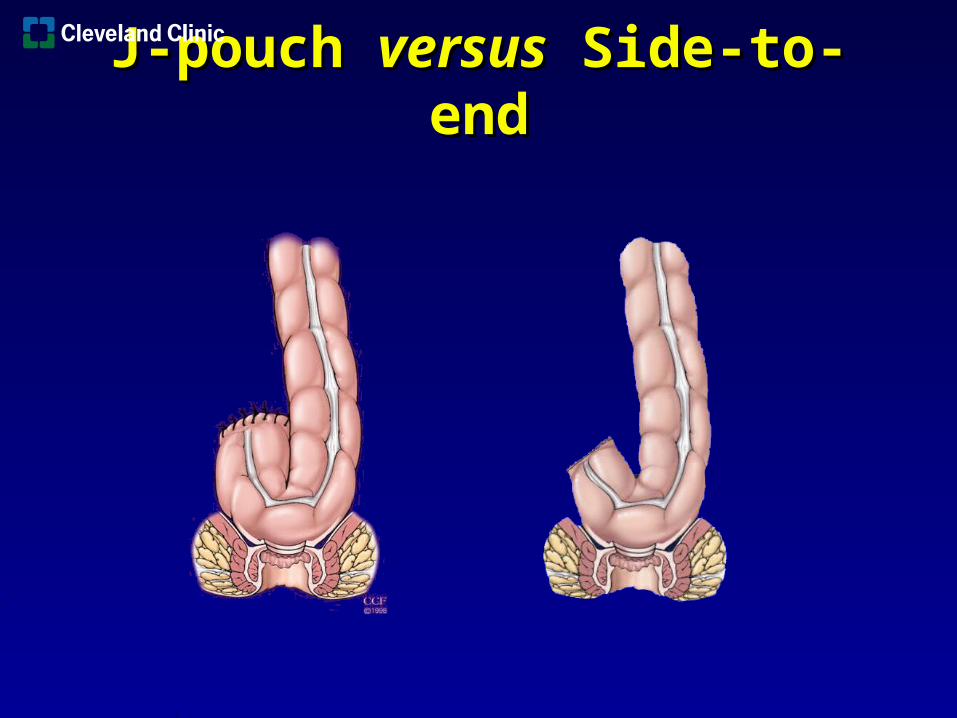
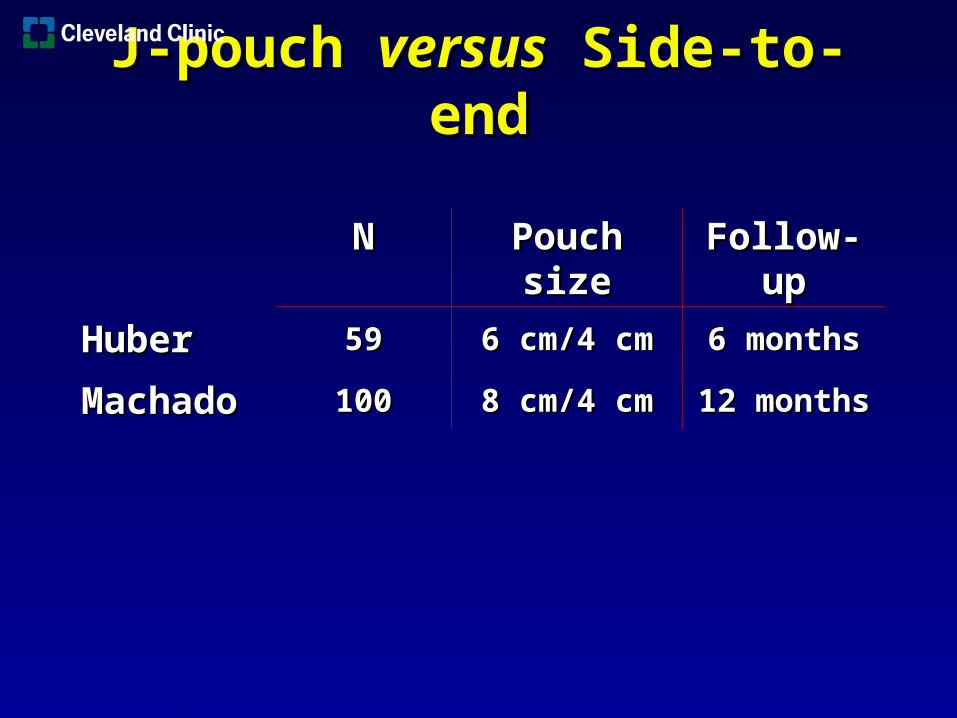
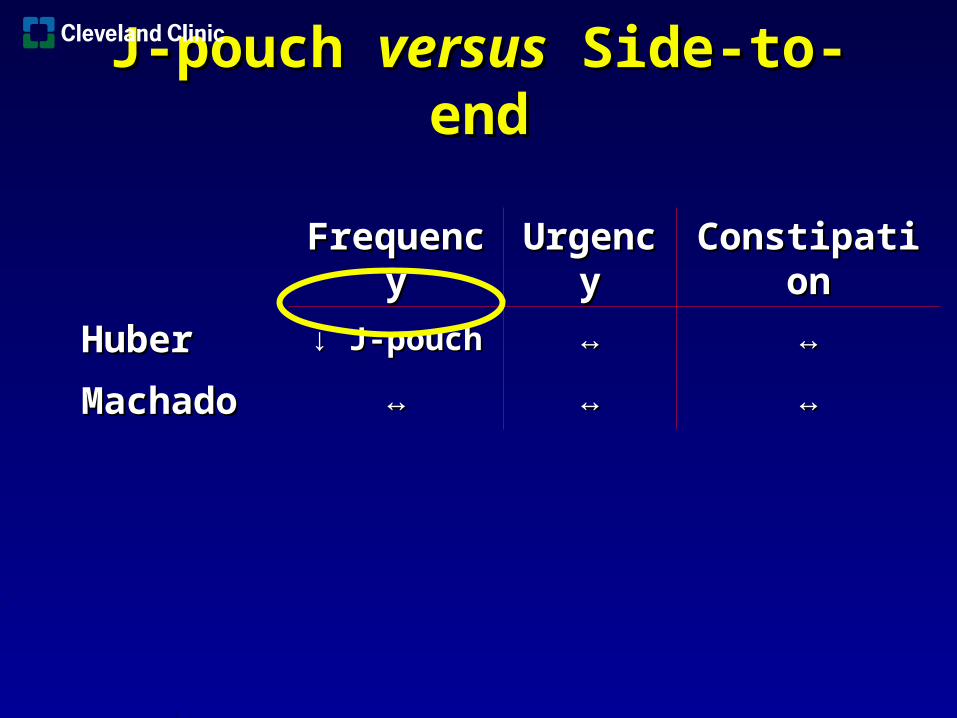
• Optimal bowel function and quality of life can be improved by colonic reservoirs
• Do not hesitate to divert
• Observation after neoadjuvant therapy can be dome under trial
• Local therapy can be alternative in selected- high morbid patient
• Maximize likelihood of cure
• Minimize risk of complications
• Sphincter preservation
• Optimal bowel function and quality of life
Treatment Goals
• Surgeon
• Radiologist
• Oncologist
• Radiation Therapist
• Enterostomal therapist
Team Approach
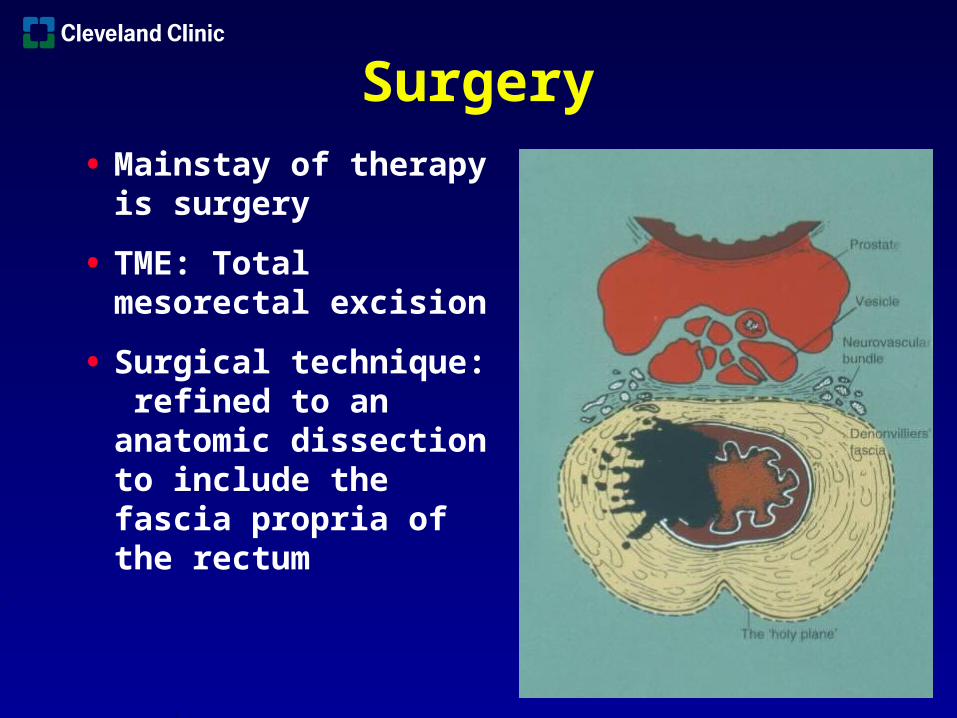
• Mainstay of therapy is surgery
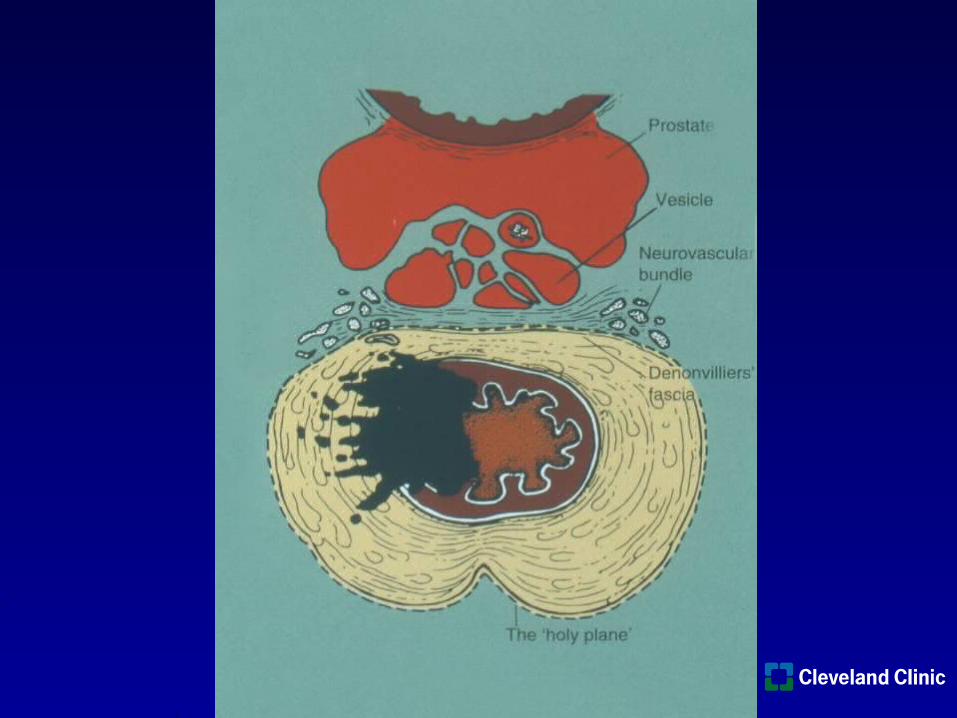
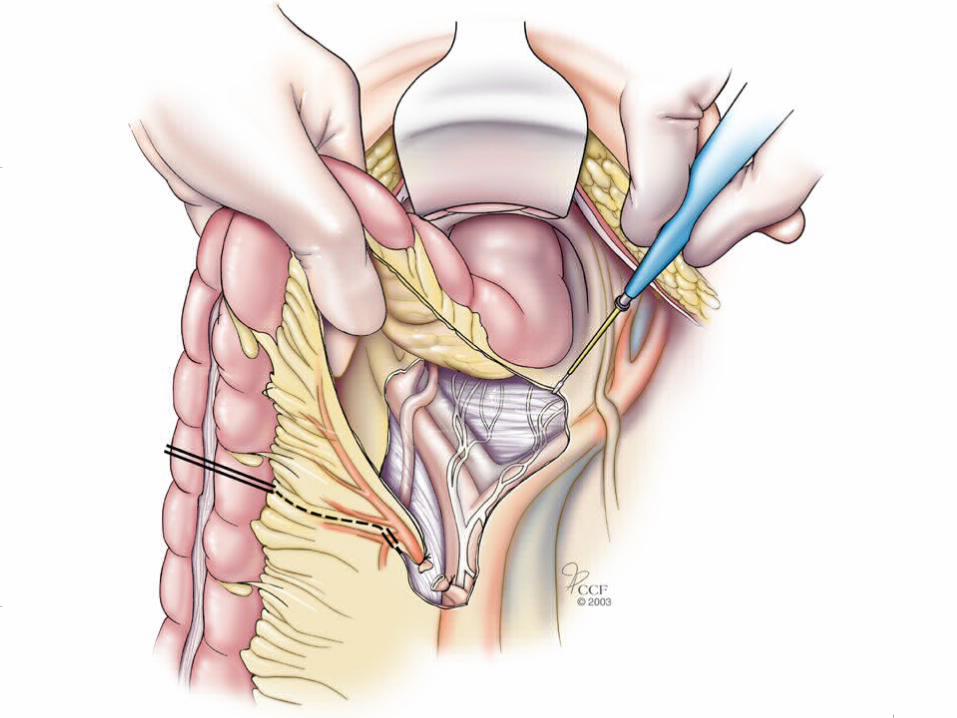
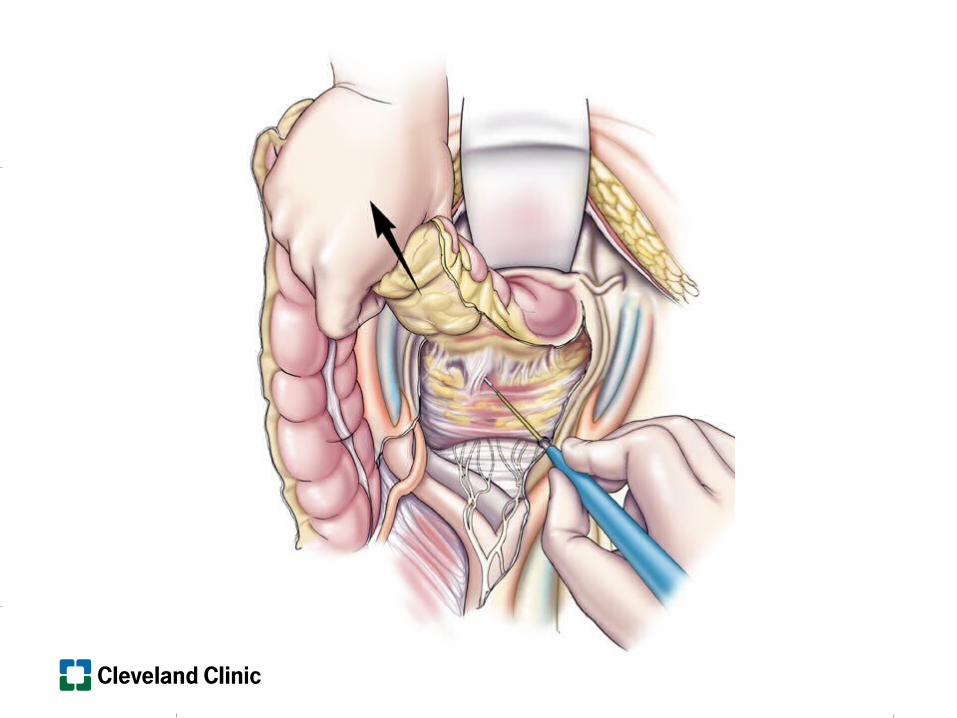
• TME: Total mesorectal excision
• Surgical technique: refined to an anatomic dissection to include the fascia propria of the rectum
Surgery
• Negative radial margins
• Distal margin�At least 5 cm of margin when there is a
distance of 5 cm distal resection
�At least 1 cm or more when there is no distance for 5 cm of distal dissection
Margin
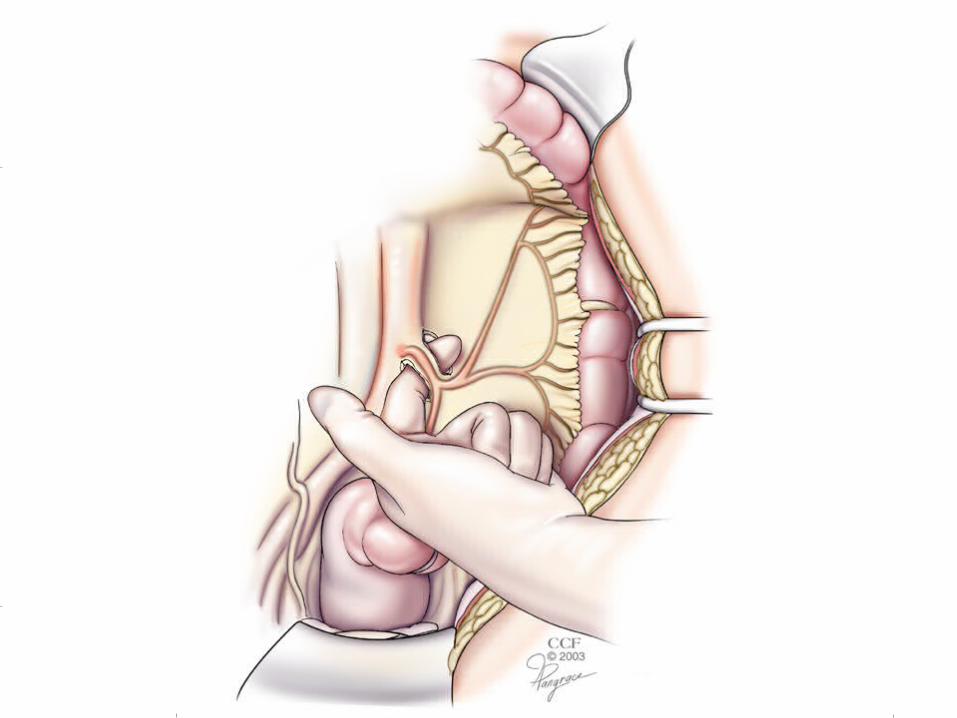
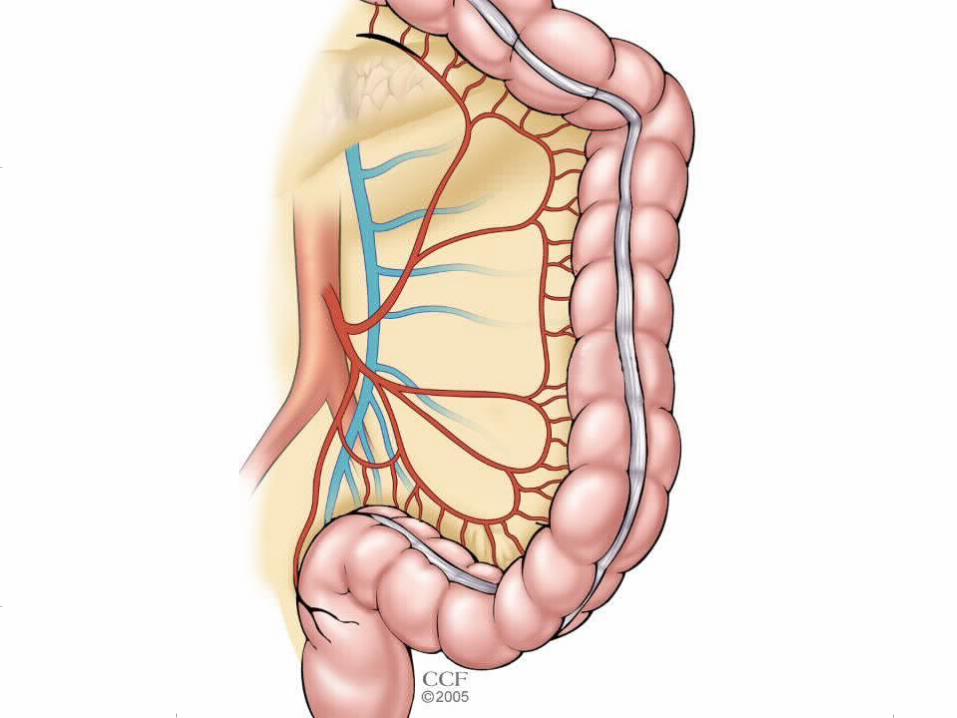
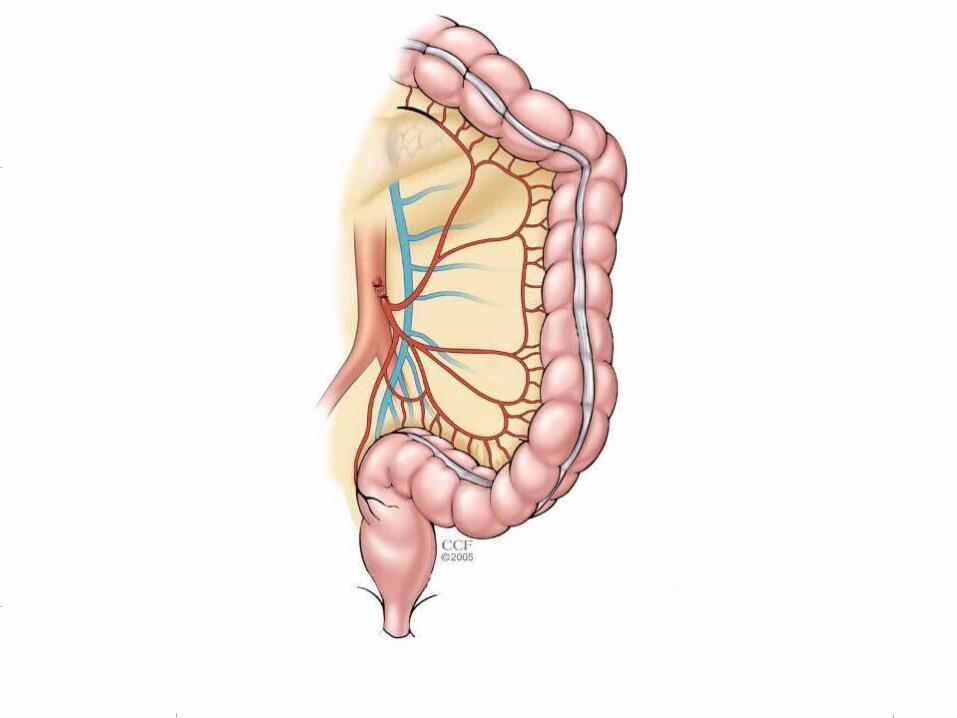
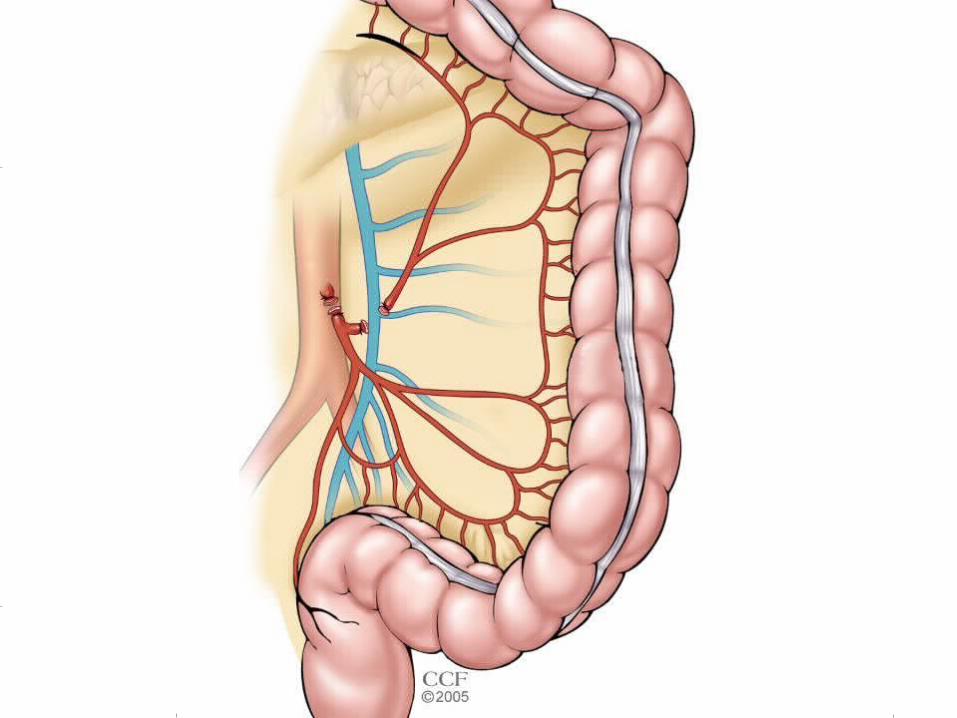
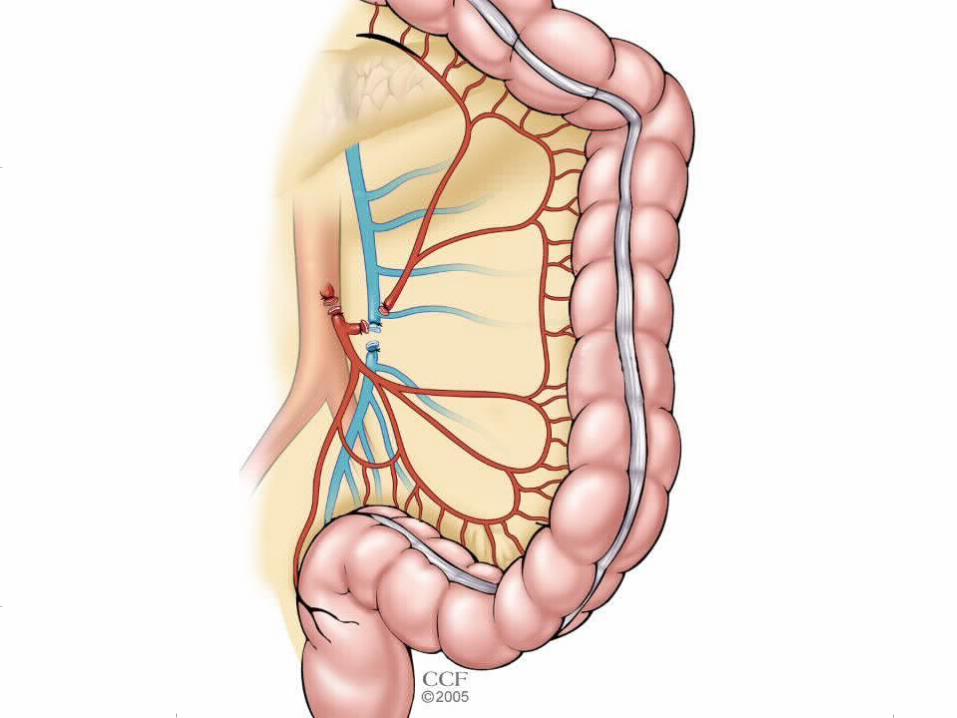
• Colon mobilization and high ligation of the mesenteric vessels
• TME
• APR versus reconnection with reconstruction
Surgery
TME
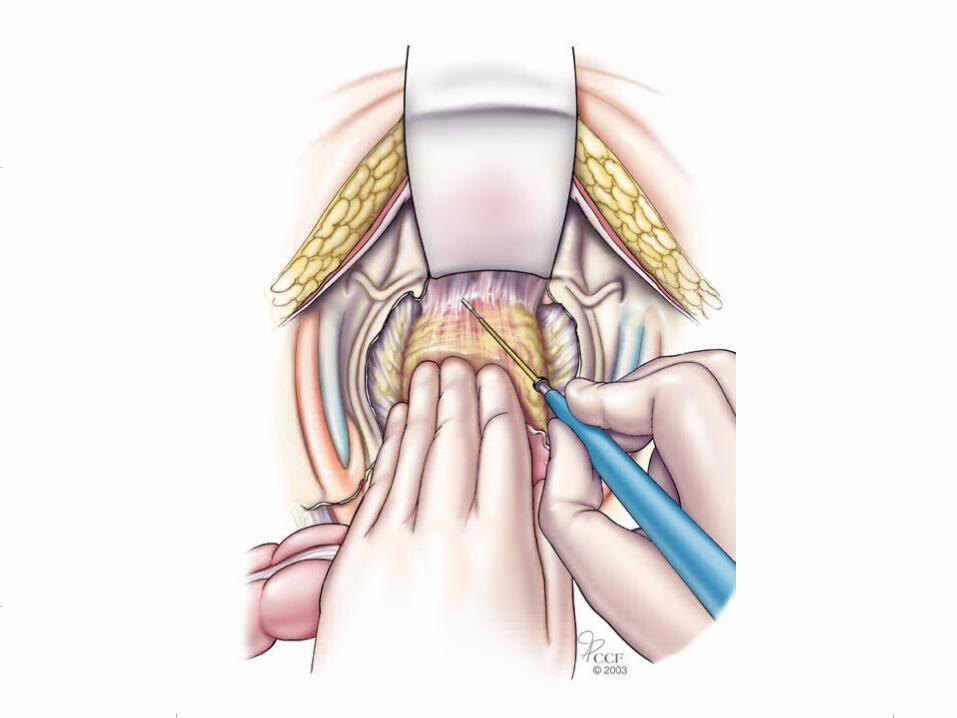
Anastomosis
Issues
• Blood Supply
• Reach
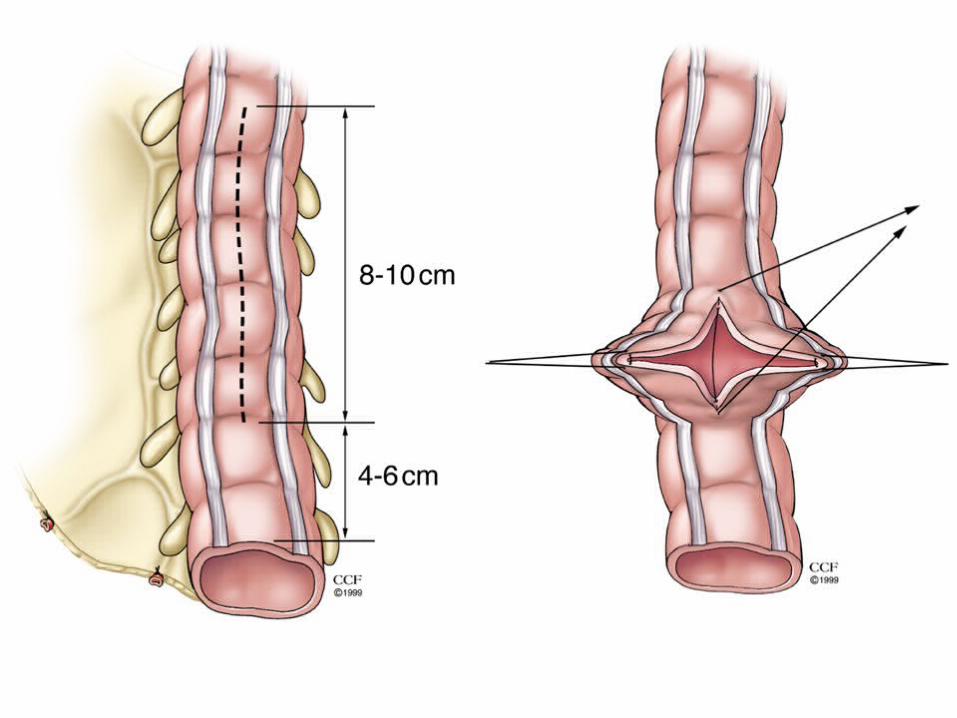
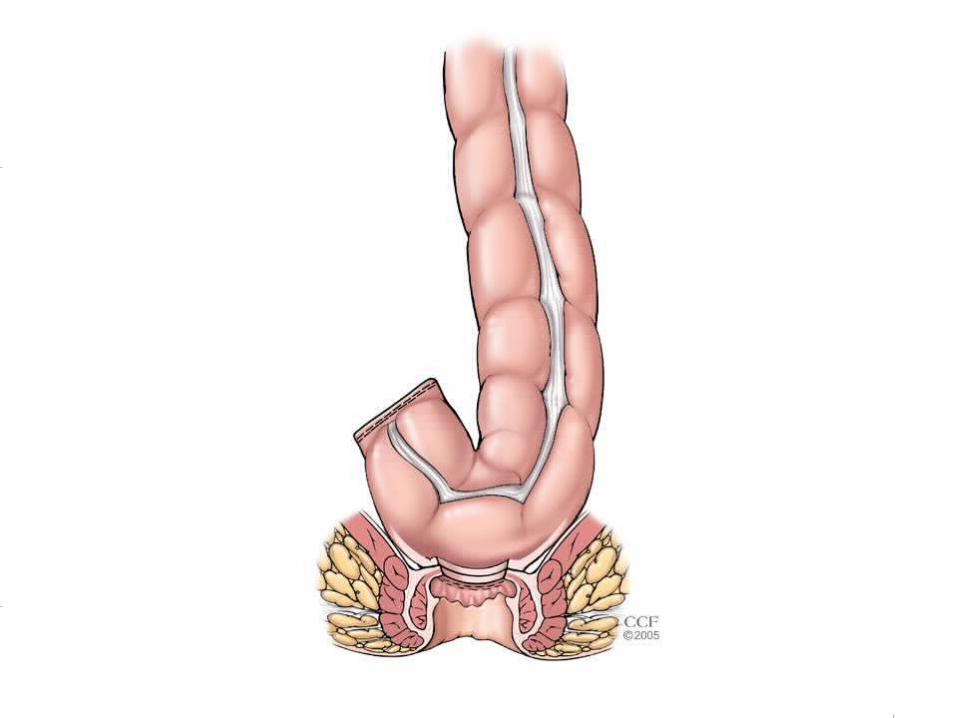
• Reconstruction
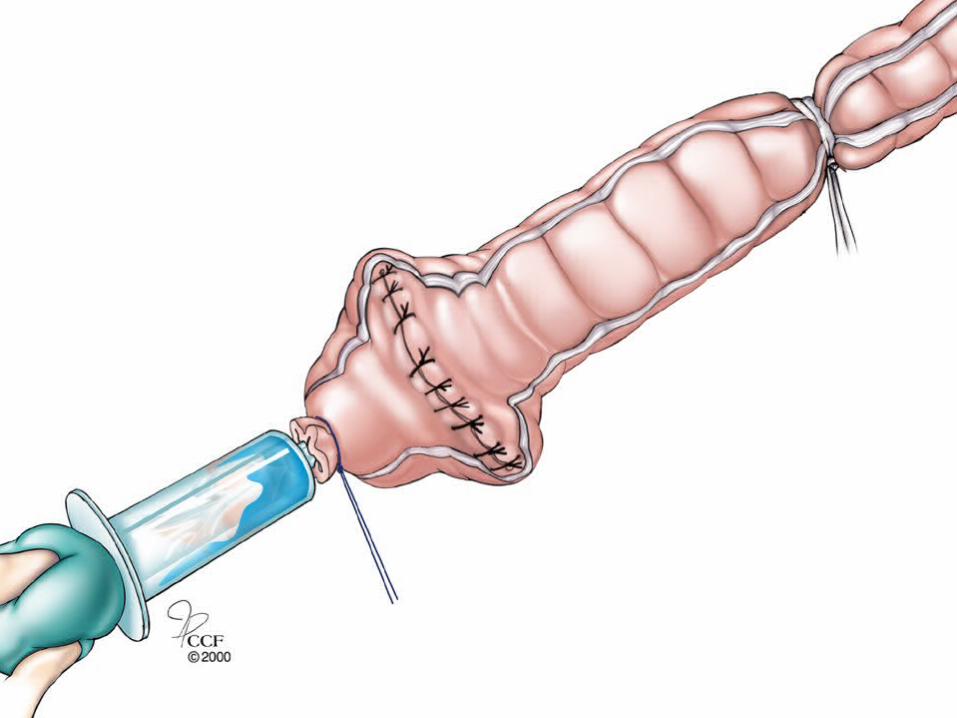
• Anastomosis
• Blood Supply
• Reach
Issues
If onclogocally feasible,
double stapled anastomosis
is the preferred technique
of anastomosis
Handsewn Anastomosis
Technique
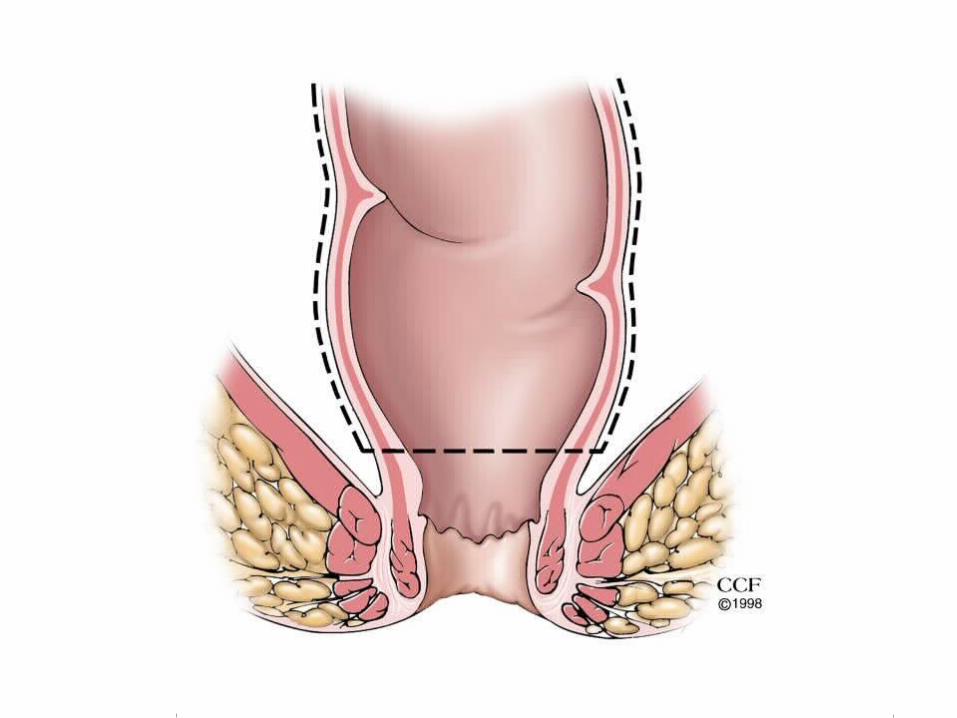
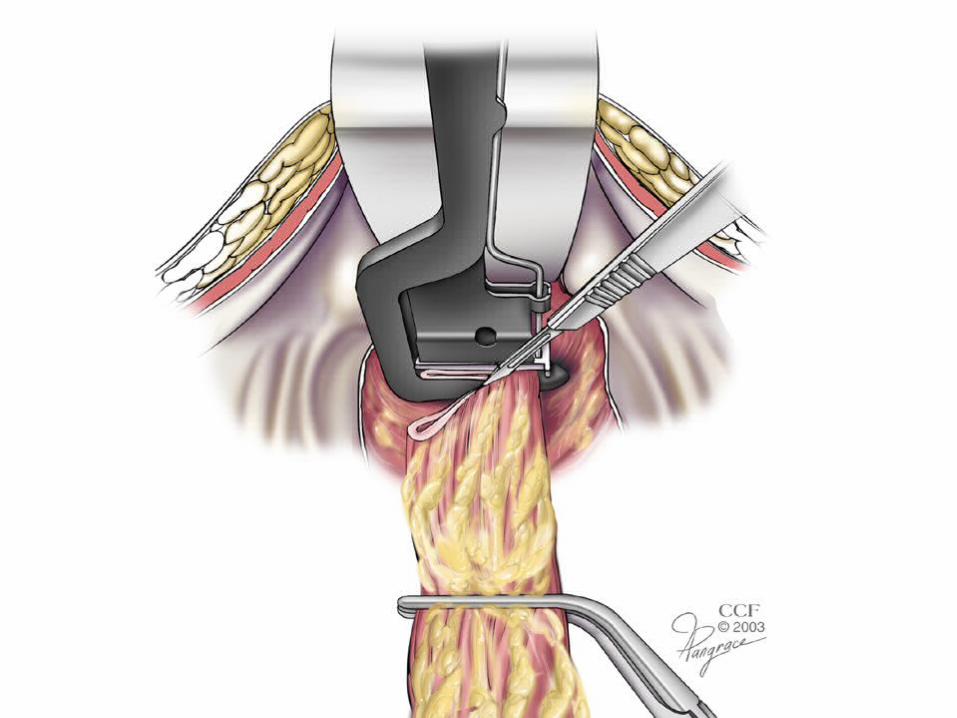
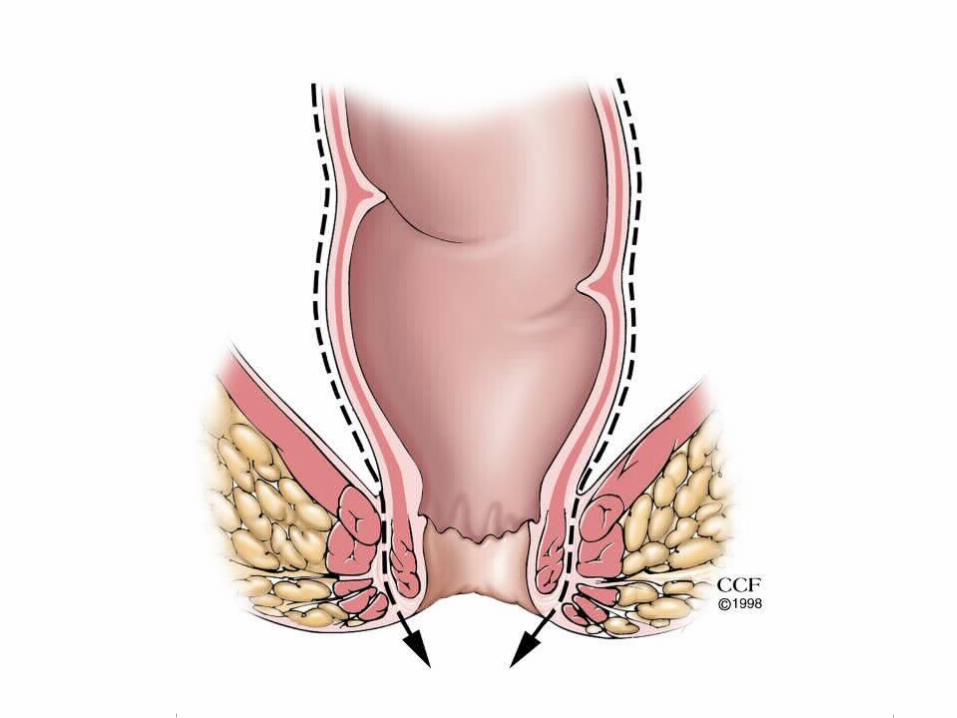
• Start in Kraske position; especially anterior lesions
• Put everting stay sutures and dissect circumferentially till you reach the plane above the levator muscles
• Use injectable epinephrine solution where mucosectomy is required
• Leave one location intact so the rectum doesn't retract
• Be careful not to do keyhole injury during the posterior dissection
• Release your stay sutures when you are ready to flip patient back to Lyodd –Davis position
Intersphincteric Proctectomy
Pros
• N=92 , R0 89%, Local recurrence 2%
• 5 yr overall and disease-free survival was 81 and 71 %
Cons
• 11 % radial margin positive
• Morbidity was N=25 (27 %) where, there was 14 patients with anastomotic complications
• Only 58 patients had minimum of two years of F/U
• Minimal information on functional outcome and final stoma status
Rullier et all Ann Surg 2005
Sphincter Preservation and QOL
• Increased associated morbidity
• Impact on QOL ?
• 30 Studies, 11 were non randomized, N= 1412 patients
• Six trials showed APR did not have poorer QOL than LAR
• Four trials showed APR had significantly poorer QOL than LAR
• Due to heterogeneity, meta-analysis was not possible
Cochrane Review 2005Cochrane Review 2005
Selection• No compromise in the oncologic clearance
• Patient must consent for the possibility of APR
• Motivated patient
• Lack of associated co-morbidity
• Good preoperative sphincter function
• If all above conditions are met, try to reconnect with diverting temporary stoma and have patient decide for himself or herself whether to live as they are or go back to stoma
1990 National Institute of Health consensus conference:
Recommends adjuvant postoperative radiotherapy and fluorouracil based chemotherapy for patients with B2-C rectal adenocarcinomas (JAMA 1990)
Pelvic Radiation and Rectal Cancer
• Pre or post op?
• Dose if preoperative
• Timing of surgery if given pre-op
• Which patients benefit
• ? If needed with TME
• Decision for APR versus reconnection, when ?
Pelvic Radiation and Rectal Cancer: Current Dilemma
• Dutch TME study
• Conclusion
�Even with good surgery, radiation improves local control for stage II and III low rectal cancers
�Patients with T3N0 tumors > 10 cm from the verge probably do not need XRT
Pelvic Radiation Preop and TME
Kapitenijn et al NEJM 2001
Summary
• Not all rectal cancers need preoperative radiation therapy
• Stage I rectal cancers probably do not need adjuvant treatment
• Predicting which stage II and III lesions require adjuvant tx not currently possible�ELUS is good, MRI is high likely the better
• Avoid the need for postoperative X-rt
• Better staging modalities in the future
Function and QOL after Radical Resection and Sphincter Preservation
• Inadvertent and uncontrollable passage of flatus to frank fecal incontinence