1 Sussex Community NHS Foundation Trust Community inpatient services Evidence Appendix Brighton General Hospital Elm Grove Brighton Tel: 01273696011 www.sussexcommunity.nhs.uk Date of inspection visit: 12 to 13 September 2017 Date of publication: xxxx> 2017 This evidence appendix provides the supporting evidence which enabled us to come to our judgements of the quality of care offered by community inpatient services. It is based on a combination of information provided to us by the hospital, nationally available data, what we found when we inspected, information given to us from patients, the public and other organisations. Community inpatient services Choose a rating
Transcript
1
Sussex Community NHS Foundation Trust
Community inpatient services
Evidence Appendix Brighton General Hospital
Elm Grove
Brighton
Tel: 01273696011
www.sussexcommunity.nhs.uk
Date of inspection visit:
12 to 13 September 2017
Date of publication:
xxxx> 2017
This evidence appendix provides the supporting evidence which enabled us to come to our judgements of the quality of care offered by community inpatient services. It is based on a combination of information provided to us by the hospital, nationally available data, what we found when we inspected, information given to us from patients, the public and other organisations.
Community inpatient services Choose a rating
2
Facts and data about this service
Community inpatient services provided a variety of services with the aim of preventing unnecessary hospital admissions and supported timely discharges from the acute hospitals. The locations provided rehabilitation and multidisciplinary care. In some cases, staff supported patients with end of life care.
Sussex Community NHS Foundation Trust has 349 Community inpatient beds at 11 locations across East and West Sussex:
Information about the sites which offer community inpatient services at this trust is shown below:
Location site name Team/ward/satellite name Patient group Number of beds
Geographical area served
Arundel & District Hospital
Ward 1 mixed 20 Coastal West Sussex (predominantly Arundel and Arun)
Bognor Regis War Memorial Hospital
Don Baines Ward mixed 24 Coastal West Sussex (predominately Bognor and Chichester)
Bognor Regis War Memorial Hospital
Leslie Smith Ward mixed 24 Coastal West Sussex (predominately Bognor and Chichester)
Crawley Hospital Piper Ward mixed 16 North West Sussex
Crawley Hospital Caravelle Ward mixed 28 North West Sussex
Crawley Hospital Stroke Rehab Ward mixed 18 North West Sussex
Crawley Hospital Viking Ward mixed 28 North West Sussex
Crowborough War Memorial Hospital
Intermediate Care beds mixed 18 High Weald, Lewes & Havens area of East Sussex
Horsham Hospital Horizon Unit mixed 38 North West Sussex
Kleinwort Centre Kleinwort Centre mixed 31 North West Sussex
Lewes Victoria Hospital
Lewes Intermediate Care Unit
mixed 26 High Weald, Lewes & Havens area of East Sussex
Midhurst Community Hospital
Bailey Ward mixed 17 West Sussex (predominately Chichester and Midhurst)
Salvington Lodge Offington Ward mixed 21 West Sussex (predominately Worthing, Arun and Adur)
Uckfield Community Hospital
Intermediate Care beds mixed 14 High Weald, Lewes & Havens area of East Sussex
Zachary Merton Swanbourne Ward mixed 26 West Sussex (predominately Arun)
We visited all of the locations above, apart from Crowborough War Memorial Hospital.
The inspection was unannounced.
During the inspection, the inspection team:
Spoke with 53 patients and 10 relatives who were using the service
3
Spoke with just over 330 members of staff , which included staff from numerous professional and non-professional backgrounds and included managers.
Reviewed 66 sets of medical records.
Observed board rounds and multidisciplinary meetings.
At the last inspection, we rated one key question as requires improvement. We reinspected all key questions because we were confident the trust had improved services.
4
Is the service safe?
Good
Mandatory training
We found staff had the right qualifications, skills, training and experience to keep people safe from avoidable harm and abuse, and to provide the right care and treatment. Staff told us it was their responsibility to ensure they were up to date with training and managers oversaw the training rates.
Mandatory training was a mixture of on-line training and face to face training. Modules included; safeguarding, information governance, infection control and prevention and fire safety. Additional modules were undertaken dependant on the staff member’s role. We saw training was appropriate for staff to deliver care in a safe way.
We saw evidence, which indicated staff were compliant with mandatory training.
The trust set a target of 85% or 90% for completion of mandatory training modules.
A breakdown of compliance for mandatory courses as of May 2017 is shown below:
Qualified Nursing and Health Visiting Staff
Training module Target % trained YTD
Back Awareness 90% 84.9%
Equality & Diversity 85% 78.2%
Fire 90% 80.7%
Health & Safety 90% 91.3%
Infection Control 90% 83.4%
Information Governance 90% 86.1%
Patient Handling 85% 76.9%
Resus 85% 67.6%
Safeguarding Adults Basic 85% 95.6%
Safeguarding Adults Level 3 85% 48.4%
Safeguarding Child Basic 90% 95.6%
Safeguarding Child Level 3 85% N/A*
* The trust did not have any staff identified as requiring this training.
The trust commented further: The 48.4% quoted is an additional internal 3 year target set for Band
5 and Band 6 staff. Band 7 and above as laid out in The Intercollegiate document is over 90% and
already achieved. The target so far in year is green and on track for delivery.
Qualified Allied Health Professionals
Training module Target % trained YTD
Back Awareness 90% 94.3%
Equality & Diversity 85% 88.6%
Fire 90% 91.4%
Health & Safety 90% 97.1%
Infection Control 90% 94.3%
5
Information Governance 90% 97.1%
Patient Handling 85% 93.9%
Resus 85% 70.6%
Safeguarding Adults Basic 85% 97.1%
Safeguarding Adults Level 3 85% 50.0%
Safeguarding Child Basic 90% 97.1%
Safeguarding Child Level 3 85% N/A*
* The service did not have any staff identified as requiring this training.
The trust added: The 48.4% quoted is an additional internal 3 year target set for Band 5 and Band
6 staff. Band 7 and above as laid out in The Intercollegiate document is over 90% The target so far
in year is green and on track for delivery.
Staff reported good access to mandatory training and commented it was very comprehensive. However, staff at Bognor Regis War Memorial Hospital (BRWMH) told us there was no time to do training during working hours and often completed training at home.
Across the trust, each staff member had a training passport which they were responsible for keeping up to date and could follow them if they changed roles within the trust.
Managers informed staff when they needed to complete training, although it was the responsibility of individual staff to ensure they completed training. The ward managers had a computer data base which showed each staff member’s compliance with mandatory training. Staff told us that they received an email when an update was required. Training data was entered manually onto the
system from sign in sheets. This could cause a time delay in the information showing on the system. Which indicated data received prior to inspection was not a true reflection of the actual training compliance seen at the time of inspection.
At Zachary Merton Hospital (ZMH), BRWMH, Salvington Lodge and Arundel and District Hospital
we saw a staff training display board that complimented the trust’s electronic training management
system. This provided a visual reference on upcoming events and training topics. In addition, the
display included a ‘red amber green’ status spreadsheet with an entry for each staff member.
Managers felt this helped encourage all staff to remain ‘up to date’.
The inpatient unit at Midhurst Community Hospital had pledged to make mandatory training compliance 100% by September 2017 and we saw evidence which indicated this could be achieved.
Mandatory training compliance had been difficult to manage on Piper Ward at Crawley Hospital as
the whole ward team started at the same time. There was a plan in place to provide the training to
the whole team but this hadn’t been possible as the ward had opened early. There was a training
spreadsheet kept by the ward manager, which showed all the staff, what training they had had,
when they were due to renew it. This was colour coded with a red, amber, green system. We
viewed the spreadsheet all staff had completed every part of their mandatory training. However, all
staff would need to renew their training at the same time. Plans were being put in place to ensure
that staff staggered their training to ensure cover. All mandatory training was booked through the
trust’s intranet system.
Safeguarding
Staff understood their safeguarding responsibilities and could describe the safeguarding policies and procedures. Staff had up to date safeguarding training at the appropriate level.
6
A safeguarding referral is a request from a member of the public or a professional to the local authority or the police to intervene to support or protect a child or vulnerable adult from abuse. Commonly recognised forms of abuse include: physical, emotional, financial, sexual, neglect and institutional.
Each authority has their own guidelines as to how to investigate and progress a safeguarding referral. Generally, if a concern is raised regarding a child or vulnerable adult, the organisation will work to ensure the safety of the person and an assessment of the concerns will be conducted to determine whether an external referral to children’s services, adult services or the police should take place. Community inpatient services made 241 safeguarding referrals between July 2016 and March 2017, of which 227 concerned adults and 14 children.
No children were treated in community inpatient services. However, staff may make a referral concerning a child if they had a concern about the child of a patient being treated in a community inpatient service or a child visiting a patient using the service, which accounted for the number of children safeguarding referrals.
The trust had comprehensive adult and child safeguarding policies that were known to staff on the
ward, accessible via the trust intranet and as hard copies on the ward. Polices followed the
Sussex Safeguarding Adults Policy and Procedures from the Sussex Safeguarding Adults Board.
The trust had a safeguarding team and staff spoken to knew how to contact them. There was an
adult safeguarding advice line and dedicated email address.
There was a safeguarding helpline available Monday to Friday from 9am to 5pm, which all staff we
spoke with at all sites knew how to access. Out of hours, an adult social care emergency line
provided cover and staff also had access to a safeguarding lead at each site who was trained to
level 4 safeguarding in accordance with the Intercollegiate Document, 2014.
The trust’s online database had a safeguarding adult’s page which provided staff with information
and guidance on what to do if they had a concern. This included information on the PREVENT anti
radicalisation strategy, the Mental Capacity Act, 2005 and the Deprivation of Liberty Safeguards.
Staff at all locations we inspected were aware of their role and responsibilities in reporting and
recording safeguarding incidents. We were told of numerous occasions where staff acted
appropriately and supported all those involved. For example, on Viking Ward at Crawley Hospital
we were advised staff suspected the partner of a patient with severe dementia might also have
dementia herself. Therefore, staff arranged for an assessment and organised extra care as part of
the discharge planning to ensure both the patient and their partner were supported when they
returned home.
A member of staff at BRWMH advised us they had never had to raise a safeguarding alert but felt
confident they knew the process and that they could rely on other staff for support. All staff we
spoke with at BRWMH knew who the trusts safeguarding lead was.
Referrals
Adults Children Total referrals
227 14 241
7
At Arundel and District Hospital, we witnessed safeguarding issues and concerns were discussed
at handover. This ensured all staff were aware of the situation and had the most up to date
information.
Cleanliness, infection control and hygiene
Across the trust, community inpatient services controlled infection risk well. Staff followed effective
systems and processes to prevent and protect people from a healthcare associated infection.
There were regular and appropriate checks in place to ensure standards were maintained.
Infection prevention and control at the trust was led by a senior infection prevention and control
(IPC) practitioner supported by five Band 7 IPC nurse specialists who each had a geographical
portfolio that included community and inpatient services.
Microbiology advice was available with a service level agreement with three acute NHS trusts.
Each consultant microbiologist covered a geographical area.
The IPC leads visited their inpatient units at least weekly to advise, to train and supervise auditing
of IPC practice.
Each unit had at least one link IPC practitioner who championed IPC practice and who, after
additional training, undertook hand hygiene training and audits. The link practitioners completed
two additional in house training courses. Link practitioners also attended monthly ‘Harm Free’
governance meetings. Staff contacted the link practitioner if they had an infection control concern.
The trust employed an antimicrobial pharmacist to ensure good antibiotic stewardship. They
worked closely with the IPC team and also with the GPs working for the local CCG to standardise
antibiotic prescribing in line with best practice guidance.
At all 10 sites visited during this inspection, we found all were clean and tidy and met the standards set out in ‘National Specifications for Cleanliness in the NHS: a framework for setting and measuring performance outcomes’ (2007). The 2017 Patient Led Assessment of the Care Environment (PLACE) score for cleanliness and
environment at the trust was 98.9%, which was better than the England average.
At all 10 sites visited during the inspection we found the ward environment and facilities were
compliant with ‘Department of Health Building Note 00-09 - Infection control in the built
environment’ (2013). For example, disposable curtains were clean, in date and we saw action
plans to ensure they were changed regularly.
All hospitals visited during the inspection provided appropriate and adequate quantities of personal protective equipment (PPE) for example, gloves and aprons in a range of sizes and available from numerous locations for easy access. Therefore, the trust was meeting standards set out by the Centre for Disease Control and Prevention ‘Guidance for the Selection and Use of Personal Protective Equipment (PPE) in Healthcare Settings’. This states “PPE must fit the individual user, and it is up to the employer to ensure that all PPE are available in sizes appropriate for the workforce that must be protected.”
8
During our inspection, we saw staff at all sites regularly using hand washing facilities and following the World Health Organisation ‘Five Moments for Hand Hygiene’ guidelines and observed all staff were bare below the elbows. Sinks across the trust had posters advising people of the most effective method of handwashing. We checked equipment at all 10 sites and found all items had ‘I am clean’ stickers on them to indicate they were ready for the next patient to use.
Don Baines ward at BRWMH kept daily cleaning equipment checklists. We saw the checklists and found in September 2017, there were a possible 187 opportunities to sign to indicate a piece of equipment had been cleaned each day. However, we saw there were only 26 signatures. In August 2017 out of a possible 280 occasions, there were only 16 signatures and in July 2017, there were 496 possible occasions and only 13 signatures. Although we saw all equipment had stickers on to indicate it had been cleaned, there was no overall assurance this was being done. When we discussed this with the ward manager she told us she knew the equipment had been cleaned, although there was no documentary evidence to support this.
Staff across all sites were able to explain isolation processes (shut doors, display signage, inform
facilities, decontamination trollies outside patient rooms, tiger bags and increase family
information).
On Don Baines Ward, we saw a patient in isolation located in a bay (being used as a single room).
We observed staff entering the room to provide care using appropriate PPE such as aprons and
gloves. However, the sign (an A4 laminated piece of paper) used to indicate that this patient had
an infection was difficult to see as it was placed at a low level on the wall adjoining the door. It was
not clear for visitors this patient had an infection and they should not enter. We spoke to the ward
manager regarding this who advised that because of the type of infection, it would not be an issue
if a relative or visitor entered the room and advised us that upon entering the ward visitors or
relatives would be informed which areas to not attend. However, this was not a clear deterrent to
enter the room and therefore posed a potential risk.
All the ward cleanliness audits met national standards and all staff we spoke with knew that 95% compliance was the pass rate. We checked cleaning schedules at all sites and found them to be completed and signed off.
The estates and facilities department audited cleanliness at every location at regular intervals in line with the national specifications of cleanliness guidelines. This states; very high risk areas should be audited weekly and achieve a score of 98%, high risk areas should be audited monthly and achieve a score of 95%. Areas of significant risk should be audited 3 monthly and score 85% and low risk should be audited 6 monthly. We saw records which indicated this was occurring and in August, July and June, all targets were met following audit. This information was recorded in the annual infection control report which we saw.
Across all sites, sharps bins were correctly assembled and labelled to ensure traceability. This was in accordance with the Health and Safety (Sharp Instruments in Healthcare) Regulations 2013 (the Sharps Regulations).
At Salvington Lodge, we saw there was clear guidance for staff on the action to take in the event of a needle stick injury. This was displayed in treatment rooms and other clinical areas.
9
Hand hygiene audit was completed at all sites monthly and met national standards. For example audits for May, July and August 2017 at Lewes were 100% compliant. At Crawley Hospital there was no hand sanitising gel at the entrance to the wards. It was explained by the infection and prevention control nurse that when designing the ward it was decided that this would be available at the entrance to the bays and at the point of care. All staff also carried a toggle of hand sanitising gel.
We saw staff at Lewes Victoria Hospital (LVH) offer patients hand cleansing wipes before they ate
their meal.
At Uckfield Community Hospital, we saw there was an active campaign to encourage staff to become infection prevention and control link staff. Link staff received infection prevention and control training every quarter, which was run by the infection prevention and control lead. One policy that had been introduced on site was a no lanyard policy, as studies had found this reduced the risk of infection. During inspection, we saw a side room at Uckfield Community Hospital was being deep cleaned in line with the trusts decontamination policy.
Uckfield Community Hospital had a service level agreement (SLA) in place with a microbiology
team at a local acute trust who provided support when needed. We noted the hospital had one
case of C.diff in August 2017.
The dirty utility on Don Baines Ward at BRWMH was open and there was no swipe access or key
code access. There was a locked cupboard containing hazardous substances. However, on the
floor underneath this, there were four, two litre bottles of macerator deodoriser which contained
hazardous substances. This was not in line with Control of Substances Hazardous to Health
(COSHH) regulations, 2002 and had been raised as an issue at our previous inspection. Also
there were 10 clean commodes stored in this room, three of which were stored directly beneath
the sink where dirty fluids and matter were tipped meaning they were at a high risk of getting
contaminated by splash before use.
Environment and equipment
Staff had access to adequate, well maintained equipment in order to perform their jobs.
The trust did not own all of the locations it provided services from and in some areas, the
environment and estate was a challenge to maintain. The estates strategy had been refreshed
recently and we saw there was oversight of the management of locations which did not belong to
the trust.
Patient Lead Assessments of the Care Environment (PLACE) are undertaken by teams of NHS
and private/independent health care providers, and include at least 50 per cent members of the
public (known as patient assessors). They focus on the environment in which care is provided, as
well as supporting non-clinical services such as cleanliness, food, hydration, the extent to which
the provision of care with privacy and dignity is supported and whether the premises are equipped
to meet the needs of people with dementia against a specified range of criteria.
The trust scored worse than the England average for four of the six aspects overall.
10
Performance across the locations was varied, with the Dementia Friendly and Disability metrics
generally performing worse than the England average.
Site Name Cleanliness Condition
Appearance
and
Maintenanc
e
Dementia
Friendly
Disability
Arundel And District Hospital 98.10% 94.33% 64.29% 78.00%
Bognor Regis War Memorial 97.91% 90.80% 71.77% 80.05%
Crawley Hospital 99.38% 90.80% 69.24% 81.04%
Crowborough War Memorial Hospital
99.70% 95.15% 71.01% 82.61%
Horsham Hospital 99.06% 91.79% 72.46% 84.18%
Kleinwort Rehabilitation Unit 98.76% 89.25% 59.35% 73.00%
Lewes Victoria Hospital 97.51% 95.43% 70.01% 82.60%
Midhurst Community Hospital 99.43% 96.32% 75.11% 86.14%
Salvington Lodge 100.00% 96.88% 72.46% 80.11%
Uckfield Community Hospital 99.11% 90.07% 65.56% 78.92%
We checked equipment across all sites and found portable devices were all serviced, tested and labelled according to electrical safety guidelines. Equipment stores at all sites were well organised, well-stocked and clean and dirty equipment was segregated appropriately.
Patients across the trust who were at increased risk of pressure damage were provided with
alternating airflow pressure mattresses to reduce the risk. Other patients, who were at less risk,
had profiling mattresses which were appropriate for their needs. Electric beds were used for most
patients to enable them to change their position with relative ease and to higher or lower the beds
before standing.
Across all sites visited during this inspection we checked resuscitation trolleys and found them to
be fully equipped and signed and checked daily.
Across all sites we checked oxygen cylinders and found they were all within their expiry date and stored according to British Compressed Gases Association ‘The Storage of Gas Cylinders (2016) guidelines. We also found the medical gas storage areas at all sites were secure and appropriately signposted. Medical gases at BRWMH were piped into the hospital via a manifold. The manifold was in a locked room outside of the hospital, within the hospital grounds where only authorised estates staff had access. Warning signs were clearly displayed on the outside of the building along with a number to call in case of an emergency. In the event, the manifold broke down; there were two emergency backup systems. Salvington Lodge had an onsite kitchen which had been given a five star rating following
inspection by the local environmental health team.
11
At BRWMH we saw an asset register, which recorded every piece of equipment, its asset number,
the last service date and when it was next due. We saw 10 pieces of equipment; all had asset
stickers and service stickers which indicated all the equipment had been serviced within 12
months.
At the Horizon Unit we saw a resuscitation bag was available and was checked daily to ensure it
was ready for use at all times.
On Piper Ward at Crawley Hospital, we saw there was a buzzer system at the entrance to the
ward that had a camera which showed pictures at the nurses station of who was at the door.
There were two buzzers that could be used, one at normal height and one lower that could be
used by visitors who were in a wheelchair. However, the fire door at the end of the ward was
opened with a green push button. Through that door was another door that led to the fire exit. This
was opened by breaking a clay bolt with a hammer that was attached to a chain. Without a poster
or pictorial explanation it could be difficult to understand what you would need to do in the event of
an emergency.
The Bailey Unit had a newly installed call bell system that was portable. This meant that if patients were away from their bed, they could call for assistance from wherever they were. During the inspection we saw that a patient that had been taken into the garden operated the call bell. The staff knew who it was and were able to collect them.
The day room at Uckfield Community Hospital was also used as a rehab area by the therapist teams. Whilst staff advised us, the area was used for dual purposes. This meant staff had to move equipment in and out, for therapy sessions and patients could not always, access the day room if a therapy session was in progress. It also meant that storage of equipment was difficult for staff. We saw the hospital had an action plan in place to make this area more user friendly and adaptable.
Staff at Uckfield Community Hospital had recently raised concerns about the front door of the hospital not closing at night. The doors had been repaired, however the week before the inspection, the hospital was subject to a theft of medical gasses. We inspected the storage area and found it to be secure. As a result, a security guard was carrying out night patrols of the area and the theft was subject to a police investigation. A review of the security cameras had also been undertaken. At Midhurst Community Hospital the doors were locked and alarmed at night. Night staff on duty were responsible for the security of the building and reported no concerns with regard to safety. Managers had carried out a risk assessment and had considered the hospital’s location within the assessment. At Zachary Merton Hospital (ZMH), staff explained that after hours, there was no security on the premises. Staff were advised to call the police if concerns and had cited examples of intruders in the past. Some staff felt vulnerable in these circumstances. At ZMH, we observed an internal door leading to the laundry that could not be locked. The latch mechanism had been removed. Inside, we saw bulk containers of laundry detergent stacked on the floor. There were also loose ‘fire exit’ signs leaning against the wall and the room appeared to have been recently decorated. Management undertook to address the risk immediately and we noted a lockable cabinet for the liquid detergent was supplied and fitted before we left the premises. We were told the door lock would be refitted as soon as possible.
12
We observed adequate equipment available to meet the needs of patients. However, staff explained that delays could occur in receiving equipment depending on how it was funded. For example, donations from the league of friends had to be backed by a proposal and product search, which caused procurement delays. Therapists reported they had no issues with obtaining bariatric equipment.
Staff at Salvington Lodge had built up a store of walking aids as they advised us it often took three
to seven days for equipment to arrive on site. Staff advised us this often delayed discharge.
We saw at all sites, clinical waste was segregated in coloured bags on wards and units. We saw
clinical waste compounds were locked and secure, the bins inside were locked. Waste was tagged
depending on the type of waste contained; non-hazardous, cytotoxic or pharmaceutical. The tags
had a bar code on so the bin could be followed electronically from the hospital to its final
destination. This occurred across the trust.
Assessing and responding to patient risk
Across all locations, we found a wide range of risk assessments, screening tools and record charts
were used to minimize risk to patients. Effective policies and procedures were in place to manage
a patient in an emergency.
The trust had escalation policies and procedures in place for deteriorating patients and they were used effectively. Any urgent medical needs were accessed via the 999 service and patient transfers could be made to local acute hospitals as necessary. Across the trust patients Zimmer frames had a piece of coloured tape on them and this indicated how they mobilised. For example, a green piece of tape meant they were able to mobilise independently. This meant staff were able to quickly identify what assistance a patient required to mobilise.
Across all hospitals, we found a wide range of risk assessments, screening tools and record charts were used appropriately and effectively and were well documented. Multifactorial risk assessments were completed and included; history of falls, medication, venous thromboembolism (VTE) and pressure area damage.
However in quarter one 2017, the trust reported that they were underperforming on VTE assessments at the central area community hospitals with 75% of patients being assessed compared to a target of 95%.
In quarter 1 2017, the trust reported two incidents of attributable pressure damage at the central
area community hospitals. This included low grade damage at level 2.
In quarter 1 2017, the trust reported that they were underperforming on falls risk assessments
within 48 hours of admission at the central area community hospitals with 75% of patients being
assessed compared to a target of 95%. The number off falls with harm was, however on target at
18% for the same period.
A trust wide falls audit was in progress with data submitted in June 2017 but had not been
analysed at the time of inspection.
Across all sites, we saw appropriate mitigation of the risk of pressure damage to patients’ skin. A
risk assessment based on a Waterlow Score was used to determine the extent to which each
patient was at risk of pressure damage. Where the patient had an increased risk, their care plan
13
included the action to reduce the risk. Measures used included specialist alternating air mattresses
for those at highest risk, pressure relieving cushions and profiling mattresses. The unit had a real
focus on rehabilitation and encouraging mobility which was the most effective means of preventing
pressure damage.
At all sites we saw comfort rounds were undertaken regularly these included safety checks on patients and assessment of needs for example, pressure areas.
At all sites we saw patients observations were used to calculate a National Early Warning Score (NEWS). This is a nationally recognised system of using key observations such as the patient’s blood pressure and pulse to help staff recognise changes in a patient’s condition that might indicate a deterioration.
An audit of NEWS at Crawley Hospital found that scores were being added up incorrectly, as staff were not completing the correct boxes. In response to this an advanced nurse practitioner created a NEWS training programme that all on site staff had completed and been signed off on. NEWS audit scores since the training had shown dramatic improvement.
If a patient fall occurred during admission at Salvington Lodge, it was recorded on a falls log. Patients then underwent a further risk assessment to ensure the risk was being managed appropriately. Actions included using fall prevention devices (mats and alarms), changing footwear and providing extra staff supervision. There was also an additional MDT which was a standard undertaken when any fall occurred on the unit. All falls were reported via the include reporting system. At LVH, we saw body maps were used to indicate any changes to the condition of the patient’s
skin, which may indicate developing pressure damage.
All patients at Midhurst Community Hospital and ZMH had a mobile call bell, this meant wherever they went in the building if they required assistance the staff were able to locate them quickly if required. When patients pressed the call bell their location was displayed on a monitor.
We saw at Midhurst Community Hospital that patients assessed as being a falls risk or who would leave their beds were given an alarm which would sound if the pressure applied while in bed was released.
At Midhurst Community Hospital we saw multidisciplinary team (MDT) falls assessments were completed within 4 hours of admission and each patient’s transfer status was displayed on the board above their bed. Any other relevant information was documented on the board. For example, we saw on one patient’s board it said must wear slippers to mobilise not slipper socks.
At Midhurst Community Hospital and ZMH, we saw there was “call don’t fall’ posters which encouraged patients to press their call bell and ask for assistance rather than having a fall.
At BRWMH we observed patients wearing coloured wrist bands. Staff told us these indicated
different risks. For example, one colour denoted the patient had allergies. We observed patients
on the wards wore different coloured wrist bands and that these corresponded with risks detailed
in their notes.
Advanced Nurse Practitioners at Crawley Hospital worked on tracking 999 transfers and found that
staff on the hospital’s inpatient wards were not recognising sepsis within the required times and
therefore there were delays in getting patients transferred to a hospital with an accident and
emergency (A&E). Since then the hospital had implemented a sepsis training programme to
14
improve understanding of the early signs and symptoms of sepsis and since January 2017, there
had been no delays in the transfer of sepsis patients to A&E.
At Arundel and District Hospital there was a board meeting held daily, which was held in a private
office. The office had a detailed board which included information including: Patient name, date of
birth, step down or step up, dementia status, whether they have had a welcome meeting, if they
were in need of physio, OT and dietary needs. The hospital had introduced a new call bell system.
This electronically recorded the time it took for staff to respond. This was due to be audited but
had only been in place a few weeks.
Staffing
Planned staff Actual staff %
Trust wide 351,789 359,951 102%
Arundel DH 21,102 20,740 98%
Caravelle Ward 25,020 26,798 107%
Crowborough Hospital 18,545 19,865 107%
Don Baines Ward 23,525 22,810 97%
Horizon Unit 33,730 34,223 101%
Kleinwort Ward 34,264 32,496 95%
Leslie Smith Ward 23,879 23,096 97%
Lewes Victoria Hospital 31,908 29,464 92%
Midhurst CH 15,786 15,789 100%
Piper Ward 17,785 19,016 107%
Salvington Lodge 20,486 20,191 99%
Stroke Rehab Ward 21,288 21,371 100%
Uckfield Hospital 15,934 17,165 108%
Viking Ward 24,644 25,116 102%
Zachary Merton Ward 23,893 31,811 133%
Source-Additional data request 2017
Between June 2016 and May 2017 the trust reported an overall vacancy rate of 27% in community
inpatient services.
Staff group Total % vacancies overall (excluding
seconded staff)
Dietician* 100%
General Practitioners 66%
Healthcare Assistant 22%
Nurse 33%
Occupational Therapist 16%
Physiotherapist 16%
SALT* 8%
Trust Scale (Medical) 65%
15
*Staff group had very low numbers
Between June 2016 and May 2017, the trust reported an overall turnover rate of 18% in community inpatient services.
Staff group
Sum of total
number of
substantive staff
per month
Total number of
substantive staff
leavers in the last
12 months
Total % of staff
leavers in the last 12
months
Qualified Allied Health
Professionals 410 76 19%
Qualified Nursing and
Health Visiting Staff 5,539 1,014 18%
Core service total 5,949 1,090 18%
Between June 2016 and May 2017 the trust reported an overall sickness rate of 6% in community inpatient services.
Staff group Total permanent staff
sick days
Total available
permanent staff days % sickness
Qualified Allied
Health
Professionals
2,192 55,369 4%
Qualified Nursing
and Health Visiting
Staff
43,182 767,907 6%
Core service total 45,374 823,276 6%
The trust advised us for community inpatient services: The inpatient units receive medical care
from GPs, not consultants, out of hours. This cover is provided by the GP out of hours (OOH)
service as part of the GP OOH contract commissioned by the CCG.
Between June 2016 and May 2017, this core service reported that there were four cases where staff had been suspended. During engagement with the trust prior to inspection it was noted that staffing was one of the trusts
biggest risks and was the second item on the trusts risk register. During inspection we noted that
there were specific sites within the trust that had difficulties recruiting compared to others. Crawley
Hospital was one of the locations within the trust that had found it difficult to recruit compared with
other locations. We asked the general manager of the hospital why they believed this was an
issue and found; easy access to London from Crawley meant they were competing with London
weighting payments. Also, Crawley Hospital building was used by many different trusts. The
general manager advised us that another trust offering services within the building paid £5,000
more per year for each band grade, and therefore SCFT was losing staff who wished to work
locally to other trusts offering better pay. We were also advised that the site used to use a local
agency company and had access to 50 staff who wished to work at the site. However, at the end
16
of the contract senior management decided to renew the agency work with a different contractor
who was not local. Since then the general manager advised us it was difficult to get enough
agency staff to cover the wards.
Senior managers at Crawley Hospital advised us that they were using band seven locums to fill
band five and six gaps in the rota. Senior staff accepted this was not a good use of trust money,
but advised us this was necessary in order to meet safe staffing levels.
At the time of inspection, there were seven nursing vacancies on Caravelle Ward at Crawley
Hospital. There were interviews planned for a band 6 the day after inspection on Viking Ward and
interviews for a new matron were due the week after inspection. There were no plans to recruit to
the Stroke Ward as the wards function was under review because it was covering patients from
both Surrey and Sussex. However, Crawley Clinical Commissioning Group (CCG) was funding the
ward. Therefore, plans for the ward were on hold until an arrangement could be met with Surrey
CCG.
We spoke with the general manager at Crawley Hospital, who told us that on the day of inspection
across the four inpatient wards, only one had a band 7 nurse in charge. The other wards had band
6 nurses in charge. However, we found that Viking Ward had a band 5 nurse in charge. Managers
told us there should be a band 7 on all wards.
We were shown the staff rota in Viking Ward at Crawley Hospital and found it was fully covered for
the day of inspection. However, the next day the team required another band five nurse. We asked
the band five nurse in charge what plans were in place to ensure this shift was covered and were
advised the bed manager organised shifts for the following day the evening before. We found the
nurse in charge was unaware of any formal processes in place for escalating staffing issues, other
than to wait for the bed manager. We also saw of the seven staff on shift, three were from an
agency.
At The Kleinwort Centre, we saw two months data that revealed 57% of ‘trained’ shifts and 24%
‘untrained’ shifts were covered by agency staff. In August 2017, the figures were 51% of trained
shifts and 24% of untrained shift covered by agency. Thirty four shifts were not covered. We heard
from staff that in addition to the high use of agency workers, the reliability of the agencies varied.
We learned of several example when agency staff failed to attend or late cancellations.
Staff at one location told us bank and agency staff often did not show up for shifts. Therefore,
permanent staff often felt they had to cover the bank shifts to ensure continuity for patients. We
reviewed a week’s rotas and found six out of 15 shifts still had gaps.
We saw staffing at BRWMH, Crawley Hospital and The Kleinwort Centre was a continuing concern
for SCFT. Staff and managers could raise staffing as an issue on the risk register. When the risk
rating got to 15 and above, it would then be discussed at the board. The trust had increased
Health Care Assistant (HCA) hours on the wards at BRWMH and was carrying out a pilot of band
4 roles at BRWMH, The Kleinwort Centre and Crawley Hospital. Staffing was constantly being
monitored at all locations.
Some of these actions were part of an improvement plan for The Kleinwort Centre. Other actions were the movement of substantive staff from other units to reduce reliance on temporary staff and the block booking of temporary staff to reduce variance.
At the time of inspection, the wards at BRWMH were fully staffed with support from bank and
agency workers. Although there were no band 5 nurses working on site, three new band 5 nurses
had been recruited and were still going through the recruitment process.
17
All staff we spoke with at BRWMH told us they completed an incident report when staffing
numbers were low. However, they all felt a lack of support from senior managers and were often
told to “Just get on with it”. The ward manager was meant to work supernumerary, however they
advised us that most weeks they worked at least one clinical shift in order to cover absence.
We were told how staffing at the Bailey Unit at Midhurst Community Hospital was the biggest risk and saw this was at the top of the risk register. This was not just staff numbers but also the wellbeing of the staff and the long shifts they worked. It was said that the staffing templates were tight and they would prefer to have more trained staff.
The Bailey Unit had been closed between April and September 2016 due to low number of staff. The decision was made to close the service with patients being transferred to other community hospitals. Following the closure of the unit, the hospital launched a recruitment drive for trained nurses and healthcare assistants. This had resulted in them having sufficient staff to re-open. At the time of the inspection the ward had vacancies for three full time qualified nurses and 1.75 full time equivalent health care assistant vacancies.
Staffing details at Arundel and District Hospital were held at the front of the rota, this was so the
ward manager could contact them if staffing issues arose. The rota also contained emergency
contact details for the matron, ward manager, clinical lead night nurse, duty director and facilities
as well as contact details for agency.
We saw there were no staffing issues at LVH, Salvington Lodge and Horizon Unit at Horsham
Community Hospital and saw from the rotas that agency staff were not required due to full staffing
levels.
Medical staffing was provided in a variety of ways at the various locations:
A consultant geriatrician from a local acute hospital visited several times a week and oversaw the
management of more complex, frail elderly patients. They also worked in the acute trust and a
local hospice so were able to ensure seamless care and appropriate discharges from the acute
trust to Horsham hospital. Where they felt a patient might be able to make better use of
rehabilitation programmes by spending an extra day or so in the acute trust to optimise their
physical health prior to rehabilitation, they could facilitate this.
Medical cover at Midhurst Community Hospital was provided by GP’s at the practice within the
grounds of the unit. Each GP undertook a session a week and provided cover Monday to Friday.
Outside of these hours support was provided by out of hours GP services or if the patient was very
unwell 999. In addition there was a ‘One Call’ service which was a telephone advice service. Calls
to the centre were triaged by a call handler and passed onto a clinical advisor. GP’s could assess
this service if they wanted to arrange an admission to hospital for a patient.
The medical cover at Uckfield Community Hospital was provided by three GP surgeries. They each had their own approach to providing cover. The cover provided was responsive and staff felt they were supported to meet patient’s needs. There was an out of hours GP service that covered the hospital at night and weekends. The medical records we viewed demonstrated patients were reviewed regularly. Patients felt they had appropriate access to medical review. GP cover at ZMH utilised advanced nurse practitioners and was provided during from 8am to 5pm Monday to Friday. The service utilized two full-time GPs and three advanced nurse practitioners. Out of hours medical cover was provided by the out of hours GP service. Locum cover was also available for holiday or sickness cover. We saw an escalation plan designed to help staff respond
18
to concerns or deteriorating patients. A community geriatrician attended weekly, timed to coincide with the multi-disciplinary meeting to give consultant support. Medical cover as well as advanced nurse practitioner (ANP) cover at Bognor Hospital was
provided Monday to Friday from 9am to 5pm. However there is out of hours GP cover on wards at
weekends.
Lewes Victoria Hospital was nurse led and medical support was provided two hours a day by the
local prison. Patients who lived in Lewes were cared for by their GP during their admission to LVH.
Quality of records
The management and quality of medical records varied across site. Some locations were using a
single record and others had information stored in a variety of documents, which meant there was
no one place for staff to access information. The trust was in the process of implementing the
single patient record. In addition to this, the standard of documentation varied across the trust.
Across all sites we found medical notes were disorganised, as some information was kept in the
end of bed notes and some was kept either in the medicine administration form or in the actual
medical record. There was not one uniform document that contained all relevant information,
therefore it was possible staff would miss important information. However, at the time of the
inspection the trust was rolling out a new system where all patients’ notes and records would be
kept together. This was not in place at the time of inspection.
We found the standard of medical notes varied greatly across inpatient sites. For example, at
Crawley Hospital we found where patient records did not contain a ‘Do Not Attempt
Cardiopulmonary Resuscitation’ (DNACPR) order, there was no description in the notes of
whether this had been discussed with the patient and discounted or whether those conversations
still needed to happen. This meant that a patient who requested DNACPR might be asked several
times whether or not they wanted it, which could affect their decision.
Notes at Arundel and District Hospital were not fully completed. There were sections not filled out
and the new documentation was largely ignored in some notes. Of particular note was DNACPR
which had not been indicated on the front of the integrated care plan. We were told all the
DNACPRs were held in a separate file in the matron’s office. However, the patient’s preference in
terms of DNACPR were also highlighted on the handover sheet. We also found an example of
patient notes which had only the patient name on the front and no other identifying information.
Therefore there was the potential for staff to mix up the notes with someone who had the same or
similar name as there was no other way to identify them.
At Uckfield Community Hospital, consent and patient involvement was not always documented in patient’s notes. The records we viewed did not reflect the care we observed being delivered. Some entries in the nursing notes were no longer than two to three sentences and did not provide a concise, systematic approach to patient needs or the care delivered. We were told that records were audited in the unit and that staff were awaiting their latest performance results. However, we reviewed the audit tool and found the concerns we identified were not incorporated into the audit and therefore would not have been identified. At Crawley Hospital, we found a discrepancy between the quality of therapist’s notes and nursing
notes. For example, of the 10 patient records we checked, all therapy assessments including
occupational kitchen assessments and joint therapy assessments were completed, signed, dated
and legible. However, of the same 10 records, we found all had a part of their nursing notes
missing or incomplete, for example discharge planning, the dementia screening tool, errors in
19
notes were not initialled and dated, mental capacity assessments and DNACPR forms were not
fully completed.
At BRWMH, 100% of notes we reviewed did not have cognitive function and dementia screening
completed, and 50% did not contain any of the following; a completed elderly mobility scale,
completed advance care plans, details of the patients ethnicity, the information sharing document
was not signed, and there was no list of approved abbreviations.
However, at all sites we saw patients’ records were stored securely in a locked cabinet with the staff room, nursing/therapy records were kept at each patients’ bedside. At Lewes Victoria Hospital, Salvington Lodge and Horsham Community Hospital patients’ records were all fully completed and legible and DNACPR forms were fully completed and signed by two consultants. There was a standardised systematic approach to the daily nursing entry’s which meant there was a clear record of patient care, and interventions. However, like Bognor there were a lot of abbreviations used throughout the notes without a list of approved abbreviations available in the record. Patient records at Midhurst clearly showed multidisciplinary team working. Therapists and nursing staff contributed to and shared information on patient care within an integrated patient care document. Patient records were clear, completed consistently and regularly reviewed. Records also included completed risk assessments, for example, bed rails as well as the patient’s own assessment of their needs. Records were all signed, dated and timed.
Across all sites we saw clear mechanisms for sharing appropriate information with GPs and other relevant providers and professionals during discharge. We saw staff ensure third parties fully understood the care that had been received and any next steps. We were told how a new trustwide system was being implemented in October 2017, which would allow staff to have read only access to inpatient notes at the local acute trust. This would enable staff to have a holistic view of patients moving from acute hospitals in to a community hospital setting.
GP notes could be obtained from the trusts ‘capacity and resilience’ team, in cases where fuller details or medical history were required. Staff explained that this was a rare requirement as most patients were ‘stepped down’ from acute hospitals or arrived with referral details from the GP.
A detailed handover sheet was provided to all staff at Salvington Lodge at the start of their shift. This document provided a wide range of information about the patients on the unit. For example, diagnosis, transfer and hygiene requirements, continence and nutrition. It also recorded the expected length of stay. The registered nurse on each shift updated the handover sheet daily.
We were told that there had been concerns in the past about electronic medication records and other details missing from the acute hospitals on discharge. This had prompted the formation a year ago of a ‘Safe transfer of care’ meeting, attended each month by matrons from acute and community trusts. This was viewed as a positive initiative and had reduced the number of errors or omissions.
Medicines
We found Medicines were stored and managed in line with best practise guidelines and legislation.
Missed dose audits were carried out regularly.
Medicines at all sites were provided by a local NHS trust who supplied all in hospital and take home medicines. A pharmacy technician visited the wards weekly and was responsible for the
20
ordering of stock drugs and arranging take home medicines. A pharmacist visited the ward weekly and undertook medicine chart reviews and provided support and advice to ward staff.
There was oversight of medicines management by the Medicines Safety & Governance Group
which met quarterly. Minutes from the group showed that medicines policies were amended in
light of changes to national guidance. The minutes from the December 2016 meeting showed that
the group had approved the Safer Administration of Insulin in Adults Procedure V4-CH which had
been updated to reflect changes to the national guidance.
There was evidence in the minutes from this group that consideration was given to patient safety
alerts. The group had reviewed the Patient Safety Alert: Risk of death and severe harm from error
with injectable phenytoin NHS/PSA/W/2016/010 and determined that this was applicable to the
trust.
We checked medicine storage across all 10 sites and found that controlled drugs were kept in
locked, secure storage. Controlled drug balances and expiry dates at across all sites were in date.
Controlled drug records were fully completed and checks had been documented daily. Trust policy
stated the key to the controlled drugs cabinet was held by the nurse in charge and was separate to
the main drug cupboard keys. We saw this was followed at all locations.
During the inspection, we checked refrigerators used to store medicines were monitored daily to ensure that the temperatures were within the safe range. At all sites we saw records of this and staff were able to describe escalation processes if the temperature was outside the safe range.
At all 10 sites visited we saw staff wore a ‘drug round in progress do not disturb’ sign when undertaking the medicine round.
We found medication trolleys were securely locked when nurses were administering medications as well as when trolleys were not in use. This occurred at all 10 locations.
The ambient air temperature in medicine storage rooms were checked daily, and we saw records, which supported this, was undertaken. However, at Bognor the emergency medicines cupboard was situated in the occupational therapy assessment room where there was no monitoring of ambient temperature, which was not in line with best practice. Staff told us this was where extra stocks were stored as it was difficult to get prescribed medication on time from pharmacy if ordered on a Friday as they were usually not delivered until the next Monday.
At Midhurst Community Hospital, we saw a missed dose medicine audit was completed at the end of each medication round. This required the nurse and another staff member to check all boxes on the medication charts were signed to confirm the medicines had been administered. We checked the audit records between 11 August 2017 and 10 September 2017 which showed 100% compliance.
We saw at Horsham that where a patient was prescribed insulin, their blood sugar level was tested
prior to administration and adjusted, as necessary. Patients who were prescribed Warfarin had a
recorded International Normalised Ratio (INR) blood level that was checked before administration
to ensure their blood clotting times were within a normal range.
At Salvington Lodge ‘patient refusals’ were clearly recorded on the medicine administration record as well as a separate record that detailed the reason for the refusal or missed dose. This meant there was a clear audit trail for missed or omitted doses. Medicines reconciliation is the process of identifying an accurate list of a person's current medicines and comparing them with the current list in use, recognising any discrepancies, and
21
documenting any changes. We saw the pharmacy team at LVH recorded the time from admission that medicines reconciliation occurred to ensure it was in line with NICE guideline ( NG 5). Patients at LVH were admitted from the acute hospital with two weeks supply of medicines. If further medicines were required, these were ordered at a local pharmacy, there was a service level agreement in place. At LVH we saw checks were undertaken at the end of each medication round to ensure no
medicines had been missed.
At Arundel and District Hospital we reviewed 10 medication charts and only one was not correctly
signed for, we were advised this was completed by an agency nurse.
Patients at Salvington Lodge who were able to self-administer their medication had a risk assessment in place to ensure they were safe to do so. This meant any risks with self-administration could be identified and managed appropriately. We also saw patients who required laxatives, had their bowel motions tracked and recorded to ensure medications were only given when they were required. At Midhurst Community Hospital, we saw an incident relating to a medicine error was discussed within the monthly incident newsletter. This involved out of date eye drops dispensed by an NHS trust pharmacy and administered in the community. Learning from this incident was highlighted within the article.
At BRWMH we saw the nurse on duty completed peer checks following every medicine round.
Records in the controlled drugs register at Uckfield Community Hospital were contemporaneous and demonstrated adherence to the Royal Pharmaceutical Society of Great Britain ‘Schedule 2, Safer Management of Controlled Drugs’. At Crawley Hospital, if there was no second registered nurse to complete the administration of a controlled drug (CD), there was a number to bleep which would be picked up and a second nurse could attend. FP10 prescribing forms were held in the cupboard that contained the CD cupboard. An FP10 is a prescription form, which can be dispensed on the NHS. There was a separate record kept which included the FP10 unique number, the patient name and who gave it to the doctor to write up. This ensured that the stock of FP10s was appropriately managed and they could not be misappropriated. At Uckfield Community Hospital, FP10s were in use and accounted for in line with national guidance. There was one nurse who had oversight of the issuing process and undertook regular audits to ensure appropriate traceability. At The Kleinwort Centre we reviewed three medicine administration charts, all contained details about patient weights, allergies, VTE assessments and pharmacy annotations. There were no missed doses and we noted systems of double checking after each drug round to ensure this. FP10 prescription pads were securely stored and controlled, however the system was not effective at identifying missing pages (prescription sheets). Therefore, the hospital was unable to prove effective auditing and tracking of prescription sheets. This was discussed with the ward manager and pharmacy technician at the time of inspection and immediate remedial action was taken.
Safety performance
The chief executive of the trust sent out weekly information newsletters, this was trust wide and
compared SCFT safety information. These were printed off and displayed in staff rooms.
22
We saw at all 10 sites visited that the NHS safety thermometer was completed on a monthly basis. This measured the occurrence of pressure ulcers, patient falls, catheter acquired urinary tract infections and venous thromboembolism (VTE).
In Quarter 1 2017, the trust reported that they were exceeding the target for harm free care at the central area community hospitals with 97% of patients receiving harm free care compared to a target of 95%. All patient deaths across the trust were reviewed clinically in a Mortality Review Meeting. The records of the meetings which we reviewed showed a detailed record of the discussions around the management of each patient. No lapses of care were identified for any of the patients who had died and feedback from families was entirely positive.
On the Bailey Unit at Midhurst Community Hospital, this information was displayed on the ward notice board, which meant staff and visitors could see the information. For example, data for August 2017 showed it had been 25 days since a patient had hospital acquired pressure damage and 66 days since a patient had an injurious fall. In August 2017, there had been zero health care acquired infections.
These displays helped relatives and visitors understand what the trust was monitoring and see how each location was performing against set targets. This indicted the organisation had a positive focus on safety and was transparent about the levels of harm-free care achieved.
At Arundel and District Hospital during August 2017 there was one fall and one pressure ulcer
reported on the safety thermometer. We looked at notes with regards to the pressure ulcer and
saw it was investigated appropriately and was caused by moisture as the patient in question
refused to have an air flow mattress.
At ZMH and The Kleinwort Centre we noted the safety thermometer data showed staffing was
meeting planned levels during August and the other indicators met or exceeded trust targets.
The Arundel and District Hospital had ‘Knowing How We Are Doing Boards’. They had two boards,
one for matrons to review and one which was displayed in the receptionist’s office for staff and
patients to access. The board had four sections 1: Improve productivity (latest figures relating to
(FFT results, feedback from patients-complaints) and 4: Patient safety (reviewing incidents, safety
performance).
There were no deaths reported at Horsham Hospital in quarter one 2017-18. However, in the preceding quarter there had been nine deaths at the hospital. These were all patients who were admitted for end of life care or who had been admitted for rehabilitation but who on admission were clearly too frail to benefit from the rehabilitation programme. Most of the patients had chosen the hospital as their preferred place of care and were either transferred from an acute hospital or were admitted from the community when their families struggled to provide the level of care they required.
Incident reporting, learning and improvement
Staff had a good understanding of when and how to report incidents. Managers investigated
incidents thoroughly and shared learning from lessons at local level and across the trust.
Trusts are required to report serious incidents to Strategic Executive Information System (STEIS). These include ‘never events’ (Never events are serious incidents that are entirely preventable as guidance, or safety recommendations providing strong systemic protective barriers, are available at a national level, and should have been implemented by all healthcare providers).
23
In accordance with the Serious Incident Framework 2015, the trust reported 27 serious incidents (SIs) in community inpatient services, which met the reporting criteria, set by NHS England between September 2016 and August 2017. Of these, the most common type of incident reported was slips/trips/falls meeting SI criteria (16 serious incidents).
Incident Type Number of Incidents
Slips/trips/falls meeting SI criteria 16
Adverse media coverage or public concern about the
organisation or the wider NHS 2
Confidential information leak/information governance breach
meeting SI criteria 2
Treatment delay meeting SI criteria 2
Diagnostic incident including delay meeting SI criteria (including
failure to act on test results) 1
HCAI/Infection control incident meeting SI criteria 1
Medical equipment/ devices/disposables incident meeting SI
criteria 1
Medication incident meeting SI criteria 1
Pending review (a category must be selected before incident is
closed) 1
Core Service Total 27
Between May 2016 and May 2017, trust staff in this core service reported 19 serious incidents. Of these, none involved the unexpected death of a patient.
The most common types of serious incidents were slips/trips/falls meeting SI criteria with 14 serious incidents. The NHS Safety Thermometer allows teams to measure harm and the proportion of patients that are ‘harm free’ during their working day. For example, at shift handover or during ward rounds. This is not limited to hospital; patients can experience harm at any point in a care pathway and the NHS Safety Thermometer helps teams in a wide range of settings, from acute wards to a patient’s own home, to measure, assess, learn and improve the safety of the care they provide. Safety Thermometer data should also not be used for attribution of causation as the tool is patient focussed.
Between August 2016 and August 2017 the trust reported 23 new pressure ulcers.
Between August 2016 and August 2017 the trust reported 14 falls with harm.
Between August 2016 and August 2017 the trust reported 44 Catheter & new UTI’s.
Between August 2016 and August 2017, the proportions of patients receiving harm free care at the trust’s Community Inpatient’s service was consistently above 90%. The Chief Coroner’s Office publishes the local coroners Reports to Prevent Future Deaths which all contain a summary of Schedule 5 recommendations, which had been made, by the local coroners with the intention of learning lessons from the cause of death and preventing deaths.
24
There has been one prevention of future death report sent to the trust in December 20161. A new electronic incident reporting system had been implemented by the trust the year previous to
our inspection. We asked senior members of staff whether incident reporting had improved during
this time. The general manager at Crawley Hospital advised us the new system allowed better
analysis of incidents. For example, the system identified a particular nurse kept making medication
errors and after further investigation management found that they had eyesight issues which the
hospital was able to support them with. At Bognor Regis Hospital, staff told us that accessing the
system was an easy process. However when we asked one of the ward managers to show us the
most recent incident, they were unable to access this on the system.
The trust was running incident systems training for managers to improve the management oversight of reporting, learning and investigation.
Across the trust, matrons and ward managers were involved in monthly area team meetings which
also fed back on incidents and action plans. Staff across most sites advised us that incidents were
discussed at handovers and team meetings.
The medical director was the chair of the Serious Incident Report Group (SIRG), which met
monthly and reported to the Trust Wide Clinical Governance Group. The SIRG scrutinised and
approved Serious Incident Reports before submitting them to the CCG for closure or downgrade.
The SIRG also monitored the delivery and effectiveness of corrective/mitigating actions and
preventative action plans.
Incidents across the trust were reported using the trust electronic recording system. Staff across all sites were trained how to identify an incident or a near miss and to use the system. We found that all staff we spoke with at all locations were confident to report incidents.
Staff at all sites were able to provide examples of incidents they had reported and their outcomes. They told us that teams and the organisation as a whole learned from incidents and there was evidence of clear action planning following reviews. We saw examples of this in the weekly ward meeting minutes. For example, at Midhurst Community Hospital, one root cause analysis identified the need for staff to ensure that pain relief was effective and to reassess pain. We saw the trust produced monthly learning from incidents newsletters these were displayed in staff rooms.
Ward managers at all sites were responsible for investigating incidents, however all managers we spoke with advised us they received support from the matron.
Staff we spoke with at all locations understood the term duty of candour and its meaning in practice and were able to give us examples on when it has been applied. The duty of candour is a regulatory duty that relates to openness and transparency and requires providers of health and social care services to notify patients (or other relevant persons) of certain ‘notifiable safety incidents’ and provide reasonable support to that person.
However, staff at Uckfield Community Hospital reported that they did not always get feedback from
incidents and that the quality of feedback was inconsistent.
The coastal inpatient senior team meeting minutes showed that learning from incidents across the
patch were discussed with learning shared and the June 2017 minutes reminded ward managers
to ensure all sites were documenting learning from incidents.
1 RPIR
25
At Arundel and District Hospital we saw a folder which detailed ongoing incidents and progress on
any action plans. This ensured staff were kept up to date on incident progression.
We found the incident culture at Arundel and District Hospital was open and honest and “Non-
Blame”.
Staff at Midhurst Community Hospital and LVH told us the most common incident they reported was patient falls.
At Horsham Hospital, we were given the example of how the incidence of completing of VTE assessments SCFT was a concern identified as a trend through incident reporting. The investigation and resultant action planning involved medical, nursing and pharmacy staff. The pharmacy staff worked with the ANPs and doctors to ensure that appropriate prophylaxis prescribing included the duration of treatment when patients were admitted from the acute hospitals following surgery. The incidence of VTE assessments had increased and the ward pharmacy team had seen an improvement in the number of charts detailing the length of time treatment should be continued for.
Staff on all four wards at Crawley Hospital advised us that lack of staffing made it difficult to have
the time to complete incident report forms.
We saw the root cause analysis for incidents on Viking Ward at Crawley Hospital and saw that
learning from all incidents had been implemented where appropriate. For example, a patient who
had fallen whilst trying to get out of bed had their call bell next to their affected limb and was
therefore unable to call for help. We saw staff had reminders on their comfort round forms to
ensure call bells were on the opposite side to an affected limb.
Therapists at Uckfield Community Hospital who were visiting from other trusts had access to the
incident reporting system and gave us examples of incidents they had reported whilst at the
hospital.
At Uckfield Community Hospital we saw that learning from incidents was discussed at handovers, in ward meetings and in the team briefing and that mortality reviews were regularly undertaken. At LVH, we saw it was documented in patients’ notes when an incident form had been completed
for the patient.
Is the service effective?
Good
Evidence-based care and treatment
Staff delivered care in line with best practise and national guidelines. We saw policies were
developed with regard to national guidelines. We saw evidence managers updated policies when
national guidelines were updated.
We saw that staff could access updated National Institute for Care Excellence guidance via the
trusts intranet system.
Generally, patient records showed the risk of falls was continually assessed in line with NICE
guideline CG21/161.
26
We saw policies and procedures followed AGILE guidelines. AGILE is a professional network of
the Chartered Society of Physiotherapy and is for therapists working with older people.
We saw evidence that all 10 sites followed the national sepsis six pathways.
Although the trust did not have a specific mental health assessment tool, appropriately trained
staff carried out an assessment of a patients mental state. The multidisciplinary team would then
create an individual care needs plan in line with best practise.
We saw at Lewes Victoria Hospital, staff had local systems in place to document identification of people approaching the end of life; this was in line with National Institute of Health and Care.
The trust had participated in 40 clinical audits in relation to this core service as part of their Clinical
Audit Programme.
We saw staff had access to trust policies and procedures via the trusts intranet. Staff we spoke
with could access the intranet and demonstrated where to locate policies. Policies we reviewed
gave reference to national guidelines and best practise and were within date for review.
At Crawley Hospital and Salvington Lodge we found that all inpatient wards had access to
computers, however staff advised us that the internet was not reliable and regularly dropped out.
Therefore, there were times when staff could not access online information when they required it.
Access to computers across the Bailey Unit at Midhurst Community Hospital was limited. There
was only one office that provided general access to computers, however there were plans to
reconfigure the space to allow for more computers to be available. Therefore access to policies
and procedures online could be an issue but hard copies were kept in the main office. The ward
manager and ward sisters kept these up to date. Clinical guidance was available in the clinic /
treatment room.
At Arundel and District Hospital, we saw hard copies of several policies and guidelines were past
their review date. When we questioned staff we were shown that the documents were correctly
updated online. Staff told us that the majority of staff reviewed policies online. However, there was
a risk staff may have followed out of date policies if they could not gain access to a computer. We
brought this to the attention of the ward manager who advised us they would update it
immediately.
Nutrition and hydration
The NHS National Patient Safety Agency ‘Protected Mealtimes Review’ studied the effects of enabling patients to eat their meals without unnecessary interruption by ensuring nursing staff stopped other duties and took the time to provide assistance to those patients unable to eat independently. Results showed that protected mealtimes reduced food waste and increased the levels of eating and drinking amongst patients. All 10 sites visited ensured patients received protected mealtimes. Across the trust we saw Malnutrition Universal Screening Tools (MUSTs) were fully completed and updated regularly. MUST is a five-step screening tool to identify adults, who are malnourished, at
27
risk of malnutrition, or obese and includes management guidelines which can be used to develop a care plan. All sites across the trust provided a variety of nutritional supplements available for patients in a
variety of different flavours. Soft and puree diets were also catered for.
Staff monitored patients input and output and offered drinks during comfort rounds. Comfort rounds took place every two hours at some sites such as Crawley Hospital (however they were done hourly at other sites such as Midhurst Community Hospital ) and allowed staff to monitor intake throughout the day. Staff at all locations advised us that if a patient’s food or fluid intake was low, this would be escalated to the nutritionist and speech and language therapist by early afternoon, rather than waiting until the end of the day. We saw training files that showed that all staff on the Stroke Ward at Crawley Hospital had to
complete dysphagia training before they were allowed to support patients with feeding and
drinking.
Bognor Regis War Memorial Hospital (BRWMH) had a dietician who attended the hospital one day
a week. Nursing staff completed MUST scores and referred a patient to the dietician if required.
We saw there was a protocol was in place for staff to be able to manage the patient intake in the
absence of the dietician. If a patient required continued dietetic input following discharge, the
dietician followed their care as they also worked in the community, therefore ensuring effective
transition.
At Lewes Victoria Hospital speech and language therapy and dietetic support was available from
the community if a referral was made. Staff did not report any issues accessing these services.
At Midhurst Community Hospital we saw posters giving advice to patients regarding eating, for
example, putting only a small amount of food in their mouth and chewing this thoroughly before
taking another mouthful. There was also information for patients on how to supplement their diets
with additional calories if required. For example, adding cream to their dessert, there was also
advice on how to reduce salt intake.
At Arundel and District Hospital we saw there was a board outside the catering department which listed each patient and their dietary needs, for example whether they required a soft diet, were diabetic, or required assistance. The dietician visited the hospital once a week, however they were available at any time if a patient required urgent referral. Horsham Hospital had a productive ward initiative that had been set up to improve patient safety
and outcomes. The focus at the time of inspection was on maintaining adequate hydration. This
focus was decided on as it had a significant impact on skin integrity, the level of urinary tract
infections and continence and patients’ cognitive state.
At Horsham Hospital we saw that there were posters and signs to remind staff to offer and assist
patients to drink. We observed staff offering drinks frequently and topping up water jugs outside of
the usual round time. Staff sat with and helped patients to drink using appropriate aids, when
necessary.
If patients at Salvington Lodge missed a meal for any reason (such as an appointment at the acute
trust or because they simply weren’t hungry) an alternative was provided. Patients were also given
the option taking a packed lunch with them. There were always sandwiches, soup and food such
as beans on toast available throughout the day on the ward.
28
Pain relief
We found that pain charts at Crawley Hospital were not fully completed. For example, on Viking
Ward we found that patients were asked during two hourly comfort rounds whether they were in
pain, which was answered either a ‘Yes’ or ‘No’. However, out of five patient records reviewed,
only one had a regular pain score, despite there being a check box on the comfort round form.
Therefore, staff were unaware of the level of pain these patients were in. We further reviewed the
patient record where pain had been given a score from 1-10 and found, despite the patient
complaining of sharp acute pain (10/10) at 8am, pain relief was not provided until the 9am
medication round, where the patient was still scoring themselves as 10/10. During the subsequent
morning and afternoon comfort rounds, the patient continued to express high levels of pain.
However, we found no evidence that a member of staff checked the effectiveness of the pain relief
as there were no further entries until the next scheduled medication round. We checked the
patient’s medical administration chart and found they were prescribed oromorph to be used ‘as
needed’ for pain relief. However, this was used sporadically and there was no correlation between
recorded levels of pain and the use of extra pain relief. On the days where the oromorph was used
there was no mention of a reason why in the administration chart or the patients notes. We noted
that ‘as needed’ medication was written up on a separate part of the administration form, therefore
staff were more likely to miss it. We also asked staff how they escalated concerns regarding a
patient’s pain relief and referred patients to a specialist team for pain management. Staff advised us
there was no formal process for referral and it relied on the staff member to escalate. This was
brought to the attention of the general manager at the time of inspection.
At Uckfield Community Hospital we saw ‘as needed’ pain relief was prescribed and readily available to patients. However, we found that pain assessments were not documented. There was also some concern with the way that ‘as needed’ paracetamol was being used in the unit. This related to the continuous administration of the maximum dose in most cases for a period excess of between 25-40 days without medical review. This meant there was no oversight of the possible risk of chronic therapeutic overdose in a high risk patient group. This was fed back to the ward manager and following inspection we were told; the pharmacy team were now conducting a medication review on admission and at regular points throughout the patient stay. They had added monitoring length of time of analgesia administration to this review in conjunction with review of the pain charts. The ward manager and her deputy were regularly auditing the pain charts. Across the other locations we found pain scores were documented regularly and it was clear to see when as required pain relief was given in response to an elevation in reported pain score.
Patient outcomes
Therapy staff measured patient outcomes using a variety of well known, validated tools to assess
the impact of treatment interventions. Patients were supported, where possible to return to their
previous level of independence through joint goal setting.
The trust was taking part in the Chartered Society of Physiotherapy (CSP) Hip splint audit 2017 for
fractured neck of femur. The audit was looking into improving quality and outcomes for patients
being delayed before entering a fractured neck of femur pathway. This audit was introduced after
CSP found the proportion of patients admitted to a multidisciplinary hip fracture program within
four hours of surgery dropped from 44% in 2015 to just 40% in 2016. At the time of this inspection
results from the audit had not been published.
Across all sites we saw therapists used the Lindop Parkinson's Assessment Scale (LPAS). The
LPAS is a validated, physiotherapy-specific function measurement tool used to assess the gait
29
and bed mobility of people with Parkinson's disease. Physiotherapists measured the score at the
start and end of treatment and measured the difference to assess the effects of treatment
intervention.
At Crawley Hospital we saw therapy teams using Therapy Outcome Measures (TOMS) as a way
of reviewing outcomes that works across occupational therapy (OT), physiotherapy (PT) and
speech and language therapy (SALT) and is widely used in the UK. The TOMS scale allows the
therapist to describe the relative abilities and difficulties of the patient in 4 domains, impairment,
activity, participation and well-being in order to monitor change over time. It can be used for both
treatment planning and auditing outcomes. We also saw Goal Attainment Scale (GAS) was used
across joint working between therapy teams and enabled patients and relatives to be involved in
setting goals. Staff worked with patients to identify goals to achieve in a timescale, for example;
walking independently with an aid in 3 weeks. Staff then reviewed the patient to see if the goal had
been met or exceeded. The therapy teams at all the units we visited at Crawley Hospital worked
together on shared goals.
On the Stroke Ward at Crawley Hospital, we checked five patient records and found all contained
relevant outcome measures and that these were reviewed regularly by the whole MDT to monitor
progress. Examples included; Postural Assessment Scale (PAS) which assesses and monitors
postural control after stroke. It contains 12 four-level items of varying difficulty for assessing ability
to maintain or change a given lying, sitting, or standing posture. Montreal Cognitive Assessment
(MOCA) which screens cognitive abilities such as, memory, attention, language and orientation.
Berg Balance Scale which measures balance, as well as many others.
At BRWMH, we saw all patients were assessed using Elderly mobility scale (EMS), which is a
scale used for assessment of mobility and considers locomotion, balance and key position
changes.
Staff at Salvington Lodge reviewed the percentage of goals attainment during therapy reviews.
These were audited every two weeks in order to track whether the unit was meeting KPI’s.
Competent staff
We saw staff were competent to perform their roles, attended regular supervision training and had
regular appraisals. Leadership development training was available to staff, which was encouraged
by managers. We spoke with staff who had attended the training and found it to be useful.
Staff were given a training passport in which all their training was recorded. Managers recorded
one to one clinical supervision and appraisals. A tracking system ensured staff kept up to date with
both. This was the most up to date record as the e-learning system had a time lag and did not
record training in real time.
The learning needs of staff were identified from incident feedback and from one to one supervision. Ward managers arranged specific training based on this feedback. For example, Arundel and District Hospital held a ‘security and conflict’ supervision session in August 2017 as they had identified this as an area where staff required further training. New staff had a six week induction and a period of supernumery work to ensure competence. We spoke to a new starter at one hospital who told us they felt well supported. At the time of inspection, the trust was running a development programme for band 6 staff to
develop their management skills. We spoke with band 6 nurses and band 6 therapy staff who were
on this course and felt it was beneficial.
30
At the time of the inspection the matron at Arundel and District Hospital had just attended further training in management ‘Leadership Masterclass’, she felt it was useful and that training was encouraged by the trust.
There was a local induction process for agency staff at The Kleinwort Centre, however when we
checked the last two week’s records, we found five staff out of nine did not have a completed
induction checklist on file. There appeared to be no formal governance or assurance around this
system, although the lead administrator did make some checks.
On Don Baines ward at Bognor Regis Hospital, 100% of staff had an appraisal within the last 6 months, which was better than the target of 94%. At Crawley Hospital, we saw that band 3 staff on Viking, Stroke and Caravelle Wards were supported through a six month development programme to move to band 4. At Crawley Hospital, we saw that during as part of supervision, staff were able to request specific training in areas where they felt they needed further support. For example, a member of staff had received extra training in dealing with physically and verbally challenging patients.
Staff on Piper Ward at Crawley Hospital had access to ‘Skills Sharing Workshops’ where staff took
it in turns to share knowledge and understanding. Staff advised us they enjoyed these sessions as
they promoted team work and gave staff the opportunity to promote their knowledge which they
could use as evidence during supervisions and revalidation.
On Viking Ward at Crawley Hospital, we saw that every Friday there was sepsis awareness training,
run by the advanced nurse practitioner. Staff advised us they found this useful in that it kept sepsis
at the forefront of their minds and gave them an opportunity to ask questions.
At Midhurst Community Hospital, we were shown a diary that was kept on the ward, and was accessible to all staff which showed which member of staff had responsibility for tasks across a shift including who they were caring for and when staff were due to take a break. This meant that everyone was accountable and should therapy staff need to get information about a particular patient, they would know which member of staff to contact.
In the ward managers office at Midhurst Community Hospital, we saw that there was a board,
which showed a list of all the staff, their mandatory training records, the date the staff members
personal development plan (appraisal) was due. There was also details on when Nursing and
Midwifery Council (NMC) revalidation was due.
The ward manager at Midhurst Community Hospital advised us they were supported in their
revalidation by the matron through fortnightly 1-1 meetings and the practice development team
based at the trust headquarters. This support was provided to all nursing staff going through the
revalidation process.
Staff at Uckfield Community Hospital advised us, clinical supervision was an informal process and that they would like this to become more formalised to ensure past issues were discussed and development opportunities were not missed. However, staff on the ward advised us that appraisal was undertaken in line with trust policy. All staff we spoke with advised us they had received an appraisal this year and felt the process was positive and worthwhile. The matron at Uckfield Community Hospital had arranged for staff to attend palliative care courses
as part of providing end of life care.
31
All nursing staff at Lewes Victoria Hospital (LVH) had completed the care certificate and we saw
certificates which confirmed this. We also saw medical devices competencies were kept in a
folder. Ten out 10 we looked at had completed competencies in the last 12 months, which was in
line with the medical devices policy dated 2016/9.
Staff at LVH told us they completed regular clinical supervision. We saw 10 records of clinical
supervision, which indicated staff were completed clinical supervision sessions every four to six
weeks in line with their clinical supervision contracts.
The advanced nurse practitioners at BRWMH hospital advised us they could prescribe, however
they were unable to request x-rays and CT scans.
Staff at Salvington Lodge advised us they were unable to cannulate or access the intravenous (IV)
team. Therefore, the ward was unable to admit patients who were on IV or long term antibiotics.
On all sites bank and agency staff were given a local induction on their first visit. This covered
emergency plans how to answer the call bell system, familiarisation and orientation to the unit.
Staff across the trust advised us that dementia training was not mandatory, although it was
available to all staff. In all locations we visited, we spoke with staff who had accessed training. At
the time of inspection, dementia training was being reviewed, including clarification of what level of
training was mandatory for each role. Dementia awareness training was to be included on the trust
statutory training day from April 2018.
The trust did provide data split down by staff group. Data in the RPIR indicates that the trust’s year to date (April and May 2017) appraisal rate for all permanent non-medical staff in this core service was 89.5%, compared to their target of 90%. A high completion rate in two months could indicate a rolling target rather than all appraisals have been completed in two months2.
The trust did provide data split down by staff group. Data in the RPIR indicates that the trust’s year to date (April and May 2017) appraisal rate for all permanent medical staff in this core service is 89.5%, compared to their target of 90%. A high completion rate in two months could indicate a rolling target rather than all appraisals have been completed in two months3.
Multidisciplinary working and coordinated care pathways
We found multidisciplinary teams worked coherently at each location we visited.
A weekly MDT meeting was held at all sites, which was attended to multi-agencies which included, GP, dementia specialist, carer support agency, therapy staff and health care assistants.
Multidisciplinary working (MDT) between therapy services at The Kleinwort Centre and Horizon
unit were effective as they shared an occupational therapy lead and a physiotherapy lead.
Therefore, the two sites worked closely together to ensure the physical and occupational needs of
patients was met.
At The Kleinwort Centre, although there was no specific mental health input into the MDT, the unit
had a dementia nurse and staff would together to assess the mental health needs of patients.
Staff handovers at Arundel and District Hospital took place at the bedside; this allowed patients to
interact with new staff taking over and gave them an opportunity to input into how they were
feeling and contribute to treatment planning.
2 RPIR
3 RPIR
32
At Arundel and District Hospital we witnessed a MDT meeting which was inclusive of all staff, and we saw staff able to challenge and that the patients’ needs were fully discussed including in a holistic and joined up way. Ongoing care, family and those close to them and their needs were also discussed. We saw arrangements for working with social workers and social care providers to help plan and deliver care, treatment and other support to people in a holistic and joined up way. For example by setting goals for patients and estimated date for discharge.
We observed handover at Bognor Regis Hospital and saw patient’s needs were clearly
communicated. There was also clear discussion of discharge planning and appropriate pathways.
New admissions were discussed fully including; physical needs, cognition, social situation,
accommodation and any need for care packages. We also observed two patients initial
assessments which were positive for patients. All areas of rehabilitation were covered using
objective and subjective measures and included the full therapy team.
The staff at Midhurst Community Hospital were supported by a group of volunteers who visited the unit weekly to undertake social events with patients. Staff reported a “Fantastic” relationship with the volunteers.
Staff at Uckfield Community Hospital advised us they had a good working relationship with staff in
social care and that the social worker lead dialled into the weekly MDT meeting. However, staff on
the unit also advised us there was mixed input from the GPs. They recently had gained access to
a consultant geriatrician, which staff were hoping would an improvement in the level of medical
input.
The therapy staff at Midhurst Community Hospital were proud of the MDT as it supported a rehabilitation model of care rather than medical. The meeting brought together all the different agencies to support the rehabilitation of patients. There was also a twice weekly MDT call where patients being discharged from the acute hospitals would be discussed.
There was a daily whiteboard meeting at midday at Midhurst Community Hospital, where patients were discussed. This meeting was observed and we saw how one member of staff was updating the computer system while one was updating the whiteboard to ensure that the information correlated. The acuity of patients was discussed as was there discharge and medication regime. This was noted to be well managed and effective.
A ‘Safer transfer of care’ meeting had been implemented at BRWMH in order to review the process of transferring patients from local acute trusts to inpatient locations in West Sussex. Staff who attended the meetings advised us both SCFT and the local acute trusts were able to provide effective criticism and feedback to each other about referrals sent, received and rejected.
Health promotion
We saw at multidisciplinary meetings staff reviewed patients’ needs fully in a holistic manner.
Ongoing care, family and those close to them and their needs were also discussed.
On admission to each unit staff spent time with patients to explain the process of their
rehabilitation and agree expectations. We saw patients were fully involved in setting their goals,
which meant their goals were realistic and achievable.
We saw staff took the time to understand patients’ lifestyle prior to admission and where
appropriate, went to lengths to ensure patients could achieve their previous potential.
We saw assessment of patients on admission identified if any additional support would be
required. This was then discussed at MDT’s so the appropriate support could be offered.
Consent, Mental Capacity Act and Deprivation of Liberty Safeguards
33
Staff had a good understanding of the Mental Capacity Act, 2005 and there were good systems in
place to assess a patient’s capacity to make decisions about their care. We saw documentation
was completed when these assessments were carried out.
The trust’s RPIR data shows that there were 48 deprivation of liberty safeguard (DoLS)
applications made to the local authority between April 2016 and March 2017. All of the DoLS
application were made by community inpatient service locations.
The greatest number of DoLS applications were made in February 2017 with eight.
The trust’s RPIR data shows that they sent 28 direct notifications to the CQC regarding their DoLS
applications. All DoLS applications should be sent to CQC in the form of a direct notification.
At Crawley Hospital we were given an example of how the ward had used the Deprivation of
Liberty Safeguards (DoLS) process. Ward staff worked with social services and a local psychiatric
hospital to ensure the patient received the right care at the right place. There were also able to
help the patient move back to another part of the country once they had completed their treatment.
At Midhurst Community Hospital, a multidisciplinary team consisting of occupational therapists, the
ward manager and a GP from the local GP practice carried out Mental Capacity Act (MCA)
assessments. Patients who were assessed as a falls risk or who had a tendency to walk would be
assessed under the Deprivation of Liberty Safeguards (DOLS) if measures needed to be put in
place.
Staff at Arundel and District Hospital understood their role and responsibilities regarding restraint.
We reviewed a patient who had a DoLS in place. The patient’s records clearly showed a MCA
assessment had taken place and the DoLS implemented in the best interest of the patient. As a
result of the DoLS, staff had alarmed ward doors in order to alert staff if doors were opened.
At LVH we saw examples of consideration of DoLS. We saw therapy and nursing staff always
sought consent before undertaking any activity and this was documented in the patients’ notes.
At Horsham Hospital, we saw one patient’s records where the patient had asked not to have their
relatives informed of their admission; this was recorded and respected, demonstrating that staff
understood their responsibilities in protecting patient’s confidential personal information.
However, at BRWMH, one patient on the ward was diagnosed with Alzheimer’s. Staff advised us
they had capacity and insight into their diagnosis; however we found no evidence of a capacity
assessment in their notes.
In addition to this, the abbreviated mental test (ABMT) score and confusion assessment method
(CAM) form part of falls risk assessment. The ABMT was not completed in three out of five sets of
notes reviewed and the ‘Do I need a mental capacity assessment?’ question was left blank on two
out of five records we reviewed. Finally the ‘Mood’ questions on assessment were not completed
on any of the five records we reviewed.
At Salvington Lodge we saw evidence of consent documented in the daily nursing and medical
documentation, however it was not routinely recorded.
Is the service caring?
Outstanding
34
Compassionate care
Staff were clearly driven to provide their patients with compassionate care. Every staff interaction
with patients we saw was carried out with kindness and respect. Staff spent as long as they
needed to with patients.
Patient Led Assessments of the Care Environment ( PLACE) are undertaken by teams of NHS
and private/independent health care providers, and include at least 50 per cent members of the
public (known as patient assessors). They focus on the environment in which care is provided, as
well as supporting non-clinical services such as cleanliness, food, hydration, the extent to which
the provision of care with privacy and dignity is supported and whether the premises are equipped
to meet the needs of people with dementia against a specified range of criteria.
The 2017 PLACE score for Privacy, dignity and wellbeing at the trust was 77.5%%.
Only one of the 11 locations scored in line with or better than the England average4.
Site Name Privacy, dignity and wellbeing
Arundel And District Hospital 70.14%
Bognor Regis War Memorial 81.43%
Crawley Hospital 86.35%
Crowborough War Memorial Hospital
76.73%
Horsham Hospital 81.97%
Kleinwort Rehabilitation Unit 70.71%
Lewes Victoria Hospital 73.55%
Midhurst Community Hospital 81.15%
Salvington Lodge 80.36%
Uckfield Community Hospital 66.67%
Zachary Merton Hospital 83.62%
Trust Overall 77.52%
England Average 85.87%
At all 10 sites visited during the inspection we saw staff interact with patients and visitors in a kind,
caring and friendly manner. Staff knocked on doors before entering a room.
We spoke to 53 patients and 10 relatives who all told us that the care they received from all staff
was excellent and that patients felt safe and cared for during their stay. Staff were respectful of
their needs and preferences and took time to understand personal requirements or to explain the
care being administered. One patient at Midhurst Community Hospital told us “every whim is
catered for here”. At Arundel and District Hospital patient comments included “It’s like a hotel”, “It
feels like it’s one big family here” and “I have been well looked after”. At Uckfield Community
Hospital comments included “First class care, couldn’t ask for better. All staff are wonderful right
down to the cleaners”. Patients at Lewes Victoria Hospital (LVH) said “It feels just like home” and
“Nothing is too much trouble”. Patients at Horsham told us they didn’t want to go home because
they received such good care at the hospital.
4 PLACE
35
During the inspection, we saw extensive and proactive engagement between staff and patients to provide rehabilitation programmes. Patients told us that they were encouraged to be as independent as possible but staff provided appropriate assistance in a sensitive way. The Bailey Unit at Midhurst Community Hospital had received 17 plaudits in August 2017. We saw 18 thank-you cards displayed which included comments “Thank-you so much for your care and attention we were well looked after” and “Many thanks for looking after my mum so beautifully”. Other comments from patients included “Its lovely here, no complaints, nurses lovely and there is a great choice of food”.
During the inspection, the friends of Midhurst Community Hospital were visiting the Bailey Unit.
We saw that the patients were playing various games, were being treated with compassion and
were clearly enjoying their interaction with other patients and the friends that were there.
We saw many examples of staff going “Above and beyond” in terms of caring and supporting
patients. For example, on Caravelle Ward at Crawley Hospital we spoke with a patient who
required new furniture at home but had to wait for family to organise this before he was able to be
discharged. As he was very eager to go home, staff supported the patient to find what he wanted
online in order to speed up the process and enable him to return home earlier.
Staff at BRWMH had used their own funds to provide clothes for a patient who was admitted to the
hospital with only the clothes that she was wearing.
At Zachary Merton Hospital (ZMH), a healthcare assistant described giving up two of their days off
to help a patient (living with dementia) attend a specialist dental appointment as the patient’s
family were unable to attend and the patient had already waited several months for the
appointment. Staff also took patient’s clothes home to repair and a therapist assembled new
garden furniture out of working hours in order that patients could take advantage of the good
weather.
One healthcare assistant at Salvington Lodge had finished their shift but stayed on an additional
three hours to settle a patient who was returning from the acute trust and who was tired and
distressed. We also saw a healthcare assistant provided manicures and nail polish to patients in
their own time and at their own expense.
Staff at the Horizon Unit welcomed patients’ pets to the ward. One patient who was receiving end
of life care had been able to have his two dogs visit until he died; staff advised us how important
this was to both the patient and their family.
A patient at Uckfield Community Hospital who was end of life had indicated their preferred place of death as their own home. The patient was very weak and required transport to their home. However, the ambulance crew did not feel confident they could meet the patients individual moving and handling requirements. The matron made sure the ward area was safely staffed, and with the help of the senior physiotherapist, travelled with the patient to ensure the patient was successfully transferred. Staff at LVH advised us that a patient, who was independently mobile and ready to be discharged home, was nervous about walking around his village as his confidence was low. Once the patient had been discharged, although this was not part of the service provided, staff visited him and accompanied him around the village to improve his confidence and enable him to return to his normal activities.
36
Staff at Arundel and District Hospital advised us they had organised a wedding blessing for a
patient who was unable to leave the ward, and that staff members gave out roses to female
patients and chocolates to male patients on St George’s day.
Staff on the Bailey Unit organised event days to celebrate special occasions or different times of the year. For example, they had a Wimbledon themed party and an August bank holiday party. A seaside theme was created for the August Bank Holiday party with fish and chips, hook a duck, rock, sand castles and ginger beer.
On Piper Ward at Crawley Hospital, we spoke with one patient that had had an extended period of
rehabilitation on the ward. They had returned to visit the staff that had cared for them during their
stay. They described the care they had received as “Amazing, all staff were great and the care I
got was really individual”. They told us how they had been concerned about going to the hospital
for rehabilitation but the level of care from the staff had stopped those concerns. We heard how
staff had considered the needs of the patients’ family as well as their own. We observed genuine
warmth between the patient and all of staff they came into contact with. They also told us how the
ward had managed their transition back home and the aftercare had also been “Amazing”.
Patients on all four wards at Crawley Hospital advised us that the care was excellent, that call
bells were answered quickly and the staff treated them with respect. This was despite the fact that
on every ward patients commented that staff were very overworked.
However, we saw staff on Viking Ward at Crawley Hospital take blood from a patient whilst the
curtain to their bay was open. This was immediately brought to the attention of staff who drew the
curtain when requested.
Emotional support
We saw staff always considered carers emotional needs in addition to patient’s emotional needs.
In addition to accessing counselling services for inpatients, staff were knowledgeable about
services patients and careers could access outside of the trust.
Patients across all sites had access to chaplaincy services and support was provided for numerous religious identities.
We saw all healthcare staff across the trust were keen to ensure that patients’ needs were met and that they were comfortable. It was evident that this mattered to staff.
Patients at Midhurst Community and LVH told us volunteers were able to provide support to them and it was good to have someone else to talk to. A Pets As Therapy (PAT) dog visited the unit fortnightly. Research shows PAT dogs can aid recovery and relax patients as well as providing interaction and companionship.
Staff at Arundel and District Hospital provided patients and families with information leaflets and
written information. We saw information being explained to a patient before they were discharged.
At Arundel and District Hospital we witnessed the needs of carers as well as patients being discussed at the MDT meetings. This meeting also had a representative from ‘Carers Support West Sussex’. At Uckfield Community Hospital we saw there was bereavement and loss counselling service
information available.
Staff at BRWMH were aware of bereavement services and carers support within the local
community. They told us they worked closely with the mental health team to provide support for
bereaved patients and their families.
37
Understanding and involvement of patients and those close to them
Patients were at the centre of everything staff did, which was consistent across the trust. Staff
supported patients to manage their own health, care and wellbeing and to maximise their
independence.
We saw patients and their families were encouraged to attend family meetings. Staff worked to
ensure patients, their carers and relatives understood and agreed with the treatment and
treatment sessions.
We saw staff at all locations explaining procedures to patients using everyday language they could
understand. Staff ensured patients and their families knew what was happening next in terms of
procedures or discharge before they left the patient.
Patients across all sites were seen to be at the centre of the action and involved in a very positive culture. Staff told us that they tried to ensure patients were involved in their care and events on the unit.
Patients across the trust were supported to manage their own health, care and wellbeing and to maximise their independence. We saw staff taking the time to enable patients to complete tasks on their own without feeling rushed. All inpatient services involved family and carer's in discharge planning to ensure the patient had the correct competencies to carry out tasks at home. This was done with the help of the Occupational Therapist and Physiotherapist. At Salvington Lodge, patient’s families were given a telephone number for contacting therapists if
they wanted to talk to them but were unable to be on the ward during therapy sessions.
We saw staff within the therapy team on Stroke Ward at Crawley Hospital used picture
communication charts to ensure patients understood what was going to happen during their
therapy session. We also saw other staff on the ward used the cards to support communication
with patients to ensure they could make their own choices. For example, when choosing what food
to eat or clothes to wear.
We spoke with patients at Crawley Hospital who were due to be sent home with medication. They
understood why they were taking each medication, when they should take it as well as any side
effects to look out for. All patients we spoke with said they were kept informed by staff and felt
comfortable to ask questions.
Patients at Midhurst Community Hospital confirmed that their care plans had been explained to them and that they understood and agreed with the content and what their goals were.
During the inspection, we were told about a patient at Midhurst Community Hospital who was ready to be discharged home and how the team had to build the trust of the family members who would be caring for them. This meant the social worker and ward manager met with the family to explain the care that the patient would need following discharge. This ultimately led to the patient being discharged home.
At Arundel and District Hospital we witnessed a healthcare assistant explaining to a patient that
they were taking him for a shower, we witnessed a caring attitude from the staff member and she
encouraged him to use available equipment to mobilise whilst explaining the benefits of this.
38
Patients were involved in planning and making decisions about their care. We spoke with an
occupational therapy technician at Arundel and District Hospital who explained they undertook
access and home visits that involved families and patients. They used the visits to not only assess
the patient’s home environment, but allow patients and their families to ask questions in a familiar,
non-clinical environment.
Staff at BRWMH showed us the details of family meetings within the patient record. This was
where relatives had the opportunity to discuss goals with the patient and staff. However, staff
advised us family meetings were often organised when goals were not realistic. Because of this
staff ensured a band six nurse or nurse in charge attend the meeting as well as therapy staff.
Is the service responsive?
Good
Planning and delivering services which meet people’s needs
The service had admission criteria. Teams had been established to work with acute hospitals to
ensure admission criteria were followed in order to prevent a patient being returned to hospital. On
admission assessments were carried out to identify what steps were required to aim for a patient’s
discharge.
The trust was asked to let us know about any ward moves for a non-clinical reason during the last
12 months. For example if a patient has to move wards several times because there is no room in
the speciality ward they should be on. The trust confirmed that they had no bed moves.
The trust were asked to list ward moves between 22:00 and 08:00am for each core service for the
most recent 12 months. The trust confirmed that they had no bed moves at night.
Mixed Sex Breaches are defined by CQC as a breach of same sex accommodation, as defined by
the NHS Confederation definition. Also included is the need to provide gender sensitive care,
which promotes privacy and dignity, applicable to all ages, and therefore includes children’s and
adolescent units. This means that boys and girls should not share bedrooms or bed bays and that
toilets and washing facilities should be same-sex. An exception to this might be in the event of a
family admission on a children’s unit, in which case brothers and sisters may, if appropriate, share
bedrooms, bathrooms or shower and toilets.
The trust confirmed that they have had no mixed sex breaches.
The largest ethnic minority group within the trust catchment area is White: Other White with 5.24%
of the population. Please note this is trustwide data rather than core service specific.
Ethnic minority group
Percentage of catchment
population
(if known)
First largest White: Other White 5.24
Second largest Asian/Asian British: Indian 1.21
Third largest Asian/Asian British: Other Asian 1.12
Fourth largest White: Irish 1.00
39
Patients across the trust were admitted on a step up basis (from the community or GP referrals),
or a step down (discharge from local acute trust). Staff indicated on the handover board which
criteria each patient fell into.
The trust had a ‘Capacity and resilience team’ based within local NHS acute trusts. Their role was to oversee referrals and ensure patients were referred to the most appropriate setting. There were two pathways for patients; an active rehab pathway and a sub-acute medical pathway. Patients on the latter could expect a longer stay in hospital.
None of the inpatient services were on sites with accident and emergency facilities. Therefore,
wards only admitted patients who had low risk of needing emergency treatment.
The trust had a patient flow and improvement programme in operation. This meant there was senior management oversight of capacity and flow.
The patient flow manager at Crawley Hospital reviewed capacity across community services and
monitored the flow of patients in and out of external hospitals and the community. They also
reviewed patient length of stay twice weekly to ensure flow through the hospital was effective.
We spoke with staff from the capacity and flow team. They told us they were responsible for
ensuring flow out of community beds back into the community and the flow from the acute trusts to
the community beds. We were told they had good relationships with the local social services as
well as those in neighbouring authorities. At the beginning of every day, the team would look at
what beds were available and the planned discharges from the acute hospitals. The local acute
hospital would also check to see what bed spaces were available. Either a male or female could
occupy side rooms that were free. The team assessed patients’ medical files and screened them
to ensure the patient was appropriate for a community bed. If any issues were identified, the team
ensured that there was a management plan in the event that a patient deteriorated. When a
patient was admitted to the ward, they started with a 28 day estimated departure date. This
allowed time for a welcome meeting to happen and the therapy teams to understand the patients’
needs. Patients that had a continuing rehabilitation plan upon discharge were seen by the
community in-reach team to see how they could assist the patient.
At all sites visited we saw posters which detailed what the different coloured staff uniform
represented.
The trust provided clear admissions criteria, however staff we spoke with at Arundel and District ,
and Crawley Hospitals said patients admitted from hospital often had need than those originally
stated in the admission plan.
The ward manager at Midhurst Community Hospital told us how, since the ward had re-opened, they had not had cause to refuse patients through lack of staff. However, there had been isolated cases where they had delayed a patient’s admittance due to their acuity and the need to have the right skill mix of staff.
The staff nurse at Arundel and District Hospital reviewed the daily referral list as there had been inappropriate referrals in the past. For example, a patient prone to walking off the unit had been admitted inappropriately. As a result the service had to close beds until a transfer could be arranged as the hospital was located near to a fast A-road. We also witnessed a patient living with dementia who had arrived the day of inspection. Staff felt he was unsuitable to be in the hospital environment. We highlighted this to the ward manager and a member of the capacity and resilience team who advised us that extra staffing was being considered to help care for the
40
patient’s needs. This further highlighted what staff had been telling us that there was a disconnect between the referrals and what the service could handle. The matron we spoke with on the morning of inspection advised us there were no issues with inappropriate referral, however five staff members on the ward highlighted it as an issue Ward areas at Uckfield Community Hospital had patients boards, which tracked their journey through their pathway, care bundles and discharge progress. We saw staff use this information in order to update the clinical commissioning group. There was an multidisciplinary team ( MDT) meeting every Monday which included adult social care input.
The inspection team had concerns about flow at Uckfield Hospital as data showed there were
empty beds on the ward when the local acute hospital was on red alert. In order for the hospital to
accept a patient, it needed to be agreed by a GP, nurse and physio. However, there were issues
with accessing GPs or finding GPs were not helpful if the patient was from outside of their area. At
the time of inspection, the matron was looking at setting time frames with GPs when accepting
referrals. Also, the average length of stay was long at this unit, in comparison to other sites within
the trust (between 24 and 28 days). Staff advised us that due to Uckfield Community Hospital
being located in a rural area, it was difficult to get adult social care staff to provide home care
packages.
At the time of inspection the trust was implementing a ‘Let’s get you home’ policy which kept
patients informed of the planned date of discharge.
Managers at Salvington Lodge had informally trialled a six day therapy service, which was very
popular with patients but currently on hold as there was no funding and the hospital had been
using resilience money for this previously. Staff had audited the impact but told us it did not
accurately reflect improvements due to the comorbidities of patients at the time of auditing.
However, we saw patient experience surveys were very positive regarding weekend workings.
Patients living with dementia at Arundel and District and Crawley Hospitals had open visiting
hours. We spoke with families who told us they appreciated this as their relatives lacked
awareness of time of day and meant they could be flexible and visit when it suited them.
The Bailey Unit displayed visiting times but staff advised us they would not turn away visitors who wanted to spend quality time with patients or those who came to help around meal times. Physiotherapists and occupational therapists at Arundel and District Hospital found it frustrating
that there was a podiatry clinic which could only be accessed through the physiotherapy gym. Staff
told us this affected patient dignity and privacy.
Therapy staff across the trust told us how they planned the discharge of patients and what they considered. The therapists visited the patient’s home to get an accurate picture of where they are returning to. They reviewed basic kitchen skills and assessed what equipment would be required.
Therapists at Salvington Lodge received administration support one day per week who input data
of outcomes. This meant therapists had time to deliver therapy sessions to patients.
At Arundel and District Hospital, the advanced nurse practitioner (ANP) worked Monday to Friday,
from 9am to 5pm. There was GP cover from Monday to Friday, occupational therapy and
physiotherapy was available Monday to Friday from 9am to 5pm. Out of hours cover was provided
by an out of hours GP provider.
Meeting the needs of people in vulnerable circumstances
41
We saw staff took account of patients’ individual needs, particularly for patients with dementia,
learning disabilities, and mental health problems. Environment and equipment was available to
cater for individual needs.
Staff identified patients’ preferred method of communication prior to admission, so appropriate
equipment or interpreters could be made available. Leaflets were available in other languages,
large, print, braille, and easy read. Communication devices were also available for patients who
had difficulty with the written word.
Kitchen staff at all sites were able to cater for different cultural dietary requirements, for example halal. Personal dietary choices were also taken into consideration and menus across the trust provided vegetarian and vegan options.
Comments regarding the quality and variety of food included “Excellent quality of food” and “Mum is fussy with food and is always offered alternatives”.
At Uckfield Community Hospital we spoke with one patient who had only ever eaten raw
vegetables. However, their diet had been reviewed by the dietician and was catered for by the
kitchen staff. Another patient reported that they didn’t feel the food was good enough for diabetic
patients as staff always put sugar in the porridge so patient had to have something else.
The occupational therapy team at Midhurst Community Hospital encouraged patients to attend the Breakfast Club to encourage independent living. Patients could use kitchen for the assessment of daily living. Therapy staff and volunteers also ran a variety of weekly exercise classes to encourage movement, mobility and to build strength.
The dining room at Midhurst Community Hospital had clear signage with a knife and fork to show that was where patients would go to eat. There was a day room adjoining the dining room which had a TV with subtitles. A large board with the time, date and weather for the day on it. All of the signage was clear, in vivid colours and designed for patients living with dementia.
Midhurst Community Hospital had a self-contained kitchen where therapy staff held ‘breakfast clubs’. This enabled patients to practice using equipment to make their breakfast in preparation for discharge home.
There was a day room on the unit at Uckfield which staff used to encourage communal dining. Use of this area was promoted to encourage a normal routine for patients as part of their rehab and as a method to avoid isolation.
Patients at Bognor whose first language was not English had access to a communications chart for food which has pictures of different types of food that they could point to. Staff advised us this was an effective tool for quick communication.
Staff across all sites received information regarding a patient’s ability to speak English prior to admission to the ward. Therefore, staff were able to put interpreting services in place. Staff at all locations knew how to access the telephone interpreting service, which was available 24 hours a day, seven days a week.
All trust leaflets on support services were able to be ordered in large print, braille, easy read, audio
tape and in other languages on request.
All sites across the trust were signed up to the Butterfly Scheme. This is a hospital care response
to people living with dementia, but also supports people with other forms of cognitive impairment.
Since our last inspection the trust had installed dementia friendly signage across all of its inpatient
wards. This meant that facilities were clearly labelled in large writing and also provided a picture.
42
Dementia friendly signage has been shown to reduce the number of falls as patients are less likely
to wander and open doors to check what is behind them.
During mealtimes across all sites we saw red trays in use. This was to indicate to staff that the
patient required additional support when eating and drinking. During mealtimes we saw that all
patients with a red tray had a member of staff assisting them with their meals.
Patients living with dementia were supported at Midhurst Community Hospital as they did not choose their food until three hours before the mealtime. This meant they could choose something they wanted at the time rather than remember a choice from the day before. We also saw Twiddle muffs were available for patients who were living with dementia or were agitated and the quilts on patient’s beds were different colours to assist those patients living with dementia find their own bed.
Staff at Uckfield Community Hospital were able to provide patients with additional care needs with
one to one care as staffing on this unit was not an issue. In addition, the hospital provided
coloured coded cutlery, crockery, toilet seats, were available to patients living with dementia,
which was in line with best practice. As well as a reminisce interactive therapy and activities
(RITA) system played music and videos from the past to help facilitate conversations between
patients, staff and families were available for those who were diagnosed with dementia.
Bariatric patients at Crawley Hospital had access to services and equipment. We saw patient
records that showed equipment was received within a day of ordering. We also saw that staff
numbers were increased when a bariatric patient was due on the ward to provide extra assistance.
At one end of the Piper Ward at Crawley Hospital, there was a day room / chat room where
patients could go, away from their bed. There was a large TV in this room as well tables, chairs
and a small kitchen area. There was also a staff room, a quiet room, where staff could have
private conversations with relatives. The ward also had a therapy room and a small gym to aid the
rehabilitation of patients. Signage on the ward indicated which room was which was large, with
vivid colours. However, the signage at the entrance to each bay was all the same. This could have
caused confusion for any patients living with dementia. We were told that the signage was subject
to review.
The Horizon Unit at Horsham Hospital had a self-contained ‘flat’ where patients could spend some
time before discharge caring for themselves with oversight or minimal assistance from the ward
staff. This was very much a step down from ward based care and an intermediate step before
patients returned to their own homes.
The Bailey Unit at Midhurst Community Hospital had a family room. There was a sofa bed, small kitchen area and patio doors leading to the garden. This room had been used for relatives of patients who were approaching the end of their life. Relatives could stay in this room overnight if they wanted to. The family room could also be used for patient assessments to establish if the patients could make themselves a drink or prepare food. The room was used to have difficult discussions with relatives as well as ‘best interest’ meetings.
There was a gymnasium available for use by patients on the Bailey Unit at Midhurst Community Hospital. However, this was quite small and was shared with the outpatient department of the hospital and was therefore not always available.
On discharge from LVH, the pharmacy team gave patients a medicines reminder card. This was
printed on yellow paper, in large print and detailed patients’ medication and details of how and
when it should be taken.
43
All sites provided contact details of local places of worship including churches, synagogue and mosque.
All patients at Arundel and District Hospital received a welcome meeting within 24/48 hours. This
was noted on the handover board in the staff office and if had not been completed it would be
allocated.
All areas of Arundel and District Hospital, Horsham Hospital and Uckfield Community Hospital were wheelchair accessible and we saw rails in bathrooms and showers along with hoists. There were also hoists available for use by physios and OT. Staff at Arundel and District General Hospital used pictorial flashcards for patients who are hard of hearing. There was also access to a hearing loop. Reminiscence therapy was available at Salvington Lodge once a week for two hours. However, this was the only activity available to patients within the unit. Arundel and District Hospital had taken part in a research trial with ‘Wishing Well’ reviewing the use of music therapy with patients living with dementia. All staff advised us this had a really positive impact on patients however the scheme was due to end due to funding. We were advised the hospital had hoped to gain funding from the ‘Friends of Arundel Hospital’ however; communication between the two had broken down when the ‘Friends of Arundel Hospital’ group voted that only patients who were from Arundel should receive funding. The matron advised us they were looking to address the issue at a meeting due to take place the week following the inspection, however, they advised us there were ongoing issues between the two groups. The patio area outside the family room at Midhurst Community Hospital had no line to demark it from the path. There was a small step that would be difficult for those with a visual impairment to see. During the inspection we saw a visitor stumble on the step. This was brought to the attention of the ward manager who said it would be raised with the contractor.
Access to the right care at the right time
Between June 2016 and May 2017 there were 466 delayed discharges within this core service.
This amounted to 11% of the total discharges.
Site Name Number of
discharges
Number of
delayed
discharges
% of
delayed
discharges
Arundel Ward.1 223 25 11%
Bailey Unit 127 5 4%
Caravelle 351 38 11%
Don Baines 339 21 6%
Harlands 149 28 19%
Horizon 437 47 11%
ICU Crowborough 232 73 31%
ICU Lewes 330 70 21%
Kleinwort 323 38 12%
Leslie Smith 286 19 7%
Offington Ward 238 16 7%
Piper 94 14 15%
Stroke Rehab 216 26 12%
44
Swanbourne 335 19 6%
Viking 406 27 7%
Staff at Salvington Lodge advised us that discharge was often delayed due to issues finding
adequate adult social care services in the rural areas surrounding the hospital.
From June 2016 to May 2017 the average bed occupancy in community inpatients was 90.3%.
The lowest was at Uckfield Community Hospital at 73.4% and the highest was in Salvington Lodge
at 95.2%.
The average length of stay was 27.4 days across community inpatient services. The longest was
in The Kleinwort Centre at 35.5 days and the shortest in Piper ward at Crawley hospital at 22.5
days.
The average length of stay at Midhurst Hospital for community inpatients was 19 days. Data on re-admission was not kept. It was explained that it was not possible to accurately record readmission data due to patients being admitted for different conditions. It was also considered that the time period between discharge and re-admission was variable so it was not possible to say if the readmission was linked to the previous discharge.
At the time of inspection, the average length of stay at Lewes was 23 days. On discharge from hospital, staff could access the joint community rehab team for a six week reablement package of care. Following this, patients were referred to community therapy or outpatient therapy if required.
At the time of inspection the average length of stay at Arundel and District Hospital was 35.2 days, however this figure had been affected by two patients the hospital had been unable to discharge due to social circumstances. The closest neighboring hospital was Midhurst which had an average length of stay of 20 days. Length of stay was reviewed during the monthly AMT matrons meeting.
The average length of stay on Piper Ward at Crawley Hospital was 37.6 days. Viking Ward was
27.9 days, Stroke Ward was 41.4 days and Caravelle Ward was 27.7 days. Parts of days were
calculated using an electronic system patient tracking system.
PLACE assessments are undertaken by teams of NHS and private/independent health care
providers, and include at least 50 per cent members of the public (known as patient assessors).
They focus on the environment in which care is provided, as well as supporting non-clinical
services such as cleanliness, food, hydration, the extent to which the provision of care with privacy
and dignity is supported and whether the premises are equipped to meet the needs of people
living with dementia against a specified range of criteria.
The 2016 PLACE score for ward food at the trust is 92.89%, which is slightly better than the
England average of 92.41%.
Seven of the 11 locations performed in line with or better than the England average.
Site Name Ward Food
Arundel And District Hospital 88.06%
Bognor Regis War Memorial 96.97%
Crawley Hospital 92.83%
Crowborough War Memorial Hospital
87.95%
45
Horsham Hospital 98.84%
Kleinwort Rehabilitation Unit 90.11%
Lewes Victoria Hospital 92.91%
Midhurst Community Hospital 98.63%
Salvington Lodge 96.40%
Uckfield Community Hospital 84.90%
Zachary Merton Hospital 94.14%
Trust Overall 92.89%
England Average 92.41%
Learning from complaints and concerns
Complaints were dealt with in line with the trusts complaints policy. We saw complaints and
compliments were shared throughout the organisation at regular meetings and we changes made
following complaints.
Complaints5
Between June 2016 and May 2017 the trust received 205 complaints, of which 24 were related to
Community Inpatient services. Of these 24 complaints, four were not yet closed, seven were
closed in under 30 days, five were closed between 30 and 60 days and eight were closed in over
61 days.
Compliments6
The trust received 165 compliments between June 2016 and May 2017. These accounted for
8.8% of all compliments received by the trust as a whole.
At Crawley Hospital, Midhurst Community Hospitals, Zachary Merton Hospital, The Kleinwort
Centre, BRWMH, Horsham Hospital and Arundel and District Hospital we could not find any
Patient Advice Liaison Service (PALS) leaflets and only saw one PALS poster on Caravelle Ward
at Crawley Hospital. At Midhurst Community Hospital we were advised there were complaint
details at reception, however we were unable to find any. All staff we spoke with told us patients
asked them for details of the PALS service. However, the inspection team felt this may dissuade
patients and visitors from complaining as they would have to advise staff that they were doing so.
At Uckfield Community Hospital, Salvington Lodge and Lewes Victoria Hospital, the PALS service
as well as information leaflets from the trust on how to complain were prominently placed on the
ward.
We saw patients using hands free phones on Caravelle Ward at Crawley Hospital following a
complaint from other patients about the use of mobile phones on the ward.
There had not been a formal complaint at Midhurst Community Hospital for over 900 days. An official complaint would be one that had come through PALS.
BRWMH had not received a complaint for 301 days, this was displayed on a white board at the entrance to the hospital.
5 add link to source
6 add link to source
46
At Arundel and District Hospital, we were advised about a recent complaint where a patient had
been left for three hours on a wet pad. The outcome of the investigation was to allocate a staff
member to take overall responsibility for specific patient in order that there would be no gap in
care. It also meant staff were clear as to who was covering for breaks and lunch hours.
We saw a complaints folder at Arundel and District Hospital that documented ongoing incidents
and complaints. However, we found it was not up to date, staff on the ward had meant to update it
over the summer but had not had opportunity. Within the folder we saw a complaint that was made
in November 2016, however the ward had not responded to it until March 2017.
At Salvington Lodge, we saw that comments and suggestion boxes were available. There was an
ample supply of leaflets available , which provided useful information on how to provide feedback
or raise a concern. Staff were aware of their role in assisting patients and their loved ones to raise
a concern or complaint about the service.
Is the service well led?
Good
Leadership
We saw there were clear lines of accountability and responsibility. Staff were aware of their responsibilities and who they reported to. Staff at each location reported to a matron. The matron reported to a clinical service manager, who reported to the general manager. Each general manager reported to a deputy area director for each of the four areas; East, west, central and children’s and wellbeing services. The area directors led to the area directorates. The trust had ‘Lunch and Learn’ opportunities for staff. This was a voluntary, staff led learning incentive to use lunch times as development opportunity. The ‘Back to the floor’ campaign was being run by the trust to ensure senior staff of band 8 or above worked set hours on the shop floor.
The recruitment drive at Midhurst Community Hospital had been driven by the ward manager and co-ordinated with the friends of the hospital who placed adverts around the local area.
Staff we spoke with at Arundel and District Hospital were all complimentary about the new matron
(in post 3 months) they felt she had made a positive impact and felt well supported by her. There
were 3 matrons working across three hospitals. The matron in charge of Arundel and District
Hospital also looked after Midhurst Community Hospital and spent 2 days onsite at each hospital
with the other day for admin and meetings.
The senior leadership team were displayed on a photo-board. The matron at Arundel and District
Hospital said she had regular contact with the board but that they rarely visited the hospital in
person.
Staff at Lewes Victoria Hospital felt well supported by the leaders and advised they would always “Muck in with the work” if required. Staff who needed additional support told us they received it and felt supported by their managers.
47
Vision and Strategy
The trusts values were; Compassionate care, Working together, Achieving ambitions and Delivering excellence.
Staff on the whole, were able to tell us what the vision and strategy of their ward was and how
they fitted into the trusts values.
We were told that Midhurst Community Hospital was aware of how their strategy was centred around the frail elderly population. There was an understanding that they may need to consider whether they could take patients other than those just requiring physical rehabilitation.
The values and vision of Arundel and District General Hospital were displayed in several staff
areas and on the ward.
Staff displays at Zachary Merton Hospital were detailed and promoted effective communication.
They detailed the trust’s vision and strategy as well as the unit’s vision and purpose. We also saw
a display detailing the costs of medical consumables designed to encourage staff to reduce waste.
Culture
We saw, on the whole, the culture within the service was one of pride in their work and a desire to
deliver high quality care which reflected the trust’s values. However, some stuff told us they did not
feel senior managers always understood the issues on the wards.
We saw across the trust that staff had a ‘Book of Good Stuff’. This was where staff could make a
note of achievements to remind staff of what they had accomplished.
At our previous inspection, we noted that silo working was an issue within the trust, largely due to
the diversity of services being provided and the geographical spread of sites. We asked the
general manager at Crawley Hospital whether this had improved and were advised that she had
made improvements within the three sites under her control; Crawley Hospital , The Kleinwort
Centre and the Horizon unit. They felt silo working across the trust was still an issue to some
degree. It was felt this was mainly down to communication systems not being in line with each
other.
We found staff culture varied greatly across sites as well as wards. For example, staff on the
Stroke Ward at Crawley Hospital told us they were very stressed at the time of inspection, as the
future of the ward was uncertain due to funding issues with the local commissioning groups. Staff
on the ward advised us they “Just have to wait for news from the top”. However, staff on the other
three inpatient wards advised us they enjoyed working for the trust, although lack of staffing was
an issue and placed extra pressure on them when working with agency staff. Many staff on these
wards expressed to us that “All staff work so hard, it’s exhausting.”
Staff at Midhurst Community Hospital stated they were reluctant to celebrate their achievements and what they were good at. We were told that a culture had developed where staff were reluctant to draw attention to the unit following the closure in 2016. There was a drive by senior managers to change this and ensure that for the service to be a success the staff needed to believe it was a successful service.
Staff at Bognor Regis War Memorial Hospital ( BRWMH) did not feel as though senior staff were
aware of the levels of stress on the shop floor. Therapists felt valued by ward team but not by the
48
trust and all advised us they would not recognise senior management. Occupational therapists
also advised us they felt therapy shortages were not taken as seriously as nursing shortages.
Staff at Uckfield Community Hospital could identify protected characteristics when asked to do so and we were told the trust was committed to the equality and diversity agenda. Staff were encouraged and supported to take part in the local Pride parade.
The matron reported being very proud of the staff at Uckfield Community Hospital and stated staff
always pulled together. All staff on the ward were very complimentary of the matron stating, “I feel
very much part of the team, the matron looks after us as if she was our mum”, “Matron is very
supportive and approachable”, “We are all one team here” and “Matron is so enthusiastic, she’s
very knowledgeable and hardworking”. However, some staff at Uckfield Community Hospital felt
there was a lack of progression and opportunity at the site because it was so small.
Staff at Salvington Lodge could identify protected characteristics when asked to do so and there was a poster in the staff room identifying the protected groups. There was many diverse staff with protected characteristics at the unit who told us they were treated with dignity and respect whist at work. They said they were “Very happy”. We saw a poster at Salvington Lodge advertising the speak up guardian. Although staff we talked with had not used the service. We found the high turnover of nursing at Zachary Merton Hospital had had a negative impact on
staff morale. Staff advised us this was further compounded by the high use of agency staff.
Governance
Structures, processes and systems of accountability, including the governance and management
of partnerships, joint working arrangements and shared services, were clearly set out, understood
and effective across all locations.
At all sites, it was the responsibility of the matron to disseminate messages from the senior executive team. This was done through the ward team meeting that was held on a Thursday. Minutes of these meetings were kept and reviewed during the inspection.
Across the trust there was a monthly senior team meeting which was attended by the band seven nurses and matron. There was also a quarterly band seven and matron meeting.
At Crawley Hospital there was a monthly AMT meeting for senior management which was fed up
to the head of nursing. The SMT meeting for band seven nurses was also held monthly, usually a
few days after the AMT meeting in order to ensure issues discussed could be passed on and staff
on the wards received the most up to date information.
Monthly ‘Harm Free’ meetings monitored the number of falls and pressure ulcers and levels of Harm Free Care.
Management of risk, issues and performance
The management of risk issues and performance had been standardised throughout the trust. All
staff contributed to a risk register at their own location which fed into the trust wide one, which they
could view if they wished. Performance dashboards were standard across the trust, so services
were assessed using the same metrics.
49
We saw regular auditing across inpatient services including; infection prevention and control,
catheter insertion and care and National Early Warning Scores (NEWS).
At Crawley Hospital the senior management team held monthly ‘productive ward’ meetings where
patient feedback was reviewed.
An audit of falls at The Kleinwort Centre found that the majority of falls were occurring during the
night. As night time care had been identified as an issue in discharge delays, the occupational
therapy team came in on night shifts to review the use of commodes and call bells. However, at
the time of inspection the results from this had not yet been produced.
When we spoke with staff at Midhurst Community Hospital about the security of the building particularly at night, we were told that it had been risk assessed. It was considered that the hospital’s relatively rural position was part of the reason security was not considered to be a significant risk.
Management at Uckfield Community Hospital produced a quality bulletin which enabled staff to be
aware of their key performance indicators (KPI’s) and current performance against targets.
We saw the minutes of the last three governance meetings at Lewes Victoria Hospital (LVH),
which showed training, staffing, pharmacy, health and safety, complaints and incidents were
regular agenda items. We saw the set agenda followed the five CQC domains.
Also, the leadership team at LVH were able to tell us their highest risks and what measures were
in place to mitigate these.
Matrons from Midhurst Community Hospital, Arundel and District Hospital, BRWMH, Salvington
Lodge and Zachary Merton Hospital met once a week to review ‘How are we doing boards’. These
included four areas; staff well-being (attendance of leadership masterclass, employee of the
month, thank you cards –presented to staff and appraisals), patient experience ( F & F test,
complaints, sit and see-where a member of staff sat and watched interactions between staff and
patients). Improving safety and reliability of care (recruitment, audits, matron walk around
feedback, staff training, agency and incidents and productivity (performance report, budget,
inpatient length of stay).
Engagement
We found staff engagement was good across the services we visited. The Pulse newsletter (available on the intranet) was used to communicate with staff across the various sites. The trust had a ‘We Active Challenge’ for staff which encouraged staff to get moving and improve their health and wellbeing. There were staff achievement awards internally and staff were also encouraged to partake in national staff awards.
There was staff engagement through yearly staff survey, however the trust had also introduced
responsive polls – such as following the new recruitment drive to get staff views specifically on that
process.
Staff across the trust had access to the monthly ‘Hot Topics’ newsletter, which provide trust key
messages, and changes to practice information to staff.
50
Salvington Lodge had just started a new recruitment initiative of open days in order that potential
employees could to get to know the staff and site to try to increase application numbers.
Staff at Crawley Hospital promoted a monthly ‘Safety Pledge’ where staff nominated something
small that was seen as a “Bug bare” and all staff pledged to focus on the winning issue for the
following month. Examples we were given included; ensuring patients drink during comfort rounds
and ensuring paperwork is up to date before the end of a shift.
Staff at Crawley Hospital had set up a ‘Relatives Clinic’ that was held monthly and gave friends
and family the opportunity to talk about rehabilitation goals, discharge planning and ask questions
away from the ward environment. Feedback from these groups was positive with families saying it
gave them a chance to be honest about their concerns without having the affected party there to
hear their concerns. The staff that ran the clinic had been nominated for employee of the month.
Staff we spoke with said the initiative was “Really positive and makes you feel like your work is not
going unnoticed”.
At Arundel and District Hospital, we saw a ‘Staff Shout Out’ board where post-it notes were stuck
with little thank you to members of staff for their good work and support. We also saw the ward
manager sent out articles of interest to the team to open up communication and help build
relationships.
Managers at BRWMH gave thank you cards to staff to recognise good work or a time when the
demonstrated the trust’s values. The thank you cards were in line with the four values.
Contact from senior managers to the staff at Midhurst was primarily done by email and messages were disseminated down from the ward manager to other staff. There were a limited number of computers for staff to access the intranet or email and some of the computers were in the ward manager’s room, which was not accessible to all staff. Senior managers recognised this and were looking to develop an area in the staff room to install another computer that staff could access.
On inspection there was a patient at Arundel and District Hospital who had been abusive to staff.
As a result, the staff attended to the patient in twos and the Matron spoke with the patient to
address any issues and explain that their behaviour was inappropriate.
Staff at the Bailey Unit at Midhurst Community Hospital had access to a staff welfare contact line. This had been used by staff following the death of a patient but could be used for any personal or professional advice and support.
Learning, continuous improvement and innovation
We saw many examples of innovation and learning which was based on issues identified at each
individual site. For example, a staff nurse at Uckfield had designed a dementia work book in her
own time which was being used as an education tool for staff. It provided staff with the most up to
date information on how to meet the care needs of those with dementia. At Salvington Lodge,
ANP’s had started working in the community in order to provide extra support to those teams.
The general manager at Crawley Hospital advised us there had been significant learning about
recruitment and although staffing was still an issue, she felt it was “Heading in the right direction”.
Since our previous inspection, the general manager had taken central control over recruitment.
Previously each ward recruited themselves and were finding that the same people were applying
for jobs across the hospital, which created competition as well as being a waste of time and
resources. The hospital had also changed the wording of adverts, which now promoted “A career
51
as individual as you” and were increasingly using social media to promote the trust in the local
area.
Staff at The Kleinwort Centre, Horizon unit and Crawley Hospitals were promoting a ‘Community
Hospital Improvement Programme’ with the trusts head of nursing. At the time of inspection, the
group was developing improvements regarding NEWS and sepsis training.
We were told that there were a high number of therapy vacancies across the trust but these were not being advertised. We were not provided with a reason why.
At Midhurst Community Hospital, there had been discussions among the senior team at the trust for a nurse to do a six month rotation between the Bailey Unit, the community nursing team and the MacMillan centre which was co-located at Midhurst Community Hospital.
Staff had also introduced a breakfast group for patients living in the community that had been discharged from the ward in order to reduce social isolation. At the time of inspection, it had been running for six to nine months, twice a week. Patients came, made their own breakfast, and ate together. All staff we spoke with advised us the scheme received good feedback, was used regularly by 4 to 5 patients and that volunteers helped to facilitate. At LVH we spoke to a return to practice nurse. They had been supported by the trust and the unit to regain their nurse registration. The nurse could not praise the support they had received enough. At Salvington Lodge advanced nurse practitioners had started working in the community setting. However, these posts were still in their infancy, and required further core competency development, and improved senior oversight and leadership to ensure the patients, staff and the organisation could truly benefit from the role.
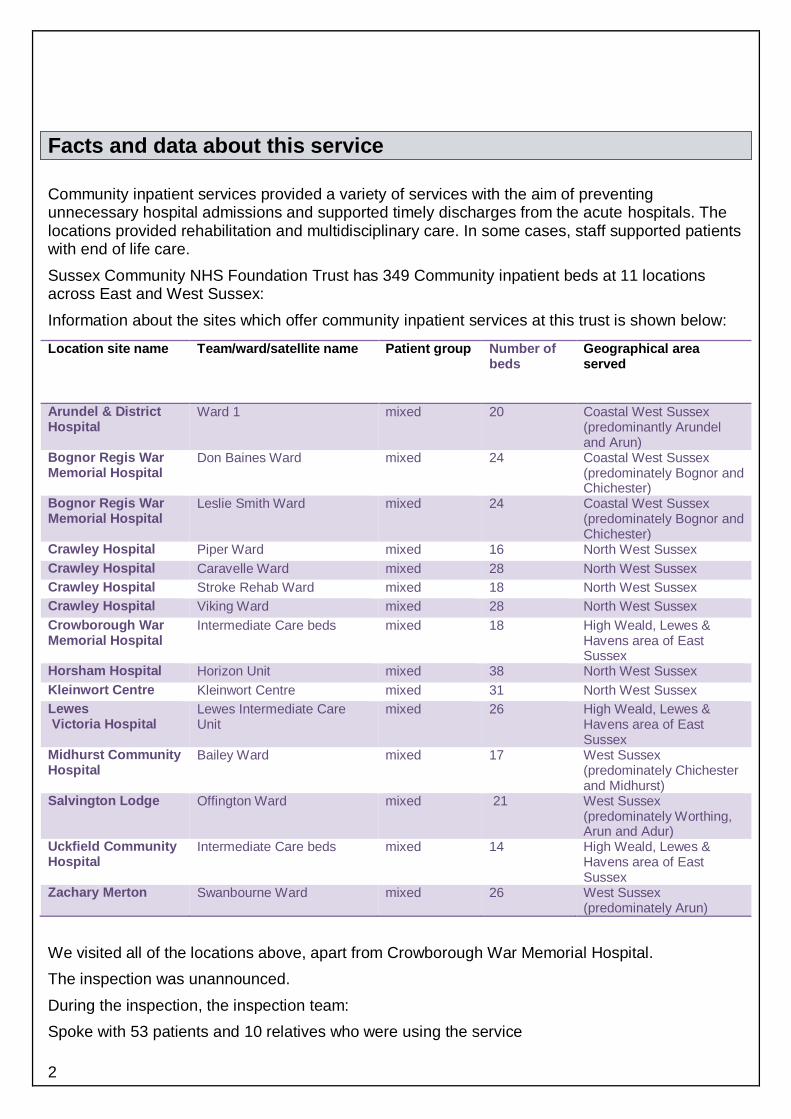

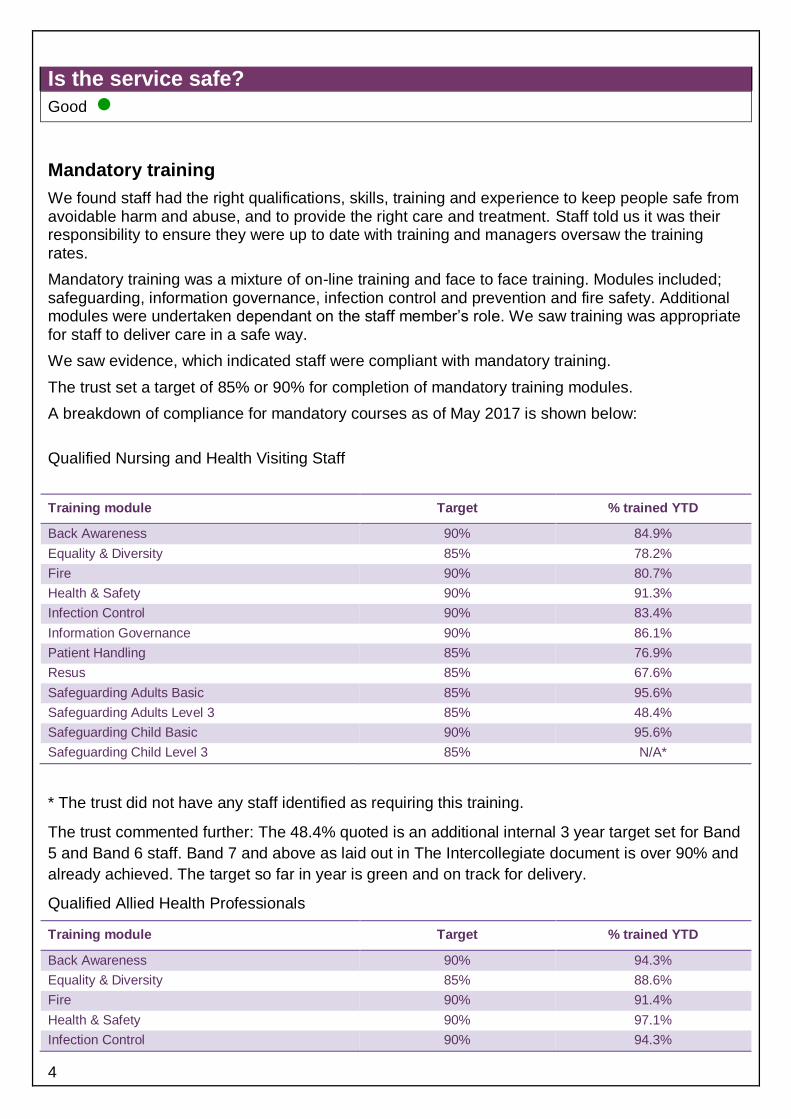

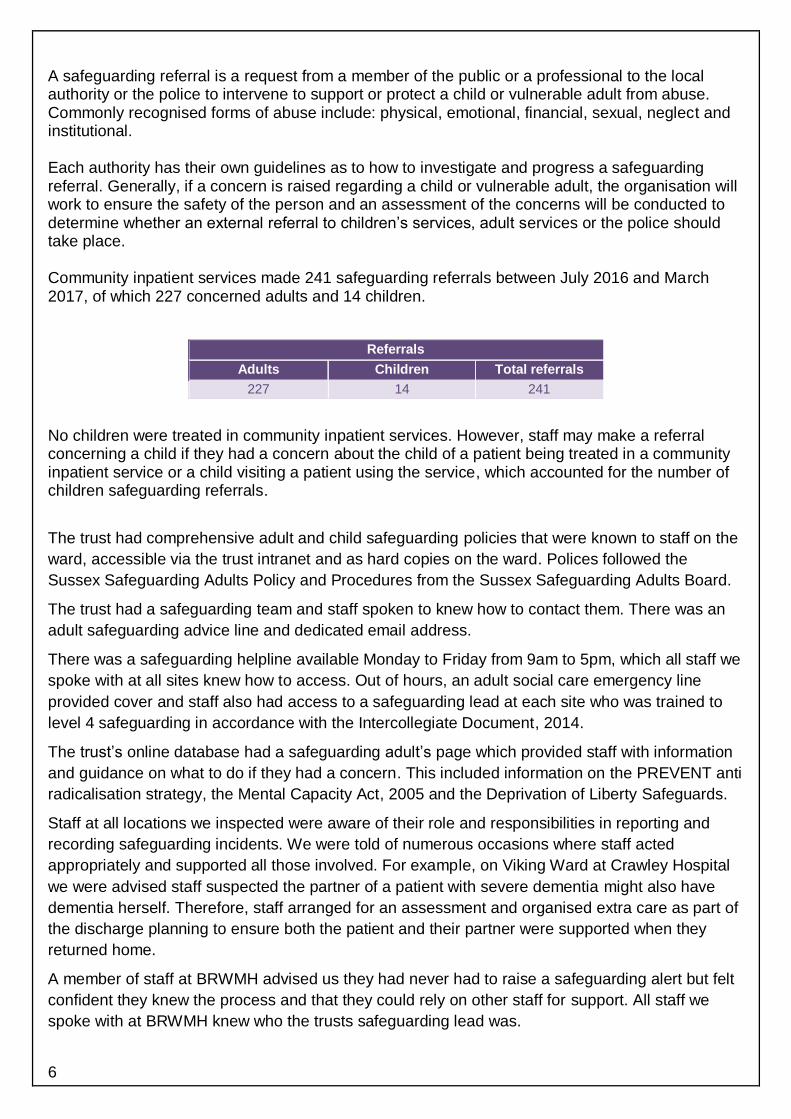


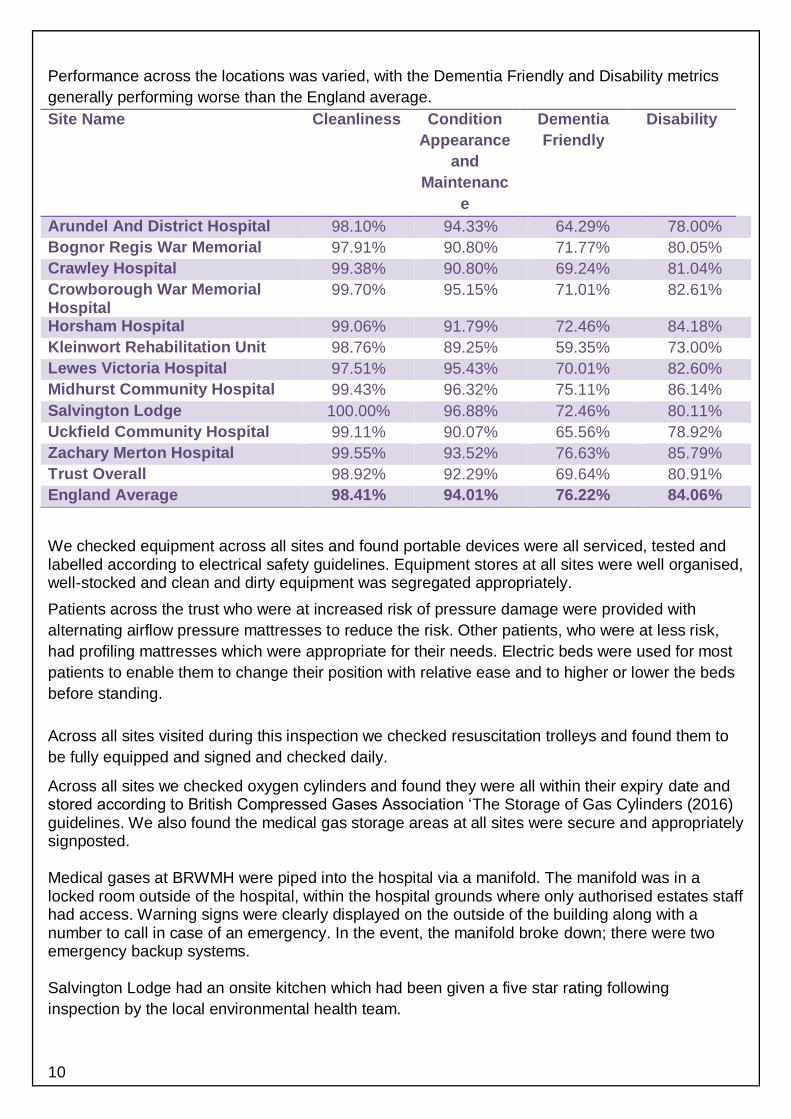



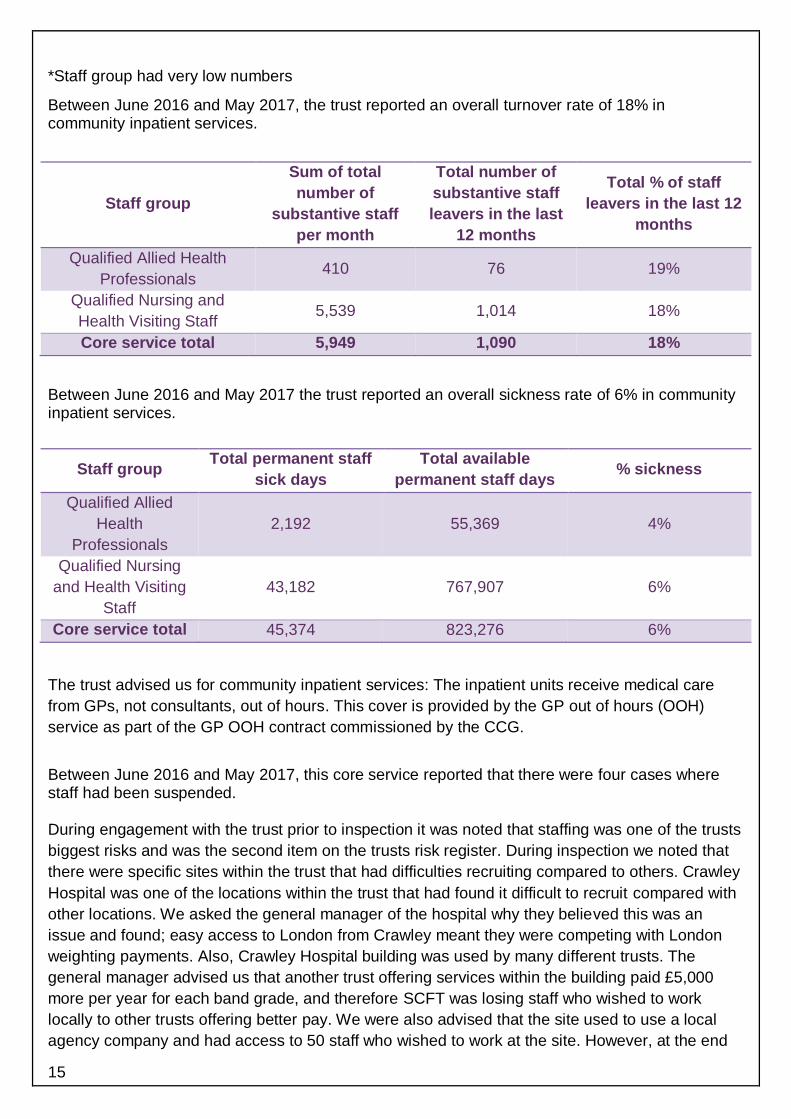






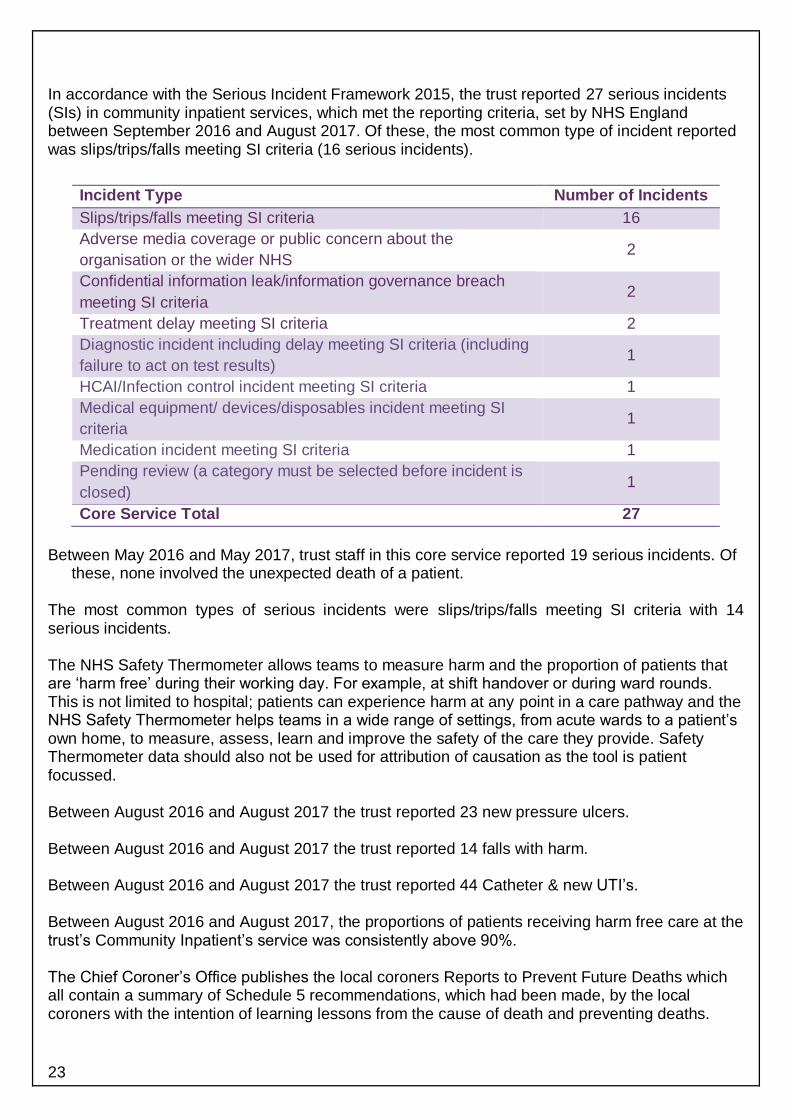





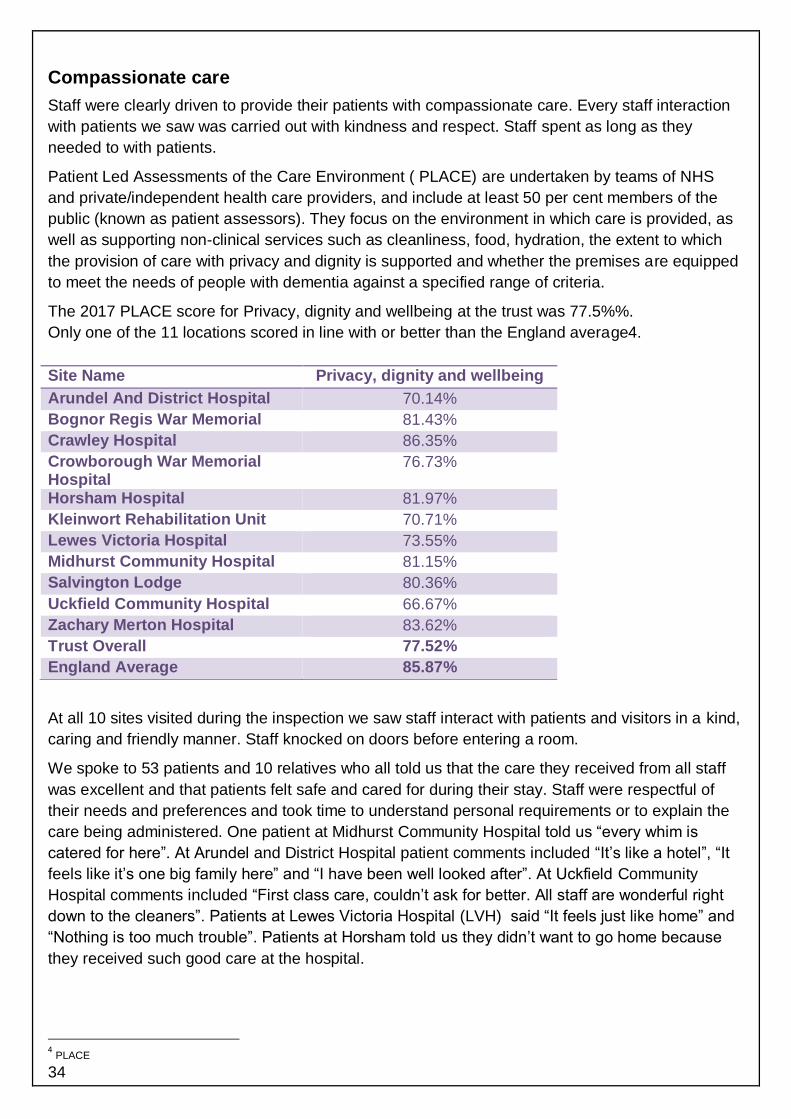






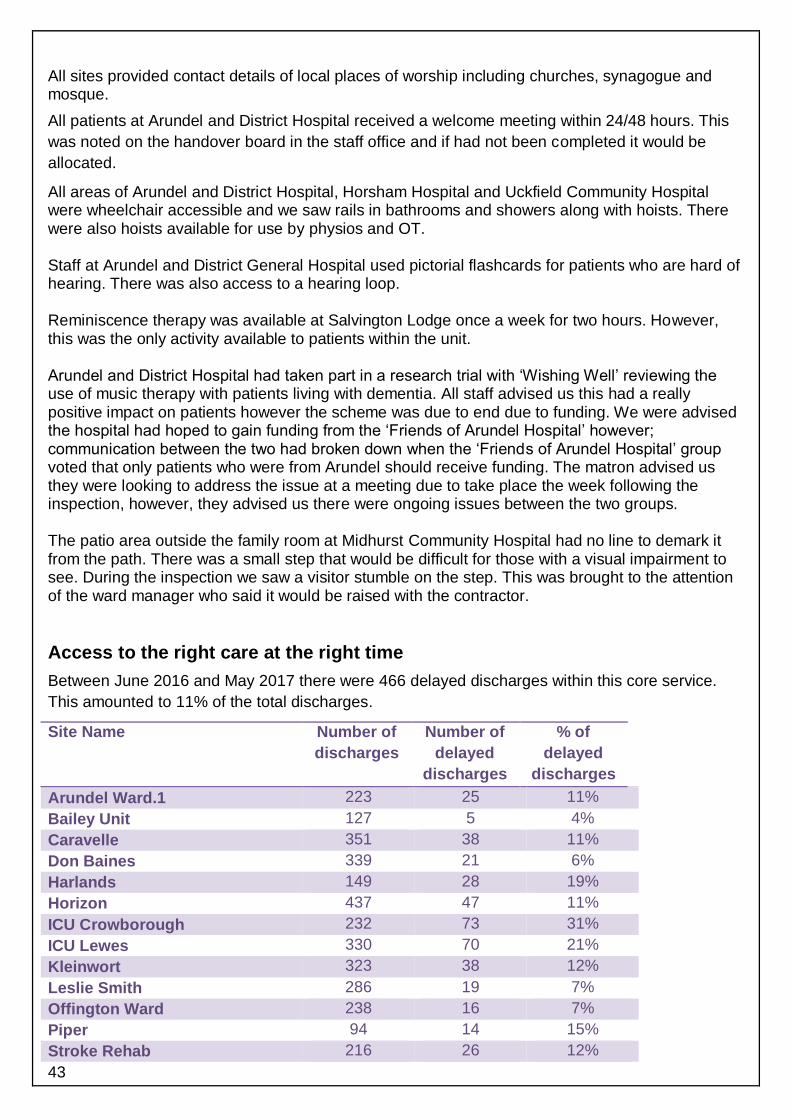






![BC DISEASE NEWS€¦ · Sussex University Hospitals NHS Trust [2018] EWHC 1063 (QB) Last week, judgment was handed down in the case of Harrap v Brighton & Sussex University Hospitals](https://static.documents.pub/doc/80x56/5fd16dfe49b466122d76e07d/bc-disease-news-sussex-university-hospitals-nhs-trust-2018-ewhc-1063-qb-last.jpg)















