Switching from first ART regimen while virologically suppressed is common in the CANOC cohort and is associated with increased risk of subsequent virologic failure M Hull, A Cescon, JM Raboud, MB Klein , S Walmsley, E Ding, W Zhang, S Shurgold, N Machouf, AN Burchell, C Cooper, MR Loutfy, JSG Montaner, C Tsoukas, RS Hogg, CANOC Collaboration 20 th International AIDS Conference Melbourne Australia July 2014
Transcript
Switching from first ART regimen while virologically suppressed is common in the
CANOC cohort and is associated with increased risk of subsequent virologic failure
M Hull, A Cescon, JM Raboud, MB Klein, S Walmsley, E Ding, W Zhang, S Shurgold, N Machouf, AN Burchell, C Cooper, MR Loutfy, JSG Montaner, C Tsoukas, RS Hogg,
CANOC Collaboration
20th International AIDS ConferenceMelbourne Australia
July 2014
Disclosures
Supported by a Chercheur Nationaux award from the Fonds de Recherche Sante, Quebec (FRQ-S)
Received honoraria and acted as a consultant: ViiV, Gilead, Janssen and Merck
Research funding from: Merck and ViiV
Background Current first-line ART regimens are well-tolerated and
associated with long-term virologic suppression Switching or modifying regimens is common for
tolerability and convenience reasons In the early ART era 44% of individuals were found to
modify their regimen at a single site1
Approximately 40% of individuals in the ART-CC analysis modified first-line ART between 2002-20092
1Mocroft A. AIDS 2001;15: 185. 2Abgrall S. AIDS 2013;27:803.
Rationale & Objectives
Outcomes after switching for tolerability are presumed to be similar to those who remain on first-line regimens
We aimed to evaluate the risk of virologic failure in people who switch for reasons other than virologic failure Describe factors associated with regimen switch for
reasons other than virologic failure
Cohort CANOC is Canada’s largest pan-provincial HIV treatment cohort study This collaboration focuses on evaluating the impact of antiretroviral care
on the health of persons living with HIV across various regions of Canada Participating cohorts (approx 10,000 pts):
• BC Centre for Excellence in HIV/AIDS
• Clinique Medicale l’Actuel
• Immune Deficiency Treatment Centre (IDTC)
• Maple Leaf Medical Clinic
• Montreal Chest Institute IDS
• OHTN Cohort Study (OCS)
• Toronto General Hospital
• University of Ottawa
BC
ONQC
Inclusion Criteria
CANOC: ≥ 18 years old with first ART date ≥ January 1st, 2000 Started ART with at least 3 individual agents while
naive (i.e., no prior antiretroviral experience) Available baseline CD4 and viral load results within six
months prior to starting therapy
Inclusion Criteria
For this analysis: Started ART January 1, 2005 – June 30, 2012 Achieved virologic suppression on ART
Defined as 2 plasma viral loads (pVL) < 50 copies/mL > 1 month apart
Subsequent regimen switch while suppressed Within same class of ART To different class of ART
Outcomes
Factors associated with regimen switch
Time to virologic failure (from first suppression) Virologic failure defined as pVL > 1000 copies/mL
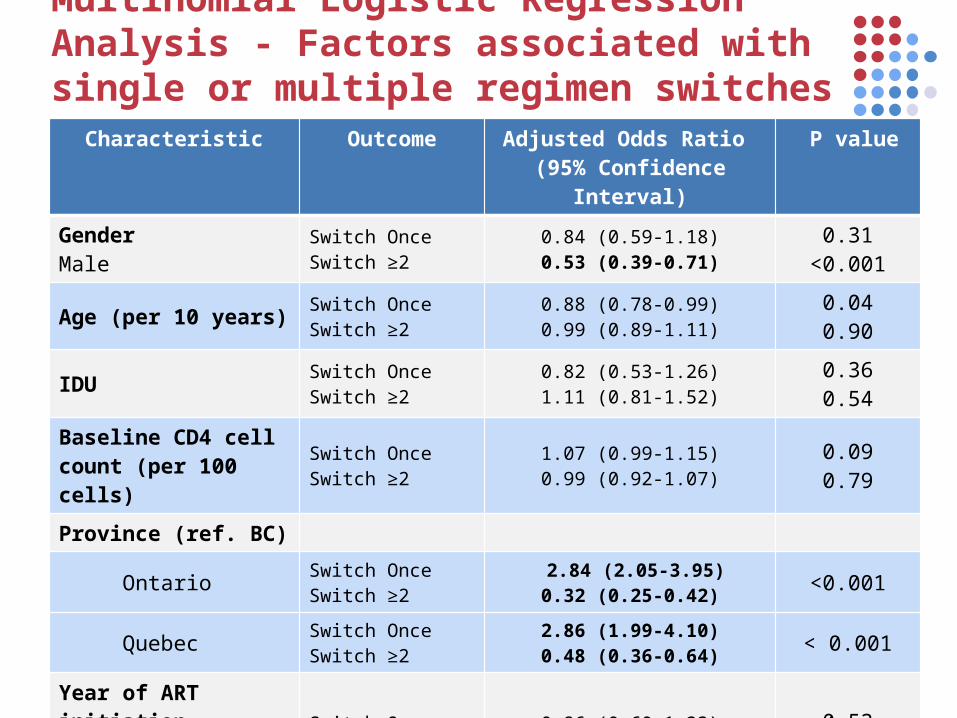
Statistical Methods Multinomial logistic regression model to assess
factors associated with first and subsequent regimen switches
Marginal Structural Model for risk of virologic failure after switch Time-varying switch as the primary variable of interest Time-varying CD4 cell count as time-dependent
confounder Time fixed covariates: age, gender, IDU status, baseline
CD4 count, province and calendar year of ART initiation
Baseline demographic and clinical characteristics (n=2807) Overall*
Never Switch 1804 (64)
Switched Regimen 1003 (36)
Switch regimen x1 391 (14)
Switch regimen ≥2 times 612 (22)
Time to first switch (years) 0.8 (0.4 – 1.7)
Age at regimen switch 42 (35 – 48)
Female 363 (13)
Province
• British Columbia 986 (35)
• Ontario 1128 (40)
• Quebec 700 (25)
Aboriginal ancestry 47 (2)
IDU history 340 (12)
HCV co-infection 425 (15)
Baseline CD4 count (cells/mm3) 260 (180 - 353)CD4 count at time of switch 450 (320 - 580)*Results are
median (Q1-Q3) or n (%).
Results
Characteristics of Individuals with ART switchCharacteristic Never Switch
(n= 1804)Switch Once
(n=391)Switch ≥2(n=612)
P value
Gender Male Female
1602 (66)202 (11)
337 (86)54 (14)
505 (84)107 (18)
<0.001
Age at first ART 41 (33 – 47) 38 (32 – 45) 42 (35 – 48) <0.001
Province (ref. BC) 0.260 Ontario 1.11 (0.63 – 1.95) Quebec 1.33 (0.78 – 2.26)Year of ART initiation(before vs. after 2008) 1.17 (0.70 – 1.93) 0.55
Discussion Even with modern ART, regimen switch while virologically
suppressed was common, occurring in 36% of individuals Presumed toxicity/tolerability/simplification/DDI
Switching was associated with longer duration of ART Switching ≥ 2 times was female gender Provincial differences in rates of switching (BC having
more persons switching ≥2 times) Switching from first ART regimen while virologically
suppressed was associated with subsequent virologic failure
Discussion Switching ART for “tolerability” reasons might represent
specific patient characteristics where ART intolerance is a marker for factors associated with poor adherence rather than with ART-agent specific concerns (e.g. IDU)
Women more likely to switch and to experience subsequent virologic failure-- may represent regimen changes around pregnancies
Limitations We could not identify specific reasons for switch We were unable to assess role of adherence We did not evaluate specific components of regimens
being switched Virologic failure was defined by virologic rebound
Development of associated resistance mutations has not yet been assessed
Conclusions
Regimen switching while virologically suppressed may not be completely benign
Closer follow up among patients switching for non-virologic reasons may be warranted as such switches may serve as a marker for problems with adherence or poorer tolerance of medications (e.g. women)
We would like to thank all of the participants for allowing their information to be a part of CANOC. CANOC is supported by the Canadian Institutes of Health Research (CIHR) and the
CIHR Canadian HIV Trials Network (CTN 242).
The CANOC Collaboration includes: Gloria Aykroyd (Ontario HIV Treatment Network), Louise Balfour (University of Ottawa, Contributes to the Ontario HIV Treatment Network), Ahmed Bayoumi (University of Toronto, Contributes to the Ontario HIV
Treatment Network), John Cairney (University of Toronto, Contributes to the Ontario HIV Treatment Network), Liviana Calzavara (University of Toronto, Contributes to the Ontario HIV Treatment Network), Angela Cescon (British Columbia Centre for
Excellence in HIV/AIDS), Curtis Cooper (University of Ottawa, Contributes to the Ontario HIV Treatment Network), Fred Crouzat (Maple Leaf Medical Clinic), Kevin Gough (University of Toronto, Contributes to the Ontario HIV Treatment Network), Silvia
Guillemi (British Columbia Centre for Excellence in HIV/AIDS, University of British Columbia), Richard Harrigan (British Columbia Centre for Excellence in HIV/AIDS, University of British Columbia), Marianne Harris (British Columbia Centre for Excellence in
HIV/AIDS), George Hatzakis (McGill University), Robert Hogg (British Columbia Centre for Excellence in HIV/AIDS, Simon Fraser University), Sean Hosein (CATIE), Don Kilby (University of Ottawa, Ontario HIV Treatment Network), Marina Klein (Montreal
Chest Institute Immunodeficiency Service Cohort, McGill University), Richard Lalonde (The Montreal Chest Institute Immunodeficiency Service Cohort and McGill University), Viviane Lima (British Columbia Centre for Excellence in HIV/AIDS,
University of British Columbia), Mona Loutfy (University of Toronto, Maple Leaf Medical Clinic), Nima Machouf (Clinique Medicale l’Actuel, University de Montreal), Ed Mills (British Columbia Centre for Excellence in HIV/AIDS, University of Ottawa), Peggy
Millson (University of Toronto, Contributes to the Ontario HIV Treatment Network), Julio Montaner (British Columbia Centre for Excellence in HIV/AIDS, University of British Columbia), David Moore (British Columbia Centre for Excellence in HIV/AIDS,
University of British Columbia), Alexis Palmer (British Columbia Centre for Excellence in HIV/AIDS), Janet Raboud (University of Toronto, University Health Network), Anita Rachlis (University of Toronto, Contributes to the Ontario HIV Treatment Network), Stanley Read (University of Toronto, Contributes to the Ontario HIV Treatment Network), Sean Rourke (Ontario HIV Treatment
Network, University of Toronto), Marek Smieja (McMaster University, Contributes to the Ontario HIV Treatment Network), Irving Salit (University of Toronto, Contributes to the Ontario HIV Treatment Network), Darien Taylor (Canadian AIDS Treatment
Information Exchange Contributes to the Ontario HIV Treatment Network), Benoit Trottier (Clinique Medicale l’Actuel, University de Montreal), Chris Tsoukas (McGill University), Sharon Walmsley (University of Toronto, Contributes to the Ontario HIV
Treatment Network), and Wendy Wobeser (Queen’s University, Contributes to the Ontario HIV Treatment Network).