II SYPHILIS OF THE LUNG By R. S. BRUCE PEARSON, D.M., Medical Registrar, Guy's Hos- pital, and S. DE NAVASQUEZ, M.D., Assistant Lecturer in Pathology, Guy's Hospital Medical School. From the Department of Pathology, Guy's Hospital Medical School. THE following two cases of syphilis of the lung are recorded mainly in order to draw attention to a condition which, though not rare, is sufficiently uncommon to be readily overlooked. The pathological findings in one case are described in detail and suggestions are made. regarding the evolution of the clinical and radiological changes in the lung which sometimes accompany acquired syphilis. An attempt is also made to relate the patho- logical state of the lung to the radiological appearances. Case i.-J. C., 59 years, was admitted for pain in the chest and breathlessness. Apart from measles as a child, he had been in good health till eight years before, when he began to have attacks of dyspncea. These came on only when he was at work, which consisted in sweeping up dust containing flour. The attacks were regarded as asthmatic in origin, precipitated by contact with flour to which he had become sensitive. About a month before admission he experienced a sharp attack of pain behind the upper end of his sternum, extending down the inner side of both arms : on standing still the pain went. It had recurred on a number of occasions since, always during exercise. Once or twice, shortly before admission, he had coughed up blood- stained sputum, and for two weeks he had had to sleep propped up with pillows, because he became breathless on lying down. He had also noticed some swelling of the feet during the week before admission. On admission he was dyspnoic, breathing shallowly and at the rate of thirty a minute. He complained of a dull pain in the precordial area. His pulse was regular between go and IOO, and collapsing in character. He was cyanosed. Republished at the request of the Editors of The British Journal of Venereal Diseases. With acknowledgements to, and permission of, the Editor of the Guy's Hospital Reports. 243 copyright. on 19 October 2018 by guest. Protected by http://sti.bmj.com/ Br J Vener Dis: first published as 10.1136/sti.14.4.243 on 1 October 1938. Downloaded from
Transcript
II
SYPHILIS OF THE LUNG
By R. S. BRUCE PEARSON, D.M., Medical Registrar, Guy's Hos-pital, and S. DE NAVASQUEZ, M.D., Assistant Lecturer inPathology, Guy's Hospital Medical School.
From the Department of Pathology, Guy's Hospital Medical School.
THE following two cases of syphilis of the lung arerecorded mainly in order to draw attention to a conditionwhich, though not rare, is sufficiently uncommon to bereadily overlooked. The pathological findings in onecase are described in detail and suggestions are made.regarding the evolution of the clinical and radiologicalchanges in the lung which sometimes accompany acquiredsyphilis. An attempt is also made to relate the patho-logical state of the lung to the radiological appearances.
Case i.-J. C., 59 years, was admitted for pain in thechest and breathlessness. Apart from measles as a child,he had been in good health till eight years before, whenhe began to have attacks of dyspncea. These came ononly when he was at work, which consisted in sweepingup dust containing flour. The attacks were regarded asasthmatic in origin, precipitated by contact with flourto which he had become sensitive.About a month before admission he experienced a
sharp attack of pain behind the upper end of his sternum,extending down the inner side of both arms : on standingstill the pain went. It had recurred on a number ofoccasions since, always during exercise. Once or twice,shortly before admission, he had coughed up blood-stained sputum, and for two weeks he had had to sleeppropped up with pillows, because he became breathlesson lying down. He had also noticed some swelling of thefeet during the week before admission.On admission he was dyspnoic, breathing shallowly
and at the rate of thirty a minute. He complained of adull pain in the precordial area. His pulse was regularbetween go and IOO, and collapsing in character. He wascyanosed.Republished at the request of the Editors of The British Journal of Venereal
Diseases. With acknowledgements to, and permission of, the Editor of theGuy's Hospital Reports.
243
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
There was some distension of the veins in the neck,and carotid pulsation was observed to be more markedon the right than the left side. The apex beat was justoutside the mid-clavicular line, suggesting moderate
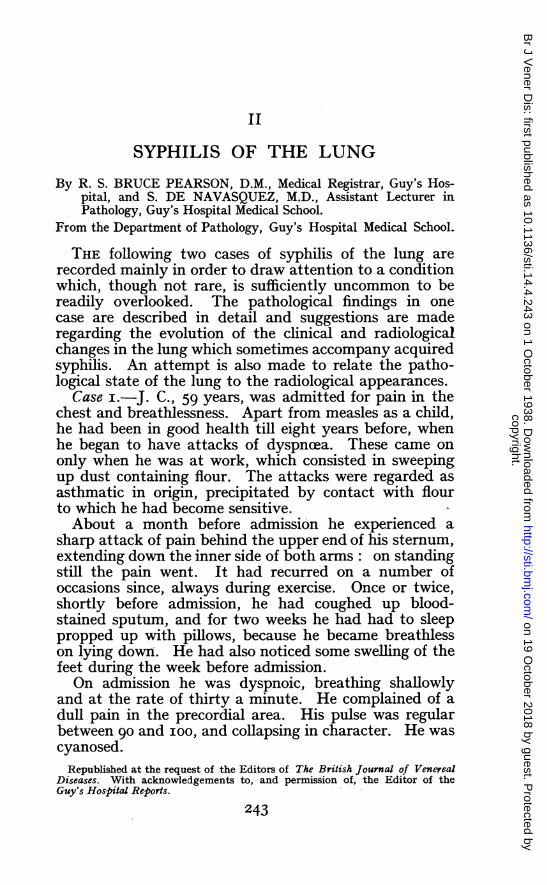
FIG. i.-Showing extensive area of infiltration in right lung.
enlargement of the heart. The blood pressure wasII2/56. There was some cedema of the feet.On auscultation loud systolic and diastolic murmurs
were heard in the aortic area. At the apex there was asoft diastolic murmur conducted from the aortic area.There were generalised rhonchi over the chest, and an
244
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
area of bronchial breathing extending outwards from thesternum at the level of the second interspace towardsthe right axilla. Above this was an area of diminishedair entry and rales. There was a corresponding area
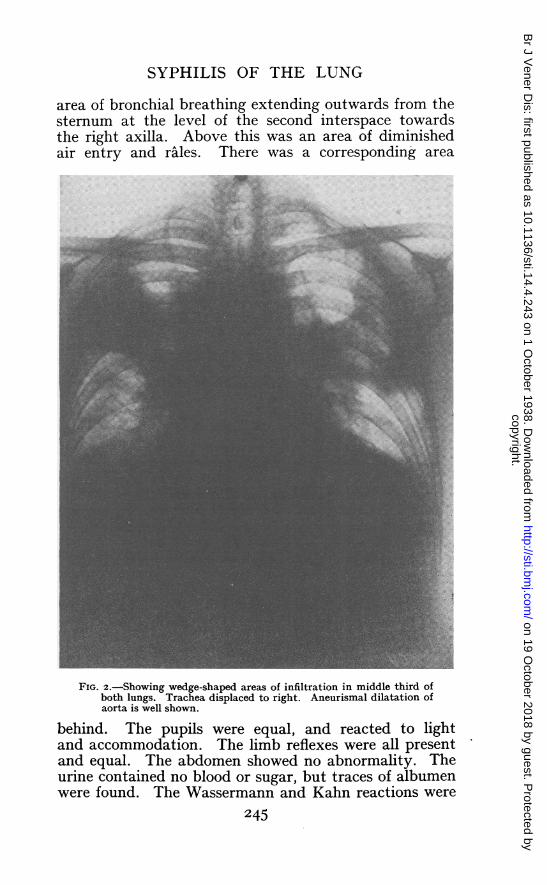
FIG. 2.-Showing wedge-shaped areas of infiltration in middle third ofboth lungs. Trachea displaced to right. Aneurismal dilatation ofaorta is well shown.
behind. The pupils were equal, and reacted to lightand accommodation. The limb reflexes were all presentand equal. The abdomen showed no abnormality. Theurine contained no blood or sugar, but traces of albumenwere found. The Wassermann and Kahn reactions were
245
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
both strongly positive. The blood picture showed ared cell count of 4-2 million, and white cells io,2oo perc.mm.; of these 69 per cent. were polymorphs, 25 percent. lymphocytes, 2 per cent. large mononuclears, and2 per cent. eosinophils.The patient was severely ill on admission, and although
he had evidence of heart failure it was observed through-out that he appeared much more cyanosed and muchmore distressed than one would have expected from thesize of his heart, the moderate aortic lesion, the slightcedema of the feet, and the fact that all evidence of con-gestion of the veins disappeared soon after admission.A radiograph (Fig. i), taken at Out Patients ten days
before admission, showed an area of infiltration on theright side of the chest in the lower and middle zoneswith slight deviation of the mediastinum to the right.The mediastinum was thickened and partly obscured inits posterior part. On admission, opacity of the lowerpart of the right upper lobe and the presence of a largeshadow at the left root were reported (Fig. 2). Radio-graphs taken ten days after admission showed no changein this appearance. No further radiographs were taken.
In the first week after admission the patient continuedto be very ill, and speaking was sufficient to make himshort of breath. He was partly relieved by administra-tion of oxygen through a nasal catheter. The mouthtemperature was persistently low and varied between950 and 970, while his pulse, which was good in quality,varied between 8o and I00. His sputum, which wasvery scanty, contained no tubercle bacilli on the twooccasions it was examined. During the second weekafter admission respiration became easier and cyanosisless marked, and he continued in this improved statefor three weeks, when he suddenly became much worse,the respiration rate rising to 40 per minute, though pulseand temperature remained unaltered. He was thenashen coloured and cyanosed, with grunting respiration.He became progressively worse and died two days later(a little over a month after admission) with a terminaltemperature of I02 and pulse of I40.
AUTOPSYAutopsy was performed twenty-two hours after death,
the body having been kept in a refrigerated mortuary.246
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
The body was that of an elderly male of slight buildwith moderate cedema of the ankles and severe haemolyticstaining of the skin and subcutaneous tissues of the trunkand limbs along the course of the superficial vessels.
Cardiovascular System.-The pericardial sac con-tained a slight excess of clear yellow fluid. The viscerallayer of the pericardium showed two large irregularmilk patches on the anterior surface of the right ven-tricle and on the posterior surface of the right auricle.The heart weighed 375 gm. All the chambers weredilated and contained post-mortem clot. The heart wasenlarged to the right and to the left but was not hyper-trophied. The myocardium was stretched and thinnedand showed severe haemolytic staining of its outer two-thirds and some adiposity of the right ventricular apex;it was soft and flabby and showed considerable loss ofmuscular texture.The endocardium was stained a dark red from haemo-
lysis. The mitral valve showed some puckering andpocketing along the entire closure line of the aortic cuspand to a point midway along the closure line of theposterior cusp; there were no vegetations. The aorticring measured 5-8 cm. in circumference and was slightlythickened but not dilated. The aortic cusps showed amoderate contraction of the free margins with irregularthickening and rolling of the edges. This was mostmarked in the anterior cusps. The mouths of the coronaryarteries were displaced in position by scars in the sur-rounding aortic wall, but were not narrowed since a4 mm. probe passed quite freely. The remaining valveswere normal. The first 5 cm. of the aorta above theaortic rings showed a few streaks of superficial atheroma.Beyond this point, there was transverse and longitudinalscarring of the intima indicating syphilitic aortitis andthe aorta gradually dilated to form a fusiform aneurysmwhose maximum circumference 8 cm. above the aorticring was greater than 9 cm. The second part of theascending thoracic aorta showed severe calcified athe-roma with thinning and scarring of the overlying intima.The arch of the aorta showed slight superficial atheromawhich was also present at the lower end of the abdominalportion. Pulmonary artery and venae cave were normalexcept for haemolytic staining of the intima.
Respiratory System.-The right and left pleural cavities:247V .D. U
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
contained 24 and 3 pints of clear light yellow fluidrespectively. The pleurae showed severe bilateral apicalscarring, which was worse at the right apex, and fibrousadhesions at both bases and mediastinum. The right andleft lungs weighed 6oo and 625 gm. respectively. Bothlungs were compressed and smaller than normal. Theapical parts of both upper lobes were dry, air containingand uniformly resilient. The right upper and middle lobeswere adherent to one another at the interlobar septum,which was in turn connected to the parietal pleura andmediastinum by fibrous adhesions. The middle third ofthe right lung, comprising the lower part of the upper lobeand the upper parts of the middle and lower lobes, wasconsolidated, firm and raised above the general surfaceof the lung. This area of consolidation formed a wedgewith its apex at the hilum and its base at the pleuralaterally. The base of the wedge contained two greyishwhite oval nodules, firm in consistency and whichmeasured 3 X 2-5 cm. These nodules were subpleuralin position and were covered by a larger circular scarmeasuring 6 cm. in diameter. The apex of the wedgeat the hilum contained three similar but smaller roundednodules, the largest of which was 2 cm. in diameter,clustered around the main bronchi. A similar wedge-shaped area, sharply demarcated from the air-containinglung above and below, occupied the middle third of theleft lung and involved the lower half of the upper lobeand the upper half of the lower lobe, but no noduleswere found in this area of consolidation. Both baseswere air containing and free from consolidation.The larynx was calcified. The trachea, main bronchi
and bronchioles showed heavy haemolytic staining of themucous membrane which was otherwise normal in everyrespect throughout. The lumen of the bronchial treewas not disturbed in any way, although the bronchiappeared to be bunched together at the hilum. Theright group of tracheo-bronchial lymph glands wasslightly enlarged and soft, but apart from heavy carbonpigmentation appeared normal.The alimentary system was normal except for moderate
congestion of the mucosa of the gastro-intestinal tract.The liver showed moderate passive congestion only.The lymphatic, urinary, endocrine and genital systems
appeared normal.248
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
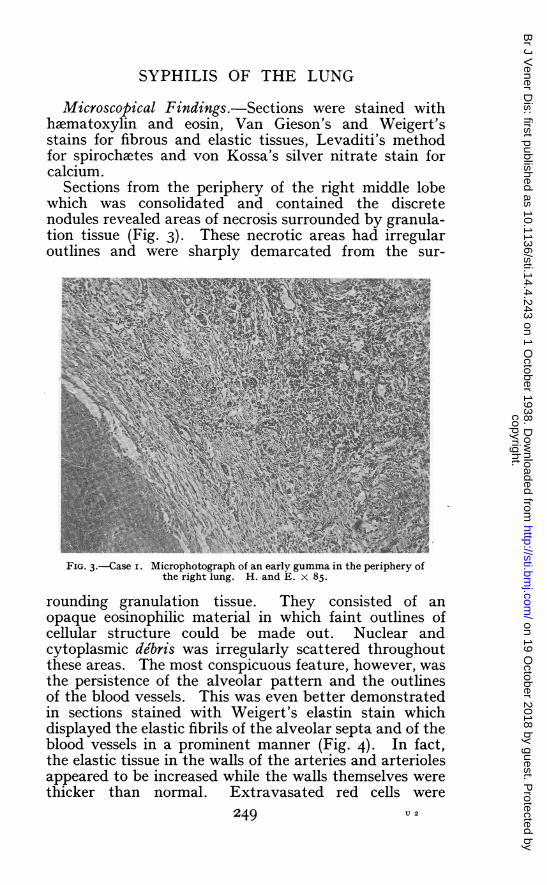
Microscopical Findings.-Sections were stained withhaematoxylin and eosin, Van Gieson's and Weigert'sstains for fibrous and elastic tissues, Levaditi's methodfor spirochetes and von Kossa's silver nitrate stain forcalcium.
Sections from the periphery of the right middle lobewhich was consolidated and contained the discretenodules revealed areas of necrosis surrounded by granula-tion tissue (Fig. 3). These necrotic areas had irregularoutlines and were sharply demarcated from the sur-~~~~~
theAihlug..n4.15
rounding granulation tissue. They consisted of anopaque eosinophilic material in which faint outlines ofcellular structure could be made out. Nuclear andcytoplasmic debris was irregularly scattered throughoutthese areas. The most conspicuous feature, however, wasthe persistence of the alveolar pattern and the outlinesof the blood vessels. This was even better demonstratedin sections stained with Weigert's elastin stain whichdisplayed the elastic fibrils of the alveolar septa and of theblood vessels in a prominent manner (Fig. 4). In fact,the elastic tissue in the walls of the arteries and arteriolesappeared to be increased while the walls themselves werethicker than normal. Extravasated red cells were
249 U 2
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
present in the periphery of the necrotic areas. The latterwere surrounded by broad zones of granulation tissueconsisting of fibrin, plasma cells, lymphocytes and fibro-blasts which filled the alveoli in the vicinity. Thisgranulation tissue showed abundant capillaries and wasintersected by strands of collagenous fibrous tissue inwhich the arteries and arterioles showed severe endar-teritis with narrowing of the lumen and thickening ofthe wall. In some areas these vessels showed infiltrationof the adventitia and media with lymphocytes, plasma
--Ft~~ ~ ~ ~~~'' .-
FIG. 4.-Case i. Microphotograph of a gumma in the right lung, showingthe survival of the elastic tissue of the alveoli and blood vessels.Weigert and Van Gieson's stains x 50.
cells, and an occasional polymorphonuclear leucocyte.The surrounding lung was consolidated, partly by com-pression and partly by a cellular exudate consisting ofplasma cells and many macrophages containing alteredblood pigment. These histological appearances werecharacteristic of a recent and active gummatous necrosis.
Sections from the hilum of the right middle lobeshowed a gumma, similar in appearance to that describedabove, and in addition two areas of gummatous necrosisof greater size. These gummata consisted of a homo-geneous eosinophilic tissue devoid of nuclear materialbut which showed the structural outlines of the lung and
250
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
blood vessels and were surrounded by collagenousfibrous tissue (Fig. 5). The medium-sized bronchi in theimmediate vicinity showed partial desquamation of themucous membrane which was replaced by granulationtissue. There was severe peri-bronchial fibrosis whichmerged into- the granulation tissue surrounding the areasof necrosis.The consolidated lung substance lying between these
two groups of gummata showed a diffuse interstitial andperi-bronchial fibrosis with endarteritis of the arterioles
N ~~~~~4:
-In~~~~~~A
- _
FIG. 5.-Case i. Microphotograph of a gumma from the hilum of theright lung, showing the surrounding fibrosis and the persistence ofthe vascular outlines in the centre. H. and E. X 50.
and scattered inflammatory foci containing many lym-phocytes and plasma cells. The alveoli were filled withcedema fluid and heavily pigmented macrophages, whilethe bronchi and bronchioles, although patent and devoidof contents, showed partial disappearance of the mucousmembrane. Apart from the inflammatory foci, thehistological appearance was similar to that of severechronic passive congestion. The absence of calcificationor carbon pigmentation was a distinct feature in the areasof necrosis and fibrosis and in sharp contrast when com-pared with tuberculomata or tuberculous fibrosis of thelung. There can be little doubt that the lesions in theright lung were of syphilitic origin. The presence of
25I
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
gummata in both the periphery and hilum of the middlelobe and the focal collections of syphilitic granulationtissue would indicate that the interstitial and peri-bronchial fibrosis was of similar origin and representedthe residual organisation of a diffuse syphilitic process.The right upper lobe showed severe fibrosis of the
apical pleura and underlying lung, which was distortedand heavily pigmented with carbon. The right lowerlobe showed severe chronic passive congestion withthickening of the alveolar walls and moderate emphysema.
0~~~~
FIG. 6.Case I. Microphotograph of the pneumonic area in the left lung,showing the sharply defined area of consolidation. H. and E. x 50.
The left lung, which on naked-eye examinationshowed a similar wedge-shaped area occupying its middlethird, revealed a somewhat different histological picturefrom that of the right lung. The appearance was moreuniform throughout the consolidated area, which wasrendered completely airless by a fibrino-cellular exudatefilling the alveoli (Fig. 6). The bronchioles and alveolarwalls were thickened by swelling of the lining epitheliumand moderate dilatation of the capillaries together withmany accompanying histiocytes and plasma cells. Thealveolar exudate consisted of fibrin, numerous large clearcells , with pale rounded nuclei of the histiocytic typeand plasma cells, while in many areas, cellular debris in
252
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
the form of eosinophilic and basophilic granules waspresent as well. In addition, there were numerous smallscattered foci involving groups of a dozen or so more orless completely necrosed alveoli (Fig. 7), though insections stained with WAeigert's stain, strands of alveolarelastic fibrils could be seen. Many of these foci weremiliary in size and showed a preponderance of granularbasophilic material, indicating dissolution of the nuclearelements, and a further stage in the necrotic process,while in others only the faint outlines of cells in a compact
H.andE. x 4IR,In36.~-
4~~~~~~~
mass couldbe seen.Polymorphouclearleucoc
:ndothelioidor giant cells of the Langhans type were
FIG.l7-CasiediMeiophtgrpof the pnereumonicartearinotes lhef
lung,rshowin an areaiof nrteroisand ithechaatera oftheeH.ventitiaandE ediwm.x 3
mases coud bcrphseen. Psolymorphonucleartleucoytesmendtheioid or gian ellstiof thes Lanhangs, atypeuwer
Thesepareusncthymartouis,canewere a ccompanentinted byalwell-efnewhlesions of the arerels anowd aterioleos.s The
vmeins,whle mrany ofthevselohwdnhoboi n
comnigoraLain
253
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
The bronchi were filled with the same fibrino-cellularexudate and necrotic material, which extended into thesurrounding alveoli. Partial or complete rings of colum-nar epithelium could be seen in the midst of a necroticarea, which indicated surviving bronchial mucosa (Fig. 8).
Sections stained with Levaditi's method failed toreveal treponemata.The lung above and below the consolidated area showed
chronic passive congestion and emphysema only.Consideration of the clinical and pathological data in
Pi
4
gu. mtu nerss._n 4E 5
ando .b
A.,,,
FtiG. 8n Case i Microphotograph of the pneumonic area in the leftlung, showing peri-bronchial consolidation and small areas ofgummatous necrosis. H. and E. x 85.
this case enables one to make a diagnosis of acquiredpulmonary syphilis with considerable certainty even inthe absence of demonstrable treponemata. The findingof characteristic gummata in various stages of formationand organisation, accompanied by a typical granulationtissue and the absence of tuberculous or pyogenic cellularreaction, confirms the pathological diagnosis.
Case 2. E. G., 42 years, admitted to Guy's Hospitalfor cough and shortness of breath on September Igth,1935. Nine months previously she began to expectoratelarge quantities of sputum. At this time she noticedthat she became easily tried, cried readily and did not
254
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
wish to go out. She also complained of a sore throatand lost her voice for a few days. During the nextmonth she developed a pain along the left costal marginwhich was brought on by coughing. A diagnosis ofbronchitis and pleurisy was made. A rub was heard inthe left axilla. She was admitted to another hospital,
FIG. 9.-Radiograph of the lungs of Case 2, showing a large denseshadow in the left lung.
and while there developed an ulcer of the then hardpalate, which was considered to be syphilitic. TheWassermann reaction was positive. On her dischargeshe attended at Guy's Hospital for anti-syphilitic treat-ment. She now complained of increasing dyspncea, andbecame pyrexial. She was admitted to Guy's Hospitalfor further investigation.
255
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
On admission she was observed to be well nourished,but pale. She had a frequent hacking cough and wasbringing up a good deal of purulent sputum. Her tem-perature was I030, pulse I30, and respiration 30. Herbreath was offensive. There was no clinical evidence ofany lesion of the heart or aorta..The left side of her chest moved very little during
respiration and was dull to percussion from apex to base.There was no impairment on the right side. Numerousrhonchi were heard on both sides of the chest, but therewas bronchial breathing, with poor air entry, over mostof the left side, especially behind. The heart appearedto be slightly displaced to the left. The blood pressurewas I24/74. The haemoglobin was 50 per cent. A largeulcer with punched-out edges was seen in the hardpalate. No abnormality was found in the alimentary,nervous or genito-urinary systems.The sputum examined at this time was muco-purulent
and on culture gave a growth of staphylococcus aureus,streptococcus haemolyticus (a and 18 types). No tuberclebacilli could be detected, and their absence was con-firmed by repeated examinations.There was some improvement in the general state of
the patient with injections of sulphostab, and the inter-mittent temperature gradually diminished and becamenormal on September 28th, I935. She continued to bringup 8 to I0 oz. of sputum daily, and this was sometimesblood-stained. On October 5th, I935, the temperaturerose and continued to swing, reaching I00° to I04° atnight. In spite of anti-syphilitic treatment, the signs inthe chest remained unaltered. The temperature becamenormal again on October 25th, I935.
In November, bronchoscopy was carried out by Mr.Brock, to whom we are indebted for the following report:"The lower one inch of the trachea and the first part ofthe left main bronchus were involved in a healing syphiliticprocess. This had caused considerable narrowing of thelower end of the trachea which had also been renderedflaccid owing to destruction of its rings and thereforeflapped on inspiration like a soft-walled tube. The mainleft bronchus was narrowed to the size of a match-stickand pus was exuding from the stricture. The carina andthe adjacent margin of the right main bronchus alsoshowed irregular scarring. The mucous membrane was
256
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
healed but the ends of broken cartilaginous rings could beseen shining through it."The general state of the patient remained about the
same ; she continued to bring up several ounces of sputumdaily and was subject to bouts of pyrexia lasting two tothree days. She was discharged to her home on December28th, I935, and died there two months later. No post-mortem was carried out.
CLINICAL AND RADIOLOGICAL ASPECTSSyphilis may affect the lung in the secondary or
tertiary stages. Secondary syphilis can be briefly dis-missed. It usually occurs in the form of a bronchitis,due to an extension of the ulcerative process that affectsthe fauces and pharynx, to the trachea and bronchi.Ornstein (I925) describes a case of this sort in which thepatient attended with symptoms of asthma which wererelieved by anti-syphilitic treatment. The conditionmay be localised so that the catarrh is limited to anapex and may give signs suggestive of phthisis (Funk,I919). Olsan (I933) believes that a true syphilitic lobarpneumonia may occur in the secondary stage and recordsa case occurring four weeks after the development of theprimary penile sore, spirochaeta pallida was demon-strated in the sputum. It is more commonly held, how-ever, that in such cases a true lobar pneumonia is com-plicating the syphilitic condition. The diagnosis is madeby the association of the lung condition with ulcerationin the mouth, secondary rash and the effect of anti-syphilitic treatment.A brief survey of the recorded cases of tertiary syphilis
of the lung suffices to show that there is no characteristicclinical picture upon which a diagnosis can be made.There is as great variety in its manifestations as in thoseof pulmonary tuberculosis itself. Most often there is ahistory of disease of some months or years durationwith signs more widespread than the clinical conditionof the patient would suggest. At other times, however,the lesion is discovered accidentally in the course ofroutine screening, in a patient whose main complaint isdue to disease of some other organ (Hartung and Fried-man, I932, Case 2). The lesion is said most often to affectthe middle and lower lobes, but this may well be because
257
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
when the apices are left clear it is more likely to bedifferentiated from tuberculous infection. In spite ofstatements to the contrary, a number of cases in whichthe upper lobes have been exclusively affected have beenrecorded (Raybaud and Jouve, I934, Stoichitza andCretzu, I935).The criteria upon which a clinical diagnosis may be
made can be briefly summarised as follows(i) An anomalous history of pulmonary disease, often
with haemoptysis, productive cough, loss of weight andfever. The history may be of brief duration or mayextend over a period of years.
(2) Exclusion of commoner causes of pulmonarylesions, such as new growth and tuberculosis; the latterby repeated failure to find tubercle bacilli in thesputum.
(3) The presence of a history of syphilitic infection,of associated syphilitic lesions in other organs, and ofpositive serum reactions such as the Wassermann andKahn tests.
(4) The effect of anti-syphilitic treatment.(5) The X-ray appearances, particularly in association
with the response to treatment.In many cases, it is impossible at present to make more
than a tentative diagnosis on clinical grounds alone. Inour second case the bronchoscopic appearance was mainlyresponsible for regarding the condition as primarilysyphilitic, while in the first case a definite diagnosis ofsyphilis of the lung was not made clinically. The X-rayappearances vary as widely as do the physical signs andfor the same reason, namely, that the underlying patho-logical changes in the lung differ considerably at differentstages of infection, and according to the extent of thelesion. This is well shown by the radiographs in the twocases described.A survey of the reports of a number of radiologists
(Robinson, I935, Watkins, I92I, Golden, I92I) taken inconjunction with the radiological reports in proven casesof pulmonary syphilis, including our own, suggest thatthe more common X-ray appearances may be grouped asfollows:
(I) Infiltration which may be lobar or patchy in dis-tribution and involving one lobe or part of one of morelobes. There is little or no deviation of the trachea.
258
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
(Stoichitza and Cretzu, Raybaud and Jouve, Case I:Denman, I932 and I933, Case 2.)
(2) Opacities roughly oval in shape, most often involvingthe lower lobes and often without connection to thehilum. These again may be single (Wigley and Saunders,1935, Hartung and Friedman, Case 2), (Lissen, I9I8,Case 3), or multiple (Hartung and Friedman, Case I:Robinson) and may vary in size from a few millimetresto several centimetres in diameter. Rarefied centralareas may indicate cavitation. Strands of increaseddensity may radiate from these areas of infiltration intonormal lung tissue. (Wile and Marshall, I92I, Case iFunk, Case 3.)
(3) Generalised accentuation of the bronchial andvascular shadows, often showing a beaded appearance,radiating from the lung roots towards the periphery.(Funk, Case I: Golden, Case 2: Raybaud and Jouve,Case 2.)
(4) One lobe or the whole of one side of the chest maybe opaque with deviation of the mediastinum towardsthe side of the lesion indicating fibrosis or pulmonarycollapse. (Golden, Case 2, Jacobs, 1935, Cases i and 3:Hartung and Friedman, Case 3.) This may be accom-panied by pleural effusion (Lissen, Case 6).The radiological appearance in many cases is not
represented by any one of the groups described above,since when the syphilitic process is present at differentstages in the same patient a composite picture may beobtained. The radiograph of Case i (Fig. 2) is of thismixed type, and is referred to again later. Beforeconsidering the probable pathological state of the lungcorresponding with each of the X-ray appearancesdescribed above, the microscopical changes associatedwith syphilitic infection will be referred to.
It is clear, however, that the diagnosis of pulmonarysyphilis can only be made during life after a number ofconsiderations have been taken into account, and com-moner canditions excluded. As Stoichitza and Cretzuremark: " La syphilis pulmonaire est une grande simu-latrice." Tuberculosis, bronchial carcinoma, pneumo-koniosis and mycotic infection may each give physicalsigns, or radiographs, which, by themselves, are indis-tinguishable from those of syphilitic infection at somestage.
259
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
Consideration of the pathological anatomy of the lesionsoffers some explanation for the various forms which maybe encountered.
PATHOLOGICAL ASPECTSThe characteristic features upon which a histological
diagnosis of pulmonary syphilis may be made have beensummarised by McIntyre (I93I) in his comprehensivereview of pulmonary syphilis. Briefly, they are:(i) Syphilis shows less caseation than tuberculosis,(2) Giant cells are rarer in syphilis, (3) Plasma cells arerarer in tuberculosis, (4) Anthracosis is rarer in the scarof syphilis, (5) The adventitia of the blood vessels is morefrequently affected in syphilis, (6) There is no endothelioidcell formation in syphilis, (7) The elastic tissue is betterpreserved in syphilis, (8) Tuberculosis does not show asmany subpleural lesions as syphilis, (9) Calcification israrer in syphilis.
In view of the complete absence of complicationseither of a mechanical nature such as stenosis of abronchus, bronchiectasis or cavitation, or of an inflamma-tory nature such as secondary infection with pyogenicmicro-organisms, our first case presented an opportunityto test the validity of such criteria. This was done andconfirmed by comparing the lesions with specimens ofpulmonary tuberculosis of various types, including onewith well-circumscribed tuberculomata.
Furthermore, it was thought that the apparent activityof the lesions and their variety might help to trace theprobable course of the syphilitic infection in the lungand its possible sequeIe.The literature on the pathology of pulmonary syphilis
is rendered doubly confusing by (i) attempts to establisha diagnosis on appearances which represent the terminalstages of a syphilitic infection, namely, the character ofthe residual fibrosis, (2) various classifications of lesions,supposedly syphilitic, without reference to the possiblerelationship to one another.
Carrera (I920), in a critical study of the lungs in I52cases of syphilis which came to autopsy, found what heconsidered characteristic syphilitic pulmonary lesions intwelve. This author considered that a diagnosis ofsyphilis without the typical inflammatory process cannot
260
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
be made. In contrasting his I52 cases of syphilis with6o cases of pulmonary tuberculosis he was unable todistinguish the fibrosis of syphilis from that of tuber-culosis.
In the description of gumma he notes angioblasts andcapillaries at the periphery with preservation of thealveolar structure and the elastic tissue of the alveolarwalls and of the vessels in the centre. Further, thescars of gummata remained vascular and unpigmentedwith carbon in contrast with those of tuberculosis. Withregard to the peribronchitis, he notes the abundance ofplasma cells while the bronchial epithelium is well pre-served. In concluding, this author divides his cases intotwo main groups: (i) five cases of gummata with peri-bronchial lesions and arteritis, (2) seven cases of fibrosiswith arteritis. All twelve showed syphilitic aortitis aswell. It is surprising that in this series not a singleexample of the more acutely pneumonic form was found.The so-called pneumonic form has been described inacquired syphilis by several authors, notably: R6ssle(I9I8), Howard (I924), Letulle and Dalsace (I926),Vivoli (I935), but under this heading are included varioustypes of consolidation, some of which were due to com-plicating factors, such as secondary infection and bron-chiectasis and therefore cannot be considered as a truesyphilitic pneumonia. (Stanley), I9II, however, describes" an intense cell proliferation which fills the alveoliand infiltrates the septa, peri-bronchial, subpleural andperi-vascular tissues. It has a peculiar gelatinousappearance and may be called a syphilitic pneumonia."This he considers the most important form of acquiredpulmonary syphilis. He describes three other forms:(i) an early diffuse sclerosis, the result of the above, inwhich the lung is not misshapen and is uniformly tough,(2) gross scarring of the lung with contraction, (3) gum-mata.
Such an uncomplicated pneumonic form undoubtedlyexists and probably represents the earliest lesion in thelung. The diffuse peri-bronchial fibrosis which frequentlyhas a lobar distribution and which is so well recognisedcan only be the result of an acute inflammatory conditionwith a similar distribution. Its apparent infrequency atautopsy may well be due to the fact that patients seldomdie in this stage. In actuality, the majority of pulmonary
26I
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
lesions found are either gummata or fibrosis which repre-sent a comparatively late stage of tertiary syphilis.What may provisionally be termed acute syphilitic
pneumonia requires definition and more detailed descrip-tion than it has hitherto received. Its probable originand course will be discussed later.We were fortunate in our case that such a condition
was present in the left lung which fits well the descriptiongiven by Stanley. Anatomically it consisted of a fan-shaped area of consolidation which occupied the middlethird of the left lung with its apex at the hilum and itsbase at the pleura. It had well-defined upper and lowermargins not unlike the edges of a lobar pneumonia.The mucous membrane of the bronchi and bronchiolesappeared normal except for congestion, while the bron-chial lumen was uniformly patent and free from exudate.On histological examination the consolidation was dueto a fibrino-cellular exudate which filled the alveoli andsome of the terminal bronchioles. The cellular portionof the exudate consisted of plasma cells and histiocyteswith a varying amount of cytoplasmic granular debris.Uniformly distributed throughout this area were focimeasuring a few millimetres in diameter in which thealveoli were necrotic and replaced by a central area ofdisintegrating cellular material loosely arranged whichwas surrounded by zones of plasma cells, lymphocytesand macrophages (Fig. 7). In many of thes3 areasstrands or rings of swollen columnar bronchiolar epithe-lium could be seen. These may be considered as foci ofnecrosis which may proceed to the formation of the so-called " miliary " gummata, of which many were present.The early age of these lesions may be gauged by thegeneral absence of fibroblasts and by the inflammationof the walls of the arteries and veins throughout theaffected area. The latter showed severe infiltration ofthe adventitia and media by plasma cells and lympho-cytes which formed well-marked perivascular collars. Amoderate number were thrombosed. There was little orno proliferation of capillaries except in the area of gumma-tous formation. A notable feature was the greaterseverity and extent of the inflammatory changes in theinterstitial tissue, particularly in the alveolar septa andin the blood vessels while the bronchiolar epithelium wasrelatively undamaged. This strongly suggests that the
262
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
condition is primarily an interstitial pneumonia, whichmay proceed to necrosis of the parenchyma and subse-quent formation of a gumma or, in the absence of necrosis,give rise to a diffuse interstitial fibrosis.The evidence in favour of such a view is demonstrated
in the relationship between the acute pneumonia in theleft lung and the multiple lesions in the right. Thelatter showed organisation and repair, which are repre-sented by well-formed gummata and the diffuse fibrosiscontaining many vessels with endarteritis obliterans.These lesions are considerably older but were distributedover a large area of lung, indicating that the inflammatoryreaction of which they are the sequel must have beensimilarly diffuse. The size and shape of the consolidatedareas in both lungs corresponded closely, and since bothconditions were typically syphilitic, differing in agerather than character, it is an economy in hypotheses toconsider them as two stages in the same process and toassume that the gummata and fibrosis in the right lungare the results of an antecedent pneumonia similar tothat in the left. This is further supported by the radio-logical appearances. The shadow in the right lungpreceded that in the left by three weeks. If such a viewbe accepted the different forms of acquired pulmonarysyphilis become related to one another and their patho-genesis is correlated with severity of the infection ratherthan with differences in the inflammatory reactions ofsyphilis. There is no essential difference between theso-called miliary gumma and its larger fellow except insize, while the scar of the former will be correspondinglysmaller. Both are the result of destruction of paren-chyma. Whether the fibrosis is localised or diffuse willdepend on the extent of the preceding inflammation andnot on differences in character.The conditions which determine the onset of pul-
monary lesions are best considered after their possibleorigin has been discussed. The earliest changes are con-fined to the vessels, peri-bronchial and alveolar tissues,indicating that the path of the infection is interstitialrather than bronchial. The respiratory passage may beexcluded as a portal of entry inasmuch as involvementof the bronchial epithelium occurs much later, if at all.The survival of the mucosa in an area of necrosis is wellillustrated in the accompanying microphotograph (Fig. 8).
V.D. 263 x
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
The fan-shaped distribution of the lesions is furtherevidence in favour of an interstitial rather than bronchialspread and again suggests an initial spread from the hilumradiating outwards to the periphery, which accountsfor the various sites in which gummata are found. Ifthis is so, infection of the mediastinum probably pre-cedes that in the lung.
Unfortunately, in the published accounts of the autopsyfindings in cases of pulmonary syphilis, examination ofthe cardiovascular system and mediastinum is oftenincomplete or is not mentioned, so that it is difficult toassess the incidence of associated mediastinal syphilis.In those cases, however, in which the mediastinum hasbeen adequately examined and which are available inthe literature, syphilitic aortitis or aneurysm of thethoracic aorta has been present.
Carrera's series of I2 cases all showed syphilis ofthe heart and aorta. Robertson and Robertson (I932)reported 2 cases of pulmonary syphilis and both showedsyphilitic aortitis. Aortitis was present in one andaneurysm in the other of the two cases reported byDenman (I933). Vivoli (I935), who reviews the clinicaland pathological forms of acquired pulmonary syphilisin a series of papers based on 25 cases, notes the presenceof aortitis and/or aneurysm in 75 per cent. Analysis ofhis cases, however, considerably increases the incidence:i8 out of 25 cases came to autopsy; and of these, I4 inwhich the pathological criteria of pulmonary syphilis weresatisfied, all showed syphilitic aortitis. Of the remaining4 which the author accepts as cases of pulmonary syphilis,but which, in view of the complicating factors, should beexcluded, i showed rupture of an aneurysm into a bronchuson the. same side as the pulmonary lesions, i showed ananeurysm adherent to and partially occluding the bronchusof the same side, i showed an aneurysm of the pulmonaryartery, and the last gangrene of the lung and py?emia.Two cases of gummata of the lung verified at autopsy
performed at this hospital both showed aortitis. Theassociation in these reported cases is much too high tobe the result of fortuitous coincidence even allowing forthe high incidence of aortitis in syphilis. Symmers (I9I6)found 3I4 cases of acquired syphilis in 4,880 autopsies,or a total incidence of 6-5 per cent. Aortitis was foundI75 times, or. in 55.7 per cent. Syphilitic changes in the
264
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
respiratory tract were encountered thirty-five times,or in IO-5 per cent. Of these 35 cases, the larynx wasaffected in I2, the trachea in 4, the nasal septum in 4,the hard palate in i, while I2 cases were called chronicinterstitial pneumonia, and therefore represented 3-8 per*cent. of all cases of syphilis.
The statistical evidence lends strong support to theview that aortitis is invariably present in syphiliticinfection of the lung parenchyma, while the anatomicalevidence strongly suggests that the lesions in the lungare preceded by and are the result of extension of theinfection from the mediastinum.
If this is accepted, another factor is added to the listof clinical and pathological criteria in the diagnosis ofpulmonary syphilis.
DIscuSSIONIt remains to attempt to correlate the clinical and
radiological findings with the probable underlying condi-tion in the lung, in view of the evidence obtained fromthe two cases reported in this paper. Tertiary syphilismay affect the lung in two ways, either by invasion ofthe pulmonary interstitial tissue from the hilum, asin Case i, or as a result of syphilitic lesions of the tracheaor bronchi, as in Case 2; in the latter group may beincluded those cases in which bronchial constrictionwith subsequent bronchiectasis occurs as the result ofpressure from an aneurysm of the aorta.
This second group needs little consideration and willbe discussed first. The signs and symptoms are thosewhich accompany bronchiectasis or fibrosis of whateverorigin and are secondary to bronchial obstruction by agummatous process. It is only possible to diagnose thecondition with certainty by actual observation of thebronchi during life, as in our second case, or possibly atpost-mortem. The lungs themselves will show no specificevidence of syphilis, and therefore a diagnosis is in manycases impossible. It is unlikely that pulmonary symp-toms will be produced till healing of the gumma withfibrosis has begun. For this reason, treatment is notlikely to be successful, since it is attempting to dealwith end results rather than with active disease. Theradiological appearances correspond with those describedin the fourth group.
265 X 2
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
The clinical findings are far more variable in thosecases in which syphilitic infiltration of the lung itselfoccurs.The pneumonic phase may give signs of consolidation
limited to one lobe or part of one or more lobes. Theradiological appearances vary similarly from completeconsolidation of one lobe with little or no displacementof the trachea or may show infiltration spreading fromthe root with tongue-like projections into presumablynormal lung and involving parts of two or more lobes.The latter appearance is shown on the *right side inCase i in the earlier Fig. i, while consolidation is presentin the left lung in Fig. 2, taken three weeks later. Com-plete resolution, as shown by subsequent radiographs,commonly follows adequate anti-syphilitic treatment inthese cases. Should necrosis develop, the formation ofa gumma or gummata may occur and will be responsiblefor the changes we have described in the second groupof radiological appearances, which will vary according tothe number and size of the gummata. Cavitation mayoccur as a result of the discharge of a gumma into abronchus and will show accordingly.
Organisation of the gummatous or pneumonic pro-cesses. leads to fibrosis, probably giving rise to the in-creased pulmonary markings described in the third group.The beaded appearance referred to is thought to indicatethe presence of miliary gummata. The simultaneousoccurrence of gummata and diffuse fibrosis is seen tohave occurred in the right lung of our first case. Theradiograph of this lung, however, shows no evidence ofthe gummata which were subsequently found, but theevident contraction of the area of infiltration (Fig. 2),shown by displacement of the trachea towards that side,was subsequently confirmed by anatomical findings asbeing due to fibrosis. Where the scarring is localisedand severe, the condition known as pulmo lobatumdevelops and can sometimes be recognised radiologically(Prevot, I935). When fibrosis has occurred, anti-syphilitictreatment can never restore the normal radiologicalappearance of the lung.
Finally, it is possible that extensive fibrosis may developas a terminal stage, giving an appearance radiologicallyindistinguishable from that produced by bronchial con-striction due to gummatous involvement of a main
266
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D
and probably represents the earliest lesion in pulmonarysyphilis.
(2) Syphilitic pneumonia is primarily interstitial andmay lead to (a) gummata ; (b) chronic interstitial fibrosis.
(3) It is suggested that pulmonary syphilis is alwaysassociated with and secondary to syphilitic aortitis andis more frequent than has hitherto been believed.
SUMMARY(i) Two cases of pulmonary syphilis are described, one
of which showed a syphilitic pneumonia at autopsy.(2) The pathogenesis and incidence of pulmonary
syphilis are discussed.
REFERENCES
CARRERA, J. L. (I920): Am. J. Syph., 4, i.DENMAN, H. C. (I932): Ann. Int. Med., 5,895 ; (I933), N. Y. S. J.
Med., 33, I438.FUNK, E. H. (I919-20), Amer. Rev. Tuberc., 3, 754 ; (I923), Med.
Clin. N. Amer.GOLDEN, R. (I92I): Amer. J. Roentgen., 8, 502.HARTUNG, A., and FRIEDMAN, I. (1932): J. Amer. med. Ass., 98,
I969.HOWARD, C. P. (I924): Am. J. Syph., 8, I.JACOBS, M. (I935): Amer. Rev. Tuberc., 31, 453.LETULLE, M., and DALSACE, J. (I926): Pr. mid., 34, 385.LISSEN, H. (I9I8): Amer. J. med. Sci., 155, 356.MCINTYRE, M. C. (193I): Arch. Path., 11, 258.OLSAN, H. T., and CHAMBERS, S. 0. (I933): Calif. and Western Med.,
39, I85.ORNSTEIN, G. G. (I925): Med. Clin. N. Amer., p. 357.PREVOT, R. (I935): Roentgen. Praxis, 7, 686.RAYBAUD, A., and JOUVE, A. (934): Arch. mid. Chir. Appar. resp.,
9, 337.ROBERTSON, W. E., and ROBERTSON, H. F. (I932): Int. Clin., 3, 23ROBINSON, W. W. (1935): Radiology, 25, 596.ROSSLE, R. (I9I8): Munch. med. Wschr., 36, 992.STANLEY, J. D. (I9II): Brit. Med. J., 2, 802.STOICHITZA, N. N., and CRETZU, V. (1935): Arch. mid. chir. Appar.
res2, 10, I.
267
copyright. on 19 O
ctober 2018 by guest. Protected by
http://sti.bmj.com
/B
r J Vener D
is: first published as 10.1136/sti.14.4.243 on 1 October 1938. D