Al‑Omari et al. BMC Pulm Med (2021) 21:196 https://doi.org/10.1186/s12890‑021‑01560‑0
RESEARCH ARTICLE
Systematic review of studies investigating ventilator associated pneumonia diagnostics in intensive careBasem Al‑Omari1,4* , Peter McMeekin2, A. Joy Allen3, Ahsan R. Akram4, Sara Graziadio3,5, Jana Suklan3, William S. Jones3, B. Clare Lendrem3, Amanda Winter6, Milo Cullinan7, Joanne Gray2, Kevin Dhaliwal4, Timothy S. Walsh8 and Thomas H. Craven4,8
Abstract
Background: Ventilator‑associated pneumonia (VAP) is an important diagnosis in critical care. VAP research is compli‑cated by the lack of agreed diagnostic criteria and reference standard test criteria. Our aim was to review which refer‑ence standard tests are used to evaluate novel index tests for suspected VAP.
Methods: We conducted a comprehensive search using electronic databases and hand reference checks. The Cochrane Library, MEDLINE, CINHAL, EMBASE, and web of science were searched from 2008 until November 2018. All terms related to VAP diagnostics in the intensive treatment unit were used to conduct the search. We adopted a checklist from the critical appraisal skills programme checklist for diagnostic studies to assess the quality of the included studies.
Results: We identified 2441 records, of which 178 were selected for full‑text review. Following methodological examination and quality assessment, 44 studies were included in narrative data synthesis. Thirty‑two (72.7%) studies utilised a sole microbiological reference standard; the remaining 12 studies utilised a composite reference standard, nine of which included a mandatory microbiological criterion. Histopathological criteria were optional in four studies but mandatory in none.
Conclusions: Nearly all reference standards for VAP used in diagnostic test research required some microbiological confirmation of infection, with BAL culture being the most common reference standard used.
Keywords: Ventilator‑associated pneumonia, Diagnostics, Intensive care, Critical care
1. This comprehensive systematic review assesses the reference standard tests used to evaluate novel index tests for suspected VAP in ICU over 10 years period
(2008 until 2018) and included high-quality studies with low risk of bias.
2. BAL culture is the most common reference standard used for VAP diagnostic in ICU and almost all refer-ence standards required some microbiological con-firmation of infection.
Open Access
*Correspondence: [email protected] College of Medicine and Health Sciences, Khalifa University, PO Box 127788, Abu Dhabi, UAEFull list of author information is available at the end of the article
Page 2 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
BackgroundVentilator-associated pneumonia (VAP) refers to inflam-mation of the lung parenchyma caused by infectious agents acquired specifically while receiving invasive mechanical ventilation [1, 2]. VAP is a preventable noso-comial complication which potentially contributes to avoidable mortality and morbidity [3, 4]. Therefore, it is considered a clinically and epidemiologically impor-tant measure of the quality of care [5, 6]. It contributes to additional resource consumption, adding time and expense to an intensive care stay, accounting for a large proportion of all antibiotic prescriptions [7]. VAP is con-sidered to be responsible for an additional cost of approx-imately $40,000 per episode in the US [8, 9] and around £9000 in the UK [10]. The contribution of an episode of VAP to mortality is difficult to definitively ascertain because of the high number and severity of confounders amongst the at-risk population [4, 11–13]. This attribut-able mortality has been reported from high to neutral or near-neutral [11–13].
Throughout recent decades investigators have not adopted a fixed set of criteria or a fixed definition for VAP [14]. This lack of a reference standard has led to an inability to make comparisons across study sets and uncertainty about VAP incidence [15]. The incidence of VAP varies widely in different studies depending on the diagnostic criteria used, type of intensive therapy unit (ITU), and patient population [16, 17].
Existing literature reports that the incidence of VAP varies widely between 4.0% and 28.8% of the at-risk pop-ulation [8, 18–24], with an event rate between 1.4 and 16.5 per 1000 ventilator days [1, 25–27]. As VAP rates have become an important quality indicator, the Centre for Disease Control and the European Centre for Disease Control use their own precise case definitions to identify VAP events [28, 29]. Both definitions return similar VAP rates making them adequate for surveillance purposes and benchmarking of critical care units internationally [1]. However, due to the lack of concordance between these two definitions, they do not make ideal reference standards [1, 28], and further highlight the difficulty in achieving consensus in diagnosing VAP. Microbiological samples, especially quantitative culture of bronchoal-veolar lavage (BAL), are considered to be integral to the diagnosis of VAP [30, 31]. However, a systematic review of diagnostic methods in 2008 found that microbiologi-cal methods did not contribute to the accuracy of diag-nosis over clinical criteria and all respiratory sampling methods were equivalent [32]. The continuing lack of an agreed reference standard hampers research into novel diagnostic methods. The aim of this review was to iden-tify what reference standards have been used in diagnos-tic evaluation research for VAP.
MethodsThe protocol for this review was published in PROS-PERO (International Prospective Register of Systematic Reviews) under registration CRD42019125449 [33].
Search strategyA comprehensive search strategy was developed by one of the authors (BA). The Cochrane Library, Pub-Med (MEDLINE), CINHAL, EMBASE, and web of sci-ence were electronically searched from January 2008 until November 2018. We limited our search to stud-ies published after 2008 following a comprehensive systematic review of diagnostic methods [32]. Medical Subject Headings (MeSH) and search terms were used to interrogate the databases. The 3 concepts used for the searches were VAP, diagnostics, and ITU (for search terms see Additional file 1). No restriction on publi-cation language was applied. In addition, electronic searching of Google and hand searching through an examination of the reference list of the published arti-cles were also used to identify additional publications (an example of MEDLINE search is provided in Addi-tional file 1).
Review strategyAll records were independently reviewed by the lead author (BA) and another author (PM or JG) and disa-greement was resolved by a third independent adjudi-cator (PM or JG). Initially, titles and abstracts review of all records, then full-text reviews were conducted against the inclusion/exclusion criteria. Studies included in the review fulfilled the following criteria: (1) adult ventilated patients of any gender, (2) ITU set-tings, (3) suspected VAP as defined in this study (after 48 h on the ventilator), (4) focused on the diagnostic procedures of VAP (clinical markers, biomarkers, chest x-ray, chest ultrasound (U/S), lung biopsy, BAL and mini-BAL, protected specimen brush (PSB), blind PSB, Endotracheal Aspirate (ETA)). Studies were excluded from the review if they: (1) were animal studies, (2) included patients under the age of 18 years old, (3) focused on the surveillance of VAP, (4) compared the diagnosis of VAP against another illness diagnostic, (5) were feasibility studies, (6) included participants who were already diagnosed with VAP, (7) investigated VAP treatment effectiveness by monitoring biomarkers or other diagnostics, (8) evaluated risk factors to predict VAP, (9) were procedures used to predict the mortal-ity in VAP, (10) were case-controlled studies. All papers that passed the full-text review and those that had some diagnostic technical terms were examined by an
Page 3 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
ITU clinician (THC) to confirm their clinical relevance to the research question.
Quality assessment and data extractionA team of 12 reviewers (systematic reviewers, clinicians, methodologists, health economists) from the Univer-sity of Northumbria, Newcastle University, The New-castle Upon Tyne Hospitals NHS Foundation Trust, and the University of Edinburgh were involved in the qual-ity assessment and data extraction process. All included papers were quality assessed and the data were extracted by two authors independently. Any disagreement was discussed between both reviewers in the first instance. The further disagreement was resolved by a third reviewer. The quality assessment scoring checklist was adopted from the Critical Appraisal Skills Programme (CASP) checklist for diagnostic studies [34], which is one of the well-recognised methodological quality or risk of bias assessment tools for primary and secondary medical studies [35, 36] and has been used to assess the quality of diagnostic studies in systematic reviews [37–39]. The quality assessment scoring checklist contains 8 questions from the overall 12 questions in the CASP checklist. Questions from section C in the CASP for diagnostics checklist “will the results help locally?” were not included in our scoring as the main aim of the review was not related to the local application of the diagnostic procedures. Studies were assigned a score of ‘1’ for each item of the checklist if they were considered to meet the aspect of this item and ‘0’ if not. A total score for each study was calculated by summing the item scores. The maximum possible final score was 8. Any study that scored ‘0’ for the first or the second question or scored less than ‘5’ out of 8 in total was excluded. According to CASP guide for diagnostic studies, if the answer to ques-tion 1 or 2 while critically appraising a study was “no”, then it is not worth continuing. That leaves 6 questions out of the total 8 we used in our quality assessment. Tak-ing in consideration that these questions are equally as important but less important than the first 2 question, we determined that a study must fulfil the quality of at least half of these 6 points (score 3 out of 6) to be consider for the review. Therefore, this threshold was derived through reviewer consensus that studies scoring less than 5 out of 8 were not of sufficient quality to adequately address the research question.
A standardised data extraction form was developed by three authors (AJA, BA, THC) and reviewed by all authors (for quality assessment and data extraction form see Additional file 2). We recorded and present study country of origin, study size, male: female ratio or enrolled participants, index test(s) under investiga-tion, reference standard used to define VAP, and test
characteristics. Although test characteristics for the index test are not relevant to the aims of this review, we present them herein because several of the index tests are also used as reference standards. Test characteristics are taken directly from the studies or calculated using data contained within the studies. Where multiple test char-acteristics are presented in the original paper, we selected those highlighted by the original authors or those which reflect the comparison best, or those which indicate the best performance. Where BAL was conducted, we recorded the details of the lavage procedure.
A narrative data synthesis approach was used to report the results from reviewed studies. Due to the large vari-ation in practice, processes, and reference standards, a meta-analysis of diagnostic accuracy was not conducted.
ResultsStudies identifiedThe searches identified a total of 2441 articles. Records that were not published in English were translated to English using Google translator. 2263 articles were excluded on the basis of title and abstract and a further 123 on the basis of full-text screening were excluded as not clinically relevant to the inclusion criteria or meeting at least one of the exclusion criteria, leaving 55 articles for quality assessment (see Fig. 1 for PRISMA flow chart).
Quality assessment and data extractionOf the 55 studies examined in the quality assessment stage, 11 studies were excluded due to either scored ‘0’ for the first or the second question or scored less than ‘5’ out of ’8’ in total score, leaving 44 studies included in this review [40–83]. All scored were agreed by at least two reviewers and reviewed by the principal investigator (PI). The lowest score assigned to any included study was ‘5’ out of ‘8’. Three studies scored 8/8, 24 studies scored 7/8, 11 studies scored 6/8, and six studies scored 5/8 (see Table 1).
As expected, all papers suffered from bias in their accuracy estimates of the index test from the use of an imperfect reference standard comparison, a well-known issue with comparative diagnostic accuracy studies [84]. The results of the quality assessment reviews conducted using the form adopted from CASP diagnostic study checklist showed that five papers [51, 54, 57, 62, 82] suffered from verification bias: not all patients received testing by both the index and the ref-erence standard. In 38 papers [41–47, 49–53, 55–59, 61–68, 70, 71, 73–82], the results of the index test could have been influenced by the reference standard result. This means that there was no evidence blinding or the tests being performed independently. The VAP status for all participants in the study was not clearly defined
Page 4 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
in two papers [47, 65]. The methodology description was not described in detail in three papers [40, 45, 82] and the results of the study were not clearly presented in five papers [46, 64, 67, 69, 75]. There was a lack of certainty regarding the results of the study on 11 occa-sions [40, 42, 43, 46, 58, 64, 65, 67, 68, 74, 75]. CASP diagnostic study checklist guide was followed in assess-ing all points.
The disagreement was solved through discussion between both reviewers on 20 papers, and adjudication of a third reviewer in one paper. Forty-three of the stud-ies were cohort studies (38 of which were prospective studies) and one was a secondary analysis of data from a randomised controlled trial (RCT) [57]. All studies were published between 2008 and 2018 with a wide geographi-cal spread; four studies conducted in the UK [41, 44, 72, 74], eight in the USA [40, 45, 47, 50, 56, 62, 67, 75], seven in France [51, 53, 55, 63, 70, 73, 78], five in Netherland [48, 61, 66, 77, 79], three each in both China [52, 65, 68] and Turkey [43, 46, 82], two each in Egypt [49, 76], Brazil
[54, 81], and Italy [71, 83], and eight in other countries [42, 57–60, 64, 69, 80]. The median sample size was 180 recruited participants, with the 21 being the lowest [58] and 2080 being the highest number of participants [61] (see Tables 2, 3).
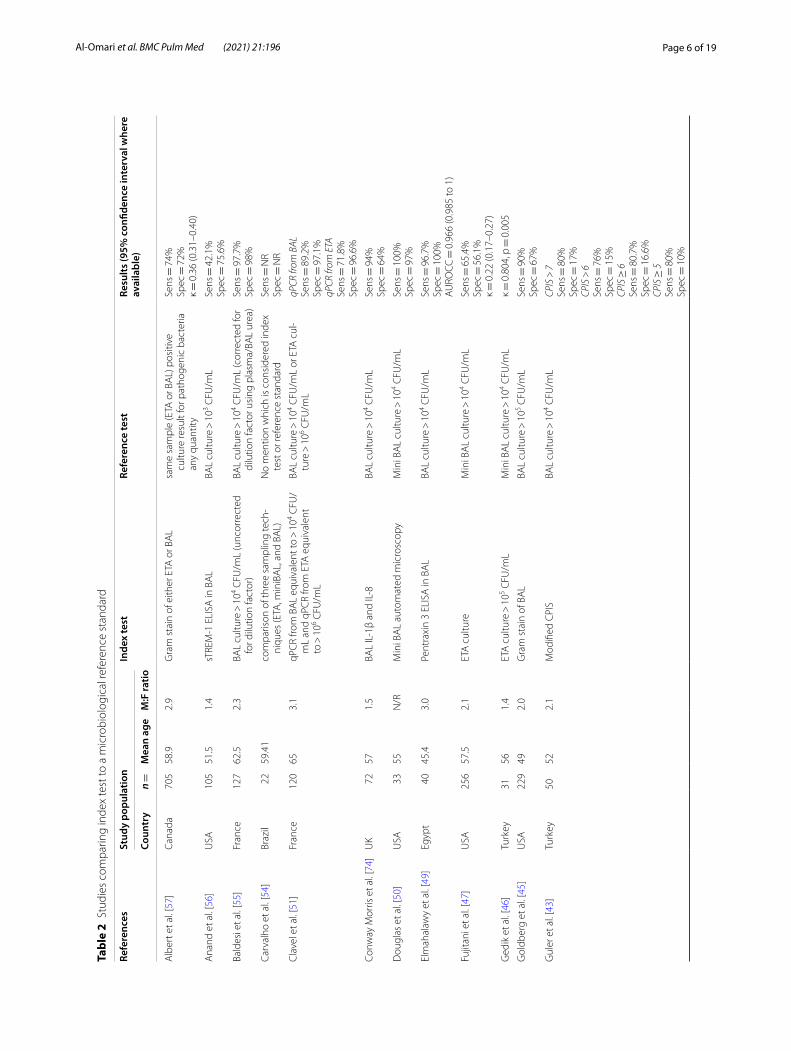
Reference standardWe did not consider enrolment criteria, including objec-tive criteria for suspicion of VAP, to be part of the refer-ence standard. Out of the 44 included studies, 32 studies (72.7%) compared an index test with a sole microbiologi-cal reference standard (see Table 2). One of these studies did not define which of the studied tests were considered index and which were considered reference [54]. Of the remaining 31 studies, culture of BAL fluid was most com-monly used as the reference test, forming at least part of the reference standard in 26 (83.8%) studies [40, 41, 43, 45, 48, 49, 51, 55–60, 63, 65–67, 69, 70, 73–77, 79, 82]. BAL culture alone was the sole reference standard in 18 (58.1%) out of the 31 studies [40, 41, 43, 45, 49, 55, 56,
Page 5 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
Table 1 Quality assessment checklist scores
green tick = acceptable quality, red box = unacceptable quality
Page 6 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
Tabl
e 2
Stud
ies
com
parin
g in
dex
test
to a
mic
robi
olog
ical
refe
renc
e st
anda
rd
Refe
renc
esSt
udy
popu
latio
nIn
dex
test
Refe
renc
e te
stRe
sults
(95%
con
fiden
ce in
terv
al w
here
av
aila
ble)
Coun
try
n =
M
ean
age
M:F
ratio
Alb
ert e
t al.
[57]
Cana
da70
558
.92.
9G
ram
sta
in o
f eith
er E
TA o
r BA
Lsa
me
sam
ple
(ETA
or B
AL)
pos
itive
cu
lture
resu
lt fo
r pat
hoge
nic
bact
eria
an
y qu
antit
y
Sens
= 7
4%Sp
ec =
72%
κ =
0.3
6 (0
.31–
0.40
)
Ana
nd e
t al.
[56]
USA
105
51.5
1.4
sTRE
M‑1
ELI
SA in
BA
LBA
L cu
lture
> 1
03 CFU
/mL
Sens
= 4
2.1%
Spec
= 7
5.6%
Bald
esi e
t al.
[55]
Fran
ce12
762
.52.
3BA
L cu
lture
> 1
04 CFU
/mL
(unc
orre
cted
fo
r dilu
tion
fact
or)
BAL
cultu
re >
104 C
FU/m
L (c
orre
cted
for
dilu
tion
fact
or u
sing
pla
sma/
BAL
urea
)Se
ns =
97.
7%Sp
ec =
98%
Carv
alho
et a
l. [5
4]Br
azil
2259
.41
com
paris
on o
f thr
ee s
ampl
ing
tech
‑ni
ques
(ETA
, min
iBA
L, a
nd B
AL)
No
men
tion
whi
ch is
con
side
red
inde
x te
st o
r ref
eren
ce s
tand
ard
Sens
= N
RSp
ec =
NR
Cla
vel e
t al.
[51]
Fran
ce12
065
3.1
qPC
R fro
m B
AL
equi
vale
nt to
> 1
04 CFU
/m
L an
d qP
CR
from
ETA
equ
ival
ent
to >
106 C
FU/m
L
BAL
cultu
re >
104 C
FU/m
L or
ETA
cul
‑tu
re >
106 C
FU/m
LqP
CR fr
om B
ALSe
ns =
89.
2%Sp
ec =
97.
1%qP
CR fr
om E
TASe
ns =
71.
8%Sp
ec =
96.
6%
Conw
ay M
orris
et a
l. [7
4]U
K72
571.
5BA
L IL
‑1β
and
IL‑8
BAL
cultu
re >
104 C
FU/m
LSe
ns =
94%
Spec
= 6
4%
Dou
glas
et a
l. [5
0]U
SA33
55N
/RM
ini B
AL
auto
mat
ed m
icro
scop
yM
ini B
AL
cultu
re >
104 C
FU/m
LSe
ns =
100
%Sp
ec =
97%
Elm
ahal
awy
et a
l. [4
9]Eg
ypt
4045
.43.
0Pe
ntra
xin
3 EL
ISA
in B
AL
BAL
cultu
re >
104 C
FU/m
LSe
ns =
96.
7%Sp
ec =
100
%AU
ROCC
= 0
.966
(0.9
85 to
1)
Fujit
ani e
t al.
[47]
USA
256
57.5
2.1
ETA
cul
ture
Min
i BA
L cu
lture
> 1
04 CFU
/mL
Sens
= 6
5.4%
Spec
= 5
6.1%
κ =
0.2
2 (0
.17–
0.27
)
Ged
ik e
t al.
[46]
Turk
ey31
561.
4ET
A c
ultu
re >
105 C
FU/m
LM
ini B
AL
cultu
re >
104 C
FU/m
Lκ =
0.8
04, p
= 0
.005
Gol
dber
g et
al.
[45]
USA
229
492.
0G
ram
sta
in o
f BA
LBA
L cu
lture
> 1
05 CFU
/mL
Sens
= 9
0%Sp
ec =
67%
Gul
er e
t al.
[43]
Turk
ey50
522.
1M
odifi
ed C
PIS
BAL
cultu
re >
104 C
FU/m
LCP
IS >
7Se
ns =
80%
Spec
= 1
7%CP
IS >
6Se
ns =
76%
Spec
= 1
5%CP
IS ≥
6Se
ns =
80.
7%Sp
ec =
16.
6%CP
IS ≥
5Se
ns =
80%
Spec
= 1
0%
Page 7 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
Tabl
e 2
(con
tinue
d)
Refe
renc
esSt
udy
popu
latio
nIn
dex
test
Refe
renc
e te
stRe
sults
(95%
con
fiden
ce in
terv
al w
here
av
aila
ble)
Coun
try
n =
M
ean
age
M:F
ratio
Has
him
oto
et a
l. [4
2]Ja
pan
5141
1.4
Sem
i‑qua
ntita
tive
Gra
m s
tain
or c
ultu
re
of E
TA o
r BA
L (n
ot o
ther
wis
e sp
ecifi
ed)
ETA
cul
ture
> 1
06 CFU
/mL
Gra
m st
ain
Sens
= 9
5%Sp
ec =
61%
κ =
0.5
9 (0
.45–
0.72
)Cu
lture
Sens
= 9
6%Sp
ec =
40%
κ =
0.4
(0.2
5–0.
54)
Hel
lyer
et a
l. [4
1]U
K15
056
.32.
9BA
L IL
‑1β
and
IL‑8
BAL
cultu
re >
104 C
FU/m
LSe
ns =
100
%Sp
ec =
44.
3%
Jack
son
et a
l. [4
0]U
SA73
523.
5BA
L—un
ilate
ral
BAL—
bila
tera
lSe
ns =
73%
Spec
= 8
2%
Jiao
et a
l. [6
5]C
hina
9248
1.0
Seru
m P
CT
Seru
m IL
‑6Se
rum
CRP
BAL
cultu
re >
104 C
FU/m
LPC
TSe
ns =
91%
Spec
= 7
1%IL-
6Se
ns =
58%
Spec
= 6
4%CR
PSe
ns =
52%
Spec
= 7
4%
Jung
et a
l. [6
3]Fr
ance
5761
2.2
BAL
Proc
alci
toni
nBA
L cu
lture
> 1
04 CFU
/mL
Sens
= 9
4%Sp
ec =
75%
Knei
ding
er e
t al.
[60]
Aus
tria
132
622.
1BA
L cu
lture
> 1
04 CFU
/mL
afte
r 24
h st
or‑
age
at 4
°C a
nd a
fter
sto
rage
at −
80
°CBA
L cu
lture
> 1
04 CFU
/mL
afte
r im
med
i‑at
e cu
lture
Imm
edia
te c
ultu
re v
s del
ayed
cul
ture
(4 °C
)Se
ns =
96.
5%Sp
ec =
100
%Im
med
iate
cul
ture
vs d
elay
ed c
ultu
re
(− 8
0 °C
)Se
ns =
50.
4%Sp
ec =
100
%
Kwon
et a
l. [5
9]Ko
rea
6465
2.6
qPC
R of
BA
L flu
id o
r bro
nchi
al w
ashi
ngs
BAL
cultu
re >
104 C
FU/m
L or
bro
nchi
al
was
hing
> 1
05 CFU
/mL
Sens
= 8
8.9%
Spec
= 8
8.9%
Leo
et a
l. [5
8]M
exic
o21
422.
0m
ini B
AL
(usi
ng c
ut N
G tu
be) >
104 C
FU/
mL
BAL
cultu
re >
104 C
FU/m
LSe
ns =
92.
8%Sp
ec =
85%
Lins
sen
et a
l. [6
7]U
SA11
7N
/RN
/RBA
L PC
T an
d C
RPBA
L cu
lture
> 1
04 CFU
/mL
or >
2%
cel
ls
with
intr
acel
lula
r org
anis
ms
PCT
AUC
ROCC
= 0
.448
CRP
AUC
ROCC
= 0
.477
Page 8 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
Tabl
e 2
(con
tinue
d)
Refe
renc
esSt
udy
popu
latio
nIn
dex
test
Refe
renc
e te
stRe
sults
(95%
con
fiden
ce in
terv
al w
here
av
aila
ble)
Coun
try
n =
M
ean
age
M:F
ratio
Lins
sen
et a
l. [7
5]U
SA28
260
.32.
1Va
rious
BA
L cy
tolo
gica
l par
amet
ers
incl
udin
g to
tal c
ell c
ount
, alv
eola
r mac
‑ro
phag
es, l
ymph
ocyt
es, n
eutr
ophi
ls,
eosi
noph
ils, m
ast c
ells
, inf
ecte
d ce
lls; i
n is
olat
ion
or in
com
bina
tion
BAL
cultu
re >
104 C
FU/m
LAU
ROCC
for v
ario
us c
ytol
ogic
al p
aram
eter
sTo
tal c
ell c
ount
= 0
.647
Alv
eola
r mac
roph
ages
= 0
.313
Lym
phoc
ytes
= 0
.381
Neu
trop
hils
= 0
.705
Eosi
noph
ils =
0.5
89M
ast c
ells
= 0
.557
Infe
cted
cel
ls (%
) = 0
.904
AURO
CC fo
r com
bina
tions
of c
ytol
ogic
al
para
met
ers
Infe
cted
cel
ls (%
) + P
MN
s (%
) = 0
.892
Infe
cted
cel
ls (%
) + To
tal c
ell c
ount
= 0
.890
Luna
et a
l. [6
9]A
rgen
tina
283
71.3
1.1
ETA
cul
ture
> 1
03 CFU
/mL
BAL
cultu
re >
104 C
FU/m
LSe
ns =
NR
Spec
= N
R
Luyt
et a
l. [7
0]Fr
ance
4160
2.4
seru
m P
CT
1st d
ay o
f clin
ical
sus
pici
on
of V
AP
BAL
cultu
re >
104 C
FU/m
LSe
ns =
72%
Spec
= 2
4%
Mon
godi
et a
l. [7
3]Fr
ance
9966
3.7
Vplu
s‑Ea
gram
(ven
tilat
or‑a
ssoc
iate
d pn
eum
onia
lung
ultr
asou
nd s
core
and
gr
am s
tain
of E
TA)
BAL
cultu
re >
104 C
FU/m
LSe
ns =
81%
Spec
= 4
1%
Oud
huis
et a
l. [6
6]N
ethe
rland
s20
762
1.7
ETA
cul
ture
> 1
05 CFU
/mL
BAL
cultu
re >
104 C
FU/m
L or
> 2
% c
ells
w
ith in
trac
ellu
lar o
rgan
ism
sSe
ns =
65%
Spec
= 4
8%
Refa
at e
t al.
[76]
Egyp
t66
NR
NR
BAL
com
posi
te b
iom
arke
r (C
RP, P
CT,
ne
utro
phils
, MIF
, sTR
EM‑1
, suP
AR)
BAL
cultu
re >
10
CFU
/mL
Sens
= 7
6%Sp
ec =
62%
Schn
abel
et a
l. [4
8]N
ethe
rland
s10
061
.32.
3VO
C in
exh
aled
bre
ath
BAL
cultu
re >
104 C
FU/m
L or
> 2
% c
ells
w
ith in
trac
ellu
lar o
rgan
ism
sSe
ns =
75.
8%Sp
ec =
73.
0%
Scho
lte e
t al.
[77]
Net
herla
nds
311
NR
NR
ETA
Gra
m s
tain
ETA
Cul
ture
BALF
Gra
m s
tain
BAL
cultu
re >
104 C
FU/m
L or
> 2
% c
ells
w
ith in
trac
ellu
lar o
rgan
ism
sET
A G
ram
stai
nSe
ns =
65%
Spec
= 7
2%ET
A Cu
lture
(any
thre
shol
d)Se
ns =
82%
Spec
= 4
2%BA
LF G
ram
stai
n (>
0)
Sens
= 8
2%Sp
ec =
66%
Vans
pauw
en e
t al.
[79]
Net
herla
nds
196
58.8
1.7
BAL
Cla
ra C
ell p
rote
in 1
0 EL
ISA
BAL
cultu
re >
104 C
FU/m
L or
> 2
% c
ells
w
ith in
trac
ellu
lar o
rgan
ism
sAU
ROCC
of 0
.586
(0.4
96–0
.676
)
Yagm
urdu
r et a
l. [8
2]Tu
rkey
5971
0.73
ETA
cul
ture
> 1
04 CFU
/mL
BAL
cultu
re >
104 C
FU/m
LSe
ns =
60%
Spec
= 3
9%
Zagl
i et a
l. [8
3]Ita
ly22
156
2.7
Che
st E
chog
raph
y an
d Pr
ocal
cito
nin
Pulm
onar
y In
fect
ion
Scor
e >
5ET
A c
ultu
re >
104 C
FU/m
LSe
ns =
80.
5%Sp
ec =
85.
2%
Page 9 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
Tabl
e 3
Stud
ies
com
parin
g in
dex
test
to a
com
posi
te re
fere
nce
stan
dard
Refe
renc
eSt
udy
popu
latio
nIn
dex
test
Refe
renc
e te
stRe
sults
(95%
con
fiden
ce in
terv
als
whe
re a
vaila
ble)
Coun
try
n =
M
ean
age
M:F
ratio
Cha
rles
et a
l. [5
3]Fr
ance
9061
.12.
3Se
rum
PC
T (d
ay o
f firs
t sus
pici
on o
f cl
inic
al in
fect
ion)
All
of (1
) new
lung
infil
trat
e on
the
ches
t X‑r
ay; (
2) E
TA c
ultu
re >
106 C
FU/
mL;
(3) C
PIS ≥
6 p
oint
s; (4
) at l
east
2
SIRS
crit
eria
Sens
= 6
5.2%
Spec
= 8
3%
Che
n et
al.
[52]
Chi
na49
541.
45Se
rum
PC
Tse
rum
CRP
CPI
S
(1) P
ersi
sten
t or n
ew in
vasi
ve s
hado
ws
in th
e lu
ng; (
2) A
t lea
st tw
o be
low
ite
ms:
tem
pera
ture
mor
e th
an
38 °C
or l
ess
than
36
°C; l
euco
cyte
co
unt >
10
or <
4 ×
10/
L; p
urul
ent
sput
um; (
3) A
ny o
f the
item
bel
ow:
bron
chos
copi
c as
pira
tion
or s
putu
m
spec
imen
bac
teria
l cul
ture
+++
or
path
ogen
ic b
acte
ria c
ultu
red
from
bl
ood
CRP
Sens
= 6
8.0%
Spec
= 5
8.3%
PCT
Sens
= 6
0.0%
Spec
= 8
7.5%
CPIS
Sens
= 7
2.0%
Spec
= 7
5.0%
Gro
ver e
t al.
[44]
UK
9159
1.5
7 m
arke
r sco
re: B
AL/
bloo
d ra
tio
mTR
EM‑1
and
mC
D11
b, B
ALF
sTR
EM‑
1, IL
‑8 a
nd IL
‑1b,
and
ser
um C
RP a
nd
IL‑6
VAP
was
pre
defin
ed a
s C
PIS
> 5
and
posi
tive
BALF
mic
robi
olog
y. N
on‑V
AP
was
pre
defin
ed a
s C
PIS
scor
e <
6 a
nd
nega
tive
mic
robi
olog
y
Sens
= 8
8.9%
Spec
= 1
00%
Jova
novi
c et
al.
[64]
Serb
ia39
47.9
5.5
Seru
m s
CD
14‑S
TPC
TC
RPLe
ucoc
yte
coun
t
New
per
sist
ent p
ulm
onar
y in
filtr
ates
(n
ot o
ther
wis
e ex
plai
nabl
e) o
n C
XR >
48
h af
ter a
dmis
sion
to th
e IC
U,
PLU
S on
e sy
stem
ic a
nd tw
o pu
lmo‑
nary
crit
eria
Syst
emic
crit
eria
Feve
r > 3
8 °C
, whi
te c
ell c
ount
< 4
000
WBC
/mm
3 or >
12,
000
WBC
/mm
3
alte
red
men
tal s
tatu
s, w
ith n
o ot
her
reco
gniz
ed c
ause
(for
adu
lts o
lder
th
an 7
0 ye
ars
of a
ge)
Pulm
onar
y cr
iteria
new
ons
et o
f pur
ulen
t spu
tum
(or a
ch
ange
in th
e ch
arac
ter o
f the
spu
‑tu
m, i
ncre
ased
resp
irato
ry s
ecre
tions
or
incr
ease
d su
ctio
ning
requ
ire‑
men
ts),
wor
seni
ng g
as e
xcha
nge
(des
atur
a‑tio
ns, i
ncre
ased
oxy
gen
requ
irem
ents
or
incr
ease
d ve
ntila
tor d
eman
d),
new
ons
et o
r wor
seni
ng c
ough
, and
dy
spno
ea, t
achy
pnoe
a, ra
les
or b
ron‑
chia
l bre
ath
soun
ds
sCD
14-S
TAU
ROCC
= 0
.908
PCT
AURO
CC =
0.8
63CR
PAU
ROCC
= 0
.703
Leuc
ocyt
e co
unt A
URO
CC =
0.6
68
Page 10 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
Tabl
e 3
(con
tinue
d)
Refe
renc
eSt
udy
popu
latio
nIn
dex
test
Refe
renc
e te
stRe
sults
(95%
con
fiden
ce in
terv
als
whe
re a
vaila
ble)
Coun
try
n =
M
ean
age
M:F
ratio
Klei
n Kl
ouw
enbe
rg e
t al.
[61]
Net
herla
nds
2080
621.
6C
DC
sur
veill
ance
defi
nitio
n (2
013)
Exis
ting
loca
l sur
veill
ance
crit
eria
di
vide
d in
to p
ossi
ble,
pro
babl
e, a
nd
defin
ite V
AP
Poss
ible
(CPI
S >
6, d
ubio
us a
bnor
mal
i‑tie
s on
radi
ogra
phic
exa
min
atio
n,
sem
i‑qua
ntita
tive
cultu
re fr
om
resp
irato
ry s
ecre
tions
—ET
A o
r bro
n‑ch
osco
pic
aspi
rate
)Pr
obab
le (C
PIS
> 6
, new
or p
rogr
es‑
sive
infil
trat
es, c
onso
lidat
ion,
ca
vita
tion
or p
leur
al e
ffusi
on, B
AL
cultu
re >
104 C
FU/m
L or
PSB
cul
‑tu
re >
103 C
FU/m
L O
R po
sitiv
e bl
ood
cultu
re w
ith p
atho
gen
also
isol
ated
fro
m a
irway
cul
ture
)D
efini
te (C
PIS
> 6
, new
or p
rogr
essi
ve
infil
trat
es, c
onso
lidat
ion,
cav
ita‑
tion
or p
leur
al e
ffusi
on O
R ra
dio‑
grap
hic
evid
ence
of l
ung
absc
ess
or
empy
ema,
his
topa
thol
ogic
evi
denc
e of
pne
umon
ia (a
bsce
ss w
ith P
MN
co
ncen
trat
ion
and
posi
tive
tissu
e cu
lture
) OR
if em
pyem
a, p
ositi
ve
cultu
re o
f asp
irate
))
Sens
= 2
2% (f
or p
roba
ble
or d
efini
te
refe
renc
e st
anda
rd V
AP)
Spec
= 9
8%
Klom
pas
et a
l. [6
2]U
SA45
955
.31.
5O
bjec
tive
algo
rithm
of e
lect
roni
c pa
tient
reco
rd (p
recu
rsor
of C
DC
su
rvei
llanc
e de
finiti
on 2
013)
CD
C d
efini
tion
(200
8)Se
ns =
95
Spec
= 1
00
Page 11 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
Tabl
e 3
(con
tinue
d)
Refe
renc
eSt
udy
popu
latio
nIn
dex
test
Refe
renc
e te
stRe
sults
(95%
con
fiden
ce in
terv
als
whe
re a
vaila
ble)
Coun
try
n =
M
ean
age
M:F
ratio
Liu
et a
l. [6
8]C
hina
162
61.6
1.5
BAL
neut
roph
il in
trac
ellu
lar o
rgan
ism
s(1
) his
topa
thol
ogic
al d
iagn
osis
per
‑fo
rmed
with
in 7
day
s of
bro
ncho
s‑co
py O
R(2
) BA
L cu
lture
≥ 1
04 CFU
/mL,
and
re
spon
ded
to a
ntib
iotic
ther
apy
OR
(3) r
apid
cav
itatio
n of
the
lung
infil
trat
e on
che
st x
‑ray
film
or C
T sc
an a
ssoc
i‑at
ed w
ith re
spon
ded
to a
ntib
iotic
th
erap
y O
R(4
) pos
itive
cul
ture
of t
he p
leur
al
effus
ion,
and
the
sam
e m
icro
orga
n‑is
ms
isol
ated
from
cul
ture
s of
ple
ural
eff
usio
n an
d lo
wer
resp
irato
ry tr
act
secr
etio
ns, a
nd re
spon
ded
to a
ntib
i‑ot
ic th
erap
y O
R(5
) com
plet
e re
solu
tion
with
app
ropr
i‑at
e an
tibio
tic th
erap
y w
ith n
o ot
her
dise
ase
expl
aini
ng c
hest
radi
ogra
ph
abno
rmal
ity
Sens
= 9
4.12
%Sp
ec =
88.
33%
Mau
ri et
al.
[71]
Italy
8259
2.6
BAL
fluid
pen
trax
in 3
1. N
ew a
nd p
ersi
sten
t rad
iogr
aphi
c in
filtr
ates
ass
ocia
ted
with
at l
east
two
of th
e fo
llow
ing:
a. In
tern
al b
ody
tem
pera
ture
> 3
8 °C
,b.
Whi
te b
lood
cel
ls c
ount
> 1
2,00
0 or
< 4
000
cells
/mm
3 and
/or
c. P
urul
ent t
rach
eobr
onch
ial s
ecre
tions
; A
ND
2. B
AL
cultu
re >
104 C
FU/m
L an
d/or
si
gnifi
cant
non
cont
amin
ant v
iral l
oad
Sens
= 9
2%Sp
ec =
60%
Page 12 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
Tabl
e 3
(con
tinue
d)
Refe
renc
eSt
udy
popu
latio
nIn
dex
test
Refe
renc
e te
stRe
sults
(95%
con
fiden
ce in
terv
als
whe
re a
vaila
ble)
Coun
try
n =
M
ean
age
M:F
ratio
Med
ford
et a
l. [7
2]U
K15
062
.31.
5ET
A c
ultu
re >
105 o
r BA
L cu
lture
> 1
04N
ew/p
rogr
essi
ve C
XR in
filtr
ates
with
‑ou
t oth
erob
viou
s ca
use
in p
atie
nts
mec
hani
cally
ve
ntila
ted
for m
ore
than
4 d
ays
in
the
ICU
and
at l
east
2 o
f the
follo
w‑
ing:
tem
pera
ture
≥ 3
8 °C
or ≤
35
°C,
whi
te c
ell c
ount
≥ 1
2 or
≤ 4
× 1
09 /L,
puru
lent
trac
heob
ronc
hial
sec
retio
ns,
with
incr
easi
ng o
xyge
n re
quire
‑m
ents
, com
pute
d to
mog
raph
y ev
i‑de
nce
of a
rapi
dly
cavi
tatin
g in
filtr
ate,
po
sitiv
e pl
eura
l flui
d cu
lture
and
/or
hist
olog
ical
evi
denc
e of
neu
trop
hilic
al
veol
itis,
bron
chio
litis
, and
con
soli‑
datio
n in
con
junc
tion
with
ple
ural
flu
id m
icro
biol
ogy,
CT
evid
ence
, and
hi
stol
ogic
al e
vide
nce
BAL
Sens
= 6
4.1%
Spec
= 8
3.0%
ETA
Sens
= 4
2.6%
Spec
= 3
3.7%
Text
oris
et a
l. [7
8]Fr
ance
7730
.75
NR
bloo
d Tr
ansc
ripto
me
DN
A m
icro
arra
y an
alys
is (H
uSG
9 k)
puru
lent
bro
nchi
al s
putu
m; b
ody
tem
pera
ture
mor
e th
an 3
8 °C
or l
ess
than
36
°C; l
euko
cyte
s m
ore
than
10
× 1
09 /L o
r les
s th
an 4
× 1
09 /L;
ches
t rad
iogr
aph
show
ing
new
or
prog
ress
ive
infil
trat
es; B
AL
cul‑
ture
≥ 1
04 CFU
/mL,
or E
TA c
ul‑
ture
≥ 1
06 CFU
/mL
Sens
= N
RSp
ec =
NR
Vern
ikos
et a
l. [8
0]G
reec
e54
721.
31)
Joh
anse
n cr
iteria
,2)
Mod
ified
CPI
S >
6 R
EF3)
Joh
anse
n cr
iteria
com
bine
d w
ith
rela
tive
neut
roph
il co
unt
4) C
PIS
> 6
com
bine
d re
lativ
e ne
utro
‑ph
il co
unt
5) R
PDM
Ia sco
re
CD
C d
efini
tion
(201
5)Jo
hans
en c
riter
iaSe
ns =
85.
7%Sp
ec =
73.
7%M
odifi
ed C
PIS
> 6
Sens
= 6
2.9%
Spec
= 7
3.7%
Joha
nsen
crit
eria
com
bine
d w
ith re
lativ
e ne
utro
phil
coun
t (20
% c
ut o
ff)
Sens
= 6
7.6%
Spec
= 8
1.3%
CPIS
> 6
com
bine
d re
lativ
e ne
utro
phil
coun
t (20
% c
ut o
ff)
Sens
= 4
7.1%
Spec
= 8
1.3%
RPD
MI s
core
Sens
= 9
4.3%
Spec
= 8
4.2%
Page 13 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
Tabl
e 3
(con
tinue
d)
Refe
renc
eSt
udy
popu
latio
nIn
dex
test
Refe
renc
e te
stRe
sults
(95%
con
fiden
ce in
terv
als
whe
re a
vaila
ble)
Coun
try
n =
M
ean
age
M:F
ratio
Wal
tric
k et
al.
[81]
Braz
il16
8N
RN
RC
DC
defi
nitio
n (2
013)
CPI
S ≥
7 a
nd m
iniB
AL
cul‑
ture
> =
104 C
FU/m
LSe
ns =
37%
Spec
= 1
00%
a RPD
MI s
core
: rad
iolo
gica
l pro
gres
sion
, pur
ulen
t sec
retio
ns, d
urat
ion
of m
echa
nica
l ven
tilat
ion,
imm
unos
uppr
essi
on
Page 14 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
58, 60, 63, 65, 69, 70, 73–76, 82]. Where used, the BAL culture threshold for positivity included > 10 CFU/mL [76], > 103 CFU/mL [56], > 104 CFU/mL [40, 41, 43, 49, 55, 58, 60, 63, 65, 69, 70, 73–75, 82], and > 105 CFU/mL [45]. Three studies using BAL culture > 104 CFU/mL added an additional stipulation on BAL culture results: one requir-ing correction of microbial growth for plasma to BAL urea ratio [55], one requiring that lavage was bilateral [40], and one specifying culture took place immediately after lavage [60]. BAL culture was used in combination with another criterion regarding assessment of BAL on an additional eight occasions out of the 26 using BAL (30.8%); five out of these eight (62.5%) BAL culture or > 2% lavage cells containing intracellular organisms [48, 66, 67, 77, 79], one out of the eight (12.5%) BAL cul-ture or bronchial washings culture (> 105 CFU/mL) [59], and two out of the eight (11.1%) BAL culture or ETA cul-ture (> 106 CFU/mL [51] or no threshold specified [57]. On the remaining five out of 31 (16.1%) occasions where BAL culture was not incorporated into the microbio-logical reference standard, three studies used mini-BAL culture > 104 CFU/mL [46, 47, 50], one study used ETA culture > 106 CFU/mL [42]m, and one study used ETA culture > 104 CFU/mL [83], as sole reference standards.
Table 3 summarises the remaining 12/44 (27.2%) stud-ies which compared an index test to a composite refer-ence standard or clinical scoring system [44, 52, 53, 61, 62, 64, 68, 71, 72, 78, 80, 81]. An iteration of the CDC VAP definition was used in two out of the 12 studies (16.7%), one using the 2008 iteration for surveillance of VAP [62] and one using the 2015 iteration for surveillance of VAP (80]. One additional study [64] used a composite reference standard almost identical to the 2008 iteration of the CDC VAP surveillance criteria. The 2008 itera-tion of the CDC surveillance criteria does not include any microbiological assessment of respiratory samples, and non-culture methods or histopathology may sup-plant microbiological culture in the 2010 and 2015 iter-ations of the CDC surveillance criteria [28, 62, 85]. For the remaining nine studies; four out of the nine (44.4%) explicitly incorporated the clinical pulmonary infection score (CPIS) into a wider set of criteria [44, 53, 61, 81]. Seven out nine (77.8%) incorporated radiological assess-ment [52, 53, 64, 68, 71, 72, 78], eight out of nine (88.9%) incorporated additional clinical signs and symptoms [44, 52, 53, 61, 71, 72, 78, 81] either as part of an existing scor-ing system such as CPIS or de novo, and all nine studies (100%) incorporated some microbiological assessment into the combined reference standard [44, 52, 53, 64, 68, 71, 72, 78, 81]. In seven of those nine studies (77.8%) positive microbiology was a mandatory criterion for VAP diagnosis [44, 52, 53, 64, 71, 78, 81], and in two of those nine (22.2%), positive microbiological cultures were an
optional criterion for VAP diagnosis [68, 72]. Amongst all included studies microbiological assessment did not form any part of the mandatory or optional criteria for VAP diagnosis in only two studies [62, 64], diagnosis of VAP included an optional microbiological assessment com-ponent in another two studies (i.e. VAP diagnosis could be made without recourse to microbiological assess-ment) [68, 72], and in 39 studies microbiological assess-ment was the sole or a mandatory component [40–53, 55–60, 63–71, 73–79, 81–83]. Four studies incorporated an optional histopathologic element into the reference standard [61, 68, 72, 80], but it was mandatory in none.
Out of all 44 included studies, 37 (84%) incorporate BAL in either the reference standard or index test [40–51, 54–60, 63, 65–79, 81, 82]. Twenty two studies (50%) included a precise lavage procedure in the methodol-ogy [40, 41, 43, 45, 48, 51, 55–58, 60, 63, 66–69, 71, 72, 74–76, 82]. Of these, 14 described an initial discard of aspirated fluid, considered to be uninformative bronchial fluid [40, 41, 43, 51, 57, 58, 60, 63, 68, 69, 71, 72, 74, 82]. The median volume of instilled fluid used to generate the discarded fluid was 20 mL (range 20 mL to 50 mL). The median total volume of instilled fluid (including that intended for discard) was 150 mL (range 80 mL to 200 mL).
DiscussionTo the best of our knowledge, this is the first and most comprehensive systematic review aiming to evaluate the reference standard tests used to evaluate novel index tests for suspected VAP since the publication of Rea-Neto and colleagues systematic review of diagnostic methods in 2008 [32]. We reviewed papers comparing a novel index test against a chosen reference standard to identify what reference standards have been used in diagnostic evalua-tion research for VAP. To deliver a high-quality system-atic review, we excluded papers with a high risk of bias and all papers included in this review fulfil at least 5 out of the 8 criteria we included from the CASP checklist.
The microbiological culture was the sole or a compo-nent criterion in the vast majority of studies. Overall, the culture of BAL fluid was the most common refer-ence standard, with the most common growth threshold being > 104 CFU/mL. This was occasionally used in com-bination with another reference standard, such as the demonstration of BAL cells with intracellular organisms exceeding 2% of the total number of cells. Composite ref-erence standards incorporating a variety of existing clini-cal scores, existing surveillance definitions, radiological assessments, clinical parameters, and microbiological methods including culture were used in the remain-ing studies. A large variation in practice, processes, and reference standards were detected, highlighting the
Page 15 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
inconsistency in the current diagnosis of VAP and mak-ing a meta-analysis of diagnostic accuracy challenging. Biological, clinical, and statistical heterogeneity makes comparisons across the different studies difficult and subjective. We display a variable and generally good qual-ity of the papers, and the review provides an indication of what has been and is being done in this area globally with respect to the use of reference standard in the diag-nostics of VAP. The line between composite criteria and a sole microbiological criterion was often blurred. Many studies in the sole microbiological criterion group had strict objective clinical and radiological enrolment crite-ria. Where these criteria are applied pre-enrolment and therefore applied to both index tests and reference stand-ards we have not incorporated them into a description of the reference standard.
A key question in diagnostic accuracy research when reference standards are imperfect is whether the refer-ence standard used to assess novel diagnostics should be ‘more inclusive’ (higher sensitivity, lower specificity) or ‘less inclusive’ (lower sensitivity, higher specificity). Using microbiological criteria alone exhibits good face validity but risks missing cases of ‘true VAP’ or including false positives through contamination (although prior speci-fication of clinically suspected VAP reduces this risk). Importantly, both possibilities are potentially strongly influenced by operator technique/expertise, especially for BAL; this contrasts with diagnostics reliant on blood sampling or imaging. BAL culture was the most com-mon microbiological method found in this review. The use of BAL culture is potentially problematic for sev-eral reasons. Firstly, in a recent systematic review, when compared to the reference standard of histopathological examination of lung tissue, BAL culture had a sensitivity of 71.1% and specificity of 79.6% [86] echoing previous findings that microbiological examination does not cor-relate well with histopathological examination [32]. Sec-ondly, the timing and nature of prior antibiotic therapy may adversely affect sample positivity [87, 88], although this problem is conceivably solved by incorporating a criterion addressing percentage of host cells contain-ing invading organisms, a measure not affected by prior antibiotic therapy [75]. Thirdly, the BAL procedure itself is not standardised, and the requirements for sample collection are not uniform. Whilst this may have little impact on bacterial growth, a fact confirmed by one of the included studies [55], the variety of studies that uti-lised bronchial discard may plausibly lead to a variety in sensitivity at detecting the causative pathogenic organ-ism. Sole microbiological criteria also risk introducing cases of ‘false VAP’ through contamination [87], although this risk is reduced by using distal or protected speci-mens. Of relevance, the quality and consistency of BAL
procedures are likely to be higher in studies than during routine clinical practice, which could further influence its validity.
Using composite criteria may conceivably address the problem of missing cases of ‘true VAP’, and the number or thresholds of additional criteria is not limited. Additional criteria can be made mandatory to increase specificity or made optional to increase sensitivity. Some studies in this review rely on existing surveillance definitions for VAP or use their own composite standards. The exist-ing surveillance definitions were designed to objectively and reproducibly monitor VAP rates not to identify true VAP in a robustly sensitive and specific manner, although as a quality indicator face validity amongst clinicians is important. Other composite studies incorporated radio-logical assessments into the reference standard. It has been shown that chest x-ray changes are not considered integral to the diagnosis by many clinicians [89], that the performance characteristics of chest x-ray may not meet the requirements as a diagnostic standard [90–92], and that inter- and intra-observer variability is high in chest x-ray assessment [93, 94]. These issues mean that incor-poration of radiology into any novel reference standard should be undertaken with caution. Many studies incor-porate clinical signs which plausibly reduces the risk of false positives, and although this makes physiological sense there is minimal evidence to support this. Klompas et al. showed, in the development of the novel CDC VAP surveillance algorithm, that deterioration in oxygenation after a period of stability was associated with clinically important outcomes but the addition of other clinical measures such as abnormal temperature, abnormal white blood cell count, or purulent secretions was not [95]. However, a lack of correlation with clinically important outcomes is not the same as a lack of correlation with a true diagnosis of VAP; this issue is relevant when the decision based on the test relates to a therapy (antibiotic use) rather than prognosis.
No studies relied upon histopathological diagnosis of VAP to confirm the diagnosis. This is not surprising for practical reasons: it cannot be routinely and safely under-taken in all patients with suspected VAP either at the time of the index test or later. Histopathological analysis may also be inaccurate due to sampling artefacts, the lack of representation of a small piece of tissue, and displace-ment in time from the period of peak infection. It is not possible to provide certainty about the appropriate refer-ence standard in diagnostic evaluation research for VAP following this systematic review, which simply identifies the methods chosen by researchers and confirms the lack of a standardised approach. Researchers must decide whether it is more important to be ‘more inclusive’ or ‘less inclusive’, and future comparisons may wish to
Page 16 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
employ the strategy deployed by one of the studies in this review [61]: using a graded certainty of VAP from pos-sible to probable to definite using a composite definition.
There are three main limitations to our review. Firstly, in order to be diagnosed with VAP, a patient must be at risk of VAP, and there is no standard definition for patients at risk. For the purposes of this study, we defined those at risk of VAP as those who have undergone more than 48 h of mechanical ventilation. Secondly, many included studies enrolled only patients with suspected VAP, and this means many listed reference standards must be prefixed with “clinically suspected VAP”. This level of clinical suspicion was not systematically collected by us. This is particularly noteworthy in considering the reference standards listed in Table 3. Thirdly, although data extraction for this review was completed before the impact of Coronavirus Disease 2019 (COVID-19), the pandemic nonetheless interfered with the delivery time of this review.
ConclusionBAL culture with a microbiological growth threshold of > 104 CFU/mL is the commonest reference stand-ard used to examine the utility of a novel index test for VAP amongst patients who are at risk for and clinically suspected of VAP. Composite reference standards were used in approximately 25% of reviewed studies. Nearly all reference standards for VAP identified in this review required some microbiological confirmation of infection. The studies identified in this review highlight the need for a standardised approach to diagnosis VAP which may include the development of a data-driven composite ref-erence standard from large cohort studies.
AbbreviationsBAL: Broncho‑alveolar lavage; CDC: Centers for disease control and prevention; CC‑10: Clara cell protein 10; COVID‑19: Coronavirus Disease 2019; CASP: Critical appraisal skills programme; CBA: Cytometric bead array; ETA: Endotracheal aspirates; ECDC: European centre for disease prevention and control; GC‑tof‑MS: Gas chromatography time‑of‑flight mass spectrometry; GS: Gram’s stain; ITU: Intensive therapy unite; LUS: Lung ultrasound; MeSH: Medical subject headings; CPIS: Modified clinical pulmonary infection score; NHSN/CDC: National healthcare safety network/Center for disease control and prevention; PCR: Polymerase chain reaction; PSB: Protected specimen brush; SQ: Semi quantitative; PCT: Serum procalcitonin; sTREM‑1: Type 1 soluble triggering receptor expressed on myeloid cells; U/S: Ultrasound; VAE: Ventilator‑asso‑ciated events; VAP: Ventilator‑associated pneumonia; VOCs: Volatile organic compounds.
Supplementary InformationThe online version contains supplementary material available at https:// doi. org/ 10. 1186/ s12890‑ 021‑ 01560‑0.
Additional file 1. MEDLINE search example.
Additional file 2. Quality assessment and data extraction form.
AcknowledgementsNot applicable.
Authors’ contributionsBA and AJA designed the review, and BA led the project. All authors con‑tribute and approve the review design and search strategy. BA, PM, and JG conducted the title/abstract screening. The quality assessment and data extraction were conducted by BA, THC, PM, ARA, SG, JS, WSJ, BCL, AW, and MC. The data and results were summarized by BA, AJA, THC, SG, JS, WSJ, BCL, AW, MC, interpreted by THC and BA, reviewed by KD and TSW, and approved by all authors. The manuscript was drafted BA and THC, checked by KD and TSW and read and approved by all authors. All authors read and approved the final manuscript.
FundingThis study was funded by Combating Antibiotic‑Resistant Bacteria Biopharma‑ceutical Accelerator (CARB‑X), https:// carb‑x. org, award Number 4500003353. AJA, JS, WJS, CL and AW were supported by the National Institute for Health Research Newcastle In Vitro Diagnostics Co‑operative. The views expressed are those of the author(s) and not necessarily those of the National Institute for Health Research, the National Health Services or the Department of Health and Social Care.
Availability of data and materialsThe datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participateNot applicable.
Consent to publishNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Author details1 College of Medicine and Health Sciences, Khalifa University, PO Box 127788, Abu Dhabi, UAE. 2 School of Health and Life Science, University of Northum‑bria, Newcastle upon Tyne, UK. 3 NIHR Newcastle In Vitro Diagnostics Co‑opera‑tive, Translational and Clinical Research Institute, Newcastle University, New‑castle upon Tyne, UK. 4 Translational Healthcare Technologies Group, Centre for Inflammation Research, Queen’s Medical Research Institute, University of Edinburgh, Edinburgh, UK. 5 York Health Economics Consortium, Enterprise House, Innovation Way, University of York, York, UK. 6 NIHR Newcastle In Vitro Diagnostics Co‑operative, The Newcastle Upon Tyne Hospitals NHS Founda‑tion Trust, Newcastle upon Tyne, UK. 7 Laboratory Medicine, Newcastle‑Upon‑Tyne Hospitals Foundation Trust, Newcastle upon Tyne, UK. 8 Edinburgh Critical Care Research Group, University of Edinburgh, Edinburgh, UK.
Received: 11 March 2021 Accepted: 2 June 2021
References 1. Craven TH, Wojcik G, McCoubrey J, Brooks O, Grant E, Keating S, et al.
Ventilator‑associated pneumonia surveillance using two methods. J Hosp Infect. 2020;104(4):522–8.
2. Fang X, Mei Q, Fan X, Zhu C, Yang T, Zhang L, et al. Diagnostic value of metagenomic next‑generation sequencing for the detection of patho‑gens in bronchoalveolar lavage fluid in ventilator‑associated pneumonia patients. Front Microbiol. 2020;11:599756.
Page 17 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
3. Keyt H, Faverio P, Restrepo MI. Prevention of ventilator‑associated pneu‑monia in the intensive care unit: a review of the clinically relevant recent advancements. Indian J Med Res. 2014;139(6):814–21.
4. Steen J, Vansteelandt S, De Bus L, Depuydt P, Gadeyne B, Benoit DD, et al. Attributable mortality of ventilator‑associated pneumonia: replicating findings, revisiting methods. Ann Am Thorac Soc. 2020;18(5):830–7.
5. Colombo SM, Palomeque AC, Li BG. The zero‑VAP sophistry and con‑troversies surrounding prevention of ventilator‑associated pneumonia. Intensive Care Med. 2020;46(2):368–71.
6. Keneally RJ, Peterson TJ, Benjamin JR, Hawkins K, Davison D. Making venti‑lator associated pneumonia rate a meaningful quality marker. J Intensive Care Med. 2020. https:// doi. org/ 10. 1177/ 08850 66620 952763.
7. Vincent JL, Bihari DJ, Suter PM, Bruining HA, White J, Nicolas‑Chanoin MH, et al. The prevalence of nosocomial infection in intensive care units in Europe. Results of the European Prevalence of Infection in Inten‑sive Care (EPIC) Study. EPIC International Advisory Committee. JAMA. 1995;274(8):639–44.
8. Rello J, Ollendorf DA, Oster G, Vera‑Llonch M, Bellm L, Redman R, et al. Epidemiology and outcomes of ventilator‑associated pneumonia in a large US database. Chest. 2002;122(6):2115–21.
9. Kollef MH, Hamilton CW, Ernst FR. Economic impact of ventilator‑associated pneumonia in a large matched cohort. Infect Control Hosp Epidemiol. 2012;33(3):250–6.
10. Luckraz H, Manga N, Senanayake EL, Abdelaziz M, Gopal S, Charman SC, et al. Cost of treating ventilator‑associated pneumonia post cardiac sur‑gery in the National Health Service: Results from a propensity‑matched cohort study. J Intensive Care Soc. 2018;19(2):94–100.
11. Fagon JY, Chastre J, Hance AJ, Montravers P, Novara A, Gibert C. Noso‑comial pneumonia in ventilated patients: a cohort study evaluating attributable mortality and hospital stay. Am J Med. 1993;94(3):281–8.
12. Heyland DK, Cook DJ, Griffith L, Keenan SP, Brun‑Buisson C. The attribut‑able morbidity and mortality of ventilator‑associated pneumonia in the critically ill patient. The Canadian Critical Trials Group. Am J Respir Crit Care Med. 1999;159(4 Pt 1):1249–56.
13. Bekaert M, Timsit J‑F, Vansteelandt S, Depuydt P, Vésin A, Garrouste‑Orgeas M, et al. Attributable mortality of ventilator‑associated pneu‑monia: a reappraisal using causal analysis. Am J Respir Crit Care Med. 2011;184(10):1133–9.
14. Ego A, Preiser J‑C, Vincent J‑L. Impact of diagnostic criteria on the inci‑dence of ventilator‑associated pneumonia. Chest. 2015;147(2):347–55.
15. Estella A, Alvarez‑Lerma F. Should the diagnosis of ventilator associated pneumonia be improved? Med Intensiva. 2011;35(9):578–82.
16. Ali HS, Khan FY, George S, Shaikh N, Al‑Ajmi J. Epidemiology and outcome of ventilator‑associated pneumonia in a heterogeneous ICU population in Qatar. Biomed Res Int. 2016;2016:8231787.
17. Papazian L, Klompas M, Luyt C‑E. Ventilator‑associated pneumonia in adults: a narrative review. Intensive Care Med. 2020;46(5):888–906.
18. Skrupky LP, McConnell K, Dallas J, Kollef MH. A comparison of ventilator‑associated pneumonia rates as identified according to the National Healthcare Safety Network and American College of Chest Physicians criteria. Crit Care Med. 2012;40(1):281–4.
19. Hyllienmark P, Gårdlund B, Persson J‑O, Ekdahl K. Nosocomial pneu‑monia in the ICU: a prospective cohort study. Scand J Infect Dis. 2007;39(8):676–82.
20. Tejerina E, Frutos‑Vivar F, Restrepo MI, Anzueto A, Abroug F, Palizas F, et al. Incidence, risk factors, and outcome of ventilator‑associated pneumonia. J Crit Care. 2006;21(1):56–65.
21. Cook DJ, Walter SD, Cook RJ, Griffith LE, Guyatt GH, Leasa D, et al. Inci‑dence of and risk factors for ventilator‑associated pneumonia in critically ill patients. Ann Intern Med. 1998;129(6):433–40.
22. Kollef MH. Ventilator‑associated pneumonia. A multivariate analysis. JAMA. 1993;270(16):1965–70.
23. Kappstein I, Schulgen G, Beyer U, Geiger K, Schumacher M, Daschner FD. Prolongation of hospital stay and extra costs due to ventilator‑associated pneumonia in an intensive care unit. Eur J Clin Microbiol Infect Dis. 1992;11(6):504–8.
24. Rello J, Quintana E, Ausina V, Castella J, Luquin M, Net A, et al. Incidence, etiology, and outcome of nosocomial pneumonia in mechanically venti‑lated patients. Chest. 1991;100(2):439–44.
25. Dudeck MA, Horan TC, Peterson KD, Allen‑Bridson K, Morrell G, Pollock DA, et al. National Healthcare Safety Network (NHSN) Report, data
summary for 2010, device‑associated module. Am J Infect Control. 2011;39(10):798–816.
26. Suetens C, Morales I, Savey A, Palomar M, Hiesmayr M, Lepape A, et al. European surveillance of ICU‑acquired infections (HELICS‑ICU): methods and main results. J Hosp Infect. 2007;65(Suppl 2):171–3.
27. De Bus L, Gadeyne B, Steen J, Boelens J, Claeys G, Benoit D, et al. A com‑plete and multifaceted overview of antibiotic use and infection diagnosis in the intensive care unit: results from a prospective four‑year registration. Crit Care. 2018;22(1):241.
28. Craven TH, Wojcik G, McCoubrey J, Brooks O, Grant E, Reilly J, et al. Lack of concordance between ECDC and CDC systems for surveillance of ventila‑tor associated pneumonia. Intensive Care Med. 2018;44(2):265–6.
29. Martin‑Loeches I, Torres A, Rinaudo M, Terraneo S, de Rosa F, Ram‑irez P, et al. Resistance patterns and outcomes in intensive care unit (ICU)‑acquired pneumonia. Validation of European Centre for Disease Prevention and Control (ECDC) and the Centers for Disease Control and Prevention (CDC) classification of multidrug resistant organisms. J Infect. 2015;70(3):213–22.
30. Baselski V, Klutts JS, Baselski V, Klutts JS. Quantitative cultures of bron‑choscopically obtained specimens should be performed for optimal management of ventilator‑associated pneumonia. J Clin Microbiol. 2013;51(3):740–4.
31. Torres A, Niederman MS, Chastre J, Ewig S, Fernandez‑Vandellos P, Hanberger H, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital‑acquired pneumonia and ventilator‑associated pneumonia: Guidelines for the management of hospital‑acquired pneumonia (HAP)/ventilator‑associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur Respir J. 2017;50(3):1700582. https:// doi. org/ 10. 1183/ 13993 003. 00582‑ 2017.
32. Rea‑Neto A, Youssef NCM, Tuche F, Brunkhorst F, Ranieri VM, Reinhart K, et al. Diagnosis of ventilator‑associated pneumonia: a systematic review of the literature. Crit Care. 2008;12(2):R56.
33. Al‑Omari B, McMeekin P, Gray J, Aleen J, Dhaliwal K, Walsh T, et al. Protocol for systematic review of studies investigating ventilator‑associated pneumonia(VAP) diagnostic procedures in secondary care [Internet]. PROSPERO; CRD42019125449. 2019. https:// www. crd. york. ac. uk/ prosp ero/ displ ay_ record. php? Recor dID= 125449. Cited 24 Nov 2020.
35. Ma L‑L, Wang Y‑Y, Yang Z‑H, Huang D, Weng H, Zeng X‑T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: what are they and which is better? Mil Med Res. 2020;7(1):7.
36. Zeng X, Zhang Y, Kwong JSW, Zhang C, Li S, Sun F, et al. The methodologi‑cal quality assessment tools for preclinical and clinical studies, systematic review and meta‑analysis, and clinical practice guideline: a systematic review. J Evid Based Med. 2015;8(1):2–10.
37. Williams P, Bond CM, Burton C, Murchie P. A systematic review of the use, quality and effects of pelvic examination in primary care for the detection of gynaecological cancer. J Obstet Gynaecol. 2018;38(5):737.
38. Gomes PTM, Lima LHL, Bueno MKG, Araújo LA, Souza NM. Autism in Brazil: a systematic review of family challenges and coping strategies. J Pediatr (Rio J). 2015;91(2):111–21.
39. Smith T, Cross J, Poland F, Clay F, Brookes A, Maidment I, et al. Systematic review investigating multi‑disciplinary team approaches to screening and early diagnosis of dementia in primary care—what are the positive and negative effects and who should deliver it? Curr Alzheimer Res. 2018;15(1):5–17.
40. Jackson S‑R, Ernst NE, Mueller EW, Butler KL. Utility of bilateral bronchoal‑veolar lavage for the diagnosis of ventilator‑associated pneumonia in critically ill surgical patients. Am J Surg. 2008;195(2):159–63.
41. Hellyer TP, Morris AC, McAuley DF, Walsh TS, Anderson NH, Singh S, et al. Diagnostic accuracy of pulmonary host inflammatory mediators in the exclusion of ventilator‑acquired pneumonia. Thorax. 2015;70(1):41–7.
42. Hashimoto S, Shime N. Evaluation of semi‑quantitative scoring of Gram staining or semi‑quantitative culture for the diagnosis of ventilator‑asso‑ciated pneumonia: a retrospective comparison with quantitative culture. J Intensive Care. 2013;1(1):2.
Page 18 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
43. Guler E, Kahveci F, Akalin H, Sinirtas M, Bayram S, Ozcan B. Evaluation of a clinical pulmonary infection score in the diagnosis of ventilator‑associ‑ated pneumonia. SV. 2012;7(1):32–7.
44. Grover V, Pantelidis P, Soni N, Takata M, Shah PL, Wells AU, et al. A bio‑marker panel (Bioscore) incorporating monocytic surface and soluble TREM‑1 has high discriminative value for ventilator‑associated pneumo‑nia: a prospective observational study. PLoS ONE. 2014;9(10):e109686.
45. Goldberg AE, Malhotra AK, Riaz OJ, Aboutanos MB, Duane TM, Borchers CT, et al. Predictive value of broncho‑alveolar lavage fluid Gram’s stain in the diagnosis of ventilator‑associated pneumonia: a prospective study. J Trauma. 2008;65(4):871–6 (discussion 876).
46. Gedik H, Yahyaoğlu M, Fincancı M. The diagnostic accuracy of endotra‑cheal aspiration and mini‑bronchoalveolar lavage cultures in the diagno‑sis of ventilator associated pneumonia. Nobel Med. 2010;6:68–74.
47. Fujitani S, Cohen‑Melamed MH, Tuttle RP, Delgado E, Taira Y, Darby JM. Comparison of semi‑quantitative endotracheal aspirates to quantitative non‑bronchoscopic bronchoalveolar lavage in diagnosing ventilator‑associated pneumonia. Respir Care. 2009;54(11):1453–61.
48. Schnabel R, Fijten R, Smolinska A, Dallinga J, Boumans M‑L, Stobberingh E, et al. Analysis of volatile organic compounds in exhaled breath to diagnose ventilator‑associated pneumonia. Sci Rep. 2015;5:17179.
49. Elmahalawy II, Ammar AS, Fathy WM, Salama AE, Mokhtar WS. Pentraxin 3 as an early marker in diagnosis of ventilator associated pneumonia. Egypt J Chest Dis Tuberc. 2017;66(4):709–12.
50. Douglas IS, Price CS, Overdier KH, Wolken RF, Metzger SW, Hance KR, et al. Rapid automated microscopy for microbiological surveil‑lance of ventilator‑associated pneumonia. Am J Respir Crit Care Med. 2015;191(5):566–73.
51. Clavel M, Barraud O, Moucadel V, Meynier F, Karam E, Ploy MC, et al. Molecular quantification of bacteria from respiratory samples in patients with suspected ventilator‑associated pneumonia. Clin Microbiol Infect. 2016;22(9):812.e1‑812.e7.
52. Chen C, Yan M, Hu C, Lv X, Zhang H, Chen S. Diagnostic efficacy of serum procalcitonin, C‑reactive protein concentration and clinical pulmonary infection score in Ventilator‑Associated Pneumonia. Med Sci (Paris). 2018;34((Focus issue F1)):26–32.
53. Charles PE, Kus E, Aho S, Prin S, Doise J‑M, Olsson N‑O, et al. Serum procal‑citonin for the early recognition of nosocomial infection in the critically ill patients: a preliminary report. BMC Infect Dis. 2009;9:49.
54. de Carvalho EM, Massarollo PCB, Levin AS, Isern MRM, Pereira WL, Abdala E, et al. Comparative study of etiological diagnosis of nosocomial pneu‑monia. Braz J Infect Dis. 2008;12(1):67–74.
55. Baldesi O, Michel F, Guervilly C, Embriaco N, Granfond A, La Scola B, et al. Bacterial ventilator‑associated pneumonia: bronchoalveolar lavage results are not influenced by dilution. Intensive Care Med. 2009;35(7):1210–5.
56. Anand NJ, Zuick S, Klesney‑Tait J, Kollef MH. Diagnostic implications of soluble triggering receptor expressed on myeloid cells‑1 in BAL fluid of patients with pulmonary infiltrates in the ICU. Chest. 2009;135(3):641–7.
57. Albert M, Friedrich JO, Adhikari NKJ, Day AG, Verdant C, Heyland DK, et al. Utility of Gram stain in the clinical management of suspected ventilator‑associated pneumonia. Secondary analysis of a multicenter randomized trial. J Crit Care. 2008;23(1):74–81.
58. Leo A, Galindo‑Galindo J, Folch E, Guerrero A, Bosques F, Mercado R, et al. Comparison of bronchoscopic bronchoalveolar lavage vs blind lavage with a modified nasogastric tube in the etiologic diagnosis of ventilator‑associated pneumonia. Med Intensiva. 2008;32(3):115–20.
59. Kwon S‑J, Jeon T, Seo D, Na M, Choi E‑G, Son J‑W, et al. Quantitative PCR for etiologic diagnosis of methicillin‑resistant Staphylococcus aureus pneumonia in Intensive Care Unit. Tuberc Respir Dis (Seoul). 2012;72(3):293–301.
60. Kneidinger N, Warszawska J, Schenk P, Fuhrmann V, Bojic A, Hirschl A, et al. Storage of bronchoalveolar lavage fluid and accuracy of microbio‑logic diagnostics in the ICU: a prospective observational study. Crit Care. 2013;17(4):R135.
61. Klein Klouwenberg PMC, van Mourik MSM, Ong DSY, Horn J, Schultz MJ, Cremer OL, et al. Electronic implementation of a novel surveillance paradigm for ventilator‑associated events. Feasibility and validation. Am J Respir Crit Care Med. 2014;189(8):947–55.
62. Klompas M, Kleinman K, Platt R. Development of an algorithm for surveillance of ventilator‑associated pneumonia with electronic data and
comparison of algorithm results with clinician diagnoses. Infect Control Hosp Epidemiol. 2008;29(1):31–7.
63. Jung B, Embriaco N, Roux F, Forel J‑M, Demory D, Allardet‑Servent J, et al. Microbiogical data, but not procalcitonin improve the accuracy of the clinical pulmonary infection score. Intensive Care Med. 2010;36(5):790–8.
64. Jovanovic B, Djuric O, Markovic‑Denic L, Isakovic A, Doklestic K, Stankovic S, et al. Prognostic value of presepsin (soluble CD14‑subtype) in diagnosis of ventilator‑associated pneumonia and sepsis in trauma patients. VSP. 2018;75(10):968–77.
65. Jiao J, Wang M, Zhang J, Shen K, Liao X, Zhou X. Procalcitonin as a diagnostic marker of ventilator‑associated pneumonia in cardiac surgery patients. Exp Ther Med. 2015;9(3):1051–7.
66. Oudhuis GJ, Beuving J, Bergmans D, Stobberingh EE, ten Velde G, Linssen CF, et al. Soluble Triggering Receptor Expressed on Myeloid cells‑1 in bronchoalveolar lavage fluid is not predictive for ventilator‑associated pneumonia. Intensive Care Med. 2009;35(7):1265–70.
67. Linssen CFM, Bekers O, Drent M, Jacobs JA. C‑reactive protein and proc‑alcitonin concentrations in bronchoalveolar lavage fluid as a predictor of ventilator‑associated pneumonia. Ann Clin Biochem. 2008;45(Pt 3):293–8.
68. Liu C, Du Z, Zhou Q, Hu B, Li Z, Yu L, et al. Microscopic examination of intracellular organisms in bronchoalveolar lavage fluid for the diagnosis of ventilator‑associated pneumonia: a prospective multi‑center study. Chin Med J. 2014;127(10):1808–13.
69. Luna CM, Sarquis S, Niederman MS, Sosa FA, Otaola M, Bailleau N, et al. Is a strategy based on routine endotracheal cultures the best way to prescribe antibiotics in ventilator‑associated pneumonia? Chest. 2013;144(1):63–71.
70. Luyt C‑E, Combes A, Reynaud C, Hekimian G, Nieszkowska A, Tonnellier M, et al. Usefulness of procalcitonin for the diagnosis of ventilator‑associated pneumonia. Intensive Care Med. 2008;34(8):1434–40.
71. Mauri T, Coppadoro A, Bombino M, Bellani G, Zambelli V, Fornari C, et al. Alveolar pentraxin 3 as an early marker of microbiologically confirmed pneumonia: a threshold‑finding prospective observational study. Crit Care. 2014;18(5):562.
72. Medford ARL, Husain SA, Turki HM, Millar AB. Diagnosis of ventilator‑associated pneumonia. J Crit Care. 2009;24(3):473.e1‑6.
73. Mongodi S, Via G, Girard M, Rouquette I, Misset B, Braschi A, et al. Lung ultrasound for early diagnosis of ventilator‑associated pneumonia. Chest. 2016;149(4):969–80.
74. Conway Morris A, Kefala K, Wilkinson TS, Moncayo‑Nieto OL, Dhaliwal K, Farrell L, et al. Diagnostic importance of pulmonary interleukin‑1beta and interleukin‑8 in ventilator‑associated pneumonia. Thorax. 2010;65(3):201–7.
75. Linssen CFM, Jacobs JA, Schouten JSAG, van Mook WNKA, Ramsay G, Drent M. Influence of antibiotic therapy on the cytological diagnosis of ventilator‑associated pneumonia. Intensive Care Med. 2008;34(5):865–72.
76. Refaat A, Affara N, Abdel‑fatah W, Hussein T, El‑gerbi M. Diagnostic accuracy of inflammatory biomarkers in bronchoalveolar lavage from patients with ventilator‑associated pneumonia. Egypt J Chest Dis Tuberc. 2014;63(3):723–30.
77. Scholte JBJ, van Dessel HA, Linssen CFM, Bergmans DCJJ, Savelkoul PHM, Roekaerts PMHJ, et al. Endotracheal aspirate and bronchoalveolar lavage fluid analysis: interchangeable diagnostic modalities in suspected ventilator‑associated pneumonia? J Clin Microbiol. 2014;52(10):3597–604.
78. Textoris J, Loriod B, Benayoun L, Gourraud P‑A, Puthier D, Albanèse J, et al. An evaluation of the role of gene expression in the prediction and diagnosis of ventilator‑associated pneumonia. Anesthesiology. 2011;115(2):344–52.
79. Vanspauwen MJ, Linssen CFM, Bruggeman CA, Jacobs JA, Drent M, Bergmans DCJJ, et al. Clara cell protein in bronchoalveolar lavage fluid: a predictor of ventilator‑associated pneumonia? Crit Care. 2011;15(1):R14.
80. Vernikos P, Kampolis CF, Konstantopoulos K, Armaganidis A, Karakitsos P. The role of bronchoscopic findings and bronchoalveolar lavage fluid cytology in early diagnosis of ventilator‑associated pneumonia. Respir Care. 2016;61(5):658–67.
81. Waltrick R, Possamai DS, de Aguiar FP, Dadam M, de Souza Filho VJ, Ramos LR, et al. Comparison between a clinical diagnosis method and the sur‑veillance technique of the Center for Disease Control and Prevention for identification of mechanical ventilator‑associated pneumonia. Rev Bras Ter Intensiva. 2015;27(3):260–5.
Page 19 of 19Al‑Omari et al. BMC Pulm Med (2021) 21:196
• fast, convenient online submission
•
thorough peer review by experienced researchers in your field
• rapid publication on acceptance
• support for research data, including large and complex data types
•
gold Open Access which fosters wider collaboration and increased citations
maximum visibility for your research: over 100M website views per year •
At BMC, research is always in progress.
Learn more biomedcentral.com/submissions
Ready to submit your researchReady to submit your research ? Choose BMC and benefit from: ? Choose BMC and benefit from:
82. Yagmurdur H, Tezcan AH, Karakurt O, Leblebici F. The efficiency of routine endotracheal aspirate cultures compared to bronchoalveolar lavage cultures in ventilator‑associated pneumonia diagnosis. Niger J Clin Pract. 2016;19(1):46–51.
83. Zagli G, Cozzolino M, Terreni A, Biagioli T, Caldini AL, Peris A. Diagnosis of ventilator‑associated pneumonia: a pilot, exploratory analysis of a new score based on procalcitonin and chest echography. Chest. 2014;146(6):1578–85.
84. Umemneku Chikere CM, Wilson K, Graziadio S, Vale L, Allen AJ. Diagnostic test evaluation methodology: a systematic review of methods employed to evaluate diagnostic tests in the absence of gold standard—an update. PLoS ONE. 2019;14(10):e0223832.
85. Lalwani S, Mathur P, Tak V, Janani S, Kumar SI, Bagla R, et al. Diagnosis of ventilator‑associated pneumonia: comparison between ante‑mortem and post‑mortem cultures in trauma patients. Indian J Med Microbiol. 2014;32(3):294–300.
86. Fernando SM, Tran A, Cheng W, Klompas M, Kyeremanteng K, Mehta S, et al. Diagnosis of ventilator‑associated pneumonia in critically ill adult patients‑a systematic review and meta‑analysis. Intensive Care Med. 2020;46(6):1170–9.
87. Morris AC, Kefala K, Simpson AJ, Wilkinson TS, Everingham K, Kerslake D, et al. Evaluation of the effect of diagnostic methodology on the reported incidence of ventilator‑associated pneumonia. Thorax. 2009;64(6):516–22.
88. Kamel T, Helms J, Janssen‑Langenstein R, Kouatchet A, Guillon A, Bourenne J, et al. Benefit‑to‑risk balance of bronchoalveolar lavage in the critically ill. A prospective, multicenter cohort study. Intensive Care Med. 2020;46(3):463–74.
89. Browne E, Hellyer TP, Baudouin SV, Conway Morris A, Linnett V, McAuley DF, et al. A national survey of the diagnosis and management of suspected ventilator‑associated pneumonia. BMJ Open Respir Res. 2014;1(1):e000066.
90. Butler KL, Sinclair KE, Henderson VJ, McKinney G, Mesidor DA, Katon‑Benitez I, et al. The chest radiograph in critically ill surgical patients is inaccurate in predicting ventilator‑associated pneumonia. Am Surg. 1999;65(9):805–9 (discussion 809).
91. Wunderink RG, Woldenberg LS, Zeiss J, Day CM, Ciemins J, Lacher DA. The radiologic diagnosis of autopsy‑proven ventilator‑associated pneumonia. Chest. 1992;101(2):458–63.
92. Lefcoe MS, Fox GA, Leasa DJ, Sparrow RK, McCormack DG. Accu‑racy of portable chest radiography in the critical care setting. Chest. 1994;105(3):885–7.
93. Beards SC, Jackson A, Hunt L, Wood A, Frerk CM, Brear G, et al. Interob‑server variation in the chest radiograph component of the lung injury score. Anaesthesia. 1995;50(11):928–32.
94. Rubenfeld GD, Caldwell E, Granton J, Hudson LD, Matthay MA. Interob‑server variability in applying a radiographic definition for ARDS. Chest. 1999;116(5):1347–53.
95. Klompas M, Magill S, Robicsek A, Strymish JM, Kleinman K, Evans RS, et al. Objective surveillance definitions for ventilator‑associated pneumonia. Crit Care Med. 2012;40(12):3154–61.
96. Moher D, Liberati A, Tatzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta‑analyses: the PRISMA statement. PLos Med. 2009; 6(6):e1000097. https:// doi. org/ 10. 1371/ journ al. pmed1 000097
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims in pub‑lished maps and institutional affiliations.