25
Systemic Treatment of Metastatic Colorectal Cancer: Living with a Moving Landscape Neal J. Meropol, MD Fox Chase Cancer Center May 16, 2005
| Date post: | 03-Jan-2016 |
| Category: |
Documents |
| Upload: | horace-baldwin |
| View: | 212 times |
| Download: | 0 times |
Systemic Treatment of Metastatic Colorectal Cancer: Living with a
Moving Landscape
Neal J. Meropol, MD
Fox Chase Cancer Center
May 16, 2005

History of Systemic Therapy for Colorectal Cancer
?
5-FU Modulation
1980’s
New Cytotoxics
1990’s
Biologics
2000’s
Pat
ien
t B
enef
it
5-FU/leucovorin
oxaliplatin
irinotecan
capecitabine/irinotecan
FOLFOX
capecitabine/oxaliplatin
capecitabine
FOLFIRI
IFL
bevacizumab
cetuximab
cetuximab/irinotecan

Treatment Summary: Front-Line
• Capecitabine = 5-fluorouracil• 2 drugs are better than 1
– Irinotecan doubles response rate and improves survival by a few months when added to 5-FU/LV
– Oxaliplatin doubles response rate and improves TTP by a few months when added to 5-FU/LV
• Irinotecan/FU/LV = oxaliplatin/FU/LV• Bevacizumab improves survival when added to
irinotecan/FU/LV; improves TTP with 5-FU/LV

Treatment Summary: 2nd-, 3rd-Line
• Irinotecan improves survival (vs. BSC) by a few months as second-line therapy
• Oxaliplatin+FU/LV improves RR and TTP over either alone
• Bevacizumab improves survival when added to oxaliplatin/FU/LV
• Cetuximab and panitumumab have modest single agent activity
• Cetuximab + irinotecan improves RR% over cetuximab alone

Grothey, A. et al. J Clin Oncol; 22:1209-1214 2004
Survival with Metastatic Colorectal Cancer: Chemotherapy
IFLIROX
FOLFIRIFOLFOX
With antibodies?

Some Practical Clinical Questions
• Capecitabine combinations?• Optimal second line?• Combinations of biologics?• Cetuximab front-line?• Cetuximab before irinotecan failure?• Non-irinotecan cetuximab combinations?• Bevacizumab for life?
Questions Addressed Today
• Capecitabine combinations?
• Optimal second line?
• Combinations of biologics?

Infusional 5-fluorouracil/folinic acid plus oxaliplatin (FUFOX) versus
capecitabine plus oxaliplatin (CAPOX) as first line treatment of metastatic
colorectal cancer: results of the safety and efficacy analysis
Arkenau et al. ASCO 2005, #3507

FUFOX vs. CAPOX: Results
• Similar toxicity profile; ~25% severe neuropathy• Equivalent PFS, 7.0 (C) vs. 8.0 (F) months
(HR=1.19, 95% CI 0.97–1.48, p=0.11)• Equivalent median S, 16.3 (C) vs. 17.2 (F)
months (HR=1.05, 95% CI 0.79-1.41, p=0.72)• Response rate ~50% in both arms
• Note: potential differences in tolerated doses in different populations (e.g. Cassidy JCO 2004, Shields Cancer 2004)

CAPOX vs. FUFOX Overall Survival
1.0
0.8
0.6
0.4
0.2
00 20 40 60 80 100 120 140
Weeks
Estimated probability Median
CAPOX (n=238) 16.3 monthsFUFOX (n=230) 17.2 months
HR = 1.05 (95% CI: 0.79–1.41)p=0.72 (Log-rank)
N9841: A randomized phase III equivalence trial of irinotecan (CPT-11) versus
oxaliplatin/5-fluorouracil /leucovorin (FOLFOX4) in patients with advanced
colorectal cancer previously treated with 5FU
Pitot et al. ASCO 2005, #3506
N9841 Results
• Equivalent overall survival, 14.7 (I) vs. 13.5 (FOLFOX) months (HR=1.05, 95% CI 0.9-1.3)
• FOLFOX less toxic (except neuropathy)
• Response rate higher with FOLFOX (27% vs 15%, p<0.01)
• TTP equivalent (trend favors FOLFOX, 5.2 vs. 4 months, p=0.10)

N9841: Overall Survival
0
10
20
30
40
50
60
70
80
90
100
0 2 4 6 8 10 12 14 16 18 20 22 24
Months from Registration
% A
live
CPT-11 N = 245
FOLFOX N = 246

Randomized phase II trial of cetuximab/bevacizumab/irinotecan (CBI) versus cetuximab/bevacizumab (CB) in irinotecan-refractory colorectal cancer
Saltz et al. ASCO 2005, #3508

Pao, W. et al. J Clin Oncol; 23:2556-2568 2005
EGFR Antibodies Block Ligand Binding and Downstream Signaling
Antibody
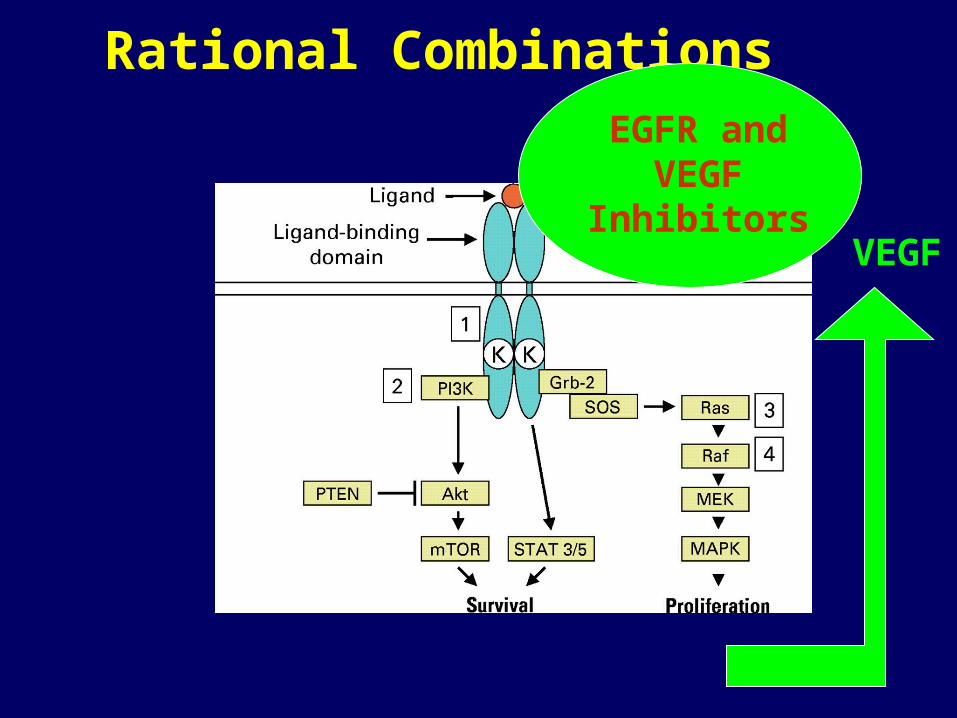
Rational Combinations EGFR and
VEGF Inhibitors
VEGF
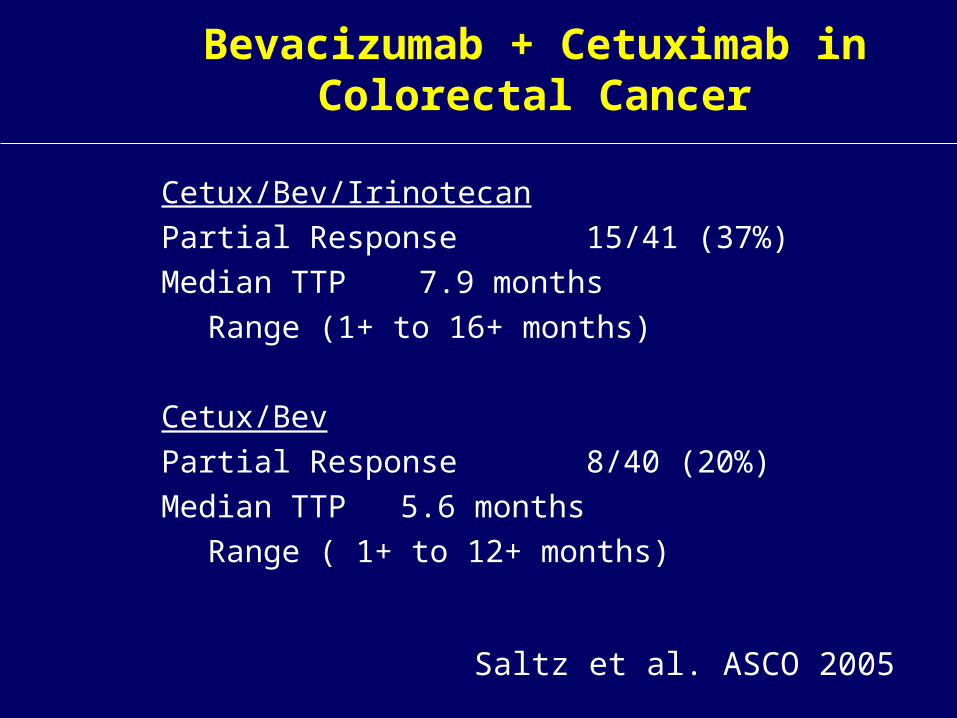
Bevacizumab + Cetuximab in Colorectal Cancer
Cetux/Bev/Irinotecan
Partial Response 15/41 (37%)
Median TTP 7.9 months
Range (1+ to 16+ months)
Cetux/Bev
Partial Response 8/40 (20%)
Median TTP 5.6 months
Range ( 1+ to 12+ months)
Saltz et al. ASCO 2005

Rational Combinations
EGFR and RAS/Raf/MEK/
MAPK Inhibitors
EGFR + IGF-1R or HER2 Inhibitors
EGFR and AKT/mTOR Inhibitors

What have we learned?
1. For many patients, metastatic colorectal cancer is no longer an acute illness
2. There is more than one correct way to use drugs with modest activity in unselected populations
3. The selection of new combinations should no longer be based primarily upon avoidance of overlapping toxicities, but rather an appreciation of colorectal cancer as a network of interrelated processes
The Big Questions that Should Guide Future Clinical
Research:
How do these drugs work and who should get them?

Matchmaking is Science
Potential Sources of Variability
• The tumor– Target characteristics– Target relevance– Drug disposition– Resistance mechanisms
• The patient– Drug metabolism– Normal tissue sensitivity

How Can Clinical Investigators Deal with a Rapidly Changing Landscape?
(This is not 1995)
• Undertake in vivo pharmacodynamic assessment to ensure target acquisition and define mechanism of action during early clinical development
• Be forward-thinking in clinical trial design; this requires acceptance of risk
• Accept that toxicity evaluation will not be complete before phase III investigation
• Work with patient advocates; ensure relevance to those asked to participate
• Bank biologic material; there is now less redundancy and more potential for missed opportunities
Can Society Afford State-of-the-Art Cancer Treatment?
Neal J. Meropol, MD, Fox Chase Cancer Center, Chair
Sue Hellmann, MD, MPH, Genentech Inc.
Kevin A. Schulman, MD, MBA, Duke University
Barry Straube, M.D., CMS
Level 4, Valencia Room, 415A
12:00-1:15
May 16, 2005

















