Systems Biology: A Necessary Methodology for Understanding the Mechanisms of Sudden Cardiac Death in Heart Failure Raimond L. Winslow 1,3 , William Baumgartner Jr 1,3 , Patrick Helm 1,3 , Christina Yung 1,3 , Faisal Beg 2,3 and Michael I. Miller 2,3 Center for Cardiovascular Bioinformatics & Modeling 1 Center for Imaging Sciences 2, and Whitaker Biomedical Engineering Institute 3 The Johns Hopkins University School of Medicine and Whiting School of Engineering
Transcript
Systems Biology: A Necessary Methodology for Understanding the Mechanisms of Sudden
Cardiac Death in Heart Failure
Raimond L. Winslow1,3, William Baumgartner Jr1,3, Patrick Helm1,3, Christina Yung1,3, Faisal Beg2,3 and Michael I. Miller2,3
Center for Cardiovascular Bioinformatics & Modeling1
Center for Imaging Sciences2, andWhitaker Biomedical Engineering Institute3
The Johns Hopkins University School of Medicine and Whiting School of Engineering
Mechanical pump failure leading to reduced cardiac output
Cause unknown
Diverse origins High blood pressure, artherosclerosis, MI, congenital heart
Mechanism of HF AP Duration Prolongation: Model Interpretations
0
0.1
0.2
0.3
0.4
0.5
0 0.1 0.2 0.3 0.4 0.5 0.6
[Ca
i] (M
)
Time (sec)
Stimulus Duration
NCX1 ATP2A2
Winslow et al (1999) Circ. Res. 84: 571
Decreased JSR Ca2+ Decreased JSR Ca2+ Release
Increased L-Type Ca2+ Current Prolonged AP Duration
Ca2+-Mediated Inactivation of ICaL is a Major Factor Regulating AP Duration: Effects of Ablation
Model
Experiment
Alseikhan et al (2002). Biophys J. 82:358a
Mutant CaM1234
disables Ca Sensor for Cainactivation
Topics
To what extent can known changes of gene/protein expression in HF account for altered cellular responses?
Develop and apply a new model of the cardiac ventricular myocyte
Model describes how “microscopic” interactions between individual ion channels influences macroscopic behavior of the myoycte
How can we best image, quantify and model changes of cardiac geometry and micro-anatomic structure that occur in HF?
Diffusion Tensor MR Imaging (DTMRI) of cardiac geometry and fiber orientation
Quantitative analysis of statistical variation of heart structure
To what extent can known changes of gene/protein expression in HF explain the origins of Sudden Cardiac Death?
Computational model of the cardiac ventricles
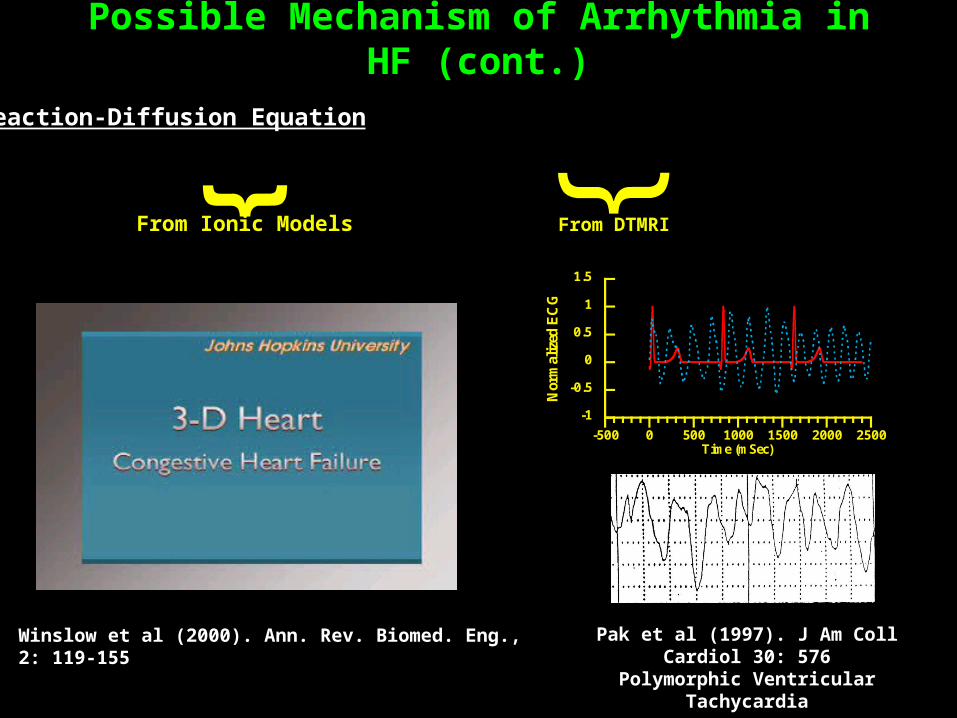
Possible origins of whole-heart arrythmias
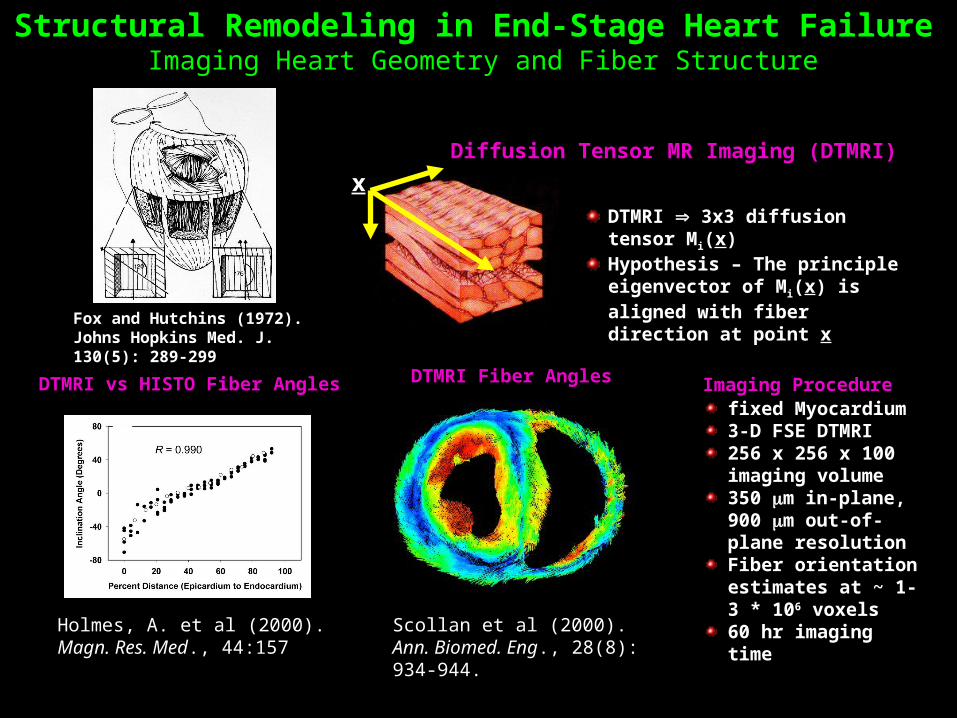
Fox and Hutchins (1972). Johns Hopkins Med. J. 130(5): 289-299
Structural Remodeling in End-Stage Heart Failure Imaging Heart Geometry and Fiber Structure
DTMRI 3x3 diffusion tensor Mi(x)Hypothesis – The principle eigenvector of Mi(x) is aligned with fiber direction at point x
Diffusion Tensor MR Imaging (DTMRI)
x
DTMRI vs HISTO Fiber Angles DTMRI Fiber AnglesIn Cross Section
Holmes, A. et al (2000). Magn. Res. Med., 44:157
Scollan et al (2000). Ann. Biomed. Eng., 28(8): 934-944.
fixed Myocardium3-D FSE DTMRI256 x 256 x 100 imaging volume350 m in-plane, 900 m out-of-plane resolutionFiber orientation estimates at ~ 1-3 * 106 voxels60 hr imaging time
Imaging Procedure
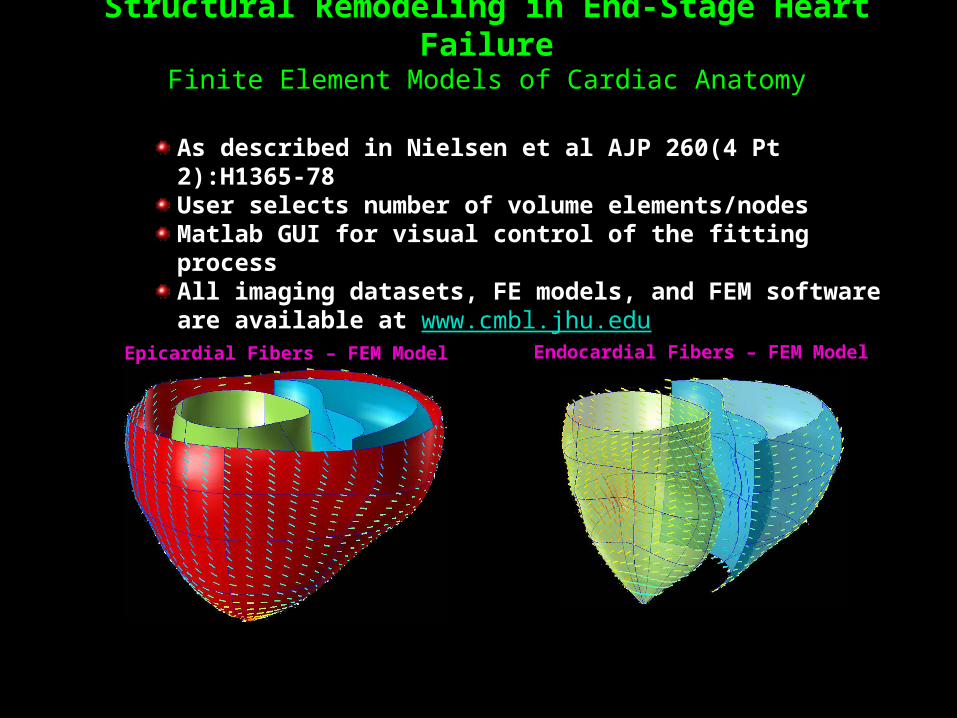
Structural Remodeling in End-Stage Heart FailureFinite Element Models of Cardiac Anatomy
Epicardial Fibers – FEM Model Endocardial Fibers – FEM Model
As described in Nielsen et al AJP 260(4 Pt 2):H1365-78 User selects number of volume elements/nodesMatlab GUI for visual control of the fitting processAll imaging datasets, FE models, and FEM software are available at www.cmbl.jhu.edu























![The Winslow mail. (Winslow, Ariz.) 1926-05-28 [p PAGE FOUR]](https://static.documents.pub/doc/80x56/621058d8c7683c59fe60e913/the-winslow-mail-winslow-ariz-1926-05-28-p-page-four.jpg)















