Systems Linkages and Access to Care for Populations at High Risk of HIV Infection Initiative Ryan White HIV/AIDS Program Part B Technical Assistance Webinar March 18, 2015 HIV/AIDS Bureau Division of State HIV/AIDS Programs (DSHAP)
Transcript
Systems Linkages and Access to Care for Populations at High Risk of HIV Infection Initiative
Ryan White HIV/AIDS Program Part BTechnical Assistance Webinar
March 18, 2015
HIV/AIDS BureauDivision of State HIV/AIDS Programs (DSHAP)
2
DSHAP Mission
• To provide leadership and support to States/Territories for developing and ensuring access to quality HIV prevention, health care, and support services.
3
Agenda
HAB Announcements Heather Hauck
Question & Answer
Introduction Harold Phillips
Systems Linkages Initiative Overview Adan Cajina
Multi-State Evaluation Overview, UCSF ETAC Stephen Morin
Demonstration States:
Virginia Steve Bailey Anne Rhodes
Wisconsin Casey Schumann
ETAC Lessons Learned Kim Koester Edwin Charlebois
Question & Answer
4
Announcements
Heather Hauck, Director Division of State HIV/AIDS Programs
HIV/AIDS Bureau
5
Question and Answer Session
6
Harold J. Phillips, Director Division of Training and Capacity
DevelopmentHIV/AIDS Bureau
Systems Linkages and Access to Care for Populations at High Risk of HIV Infection Initiative
Special Projects of National Significance (SPNS) Program
8
Overview Division of Training and Capacity
Development
• Mission: Strengthen and transform health care systems by supporting the development of leadership, evaluation, training and capacity development to assure the provision of high quality HIV/AIDS prevention, care and treatment services.
8
9
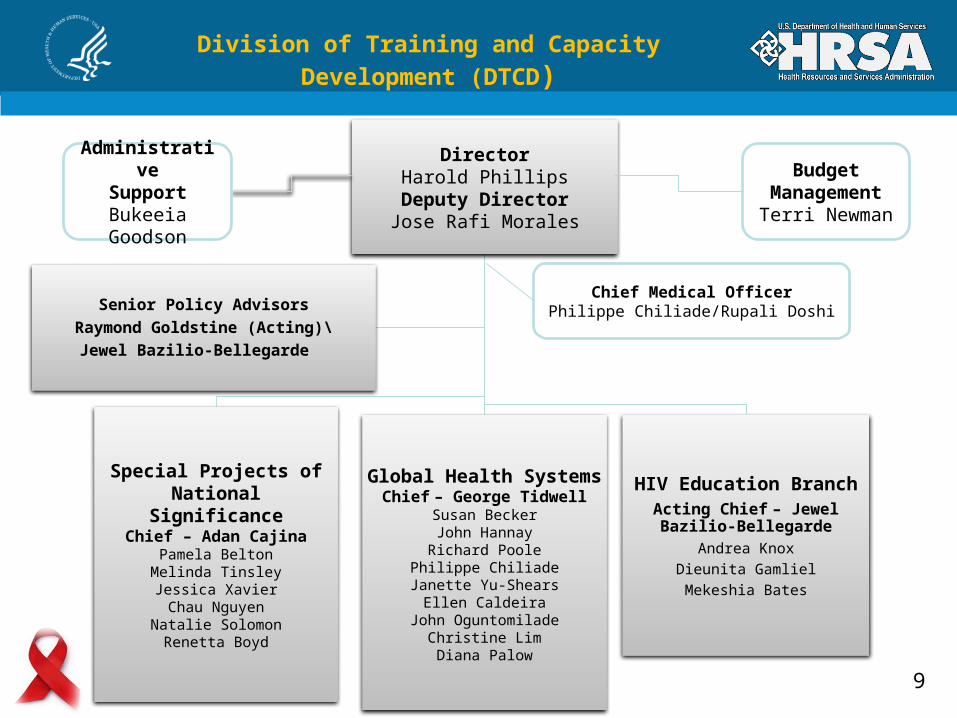
Division of Training and Capacity Development (DTCD)
HIV Education BranchActing Chief – Jewel Bazilio-Bellegarde
Andrea KnoxDieunita GamlielMekeshia Bates
Senior Policy AdvisorsRaymond Goldstine (Acting)\
Jewel Bazilio-Bellegarde
Administrative
Support Bukeeia Goodson
Budget ManagementTerri Newman
Chief Medical OfficerPhilippe Chiliade/Rupali Doshi
10
SPNS Program (Part-F)
• The SPNS Program supports the development of innovative models of HIV care to quickly respond to the emerging needs of clients served by the Ryan White HIV/ AIDS Program.
• Evaluation• Dissemination• Replication• Build and Improve IT capacity
Chief, Special Projects of National Significance (SPNS), Division of Training and Capacity Development
Adan Cajina
12
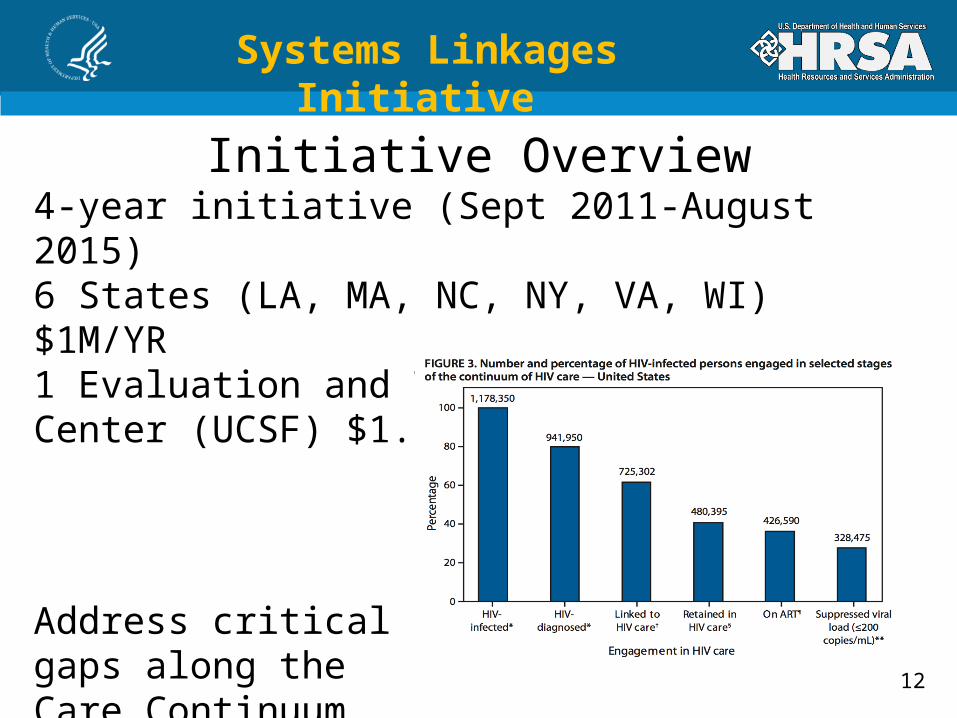
Systems Linkages Initiative
Initiative Overview4-year initiative (Sept 2011-August 2015)6 States (LA, MA, NC, NY, VA, WI) $1M/YR1 Evaluation and Technical Assistance Center (UCSF) $1.5M/YR
Address critical gaps along the Care Continuum
13
Systems Linkages Initiative
Goal and Target PopulationGoal:
Improve access to and retention in high quality, competent HIV care and services for hard-to-reach populations of HIV-infected persons
Objectives:1. Test linkage interventions in six states2. Evaluate effectiveness of interventions and disseminate
findings
Target Population:At high risk for or infected with HIV but unawareAware but have never been referred to careAware but have refuse referral to careAware but have dropped out of care
14
Systems Linkages Initiative
What are Systems Linkages?
Enhancement of existing – or implementation of new collaborative relationships or partnerships among Ryan White and other, non-traditional HIV organizations
IT/data systems linkage interventions • Data system integration (testing, surveillance, care)
Community linkage interventions• Disease Intervention Specialists• Navigation• Corrections• Enhanced testing• Social Networks
15
Systems Linkages Initiative
Develop and pilot test innovative linkage interventions using the Collaborative Model
Host collaboration meetings/learning sessions with assistance from ETAC
• Introduce PDSA techniques and pilot linkage interventions• Review results of pilot tests• Identify linkage interventions for wider-scale implementation
Develop state-level evaluation plan
IHI Collaborative ModelYears 1 and 2
16
Systems Linkages Initiative
Linkage Implementation and Evaluation Years 3 and 4
• Implement successful linkage interventions on wider scale
• Implement state-level evaluation plan
• Participate in cross-state evaluation with ETAC
• Disseminate project findings and lessons learned
17
Systems Linkages Initiative
Role of the Evaluation and Technical Assistance Center (ETAC)
Regents of the University of California, San Francisco
• Design and implement a cross-state evaluation of systems linkage interventions
• TA on state local evaluations
• Data collection systems support
• Dissemination
18
Systems Linkages Initiative
Key Research Questions
What characteristics of system linkage interventions most successfully lead to:
• Increases in identifying people living with HIV?• Increases in the proportion of newly diagnosed individuals
entering care within 3 months of first testing HIV positive?• Increases in the proportion of people living with HIV who are
continuously in care?• Increases in successful viral suppression among people
living with HIV?• What are the structural, policy, provider, and patient
characteristics that facilitate or hinder implementation of system linkage interventions?
where health departments work with providers, e.g. “line lists” (MA, NC).
• Contracts with providers for services, e.g. patient navigation (VA, NY), peer navigation (NY), peer-nurse teams (MA) or Linkage to Care Specialists (WI).
22
Direct Outreach
• Health Department Disease Investigation Specialists (DIS officers) are retrained to work with clients on linkage and re-engagement, e.g. State Bridge Counselors (NC); Active Referral (VA).
23
Technology Approaches
• Technology-mediated interventions where surveillance data meet emergency department admissions e.g. public health information exchanges (LA) or systematic appointment reminders (NY).
24
Special Populations
• Focused attention on corrections, e.g. video conferencing prior to release (LA), Care Coordination (VA) or mental health screening and treatment (VA).
25
Increased Case Detection
• Expansion of existing or pilot HIV testing for increased case detection (LA, NC, WI).
26
Policy Implications
• Increasingly states are using surveillance data to facilitate linkage and retention in care and to monitor viral suppression.
• Variations on patient navigation beyond traditional case management have emerged as key strategy.
27
Policy Implications• Policy environments matter; in particular
states differ in access to care, e.g. ACA, Medicaid expansion, ADAP policies, state budgets, hiring freezes, etc.
• Without increased resources, states and cities need to redirect funds toward Ryan White early intervention services.
• Ryan White itself may need to be increasingly used with a goal to increase the proportion of HIV patients virally suppressed.
Virginia Special Projects of National Significance: Systems
Linkages Interventions
Steve BaileyAnne Rhodes
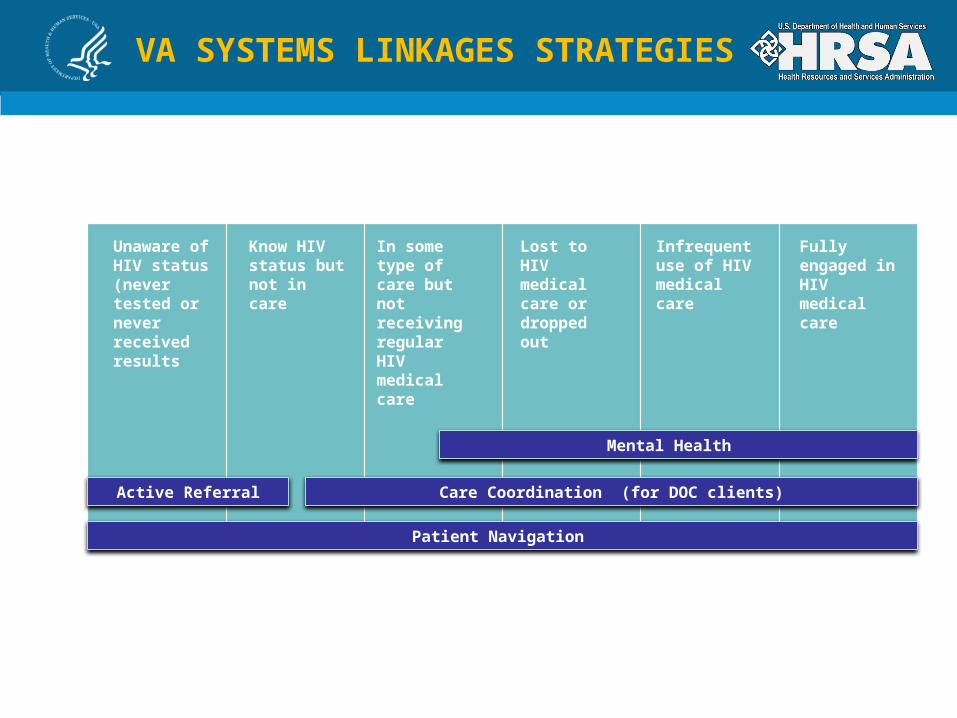
VA SYSTEMS LINKAGES STRATEGIES
Unaware of HIV status (never tested or never received results
Know HIV status but not in care
Infrequent use of HIV medical care
In some type of care but not receiving regular HIV medical care
Lost to HIV medical care or dropped out
Fully engaged in HIV medical care
Care Coordination (for DOC clients)
Patient Navigation
Active Referral
Mental Health
30
Mental Health:• Standardized screening
and referral process to provide mental health (MH) services for clients with MH barriers for linking and retaining in care.
• Sites: Virginia Commonwealth University (VCU)
• Populations Targeted: HIV-positive persons with MH needs
• Outcomes: LINKAGE, RETENTION, SUPPRESSION
Care Coordination:Coordinated access to medical care and medications for inmates released from Virginia Department of Corrections (VADOC) and Virginia Local/Regional Jail (VLRJ) facilities.
Sites: Statewide coverage
Populations Targeted:Released from VDOCs and jails
Outcomes: LINKAGE, RETENTION, SUPPRESSION
31
Active Referral:Referral process that requires Disease Intervention Specialists (DIS) to actively link patients directly to care via Patient Navigators (PNs) or medical providers.
Patient Navigation:A client-centered PN model• 90 days of services focused on
linking client to care and 12 month retention support
• Use Fidelity Monitoring (FM) to evaluate Motivational Interviewing (MI) skills
• Sites: VCU, Carilion, and Centra• Populations Targeted: Newly
diagnosed and lost to care• Outcomes: LINKAGE, RETENTION,
SUPPRESSION
32
Care and Prevention in the United States (CAPUS) in Virginia
• CAPUS, awarded by CDC, through HIV Prevention, funds PN, expanded testing, housing pilot, and social media campaigns as well as enhanced use of surveillance data
• SPNS and CAPUS collaborated on protocol development for active referral and selection of PN sites
• SPNS and CAPUS PN sites were located in different geographical regions of the state to avoid cross contamination
33
SPNS and CAPUS Sites in Virginia
34
Successes• Increased referrals from DOC to health department and referrals for support services for inmates post-release
• Built communications between Care Coordinator and DOC and local jails
• Increased medication pick up rates post-release, and set up tracking for retention
• Coordination with other inmate programs (Comprehensive HIV/AIDS Linkages for Inmates – CHARLI)
Successes: Care Coordination
35
Successes• Difficult to get information from DOC/jails prior to release, including consistent release dates
• Relationships with local jails often took a long time to build, medication provision not consistent in jails prior to release
• No consistent method for tracking medication pick up at local health departments
Challenges: Care Coordination
36
Interim Outcomes
37
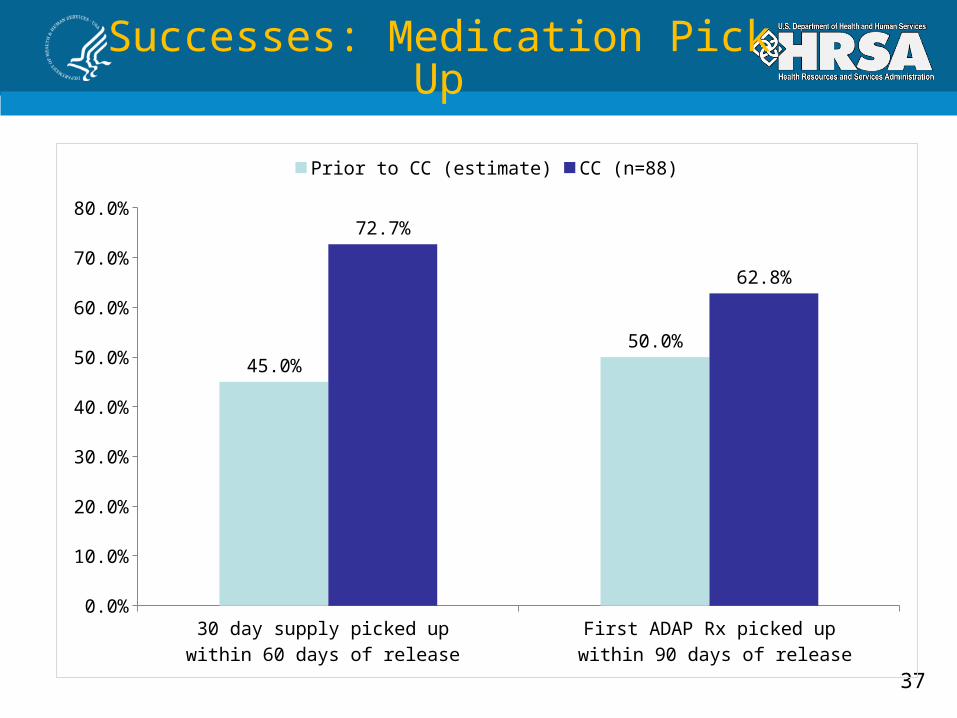
Successes: Medication Pick Up
30 day supply picked up within 60 days of release
First ADAP Rx picked up within 90 days of release
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
45.0%50.0%
72.7%
62.8%
Prior to CC (estimate) CC (n=88)
38
Successes : Continuum of Care
*Includes all clients served only by the CC intervention during the timeframe 1/1/2012-12/31/2014. **Includes all clients served by the CC intervention during the timeframe 1/1/2012-12/31/2014 and who also received CHARLI services during the timeframe 1/1/2014-12/31/2014
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%100.0%
78.3%
66.3% 67.5%
54.2%
85.7%
76.8% 77.4%
60.7%
92.9%87.1% 87.1%
67.1%
Overall Care Coordination (N=168) Care Coordination Only (N=83)
Care Coordination and CHARLI (N=85)
39
Successes: Client Perspective
• Barriers• Unable to afford medications or medical visits copayments• Nearest clinic 2 hours away• Unemployed with unstable housing• Limited social support• Clients had ”given up”
• Intervention: Care Coordinator initiated client contact, noticing medical and medications had not been accessed
Complex care plan involving 3 different agencies• Facilitated medical transportation• Identified copayment assistance resources• Incorporating telemedicine once medically stable• Housing and employment assistance
• Target population is difficult to track with many needs and barriers
• Centralized service is beneficial in areas that do not have many resources or a referral network; however, face to face involvement through collaboration with community partners is needed as well
• Access to medications/medical care not primary perceived need
• Territoriality can impede collaboration
• Referral systems from VADOC and VLRJ vary and require time intensive exploration
• Prescription authority and procedures are inconsistent across correctional facilities
41
Sustainability Plan
Care Coordination has been added to the state ADAP model and will continue to be funded as a part of ADAP
PN will be funded through Ryan White, HIV Prevention and other ongoing sources
Mental Health providers are working to utilize third-party billing
Active Referral is part of standard Disease Intervention Specialist (DIS) protocol
Wisconsin Special Project of National Significance: Systems
Linkages Interventions
Casey SchumannMarch 18, 2015
Wisconsin Department of Health Services
• Community-based strategy utilizing peers to identify individuals at high risk for HIV and connect them with HIV testing services
• Testing agency enlists and coaches recruiters who have relationships with high-risk networks
• Recruiter identifies associates from their network and refers them to HIV testing
• Goal to standardize program across agencies (e.g. limit number of associates, provide minimum number of coaching sessions, standardize incentives across agencies)
Social Networks TestingOverview
• New patient navigation position located in ASOs, HIV clinics, and community-based organizations
• Employ ten full-time, non-medical professionals• Work with newly diagnosed, new to care, out of care,
post-incarcerated and at risk clients• Identify and address client barriers to medical care
over a period of nine months• Transition clients to case management or self-
management
Linkage to Care Specialist (LTCS) Overview
45
Reported cases of HIV infection presumed to be alive by county, Wisconsin, as of 12/31/13
*Excludes 168 cases with the Wisconsin Department of Corrections as the last known address.
Number of Cases
1-20
21-40
41-100
101-200
201-3320
Dane County:AIDS Network UW HIV/AIDS Care Program
Milwaukee County:ARCWMCW ID Clinic16th Street CHCOutreach CHCMilwaukee Health Services
Linkage to Care Specialist Service Locations
• Similarities to Case Management:• Service provision via assessment, individualized service
plan development, and making referrals for needed services
• Differences from Case Management:• Specialist approach to barriers preventing linkage or
engagement in medical care• Smaller case loads (15 clients vs. 60 clients)• Use of motivational interviewing• More field work opportunities• Time limited
Linkage to Care Specialist Overview (continued)
47
Challenges
• Initial role confusion between LTCS and case managers
• Initial resistance among some providers• Referrals to LTCS for out of care clients limited to on-
site LTCS• Client resistance to transition out of Linkage to Care
(LTC) Program• Limits of existing case management system to serve
high need clients
48
Interim Outcomes
49
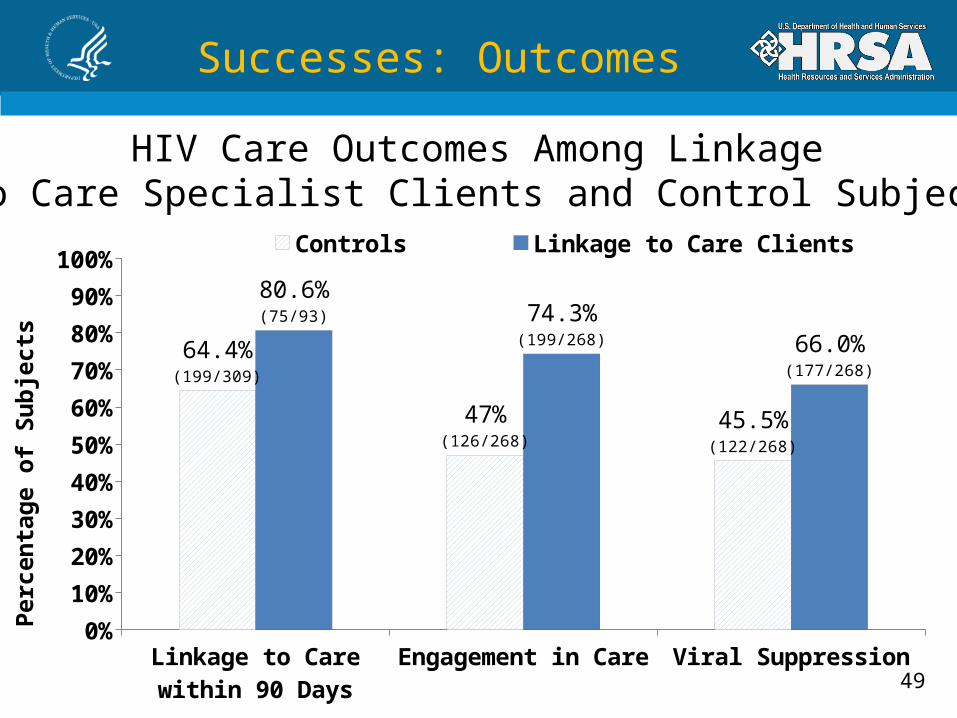
Successes: Outcomes
HIV Care Outcomes Among Linkage to Care Specialist Clients and Control Subjects
Linkage to Care within 90 Days
Engagement in Care Viral Suppression0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
64.4%(199/309)
47%(126/268)
45.5%(122/268)
80.6%(75/93) 74.3%
(199/268) 66.0%(177/268)
Controls Linkage to Care Clients
Per
cen
tag
e o
f S
ub
ject
s
50
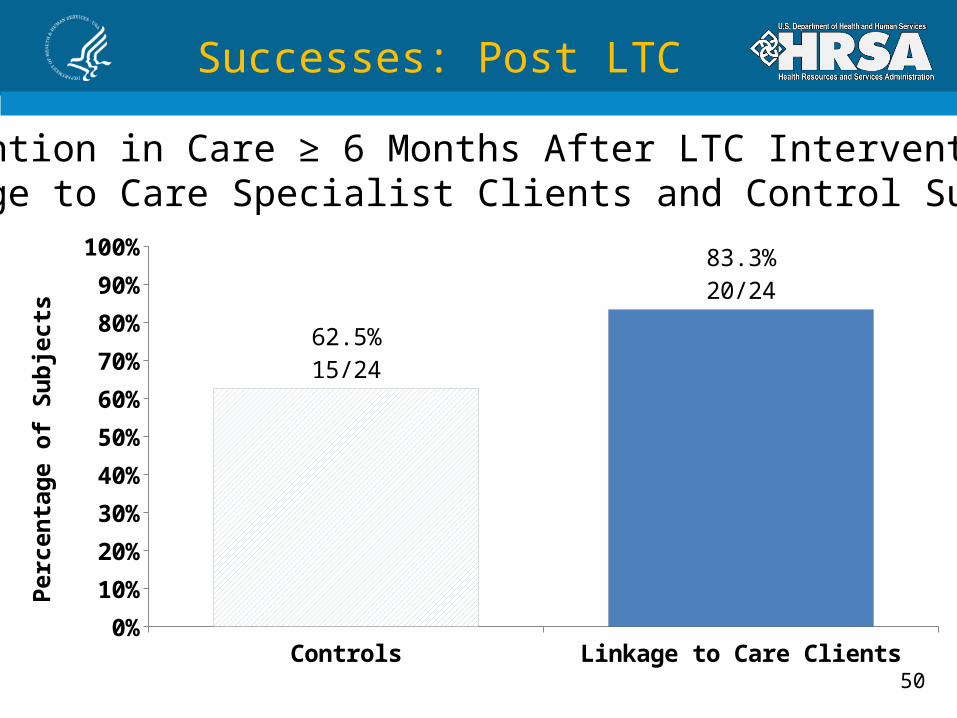
Successes: Post LTC
Retention in Care ≥ 6 Months After LTC Intervention: Linkage to Care Specialist Clients and Control Subjects
Controls Linkage to Care Clients0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
62.5%15/24
83.3%20/24
Per
cen
tag
e o
f S
ub
ject
s
51
Successes: Client Perspective
• Linkage to Care Specialists provided multiple forms of social support:• Mitigated negative feelings associated with HIV stigma• Increased motivation to adhere to medical care• Increased comfort with medical care• Caused reluctance to transition out of LTC
52
Successes: Client Perspective
“When I had to make appointments she made sure I got there. She would come and pick me up all of the time, every time. She never missed a time...That made me feel more positive to go and do what I had to do…that is why I’m non-detectable right now...”
53
Successes: Provider Perspective
“I can’t imagine now trying to function effectively in clinic without [our LTCS]... I have had numerous cases where [the LTCS] was instrumental in getting the patient in to clinic with me, [and] many more where she was instrumental in keeping the patient engaged in care…I can’t imagine how any of these people would have been successfully engaged in care without the intensive efforts of [the LTCS]...”
54
Lessons Learned
• The collaborative process led to better integration of care and prevention services
• Setting client expectations up front was critical to success and eases transition out of the program
• Both LTCSs with formal social work education and those without can have success with clients
• Numerous best practices were identified that will be applied to case management
• All Ryan White funded services will be evaluated based on their impact on linkage, retention, and viral suppression
55
Sustainability Plan
• Commit to funding LTCS until final evaluation results are available (ADAP rebate, Part B case management dollars, agency revenue)
• Incorporate lessons learned from the LTC Initiative into newly developed Medical Case Management Practice Standards• Motivational interviewing• Use of text messaging • More focus on behavior change rather than just referral to
other services
SYSTEMIC LINKAGES QUALITATIVE CROSS-SITE PRELIMINARY DATAKimberly Koester, MADirector of Qualitative Research Evaluation and Technical Assistance CenterUniversity of California, San Francisco
57
Developing Interventions
• Over two years, State Health Departments convened multi-day “learning sessions” with stakeholders (45-80 people) from organizations and institutions serving people living with HIV.
• Meetings led to communication channels opened where they had not previously existed.
• Tremendous buy-in on the importance of linkage, retention and re-engagement efforts emerged as a priority.
58
Navigation Interventions
• “Navigation” interventions resemble case management, but have unique elements:
• Intensive services offered to a select group of patients.
• Services are offered on a short-term basis.
• Caseloads are intentionally small.• Interventionists are encouraged to
leave the office to meet with patients in non-clinical environments.
59
Implementation Observations
• Overall, patients are responding well to the interventions.
• Interventionists are spending more time with patients than any one else in the clinic.
• “Fieldwork” is a common feature and a necessary activity to reach out of care patients.
• Newly diagnosed patients have different (lesser) needs than those who are out of care.
• Goals to support newly diagnosed patients are clear: support to 1) cope with diagnosis and 2) link and remain in care.
SYSTEMIC LINKAGES QUANTITATIVE CROSS-SITE PRELIMINARY DATAEdwin D. Charlebois, III, MPH PhDProfessor of Medicine, Evaluation and Technical Assistance CenterUniversity of California, San Francisco
61
Cross-Site Evaluation
The primary goal of the cross-site intervention outcomes evaluation is:
• To identify significant improvement across demonstration states in access to and retention in high quality HIV care for hard-to-reach populations of HIV-infected persons that are associated with innovative mechanisms which establish effective and sustainable linkages among Ryan White and other, community and non-traditional organizations that provide HIV-related services.
62
• Large Population Size to be Touched by the Collective SPNS Interventions (N = 68,636)
• Significant Diversity in:• Geographic Settings
• Race/Ethnicity
• Risk Groups
• Insurance Status
• Client Types (new Dx, Out-of-Care, never linked)
SPNS Intervention Study Populations
63
Patient Characteristics – New Diagnoses
Based on data reported to the ETAC as of 12/2/2014.
64
Patient Characteristics – New Diagnoses
Newly diagnosed client type was diagnosed with HIV within one year of enrollment in the intervention.Other race/ethnicity includes Asian, Native Hawaiian/Pacific Islander, American Indian or Alaska Native, and multiracial.Excludes data from testing intervention clients submitted as a separate dataset.Based on data reported to the ETAC as of 12/2/2014. Preliminary Data – DO NOT CITE