Patient Information The following patient information is required to process the lab order:
● Patient first name ● Patient last name ● Ethnicity ● Race ● DOB
○ If testing is made available to minors, Partner MUST pass guardian first and last name. Order information, including telephone number and email address MUST match those of the guardian, instead of the minor.
● Gender ● Telephone # ● Address
○ Street Info ○ City ○ State ○ Zip
● Eligibility Questionnaire Responses (using Custom Attributes. See details below.)
3
PWN Proprietary and Confidential
Sample API Calls Below is a sample of the various API calls you can use for interacting with our platform.
● All of this and additional functionality can be found in our API Documentation: https://docs.pwnhealth.com Password: labs_module
Create Order API Documentation Reference POST https://api-staging.pwnhealth.com/v2/labs/orders
Mock Order Approval API Documentation Reference Put https://api-staging.pwnhealth.com/v2/orders/{{order_id}}/mock/approval
Get Requisition PDF API Documentation Reference GET https://api-staging.pwnhealth.com/v2/labs/orders/{{order_id}}/pdfs/requisition
Replace {{order_id}} with the unique ID of the order.
Get Order API Documentation Reference GET https://api-staging.pwnhealth.com/v2/labs/orders/{{order_id}}
Replace {{order_id}} with the unique ID of the order.
Get Order Results PDF API Documentation Reference GET https://api-staging.pwnhealth.com/v2/labs/orders/{{order_id}}/pdfs/results
Replace {{order_id}} with the unique ID of the order.
"reference": "####", // External ID or Barcode ID when present "Collection_date":"202005011445", // This should be used if the collection date of the sample is known. Format for the data is YYYYMMDDHHMM. May 1, 2020 at 2:45pm is
"next_of_kin": { // Required if patient is under 16, see the section on minors and testing.
"first_name": "next_first_name",
"last_name": "next_last_name",
"phone": "555-555-5555"
},
"ethnicity": "Prefer not to share", // SEE NOTES BELOW RELATED TO ETHNICITY FIELD "custom_attributes": { // SEE NOTES BELOW RELATED TO CUSTOM ATTRIBUTES "Race": [
"Black or African American",
"Asian"
],
//The following questions are required for HHS reporting. Acceptable answers for the following are "Yes", "No", or "Unknown" unless otherwise specified.
"Is this your first COVID-19 test (PCR or antibody)?":"No",
"Are you employed in a healthcare setting?":"Yes",
"Do you have COVID-19 symptoms (fever, cough, shortness of breath,
etc.)?":"Yes",
"If yes, what was the date that your symptoms started?": "mm/dd/yyyy",
//Conditional on the question above it, use mm/dd/yyyy format for answer
"Are you currently in the hospital?":"No",
"Are you currently in the ICU?":"No",
"Do you live or work in a congregate setting?":"Unknown",
"Are you pregnant?":"No",
//THE QUESTIONS BELOW ARE JUST EXAMPLES, SEE CLINICAL DOCUMENTATION FOR QUESTIONNAIRE
INFORMATION AND THE NOTES SECTION BELOW.
"Please select the option that best describes your symptoms":"Severe/Limiting
Symptoms",
5
PWN Proprietary and Confidential
"Please select the option that most closely describes you":"Testing
Recommended",
"Choose the statement that applies to you":"Option 1",
"Do any of the following statements apply to you?":"Option 2",
"Do any of the following statements apply to you?":"I am 65 years of age or
older|I have been told by my doctor that I am very overweight or obese"
Custom Attributes (Patient Questionnaire) Custom attributes are being utilized for providing the questions/answers to the physician who is reviewing the orders. The questionnaire for this program will be listed below, but it does not include the extensive list as there are branching questions to the questionnaire, so not all of them may be necessary.. To reiterate, the questionnaire that is being asked to the patient, the questions and answers need to be submitted within the custom attributes.
Custom Attribute Functionality
Custom attributes when adding them to the order creation payload, can be considered as "attribute" and "value". "Attributes" can be considered the question that is being asked. "Value" can be considered the answer for the preceding attribute. So when adding it to the order payload, you can see the example below:
custom_attributes": {
"attribute": "value",
"attribute": "value",
...
...
7
PWN Proprietary and Confidential
...
"Exposure": "Known exposure",
"Comorbidities": "High risk"
},
See the sample order payload for more examples. For any additional information, please see the API documentation.
HHS Reporting Questions
Included in the custom attribute section, in addition to the eligibility screener questions outlined above, are the questions required by HHS. The questions are outlined below
1. Is this your first COVID-19 test (PCR or antibody)? a. Yes, No, Unknown
2. Are you employed in a healthcare setting? a. Yes, No, Unknown
3. Do you have COVID-19 symptoms (fever, cough, shortness of breath, etc.)? a. Yes, No Unknown b. If yes, what was the date that your symptoms started? mm/dd/yyyy
4. Are you currently in the hospital? a. Yes, No, Unknown
5. Are you currently in the ICU? a. Yes, No, Unknown
6. Do you live or work in a congregate setting (including nursing homes, residential care for people with intellectual and developmental disabilities, psychiatric treatment facilities, group homes, board and care homes, homeless shelter, foster care or other setting)?
a. Yes, No, Unknown 7. Are you pregnant?
a. Yes, No, Unknown
8
PWN Proprietary and Confidential
Questionnaire Extract
Question 1
Question 2
Question 3
9
PWN Proprietary and Confidential
Question 4
Question 5
10
PWN Proprietary and Confidential
Testing for Minors, Guardian information If the patient is under the age of 16, it is required that you collect guardian information along with the order. Guardian name MUST be passed to PWN if the patient is under 16 only by adding guardian name in the "next_of_kin" section of the order. Guardian name is NOT required if the patient is an employee of the Partner AND between the ages of 16 and 18. Sample below: "next_of_kin": {
"first_name": "next_first_name",
"last_name": "next_last_name",
"phone": "555-555-5555"
}, Note, “first_name” and “last_name” are required, “phone” is optional.
Subscription_ID Subscription_ID is a field that you will need to pass in the previous order # of the patient if it is related to serology. We will use this number in our system to link the orders together so that when the patient receives results from PWN, they can have access to them via the platform rather than having to open them separately.
11
PWN Proprietary and Confidential
Race/Ethnicity
Race
Race information is to be stored under the custom attributes in a list format either before or after the patient questionnaire information. Rather than the typical format for custom attributes mentioned in the section above, this one is formatted as "attribute: [value, value, value]". An example is below where two options are selected for Race.
"Race": [
"Black or African American",
"Asian"
], Race should be submitted in this format regardless of the number of selections. Minimum is one item to be listed and there is no upper limit. An example list of acceptable values can be found below, but please see the other clinical related documentation and requirements for the full and accurate list.
"American Indian or Alaska Native" "Asian", "Black or African American" "Native Hawaiian and other Pacific Islander" "Two or more races" "White" "Other" "Prefer not to answer"
Ethnicity
There is a specific field in the system for ethnicity to be stored. This field should only be receiving one value. An example list of acceptable values can be found below, but please see the other clinical related documentation and requirements for the full and accurate list.
"Hispanic or Latino" "Not Hispanic or Latino" "Other"
Insurance When sending over insurance information, the PWNHealth system supports both Primary and Secondary information to be associated with the order. Please take a look at the API documentation related to insurance, but the information is duplicated below as well. When submitting an order, you need to include the following information
● Bill_type
12
PWN Proprietary and Confidential
○ The default bill type per account is set as client. To utilize third party/insurance billing is to include this flag with the value ‘3’ for insurance billing.
○ NOTE: In the event of no insurance plan being available, bill type "3" should still be utilized and dummy/placeholder values should be used for the required fields.
● Primary_insurance_info ○ See the table below for the specific fields related to insurance.
● Secondary_insurance_info ○ If the patient has secondary insurance, PWNHealth does accept that as well, but
primary_insurance_info is required.
Insurance API Fields
Property Required Description
carrier_code Yes Insurance Company Payer or Carrier Code
company_name Yes Insurance Company Name
Company_address block Yes Block containing Company Address information.
Line1 Yes Insurance Company Address Line 1
Line2 No Insurance Company Address Line 2
City Yes Insurance Company City
State Yes Insurance Company State
Zip Yes Insurance Company Zip Code
policy_number Yes Patient Insurance Policy Number
group_number Yes Patient Insurance Group Number
name No Insurance Policy Name
group_employer_name No* (some labs require this field, if not provided it will be sent as a “null” string).
Insurance Group Employer Name
relationship No* Patients relationship to insurance policy holder "1" - Self "2" - Spouse "3" - Other "4" - Parent "5" - Child NOTE: By default, if this is not provided this will default to "1" - Self NOTE 2: If any value other than “1”
13
PWN Proprietary and Confidential
is selected, policyholder information will be required.
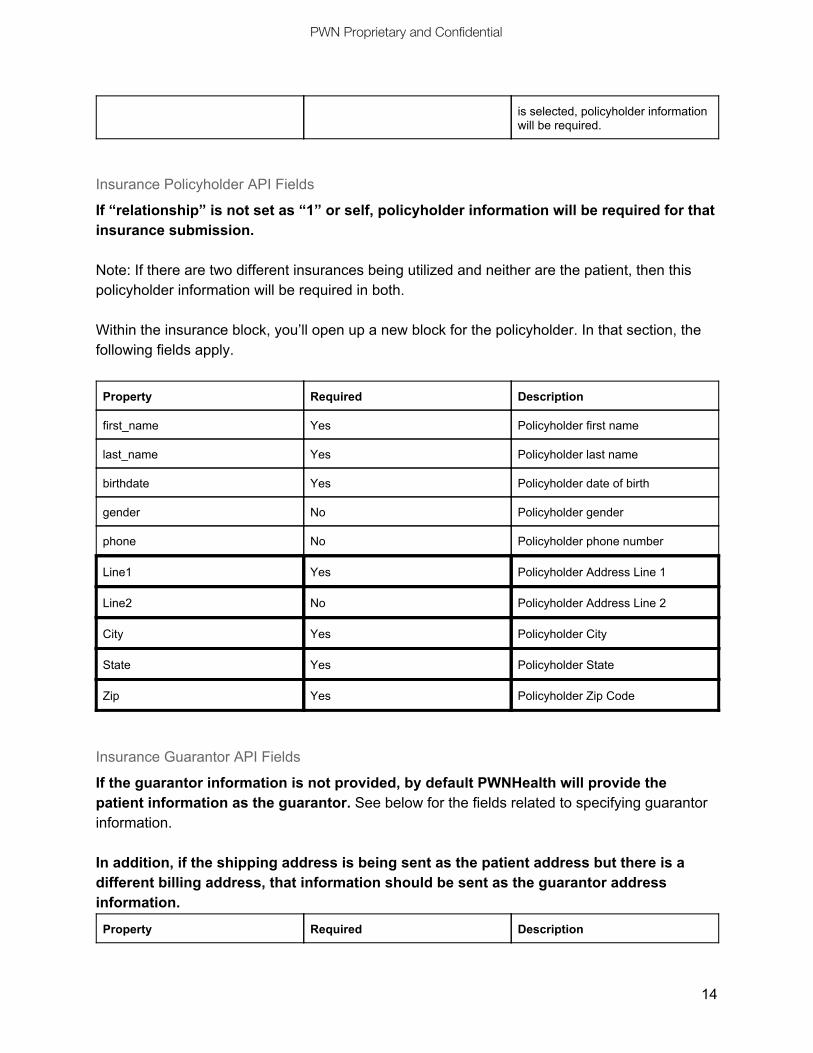
Insurance Policyholder API Fields
If “relationship” is not set as “1” or self, policyholder information will be required for that insurance submission. Note: If there are two different insurances being utilized and neither are the patient, then this policyholder information will be required in both. Within the insurance block, you’ll open up a new block for the policyholder. In that section, the following fields apply.
Property Required Description
first_name Yes Policyholder first name
last_name Yes Policyholder last name
birthdate Yes Policyholder date of birth
gender No Policyholder gender
phone No Policyholder phone number
Line1 Yes Policyholder Address Line 1
Line2 No Policyholder Address Line 2
City Yes Policyholder City
State Yes Policyholder State
Zip Yes Policyholder Zip Code
Insurance Guarantor API Fields
If the guarantor information is not provided, by default PWNHealth will provide the patient information as the guarantor. See below for the fields related to specifying guarantor information. In addition, if the shipping address is being sent as the patient address but there is a different billing address, that information should be sent as the guarantor address information.
Property Required Description
14
PWN Proprietary and Confidential
guarantor_relationship No* Guarantor’s relationship to patient "1" - Self "2" - Spouse "3" - Other "4" - Parent "5" - Child NOTE: By default, if this is not provided this will default to "1" - Self
guarantor_name Yes (if guarantor_relationship is not Self)
Guarantor Name (First and Last)
guarantor_phone Yes (if guarantor_relationship is not Self)
Guarantor Phone
Guarantor_Address Yes (if guarantor_relationship is not Self)
Address block for Guarantor
Line1 Yes (if guarantor_relationship is not Self)
Guarantor Address Line 1
Line2 No Guarantor Address Line 2
City Yes (if guarantor_relationship is not Self)
Guarantor City
State Yes (if guarantor_relationship is not Self)
Guarantor State
Zip Yes (if guarantor_relationship is not Self)
Guarantor Zip Code
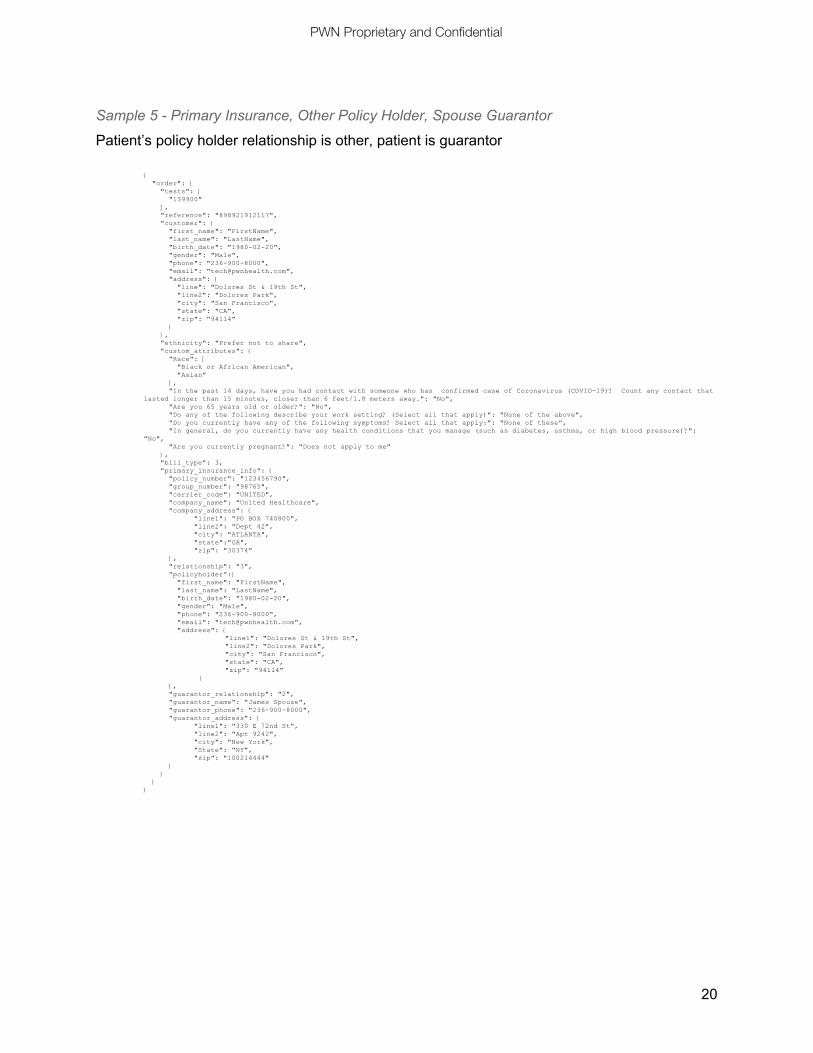
Sample Insurance Order Payloads (Postman samples)
Sample 1 - Primary and Secondary Insurance
Primary insurance policy holder is the patient, the guarantor is the spouse. Secondary insurance policyholder is the spouse, the guarantor is the spouse.
The patient is the policyholder and guarantor, but they are having their test shipped somewhere other than their billing address. Shipping address is located in the Patient information, and the billing address is in Guarantor information.
● Question: Which Bill Type should I use? ○ For most COVID related insurance use cases, you’ll need to use Bill Type "3" for
insurance. Even if the patient doesn’t necessarily have insurance, you’ll need to include some dummy values there so it is properly sent to the labs.
21
PWN Proprietary and Confidential
Document Changelog
Date Changes
May 14th, 2020 Added information related to insurance. Added documentation for Race/Ethnicity submissions. Improved documentation surrounding Custom Attributes. Added sample order payloads for insurance orders and configurations.
May 20th, 2020 Added information related to policyholder for insurance Updated API section to include policyholder details Updated sample API calls to include policyholder examples
June 3rd, 2020 Added a section for subscription_id Updated sample payload to include subscription_id
June 5th, 2020 Added next_of_kin section details for use of guardian information for patients under the age of 18.
June 24th, 2020 Clarified guardian requirements for minor testing.
June 25th, 2020 Guide updated to include questionnaire for specific program and sample payload updated with example.
June 30th, 2020 Changed Testing for Minors, Guardian information age information
July 10, 2020 Updated Sample API payload to include HHS requirements as well as a description of the questions in the custom attribute section description.