T-regulatory Cells in Renal Ischemic injury Alvaro Pacheco-Silva Laboratory of Clinical and Experimental Immunology Division of Nephrology Universidade Federal de São Paulo Hospital do Rim e Hipertensão Hospital Israelita Albert Einstein São Paulo, Brasil
Transcript
T-regulatory Cells in Renal Ischemic injury
Alvaro Pacheco-Silva
Laboratory of Clinical and Experimental Immunology Division of Nephrology
Universidade Federal de São Paulo Hospital do Rim e Hipertensão
Hospital Israelita Albert EinsteinSão Paulo, Brasil
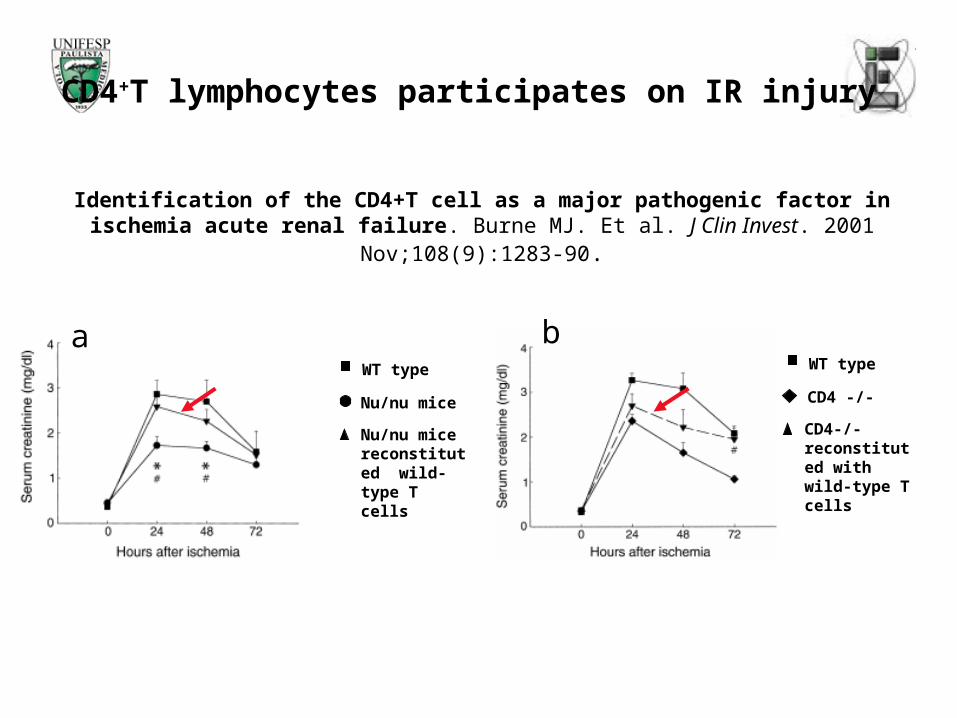
Identification of the CD4+T cell as a major pathogenic factor in ischemia acute renal failure. Burne MJ. Et al. J Clin Invest. 2001 Nov;108(9):1283-90.
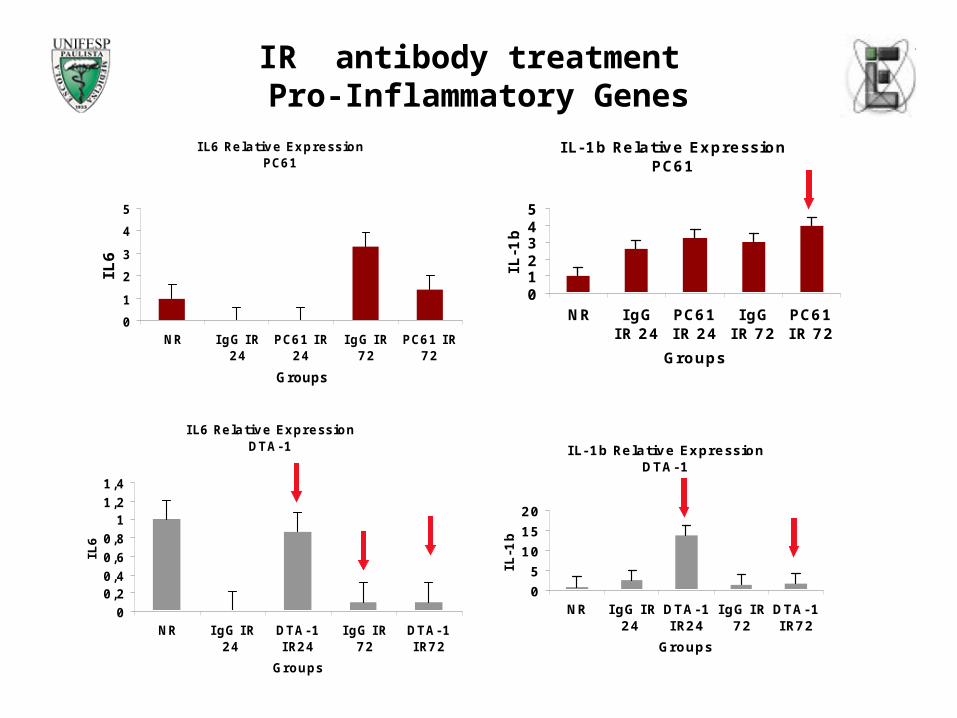
IR antibody treatment Conclusions and Perspectives
At 24 hours of reperfusion, depletion of TCD4+CTLA-4+Foxp3+ cells was 30,3% (spleen) and 67,8% (para renal lymphnodes).After 72 hours of reperfusion, depletion of TCD4+CTLA-4+Foxp3+ was 43,1% (spleen) and 90,22% (para renal lymphnodes). This depletion was efficient in generate significant responses in both 24 hours and 72 hours if reperfusion Depleted mice presented similar renal function to control animals at 24 hours, but 72 hours after IRI, PC61 treated mice presented significant worst renal function compared to the group that received IgG. DTA-1 treated animals presented significant protection at the same timepoint, indicating that different subsets of cells can be acting at these timepoints.
Furthermore, histopathological analyses showed that there was a pronounced incidence of necrosis for both PC61 treated and IgG in IR 24 hours experiments. On the other hand, in IR 72 hours experiments we observed a regeneration pattern in both PC61 and IgG treated animals, but in the PC61 treated group there was a significant necrosis index (p<0.001), comparing with IgG treated group, suggesting that TCD4+CTLA4+FOXP3+ cell population could be important in a late phase of injury recover.
It is known that the stress and tissue damage associated with IRI influence the development of a immune response to protect the tissue damage. Thus, our results suggests a role for TCD4+CTLA4+FOXP3+ cells (naturally arising T teg cells) in renal IRI experimental model.
24 hs:TCD4+ effectorStimulated by DTA-1escape from T Reg suppression and make injury worst
Proinflamatory cytokinesProinflamatory cytokinesIL-1b and IL-6IL-1b and IL-6
72 hs:TRegs GITRhigh stimulated by DTA-1 start to suppressTCD4+ response
Anti inflamatory Anti inflamatory genesgenesSuch as HO-1 and Such as HO-1 and polarizationpolarizationtoward Th2 (GATA-3) toward Th2 (GATA-3) transcription factortranscription factor
72 hs:If there is no T Reg at this point (PC61 treatment), there is no recovery from injury
Rebecca M. M. MonteiroMarcio J. DamiãoGiselle GonçalvesCarla Q. FeitozaMarcos CenedezeNephrology Division - Universidade Federal de São PauloBrazil
Prof. Dr.Mauricio M. RodriguesFanny TzelepisInterdisciplinary Center for Gene Therapy CINTERGENUniversidade Federal de São Paulo, Brazil
Prof. Dr.Niels Olsen S. CamaraImmunology Division Universidade de São Paulo USP, Brazil
Vicente de Paula A. TeixeiraMarlene A. dos ReisDepartment of Pathology, Universidade Federal de Uberaba, Minas Gerais, Brazil
Prof Dr. S. SakaguchiT. Yamaguchi (DTA-1)H. Uryu (PC61)K. Nagahama (IRI)M. Ono (Real Time PCR)Institute for Frontier Medical SciencesKyoto University Japan