29
Taking the Fear out of Government Audits: Successful Strategies for Preparing, Surviving and Thriving

Taking the Fear out of Government Audits: SuccessfulStrategies for Preparing, Surviving and Thriving

9/26/2019
1
Taking the Fear Out of Government Audits: Successful Strategies for
Preparing, Surviving and Thriving
Learning Objectives
Participants will be able to discuss current government audit risk areas and common reasons for claim denials.
Participants will be able to discuss operational and legal strategies for implementing an effective “audit game plan” and proven tactics for defending adverse audit findings.
Participants will be able to describe best practices and necessary steps for being prepared, surviving and thriving under government contractor scrutiny.
2

9/26/2019
2
AGENDA
Post-Acute Care Enforcement
Contractor Landscape
Major Risk Areas and Focus for Contractor Review
Practical Strategies
Defending Adverse Audit Findings
60-Day Overpayment Rule Implications
Resources & Take-Home References
Questions
3
POST-ACUTE CARE ENFORCEMENT
9/26/2019
3
Increased Focus on Post-Acute Care
In recent years, government payment policies have been geared towards limiting time spent in the acute care setting.
― This has naturally shifted more focus on the post-acute care setting, including:o Hospiceo Home Healtho Inpatient Rehabilitation Facilities (IRFs)o Skilled Nursing Facilities (SNFs)
In 2018, 764 criminal actions, 813 civil enforcement actions, and recoveries over $1.4 billion related to home health fraud
Medicare hospice payments = $16.8 billion in 2016
This also means INCREASED OVERSIGHT
*Source: MedPAC March 2018 Report to Congress 5
Post-Acute Enforcement Is Intensifying
6

9/26/2019
4
OVERVIEW OF CONTRACTOR LANDSCAPE
Contractors - Big Picture
Federal and state governments outsourcing oversight responsibilities
Greater number of private companies authorized to request and analyze information from provider community
Contractors are not created equally
Understanding different roles and authority of each contractor category will enhance providers’ ability to succeed in new contractor world
8

9/26/2019
5
Contractors - Big Picture
Effectively managing contractor audits requires a multi-layered approach, including: 1. Understanding the scope of authority for each contractor category;
2. Equipping employees with sufficient knowledge to identify and respond to contractor requests;
3. Monitoring for improper recoupments;
4. Formulating appeal packages that demonstrate the appropriateness of the services being challenged; and
5. Understanding the potential consequences of audit findings.
9
Government Audits Focused in Home Health & Hospice
Unified Program Integrity Contractors (UPICs)– Perform fraud, waste, and abuse detection, deterrence and
prevention activities for Medicare and Medicaid claims.
Medicare Administrative Contractor (MACs): – Target, Probe & Educate (TPE) replacing the previous ADR process– Denials > than 15% may trigger referral to UPIC
Comprehensive Error Rate Testing Program (CERT)
Recovery Audit Contractors (RACs)
– Audit focus must be pre-approved
10

9/26/2019
6
Government Audits Focused in Home Health & Hospice (cont.)
Office of Inspector General (OIG)
Department of Justice (DOJ)
Medicaid Fraud Control Units (MFCUs)
11
What Does this Mean for Washington HH & Hospice Providers?Consider…Medicare• National Government Services,
Inc. (HH & H MAC)• Performant Recovery, Inc. (HH
& H RAC)• Livanta LLC. (CERT Documentation
Contractor)• AdvanceMed Corp. (CERT Review
Contractor)• The Lewin Group (CERT Statistical
Contractor)
Potential Fraud• Qlarant Integrity Solutions,
LLC (formerly Health Integrity) (UPIC Western
Jurisdiction)• MFCD (Medicaid)
Medicaid• Washington State Medicaid
Fraud Control Division (MFCD)
• (Medicaid RAC pending)
12
9/26/2019
7
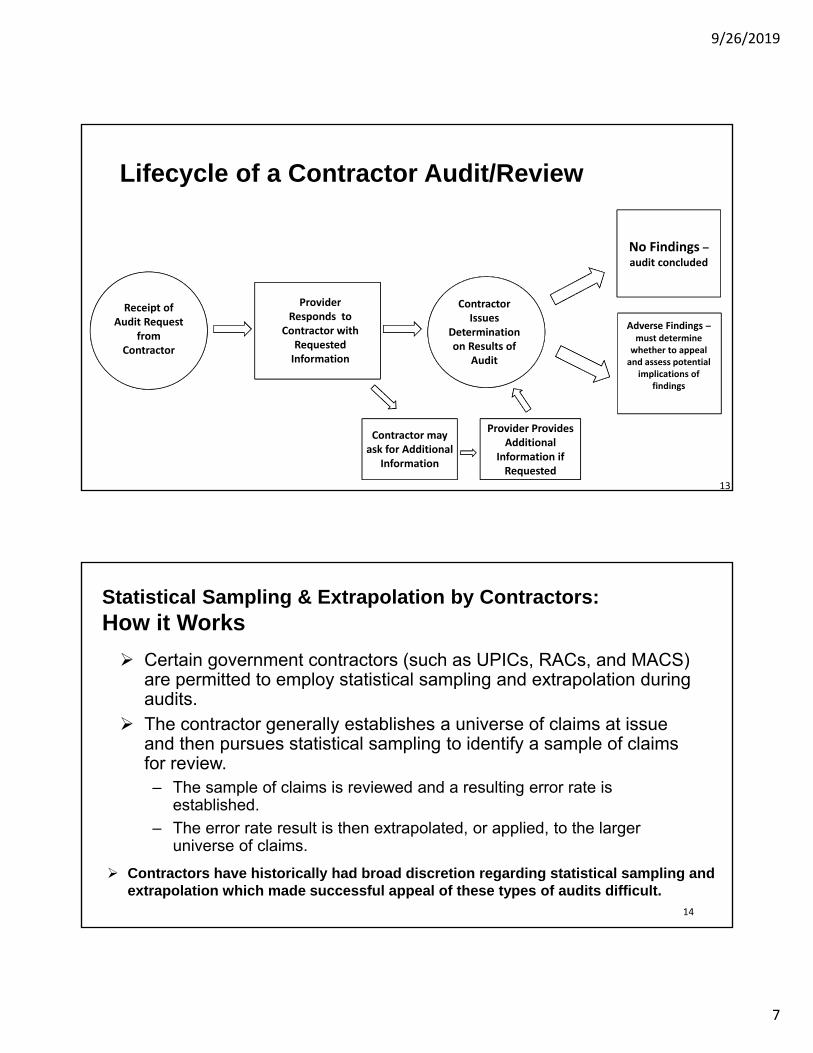
Lifecycle of a Contractor Audit/Review
Receipt of Audit Request
from Contractor
Provider Responds to
Contractor with Requested Information
Contractor Issues
Determination on Results of
Audit
No Findings –audit concluded
Adverse Findings –must determine whether to appeal and assess potential
implications of findings
Contractor may ask for Additional
Information
Provider Provides Additional
Information if Requested
13
Statistical Sampling & Extrapolation by Contractors: How it Works
Certain government contractors (such as UPICs, RACs, and MACS) are permitted to employ statistical sampling and extrapolation during audits.
The contractor generally establishes a universe of claims at issue and then pursues statistical sampling to identify a sample of claims for review. – The sample of claims is reviewed and a resulting error rate is
established.
– The error rate result is then extrapolated, or applied, to the larger universe of claims.
Contractors have historically had broad discretion regarding statistical sampling and extrapolation which made successful appeal of these types of audits difficult.
14

9/26/2019
8
RISK AREAS AND FOCUS FOR CONTRACTOR REVIEW
15
Enforcement Trends: General Risk Areas Billing for services not rendered
Misrepresentation or upcoding of services
Medically unnecessary services
Falsification of medical records and physician authorizations
False certification of patients as homebound
Unlawful relationships with patient recruiters and referral sources
Employing Excluded Individuals
Insufficient documentation to support reimbursement
Kickbacks to referral sources and patients16
9/26/2019
9
Enforcement Focus:Hospice
Admitting or retaining ineligible patients without adequate documentation
Multiple changes to terminal diagnosis
Length of stay outliers
Revocation and prompt re-admission
Level of care outliers
Failure to cover drugs or services related to terminal condition
Use of blank signed physician certifications
17
Hospice Data Mining
Length of Stay (LOS)― High percentage of beneficiaries with LOS greater than
180 days and LOS less than 7 days Level of Care (LOC)
― Percent of higher paid LOC - General Inpatient Care (GIP) and Continuous
Terminal Diagnosis Live Discharges and/or Revocations
― High percentage of live discharges― Concern inappropriate admissions and/or patients
discharged due to CAP risk QAPI Data
― High percentage poor quality scores 18
9/26/2019
10
Case-Mix Weight / Therapy Overutilization
Poor publically reported Outcome Data
Missing or incomplete Certifications
Diagnosis Coding
Insufficient documentation to support skilled medically necessary care
Multiple Re-Certifications
OASIS un-timely submission
Past deficiencies with no improvement19
Enforcement Focus:Home Health
Home Health Data Mining
Visit Utilization− High percentage of therapy utilization− High percentage of beneficiaries with 5 – 7 visits− High percentage of episodes the beneficiary had no recent visits with certifying MD
Admissions/Re-Admissions− High percentage of beneficiaries with multiple readmissions in short period of time− High percentage of episodes not preceded by a hospital or nursing home stay
Diagnosis Coding− High percentage of episodes with a primary diagnosis of Diabetes or Hypertension
Claims− High percentage of beneficiaries with claims from multiple HHAs
QAPI Data− High percentage poor quality scores
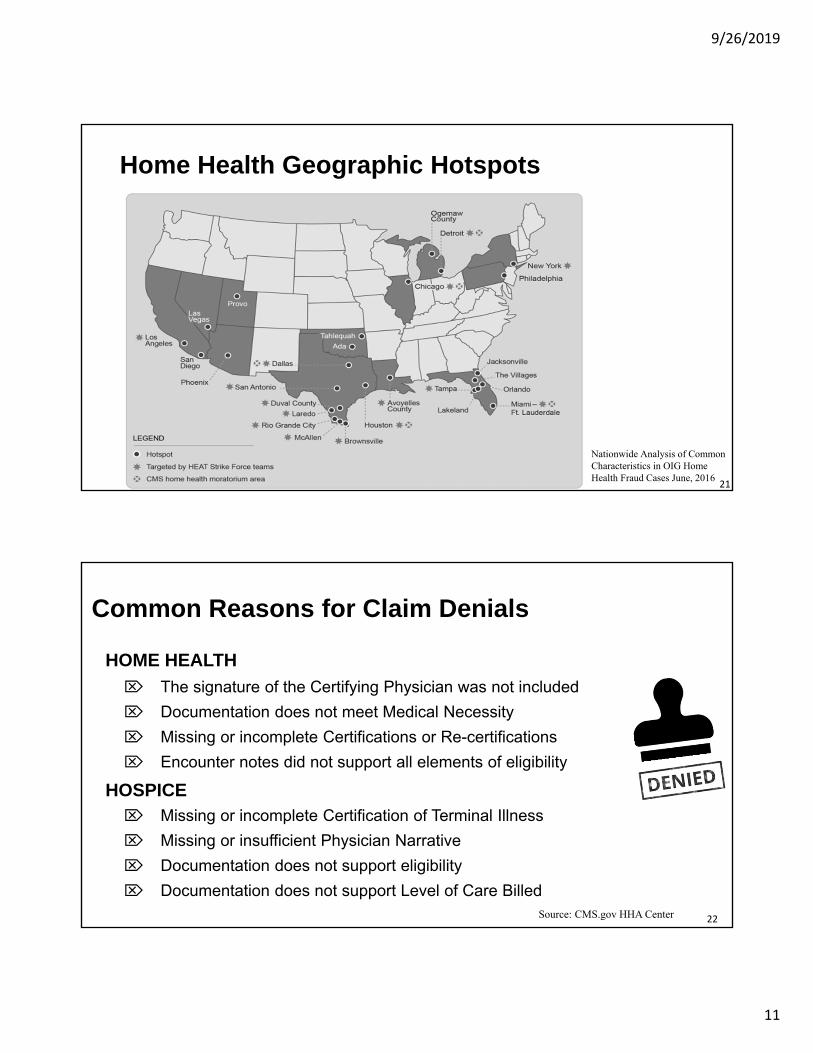
OIG Data Brief “Nationwide Analysis of Common Characteristics in OIG Home Health Fraud Cases” (June 2016)20
9/26/2019
11
Home Health Geographic Hotspots
Nationwide Analysis of Common Characteristics in OIG Home Health Fraud Cases June, 2016
21
Common Reasons for Claim Denials
HOME HEALTH
The signature of the Certifying Physician was not included
Documentation does not meet Medical Necessity
Missing or incomplete Certifications or Re-certifications
Encounter notes did not support all elements of eligibility
Missing or incomplete Certification of Terminal Illness
Missing or insufficient Physician Narrative
Documentation does not support eligibility
Documentation does not support Level of Care Billed
HOSPICE
22Source: CMS.gov HHA Center

9/26/2019
12
Most Popular Denial Statement:TPE Denial - NGS
2323
PRACTICAL STRATEGIES
24

9/26/2019
13
Practical Strategies: Building a Solid Foundation
Organization Mission, Ethics & Compliance Plan
QAPI needs to be part of day-to-day operations, revenue cycle & compliance– QAPI Program determines the direction of agency
operations & priorities– Prioritize based on agency performance (poor outcomes,
high-risk)– Comprehensive review of what related activities are you
already doingo Many agencies have been doing performance
improvement projects - may need to formalize
2525
Practical Strategies: Building a Solid Foundation
Invest in Education & Training Programs
– Start with your onboarding & orientation program
o Structured preceptor led (min 12 weeks)
o Incorporate Compliance Program Training Establish your company’s Culture of Compliance
o Use competency testing for “experienced” employees BEFORE they go out in the field to determine level of orientation needed
– Annual Training
o Ethics & Compliance; Regulations (“Rapid Regs”)
o Documentation
o Clinical Skills26
26

9/26/2019
14
Practical Strategies: Leverage Technology & Data
Know Your Technology & Data Available
– EMR, Industry Statistical Tools, Point of Care
– Key Performance Indicators & Benchmarkso Operational & Financial Data
− Publically Reported Datao Star Ratings / Home Health Compareo Patient Experience - CAHPs
− Review CASPER Reportso Summarizes OASIS Data - Outcomes, Adverse Events, Agency Characteristics
− Review PEPPER reportso Comparative Medicare claims data statistics
Evaluate your data to identify trends and investigate outliers
Refer to RESOURCES:List of KPIs
27
Know the regulatory trends & audit focus areas internally & externally
Use your Compliance & QAPI Plans to direct audits
– Sample size should be relative and adjusted based on historic results
– Assess audit needs to ensure appropriate scope and do not re-create the “wheel”
– Create audit tools for collecting reimbursement vs. clinical requirementso Use descriptive terms –”Adequate” “Needs Improvement” in place of
“Yes/No” answers when testing open to interpretation requirements
– Must have Accountability & follow-up Action Plan for deficiencies identified
Practical Strategies: Audit Game Plan
28

9/26/2019
15
Tips for Documentation Compliance
– Orientation & Education….It IS all about the DOCUMENTATION
– Annual training & competency
– Eliminate unnecessary processes that involve additional documentation & tracking
o Forms (Certification, F2F); physician orders vs. communication
Evaluate and Monitor – Ongoing
– Establish PIPs according to audit results to track improvement
– Once threshold is met – suspend the audit!
Practical Strategies: Audit Game Plan
29
Practical Strategies:Prepare for Contractor Reviews
Implement policy & provide training– Internal notification – Management, Compliance Officer, Legal Counsel– Internal tracking – spreadsheet for responses & appeals– Preparing records
All contractor requests are not equal
Know the type of Auditor you are dealing with (UPIC, RAC, MAC, OIG)
Any request for records from a Medicare/Medicaid contractor should be given a consistently high level of attention
Contractor audits are anticipated in today’s environment – Do not panic! It may happen– An audit does not mean you have necessarily done something wrong – Be prepared to “show-off” your Compliance Program, QAPI & Audit Action Plans
30
Refer to RESOURCES:“Preparing for Submission”

9/26/2019
16
Lessons Learned
Illinois providers under Pre-Claim Review (now Review Choice Demo)– Primary reasons for non or partial affirmation related to technical focus on POC
and MD Certification requirements:o Certification Statement on POC was not all inclusiveo Still using F2F form; looking for “actual” encounter visit note (H&P)o Secondary reasons for “open to interpretation” issues we are well acquainted
with: Homebound and Medical Necessity
Similar results for Target, Probe & Educate (TPE) Medical Review− High percentage of denials on 1st round – certification & eligibility
OIG – Office of Audit Services− Review completed reports
31
Refer to RESOURCES:“Helpful Links – OIG Work Plan & Audits”
Home Health Certification of Eligibility Clarification
The F2F encounter is 1 of 5 eligibility criteria that require “Certification”
– HH agencies are required to ensure that all Medicare beneficiaries are eligible for services by ensuring of all 5 eligibility criteria have been met and are certified, including the face-to-face encounter documentation
– The CMS Form 485 is no longer an up-to-date or CMS endorsed document, as its certification statement does not encompass the face-to-face encounter; however, the F2F encounter does not require a separate certification statement.
– Agencies may develop a certification statement to encompass all five criteria that the physician just “signs-off”
– Although an NPP may complete and document a face-to-face encounter, NPP’s cannot certify eligibility criteria.
o NPP completes and documents the F2F encounter, a co-signature is not required.
3232

9/26/2019
17
Home Health Encounter (F2F) Clarification
“Based on preliminary reviews of documentation for the current HHA Probe and Educate endeavor, CMS is reminding providers that a face-to-face encounter form is not adequate documentation to support that a face-to-face encounter occurred” NGS Medicare
In CR 9119, CMS eliminated the narrative requirement (regarding the patient’s homebound status and need for skilled services) in the F2F encounter documentation.
– There is no mandatory form for the F2F Encounter.
– Examples of Acceptable Documentation of the F2F encounter – “Actual” visit note: Emergency Room Assessment Hospital Admission Assessment Hospital Physician Consultation Physician/NP/PA History & Physical Physician/NP/PA Office H&P Progress Note
– ASK FOR “H&P or Consult”, not looking for MD to write something specific for HH–Use their language NOT ours
3333
Compliant Certification Statement Example:
► I certify that a Face-to-Face Encounter occurred within the required timeframe; was performed on ________; was related to the primary reason for home health services; and was performed by an allowed provider.
► I certify that this patient is confined to his/her home and needs intermittent skilled nursing care, physical therapy and/or speech therapy or continues to need occupational therapy. The patient is under my care, and I have authorized the services on this plan of care and will periodically review the plan. (From 485)
► I attest that my signature on this document indicates my review and incorporation into this patient's medical record.
34
→ Include this Certification Statement on POC for Certifying MD to “sign off”
→ HH Agency is responsible for summarizing the required eligibility documentation of skilled, medically necessary & homebound…..
→ Agency fills in Date & Attach Visit Encounter Note for review/records 34
Refer to RESOURCES: “Final Certification Regulation”

9/26/2019
18
DEFENDING ADVERSE AUDIT FINDINGS
35
Defending Adverse Audit Findings:To Appeal or Not to Appeal
Things to Consider for AppealDepends on type of denial…Is the denial technical? Medical
necessity denial?
Do you agree with the denial reason?
Is there additional and/or clarifying documentation that you could submit that would support your claim?
Are there other items that may influence the decision that were not considered?
Amount of the denial vs. resources required to appeal.
3636

9/26/2019
19
Defending Adverse Audit Findings:Tips to Respond
Follow your policy/process for government audit response
– Refer back to “not all contractors are created equal”
Conduct internal comprehensive review
– Know and understand the issues identified
Determine what internal & external resources needed
– Evaluate what clinical and legal expertise may be needed to defend the audit findings
– Evaluate defenses to the use of statistical sampling or the methodology used (if applicable)
37
60-DAY OVERPAYMENT RULE IMPLICATIONS
38

9/26/2019
20
60-Day Overpayment Rule
March 23, 2010: Enactment of the Affordable Care Act (ACA)
Section 6402(a) of the ACA (now codified at 42 U.S.C. § 1320a-7k(d)):
– A person who has received an overpayment must report and return the overpayment within either 60 days after the date on which the overpayment was identified or on the date any corresponding cost report is due, whichever is later
– The term “overpayment” means any Medicare or Medicaid funds that a person receives or retains to which the person, after applicable reconciliation, is not entitled
Failure to report and return an overpayment can result in False Claims Act and Civil Monetary Penalties liability, as well as exclusion
from participation in federal health care programs39
60-Day Overpayment Rule
Medicare Parts A /B: Regulatory definition in 42 C.F.R. § 401.305(a)(2)
– An overpayment is identified “when the person has, or should have through the exercise of reasonable diligence, determined that the person has received an overpayment and quantified the amount of the overpayment”
42 C.F.R. § 401.305(a)(2)’s definition of “identification” incorporates concept of “reasonable diligence”
In its Final Rule, CMS stated that reasonable diligence includes both proactive compliance activities and reactive investigative activities
– Providers have an affirmative duty to investigate potential overpayments
40

9/26/2019
21
Implications for 60-Day Overpayment Rule (cont.)
CMS has stated that it believes that “contractor overpayment determinations are always a credible source of information for other potential overpayments” and that “in certain cases, the conduct that serves as the basis for the contractor identified overpayment may be nearly identical to conduct in some additional time period not covered by the contractor audit”
Consider implications of contractor findings and/or agreeing with contractor findings and whether this triggers a duty to investigate other similar claims for overpayment.
41
Key Performance Indicators
Tips for Responding to Government Review & Audit
Sample Appeal Responses
Regulatory References
Helpful Website Links
42
RESOURCES
42

9/26/2019
22
Key Performance Indicators (KPI)
Case Mix Visit Utilization by Discipline Patients by Diagnosis Patient Outcomes Patient Experience Scores Productivity Average LOS Recertification Rate LUPA % Admissions/Discharges Days to RAP/Final Claim Accounts Receivable/Write-Offs Unbilled Claims Referral Data (Conversion Ratio/NTUCs) Compliance Audit Scores
Average & Median Length of Stay Average Daily Census Visits Per Day Patients by Diagnosis Patient Experience Scores Quality Measures/QAPI Staffing Ratios Days by Level of Care Live Discharges/Revocations/Deaths Revenue by Level of Care Cost per Day/Visit Accounts Receivable/Write-Offs Unbilled Claims Referral Data (Conversion Ratio/NTUCs) Compliance Audit Scores
KPI help highlight agency strengths and potential areas for improvement
HOME HEALTH HOSPICE
43
Preparing for Initial ADR/TPE Submission
• Organizing the Record
Respond to only what was asked for - put in order:
o Attach the ADR; Cover Letter (optional) Plan of Care/Certification of Eligibility; MD Interim Orders; OASIS Assessment; OASIS Submission; Visit Notes; selective supporting documentation (i.e. Signature Log if applicable)
Keep exact copy of what was sent & paginate
MACs Accept: Fax, Mail or Electronic- MAC preference
Allow time for record to be received
o If mailing get confirmation from FISS when received SB60001 changes to S50MR
DO NOT: Bind together, highlight records, attach sticky notes, change or alter records, copy 1 page as pdf file
Source: Medicare University
4444

9/26/2019
23
SAMPLE:
TPE/ADR Response
4545
SAMPLE Appeal Response:
Missing Date in Cert Statement Defense: MD did in fact “certify” a F2F was done timely AND the Encounter Note was dated & signed by qualifying practitioner according to regulations.
4646

9/26/2019
24
SAMPLE: Request for Redetermination
47
Medical Necessity 5-7 Visits Denial
47
SAMPLE: Request for Redetermination (cont.)
48
• Medical Necessity 5-7 Visits Denial
48
9/26/2019
25
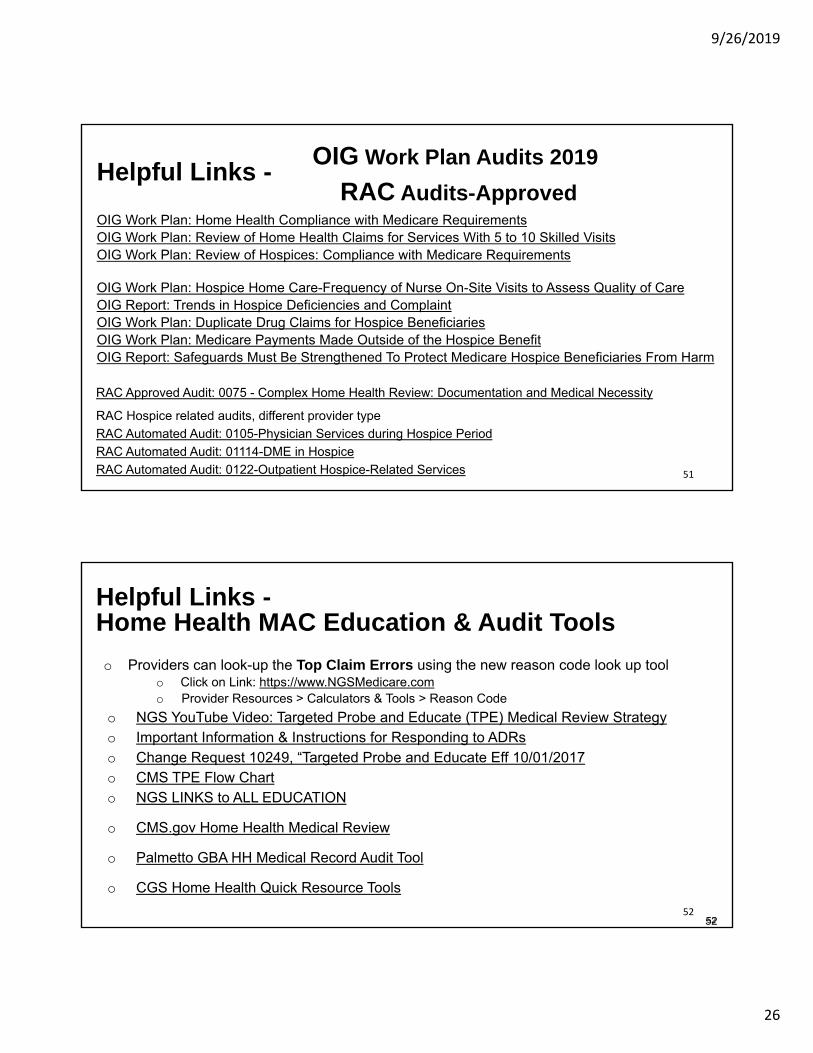
Regulation to support Medical Necessity
4949
→ Look for any documentation in the patient’s record that refers to instability or complication requiring skilled assessment , observation &/or teaching
→ Use this regulation to support
CMS Final Rule – Certifying PhysicianSupporting Regulation: Physician Communication Now Permissible
5050
9/26/2019
26
Helpful Links -
OIG Work Plan: Home Health Compliance with Medicare RequirementsOIG Work Plan: Review of Home Health Claims for Services With 5 to 10 Skilled VisitsOIG Work Plan: Review of Hospices: Compliance with Medicare Requirements
OIG Work Plan: Hospice Home Care-Frequency of Nurse On-Site Visits to Assess Quality of CareOIG Report: Trends in Hospice Deficiencies and ComplaintOIG Work Plan: Duplicate Drug Claims for Hospice BeneficiariesOIG Work Plan: Medicare Payments Made Outside of the Hospice BenefitOIG Report: Safeguards Must Be Strengthened To Protect Medicare Hospice Beneficiaries From Harm
RAC Approved Audit: 0075 - Complex Home Health Review: Documentation and Medical Necessity
RAC Hospice related audits, different provider type
RAC Automated Audit: 0105-Physician Services during Hospice Period
RAC Automated Audit: 01114-DME in Hospice
RAC Automated Audit: 0122-Outpatient Hospice-Related Services
OIG Work Plan Audits 2019
RAC Audits-Approved
51
Helpful Links -
o Providers can look-up the Top Claim Errors using the new reason code look up toolo Click on Link: https://www.NGSMedicare.como Provider Resources > Calculators & Tools > Reason Code
o NGS YouTube Video: Targeted Probe and Educate (TPE) Medical Review Strategy o Important Information & Instructions for Responding to ADRso Change Request 10249, “Targeted Probe and Educate Eff 10/01/2017o CMS TPE Flow Charto NGS LINKS to ALL EDUCATION
o CMS.gov Home Health Medical Review
o Palmetto GBA HH Medical Record Audit Tool
o CGS Home Health Quick Resource Tools
5252
Home Health MAC Education & Audit Tools
52
9/26/2019
27
Helpful Links -
• Pre-Claim Internal Audit
– Use the Palmetto GBA checklist to ensure PCR request is complete
RCD Pre-Claim Review Initial Episode Checklist
RCD Pre-Claim Review Subsequent Episode Checklist
– Modify audit tool to focus on technical requirements for pre-claim review – non-clinical
• Additional Resources:
– RCD Frequently Asked Questions (FAQs); updated 6/14/2019
RCD for Home Health FAQs
– CMS RCD Operations Guide updated May 9, 2019
RCD Operations Guide
Pre-Claim Review
53
Helpful Links -
o CMS.gov Hospice Toolkit
o Palmetto GBA Hospice Documentation Audit Tool
o CGS Hospice Quick Resource Tools
o CGS Hospice Documentation Checklist Tool
o CMS Comprehensive Hospice Clinical Record Review Tool
o NGS Hospice Documentation Tips
o CMS Update on Physician Signature Requirement and Face-to-Face Encounter Requirements
o CMS.gov Local Coverage Determinations (LCD) by State Index
5454
HOSPICE MAC Education & Audit Tools
54

9/26/2019
28
Thank You for Listening
Contact Information
Stephanie Johnson, JDKing & Spalding, LLP
Robin Seidman, RN, MSN, MBA, LNCC, HCS-D
Documentation Compliance Solutions, LLC
56
















