1 Tara Greenhow, M.D. Kaiser Permanente San Francisco April 27 th , 2011 10 year old Filipino male presented to his pediatrician on 12/10/10 with 2 weeks of persistent nonproductive cough Over the next month, the cough persisted Seen by PMD 1/12/11 with persistent cough and 10lb weight loss 1/21/11 Continued with cough and fatigue ‒ On exam: afebrile RR 20. Wt 43kg. Lungs: coarse. No palpable adenopathy ‒ CXR unchanged LUL pneumonia, cannot rule out mediastinal mass
Transcript
1
Tara Greenhow, M.D. Kaiser Permanente San Francisco
April 27th, 2011
10 year old Filipino male presented to his pediatrician on 12/10/10 with 2 weeks of persistent nonproductive cough
Over the next month, the cough persisted
Seen by PMD 1/12/11 with persistent cough and 10lb weight loss
1/21/11 Continued with cough and fatigue ‒ On exam: afebrile RR 20. Wt 43kg. Lungs: coarse. No palpable adenopathy
‒ CXR unchanged LUL pneumonia, cannot rule out mediastinal mass
2
Nodal mass in the left hilum, which is contiguous with the heterogeneous mass 4.5 x 3.3 cm
Left upper lobe masslike density, measuring 3.4 x 2.7 cm likely due to atelectasis
Diffuse small reticulonodular opacities throughout the left and right lung, ranging between 2 and 5 mm
10/31/10 mid 11/10 1/12/11 1/21 2/6 2/22 3/16
Cough begins
Diagnosis of coccidioidomyosis. Therapy started. Titer 1:4096
First visit to Antioch
Titer 1:1024. Repeat CXR
Repeat CXR
Cough continues. CXR LUL pna
Repeat CXR and chest CT
3
Coccidioides immitis and C. posadasii cause coccidioidomycosis (San Joaquin valley fever) ‒ The two species show little or no phenotypic, antigenic, virulence, or morphologic differences
‒ C. immitis is found in California ‒ C. posadasii is found in Mexico and areas of Central and South America
Should a patient with active pulmonary coccidioidomycosis be placed in isolation because this is routinely contagious person-to-person? 1. YES 2. NO
Maricopa County DPH
4
Coccidioidomycosis occurs in hot, arid regions of the southwestern United States and is endemic to southern California, Arizona, western and southern Texas, and New Mexico
Infection also occurs in regions of Mexico and Central and South America Environments with hot summers, infrequent winter freezes, alkaline soil, and
alternating periods of rain and drought support fungal growth and aerosolization of arthroconidia
Centers for Disease Control and Prevention. Summary of notifiable diseases – United States, 2003. Morbid Mortal Wkly Rep MMWR 2006;53:45
Coccidioidomycosis cases fluctuate from year to year More than 4,000 cases were reported in California last year, up from
2,488 in 2009 ‒ Counties in the San Joaquin Valley reported increases
• In Fresno County, there were 727 cases in 2010, compared with 518 in 2009. • In Kern County, the state hot spot for Valley fever, more than 2,000 cases were
reported in 2010, up significantly from the 595 cases reported in 2009 Since summer 2010, Children's Hospital Central California has had
about 15 children admitted for Valley fever Last cocci spike in 2006, when the state reported more than 3,000
cases Possible causes
‒ Weather pattern -- heavy spring rains followed by a hot, dry summer and fall wind gusts
Beginning 1/1/11, coccidioidomycosis became a reportable disease
Fresno Bee 2/20/11 Barbara Anderson
Of those infected with coccidioidomycosis, this percentage has mild or asymptomatic, primary pulmonary infections 1. None, all have symptoms 2. 5-10% 3. 25-50% 4. 95% 5. 100%
5
Asymptomatic or mild in 95% of cases ‒ Subclinical in about 60% of infected people ‒ Most others have self-limited, primary pulmonary infections
Also causes life-threatening infections in immunocompetent and immunocompromised hosts ‒ Pulmonary complications occur in less than 5% ‒ Disseminated infections in < 1% of infected people
Pulmonary complications and extrapulmonary infections can occur without recognized antecedent illness
RISK FACTORS FOR DISSEMINATION 1. Primary or acquired cellular immune dysfunction 2. Extremes of age 3. Male gender 4. Filipino, African American, Native American,
Hispanic ethnicity 5. Pregnancy 6. All of the above
Clinical manifestations of dissemination to extrapulmonary sites occur in about 1% of patients ‒ Usually within several months of the primary pulmonary infection ‒ Rarely after 1 year
Persistent fever is common and frequently affected sites include the lungs, skin, bones, joints, and central nervous system
RISK FACTORS FOR DISSEMINATION ‒ Primary or acquired cellular immune dysfunction (including people receiving tumor
necrosis factor-alpha antagonists) ‒ Neonates, infants, and the elderly ‒ Male (adult) ‒ Filipino, African American, Native American, Hispanic ethnicity ‒ Skin test anergy ‒ Pregnancy ‒ Standardized complement fixation antibody titer ≥1:32 or increasing titer with persistent
symptoms
6
Lytic lesions of the right iliac bone, left sacral wing, and right proximal tibial metaphysis, consistent with systemic coccidioidomycosis
Amphotericin B is generally reserved for initial management of patients with ‒ Respiratory failure ‒ Rapidly progressive disease ‒ Women during pregnancy since the azole agents have the potential
for teratogenicity Ketoconazole, fluconazole, and itraconazole are the principal
agents used for treatment ‒ Most trials with the azole agents have been conducted in open-
label, nonrandomized, multicenter studies in adults and have differed in design and follow-up
‒ A comparative study of the azole agents has also been reported ‒ Recommendations for children are derived from published
experience in adults
Previously healthy 3 year old girl admitted to Kaiser Oakland with Henoch-Schönlein purpura
Hospitalization uneventful and discharged home
2 months later, with mild cough and rhinorrhea. No fevers
Unfortunately, during hospitalization shared room with another child with active, pulmonary TB
7
Baseline TST 0mm. Baseline CXR normal TST 2 months after exposure 20mm CXR with hilar adenopathy and RML infiltrate
Admitted to Kaiser SFO Am gastric aspirates x 3 performed AFB stain (-) x 3 Started on isoniazid, rifampin, pyrazinamide and vitamin B6 AFB cultures (-) Total course: 6 months (04/09-10/09) CXR below ‒ 4/09, 7/09, 11/09, 02/11
TB infects this proportion of the world’s population 1. 1/1000 2. 1/100 3. 1/10 4. 1/3 5. 1/2
8
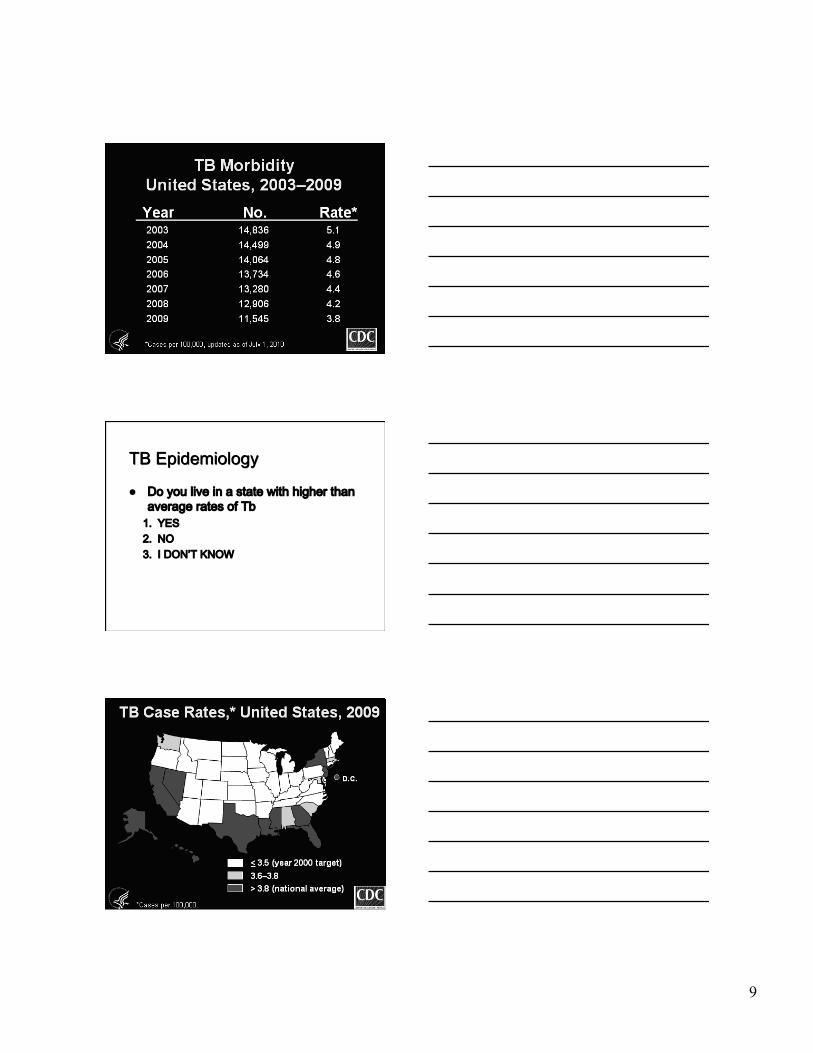
TB facts on the world’s TB problem: ‒ TB presents a larger problem in the world, particularly in developing countries where it accounts for > 1/4 of all preventable deaths
‒ 2,000,000,000 people are infected with the TB bacteria, 1/3 of the world’s population
‒ Someone in the world is newly infected with TB every second
WHO, Global Task Force, 2006 http://www.cdc.gov/tb/statistics/default.htm
‒ Each year • > 9 million people around the world become sick with TB • 2 million TB-related deaths worldwide.
‒ Each day • 20,000 people develop TB • 5,000 people die from it
‒ One person dies of TB every 10 seconds. ‒ TB is the single most opportunistic infection for people living
with HIV/AIDS, accounting for 13% of AIDS deaths worldwide
‒ TB causes more deaths among women than all causes of maternal mortality combined
WHO, Global Task Force, 2006 http://www.cdc.gov/tb/statistics/default.htm
9
Do you live in a state with higher than average rates of Tb 1. YES 2. NO 3. I DON’T KNOW
Marais BJ, et al. Int J Tuberc Lung Dis 2004 Cruz & Starke Ped Resp Rev 2007
Inhalation of TB into a terminal airway can result in a Ghon complex, comprising ‒ The initial focus of infection ‒ Draining lymphatic vessels ‒ Enlargement of regional lymph nodes
Four potential outcomes ‒ Containment (no disease) ‒ Primary parenchymal disease ‒ Progressive primary disease ‒ Reactivation disease
Marais BJ, et al. Int J Tuberc Lung Dis 2004 Cruz & Starke Ped Resp Rev 2007
12
Most children with TB commonly have these symptoms 1. Cough 2. Fever 3. Night sweats 4. Weight loss 5. All of the above
Clinical Feature Infants Children Adolescents Symptom Fever Common Uncommon Common Night sweats Rare Rare Uncommon Cough Common Common Common Productive cough Rare Rare Common Hemoptysis Never Rare Rare Dyspnea Common Rare Rare Sign Rales Common Uncommon Rare Wheezing Common Uncommon Uncommon Dullness to percussion Rare Rare Uncommon Decreased breath sounds Common Rare Uncommon
Cruz & Starke Ped Resp Rev 2007
Low burden of organisms ‒ 95% are AFB smear (-) ‒ 60-70% are AFB culture (-)
Diagnosis often difficult ‒ Gold standard is positive TB culture, or ‒ Clinical diagnosis: abnormal CXR, laboratory or physical
exam consistent with TB and 1 or more of the following • Tuberculin skin test (+) • Contagious source case identified • Clinical course consistent with TB • Response to TB therapy
Menzies, D et al. Ann Intern Med 2007; 146:340-54 Starke, JR PIDJ 2006 Nienhaus A, et al. PLoS ONE 2008
Whole blood test used to diagnose TB infection Blood mixed with TB peptides that stimulate WBC to release IFN
gamma if the patient is infected FDA approved
Courtesy of Cellestis
Nil Control"
Positive Control"
Infection"
Infection"
Courtesy of Oxford Immunotec
14
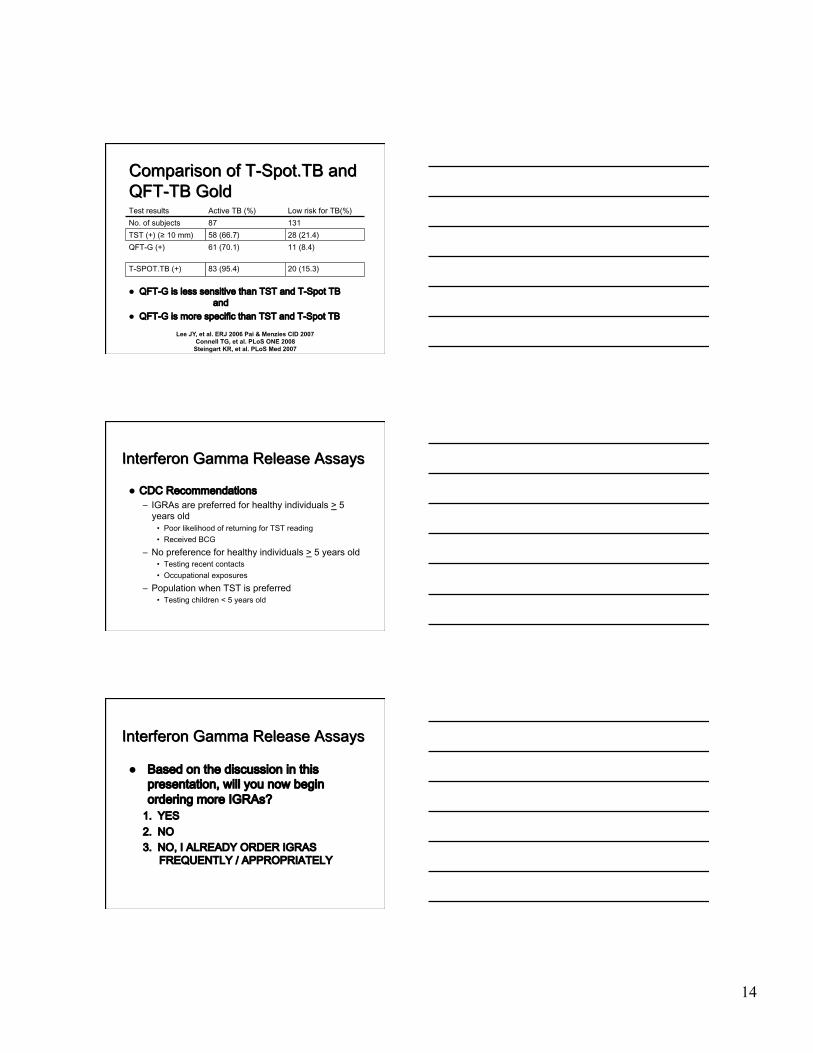
Test results Active TB (%) Low risk for TB(%) No. of subjects 87 131 TST (+) (≥ 10 mm) 58 (66.7) 28 (21.4) QFT-G (+) 61 (70.1) 11 (8.4)
T-SPOT.TB (+) 83 (95.4) 20 (15.3)
QFT-G is less sensitive than TST and T-Spot TB and
QFT-G is more specific than TST and T-Spot TB
Lee JY, et al. ERJ 2006 Pai & Menzies CID 2007 Connell TG, et al. PLoS ONE 2008
Steingart KR, et al. PLoS Med 2007
CDC Recommendations ‒ IGRAs are preferred for healthy individuals > 5 years old • Poor likelihood of returning for TST reading • Received BCG
‒ No preference for healthy individuals > 5 years old • Testing recent contacts • Occupational exposures
‒ Population when TST is preferred • Testing children < 5 years old
Based on the discussion in this presentation, will you now begin ordering more IGRAs? 1. YES 2. NO 3. NO, I ALREADY ORDER IGRAS
FREQUENTLY / APPROPRIATELY
15
Previously healthy 16 year old adm 2/26/11 with 5 days of ‒ Muscle ache ‒ Cough ‒ Fever ‒ Vomiting and diarrhea
In ED, ‒ Hypotensive 68/54 ‒ CXR with right middle lobe
infiltrate ‒ WBC 31 with 34 bands,
and lactate 3.17 CXR opacification of the mid to lower right lung
Admitted to the PICU 2/27 chest tube placed and fluid sent for culture. Culture negative
2/28 intrapleural fibrinolytic given per protocol
Fevers persisted, respiratory status unchanged / worsened and chest tube stopped draining
3/1 Chest CT ‒ Very large loculated right pleural effusion
‒ The anterolateral underperfused area contains air bubbles, pockets of aerated lung vs necrosis vs abscess
‒ Mild right pleural enhancement and thickening, suggesting infection of the loculated fluid
16
3/1 Taken to OR for video assisted thoracoscopy (VATs) ‒ Findings consistent with multiloculated empyema ‒ Intraoperative drainage of ̃500ml fluid ‒ Good lung compliance hopefully indicative of viable tissue
‒ Gram stain mod WBC, no organism no growth Hospitalized for 2 weeks on IV antibiotics Completed a 4 week course of antibiotics
• Since the introduction of PCV7 in 2000, invasive pneumococcal disease (IPD) has decreased in all age groups
• PCV7 provides protection from pneumonia • Since 2004, rates of pneumonia hospitalizations and clinic visits in children < 2 years old have decreased
Li, S.-T. T. et al. Pediatrics 2010;125:26-33 Kaplan, SL Sem PID 2006
• In children hospitalized with pneumococcal pneumonia, empyema is a complication in
1. 1/10 2. 1/5 3. 1/3 4. 1/2 5. 2/3
17
• In the US, pneumonia is the most common cause of hospitalization in children
• Empyema is associated with • 3% of pneumonia hospitalizations • 1/3 of pneumococcal pneumonia hospitalizations
Li, S.-T. T. et al. Pediatrics 2010;125:26-33 Kaplan, SL Sem PID 2006
• In Houston, CA-MRSA most common culture-proven cause of pleural empyema
Clinical findings no different compared to other organisms
Longer duration of hospital stay (18.8 days) compared to MSSA (14 days)
Increased association with concomitant respiratory virus
Li, S.-T. T. et al. Pediatrics 2010;125:26-33 Kaplan, SL Sem PID 2006
• In children rates of pulmonary empyema is 1. Increasing 2. Decreasing 3. Staying the same
18
Grijalva C G et al. Clin Infect Dis. 2010;50:805-813
Li, S.-T. T. et al. Pediatrics 2010;125:26-33
Grijalva C G et al. Clin Infect Dis. 2010;50:805-813
19
Grijalva C G et al. Clin Infect Dis. 2010;50:805-813
Grijalva C G et al. Clin Infect Dis. 2010;50:805-813
Grijalva C G et al. Clin Infect Dis. 2010;50:805-813
Presence of labored breathing, oxygen requirement and persistent fevers in the face of an effusion or empyema supports the decision to proceed with surgical drainage
Laboratory studies such as white blood count or blood cultures can complement a diagnosis but should not be used in isolation of the clinical picture
Fuller MK et al. Curr Op Ped. June 2007
Exudative ‒ Simple, uncomplicated effusion ‒ Layers clearly on CXR
Fibrinopurulent ‒ Fluid becomes infected leading to
• Thick exudate • Loculations
Organizational ‒ Pleural peel
• Restricts lung expansion • Impairs lung function • Persistent pleural space for infection
Fuller MK et al. Curr Op Ped. June 2007 Adapted from Kate Gregg, MD
Plain radiographs ‒ Initial study of choice ‒ Layering on decubitus films is indication of clinically significant
pleural effusion ‒ Pneumothorax, pneumatocele, consolidation, or air-fluid levels may
also be visualized ‒ Accuracy in detecting free fluid in adults is 67% sensitive and 70%
specific Ultrasound
‒ Useful in determining free-flowing fluid collections versus septated fluid collections
CT ‒ Provides detailed imaging of the pleural cavity ‒ Most useful when complete opacification of a lung field is seen on
plain radiograph
Fuller MK et al. Curr Op Ped. June 2007
21
Parenteral therapy • Ampicillin or • Ceftriaxone +/- • Clindamycin or • Vancomycin
Severe Infections ‒ Ceftriaxone + Vancomycin
The goals of surgical treatment ‒ Re-expand the lung ‒ Restore compliance ‒ Improve respiratory function ‒ Reduce morbidity and recurrence ‒ Prevent mortality, and ‒ Reduce the length of hospital stay
Previously healthy, Hispanic female, Fresno County Father had cough illness for several weeks Cough onset at age 5 weeks, one week prior to
admission Hospitalized in children’s hospital for one week
before transfer to PICU and intubation WBC 80,000; pulmonary HTN - single volume
exchange transfusion done Transferred to second children’s hospital PICU for
ECMO, but not done due to multiorgan failure
Courtesy of the Pennsylvania Chapter of the American Academy of Pediatrics
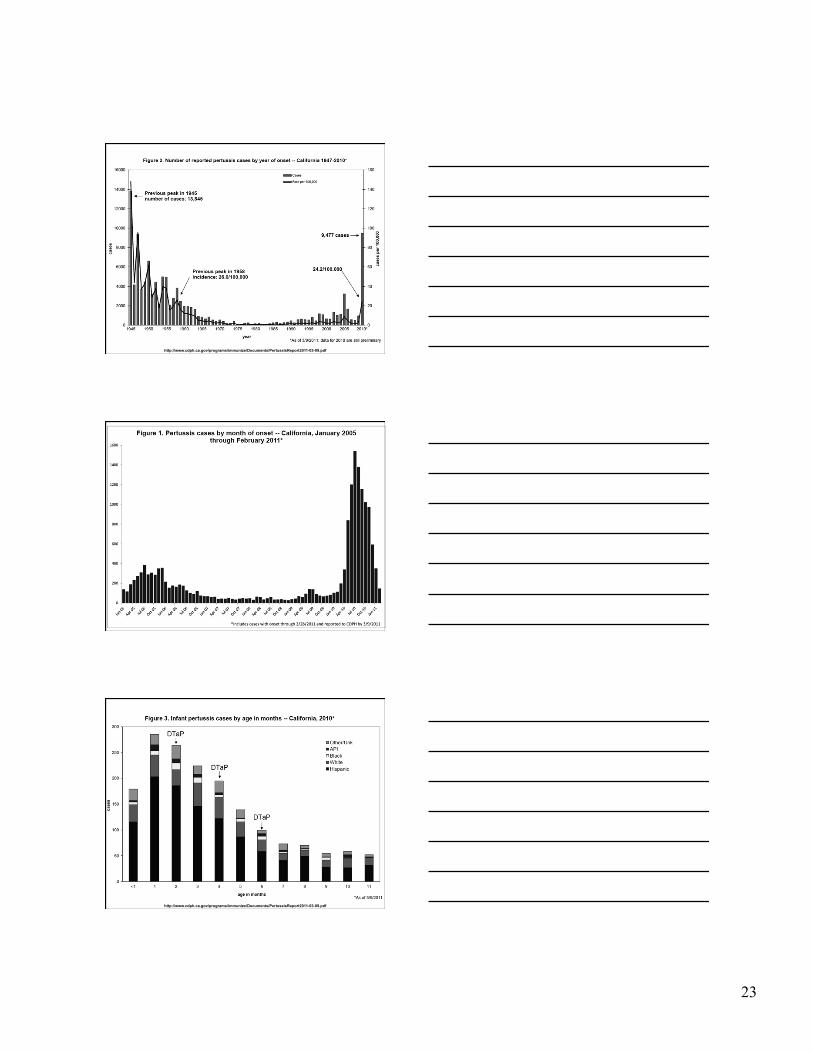
Pertussis remains the most poorly controlled vaccine preventable disease ‒ TRUE ‒ FALSE
Pertussis cases in 2010 in CA were ‒ Unchanged from previous years ‒ On par with previous peak years occurring every 2-5 years
‒ Highest seen in 65 years
Worldwide ‒ 50 million cases annually with 300,000 deaths
During the prevaccine era in US, leading cause of death from communicable disease in children < 14 years
Most poorly controlled vaccine-preventable disease ‒ Incidence increasing since the 1990s ‒ Cyclical: peaks every 2-5 years ‒ Until 2010, last peak year 2005 with 25,616 U.S. cases, a 45 year high