49
Asthma in our Community Tarig Ali-Dinar, MD Division of Pediatric Pulmonology & Sleep Medicine Nemours Children’s Hospital

Asthma in our Community
Tarig Ali-Dinar, MD
Division of Pediatric Pulmonology & Sleep Medicine
Nemours Children’s Hospital

Objectives
• Evaluate and Identify diagnostic and management approaches of pediatric asthma
• Review epidemiology of pediatric asthma in the state of Florida
• Identify asthma community resources in central Florida
• Provide resources for patients and families with further questions about children’s asthma and environmental health

Asthma
• Chronic disease of the airways that may cause• coughing• wheezing• breathlessness• chest tightness

Asthma Triggers
• Allergens ( pollen, mold, animal dander, dust mites, etc)
• Infections
• Exercise
• Tobacco smoke
• Air pollution
• Occupational hazards

Asthma PathophysiologyTrigger Factor
Cytokines and IgE
Airway smooth muscle
Immune cells
Airway Inflammation
Hypersecretion of mucus
Asthma
Swelling bronchial membranes
Airway narrowing

Asthma Pathophysiology
Diagnosis
• Lung function testing
• Exhaled nitric oxide
• Chest X-ray
• Arterial blood gas analysis
• Serum eosinophils
• Sputum eosinophils
• Serum IgE
• Skin testing

Stepwise Approach of Managing Asthma in Children

Treatment
• Short and long acting b agonist
• Anti cholinergic
• Inhaled corticosteroids
• Leukotrienes modifiers
• Systemic steroids
• Methylxanthines
• Anti IgE
• Immunotherapy

Novel Therapy –Clinical trial
Anti IL4 R: a dupilumabAnti IL 13: lebikizumab
Tralokinumab
Anti IL5:Mepolizumab ReslizumabBenralizumab
Pelaia G et al, Therapeutic and Clinical Risk Management 2016J.Carlos et al. Expert Opin Biol Therrapy 2015
Expert opinion—Reslizumab and other anti-IL5 therapies have seen success targeting eosinophilic inflammation

Managing Asthma: Asthma Management Goals
Control of symptomsAchieve
Normal activity levelsMaintain
Asthma exacerbationsPrevent
Adverse effects from asthma medicationsAvoid
Asthma mortality Prevent

Is asthma really a problem?

1 in 12Children
has asthma

One in 12 people (about 26 million, of the U.S. population) had asthma in 2015 CDC

• About 6 million children reported with asthma
• More than half of all children with asthma had one or more attacks
• One in six children with asthma visits the ED
• One in twenty children with asthma hospitalized
Attacks have gone down in children of all races and ethnicities from 2001 through 2016
Asthma Prevalence, 2016

Asthma Prevalence: Florida

Hospitalization: Florida

A Public Health Response to Asthma
Asthma needs government and non-government agencies to partner in reducing its public health burden

History Of Florida Asthma Coalition
Established in 2009
Vision
Floridians with asthma will achieve optimal health and quality of life
Mission
To reduce the overall burden of asthma, with a focus on minimizing the disproportionate impact of asthma in racial/ethnic and low-income populations, by promoting asthma awareness and disease prevention at the community level and expanding and improving the quality of asthma education, management, and services through system and policy changes

Florida State Asthma Plan
Goal
Reduce asthma morbidity
Long term objective
Strengthen the collective capacity in Florida to lessen the burden of asthma and improve the quality of life for Floridians living with asthma, increase the provision and quality of comprehensive asthma control services, and reduce disparities in asthma care and health outcomes

Florida State Asthma Plan 2015-2019
Recognize organizations for implementing best practice for asthma care
Objectives to increase the number of :
1) Schools recognized from 16 to 30
2) Health plans from 0 to 5
3) Hospitals from 0 to 3
4) Primary care providers from 0 to 10
5) Pharmacies from 0 to 3

DOING
THE
RIGHT
THINGS
RIGHT
A Public Health Response to Asthma

KNOWLEDGE
PRACTICE

National Asthma Education and Prevention Program (NAEPP)
• Expert Panels to prepare guidelines (EPR-3) for the diagnosis and management of asthma
• The Guidelines include recommendations for Home-Based Interventions including asthma education for caregivers and allergen-control
• EPR that multifaceted allergen (cockroach, rodent, and dust mite education and control interventions in the home setting to be considered for asthma patients sensitive to those allergens

The Florida Department of Health and the FAC Home Visit Model
Individualized needs assessments/case management by: two staff members
• Respiratory Therapist • Certified Asthma Educator • Environmental Specialist • Community Health Worker • School Nurse

Home Visit Model
• One staff member to conduct an environmental assessment and interventions
• The other member to facilitate:
• Asthma self management education and focusing on asthma good control barriers
• Asthma control training for caregivers
• A minimum of three home visits
• Care coordination with asthma specialists and school nurses
• Advocacy and connection to resources

Home visits
• Asthma education for caregivers
• Allergen-control
• Toxic stress measures

Asthma Education for Caregivers
• Teach and reinforce at every opportunity: • Basic facts about asthma
• Roles of medications: Controller vs. Quick-relief medications
• Patient Skills (NIH/ EPR-3): Allergic & non-allergic trigger management: • Understand the need for allergy testing to determine sensitivity to indoor
allergens and to focus on exposure reduction

Allergens and Irritants Control
Allergens • House dust mites
• Animal dander
• Molds
• Pollen
• Cockroach droppings
Irritants• Tobacco smoke
• Air pollution
• Smoke from burning wood or grass
• Strong odors or fumes

Home Visit Resources and Supplies
• Allergy testing
• Asthma action plan
• Asthma basics—ALA resources available online
• Asthma control test (ACT)
• Asthma home environment checklist (EPA)
• Cleaning supplies
• Mattress/pillow casings
• Indoor air quality testing
• Patient health questionnaire (PHQ9)
• Pediatric symptom checklist
• Generalized anxiety disorder (GAD7)
• Adverse child events survey (ACE)
• Peak flow meter
• Pest control
• Spacers for inhalers
• Spirometer


Toxic Stress in Children
• Toxic stress involves exposure to stressful and adverse experiences over a long period of time
• Children are especially vulnerable to the effects of toxic stress
• Long term consequences of toxic stress
(Anxiety, Asthma, Cancer, Depression, Back Pain, Headaches,
Heart diseases, Weakened immune system, etc..)

Toxic Stress in Children
• Addiction to drugs/alcohol (family member)
• Divorce/separation
• Death of a loved one
• Exposure to domestic violence
• Extreme poverty
• Incarceration of parent or family member
• Neighborhood violence
• Mental Illness (family member)
• Neglect

Toxic Stress Screening Tools
• Children aged 5-11 • Patient health questionnaire (PHQ-9) • Pediatric symptom checklist • Adverse child events survey (ACE)
• Youth aged 12 and older • Patient health questionnaire modified for adolescents (PHQ-A) • Pediatric symptom checklist youth self-report (PSC-Y) • Pediatric symptom checklist • Adverse child events survey (ACE)
• Referrals to behavioral health care should be made if the screening results indicate the individual is at risk

Results of a Home-Based Environmental Intervention among Urban Children with Asthma
Methods:
Seven sites
N: 937 children with atopic asthma
Age (5 -11 years)
Trial of an environmental intervention that lasted one year :
• Education and remediation for exposure to both allergens and tobacco
• Home environmental exposures
• Asthma-related complications
Morgan W et al, NEJM 2004

Results of a Home-Based Environmental Intervention among Urban Children with Asthma
Results: 1 year follow up• Fewer days with symptoms • Declines in the levels of allergens at home• Decreased dust mites and cockroach significantly correlated with reduced
complications of asthma
Conclusions:
Among inner-city children with atopic asthma, an individualized, home-based, comprehensive environmental intervention decreases exposure to indoor allergens, including cockroach and dust-mite allergens, resulting in reduced asthma-associated morbidity
Morgan W et al, NEJM 2004

Home-based Educational Interventions for Children with Asthma
Conclusions
• Inconsistent evidence for home-based asthma educational interventions compared to standard care Education delivered outside of the home or a less intensive educational intervention delivered at home
• Education remains a key component of managing asthma in children (advocated in numerous guidelines)
• This review does not contribute further information on the fundamental content and optimum setting for such educational interventions
Welsh EJ, Hasan M, Cochrane Database 2011

Methods:
N: 283 children (urban, low income)
Logs of ED visits or hospitalizations ( 4 zip codes)
Offered enhanced care including nurse case management and home visits
Parent-completed interviews at enrollment, and at 6- and 12-month contacts
Hospital costs of the program were compared with the hospital costs of a
neighboring community with similar demographics
Wood ER et al, Pediatrics 2012
Community Asthma Initiative: Evaluation of a Quality Improvement Program for Comprehensive Asthma Care

Community Asthma Initiative: Evaluation of a Quality Improvement Program for Comprehensive Asthma Care
Results: 1 yearDecrease in
• (≥1) asthma ED visits (68.0%)• Hospitalizations (84.8%)• Days of limitation of physical activity (42.6%)• Missed school (41.0%), and parent missed work (49.7%)
Significant reduction in hospital costs compared with the comparison community and a return on investmentConclusions:
The program showed improved health outcomes and cost-effectiveness and generated information to guide advocacy efforts to finance comprehensive asthma care
Wood ER et al, Pediatrics 2012

Boston Children’s Hospital Community Asthma Initiative:Five-year Cost Analyses of a Home Visiting Program
Methods:
n: 268 patients enrolled in the CAI program• 818 patients from a similar cohort in neighboring ZIP codes without CAI
• 33 months
• Examine cost changes and calculate an adjusted ROI over a 5-year post-intervention period
Results:
CAI patients had a cost reduction greater than the comparison group of $1,216 in Year 1 (P = 0.001), $1,320 in Year 2 (P < 0.001), $1,132 (P = 0.002) in Year 3, $1,123 (P = 0.004) in Year 4, and $997 (P = 0.022) in Year 5
Bhaumik et al, Journal of Asthma 2017

Boston Children’s Hospital Community Asthma Initiative: Five-year Cost Analyses of a Home Visiting Program
Conclusions:
Community-based, multidisciplinary, coordinated disease management programs can decrease the incidence of costly hospitalizations and ED visits from asthma. Analysis supports the business case for the provision of community-based asthma services as part of patient-centered medical homes and Accountable Care Organizations
Bhaumik et al, Journal of Asthma 2017
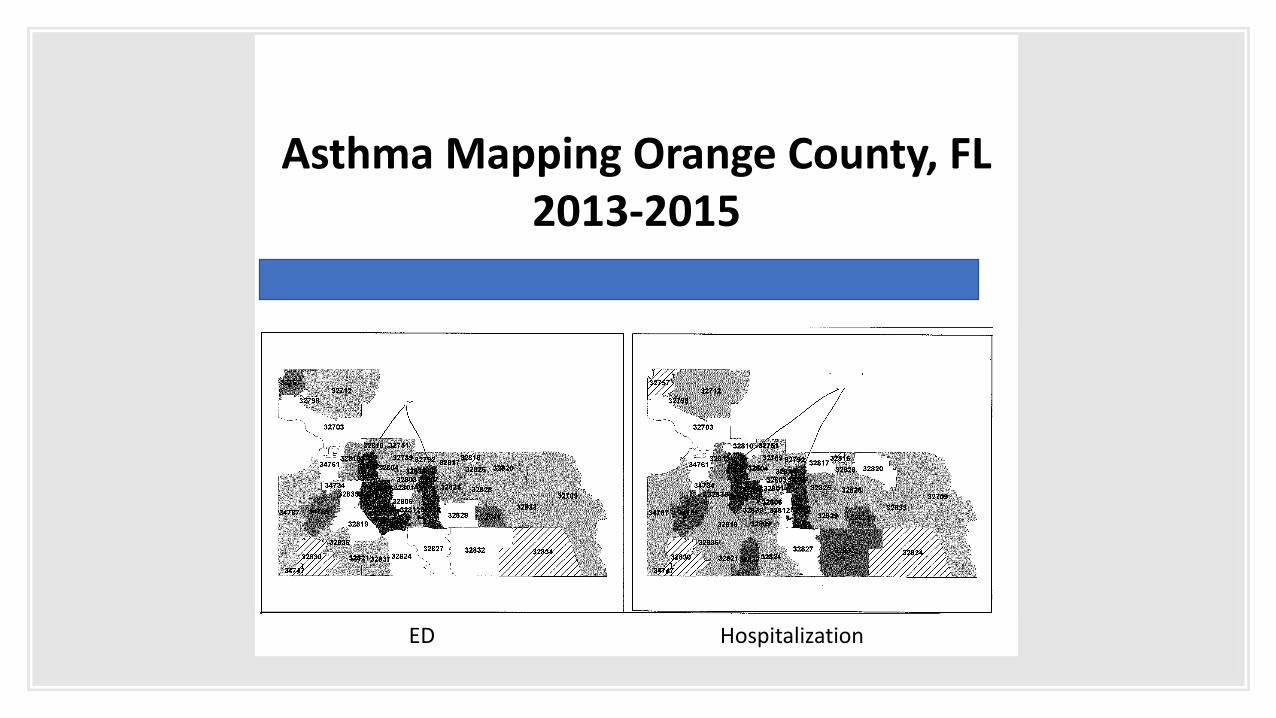
Asthma Mapping Orange County, FL2013-2015
ED Hospitalization

Orange County Hospitalization


Home Visit Steps
• Step 1
• Referral to the department of health
• Step 2
• First Home visit conducted
• Asthma knowledge assessment completed
• Asthma indoor environment and assessment completed
• Receive asthma friendly cleaning products
• Step 3
• Second home visit
• Asthma individual education plan completed
• Asthma education and indoor environment
• Receive asthma friendly pillowcase and bedcover

Home Visit Steps
• Step 4• Third home visit
• Asthma knowledge assessment completed• Asthma indoor environment assessment completed ( exit)• Self administration of asthma medication
• Receive asthma friendly AC filters
• Step 5• Follow up courtesy call from department of health (3 months after last visit)
• Step 6• Final call 6 months after last home visit• Follow up visit to referring provider

State of Tobacco Control 2018:Who's at greatest risk for tobacco-related death and disease?
Did Florida make the grade?

Tobacco Prevention
and Cessation Funding
Smoke free Air
F
Tobacco Taxes
Access to cessation services
Tobacco21
F B F D
Effects of Second-Hand Smoke
• Tobacco smoke is one of the most common asthma triggers
• About 1.6 million Floridians with asthma at risk for an attack
• Secondhand smoke contains hundreds of toxic and carcinogenic chemicals
• Referrals

















