50
| Date post: | 03-Jun-2018 |
| Category: |
Documents |
| Upload: | juanitocabatanalimiii |
| View: | 219 times |
| Download: | 0 times |
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 1/50
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 2/50
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 3/50
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 4/50
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 5/50
Traumatic Brain Injury
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 6/50
Definition
Traumatic Brain Injury (TBI)
Any head injury with evidence of brain
involvement.
This term is preferred because it clearly
denotes that injury to the brain is the major
cause of morbidity and mortality and that
injury is caused by external forces.

8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 7/50
Other terms
Craniocerebral trauma
Head injury / head trauma
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 8/50
TBI is one subset of Acquired Brain
Injuries (ABI)
ABI are any injury to the brain acquired after
birth.
The other subset is Non-traumatic Brain
Injury.
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 9/50
Classification
As to severity:
Mild GCS 13-15
Loss of consciousness < 20 min No TBI related abnormalities on neurological
examination and normal CT of the brain If positive, classify patient as moderate TBI or mild TBI
with complications
Moderate GCS 9-12
Severe
GCS 3-8
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 10/50
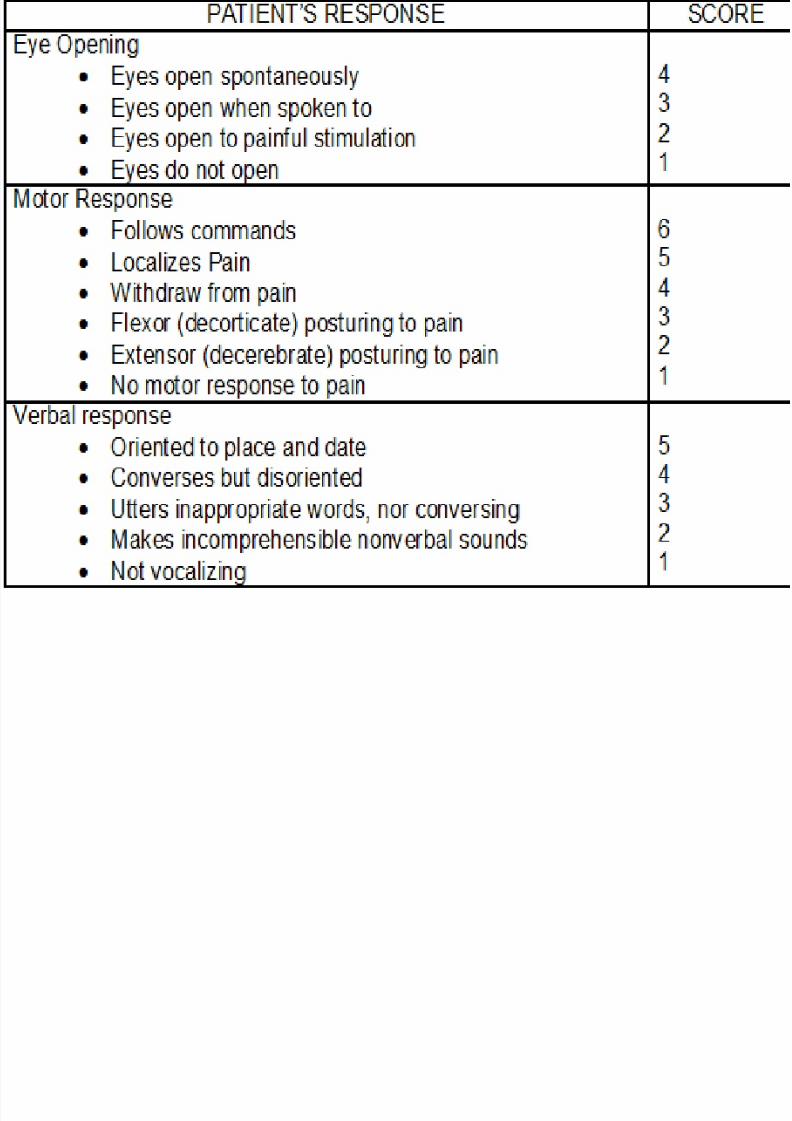
Glasgow Coma Scale (GCS)
Consists of:
Eye Opening (E)
Best Motor Response (M)
Verbal Response (V)
GCS=E+M+V
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 11/50
Glasgow Coma Scale (GCS)
Eye Opening (E)
(4) Spontaneous
(3) To loud voice
(2) To pain
(1) Nil
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 12/50
Glasgow Coma Scale (GCS)
Best Motor Response (M)
(6) Obeys
(5) Localizes
(4) Withdraws (flexion)
(3) Abnormal flexion posturing
(2) Extension posturing (1) Nil
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 13/50
Glasgow Coma Scale (GCS)
Verbal Response (V)
(5) Oriented
(4) Confused, disoriented
(3) Inappropriate words
(2) Incomprehensible sounds
(1) Nil
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 14/50

8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 15/50
As to Primary Injury
Closed
Open
Piercing
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 16/50
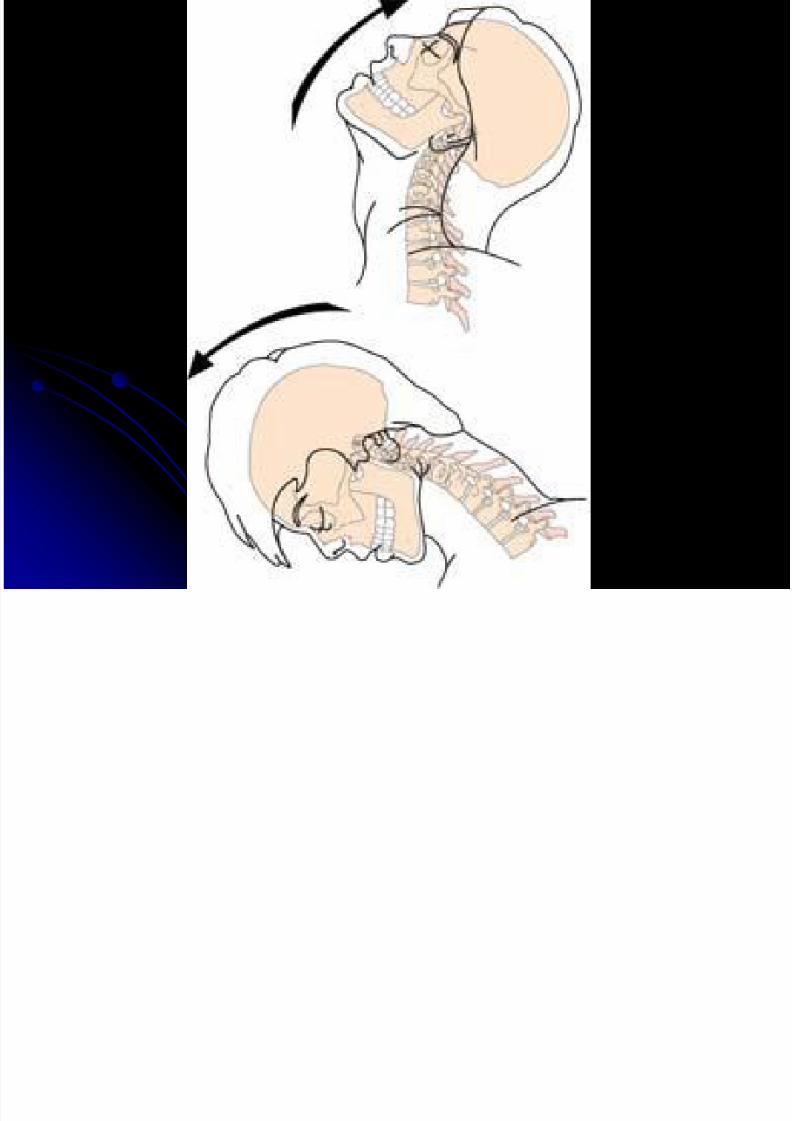
As to Primary Injury
Closed
Concussion
Contusion
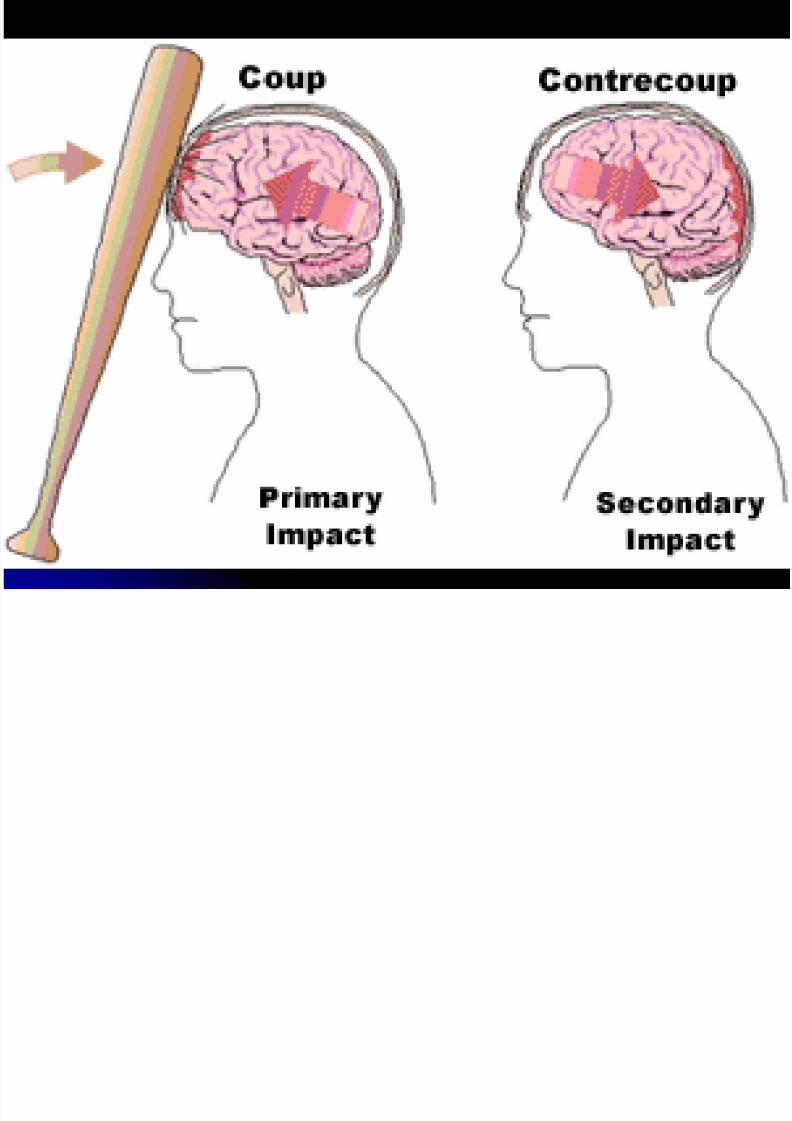
Local brain damage
Coup-contrecoup injury
Polar brain damage
Diffuse axonal injury
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 17/50
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 18/50
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 19/50
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 20/50
As to Primary Injury
Open
Piercing
Stab
Missile
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 21/50
As to Secondary Injury
Hypoxic-Ischemic Injury (HII)
Late-occurring Intracranial Hematomas
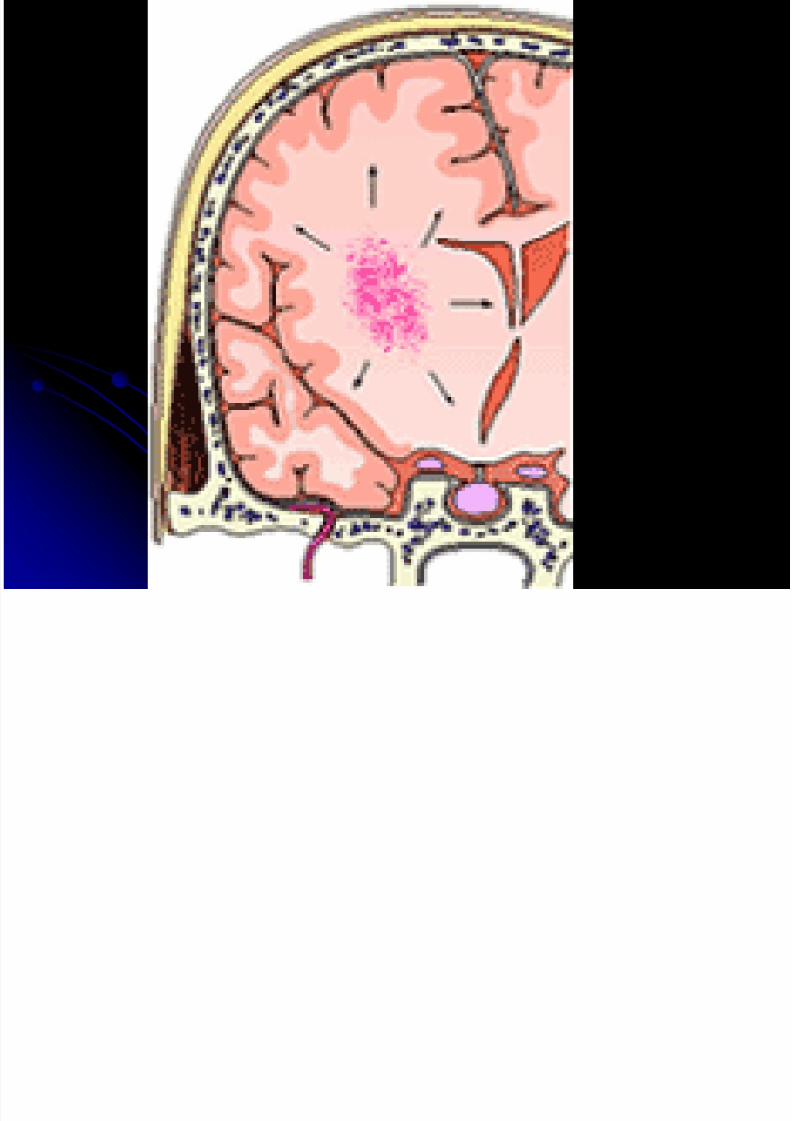
Increased Intracranial Pressure (ICP)
Intracranial Infection
Cerebral Artery Vasospasm
Tumors
Obstructive Hydrocephalus
Post-traumatic Epilepsy
Neurochemical Changes
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 22/50

8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 23/50
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 24/50
Types as to Affectation:
Focal
Diffuse
Types as to Trauma Velocity:
High-velocity impact
Low-velocity impact
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 25/50
Epidemiology
Worldwide (1996 data):
Of all types of injury, those to the brain are
among the most likely to result in death or
permanent disability. The leading cause of death and disability.
Traumatic brain injury is the leading cause of
seizure disorders. Closed head injury with or without skull
fracture constitutes the majority of cases.
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 26/50
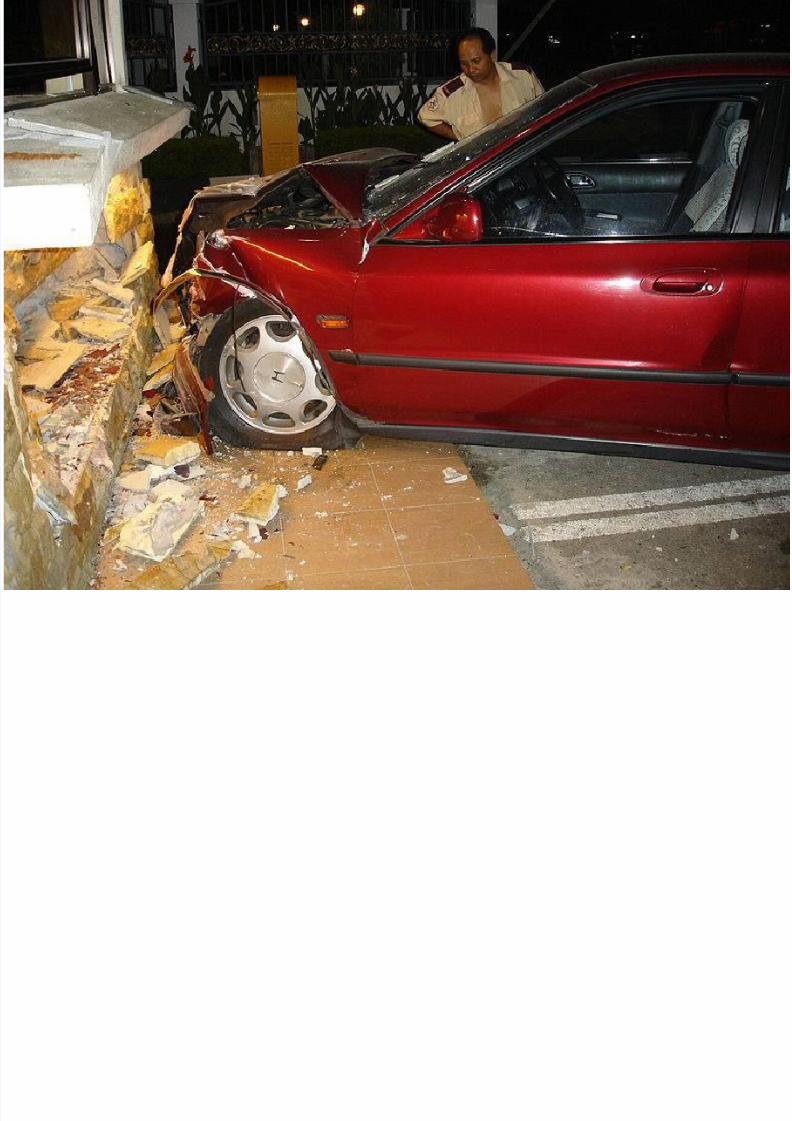
Etiology
Motor Vehicle Accidents (MVA) – 50%
Falls – 21%
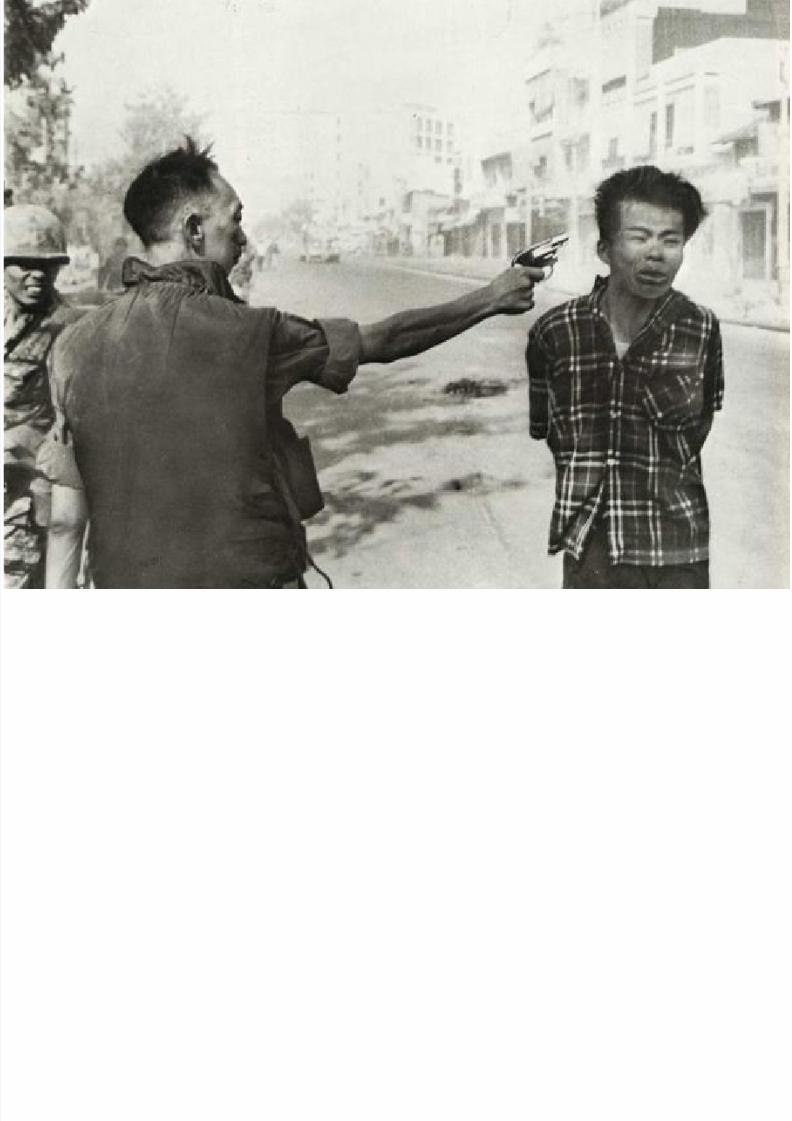
Violence, Assaults, Gunshot wounds – 12%
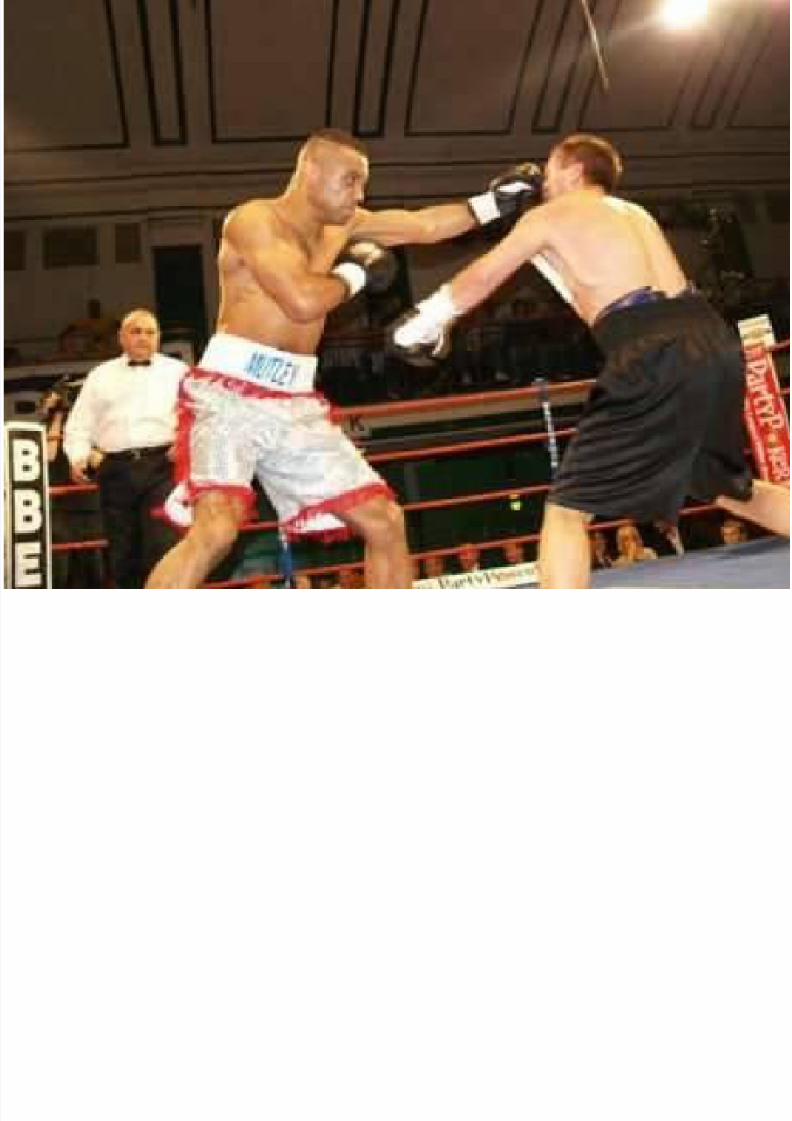
Sports, athletic events – 10%

8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 27/50
Pathophysiology/Pathomechanics
Pathomechanics
Types as to Primary Injury
Pathophysiology
Types as to Secondary Injury

8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 28/50
Clinical Manifestation
Signs/Symptoms:
Loss of consciousness
Signs of increased ICP
Brainstem damage
Localizing symptoms

8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 29/50
Direct Impairments
Cognitive
Neuromuscular
Visual – Perceptual
Swallowing
Behavioral
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 30/50
Nature of Residual Disabilities:
Permanent neuromuscular deficit
Seizures
Cognitive and behavioral problems
Resolution of neurologic signs may
continue as long as 3 years post-trauma.

8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 31/50
Complications
Sequelae of Head Injuries
Secondary injuries
Infection – meningitis, abscess
Extradural infection
Meningitis
Brain abscess
Focal cerebral lesions
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 32/50
Indirect Impairments
Contractures
Mobility deficits
Skin breakdown
Heterotopic ossification
Decreased endurance
Infection
Pneumonia
Impaired speech (if with tracheostomy)
DVT
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 33/50
Diagnosis
CT Scan
MRI
Positron emission tomography (PET)scan
Standard EMG/NCV
Electroencephalograms (EEG) andEvoked Potentials
Clinical Rating Scales
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 34/50
Clinical rating scales
Glasgow Coma Scale (GCS)
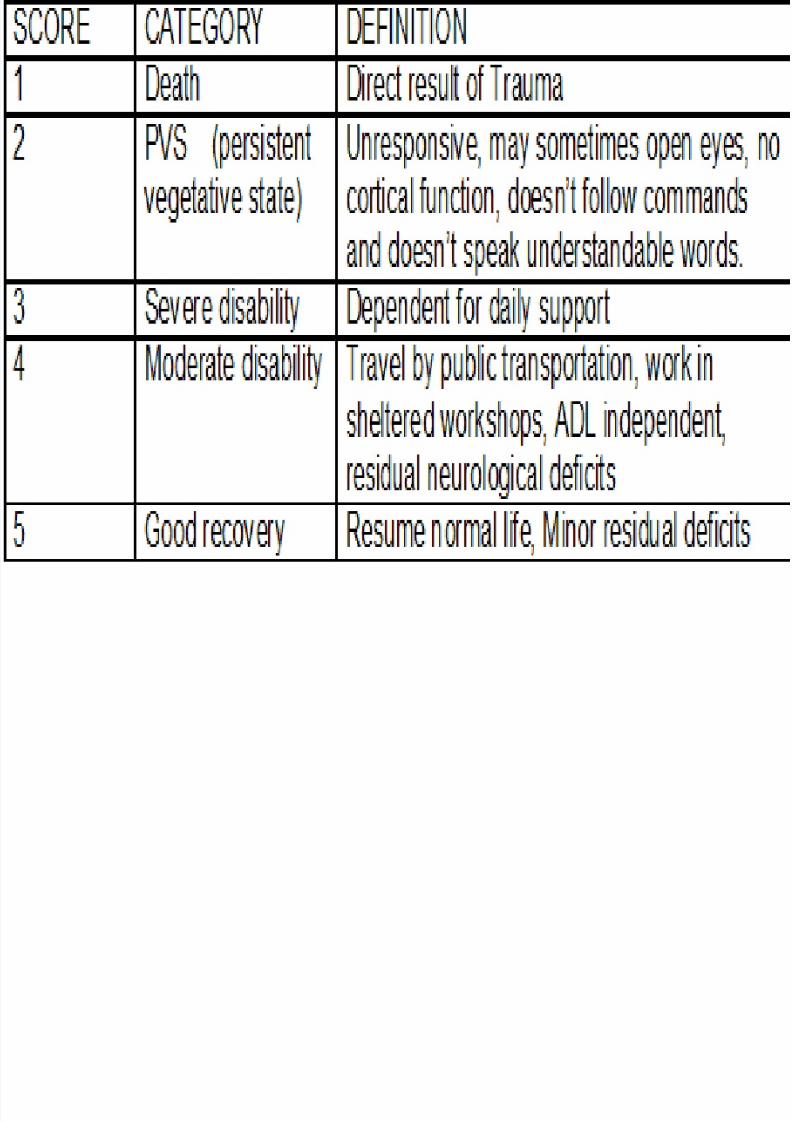
Glasgow Outcome Scale (GOS)
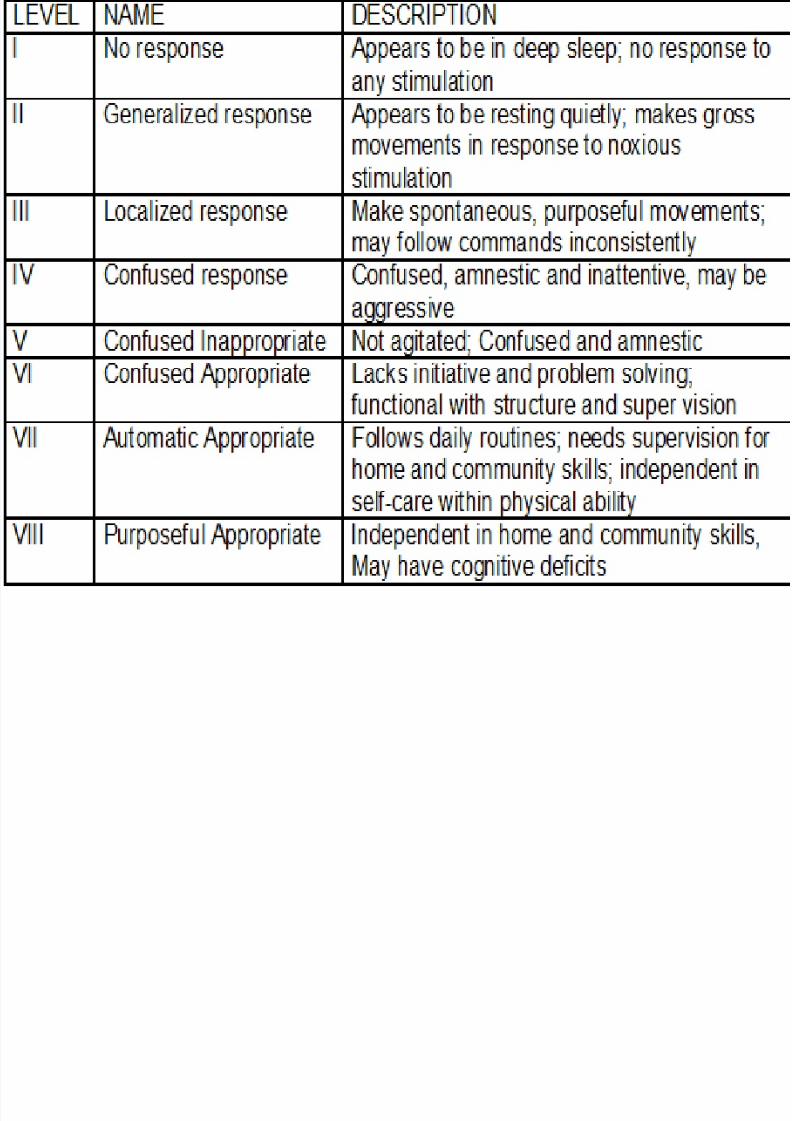
Ranchos Los Amigos Level of Cognitive
Functioning
Rappaport’s Disability Rating Scale (DRS)
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 35/50
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 36/50
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 37/50
Differential Diagnosis
Non-traumatic Brain Injury
Cerebral Palsy
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 38/50
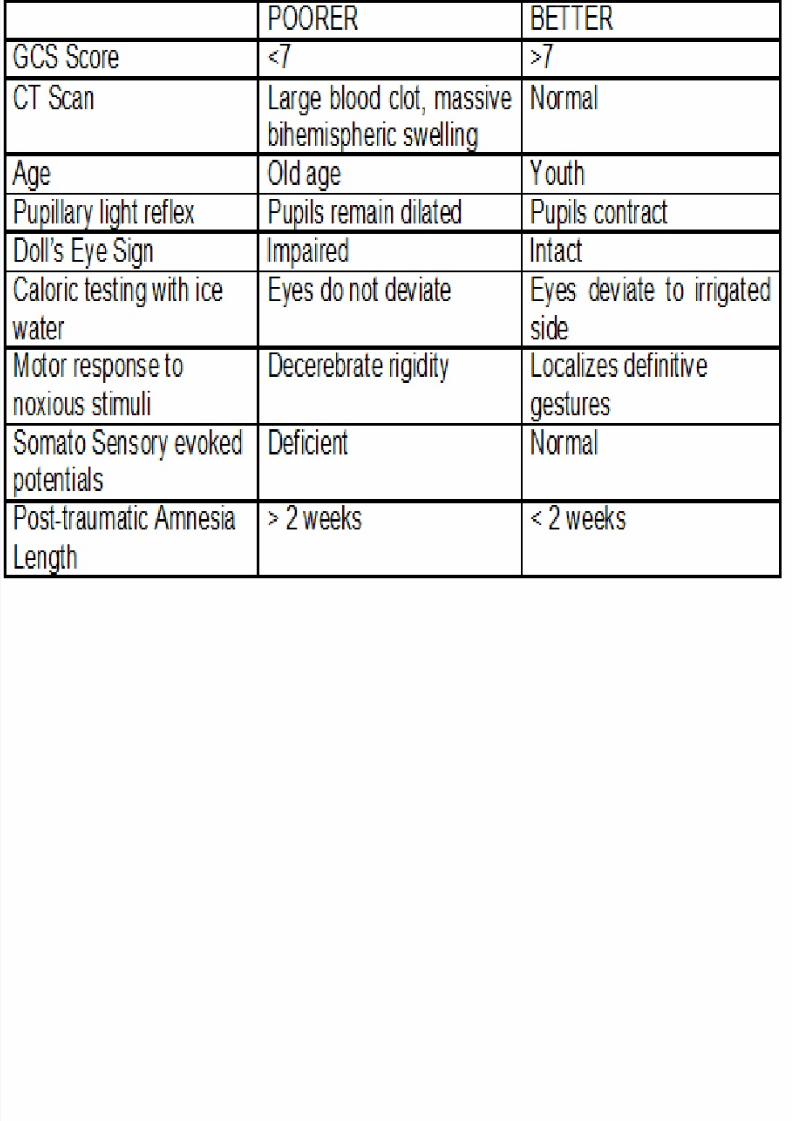
Prognosis
Prognostic Factors:
Patient’s age
Extracranial injuries
Availability of family support
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 39/50

8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 40/50
Medical/Surgical Management
Early medical management focuses on
determination of the severity of injury,
preservation of life and prevention of
further damage. LOC determined by GCS-neurologic exam
radiographic exam of the skull and cervical
spine
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 41/50
ICP monitoring via catheter in lateral ventricle
if ICP is over main value of 25 mmHg, decrease it
if ICP is below 25 mmHg value for 24 hours
consistent, system can be discontinued.
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 42/50
Pharmacologic Management
Elavil
Tofrani
Ritalin
Phenobarbital
Tegretol
Dantrium
Lioresal (Baclofen)
Valium
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 43/50
PT Assessment
Major focus is on
Communication Ability, Affect, Cognition,
Language, and Learning Style
Neurologic Assessment
Musculoskeletal Assessment
Functional Assessment
Other things to assess All other objective data (only when affected)
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 44/50
If purely TBI without associated injuries,
usual diagnostic classification is:
Impaired arousal, range of motion, and motor
control associated with coma, near coma, orvegetative state

8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 45/50
PT Management
Acute Management
Prevention of complication: e.g. respiratory
distress, contracture development, skin
breakdown Frequent position changes will assist
pulmonary hygiene and skin integrity
Postural drainage, percussion, and vibrationare used to keep the patient’s lung clear
PROM should be performed regularly but may
not be enough to prevent development of
deformities
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 46/50
Other management
Use of splints or prophylactic short leg casts
and passive standing on a tilt table
Functional mobility training may begin whenhe patient’s medical status is stable
Initial goals:
Patient tolerance to upright positioning Increase patient’s active movement capabilities
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 47/50
Rehabilitative management
Goal: Returning the patient to society at the
highest possible level of function
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 48/50
Issues that cross all levels
ROM – must be continued at all levels of
rehabilitation
Mobility – important to encourage activemobility ASAP

8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 49/50
Management based on RLASOCF
Low
Mid
High
8/12/2019 TBI(Compressed)
http://slidepdf.com/reader/full/tbicompressed 50/50
Thank You

















