Introduction Subarachnoid hemorrhage (SAH) from the rupture of intracranial aneurysms occurs in more than 26,000 indi- viduals in North America each year [1], two thirds of whom will succumb to their disease or be left perma- nently disabled. Of patients reaching referral centers after SAH, 10–20 % die or have permanent neurologic damage associated with ischemic complications of cere- bral vasospasm [1, 2]. Vasospasm can be categorized as angiographic or clinical. Angiographic vasospasm is reported in up to 70 % of patients undergoing angiography following an- eurysmal SAH [2, 3]. It is usually demonstrated between 4 and 9 days after hemorrhage [4–6]. Clinical vasospasm occurs when there are associated neurologic symptoms or signs such as the development of confusion, a de- crease in the level of consciousness or focal neurologic deficits. It is temporally associated with angiographic vasospasm but manifests itself with less frequency and affects only 20–30 % of patients with SAH [7]. A number of therapeutic measures have been used in an attempt to prevent or counteract cerebral vasospasm. Those that have shown benefit or promise include: medical treatment (hypertensive, hypervolemic ther- apy), pharmacologic (nimodipine) and endovascular regimens (angioplasty) [8–11]. Medical and pharmaco- logic therapy has shown benefits in counteracting the effects of ischemia in clinical vasospasm. However, not all vasospasm can be alleviated by these measures and, since its introduction in 1984 by Zubkov, mechanical vasodilatation by intra-arterial angioplasty has added an alternative mode of treatment when medical and phar- macologic means fail. Angioplasty has proven effective in reversing vasospasm in large, proximal cerebral ves- sels but is not effective in reaching small convexity or perforating branches. It also carries the risk of vessel rupture or occlusion [11]. In 1992, two small series of patients with clinical va- sospasm from aneurysmal SAH, treated with intra-ar- terial papaverine infusion, were reported [12, 13]. Pa- paverine infusion has demonstrated definite efficacy in reversing angiographic vasospasm and, in some patients, clinical vasospasm. In 1995 Clouston et al. [14] found therapeutic benefit in 50 % of patients receiving papav- erine hydrochloride infusion for clinical vasospasm. However, no large controlled series is yet available that tests the efficacy of intra-arterial papaverine infusion for improving immediate and long-term clinical out- come after SAH. This paper details present knowledge about papaverine pharmacology, side effects, method of administration, and potential utility. It is our hope that it will serve as a basis for better understanding of this drug as a potential tool in the treatment of cerebral vasos- pasm and prepare for evaluation of the true efficacy of papaverine in improving the long term outcome of pa- tients with clinical vasospasm after SAH. Neuroradiology (1997) 39: 90–98 Springer-Verlag 1997 INTERVENTIONAL NEURORADIOLOGY J. M. Mathis M. E. Jensen J. E. Dion Technical considerations on intra-arterial papaverine hydrochloride for cerebral vasospasm Received: 6 October 1995 Accepted: 4 March 1996 J. M. Mathis ( ) ⋅ M. E. Jensen ⋅ J. E. Dion Radiology, Johns Hopkins Hospital 600 N. Wolfe St., Baltimore MD 21287, USA Abstract Intra-arterial infusion of papaverine hydrochloride for sub- arachnoid hemorrhage-induced cer- ebral vasospasm has become an ad- junctive endovascular therapy along with cerebral angioplasty. Our knowledge concerning the mechan- ism of action, method of adminis- tration and potential side effects of this therapeutic alternative are re- viewed. Key words Vasospasm · Interventional neuroradiology · Subarachnoid space, hemorrhage · Drugs · intraarterial injection
Transcript
Introduction
Subarachnoid hemorrhage (SAH) from the rupture ofintracranial aneurysms occurs in more than 26,000 indi-viduals in North America each year [1], two thirds ofwhom will succumb to their disease or be left perma-nently disabled. Of patients reaching referral centersafter SAH, 10–20 % die or have permanent neurologicdamage associated with ischemic complications of cere-bral vasospasm [1, 2].
Vasospasm can be categorized as angiographic orclinical. Angiographic vasospasm is reported in up to70% of patients undergoing angiography following an-eurysmal SAH [2, 3]. It is usually demonstrated between4 and 9 days after hemorrhage [4–6]. Clinical vasospasmoccurs when there are associated neurologic symptomsor signs such as the development of confusion, a de-crease in the level of consciousness or focal neurologicdeficits. It is temporally associated with angiographicvasospasm but manifests itself with less frequency andaffects only 20–30 % of patients with SAH [7].
A number of therapeutic measures have been used inan attempt to prevent or counteract cerebral vasospasm.Those that have shown benefit or promise include:medical treatment (hypertensive, hypervolemic ther-apy), pharmacologic (nimodipine) and endovascularregimens (angioplasty) [8–11]. Medical and pharmaco-logic therapy has shown benefits in counteracting theeffects of ischemia in clinical vasospasm. However, not
all vasospasm can be alleviated by these measures and,since its introduction in 1984 by Zubkov, mechanicalvasodilatation by intra-arterial angioplasty has added analternative mode of treatment when medical and phar-macologic means fail. Angioplasty has proven effectivein reversing vasospasm in large, proximal cerebral ves-sels but is not effective in reaching small convexity orperforating branches. It also carries the risk of vesselrupture or occlusion [11].
In 1992, two small series of patients with clinical va-sospasm from aneurysmal SAH, treated with intra-ar-terial papaverine infusion, were reported [12, 13]. Pa-paverine infusion has demonstrated definite efficacy inreversing angiographic vasospasm and, in some patients,clinical vasospasm. In 1995 Clouston et al. [14] foundtherapeutic benefit in 50 % of patients receiving papav-erine hydrochloride infusion for clinical vasospasm.However, no large controlled series is yet available thattests the efficacy of intra-arterial papaverine infusionfor improving immediate and long-term clinical out-come after SAH. This paper details present knowledgeabout papaverine pharmacology, side effects, method ofadministration, and potential utility. It is our hope that itwill serve as a basis for better understanding of this drugas a potential tool in the treatment of cerebral vasos-pasm and prepare for evaluation of the true efficacy ofpapaverine in improving the long term outcome of pa-tients with clinical vasospasm after SAH.
J. M. Mathis ()) ⋅ M. E.Jensen ⋅ J.E.DionRadiology, Johns Hopkins Hospital600 N. Wolfe St., BaltimoreMD 21287, USA
Abstract Intra-arterial infusion ofpapaverine hydrochloride for sub-arachnoid hemorrhage-induced cer-ebral vasospasm has become an ad-junctive endovascular therapy alongwith cerebral angioplasty. Ourknowledge concerning the mechan-ism of action, method of adminis-
tration and potential side effects ofthis therapeutic alternative are re-viewed.
Papaverine hydrochloride is a member of the benzylis-quinoline group of alkaloids. It was originally preparedas a crude alkaloid derivative of opium but now is man-ufactured synthetically. It appears to have no narcoticproperties. The drug is a potent nonspecific smooth-muscle relaxant capable of producing diffuse dilatationof arteries and arterioles [15]. Its mechanism of action isnot known with certainty; it is, however, believed to actby inhibiting both cyclic adenosine monophosphate(CAMP) and cyclic guanosine 3,5-monophosphate(CGMP) phosphodiesterase activity in smooth musclecells and increasing intracellular CAMP and CGMPturnover [16–19]. The average blood half-life has beenestimated at 0.8 h (standard deviation 0,5 h) [20]. How-ever, this may represent an underestimate, as plasmalevels have been noted to rise continually throughout a4-day administration cycle (Q 6 h dosing) which sug-gests a true half-life of closer to 24 h [15]. The actual ef-fective half-life of smooth muscle relaxation in the ce-rebral vasculature has not been determined accurately.Oral and intravenous papaverine have both been shownto increase regional cerebral blood flow in humans [21].
Papaverine hydrochloride is supplied as a 3.0 % con-centration, 30 mg/ml, in an acidic mixture of pH 3.3. Thepreparation also contains the preservative chlorobu-tanol. A similar concentration of papaverine hydro-chloride without chlorobutanol preservative may beobtained in single-dose glass vials.
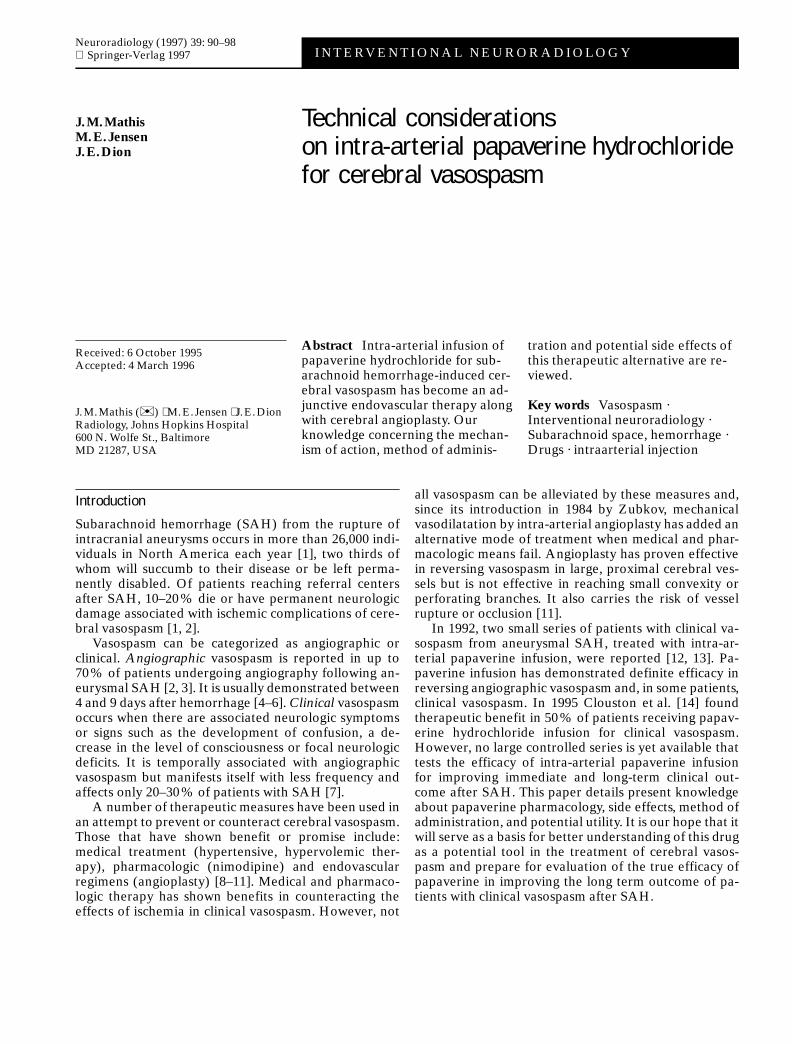
Papaverine hydrochloride is unstable in solution withcertain mixtures or in neutral and basic solutions. Westudied substances potentially mixed with papaverineduring an infusion for cerebral vasospasm [22] (Table 1).Both concentration and pH dependency were found forpapaverine stability in solution. Papaverine formedcrystal precipitates (with crystal size up to 100 mm)when mixed with human serum at 3.0 % or 0.3 % con-centrations (Fig. 1). The lower of these concentrations iseasily resuspended with agitation or turbulence of thehuman serum. A precipitate was seen to form when a3.0 % papaverine solution was mixed with heparinized
saline (with concentrations of 2,000–10,000 units hepa-rin/l). Finally, precipitate formation has been reportedwith ionic contrast media (most notably Hexabrix) inmultiple situations [22]. However, studies of commonlyused nonionic contrast media revealed no precipitationat any papaverine concentration tested (Table 1).
Although papaverine precipitation is pH-sensi-tive(precipitating pH between 5.3 and 5.4 in a normalsaline solution), the addition of papaverine to serum (attypical pH 7.4) does not automatically generate precip-itation when the papaverine solution is very dilute. Thisagain indicates both pH and concentration dependentcrystal formation. Precipitate, once formed in serum,can be resuspended with appropriate dilution.
Administration
The initial selection of a papaverine concentration anddose to be used intra-arterially for cerebral vasospasmwas empiric [12, 13]. At present, the typical papaverineconcentration infused is 0.3%, produced by diluting300 mg papaverine in 100 cc normal saline [23]. The en-tire 300 mg dose is administered into the affected vas-cular territory over 20–30 min. This assumes a micro-catheter position within a major cerebral vessel withoutwedging or demonstration of laminar flow into a smallbranch such as a perforating vessel or the ophthalmicartery. If more than one vascular territory is involved,additional infusions of 300 mg papaverine are given, thelimitation being the development of systemic hypoten-sion, increased intracranial pressure or neurologicalsymptoms or signs.
91
Table 1 Papaverine incompatibility (reproduced with permissionfrom [15])
(w) with chlorobutanol; (wo) without chlorobutanol; + precipitate;– no precipitate; heparin 2,000–10,000 U/l NS; saline 0.9 % NaCl(NS); contrast Iohexol 300 mgI/ml, Ioversol 320 mgI/ml, Iopamidol300 mgI/ml
Fig. 1 Photomicrograph of a papaverine precipitate crystal. Themaximum crystal dimension is 100 mm. (Reproduced with permis-sion)
92
a b
c d
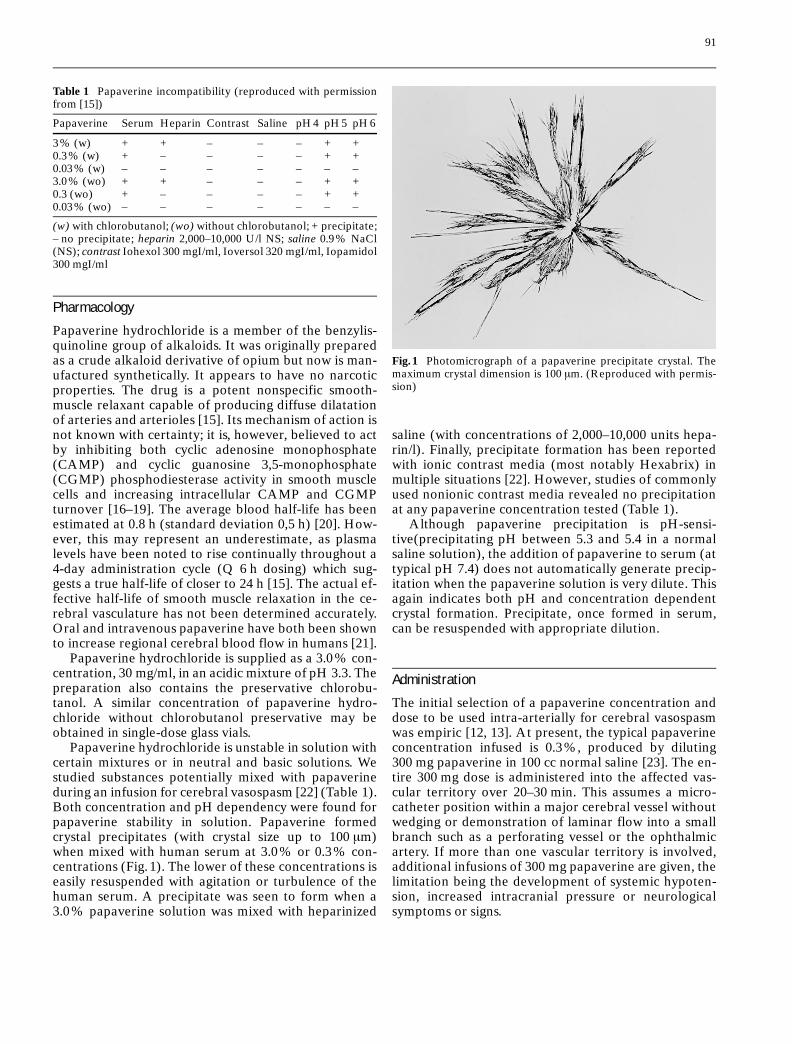
Fig. 2 a–m A patient with clinical vasospasm. Severe vasospasm was pre-sent in both carotid territories. Angioplasty initially followed papaverine inthe left carotid territory. Vasospasm recurred even in the region in whichangioplasty had been performed. However, angioplasty performed prior topapaverine on the right (day 1) and on the left (for recurrent vasospasm on
day 2) proved permanent on follow-up angiograms (day 3). a Pretreatmentright carotid angiogram (AP) showing an unclipped anterior communicatingartery aneurysm (asterisk) and severe vasospasm (arrows) (day 1). b Repeatangiogram following supraclinoid and middle cerebral artery (M1) angio-plasty (arrows).
c On day 2 (following clipping) the regions treated (arrows) re-main widely patient.
d On day 3 these segments (arrows) are unchanged, but more distalvessels show increased spasm and attenuated flow.
93
e f
g h
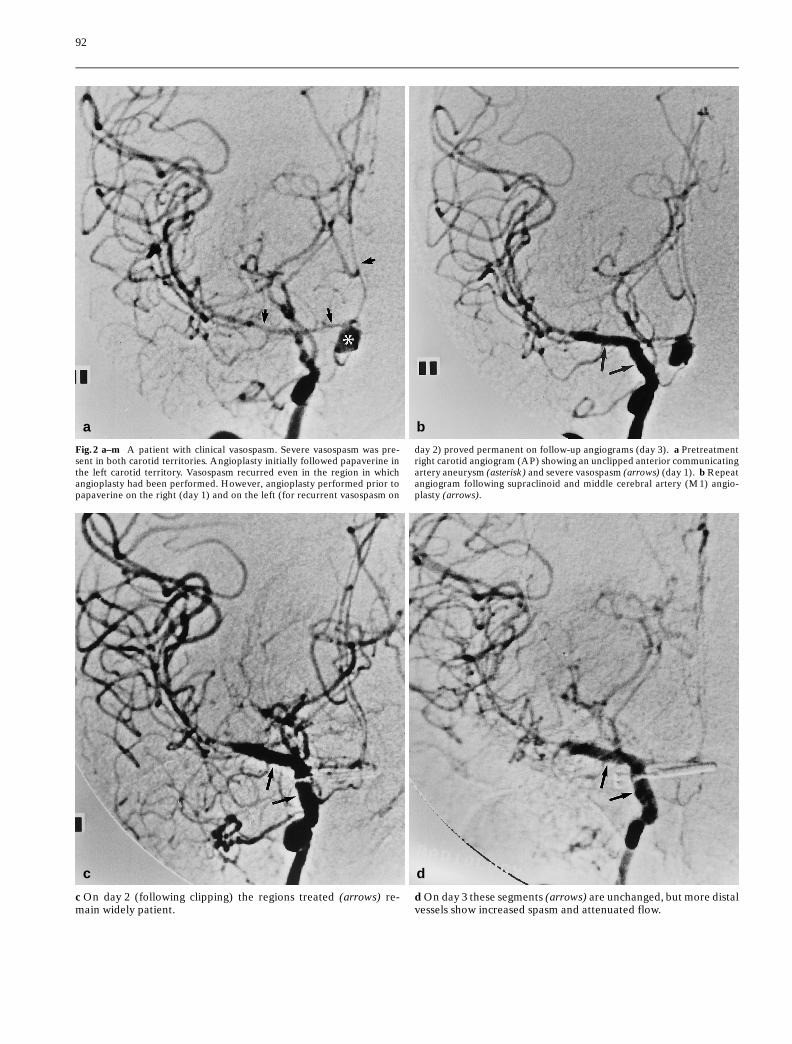
Fig. 2 e After papaverine (day 3) the distal middle (MCA) andposterior cerebral artery (PCA), territories have improved perfu-sion. The anterior cerebral artery (ACA) territory showed moremodest improvement.
Fig. 2 f Left carotid angiogram (day 1) prior to treatment demon-strates severe supraclinoid, ACA and MCA vasospasm (arrows).
Fig. 2 g After papaverine infusion there is a reduction in vasospasmreflected by increased proximal vessel diameter (arrows).
Fig. 2 h Angioplasty of the supraclinoid ICA and M 1 segment ofthe MCA was performed with little additional vascular dilatation.
94
i j
k l
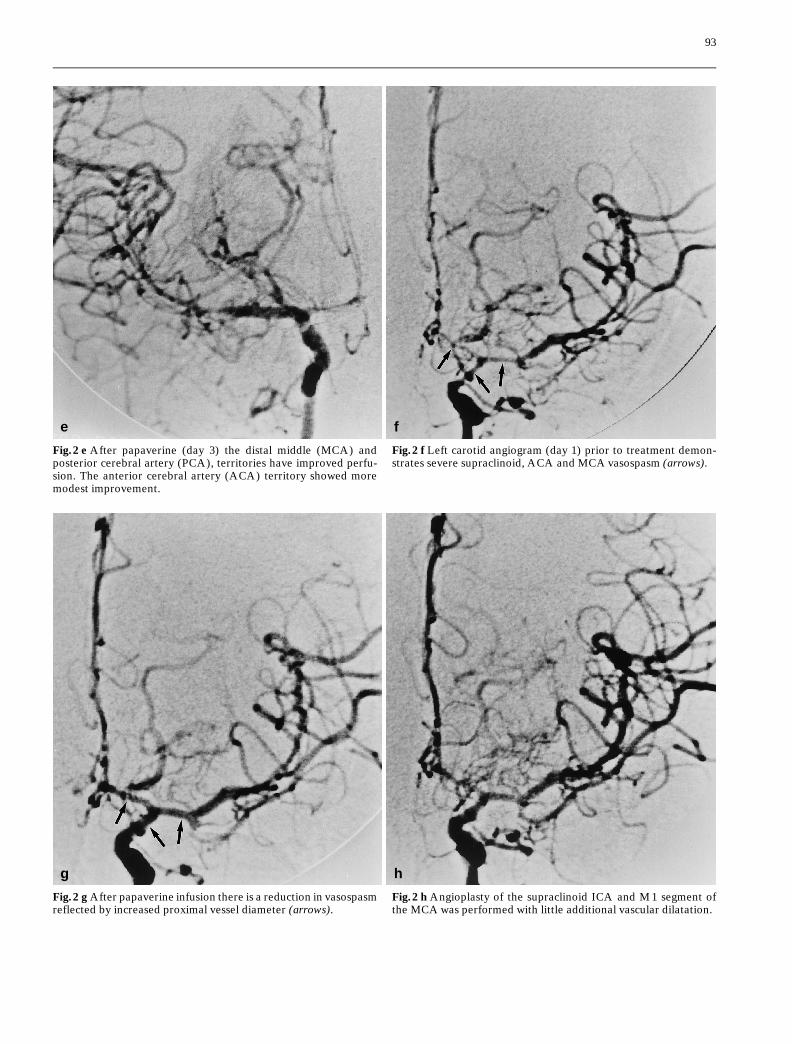
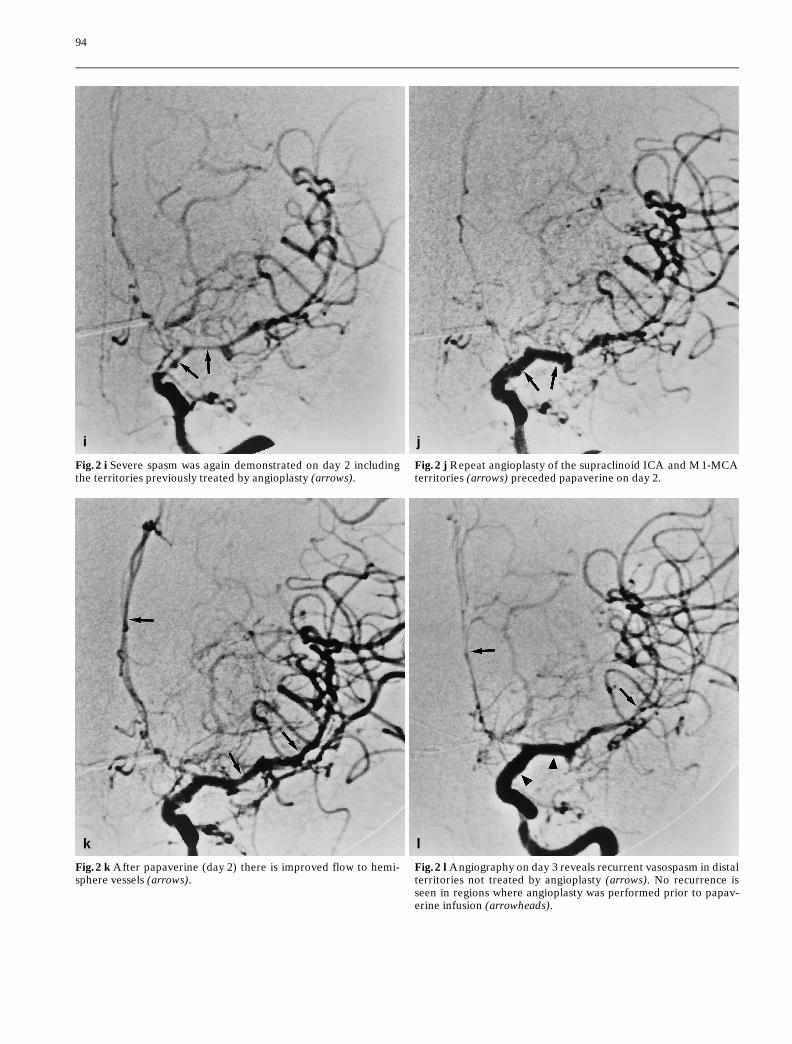
Fig. 2 i Severe spasm was again demonstrated on day 2 includingthe territories previously treated by angioplasty (arrows).
Fig. 2 j Repeat angioplasty of the supraclinoid ICA and M 1-MCAterritories (arrows) preceded papaverine on day 2.
Fig. 2 k After papaverine (day 2) there is improved flow to hemi-sphere vessels (arrows).
Fig. 2 l Angiography on day 3 reveals recurrent vasospasm in distalterritories not treated by angioplasty (arrows). No recurrence isseen in regions where angioplasty was performed prior to papav-erine infusion (arrowheads).
Typically, infusion is via a microcatheter. In the ante-rior circulation, the catheter tip is usually placed abovethe ophthalmic artery, in the supraclinoid internal ca-rotid artery (ICA). This allows the papaverine to infuseboth the middle and anterior cerebral circulations with aminimal amount of dilution. In the posterior circulation,the catheter is typically placed immediately below theregion affected by the vasospasm. When an infusion inthe distal vertebral or proximal basilar is necessary, onemust be careful to observe for medullary and lowerbrain stem dysfunction (see section on side effects, be-low). Although papaverine infusion in the proximal ICAor vertebral artery is possible, dilution and run-off toother vascular territories are increased and limit the ef-fectiveness of the papaverine on distal spastic vessels.
The primary indication for papaverine infusion is totreat arteries and arterioles too small for or inaccessibleto balloon angioplasty. The effect of balloon angioplastyon a spastic segment appears to be a permanent or long-lasting vasodilatation (possibly a functional impairmentin vasoreactivity of the vessel wall due to mechanicalstretching), as opposed to the shorter-term effect of pa-paverine infusion [24]. We observed in one patient amore transient effect of angioplasty following papaver-ine infusion than with angioplasty alone or preceding
papaverine (Fig. 2). For this reason, we perform papav-erine infusion after angioplasty when the latter is appli-cable. Papaverine infusion prior to angioplasty has beenreported in a patient whose vasospasm was so severe asto preclude initial balloon introduction [25]. In thesecircumstances papaverine infusion preceding angio-plasty seems warranted.
In the unusual case where a patient presents in clini-cal vasospasm with an unsecured and recently rupturedaneurysm, a microcatheter can usually be manipulatedbeyond the lesion or vascular territory with minimalrisk. In this situation, infusion beyond the unsecuredaneurysm allows the treatment of distal vasospasmwithout infusion of the area of the aneurysm itself.
Side effects
In our institution, 36 patients have received intra-arte-rial papaverine in 48 vascular territories. Six of thesepatients have had transient neurologic events: pupillarydilatation (4 patients), transient hemiparesis (1 patient)and respiratory arrest (1 patient). Mydriasis is nowknown to be a common phenomenon with papaverineinfusion particularly when the catheter is proximal tothe ophthalmic artery [26]. The effect on the pupil istransient and resolves quickly with discontinuation ofthe papaverine infusion. As long as there is not selectiveinfusion into the ophthalmic artery, especially with awedged microcatheter, no permanent side effect shouldbe expected. However, personnel responsible for moni-toring the patient should be aware that transient mydri-asis is expected during an infraophthalmic carotid pa-paverine infusion, so as to obviate unwarranted concernabout change in the patient’s neurologic status.
Infusions into the posterior circulation have been as-sociated with respiratory arrest and also carry the po-tential for cardiac dysfunction [23, 27]. This is increasedwith infusion in the distal vertebral artery or proximalbasilar trunk, below the anterior inferior cerebellar ar-tery. Transient depression of medullary respiratory andcardiovascular centers appears to be responsible for thisresponse. Although the effects have to date been tran-sient in all patients, respiratory and cardiovascular sup-port may be necessary even if such transient neurologicchanges are experienced.
Hypotension has not been a side effect when papav-erine has been infused at the rates described above.However, faster infusion of papaverine, particularlywhen associated with the need to infuse multiple vascu-lar territories, can be associated with diminished perfu-sion pressure and blood pressure should be constantlymonitored during such administration. If hypotension isobserved the papaverine infusion should be terminated.
The etiology of the transient neurologic events asso-ciated with papaverine infusion has not been completely
95
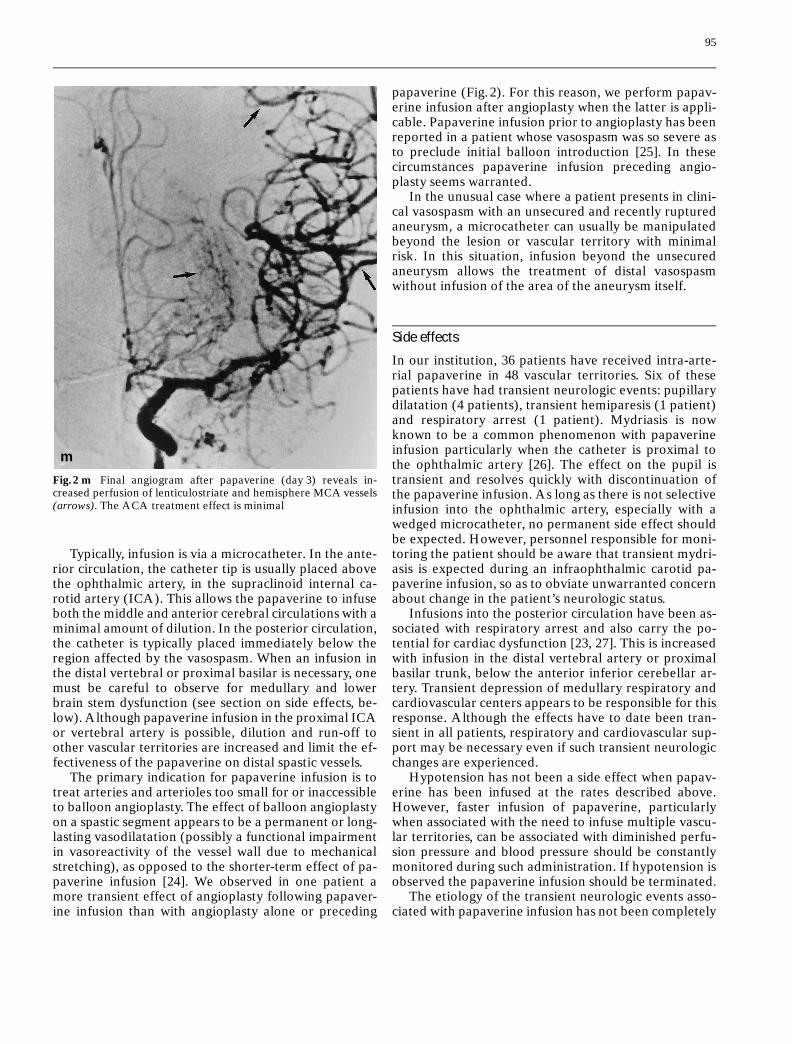
m
Fig. 2 m Final angiogram after papaverine (day 3) reveals in-creased perfusion of lenticulostriate and hemisphere MCA vessels(arrows). The ACA treatment effect is minimal
determined. We have demonstrated formation of pa-paverine microcrystals in vitro [22] and extrapolationfrom this work suggests that the possibility for micro-emboli exists when papaverine is infused in regionswhere vasospasm is severe and blood flow markedly re-duced. Under these circumstances, diminished infusionrates may be indicated to insure the avoidance of mi-crocrystal formation. Crystal formation did not appearto be dependent on whether the papaverine preparationcontained chlorobutanol. Another explanation for thetransient events may be a direct pharmacologic effect onneurologic function by papaverine itself or by chloro-butanol on the territories infused. Papaverine infusionin patients with SAH has been found to be associatedwith a statistically significant, transient increase in in-tracranial pressure [28]. Since papaverine precipitateshave been shown to be resuspendible in serum with agi-tation, an embolic, pharmacologic or mechanical mech-anism could explain the transient nature of these events.
A single case of thrombocytopenia has been reportedfollowing papaverine infusion for vasospasm secondaryto SAH. The effects were transient but prompted re-placement therapy [29].
Effects of therapy
Vorkapic et al. [30] successfully produced vasospasmafter SAH in the rabbit. In this situation, intra-arterialpapaverine was effective in reversing angiographic va-
sospasm in the first 3 days following its appearance.However, vasospasm became refractory to papaverinetreatment on days 5–9. There was a positive correlationbetween decreased vessel-wall distensibility (in vitro)and refractoriness of vasospasm to papaverine infusion(in vivo). They suggested that initially, arterial narrow-ing after SAH is due to vasoactive substances releasedin the close vicinity of the arterial wall, and that subse-quent changes in vessel wall distensibility are late phe-nomena associated with tissue damage and permanentstructural change.
Angiographic vasospasm is often relieved followingintraarterial infusion of papaverine (Fig. 3). Althoughoutcome analysis of a large group of patients treatedwith papaverine infusion for clinical vasospasm does notexist, initial reports of small series are encouraging.Kaku et al. [13] found that 34 of 37 vascular territorieswere successfully dilated and 8 of 10 patients showedimprovement in neurologic function following the pro-cedure. Similar improvement is suggested by other au-thors [12, 14, 25, 31].
Clinical disturbances associated with vasospasm arebelieved to be related to ischemia and reduction in re-gional cerebral blood flow. For any therapy to have apositive impact there must be quick initiation after therecognition of symptoms or signs. This is no less the casefor papaverine infusion. We recommend an initial trialof hypertensive, hypervolemic therapy (HHT) when notclinically contraindicated. Endovascular therapy (pa-paverine infusion and/or angioplasty) is initiated if there
96
a b
Fig. 3 a Right carotid angio-gram showing severe vasos-pasm of the entire carotid terri-tory with poor hemisphere per-fusion. b Angiogram followingpapaverine infusion. Vessel di-ameter is increased and flow tothe right hemisphere is en-hanced (arrows)
is no clinical improvement following a 1–2 h course ofHHT.
The effects of papaverine on vasospasm appear to bemore transient than those of proximal, large vessel an-gioplasty. Patients may therefore have to be reinfused ifsymptoms recur. The transient nature of the effect var-ies from patient to patient and the decision to repeattherapy should be based on available clinical alterna-tives and previous response to papaverine infusion.
Conclusions
Papaverine hydrochloride infusion for clinical cerebralvasospasm is a relatively new technique which has beenadded to the armamentarium of treatment possibilitiesfor this severely disabling and potentially lethal side ef-fect of SAH. To date, papaverine infusions have beennoted to reverse angiographic vasospasm and improveregional cerebral blood flow with variable success. Ini-tial reports also suggest clinical improvement associatedwith papaverine infusion. However, outcome results inlarge, controlled series are not yet available. In light ofthe potentially devastating impact of clinical vasospasmfollowing SAH and the initial encouraging results frompapaverine therapy, additional clinical study and evalu-ation seems warranted.
97
References
1. Awad IA, Carter P, Spetzler RF et al(1987) Clinical vasospasm after sub-arachnoid hemorrhage: response to hy-pervolemic hemodilution and arterialhypertension. Stroke 18: 365–372
3. Spetzler RF (1989) An overview of theinternational clinical literature on useof nimodipine in subarachnoid hemor-rhage. Hosp Formul 24: 2–7
4. Saito I, Sano K (1980) Vasospasm afteraneurysm rupture: incidence, onset andcourse. In: Wilkes RH (ed) Cerebralarterial spasm. Williams and Wilkins,Baltimore pp 294–301
5. Kwak R, Ziisuama H, Ohi Tet al (1979)Angiographic study of cerebral vaso-spasm following rupture of intracranialaneurysms: time of appearance. SurgNeurol 11: 257–262
6. Weir B, Grace M, Hansen J et al (1978)Time course of vasospasm in man.J Neurosurg 48: 173–178
7. Kodama N, Mizoik A, Sakurai Y et al(1980) Incidence and onset of vaso-spasm. In Wilkes RH (ed) Cerebral ar-terial spasm. Williams and Wilkins,Baltimore, pp 361–365
8. Brothers MF, Holgate RC (1990) Intra-cranial angioplasty for treatment of va-sospasm after subarachnoid hemor-rhage: technique and modifications toimprove branch access. AJNR 11: 239–247
9. Dion JE, Duckwiler GR, Vinuela F(1990) Pre-operative microangioplastyof refractory vasospasm secondary tosubarachnoid hemorrhage. Neuroradi-ology 32: 232–236
11. Newell DW, Eskridge JM, Mayberg MR(1989) Angioplasty for the treatment ofsymptomatic vasospasm following sub-arachnoid hemorrhage. J Neurosurg 71:654–660
12. Kassell NF, Helm G, Simmons N et al(1992) Treatment of cerebral vasospasmwith intra-arterial papaverine. J Neuro-surg 77: 848–852
13. Kaku Y, Yonekawa Y, Tsukahara Tet al(1992) Superselective intraarterial infu-sion of papaverine for the treatment ofcerebral vasospasm after subarachnoidhemorrhage. J Neurosurg 77: 842–847
14. Clouston JE, Numaguchi Y, ZoarskiGH et al (1995) Intra-arterial papaver-ine infusion for cerebral vasospasm af-ter subarachnoid hemorrhage. AJNR16: 27–38
15. Cook P, James I (1981) Cerebral vaso-dilators. N Engl J Med 305: 1508–1513
16. Bolton TB (1979) Mechanisms of actionof transmitters and other substances onsmooth muscle. Physiol Rev 59: 606–718
17. Miyamoto M, Takayanagi I, Ohkubo Het al (1976) Actions of papaverine onintestinal smooth muscle and its inhibi-tion of cyclic AMP and cyclic GMPphosphodiesterases. Jpn J Pharmacol26: 114–117
18. Polson JB, Krzanowksi JJ, FitzpatrickDF et al (1978) Studies on the inhibitionof phosphodiesterase – catalysed cyclicAMP and cyclic GMP breakdown andrelaxation of canine tracheal smoothmuscle. Biochem Pharmacol 27: 254–256
19. Poch G, Kukovetz WR (1971) Papaver-ine-induced inhibition of phosphodi-esterase activity in various mammaliantissues. Life Sci 10: 133–144
20. Arnold JD, Eldridge J, Riley B et al(1977) Papaverine hydrochloride: theevaluation of two new dosage forms. IntJ Clin Pharmacol 15: 230–233
21. McHenry LC, Stump DA, Howard G etal (1983) Comparison of the effects ofintravenous papaverine hydrochlorideand oral pavabid HP capsulets on re-gional cerebral blood flow in normalindividuals. J Cereb Blood Flow Metab3: 442–447
22. Mathis JM, DeNardo A, Thibault L etal (1994) In vitro evaluation of papav-erine hydrochloride incompatibilities: asimulation of intra-arterial infusion forcerebral vasospasm. AJNR 15: 1665–1670
23. Mathis JM, DeNardo A, Jensen ME etal (1994) Transient neurological eventsassociated with intra-arterial papaver-ine infusion for subarachnoid hemor-rhage induced vasospasm. AJNR 15:1671–1674
24. Chan PD, Findley JM, Vollrath B et al(1995) Pharmacological and morpho-logical effects of intra-transluminal bal-loon angioplasty on normal and vaso-spastic canine basilar arteries. J Neuro-surg 83: 522–530
98
25. Livingston K, Hopkins LN (1993) Intra-arterial papaverine as an adjunct totransluminal angioplasty for vasospasminduced by subarachnoid hemorrhage.AJNR 14: 346–347
26. Hendrix LE, Dion JE, Jensen ME et al(1994) Papaverine induced mydriasis.AJNR 15: 716–718
27. Barr JD, Mathis JM, Horton JA (1994)Severe transient brainstem depressionduring intra-arterial papaverine infu-sion for treatment of cerebral vaso-spasm. AJNR 15: 719–723
28. McAuliffe W, Townsend M, EskridgeJM et al (1995) Intracranial pressurechanges induced during papaverine in-fusion for the treatment of vasospasm.J Neurosurg 83: 430–434
29. Miller JA, Cross DT, Moran CJ et al(1995) Severe thrombocytopenia fol-lowing intra-arterial papaverine admin-istration for treatment of vasospasm.J Neurosurg 83: 435–437
30. Vorkapic P, Bevan RD, Benan JA(1990) Pharmacologic irreversible nar-rowing in chronic cerebral vasospasm inrabbits is associated with functionaldamage. Stroke 21: 1478–1484
31. Marks MP, Steinberg GK, Lane B(1993) Intra-arterial papaverine for thetreatment of vasospasm. AJNR 14: 822–826
Neurosurgery Clinics of North America:Vol 7. No.1 Percutaneous Spine Techniques.Guest Editor: Richard G.Fessler. W.B.Saun-ders Company 1996, (ISBN 1042-3680)
This 170-page book is a collection of 16well-referenced review papers, some withpersonal series, by American and Euro-pean authors documenting developmentsin the exciting new field of minimally trau-matic spinal surgery. “Percutaneous”,otherwise unqualified, is a poor descriptionas it fails to separate the modern imaging-guided and endoscopic techniques fromconventional spinal surgery which, ofcourse, is also percutaneous. The paperscover Cervical and lumbar chymopapainnucleolysis; Automated percutaneous disc-ectomy; Percutaneous laser discectomy;Automated percutaneous nucleotomy; Ste-reotactic lumbar microdiscectomy; Trans-foraminal endoscopic microdiscectomy;Diagnostic and therapeutic spinal arthro-scopy; Laparoscopic lumbar discectomy;Endoscopic thoracic discectomy; Percuta-neous lumbosacral fixation and fusion;Percutaneous endoscopic lumbar spine fu-sion; Percutaneous facet coagulation; Per-cutaneous Biopsy of the thoracic spine;Automated percutaneous biopsy in the di-
agnosis and treatment of infectious discitisand finally, Diagnostic spinal injection pro-cedures. They are aimed mainly at neuro-surgeons and will be of mainly academicinterest in most hard-pressed departmentsof neuroradiology. Some neuroradiologistsmay be tempted by chymopapain nucleoly-sis, APLD, facet injections or diagnosticspinal injection techniques. Those who al-ready practice percutaneous biopsy of thespine are unlikely to find enough in thissection to justify purchase of this book.Most of the techniques are described insufficient detail to give the uninitiated agood idea of what is involved, althoughthere would be no substitute for supervisedtraining. Each paper is written without re-ference to others and this results in a cer-tain degree of repetition, for instance thetechnique of automated percutaneous disc-ectomy is repeated with better illustrationsbut with less helpful text in the paper onautomated percutaneous biopsy in discitis.There are occasional editorial errors, forinstance in the paper on percutaneousbiopsy of the thoracic spine the dose ofmidazolam is given as 1–2 g, enough to se-date a small town. On page 31 Figures 1 and2 are transposed with respect to their cap-tions. On page 54 Figures 7 and 8 are verysimilar sagittal images of the same patient’slumbar spine. Figure 7 is said to show aprotruded disc whilst the same disc is de-
scribed as extruded in Figure 8. On page121 the caption to Figure 1 appears to haveno relevance to it. In the paper on laserDiscectomy, although the description of thephysics of laser is interesting, we are ex-pected to know what Nd, Ho and YAG arewithout explanation. The principal pro-blem with the book is one of balance. Eachpaper is written by an enthusiast who, notsurprisingly, will try to sell his technique tothe reader. Thus we are told that “the totallack of complications with cervical chymo-papain nucleolysis, makes it especially at-tractive as compared with conventionalsurgery”. One can only hope that long ex-perience will bear this out; however, asthere were neither conservatively or surgi-cally treated controls we have no means ofknowing whether this technique can be re-commended above either. Of the eight pa-pers on different direct interventions on thedisc, only four describe their authors’ seriesin more than passing detail and in only oneof these is there reference to a controlgroup.
This book brings together useful de-scriptions of minimally traumatic interven-tions which may have an important part toplay in the treatment of spinal disc disease.We have, however, some way to go beforewe know which ones and in what circum-stances.