43
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 1 Ted Cohen, M.S., CCE Manager, Clinical Engineering, UC Davis Health System
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 1
Ted Cohen, M.S., CCE
Manager, Clinical Engineering,
UC Davis Health System
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 2
Introduction Brief history and evolution of Philips
hemodynamic monitoring networks UCDMC: Widespread monitor integration
implementation in 2007 UCDMC: 2010 “Pavilion project” and
Philips Customer Supplied Clinical Network (CSCN)
Support Considerations Conclusions
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 3
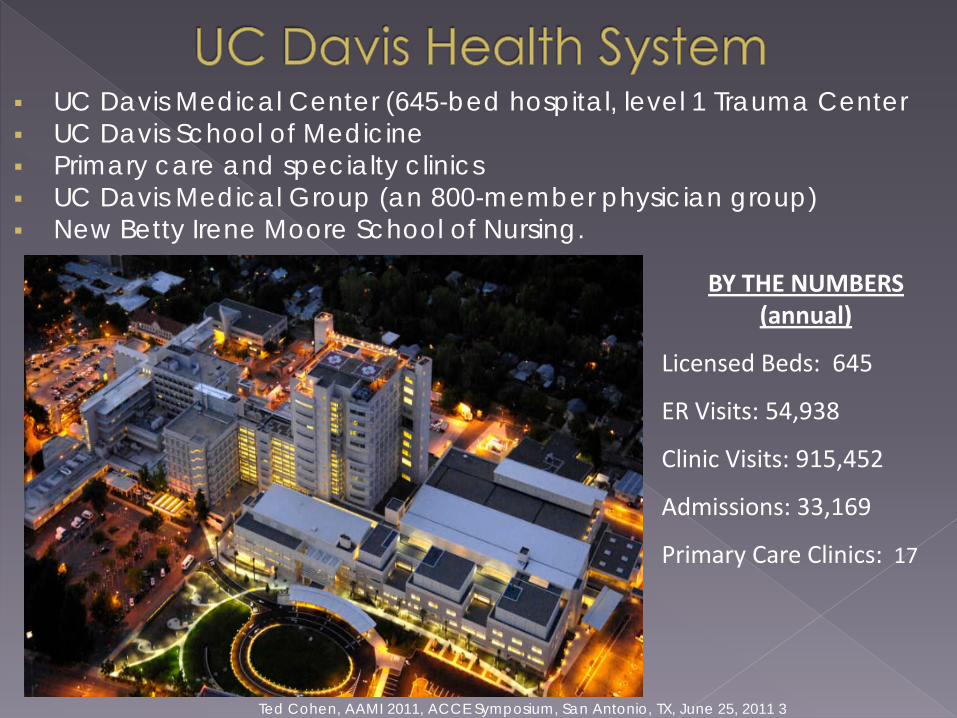
UC Davis Medical Center (645-bed hospital, level 1 Trauma Center UC Davis School of Medicine Primary care and specialty clinics UC Davis Medical Group (an 800-member physician group) New Betty Irene Moore School of Nursing.
BY THE NUMBERS (annual)
Licensed Beds: 645
ER Visits: 54,938
Clinic Visits: 915,452
Admissions: 33,169
Primary Care Clinics: 17
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 4
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 5
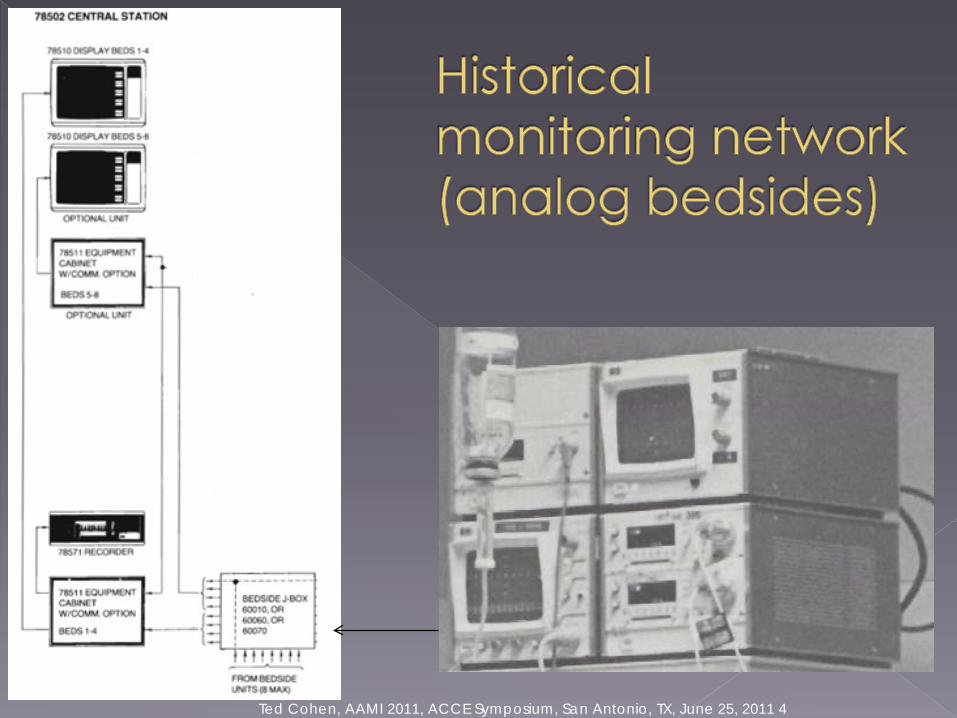
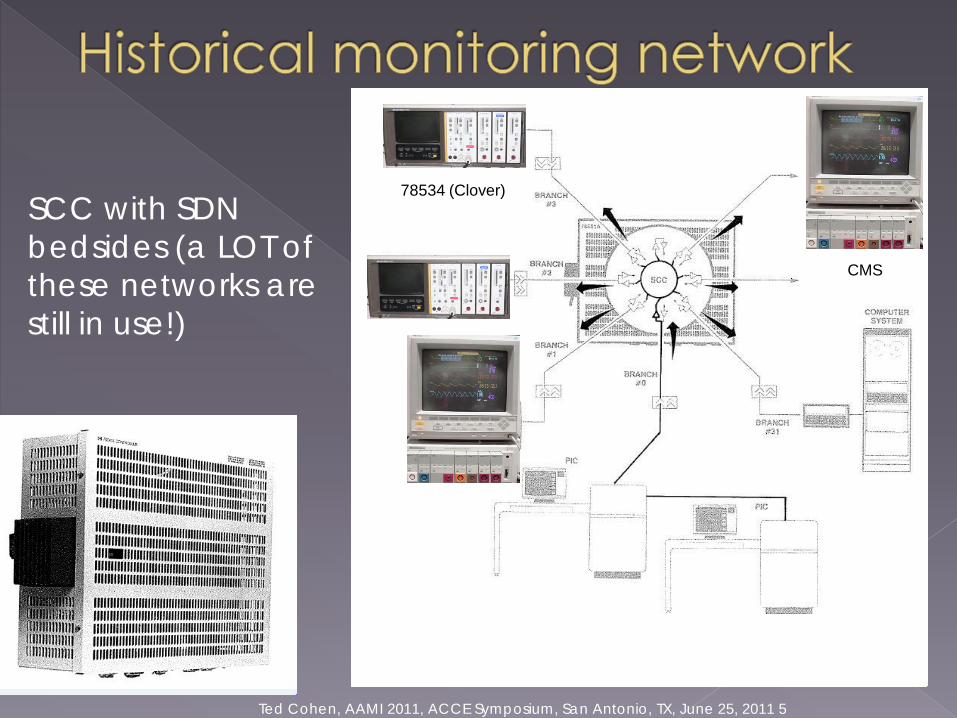
SCC with SDN bedsides (a LOT of these networks are still in use!)
78534 (Clover)
CMS
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 6
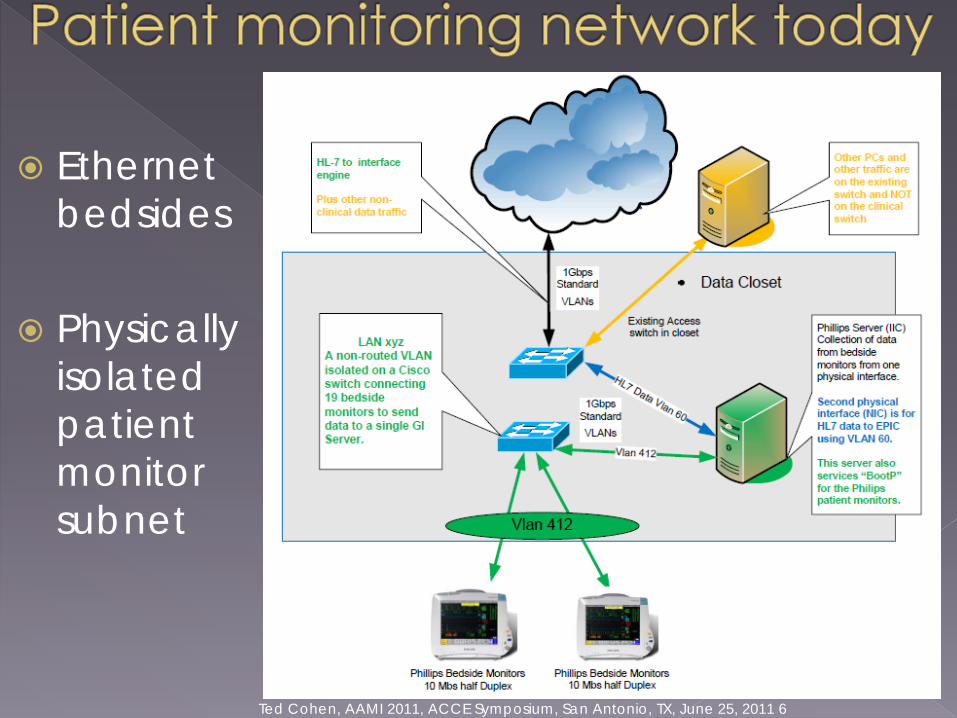
Ethernet bedsides
Physically isolated patient monitor subnet
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 7
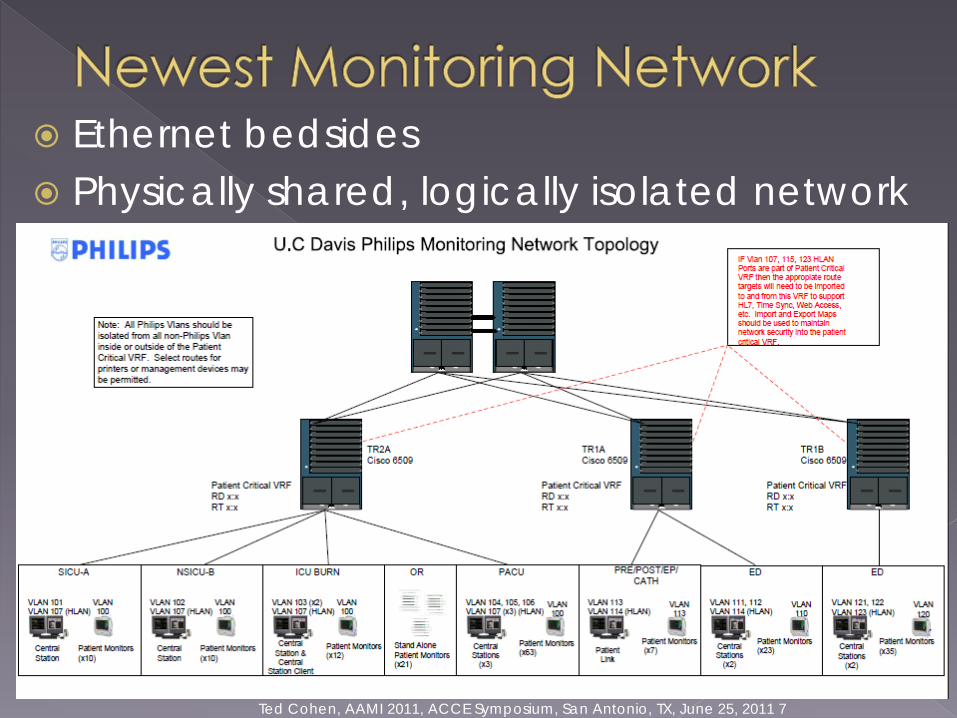
Ethernet bedsides Physically shared, logically isolated network
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 8
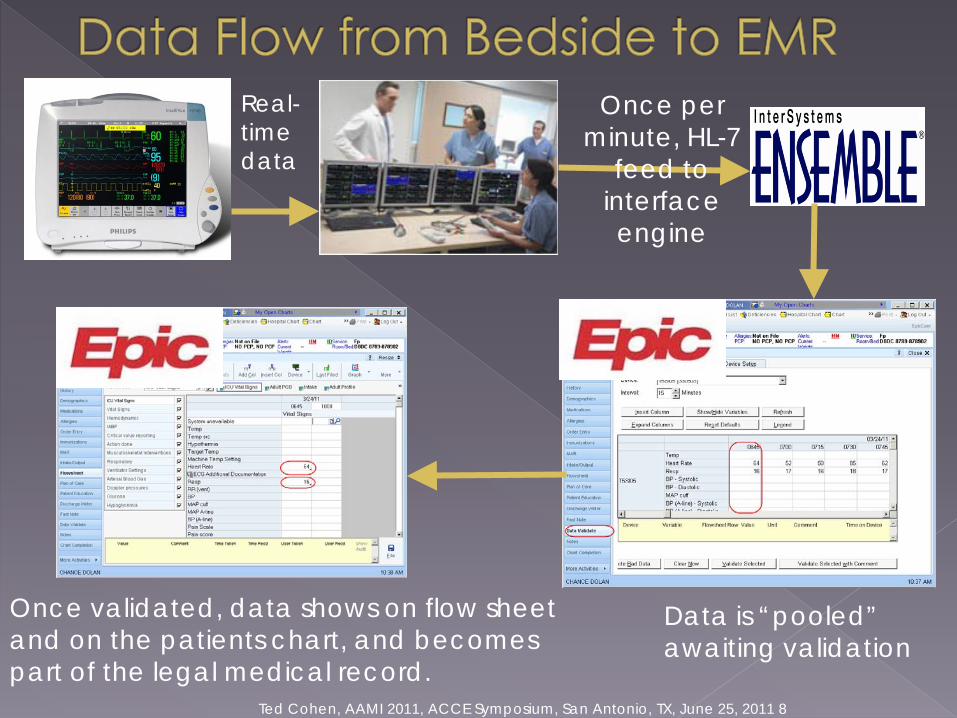
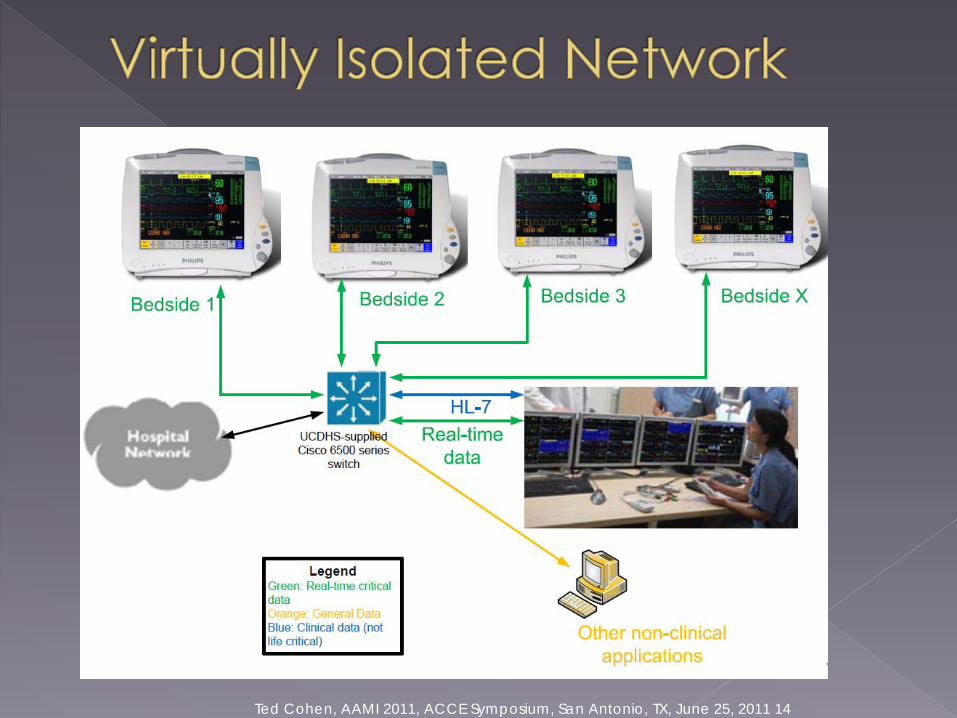
Real-time data
Once per minute, HL-7
feed to interface engine
Data is “pooled” awaiting validation
Once validated, data shows on flow sheet and on the patients chart, and becomes part of the legal medical record.
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 9
In calendar 2010, over 5 MILLION vital signs entries from over 500 devices were validated
~ 50% of vital signs entered, were via monitor integration
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 10
New building opened in 2010 188 wired Philips bedside monitors, 11
central stations in 7 departments One department (ED) has routed bedsides No Database servers (direct connect to
EMR via dual-NIC’d central stations) Clinical life-critical (CLC) network concept IICs located in data closet Interface engine
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 11
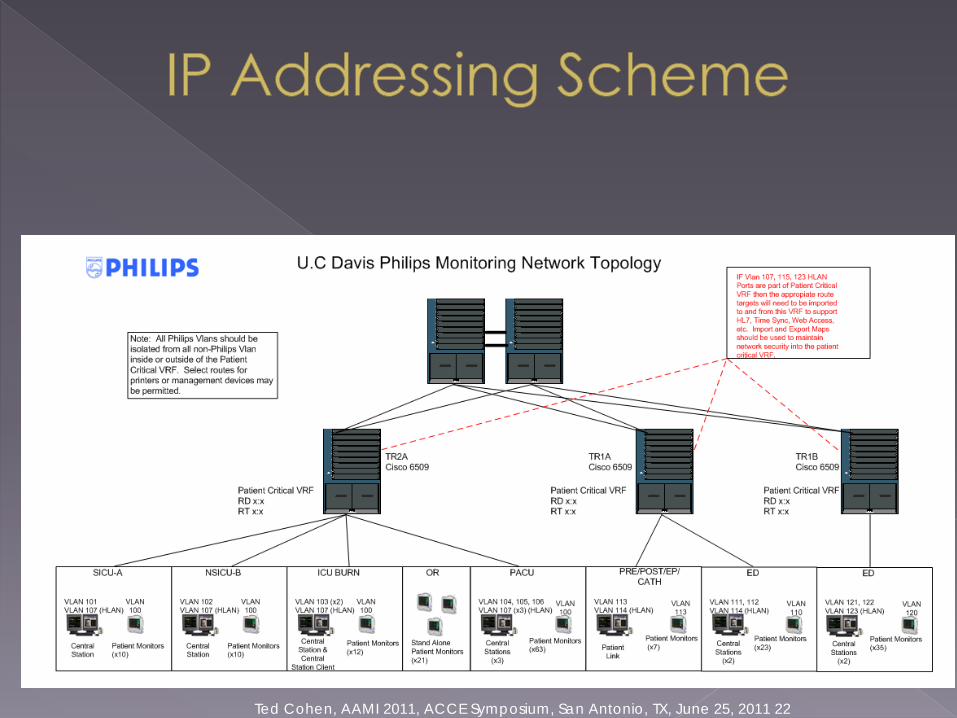
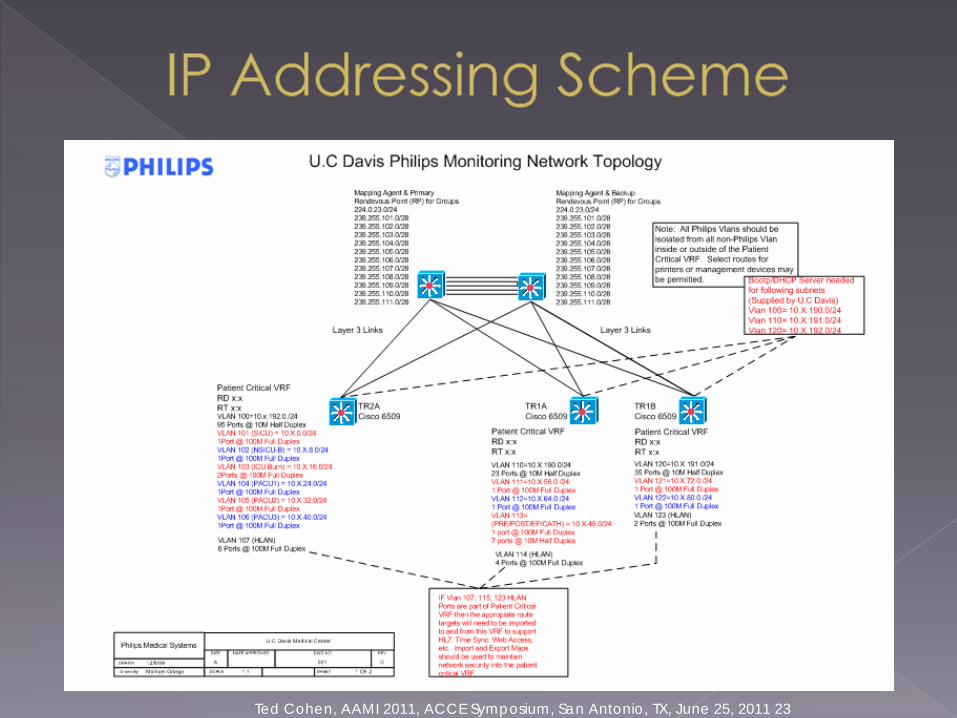
CSCN provides guidelines for hospital-provided VLANs (virtual local area networks) for patient physiological monitoring
A 250 page book (includes wired and wireless, but we will only be discussing WIRED networks today)
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 12
Summary of requirements:› 100 Meg bits/sec network speed to the
device
› Use Gigabit links for trunks that are shared with other non-ICN traffic
› Use QoS for trunks shared with other non-ICN traffic
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 13
Summary of requirements continued:› Hard set all speed and duplex settings for
each Philips switch port (NO auto-negotiate)
› Routing between the Hospital LAN (e.g. GP and CGP) and the Philips LAN (CLC) are only allowed where specified in the special cases listed
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 14
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 15
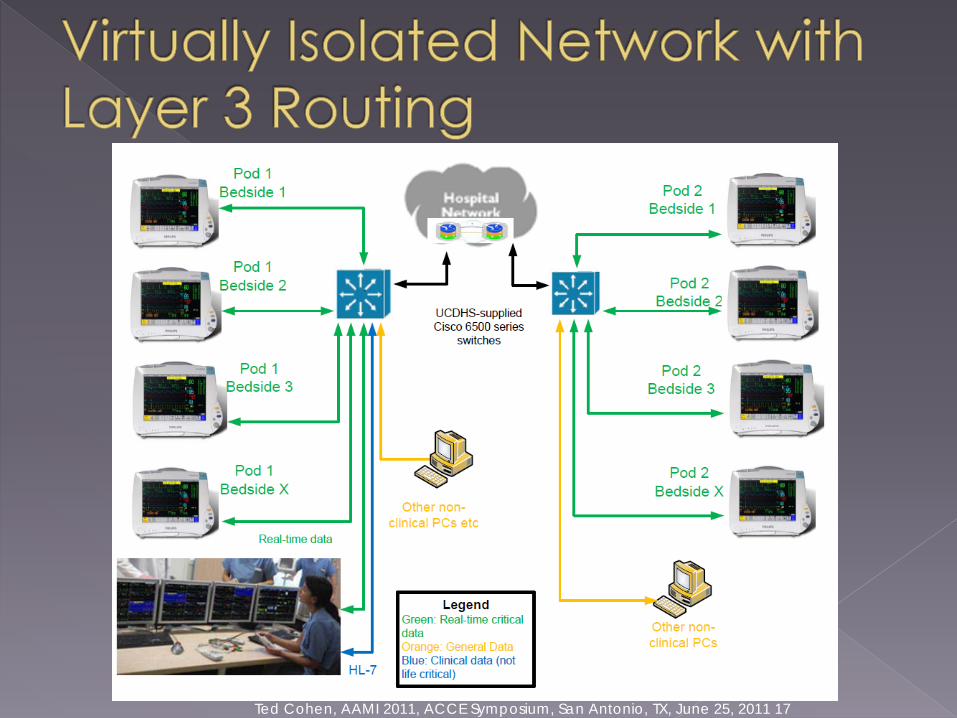
VRF technology allows single router to support multiple virtual routers with simultaneous and independent instances of routing and forwarding tables.
VRFs separate the physical network into secure virtual networks by overlaying logical partitioning mechanisms onto the physical design providing layer 3 path isolation
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 16
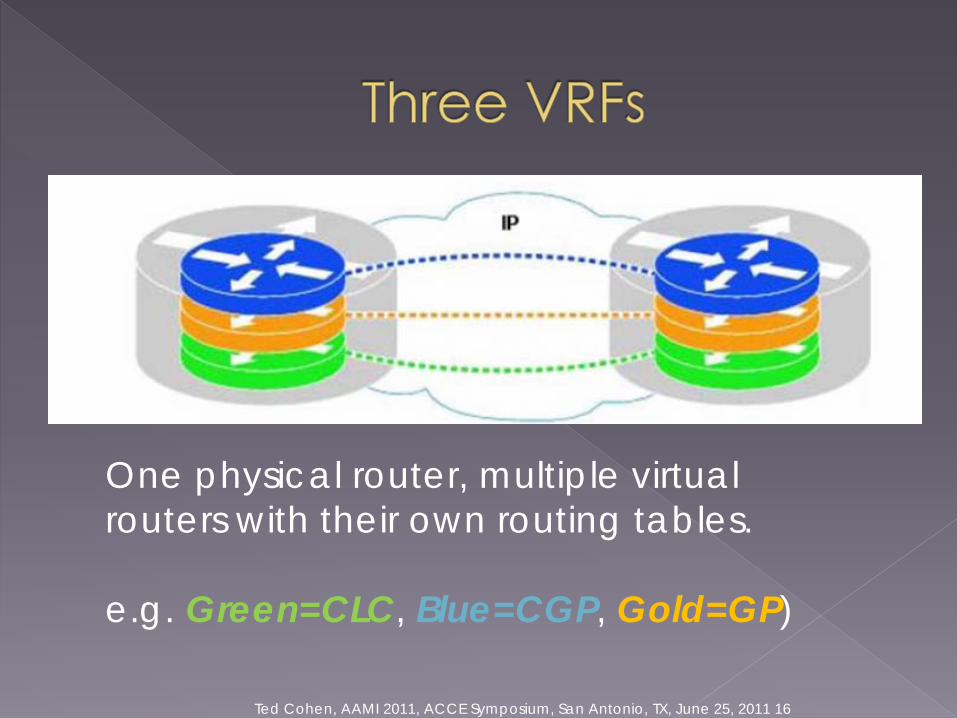
One physical router, multiple virtual routers with their own routing tables.
e.g. Green=CLC, Blue=CGP, Gold=GP)
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 17
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 18
Example: Hemodynamic monitors sending central stations constant stream of ECG and other real-time physiological data.
Timely, reliable, low latency delivery of data for primary clinical alarms.
Applications have only a few seconds to determine critical alarms including bedside, network and central station processing
Relatively low bandwidth, but extremely latency and loss sensitive.

Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 19
FDA/AAMI standard for ECG alarms allots less than a 10 second period of time from the inception of a monitored patient alarm condition to audible/visual central station alarm
Network must reliably and efficiently carry data to the central station, 24 x 7, for multiple bedside monitors
Clinical Engineering determines which networked patient care devices requires “Clinical Life Critical” (CLC) network designation
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 20
QoS: Priority Queues › when there is congestion, what goes first
VRFs (Virtual Routing and Forwarding)› Layer 3 logical segregation
Together with a fast network, they provide capability to reliably communicate a variety of data types at different priority
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 21
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 22
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 23
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 24
Layer 3 routing required if:› Bedsides for one department are connected
on different subnets/networks (e.g. 100 meter cable length restriction)
Network needs to be configured for multicast support (i.e. instead of broadcast, router only sends data to multi-cast group)
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 25
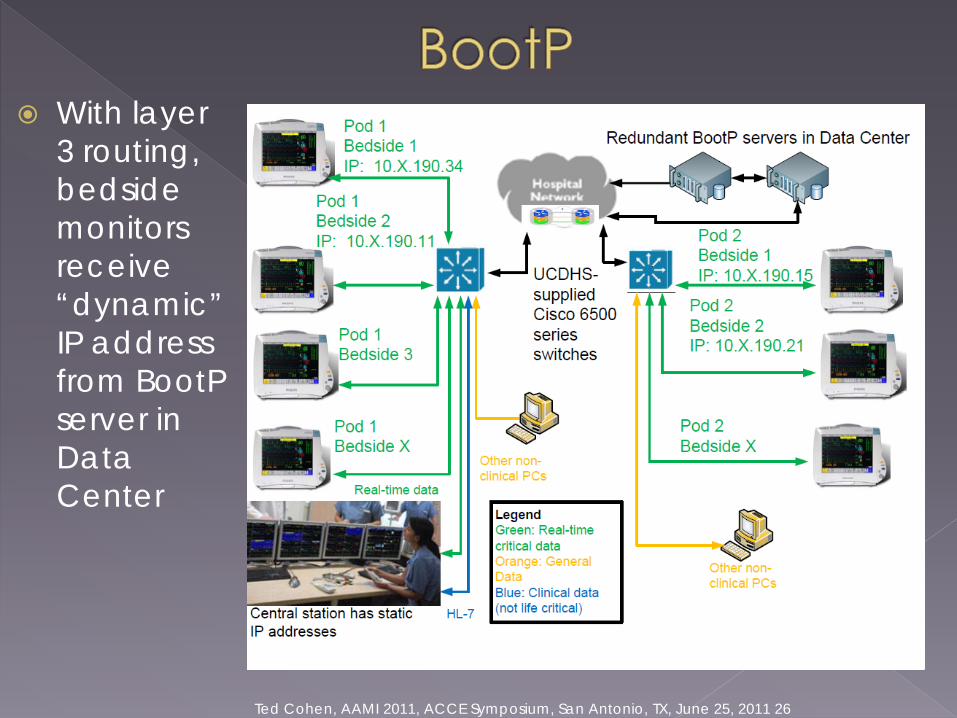
Required if Routed Bedside Monitors (RBM) are on a different subnet from the PIIC (central station computer)
PIIC BOOTP server only provides addresses for its own subnet, therefore the RBM cannot obtain dynamic IP addresses
Therefore, an external DHCP/BOOTP server is required
Note: Some DHCP servers are no longer configured to provide BootP services
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 26
With layer 3 routing, bedside monitors receive “dynamic” IP address from BootP server in Data Center
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 27
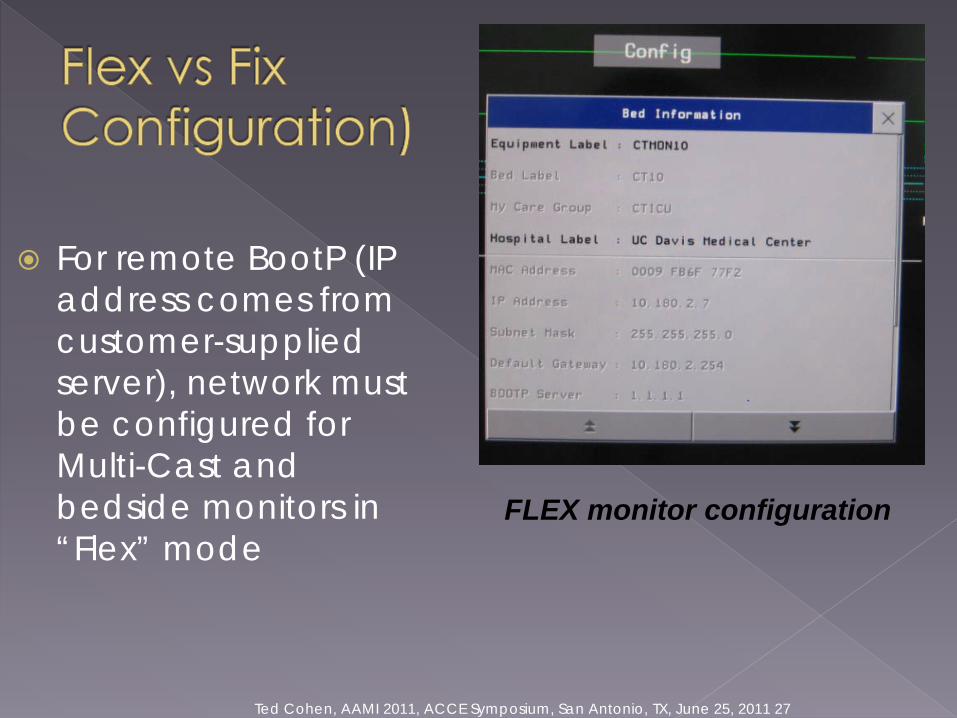
For remote BootP (IP address comes from customer-supplied server), network must be configured for Multi-Cast and bedside monitors in “Flex” mode
FLEX monitor configuration
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 28
Lower hardware costs (eliminates duplicate hardware and cabling)
Common redundant hardware platform Robust, redundant network with logical
isolation, security and relatively easy WAN connectivity
UPS with multiple power sources Upgradable Network
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 29
Common hardware platform: one failure can bring down a LOT of systems
Upgradable Network with FDA devices that may not be compatible with upgrade
Connectivity to network can make system vulnerable to malware
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 30
Understand who has responsibility for what First call Escalation Backup Parts Scheduled Maintenance Regular updates (firmware etc)
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 31
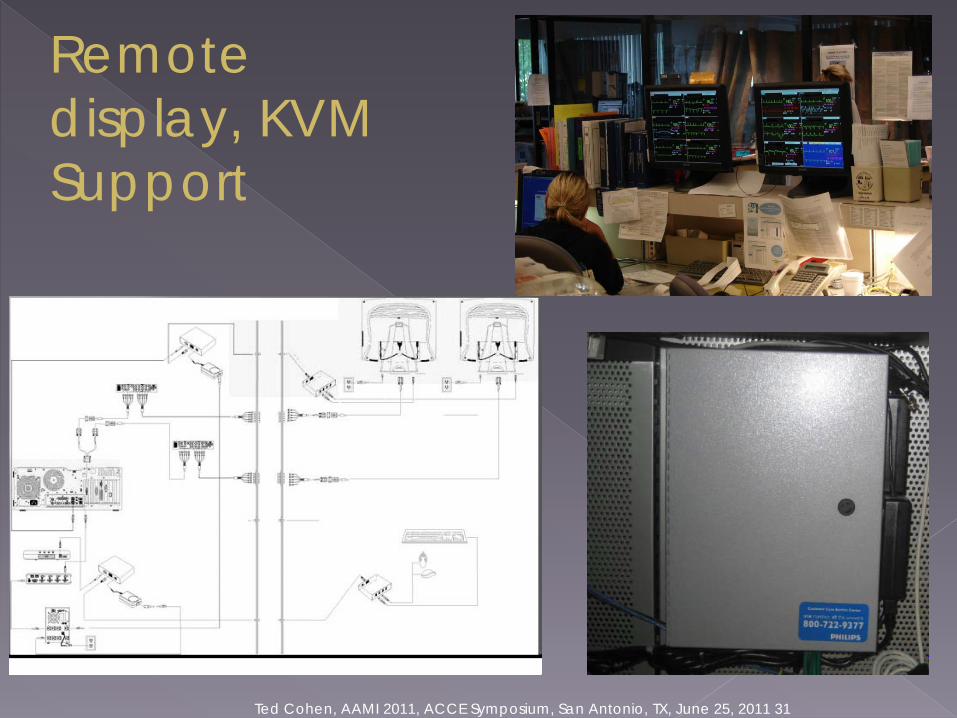
Remote display, KVM Support
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 32
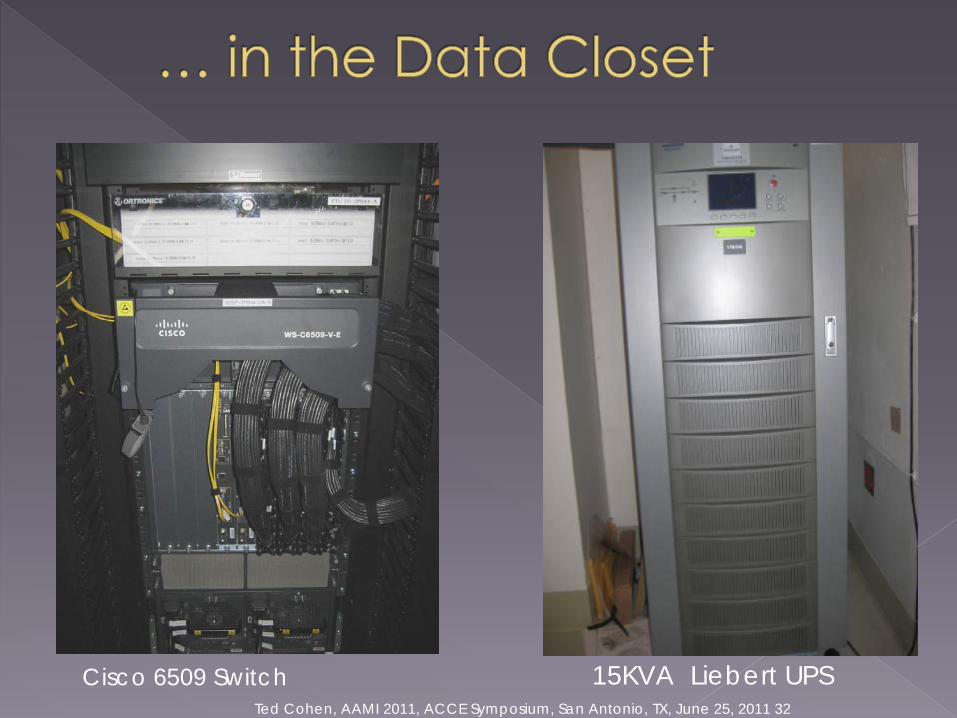
15KVA Liebert UPSCisco 6509 Switch
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 33
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 34
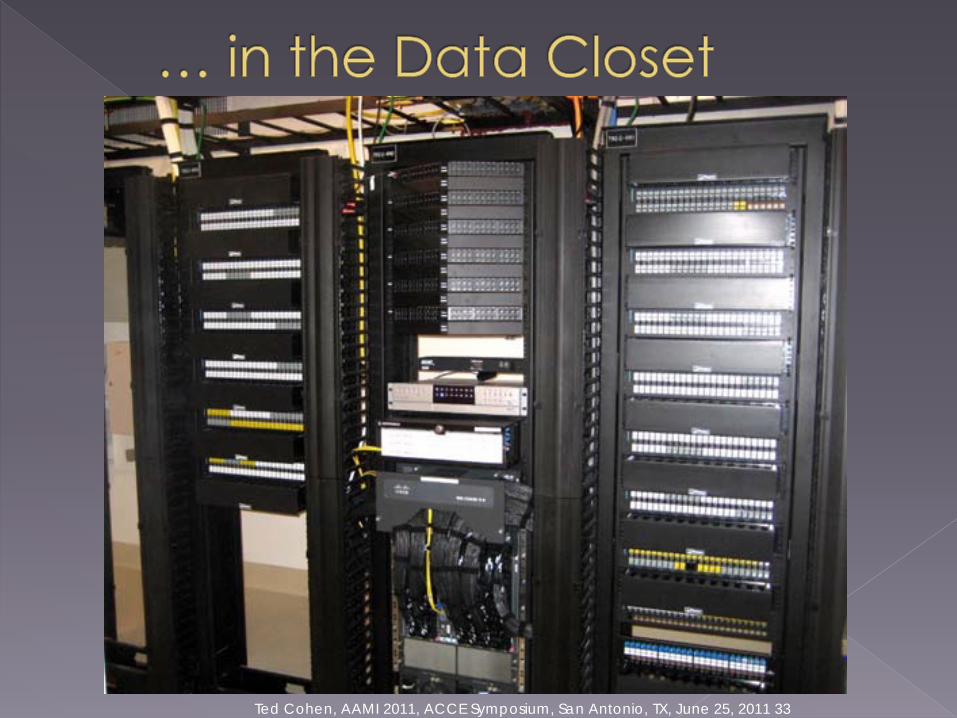
In the Data Closet
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 35
Access security› Configuration security› Configuration change logging
Network perimeter security (firewall/IPS) Restrictions on virus scanning yet
requirements for high-security› Timeouts› Strong passwords with frequent changes› Disable necessary services
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 36
Virus scanning restricted by Philips as follows:› Automated updates must be disabled› Full system scans while PIC is in monitoring mode
are not supported› Directory exclusions are required› Intrusion detection technology (IPS) is not
allowed See Anti-Virus Software on Patient
Monitoring IntelliVue Clinical Network Devices (P/N M3150-91053) for more information
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 37
In a Philips supplied network, no periodic switch maintenance is normally performed
Changes to a hospital's enterprise network are likely to be more frequent
Switch configuration changes must be carefully performed to prevent accidental network outages.
Reboot(s) may be required and take up to 3-4 minutes with no patient monitoring during those times
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 38
Consult with Philips if a major change is planned
Consider a risk assessment update (e.g. IEC 80001)
Develop a “back-out” plan. Understand IIC network topology (e.g.
Switch, IIC and bedsides on same switch, may allow basic monitoring by isolating switch from the rest of network) (Note BootPissue)
Develop a test plan for each planned network change
Document the changes
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 39
One common network hardware platform
High availability including› Fail-over backbone› Fail-over switches› Fail-over UPSs
IT-managed network (they are the experts)
Monitored network (with restrictions) High-security
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 40
High Complexity High availability, but one hardware
platform Vulnerability to downtime problems
during updates Incompatibility between layer 3 routing
and Philips Patient Link (“headless” IIC) product
BootP is obsolete, Philips does not support DHCP
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 41
Obviously, don’t forget patient safety! IEC 80001: New standard for performing risk
assessment on networked medical devices Manufactures and Facilities BOTH have new
responsibilities to provide device integration in a safe manner
Be on the look out for new IEC 80001 guidance documents coming out soon
Pester your manufacturer contacts (BOTH medical and IT) to pay attention to these new standards and guidance documents
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 42
Central station as software only, “thin client” hardware
Philips Patient Link product with layer 3 routing
Improved patient association (e.g., ADT on central station, bar code, proximity RFID)
Ted Cohen, AAMI 2011, ACCE Symposium, San Antonio, TX, June 25, 2011 43

















