Telomerase Expression in Noncancerous Bronchial Epithelia
Is a Possible Marker of Early Development of Lung Cancer
Yuka Matsuoka Miyazu,1,7Teruomi Miyazawa,
1,7Keiko Hiyama,
3Noriaki Kurimoto,
4,8
Yasuo Iwamoto,1Hiroo Matsuura,
2Koji Kanoh,
1Nobuoki Kohno,
5
Masahiko Nishiyama,3and Eiso Hiyama
6
Departments of 1Pulmonary Medicine and 2Pathology, Hiroshima City Hospital; 3Department of Translational Cancer Research,Research Institute for Radiation Biology and Medicine Hiroshima University; 4Department of Surgery, Hiroshima National Hospital;5Department of Molecular and Internal Medicine, Graduate School of Biomedical Sciences; and 6Natural Science Center forBasic Research and Development, Hiroshima University, Hiroshima, Japan; and Departments of 7Respiratory andInfectious Diseases and 8Surgery, St. Marianna University School of Medicine, Kawasaki, Japan
Abstract
Centrally located lung cancers in smokers frequently associ-ated with subsequent primary tumors. We evaluated thetelomerase expression chronologically in noncancerous epi-thelia as a risk factor of susceptibility to lung cancerdevelopment. Telomerase protein expression was examinedin situ by immunohistochemistry in 26 noncancerousbronchial epithelia adjacent to centrally located early-stagelung cancers in sequential 23 patients treated by photody-namic therapy or surgery among 206 patients who under-went autofluorescence bronchoscopy from 1997 to 2003.Among the 15 lesions in 12 patients treated by photodynamictherapy alone, 11 lesions achieved complete remission afterphotodynamic therapy, and none of their noncancerousbronchial epithelia was telomerase positive. On the contrary,in the remaining four lesions, either recurrence or secondarylung cancer developed adjacent to the successfully treatedprimary cancer within 26 months, and the telomeraseprotein expression in noncancerous epithelia was detectedbefore the secondary cancer development (P < 0.001). Theoverall relationship of human telomerase reverse transcrip-tase positivity in noncancerous epithelia and subsequentlung cancer development, including patients treated byradiation or surgery, showed higher significance (P <0.0001). Histologically ‘‘normal’’ bronchial epithelia insmokers may unphysiologically express telomerase as a field,and such epithelia are likely susceptible to develop lungcancer. We propose that ectopic expression of telomerase inbronchial epithelia may precede transformation in humanlung cancer development and that detection of telomeraseprotein in noncancerous bronchial epithelia will become auseful marker detecting high-risk patients for lung cancerdevelopment. (Cancer Res 2005; 65(21): 9623-7)
Introduction
Most patients with centrally located lung cancers have beenexposed to carcinogens in tobacco smoke and frequently develop
subsequent primary and/or multicentric tumors (1, 2). Autofluor-escence bronchoscopy has increased the detection rate of centrallylocated early-stage lung cancers and enhanced opportunities forcurative endobronchial therapeutic strategies, such as photo-dynamic therapy (3, 4), as well as enabling chronologicalobservation of lesion development. Although most of properlyselected candidates for photodynamic therapy have a good thera-peutic outcome, some cases, mainly heavy smokers, develop recur-rence or multiple metachronous cancers shortly after a successfulphotodynamic therapy.Telomerase is expressed in immortal cells and germ line cells
maintaining chromosome termini called telomeres, so that thesecells can proliferate indefinitely (5). Telomerase activity isdetectable in 80% to 90% of human cancer tissues, whereas normaladjacent tissues usually lack measurable activity, indicating thattelomere stability is required for immortalization of cancer cells (6).It is generally believed that activation of telomerase in canceroccurs after many cell divisions through several clonal selections(7). Despite these common understandings, we here propose withevidence that ectopic expression of telomerase in epithelia mayprecede transformation as a field and predispose the lesion tocancer development.
Patients and Methods
We did autofluorescence bronchoscopy in 206 patients at high risk for
developing lung cancer from September 1997 to March 2003 at Hiroshima
City Hospital. When suspicious lesions were detected, patients underwentautofluorescence bronchoscopy every 3 to 6 months. Written informed
consent was obtained from all patients. In 12 patients, 15 lesions have
been treated by photodynamic therapy with curative intent for biopsy-
proven carcinoma in situ or squamous cell carcinomas, which satisfied thecriteria of centrally located early-stage lung cancer and followed without
any other intervention, such as chemotherapy, radiation, or operation
(group P). We confirmed by endobronchial ultrasonography that the depth
of cancer invasion did not extend to the cartilage in all group P cases (4).Among the remaining cases who had a centrally located early-stage lung
cancers, three patients underwent radiation or chemotherapy after
photodynamic therapy (group R) and nine patients underwent surgery(group O), since the cancer invaded beyond the cartilage, and were
followed for >2 years.
Before photodynamic therapy or surgery, at 3-month intervals during thefirst year after the therapy, at 6-month intervals in the second year, and once
a year thereafter, bronchoscopy, including autofluorescence bronchoscopy,
was repeated. Biopsy specimens were taken from all areas suspicious fordysplasia or worse on bronchoscopic examination in addition to a random
biopsy. Routine H&E staining was carried out for all specimens, and the
preserved formalin-fixed, paraffin-embedded specimens available for this
Note: Presented in part at the 13th World Congress for Bronchology, June 20-23,2004, Barcelona, Spain.
Requests for reprints: Eiso Hiyama, Natural Science Center for Basic Research andDevelopment, Hiroshima University, 1-2-3 Kasumi, Minami-ku, Hiroshima, 734-8551Japan. Phone: 81-82-257-5951; Fax: 81-82-257-5219; E-mail: [email protected].
I2005 American Association for Cancer Research.doi:10.1158/0008-5472.CAN-05-0976
www.aacrjournals.org 9623 Cancer Res 2005; 65: (21). November 1, 2005
study were stained by immunohistochemistry using a polyclonal antibody
against human telomerase reverse transcriptase (hTERT; EST21A, Alpha
Diagnostic International, San Antonio TX) as previously described (8).
Telomerase protein expression was evaluated as positive when nuclear
staining was confirmed by two molecular oncologists, in a blinded manner
by one and confirmed by another.
Statistical analysis on the relationship between hTERT positivity in
noncancerous epithelia and subsequent lung cancer development was
carried out using Fisher’s exact test. This study was approved by our
institutional ethics committee.
Result
In group P, 11 of 15 lesions treated by photodynamic therapy innine patients achieved complete remission (CR) with a medianfollow-up term of 52 months after photodynamic therapy. In theremaining four lesions, either recurrence (case 1) or secondarylung cancer (cases 2-4) developed adjacent to the successfully
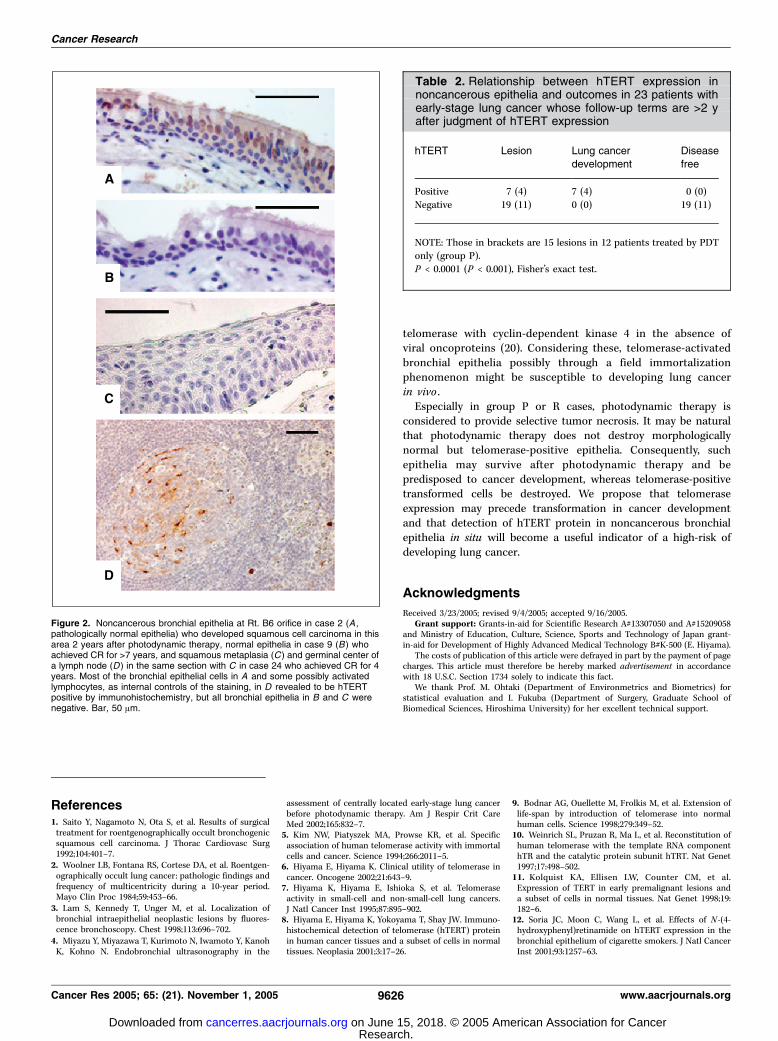
treated primary cancer within 26 months (Table 1). Theimmunohistochemistry of noncancerous bronchial biopsy speci-mens in cases 1 to 4 showed positive telomerase proteinexpression in the nuclei of adjacent bronchial epithelia diagnosedas ‘‘normal’’ or atypical epithelia by H&E staining before cancerdevelopment (Fig. 1F and Fig. 2A), and greater parts of thesubsequently developed cancers were telomerase positive (Fig. 1I).However, all of the remaining 11 lesions repeatedly examinedbefore photodynamic therapy and during the follow-up term innine patients that achieved CR after photodynamic therapyshowed no telomerase protein expression in noncancerousepithelia (Fig. 2B ; Table 2, in brackets; P < 0.001).To investigate this relationship further, we additionally
examined 11 patients who underwent radiation or chemotherapyafter photodynamic therapy (group R) or operation (group O) andwere followed for >2 years. Also in group R, case 13, whoseadjacent noncancerous epithelia was positive for hTERT expres-sion, developed secondary cancer after photodynamic therapy
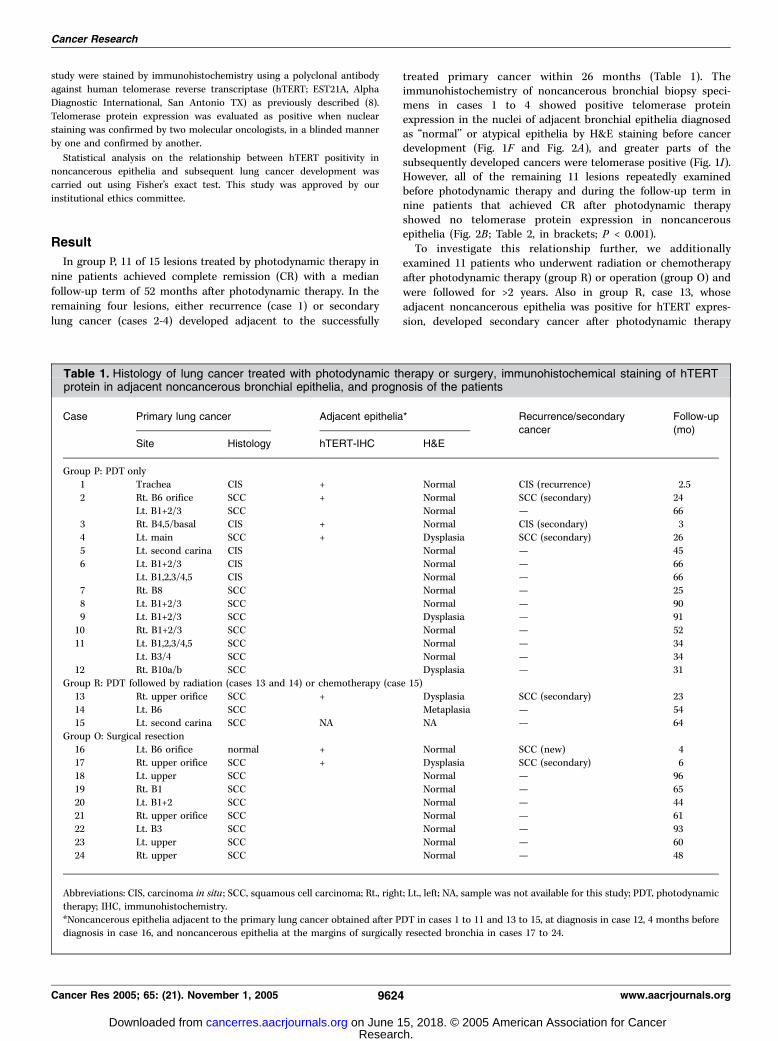
Table 1. Histology of lung cancer treated with photodynamic therapy or surgery, immunohistochemical staining of hTERTprotein in adjacent noncancerous bronchial epithelia, and prognosis of the patients
Case Primary lung cancer Adjacent epithelia* Recurrence/secondary
cancer
Follow-up
(mo)
Site Histology hTERT-IHC H&E
Group P: PDT only
1 Trachea CIS + Normal CIS (recurrence) 2.5
2 Rt. B6 orifice SCC + Normal SCC (secondary) 24
Lt. B1+2/3 SCC � Normal — 663 Rt. B4,5/basal CIS + Normal CIS (secondary) 3
4 Lt. main SCC + Dysplasia SCC (secondary) 26
5 Lt. second carina CIS � Normal — 45
6 Lt. B1+2/3 CIS � Normal — 66Lt. B1,2,3/4,5 CIS � Normal — 66
20 Lt. B1+2 SCC � Normal — 4421 Rt. upper orifice SCC � Normal — 61
22 Lt. B3 SCC � Normal — 93
23 Lt. upper SCC � Normal — 60
24 Rt. upper SCC � Normal — 48
Abbreviations: CIS, carcinoma in situ ; SCC, squamous cell carcinoma; Rt., right; Lt., left; NA, sample was not available for this study; PDT, photodynamic
therapy; IHC, immunohistochemistry.
*Noncancerous epithelia adjacent to the primary lung cancer obtained after PDT in cases 1 to 11 and 13 to 15, at diagnosis in case 12, 4 months before
diagnosis in case 16, and noncancerous epithelia at the margins of surgically resected bronchia in cases 17 to 24.
Cancer Research
Cancer Res 2005; 65: (21). November 1, 2005 9624 www.aacrjournals.org
and radiation therapy, whereas case 14 without hTERTexpression in noncancerous epithelia did not. In group O, case16 developed the first lung cancer 4 months after the biopsy ofnormal epithelia with positive hTERT protein. In the remainingeight cases, we examined hTERT protein expression in noncan-cerous epithelia at surgical margins in the resected tissues, sothat the hTERT protein expression status at the margins ofnoncancerous epithelia remained in patients after surgery couldbe inferred. The case 17 with positive hTERT expression innoncancerous epithelia developed secondary squamous cellcarcinoma at this region, whereas the remaining seven caseswithout hTERT expression (Fig. 2C) remain disease free untilnow. Including these groups R and O, the overall relationshipbetween hTERT positivity in noncancerous epithelia andsubsequent lung cancer development was summarized in Table2 and revealed to be highly significant (n = 26, P < 0.0001) byFisher’s exact test.
Discussion
In the present study, we evaluated the expression of hTERTprotein in the bronchial epithelia in situ . The hTERT protein, acatalytic reverse transcriptase, and a 451-bp template RNA(human telomerase RNA) are essential components of telomerasethat endow human cells with immortalization (9, 10). Amongthese components, human telomerase RNA is known to beconstitutively expressed even in cells without telomerase activity(10). Then, the detection of hTERT mRNA has been used as anindicator of positive telomerase activity, including in bronchial
epithelia (11–14). However, it was proved that hTERT mRNA isoften alternatively spliced, prohibiting the expression of hTERTprotein in a dominant-negative manner (15). Moreover, detectionof telomerase activity in clinical materials without in situanalysis may cause a false positive due to the infiltrated lym-phocytes (16). Thus, detection of human telomerase RNA overex-pression (17), hTERT mRNA expression (12–14), or telomeraseactivity without in situ evaluation (13, 17, 18) in noncancerousbronchial epithelia or lung tissues in smokers might haverepresented the expression of an alternatively spliced dominant-negative form of hTERT mRNA or lymphocyte inflammationrather than substantial telomerase expression in epithelia insome cases.Telomerase activation in solid tumors has been considered to
occur after many cell divisions through several clonal selections(7). However, cases 1 to 4, 13, 16, and 17, all heavy smokers,showed expression of telomerase protein in noncancerousepithelia as a field before the development of cancer. Onepossible explanation for this finding may be ‘‘field immortali-zation’’ in the bronchial epithelia in heavy smokers, in a mannersimilar to ‘‘field cancerization’’ as a step of carcinogenesis. Thefact that majority of cancer cells in subsequently developedcancers showed positive telomerase protein even at an earlystage, whereas it is uncommon in non–small cell lung cancers(7), supports our hypothesis that the second cancers havedeveloped from the telomerase-positive epithelia. Recently, itwas proved in vitro that once telomerase is activated, humancells are susceptible to transformation (19), and humanbronchial epithelial cells can be immortalized by activation of
Figure 1. Case 1. Lower tracheaexamined by autofluorescencebronchoscopy (A, D , and G) and tracheaepithelia with H&E staining (B, E , and H )and with immunohistochemistry usinghTERT antibody (C, F , and I ). Carcinomain situ and adjacent atypical lesion beforephotodynamic therapy (B and C ) witha wide area of decreased greenautofluorescence by autofluorescencebronchoscopy (A ), stratified ciliatedcolumnar cells without atypia 4 weeksafter successful photodynamic therapy(E and F ) with normal greenautofluorescence (D ), and carcinomain situ as well as the superficial normalciliated columnar cells 10 weeks afterphotodynamic therapy (H and I)with marked dark red findings byautofluorescence bronchoscopy (G) wereall hTERT positive. Bar, 50 Am.
Lung Cancer Preceded by Telomerase Expression
www.aacrjournals.org 9625 Cancer Res 2005; 65: (21). November 1, 2005
telomerase with cyclin-dependent kinase 4 in the absence ofviral oncoproteins (20). Considering these, telomerase-activatedbronchial epithelia possibly through a field immortalizationphenomenon might be susceptible to developing lung cancerin vivo .Especially in group P or R cases, photodynamic therapy is
considered to provide selective tumor necrosis. It may be naturalthat photodynamic therapy does not destroy morphologicallynormal but telomerase-positive epithelia. Consequently, suchepithelia may survive after photodynamic therapy and bepredisposed to cancer development, whereas telomerase-positivetransformed cells be destroyed. We propose that telomeraseexpression may precede transformation in cancer developmentand that detection of hTERT protein in noncancerous bronchialepithelia in situ will become a useful indicator of a high-risk ofdeveloping lung cancer.
Acknowledgments
Received 3/23/2005; revised 9/4/2005; accepted 9/16/2005.Grant support: Grants-in-aid for Scientific Research A#13307050 and A#15209058
and Ministry of Education, Culture, Science, Sports and Technology of Japan grant-in-aid for Development of Highly Advanced Medical Technology B#K-500 (E. Hiyama).
The costs of publication of this article were defrayed in part by the payment of pagecharges. This article must therefore be hereby marked advertisement in accordancewith 18 U.S.C. Section 1734 solely to indicate this fact.
We thank Prof. M. Ohtaki (Department of Environmetrics and Biometrics) forstatistical evaluation and I. Fukuba (Department of Surgery, Graduate School ofBiomedical Sciences, Hiroshima University) for her excellent technical support.
Figure 2. Noncancerous bronchial epithelia at Rt. B6 orifice in case 2 (A ,pathologically normal epithelia) who developed squamous cell carcinoma in thisarea 2 years after photodynamic therapy, normal epithelia in case 9 (B ) whoachieved CR for >7 years, and squamous metaplasia (C ) and germinal center ofa lymph node (D ) in the same section with C in case 24 who achieved CR for 4years. Most of the bronchial epithelial cells in A and some possibly activatedlymphocytes, as internal controls of the staining, in D revealed to be hTERTpositive by immunohistochemistry, but all bronchial epithelia in B and C werenegative. Bar, 50 Am.
Table 2. Relationship between hTERT expression innoncancerous epithelia and outcomes in 23 patients withearly-stage lung cancer whose follow-up terms are >2 yafter judgment of hTERT expression
hTERT Lesion Lung cancer
development
Disease
free
Positive 7 (4) 7 (4) 0 (0)
Negative 19 (11) 0 (0) 19 (11)
NOTE: Those in brackets are 15 lesions in 12 patients treated by PDTonly (group P).
P < 0.0001 (P < 0.001), Fisher’s exact test.
References1. Saito Y, Nagamoto N, Ota S, et al. Results of surgicaltreatment for roentgenographically occult bronchogenicsquamous cell carcinoma. J Thorac Cardiovasc Surg1992;104:401–7.
2. Woolner LB, Fontana RS, Cortese DA, et al. Roentgen-ographically occult lung cancer: pathologic findings andfrequency of multicentricity during a 10-year period.Mayo Clin Proc 1984;59:453–66.
3. Lam S, Kennedy T, Unger M, et al. Localization ofbronchial intraepithelial neoplastic lesions by fluores-cence bronchoscopy. Chest 1998;113:696–702.
4. Miyazu Y, Miyazawa T, Kurimoto N, Iwamoto Y, KanohK, Kohno N. Endobronchial ultrasonography in the
assessment of centrally located early-stage lung cancerbefore photodynamic therapy. Am J Respir Crit CareMed 2002;165:832–7.
5. Kim NW, Piatyszek MA, Prowse KR, et al. Specificassociation of human telomerase activity with immortalcells and cancer. Science 1994;266:2011–5.
6. Hiyama E, Hiyama K. Clinical utility of telomerase incancer. Oncogene 2002;21:643–9.
7. Hiyama K, Hiyama E, Ishioka S, et al. Telomeraseactivity in small-cell and non-small-cell lung cancers.J Natl Cancer Inst 1995;87:895–902.
8. Hiyama E, Hiyama K, Yokoyama T, Shay JW. Immuno-histochemical detection of telomerase (hTERT) proteinin human cancer tissues and a subset of cells in normaltissues. Neoplasia 2001;3:17–26.
9. Bodnar AG, Ouellette M, Frolkis M, et al. Extension oflife-span by introduction of telomerase into normalhuman cells. Science 1998;279:349–52.
10. Weinrich SL, Pruzan R, Ma L, et al. Reconstitution ofhuman telomerase with the template RNA componenthTR and the catalytic protein subunit hTRT. Nat Genet1997;17:498–502.
11. Kolquist KA, Ellisen LW, Counter CM, et al.Expression of TERT in early premalignant lesions anda subset of cells in normal tissues. Nat Genet 1998;19:182–6.
12. Soria JC, Moon C, Wang L, et al. Effects of N -(4-hydroxyphenyl)retinamide on hTERT expression in thebronchial epithelium of cigarette smokers. J Natl CancerInst 2001;93:1257–63.
Cancer Research
Cancer Res 2005; 65: (21). November 1, 2005 9626 www.aacrjournals.org
13. Shibuya K, Fujisawa T, Hoshino H, et al.Increased telomerase activity and elevated hTERTmRNA expression during multistage carcinogenesis ofsquamous cell carcinoma of the lung. Cancer 2001;92:849–55.
14. Soria JC, Xu X, Liu DD, et al. Retinoic acid receptor hand telomerase catalytic subunit expression in bronchialepithelium of heavy smokers. J Natl Cancer Inst 2003;95:165–8.
15. Ulaner GA, Hu JF, Vu TH, Giudice LC, Hoffman AR.Tissue-specific alternate splicing of human telomerase
reverse transcriptase (hTERT) influences telomerelengths during human development. Int J Cancer 2001;91:644–9.
16. Hiyama K, Hirai Y, Kyoizumi S, et al. Activation oftelomerase in human lymphocytes and hematopoieticprogenitor cells. J Immunol 1995;155:3711–5.
17. Yashima K, Litzky LA, Kaiser L, et al. Telomeraseexpression in respiratory epithelium during the multi-stage pathogenesis of lung carcinomas. Cancer Res 1997;57:2373–7.
18. Gonzalez-Quevedo R, Iniesta P, Moran A, et al.
Cooperative role of telomerase activity and p16expression in the prognosis of non-small-cell lungcancer. J Clin Oncol 2002;20:254–62.
19. Stewart SA, Hahn WC, O’Connor BF, et al. Telomer-ase contributes to tumorigenesis by a telomere length-independent mechanism. Proc Natl Acad Sci U S A 2002;99:12606–11.
20. Ramirez RD, Sheridan S, Girard L, et al. Immortal-ization of human bronchial epithelial cells in theabsence of viral oncoproteins. Cancer Res 2004;64:9027–34.
Lung Cancer Preceded by Telomerase Expression
www.aacrjournals.org 9627 Cancer Res 2005; 65: (21). November 1, 2005
2005;65:9623-9627. Cancer Res Yuka Matsuoka Miyazu, Teruomi Miyazawa, Keiko Hiyama, et al. Is a Possible Marker of Early Development of Lung CancerTelomerase Expression in Noncancerous Bronchial Epithelia