Annals of the Rheumatic Diseases 1992; 51: 797-802 Aberrant cytokine production from tenosynovium in dialysis associated amyloidosis Nobuyuki Miyasaka, Kazuto Sato, Yuri Kitano, Megumu Higaki, Kusuki Nishioka, Kazuo Ohta Department of Immunological Diseases, Medical Research Institute, Tokyo Medical and Dental University, Tokyo, Japan N Miyasaka M Higaki Institute of Rheumatology, Tokyo Women's Medical College, Tokyo, Japan K Sato K Nishioka Institute of Nephrology, Tokyo Women's Medical Coliege, Tokyo, Japan Y Kitano K Ohta Correspondence to: Dr Nobuyuki Miyasaka, Department of Immunological Diseases, Medical Research Institute, Tokyo Medical and Dental University, 1-5-45, Yushima, Bunkyo-ku, Tokyo, Japan 113. Accepted for publication 8 November 1991 Abstract Culture supernatants of tenosynovial tissues from patients with carpal tunnel syndrome undergoing chronic haemodialysis contained interleukin (IL) 1-like and IL6-like activity. These culture supernatants also induced active proliferation of rheumatoid synovial cells. Immunohistochemical analysis of teno- synovial tissues showed the accumulation of mononuclear cells bearing CD14 and HLA- DR antigens adjacent to the deposition of amyloid protein ((32 microglobulin). These cells also reacted with antibodies to ILl and IL6 respectively. These data suggest that multiple cytokines, including ILI and IL6, produced from tenosynovial tissues in patients with dialysis associated amyloidosis might induce the proliferation of synovial cells that, together with deposition of amyloid protein, might cause carpal tunnel syndrome. Carpal tunnel syndrome is often found in patients undergoing long term haemodialysis.' There is a positive correlation between the incidence of carpal tunnel syndrome and the duration of haemodialysis.2 Patients who undergo haemodialysis for more than 15 years are always affected by carpal tunnel syndrome.3 Deposition of amyloid protein in the carpal tunnel area is believed to cause compression of the median nerve resulting in carpal tunnel syndrome,4 a clinical condition referred to as dialysis associated amyloidosis. The major component of amyloid protein in this situation was found by Gejyo et al 5 to be (2 micro- globulin, a low molecular weight amyloidogenic protein (molecular weight 11 8 kilodaltons)6 that cannot be removed by conventional haemodialysis. In addition to amyloid deposition, however, we found the proliferation of synovial cells in biopsy samples of tenosynovial tissues from the carpal tunnel area of patients undergoing long term haemodialysis and therefore reconsidered whether carpal tunnel syndrome is solely attri- butable to the local deposition of (32 micro- globulin. We report here the augmented production of cytokines with activities of inter- leukin (IL) 1 and IL6 from biopsy samples of tenosynovial tissues from the carpal tunnel area and speculate that cytokines produced in situ might be responsible for the proliferation in tenosynovial tissues which subsequently causes carpal tunnel syndrome. We also suggest that local accumulation of (32 microglobulin might stimulate synovial cells to induce constitutive production of cytokines from tenosynovial tissues. Patients and methods PATIENTS Fifteen patients with carpal tunnel syndrome undergoing long term haemodialysis (mean duration 10-4 years) were selected for the study (table 1). Informed consent was obtained from all patients. Surgical decompression of the median nerve was performed and biopsy samples of tenosynovial tissues were taken at the same time from the carpal tunnel area without complications. These samples were used for assays of cytokine activity and immuno- histochemical staining. Tenosynovial tissues obtained from eight patients with trauma were used as controls. Table 1 Cytokine production from tenosynovial tissues of patients wnth haemodialysis associated amyloidosis and carpal tunnel syndrome Patient Age Sex Cause of Cytokine production (Ulml) No (years) renal failure* ILif IL6t 1 42 F CGN 97 165 2 69 M CGN 137 115 3 64 M CGN 37 180 4 52 F CGN 62 110 5 63 M DM 12 100 6 37 M CGN 12 115 7 65 M CGN 21 150 8 48 M CGN 0 20 9 55 M CGN 10 0 10 58 F CGN 0 57 11 66 M CGN 0 58 12 49 F CGN 128 81 13 47 M CGN 135 28 14 54 F CGN 30 123 15 59 M CGN 42 55 *(CGN) chronic glomerulonephritis; (DM) diabetes mellitus. tMeasured using A375 melanoma cell line. fMeasured using SKW-C1-4 cell line. CULTURES Biopsy samples were processed as reported previously.7 Briefly, biopsy specimens were dissected into fragments 3 mm in diameter, washed extensively with RPMI 1640 (Gibco, Grand Island, NY, USA) and a fragment was plated into each well in 24 well culture plates (Sumitomo, Japan) as an organ culture with RPMI 1640 supplemented with 10% heat inactivated fetal calf serum (Gibco), 100 U/ml penicillin, 100 ,ug/ml streptomycin, and 10 mM HEPES. Cultures for ILl and IL6 were performed as described in the following. MEASUREMENT OF ILl ACTIVITY Interleukin 1 activity was measured by a growth inhibition assay using the melanoma cell line 797 on 12 June 2018 by guest. Protected by copyright. http://ard.bmj.com/ Ann Rheum Dis: first published as 10.1136/ard.51.6.797 on 1 June 1992. Downloaded from
Transcript
Annals of the Rheumatic Diseases 1992; 51: 797-802
Aberrant cytokine production from tenosynoviumin dialysis associated amyloidosis
Department ofImmunological Diseases,Medical ResearchInstitute,Tokyo Medical andDental University,Tokyo, JapanN MiyasakaM HigakiInstitute ofRheumatology,Tokyo Women'sMedical College,Tokyo, JapanK SatoK NishiokaInstitute ofNephrology, TokyoWomen's MedicalColiege, Tokyo,JapanY KitanoK OhtaCorrespondence to:Dr Nobuyuki Miyasaka,Department ofImmunological Diseases,Medical ResearchInstitute, Tokyo Medicaland Dental University,1-5-45, Yushima,Bunkyo-ku, Tokyo,Japan 113.Accepted for publication8 November 1991
AbstractCulture supernatants of tenosynovial tissuesfrom patients with carpal tunnel syndromeundergoing chronic haemodialysis containedinterleukin (IL) 1-like and IL6-like activity.These culture supernatants also inducedactive proliferation of rheumatoid synovialcells. Immunohistochemical analysis of teno-synovial tissues showed the accumulation ofmononuclear cells bearing CD14 and HLA-DR antigens adjacent to the deposition ofamyloid protein ((32 microglobulin). Thesecells also reacted with antibodies to ILl andIL6 respectively. These data suggest thatmultiple cytokines, including ILI and IL6,produced from tenosynovial tissues in patientswith dialysis associated amyloidosis mightinduce the proliferation of synovial cells that,together with deposition of amyloid protein,might cause carpal tunnel syndrome.
Carpal tunnel syndrome is often found inpatients undergoing long term haemodialysis.'There is a positive correlation between theincidence of carpal tunnel syndrome and theduration of haemodialysis.2 Patients whoundergo haemodialysis for more than 15 yearsare always affected by carpal tunnel syndrome.3Deposition of amyloid protein in the carpaltunnel area is believed to cause compression ofthe median nerve resulting in carpal tunnelsyndrome,4 a clinical condition referred to asdialysis associated amyloidosis. The majorcomponent of amyloid protein in this situationwas found by Gejyo et al 5 to be (2 micro-globulin, a low molecular weight amyloidogenicprotein (molecular weight 11 8 kilodaltons)6
that cannot be removed by conventionalhaemodialysis.
In addition to amyloid deposition, however,we found the proliferation of synovial cells inbiopsy samples of tenosynovial tissues from thecarpal tunnel area of patients undergoing longterm haemodialysis and therefore reconsideredwhether carpal tunnel syndrome is solely attri-butable to the local deposition of (32 micro-globulin. We report here the augmentedproduction of cytokines with activities of inter-leukin (IL) 1 and IL6 from biopsy samples oftenosynovial tissues from the carpal tunnel areaand speculate that cytokines produced in situmight be responsible for the proliferation intenosynovial tissues which subsequently causescarpal tunnel syndrome. We also suggest thatlocal accumulation of (32 microglobulin mightstimulate synovial cells to induce constitutiveproduction of cytokines from tenosynovialtissues.
Patients and methodsPATIENTSFifteen patients with carpal tunnel syndromeundergoing long term haemodialysis (meanduration 10-4 years) were selected for the study(table 1). Informed consent was obtained fromall patients. Surgical decompression of themedian nerve was performed and biopsysamples of tenosynovial tissues were taken atthe same time from the carpal tunnel areawithout complications. These samples wereused for assays of cytokine activity and immuno-histochemical staining. Tenosynovial tissuesobtained from eight patients with trauma wereused as controls.
Table 1 Cytokine production from tenosynovial tissues of patients wnth haemodialysisassociated amyloidosis and carpal tunnel syndrome
Patient Age Sex Cause of Cytokine production (Ulml)No (years) renal failure*
ILif IL6t
1 42 F CGN 97 1652 69 M CGN 137 1153 64 M CGN 37 1804 52 F CGN 62 1105 63 M DM 12 1006 37 M CGN 12 1157 65 M CGN 21 1508 48 M CGN 0 209 55 M CGN 10 010 58 F CGN 0 5711 66 M CGN 0 5812 49 F CGN 128 8113 47 M CGN 135 2814 54 F CGN 30 12315 59 M CGN 42 55
*(CGN) chronic glomerulonephritis; (DM) diabetes mellitus.tMeasured using A375 melanoma cell line.fMeasured using SKW-C1-4 cell line.
CULTURESBiopsy samples were processed as reportedpreviously.7 Briefly, biopsy specimens weredissected into fragments 3 mm in diameter,washed extensively with RPMI 1640 (Gibco,Grand Island, NY, USA) and a fragment wasplated into each well in 24 well culture plates(Sumitomo, Japan) as an organ culture withRPMI 1640 supplemented with 10% heatinactivated fetal calf serum (Gibco), 100 U/mlpenicillin, 100 ,ug/ml streptomycin, and 10 mMHEPES. Cultures for ILl and IL6 wereperformed as described in the following.
MEASUREMENT OF ILl ACTIVITYInterleukin 1 activity was measured by a growthinhibition assay using the melanoma cell line
797
on 12 June 2018 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.51.6.797 on 1 June 1992. D
A375.' ' Briefly, A375 cells were plated into 96well flat bottom culture plates (1xl 104/well) inEagle's minimal essential medium supplementedwith 10% fetal calf serum with various dilutionsof test samples or recombinant IL1,. After fourdays' incubation at 37°C, 0-5% neutral red wasadded to each well. Neutral red incorporated inviable cells was extracted with ethanol after twohours of culture. The absorbance of each wellwas measured at 540 nm by a multiscanspectrophotometer. One unit of growthinhibitory factor per millilitre represented thereciprocal of the dilution of samples causing50% cytostasis or cytolysis after four days ofculture, which is equivalent to the activityexerted by 50 pg/ml of recombinant IL113. Inpreliminary experiments, recombinant ILlaactivity was blocked by antibodies to humanILla, and recombinant IL,13 activity wasneutralised by antibodies to human IL1I3. Thespecificity of the assay was further confirmed byusing recombinant human tumour necrosisfactor a, IL2, and IL6. With this assay, 2-1000pg/ml of ILl was detectable. In addition, athymocyte proliferation assay was used toconfirm ILl activity.'0 One ILl unit in thisassay is defined as the half maximum responseof thymocytes to recombinant human IL113. Anenzyme linked immunosorbent assay (ELISA)for ILI1 was also performed in some of thesamples using a commercial kit (Ohtsuka AssayCo. Ltd, Japan)."
In part of the experiments using the A375 cellline, samples with known IL1-like activity wereadded to A375 cells with either polyclonalantibodies to human ILla (1:400 dilution),antibodies to ILl1 (1:400), or an equivalentdose of normal rabbit IgG to determine whethertheir IL1-like activity in the samples wasneutralised by these antibodies. These antibodieshave been described in detail elsewhere. "l
In addition, part of the samples with increasedIL1 activity were preincubated for two hours at37°C in the presence or absence of 5 [tg ofpolymyxin B (Pfizer, New York, NY, USA) toremove any lipopolysaccharide in the samples.
MEASUREMENT OF IL6 ACTIVITYInterleukin 6 activity was determined with anEpstein-Barr virus transformed B cell line,SKW-C1-4, as described previously.'2 Briefly,1 x 104 cells/200 dl/well were cultured with testsamples or recombinant IL6 for four days, andthe concentration of IgM in the culture super-natants was determined by an ELISA. Inter-leukin 6 activity was also measured using theIL6 dependent murine hybridoma MH60.BSF2cell clone. '3 The growth of MH60.BSF2 cellswas dependent on IL6; none of the otherlymphokines examined (human ILla, IL13,IL3, IL4, interferon y, interferon a, or granulo-cyte colony stimulating factor supported thegrowth of this clone. MH6O.BSF2 cells (1 x i04cells/200 [il/well) were cultured with variousconcentrations of test samples or recombinantIL6 for 48 hours, and DNA synthesis wasmeasured by a spectrophotometric assay using3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetra-zolium bromide. 4 In some of the experiments,
MH60.BSF2 cells were cultured with the testsample together with the IgG fraction ofantibodies to IL6 or preimmune rabbit serum todetermine whether IL6-like activity was neu-tralised.
ASSAY FOR SYNOVIAL CELL GROWTH PROMOTINGACTIVITYA source of synovial cells was derived fromrheumatoid synovium as sufficient amounts ofsynovial cells were not obtained from normalsynovium. The synovial tissue obtained byarthroscopic synovectomy from the knee jointsof a patient with rheumatoid arthritis wasminced, washed extensively with phosphatebuffered saline (PBS), and treated with PBSplus 0-25% trypsin for 40 minutes at 37TC.'5The cells were washed three times with PBS andfinally suspended in HAM F-12 medium(Gibco) supplemented with 10% fetal calfserum, 5 x 10-5 M 2-mercaptoethanol, 100 U/mlpenicillin, and 100 ig/ml streptomycin. Thecells were incubated in culture flasks untilconfluence, then treated with 0-05% trypsin forfive minutes at room temperature. Morpho-logically, most of these cells were fibroblast-likecells. After they were adjusted to 2x i04 cells/mlwith 10% fetal calf serum-RPMI 1640, 100 ,ul ofthe cell suspension was plated in 96 well cultureplates with various concentrations of testsamples or recombinant IL1I3 for 72 hours, andneutral red uptake was measured by the methoddescribed earlier.
IMMUNOHISTOCHEMICAL ANALYSISImmunohistochemical staining was performedas described previously.7 In brief, specimensembedded in OCT medium (Miles, Naperville,IL, USA) were frozen in liquid nitrogen andstored at - 70°C. Frozen tissues were fixed withacetone and stained by monoclonal or polyclonalantibodies as described below. Antibodies toCD2, CD4, CD8, CD20, CD21 (reactive with Bcells), I2 (reactive with HLA-DR antigens),CD13 (reactive with myelocytes, granulocytes,and monocytes), and CD14 (reactive withmonocytes and macrophages) were all fromCoulter Immunology (Hialeah, FL, USA). Thetissue sections were incubated with a specificantibody or a control antibody of the sameisotype. After rinsing, the sections were reactedwith a serum sample containing biotinylatedgoat antimouse (IgG plus IgM) antibodies(Tago, Burlingame, CA, USA), followed byavidin-biotin complex (Vector Laboratories,Burlingame, CA, USA) and then the substrate,3', 3'-diaminobenzidine. When rabbit antibodiesto human IL1I3 (OCT204) or IL6 was used, thesections were reacted with the serum samplecontaining biotinylated goat antirabbit (IgGplus IgM) antibodies, followed by avidin-biotincomplex.
STATISTICAL ANALYSISStatistical analysis was performed by Wilcoxon'srank sum test.
798
on 12 June 2018 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.51.6.797 on 1 June 1992. D
Cytokine production in dialysis associated amyloidosis
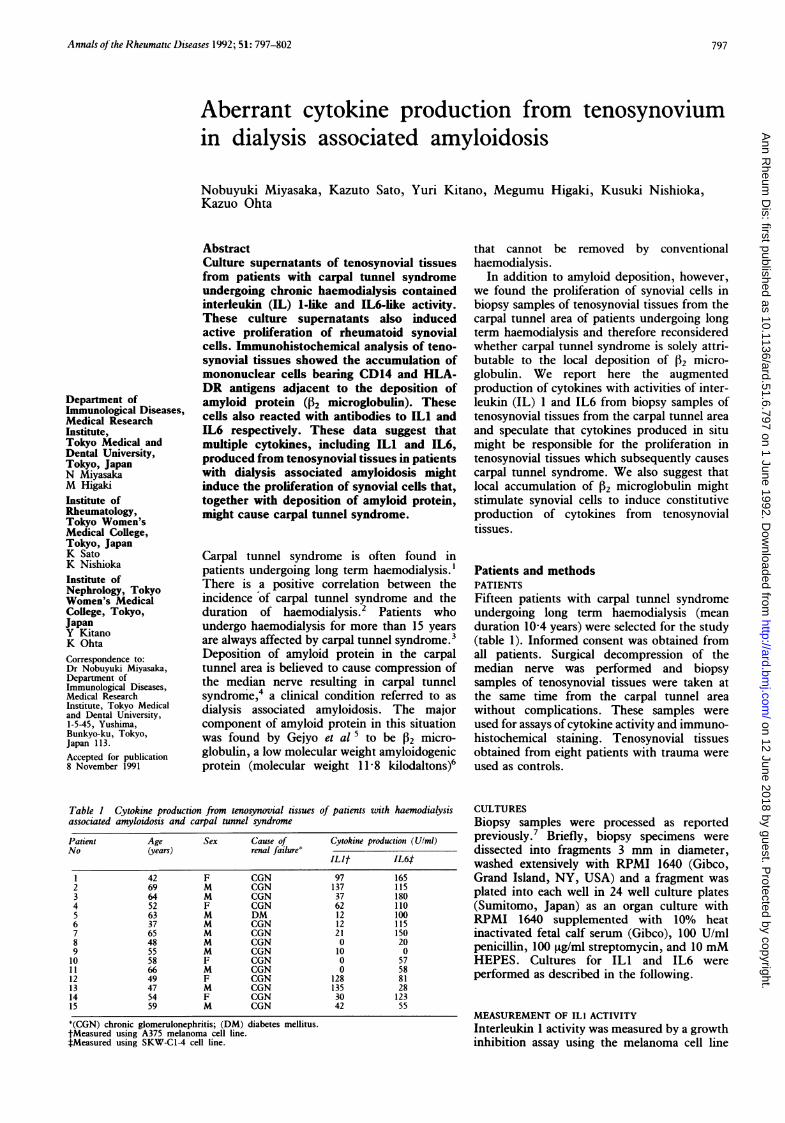
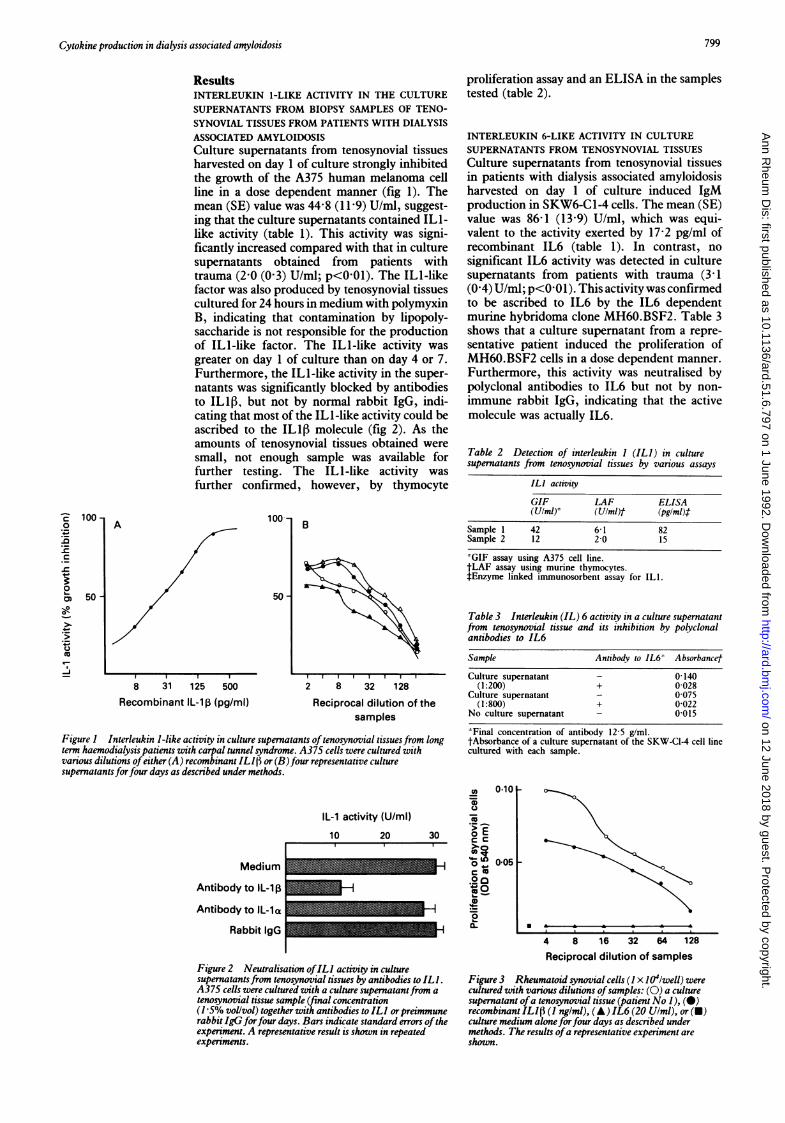
ResultsINTERLEUKIN 1-LIKE ACTIVITY IN THE CULTURESUPERNATANTS FROM BIOPSY SAMPLES OF TENO-SYNOVIAL TISSUES FROM PATIENTS WITH DIALYSISASSOCIATED AMYLOIDOSISCulture supernatants from tenosynovial tissuesharvested on day 1 of culture strongly inhibitedthe growth of the A375 human melanoma cellline in a dose dependent manner (fig 1). Themean (SE) value was 44'8 (11-9) U/ml, suggest-ing that the culture supernatants contained ILl-like activity (table 1). This activity was signi-ficantly increased compared with that in culturesupernatants obtained from patients withtrauma (2-0 (0-3) U/ml; p<001). The ILl-likefactor was also produced by tenosynovial tissuescultured for 24 hours in medium with polymyxinB, indicating that contamination by lipopoly-saccharide is not responsible for the productionof IL1-like factor. The IL1-like activity wasgreater on day 1 of culture than on day 4 or 7.Furthermore, the IL1-like activity in the super-natants was significantly blocked by antibodiesto ILI1, but not by normal rabbit IgG, indi-cating that most of the ILI -like activity could beascribed to the IL1P molecule (fig 2). As theamounts of tenosynovial tissues obtained weresmall, not enough sample was available forfurther testing. The IL1-like activity wasfurther confirmed, however, by thymocyte
1001 B
50
8 31 125 500
Recombinant IL-lp (pg/ml)2 8 32 128
Reciprocal dilution of thesamples
Figure 1 Interleukin 1-like activity in culture supernatants oftenosynovial tissues from longterm haemodialysis patients with carpal tunnel syndrome. A375 cells were cultured withvarious dilutions ofeither (A) recombinant ILl pt or (B)four representative culturesupernatants forfour days as described under methods.
IL-1 activity (U/ml)10 20 30
Medium
Antibody to IL-1
Antibody to IL-la
Rabbit IgG
Figure 2 Neutralisation ofIL1 activity in culturesupernatantsfrom tenosynovial tissues by antibodies to ILI .
A375 cells were cultured with a culture supernatantfrom a
tenosynovial tissue sample (final concentration(1-5% vol/vol) together with antibodies to ILI orpreimmunerabbit IgG forfour days. Bars indicate standard errors oftheexperiment. A representative result is shown in repeatedexperiments.
proliferation assay and an ELISA in the samplestested (table 2).
INTERLEUKIN 6-LIKE ACTIVITY IN CULTURESUPERNATANTS FROM TENOSYNOVIAL TISSUESCulture supernatants from tenosynovial tissuesin patients with dialysis associated amyloidosisharvested on day 1 of culture induced IgMproduction in SKW6-C1-4 cells. The mean (SE)value was 86-1 (13-9) U/ml, which was equi-valent to the activity exerted by 17-2 pg/ml ofrecombinant IL6 (table 1). In contrast, nosignificant IL6 activity was detected in culturesupernatants from patients with trauma (3 1(0-4) U/ml; p<0 01). This activity was confirmedto be ascribed to IL6 by the IL6 dependentmurine hybridoma clone MH60.BSF2. Table 3shows that a culture supernatant from a repre-sentative patient induced the proliferation ofMH60.BSF2 cells in a dose dependent manner.Furthermore, this activity was neutralised bypolyclonal antibodies to IL6 but not by non-immune rabbit IgG, indicating that the activemolecule was actually IL6.
Table 2 Detection of interleukin I (ILI) in culturesupernatants from tenosynovial tissues by various assays
ILI activityGIF LAF ELISA(U/ml) (Ulml)t (pg/ml)t
Sample 1 42 6-1 82Sample 2 12 2-0 15
*GIF assay using A375 cell line.tLAF assay using murine thymocytes.fEnzyme linked immunosorbent assay for ILl.
Table 3 Interleukin (IL) 6 activity in a culture supernatantfrom tenosynovial tissue and its inhibition by polyclonalantibodies to IL6
Sample Antibody to IL6t AbsorbancefCulture supernatant 0-140
(1:200) + 0-028Culture supernatant - 0075
(1:800) + 0-022No culture supernatant 0-015
*Final concentration of antibody 12 5 g/ml.tAbsorbance of a culture supernatant of the SKW-CI-4 cell linecultured with each sample.
0101-
005
4 8 16 32 64 128Reciprocal dilution of samples
Figure 3 Rheumatoid synovial cells (I x 104/well) werecultured with various dilutions ofsamples: (0) a culturesupernatant ofa tenosynovial tissue (patient No 1), (0)recombinant ILI (1( ng/ml), (A) IL6 (20 Ulml), or (v)culture medium aloneforfour days as described undermethods. The results ofa representative experiment areshown.
AC 1000
._
.C
._
m 50--J
r-
799
0-..
on 12 June 2018 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.51.6.797 on 1 June 1992. D
SYNOVIAL CELL GROWTH PROMOTING ACTIVITY INCULTURE SUPERNATANTS FROM TENOSYNOVIALTISSUESSynovial cells obtained from rheumatoidsynovial tissue as described under methods werecultured for approximately two weeks. Thesecultured synovial cells were plated (2x IO'cells/well) and incubated with various concen-trations of culture supernatants from teno-synovial tissues or recombinant IL113 for 72hours at 37°C. Figure 3 shows that thesesupernatants promoted the growth of synovialcells in a dose dependent manner; this capacitywas more potent than that obtained with1 ng/ml of recombinant IL1,B. In addition, thisactivity was also blocked by antibodies to IL1,B.
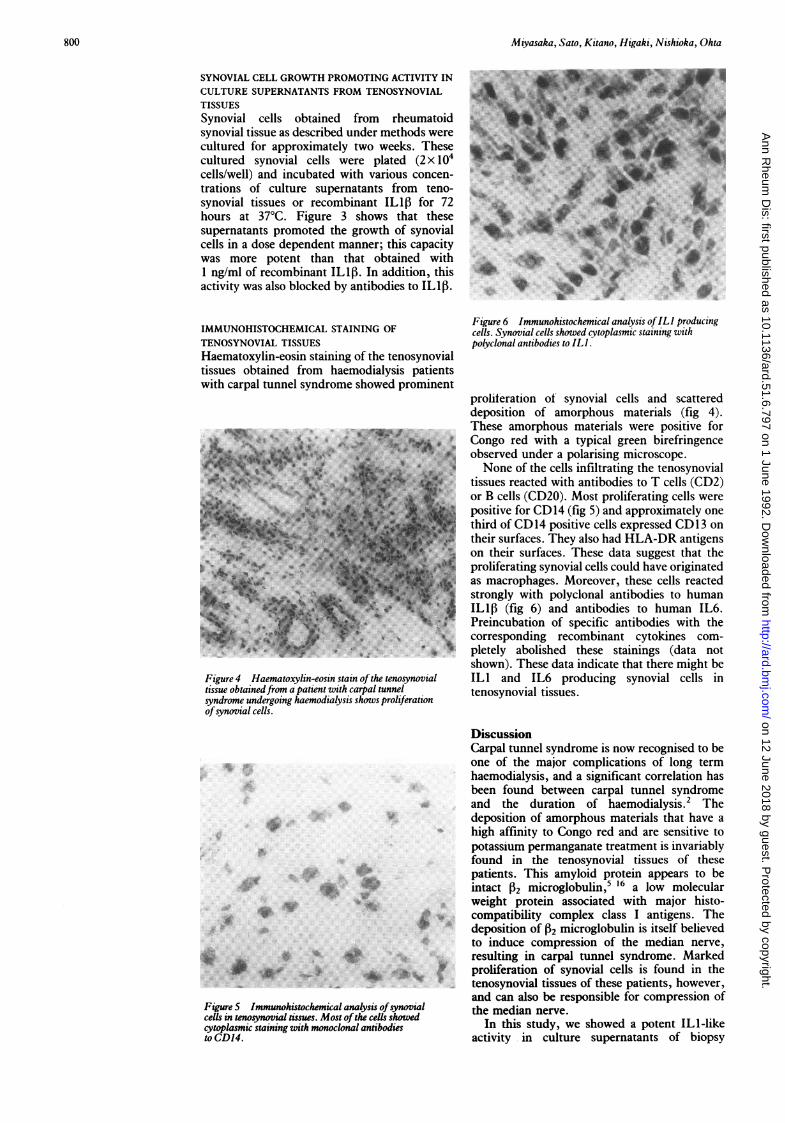
IMMUNOHISTOCHEMICAL STAINING OFTENOSYNOVIAL TISSUESHaematoxylin-eosin staining of the tenosynovialtissues obtained from haemodialysis patientswith carpal tunnel syndrome showed prominent
f-A4:z; s ! 1J||
9 N F#
:..
.%
Figure 4 Haematoxylin-eosin stain ofthe tenosynovialtissue obtainedfrom a patient with carpal tunnelsyndrome undergoing haemodialysis shows proliferationofsynovial cells.
proliteration of synovial cells and scattereddeposition of amorphous materials (fig 4).These amorphous materials were positive forCongo red with a typical green birefringenceobserved under a polarising microscope.None of the cells infiltrating the tenosynovial
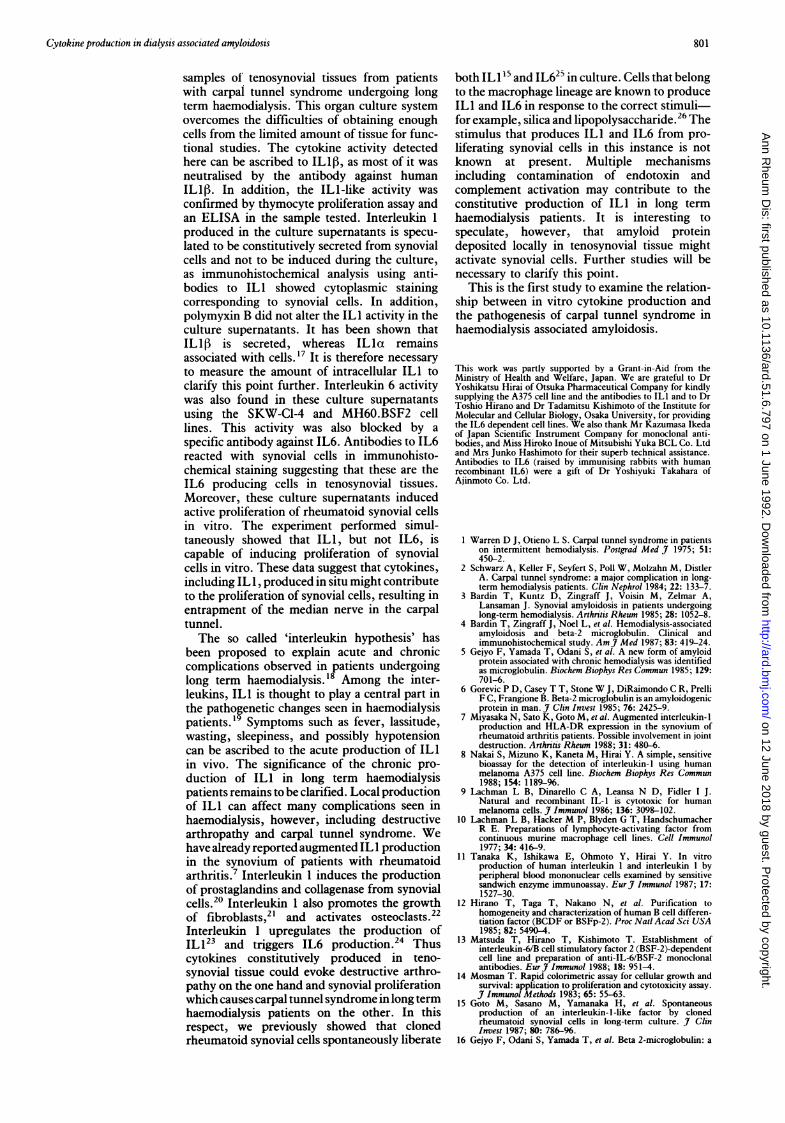
tissues reacted with antibodies to T cells (CD2)or B cells (CD20). Most proliferating cells werepositive for CD14 (fig 5) and approximately onethird of CD14 positive cells expressed CD 13 ontheir surfaces. They also had HLA-DR antigenson their surfaces. These data suggest that theproliferating synovial cells could have originatedas macrophages. Moreover, these cells reactedstrongly with polyclonal antibodies to humanIL13 (fig 6) and antibodies to human IL6.Preincubation of specific antibodies with thecorresponding recombinant cytokines com-pletely abolished these stainings (data notshown). These data indicate that there might beILl and IL6 producing synovial cells intenosynovial tissues.
....
.:i: :.::.:WA P
FigureS Immunohistochemical ana,cells in tenosynovial tissues. Most of ticytoplasmic staining with monoclonalto CD 14.
DiscussionCarpal tunnel syndrome is now recognised to beone of the major complications of long termhaemodialysis, and a significant correlation hasbeen found between carpal tunnel syndromeand the duration of haemodialysis.2 Thedeposition of amorphous materials that have ahigh affinity to Congo red and are sensitive topotassium permanganate treatment is invariablyfound in the tenosynovial tissues of thesepatients. This amyloid protein appears to beintact 12 microglobulin,5 16 a low molecularweight protein associated with major histo-compatibility complex class I antigens. The
W deposition of 2 microglobulin is itself believedto induce compression of the median nerve,resulting in carpal tunnel syndrome. Markedproliferation of synovial cells is found in thetenosynovial tissues of these patients, however,and can also be responsible for compression of
lysis ofsynovial the median nerve.
antibodies In this study, we showed a potent IL1-likeactivity in culture supernatants of biopsy
800
on 12 June 2018 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.51.6.797 on 1 June 1992. D
Cytokine production in dialysis associated amyloidosis
samples of tenosynovial tissues from patientswith carpal tunnel syndrome undergoing longterm haemodialysis. This organ culture systemovercomes the difficulties of obtaining enoughcells from the limited amount of tissue for func-tional studies. The cytokine activity detectedhere can be ascribed to IL1,, as most of it wasneutralised by the antibody against humanIL1IB. In addition, the ILl-like activity was
confirmed by thymocyte proliferation assay andan ELISA in the sample tested. Interleukin 1
produced in the culture supernatants is specu-
lated to be constitutively secreted from synovialcells and not to be induced during the culture,as immunohistochemical analysis using anti-bodies to IL 1 showed cytoplasmic stainingcorresponding to synovial cells. In addition,polymyxin B did not alter the ILl activity in theculture supernatants. It has been shown thatILlf is secreted, whereas ILla remainsassociated with cells.'7 It is therefore necessaryto measure the amount of intracellular ILl toclarify this point further. Interleukin 6 activitywas also found in these culture supernatantsusing the SKW-C1-4 and MH60.BSF2 celllines. This activity was also blocked by a
specific antibody against IL6. Antibodies to IL6reacted with synovial cells in immunohisto-chemical staining suggesting that these are theIL6 producing cells in tenosynovial tissues.Moreover, these culture supernatants inducedactive proliferation of rheumatoid synovial cellsin vitro. The experiment performed simul-taneously showed that ILl, but not IL6, iscapable of inducing proliferation of synovialcells in vitro. These data suggest that cytokines,including IL 1, produced in situ might contributeto the proliferation of synovial cells, resulting inentrapment of the median nerve in the carpaltunnel.The so called 'interleukin hypothesis' has
been proposed to explain acute and chroniccomplications observed in patients undergoinglong term haemodialysis.'8 Among the inter-leukins, ILl is thought to play a central part inthe pathogenetic changes seen in haemodialysispatients.'9 Symptoms such as fever, lassitude,wasting, sleepiness, and possibly hypotensioncan be ascribed to the acute production of IL1in vivo. The significance of the chronic pro-duction of ILl in long term haemodialysispatients remains to be clarified. Local productionof IL1 can affect many complications seen inhaemodialysis, however, including destructivearthropathy and carpal tunnel syndrome. Wehave already reported augmented IL 1 productionin the synovium of patients with rheumatoidarthritis.7 Interleukin 1 induces the productionof prostaglandins and collagenase from synovialcells.20 Interleukin 1 also promotes the growthof fibroblasts,2' and activates osteoclasts.22Interleukin 1 upregulates the production ofIL 123 and triggers IL6 production.24 Thuscytokines constitutively produced in teno-synovial tissue could evoke destructive arthro-pathy on the one hand and synovial proliferationwhich causes carpal tunnel syndrome in long termhaemodialysis patients on the other. In thisrespect, we previously showed that clonedrheumatoid synovial cells spontaneously liberate
both IL I1 and IL625 in culture. Cells that belongto the macrophage lineage are known to produceILI and IL6 in response to the correct stimuli-for example, silica and lipopolysaccharide.26 Thestimulus that produces ILl and IL6 from pro-liferating synovial cells in this instance is notknown at present. Multiple mechanismsincluding contamination of endotoxin andcomplement activation may contribute to theconstitutive production of ILl in long termhaemodialysis patients. It is interesting tospeculate, however, that amyloid proteindeposited locally in tenosynovial tissue mightactivate synovial cells. Further studies will benecessary to clarify this point.
This is the first study to examine the relation-ship between in vitro cytokine production andthe pathogenesis of carpal tunnel syndrome inhaemodialysis associated amyloidosis.
This work was partly supported by a Grant-in-Aid from theMinistry of Health and Welfare, Japan. We are grateful to DrYoshikatsu Hirai of Otsuka Pharmaceutical Company for kindlysupplying the A375 cell line and the antibodies to ILl and to DrToshio Hirano and Dr Tadamitsu Kishimoto of the Institute forMolecular and Cellular Biology, Osaka University, for providingthe IL6 dependent cell lines. We also thank Mr Kazumasa Ikedaof Japan Scientific Instrument Company for monoclonal anti-bodies, and Miss Hiroko Inoue of Mitsubishi Yuka BCL Co. Ltdand Mrs Junko Hashimoto for their superb technical assistance.Antibodies to IL6 (raised by immunising rabbits with humanrecombinant IL6) were a gift of Dr Yoshiyuki Takahara ofAjinmoto Co. Ltd.
I Warren D J, Otieno L S. Carpal tunnel syndrome in patientson intermittent hemodialysis. Postgrad Med J 1975; 51:450-2.
2 Schwarz A, Keller F, Seyfert S, Poll W, Molzahn M, DistlerA. Carpal tunnel syndrome: a major complication in long-term hemodialysis patients. Clin Nephrol 1984; 22: 133-7.
3 Bardin T, Kuntz D, Zingraff J, Voisin M, Zelmar A,Lansaman J. Synovial amyloidosis in patients undergoinglong-term hemodialysis. Arthritis Rheum 1985; 28: 1052-8.
4 Bardin T, Zingraff J, Noel L, et al. Hemodialysis-associatedamyloidosis and beta-2 microglobulin. Clinical andimmunohistochemical study. AmJ Med 1987; 83: 419-24.
5 Gejyo F, Yamada T, Odani S, et al. A new form of amyloidprotein associated with chronic hemodialysis was identifiedas microglobulin. Biochem Biophys Res Commun 1985; 129:701-6.
6 Gorevic P D, Casey T T, Stone W J, DiRaimondo C R, PrelliF C, Frangione B. Beta-2 microglobulin is an amyloidogenicprotein in man. J C'Gn Invest 1985; 76: 2425-9.
7 Miyasaka N, Sato K, Goto M, et al. Augmented interleukin-1production and HLA-DR expression in the synovium ofrheumatoid arthritis patients. Possible involvement in jointdestruction. Arthritis Rheum 1988; 31: 480-6.
8 Nakai S, Mizuno K, Kaneta M, Hirai Y. A simple, sensitivebioassay for the detection of interleukin-1 using humanmelanoma A375 cell line. Biochem Biophys Res Commun1988; 154: 1189-96.
9 Lachman L B, Dinarello C A, Leansa N D, Fidler I J.Natural and recombinant IL- 1 is cytotoxic for humanmelanoma cells. J Immunol 1986; 136: 3098-102.
10 Lachman L B, Hacker M P, Blyden G T, HandschumacherR E. Preparations of lymphocyte-activating factor fromcontinuous murine macrophage cell lines. Cell Immunol1977; 34: 416-9.
11 Tanaka K, Ishikawa E, Ohmoto Y, Hirai Y. In vitroproduction of human interleukin 1 and interleukin 1 byperipheral blood mononuclear cells examined by sensitivesandwich enzyme immunoassay. Eur_J Immunol 1987; 17:1527-30.
12 Hirano T, Taga T, Nakano N, et al. Purification tohomogeneity and characterization of human B cell differen-tiation factor (BCDF or BSFp-2). Proc Natl Acad Sci USA1985; 82: 5490-4.
13 Matsuda T, Hirano T, Kishimoto T. Establishment ofinterleukin-6/B cell stimulatory factor 2 (BSF-2)-dependentcell line and preparation of anti-IL-6/BSF-2 monoclonalantibodies. EurJ7 Immunol 1988; 18: 951-4.
14 Mosman T. Rapid colorimetric assay for cellular growth andsurvival: application to proliferation and cytotoxicity assay.J Immunol Methods 1983; 65: 55-63.
15 Goto M, Sasano M, Yamanaka H, et al. Spontaneousproduction of an interleukin- 1-like factor by clonedrheumatoid synovial cells in long-term culture. J ClinInvest 1987; 80: 786-96.
16 Gejyo F, Odani S, Yamada T, et al. Beta 2-microglobulin: a
801
on 12 June 2018 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.51.6.797 on 1 June 1992. D
new form of amyloid protein associated with chronichemodialysis. Kidney Int 1986; 30: 385-90.
17 Conlon P J, Grabstein K H, Alpert A, Prickett K S, HoppT P, Gillis S. Localization of human mononuclear cellinterleukin 1. J7 Immunol 1987; 139: 98-102.
18 Dinarello C A, Koch K M, Shaldon S. The interleukinhypothesis. Interleukin- 1 and its relevance in patientstreated with hemodialysis. Kidney Int 1988; 33 (suppl 24):S21-6.
19 Bingel M, Lonnemann G, Shaldon S, Koch K M, DinarelloC A. Human interleukin- I production during hemodialysis.Nephron 1986; 43: 161-3.
20 Dayer J M, de Rochemonteix B, Burrus B, Demczuk S,Dinarello C A. Human recombinant interleukin 1 stimulatescollagenase and prostaglandin E production by humansynovial cells. Clin Invest 1986; 77: 645-8.
21 Schmidt J A, Mizel S B, Cohen D, Green I. Interleukin 1: apotential regulator of fibroblast proliferation. J7 Immunol1982; 128: 2177-82.
22 Dewhirst F E, Stashenko P P, Mole J E, Tsurumachi r.Purification and partial sequence of human osteoclast-activating factor: identity with interleukin I1). 7 Immunol1985; 135: 2562-8.
23 Dinarello C A, Ikejima T, Warner S J C, et al. Interleukin Iinduces interleukin 1. I. Induction of circulating inter-leukin I in rabbits in vivo and human mononuclear cells invitro. 7 Immunol 1987; 139: 1902-10.
24 Content J, De Wit L, Poupart P, Opdenakker G, VanDamme J, Billiau A. Induction of a 26-kDa-protein mRNAin human cells treated with an interleukin- 1-related,leukocyte-derived factor. Eur]7 Biochem 1985; 152: 253-7.
25 Miyasaka N, Sato K, Hashimoto J, et al. Constitutiveproduction of interleukin 6/B cell stimulatory factor-2 frominflammatory synovium. Clin Immunol Immunopathol 1989;52: 238-47.
26 Kishimoto T, Hirano T. Molecular regulation of B lympho-cyte response. Ann Rev Immunol 1988; 6: 485-512.
802
on 12 June 2018 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.51.6.797 on 1 June 1992. D