MEMORANDUM March 31, 2015 From: Susan R. Griffin, PT, DPT, MS, GCS, RP, speaker, House of Delegates Marie Stravlo, manager, National Governance and Leadership – House of Delegates RE: 2015 House of Delegates Packet I, Background Papers, and House of Delegates Handbook Packet I, which contains all proposed main motions received by the March 2 deadline, is attached, along with subsequent appendices (Appendices A–D) that contain information about additional materials, planning, and resources. Business of the House of Delegates (House) is conducted through the introduction of main motions. Therefore, in order to be thoroughly prepared to represent your component, delegates must make the time to read and educate themselves about each motion and stay current with all information found on the House of Delegates HUB. Questions, concerns, or opinions about a motion should be directed to the maker of the motion. When information is desired from the Board of Directors (Board) or staff, this request should be posted to the appropriate discussion thread under ‘Packet I Discussions ’ on the House of Delegates Community to allow all delegates to benefit from the reply. Delegates contemplating amendments to motions should communicate with the motion maker, and the Reference Committee contact listed on the motion. In addition, all delegates are encouraged to participate in the Virtual Town Halls on Thursday, April 23 and Thursday, May 14. Within Packet I, delegates will find the Rules of the House of Delegates and the General Order of Business, both adopted by the House as the first and second orders of business, and Implications for Motion Language, developed by the Reference Committee to identify the implication of certain terms when used within House motions. The Detailed Agenda, a subset of the General Order of Business, is adopted immediately prior to the start of new business, and delineates the proposed order of motions to come before the House of Delegates. Motions are placed into categories adopted by the Reference Committee to guide the order. However, ultimately, the order of motions is determined at the discretion of the speaker, in consultation with the House Officers and the Reference Committee chair, in order to facilitate the business of the House in the way deemed most logical and efficient. Much more information will be provided to you over the next 2 months. Please allot time weekly (at a minimum!) to devote solely to reading motions, background information, reports, and delegate comments, and to reflect on how this information relates to the transformation of the association, profession,
Transcript
MEMORANDUM
March 31, 2015
From: Susan R. Griffin, PT, DPT, MS, GCS, RP, speaker, House of DelegatesMarie Stravlo, manager, National Governance and Leadership – House of Delegates
RE: 2015 House of Delegates Packet I, Background Papers, and House of Delegates Handbook
Packet I, which contains all proposed main motions received by the March 2 deadline, is attached, along with subsequent appendices (Appendices A–D) that contain information about additional materials, planning, and resources. Business of the House of Delegates (House) is conducted through the introduction of main motions. Therefore, in order to be thoroughly prepared to represent your component, delegates must make the time to read and educate themselves about each motion and stay current with all information found on the House of Delegates HUB. Questions, concerns, or opinions about a motion should be directed to the maker of the motion. When information is desired from the Board of Directors (Board) or staff, this request should be posted to the appropriate discussion thread under ‘Packet I Discussions’ on the House of Delegates Community to allow all delegates to benefit from the reply. Delegates contemplating amendments to motions should communicate with the motion maker, and the Reference Committee contact listed on the motion. In addition, all delegates are encouraged to participate in the Virtual Town Halls on Thursday, April 23 and Thursday, May 14.
Within Packet I, delegates will find the Rules of the House of Delegates and the General Order of Business, both adopted by the House as the first and second orders of business, and Implications for Motion Language, developed by the Reference Committee to identify the implication of certain terms when used within House motions.
The Detailed Agenda, a subset of the General Order of Business, is adopted immediately prior to the start of new business, and delineates the proposed order of motions to come before the House of Delegates. Motions are placed into categories adopted by the Reference Committee to guide the order. However, ultimately, the order of motions is determined at the discretion of the speaker, in consultation with the House Officers and the Reference Committee chair, in order to facilitate the business of the House in the way deemed most logical and efficient.
Much more information will be provided to you over the next 2 months. Please allot time weekly (at a minimum!) to devote solely to reading motions, background information, reports, and delegate comments, and to reflect on how this information relates to the transformation of the association, profession, and society. This will ensure that you are prepared to fully engage in the serious and weighty responsibilities of a delegate.
Downloading Packet I is accomplished by accessing the documents from the House community. From the APTA homepage, at the top of the page in the teal horizontal tool bar, select “APTA Communities.” Click on “Communities” and select “House of Delegates.” Under “File Library” select “Motions, House Handbook, and Background Papers.”
As you read through Packet I, you will notice 5 motions with conforming amendments (RC 1-15; RC 5-15; RC 6-15;RC 7-15; RC 8-15 ) with each amendment named as a separate part (Part A, Part B, Part C, etc.). The concept of conforming amendments was introduced in Robert’s Rules of Order Newly Revised, 11th edition. When several changes are required to achieve one end, these separate changes are considered conforming amendments, and are adopted by a single motion.
The House officers wish to thank the delegates for their preparation thus far and for their timely submission of motions. We are confident that the House can complete all the business to come before it this year if we work together efficiently and openly. Early and frequent networking with delegates and motion makers will greatly improve our ability to resolve conflict and reach mutual understanding for the good of the association and the profession. Do not hesitate to contact us if you have questions, concerns, or suggestions for expediting the business of the House. We look forward to seeing you soon!
The House of Delegates Handbook (Handbook) contains annual and special reports to the House. All reports published within the Handbook, with the exception of the House officers, Reference Committee, Secretary, and Nominating Committee reports, have been written in response to charges from the House. Be sure to read these thoroughly. Questions related to these reports should be posted under ‘House Report Discussions’ on the House of Delegates Community. Delegates may also ask questions or share comments during the House on Monday, June 1 when reports are taken up. The House of Delegates Handbook will be posted to the House Community on Friday, April 10.
Background Papers, which are written by APTA staff, are an invaluable resource to delegates in helping to understand the implications of motions published in Packet I. Due to the complexity of the motions, the background papers will be made available to delegates by Thursday, April 30.
Reference Committee Onsite Appointments will be held Sunday, May 31, and Tuesday, June 2. For specific information regarding appointment times and guidance regarding what materials to bring to your appointment, please refer to the House Community.
Reference Committee Virtual Appointments will be held on Thursday, May 14. The Reference Committee will be available from 12:00 pm – 2:00 pm, ET, for 15 minute appointments. Please refer to the House Community for more information.
The Reference Committee and House officers will lead 2 Virtual Town Halls: Thursday, April 23, 8:00 – 9:30 pm, ET, and Thursday, May 14, 8:00 – 9:30 pm, ET. The purpose of the spring town halls is to discuss motions, the implications should the motion be adopted, and ask informational questions. To present a motion please contact Camille Fredrickson with any motion you would like to discuss. Please note that based on conversations taking place on the House Discussion board, the Reference Committee and House officers may add specific motions to the agenda as well.
Pre-House Motions Discussion Groups will be held on Sunday, May 31, 6:00 pm – 7:45 pm, ET. The agenda will be posted to the House Community.
The House of Delegates Community (House community) is the most important resource available to delegates. The House Community is your source for all of the important materials necessary to prepare for the House.
The House Community may be accessed from the APTA homepage (www.apta.org) by logging on and, at the very top of the page in the teal horizontal tool bar, selecting “APTA Communities.” Once on the main community page, select “House of Delegates” under “My Communities.”
The House Community is organized into 2 sections:
1. Forum – the sole purposes of these forums are to facilitate motion discussion prior to arrival onsite. All delegates should subscribe for alerts to each one of the discussion boards listed on the House Community. Discussion boards are organized as follows:
House of Delegate Updates – This forum is used to alert delegates about any upcoming deadline, events, or the posting of new material to the file library.
Packet I - This forum is used by all delegates to provide opinion or to ask questions related to the motions that have been released in Packet I. Although the forum is open to all delegates, chief, section, and assembly delegates are the only individuals who may post the official opinion of a delegation, and should identify themselves within a post when providing official opinion.
House Report – This new forum is used by all delegates to provide opinion or to ask questions related to the House reports released in the House of Delegates Handbook.
2. File Library – contains materials in document formats (i.e. PDF, Word, PowerPoint, etc). Folders are organized as follows:
To assist with delegate preparation for the House a downloadable file that contains materials that each delegate is responsible for having in his/her possession during House proceedings, will be made available by Friday, May 22, 2015. The file will contain the following materials:
POSITIONS, BYLAWS, AND CORE DOCUMENTS APTA Bylaws APTA Standing Rules Association Positions, Standards, Guidelines, Policies, and Procedures Code of Ethics for the Physical Therapist Guide for Professional Conduct Guide for Conduct of the Physical Therapist Assistant Standards of Ethical Conduct for the Physical Therapist Assistant Vision Statement for the Physical Therapy Profession and Guiding Principles to Achieve the Vision
HOUSE REFERENCE MATERIALS House of Delegates Schedule Seating Chart and Microphone List House of Delegates Dates and Deadlines Apportionment Packet I Background Papers House of Delegates Handbook Motions Discussion Group Agendas
REFERENCE COMMITTEE MATERIALS Reference Committee Roster and Liaison List House of Delegates Motion Development Form
ELECTIONS MATERIALS Nominating Committee Roster and Liaison List Slate of Candidates Candidate Statements and Bios Candidate Interview Schedule
To access and download the Downloadable File, access the House Community and in the House Resources File Library, select HOD Download File. Please refer to the instructions listed below which are organized by operating system.
The Downloadable File is comprised of self-extracting Zip files, which compress large documents for fast and easy downloading and enable the user to then “expand” the file in its native format – MS Word. Self-extracting zip files do not require the user to have a special computer program necessary for “unzipping.”
Windows: Click on the file link. When the security dialogue box pops up click "Run," and then click "run" again if a
second security dialogue box appears. When the Winzip Self Extractor dialogue box appears, click "Browse" and then select the folder on your
computer where you would like the file saved. Click "OK." Then click "Unzip." The files will be loaded, and an alert will appear when the files have been extracted onto your computer.
Macs:It is recommended that you use either Unarchiver (current version 3.7) or Stuffit Expander (current version 15.0.7) – both are available from the App Store.
If either Unarchiver or Stuffit Expander is your only extracting software, double click the .exe file. Tell Unarchiver/Stuffit Expander where you want the files to be extracted. If you have multiple zip extraction programs installed, right click on the .exe file and select “Open With.” Select the program you want to use or select “Other” and find the application you want to use. Follow the prompts to save the file to your preferred location and unzip.
1 Fix the Time to Which to Adjourn Sets the time for a continued meeting No Yes No1 Yes Majority2 Adjourn Closes the meeting No Yes No No Majority3 Recess Establishes a brief break No Yes No2 Yes Majority
4 Raise a Question of Privilege Asks an urgent question regarding rights Yes No No No Ruled by chair
5 Call for Orders of the Day Requires that the meeting follow the agenda Yes No No No One member6 Lay on the Table Puts the motion aside for later consideration No Yes No No Majority7 Previous Question Ends debate and moves directly to the vote No Yes No No Two-thirds8 Limit or Extend Limits of Debate Changes the debate limits No Yes No Yes Two-thirds9 Postpone to a Certain Time Puts off the motion to a specific time No Yes Yes Yes Majority3
10 Commit or Refer Refers the motion to a committee No Yes Yes Yes Majority
11 Amend an amendment(Secondary Amendment)
Proposes a change to an amendment No Yes Yes4 No Majority
12 Amend a motion or resolution(Primary Amendment)
Proposes a change to a main motion No Yes Yes4 Yes Majority
13 Postpone Indefinitely Kills the motion No Yes Yes No Majority14 MAIN MOTION Brings business before the assembly No Yes Yes Yes Majority
1 Is debatable if the motion is made while no question is pending2 Unless no question is pending
Note: Motions above are in the Order of Precedence of motions.
3 Majority, unless it makes the question a special order4 If the motion it is being applied to is debatable
Based on Robert’s Rules of Order Newly Revised, 11th Edition
The Guerrilla’s Guide to Robert’s RulesNancy Sylvester, MA, PRP, CPP-T www.nancysylvester.com
Motion Purpose Interrupt speaker?
Second Needed? Debatable? Amendable? Vote Needed
Point of Order Requests that the rules be followed Yes No No No Ruled by chair
Appeal from the Decision of the Chair Challenges a ruling of the chair Yes Yes Depends4 No Majority5
Suspend the Rules Allows the group to violate the rules No Yes No No Two-thirds(not bylaws)
Objection to Consideration Keeps the motion from being considered Yes6 No No No Two-thirds7
Division of the Question Separates consideration of the motion No Yes No Yes MajorityDivision of the Assembly Requires a standing vote Yes No No No One member
Parliamentary Inquiry or Allows a member to ask a question Yes No No No Responded to
Request for Information about the business at hand by chairWithdraw a Motion Removes a motion from Yes Depends8 No No Majority(after stated by the chair) considerationTake from the Table Resumes consideration of a motion No Yes No No Majority
that was laid on the tableReconsider Considers a motion again Yes9 Yes Depends10 No MajorityRescind or Amend Something Repeals a previously adopted motion No Yes Yes Yes Depends11
Previously Adopted or amends it after it has been adopted
4 If the motion it is being applied to is debatable5 Majority in negative required to reverse chair's decision6 Yes, until debate has begun or a subsidiary motion other than Lay on the Table has been stated by the chair7 Two- thirds against consideration sustains objection
8 Yes, if motion is made by the person requesting permission; no, if made by another member9 When another member has been assigned the floor, but not after he or she has begun to speak10 Only if the motion to be reconsidered is debatable11 Requires a) a majority with notice, b) two- thirds, OR c) majority of entire membership
American Physical Therapy Association
2015 HOUSE OF DELEGATES
PACKET I
March 31, 2015
2015 PACKET I
TABLE OF CONTENTS
DOCUMENT TITLE PAGE
Rules of the House of Delegates 1
General Order of Business 5
Detailed Agenda 7
RC # CAT TITLE CONTACT PAGE
1 1 RC 1-15 Amend: Bylaws of the American Physical Therapy Association and Standing Rules of the American Physical Therapy Association to Change the Length and Number of Terms for Members of the APTA Board of Directors
HPA 10
2 1 RC 2-15 Amend: Bylaws of the American Physical Therapy Association to Change the Qualifications for President, Vice President, Secretary, and Treasurer
HPA 13
3 1 RC 3-15 Amend: Bylaws of the American Physical Therapy Association to Grant Components the Option of Amending their Bylaws to Provide a Full Vote for Physical Therapist Assistant Members
BOD 14
4 1 RC 4-15 Amend: Bylaws of the American Physical Therapy Association to Provide Chapters the Option of Amending their Bylaws to Enable Physical Therapist Assistant Members to Serve as Chapter Delegates
BOD 16
5 1 RC 5-15 Amend: Bylaws of the American Physical Therapy Association to Allow Sections to Vote in the House of Delegates
HPA 18
6 1 RC 6-15 Amend: Bylaws of the American Physical Therapy Association to Grant Life Members the Privilege of Serving as Delegates to the House of Delegates
FL 30
7 1 RC 7-15 Amend: Bylaws of the American Physical Therapy Association to Grant Physical Therapist Assistant Members the Privilege to Serve on the APTA Board of Directors
BOD 36
8 6 RC 8-15 Delivery of Value-Based Physical Therapist Services BOD 38
10 4 RC 10-15 Rescind: Health Care Coverage for all Americans(HOD P06-05-18-27)
BOD 50
11 6 RC 11-15 Adopt: Health Priorities for Populations and Individuals BOD 51
12 6 RC 12-15 Adopt: The Role of the Physical Therapist in Diet and Nutrition MI 53
13 6 RC 13-15 Adopt: The Association’s Role in Advocacy for Prevention, Wellness, Fitness, and Health Promotion, and for Management of Disease and Disability
BOD 55
14 6 RC 14-15 Adopt: Physical Therapists’ Role in Prevention, Wellness, Fitness, Health Promotion, and Management of Disease and Disability
BOD 56
15 4 RC 15-15 Rescind: Positions Related to Prevention, Wellness, Fitness, Health Promotion, and Management of Disease and Disability
BOD 59
16 6 RC 16-15 Adopt: Management of the Movement System AZ 61
17 6 RC 17-15 Adopt: Identification of Physical Therapists by Professional Title NY 65
18 6 RC 18-15 Adopt: Position Statement on Bullying PA 66
19 7 RC 19-15 Explore the Feasibility of Obtaining Primary Care Practitioner Status
AL 70
20 7 RC 20-15 Collaborations to Address Childhood and Adult Obesity AZ 73
21 7 RC 21-15 Incorporation of Standardized Physical Therapist Patient/Client Management Elements in Electronic Health Records
MA 75
22 7 RC 22-15 Standards and Interoperability for Health Information Technology and Electronic Health Records
DC 76
23 6 RC 23-15 Adopt: Designation of Individuals with Intellectual and Developmental Disabilities as a Medically Underserved Population
NC 79
RULES OF THE HOUSE OF DELEGATES
The following rules govern the conduct of business at the House of Delegates. Only Section III – Rules of the House of Delegates – Adopted for the Session: May be Suspended, are adopted by the House of Delegates.
I. RULES OF THE HOUSE OF DELEGATES REQUIRED BY APTA BYLAWS - MAY NOT BE SUSPENDED
Rules of the House as outlined within the Bylaws of the American Physical Therapy Association:
ARTICLE IV. MEMBERSHIP, Section 2: Rights and Privileges of Members
ARTICLE VIII. HOUSE OF DELEGATES
ARTICLE IX. BOARD OF DIRECTORS, Section 2: Qualifications
ARTICLE X. COMMITTEES AND COUNCILS, Section 2: Committees of the House of Delegates
ARTICLE XIV. AMENDMENTS
II. RULES OF THE HOUSE OF DELEGATES - REQUIRED BY RELEVANT APTA STANDING RULES - MAY BE SUSPENDED
Rules of the House as outlined with the Standing Rules of the American Physical Therapy Association:
13. ELECTIONS: TELLER’S REPORTS
A. The teller’s report to the House of Delegates shall include for each position to be filled:(1) The number eligible to vote.(2) The number of votes cast.(3) The number of votes necessary for election (for officers).(4) The number of votes cast for each eligible candidate.(5) The number of illegal votes, and the reason therefore.
14. VACANCIES -- OFFICERS AND DIRECTORS
A. If a vacancy occurs within the first year of a 3-year term, the Nominating Committee shall select a candidate(s) for election at the next annual session of the House of Delegates; the elected person shall serve for the remaining 2 years of the term.
B. If a vacancy occurs after the first year of a 3-year term, the vacancy shall be filled by appointment by the Board of Directors.
C. Not withstanding Standing Rule 13(B), if a vacancy occurs on the Board of Directors as a result of an election, a second election shall be required. The Nominating Committee shall prepare the slate for the second election and additional nominations from the floor shall be in order.
All candidates who were slated for any position on the Board of Directors and were not elected in the first election will be slated in the second election unless they have indicated otherwise. Candidates who were not elected for the Nominating Committee shall not be automatically slated but may be nominated from the floor.
A. The committee shall receive and correlate motions and resolutions to be presented to the House of Delegates and shall identify motions which fall outside the object or functions of the Association. The committee shall provide advice and counsel regarding form, wording, and method of presentation of matters to be presented to the House.
B. All main motions and resolutions, except for procedural motions presented for action by the House of Delegates, shall be referred to the Reference Committee unless this rule is suspended in any particular case by a majority vote of the House of Delegates.
C. The committee will review main motions that are submitted by the established deadline and in the manner prescribed in the standing rule titled Main Motion Criteria.
D. Appointed members of the committee shall be seated in the House of Delegates and shall reply to inquiries directed to the committee by the Speaker of the House.
E. On a regular basis the committee will review the Association bylaws and standing rules and, as it deems appropriate, propose to the Board of Directors that it bring amendments to the House of Delegates for consideration.
16. DEADLINE FOR MAIN MOTIONS
All main motions to be considered by the House of Delegates shall be submitted in writing to APTA headquarters by a date set by the Speaker of the House of Delegates, which shall be at least 2 months and no more than 3 months prior to the date of the House of Delegates meeting. Any main motion which has not been so submitted shall require a majority vote, without debate, to be considered by the House.
17. MAIN MOTION CRITERIA
All main motions submitted by the established deadline shall meet the following criteria.
It is the responsibility of the maker of the motion to:
(1) Provide a statement of the intended outcome of the motion.
(2) Demonstrate that the motion’s subject is national in scope or importance.
(3) Provide pertinent background information, in collaboration with the APTA Board of Directors or staff including (a) a description of previous House, Board, or staff activity relating to the subject and (b) an identification of the stakeholders affected by the motion.
(4) When possible, demonstrate that the motion concept has been disseminated to delegates of other delegations prior to the deadline for submission of main motions.
(5) Provide a description of the potential fiscal impact of adopting and implementing the motion.
The Reference Committee determines how criteria have been met. If it is determined that the criteria are not adequately met, the motion shall be placed at the end of the agenda of the House of Delegates and shall not be considered unless a majority of the delegates vote, without debate, to consider the motion. The Reference Committee shall develop and make available to the delegates guidance designed to help delegates satisfy the foregoing criteria.
20. CONSENT CALENDAR
A. The officers of the House of Delegates shall prepare a list of recommended motions that are routine, standard, non-controversial, or self-explanatory and where general approval is anticipated, for placement on a consent calendar.
B. The preliminary consent calendar will be distributed 3 weeks prior to the start of the first meeting of the House of Delegates.
2
C. Prior to the first meeting of the House of Delegates motions may be removed from the consent calendar by the officers of the House of Delegates or at the request of 5 chief delegates.
D. The revised consent calendar will be prepared by the officers of the House of Delegates for presentation to chief, section, and assembly delegates prior to the first meeting of the House of Delegates.
E. Following the opening of the House of Delegates motions may be removed from the consent calendar by an affirmative vote of one-third of the voting body of the House of Delegates.
F. If a motion is removed from the consent calendar, it shall be placed appropriately in the order of business previously assigned by the Speaker of the House and the chair of the Reference Committee.
G. The consent calendar shall be presented for adoption in a single motion.
III. RULES OF THE HOUSE OF DELEGATES – ADOPTED FOR THE SESSION - MAY BE SUSPENDED
1. Only members of the American Physical Therapy Association, Association headquarters staff, component executive personnel, and nonmember guests approved by an officer of the House of Delegates may attend meetings of the House of Delegates. If the House of Delegates votes to go into executive session, the speaker, in consultation with the president and chief executive officer, may invite the following non-APTA members to remain in the House proper during the session: the parliamentarian, the House recorder, APTA staff, component executive personnel, and others.
2. An official delegate badge is required for admission of delegates to the meetings of the House. Admission cards, signed by an officer of the House, are required for the admission of nonmember guests to the House.
3. Delegates shall keep badges in evidence when attending the meetings of the House of Delegates.4. All registered delegates (chapter, section, PTA Caucus delegates, and assembly delegates) and members of the
Board of Directors, consultants to the House, and Nominating Committee shall be seated in designated areas within the House proper. PTA Caucus representatives, designated APTA staff, and Component Executives shall be seated in a designated area of the gallery.
5. All members of APTA may have the floor to speak, but registered delegates will be recognized first.6. No delegate or member shall be entitled to the floor until recognized by the speaker of the House. Individuals
recognized to speak shall provide their name, delegate affiliation if appropriate (e.g., name of chapter, section or assembly), and speak with the aid of a microphone.
7. Members of APTA headquarters staff and members of APTA appointed groups may be recognized for the purpose of giving information and participating in discussions.
8. The vice speaker shall be the official timekeeper at all meetings.9. When speaking to a motion, each speaker shall be limited to 3 minutes. The vice speaker will indicate when 30
seconds remain in the allotted time.10. A speaker may not speak twice to the same motion until everyone wishing to speak has done so.11. A delegate may not rise to debate and close by moving the previous question.12. A motion may not be seconded by a delegate from the same component as the delegate making the motion.13. A motion made by a member of the Board of Directors may not be seconded by another member of the Board of
Directors.14. The delegate who moves the motion may not speak in opposition to the motion.15. Motions to amend must be in writing; Preferably electronically, but if handwritten six (6) copies forwarded to the
secretary prior to the opening of the meeting, if possible, or prior to the motion being made on the floor.16. The motion to suspend the requirement that all main motions and resolutions be referred to the Reference
Committee must identify the subject of the motion to be presented.17. Any motion to amend something previously adopted is a main motion and falls under the standing rule of
submitting main motions by the deadline date set by the speaker of the House. In addition, the vote required for such motions is a majority if notice is given. If notice is not given, a two-thirds vote or a vote of a majority of the entire voting membership of the House is required.
18. Replacement or substitute motions for motions contained in Packet I will be published in a subsequent packet. These motions must be reviewed by the Reference Committee no later than Sunday, May 31 for Packet II and Tuesday, June 2 for Packet III.
19. Motions may be withdrawn by the motion maker after notice has been given via Packet I and only without objection by the delegates.
20. When voting during elections by use of an electronic keypad, a mechanism for indicating a “write-in” candidate will be provided.
3
21. If the number of anonymous write-in candidates is sufficient to preclude the election of a candidate or candidates, the floor will be opened for nominations and the election will proceed with the addition of those nominees to the ballot.
22. When a nomination comes from the floor of the House, the candidate will be provided the opportunity to present a statement in support of their candidacy that is no more than 5 minutes in length.
23. There must be an affirmative vote of one-fifth (1/5) of the voting body of the House of Delegates to order a roll call vote, except when ordered by the speaker of the House.
24. Electronic keypads may be used for counted votes at the discretion of the speaker of the House.25. The secretary, in consultation with the speaker, shall: 1) Edit all House motions for grammar and punctuation;
2) Edit related items (positions, policies, guidelines) when newly adopted motions require editorial changes in previously adopted motions; and 3) Provide documentation of editorial changes to any delegate upon request.
26. No tape or other recordings may be made of the proceedings of the House of Delegates other than those made by the individuals approved by House officers.
27. Exhibitors are not to distribute promotional items in the House of Delegates, other than those approved by the House officers.
28. Delegates who are recognized to speak should consider those individuals who are hearing impaired and position themselves at the microphone so that their mouth and lips are not obscured from view.
29. Delegates who require a reasonable accommodation for a qualified disability should make their request known to the speaker of the House.
30. Service animals are permitted in the House proper and gallery.
4
2015 HOUSE OF DELEGATES
AMERICAN PHYSICAL THERAPY ASSOCIATION
GENERAL ORDER OF BUSINESS
MONDAY, JUNE 1
Call to Order
Opening Ceremonies
1. Pledge of Allegiance
2. Introductions
3. In Memoriam (2015 HOD Handbook)
Adoption of the Rules of House of Delegates (Packet I)
Adoption of General Order of Business (Packet I)
(Adoption of Detailed Agenda deferred until Tuesday morning)
Report from the Nominating Committee
Introduction of Candidates
Appointments
1. Committee to Approve the Minutes
2. Elections Chair and Vice-Chair
Elections for National Office
Recognition of Catherine Worthingham Fellows
APTA President Address to the House of Delegates
Chief Executive Officer Address to the House of Delegates
Reports
1. President (Annual Report)
2. House Officers (2015 House Handbook)
3. Secretary’s Report (2015 House Handbook)
4. Treasurer (Annual Report)
5. Nominating Committee (2015 House Handbook)
6. Reference Committee (2015 House Handbook)
7. Reports from Board of Directors to House of Delegates (2015 House Handbook)
Recognition of New Delegates
Introduction of Student House Ushers
Report of Elections
Adjournment
5
TUESDAY, JUNE 2
Adoption of Detailed Agenda (Packet I)
New Business (Packet I)
Adjournment
WEDNESDAY, JUNE 3
Continuation of New Business
Special Orders: 2:00 pm–3:00 pm:
Installation of New Nominating Committee Members
Installation of New Officers and Directors
Recognition of Retiring Nominating Committee Members
Recognition of Retiring Members of the Board of Directors
Adjournment
6
2015 HOUSE OF DELEGATES
AMERICAN PHYSICAL THERAPY ASSOCIATION
DETAILED AGENDA
RC 01-15 Amend: Bylaws of the American Physical Therapy Association and Standing Rules of the American Physical Therapy Association to Change the Length and Number of Terms for Members of the APTA Board of Directors
RC 02-15 Amend: Bylaws of the American Physical Therapy Association to Change the Qualifications for President, Vice President, Secretary, and Treasurer
RC 03-15 Amend: Bylaws of the American Physical Therapy Association to Grant Components the Option of Amending their Bylaws to Provide a Full Vote for Physical Therapist Assistant Members
RC 04-15 Amend: Bylaws of the American Physical Therapy Association to Provide Chapters the Option of Amending their Bylaws to Enable Physical Therapist Assistant Members to Serve as Chapter Delegates
RC 05-15 Amend: Bylaws of the American Physical Therapy Association to Allow Sections to Vote in the House of Delegates
RC 06-15 Amend: Bylaws of the American Physical Therapy Association to Grant Life Members the Privilege of Serving as Delegates to the House of Delegates
RC 07-15 Amend: Bylaws of the American Physical Therapy Association to Grant Physical Therapist Assistant Members the Privilege to Serve on the APTA Board of Directors
RC 08-15 Delivery of Value-Based Physical Therapist Services
RC 10-15 Rescind: Health Care Coverage for All Americans (HOD P06-05-18-27)
RC 11-15 Adopt: Health Priorities for Populations and Individuals
RC 12-15 Adopt: The Role of the Physical Therapist in Diet and Nutrition
RC 13-15 Adopt: The Association’s Role in Advocacy for Prevention, Wellness, Fitness, and Health Promotion, and for Management of Disease and Disability
RC 14-15 Adopt: Physical Therapists’ Role in Prevention, Wellness, Fitness, Health Promotion, and Management of Disease and Disability
RC 15-15 Rescind: Positions Related to Prevention, Wellness, Fitness, Health Promotion, and Management of Disease and Disability
RC 16-15 Adopt: Management of the Movement System
RC 17-15 Adopt: Identification of Physical Therapists by Professional Title
RC 18-15 Adopt: Position Statement on Bullying
7
RC 19-15 Explore the Feasibility of Obtaining Primary Care Practitioner Status
RC 20-15 Collaborations to Address Childhood and Adult Obesity
RC 21-15 Incorporation of Standardized Physical Therapist Patient/Client Management Elements in Electronic Health Records
RC 22-15 Standards and Interoperability for Health Information Technology and Electronic Health Records
RC 23-15 Adopt: Designation of Individuals with Intellectual and Developmental Disabilities as a Medically Underserved Population
For the logic behind the ordering of the motions, please see Appendix A.
8
Appendix A
The Reference Committee has adopted the following categories as a guide for ordering the business of the House.
Category:0 Consent Calendar1 Bylaws2 Standing Rules3 Adoption/Amendment of Mission/Vision/Goals4 Amending/Rescinding Previously Adopted Positions/Standards/Guidelines/Policies/Procedures5 Motions in Response to Previous House Referrals6 Association Positions/Standards/Guidelines/Policies/Procedures - New items7 New Business Related to APTA Vision Statement for the Physical Therapy Profession8 Other New Business
Categories 1-6 consist of motions that can only be handled by the House of Delegates.
Category 7 provides information about activities the House of Delegates would like to debate and potentially direct the Board of Directors to accomplish.
9
Required for Adoption: Previous Notice, 2/3 Vote Category: 1
Motion Contact: Ira Gorman, PT, PhD, MSPH, delegate, Heath Policy and AdministrationPhone: 303/941-2700 E-mail: [email protected]
PROPOSED BY: HEALTH POLICY AND ADMINISTRATION SECTION
COSPONSORED BY:
RC 1-15 AMEND: BYLAWS OF THE AMERICAN PHYSICAL THERAPY ASSOCIATION AND STANDING RULES OF THE AMERICAN PHYSICAL THERAPY ASSOCIATION TO CHANGE THE LENGTH AND NUMBER OF TERMS FOR MEMBERS OF THE APTA BOARD OF DIRECTORS
Note: Triple asterisks (* * *) indicate language that is not being amended and therefore has not been included in order to make the document more concise.
(Note: This is a motion with 2 conforming amendments - Parts A and B.)
That Bylaws of the American Physical Therapy Association and Standing Rules of the American Physical Therapy Association be amended as follows to change the length and number of terms for members of the APTA Board of Directors.
PART A
That Bylaws of the American Physical Therapy Association, Article IX. Board of Directors, Section 4: Tenure, be amended by substitution:
ARTICLE IX. BOARD OF DIRECTORS* * *
Section 4: Tenure
A. The members of the Board of Directors shall be divided into 3 classes for the purposes of election, and the members of each class shall serve the term prescribed by these bylaws. which shall be equal in size or as nearly equal as possible. Each class will include one-third or approximately one-third of the members who are not officers, plus two officers. The Secretary and the Vice Speaker of the House of Delegates shall belong to the first class, which shall be elected in years that are multiples of 3. The Treasurer and the Speaker of the House of Delegates shall belong to the second class, which shall be elected the year after the first class. The President and the Vice President shall belong to the third class, which shall be elected the year after the second class.
B. Members of the Board of Directors shall assume office at the close of the annual session of the House of Delegates at which they were elected.
C. The term of office of each member of the Board of Directors shall be 3 4 years or until their successors are elected.D. No member shall serve more than 3 complete consecutive terms on the Board of Directors or more than 2 complete
consecutive terms 1 complete term in the same office.E. A complete term for a member of the Board of Directors shall be defined as 3 4 years.F. Vacancies
In the event that a position on the Board of Directors becomes vacant, the vacancy shall be filled in the manner prescribed in the standing rules. (Exceptions: President and Speaker of the House of Delegates.)
Proviso: These changes shall affect any member elected at the 2016 annual session or later.
That Standing Rules of the American Physical Therapy Association, 14. Vacancies: Officers and Directors, be amended by substitution:
A. If a vacancy occurs within the first year of a 3 4-year term, the Nominating Committee shall select a candidate(s) for election at the next annual session of the House of Delegates; the elected person shall serve for the remaining 2 3 years of the term.
B. If a vacancy occurs after the first year of a 3 4-year term, the vacancy shall be filled by appointment by the Board of Directors.
C. Notwithstanding Standing Rule 13(B), if a vacancy occurs on the Board of Directors as a result of an election, a second election shall be required. The Nominating Committee shall prepare the slate for the second election, and additional nominations from the floor shall be in order.
All candidates who were slated for any position on the Board of Directors and were not elected in the first election shall will be slated in the second election unless they have indicated otherwise. Candidates who were not elected for the Nominating Committee shall not be automatically slated but may be nominated from the floor.
Proviso: These changes shall affect any member elected at the 2016 annual session or later.
SS: With the limitation of a single term of office the present 3-year term may be too short to accomplish all that a director may wish, and may account for the desire to seek a second term. Lengthening the term of office to a single 4-year term would allow a director to serve a single term and feel fulfilled in their role as director in that office. Additional terms in a different office can still be sought according to the present bylaws.
Many professional associations limit the terms of their officers to 1 term and encourage a healthy turnover of leadership. Nonprofit best practices state that term limits prevent stagnation, perpetual concentration of power within a small group, tiredness, boredom, and loss of commitment by the board.
The advantages of term limits are diversity enhancement, built-in balance of continuity and turnover, regular infusion of fresh ideas and new perspectives, and an increased pool of interested and qualified members to serve on the board of directors. Lack of term limits stifle the interest of members who would like to run for office, but are intimidated by the strength of longstanding incumbents. Leaders should be willing to step up, step away, or step down in order to make way for new leaders, and this process should be planned thoughtfully.1
In addition, by not allowing officers to run for reelection for their same office it prevents the problems of incumbency during the election process.
References:1. Lundy L. Lead, Follow, or Get Out of the Way: Invaluable Insights into Leadership Style. NJ: Pfeiffer & Co; 1996.
CURRENT BYLAW:ARTICLE IX. BOARD OF DIRECTORS
* * *Section 4: Tenure
A. The members of the Board of Directors shall be divided into 3 classes, which shall be equal in size or as nearly equal as possible. Each class will include one-third or approximately one-third of the members who are not officers, plus two officers. The Secretary and the Vice Speaker of the House of Delegates shall belong to the first class, which shall be elected in years that are multiples of 3. The Treasurer and the Speaker of the House of Delegates shall belong to the second class, which shall be elected the year after the first class. The President and the Vice President shall belong to the third class, which shall be elected the year after the second class.
B. Members of the Board of Directors shall assume office at the close of the annual session of the House of Delegates at which they were elected.
C. The term of office of each member of the Board of Directors shall be 3 years or until their successors are elected.D. No member shall serve more than 3 complete consecutive terms on the Board of Directors or more than 2 complete
consecutive terms in the same office.E. A complete term for a member of the Board of Directors shall be defined as 3 years.
F. VacanciesIn the event that a position on the Board of Directors becomes vacant, the vacancy shall be filled in the manner prescribed in the standing rules. (Exceptions: President and Speaker of the House of Delegates.)
CURRENT STANDING RULE:14. VACANCIES: OFFICERS AND DIRECTORS
A. If a vacancy occurs within the first year of a 3-year term, the Nominating Committee shall select a candidate(s) for election at the next annual session of the House of Delegates; the elected person shall serve for the remaining 2 years of the term.
B. If a vacancy occurs after the first year of a 3-year term, the vacancy shall be filled by appointment by the Board of Directors.C. Notwithstanding Standing Rule 13(B), if a vacancy occurs on the Board of Directors as a result of an election, a second
election shall be required. The Nominating Committee shall prepare the slate for the second election and additional nominations from the floor shall be in order.
All candidates who were slated for any position on the Board of Directors and were not elected in the first election will be slated in the second election unless they have indicated otherwise. Candidates who were not elected for the Nominating Committee shall not be automatically slated but may be nominated from the floor.
12
1234567891011121314151617
Required for Adoption: Previous Notice, 2/3 Vote Category: 1
Motion Contact: Ira Gorman, PT, PhD, MSPH, delegate, Health Policy and AdministrationPhone: 303/941-2700 E-mail: [email protected]
RC 2-15 AMEND: BYLAWS OF THE AMERICAN PHYSICAL THERAPY ASSOCIATION TO CHANGE THE QUALIFICATIONS FOR PRESIDENT, VICE PRESIDENT, SECRETARY, AND TREASURER
Note: Triple asterisks (* * *) indicate language that is not being amended and therefore has not been included in order to make the document more concise.
That Bylaws of the American Physical Therapy Association, Article IX. Board of Directors, Section 2: Qualifications, be amended by adding a new C. so that it would read:
ARTICLE IX. BOARD OF DIRECTORS* * *
Section 2: Qualifications
Only Physical Therapist members of the Association can serve, and they are eligible to serve if they have:
A. Have Bbeen Physical Therapist member in good standing for at least 5 years immediately preceding their election or appointment; and,
B. Have Cconsented to serve.; and,C. In the case of the office of President, Vice President, Secretary, and Treasurer, are currently serving or have
previously served as a member of the Board of Directors.
Proviso: This change shall affect any member initially elected to the office of President, Vice President, Secretary, or Treasurer at the 2016 Annual Session or later.
SS: With the proposal to limit the terms of the officers to 1 term it is essential that these members are qualified and prepared to serve and be effective in 1 term. Prior experience on the Board will ensure that these officers are prepared and can then be effective with 1 term of service.
[Note: Changes to the stem and to A. and B. are made for grammatical accuracy if C. is adopted.]
CURRENT BYLAW:
ARTICLE IX. BOARD OF DIRECTORS* * *
Section 2: Qualifications
Only Physical Therapist members of the Association can serve, and they are eligible to serve if they have:
A. Been Physical Therapist members in good standing for at least 5 years immediately preceding their election or appointment, andB. Consented to serve.
RC 3-15 AMEND: BYLAWS OF THE AMERICAN PHYSICAL THERAPY ASSOCIATION TO GRANT COMPONENTS THE OPTION OF AMENDING THEIR BYLAWS TO PROVIDE A FULL VOTE FOR PHYSICAL THERAPIST ASSISTANT MEMBERS
Note: Triple asterisks (* * *) indicate language that is not being amended and therefore has not been included in order to make the document more concise.
That Bylaws of the American Physical Therapy Association, Article IV. Membership, Section 2: Rights and Privileges of Members, B., (2), b., be amended by inserting the words “unless the chapter or section allows such members 1 vote” after the words “one-half vote” so that it would read:
ARTICLE IV. MEMBERSHIP* * *
Section 2: Rights and Privileges of Members * * *
B. Only members in certain categories have the following privileges (subject to restriction as otherwise provided in Association bylaws):
* * *(2) To vote.
a. At House of Delegates meetings: Chapter delegates, 1 vote.b. At chapter or section meetings by members of the chapter or section: Physical Therapist, Retired Physical
Therapist, and Life Physical Therapist, 1 vote; Physical Therapist Assistant, Retired Physical Therapist Assistant, and Life Physical Therapist Assistant, one-half vote unless the chapter or section allows such members 1 vote; except when chapter or section bylaws provide for a representative body.
c. At assembly meetings: Members of the assembly, 1 vote.d. At committee meetings: Any member serving on the committee, 1 vote.
SS: At its November 2014 meeting, the Board of Directors acted on decisions made at its April 2014 meeting to forward several motions to the House of Delegates related to the physical therapist assistant (PTA). The Physical Therapist Assistant Board Work Group was created to address challenges the PTA Caucus was encountering in trying to achieve its goals. This motion is the result of one of the recommendations of the board work group, which ranked the issue of component level vote as the second most important issue under the topic of inclusiveness of the PTA in the Association. Providing the components the option of changing their bylaws to provide a full vote for PTA members respects the rights of components to make this determination.
CURRENT BYLAW:
ARTICLE IV. MEMBERSHIP* * *
Section 2: Rights and Privileges of Members* * *
B. Only members in certain categories have the following privileges (subject to restriction as otherwise provided in Association bylaws):
(2) To vote.a. At House of Delegates meetings: Chapter delegates, 1 vote.b. At chapter or section meetings by members of the chapter or section: Physical Therapist, Retired Physical
Therapist, and Life Physical Therapist, 1 vote; Physical Therapist Assistant, Retired Physical Therapist Assistant, and Life Physical Therapist Assistant, one-half vote; except when chapter or section bylaws provide for a representative body.
c. At assembly meetings: Members of the assembly, 1 vote.d. At committee meetings: Any member serving on the committee, 1 vote.
15
12345678
Required for Adoption: Previous Notice, 2/3 Vote Category: 1
RC 4-15 AMEND: BYLAWS OF THE AMERICAN PHYSICAL THERAPY ASSOCIATION TO PROVIDE CHAPTERS THE OPTION OF AMENDING THEIR BYLAWS TO ENABLE PHYSICAL THERAPIST ASSISTANT MEMBERS TO SERVE AS CHAPTER DELEGATES
Note: Triple asterisks (* * *) indicate language that is not being amended and therefore has not been included in order to make the document more concise.
That Bylaws of the American Physical Therapy Association, Article IV. Membership, Section 2: Rights and Privileges of Members, B., (4), a., be amended by adding the words “and, if permitted by chapter bylaws, Physical Therapist Assistant” after the words “Physical Therapist” so that it would read:
ARTICLE IV. MEMBERSHIP* * *
Section 2: Rights and Privileges of Members * * *
B. Only members in certain categories have the following privileges (subject to restriction as otherwise provided in Association bylaws):
* * *(4) To serve as a delegate to the House of Delegates.
a. As chapter delegate: Physical Therapist and, if permitted by chapter bylaws, Physical Therapist Assistant.b. As section delegate: Physical Therapist and Physical Therapist Assistant.c. As PTA Caucus delegate: Physical Therapist Assistant, subject to qualifications identified in Article VIII., Section
4., of these bylaws.d. As assembly delegate: Assembly member, subject to additional eligibility requirements in the assembly bylaws.
SS: At its November 2014 meeting, the Board of Directors (Board) acted on decisions made at its April 2014 meeting to forward several motions to the House of Delegates (House) related to the physical therapist assistant (PTA). The Physical Therapist Assistant Board Work Group was created to address challenges the PTA Caucus was encountering in trying to achieve its goals. This motion is the result of one of the recommendations of the board work group. The work group members ranked the issue of PTA involvement in the House as the third most important issue under the topic of inclusiveness of the PTA in the association. PTAs prior to RC 1-98 served in chapter delegations and were voting delegates with a different level of apportionment (represented twice as many members) from that of physical therapist (PT) delegates. Providing the chapters the option of changing their bylaws to enable PTA members to serve as delegates respects the rights of chapters to make this determination. This approach would provide an opportunity to intentionally establish a culture of inclusiveness, while allowing each chapter the option to determine if a PTA member candidate for delegate is the preferred choice to represent that chapter.1 The intention with this motion is that PTA member delegates serving as chapter and section delegates would have the same rights and privileges as PT member delegates serving as chapter and section delegates.
B. Only members in certain categories have the following privileges (subject to restriction as otherwise provided in Association bylaws):
* * *(4) To serve as a delegate to the House of Delegates.
a. As chapter delegate: Physical Therapist.b. As section delegate: Physical Therapist and Physical Therapist Assistant.c. As PTA Caucus delegate: Physical Therapist Assistant, subject to qualifications identified in Article VIII., Section 4.,
of these bylaws.d. As assembly delegate: Assembly member, subject to additional eligibility requirements in the assembly bylaws.
17
123456789101112131415
Required for Adoption: Previous Notice, 2/3 Vote Category: 1
Motion Contact: Ira Gorman, PT, PhD, MSPH, delegate, Health Policy and AdministrationPhone: 303/941-2700 E-mail: [email protected]
PROPOSED BY: HEALTH POLICY AND ADMINISTRATION SECTION
COSPONSORED BY: ACUTE CARE, AQUATICS, CARDIOVASCULAR & PULMONARY, CLINICAL ELECTROPHYSIOLOGY & WOUND MANAGEMENT, EDUCATION, FEDERAL, GERIATRICS, HAND REHABILITATION, HOME HEALTH, NEUROLOGY, ONCOLOGY, PEDIATRICS, PRIVATE PRACTICE, RESEARCH, SPORTS, AND WOMEN’S HEALTH SECTIONS
RC 5-15 AMEND: BYLAWS OF THE AMERICAN PHYSICAL THERAPY ASSOCIATION TO ALLOW SECTIONS TO VOTE IN THE HOUSE OF DELEGATES
Note: Triple asterisks (* * *) indicate language that is not being amended and therefore has not been included in order to make the document more concise.
(Note: This is a motion with 11 conforming amendments - Parts A–K.)
PART A
That Bylaws of the American Physical Therapy Association, Article IV. Membership, Section 2: Rights and Privileges of Members, B., (2), a., be amended by inserting the words “and section” after the word “chapter” so that it would read:
Article IV. MEMBERSHIP* * *
Section 2: Rights and Privileges of Members* * *
B. Only members in certain categories have the following privileges (subject to restriction as otherwise provided in Association bylaws):
* * * (2) To vote.
a. At House of Delegates meetings: chapter and section delegates, 1 vote.b. At chapter or section meetings by members of the chapter or section: Physical Therapist, Retired Physical
Therapist, and Life Physical Therapist, 1 vote; Physical Therapist Assistant, Retired Physical Therapist Assistant, and Life Physical Therapist Assistant, one-half vote; except when chapter or section bylaws provide for a representative body.
c. At assembly meetings: Members of the assembly, 1 vote.d. At committee meetings: Any member serving on the committee, 1 vote.
PART B
That Bylaws of the American Physical Therapy Association, Article IV. Membership, Section 2: Rights and Privileges of Members, B., (4), b, be amended by striking out the words “and Physical Therapist Assistant” after the words “Physical Therapist” so that it would read:
Article IV. MEMBERSHIP* * *
Section 2: Rights and Privileges of Members* * *
B. Only members in certain categories have the following privileges (subject to restriction as otherwise provided in Association bylaws):
(4) To serve as a delegate to the House of Delegates.a. As chapter delegate: Physical Therapist.b. As section delegate: Physical Therapist and Physical Therapist Assistant.c. As PTA Caucus delegate: Physical Therapist Assistant, subject to qualifications identified in Article VIII.,
Section 4., of these bylaws.d. As assembly delegate: Assembly member, subject to additional eligibility requirements in the assembly
bylaws.
PART C
That Bylaws of the American Physical Therapy Association, Article VII. Meetings, Section 3: Notice of Sessions, A. Annual Session, be amended by striking out the word “chapter” after the words “to each” so that it would read:
ARTICLE VII. MEETINGS* * *
Section 3: Notice of Sessions
A. Annual SessionThe time and place of the annual session shall be announced in the official journal of the Association, and notice shall be sent to each component president or chair and to each chapter chief delegate at least six weeks before the session is scheduled to convene. This notice may be made by mail or any telecommunications method including, but not limited to, fax and e-mail transmissions which must ensure the timely receipt of the notice and may ensure verifiable receipt of the notice by the intended recipients.
PART D
That Bylaws of the American Physical Therapy Association, Article VIII. House of Delegates, Section 3: Voting Delegates, be amended by substitution:
ARTICLE VIII. HOUSE OF DELEGATES* * *
Section 3: Voting Delegates
The voting delegates of the House of Delegates shall be the chapter and section delegates.
A. Qualifications of Voting Delegates(1) Chapter and section delegates: Only Physical Therapist members may serve as chapter or section delegates.
Only Physical Therapist members who have been Association members in good standing in any category of membership for no fewer than the 2 years immediately preceding the start of the House session may serve as chapter or section delegates.
(2) Members of the Board of Directors may not serve as chapter or section delegates.(3) A delegate of any one component may not serve concurrently as a delegate of another component.
B. Number of Voting DelegatesThe number of each section’s delegates shall be determined according to the standing rules. The number of chapter delegates shall be based on, but not limited to, 400, which shall be apportioned among the chapters on the basis of the number of Physical Therapist, Retired Physical Therapist, Life Physical Therapist, Physical Therapist Assistant, Retired Physical Therapist Assistant, and Life Physical Therapist Assistant members in each chapter according to membership records in the Association headquarters and as described in the standing rules. a target number equal to 436 minus the number of section delegates. The number of each chapter’s delegates shall be based on its member count as determined according to the standing rules. No chapter or section shall have fewer than 2 delegates.
19
12345678910111213141516
181920212223242526272829303132
3435363738394041424344454647484950
C. Selection of Voting DelegatesEach chapter and section shall select the delegates who will represent it at the annual session. Each chapter and section shall designate 1 delegate as its chief delegate.
D. CredentialsCredentials shall be issued by the Association. Delegates shall register and file credentials before the first meeting of the House of Delegates and at such other times as designated by the Officers of the House of Delegates.
E. Voting BodyEach chapter voting delegate shall have 1 vote, except that if any of the delegates to which a chapter or section is entitled does not attend a meeting of the House of Delegates, the vote(s) may be transferred to the remaining member(s) of the delegation who are present in attendance.
PART E
That Bylaws of the American Physical Therapy Association, Article VIII. House of Delegates, Section 4: Nonvoting Delegates, be amended by substitution:
ARTICLE VIII. HOUSE OF DELEGATES* * *
Section 4: Nonvoting Delegates
The nonvoting delegates of the House of Delegates shall be the section delegates, PTA Caucus delegates, Student Assembly delegates, and the members of the Board of Directors.
A. Qualifications of Nonvoting Delegates(1) Section delegates: Only Physical Therapist and Physical Therapist Assistant members may serve as section
delegates. Only Physical Therapist and Physical Therapist Assistant members who have been Association members in good standing in any category of membership for no fewer than the 2 years immediately preceding the start of the House session may serve as section delegates.
(2 1)PTA Caucus delegates: Only Physical Therapist Assistant members who have been Association members in good standing for no fewer than 2 years immediately preceding the start of the House session may serve as PTA Caucus delegates.
(3 2)Student Assembly delegates: Only Student Physical Therapist and Student Physical Therapist Assistant members who have been Association members in good standing for the 4 months immediately preceding the start of the House session may serve as Student Assembly delegates.For the purposes of this subparagraph (2), members who have converted under Article XI, Section 3, from Student Physical Therapist to Physical Therapist or from Student Physical Therapist Assistant to Physical Therapist Assistant shall be deemed members of the Student Assembly until the close of the House of Delegates meeting immediately following the date of graduation and shall be eligible to serve as Student Assembly delegates during that period.
(4 3)Members of the Board of Directors may not serve as section or assembly delegates.(5 4)A section delegate or Student Assembly delegate may not serve concurrently as a delegate of another
component. A PTA Caucus delegate may not serve concurrently as a section delegate.B. Number of Nonvoting Delegates
(1) Section delegates: Each section shall be entitled to 1 delegate.(2 1) PTA Caucus delegates: The PTA Caucus shall be entitled to 5 delegates.(3 2)Student Assembly delegates: The Student Assembly shall be entitled to 2 delegates.
C. Selection of Nonvoting DelegatesEach section, t The PTA Caucus, and the Student Assembly shall select the delegate(s) who will represent it at the House session.
D. CredentialsCredentials shall be issued by the Association. Delegates shall register and file credentials before the first meeting of the House of Delegates and at such other times as designated by the Officers of the House of Delegates.
E. Rights and privileges of nonvoting delegatesSection delegates, PTA Caucus delegates, Student Assembly delegates, and members of the Board of Directors may speak, debate, and make and second motions.
PART F
That Bylaws of the American Physical Therapy Association, Article VIII. House of Delegates, Section 5: Conduct of Business, be amended by substitution:
ARTICLE VIII. HOUSE OF DELEGATES * * *
Section 5: Conduct of Business
A. Officers of the House of Delegates(1) The officers shall be the Speaker of the House of Delegates, the Vice Speaker of the House of Delegates, and the
Secretary.(2) The officers shall be responsible for registering delegates, transferring voting privileges, preparing rules of order
and an agenda for the consideration of the House of Delegates, recording and reporting the proceedings, appointing the Committee to Approve the Minutes, making appointments to the Reference Committee, conducting elections, making editorial changes to the bylaws and standing rules, and performing other duties as determined by these bylaws or the standing rules.
B. QuorumDelegates representing one-third of the chapters and one-third of the sections and numbering one-third of the total number of chapter votes that could be cast if all voting delegates from all chapters were present shall constitute a quorum.
C. Voting(1) Voting on motions and resolutions in the House may be by voice, show of hands, standing, roll call, or use of
electronic equipment.(2) If a decision must be made during the interval between annual sessions, a majority vote of the Board of
Directors may determine that the chapter voting delegates be polled by mail. These delegates shall be those registered at the immediately preceding session of the House of Delegates. If the delegate is no longer a member of the chapter or section or holds membership in a category other than that held when the delegate registered at the immediately preceding session of the House of Delegates or for any other reason no longer meets the qualifications for delegate, an alternate delegate shall be named by that chapter or section. At least 50 percent of the ballots of the eligible delegates must be returned to validate the vote.
(3) Election of officers, directors, and members of the Nominating Committee shall be by ballot or use of electronic equipment. Officers shall be elected by a majority of the votes cast. Directors and members of the Nominating Committee shall be elected by a plurality of the votes cast. If the vote fails to determine election, reballoting shall be conducted under procedures determined by the Officers of the House of Delegates.
D. Memorials and ResolutionsOnly memorials or resolutions adopted by the House of Delegates can be issued validly in the name of the Association.
PART G
That Bylaws of the American Physical Therapy Association, Article XIV. Amendments be amended by substitution:
ARTICLE XIV. AMENDMENTS
These bylaws may be amended at the Annual Session of the House of Delegates in years ending in 0 and 5 by the affirmative vote of at least two-thirds of the chapter voting delegates present and voting, or at any special session of the House of Delegates or the Annual Session of the House of Delegates during years not ending in 0 or 5 by the consent to consider, without debate, of two-thirds of the chapter voting delegates present and voting and by the affirmative vote of at least two-thirds of the chapter voting delegates present and voting, providing the following:A. Any proposed amendment has been submitted in writing to the Association’s headquarters by a date set by the Speaker
of the House of Delegates, which shall be at least 4 months but no more than 5 months before the session of the House of Delegates.
B. Copies of all proposed amendments have been printed in an Association publication or distributed to all Association members at least 2 months before the session of the House of Delegates. This distribution may be made by mail or any telecommunications method including, but not limited to, fax and e-mail transmissions, which must ensure the timely receipt of the notice and may ensure verifiable receipt of the notice by the intended recipients.
Bylaw amendments pertaining to Article XI: Finance, Section 3: Dues, may be amended at any Annual Session or special session of the House of Delegates by the affirmative vote of at least two-thirds of the chapter voting delegates present and voting, provided that the conditions of subparagraphs A and B above are satisfied.
PART H
That Standing Rules of the American Physical Therapy Association, 10. Delegate Credentials, be amended by substitution:
10. DELEGATE CREDENTIALS
Component Delegates: Chapter or section delegate credentials shall be signed by the chapter or section president or the chapter or section chief delegate. The designation of chief delegate shall be indicated on the appropriate chapter or section credential. Section or aAssembly delegate credentials shall be signed by the section or assembly president.
PART I
That Standing Rules of the American Physical Therapy Association, 11. Formula for Determining the Size of the House of Delegates, be amended by substitution:
11. FORMULA FOR DETERMINING THE SIZE OF THE HOUSE OF DELEGATES
(1) Add the number of Physical Therapist, Retired Physical Therapist, and Life Physical Therapist members and one-half of the number of Physical Therapist Assistant, Retired Physical Therapist Assistant, and Life Physical Therapist Assistant members of the Association who are assigned to chapters as of June 30 of the year preceding the House of Delegates in which they will serve.
(2) Divide the total found in Step 1 by 400. This shall be the apportionment number.(3) Divide the total number of Physical Therapist, Retired Physical Therapist, and Life Physical Therapist members and
one-half of the number of Physical Therapist Assistant, Retired Physical Therapist Assistant, and Life Physical Therapist Assistant members for each chapter by the apportionment number.
(4) Chapters shall be allowed one delegate for each whole number and one additional delegate for any remainder equaling or exceeding 50 percent of the apportionment number.
(5) Any chapter that would be entitled to fewer than 2 delegates according to the above shall be allowed 2 delegates.(1) For each year the number of voting delegates in the House of Delegates shall be the sum of the section delegates
and the chapter delegates, as determined in accordance with this Standing Rule.(2) For the purpose of determining the number of voting delegates to the House of Delegates for any year, the member
count of each chapter shall be determined by adding the number of its Physical Therapist, Retired Physical Therapist, and Life Physical Therapist members and one-half of the number of its Physical Therapist Assistant, Retired Physical Therapist Assistant, and Life Physical Therapist Assistant members as of June 30 of the preceding year.
(3) Each section shall be entitled to 2 delegates . (4) The chapter delegate target shall be the difference between 436 and the number of section delegates. (5) The number of delegates to which each chapter is entitled shall be determined as follows:
(a) Add the member counts of all chapters and divide the sum by the chapter delegate target. This quotient shall be the chapter apportionment number.
(b) For each chapter, divide its member count by the chapter apportionment number. The chapter shall be allowed the number of delegates obtained by rounding this quotient to the nearest whole number, except that each chapter shall be allowed at least 2 delegates.
PART J
That Standing Rules of the American Physical Therapy Association, 12. Mail Ballot, be amended by substitution:
12. MAIL BALLOTWhen the Board of Directors determines to conduct a mail ballot, according to Article VIII, Section 5., C., (2) of the bylaws, a ballot shall be prepared and distributed as follows:
A. The question to be decided and appropriate supporting information shall be provided with the ballot.B. Instructions for completing and returning the ballot shall be printed on the ballot.C. The deadline for receipt of ballots at the Association's headquarters shall be printed on the ballot, and this
deadline shall be no fewer than 30 days after the date mailed to the all voting delegates.D. An addressed envelope (to the Association's headquarters) and a plain envelope shall be included in the mailing.E. The ballots shall be mailed by first class mail to each chapter voting delegate.F. The voting delegate shall place the completed ballot in the plain envelope, place the plain envelope in the
envelope addressed to the Association's headquarters, sign the outside envelope, and mail it to Association headquarters.
G. The Officers of the House of Delegates shall be responsible for opening and counting the returned ballots and preparing a report of the results of the vote.
PART K
That Standing Rules of the American Physical Therapy Association, 20. Consent Calendar, D., be amended by striking out the word “section,” after the word “chief,” so that it would read:
20. CONSENT CALENDAR
A. The officers of the House of Delegates shall prepare a list of recommended motions that are routine, standard, non-controversial, or self-explanatory and where general approval is anticipated, for placement on a consent calendar.
B. The preliminary consent calendar will be distributed 3 weeks prior to the start of the first meeting of the House of Delegates.
C. Prior to the first meeting of the House of Delegates motions may be removed from the consent calendar by the officers of the House of Delegates or at the request of 5 chief delegates.
D. The revised consent calendar will be prepared by the officers of the House of Delegates for presentation to chief, section, and assembly delegates prior to the first meeting of the House of Delegates.
E. Following the opening of the House of Delegates motions may be removed from the consent calendar by an affirmative vote of one-third of the voting body of the House of Delegates.
F. If a motion is removed from the consent calendar, it shall be placed appropriately in the order of business previously assigned by the Speaker of the House and the chair of the Reference Committee.
G. The consent calendar shall be presented for adoption in a single motion.
Proviso: These amendments to the bylaws and standing rules shall take effect at the close of business of the 2015 House of Delegates.
SS: The APTA House of Delegates (House) is the policy-making body of the association comprising voting chapter delegates and non-voting delegates representing the sections, assemblies and PTA Caucus and consultants. At present, the number of voting delegates is 400 and this is determined each year based on membership numbers within the 51 chapters operating in the United States and its territories, as of June 30, annually. Voting delegates make decisions on issues that may have far-reaching implications for the association, the APTA membership and for the profession of physical therapy. Data indicate that members are motivated to join and participate in APTA primarily through the sections. Providing voting rights to sections increases membership participation and representation. Raising the target number for the House of Delegates to 436 provides each of the 18 sections 2 voting delegates. The chapters will not lose any voting delegates relative to the current apportionment.
When the House was formed in 1944, only the Schools Section, later to become the Education Section, existed. APTA and the sections have continued to evolve, but the House has retained its apportionment model giving voting rights solely to chapter delegates. In 2013, 18 sections represent the breadth and depth of professional practice, education, and research in physical therapy. Year-end membership data (as of December 31, 2012) indicates that 63.0% of physical therapist members belong to at least 1 section and 50.3% of all members belong to at least 1 section. The APTA Governance Review Task Force (GRTF) conducted a survey in 2010, and results revealed that APTA members believe section delegates should be provided a vote in the House. The survey results indicate that this change to voting structure of APTA governance was the fourth most important topic that the House should consider.
The 18 special interest sections—Acute Care, Aquatic Physical Therapy, Cardiovascular and Pulmonary, Clinical Electrophysiology and Wound Management, Education, Federal Physical Therapy, Geriatric Physical Therapy, Hand Rehabilitation, Health Policy and Administration, Home Health, Neurology, Oncology, Orthopaedic, Pediatric, Private Practice, Research, Sports Physical Therapy, and Women’s Health—have maintained a longstanding and influential voice in the APTA House of Delegates, exercising all delegate rights except for the opportunity to vote. Providing each section with a vote is inclusive of all stakeholders, relative to the multifaceted decision-making that occurs within the APTA House of Delegates. The sections and the APTA membership have indicated a ”vote for the voice” is of importance. Chapters have clearly indicated that the representative apportionment vote for the chapters should not be altered in this member-driven association, and chapters would not lose any representative voice by providing voting rights to the sections.
CURRENT BYLAW:PART A
Article IV. MEMBERSHIP* * *
Section 2: Rights and Privileges of Members* * *
B. Only members in certain categories have the following privileges (subject to restriction as otherwise provided in Association bylaws):
* * * (2) To vote.
a. At House of Delegates meetings: Chapter delegates, 1 vote.b. At chapter or section meetings by members of the chapter or section: Physical Therapist, Retired Physical
Therapist, and Life Physical Therapist, 1 vote; Physical Therapist Assistant, Retired Physical Therapist Assistant, and Life Physical Therapist Assistant, one-half vote; except when chapter or section bylaws provide for a representative body.
c. At assembly meetings: Members of the assembly, 1 vote.d. At committee meetings: Any member serving on the committee, 1 vote.
B. Only members in certain categories have the following privileges (subject to restriction as otherwise provided in Association bylaws):
* * * (4) To serve as a delegate to the House of Delegates.
a. As chapter delegate: Physical Therapist.b. As section delegate: Physical Therapist and Physical Therapist Assistant.c. As PTA Caucus delegate: Physical Therapist Assistant, subject to qualifications identified in Article VIII.,
Section 4., of these bylaws.d. As assembly delegate: Assembly member, subject to additional eligibility requirements in the assembly
bylaws.
PART C
A. ANNUAL SESSION
Article IV. MEETINGS* * *
Section 3: Notice of Sessions* * *
A. Annual Session The time and place of the annual session shall be announced in the official journal of the Association, and notice shall be sent to each component president or chair and to each chapter chief delegate at least six weeks before the session is scheduled to convene. This notice may be made by mail or any telecommunications method including, but not limited to, fax and e-mail transmissions which must ensure the timely receipt of the notice and may ensure verifiable receipt of the notice by the intended recipients.
Part D
Article VIII. House of Delegates* * *
Section 3: Voting Delegates* * *
The voting delegates of the House of Delegates shall be the chapter delegates.A. Qualifications of Voting Delegates
(1) Chapter delegates: Only Physical Therapist members may serve as chapter delegates. Only Physical Therapist members who have been Association members in good standing in any category of membership for no fewer than the 2 years immediately preceding the start of the House session may serve as chapter delegates.
(2) Members of the Board of Directors may not serve as chapter delegates.(3) A delegate of any one component may not serve concurrently as a delegate of another component.
B. Number of Voting DelegatesThe number of chapter delegates shall be based on, but not limited to 400, which shall be apportioned among the chapters on the basis of the number of Physical Therapist, Retired Physical Therapist, Life Physical Therapist, Physical Therapist Assistant, Retired Physical Therapist Assistant, and Life Physical Therapist Assistant members in each chapter according to membership records in the Association headquarters and as described in the standing rules.
C. Selection of Voting DelegatesEach chapters shall select the delegates who will represent it at the annual session. Each chapter shall designate 1 delegate as its chief delegate.
D. CredentialsCredentials shall be issued by the Association. Delegates shall register and file credentials before the first meeting of the House of Delegates and at such other times as designated by the Officers of the House of Delegates.
E. Voting BodyEach delegate shall have 1 vote, except that if any of the delegates to which a chapter is entitled does not attend a meeting of the House of Delegates, the vote(s) may be transferred to the remaining member(s) of the delegation who are present.
PART E
Article VIII. House of Delegates * * *
Section 4: Nonvoting Delegates* * *
The nonvoting delegates of the House of Delegates shall be the section delegates, PTA Caucus delegates, Student Assembly delegates, and the members of the Board of Directors.
A. Qualifications of Nonvoting Delegates(1) Section delegates: Only Physical Therapist and Physical Therapist Assistant members may serve as section
delegates. Only Physical Therapist and Physical Therapist Assistant members who have been Association members in good standing in any category of membership for no fewer than the 2 years immediately preceding the start of the House session may serve as section delegates.
(2) PTA Caucus delegates: Only Physical Therapist Assistant members who have been Association members in good standing for no fewer than 2 years immediately preceding the start of the House session may serve as PTA Caucus delegates.
(3) Student Assembly delegates: Only Student Physical Therapist and Student Physical Therapist Assistant members who have been Association members in good standing for the 4 months immediately preceding the start of the House session may serve as Student Assembly delegates.For the purposes of this subparagraph (3), members who have converted under Article XI, Section 3, from Student Physical Therapist to Physical Therapist or from Student Physical Therapist Assistant to Physical Therapist Assistant shall be deemed members of the Student Assembly until the close of the House of Delegates meeting immediately following the date of graduation and shall be eligible to serve as Student Assembly delegates during that period.
(4) Members of the Board of Directors may not serve as section or assembly delegates.(5) A section delegate or Student Assembly delegate may not serve concurrently as a delegate of another component.
A PTA Caucus delegate may not serve concurrently as a section delegate.B. Number of Nonvoting Delegates
(1) Section delegates: Each section shall be entitled to 1 delegate.(2) PTA Caucus delegates: The PTA Caucus shall be entitled to 5 delegates.(3) Student Assembly delegates: The Student Assembly shall be entitled to 2 delegates.
C. Selection of Nonvoting DelegatesEach section, the PTA Caucus, and the Student Assembly shall select the delegate(s) who will represent it at the House session.
D. CredentialsCredentials shall be issued by the Association. Delegates shall register and file credentials before the first meeting of the House of Delegates and at such other times as designated by the Officers of the House of Delegates.
E. Rights and privileges of nonvoting delegatesSection delegates, PTA Caucus delegates, Student Assembly delegates, and members of the Board of Directors may speak, debate, and make and second motions.
A. Officers of the House of Delegates(1) The officers shall be the Speaker of the House of Delegates, the Vice Speaker of the House of Delegates, and the
Secretary.(2) The officers shall be responsible for registering delegates, transferring voting privileges, preparing rules of order
and an agenda for the consideration of the House of Delegates, recording and reporting the proceedings, appointing the Committee to Approve the Minutes, making appointments to the Reference Committee, conducting elections, making editorial changes to the bylaws and standing rules, and performing other duties as determined by these bylaws or the standing rules.
B. QuorumDelegates representing one-third of the chapters and numbering one-third of the total number of chapter votes that could be cast if all delegates from all chapters were present shall constitute a quorum.
C. Voting(1) Voting on motions and resolutions in the House may be by voice, show of hands, standing, roll call, or use of
electronic equipment.(2) If a decision must be made during the interval between annual sessions, a majority vote of the Board of Directors
may determine that the chapter voting delegates be polled by mail. These delegates shall be those registered at the immediately preceding session of the House of Delegates. If the delegate is no longer a member of the chapter or holds membership in a category other than that held when the delegate registered at the immediately preceding session of the House of Delegates or for any other reason no longer meets the qualifications for delegate, an alternate delegate shall be named by that chapter. At least 50 percent of the ballots of the eligible delegates must be returned to validate the vote.
(3) Election of officers, directors, and members of the Nominating Committee shall be by ballot or use of electronic equipment. Officers shall be elected by a majority of the votes cast. Directors and members of the Nominating Committee shall be elected by a plurality of the votes cast. If the vote fails to determine election, reballoting shall be conducted under procedures determined by the Officers of the House of Delegates.
D. Memorials and ResolutionsOnly memorials or resolutions adopted by the House of Delegates can be issued validly in the name of the Association.
PART G
ARTICLE XIV. AMENDMENTS
These bylaws may be amended at the Annual Session of the House of Delegates in years ending in 0 and 5 by the affirmative vote of at least two-thirds of the chapter delegates present and voting, or at any special session of the House of Delegates or the Annual Session of the House of Delegates during years not ending in 0 or 5 by the consent to consider, without debate, of two-thirds of the chapter delegates present and voting and by the affirmative vote of at least two-thirds of the chapter delegates present and voting, providing the following:
A. Any proposed amendment has been submitted in writing to the Association’s headquarters by a date set by the Speaker of the House of Delegates, which shall be at least 4 months but no more than 5 months before the session of the House of Delegates.
B. Copies of all proposed amendments have been printed in an Association publication or distributed to all Association members at least 2 months before the session of the House of Delegates. This distribution may be made by mail or any telecommunications method including, but not limited to, fax and e-mail transmissions, which must ensure the timely receipt of the notice and may ensure verifiable receipt of the notice by the intended recipients.
Bylaw amendments pertaining to Article XI: Finance, Section 3: Dues, may be amended at any Annual Session or special session of the House of Delegates by the affirmative vote of at least two-thirds of the chapter delegates present and voting, provided that the conditions of subparagraphs A and B above are satisfied.
Component Delegates: Chapter delegate credentials shall be signed by the chapter president or the chapter chief delegate. The designation of chief delegate shall be indicated on the appropriate chapter credential. Section or assembly delegate credentials shall be signed by the section or assembly president.
PART I
11. FORMULA FOR DETERMINING THE SIZE OF THE HOUSE OF DELEGATES
(1) Add the number of Physical Therapist, Retired Physical Therapist, and Life Physical Therapist members and one-half of the number of Physical Therapist Assistant, Retired Physical Therapist Assistant, and Life Physical Therapist Assistant members of the Association who are assigned to chapters as of June 30 of the year preceding the House of Delegates in which they will serve.
(2) Divide the total found in Step 1 by 400. This shall be the apportionment number.(3) Divide the total number of Physical Therapist, Retired Physical Therapist, and Life Physical Therapist members and one-
half of the number of Physical Therapist Assistant, Retired Physical Therapist Assistant, and Life Physical Therapist Assistant members for each chapter by the apportionment number.
(4) Chapters shall be allowed one delegate for each whole number and one additional delegate for any remainder equaling or exceeding 50 percent of the apportionment number.
(5) Any chapter that would be entitled to fewer than 2 delegates according to the above shall be allowed 2 delegates.
PART J
12. MAIL BALLOT
When the Board of Directors determines to conduct a mail ballot, according to Article VIII, Section 5., C., (2) of the bylaws, a ballot shall be prepared and distributed as follows:
A. The question to be decided and appropriate supporting information shall be provided with the ballot.B. Instructions for completing and returning the ballot shall be printed on the ballot.C. The deadline for receipt of ballots at the Association's headquarters shall be printed on the ballot, and this
deadline shall be no fewer than 30 days after the date mailed to the delegates.D. An addressed envelope (to the Association's headquarters) and a plain envelope shall be included in the mailing.E. The ballots shall be mailed by first class mail to each chapter delegate.F. The delegate shall place the completed ballot in the plain envelope, place the plain envelope in the envelope
addressed to the Association's headquarters, sign the outside envelope, and mail it to Association headquarters.G. The Officers of the House of Delegates shall be responsible for opening and counting the returned ballots and
preparing a report of the results of the vote.
PART K
20. CONSENT CALENDAR
A. The officers of the House of Delegates shall prepare a list of recommended motions that are routine, standard, non-controversial, or self-explanatory and where general approval is anticipated, for placement on a consent calendar.
B. The preliminary consent calendar will be distributed 3 weeks prior to the start of the first meeting of the House of Delegates.
C. Prior to the first meeting of the House of Delegates motions may be removed from the consent calendar by the officers of the House of Delegates or at the request of 5 chief delegates.
D. The revised consent calendar will be prepared by the officers of the House of Delegates for presentation to chief, section, and assembly delegates prior to the first meeting of the House of Delegates.
E. Following the opening of the House of Delegates motions may be removed from the consent calendar by an affirmative vote of one-third of the voting body of the House of Delegates.
F. If a motion is removed from the consent calendar, it shall be placed appropriately in the order of business previously assigned by the Speaker of the House and the chair of the Reference Committee.
G. The consent calendar shall be presented for adoption in a single motion.
29
123
Required for Adoption: Previous Notice, 2/3 Vote Category: 1
COSPONSORED BY: KENTUCKY, MISSISSIPPI, VIRGINIA AND WEST VIRGINA CHAPTERS AND FEDERAL, ONCOLOGY, PEDIATRICS AND RESEARCH SECTIONS
RC 6-15 AMEND: BYLAWS OF THE AMERICAN PHYSICAL THERAPY ASSOCIATION TO GRANT LIFE MEMBERS THE PRIVILEGE OF SERVING AS DELEGATES TO THE HOUSE OF DELEGATES
Note: Triple asterisks (* * *) indicate language that is not being amended and therefore has not been included in order to make the document more concise.
(Note: This is a motion with 3 conforming amendments - Parts A–C.)
That Bylaws of the American Physical Therapy Association be amended to grant Life Members the privilege to serve as delegates to the House of Delegates:
PART A
That Bylaws of the American Physical Therapy Association, Article IV. Membership, Section 2: Rights and Privileges of Members, B., (4), To serve as a delegate to the House of Delegates, be amended by substitution:
ARTICLE IV. MEMBERSHIP* * *
Section 2: Rights and Privileges of Members* * *
B. Only members in certain categories have the following privileges (subject to restriction as otherwise provided in Association bylaws):
* * *(4) To serve as a delegate to the House of Delegates.
a. As chapter delegate: Physical Therapist and Life Physical Therapist.b. As a section delegate: Physical Therapist and Life Physical Therapist, and Physical Therapist Assistant and Life
Physical Therapist Assistant.c. As PTA Caucus delegate: Physical Therapist Assistant, subject to qualifications identified in Article VIII., Section
4., of these bylaws.d. As assembly delegate: Assembly member, subject to additional eligibility requirements in the assembly bylaws.
That Bylaws of the American Physical Therapy Association, Article VIII. House of Delegates, Section 3: Voting Delegates, A., (1), be amended by substitution:
ARTICLE VIII. HOUSE OF DELEGATES* * *
Section 3: Voting Delegates* * *
A. Qualifications of Voting Delegates(1) Chapter delegates: Only Physical Therapist and Life Physical Therapist members may serve as chapter delegates.
Only Physical Therapist and Life Physical Therapist members who have been Association members in good standing in any category of membership for no fewer than the 2 years immediately preceding the start of the House session may serve as chapter delegates.
PART C
That Bylaws of the American Physical Therapy Association, Article VIII. House of Delegates, Section 4: Nonvoting Delegates, A., (1), be amended by substitution:
Article VIII. House of Delegates* * *
Section 4: Nonvoting Delegates* * *
A. Qualifications of Nonvoting Delegates(1) Section delegates: Only Physical Therapist, Life Physical Therapist, Physical Therapist Assistant and Life Physical
Therapist Assistant members may serve as section delegates. Only Physical Therapist, Life Physical Therapist, Physical Therapist Assistant, and Life Physical Therapist Assistant members who have been Association members in good standing in any category of membership for no fewer than the 2 years immediately preceding the start of the House session may serve as section delegates.
SS: To qualify for Life membership, a physical therapist must meet 1 of the following qualifications: Be 65 years of age or older and have completed 30 years of membership; or No longer be able to practice physical therapy due to a permanent disability and have been an APTA member for at
least 5 years
Life members have a wealth of knowledge and experience that is incredibly valuable to both the profession and the Association. While these members have elected, by virtue of age and length of active membership or due to disability, to choose the Life membership category, their contributions and opportunities to influence the direction of the profession and association should be welcomed and embraced, rather than subdued.
According to APTA Membership1 statistics, there are currently 1,307 current PT members qualified for Life membership based strictly on age (65>) and years of membership (30>=); as of October 2014 there were 777 Life members (dues) and 1,789 Life members (no dues). Life members prior to 2003 pay no dues; Life members following 2003 or later pay $60 annual national dues. There is no way of knowing how many active members would choose to change to the Life category should this bylaw amendment pass. The likely fiscal impact would not seem to be a major impact to APTA’s financial position.
Sarah Sladek makes important points in her book, The End of Membership as We Know It, based on best practice for membership organizations. She discusses 3 key shifts in society that have caused a decline in membership for organizations.2 While this is not the case for APTA, a thriving membership organization approaching the 90,000 mark, it is prudent to heed the advice, to continue the course. Fundamentally, Sladek states that shifts in declining membership are related to: “economic recession, demographic shifts, and rapidly changing technology.”2 This amendment addresses the opportunity to offer benefits to those who have given much to the profession and, for those who are interested, to offer viability for them to continue to serve as delegates for the highest policymaking body of the profession; while they retain their honored category of Life member, which is well earned and deserved.
References:1. APTA Membership Statistics, provided by Scharan Johnson, CAE, Director Membership Development, APTA, email communication, October 20, 2014.2. Sladek SL. The End of Membership as We Know It: Building the Fortune-Flipping, Must-Have Association of the Next Century. Wiley; August 2013.
APTA Membership DataProvided by Scharan M. Johnson, CAE, Director Membership Development APTA
Member Qualifications Prescribed by the Board of Directors:http://www.apta.org/Policies/Membership/Membership Rights and Privileges/Eligibility:http://www.apta.org/uploadedFiles/APTAorg/About_Us/Policies/General/MembershipRightsPrivileges.pdfhttp://www.apta.org/Membership/TypesEligibility/RetiredorLife/
Life Member Eligibility: Members can apply for Life Member Status with reduced membership dues and access to benefits when they reach the age of 65 or older and have completed at least 30 years of membership. They may also be eligible if they are no longer able to practice physical therapy due to a permanent disability and have been members for at least 5 years
Retired Member Eligibility: Members can apply for Retired Member Status with reduced membership dues and access to benefits when they reach the age of 55 or older and have completed at least 20 years of membership. Retired applicants must no longer work in an occupation related to physical therapy.
Current Members (as of October 2014)
1,307 current PT members qualify for LIFE membership based strictly on age (65>=) and years member (30>=). 7,201 current PT members may qualify for Retired membership based on age (55>=) and years member (20>=).
However, a key eligibility requirement for Retired membership is that an applicant must attest annually that he/she no longer works in an occupation related to physical therapy .
Count of Life/Retired Members by Chapter (October 2014) Life/Retired Members Trends*
LIFE – PT Life member became a life member prior to 2003 and pays no dues. Existing life members were grandfathered into this category back in 2003.
LIFE2 – PT Life member became a life member in 2003 or later and pays reduced dues ($60 National + Chapter/Section Dues if applicable).
RETIR – PT member is retired and pays reduced dues ($120 National + Chapter/Section Dues if applicable).
B. Only members in certain categories have the following privileges (subject to restriction as otherwise provided in Association bylaws):
* * *(4) To serve as a delegate to the House of Delegates.
a. As chapter delegate: Physical Therapist.b. As a section delegate: Physical Therapist and Physical Therapist Assistant.c. As PTA Caucus delegate: Physical Therapist Assistant, subject to qualifications identified in Article VIII., Section 4.,
of these bylaws.d. As assembly delegate: Assembly member, subject to additional eligibility requirements in the assembly bylaws.
PART B
ARTICLE VIII. HOUSE OF DELEGATES* * *
Section 3: Voting Delegates
A. Qualifications of Voting Delegates(1) Chapter delegates: Only Physical Therapist members may serve as chapter delegates. Only Physical Therapist members
who have been Association members in good standing in any category of membership for no fewer than the 2 years immediately preceding the start of the House session may serve as chapter delegates.
(2) Members of the Board of Directors may not serve as chapter delegates.(3) A delegate of any one component may not serve concurrently as a delegate of another component.
PART C
ARTICLE VIII. HOUSE OF DELEGATES* * *
Section 4: Nonvoting Delegates
A. Qualifications of Nonvoting Delegates(1) Section delegates: Only Physical Therapist and Physical Therapist Assistant members may serve as section delegates.
Only Physical Therapist and Physical Therapist Assistant members who have been Association members in good standing in any category of membership for no fewer than the 2 years immediately preceding the start of the House session may serve as section delegates.
(2) PTA Caucus delegates: Only Physical Therapist Assistant members who have been Association members in good standing for no fewer than 2 years immediately preceding the start of the House session may serve as PTA Caucus delegates.
(3) Student Assembly delegates: Only Student Physical Therapist and Student Physical Therapist Assistant members who have been Association members in good standing for the 4 months immediately preceding the start of the House session may serve as Student Assembly delegates.
For the purposes of this subparagraph (3), members who have converted under Article XI, Section 3, from Student Physical Therapist to Physical Therapist or from Student Physical Therapist Assistant to Physical Therapist Assistant shall be deemed members of the Student Assembly until the close of the House of Delegates meeting immediately following the date of graduation and shall be eligible to serve as Student Assembly delegates during that period.
(4) Members of the Board of Directors may not serve as section or assembly delegates.(5) A section delegate or Student Assembly delegate may not serve concurrently as a delegate of another component.
APTA Caucus delegate may not serve concurrently as a section delegate.
35
1234567
Required for Adoption: Previous Notice, 2/3 Vote Category: 1
RC 7-15 AMEND: BYLAWS OF THE AMERICAN PHYSICAL THERAPY ASSOCIATION TO GRANT PHYSICAL THERAPIST ASSISTANT MEMBERS THE PRIVILEGE TO SERVE ON THE APTA BOARD OF DIRECTORS
Note: Triple asterisks (* * *) indicate language that is not being amended and therefore has not been included in order to make the document more concise.
(Note: This is a motion with 2 conforming amendments - Parts A and B.)
That Bylaws of the American Physical Therapy Association be amended as follows to grant Physical Therapist Assistant members the privilege to serve on the APTA Board of Directors:
PART A
That Bylaws of the American Physical Therapy Association, Article IV. Membership, Section 2: Rights and Privileges of Members, B., (3), a., be amended by adding the words “; Physical Therapist Assistant members may serve on the Board of Directors, but not as President, Vice President, Treasurer, Secretary, Speaker of the House of Delegates, or Vice Speaker of the House of Delegates” after the words “Physical Therapist” so that it would read:
ARTICLE IV. MEMBERSHIP* * *
Section 2: Rights and Privileges of Members* * *
B. Only members in certain categories have the following privileges (subject to restriction as otherwise provided in Association bylaws):
* * *(3) To hold office.
a. For the Association: Physical Therapist; Physical Therapist Assistant members may serve on the Board of Directors, but not as President, Vice President, Treasurer, Secretary, Speaker of the House of Delegates, or Vice Speaker of the House of Delegates.
PART B
That Bylaws of the American Physical Therapy Association, Article IX. Board of Directors, Section 2: Qualifications, be amended by substitution so that it would read:
ARTICLE IX. BOARD OF DIRECTORS* * *
Section 2: Qualifications
Only Physical Therapist or Physical Therapist Assistant members of the Association can are eligible to serve, except that only Physical Therapist members are eligible to serve as President, Vice President, Treasurer, Secretary, Speaker of the House of Delegates, or Vice Speaker of the House of Delegates. and they Members are not eligible to serve if unless they have:A. Been Physical Therapist or Physical Therapist Assistant members in good standing for at least 5 years immediately
preceding their election or appointment, and B. Consented to serve.
SS: At its November 2014 meeting, the Board of Directors acted on decisions, made at its April 2014 meeting, to forward several motions to the House of Delegates related to the physical therapist assistant (PTA). The Physical Therapist Assistant Board Work
Group was created to address challenges the PTA Caucus was encountering in trying to achieve its goals. This motion is the result of 1 of the recommendations of the work group, which ranked the issue of representation on the Board as the most important issue under the topic of inclusiveness of the PTA in the association.
CURRENT BYLAW:PART A
ARTICLE IV. MEMBERSHIP* * *
2: Rights and Privileges of Members* * *
B. Only members in certain categories have the following privileges (subject to restriction as otherwise provided in Association bylaws):
* * *(3) To hold office.
a. For the Association: Physical Therapist.b. For the chapter or section: Physical Therapist, Retired Physical Therapist, and Life Physical Therapist, subject to
additional eligibility requirements in the chapter or section bylaws; when provided for in the chapter or section bylaws, Physical Therapist Assistant, Retired Physical Therapist Assistant, and Life Physical Therapist Assistant members may hold office, with the exception of the office of president, president elect, vice president, chief delegate, or any position that may succeed to the presidency, subject to additional eligibility requirements in the chapter or section bylaws.
c. For the assembly: Assembly member, subject to additional eligibility requirements in the assembly bylaws.
PART B
ARTICLE IX. BOARD OF DIRECTORS* * *
Section 2: Qualifications* * *
Only Physical Therapist members of the Association can serve, and they are eligible to serve if they have:A. Been Physical Therapist members in good standing for at least 5 years immediately preceding their election or
RC 8-15 DELIVERY OF VALUE-BASED PHYSICAL THERAPIST SERVICES
(Note: This is a motion with 2 conforming amendments - Parts A and B.)
PART AThat the following position be adopted:
DELIVERY OF VALUE-BASED PHYSICAL THERAPIST SERVICES
Physical therapists are health professionals who transform society by optimizing movement to improve the human experience. As such, it is the position of the American Physical Therapy Association (APTA) that all individuals should have access to physical therapist services, and that physical therapists should be accountable for the quality and effectiveness of those services. Achieving these goals requires a value-based system for the delivery of physical therapist services that compensates physical therapists fairly and equitably. The principles of a value-based system include access, quality, and accountability, each grounded in a patient- and client-centered approach to delivery.
PRINCIPLE I. ACCESS TO PHYSICAL THERAPIST SERVICES
A. REDUCING BARRIERS TO PHYSICAL THERAPIST SERVICES
1. As an essential health benefit, APTA supports the inclusion of physical therapist services in all appropriate health care policies, including, but not limited to:a. Insurance policies by third-party payers and state, federal, or any other regulatory agencies;b. Title XIX of the Social Security Act (the Medicaid program) at the state and federal levels; andc. State and federal workers’ compensation programs.
2. APTA supports state and federal legislation that limits the patient’s and client’s financial responsibility to less than the actual amount paid by insurance carriers and insurance intermediaries to the provider for physical therapist services.
3. APTA supports state and federal legislation that requires payers to develop and use consistent terminology regarding coverage of physical therapist services.
4. APTA supports the inclusion of physical therapist services in all appropriate telehealth policies, regulations, and legislation by third-party payers and state, federal, and any other regulatory agencies.
B. LIABILITY REFORM FOR PHYSICAL THERAPIST SERVICES
APTA supports comprehensive liability reform that puts patient and client safety first while working to reduce preventable injuries and improve communication between physical therapists and their patients and clients. To achieve these goals, protections must be put in place for physical therapists and their patients and clients. Such protections include:
1. Access to personnel and funding for patients and clients to pursue legitimate claims;2. Fair and timely compensation for injuries to patients and clients;3. Reasonable caps on non-economic damages;4. Reduction of liability premiums for physical therapists; and5. Mechanisms to protect the health service delivery system from repeat malpractice offenders and frivolous lawsuits.
1. APTA supports collaborative, collegial practice relationships between physical therapists and other health providers that promote access to and integration of physical therapists services in the health services delivery continuum.
2. APTA opposes legal restrictions and relationships with other health care providers that hinder the ability of physical therapists to use their clinical judgment and skills in relation to patient and client services, and that limit access to physical therapist services.
PRINCIPLE II. QUALITY OF PHYSICAL THERAPIST SERVICES
A. MEDICALLY NECESSARY PHYSICAL THERAPIST SERVICESPhysical therapist services are considered medically necessary as determined by a licensed physical therapist, based on the results of a physical therapist evaluation, and when provided to improve or maintain the current level of function or to prevent, minimize, maintain, slow the decline of, or eliminate impairments, activity limitations, or participation restrictions.
B. PAYMENT REFORM FOR PHYSICAL THERAPIST SERVICESAPTA supports efforts to reform payment for physical therapist services. Payment reform should:
1. Reflect efforts to tie payment to health outcomes, performance, and quality;2. Recognize and reward the value of physical therapist services based on the clinical reasoning and decision-making of
the physical therapist;3. Recognize physical therapists’ role in prevention;4. Reduce unnecessary and unwarranted regulations that add cost, reduce efficiency, and do not improve clinical
outcomes;5. Integrate physical therapist services into various models of service delivery, while separately identifying and
reporting these services;6. Be transparent and accountable to patients and clients, payers, and policy makers;7. Promote the use of evidence-based physical therapy;8. Reduce fraud, abuse, and waste within the health service delivery system; and9. Use standardized language and data sets across the health service delivery system.
C. USE OF DATA TO IMPROVE THE QUALITY OF PHYSICAL THERAPIST SERVICES
1. APTA supports the collection and tracking of data to improve the quality of physical therapist services. Data collection systems should:a. Demonstrate the value of physical therapist services;b. Promote health services research;c. Guide payment policies and quality improvement initiatives; andd. Determine clinical practice patterns and promote adherence to clinical practice guidelines. APTA supports and
promotes participation in quality assurance and quality improvement activities that are incorporated into physical therapist services.
2. APTA supports the use of electronic health record (EHR) systems in physical therapist practice and promotes the widespread adoption of interoperable EHRs in all practice settings.
D. PATIENT- AND CLIENT-CENTERED PHYSICAL THERAPIST SERVICES
APTA supports patient- and client-centered health services delivery. As such, physical therapist services include patients’ and clients’ goals. Physical therapists engage patients, clients, families, and caregivers in dialog to determine desired outcomes, while maximizing patient and client satisfaction. Physical therapists coordinate with other health professionals as needed to ensure continuity throughout episodes of care.
PRINCIPLE III. ACCOUNTABILITY FOR PHYSICAL THERAPIST SERVICES
A. PERFORMANCE OF PHYSICAL THERAPIST SERVICES
1. The patient/client management elements of examination, evaluation, diagnosis, and prognosis should be represented and paid as physical therapist services only when they are performed by a physical therapist.
2. The patient/client management element of intervention should be represented and paid as physical therapist services only when performed by a physical therapist or, for selected interventions, by a physical therapist assistant under the direction and supervision of a physical therapist.
3. Notwithstanding the foregoing, when physical therapist students and physical therapist assistant students perform elements of patient/client management as a part of their clinical education within a program accredited by, or developing programs recognized by, the Commission on Accreditation in Physical Therapy Education, these elements of patient/client management should be represented and paid as physical therapist services.
B. REASONABLE FEES FOR PHYSICAL THERAPIST SERVICES
1. APTA supports charging reasonable fees for physical therapist services. APTA encourages physical therapists to:a. Be knowledgeable of practice or institutional fee schedules, contractual relationships and payment
methodologies used in relation to physical therapist services.b. Participate in establishing practice or institutional fee schedules/contractual relationships and attempt to ensure
that providers, agencies, or other employers adopt physical therapy fee schedules and contractual relationships that are reasonable and encourage access to necessary services.
c. Seek guidance from the Code of Ethics for the Physical Therapist and Guide for Professional Conduct, applicable state law, and other institutional or payer policies if any question or disagreement arises regarding professional fees.
2. APTA opposes any acts by physical therapists or physical therapist assistants that place financial interest above the welfare of patients and clients, including but not limited to:a. Over or underutilization of services for institutional or personal gain; andb. Participating in services that are linked in any way to the financial gain of the referral source.
C. PEER REVIEW OF PHYSICAL THERAPIST SERVICES
1. APTA supports peer review of physical therapist services only when provided by a physical therapist who possesses an active license without sanctions to practice physical therapy. Peer review shall be based on APTA’s Standards of Practice for Physical Therapy, the Guide to Physical Therapist Practice, additional APTA documents supporting evidence-based literature, state practice acts, and other jurisdictional state and federal laws relevant to physical therapist services.
2. APTA supports that peer review policies and procedures should be clearly outlined in all provider contracts or manuals.
3. APTA opposes conducting a peer review without proper notice to providers before conducting the review. APTA strongly encourages payers to provide training to providers before implementing a peer review policy.
D. INTEGRITY OF PHYSICAL THERAPIST SERVICES
1. APTA supports the identification and mitigation of fraud, abuse, and waste in physical therapist services. Within the profession, physical therapists and physical therapists assistants are obligated to:a. Understand compliance by being aware and staying up-to-date on applicable laws, regulations, and policies;b. Take action to prevent and report suspected fraud, abuse, and waste; andc. Provide and bill for services legally and ethically and exercise sound clinical judgment.
2. APTA supports efforts by payers to prevent fraud, abuse and waste. APTA expects payers to provide notice to providers when new fraud, abuse and waste policies and regulations are implemented and to work with providers to ensure such policies and regulations are applied properly.
3. APTA supports best practices in business arrangements and professional relationships in connection with physical therapist practice, including the following:a. Integrity: Business arrangements and professional relationships are free of avoidable conflicts of interest and
comply with all APTA positions, standards, guidelines, policies, and procedures.b. Equity: Physical therapist ownership is proportional to investment and shared risk.c. Incentive: Physical therapists are compensated based on the value, quality, and complexity of their services.
d. Decision-making: Physical therapists are responsible for and control all clinical decision-making and patient/client management relating to physical therapist services. This responsibility is not delegated to other personnel or the employer.
PART B
That the following positions be rescinded:
Insurance Benefits for Physical Therapy Services (HOD P06-02-25-05) Physical Therapy as a Mandated Service under Medicaid (HOD P06-03-21-17) Transparency Requirements for Contractual Agreements between Patients/Clients, Payers and Intermediaries (HOD P06-
11-11-09) Health Care Liability Reform (HOD P06-04-28-24) Professional Practice Relationships (HOD P06-02-24-47) Quality Assurance and Performance Improvement (HOD P06-98-13-13) Support of Electronic Health Record in Physical Therapy (HOD P06-08-13-11) Reimbursement for Physical Therapy Services (HOD P06-01-12-15) Professional Fees for Physical Therapy Services (HOD P06-00-22-34) Financial Considerations in Practice (HOD P06-99-13-17) Peer Review of Physical Therapy Services (HOD P06-04-16-15) Reimbursement Policies (Federal and State) Affecting Physical Therapy Services (HOD P06-00-31-09) Methods for Investigating Fraud and Abuse (HOD P06-00-31-10) Guidelines: Principles of Professionalism Guiding Physical Therapist Business Relationships (HOD G06-10-12-10)
SS: The American Physical Therapy Association’s (APTA) Public Policy and Advocacy Committee (PPAC) and Board of Directors believe the proposed position, Delivery of Value-Based Physical Therapist Services, effectively articulates in a single position the association’s existing multiple positions related to payment, quality, and accountability in the delivery of physical therapist services. These concepts are relevant and timely, as the US health delivery system is being disrupted and moving from volume-based incentives toward quality and value-based payment and delivery. As the profession navigates this environment, it is important for us to focus on our societal impact and patient- and client-centered obligations.
Changes made to existing APTA House positions are identified and outlined in the Appendix to this motion. The changes noted in the Appendix are primarily editorial in nature to provide clarity and ensure terminology is contemporary. The relevant Board positions will be considered by the Board of Directors after 2015 House action to determine whether they need to be modified to remain compliant. Four new proposed House positions are also included in the proposed motion and are related to medical necessity (II A), payment reform (II B), patient-centered physical therapist services (IID), and integrity (III D, 1 and 2).
Should the House of Delegates adopt the position Delivery of Value-Based Physical Therapist Services, the positions listed in Part B will no longer be necessary.APTA’s PPAC will continue in its efforts to propose updates to APTA policies and positions in the public policy and advocacy area with the goal of having decision makers either rescind, consolidate, modernize, amend, and/or organize these policies. Ultimately, clarity is beneficial to the association’s policymaking bodies (the House of Delegates and Board of Directors) and for member and external use of APTA’s positions.
CURRENT POSITION/STANDARD/GUIDELINE/POLICY/PROCEDURE:NONE
RELATED POSITION/ STANDARD/GUIDELINE/POLICY/PROCEDURE :GUIDELINES: PRINCIPLES OF PROFESSIONALISM GUIDING PHYSICAL THERAPIST BUSINESS RELATIONSHIPS(HOD G06-10-12-10)FINANCIAL CONSIDERATIONS IN PRACTICE (HOD P06-99-13-17)HEALTH CARE LIABILITY REFORM (HOD P06-04-28-24)INSURANCE BENEFITS FOR PHYSICAL THERAPY SERVICES (HOD P06-02-25-05)MEDICALLY NECESSARY PHYSICAL THERAPY SERVICES (BOD P08-11-03-04)METHODS FOR INVESTIGATING FRAUD AND ABUSE (HOD P06-00-31-10)PEER REVIEW OF PHYSICAL THERAPY SERVICES (HOD P06-04-16-15)PHYSICAL THERAPY AS A MANDATED SERVICE UNDER MEDICAID (HOD P06-03-21-17)PROFESSIONAL FEES FOR PHYSICAL THERAPY SERVICES (HOD P06-00-22-34)PROFESSIONAL PRACTICE RELATIONSHIPS (HOD P06-02-24-47)QUALITY ASSURANCE AND PERFORMANCE IMPROVEMENT (HOD P06-98-13-13)REFORMING PAYMENT FOR OUTPATIENT PHYSICAL THERAPY SERVICES (BOD P03-11-04-09)REIMBURSEMENT FOR PHYSICAL THERAPY SERVICES (HOD P06-01-12-15)REIMBURSEMENT POLICIES (FEDERAL AND STATE) AFFECTING PHYSICAL THERAPY SERVICES (HOD P06-00-31-09)SUPPORT OF ELECTRONIC HEALTH RECORD IN PHYSICAL THERAPY (HOD P06-08-13-11)TRANSPARENCY REQUIREMENTS FOR CONTRACTUAL AGREEMENTS BETWEEN PATIENTS/CLIENTS, PAYERS AND INTERMEDIARIES (HOD P06-11-11-09)
42
12345678910111213141516171819
APPENDIX
IDENTIFICATION OF CHANGES TO EXISTING HOUSE OF DELEGATES AND BOARD OF DIRECTORS POSITIONS
INSURANCE BENEFITS FOR PHYSICAL THERAPY SERVICES (HOD P06-02-25-05)The American Physical Therapy Association (APTA) As an essential health benefit, APTA supports the inclusion of shall pursue and promote the incorporation of physical therapist services in accordance with APTA policies, positions, guidelines, standards, and Code of Ethics as a benefit in all appropriate insurance health care policies, including but not limited to: . Such policies include those developed Insurance policies by any third-party payers, and or state, federal, and other regulatory agencyies Plus the inclusion of physical therapists services in state and federal workers’ compensation programs and all appropriate telehealth policies, regulations, and legislation.
PHYSICAL THERAPY AS A MANDATED SERVICE UNDER MEDICAID (HOD P06-03-21-17)Physical therapist services should be a mandated service as a basic component of health care under Title XIX of the Social Security Act (the Medicaid program) at both the federal and state levels. The American Physical Therapy Association supports state and federal government actions that retain or enhance physical therapy benefits and opposes state and federal government actions that reduce physical therapy benefits under Title XIX.
TRANSPARENCY REQUIREMENTS FOR CONTRACTUAL AGREEMENTS BETWEEN PATIENTS/CLIENTS, PAYERS AND INTERMEDIARIES (HOD P06-11-11-09)Whereas, Physical therapy plays an essential role in the wellness and rehabilitation of all age groups;Whereas, Consumers should have access to physical therapy services through their health insurance coverage and be clearly informed of their coverage benefit and limitations prior to accessing physical therapy;Whereas, Under contemporary health insurance contracts and policies offered by carriers in their various health insurance plans, the health care consumer is frequently bearing an increased proportion of paid benefits for physical therapy services;Whereas, Patients/clients in need of physical therapy services who find that they are not able to afford the out-of-pocket expense of copays and coinsurance for multiple therapy sessions may be forced to terminate therapy before they can achieve their recovery outcomes or wellness goals; and,Whereas, Prematurely ending physical therapy treatment may reduce the full potential for recovery; prolong time away from employment; increase the chance of hospital readmission; increase the need for other treatments; prolong pain, other impairments and suffering; or prevent return to an active role in society;Resolved, That the American Physical Therapy (APTA) supports the inclusion of policies by payers, or the enactment of federal and state legislation or regulation, that ensures consumers (1) receive access to physical therapy services through their health insurance coverage; and (2) receive complete representation of the extent and nature of, and any limitation on, physical therapy coverage;1,2Resolved, That APTA supports change in through federal state and state federal legislation that limits that would require payers to limit the patient’s and client’s financial responsibility to less than the actual amount paid by the insurance carriers and insurance intermediaries to the provider for physical therapist services. , when the patient/client chooses to use his/her insurance carrier and intermediary entity; and,Resolved, That APTA supports change in federal state and state federal legislation that would that requires payers to develop and use consistent terminology regarding physical therapy coverage of physical therapist services. throughout the health insurance industry that is written in “plain language” that the public can easily read and interpret.21. Agency for Healthcare Research and Quality. What’s Your Health Literacy Score? Navigating the Healthcare System: ARHQ Web site. http://www.ahrq.gov/consumer/cc/cc052008.htm. 2008. Accessed March 1, 2011.
2. Boodman, S. Kaiser Health News. Many Americans have Poor Health Literacy. Washington Post Web site. http://www.washingontpost.com/wp-dyn/content/article/2011/02/28/AR2011022805957.html2. 2011. Accessed March 3, 2011.
HEALTH CARE LIABILITY REFORM (HOD P06-04-28-24)The American Physical Therapy Association endorses APTA supports comprehensive health care liability reform that puts patient and client safety first while working to reduce preventable injuries and improve communication between physical therapists and their patients and clients. To achieve these goals, protections must be put in place for physical therapists and their patients and clients. Such protections include: includes physical therapy and promotes:• Reasonable caps on non-economic damages. Access to personnel and funding for patients and clients to pursue legitimate claims;• Protection of awards to plaintiffs to meet the costs and the needs of their long term care. Fair and timely compensation for injuries to patients and clients;
• Support for rural areas that have limited resources in personnel and funding. Reasonable caps on non-economic damages;• Effective self-regulation by provider boards of repeat malpractice offenders. Reduction of liability premiums for physical therapists; and• Reasonable controls of malpractice insurance premiums. Mechanisms to protect the health service delivery system from repeat malpractice offenders and frivolous lawsuits• Increased statutory protection for internal medical review and quality improvement data.
PROFESSIONAL PRACTICE RELATIONSHIPS (HOD P06-02-24-47)The American Physical Therapy Association endorses APTA supports collaborative, collegial practice relationships between physical therapists and other health providers that promote access to and integration of physical therapist services in the health services delivery continuum. APTA opposes lLegal restrictions and relationships with other health care providers that hinder the ability of physical therapists to use their clinical judgment and skills in relation to patient and client services, and limit access to physical therapist services. autonomous physical therapist practice are not conducive to such relationships.
MEDICALLY NECESSARY PHYSICAL THERAPY SERVICES (BOD P08-11-03-04)Physical therapy, as part of an individual’s health care, is Physical therapist services are considered medically necessary as determined by the a licensed physical therapist, based on the results of a physical therapyist evaluation and when provided to improve or maintain the current level of function; or for the purpose of preventing, minimizeing, slow the decline of, or eliminateing impairments, activity limitations, or participation restrictions. Physical therapy is delivered throughout the episode of care by the physical therapist or under his or her direction and supervision; requires the knowledge, clinical judgment, and abilities of the therapist; takes into consideration the potential benefits and harms to the patient/client; and is not provided exclusively for the convenience of the patient/client. Physical therapy is provided using evidence of effectiveness and applicable physical therapy standards of practice and is considered medically necessary if the type, amount, and duration of services outlined in the plan of care increase the likelihood of meeting one or more of these stated goals: to improve function, minimize loss of function, or decrease risk of injury and disease.
REFORMING PAYMENT FOR OUTPATIENT PHYSICAL THERAPY SERVICES (BOD P03-11-04-09)The APTA Board of Directors endorses the development of an alternative payment system for outpatient physical therapist services that transitions from a timed procedure-based system to one that recognizes the quality and value of physical therapist directed health care and includes the APTA supports efforts to reform payment for physical therapist services. Payment reform should following 6 principles:
Reflect efforts to tie payment to health outcomes, performance, and quality; Recognize the clinical judgment of the physical therapists through their examination, evaluation, diagnosis and
prognosis of patients and clients; Recognize and reward the value of physical therapist the services based on the clinical complexity of the patient and
the intensity of skill and expertise of the physical therapist to direct physical therapy services to address the patient’s health needs reasoning and decision making of the physical therapist;
Recognize physical therapists’ role in prevention; Reduce unnecessary and unwarranted regulations that add cost, reduce efficiency, and do not improve clinical
outcomes; Facilitate integrateion of physical therapists services into various models of service care delivery, while maintaining an
ability to separately identifying and reporting these services as well as provide independent community based care; Be transparent and accountable to patients and clients, payers, and policy makers; Promote the use of evidence based physical therapy; Reduce fraud, abuse, and waste within the health service delivery system; and Improve patient outcomes and health status as a measurable result of physical therapists involvement in their health
care. Use standardized language and data sets across the health care system.QUALITY ASSURANCE AND PERFORMANCE IMPROVEMENT (HOD P06-98-13-13)The American Physical Therapy Association (APTA) is committed to excellence in physical therapy practice. Toward this effort, APTA is involved in monitoring systems and requirements aimed at APTA supports the collection and tracking of data to improvinge the quality of physical therapist services. Data collection systems should: and performance, facilitating distribution of information about activities of and requirements for performance improvement systems, and developing mechanisms to promote the use of physical therapists in performance improvement and peer review.
Demonstrate the value of physical therapist services; Promote health services research; Guide payment policies and quality improvement initiatives; and Determine clinical practice patterns and promote adherence to clinical practice guidelines.
APTA advocates voluntary member supports and promotes participation in quality assurance and performance quality improvement activities that which are incorporated into daily practice physical therapist services. The commitment to quality assurance and performance improvement is primarily a professional responsibility and is to be promoted and fostered by Association members through individual and collective efforts. APTA has adopted and maintains a Guide for Professional Conduct and Code of Ethics for the physicaltherapist, a Standards of Practice for Physical Therapy, and a Standards of Ethical Conduct for the Physical Therapist Assistant. Each APTA chapter shall create a means to promote quality assurance and performance improvement activities.
SUPPORT OF ELECTRONIC HEALTH RECORD IN PHYSICAL THERAPY (HOD P06-08-13-11)Whereas, It is in the best interest of patients/clients to ensure health care practitioners have the full picture of a patient’s/client’s health by integrating the health history, lab results, current medications, and effects of clinical interventions into one electronic interface;Whereas, In addition to improving efficiency and reducing medical errors, a well-designed electronic health record that meets recognized standards for privacy, security, and interoperability can assist health care practitioners to monitor and manage health risks to entire groups of patients/clients;Whereas, The President of the United States issued an executive order in 2004 with the goal of widespread adoption of interoperable electronic records by 20141; andWhereas, Using electronic health record systems may improve reporting, operational efficiency, communication, data accuracy, the capability for research, and some aspects of clinical decision making;Resolved, That the American Physical Therapy Association APTA supports the use of electronic health record systems (EHRs) in physical therapist practice and promotes the widespread adoption of interoperable EHRs in all physical therapy practice settings.1. President Unveils Tech Initiatives for Energy, Health Care, Internet. Remarks by the President at American Association of Community Colleges Annual Convention [press release]. Minneapolis, Minn: The White House; April 26, 2004. Available at: http://www.whitehouse.gov/news/releases/2004/04/20040426-6.html. Accessed March 24, 2008.
REIMBURSEMENT FOR PHYSICAL THERAPY SERVICES (HOD P06-01-12-15)The patient/client management elements of examination, evaluation, diagnosis, and prognosis should be represented and reimbursed paid as physical therapist services only when they are performed by a physical therapist. The patient/client management element of interventions should be represented and reimbursed paid as physical therapist services only when performed by a physical therapist or for selected interventions by a physical therapist assistant performing selected interventions under the direction and supervision of a physical therapist in accordance with American Physical Therapy Association (APTA) APTA policies, positions, guidelines, standards, and Code of Ethics.
Not withstanding the foregoing, when physical therapist students and physical therapist assistant students are performing elements of patient/client management in accordance with APTA policies, positions, guidelines, standards, and Code of Ethics and as a part of their clinical education within a component of an educational program accredited by, or developing programs recognized by, the Commission on Accreditation in Physical Therapy Education, these elements of patient/client management should be represented and reimbursed paid as physical therapyist services.
PROFESSIONAL FEES FOR PHYSICAL THERAPY SERVICES (HOD P06-00-22-34)Physical therapists are professionally responsible for fees charged for their services. Physical therapists should charge fees for their services that are APTA supports charging reasonable fees for physical therapist services. APTA encourages physical therapists to: In cases where the fee for service cannot be determined because of the payment methodology, the physical therapist should be aware of the payment methodology.
Physical therapists should: Be knowledgeable of practice or institutional fee schedules, contractual relationships and payment methodologies used
in relation to physical therapyist services. Participate, to the extent possible, in establishing practice or institutional fee schedules/contractual relationships and
attempt to ensure that providers, agencies, or other employers adopt physical therapy fee schedules and contractual relationships that are reasonable and that encourage access to necessary services.
Accurately document services provided including the selection of correct description and billing codes. Charge professional fees that are reasonable, never placing their own financial interest above the welfare of individuals
under their care. Include, where feasible, their license number on all billing for their professional services. Seek guidance from the Code of Ethics and Guide for Professional Conduct, applicable state law, and other institutional
or payer policies if any question or disagreement arises regarding professional fees.
FINANCIAL CONSIDERATIONS IN PRACTICE (HOD P06-99-13-17)The American Physical Therapy Association APTA opposes any acts by physical therapists or physical therapist assistants that place financial interest above the welfare of patients/clients, including but not limited to:
participation in underutilization or Oover or underutilization of services for personal institutional or institutional personal gain,; and
or Pparticipation in services that is are in any way linked to the financial gain of the referral source.
PEER REVIEW OF PHYSICAL THERAPY SERVICES (HOD P06-04-16-15)Peer review of physical therapy services is provided only APTA supports peer review of physical therapist services only when provided by a physical therapists who possesses an active license without sanctions to practice physical therapy. This Ppeer review shall be based on the following: American Physical Therapy Association (APTA) APTA’s Standards of Practice for Physical Therapy;, the Guide to Physical Therapist Practice;, other pertinent additional APTA documents and supporting evidence-based literature, when available, state practice acts, and other jurisdiction practice acts; and additional state, other jurisdiction jurisdictional state and federal laws relevant to the physical therapist practice services.
APTA is opposed to any activities related to peer review that may adversely impact a physical therapist’s plan of care or intervention without the involvement of a physical therapist peer reviewer. Adverse physical therapy patient/client management decisions made without the involvement of a physical therapist reviewer may constitute the unlawful practice of physical therapist services.
APTA supports that peer review policies and procedures should be clearly outlined in all provider contracts or manuals
REIMBURSEMENT POLICIES (FEDERAL AND STATE) AFFECTING PHYSICAL THERAPY SERVICES (HOD P06-00-31-09)The American Physical Therapy Association APTA opposes ex post facto application of conducting a peer review, utilization review, policies, or regulations that result in adverse decisions regarding reimbursement for physical therapy services rendered without proper notice to providers before conducting prior to the implementation of such policies or regulations the review. APTA strongly encourages payers to provide training to providers before implementing a peer review policy.
METHODS FOR INVESTIGATING FRAUD AND ABUSE (HOD P06-00-31-10)The American Physical Therapy Association APTA opposes ex post facto the application of fraud, waste, and abuse policies and regulations by payers that are implemented without prior notification to providers. relating to the provision, documentation, and billing of physical therapy services rendered prior to the implementation of such policies and regulations. APTA supports efforts by payers to prevent fraud, waste and abuse. APTA expects payers to provide notice to providers when new fraud, waste and abuse policies and regulations are implemented and to work with providers to ensure such policies and regulations are applied properly.
GUIDELINES: PRINCIPLES OF PROFESSIONALISM GUIDING PHYSICAL THERAPIST BUSINESS RELATIONSHIPS (HOD G06-10-12-10)
Whereas, Future compensation, practice ownership and employment opportunities will expand and change as the physical therapist profession achieves APTA Vision Statement for Physical Therapy 2020; and,Whereas, Physical therapists should uphold best practice principles in their professional and business arrangements, just as they should in their clinical practice;Resolved, That the following principles will promote APTA supports best practices in business arrangements and professional relationships and arrangements in connection with physical therapist practice, including the following:
Autonomy: Physical therapists shall have control over all clinical decisions relating to physical therapy. Integrity: Business arrangements and professional relationships are free of avoidable conflicts of interest and comply with all APTA positions, standards, guidelines, policies, and procedures.
Integrity: Business relationships shall be free of avoidable conflicts of interest and comply with all American Physical Therapy Association positions, standards, guidelines, policies, and procedures. Equity: Physical therapist ownership is proportional to investment and shared risk.
Equity: Physical therapist ownership should be proportional to investment and shared risk. Incentive: Physical therapists are compensated based on the value, quality, and complexity of their services.
Incentive: Physical therapists should be compensated based on the value of their services, which may be measured through components such as quantity, quality, and complexity. Decision-making: Physical therapists are responsible for and control all clinical decision making and patient/client management relating to physical therapist services. This responsibility is not delegated to other personnel or the employer.
Physical therapist services are considered medically necessary as determined by a licensed physical therapist, based on the results of a physical therapist evaluation, and when provided to improve or maintain the current level of function or to prevent, minimize, maintain, slow the decline of, or eliminate impairments, activity limitations, or participation restrictions.
SS: The term “medically necessary” physical therapy is a common term used to determine eligibility for physical therapist services and associated payment or reimbursement. In the Jimmo v Sebelius1 settlement agreement in January 2013, clarity was provided regarding the determination of medical necessity for payment for physical therapist services to maintain the level or slow the decline of an impairment, functional limitation, or participation restriction. This concept is especially important in the current evolution of chronic disease management by physical therapists (PT) where the patient may have an incurable, degenerative, chronic, or life-threatening illness.
The intent of this motion is to incorporate the concepts summarized by Jimmo v Sebelius and clarify that this definition of medically necessary physical therapist services includes circumstances where physical therapist services are required to slow the decline of or maintain a patient’s condition.
The House of Delegates is the highest policy making body in the American Physical Therapy Association (APTA) and it is appropriate that the House of Delegates adopt this position to make it the official stance of the entire association. This motion adoption has the following goals:
1. It will provide increased clarity to PTs and physical therapist assistants (PTA), payment entities and organizations, external stakeholders, other health care providers, and the public that the PT providing direct care to the patient should be the ultimate decision maker regarding medically necessary services.
2. It will be used as a resource for insurance companies and individual medical consultant case reviewers when ruling on medical necessity determinations as well as subsequent appeals.
3. It will be used by educational programs in the entry-level and postprofessional training of PTs and PTAs to integrate the concepts of longitudinal management of the patient with a degenerative, chronic, incurable, or life-threatening condition.
The proposed position would clarify APTA’s official position that regardless of payer or diagnosis or prognosis, it is the right of every patient to have access to physical therapist services if the services are medically necessary to maintain their current level of functioning or if physical therapy is medically necessary to slow the decline in functional status. In addition, it is the ethical imperative of the PT to provide these services regardless of the overall prognosis of the patient, even in the presence of a terminal or life-threatening illness.
Reference:1. Jimmo v Sebelius Settlement Agreement Fact Sheet. Center for Medicare and Medicaid Services website. http://www.cms.gov/Medicare/Medicare-
Fee-for-Service-Payment/SNFPPS/Downloads/Jimmo-FactSheet.pdf . Accessed September 29, 2014.
RC 10-15 RESCIND: HEALTH CARE COVERAGE FOR ALL AMERICANS (HOD P06-05-18-27)
That Health Care Coverage For All Americans (HOD P06-05-18-27) be rescinded.
SS: The intent of this House of Delegates position has been incorporated into Principles and Objectives for the United States Health Care System (HOD P06-13-20-18), and therefore is no longer necessary.
CURRENT POSITION/STANDARD/GUIDELINE/POLICY/PROCEDURE:HEALTH CARE COVERAGE FOR ALL AMERICANS (HOD P06-05-18-27)
RELATED POSITION/ STANDARD/GUIDELINE/POLICY/PROCEDURE :PRINCIPLES AND OBJECTIVES FOR THE UNITED STATES HEALTH CARE SYSTEM (HOD P06-13-20-18)
RC 11-15 ADOPT: HEALTH PRIORITIES FOR POPULATIONS AND INDIVIDUALS
That the following position be adopted:
HEALTH PRIORITIES FOR POPULATIONS AND INDIVIDUALS
That the following population health priorities guide the American Physical Therapy Association (APTA) work in the areas of prevention, wellness, fitness, health promotion, and management of disease and disability. Physical therapists can positively impact these areas and, where opportunity exists, can improve the health status of populations and individuals.
Physical therapists also can help prevent secondary health conditions commonly associated with many chronic diseases and disabilities. The population health priorities identified to most relate to physical therapist practice in primary and secondary prevention and in disease management are:
I. Active living1
A. Physical inactivity is a risk factor that contributes to onset and progression of diseases and conditions in individuals of all ages, including diabetes, heart disease, pulmonary disease, obesity, metabolic syndrome, psychosocial health, stroke, certain cancers, and certain musculoskeletal conditions.
B. Physical therapists have unique opportunities with the following populations identified by the US National Prevention Strategy (USNPS):1. Aging individuals and populations (risk of falls, more individuals living longer with chronic diseases and
conditions, impact of reduced physical fitness on quality of life)2. Individuals and populations of all ages with health disparities3. Individuals and populations of all ages with chronic conditions, disabilities, and diseases that impact their
ability to remain independent and physically active
II. Injury prevention1
A. Reducing injury improves physical and emotional health. Injury can be prevented by making homes, communities, schools, and worksites safer and by implementing community-based prevention policies and programs.
B. Physical therapists have unique opportunities in the following areas of injury prevention identified by USNPS:1. Falls prevention2. Workplace injury prevention3. Community-based injury prevention
III. Secondary prevention in chronic disease and disability managementA. Reducing or preventing health conditions that accompany many chronic diseases and disabilities helps to
improve physical and emotional health and optimize individuals’ participation in society. Secondary conditions and their risk factors can be identified and ameliorated through screening and recognition.
B. Priorities for physical therapists in secondary prevention in chronic disease and disability management include:1. Diseases and disabilities that impair an individual’s body function or structure2. Diseases and disabilities that limit an individual’s activity3. Diseases and disabilities that restrict an individual’s participation in society4. Diseases and disabilities that require modification of environmental factors to allow for full participation in
society
IV. Physical therapists could provide education, behavioral strategies, patient advocacy, referral opportunities, and identification of supportive resources for the following additional USNPS1 health priorities:A. Stress managementB. Smoking cessationC. Sleep healthD. Nutrition optimizationE. Weight managementF. Alcohol moderation and substance-free livingG. Violence-free livingH. Adherence to health care recommendations
Reference : 1 US Department of Health and Human Services. National Prevention Strategy.
SS: In 2010, the National Prevention, Health Promotion and Public Health Council of the Office of the Surgeon General of the United States adopted the nation’s first ever national Prevention and Health Promotion Strategy (National Prevention Strategy) to champion the policies and programs needed to ensure the health of Americans and to move our country from a system of sick care to one based on health and prevention. The National Prevention Strategy identifies 7 targeted priorities along with evidence-based recommendations intended to reduce the burden of the leading causes of preventable death and disease:
1. Tobacco-free living2. Preventing drug abuse and excessive alcohol use3. Healthy eating4. Active living5. Injury- and violence-free living6. Reproductive and sexual health7. Mental and emotional well-being
The Physical Therapists’ Role in Prevention, Wellness, Fitness, and Disease Management for Public Policy Purposes Task Force identified that physical therapists have a unique opportunity to impact the population health priorities of active living (4) and injury free living (5). Additionally, physical therapists are in an excellent position to support the remaining National Prevention Strategy priorities through identification, patient and client education, and appropriate referrals.The APTA Board of Directors adopted these health priorities at its March 2014 Board Meeting. Based on review and recommendation by the APTA Public Policy and Advocacy Committee, these priorities are forwarded to the House of Delegates to provide guidance for APTA staff in policy, practice, education, and research initiatives.
CURRENT POSITION/STANDARD/GUIDELINE/POLICY/PROCEDURE:NONE
RELATED POSITION/ STANDARD/GUIDELINE/POLICY/PROCEDURE :ENDORSEMENT OF THE FALLS FREE: PROMOTING A NATIONAL FALLS PREVENTION ACTION PLAN (HOD P06-05-19-10)HEALTH PROMOTION AND WELLNESS BY PHYSICAL THERAPISTS AND PHYSICAL THERAPIST ASSISTANTS(HOD P06-93-25-50)PHYSICAL ACTIVITY ADVOCACY (HOD P06-05-19-09)PHYSICAL EDUCATION, PHYSICAL CONDITIONING, AND WELLNESS ADVOCACY (HOD P06-04-22-18)PHYSICAL THERAPISTS AND PHYSICAL THERAPIST ASSISTANTS AS PROMOTERS AND ADVOCATES FOR PHYSICAL ACTIVITY/EXERCISE (HOD P06-08-07-08)PHYSICAL THERAPISTS AS EXPERT PROVIDERS OF EXERCISE AND PHYSICAL ACTIVITY PRESCRIPTION (HOD P06-12-20-07)
RC 12-15 ADOPT: THE ROLE OF THE PHYSICAL THERAPIST IN DIET AND NUTRITION
That the following position be adopted:
THE ROLE OF THE PHYSICAL THERAPIST IN DIET AND NUTRITION
As diet and nutrition are key components of primary, secondary, and tertiary prevention of many conditions managed by physical therapists, it is the role of the physical therapist to evaluate for and provide information on diet and nutritional issues to patients, clients, and the community within the scope of physical therapist practice. This includes appropriate referrals to nutrition and dietary medical professionals when the required advice and education lie outside the education level of the physical therapist.
SS: According to the US Centers for Disease Control and Prevention, “During the past 20 years, there has been a dramatic increase in obesity in the United States and rates remain high. More than one-third of U.S. adults (34.9%) and approximately 17% of children and adolescents aged 219 years (12.7 million) have obesity.”1 A significant portion of the major causes of death in the United States are related to lifestyle. The morbidity and mortality related to obesity represent a great cost to the health care system and the economy. Many of these conditions are directly impacted by nutrition and diet, including heart disease, cancer, stroke, and diabetes, and are contributing factors to the management of many other conditions that the physical therapist is involved in managing.2 This motion is intended to recognize the role of the physical therapist in addressing this societal issue.
Several organizations have suggested actions to manage this health issue. The American Cancer Society notes that a healthy diet can improve outcomes in cancer treatments and prevent some cancers.2 US Centers for Medicare and Medicaid Services guidelines recommend that health care providers, including physical therapists, conduct BMI assessments of all patients.3 The US Preventive Services Task Force recommendation statement provides support for our role in behavioral counseling. From the Clinical Practice Guideline (CPG): “Most studies evaluated interventions that combined counseling on a healthful diet and physical activity and were intensive ... Interventions were delivered by specially trained professionals, including dietitians or nutritionists, physiotherapists or exercise professionals, health educators, and psychologists ...”4
Physical therapist education programs are required to include health promotion and wellness in their curricula. Current Commission on Accreditation in Physical Therapy Education (CAPTE) evaluative criteria for physical therapist education programs related to these concepts include: “CC-5.50 Provide culturally competent physical therapy services for prevention, health promotion, fitness, and wellness to individuals, groups, and communities”; “CC-5.51 Promote health and quality of life by providing information on health promotion, fitness, wellness, disease, impairment, functional limitation, disability, and health risks related to age, gender, culture, and lifestyle within the scope of physical therapist practice”; and“CC-5.52 Apply principles of prevention to defined population groups.” The revised CAPTE PT Standards for items 5.50-5.52 is encapsulated as “7D33: Provide physical therapy services that address primary, secondary, and tertiary prevention, health promotion, and wellness to individuals, groups, and communities.”5
In an article on The First Physical Therapy Summit on Global Health, Dean, et al, noted, "... lifestyle-related conditions consistent with physical therapy practice include smoking cessation counseling in the form of brief advice that is either initiated or supports other ongoing cessation strategies; basic nutrition advice with referral to a nutritionist or dietician if detailed assessment and intervention are needed beyond basic nutritional guidelines …”6 In an article on physical therapy for the 21st century, Dean also wrote, "A compelling argument can be made that clinical competencies in 21st century physical therapy need to include assessment of smoking and smoking cessation (or at least its initiation), basic nutritional assessment and counseling, recommendations for physical activity and exercise, stress assessment and basic stress reduction recommendations, and sleep assessment and basic sleep hygiene recommendations."7
This motion clearly incorporates the intent of the new Vision Statement for the Physical Therapy Profession by transforming society and improving the human experience. As it is recognized that there are medical complexities of providing comprehensive dietary counseling, it is the ethical imperative of the physical therapist to provide referrals to appropriate health care professionals including dieticians and physicians when the dietary counseling or medical complexity of the related condition extends beyond the education level and scope of the physical therapist.
References:1. Overweight and Obesity. Centers for Disease Control and Prevention Website. http://www.cdc.gov/obesity/data/. Accessed November 29, 2014.2. Eat Healthy and Get Active. American Cancer Society consumer website. http://www.cancer.org/healthy/eathealthygetactive/index. Accessed
February 16, 2015.3. Measure #128 (NQF 0421): Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-Up. Centers for Medicare and Medicaid
Services website. http://www.apta.org/uploadedFiles/APTAorg/Payment/Medicare/Pay_for_Performance/PQRS/2011/PQRSMeasure128.pdf. Accessed January 13, 2015.
4. Clinical practice guideline (CPG) recommendation statement: Behavioral counseling to promote a healthful diet and physical activity for cardiovascular disease prevention in adults with cardiovascular risk factors. US Preventive Services Task Force website. http://www.guideline.gov/content.aspx?id=48483#Section420 . Accessed February 16, 2015.
5. Educational Criteria. Commission on Accreditation of Physical Therapy Education website. http://www.capteonline.org/uploadedFiles/CAPTEorg/About_CAPTE/What_We_Do/Whats_New/CAPTEEvaluativeCriteriaPT_ProposedandCurrent.pdf. Accessed January 13, 2015.
6. Dean E, Al-Obaidi S, De Andrade AD, et al. The First Physical Therapy Summit on Global Health: implications and recommendations for the 21st century. Physiother Theory Pract. 2011;27:531-47.
7. Dean E. Physical therapy in the 21st century (Part I): toward practice informed by epidemiology and the crisis of lifestyle conditions. Physiother Theory Pract. 2009;25:330-53.
CURRENT POSITION/STANDARD/GUIDELINE/POLICY/PROCEDURE:NONE
RELATED POSITION/STANDARD/GUIDELINE/POLICY/PROCEDURE:PHYSICAL THERAPISTS AS EXPERT PROVIDERS OF EXERCISE AND PHYSICAL ACTIVITY PRESCRIPTION (HOD P06-12-20-07)
RC 13-15 ADOPT: THE ASSOCIATION’S ROLE IN ADVOCACY FOR PREVENTION, WELLNESS, FITNESS, AND HEALTH PROMOTION, AND FOR MANAGEMENT OF DISEASE AND DISABILITY
That the following position be adopted:
THE ASSOCIATION’S ROLE IN ADVOCACY FOR PREVENTION, WELLNESS, FITNESS, AND HEALTH PROMOTION, AND FOR MANAGEMENT OF DISEASE AND DISABILITY
The American Physical Therapy Association (APTA) advocates for prevention, wellness, fitness, and health promotion, and for management of disease and disability.
Advocacy includes but is not limited to scientific, educational, regulatory, and legislative activities that promote regular physical activity and exercise to enhance health and prevent disease. It includes developing collaborative, interprofessional and partnering relationships with health care and community organizations that promote prevention, wellness, fitness, and health promotion, and management of disease and disability.
Priorities for association advocacy include, but are not limited to:
Appropriate physical activity and exercise goals and objectives put forth by government and other nationally recognized agencies and organizations
Consumer recognition of the value of the physical therapist to provide services for prevention, wellness, fitness, and health promotion, and for management of disease and disability for all populations and conditions
Physical education, physical conditioning, and wellness instruction at all levels of education, from preschool through higher education
Physical therapists making healthy personal lifestyle choices that include meeting national guidelines for participation in physical activity and exercise
SS: This position provides for an updated and streamlined comprehensive House of Delegates (House) position that effectively articulates the association’s positions related to APTA’s role in prevention. This broad public policy and advocacy position is beneficial to both the Association’s policy making bodies (the House and Board of Directors) and for member and external use of APTA’s positions. This comprehensive position also allows for inclusion of new initiatives within APTA’s policy and advocacy scope of work.
CURRENT POSITION/STANDARD/GUIDELINE/POLICY/PROCEDURE:NONE
RELATED POSITION/ STANDARD/GUIDELINE/POLICY/PROCEDURE :ENDORSEMENT OF THE FALLS FREE: PROMOTING A NATIONAL FALLS PREVENTION ACTION PLAN (HOD P06-05-19-10)HEALTH PROMOTION AND WELLNESS BY PHYSICAL THERAPISTS AND PHYSICAL THERAPIST ASSISTANTS (HOD P06-93-25-50)PHYSICAL ACTIVITY ADVOCACY (HOD P06-05-19-09)PHYSICAL EDUCATION, PHYSICAL CONDITIONING, AND WELLNESS ADVOCACY (HOD P06-04-22-18)PHYSICAL THERAPISTS AND PHYSICAL THERAPIST ASSISTANTS AS PROMOTERS AND ADVOCATES FOR PHYSICAL ACTIVITY/EXERCISE (HOD P06-08-07-08)PHYSICAL THERAPISTS AS EXPERT PROVIDERS OF EXERCISE AND PHYSICAL ACTIVITY PRESCRIPTION (HOD P06-12-20-07)
RC 14-15 ADOPT: PHYSICAL THERAPISTS’ ROLE IN PREVENTION, WELLNESS, FITNESS, HEALTH PROMOTION, AND MANAGEMENT OF DISEASE AND DISABILITY
That the following position be adopted:
PHYSICAL THERAPISTS’ ROLE IN PREVENTION, WELLNESS, FITNESS, HEALTH PROMOTION, AND MANAGEMENT OF DISEASE AND DISABILITY
Physical therapists play a unique role in society in prevention, wellness, fitness, health promotion, and management of disease and disability by serving as a dynamic bridge between health and health care for individuals and populations. This means that although physical therapists are experts in rehabilitation and habilitation, they also have the knowledge and the opportunity to help individuals and populations improve overall health and prevent the need for avoidable health care services. Physical therapists’ roles may include education, direct intervention, research, and collaborative consultation. These roles are essential to the profession’s vision of transforming society by optimizing movement to improve the human experience.
Physical therapists, like most health professionals, are educated to provide services in the health care environment. Physical therapists also are uniquely educated and trained to adapt health care recommendations to the community environment where individuals live, work, learn, and play. This knowledge and ability enables physical therapists to adapt medical recommendations to specific environments, to meaningfully interpret health recommendations, and to help individuals modify their health behaviors.
For their role in prevention, wellness, fitness, and health promotion, physical therapists:
1. Integrate decision-making skills across all dimensions and contextual factors of the International Classification of Function (ICF)
2. Incorporate personal factors of medical and health history into a plan of care that includes data related to body functions and structures, activities and participation, and relevant environmental factors
3. Integrate scientific principles of movement, function, and exercise progression to promote physical activity and improve health outcomes
4. Incorporate concepts of prevention, wellness, fitness, and health promotion with every patient or client as appropriate
5. Integrate and interpret the elements of medical, biopsychosocial, and health promotion models that allow them to monitor health status over time
6. Screen to prevent and manage disease and disability, referring as appropriate as part of an interprofessional healthy-lifestyle team
7. Apply best available evidence in selecting, prescribing, and using intervention and measurement strategies in establishing exercise prescriptions and planning programs for individuals and communities
8. Use skills in behavior change to promote healthy lifestyles in individuals and communities9. Adapt tasks and the environment to promote healthy behaviors and improved health outcomes for individuals of all
ages, including those with complex medical and functional needs10. Adopt healthy lifestyle choices for themselves that include meeting national guidelines for participation in physical
For their role in management of disease and disability, physical therapists:
1. Recognize the risk factors for, and the course of, chronic diseases and the potential impact on quality of life and on activities and participation
2. Establish and facilitate collaborative, interprofessional, patient- and client-centric relationships that empower individuals in self-care across the lifespan and through the health continuum, with an emphasis on movement and function
3. Apply best available evidence in selecting, prescribing, and using intervention and measurement strategies in establishing exercise prescription and planning programs to educate individuals and help them prevent primary, secondary, and tertiary conditions or restore functional mobility
4. Provide nonsurgical and nonpharmacological care as a hallmark of physical therapist practice5. Predict and interpret health outcomes and functional needs where people live, work, learn, and play
For their role as a dynamic link between health and health care, physical therapists:
1. Apply their expertise in exercise and physical activity prescription to adapt health recommendations to the individual’s environment, from acute medical settings to the community
2. Collaborate with a variety of providers in health care and in health, wellness, and fitness to help individuals along the full continuum of health reduce their disease risk and improve their health and quality of life
3. Communicate and collaborate with relevant health care professionals to help individuals receive appropriate health care
For their role as advocates for prevention, wellness, fitness, health promotion, and management of disease and disability, physical therapists:
1. Support scientific, educational, legislative, and other policy initiatives that promote regular physical activity and exercise to enhance health and prevent disease
2. Advocate for physical education, physical conditioning, and wellness instruction at all levels of education, from preschool through higher education
SS: For many years, the American Physical Therapy Association (APTA) has attempted to describe and promote the role of physical therapists in prevention, wellness, fitness, health promotion, and management of disease and disability. As a result of these efforts, numerous House of Delegates policies and positions, APTA core documents, and other APTA documents and resources such as the Guide to Physical Therapist Practice and Today’s Physical Therapist include various descriptions of physical therapist roles in these areas of practice. The language in these policies and documents is not always consistent and clear.
In 2011, the Board of Directors (Board) held 2 generative discussions to consider whether APTA should develop and implement strategies to enhance member abilities to integrate prevention, wellness, and health promotion strategies into practice. These generative discussions revealed a need for APTA to more clearly describe physical therapist roles in these areas. In July 2012, the APTA Board appointed a task force to develop and present to the Board a description of the role of physical therapists in prevention, wellness, and disease management for both individuals and populations.
Current APTA policies and documents, along with these Board of Directors’ deliberations, informed the work of the task force in completing its charge. The health of our population and the many changes in health care delivery require clear direction for the physical therapy profession in the important areas of prevention, wellness, fitness, health promotion, and management of disease and disability.
The Physical Therapists’ Role in Prevention, Wellness, Fitness, and Disease Management for Public Policy Purposes Task Force recommended to the Board that an overarching position on the role of the physical therapist in prevention,
wellness, and health promotion be developed. It was recommended that the new position allow for the consolidation of the following APTA positions.
Endorsement Of The Falls Free: Promoting A National Falls Prevention Action Plan (HOD P06-05-19-10) Physical Activity Advocacy (HOD P06-05-19-09) Physical Education, Physical conditioning, and Wellness Advocacy (HOD P06-04-22-18) Physical Therapists and Physical Therapist Assistants as Promoters and Advocates for Physical Activity/Exercise (HOD
P06-08-07-08) Physical Therapists as Expert Providers of Exercise and Physical Activity Prescription (HOD P06-12-20-07) Health Promotion and Wellness by Physical Therapists and Physical Therapist Assistants ( HOD P06-93-25-50) Prevention, Wellness, Fitness, and Health Promotion Definitions (BOD Y03-06-16)
At its December 2013 meeting, the Board approved an interim Plan for Review of APTA Positions, Standards, Guidelines, Policies, and Procedures in the Public Policy Area, with the intent of bringing amendments to the Board for consideration as potential motions for the 2014 and 2015 House of Delegates. The licensure principles were adopted by the 2014 House. Specific policy areas identified for review in the plan for 2015 were House policies related to payment, quality, and prevention.
Based on the Physical Therapists’ Role in Prevention, Wellness, Fitness, and Disease Management for Public Policy Purposes Task Force report, the APTA Board of Directors adopted a Board position Physical Therapists’ Role In Prevention, Wellness, Fitness, And Disease Management at the February 2014 Board Meeting, with a proviso that this position was adopted with the understanding that this position and all other positions on this topic be incorporated into the policy review project with a comprehensive position forwarded to the 2015 House of Delegates.
The Public Policy and Advocacy Committee Prevention subgroup reviewed all existing APTA House of Delegates positions related to prevention and wellness, and investigated any issues on the horizon that warranted the adoption of new positions by the House. The APTA Public Policy and Advocacy Committee recommended that the Board position be expanded to include a new section on individual physical therapist advocacy, and a new position on association advocacy (RC 13-15).
APTA’s bold new vision statement, Transforming society by optimizing movement to improve the human experience, places new responsibility on physical therapists and the profession to assume a leadership role to improve the health of our population. Physical inactivity is a significant risk factor for many chronic diseases and conditions and is an even greater problem for those with limited mobility. Physical therapists are uniquely qualified to have a significant impact on health and quality of life by serving as a dynamic link between the clinic and the community.
It is essential that APTA clearly describe, promote, and advocate for the role of physical therapists in prevention, wellness, fitness, health promotion, and management of disease and disability for individuals and for populations. A clear description of this role is an important early step in achieving the new vision.
This motion is consistent with APTA’s current initiative to review and revise existing association positions, standards, guidelines, policies, and procedures.
CURRENT POSITION/STANDARD/GUIDELINE/POLICY/PROCEDURE:NONE
RELATED POSITION/ STANDARD/GUIDELINE/POLICY/PROCEDURE :ENDORSEMENT OF THE FALLS FREE: PROMOTING A NATIONAL FALLS PREVENTION ACTION PLAN (HOD P06-05-19-10)HEALTH PROMOTION AND WELLNESS BY PHYSICAL THERAPISTS AND PHYSICAL THERAPIST ASSISTANTS(HOD P06-93-25-50)PHYSICAL ACTIVITY ADVOCACY (HOD P06-05-19-09)PHYSICAL EDUCATION, PHYSICAL CONDITIONING, AND WELLNESS ADVOCACY (HOD P06-04-22-18)PHYSICAL THERAPISTS AND PHYSICAL THERAPIST ASSISTANTS AS PROMOTERS AND ADVOCATES FOR PHYSICAL ACTIVITY/EXERCISE (HOD P06-08-07-08)PHYSICAL THERAPISTS AS EXPERT PROVIDERS OF EXERCISE AND PHYSICAL ACTIVITY PRESCRIPTION (HOD P06-12-20-07)
RC 15-15 RESCIND: POSITIONS RELATED TO PREVENTION, WELLNESS, FITNESS, HEALTH PROMOTION, AND MANAGEMENT OF DISEASE AND DISABILITY
That the following positions be rescinded:
Endorsement of the Falls Free: Promoting a National Falls Prevention Action Plan (HOD P06-05-19-10) Health Promotion and Wellness By Physical Therapists and Physical Therapist Assistants
(HOD P06-93-25-50) Physical Activity Advocacy (HOD P06-05-19-09) Physical Education, Physical Conditioning, and Wellness Advocacy (HOD P06-04-22-18) Physical Therapists and Physical Therapist Assistants as Promoters and Advocates for Physical Activity/Exercise (HOD
P06-08-07-08) Physical Therapists as Expert Providers of Exercise and Physical Activity Prescription (HOD P06-12-20-07)
SS: These House of Delegates positions have been incorporated into the proposed positions Physical Therapists’ Role in Prevention, Wellness, Fitness, and Health Promotion, and in Management of Disease and Disability, and The Association’s Role in Advocacy for Prevention Wellness, Fitness, and Health Promotion, and for Management of Disease and Disability, and therefore separate positions are no longer necessary.
Descriptions of changes to these existing positions follows:
1. ENDORSEMENT OF THE FALLS FREE: PROMOTING A NATIONAL FALLS PREVENTION ACTION PLAN (HOD P06-05-19-10)The language “For their role as advocates for prevention, wellness, fitness, health promotion, and management of disease and disability, physical therapists: Support scientific, educational, legislative, and other policy initiatives that promote regular physical activity and exercise to enhance health and prevent disease” was added to the Advocacy section of the proposed amended PHYSICAL THERAPISTS’ ROLE IN PREVENTION, WELLNESS, FITNESS, AND DISEASE MANAGEMENT (BOD P02-14- 02-01) and “Priorities for association include, but are not limited to, advocating for: Appropriate physical activity and exercise goals and objectives put forth by government and other nationally recognized agencies and organizations” to the proposed new position THE ASSOCIATION’S ROLE IN ADVOCACY FOR PREVENTION WELLNESS, FITNESS, HEALTH PROMOTION, AND DISEASE AND DISABILITY MANAGEMENT.
2. HEALTH PROMOTION AND WELLNESS BY PHYSICAL THERAPISTS AND PHYSICAL THERAPIST ASSISTANTS (HOD P06-93-25-50)The concepts of health promotion and wellness by physical therapists are included in the proposed amended PHYSICAL THERAPISTS’ ROLE IN PREVENTION, WELLNESS, FITNESS, AND DISEASE MANAGEMENT(BOD P02-14- 02-01) but with a greater emphasis on interprofessional collaboration as opposed to leadership.
3. PHYSICAL ACTIVITY ADVOCACY (HOD P06-05-19-09)The language “For their role as advocates for prevention, wellness, fitness, health promotion, and management of disease and disability, physical therapists: Support scientific, educational, legislative, and other policy initiatives that promote regular physical activity and exercise to enhance health and prevent disease” was added to the Advocacy section of the proposed amended PHYSICAL THERAPISTS’ ROLE IN PREVENTION, WELLNESS, FITNESS, AND DISEASE MANAGEMENT (BOD P02-14- 02-01) and “Endorsement of appropriate physical activity and exercise goals and objectives put forth by government and other nationally recognized agencies and organizations” to the proposed new position THE ASSOCIATION’S ROLE IN ADVOCACY FOR PREVENTION WELLNESS, FITNESS, HEALTH PROMOTION, AND FOR MANAGEMENT OF DISEASE AND DISABILITY MANAGEMENT.
4. PHYSICAL EDUCATION, PHYSICAL CONDITIONING, AND WELLNESS ADVOCACY (HOD P06-04-22-18)Language to advocate “for physical education and for physical conditioning and wellness instruction at all levels of education from preschool through higher education” is included in both the proposed amendments to PHYSICAL THERAPISTS’ ROLE IN PREVENTION, WELLNESS, FITNESS, AND DISEASE MANAGEMENT (BOD P02-14- 02-01) and in the proposed new position THE ASSOCIATION’S ROLE IN ADVOCACY FOR PREVENTION WELLNESS, FITNESS, HEALTH PROMOTION AND DISEASE AND FOR MANAGEMENT OF DISEASE AND DISABILITY.
5. PHYSICAL THERAPISTS AND PHYSICAL THERAPIST ASSISTANTS AS PROMOTERS AND ADVOCATES FOR PHYSICAL ACTIVITY/EXERCISE (HOD P06-08-07-08)Language that calls for “meeting national guidelines for participation in physical activity and exercise” is included in the proposed amendments to PHYSICAL THERAPISTS’ ROLE IN PREVENTION, WELLNESS, FITNESS, AND DISEASE MANAGEMENT (BOD P02-14- 02-01) and the resolved statement is included in the proposed new position THE ASSOCIATION’S ROLE IN ADVOCACY FOR PREVENTION, WELLNESS, FITNESS, HEALTH PROMOTION, AND FOR MANAGEMENT OF DISEASE AND DISABILITY.
6. PHYSICAL THERAPISTS AS EXPERT PROVIDERS OF EXERCISE AND PHYSICAL ACTIVITY PRESCRIPTION (HOD P06-12-20-07)Prescription language is included in the proposed amended PHYSICAL THERAPISTS’ ROLE IN PREVENTION, WELLNESS, FITNESS, AND DISEASE MANAGEMENT (BOD P02-14- 02-01)
CURRENT POSITION/STANDARD/GUIDELINE/POLICY/PROCEDURE: SEE ABOVE
RELATED POSITION/ STANDARD/GUIDELINE/POLICY/PROCEDURE : SEE ABOVE
Whereas, It is the vision of the physical therapy profession1 to optimize movement to improve the human experience;
Whereas, The vision’s guiding principle of identity is that the physical therapy profession will define and promote the movement system as the foundation for optimizing movement to improve the health of society;
Whereas, The vision’s guiding principle of quality is that the physical therapy profession will commit to establishing and adopting best practice standards across the domains of practice, education, and research;
Whereas, The vision’s guiding principle of collaboration is that the physical therapy profession will demonstrate the value of collaboration with other health care providers, consumers, community organizations, and other disciplines to solve the health-related challenges that society faces; and,
Whereas, APTA supports the development of best practice standards within and across the domains of practice, education, and research that will lead to improving the ability and skill of physical therapists to diagnose, plan, and provide effective interventions for movement system disorders;
Resolved, APTA supports the development of diagnostic labels that may form the basis of physical therapists’ expertise in being able to properly and effectively diagnose disorders of the movement system;
Resolved, APTA supports the strengthening of interdisciplinary collaboration and changes in education, practice, and legal requirements that will increase physical therapists’ ability to use the diagnostic tools specifically related to the movement system; to include the ordering of appropriate imaging and laboratory tests consistent with the clinical areas of practice of the physical therapist; and,
Resolved, APTA supports the strengthening of interdisciplinary collaboration and changes in education, practice, and legal requirements that will allow physical therapists to prescribe appropriate classes of medication, as they do in the military that are consistent with the clinical area of practice of the physical therapist and the movement system.
Reference : 1. American Physical Therapy Association. Vision Statement for the Physical Therapy Profession; 2013. http://www.apta.org/Vision/. Accessed 3-14-
15.
SS: The APTA Board of Directors at its November 2014 meeting adopted a final definition of the movement system, inclusive of the unique roles and contributions of physical therapists integrating movement system within practice, education, and research.
The human movement system comprises the anatomic structures and physiologic functions that interact to move the body or its components parts.
Physical therapists provide a unique perspective on purposeful, precise and efficient movement across the lifespan based upon the synthesis of their distinctive knowledge of the movement system and expertise in mobility and locomotion.
Physical therapists examine and evaluate the movement system (including diagnosis and prognosis) to provide a customized and integrated plan of care to achieve the individual’s goal directed outcomes.
Physical therapists maximize an individual’s ability to engage with and respond to their environment using movement-related interventions to optimize functional capacity and performance.
To achieve the APTA vision of transforming society by optimizing movement to improve the human experience, physical therapists (PTs) will need an enhanced use of movement-related interventions as well as diagnostic tools that address movement system impairments. To effectively diagnose disorders of the movement system, PTs need a systematic approach of diagnostic categories or labels that will assist the profession in determining the movement system disorder. Reaching agreement within the profession on diagnostic labels will take a concentrated effort, but by achieving this, we can diminish variability of clinical practice.
In 2012, Colorado and Connecticut brought forth RC 13-12 Diagnosis by Physical Therapist, regarding Imaging for physical therapists. This important motion started the process of allowing physical therapists to order imaging. To continue this process we will need to strengthen interdisciplinary collaboration and eliminate regulatory boundaries to allow physical therapists to order imaging that is appropriate and consistent with practice. In England and Australia, physiotherapists already have ordering privileges.1 In the United States, physical therapists in the Armed Forces are able to order imaging that is appropriate to practice. In 1972, the US Army did not have enough orthopedic surgeons to evaluate neuromusculoskeletal conditions, which resulted in significant delays in primary care.2 Physical therapists in the Armed Forces were asked to become physician extenders and were able to refer patients for imaging. James and Stuart investigated physical therapists ordering imaging and found that patients receiving expedited care, and referral to radiology was reduced by 50%. In addition 14 orthopedic surgeons were surveyed and all 14 surveyed felt that physical therapists should become primary care extenders and order imaging that is appropriate.3
Kaiser Permanente serves over 8 million members as a not-for-profit health maintenance organization. Physical therapists working for Kaiser Permanente may refer patients for imaging. Similar to the US Army, physical therapists were asked to become primary care extenders because of the challenges faced by primary care physicians.1
Boissonnault conducted a pilot study of 81 patients within a direct access program at a university medical center in which physical therapists were able to order plain film radiographs. Physical therapists referred patients 9.9% of the time for imaging. A physician reviewed the charts of those patients referred for imaging and determined the physical therapist made appropriate decisions on referral 100% of the time.3
In a separate study, Moore et al4 examined the diagnostic accuracy and appropriateness of ordering magnetic resonance imaging for musculoskeletal conditions among orthopedic surgeons, physical therapists, and non-orthopedic surgeons. The clinical diagnostic accuracy was significantly better by orthopedic surgeons and physical therapists than by non-orthopedic surgeons, and there was no significant difference in accuracy between physical therapists and orthopedic surgeons. Physical therapists understand the appropriate referral of a patient who needs imaging.
To improve physical therapists’ abilities to diagnose musculoskeletal conditions and achieve our vision, therapists also need to be able to order laboratory tests that are appropriate to practice setting. Physical therapists are considered musculoskeletal experts and understand conditions that affect a patient’s mobility. For example, a physical therapist working in the acute care setting who is seeing a patient with a deep vein thrombosis (DVT) is currently able to use clinical assessment tools to determine if a DVT is “likely” or “unlikely.” If the patient is likely to have a DVT, the patient is referred for an ultrasound duplex. If this is positive, the patient is treated for a DVT. If this is negative, the patient should receive a D-dimer test. A D-dimer is a simple blood test of fibrin degradation. D-dimer levels in the blood are increased by any condition that produces fibrin and are highly sensitive tests for DVTs. Physical therapists should be able to order laboratory tests that improve the efficiency of health care and are appropriate to the therapist’s clinical setting.
The prescriptive rights portion of this motion was brought forward by Northern Arizona University (NAU) Physical Therapy students from the Class of 2016 as well as NAU faculty. As a delegation, Arizona agreed to bring this issue forward. Here are some thoughts for your consideration.
Physiotherapists in the United Kingdom have had prescribing rights since 2012. “Prescribing rights” refers to all medications and includes medications that may be dispensed from a pharmacy as well as medication dispensed in a hospital setting.
The Australian Physiotherapy Association (APA) began to investigate the possibility of extending prescribing rights to physiotherapists in 2006. Although hospital-based programs are experimenting with limited prescribing rights for physiotherapists, nonmedical prescribing rights in Australia are currently authorized for dentists, midwifes, nurse practitioners, and podiatrists.
APA recently commissioned a study to investigate the financial implications for governments and for patients associated with extending prescribing rights to appropriately qualified and credentialed physiotherapists. Survey link here: surveymonkey.com/r/L6DPRYX
In the United States, physicians, nurse practitioners, dentists, chiropractors, and podiatrists are considered points of entry into the health system with rights to prescribe medications to their patients.
Here are several examples of what would seem to be appropriate practice settings whereby physical therapists should be able to order an appropriate medication:
1. Physical therapists practicing sharp debridement currently need to call a physician to ask for Lidocaine for topical application to a wound to control the amount of pain that a patient will experience during sharp debridement.
2. Physical therapists practicing in the wound care setting currently need to call a physician to ask for a prescription for enzymatic debriding medication that would facilitate autolytic debridement in treating patients with copious adherent slough on a wound bed.
3. Physical therapists practicing in the wound care setting currently need to call a physician to ask for a prescription to treat patients with fungal infections that need antifungal medications
4. Physical therapists practicing in the orthopedic setting currently need to call a physician to order pain medications for topical application to an iontophoresis patch.
The Arizona delegation and the NAU Class of 2016 feel that the concept of prescribing rights needs to be brought forward and investigated. Areas that would need to be investigated to make this change may include the following:
1. Perform value analysis to determine the socioeconomic impact2. Determine the classes of medication appropriate for physical therapist practice (e.g, spasticity medication for
neurological specialists, and pain or anti-inflammatory medications for orthopedic specialists)3. Develop a plan for educating current and future physical therapists (e.g, continuing education courses, DPT program
curricula)4. Gauge interest of the proposed changes among the medical and patient communities5. Develop a strategy for legislative action for the policy and inclusion in state practice acts
Knowing that this is a controversial issue and that implementation of this motion may take several years, the Arizona delegation would like to start the discussion now.
References:1. Burley T. The diagnostic dilemma. Physical therapists lack of imaging privileges. Unpublished data, paper submitted for Rocky Mountain University of
Health Professions class OS 606.2, Fall 2012.2. James JJ, Stuart RB. Expanded role for the physical therapist. Screening musculoskeletal disorders. Phys Ther. 1975;55(2):121-131.3. Boissonnault WG, Badke MB, Powers JM. Pursuit and implementation of hospital-based outpatient direct access to physical therapy services: an
administrative case report. Phys Ther. 2010; 90(1):100-109.4. Moore JH, Goss DL, Baxter RE, et al. Clinical diagnostic accuracy and magnetic resonance imaging of patients referred by physical therapists,
RC 17-15 ADOPT: IDENTIFICATION OF PHYSICAL THERAPISTS BY PROFESSIONAL TITLE
That the following position be adopted:
IDENTIFICATION OF PHYSICAL THERAPISTS BY PROFESSIONAL TITLE
Physical therapists should be identified by their professional title (physical therapist or doctor of physical therapy) and not by generic terms such as allied health, nonphysician provider, or physician extender.
SS: Some health service delivery providers have begun phasing out the use of generic terminology, such as allied health and nonphysician provider, when referring to nonphysician health professionals in favor of using individual professional titles.1 As the American Physical Therapy Association (APTA) continues its efforts to transform the profession as part of achieving the vision, clarifying our identity of self-determined, professional practitioners and being described by the professional title earned, rather than by inaccurate nomenclature, could help to highlight our value and expertise to external entities.
Consumer Protection Through Licensure of Physical Therapists and Physical Therapist Assistants (HOD P06-14-08-18) includes positions related to appropriate legal terminology for identifying physical therapists (regulatory designation, title protection), but no APTA positions exist on how physical therapists should be identified in other avenues of communication (eg, interprofessional communications, health services delivery language).
RC 21-112, adopted by the 2011 House of Delegates (House), charged APTA to advocate for physical therapy to be recognized as a distinct, self-determined profession and stated efforts should include pursuing appropriate opportunities to eliminate the terms “allied,” “allied health,” and “ancillary” when used in association with or classifying the profession of physical therapy and the physical therapist. This charge, however, did not create a position statement.
A House position on this issue of appropriate nomenclature would provide direction to APTA staff so that when opportunities to support this change in nomenclature are encountered, staff could move forward with them. In addition, this position could lend support to any members who may want to promote such a change in nomenclature within their workplaces .
References:1. Shank B. Society of Hospital Medicine phases out inaccurate nomenclature for healthcare professionals. The Hospitalist. May 1, 2014. Accessed
February 5, 2015. Available at: http://www.the-hospitalist.org/article/society-of-hospital-medicine-phases-out-inaccurate-nomenclature-for-healthcare-professionals/
2. American Physical Therapy Association House of Delegates. RC 21-11 Recognition of Physical Therapy as a Distinct, Self-Determined Profession. In Summary of House of Delegates Activities APTA 2011 House of Delegates. American Physical Therapy Association. Alexandria, VA: 2011.
CURRENT POSITION/ STANDARD/GUIDELINE/POLICY/PROCEDURE : NONE
RELATED POSITION/ STANDARD/GUIDELINE/POLICY/PROCEDURE : PREFERRED NOMENCLATURE FOR THE PROVISION OF PHYSICAL THERAPY (HOD P06-13-25-20)CONSUMER PROTECTION THROUGH LICENSURE OF PHYSICAL THERAPISTS AND PHYSICAL THERAPIST ASSISTANTS(HOD P06-14-08-18)
Whereas, Bullying among health care professionals has been extensively reported and documented as having serious negative outcomes for practitioners and their professions, patients, and health care organizations;
Whereas, Bullying is defined as an ongoing conflict in which the victim is subjected to 2 or more negative incidents on at least a weekly basis over at least a 6-month period1; and,
Whereas, Bullying behaviors can occur in any setting where physical therapists and physical therapist assistants practice, learn, teach, research, and lead;
Resolved, The American Physical Therapy Association advocates for professional practice environments that are free of bullying among and between physical therapists, physical therapist assistants, and other health care professionals.
Reference:1. Leymann H. The content and development of mobbing at work. Eur J of Work and Org Psych. 1996; 5: 165-184.
SS: The definition of bullying used in many studies in the health care literature is that of Swedish psychologist Leymann who defines it as an ongoing conflict in which the victim is subjected to 2 or more negative incidents on at least a weekly basis over at least a 6-month period.1 Lutgen-Sandvik adds to this definition power disparity, where targets find it difficult to defend against and stop the abuse.2 The Workplace Bullying Institute defines workplace bullying as “the repeated mistreatment of one or more employees with a malicious mix of humiliation, intimidation and sabotage of performance as well as the deliberate, hurtful, repeated mistreatment of employees driven by the desire to control.”3 The working definitions of bullying in the literature have in common the concept that the bully’s behavior is deliberate and targeted to a specific victim, occurring frequently and with a level of intensity over a period of time.
Bullying behaviors are both overt and covert, which often make it difficult for the victim to recognize, identify, respond to, and report bullying. Raynor and Hoel identify 5 categories of bullying behaviors4:
66
Threat to Professional Status
Belittling opinionsPublic professional humiliationAccusation of lack of effort
Threat to Personal Standing
Gossiping about youName callingInsultsTeasing
Isolation
Preventing access to opportunities for leave or trainingPhysical or social isolationWithholding of information
Overwork
Undue pressure to produce workImpossible deadlinesUnnecessary disruptions
Destabilization
Failure to give credit where credit is dueMeaningless tasksRemoval of responsibilitiesShifting of goalpostsRepeated reminders of errorsSetting up to fail
The term “disruptive behavior,” as defined by the American Medical Association,5 includes the overt behaviors of bullying listed above under threat to professional status and threat to personal standing, but not the covert behaviors listed under isolation, overwork, and destabilization. As per the Workplace Bullying Institute, not calling bullying "bullying," to avoid offending the sensibilities of those who made the bullying possible, is a disservice to bullied individuals whose jobs, careers, and health have been threatened as the result.3
While there are only 2 studies specifically examining bullying in the physical therapy profession (conducted on small samples in Ireland and the UK6,7), it is evident from multiple studies of bullying in health care that anywhere from 30%-35% of health care providers have experienced bullying, and even more have witnessed it. In a survey of the National Health Service in England by Quine, 38% of health care workers and 37% of therapists reported incidents of 1 or more types of bullying.8 A survey on intimidation conducted by the Institute for Safe Medication Practices found that 40% of clinicians have kept quiet or remained passive during patient care events rather than question a known intimidator.9 The Workplace Bullying Institute 2014 Survey found that 27% of workers have experienced bullying firsthand.10
The repercussions of bullying are far reaching, affecting all levels: the employee or volunteer, the team/unit/department and the organization, association, and profession. Victims display serious physical, emotional, and psychological effects. Teams experience decreased morale, productivity, and attendance. Organizations encounter increased turnover, higher costs, compromised employee and patient safety, and, at times, legal action.
Solutions rally around education for both employees and managers, and development of organizational policies. There are currently no legal protections for the victims or the organizations who have actually implemented strategies to protect their employees from bullying. Nursing has struggled with its culture, which some believe tolerates this behavior and has perpetuated it over time. However, nursing has also become very active in addressing this detriment to that profession. The American Nurses Association House of Delegates adopted a resolution regarding “Hostility, Abuse and Bullying in the Workplace” in 2010 which was a reaffirmation of its existing principles from the 2006 resolution related to workplace abuse and harassment of nurses. Additionally, the 2010 resolution included additional recommendations for action to proactively reduce the growing problem of workplace, abuse, harassment, and bullying of nurses and to explore collaborative solutions with other disciplines and organizations to leverage resources for research and education.11 In early 2012, the American Nurses Association (ANA) updated its educational booklet, Bullying in the Workplace: Reversing a Culture, and an accompanying continuing education module to help nurses understand and deal with bullying and its perpetrators and to counter the culture of bullying in their work environments. This publication is for nurses who want to increase their professional awareness and knowledge and develop the skills needed to create safe workplaces.
Key topics include the following12:
Recognizing acts of bullying Identifying the causes and consequences of bullying Learning about the expected actions and responsibilities of individual nurses, nurse managers, and health care
organizations, including zero-tolerance policiesIn addition, the American Medical Association, through its Council on Ethical and Judicial Affairs, supports the designation of “disruptive physician” as a potential disciplinary mechanism. It has defined 2 distinct forms of physician behaviors (inappropriate and disruptive) upon which such actions can be based.5
The Joint Commission (TJC), in Sentinel Event Alert, Issue 40, July 9, 2008, proclaims its intolerance of intimidating and disruptive behaviors in the document “Behaviors That Undermine a Culture of Safety.” In January 2009, TJC implemented a Leadership Standard (LD.03.01.01) that addresses disruptive and inappropriate behaviors in 2 of its elements of performance: EP 4: The hospital/organization has a code of conduct that defines acceptable and disruptive and inappropriate behaviors; and EP 5: Leaders create and implement a process for managing disruptive and inappropriate behaviors. This document also includes 11 suggested actions to ensure compliance.13
APTA has not specifically addressed bullying in our profession; however, members are bringing the issue to the forefront through education. Most recently, an article “5 Myths about Bullying in the Workplace, written by a member, appeared in the February 2015 PT in Motion.14 A year before, a member delivered a 2-hour presentation at CSM on bullying in health care. The APTA Code of Ethics for the Physical Therapist and the Standards of Ethical Conduct for the Physical Therapist Assistant address discrimination and sexual harassment specifically, but not bullying.15,16 Discrimination and sexual harassment are already covered by Title VII of the Civil Rights Act and under state fair employment laws.17 However, no state or federal laws exist to protect employees against bullying, making it that much more important for APTA to take a position on this detriment to its members.
The Healthy Workplace Bill, which provides protection from bullying to both employees and employers, was initiated in 2001. Twenty-eight states and 2 territories have introduced the bill, but no laws have been enacted. Five states currently have a bill active, most recently Virginia in January 2015. In 2010, the New York and Illinois state senates passed the bill. Discussions about a federal law were begun in 2010 with members of the US House of Representatives and the US Senate.18
The intention of this motion is to bring awareness to physical therapists and physical therapist assistants of the covert behaviors that are bullying, as often victims don’t even realize until after they have been educated that indeed they were being bullied. Bullying is a bit like the silent killer heart disease. It is quietly undermining the “just cultures” that we strive to implement in health care and therefore compromising patient safety. Bullying has the potential, like it has clearly in nursing, to undermine our efforts to recruit and retain physical therapists into our organizations and even our profession.
Bullying is an issue that is often ignored or swept under the rug because it is underreported and difficult to address. As Lewis Maltby, president of the National Workrights Institute, states: “Bullying is the sexual harassment of 20 years ago; everybody knows about it, but nobody wants to admit it.”19 A position statement would clarify that APTA is not falling into this trap but is clarifying its knowledge of the problem and in turn taking a step toward protecting its members, as there are no state or federal laws to do so at this point. This action in itself will increase awareness and may provide support for the development of educational tools for members regarding this serious obstacle to professional practice and personal well-being. It will also support state chapters such as the American Physical Therapy Association of New Jersey (APTANJ), which, in January 2015, supported a member who was bullied by another profession’s state association and in turn distributed its position to its membership: “As an association, we will not tolerate harassment, intimidation, or bullying at any level. There is no excuse for using intimidation or harassment to inject fear into any health care practitioner; especially when done by another individual or professional association. The APTANJ does not condone this type of behavior nor would we expect it from any member, nonmember, or representative of our Association.”20
References:1. Leymann H. The content and development of mobbing at work. Eur J of Work and Org Psych. 1996; 5: 165-184.2. Lutgen-Sandvik P, Tracy S, Alberts, J. Burned by Bullying in the American Workplace: Prevalence, Perception, Degree and Impact. Journal of
Management Studies. 2007; 44:6: 837-862.3. The WBI Definition of Workplace Bullying. Workplace Bullying Institute. http://www.workplacebullying.org/individuals/problem/definition/ Accessed
March 1, 20154. Raynor C, Hoel H. A summary review of literature relating to workplace bullying. J Community Appl Soc Psych. 1997; 7: 181-191.5. Schoppmann M. The Law and the “Disruptive Physician”. American Academy of Orthopedic Surgeons NOW. August 2011.
http://www.aaos.org/news/aaosnow/aug11/managing6.asp Accessed March 1, 2015.6. Seager A. Workplace bullying of physiotherapists in Ireland: what actions do victims take? Physiother Ireland. 2004;25: 3-13.7. Whiteside D, Stubbs b, Soundy A. Physiotherapy students’ experiences of bullying on clinical internships: a qualitative study. Physiotherapy. 2014;
100: 41–46.8. Quine L. Workplace bullying in NHS community trust: staff questionnaire survey. BMJ. 1999; 318: 228-232.9. Institute for Safe Medication Practices: Survey on workplace intimidation. 2003. https://ismp.org/Survey/surveyresults/Survey0311.asp Accessed
November 30, 201310. 2014 WBI US Workplace Bullying Survey. Workplace Bullying Institute. April 8, 2014. http://www.workplacebullying.org/2014/04/08/2014-
prevalence/ Accessed March 1, 2015.11. American Nurses Association (ANA) 2010 House of Delegates resolution: hostility, abuse and bullying in the workplace.
http://nursing2015.files.wordpress.com/2012/04/hostilty.pdf Accessed November 30, 201312. ANA releases updated edition of anti-bullying booklet, CE. April 2. 2012. The American Nurse.
http://www.theamericannurse.org/index.php/2012/04/02/ana-releases-updated-edition-of-anti-bullying-booklet-ce/ Accessed January 18, 2015.13. The Joint Commission, Sentinel Event Alert, Issue 40, July 9, 2008. Behaviors that undermine a culture of safety.
http://www.jointcommission.org/assets/1/18/SEA_40.PDF Accessed March 1, 2015.14. Green-Wilson, J. 5 myths about bullying in the workplace. PT in Motion. 2015; 54. 15. American Physical Therapy Association House of Delegates. Code of Ethics for the Physical Therapist (HOD S06-09-07-12). Alexandria, Virginia:
American Physical Therapy Association; 2009.16. American Physical Therapy Association House of Delegates. Standards of Ethical Conduct for the Physical Therapist Assistant (HOD S06-09-20-18).
Alexandria, Virginia: American Physical Therapy Association; 2009.17. Title VII of the Civil Rights Act of 1964. US Equal Employment Opportunity Commission. http://www.eeoc.gov/laws/statutes/titlevii.cfm Accessed
March 1, 2015.18. The Healthy Workplace Bill. http://www.healthyworkplacebill.org/bill.php Accessed March 1, 2015.19. Daniel, T. A White Paper from the Society for Human Resource Management. http://thepeoplegroup.com/wp-content/uploads/2008/04/article-
bullies-in-the-workplace1.pdf Accessed March 23, 2015.20. Professional Harrassment in New Jersey Will Not Be Tolerated. American Physical Therapy Association of New Jersey. January 14, 2015
http://aptanj.org/news/210757/PROFESSIONAL-HARASSMENT-IN-NEW-JERSEY-WILL-NOT-BE-TOLERATED.htm Accessed March 1, 2015.
CURRENT POSITION/STANDARD/GUIDELINE/POLICY/PROCEDURE:NONERELATED POSITION/ STANDARD/GUIDELINE/POLICY/PROCEDURE :CODE OF ETHICS FOR THE PHYSICAL THERAPIST (HOD S06-09-07-12)
RC 19-15 EXPLORE THE FEASIBILITY OF OBTAINING PRIMARY CARE PRACTITIONER STATUS
That the American Physical Therapy Association explore the feasibility of obtaining “primary care practitioner” status for physical therapists as determined by the US Department of Health and Human Services and its operating divisions, with a report to the 2017 House of Delegates.
SS: In these times of ever-changing health care, it is imperative that the American Physical Therapy Association (APTA) ensure that physical therapy is at the forefront. With the change in the vision statement, “Transforming society by optimizing movement to improve the human experience,” APTA is working to address societal change and changes in the profession. The tools that we, as professionals and lifelong learners, use to provide the best care are analyzed, rearranged, and added. With increased knowledge and educational advances, new tools are added to advance the professional’s response to new challenges. Communication and collaboration are needed internally and externally for advancement of professional tools to be successful. Without external communication and collaboration, the ability is not perceived outside APTA, and the ability of the professional to address the need goes untapped. Physical therapists (PTs) are in a position to assist in health care reform by developing strategies for external entities to realize our specific abilities. The education, collaborative ability, sense of community and family, and ability to have lasting relationships with health care beneficiaries places the PT in a perfect position to petition the Department of Health and Human Services (HHS), Human Services and Health Resources and Services Administration (HRSA), Centers for Medicare and Medicaid Services (CMS), and the administration to include PTs among the professionals designated as a “primary care practitioner” (PCP). This RC will examine the feasibility and enhance the focus on the ability of the physical therapist within health care reform. The urgency is real. Our vision can be achieved, but an aggressive strategy must be set forth to address this goal.
CMS, HHS, and HRSA are all looking for demonstration models to address health care reform. These projects are available to demonstrate how new models can increase efficiency, reduce cost, cut wait time, and increase satisfaction. In the white paper “Projecting the Supply and Demand for Primary Care Providers Through 2020,”1 the needs, expectations, and definitions are laid out concisely. It makes evident that the physical therapist by definition, education curriculum, and training is capable of addressing this issue. The need for PCPs is a current dilemma and will only increase as the years pass. Millions of dollars are being spent to educate new PCPs, while the PT is a qualified professional currently available to address the issue. Multiple research projects have been published related to the physical therapist’s ability to address the needs indicated by HHS. The doctor of physical therapy degree demonstrates the education, ability, and knowledge to satisfy the need and in all cases demonstrate higher satisfaction among patients and physicians involved in the research demonstrations. It is estimated that individuals with neuromusculoskeletal complaints and conditions account for 33% of the population seen by the general practitioner, and in the research, the PT has demonstrated the ability to evaluate, assess, treat, and/or refer this population.
The Institute of Medicine’s Committee on the Future of Primary Care defined primary care as “The provision of integrated, accessible health services by clinicians who are accountable for addressing a large majority of personal health care needs, developing a sustained partnership with patients, and practicing in the context of family and community.”2 Disciplines generally considered in the definition of PCPs may include physicians, nurse practitioners, and physician assistants who trained and practice in primary care specialties. The DPT graduate is educated in primary care, differential diagnosis, diagnostic imaging, cultural competencies, evidence-based practice, and research in health professions, all of which address the definition above.
In 2009, the Association of American Medical Colleges (AAMC) conducted a survey of primary care physicians and asked the physicians what steps they would take if their practice experienced a significant increase in demand, such as from the Affordable Care Act. Preliminary findings suggest that many practices would likely respond by hiring additional support staff. When asked what they thought society should do to expand primary care capacity, these same physicians responded that various health care system redesign initiatives would have an impact. The most common response was to increase the efficiency of care delivery by reducing paperwork (90% response), improving productivity (69%), and providing technology (66%). Literature indicates that the PT increases efficiency and satisfaction while reducing wait time and reducing the load on the general practitioner through examination, evaluation, treatment, treatment and referral, or referral only, thus improving the provision of health care at an improved cost. The national demand for primary care services can be defined as the quantity and mix of services that society is willing to pay for based on population needs, economic constraints such as income and prices, and technological considerations of what is possible to provide. The demand for PCPs is the number and mix of clinicians needed to meet the demand for services. Therefore, practitioner productivity, scope of practice, and how the health care system is structured for care delivery influence the demand for practitioners in specific disciplines. Changing population demographics, including the aging and growth of the population, account for the majority (81%) of the projected increase in demand for PCPs between 2010 and 2020. In contrast, only 19% of the increased demand for PCPs from 2010 through 2020 is associated with the estimated expansion of the population covered by health insurance with the full implementation of the Affordable Care Act.
In her 2005 Journal of Orthopaedic and Sports Physical Therapy article, "Are Physical Therapists Fulfilling Their Reasonability as Diagnosticians," Shirley Sahrmann, PT, PhD, FAPTA, stated, “I believe that we are seriously compromising recognition and respect for the profession because we are not engendering in every PT the responsibility of being a diagnostician. If physical therapists wait to change the expectation that we are diagnosticians until randomized control trials have supported every diagnoses for our scope of practice, the day will never come.”3 This is a critical time to demonstrate the invaluable role we, as movement experts with diagnostic expertise, have in the delivery of safe and efficient health care. Physical therapy cannot afford to wait until the medical community identifies another health professional who will fit the need for skill in performing the diagnostic physical exam. It could be said that the opportunities physical therapists have today are more visionary than could have been realized in 2005 and have indeed come to actuality with health care reform. Our expertise has overwhelmingly increased as physical therapy has moved into a doctoring profession with enhanced professional skills and expertise.
As PCPs, PTs have an opportunity to meet societal needs. Currently PTs are being used as “nonphysician” health care providers (Virginia Mason, Kaiser-Permanente) and used with success in the military, some hospitals, Great Britain, and Australia. By using PTs for their training, education, and experience to perform neuromusculature and musculoskeletal evaluations, wait times are reduced, and satisfactions levels are higher.
There are many possibilities that come with the classification of PCP, tangible and intangible. A pathway to full direct access, research grants, program development, demonstrations projects, and funding for residency and internships are a few of the tangible benefits that could be available. Recently HHS awarded $83.4 million to train new primacy care providers. The funding will help to train more than 550 residents during the 2014-2015 academic year. HHS also announced the availability of $100 million in Affordable Care Act funding to expand primacy care through new community health centers. The health centers will increase access to primary health care services for those who need it most. The opportunities for primary care practitioners are available immediately. The urgency for PTs to be included in these opportunities is great. To learn more about this funding opportunity, visit http://www.hrsa.gov/grants/apply/assistance/nap . A list of awards (asterisk indicates new awardees) is available at www.hrsa.gov/about/news/2014tables/teachinghealthcenters/
References:1. Health Resources and Services Administration Bureau of Health Professions, National Center for Health Workforce Analysis. Projecting the supply and
Demand for Primary Care Practitioners Through 2020. 2013.2. Institute of Medicine, Division of Health Care Services, Committee on the Future of Primary Care. Donaldson MS, Yardy KD, Lohr KN, Vaselow NA
(Eds). Primary Care: America’s Health in a New Era. Washington, DC: National Academy Press; 1996.3. Sharman S. Are physical therapists fulfilling their responsibility as diagnosticians. JOSPT. 2005;35(9).
CURRENT POSITION/STANDARD/GUIDELINE/POLICY/PROCEDURE: NONE
RELATED POSITION/ STANDARD/GUIDELINE/POLICY/PROCEDURE :ENTRY POINT INTO HEALTH CARE (HOD P06-14-07-11) PRIMARY CARE AND THE ROLE OF THE PHYSICAL THERAPIST (HOD P06-06-07-03)
RC 20-15: COLLABORATIONS TO ADDRESS CHILDHOOD AND ADULT OBESITY
Consistent with Vision Statement for the Physical Therapy Profession (HOD P06-13-18-22), the American Physical Therapy Association shall pursue opportunities to participate as a partner in and/or endorse national campaigns against childhood and adult obesity. Potential partnerships or endorsements may include campaigns sponsored by government entities, other health professions and associations, corporate and industry initiatives, sports organizations, schools, and private foundations.
SS: Two key guiding principles of the American Physical Therapy Association‘s (APTA) Vision—Identity and Collaboration—are potentially addressed and put into play in an initiative to join nationwide high-profile campaigns against obesity. Such activity by APTA will highlight our expertise in the movement system and demonstrate our commitment to work collaboratively with a variety of entities to help in a very complex challenge to societal health. In the Identity guiding principle, we state, “The physical therapy profession will define and promote the movement system as the foundation for optimizing movement to improve the health of society.”
In the guiding principle addressing Collaboration, we state, “The physical therapy profession will demonstrate the value of collaboration with other health care providers, consumers, community organizations, and other disciplines to solve the health-related challenges that society faces.”
One of the greatest societal challenges currently facing Americans and the world is obesity. In a widely publicized report of the McKinsey Global Institute in November 2014, Overcoming Obesity: An Initial Economic Analysis, the authors present the significant reality of this problem. They state:
Obesity is now a critical global issue, requiring a comprehensive intervention strategy rolled out at scale. More than 2.1 billion people—nearly 30 percent of the global population—are overweight or obese. That’s nearly 2 and a half times the number who are undernourished. Obesity, which should be preventable, is now responsible for about 5 percent of all deaths worldwide. If its prevalence continues on its current trajectory, almost half of the world’s adult population will be overweight or obese by 2030.
The global economic impact from obesity is roughly $2.0 trillion, or 2.8 percent of global GDP, roughly equivalent to the global impact from smoking or from armed violence, war, and terrorism.1
The report outlines many potential large-scale interventions, some of which relate to physical activity and movement. Many major initiatives against childhood and adult obesity receive regular media attention and offer opportunities for our profession, which espouses a core identity with the movement system, to demonstrate support. Individual physical therapists may also find avenues (and indeed already have) to contribute. Here is a sample of large-scale activities currently under way:
Let’s Move, First Lady Michelle Obama's campaign against childhood obesity (www.letsmove.gov/) The NFL’s “Play 60 Movement” to get kids active and moving for 60 minutes a day
(www.nfl.com/news/story/09000d5d80b4a489/article/nfl-play-60-the-nfl-movement-for-an-active-generation) The Alliance for a Healthier Generation, a partnership between the American Heart Association and the Clinton
Foundation (www.healthiergeneration.org/) The Campaign to End Obesity, a policy advocacy group (www.obesitycampaign.org / ) The Healthy Weight Commitment Foundation, a food industry CEO organization
There are many other avenues and campaigns for potential involvement. We, the physical therapy profession, need to find the way to get off the sidelines and into the game.
One of the summary recommendations of the McKinsey Global Institute report is that “No single solution creates sufficient impact to reverse obesity: only a comprehensive, systemic program of multiple interventions is likely to be effective.”1
Why not get involved in this major society challenge with our unique knowledge and skill set in the promotion and health interventions involving the movement system?
Reference:1. McKinsey Global Institute. Overcoming Obesity: An Initial Economic Analysis. McKinsey&Company; November 2014.
http://www.mckinsey.com/insights/economic_studies/how_the_world_could_better_fight_obesity . Accessed March 12, 2015.
CURRENT POSITION/STANDARD/GUIDELINE/POLICY/PROCEDURE:NONE
RELATED POSITION/ STANDARD/GUIDELINE/POLICY/PROCEDURE :PHYSICAL THERAPISTS AS EXPERT PROVIDERS OF EXERCISE AND PHYSICAL ACTIVITY PRESCRIPTION (HOD P06-12-20-07)
RC 21-15: INCORPORATION OF STANDARDIZED PHYSICAL THERAPIST PATIENT/CLIENT MANAGEMENT ELEMENTS IN ELECTRONIC HEALTH RECORDS
That the American Physical Therapy Association develop and implement a plan to promote to external stakeholders the value of appropriately incorporating standardized elements of physical therapist patient/client management into electronic health records. A report will be submitted to the 2016 House of Delegates delineating this plan with expected implementation in 2016. Subsequent reports will be submitted to the House of Delegates until the charge of the motion has been met.
SS: In 2013, The House of Delegates adopted our new vision statement, which asserts that we will “transform society by optimizing movement to improve the human experience.”1 To achieve this vision, we must continue to provide and document quality, value, innovation, and consumer-centricity. This documentation will be enhanced by the availability of reliable, valid, patient-focused outcome data and financial data.2 Current large longitudinal electronic health record (EHR) systems have not been designed to easily capture data from physical therapist services to support patient/client management, clinical improvement activities, and research. Given that the American Physical Therapy Association has committed major resources to build the physical therapy outcomes registry, it is imperative that EHRs provide for standardization in operation, standardized measures, and interoperability to support clinicians as well as secondary data sharing for research purposes. This will, at a minimum, include the following:
Reaching consensus on standard outcome measures to use based on diagnosis/condition, and establishing standard conventions for capturing those data and entering into EHR systems
Advocating for operational standardization to ensure interoperability between different systems necessary to participate in national benchmarking and outcome registry creation
Engaging in the Standards and Interoperability (S&I) Framework Initiative and in electronic eealth record (EHR) standards development as well as with policy makers and other stakeholders to leverage the marketplace to build EHR systems that meet these objectives
Developing systems that fully integrate clinical documentation, patient/client management, financial performance data collection, and analytics; including real-time ability to trend, compare, and aggregate data for uses that range from individual patient/client management to well-designed clinical research
By participating in the construction of these systems, the physical therapy profession will be able to demonstrate that we can and do transform society by optimizing movement to improve the human experience.
References:1. American Physical Therapy Association House of Delegates. Vision Statement for the Physical Therapy Profession (HOD P06-13-18-22). Alexandria,
VA: American Physical Therapy Association, 2013.2. American Physical Therapy Association House of Delegates. Guiding Principles to Achieve the Vision (HOD P06-13-19-23). Alexandria, VA: American
Physical Therapy Association, 2013.
CURRENT POSITION/STANDARD/GUIDELINE/POLICY/PROCEDURE:NONE
RELATED POSITION/ STANDARD/GUIDELINE/POLICY/PROCEDURE :SUPPORT OF ELECTRONIC HEALTH RECORD IN PHYSICAL THERAPY (HOD P06-08-13-11)
RC 22-15: STANDARDS AND INTEROPERABILITY FOR HEALTH INFORMATION TECHNOLOGY AND ELECTRONIC HEALTH RECORDS
The American Physical Therapy Association (APTA) shall engage in the Standards and Interoperability (S&I) Framework Initiative and in the iterative process of the development of standards in health information technology (HIT) and electronic health records (EHR) for the purpose of:
Increasing the usability, functionality, interoperability, and security of EHRs; Defining common terminology and guidelines to improve software quality and ensure that structured data capture is
consistent with physical therapist practice, research, and outcomes data needs; Identifying EHR software testing pilots that are clinically plausible and consistent with cognitive workflow design,
and incorporate clinically relevant physical therapy-specific scenarios; Ensuring the ability to use electronic data within and across EHR systems and in the continuum of physical therapist
practice settings; and, Defining clinical decision support criteria to be used for physical therapy coverage and payment decisions.
The EHR standards in development include, but are not limited to HL7,1 SNOMED,2 and LOINC.3
APTA shall develop and implement a plan in 2015 to accomplish the above-stated purposes with reports to the House of Delegates in 2016 and 2017. Members will continue to receive information about APTA activities and developments in standards and interoperability in HIT and EHRs in appropriate venues.
References:1. HL7, Health Level Seven International (HL7) is a not-for-profit, ANSI-accredited standards developing organization dedicated to providing a
comprehensive framework and related standards for the exchange, integration, sharing, and retrieval of electronic health information that supports clinical practice and the management, delivery, and evaluation of health services.
2. SNOMED CT (Systematized Nomenclature of Medicine--Clinical Terms) is a comprehensive clinical terminology owned, maintained, and distributed by the International Health Terminology Standards Development Organisation (IHTSDO), a not-for-profit association.
3. LOINC is a universal code system for tests, measurements, and observations used for the electronic exchange of clinical health information. LOINC is one of a suite of designated standards for use in US-federal government systems and is likely to become a HIPAA standard for some segments of the Claims Attachment transaction to facilitate the exchange and pooling of results for clinical care, outcomes management, and research.
SS: Health information technology (Health IT) that facilitates the secure, efficient, and effective sharing and use of electronic health information when and where it is needed is an important contributor to improving health outcomes, improving health care quality, and lowering health care costs.
Health IT can help physical therapists make better treatment decisions, and can help reduce care delivery redundancy and cost by allowing sharing of information, test results, and outcomes. Health IT can also be leveraged for registries and research and in due course will be used for automated clinical decision support for coverage and payment decisions. Engagement of APTA in ongoing health IT initiatives is needed to shape emerging health IT standards and interoperability requirements to meet the immediate and future IT and EHR needs of physical therapists.
The 2015 Interoperability Standards Advisory represents the model by which the Office of the National Coordinator for Health Information Technology (ONC) will coordinate the identification, assessment, and determination of the best available interoperability standards and implementation specifications for industry use toward specific health care purposes. The Standards & Interoperability (S&I) Framework is ONC’s health information exchange forum where health care stakeholders can focus on solving real-world interoperability challenges and identify standards and implementation specifications for specific purposes.
INTENDED OUTCOME OF MOTIONAPTA and member engagement in the ongoing public-private health information exchange (Standards & Interoperability Framework) can influence and shape Health IT and EHR standards development and pilot testing to represent the needs of physical therapists with the purpose as outlined in the motion above.
APTA ACTIVITIES RELATED TO HIT/EHRThis motion has been discussed with APTA leadership and staff and with the Reference Committee, posted to the House of Delegates discussion board and the NE Caucus listserv. District of Columbia is collaborating with Massachusetts on a similar motion and the chapters plan to work together to streamline the process. To date, as reported by staff, APTA has been involved in 2 major activities related to Health IT, EHR, and HOD 06-08: (1) member education and (2) advocacy. Member education is primarily seen in the website resources at http://www.apta.org/EHR/. APTA has provided public comments in the website resources at http://www.apta.org/FederalIssues/HIT/ to policy bodies in the Health IT issue space and continues to do so. In the 2015 strategic plan, the APTA Payment Policy and Advocacy Committee and Board of Directors, with input from membership stakeholders, identified public policy priorities for 2015-2016 that promote payment reform, innovative care delivery, improved access to care, advancement of quality initiatives, and demonstration of the value and integrity of physical therapy. Missing is a detailed strategic plan that crosses all of these areas and links these important silos together—health information technology and electronic health records--hence the necessity and importance of this motion. The strategic priorities identify the Physical Therapy Outcomes Registry, Physical Therapy Classification and Payment System, Integrity in Practice, and Medicare PQRS. Each of these are directly impacted by Health IT and EHRs. Commitment and participation of APTA and membership is needed to shape HIT and EHR standards to represent the needs of physical therapists.
The Board has proposed adoption of a new 2015 motion that includes a statement “APTA supports the use of electronic health record systems (EHRs) in physical therapist practice and promotes the widespread adoption of interoperable EHRs in all practice settings” and the rescinding of SUPPORT OF ELECTRONIC HEALTH RECORD IN PHYSICAL THERAPY HOD P06-08-13-11 [Position]. Yet more is still needed; hence this motion.
NATIONAL SCOPEIn June 2014, the ONC laid out a 10-year vision for a future health IT ecosystem where electronic health information is appropriately and readily available to empower consumers, support clinical decision-making, inform population and public health, promote value-based payment, and advance science. ONC is engaged in working on the development and harmonization of domestic and international health IT standards, to promote best practices.
In Connecting Health and Care for the Nation: A 10-Year Vision to Achieve an Interoperable Health IT Infrastructure (ONC’s 10-Year Interoperability Concept Paper), ONC committed to leading and collaborating with the health IT and health sector to define a shared Roadmap for achieving interoperable health IT that supports a broad-scale learning health system by 2024. It lays out a plan for what needs to happen, by when, and by whom, to see that electronic health information is available when and where it matters most.
IMPORTANCE OF MOTION Engagement in the S&I Framework is important to APTA and the profession. To participate in the federal government’s EHR incentive program participants are required to use certified EHR technology. The S&I Framework is a public-private partnership to define standards and minimal requirements for certified EHR products. This motion is strategic and visionary to shape the future of health IT and EHR standards, interoperability, and policy to ensure consistency with physical therapist practice, research, and outcomes data needs.
This is the window of opportunity, and the S&I Framework is the forum to shape the health IT system standards to ensure they represent the needs of physical therapists. If physical therapists want EHRs to reflect what we do we must be involved at the standards-making level. Standards are under development to define structured data capture. PTs should be engaged in defining what is included in structured data capture as this is the foundation for our documentation and must be consistent with practice, is critical for registry and outcomes research, and ultimately will dictate what proprietary EHR companies may, shall, or should include in their products. Furthermore, physical therapists should be included in providing rationale and defining rules for automated decision support for important issues such as coverage and payment.Barriers remain to the seamless sharing and use of electronic health information by physical therapists. The ONC draft Roadmap proposes critical actions that the public and private sector need to take to advance the country toward an interoperable health IT ecosystem. Achieving a better care system through health IT interoperability will ensure that the privacy expectations of consumers are respected, that states are aligned in policy, that ONC is aligning payment and other levers to advance and sustain a durable interoperable ecosystem, to make data more portable, and to have a set of standards that allow more seamless sharing of electronic health information for “small” (individual patient), “big” (population level and beyond), and “long” data
(wrapping around individuals and telling their health stories over time). If physical therapists desire financial incentives to advance EHRs to meet our system and practice needs, this is the forum to provide input.
The Roadmap identifies critical actions that should be taken by a wide range of stakeholders to help advance nationwide interoperability. This motion calls for APTA engagement in this process to shape health IT to meet the needs of physical therapist practice, research, outcomes, and ultimately automated clinical decision support for coverage and payment.
It is only through combined APTA and member efforts that we will achieve a learning health system that brings real value to physical therapy electronic health information and EHRs as a means to better care, wiser spending, and healthier people.
Further reading:Conn, J. Federal health IT coordinator sets 2017 deadline for interoperability. Modern Healthcare http://www.modernhealthcare.com/article/20150130/NEWS/301309955?utm_source=modernhealthcare&utm_medium=email&utm_content=20150130-NEWS-301309955&utm_campaign=mh-alert January 30, 2015. Accessed February 20, 2015.
Conn.J. AMA-led group asks feds to redo EHR testing program. Modern Healthcare http://www.modernhealthcare.com/article/20150123/NEWS/150129980 January 23, 2015. Accessed February 20, 2015.
The Office of the National Coordinator for Health Information Technology. Connecting Health and Care for the Nation: A Shared Nationwide Interoperability Roadmap Draft Version 1.0, file:///L:/Documents/APTA/HOD/2015%20HOD%20Materials/nationwide-interoperability-roadmap-draft-version-1.0.pdf January 30, 2015. Accessed February 20, 2015.
Reid, M. American Medical Association Letter to Office of the National Coordinator Health Information Technology. http://mb.cision.com/Public/373/9710840/9053557230dbb768.pdf January 21, 2015. Accessed February 20, 2015.
Mills, R. AMA Press Release. AMA Calls for Design Overhaul of Electronic Health Records to Improve Usability http://www.ama-assn.org/ama/pub/news/news/2014/2014-09-16-solutions-to-ehr-systems.page . September 16, 2014. Accessed February 20, 2015.
CURRENT POSITION/STANDARD/GUIDELINE/POLICY/PROCEDURE:POSITION SUPPORT OF ELECTRONIC HEALTH RECORD IN PHYSICAL THERAPY (HOD P06-08-13-11)
RELATED POSITION/ STANDARD/GUIDELINE/POLICY/PROCEDURE :NONE
(Note: Per Standing Rule 17. Main Motion Criteria, this motion was placed at the end of the agenda because criteria3 and 4 were not met. Consequently, this motion will require a majority vote without debate to be considered.)
Required for Adoption: Majority Vote Category: 6
Motion Contact: Victoria Tilley, PT, GCS, delegate, North CarolinaPhone: 919/614-1923 E-mail: [email protected]
COSPONSORED BY: WISCONSIN CHAPTER AND PEDIATRICS AND HPA SECTIONS
RC 23-15 ADOPT: DESIGNATION OF INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES AS A MEDICALLY UNDERSERVED POPULATION
That the following position be adopted:
DESIGNATION OF INDIVIDUALS WITH INTELLECTUAL AND DEVELOPMENTAL DISABILITIES AS A MEDICALLY UNDERSERVED POPULATION
Whereas, Medically underserved populations (MUPs) may include groups of persons who face economic, cultural, or linguistic barriers to health care;
Whereas, The formula for determining a MUP comprises 4 variables that, when added together, represent the extent to which a population is underserved;
Whereas, The intellectually and developmentally disabled (IDD) population currently qualifies under 3 of the 4 variables and is projected to meet the fourth due to increase in lifespan;
Whereas, The MUP designation is used to help prioritize the distribution of federal and state funds to meet the needs of the population;
Whereas, The MUP designation is seen as a potential avenue to increase the supply of health care providers serving the population;
Whereas, In 2004, the American Academy of Developmental Medicine and Dentistry used the 4 variables to determine that the IDD population should be designated a MUP, and;
Whereas, The American Medical Association passed a resolution in 2011 supporting the IDD population as a MUP1;
Resolved, The American Physical Therapy Association supports the designation of individuals with IDD as a special medically underserved population by appropriate government agencies.
SS: Approximately 7 to 8 million Americans of all ages experience some level of IDD (American Association of Intellectual and Developmental Disabilities- 2009). Intellectual disability is a disability characterized by significant limitations in both intellectual functioning and in adaptive behavior, which covers many everyday social, functional, and practical skills. This disability originates before the age of 18. The degree of disability, which has great variability, can be categorized as mild, moderate, severe, or profound based on the ability to communicate, socialize, and perform activities of daily living.2
The Department of Health and Human Services (DHHS) oversees the Health Resources and Services Administration (HRSA), which is the primary federal agency designed to administer the primary care Health Professional Shortage Area (HPSA) designation system. There are 3 types of HPSA used to prioritize the distribution of federal and state funds based on medical need: geographic, population/group, and facility. Geographic HPSAs, designated as medically underserved areas (MUAs) include entire counties, a portion of a county, or a group of contiguous counties. Population/group HPSAs, designated as medically underserved populations (MUPs), include groups such as immigrant farm workers, low-income urban areas, or federally recognized Native American Tribes within particular geographic areas. Facility HPSAs include federal or state correctional institutions, health centers, and certain rural health clinics.3
To qualify for a MUP designation, HRSA needs to specifically identify the group in its definition. The formula for MUP designation comprises 4 variables that, when added together, represent the extent to which the population is underserved. The 4 variables are: (1) the ratio of primary care physicians to 1,000 individuals in the population with incomes at or below 100% of the federal poverty level in a specific area; (2) the percentage below the federal poverty level; (3) the percentage aged 65 or older; and (4) the infant mortality rate. In 2004, the American Academy of Developmental Medicine and Dentistry (AADMD) used these 4 variables to determine that the IDD population should be designated a MUP.3 However, Congress can legislatively designate that population as a “special medically underserved population,” a designation currently shared by populations that comprise “migratory and seasonal agricultural workers, the homeless, and residents of public housing.”4
The 2012 joint AAIDD/ARC Position on Health, Mental Health, Vision, and Dental Care identifies that the population continues to be significantly medically underserved with the following issues:
While many people encounter difficulty in finding affordable, high-quality health care, people with IDD face additional barriers, sometimes life-threatening, when attempting to access timely, appropriate health services in their communities. These barriers include:
• Access - Underinvestment in public health and wellness targeted to people with IDD results in preventable health care disparities and poorer health outcomes. Inadequate training, lack of coordinated care, and inadequate levels of reimbursement are some of the factors that create programmatic barriers while inaccessible clinical settings and diagnostic and medical equipment, along with translation and interpretation challenges, create physical barriers.
• Discrimination - Health care providers sometimes provide inadequate or inappropriate interventions and treatments or deny appropriate care for people with IDD because of professional ignorance as well as personal and/or societal bias. State statutory liability damage limits discriminate against people with severe and/or life-long disabilities because they fail to provide sufficient compensation.
• Affordability - People with IDD are more likely to live in poverty and cannot afford cost-sharing. For cost containment purposes, many public and private health care plans limit access to specialists and critical services. Even when services are available in a community, many people with IDD lack adequate public or private insurance to pay for them.
• Communication and personal decision making - People with IDD may have difficulties communicating their needs and making health care decisions without support. Their decisions may not be respected and implemented by health care providers and, where applicable, surrogate decision makers.** People have not been ensured access to all necessary supports and information required to understand a health care decision and communicate their choices.5
The funding from HRSA generally flows through community health clinics and other federally funded clinics that are required to serve the MUP. Admittedly, this does not specifically open up access to care by physical therapists, but this position does support our professional beliefs in equal access to quality health care for all members of society.
References: 1. American Medical Association House of Delegates. Designation of the Intellectually Disabled as a Medically Underserved Population (AMA
Resolution 805-I-10). Chicago, IL . 2011.2. Definition of Intellectual Disability. American Association on Intellectual and Developmental Disabilities website. http://aaidd.org/intellectual-
disability/definition#.VQmZ447F_ng. Updated 2013. Accessed March 2015. 3. Sullivan TE. Designation of the Intellectually Disabled as a Medically Underserved Population. CMS Report 3-I-11. Resolution 805-I-10. Page 2, lines
31-40. 4. Kornblau,BL; The Case for Designating People with Intellectual and Developmental Disabilities as a Medically Underserved Population. Autistic Self
Advocacy Network Policy Brief, pg.4, April 2014. Accessed March 2014. 5. Position on Health, Mental Health, Vision, and Dental Care. Joint position by The Arc and American Association on Intellectual and Developmental
Disabilities. AAIDD website. http://aaidd.org/news-policy/policy/position-statements/health-mental-health-vision-and-dental-care#.VQnEG47F_ng. Adopted AAIDD BOD February 2013. Accessed March 2015.
CURRENT POSITION/STANDARD/GUIDELINE/POLICY/PROCEDURE:NONE
RELATED POSITION/ STANDARD/GUIDELINE/POLICY/PROCEDURE :NONE





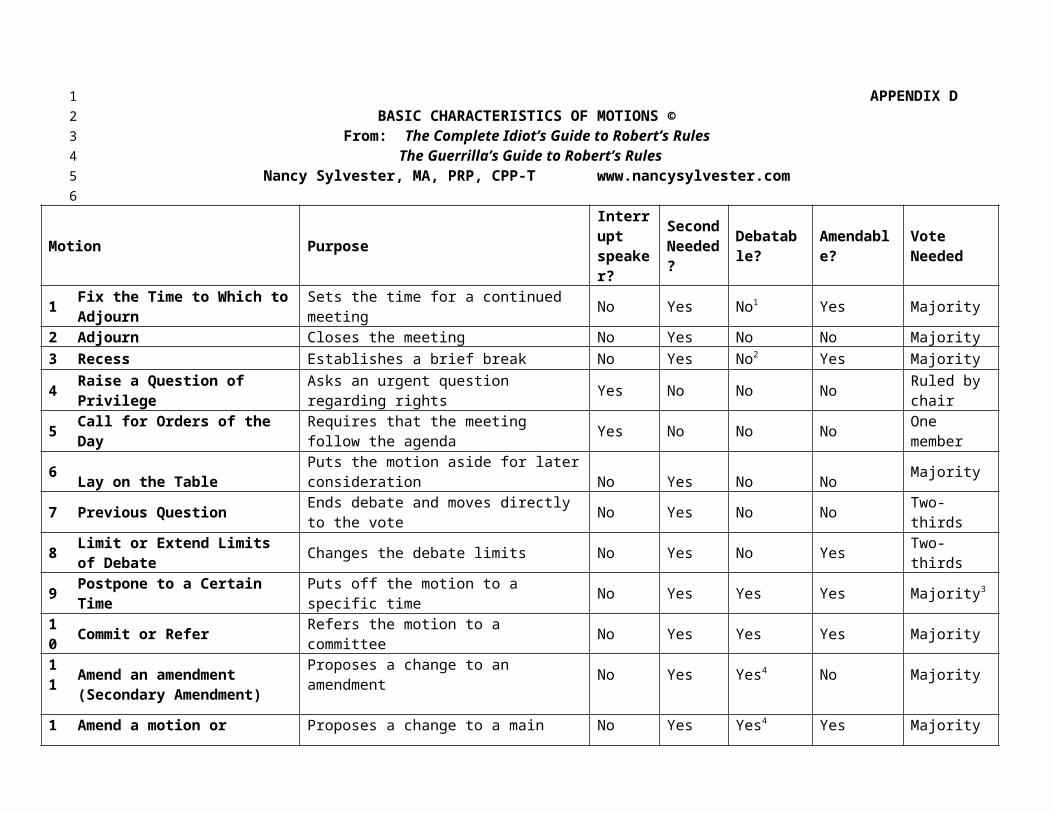



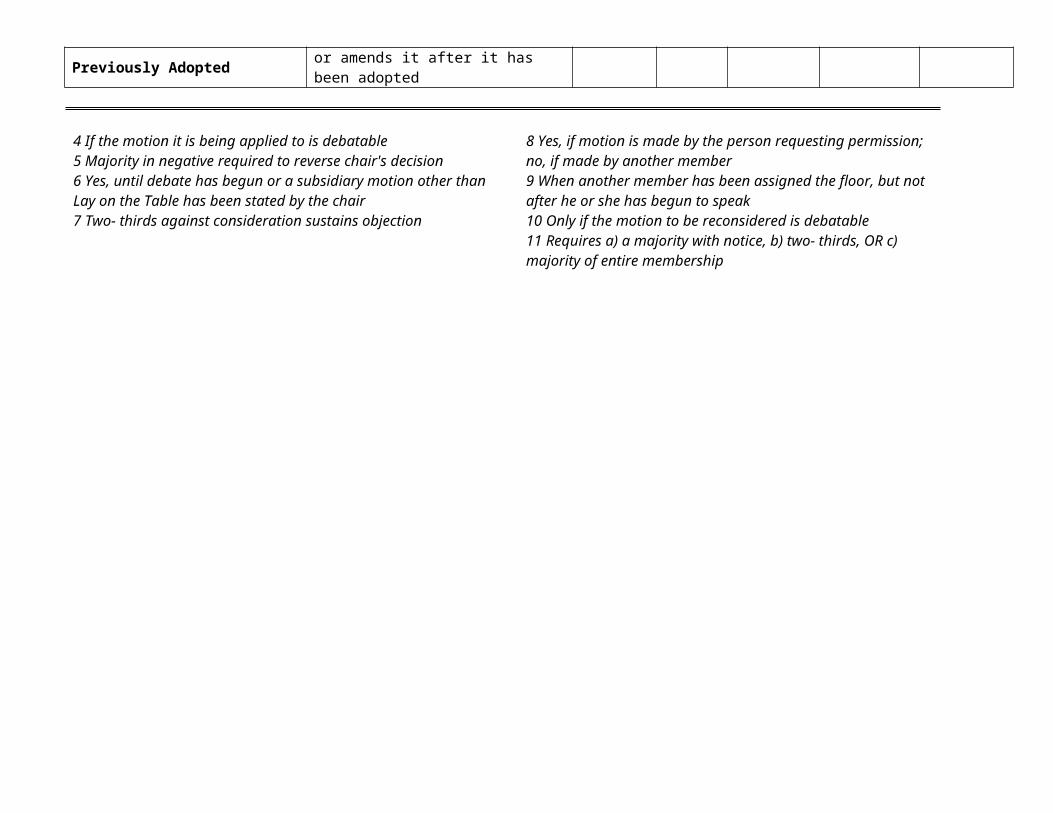














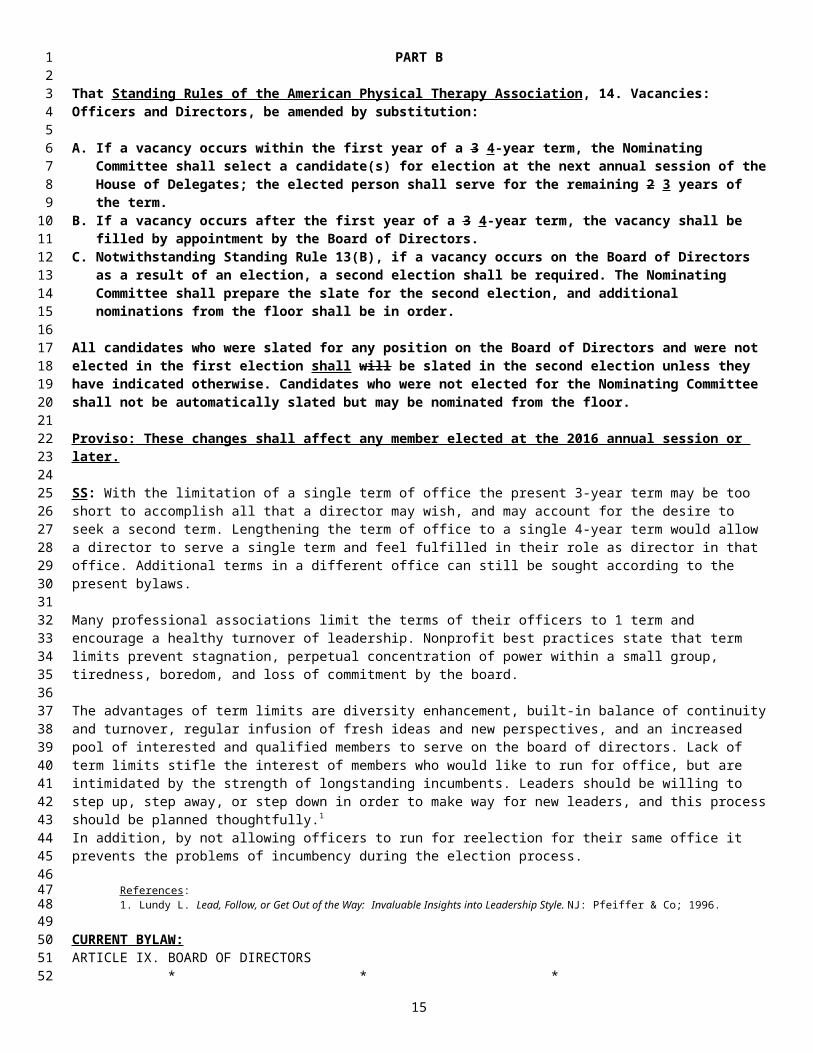












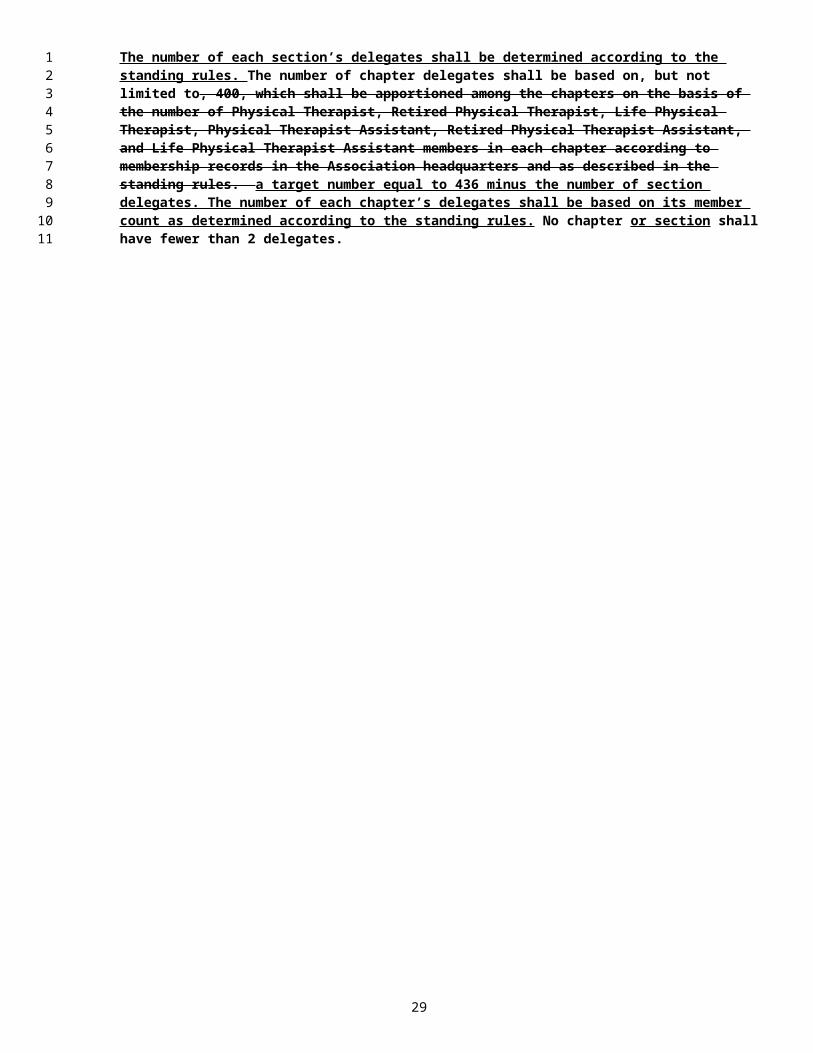








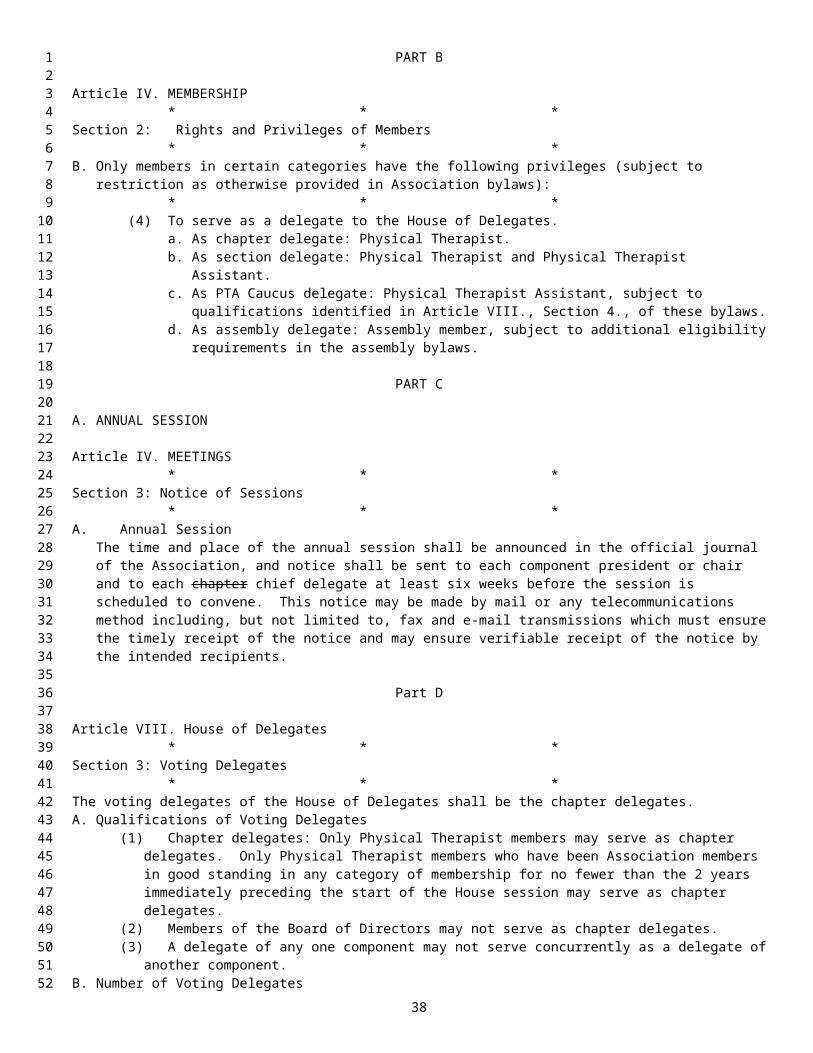
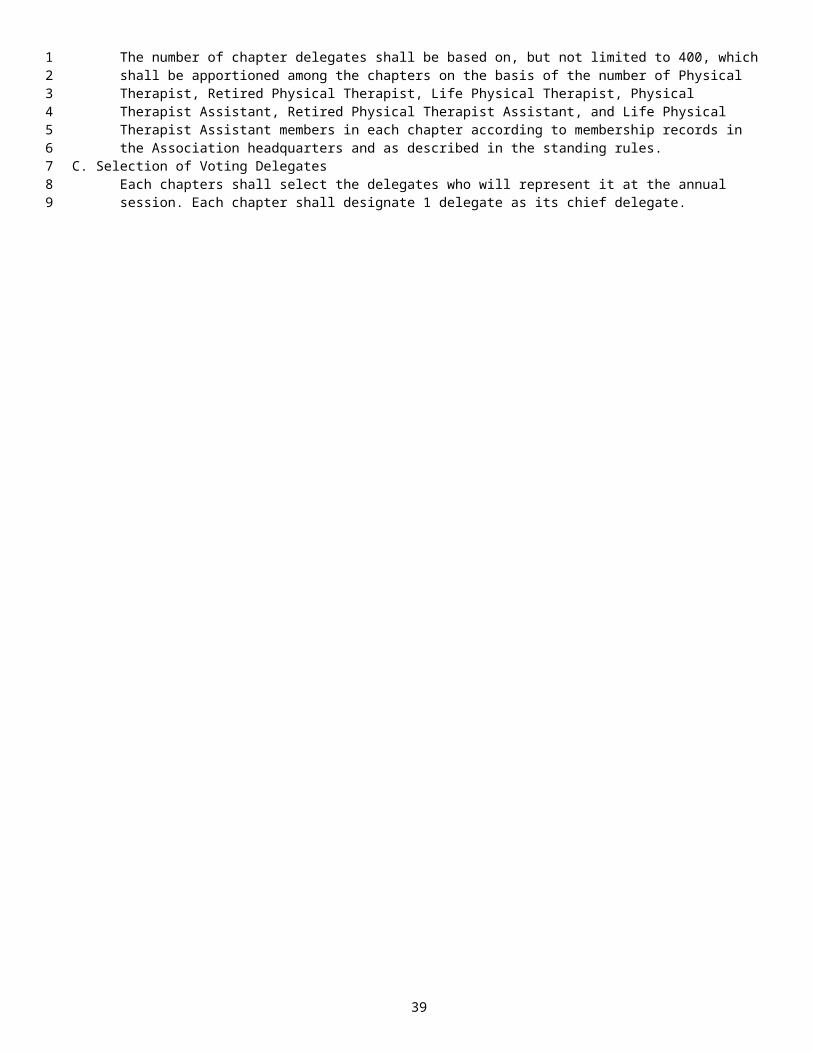

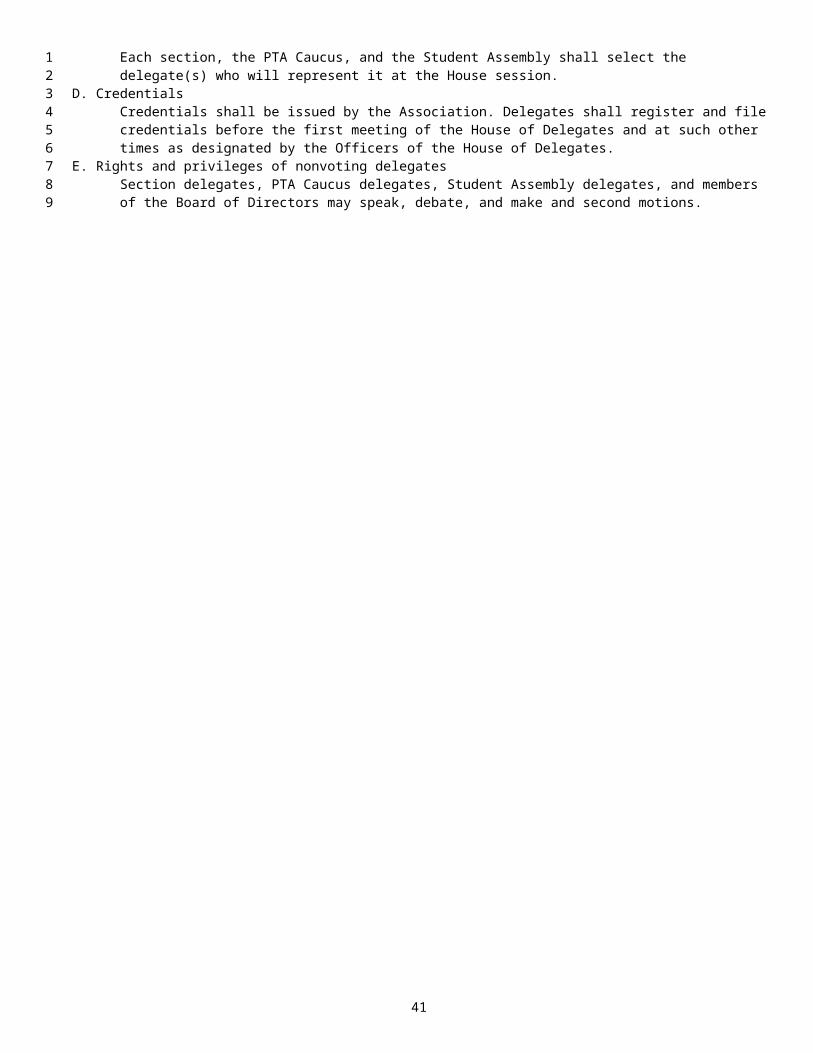





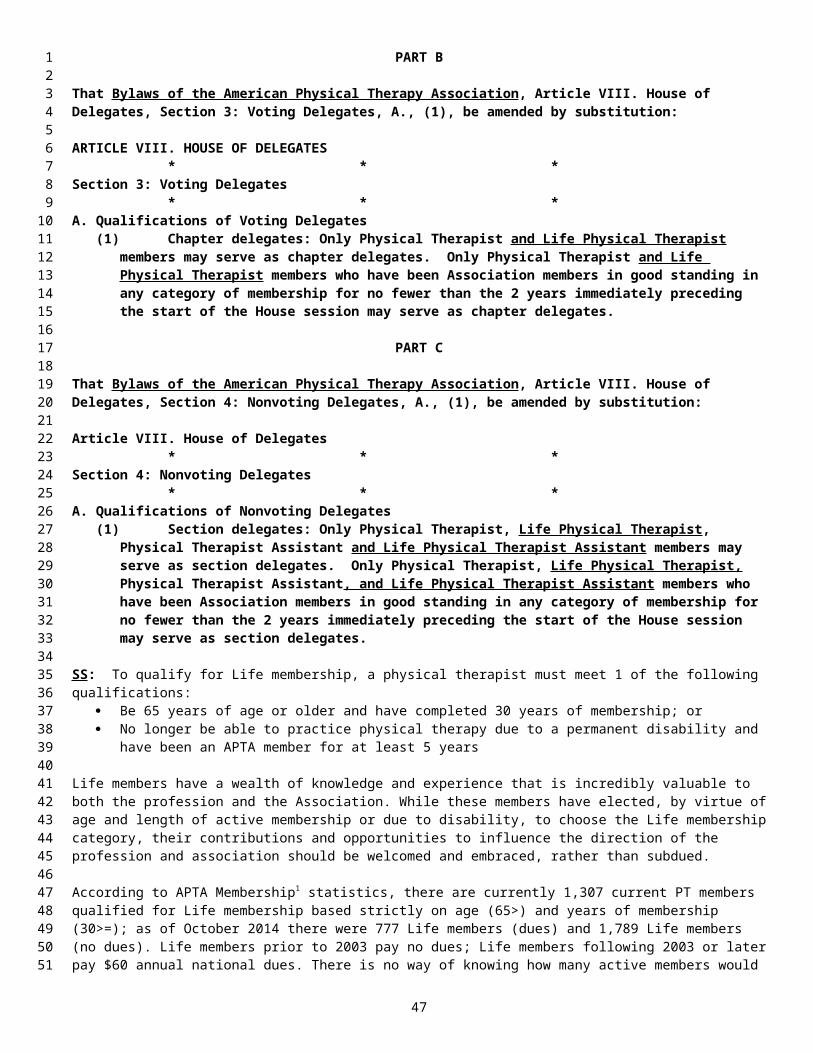








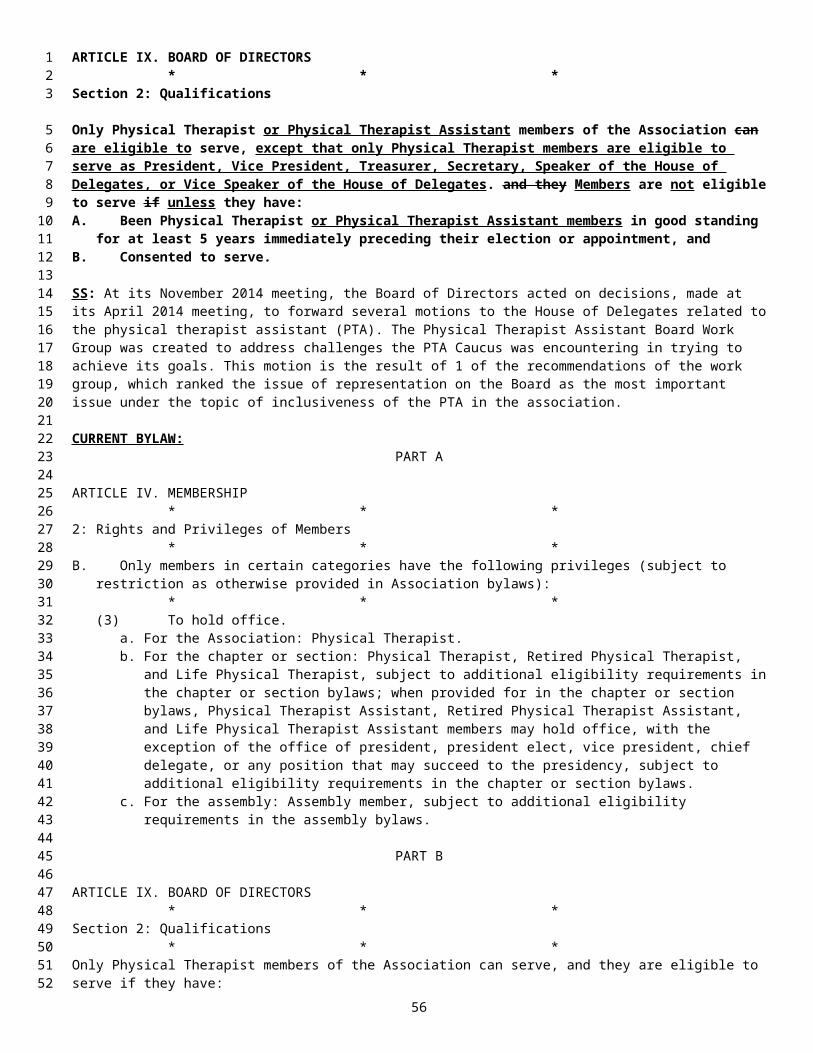






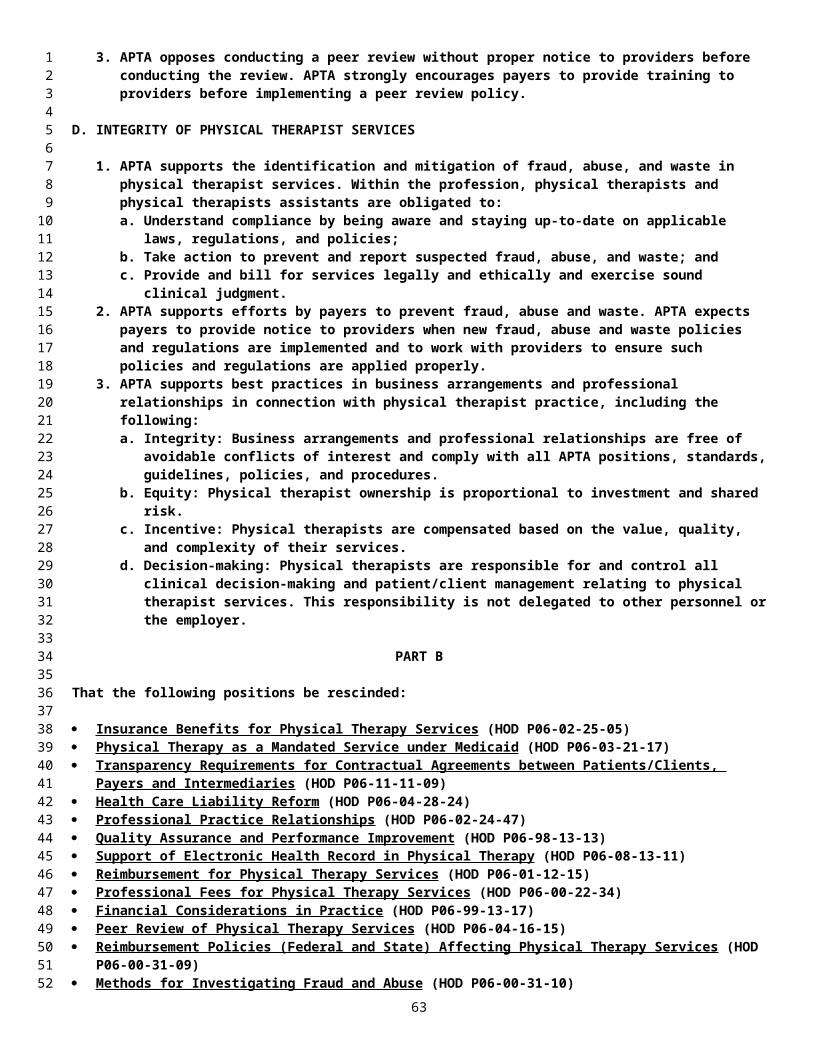
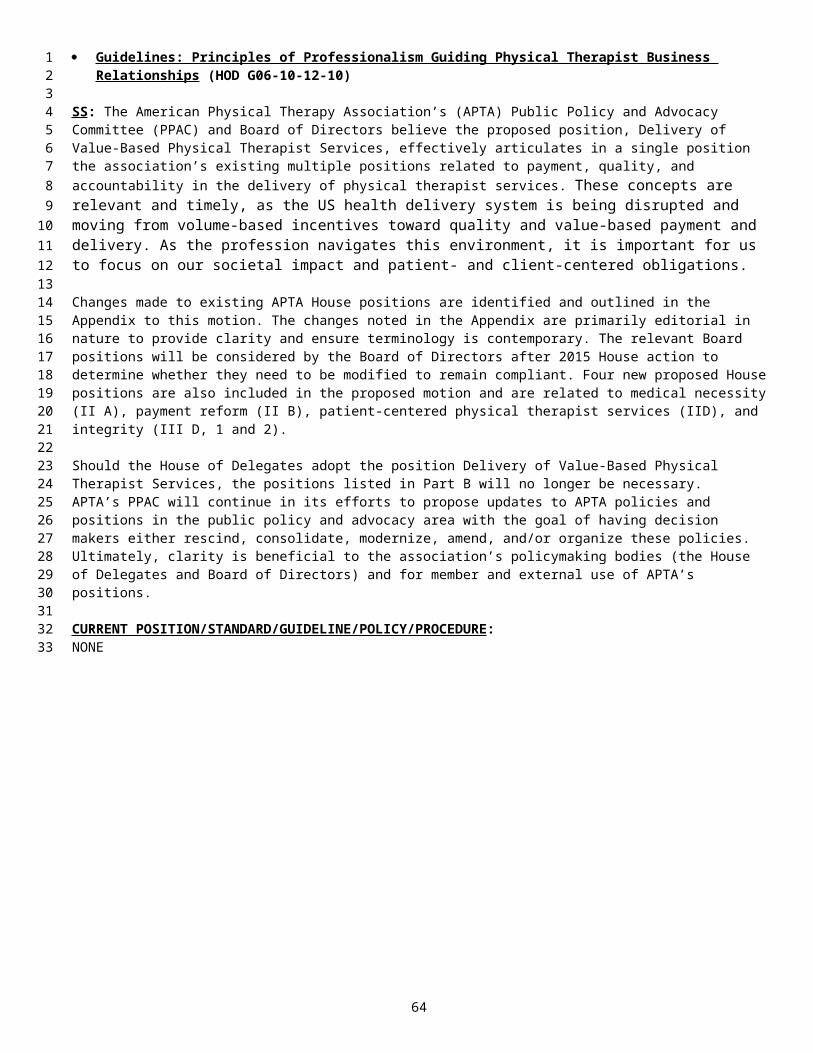

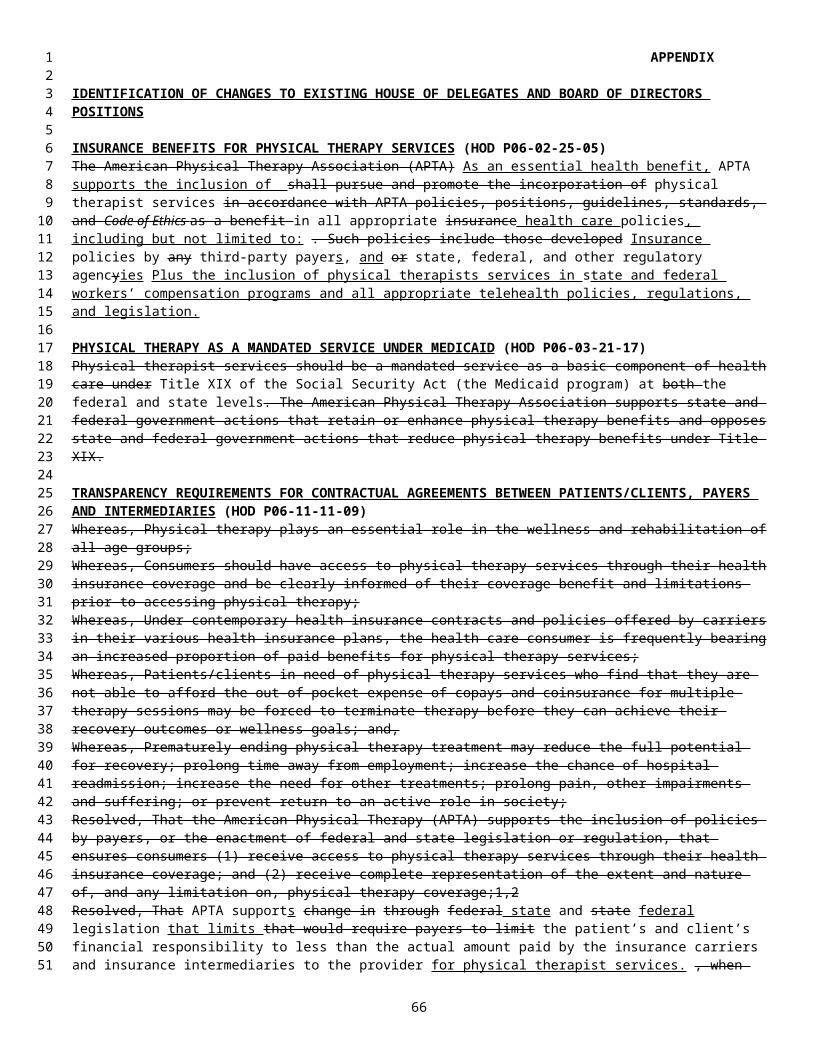












![[Tentative Vacancy Position of all grades of ISS as …mospi.nic.in/sites/default/files/main_menu/iss/VP as on...[Tentative Vacancy Position of all grades of ISS as on 01.02.2020]](https://static.documents.pub/doc/80x56/5ea9d0895909f65ecf4902d6/tentative-vacancy-position-of-all-grades-of-iss-as-mospinicinsitesdefaultfilesmainmenuissvp.jpg)
![[Tentative Vacancy Position of all grades of ISS as on 01.04.2020]mospi.nic.in/sites/default/files/main_menu/iss/ISS_VP_as... · 2020. 4. 15. · [Tentative Vacancy Position of all](https://static.documents.pub/doc/80x56/5fe849f91d772a666276dd1e/tentative-vacancy-position-of-all-grades-of-iss-as-on-01042020mospinicinsitesdefaultfilesmainmenuississvpas.jpg)


![[Tentative Vacancy Position of all grades of ISS as …mospi.nic.in/sites/default/files/main_menu/iss/VP.pdf[Tentative Vacancy Position of all grades of ISS as on 01.09.2019] S. No.](https://static.documents.pub/doc/80x56/5ea9d0895909f65ecf4902d7/tentative-vacancy-position-of-all-grades-of-iss-as-mospinicinsitesdefaultfilesmainmenuissvppdf.jpg)








