Central Medical Journal of Obstetrics and Gynecology
Cite this article: Ahmed SM, Moukaddam N, Worley AV, Patel KR, Shah A, et al. (2016) Teratogenic Potential of Commonly Prescribed Psychotropic Drugs. Med J Obstet Gynecol 4(4): 1091.
*Corresponding authorsVeronica Tucci, Section of Emergency Medicine, Baylor College of Medicine; Ben Taub General Hospital, 1504 Taub Loop, Houston, Texas 77030, USA, Email:
Teratogenic Potential of Commonly Prescribed Psychotropic DrugsSyed Moiz Ahmed1, Nidal Moukaddam2, Ameigh V. Worley3, Krupa R. Patel4, Asim Shah2, and Veronica Tucci5*1Emergency and Accident Centre, Pakistan Institute of Medical Sciences, Pakistan2Menninger Department of Psychiatry and Behavioral Sciences, Baylor College of Medicine, USA3Department of Obstetrics and Gynecology, Wake Forest University, USA4Department of Pharmacy, Ben Taub General Hospital, USA5Section of Emergency Medicine, Baylor College of Medicine, USA
ABBREVIATIONSTID: Three Times a Day; SSRIS: Selective Serotonin Reuptake
Inhibitors; FDA: Food and Drug Administration; TCAS: Tricyclic Antidepressants; OR: Odds Ratio; CI: Confidence Interval; ACOG: American College of Obstetrics and Gynecology; NTDs: Neural Tube Defects; CNS: Central Nervous System
INTRODUCTIONIncreased morbidity has been reported from psychiatric
illnesses during the pregnant state in women [1], with prevalence ranging from 15-29% [2-14]. To prevent any untoward effects of these conditions on both pregnancy outcomes and the developing fetus, there has been increased use of psychotropic medications during pregnancy. It is estimated that about 3.5% of all women in the Western world use psychotropic medication during pregnancy [15]. This has raised concerns about the teratogenic effects of these drugs, and the dilemmas that the physicians face in weighing the risk between adverse effects from untreated psychiatric illness and the adverse effects resulting from the use of psychotropic medications in a pregnant patient. In this case report, we will present a case in which congenital malformation in the fetus is suspected due to the possible use of psychotropic drugs, and discuss the current literature supporting
the teratogenic potential of commonly prescribed psychotropic medications.
CASE PRESENTATIONA 21 year old Hispanic female G1P0A0L0, presented to her
obstetrician at 20 weeks of gestation for a well pregnancy check. She has poor social support, and this was her first prenatal checkup. During a detailed history she mentions that she had been diagnosed with bipolar disorder and severe anxiety and has been on Valproic acid 1000 mg at bedtime and Clonazepam 1 mg TID. The obstetrician performed an anomaly scan and found that the fetus has cleft lip and palate. The patient has no family history of congenital malformations, and she regularly took folic acid supplementation throughout her pregnancy. She does not use any drugs of abuse. The obstetrician believes that the congenital malformation is as a result of her prescription medications. The patient is informed of the congenital anomaly and the most probable cause for it. She has been referred to a psychiatrist for counselling.
DISCUSSIONThis scenario is a perfect example of what obstetricians
have to face on a regular basis. Most of the teratogenic damage done by drugs is typically during the first trimester during
Abstract
Increasing use of psychotropic medications during pregnancy has highlighted the issue of teratogenic risks associated with these drugs. No drug has been deemed completely safe for use during pregnancy by the FDA as all of them have been shown to cross the placenta; however research has shown that different psychotropic drugs contribute variably towards the development of major congenital malformations in the fetus. Most of this risk is associated with the use of these drugs during the first trimester. In this case report we present a female patient whose fetus developed cleft lip and palate possibly due to the use of prescription medications for her psychiatric illness, and then review the literature regarding the teratogenic potential of the commonly prescribed psychotropic medications during pregnancy.
Central
Tucci et al. (2016)Email:
Med J Obstet Gynecol 4(4): 1091 (2016) 2/9
which organogenesis is taking place. So if a woman is already taking such medications at the time of conception, by the time pregnancy is confirmed, most or all of the organ development has already taken place, thereby increasing the risks of congenital malformations. Here we will first discuss the teratogenic potential of the commonly prescribed psychotropic drugs (Table 1) and then in light of that literature review the present case.
Traditionally, the Food and Drug Administration (FDA) placed medications into five categories based on their potential for causing birth defects (Table 2) [16]. More recently in 2014, however, the FDA determined that the five category classification system was too simplistic and abolished it under the Pregnancy and Lactation Labeling Final Rule (PLLR). The PLLR established labeling requirements for the pregnancy and lactation sections for prescription drugs and biological agents and utilizes descriptive subsections for pregnancy exposure and risk, lactation, and effects to reproductive potential for females and males [17]. Labeling changes from this rule begin on June 30, 2015 [18]. Manufacturers with drugs approved before June 30, 2001 are required to remove the pregnancy category within 3 years of the effective date of the final rule.We provide examples of the new labeling requirements with respect to pregnancy and lactation in Boxes 1 and 2. Nuplazid is a medication recently approved by the FDA for Parkinson’s induced psychosis, whereas Aristada is an atypical antipsychotic indicated for schizophrenia.
Antidepressants are a class of psychotropic drugs which have been studied most extensively for their teratogenic potential. Selective serotonin reuptake inhibitors (SSRIs) are usually the first line antidepressants used in pregnancy because studies show that, with the exception of paroxetine, most SSRIs are not associated with an increased risk of congenital malformations [19-29]. Paroxetine, on the other hand, has been shown to cause cardiac anomalies, especially atrial and ventricular septal defects [28,30-32]. In one meta-analysis comparing almost 2.3 million controls with around 4000 neonates exposed to paroxetine in utero, showed a significantly increased risk of cardiac malformations with an odds ratio of 1.5 (95% CI: 1.1-1.9) [33]. Another meta-analysis comparing 1.6 million controls with 18,000 exposed neonates revealed similar results (RR 1.4, 95% CI: 1.1-1.9) [34]. Therefore, while all SSRIs are classified as category C by FDA, paroxetine is classified as category D. Some recent evidence also indicates that fluoxetine might be associated with an increased risk of congenital malformations and cardiac defects [27], however the results are inconclusive. In light of the evidence, among SSRIs, sertraline and citalopram are usually the first line agents, as they have little or no teratogenic potential and safe for use during lactation as well [19]. Escitalopram and fluvoxamine are relatively studied less for their effects during pregnancy and are thus not prescribed routinely.
With regards to tricyclic antidepressants (TCAs), most
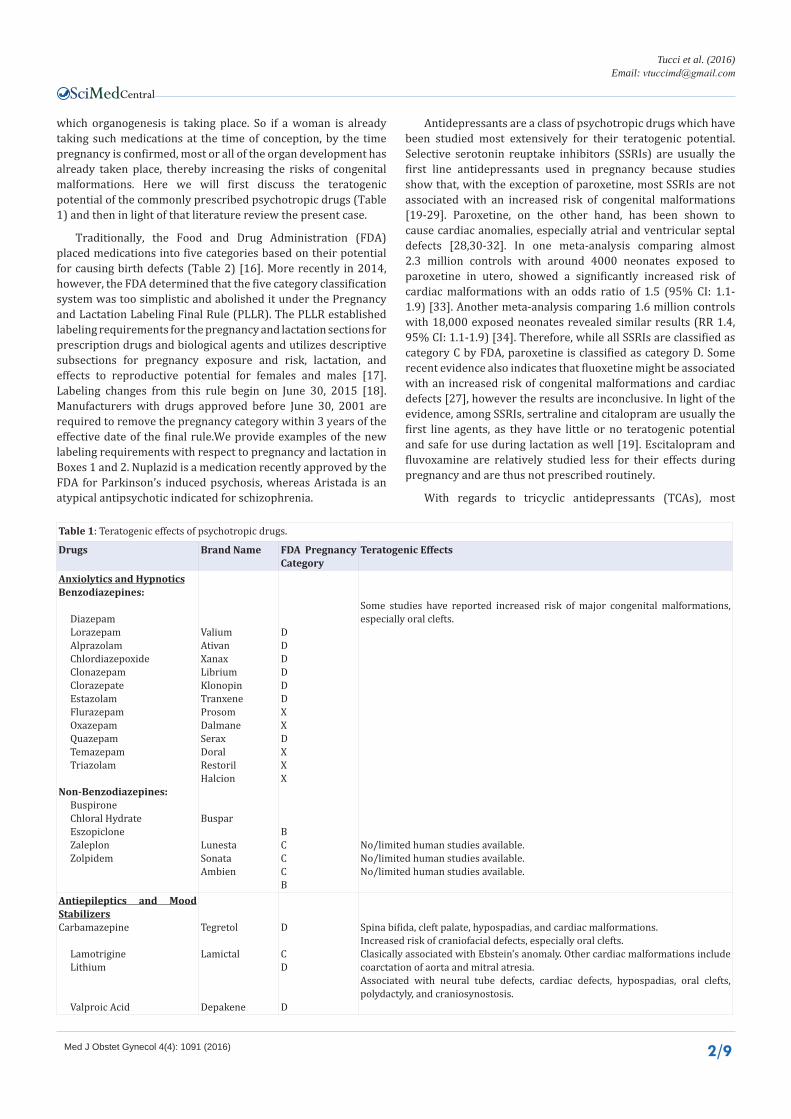
Table 1: Teratogenic effects of psychotropic drugs.
Some studies have reported increased risk of major congenital malformations, especially oral clefts.
No/limited human studies available.No/limited human studies available.No/limited human studies available.
Antiepileptics and Mood StabilizersCarbamazepine
Lamotrigine Lithium
Valproic Acid
Tegretol
Lamictal
Depakene
D
CD
D
Spina bifida, cleft palate, hypospadias, and cardiac malformations.Increased risk of craniofacial defects, especially oral clefts.Clasically associated with Ebstein’s anomaly. Other cardiac malformations include coarctation of aorta and mitral atresia. Associated with neural tube defects, cardiac defects, hypospadias, oral clefts, polydactyly, and craniosynostosis.
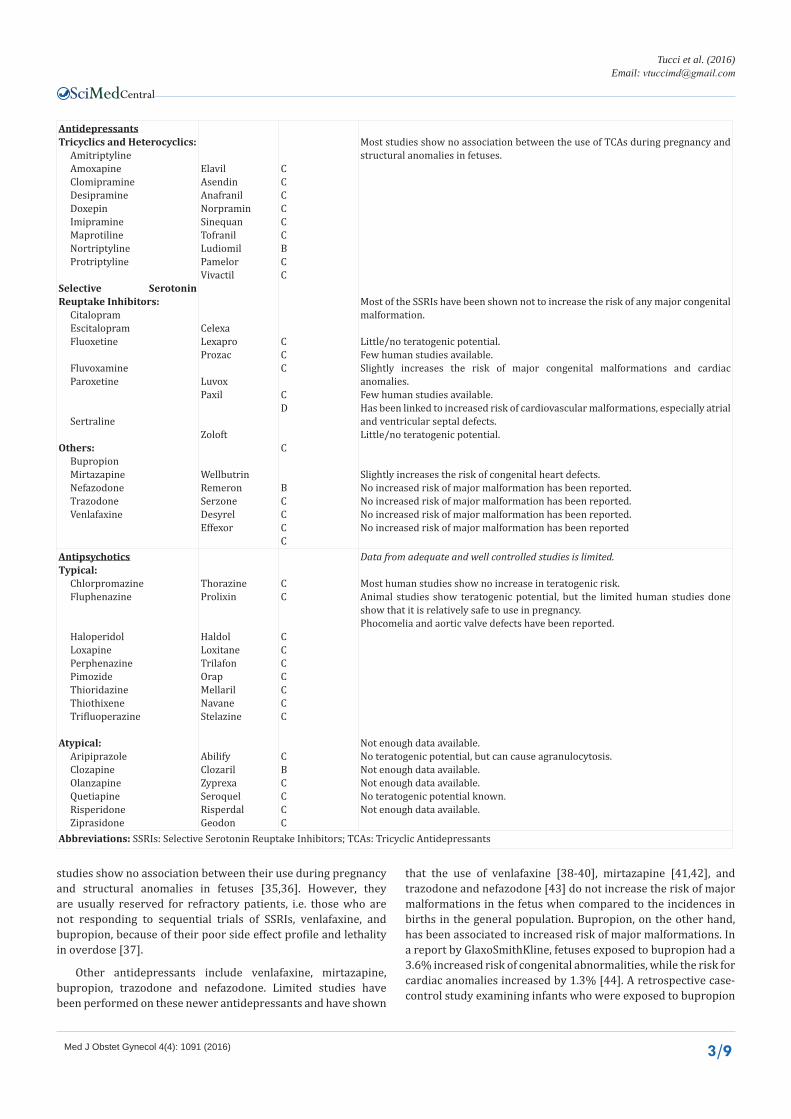
Most studies show no association between the use of TCAs during pregnancy and structural anomalies in fetuses.
Most of the SSRIs have been shown not to increase the risk of any major congenital malformation.
Little/no teratogenic potential.Few human studies available.Slightly increases the risk of major congenital malformations and cardiac anomalies.Few human studies available.Has been linked to increased risk of cardiovascular malformations, especially atrial and ventricular septal defects. Little/no teratogenic potential.
Slightly increases the risk of congenital heart defects.No increased risk of major malformation has been reported.No increased risk of major malformation has been reported.No increased risk of major malformation has been reported.No increased risk of major malformation has been reported
Data from adequate and well controlled studies is limited.
Most human studies show no increase in teratogenic risk.Animal studies show teratogenic potential, but the limited human studies done show that it is relatively safe to use in pregnancy.Phocomelia and aortic valve defects have been reported.
Not enough data available.No teratogenic potential, but can cause agranulocytosis.Not enough data available.Not enough data available.No teratogenic potential known.Not enough data available.
studies show no association between their use during pregnancy and structural anomalies in fetuses [35,36]. However, they are usually reserved for refractory patients, i.e. those who are not responding to sequential trials of SSRIs, venlafaxine, and bupropion, because of their poor side effect profile and lethality in overdose [37].
Other antidepressants include venlafaxine, mirtazapine, bupropion, trazodone and nefazodone. Limited studies have been performed on these newer antidepressants and have shown
that the use of venlafaxine [38-40], mirtazapine [41,42], and trazodone and nefazodone [43] do not increase the risk of major malformations in the fetus when compared to the incidences in births in the general population. Bupropion, on the other hand, has been associated to increased risk of major malformations. In a report by GlaxoSmithKline, fetuses exposed to bupropion had a 3.6% increased risk of congenital abnormalities, while the risk for cardiac anomalies increased by 1.3% [44]. A retrospective case-control study examining infants who were exposed to bupropion
Central
Tucci et al. (2016)Email:
Med J Obstet Gynecol 4(4): 1091 (2016) 4/9
Table 2: FDA Classifications of Medication.
Category Definition Examples
AAdequate and well-controlled studies have failed to demonstrate a risk to the fetus in the first trimester of pregnancy (and there is no evidence of risk in later trimesters).
Folic Acid
B Animal reproduction studies have failed to demonstrate a risk to the fetus and there are no adequate and well-controlled studies in pregnant women. Clozapine, Buproprion
CAnimal reproduction studies have shown an adverse effect on the fetus and there are no adequate and well-controlled studies in humans, but potential benefits may warrant use of the drug in pregnant women despite potential risks.
Haloperidol, Fluoxetine
DThere is positive evidence of human fetal risk based on adverse reaction data from investigational or marketing experience or studies in humans, but potential benefits may warrant use of the drug in pregnant women despite potential risks.
Carbamezapine, Lithium, Valproic Acid for mood disorder
X
Studies in animals or humans have demonstrated fetal abnormalities and/or there is positive evidence of human fetal risk based on adverse reaction data from investigational or marketing experience, and the risks involved in use of the drug in pregnant women clearly outweigh potential benefits.
Temazepam, Valproic Acid for migraine use changed to X
N Not classified by the FDA Aspirin
According to CDC about 37% of births in the US are the result of unintended pregnancies, a number which has stayed fairly
steady since 1982
Since the number is very high, it is recommended that all prescribers who see psychiatric patients or patients on
psychiatric medications of reproductive age, should educate them about the risks associated with some psychiatric
medications
Patients who are planning to be pregnant need to be educated about psychiatric medications which can adversely affect the
fetus, namely valproic acid, carbamazepine, lithium, paroxetine and benzodiazepines
Since the teratogenic effects are most prevalent in the first trimester, it is much better to educate patients before they get pregnant, as otherwise by the time they see a physician it may
be too late to avoid potential damage
Psychiatric illnesses usually get worse during pregnancy, therefore it is not recommended to stop psychiatric medications
during pregnancy without checking with the prescriber
Patients also need to be educated about potential issues with breastfeeding, as they need to choose a medication which is
both safe in pregnancy and after delivery
Figure 1 Psycho-education Pearls for Patients of Reproductive Age.
from 1 month prior to conception to 3 months post-conception showed increased risk of left outflow tract heart defects, with an odds ratio of 2.6 (95% CI: 1.2-5.7) [45]. In a recent review by Byatt et al, the authors pointed out that in utero bupropion exposure does increase the risk of congenital heart defects, however this increase is small (2.1/1000) when compared to the births in general population (0.82/1000) [46].
Coming to anxiolytics and hypnotics, the literature on the teratogenic effects of Benzodiazepines is ambiguous [47]. In a meta-analysis of 23 studies, looking only at the cohort studies from the group showed no association between in utero benzodiazepine exposure and increased risk of major congenital
malformations or oral clefts. While segregating the case-control studies from the same group revealed an association between benzodiazepine use in pregnancy and the development of major malformations (OR 3.01; 95% CI: 1.32-6.84) and even oral clefts alone (OR 1.79; 95% CI: 1.13-2.82) [48]. Two studies using the data from Swedish Birth Registry report conflicting outcomes. One [49] reports that in utero exposure to benzodiazepines during first trimester increases the risk of major malformations with an odds ratio of 1.79 (95% CI: 1.00-1.55), while the other [50] finds no association whatsoever. Another recent study by Ban et al found no significant teratogenic potential of benzodiazepine use in first trimester [51]. Even in studies which report an increase in
Central
Tucci et al. (2016)Email:
Med J Obstet Gynecol 4(4): 1091 (2016) 5/9
Pregnancy
Risk Summary
‘There are no data on NUPLAZID use in pregnant women that would allow assessment of the drug-associated risk of major congenital malformations or miscarriage. In animal reproduction studies, no adverse developmental effects were seen when Pimavanserin was administered orally to rats or rabbits during the period of organogenesis at doses up to 10- or 12-times the maximum recommended human dose (MRHD) of 34 mg/day, respectively. Administration of Pimavanserin to pregnant rats during pregnancy and lactation resulted in maternal toxicity and lower pup survival and body weight at doses which are 2-times the MRHD of 34 mg/day [see Data].
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.’
Data
Animal Studies
‘Pimavanserin was not teratogenic in pregnant rats when administered during the period of organogenesis at oral doses of 0.9, 8.5, and 51 mg/kg/day, which are 0.2- and 10-times the maximum recommended human dose (MRHD) of 34 mg/day based on AUC at mid and high doses, respectively. Maternal toxicity included reduction in body weight and food consumption at the highest dose.Administration of Pimavanserin to pregnant rats during pregnancy and lactation at oral doses of 8.5, 26, and 51 mg/kg/day, which are 0.14- to 14-times the MRHD of 34 mg/day based on AUC, caused maternal toxicity, including mortality, clinical signs including dehydration, hunched posture, and rales, and decreases in body weight, and/or food consumption at doses ≥26 mg/kg/day (2 -times the MRHD based on AUC). At these maternally toxic doses there was a decrease in pup survival, reduced litter size, and reduced pup weights, and food consumption. Pimavanserin had no effect on sexual maturation, neurobehavioral function including learning and memory, or reproductive function in the first generation pups up to 14-times the MHRD of 34 mg/day based on AUC.Pimavanserin was not teratogenic in pregnant rabbits during the period of organogenesis at oral doses of 4.3, 43, and 85 mg/kg/day, which are 0.2- to 12-times the MHRD of 34 mg/day based on AUC. Maternal toxicity, including mortality, clinical signs of dyspnea and rales, decreases in body weight and/or food consumption, and abortions occurred at doses 12-times the MRHD of 34 mg/day based on AUC.’
Lactation
Risk Summary
Box 1 Risks of using Pimavanserin (Nuplazid) in Special Populations.
teratogenic risk, the absolute value is small. The risk of oral clefts in the general population is 6 per 10,000 births, while the use of benzodiazepines during pregnancy increases this risk up to 7 per 10,000 births [36] to 11 per 10,000 births [51]. Therefore, benzodiazepines should be avoided in pregnancy especially during the first and the last trimester, especially those drugs in the group which belong to category X in pregnancy [53].
With regards to non-benzodiazepine hypnotics limited human studies are available to assess the true teratogenic risks of these drugs. Buspirone is categorized as class B by FDA, based on animal studies which show no evidence of fetal damage [54]. Same is the case with Zolpidem, which is classified as category B by FDA, because of lack of teratogenic risks shown in animal models [55]. Zaleplon, eszopiclone, and chloral hydrate belong to category C. Animal studies regarding zaleplon and eszopiclone show no teratogenic potential [56,57], while no animal studies
with regards to chloral hydrate have been reported [58]. Therefore, these drugs should only be used during pregnancy if need is clearly established.
In the group of anti-epileptics and mood stabilizers, the drugs commonly prescribed during pregnancy are carbamazepine, lamotrigine, lithium, and valproate. Lithium, for decades, has been classically associated with Ebstein’s anomaly (i.e. the malformation of tricuspid valve and the right ventricle). Lithium is only expected to carry a teratogenic potential if taken before 12 weeks of gestation, as the heart is fully formed by then, and thus any exposure to the fetus thereafter could not affect the structure of the heart. It has been shown to increase the risk ratio of cardiac malformations to 1.2-7.7, and the risk ratio for all congenital defects to 1.5-3 [59,60]. The prevalence of Ebstein’s anomaly in the general population is 1 per 20,000 live births [61], which jumps up to 1 per 1000 live births with first trimester lithium
Central
Tucci et al. (2016)Email:
Med J Obstet Gynecol 4(4): 1091 (2016) 6/9
exposure [62]. Other reported cardiac defects are coarctation of aorta and mitral atresia. American College of Obstetrics and Gynecology (ACOG) [59] recommends that females with bipolar disorder who are currently on lithium and wish to conceive, should gradually taper dose of the drug if the episodes are mild and infrequent. In patients who suffer from moderate-severe episodes and have a mild risk of relapse in short-term, it is recommended that the drug should be tapered but should be restarted once organogenesis is complete. For those women who suffer from severe and frequent manic episodes, lithium should be continued throughout pregnancy irrespective of the risk it poses to the developing fetus. Briggs et al suggests that in cases where continuation of the drug is necessary, adequate screening tests should be performed such as level II ultrasound and fetal echocardiography [63].
Sodium valproate is a well-established teratogen with evidence from both animal and human studies. When compared to exposure to other anti-epileptics, valproate exposure increases the risk of congenital malformations four folds [64]. However, it increases the risk of major malformations by almost 9% when compared to groups not exposed to any anti-epileptics [65]. In utero exposure to valproate has been associated with increased risk of neural tube defects (NTDs), cardiac defects, hypospadias, oral clefts, polydactyly, and craniosynostosis [46,64]. About 1-2% of the fetuses exposed to valproate in utero develop NTDs, which is 10-20 folds increased risk when compared to births in the general population [66,67]. Folic acid supplementation decreases the risk of NTDs among births in the general population, and so is recommended in pregnant females on valproate, even though studies have shown no decrease in the risk of NTDs in pregnant females who are on anti-epileptics and take folic acid supplementation [68]. This is probably due to the fact that folate supplementation has only shown some value if the dose of valproate is less than 750mg, however the dose that is generally prescribed is between 1500-2000mg. A distinct pattern of facial dysmorphism along with a characteristic constellation of defects is also described in some fetuses exposed to valproate in utero, which includes craniofacial, skeletal, urogenital, and cardiovascular defects along with stunted development [63]. Therefore, it is recommended that sodium valproate should be avoided during pregnancy, especially the first trimester, but in cases where females are already on the drug, it should not be discontinued due to risk of relapse. Rather it should be substituted by another less teratogenic mood stabilizer such as an atypical antipsychotic [53].
Carbamazepine has a similar teratogenic profile as valproate, but less in severity. In utero exposure to the drug has been shown to increase the risk of NTDs (especially spina bifida), cleft palate, hypospadias, and cardiac malformations [69]. Up to 1% of the exposed fetuses develop spina bifida, which means an approximately 7 fold increased risk when compared to births in the general population [70]. Some studies have also described a ‘Fetal Carbamazepine Syndrome’ characterized by facial dysmorphism, finger nail hypoplasia, and developmental delays, however the existence of this syndrome remains to be a controversy [59,63]. Recommendations regarding carbamazepine use during pregnancy are the same as for sodium valproate.
There have been fewer studies assessing the safety of Lamotrigine use during pregnancy, but from what limited data is available, it is clear that the risk of major congenital malformations is less when compared to valproate exposure [71]. In utero exposure to lamotrigine has been shown to increase the risk of craniofacial defects. Holmes et al showed that lamotrigine use during pregnancy increased the risk of oral clefts by 10.4 folds (95% CI 4.3-24.9) when compared with control groups [72].
Among antipsychotics, the ones that are commonly prescribed are chlorpromazine, haloperidol, fluphenazine, clozapine, risperidone, quetiapine, olanzapine, ziprasidone, and aripiprazole. Although adequate and well controlled studies have not been performed in case of most of these drugs, but animal studies show teratogenic potential in most of them.
Chlorpromazine has been shown to cause congenital malformations in animal studies, including those involving the skeletal system, central nervous system (CNS), eye, and cleft palate [73-75]. A few human studies show an increased incidence of malformations and perinatal deaths in fetuses exposed to chlorpromazine in utero [76-78], whereas most fail to elucidate any such association [79-83]. In summary, most evidence suggests that chlorpromazine is not teratogenic, but still it should be used cautiously during pregnancy, by weighing the risks and benefits of the drug.
In animal studies regarding fluphenazine, two studies showed no teratogenic adverse effects in pregnancy [84]. However, in other studies it has been reported that exposure to the drug results in dilated ventricles of the CNS, skeletal defects, oral clefts, and reduction in fetal weight and length [85,86]. In humans, no well controlled studies have been performed to test the teratogenic potential of the drug, however they are considered relatively safe to use during pregnancy [87,88].
Haloperidol use in animal reproductive studies has been linked to increased risk of cleft palate, micromelia [86,89], and CNS and skeletal malformations [86,90-92]. Among human studies, Kopelman et al. [93], reported multiple upper and lower limb defects, and an aortic valve defect in one infant, and similarly phocomelia was reported in another infant who was exposed to haloperidol during first trimester [94]. However, limb reduction defects have not been reported with haloperidol use outside of the first trimester.
With regards to clozapine, animal studies have shown no teratogenic effects, and the human studies also deem the drug safe for use during pregnancy [95-97]. Despite the lack of teratogenic potential, clozapine can cause fetal agranulocytosis and should only be reserved for patients with severe schizophrenia who fail to respond to other neuroleptic drugs.
Risperidone use has also failed to show any teratogenic effects in both animal and human studies [98,99]. No adequate and well controlled studies have been performed to assess the safety of Quetiapine, and so it should be used with caution [100]. Same is the case with Olanzapine [101,102], Ziprasidone, and Aripiprazole [101-103].
With respect to the current case, it is difficult to establish which medication was the culprit or offending agent and had the
Central
Tucci et al. (2016)Email:
Med J Obstet Gynecol 4(4): 1091 (2016) 7/9
teratogenic effect on the fetus’ development. As noted previously, our patient was taking both valproic acid and clonazepam at the time she presented for her first prenatal evaluation. Indeed, many women of childbearing age suffer from anxiety and unipolar or bipolar depression and therefore, take multiple psychiatric medications including mood stabilizers and anxiolytics. It is imperative that family practitioners, internists, gynecologists and psychiatrists cautiously prescribe category D drug in women of reproductive age and when such medications are warranted to counsel and warn patients. We also recommend that physicians document all the potential side effects prior to prescribing such medications to minimize the chances of adverse effects as well as any litigations resulting from an unplanned pregnancy with birth defects.
REFERENCES1. Cox JL. Psychiatric morbidity and pregnancy: a controlled study of 263
2. Kelly RH, Russo J, Katon W. Somatic complaints among pregnant women cared for in obstetrics: normal pregnancy or depressive and anxiety symptom amplification revisited? Gen Hosp Psychiatry. 2001; 23: 107-113.
3. Kelly RH, Danielsen BH, Golding JM, Anders TF, Gilbert WM, Zatzick DF. Adequacy of prenatal care among women with psychiatric diagnoses giving birth in California in 1994 and 1995. Psychiatr Serv. 1999; 50: 1584-1590.
4. Kelly RH, Danielson BH, Zatzick DF, Haan MN, Anders TF, Gilbert WM, et al. Chart-recorded psychiatric diagnoses in women giving birth in California in 1992. Am J Psychiatry. 1999; 156: 955-957.
5. Kim HG, Mandell M, Crandall C, Kuskowski MA, Dieperink B, Buchberger RL. Antenatal psychiatric illness and adequacy of prenatal care in an ethnically diverse inner-city obstetric population. Arch Womens Ment Health. 2006; 9: 103-107.
6. Kelly RH, Russo J, Holt VL, Danielsen BH, Zatzick DF, Walker E, et al. Psychiatric and substance use disorders as risk factors for low birth weight and preterm delivery. Obstet Gynecol. 2002; 100: 297-304.
7. Andersson L, Sundström-Poromaa I, Bixo M, Wulff M, Bondestam K, åStröm M. Point prevalence of psychiatric disorders during the second trimester of pregnancy: a population-based study. Am J Obstet Gynecol. 2003; 189: 148-54.
8. Andersson L, Sundström-Poromaa I, Wulff M, Aström M, Bixo M. Depression and anxiety during pregnancy and six months postpartum: a follow-up study. Acta Obstet Gynecol Scand. 2006; 85: 937-944.
9. Battle CL, Zlotnick C, Miller IW, Pearlstein T, Howard M. Clinical characteristics of perinatal psychiatric patients: a chart review study. J Nerv Ment Dis. 2006; 194: 369-377.
10. Howard M, Battle CL, Pearlstein T, Rosene-Montella K. A psychiatric mother-baby day hospital for pregnant and postpartum women. Arch Womens Ment Health. 2006; 9: 213-218.
11. van Bussel JC, Spitz B, Demyttenaere K. Women’s mental health before, during, and after pregnancy: a population-based controlled cohort study. Birth. 2006; 33: 297-302.
12. Faisal-Cury A, Rossi Menezes P. Prevalence of anxiety and depression during pregnancy in a private setting sample. Arch Womens Ment Health. 2007; 10: 25-32.
13. Kelly R, Zatzick D, Anders T. The detection and treatment of psychiatric disorders and substance use among pregnant women cared for in obstetrics. Am J Psychiatry. 2001; 158: 213-219.
14. Adewuya AO, Ola BA, Aloba OO, Mapayi BM. Anxiety disorders among Nigerian women in late pregnancy: a controlled study. Arch Womens Ment Health. 2006; 9: 325-328.
15. Bellantuono C, Migliarese G, Gentile S. Serotonin reuptake inhibitors in pregnancy and the risk of major malformations: a systematic review. Hum Psychopharmacol. 2007; 22: 121-128.
16. Ramoz LL, Patel-Shori NM. Recent changes in pregnancy and lactation labeling: retirement of risk categories. Pharmacotherapy. 2014; 34: 389-395.
17. Mosley JF 2nd, Smith LL, Dezan MD. An overview of upcoming changes in pregnancy and lactation labeling information. Pharm Pract (Granada). 2015; 605.
18. Lal R. Drugs in pregnancy and lactation: improved benefit-risk information. FDA/CDER SBIA Chronicles. 2015.
19. Byatt N, Deligiannidis KM, Freeman MP. Antidepressant use in pregnancy: a critical review focused on risks and controversies. Acta Psychiatr Scand. 2013; 127: 94-114.
20. Reis M, Källén B. Delivery outcome after maternal use of antidepressant drugs in pregnancy: an update using Swedish data. Psychol Med. 2010; 40: 1723-1733.
22. Källén BA, Otterblad Olausson P. Maternal use of selective serotonin re-uptake inhibitors in early pregnancy and infant congenital malformations. Birth Defects Res A Clin Mol Teratol. 2007; 79: 301-308.
23. Louik C, Lin AE, Werler MM, Hernández-Díaz S, Mitchell AA. First-trimester use of selective serotonin-reuptake inhibitors and the risk of birth defects. N Engl J Med. 2007; 356: 2675-2683.
24. Alwan S, Reefhuis J, Rasmussen SA, Olney RS, Friedman JM; National Birth Defects Prevention Study. Use of selective serotonin-reuptake inhibitors in pregnancy and the risk of birth defects. N Engl J Med. 2007; 356: 2684-2692.
25. Huybrechts KF, Hernández-Díaz S, Avorn J. Antidepressant use in pregnancy and the risk of cardiac defects. N Engl J Med. 2014; 371: 1168-1169.
26. Nordeng H, van Gelder MM, Spigset O, Koren G, Einarson A, Eberhard-Gran M. Pregnancy outcome after exposure to antidepressants and the role of maternal depression: results from the Norwegian Mother and Child Cohort Study. J Clin Psychopharmacol. 2012; 32: 186-194.
27. Furu K, Kieler H, Haglund B, Engeland A, Selmer R, Stephansson O, et al. Selective serotonin reuptake inhibitors and venlafaxine in early pregnancy and risk of birth defects: population based cohort study and sibling design. BMJ. 2015; 350: 1798.
28. Reefhuis J, Devine O, Friedman JM, Louik C, Honein MA; National Birth Defects Prevention Study. Specific SSRIs and birth defects: Bayesian analysis to interpret new data in the context of previous reports. BMJ. 2015; 351: 3190.
29. Ban L, Gibson JE, West J, Fiaschi L, Sokal R, Smeeth L, et al. Maternal depression, antidepressant prescriptions, and congenital anomaly risk in offspring: a population-based cohort study. BJOG. 2014; 121: 1471-1481.
30. Greene MF. Teratogenicity of SSRIs--serious concern or much ado about little? N Engl J Med. 2007; 356: 2732-2733.
31. Malm H, Artama M, Gissler M, Ritvanen A. Selective serotonin reuptake inhibitors and risk for major congenital anomalies. Obstet Gynecol. 2011; 118: 111-120.
32. Pedersen LH, Henriksen TB, Vestergaard M, Olsen J, Bech BD. Selective serotonin reuptake inhibitors in pregnancy and congenital malformations: population based cohort study. BMJ. 2009; 339: 3569.
33. EditorsNational Collaborating Centre for Mental Health (UK). Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance: Updated edition
34. Grigoriadis S, VonderPorten EH, Mamisashvili L, Roerecke M, Rehm J, Dennis CL, et al. Antidepressant exposure during pregnancy and congenital malformations: is there an association? A systematic review and meta-analysis of the best evidence. J Clin Psychiatry. 2013; 74: 293-308.
35. Simon GE, Cunningham ML, Davis RL. Outcomes of prenatal antidepressant exposure. Am J Psychiatry. 2002; 159: 2055-2061.
36. Altshuler LL, Cohen L, Szuba MP, Burt VK, Gitlin M, Mintz J. Pharmacologic management of psychiatric illness during pregnancy: dilemmas and guidelines. Am J Psychiatry. 1996; 153: 592-606.
37. Yonkers K, Wisner K, Stewart D, Oberlander TF, Dell DL, Stotland N, et al. The management of depression during pregnancy: a report from the American Psychiatric Association and the American College of Obstetricians and Gynecologists. Gen Hosp Psychiatry. 2009; 31: 403-413.
38. Einarson A, Fatoye B, Sarkar M, Lavigne SV, Brochu J, Chambers C, et al. Pregnancy outcome following gestational exposure to venlafaxine: A multicenter prospective controlled study. Am J Psychiatry. 2001; 158:1728-1730.
39. Einarson A, Choi J, Einarson TR, Koren G. Incidence of major malformations in infants following antidepressant exposure in pregnancy: Results of a large prospective cohort study. Can J Psychiatry. 2009; 54: 242-246.
40. Yaris F, Kadioglu M, Kesim M, Ulku C, Yaris E, Kalyoncu NI, et al. Newer antidepressants in pregnancy: prospective outcome of a case series. Reprod Toxicol. 2004; 19: 235-238.
41. Saks BR. Mirtazapine: Treatment of depression, anxiety, and hyperemesis gravidarum in the pregnant patient: A report of 7 cases. Arch Womens Ment Health. 2001; 4: 165-170.
42. Djulus J, Koren G, Einarson TR, Wilton L, Shakir S, Diav-Citrin O, et al. Exposure to mirtazapine during pregnancy: a prospective, comparative study of birth outcomes. J Clin Psychiatry. 2006; 67: 1280-1284.
43. Einarson A, Bonari L, Voyer-Lavigne S, Addis A, Matsui D, Johnson Y, et al. A multicentre prospective controlled study to determine the safety of trazodone and nefazodone use during pregnancy. Can J Psychiatry. 2003; 48: 106-110.
44. Glaxosmithkline. The Bupropion Pregnancy Registry Final Report. 2008.
45. Cole JA, Modell JG, Haight BR, Cosmatos IS, Stoler JM, Walker AM. Bupropion in pregnancy and the prevalence of congenital malformations. Pharmacoepidemiol Drug Saf. 2007; 16: 474-484.
46. Jentink J, Loane MA, Dolk H, Barisic I, Garne E, Morris JK, et al. Valproic acid monotherapy in pregnancy and major congenital malformations. N Engl J Med. 2010; 362: 2185-2193.
47. Hendrick V. Bipolar Disorder in Adults: Teratogenic and Postnatal Risks of Pharmacotherapy. In: Keck P, ed. Waltham, MA: UpToDate; 2014.
48. Dolovich LR, Addis A, Vaillancourt JM, Power JD, Koren G, Einarson TR. Benzodiazepine use in pregnancy and major malformations or oral cleft: meta-analysis of cohort and case-control studies. BMJ. 1998; 317: 839-843.
49. Wikner BN, Stiller CO, Bergman U, Asker C, Källén B. Use of benzodiazepines and benzodiazepine receptor agonists during pregnancy: neonatal outcome and congenital malformations. Pharmacoepidemiol Drug Saf. 2007; 16: 1203-1210.
50. Wikner BN, Källén B. Are hypnotic benzodiazepine receptor agonists teratogenic in humans? J Clin Psychopharmacol. 2011; 31: 356-359.
51. Ban L, West J, Gibson JE, Fiaschi L, Sokal R, Doyle P, et al. First trimester exposure to anxiolytic and hypnotic drugs and the risks of major congenital anomalies: a United Kingdom population-based cohort study. PLoS One. 2014; 9: 100996.
52. Yonkers KA, Wisner KL, Stowe Z, Leibenluft E, Cohen L, Miller L, et al. Management of bipolar disorder during pregnancy and the postpartum period. Am J Psychiatry. 2004; 161: 608-620.
53. Shah AA, Khawaja IS, Aftab A. Are psychotropic drugs safe to use during pregnancy? Psychiatr Ann. 2015; 45: 71-76.
58. PDR Generics. Montvale, NJ: Medical Economics .1995.
59. ACOG Practice Bulletin. Use of psychiatric medications during pregnancy and lactation. Obstet Gynecol. 2008; 111: 1001-1020.
60. Cohen LS, Friedman JM, Jefferson JW, Johnson EM, Weiner ML. A reevaluation of risk of in utero exposure to lithium. JAMA. 1994; 271: 146-150.
61. Correa-Villasenor A, Ferencz C, Neill CA, Wilson PD, Boughman JA. Ebstein’s malformation of the tricuspid valve: genetic and environmental factors. The Baltimore-Washington Infant Study Group. Teratology. 1994; 50: 137-147.
62. Cohen LS. Treatment of bipolar disorder during pregnancy. J Clin Psychiatry. 2007; 68: 4-9.
63. Briggs GG, Freeman RK, Yaffe SJ. Drugs in Pregnancy and Lactation: A Reference Guide to Fetal and Neonatal Risk. 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.
64. Wyszynski DF, Nambisan M, Surve T, Alsdorf RM, Smith CR, Holmes LB, et al. Increased rate of major malformations in offspring exposed to valproate during pregnancy. Neurology. 2005; 64: 961-965.
65. Hernández-Díaz S, Smith CR, Shen A, Mittendorf R, Hauser WA, Yerby M, et al. Comparative safety of antiepileptic drugs during pregnancy. Neurology. 2012; 78: 1692-1699.
66. Valproate: Drug Information. Waltham, MA: UpToDate; 2014.
67. Schachter SC. Risks Associated with Epilepsy and Pregnancy. In: Pedley TA, Lockwood CJ, eds. Waltham, MA: UpToDate; 2014.
68. Hernández-Díaz S, Werler MM, Walker AM, Mitchell AA. Folic acid antagonists during pregnancy and the risk of birth defects. N Engl J Med. 2000; 343: 1608-1614.
69. Carbamazepine: Drug Information. Waltham, MA: UpToDate; 2014.
70. Rosa FW. Spina bifida in infants of women treated with carbamazepine during pregnancy. N Engl J Med. 1991; 324: 674-677.
71. Morrow J, Russell A, Guthrie E, Parsons L, Robertson I, Waddell R, et al. Malformation risks of antiepileptic drugs in pregnancy: a prospective study from the UK Epilepsy and Pregnancy Register. J Neurol
72. Holmes LB, Baldwin EJ, Smith CR, Habecker E, Glassman L, Wong SL, et al. Increased frequency of isolated cleft palate in infants exposed to lamotrigine during pregnancy. Neurology. 2008; 70: 2152-2158.
73. Singh S, Padmanabhan R. Teratogenic effects of chlorpromazine hydrochloride in rat foetuses. Indian J Med Res. 1978; 67: 300-309.
74. Alexander GJ, Miles BE, Gold GM, Alexander RB. LSD: injection early in pregnancy produces abnormalities in offspring of rats. Science. 1967; 157: 459-460.
75. Hannah RS, Roth SH, Spira AW. The effects of chlorpromazine and phenobarbital on cerebellar Purkinje cells. Teratology. 1982; 26: 21-25.
76. Sobel DE. Infant mortality and malformations in children of schizophrenic women. Psychiatr Q. 1961; 35: 60-65.
77. Rieder RO, Rosenthal D, Wender P, Blumenthal H. The offspring of schizophrenics. Fetal and neonatal deaths. Arch Gen Psychiatry. 1975; 32: 200-211.
78. Rumeau-Rouquette C, Goujard J, Huel G. Possible teratogenic effect of phenothiazines in human beings. Teratology. 1977; 15: 57-64.
79. Slone D, Siskind V, Heinonen OP, Monson RR, Kaufman DW, Shapiro S. Antenatal exposure to the phenothiazines in relation to congenital malformations, perinatal mortality rate, birth weight, and intelligence quotient score. Am J Obstet Gynecol. 1977; 128: 486-488.
80. Heinonen OP, Slone D, Shapiro S. Birth defects and drugs in pregnancy. Littleton, Mass: John Wright-PSG. 1977.
81. KRIS EB, CARMICHAEL DM. Chlorpromazine maintenance therapy during pregnancy and confinement. Psychiatr Q. 1957; 31: 690-695.
82. Ananth J. Congenital malformations with psychopharmacologic agents. Compr Psychiatry. 1975; 16: 437-445.
83. Nurnberg HG, Prudic J. Guidelines for treatment of psychosis during pregnancy. Hosp Community Psychiatry. 1984; 35: 67-71.
84. Nath SP, Miller DA, Muraskas JK. Severe rhinorrhea and respiratory distress in a neonate exposed to fluphenazine hydrochloride prenatally. Ann Pharmacother. 1996; 30: 35-37.
85. Shepard TH. Catalog of Teratogenic Agents. 7th Ed. Maryland: The John Hopkins University Press; 1992.
86. Abdel-Hamid HA, Abdel-Rahman MS, Abdel-Rahman SA. Teratogenic effect of diphenylhydantoin and/or fluphenazine in mice. J Appl Toxicol. 1996; 16: 221-225.
87. Grimaldi R. The clinical use of fluphenazine in pregnancy. N Y Med Coll News Notes. 1960; 2: 42-49.
88. King JT, Barry MC, Neary ER. Perinatal findings in women treated during pregnancy with oral fluphenazine. J New Drugs. 1963; 3: 21-25.
89. Druga A, Nyitray M. Maternal drug metabolism related to teratogenicity of perphenazine in the rat. Teratology. 1981; 24: 38-39.
96. Rawlings WJ, Ferguson R. Maddison TG: Phenmetrazine and trifluperazine. Med J Aust. 1963; 1: 370.
97. Russell T. Drugs In Pregnancy Survey. Practitioner. 1963; 191: 775-780.
98. Ratnayake T, Libretto SE. No complications with risperidone treatment before and throughout pregnancy and during the nursing period. J Clin Psychiatry. 2002; 63: 76-77.
99. Mackay FJ, Wilton LV, Pearce GL. The safety of risperidone: A post-marketing study on 7684 patients. Hum Psychopharmacol. 1998; 13: 413-418.
101. Schenker S, Yang Y, Mattiuz E, Tatum D, Lee M. Olanzapine transfer by human placenta. Clin Exp Pharmacol Physiol. 1999; 26: 691-967.
102. Kirchheiner J, Berghöfer A, Bolk-Weischedel D. Healthy outcome under olanzapine treatment in a pregnant woman. Pharmacopsychiatry. 2000; 33: 78-80.
103. Bristol Myers Squibb Company, Princeton, NJ 08543, USA. New Abilify (aripiprazole). 2002.
Ahmed SM, Moukaddam N, Worley AV, Patel KR, Shah A, et al. (2016) Teratogenic Potential of Commonly Prescribed Psychotropic Drugs. Med J Obstet Gynecol 4(4): 1091.