Nearly 24 million adults in the United States have diabetes.1 Of those, most—approximately 90% to 95%—have type 2 diabetes.2 Both environmental and genetic factors are believed to contribute
to the pathogenesis of type 2 diabetes.3
Type 2 diabetes is associated with substantial morbidity and mortality. Poorly controlled diabetes often leads to serious long-term complications that include both microvascular disease (e.g., retinopathy, neuropathy, nephropathy) and macrovascular disease (e.g., coronary artery disease, cerebrovascular disease, and peripheral arterial disease).3,4 In the United States, diabetes is the most frequent cause of new cases of blindness among adults 20 to 74 years of age, as well as the leading cause of end-stage renal disease.1,4 More than 60% of nontraumatic lower-limb ampu-tations are performed in people with diabetes.1 Atherosclerosis occurs at an earlier age and with greater frequency among people with diabetes, such that diabetes is counted as a coronary heart disease risk equiva-lent.3-5 Two out of three patients with diabetes die from some form of cardiovascular disease (CVD).6,7 Overall, the risk for death among people with diabetes is approximately twice that of people without diabetes of similar age.1
The long-term complications of type 2 diabetes contribute to excep-tionally high disease-related costs. In 2007 (the latest year for which data are available), the direct medical costs and indirect costs (e.g., disability, work loss, premature mortality) associated with diagnosed diabetes in the United States totaled $174 billion.8 Nearly one in five hospitaliza-tions in 2008 was related to diabetes, representing more than 7.7 million stays and $83 billion in hospital costs—23% of the total hospital costs in the United States.9 Average medical expenditures among people with diagnosed diabetes are estimated to be 2.3 times higher than what expen-ditures would be in the absence of diabetes.8
Because pharmacists have frequent contact with patients with type 2 diabetes, they are ideally positioned to make substantial contribu-tions to diabetes care. This monograph employs case vignettes to ex-plore common clinical scenarios and emerging problems encountered by pharmacists. As is true in practice, the vignettes may not have a clear resolution. When firm recommendations cannot be made, summaries of the latest thinking about each situation are provided.
Are you on the right path?Before participating in the activity, test your knowledge by answering the following questions. These questions will also be a part of the CPE exam.
1. In the American Association of Clinical Endocrinologists/American College of Endocrinology algorithm for glycemic control in type 2 diabetes, which of the following regimens would be preferred for initial therapy in a patient with an A1C level of 8.9%?
a. Metformin monotherapy.b. Metformin + a sulfonylurea.c. Metformin + a glucagon-like peptide-1 agonist.d. Insulin alone or with other agents.
2. Tom Rogers has a current total daily insulin dose of 250 units. His most recent A1C level was 7.8%. Tom’s primary care provider wants to switch him to U-500 insulin and calculates an initial total dose of 200 units. If twice daily dosing is desired, which U-100 syringe marking should Tom use to measure each dose?
a. 20.b. 25.c. 40.d. 50.
3. A patient with type 2 diabetes has a blood pressure reading of 137/85 mm Hg. Which of the following options represents a recommended course of action?
a. Do nothing—this reading is below the goal of 140/90 mm Hg.
b. Initiate antihypertensive therapy with a thiazide diuretic.
c. Initiate antihypertensive therapy with an
angiotensin-converting enzyme inhibitor.
d. Initiate antihypertensive therapy with a calcium-
channel blocker.
Continuing Pharmacy Education • November 2010 • Supplement to Pharmacy Today
Learning ObjectivesAt the completion of this activity, the pharmacist will be able to:
1. State key statistics regarding the impact of type 2 diabetes in the United States.
2. Summarize the latest thinking about the pathogenesis of type 2 diabetes.
3. Recall treatment goals and options for patients with type 2 diabetes.4. Compare and contrast current treatment recommendations for
glycemic control in type 2 diabetes.5. Identify effective strategies for addressing patient concerns
about initiating insulin therapy.6. Explain the appropriate use of U-500 insulin.7. Discuss nonglycemic goals in comprehensive type 2 diabetes
management.
Advisory BoardTommy Johnson, PharmD, BC-ADM, CDE, FAADEChair and Professor of Pharmacy PracticePresbyterian College School of PharmacyClinton, South Carolina
Karen Reed, RPh, FAPhAStaff PharmacistKmart PharmacyBeckley, West Virginia
DisclosuresTommy Johnson, PharmD, BC-ADM, CDE, FAADE, has served as an advisory board member for Can-Am Care. He declares no other conflicts of interest or financial interests in any product or service mentioned in this activity, including grants, employment, gifts, stock holdings, and honoraria.
Karen Reed, RPh, FAPhA, declares she has served on an advisory board and received honoraria from GlaxoSmithKline and Eli Lilly and Company. She declares that her spouse is a former employee of GlaxoSmithKline. She declares no other conflicts of interest or financial interests in any product or service mentioned in this activity, including grants, employment, gifts, stock holdings, and honoraria.
APhA’s editorial staff declare no conflicts of interest or financial interests in any product or service mentioned in this activity, including grants, employment, gifts, stock holdings, and honoraria.
This publication was prepared by Cynthia Knapp Dlugosz, BSPharm, of CKD Associates, LLC, on behalf of the American Pharmacists Association.
Accreditation InformationThe American Pharmacists Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education (CPE). The ACPE Universal Activity Number assigned to this activity
by the accredited provider is 202-000-10-260-H01-P.
To obtain 2 hours of CPE credit (0.2 CEUs) for this activity, com-plete the CPE exam and submit it online at www.pharmacist.com/education. A Statement of Credit will be awarded for a passing grade of 70% or better. You will have two opportunities to success-fully complete the CPE exam. Pharmacists who successfully com-plete this activity before November 1, 2013, can receive credit.
Your Statement of Credit will be available online immediately upon successful completion of the CPE exam.
DevelopmentThis home-study CPE activity was developed by the American Pharmacists Association.
SupportThis activity is supported by an independent educational grant from Merck.
Provider: American Pharmacists AssociationTarget Audience: PharmacistsRelease Date: November 1, 2010Expiration Date: November 1, 2013Learning Level: 2
ACPE Number: 202-000-10-260-H01-PCPE Credit: 2 hours (0.2 CEUs))ACPE Activity Type: Application-basedFee: There is no fee associated with this activity.
American Pharmacists Association • 2215 Constitution Avenue, NW • Washington, DC 20037 • 800-237-APhA • www.pharmacist.com
Test Your Knowledge: Diabetes 3
Mini-Review: Pathogenesis of Type 2 Diabetes
Type 2 diabetes is characterized by the dual defects of insulin resistance (i.e., diminished liver, muscle, and adipose sensitivity to insulin) and impaired pancreatic β-cell secretory function (i.e., impaired insulin secretion).3 Insulin resistance is associated with a decrease in the uptake and utilization of glucose by insulin-sensitive tissues (primarily muscle and adipose tissue) as well as ineffective suppression of hepatic glucose production.3,10 β-Cells are able to compensate for the decrease in insulin action (and resulting hyper-glycemia) by increasing their production of insulin.3,11,12 However, as the fasting plasma glucose concentration continues to rise, the β-cells become less and less able to sustain the necessary levels of in-sulin secretion. A cycle of diminished insulin secretion and worsen-ing insulin resistance ensues; the β-cells eventually fail altogether.
Because not everyone with insulin resistance goes on to develop type 2 diabetes, there is growing speculation that β-cell deteriora-tion—reflecting both intrinsic secretion failure and reductions in β-cell mass—may actually precede insulin resistance and even contribute to its development.3,10,11 β-Cell dysfunction is now known to occur much earlier in the natural history of type 2 diabetes than originally thought; the landmark United Kingdom Prospective Diabetes Study (UKPDS) demonstrated that approximately 50% of β-cell function already has been lost by the time type 2 diabetes is diagnosed, and some experts posit that as much as 80% of function may be lost.12-14 Data from the Belfast Diet Study show that β-cell deterioration proceeds relatively slowly at first—at a rate of 1.7% per year for as long as 15 to 17 years—then accelerates abruptly to more than 18% per year between 3 and 5 years after diagnosis.11,15 β-Cell failure currently is considered to be more important than insulin resistance in the natural history of type 2 diabetes.11,12,16
There also is growing appreciation of the role of etiologic mecha-nisms beyond β-cell dysfunction and insulin resistance. Diabetes expert Ralph DeFronzo, MD, refers to the multiple pathogenic mech-anisms of type 2 diabetes as the “ominous octet” (Figure 1).12,13 In addition to decreased insulin secretion and decreased uptake of glu-cose, these mechanisms include increased hepatic glucose produc-
tion, accelerated lipolysis in adipocytes (elevated plasma free fatty acid levels), diminished incretin effect, hypersecretion of glucagon by pancreatic α-cells, enhanced renal glucose reabsorption, and central nervous system insulin resistance resulting from neurotrans-mitter dysfunction.12,17
Mini-Review: Approach to TreatmentAbundant conclusive evidence from long-term, randomized clini-
cal trials shows that maintaining hemoglobin A1C levels close to the normal range reduces the incidence and progression of microvascu-lar complications of type 2 diabetes.4,18-21 In general, every percentage point drop in A1C (e.g., from 8.0% to 7.0%) decreases the risk of microvascular complications by 40%.1 Early intervention to reduce A1C levels also appears to contribute to a long-term reduction in the risk of macrovascular disease.18
Accordingly, A1C has become the primary target for glycemic con-trol. The American Diabetes Association (ADA) Standards of Medical Care in Diabetes recommend an A1C goal of <7%.4 The American College of Endocrinology (ACE) and the American Association of Clinical Endocrinologists (AACE) recommend a more stringent A1C goal of ≤6.5%.22,23 All of these organizations recognize that more or less stringent A1C goals may be appropriate for certain patients, de-pending on the risk for hypoglycemia, comorbid conditions that lim-it life expectancy, and factors that may limit the safety of attempting aggressive glucose control.4,18,22-24
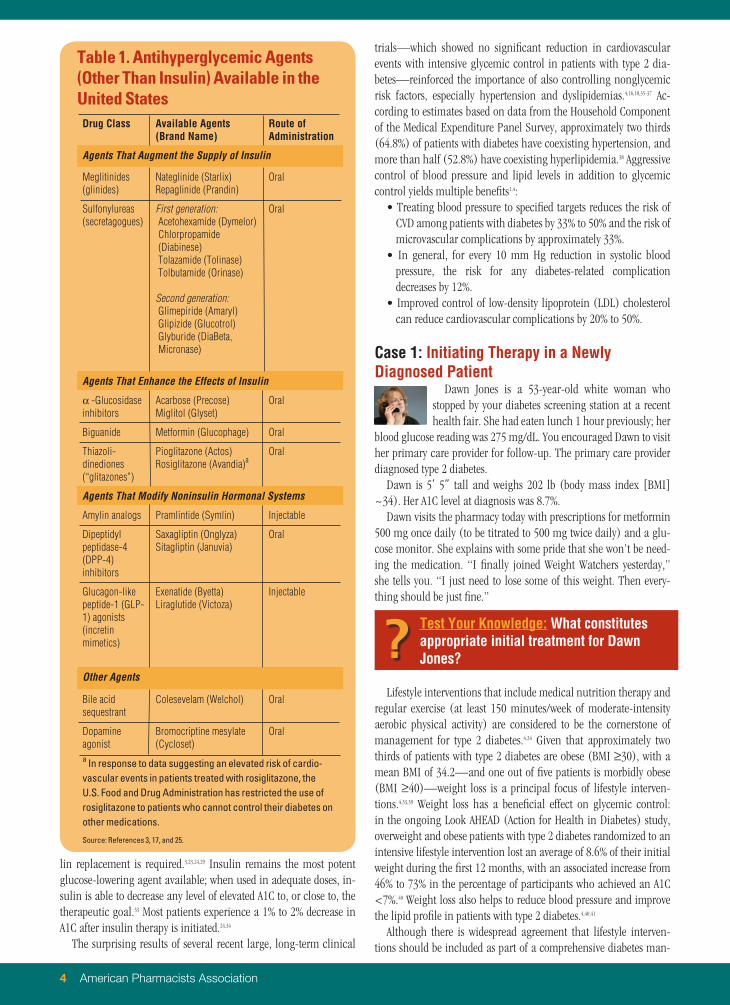
A range of noninsulin oral and injectable antihyperglycemic agents (Table 1) and insulins are used in the treatment of type 2 diabetes.3,17,25 All agents (other than insulin) are limited in their abil-ity to lower A1C.26 In one recent systematic review and meta-analysis of 61 double-blind, randomized controlled trials that met predefined methodologic criteria, most oral antihyperglycemic agents were found to decrease A1C levels by 0.5% to 1.25% (thiazolidinediones and sulfonylureas lowered A1C levels by approximately 1.0% to 1.25%).27 An increase in dose yielded a further decrease in A1C ini-tially, with most of the treatment effect evident by 3 to 6 months. Higher baseline A1C levels were associated with greater declines in A1C; every 1% higher pretreatment A1C level predicted a 0.5% greater fall of A1C levels after 6 months of therapy. Disease duration had no clear effect on treatment response.
Because of the progressive loss of β-cell function in patients with type 2 diabetes, most available antihyperglycemic therapies are un-able to maintain glycemic control over time, and the majority of patients eventually require combination therapy.3,24,28-31 The response to antihyperglycemic agents (other than insulin) usually is more pronounced in patients who are treatment naïve than in those who already are receiving therapy.28 This was demonstrated in a recent mixed-treatment comparison meta-analysis by Phung and col-leagues.32 The analysis evaluated the efficacy of antihyperglycemic agents used as second-line therapy in patients experiencing an in-adequate response to maximized and stable metformin therapy (≥4 weeks at ≥1,500 mg daily, or the maximally tolerated dose); it in-cluded 27 randomized clinical trials that enrolled more than 11,000 participants. The additional reductions in A1C provided by the differ-ent classes of drugs ranged from 0.64% to 0.97%.
Eventually, β-cell function deteriorates to such a degree that the secretory capacity of the cells is exceeded and exogenous insu-
Figure 1. Multiple Defects That Contribute to the Progression of Type 2 Diabetes
HGP = hepatic glucose production.
Source: Reference 13. Reprinted with permission from the American Diabetes Association.
Test Your Knowledge: Diabetes 3
4 American Pharmacists Association
lin replacement is required.3,23,24,29 Insulin remains the most potent glucose-lowering agent available; when used in adequate doses, in-sulin is able to decrease any level of elevated A1C to, or close to, the therapeutic goal.33 Most patients experience a 1% to 2% decrease in A1C after insulin therapy is initiated.24,34
The surprising results of several recent large, long-term clinical
trials—which showed no significant reduction in cardiovascular events with intensive glycemic control in patients with type 2 dia-betes—reinforced the importance of also controlling nonglycemic risk factors, especially hypertension and dyslipidemias.4,16,18,35-37 Ac-cording to estimates based on data from the Household Component of the Medical Expenditure Panel Survey, approximately two thirds (64.8%) of patients with diabetes have coexisting hypertension, and more than half (52.8%) have coexisting hyperlipidemia.38 Aggressive control of blood pressure and lipid levels in addition to glycemic control yields multiple benefits1,4:
• Treating blood pressure to specified targets reduces the risk of CVD among patients with diabetes by 33% to 50% and the risk of microvascular complications by approximately 33%.
• In general, for every 10 mm Hg reduction in systolic blood pressure, the risk for any diabetes-related complication decreases by 12%.
• Improved control of low-density lipoprotein (LDL) cholesterol can reduce cardiovascular complications by 20% to 50%.
Case 1: Initiating Therapy in a Newly Diagnosed Patient
Dawn Jones is a 53-year-old white woman who stopped by your diabetes screening station at a recent health fair. She had eaten lunch 1 hour previously; her
blood glucose reading was 275 mg/dL. You encouraged Dawn to visit her primary care provider for follow-up. The primary care provider diagnosed type 2 diabetes.
Dawn is 5’ 5” tall and weighs 202 lb (body mass index [BMI] ~34). Her A1C level at diagnosis was 8.7%.
Dawn visits the pharmacy today with prescriptions for metformin 500 mg once daily (to be titrated to 500 mg twice daily) and a glu-cose monitor. She explains with some pride that she won’t be need-ing the medication. “I finally joined Weight Watchers yesterday,” she tells you. “I just need to lose some of this weight. Then every-thing should be just fine.”
Lifestyle interventions that include medical nutrition therapy and regular exercise (at least 150 minutes/week of moderate-intensity aerobic physical activity) are considered to be the cornerstone of management for type 2 diabetes.4,24 Given that approximately two thirds of patients with type 2 diabetes are obese (BMI ≥30), with a mean BMI of 34.2—and one out of five patients is morbidly obese (BMI ≥40)—weight loss is a principal focus of lifestyle interven-tions.4,33,39 Weight loss has a beneficial effect on glycemic control: in the ongoing Look AHEAD (Action for Health in Diabetes) study, overweight and obese patients with type 2 diabetes randomized to an intensive lifestyle intervention lost an average of 8.6% of their initial weight during the first 12 months, with an associated increase from 46% to 73% in the percentage of participants who achieved an A1C <7%.40 Weight loss also helps to reduce blood pressure and improve the lipid profile in patients with type 2 diabetes.4,40,41
Although there is widespread agreement that lifestyle interven-tions should be included as part of a comprehensive diabetes man-
Table 1. Antihyperglycemic Agents (Other Than Insulin) Available in the United StatesDrug Class Available Agents
(Brand Name)Route of Administration
Agents That Augment the Supply of Insulin
Meglitinides (glinides)
Nateglinide (Starlix)Repaglinide (Prandin)
Oral
Sulfonylureas (secretagogues)
First generation:Acetohexamide (Dymelor)Chlorpropamide (Diabinese)Tolazamide (Tolinase)Tolbutamide (Orinase)
Second generation:Glimepiride (Amaryl)Glipizide (Glucotrol)Glyburide (DiaBeta, Micronase)
a In response to data suggesting an elevated risk of cardio-vascular events in patients treated with rosiglitazone, the U.S. Food and Drug Administration has restricted the use of rosiglitazone to patients who cannot control their diabetes on other medications.
Source: References 3, 17, and 25.
Test Your Knowledge: What constitutes appropriate initial treatment for Dawn Jones??
Test Your Knowledge: Diabetes 5
agement strategy, implementing and maintaining these changes poses an exceedingly high hurdle for many patients.3,25,33 It is now generally accepted that most patients with type 2 diabetes require pharmacologic therapy superimposed on lifestyle interventions to achieve desired glycemic targets.24,31,33
A consensus algorithm (Figure 2) developed jointly by the ADA and the European Association for the Study of Diabetes (EASD) calls for metformin to be initiated concurrently with lifestyle interven-tions at the time of diagnosis and titrated to its maximally effective dose over a period of 1 to 2 months, as tolerated.4,33 Factors support-ing this recommendation include the following33:
• Metformin usually does not cause either hypoglycemia or weight gain.
• Metformin is associated with a generally low level of adverse effects (primarily gastrointestinal).
• The availability of generic versions of metformin contributes to a generally low cost of therapy.
Metformin therapy is recommended for all newly diagnosed patients unless specific contraindications (e.g., renal impairment, hepatic dysfunction, heart failure) are present.26,33
A growing number of primary care providers are aware of the ADA/EASD algorithm, so it is becoming increasingly common to see newly diagnosed patients present with a prescription for metformin. Clinicians may not be aware that the algorithm has been the subject of much controversy; they also may not know that the algorithm reflects the expert opinion of the authors rather than official ADA position.13,17,42 Thus, it is not considered a “universal guideline” for
diabetes management.17
Other algorithms based on expert opinion are available. Nota-bly, the AACE and ACE collaborated on “Diabetes Road Maps” and a glycemic control algorithm that incorporate all major classes of currently available antihyperglycemic therapies.22,23 The treatment pathways in these documents are stratified by A1C level as well as whether the patient is drug naïve or already receiving treatment.23 The stated concerns in prioritizing choices of medications include23:
• Minimizing the risk and severity of hypoglycemia.• Minimizing the risk and magnitude of weight gain.• Consideration of both fasting and postprandial glucose levels
as end points.• Anticipated degree of patient adherence.
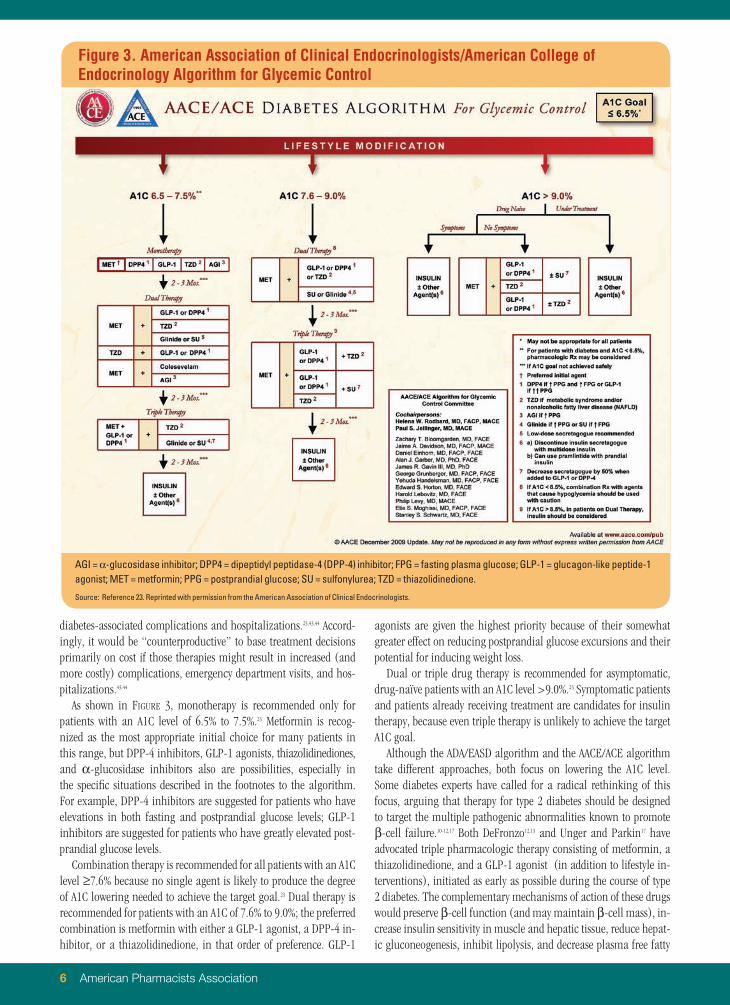
The algorithm (Figure 3) emphasizes the appropriate use of dipep-tidyl peptidase-4 (DPP-4) inhibitors and glucagon-like peptide-1 (GLP-1) agonists because of their effectiveness in reducing A1C levels, lower risk of hypoglycemia, and beneficial effects on weight (weight neutrality with DPP-4 inhibitors, weight loss with GLP-1 ag-onists). Sulfonylureas and meglitinides are assigned a lower priority in the algorithm because they cause hypoglycemia and weight gain and provide only short-term beneficial effects on glycemic control.
Although medication costs also were considered when prioritiz-ing choices of medications in the AACE/ACE algorithm, safety and efficacy were viewed as higher priorities than cost.23 The authors reasoned that the cost of medications represents only a very small portion (approximately 10%) of the total cost of care for patients with diabetes; the majority of total cost is related to the treatment of
Figure 2. American Diabetes Association/European Association for the Study of Diabetes Algorithm for the Treatment of Type 2 Diabetes
Source: Reference 33. Copyright 2009 American Diabetes Association from Diabetes Care, Vol. 32, 2009; 193-203. Reprinted with permission from the American Diabetes Association.
6 American Pharmacists Association
diabetes-associated complications and hospitalizations.23,43,44 Accord-ingly, it would be “counterproductive” to base treatment decisions primarily on cost if those therapies might result in increased (and more costly) complications, emergency department visits, and hos-pitalizations.43,44
As shown in Figure 3, monotherapy is recommended only for patients with an A1C level of 6.5% to 7.5%.23 Metformin is recog-nized as the most appropriate initial choice for many patients in this range, but DPP-4 inhibitors, GLP-1 agonists, thiazolidinediones, and α-glucosidase inhibitors also are possibilities, especially in the specific situations described in the footnotes to the algorithm. For example, DPP-4 inhibitors are suggested for patients who have elevations in both fasting and postprandial glucose levels; GLP-1 inhibitors are suggested for patients who have greatly elevated post-prandial glucose levels.
Combination therapy is recommended for all patients with an A1C level ≥7.6% because no single agent is likely to produce the degree of A1C lowering needed to achieve the target goal.23 Dual therapy is recommended for patients with an A1C of 7.6% to 9.0%; the preferred combination is metformin with either a GLP-1 agonist, a DPP-4 in-hibitor, or a thiazolidinedione, in that order of preference. GLP-1
agonists are given the highest priority because of their somewhat greater effect on reducing postprandial glucose excursions and their potential for inducing weight loss.
Dual or triple drug therapy is recommended for asymptomatic, drug-naïve patients with an A1C level >9.0%.23 Symptomatic patients and patients already receiving treatment are candidates for insulin therapy, because even triple therapy is unlikely to achieve the target A1C goal.
Although the ADA/EASD algorithm and the AACE/ACE algorithm take different approaches, both focus on lowering the A1C level. Some diabetes experts have called for a radical rethinking of this focus, arguing that therapy for type 2 diabetes should be designed to target the multiple pathogenic abnormalities known to promote β-cell failure.10-12,17 Both DeFronzo12,13 and Unger and Parkin17 have advocated triple pharmacologic therapy consisting of metformin, a thiazolidinedione, and a GLP-1 agonist (in addition to lifestyle in-terventions), initiated as early as possible during the course of type 2 diabetes. The complementary mechanisms of action of these drugs would preserve β-cell function (and may maintain β-cell mass), in-crease insulin sensitivity in muscle and hepatic tissue, reduce hepat-ic gluconeogenesis, inhibit lipolysis, and decrease plasma free fatty
Figure 3. American Association of Clinical Endocrinologists/American College of Endocrinology Algorithm for Glycemic Control
Source: Reference 23. Reprinted with permission from the American Association of Clinical Endocrinologists.
Test Your Knowledge: Diabetes 7
acid levels, as well as provide antiatherogenic effects and support weight loss.10,12,13,17,31 Importantly, this combination would not cause hypoglycemia.12,17 According to DeFronzo, this triple combination approach offers the greatest likelihood of providing durable glucose control through a blunting of disease progression.12 DPP-4 inhibi-tors could be an alternative to GLP-1 agonists in the combination if they are shown to preserve β-cell function on a long-term basis.12 (Pharmacists should note that the efficacy and safety of this strategy have not been confirmed; a randomized clinical trial is planned.10)
As the treatment options for type 2 diabetes expand, the ques-tion of which medication or medications represents the best option for initial therapy in a given patient increasingly will lack a clear, evidence-based solution. The approach recommended to prescrib-ers in the absence of evidence is to inform patients of all treatment options, explain the benefits and risks of each, and engage patients in the decision-making process.45 Initiating aggressive combination therapy would be of little benefit if, for example, a patient chose to fill only the least expensive prescription, thereby defaulting to an approach that would fail to fulfill the treatment plan.25
Case 2: When to Adjust TherapyLeroy Thomas is a 58-year-old African American man
who was diagnosed with type 2 diabetes approximately 3 years ago. He visits the pharmacy today with a prescrip-tion for metformin extended-release 2,000 mg daily. Leroy
is not new to your practice; dispensing records for the past 2 years show periodic prescriptions for the same dosage of metformin. Based on transfer notations and a brief discussion with Leroy about ad-herence, you suspect that he has been “coupon chasing”—visiting other pharmacies to take advantage of the latest promotion. You also are aware that Leroy receives most of his care from a busy group practice and rarely sees the same provider twice in a row.
Leroy is 5’ 10” tall and weighs 218 lb (BMI ~31). You collect the following additional information during today’s visit:
• A1C: 8.9%.• Blood pressure: 128/78 mm Hg.
In addition to metformin, Leroy Thomas’s other current medica-tions include:
For decades, the paradigm for long-term management of type 2 dia-betes involved a stepwise “treat to failure” approach.10,34,46 Therapy was initiated with lifestyle modifications alone; medications were added slowly and sequentially only when a trial of diet and exercise proved to be inadequate for achieving glycemic control.28,34 A single oral agent was titrated to its maximal recommended dose, followed by a second oral agent added and titrated to its maximal dose, and so on.10
As a result, prescribers often failed to adjust antihyperglycemic therapy in a timely manner—a problem referred to as clinical iner-
tia.17,23,46,47 Long delays were incurred between treatment steps, leaving patients with uncontrolled hyperglycemia for extended periods.46,48 For example, in a study published in 2004, Brown and colleagues found that patients remained on sulfonylurea monotherapy (the usual initial treatment at the time of the study) for a mean of 35.1 ± 17.8 months before a new or additional treatment was started.48 During that interval, the patients’ A1C level exceeded 8.0% (the rec-ommended “action threshold” at the time of the study) for a mean of 20.5 ± 18.0 months. Patients who followed the usual treatment progression—lifestyle intervention first, then oral monotherapy, then oral combination therapy, and finally insulin—would have spent approximately 10 years with an A1C level >7% and nearly 5 years with an A1C level >8%.
The current treatment paradigm calls for patients to be evaluated frequently to monitor response to treatment, and for therapy to be intensified rapidly if glycemic goals are not achieved.16,34,46 Yet clini-cal inertia persists in today’s practice environment.10 This may be attributed in part to the lack of direct evidence regarding the ideal frequency of physician visits for patients with type 2 diabetes.24 The 2010 ADA Standards of Medical Care in Diabetes call for routine A1C testing in all patients with diabetes, at the following recommended intervals4 :
• At least twice yearly in patients who are meeting treatment goals and have stable glycemic control (A1C <7%).
• Quarterly in patients whose therapy has changed or who are not meeting glycemic goals.
Some clinicians schedule follow-up visits to coincide with these test-ing intervals (i.e., two to four visits per year). Anecdotal evidence suggests that many patients are seen far less frequently, and that A1C testing does not occur as recommended.23 The fault does not necessarily lie entirely with health care providers; in some cases, pa-tients may receive inadequate follow-up because they fail to return for routine visits.25
Both the ADA/EASD and AACE/ACE algorithms challenge clini-cians to monitor therapy closely and adjust the treatment plan every 2 to 3 months as needed until the goal for A1C has been achieved.23,33 Because the response from dose escalation usually is limited, adjust-ing the treatment plan generally means adding another agent.24
Pharmacists can help to combat clinical inertia by offering point-of-care A1C testing and intervening with prescribers as appropriate. Several devices appropriate for use in pharmacies (e.g., Bayer A1C Now+) have been granted waived status under the Clinical Labo-ratory Improvement Amendments. However, pharmacists should be aware that the results obtained with these devices may be less sensi-tive and specific than laboratory testing.49
Case 3: How to Adjust TherapyMartina Hernandez is a 48-year-old Hispanic woman
of Mexican descent who was diagnosed with type 2 dia-betes approximately 2 years ago. Therapy was initiated
with metformin 500 mg twice daily and titrated to the current dose of metformin 1,000 mg twice daily.
Martina is 5’ 1” tall and weighs 180 lb (BMI 34). Although she has successfully lost weight (as much as 25 lb) on various diets in the past, she regained all of the lost weight each time. She is better able to adhere to her goal of taking a 30-minute walk on at least 5 days each week.
Test Your Knowledge: At what point should Leroy Thomas’s antihyperglycemic regimen ideally have been adjusted??
8 American Pharmacists Association
When Martina visited her primary care provider earlier this week, her measured A1C level was 8.1%. She comes to the pharmacy today with a prescription for glipizide 10 mg once daily in addition to a metformin refill. She asks the pharmacy technician to make sure that glipizide is on the list of medications that cost $4.
The care of patients with type 2 diabetes whose A1C level remains above target despite metformin therapy and lifestyle modifications is another area of clinical controversy. The ADA/EASD and AACE/ACE algorithms provide strikingly different advice about escalating antihyperglycemic therapy.
The ADA/EASD algorithm calls for a second agent to be added to metformin monotherapy within 2 to 3 months if the maximum tolerated dose of metformin fails to achieve or sustain the glycemic goals (Figure 2).33 The preferred options for the second agent are a sulfonylurea or insulin, with insulin therapy (basal therapy with an intermediate- or long-acting formulation) recommended for patients with an A1C level >8.5% or symptoms secondary to hyper-glycemia.
The ADA/EASD algorithm also offers two “tier 2” options for the second agent: pioglitazone and a GLP-1 agonist.33 (“Tier 2” repre-sents less well-validated therapies.) Either agent may be considered when the risk of hypoglycemia is especially undesirable (e.g., in pa-tients who have hazardous jobs); a GLP-1 agonist may be considered if weight loss is a major goal of therapy and the patient’s A1C level is <8.0%.
As illustrated in Figure 2, the options for further escalation of therapy depend on which second agent was added.33 Ultimately, a combination of metformin and intensive insulin therapy (i.e., basal therapy plus bolus injections of a short- or rapid-acting insulin be-fore selected meals to reduce postprandial glucose excursions) is recommended for all patients.
It is noteworthy that none of the other available antihypergly-cemic agents—amylin agonists, α-glucosidase inhibitors, megli-tinides, or DPP-4 inhibitors—are included in the algorithm. The authors state that these agents were omitted for one or more of the following reasons33:
• They have lower or equivalent overall glucose-lowering effectiveness compared with the recommended agents.
• Limited clinical data regarding their use are available.• They are relatively expensive compared with the
recommended agents.The authors do note that these agents may be appropriate choices in selected patients.
In clinical practice, the choice of a sulfonylurea for second-line therapy is reinforced by the pricing policies of a growing number of pharmacies, which offer select diabetes medications—typically generic versions of metformin and sulfonylureas—to patients at low (e.g., $4) or no cost. Combination therapy with metformin and a sulfonylurea thus becomes the least expensive option by far. A key criticism of the ADA/EASD algorithm is that neither metformin nor the sulfonylureas have been shown to preserve β-cell function.12,17
Sulfonylureas also are associated with a substantial risk of hypogly-cemia and weight gain.17,23
In the AACE/ACE algorithm (Figure 3), metformin remains the foundation of combination therapy for most patients because of its safety and mechanism of action as an insulin sensitizer.23 For pa-tients with an A1C level of 6.5% to 7.5%, the recommended second component of dual therapy is a GLP-1 agonist, a DPP-4 inhibitor, a thiazolidinedione, or a meglitinide or sulfonylurea, in that order of preference. Again, GLP-1 agonists are given the highest priority because of their somewhat greater effectiveness in reducing post-prandial glucose excursions relative and their potential for inducing weight loss. When triple therapy is indicated for patients with an A1C level of 6.5% to 7.5%, six combinations are possible, based on the ad-dition of a thiazolidinedione, meglitinide, or sulfonylurea:
A thiazolidinedione is preferred to minimize the risk of hypoglycemia.Patients with an A1C level of 7.6% to 9.0% would have been started
on dual therapy (Figure 3).23 The preferred strategy for triple therapy is to add a thiazolidinedione to the combination of either metformin plus a GLP-1 agonist or metformin plus a DPP-4 inhibitor. The least preferred combination is metformin, a thiazolidinedione, and a sul-fonylurea because of the high risk of weight gain and hypoglycemia. Meglitinides and α-glucosidase inhibitors do not have sufficient A1C-lowering potential to be considered for triple therapy.
The one place in the AACE/ACE algorithm where sulfonylureas are preferred is in triple therapy for asymptomatic patients with an A1C level >9.0% who were started on dual therapy.23 The recommenda-tion is based on the somewhat greater efficacy and more rapid onset of action of the sulfonylurea compared with a thiazolidinedione.
Nauck and colleagues recently speculated on the most likely fu-ture roles of the various incretin-based therapies in the treatment of type 2 diabetes.50 One of the authors suggested that DPP-4 inhibitors eventually will be ranked before GLP-1 agonists in treatment algo-rithms because of the greater acceptability of oral administration. Ultimately, DPP-4 inhibitors may replace existing oral antihyper-glycemic agents, while the GLP-1 agonists (which are administered by subcutaneous injection) may be viewed as competitors for insulin treatment.
As is the case when therapy for type 2 diabetes is initiated, pre-scribers seeking to intensify a patient’s treatment regimen are ad-vised to inform the patients of all options available, explain the benefits and risks of each, and include the patient in the decision-making process.45
Initiating Insulin TherapyIt is 4 years later. Martina Hernandez is now 52 years old. Her
current medication regimen includes:• Metformin 1,000 mg/sitagliptin 50 mg (administered as a
combination product).• Glipizide 10 mg once daily.
Martina visited her primary care provider earlier this week to assess the current level of glycemic control after 11 months on this regi-
Test Your Knowledge: What constitutes appropriate intensification of antihyperglycemic therapy for Martina Hernandez?
?
Test Your Knowledge: Diabetes 9
men. Her measured A1C was 9.2%.Martina comes to the pharmacy today with a prescription for in-
sulin glargine. As the pharmacy technician readies the product and associated supplies for dispensing, you sit down with Martina to teach her how to use and inject insulin. She begins to cry. “I knew this would happen,” Martina says. “It’s all my fault because I couldn’t lose weight. My mother had to use insulin when I was a little girl—I’ll never forget what she went through, how painful it was.”
All current treatment algorithms for type 2 diabetes culminate in the initiation of insulin therapy.23,33 Because most patients will require insulin therapy at some point during the course of treat-ment—and because insulin is considered to have a greater potential than other agents for preserving β-cell function—early initiation of insulin is becoming more widely accepted.23,26,33 There is growing consensus that insulin no longer should be considered a “treatment of last resort” after other therapies have failed.51
Unfortunately, many patients who could benefit from insulin therapy do not receive it in a timely manner, or may not receive it at all.51 A retrospective cohort analysis by Rubino and colleagues in-volving more than 2,500 patients with type 2 diabetes illustrates this point.52 In fully half of the patients, insulin initiation was delayed for almost 5 years after combination therapy with oral agents failed to maintain glycemic control, even in the presence of diabetes-related complications.
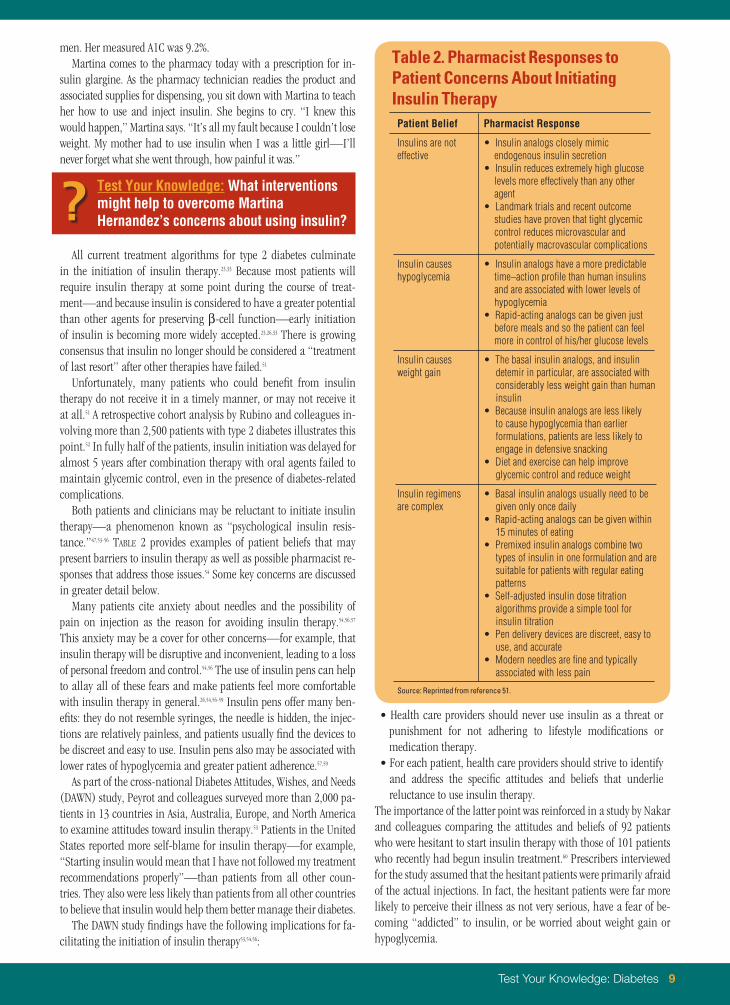
Both patients and clinicians may be reluctant to initiate insulin therapy—a phenomenon known as “psychological insulin resis-tance.”47,53-56 Table 2 provides examples of patient beliefs that may present barriers to insulin therapy as well as possible pharmacist re-sponses that address those issues.54 Some key concerns are discussed in greater detail below.
Many patients cite anxiety about needles and the possibility of pain on injection as the reason for avoiding insulin therapy.54,56,57 This anxiety may be a cover for other concerns—for example, that insulin therapy will be disruptive and inconvenient, leading to a loss of personal freedom and control.54,56 The use of insulin pens can help to allay all of these fears and make patients feel more comfortable with insulin therapy in general.26,54,56-59 Insulin pens offer many ben-efits: they do not resemble syringes, the needle is hidden, the injec-tions are relatively painless, and patients usually find the devices to be discreet and easy to use. Insulin pens also may be associated with lower rates of hypoglycemia and greater patient adherence.57,59
As part of the cross-national Diabetes Attitudes, Wishes, and Needs (DAWN) study, Peyrot and colleagues surveyed more than 2,000 pa-tients in 13 countries in Asia, Australia, Europe, and North America to examine attitudes toward insulin therapy.53 Patients in the United States reported more self-blame for insulin therapy—for example, “Starting insulin would mean that I have not followed my treatment recommendations properly”—than patients from all other coun-tries. They also were less likely than patients from all other countries to believe that insulin would help them better manage their diabetes.
The DAWN study findings have the following implications for fa-cilitating the initiation of insulin therapy53,54,56:
• Health care providers should never use insulin as a threat or punishment for not adhering to lifestyle modifications or medication therapy.
• For each patient, health care providers should strive to identify and address the specific attitudes and beliefs that underlie reluctance to use insulin therapy.
The importance of the latter point was reinforced in a study by Nakar and colleagues comparing the attitudes and beliefs of 92 patients who were hesitant to start insulin therapy with those of 101 patients who recently had begun insulin treatment.60 Prescribers interviewed for the study assumed that the hesitant patients were primarily afraid of the actual injections. In fact, the hesitant patients were far more likely to perceive their illness as not very serious, have a fear of be-coming “addicted” to insulin, or be worried about weight gain or hypoglycemia.
Table 2. Pharmacist Responses to Patient Concerns About Initiating Insulin TherapyPatient Belief Pharmacist Response
• Insulin reduces extremely high glucose levels more effectively than any other agent
• Landmark trials and recent outcome studies have proven that tight glycemic control reduces microvascular and potentially macrovascular complications
Insulin causes hypoglycemia
• Insulin analogs have a more predictable time–action profile than human insulins and are associated with lower levels of hypoglycemia
• Rapid-acting analogs can be given just before meals and so the patient can feel more in control of his/her glucose levels
Insulin causes weight gain
• The basal insulin analogs, and insulin detemir in particular, are associated with considerably less weight gain than human insulin
• Because insulin analogs are less likely to cause hypoglycemia than earlier formulations, patients are less likely to engage in defensive snacking
• Diet and exercise can help improve glycemic control and reduce weight
Insulin regimens are complex
• Basal insulin analogs usually need to be given only once daily
• Rapid-acting analogs can be given within 15 minutes of eating
• Premixed insulin analogs combine two types of insulin in one formulation and are suitable for patients with regular eating patterns
• Self-adjusted insulin dose titration algorithms provide a simple tool for insulin titration
• Pen delivery devices are discreet, easy to use, and accurate
• Modern needles are fine and typically associated with less pain
Source: Reprinted from reference 51.
Test Your Knowledge: What interventions might help to overcome Martina Hernandez’s concerns about using insulin??
10 American Pharmacists Association
Pharmacists can help to overcome psychological insulin re-sistance by discussing insulin therapy with patients from the time they are first diagnosed with type 2 diabetes.51,54,56 Patients need to understand both the progressive nature of their condition—and the concomitant decrease in insulin production—and the very real possibility that insulin “replacement” will be needed at some point, through no fault of their own.34,57 Pharmacists should explain that insulin is an effective means of improving glycemic control at any time during the course of type 2 diabetes; it should not be perceived as a last resort.47,56 Insulin pens should be considered for all appropri-ate patients.
Case 4: Insulin Therapy in Severe Insulin Resistance
James Smith is a 67-year-old white man who was diag-nosed with type 2 diabetes 10 years ago. He is 5’ 8” tall and weighs 308 lb (BMI ~47). His current daily insulin regi-
men—180 units of NPH insulin in the morning, 120 units of NPH insulin in the evening, and 25 units of regular insulin before each meal— provides a total of 375 units. Despite this regimen, James’s A1C has not dropped below 8.9%. You know that he has struggled to inject the appropriate volume each day because of the associated dis-comfort. He assumes that he is likely to die soon because he “needs to use so much insulin.”
James visits the pharmacy today with a prescription that reads: U-500 insulin regular Inject “30 units” SQ bid
James Smith’s other current medications include:• Lisinopril 20 mg daily.• Simvastatin 20 mg daily.• Gabapentin 300 mg three times daily.• Omeprazole 20 mg daily.• Paroxetine 20 mg daily.
The typical patient with type 2 diabetes who uses insulin requires a total daily dose of approximately 80 units.61 One of the conse-quences of the high prevalence of obesity among patients with type 2 diabetes is a growing number of patients with “severe insulin re-sistance” who require insulin doses in excess of 200 units per day to achieve glycemic control.61,62
The treatment of patients with such large daily insulin require-ments can be problematic.62,63 Injecting large volumes of insulin (e.g., 2 mL with a dose of 200 units of U-100 insulin) may cause considerable injection site discomfort.61,62 The volume of U-100 in-sulin needed often exceeds the capacity of the delivery device (1 mL maximum for U-100 syringes; 60 to 80 units maximum for insulin pens), necessitating multiple injections to deliver a single dose.61-63 Adherence inevitably suffers, resulting in poor glycemic control.62-64
U-500 insulin—a highly concentrated form of human regular insulin containing 500 units per milliliter (i.e., five times more
concentrated than U-100 insulin)—represents an attractive alter-native for patients with severe insulin resistance.65 It enables large doses of insulin to be administered in small volumes (e.g., 0.4 mL for a dose of 200 units).61,63 Although the cost per vial is considerably higher than the cost for U-100 insulin, the cost per unit ends up being substantially lower because of the smaller volumes required, the possibility of fewer injections per day, use of fewer syringes and supplies, and other savings.63,64,66 Patients who are switched from standard insulin to U-500 typically experience reductions in A1C of about 2% without significant hypoglycemia; the improvement in glycemic control is attributed to increased patient satisfaction and adherence.62-64,66
Diabetes expert Irl Hirsch, MD, has called U-500 insulin “perhaps the most important underused tool for the type 2 diabetes popula-tion.”65 The underuse he refers to appears to be changing: use of U-500 insulin increased by 137% from June 2007 to June 2009.62 Pharmacists who are not already seeing prescriptions for U-500 should anticipate encountering them.63
Although U-500 insulin is nonmodified regular insulin, its onset, peak, and duration of action are similar to NPH insulin.63,64,66 The dosing thus is similar to NPH, with up to four injections per day (including a bedtime dose when needed).61,63,64,66 The actual dose of U-500 insulin may be determined by adding up the total daily dose of U-100 insulin and dividing by 5; an initial dose reduction of 10% to 20% has been recommended by some experts, especially for patients with an A1C level <8%.62,64 The dose usually is titrated over the first few days and weeks.64
Pharmacists have an important opportunity to help patients and prescribers avoid errors with U-500 insulin. For example, ambiguity in the dosage and administration instructions could result in a five-fold overdosage or underdosage.62-64 In the case vignette that intro-duces this section, does “inject 30 units of U-500 insulin” mean that James Smith should draw up 30 actual units of U-500—or should he draw U-500 insulin up to the 30-unit mark on a U-100 syringe, corresponding to an actual insulin dose of 150 units?62 The dose ide-ally should be expressed in both volume and total units (e.g., “inject 0.3 mL (150 units) SQ twice daily”).63 The dosing instructions can be verified using a dose-equivalence chart such as the one presented in Table 3.62
As implied in the preceding paragraph, syringes are another pos-sible source of confusion and error. Standard insulin syringes are marked for U-100 insulin, so the dose of U-500 insulin does not correspond to the unit markings on the syringe.63,66 (U-500 insulin is not available in insulin pens.) Most published guidance advises using 0.3-mL, 0.5-mL, or tuberculin syringes instead of a 1-mL sy-ringe.61,63,64,66 However, tuberculin syringes may not be readily avail-able, and some insurers may not provide reimbursement for them (tuberculin syringes may not be viewed as diabetes supplies).63,66 If a U-100 syringe must be used, the pharmacist should take special care to explain the amount to be taken in both dose and volume terms, and preferably mark the appropriate level on the syringe.62,63,66 Pharmacists should teach all patients how to draw up the exact dose required by first demonstrating the amount to be measured and then having the patient practice drawing up the correct volume.63
The need for caution when using a highly concentrated insulin product should be apparent to pharmacists, especially if there is
Test Your Knowledge: Is the prescription for U-500 insulin a valid and appropriate intervention for James Smith? What potential problems (if any) are associated with the use of U-500 insulin?
?
Test Your Knowledge: Diabetes 11
any potential for patients to confuse it with U-100 regular insulin.65 Pharmacists should ensure that the patient, the patient’s family members, and any caregivers are aware that U-500 insulin is five times more concentrated than U-100 insulins.62,63 Patients should be warned that small changes in a dose of U-500 insulin have the potential to cause both greater shifts in blood glucose readings and prolonged, severe hypoglycemia.61,62 Doses of U-500 insulin should be adjusted only with the approval of the presciber.63
U-500 insulin is provided in 20-mL vials with the word ‘‘concen-trated’’ marked on them.61,63 To avoid the possibility of drug adminis-tration errors, U-500 insulin should be stored separately from U-100 insulin.61-64 This is of critical importance if any family members in the same household use U-100 insulin. Patients also should be aware of the possibility for mix-ups during transitions between care settings (e.g., when admitted to a hospital or long-term care facil-ity); adding the use of U-500 insulin to medical alert identification is one strategy for avoiding errors.62
Case 5: Controlling Nonglycemic Risk Factors Gail Burton is a 53-year-old African American woman
who was diagnosed with type 2 diabetes 3 years ago. Her A1C level is controlled to 6.7% on a combination of metformin 1,000 mg twice daily and exenatide 10 μg twice daily.
Through dedicated adherence to lifestyle modifications (and likely with assistance from the GLP-1 agonist), Gail has managed to reduce her weight from 211 lb to 182 lb and maintain it at that level. She is 5’ 7” tall (BMI ~29).
Gail visits the pharmacy to take advantage of a cholesterol and blood pressure screening event you are offering in conjunction with National Cholesterol Education Month. Results show her blood pres-sure to be 172/100 mm Hg and the following lipid levels:
• Total cholesterol: 280 mg/dL.• Low-density lipoprotein cholesterol: 200 mg/dL.• High-density lipoprotein cholesterol: 35 mg/dL.• Triglycerides: 225 mg/dL.Gail is surprised by these results. “I feel really good, I’ve lost
weight, I don’t smoke, and I’ve worked hard to get my diabetes un-der control,” she says with frustration. “Why am I having these other problems?” As you talk with Gail, you discover that her primary care provider had prescribed both simvastatin and lisinopril at her last visit approximately 10 months ago. Gail elected not to fill those pre-scriptions because, as she explains, “I’m not a really sick person—I don’t need to be taking all these medications.” You question Gail about other aspects of care and find out that she has never been vaccinated against either influenza or pneumococcal pneumonia.
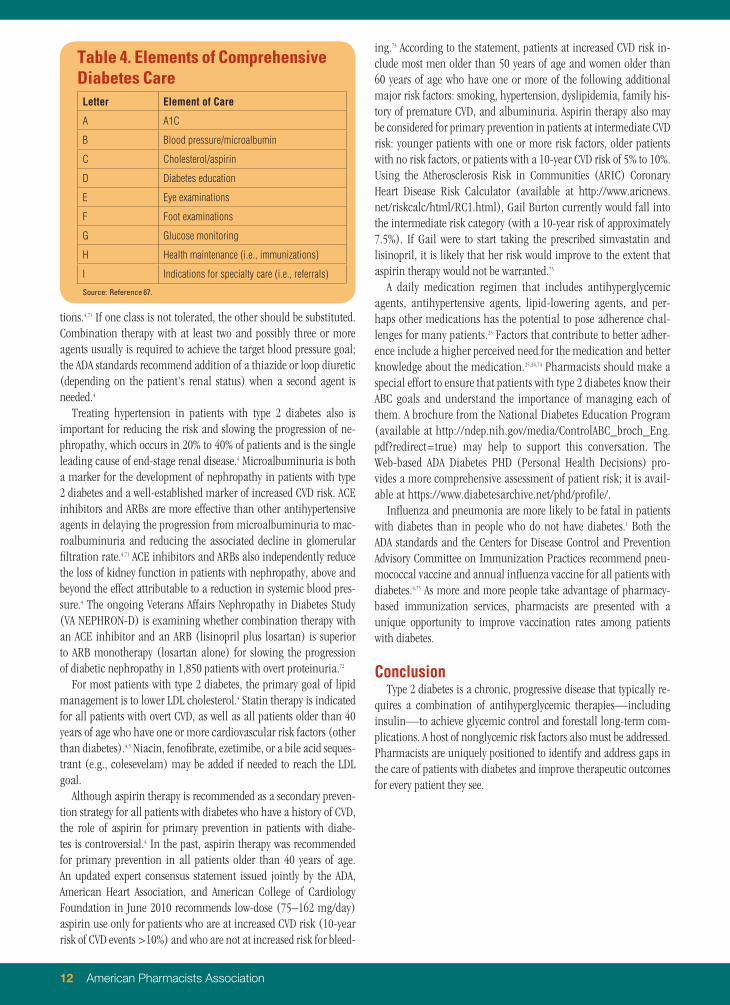
Patients such as Gail Burton must appreciate that the man-agement of type 2 diabetes involves much more than controlling hyperglycemia. Many pharmacists already are familiar with the “ABCs” of diabetes, which correspond to goals for A1C, blood pres-sure (<130/80 mm Hg), and LDL cholesterol (<100 mg/dL).67 An extended alphabet mnemonic (Table 4) can help pharmacists recall additional elements of comprehensive diabetes management.67
Attainment of nonglycemic goals for diabetes management re-mains disappointingly low. Using National Health and Nutrition Ex-amination Survey data from 1999 to 2006, Cheung and colleagues found that only 57.1% of participants with diagnosed diabetes had achieved the target A1C level <7%, 45.5% had achieved the target blood pressure, and 46.5% had achieved the target LDL cholesterol level.68 Only 12.2% of participants—one in eight—had attained all three targets. In a recent analysis of Medical Expenditure Panel Sur-vey data from 2005, more than 40% of the study population (2,003 adults with diagnosed diabetes) had not received a flu shot within the previous year.69
Effective long-term blood pressure control may be the most im-portant intervention for preventing complications in patients with diabetes.24,70 The ADA Standards of Medical Care in Diabetes call for blood pressure to be measured at every routine diabetes visit.4 When hypertension is present, the treatment regimen should include either an angiotensin-converting enzyme (ACE) inhibitor or an angio-tensin II receptor blocker (ARB) in addition to lifestyle modifica-
Table 3. Dosing Conversion Table and Formulas for Dose and Syringe Markingsa
U-500 Insulin Dose (Actual Units)
U-100 Syringe (Unit Markings)
Volume for Tuberculin Syringe (mL)
25 5 0.05
50 10 0.10
75 15 0.15
100 20 0.20
125 25 0.25
150 30 0.30
175 35 0.35
200 40 0.40
225 45 0.45
250 50 0.50
275 55 0.55
300 60 0.60
325 65 0.65
350 70 0.70
375 75 0.75
400 80 0.80
425 85 0.85
450 90 0.90
475 95 0.95
500 100 1.00
aThe following dosing formulas also may be used: dose (actual units) x 0.2 = unit markings in a U-100 insulin syringe; dose (actual units) x 0.002 = volume (mL) in a tuberculin syringe.
Test Your Knowledge: What nonglycemic elements of diabetes care are appropriate and important for Gail Burton??
12 American Pharmacists Association
tions.4,71 If one class is not tolerated, the other should be substituted. Combination therapy with at least two and possibly three or more agents usually is required to achieve the target blood pressure goal; the ADA standards recommend addition of a thiazide or loop diuretic (depending on the patient’s renal status) when a second agent is needed.4
Treating hypertension in patients with type 2 diabetes also is important for reducing the risk and slowing the progression of ne-phropathy, which occurs in 20% to 40% of patients and is the single leading cause of end-stage renal disease.4 Microalbuminuria is both a marker for the development of nephropathy in patients with type 2 diabetes and a well-established marker of increased CVD risk. ACE inhibitors and ARBs are more effective than other antihypertensive agents in delaying the progression from microalbuminuria to mac-roalbuminuria and reducing the associated decline in glomerular filtration rate.4,71 ACE inhibitors and ARBs also independently reduce the loss of kidney function in patients with nephropathy, above and beyond the effect attributable to a reduction in systemic blood pres-sure.4 The ongoing Veterans Affairs Nephropathy in Diabetes Study (VA NEPHRON-D) is examining whether combination therapy with an ACE inhibitor and an ARB (lisinopril plus losartan) is superior to ARB monotherapy (losartan alone) for slowing the progression of diabetic nephropathy in 1,850 patients with overt proteinuria.72
For most patients with type 2 diabetes, the primary goal of lipid management is to lower LDL cholesterol.4 Statin therapy is indicated for all patients with overt CVD, as well as all patients older than 40 years of age who have one or more cardiovascular risk factors (other than diabetes).4,5 Niacin, fenofibrate, ezetimibe, or a bile acid seques-trant (e.g., colesevelam) may be added if needed to reach the LDL goal.
Although aspirin therapy is recommended as a secondary preven-tion strategy for all patients with diabetes who have a history of CVD, the role of aspirin for primary prevention in patients with diabe-tes is controversial.4 In the past, aspirin therapy was recommended for primary prevention in all patients older than 40 years of age. An updated expert consensus statement issued jointly by the ADA, American Heart Association, and American College of Cardiology Foundation in June 2010 recommends low-dose (75–162 mg/day) aspirin use only for patients who are at increased CVD risk (10-year risk of CVD events >10%) and who are not at increased risk for bleed-
ing.73 According to the statement, patients at increased CVD risk in-clude most men older than 50 years of age and women older than 60 years of age who have one or more of the following additional major risk factors: smoking, hypertension, dyslipidemia, family his-tory of premature CVD, and albuminuria. Aspirin therapy also may be considered for primary prevention in patients at intermediate CVD risk: younger patients with one or more risk factors, older patients with no risk factors, or patients with a 10-year CVD risk of 5% to 10%. Using the Atherosclerosis Risk in Communities (ARIC) Coronary Heart Disease Risk Calculator (available at http://www.aricnews.net/riskcalc/html/RC1.html), Gail Burton currently would fall into the intermediate risk category (with a 10-year risk of approximately 7.5%). If Gail were to start taking the prescribed simvastatin and lisinopril, it is likely that her risk would improve to the extent that aspirin therapy would not be warranted.73
A daily medication regimen that includes antihyperglycemic agents, antihypertensive agents, lipid-lowering agents, and per-haps other medications has the potential to pose adherence chal-lenges for many patients.25 Factors that contribute to better adher-ence include a higher perceived need for the medication and better knowledge about the medication.25,34,74 Pharmacists should make a special effort to ensure that patients with type 2 diabetes know their ABC goals and understand the importance of managing each of them. A brochure from the National Diabetes Education Program (available at http://ndep.nih.gov/media/ControlABC_broch_Eng.pdf?redirect=true) may help to support this conversation. The Web-based ADA Diabetes PHD (Personal Health Decisions) pro-vides a more comprehensive assessment of patient risk; it is avail-able at https://www.diabetesarchive.net/phd/profile/.
Influenza and pneumonia are more likely to be fatal in patients with diabetes than in people who do not have diabetes.1 Both the ADA standards and the Centers for Disease Control and Prevention Advisory Committee on Immunization Practices recommend pneu-mococcal vaccine and annual influenza vaccine for all patients with diabetes.4,75 As more and more people take advantage of pharmacy-based immunization services, pharmacists are presented with a unique opportunity to improve vaccination rates among patients with diabetes.
ConclusionType 2 diabetes is a chronic, progressive disease that typically re-
quires a combination of antihyperglycemic therapies—including insulin—to achieve glycemic control and forestall long-term com-plications. A host of nonglycemic risk factors also must be addressed. Pharmacists are uniquely positioned to identify and address gaps in the care of patients with diabetes and improve therapeutic outcomes for every patient they see.
Table 4. Elements of Comprehensive Diabetes CareLetter Element of Care
A A1C
B Blood pressure/microalbumin
C Cholesterol/aspirin
D Diabetes education
E Eye examinations
F Foot examinations
G Glucose monitoring
H Health maintenance (i.e., immunizations)
I Indications for specialty care (i.e., referrals)
Source: Reference 67.
Test Your Knowledge: Diabetes 13
References
1. Centers for Disease Control and Prevention. National Diabetes Fact Sheet, 2007. Available at: http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2007.pdf. Accessed September 12, 2010.
2. National Diabetes Statistics, 2007. National Diabetes Information Clear-inghouse Web site. June 2008. Available at: http://diabetes.niddk.nih.gov/dm/pubs/statistics/index.htm. Accessed September 12, 2010.
3. Burant CF, ed. Medical Management of Type 2 Diabetes. 6th ed. Alexan-dria, VA: American Diabetes Association; 2008.
4. American Diabetes Association. Standards of medical care in diabetes–2010. Diabetes Care. 2010;33(suppl 1):S11–61.
5. National Cholesterol Education Program. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Bethesda, MD: National Institutes of Health; 2002. NIH Publication 02-5215. Available at: http://www.nhlbi.nih.gov/guidelines/cholesterol/atp3_rpt.htm. Accessed September 12, 2010.
6. The facts about diabetes: America’s seventh leading cause of death. National Diabetes Education Program Web site. Available at: http://ndep.nih.gov/diabetes-facts/index.aspx#linkedtodiabetes. Accessed September 12, 2010.
7. Diabetes myths. American Diabetes Association Web site. Available at: http://www.diabetes.org/diabetes-basics/diabetes-myths/. Accessed September 12, 2010.
8. Diabetes statistics. American Diabetes Association Web site. Available at: http://www.diabetes.org/diabetes-basics/diabetes-statistics/. Accessed September 12, 2010.
9. Fraze T, Jiang J, Burgess J. Hospital stays for patients with diabetes, 2008. Healthcare Cost and Utilization Project Statistical Brief #93. Rockville, MD: Agency for Healthcare Research and Quality; August 2010. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb93.pdf. Accessed September 12, 2010.
10. Del Prato S, Penno G, Miccoli R. Changing the treatment paradigm for type 2 diabetes. Diabetes Care. 2009;32(suppl 2):S217–22.
11. Campbell RK. Fate of the beta-cell in the pathophysiology of type 2 diabetes. J Am Pharm Assoc. 2009;49(suppl 1):S10–5.
12. DeFronzo RA. Overview of newer agents: where treatment is going. Am J Med. 2010;123(suppl):S38–48.
13. DeFronzo RA. From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus [Banting Lecture]. Diabetes. 2009;58:773–95.
14. UK Prospective Diabetes Study Group. UK prospective diabetes study 16. Overview of 6 years’ therapy of type II diabetes: a progressive disease. Diabetes. 1995;44:1249–58.
15. Bagust A, Beale S. Deteriorating beta-cell function in type 2 diabetes: a long-term model. QJM. 2003;96:281–8.
16. Davis SN, Renda SM. Treating to target in type 2 diabetes: a case presenta-tion. Diabetes Educ. 2006;32(suppl 4):137S–45S.
17. Unger J, Parkin CG. Type 2 diabetes: an expanded view of pathophysiology and treatment. Postgrad Med. 2010;122:145–57.
18. Skyler JS, Bergenstal R, Bonow RO, et al. Intensive glycemic control and the prevention of cardiovascular events: implications of the ACCORD, ADVANCE, and VA diabetes trials: a position statement of the American Diabetes Associa-tion and a scientific statement of the American College of Cardiology Foun-dation and the American Heart Association. Diabetes Care. 2009;32:187–92.
19. Ohkubo Y, Kishikawa H, Araki E, et al. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: a randomized prospective 6-year study. Diabetes Res Clin Pract. 1995;28:103–17.
20. UK Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352:837–53.
21. UK Prospective Diabetes Study Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet. 1998;352:854–65.
22. Jellinger PS, Davidson JA, Blonde L, et al.; ACE/AACE Diabetes Road Map Task Force. Road maps to achieve glycemic control in type 2 diabetes mellitus. Endocr Pract. 2007;13:260–8.
23. Rodbard HW, Jellinger PS, Davidson JA, et al. Statement by an American Association of Clinical Endocrinologists/American College of Endocri-nology consensus panel on type 2 diabetes mellitus: an algorithm for glycemic control. Endocr Pract. 2009;15:540–59.
24. Vijan S. Type 2 diabetes. Ann Intern Med. 2010;152:ITC3-1–15.
25. Kogan AJ. Overcoming obstacles to effective care of type 2 diabetes. Am J Manag Care. 2009;15:S265–2.
26. Brunton S. Implementing treatment guidelines for type 2 diabetes in primary care. Postgrad Med. 2009;121:125–38.
27. Sherifali D, Nerenberg K, Pullenayegum E, et al. The effect of oral antidiabetic agents on A1C levels: a systematic review and meta-analysis. Diabetes Care. 2010;33:1859–64.
28. Gavin JR III, Bohannon NJ. A review of the response to oral antidiabetes agents in patients with type 2 diabetes. Postgrad Med. 2010;122:43–51.
29. Turner RC, Cull CA, Frighi V, et al. Glycemic control with diet, sulfonyl-urea, metformin, or insulin in patients with type 2 diabetes mellitus: progressive requirement for multiple therapies (UKPDS 49). JAMA. 1999;281:2005–12.
30. Campbell RK. Type 2 diabetes: where we are today: an overview of disease burden, current treatments, and treatment strategies. J Am Pharm Assoc. 2009;49(suppl 1):S3–9.
31. Blonde L. Current antihyperglycemic treatment guidelines and algorithms for patients with type 2 diabetes mellitus. Am J Med. 2010;123:S12–8.
32. Phung OJ, Scholle JM, Talwar M, et al. Effect of noninsulin antidiabetic drugs added to metformin therapy on glycemic control, weight gain, and hypoglycemia in type 2 diabetes. JAMA. 2010;303:1410–8.
33. Nathan DM, Buse JB, Davidson MB, et al. Medical management of hyper-glycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy. A consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2009;32:193–203.
34. Cobble ME, Peters AL. Clinical practice in type 2 diabetes: after metformin and lifestyle, then what? J Fam Pract. 2009;58(11 suppl):S7–14.
35. Gerstein HC, Miller ME, Byington RP, et al.; Action to Control Cardiovas-cular Risk in Diabetes Study Group. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358:2545–59.
36. Patel A, MacMahon S, Chalmers J, et al.; ADVANCE Collaborative Group. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358:2560–72.
37. Duckworth W, Abraira C, Moritz T, et al.; VADT Investigators. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med. 2009;360:129–39.
38. Sarpong E, Miller GE. Trends in the pharmaceutical treatment of diabetes: a comparison of utilization and expenditures, 1997 to 2007. Medical Expenditure Panel Survey Statistical Brief #293. Rockville, MD: Agency for Healthcare Research and Quality; September 2010. Available at: http://www.meps.ahrq.gov/mepsweb/data_files/publications/st293/stat293.shtml. Accessed September 28, 2010.
14 American Pharmacists Association
39. Kramer H, Cao G, Dugas L, et al. Increasing BMI and waist circumference and prevalence of obesity among adults with type 2 diabetes: the National Health and Nutrition Examination Surveys. J Diabetes Complications. 2009 Nov 13. [Epub ahead of print]
40. Look AHEAD Research Group. Reduction in weight and cardiovascular disease risk factors in individuals with type 2 diabetes: one-year results of the Look AHEAD trial. Diabetes Care. 2007;30:1374–83.
41. Klein S, Sheard NF, Pi-Sunyer X, et al.; American Diabetes Association; North American Association for the Study of Obesity; American Society for Clinical Nutrition. Weight management through lifestyle modification for the prevention and management of type 2 diabetes: rationale and strategies: a statement of the American Diabetes Association, the North American Association for the Study of Obesity, and the American Society for Clinical Nutrition. Diabetes Care. 2004;27:2067–73.
42. American Diabetes Association statement on blood glucose lowering drugs. American Diabetes Association Web site. June 30, 2010. Available at: http://www.diabetes.org/for-media/2010/american-diabetes-association-blood-glucose-lowering-drugs.html. Accessed September 12, 2010.
43. Rodbard HW, Jellinger PS. Adding noninsulin antidiabetic drugs to metformin therapy for type 2 diabetes [letter]. JAMA. 2010;304:405–6; author reply 406–7.
44. American Diabetes Association. Economic costs of diabetes in the U.S. in 2007. Diabetes Care. 2008;31:596–615.
45. Halperin F, Ingelfinger JR, McMahon GT. Clinical decisions. Management of type 2 diabetes—polling results. N Engl J Med. 2008;358:e8.
46. Kuritzky L, Epstein BJ, Lavernia F. How to obtain appropriate type 2 diabetes control in the first 180 days of treatment initiation. Postgrad Med. 2010;122:33–42.
47. Berger JE, Ahmann AJ, Balfour DC, et al. Treating to target: implementing an effective diabetes care paradigm for managed care. Am J Manag Care. 2010;16(suppl treating):S4–35.
48. Brown JB, Nichols GA, Perry A. The burden of treatment failure in type 2 diabetes. Diabetes Care. 2004; 27:1535–40.
49. Schwartz KL, Monsur J, Hammad A, et al. Comparison of point of care and laboratory HbA1c analysis: a MetroNet study. J Am Board Fam Med. 2009;22:461–3.
50. Nauck MA, Vilsbøll T, Gallwitz B, et al. Incretin-based therapies: viewpoints on the way to consensus. Diabetes Care. 2009;32(suppl 2): S223–31.
51. Drab S. Translating clinical guidelines into clinical practice: role of the pharmacist in type 2 diabetes management. J Am Pharm Assoc. 2009;49:e152–62.
52. Rubino A, McQuay LJ, Gough SC, et al. Delayed initiation of subcutane-ous insulin therapy after failure of oral glucose-lowering agents in patients with type 2 diabetes: a population-based analysis in the UK. Diabet Med. 2007;24:1412–8.
53. Peyrot M, Rubin RR, Lauritzen T, et al. Resistance to insulin therapy among patients and providers: results of the cross-national Diabetes Attitudes, Wishes, and Needs (DAWN) study. Diabetes Care. 2005;28:2673–9.
54. Peyrot M, Rubin RR, Khunti K. Addressing barriers to initiation of insulin in patients with type 2 diabetes. Prim Care Diabetes. 2010;4(suppl 1): S11–8.
55. Polonsky WH, Fisher L, Guzman S, et al. Psychological insulin resistance in patients with type 2 diabetes: the scope of the problem. Diabetes Care. 2005;28:2543–5.
56. Davis SN, Renda SM. Psychological insulin resistance: overcoming barriers to starting insulin therapy. Diabetes Educ. 2006;32(suppl 4): 146S–52S.
57. LaSalle JR. Empowering patients during insulin initiation: a real-world approach. J Am Osteopath Assoc. 2010;110:69–78.
58. Goldstein HH. Pen devices to improve patient adherence with insulin therapy in type 2 diabetes. Postgrad Med. 2008;120:172–9.
59. McCoy EK, Wright BM. A review of insulin pen devices. Postgrad Med. 2010;122:81–8.
60. Nakar S, Yitzhaki G, Rosenberg R, et al. Transition to insulin in type 2 diabetes: family physicians’ misconception of patients’ fears contributes to existing barriers. J Diabetes Complications. 2007;21:220–6.
61. Crasto W, Jarvis J, Hackett E, et al. Insulin U-500 in severe insulin resis-tance in type 2 diabetes mellitus. Postgrad Med J. 2009;85:219–22.
62. Segal AR, Brunner JE, Burch FT, et al. Use of concentrated insulin human regular (U-500) for patients with diabetes. Am J Health Syst Pharm. 2010;67:1526–35.
63. Clark A. U-500 insulin: not for ordinary use. US Pharm. 2010;35(diabetes suppl):14–7. Available at: http://www.uspharmacist.com/content/s/126/c/20822/. Accessed September 12, 2010.
64. Garg R, Johnston V, McNally PG, et al. U-500 insulin: why, when and how to use in clinical practice. Diabetes Metab Res Rev. 2007;23:265–8.
65. Hirsch IB. Intensifying insulin therapy in patients with type 2 diabetes mellitus. Am J Med. 2005;118(5A):21S–6S.
66. Cochran E, Musso C, Gorden P. The use of U-500 in patients with extreme insulin resistance. Diabetes Care. 2005;28:1240–4.
67. Abbate SL. Expanded ABCs of diabetes. Clin Diabetes. 2003;21:128–33.
68. Cheung BMY, Ong KL, Cherny SS, et al. Diabetes prevalence and thera-peutic target achievement in the United States, 1999 to 2006. Am J Med. 2009;122:443–53.
69. Wang J, Thomas J, Byrd D, et al. Status of diabetes care among commu-nity pharmacy patients with diabetes: analysis of the Medical Expenditure Panel Survey. J Am Pharm Assoc. 2010;50:478–84.
70. Holman RR, Paul SK, Bethel MA, et al. 10-Year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359:1577–89.
71. Chobanian AV, Bakris GL, Black HR, et al.; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Bethesda, MD: National Institutes of Health; 2004. NIH Publication 04-5230. Available at: http://www.nhlbi.nih.gov/guidelines/hypertension/jnc7full.pdf. Accessed September 12, 2010.
72. Fried LF, Duckworth W, Zhang JH, et al.; VA NEPHRON-D Investigators. Design of combination angiotensin receptor blocker and angiotensin-converting enzyme inhibitor for treatment of diabetic nephropathy (VA NEPHRON-D). Clin J Am Soc Nephrol. 2009;4:361–8.
73. Pignone M, Alberts MJ, Colwell JA, et al.; American Diabetes Association; American Heart Association; American College of Cardiology Foundation. Aspirin for primary prevention of cardiovascular events in people with diabetes. J Am Coll Cardiol. 2010;55:2878–86.
74. McHorney CA, Gadkari AS. Individual patients hold different beliefs to prescription medications to which they persist vs nonpersist and persist vs nonfulfill. Patient Prefer Adherence. 2010;4:187–95.
75. Centers for Disease Control and Prevention. Recommended adult im-munization schedule—United States, 2010. January 15, 2010. Available at: http://www.cdc.gov/mmwr/PDF/wk/mm5901-Immunization.pdf. Accessed September 12, 2010.
Test Your Knowledge: Diabetes 15
Test Your Knowledge:DiabetesCPE Exam
Instructions: The assessment questions printed below allow you to preview the online CPE exam. Please review all of your answers to be sure you have marked the proper letter on the online CPE exam. There is only one correct answer to each question.
1. Approximately what percentage of adults in the United States with diabetes has type 2 diabetes?a. 30%. b. 50%.
2. Cardiovascular disease is the cause of death in what percentage of patients with type 2 diabetes?a. 33%.b. 50%.
3. Which of the following are considered to be the dual defects that characterize type 2 diabetes?a. Impaired β-cell function and insulin resistance.b. Glucagon hypersecretion and reduced incretin
secretion.c. Peripheral and central insulin resistance.d. Increased lipolysis and impaired β-cell function.
4. What percentage of β-cell function is lost by the time type 2 diabetes is diagnosed? a. 10%.b. 18%.
5. The American Diabetes Association (ADA) recommends an A1C goal of _____%, while the American College of Endocrinology (ACE) and the American Association of Clinical Endocrinologists (AACE) recommend an A1C goal of _____%.a. <8.0; ≤7.0.b. <7.0; ≤6.5.
6. In general, most oral antihyperglycemic agents are able to decrease A1C levels by an average maximum of:a. 0.5%.b. 1.0%.
7. Which of the following statements is true?a. Patients with type 2 diabetes are unlikely to
require insulin therapy if they are adherent to oral antihyperglycemic therapy.
b. Intensive glycemic control is an effective intervention for reducing the risk of cardiovascular events.
c. Sulfonylureas are the most potent glucose-lowering agents available.
d. Aggressive treatment of hypertension and dyslipidemias is an important aspect of type 2 diabetes management.
8. In the ADA/European Association for the Study of Diabetes (EASD) algorithm, what is the preferred initial therapy for newly diagnosed patients with type 2 diabetes?
a. Lifestyle interventions alone.b. Lifestyle interventions + metformin.c. Lifestyle interventions + a sulfonylurea.d. Lifestyle interventions + basal insulin.
9. In the AACE/ACE algorithm, which of the following agents is not recommended for initial antihyperglycemic therapy in a patient with an A1C level of 7.2%?
a. Metformin.b. A sulfonylurea.c. A dipeptidyl peptidase-4 (DPP-4) inhibitor.d. A thiazolidinedione.
10. In the AACE/ACE algorithm, which of the following regimens would be preferred for initial therapy in a patient with an A1C level of 8.9%? a. Metformin monotherapy.b. Metformin + a sulfonylurea.c. Metformin + a glucagon-like peptide-1 (GLP-1)
agonist.d. Insulin alone or with other agents.
11. Which of the following triple medication regimens is advocated by DeFronzo for early treatment of the pathogenic abnormalities of type 2 diabetes?a. Metformin, a thiazolidinedione, and a GLP-1 agonist.b. Metformin, a thiazolidinedione, and a DPP-4 inhibitor.c. Metformin, a sulfonylurea, and a thiazolidinedione.d. Metformin, a sulfonylurea, and a GLP-1 agonist.
12. According to the ADA/EASD and AACE/ACE algorithms, how frequently should the therapeutic regimen for patients with type 2 diabetes be evaluated?a. Every 2 to 3 months.b. Every 6 months.c. Annually.d. Whenever the patient experiences symptoms of
hyperglycemia.
c. 70%.d. 90%.
c. 66%.d. 75%.
c. 35%.d. 50%.
c. <6.5; ≤7.0.d. <6.0; ≤6.5.
c. 1.25%.d. 2.0%.
13. In the ADA/EASD algorithm, which of the following options is recommended when therapy needs to be intensified in a patient with an A1C level >8.5%?a. Increase the dose of metformin.b. Add basal insulin to lifestyle interventions +
metformin.c. Add a GLP-1 agonist to lifestyle interventions +
metformin.d. Add a sulfonylurea to lifestyle interventions +
metformin.
14. A patient with type 2 diabetes has an A1C level of 7.4% despite therapy consisting of lifestyle modifications and metformin. In the AACE/ACE algorithm, what is the preferred second component of dual pharmacotherapy for this patient?a. A GLP-1 agonist.b. A meglitinide.
15. A man with type 2 diabetes needs to have insulin added to the treatment regimen to improve glycemic control. With some embarrassment, he admits that he is afraid of needles. Which of the following interventions is most likely to address his concern effectively?a. Ask him if a family member or friend could assist him
in administering the injections.b. Assure him that insulin will improve his symptoms and
make him feel better.c. Recommend a long-acting insulin that only needs to be
administered at bedtime.d. Suggest that he try using an insulin pen device.
16. Pharmacists might help patients to overcome “psychological insulin resistance” by:a. Empowering patients—explaining that they are
unlikely to need insulin if they make all of the recommended lifestyle modifications.
b. Introducing the possibility of insulin use when patients are first diagnosed with type 2 diabetes.
c. Reassuring patients that insulin therapy is introduced only as a last resort and therefore would not be a concern for many years.
d. Referring patients to a mental health professional.
17. Tom Rogers has a current total daily insulin dose of 250 units. His most recent A1C level was 7.8%. Tom’s primary care provider wants to switch him to U-500 insulin and calculates an initial total dose of 200 units. If twice daily dosing is desired, which U-100 syringe marking should Tom use to measure each dose? a. 20.b. 25.
18. Approximately what percentage of adults with type 2 diabetes currently achieves the recommended goals for A1C, blood pressure, and cholesterol?a. 12%.b. 21%.
19. A patient with type 2 diabetes has a blood pressure reading of 137/85 mm Hg. Which of the following options represents a recommended course of action?a. Do nothing—this reading is below the goal of
140/90 mm Hg.b. Initiate antihypertensive therapy with a thiazide
diuretic.c. Initiate antihypertensive therapy with an angiotensin-
converting enzyme inhibitor.d. Initiate antihypertensive therapy with a calcium-
channel blocker.
20. In addition to an annual influenza vaccine, which of the following vaccines is recommended for all patients with type 2 diabetes?a. Hepatitis B.b. Human papillomavirus.c. Meningococcal.d. Pneumococcal.
c. A sulfonylurea.d. A thiazolidinedione.
c. 40.d. 50.
c. 33%.d. 45%.
CPE Instructions Completing a posttest at www.pharmacist.com/education is as easy as 1-2-3…
1. Go to Online CPE Quick List and click on the title of this activity.2. Log in. APhA members enter your user name and password. Not an APhA member? Just click “Create one now” to open an account.
No fee is required to register.3. Successfully complete the CPE exam and evaluation form to gain immediate access to your Statement of Credit.
Live step-by-step assistance is available Monday through Friday, 8:30 am to 5:00 pm ET from APhA Member Services at 800-237-APhA (2742) or e-mail [email protected].
American Pharmacists Association • 2215 Constitution Avenue, NW • Washington, DC 20037 • 800-237-APhA • www.pharmacist.com