The Low Energy Neurofeedback System(LENS) is an EEG biofeedback system used inclinical applications and research in the treat-ment of central nervous system functioning. Itis unique in the field of neurofeedback in thatinstead of only displaying information on acomputer screen to assist the patient in condi-tioninghealthierbrainwave patterns, the LENSuses weak electromagnetic signals as a carrierwave for the feedback to assist in reorganizingbrain physiology. The following describes therationalefor theLENSsystem,aswellassubse-quent discoveries. Also presented are somesuggestions for future research and practicalapplication of the LENS technology.
Evolution of LENS and Relevant Concepts
The major implication of this paper is thatboth the physically and psychologically trau-matized brain has demonstrated vastly greatercapacity for recovery than has previously beenappreciated. Secondarily, the LENS appears tohelp the traumatized person achieve clearly in-creased performance in relatively short periodsof time, with a quite non-invasive, low technol-ogy procedure. On the other hand, other kindsof EEG biofeedback may be just as effective asthe LENS under some conditions. Although noclaims are being made here that the LENS isbetter than any other form of treatment, it is,however quite different from other neuro-feedback modalities, as well as from other
Len Ochs is affiliated with Ochs Labs, Sebastopol, CA.Address correspondence to: Len Ochs, 8151 Elphick Lane, Sebastopol, CA 94596 (E-mail: lochs@earthlink.
net).
[Haworth co-indexing entry note]: “The Low Energy Neurofeedback System (LENS): Theory, Background, and Introduction.” Ochs, Len.Co-published simultaneously in Journal of Neurotherapy (The Haworth Medical Press, an imprint of The Haworth Press, Inc.) Vol. 10, No. 2/3,2006, pp. 5-39; and: LENS: The Low Energy Neurofeedback System (ed: D. Corydon Hammond) The Haworth Medical Press, an imprint of TheHaworth Press, Inc., 2006, pp. 5-39. Single or multiple copies of this article are available for a fee from The Haworth Document Delivery Service[1-800-HAWORTH, 9:00 a.m. - 5:00 p.m. (EST). E-mail address: [email protected]].
neurostimulation techniques such as audio/vi-sual stimulation and particularly transcranialmagnetic stimulation, where the intensitiesused are thousands of times stronger thanLENS uses. Lastly, there appears to be no basicscienceyet revealed tohelpunderstand thephe-nomena described here, thus creating a newareaofinquiryintheneuro-behavioralsciences.
Thefollowingsectionispresentedforhistor-ical purposes to outline the order and context inwhich the significant components in the devel-opment of the LENS were observed including:a description of the instrumentation; the meansof measuring and controlling the feedback in-tensity; the problems and benefits observed inthe development of this system; and treatmentmanagement problems and how they evolved,particularly with regard to different popula-tions.
History. During the summer of 1990, HaroldL. Russell, PhD of Galveston, Texas, tele-phoned Len Ochs, PhD in Concord, California.He asked Ochs to develop a device which pro-vided fixed-frequency photic stimulation. Hisinterest was based upon the work of Marion Di-amond,PhD(1988) inherworkontheeffectsofenvironmental stimulation on cortical com-plexity in rats. Russell (Carter & Russell, 1981,1984, 1993) had experimented with exposingschool children with performance problemsand high inter-test variability to daily, 20-min-ute repeated cycles of 10 Hz, for one minute,then 18 Hz for a minute, for six weeks. Russellused bright red flashing lights inside impro-vised welder’s goggles. His idea was to use theflashing lights to stimulate the brains of theschool children.
It was my impression that any simple fixed-frequency stimulation would be an inefficientway to provide the desired stimulation to alterbrainwave activity. The degree to which a per-son’s EEG (electroencephalographic activity)is influenced by external (e.g., photic) stimula-tion depends on many factors, including theirdominant brainwave frequency from moment-to-moment, and the intensity and frequency ofthe stimulus used. Although the intensity andfrequency of a fixed stimulation frequencycould influence the EEG, another factor thatmight have bearing on entrainability of theEEG is the size of the difference, at any mo-ment, between the stimulation frequency and
the predominant energy of the EEG, in whichlies the dominant frequency. The dominant fre-quency is the frequency at that momentat a spoton the person’s head which is stronger than anyother frequency. With that as a hypothesis, itseemed appropriate to suggest that a treatmentapproach might be to tie the stimulation fre-quencytothedominant,orpeak,EEGfrequency.
Since from 1 in 4,000 children and about 1 in20,000 adults are estimated to be photosensi-tive (Quirk et al., 1995), and thus vulnerable toexperiencing a seizure with photic stimulation,this could occasionally present severe prob-lems. Photo-hypersensitivity refers to the reac-tivity to light that is strong enough to elicit con-vulsions–whether the person is epileptic or not.If, for instance, the person were to have a sei-zure–whether from epilepsy or the stimulationevoking a photohypersensitive seizure–the fre-quency of that seizure would become the domi-nant frequency.Inotherwords, if thestimulationfrequency equaled the dominant frequency, thestimulationwouldfurtherstimulateanypre-ex-isting seizure. Fortunately this could be dealtwith easily by programming the software toprevent the software from ever being equal tothe dominant frequency. An example of how todo this was to define the stimulation frequencyas some percentage of the dominant frequency.It was anticipated that this strategywould beginto displace and disperse some of the energy ofany seizure activity to other non-seizure brain-wave frequencies. Fortunately, setting the stim-ulation frequency to some percentage greaterthan 100% of the dominant EEG might satisfythose in the neurofeedback community (Lubar,1985) advocating for increasing EEG frequen-cies for enhanced cognitive control. Further,using a percentage less than 100% of the domi-nant frequency might satisfy those advocatingdecreasing EEG frequencies for enhancingemotional integrity and decreasing chemicaldependence (Peniston & Kulkosky, 1991).Russell agreed to pay for the programming ofthe original software according to this concep-tion. Hence, the software was programmed intodevices that would be called electroencephal-ographic entrainment feedback (EEF).
The original EEF software was designed tolink together the J&J I-330 EEG module 201(and afterward the J&J I-400), and the SyneticSystems Synergizer (Seattle, Washington), a
6 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
light-and-sound generation device which fit in-side an IBM-clone computer through softwareknow as BOS, a DOS-based interpreted plat-form developed by William Stuart, of Bain-bridge Island, Washington. As originally con-ceived, the software was to allow the Synergizercard to set the flash frequency of the lights in-side some welder-type goggles, and to continu-ouslyreset theirspeedas thedominantEEGfre-quency of the person’s brain changed on amoment-to-moment basis. The software alsoset and reset the frequency of binaural auditorytones coming through ear phones, in the sameway it set the light frequency. The feedbackmight pulsate at 105% of the dominant fre-quency during one 10-second period, then 95%of the dominant frequency during the next, andalternate between the two conditions. The soft-ware never let the flash frequency equal thedominant frequency.
The initial system, funded by Russell’s AVSgroup, involved many features that have nowbeen discarded, while the current software nowincludes many features that were not yet con-ceived. Discarded features central to the origi-nal conception were: the necessary use of visi-ble light feedback, the use of sound feedback,the use of fixed time limits for changingoffsets,the use of the same size offsets from the domi-nant frequency, thenecessary use of offsets, thenecessary use of alternating offsets, and thenecessary use of offsets of arbitrary sizes.
New features include the generation of thefeedback signal from within the EEG (the elec-troencephalograph) device itself, as well as theability to control the feedback, using the J&JI-330 C2 family of EEGs. The use of the J&JI-330 C2 permitted the portable use of the sys-tem from a suitable desktop or notebookcomputer.
It is important to note that there were manytechnical inadequacies of the first generationEEF system. Yet the results from this techni-cally“inadequate”systemappeared tobebetterthan any other treatment for closed-headtrauma. Interestingly, the results were not quiteas good when the more technically sophisti-cated second generation system was intro-duced. This led those involved to try to dupli-cate some of the inadequacies of the originalsystem. The major required change was to re-tard the feedback, which was produced much
more rapidly in the replacement unit for theI-330 C2. We had to introduce a time lag be-tween the occurrence of any EEG event and thefeedback tied to its occurrence. The criticallearning from this experiment was that techni-cal precision does not necessarily lead to clini-cal efficacy. The current use of the LENS em-ploys extremely weak intensities of feedbackanddoes involvethepatient’sownEEGdrivingthefeedback,butdoesnot involveanyconsciousparticipation or even positive intention.
Differences Between the LENSand Traditional Neurofeedback
The following statements reflect the currentstatusof theEEGbiofeedbackfieldat this time.
1. The field of EEG biofeedback or neuro-feedback is relatively new. There are rel-atively few studies with chronic condi-tions, controlled or otherwise, that offerunderstandings of what will work, underwhat conditions, to what extent, and withwhat time,physical, andmonetarycosts.
2. Each of the various kinds of EEG bio-feedback involves its own set of rituals,with relatively little analysis of what al-ternatives might be used.
3. None of the forms of EEG biofeedbackappear to have ever cured a progressivecondition such as Alzheimer’s, multiplesclerosis, Parkinsonism, or dementia.However, they probably have increasedfunctioning and quality of life for manypeople in the earliest stages of any ofthesediseases, perhaps for at least severalyears and when applied properly.
4. Each form of EEG biofeedback seems tocomplement and enhance the effects ofall of the others, as well as other forms oftherapy.
5. Based on interviews with former patientsof nearly each form of EEG biofeedback,each approach seems roughly compara-ble in effects, no matter how inexpensiveor how expensive the treatment was, withsome specific differences from treat-ment-to-treatment to be defined withlater research.
6. Nearly all forms of EEG biofeedbackwork with easy cases and become more
Len Ochs 7
cumbersome and delicate (with satisfac-tory outcomes) with complex cases, butappear nevertheless at their clinical effi-cacy limit with the current technologiesbecause of technical problems of manag-ing coherence and other issues.
7. Finally, while each form of EEG biofeed-back may appear scientific, the applica-tion of each is probably more of aphysiologically-based art than science atthis stage of the game. Even so, all of theforms of EEG biofeedback seem to offerprovocative and interesting hope formany who have been declared to be at theend of their options for improvement.
The LENS differs from traditional EEG bio-feedback in that the LENS does not require theperson to understand the meaning of, or labori-ouslyattendforahalfhour to thefeedbackinor-der to influence their brainwave activity andbenefit from the treatment. No attentional, dis-crimination, prolonged stillness, or learningdemands are placed on the individual. In addi-tion, the LENS uses a somewhat different con-ceptual approach to selection of which EEGsites to train. Traditional neurofeedback usesprotocols based on either symptoms or on ab-normalities found in QEEG brain maps, withboth approaches often utilizing only a limitednumber of electrode sites for training. In con-trast, the LENS treatment is also guided by atopographicEEGmap,butonewhichprioritizeselectrodesite abnormalitiesbased on both EEGamplitude and EEG variability. Unlike otherneurofeedback approaches, LENS treatment isthen administered at all 19 (or more) electrodesites. Treatment consists of the delivery of atiny electromagnetic field carrying the feed-back signal down the electrode wires for onlyone second at each of the chosen electrode sitesduring every session. This input stimulationvaries from moment-to-moment, updated 16times per second based on the dominant EEGfrequency changes. Generallybetween one andseven of the ordinary electrode sites are treatedduring each session.
Finally, central to the application of LENStreatment is the concept of patient reactivity/sensitivityand the response of thepatient’s ner-vous system. We adapt the duration of stimula-tion,sessionfrequency,anddegree towhichthe
stimulus is offset from the dominant EEG fre-quency to the patient’s reactivity, and closelyrelated to their vitality and degree of symptomsuppression.
The LENS may be used as a tool to use in atreatment context with other EEG biofeedbackor neurofeedbackmodalitiesor as a single solu-tion to several problems. The LENS is beingstudied as a potential treatment of adults andchildren with CNS-mediated disorders in theUSA, Australia, Canada, Germany and Mex-ico. It has been shown to produce rapid resolu-tion of difficult cognitive, mood, anxiety, clar-ity, energy, physical movement and painproblems when compared with more tradi-tional forms of psychotherapy or medicationtreatment.No efficacycomparisons are offeredin relation to other forms of EEG biofeedback,or neurofeedback, since no comparative studieshave been undertaken.
It is important to note that the LENS does notrequire the patient’s attention, focus, orientingtoward feedback, home practice of self-regula-tion techniques, or, indeed, any conscious par-ticipation in any self-regulatory activity (ex-cept showing up and not removing theelectrodes from the head). The LENS appearsto operate on the basis of the biophysical prop-ertiesof thefeedbacksignals themselves,onthetissues of the brain and related structures suchas thevascular system. Inaddition tonot requir-ing attention, focus, and attention toward feed-back, the LENS approach, tolerates grossmovement and artifact without reducing effi-cacy, or inappropriately rewarding maladaptivebehavior or physiological reactions.
Feedbacksignalsofdifferent intensities, fre-quencies, and wave form shapes appear to havedifferent clinical effects. There are only the be-ginnings of sophisticated research into theproperties of the OchsLabs system. It is still tooearly to draw any conclusions about the mecha-nisms or properties of the systems used. TheLENS can be used with extremely hyperactivepatients and still maintain apparent efficacy.The LENS feedback exposures can be as shortas one second per session for the appropriatepatient and still have apparent efficacy, whichmeans that it demands relatively little coopera-tion from the patient.
8 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
Benefits of LENS
The LENS appears to: (a) increase ease offunctioning; (b) increase clarity of functioning;(c) reduce the amplitude and variability (in-cluding spiking) of the EEG activity across the1-40 Hz spectrum at each of the standard 10-20electrode sites when there is some amplitudeandvariability tostartwith; (d) increase theam-plitude and variability of the EEG when there istoo little variability sometimes to show the fullextentof thepathology,before itdiminishes theamplitude and variability; (e) reduce or alleviatecentral nervous system problems as describedbelow; (f) allow new information (psychother-apy, counseling, education, relationship-spe-cific information from a spouse or co-worker,etc.) to be recognized, taken in, used and re-membered much more easily without interfer-ence or defensiveness.
The LENS appears to shorten the treatmenttimes required for the improvement of some se-rious cognitive, mood, energy, pain, and motorcontrol impairments.TheLENSalsoappears tooffer patients previously considered untreat-ableanewoptionfor remediationofsymptoms.Based on experience with both EEG biofeed-back research, and the use of pulsating lightsand other energy fields in neurological exami-nations to study seizure activity, it is hypothe-sized that the mechanism of action involves al-tering the person’s maladaptive inhibitoryneurotransmitter activity. The LENS has beendeclared a “minimal-risk” device by severalindependent human subject review boards(IRBs).
Improved functioning has been observed forthose patients receiving the LENS treatmentwhohadplateauedin their recoveryfrommotorparalysis and CNS-mediated cognitive andmood impairment after mechanical and psy-chological trauma. Reported improvementshave persisted since data collection was begunin 1994 (and even earlier with antecedentsystems).
Improvement has been reported in most ofthe subjects (N = 2500, in approximately90,000 sessions as of 2005) who have beentreated with the LENS. When the subjects forthis research and treatment have fallen withinthe areas that are known to be particularly treat-able such as mild traumatic brain injury, fibro-
myalgia, and explosive autism, the success ratehas reached over 80%. The more the patient’shistory has been complicated by lifelong prob-lems preceded by an intergenerational historyof problems in parents and grandparents, andwhen the patient’s problems have been numer-ous and complex, it is much more complicatedto judge the efficacy of this approach; thus, the“success rate” may drop precipitously.
Side effects from the use of the LENS havebeen similar to those that result from anychange in situation (biofeedback, meditation,moving a household, body work; i.e., disrup-tive upon over stimulation) but transient andnot involving any organ system damage or dys-function. The three most common side effectswhen therehasbeenoverstimulationhavebeenfatigue, anxiety or hyperactivity, and no im-provement in clinical symptoms. All of thesesituations resolved themselves, usually withina few hours or days, by temporary withdrawalfrom treatment and decreased exposure tofeedback.
Optimal Kinds of Cases. The LENS appearsto have its best effects for: (a) mild traumaticbrain injury if the person was formerly highfunctioning; (b) the diffuse pain of fibromy-algia and its associated fatigue and mental fog-giness, but leaving untouched any underlyingmyofascial pain for conventional treatment;and (c) explosive behavior, regardless of itscause, whether it is in an adult, a non-autisticchild, or an autistic child.
MoreDifficultButPositiveCases.TheLENShas been shown in uncontrolled, anecdotal ex-perience, to produce less consistent, less reli-able, andmoredifficult-to-obtain–butneverthe-less still positive, results in cases of: (a) autism:more sociability, greater affection, verbal skill,more grace and balance; (b) trauma from child-hood sexual or physical abuse, work, and warstress; (c) clinical depression secondary to anx-iety disorder; (d) bipolar disorder secondary toanxiety disorder; (e) alcohol and cocaine ad-diction: less craving, less defensiveness anddepression; (f) childhood schizophrenia andAsperger’s syndrome: less fear, greater inde-pendence and achievement; less compliance(not to be equated with oppositional), greaterindependence, less fearfulnessandanxiety,andmore self-direction; (g) some types of chronicfatigue syndrome: greater energy and clarity;
Len Ochs 9
(h)attention-deficitdisorders; (i)physicalheadinjury symptoms from moderate to severe. Inthe latter case positive outcomes were found inclinical research that was conducted under Of-fice of Alternative Medicine-National Insti-tutes of Health Grant to determine the efficacyof the LENS on reducing cognitive deficitsamong people suffering from closed head inju-ries (Schoenberger, Shiflett, Esty, Ochs, &Matheis, 2001).
It is important to note that while clinical im-provement has been noted in all of the condi-tions cited above, the course of treatment withthe LENS alone was often inelegant, cumber-some, involving trial and error and clinicalskill. The reasons for the complexity of treat-mentare reasonablywellunderstood.Howeverwe still have not evolved treatment protocols tosolve the treatment complexity problems andmake them as apparently successful and easy inthe discreteconditions thatwere noted above asareas of application where the best effects havebeen achieved.
METHODOLOGY AND DISCUSSION
The LENS Treatment Process
The LENS works by continuously monitor-ingEEGactivityand thenuses these readings todetermine the frequency of very small electro-magnetic fields that are “offset” several cyclesper second(hertz) faster than thepatient’sdom-inant brainwave. This feedback stimulus inputis thendelivereddownelectrodewiresatgener-ally seven or fewer electrode sites in the courseof a treatment session, for only one second persite. This input is much weaker than what thebrain receives from holding a cell phone toone’s ear.
How can non-perceivable feedback to thebrain that is of such minimal magnitude still beinfluential? While the mechanism of how thishappens remains to be determined, it is clearfromboth thedocumentedeffectsof these feed-back signals on the amplitudes and variabilityof brainwaves, that (a) this feedback is beingprocessed by the brain, and (b) the impact ofthesesignals,whenusedcorrectly,canimprovepeople’s functioning in their own experienceand the experienceof others who observe them.
While these effects are clear to the profession-als who use the LENS, it remains the job forcontrolled, double-blind, randomized studiesto demonstrate these effects to others. It also re-mains for basic research to describe the mecha-nisms that allow these effects to take place, aswell as the variables which minimize andmaximize the effects.
The current the LENS process involves:
1. Assessing the sensitivity, reactivity, fra-gility, hardiness, and prior history ofproblematic symptoms that are no longerpresent. This is done with a simple ques-tionnaire found in the Appendix B.
2. Anassessment lookingat the following:
a. The relative proportion of differentfrequency band activity within theraw EEG. If there is more delta ampli-tude, then it is likely there may be anacquired problem such as head injury.If alpha is predominant then there maybe more of a pervasive developmentalissue such as ADD with genetic influ-ences.
b. The clinical reaction to a standarddose of stimulation feedback. There isno substitute to putting a toe in the wa-ter, experiencing some of the feed-back, and then lookingatwhathappensover the next twenty-four hours.Then, despite theoretical ideas aboutthe appropriateness of the dose, theperson may find that the dose in thatadministration is just right, or toomuch. Signs that it may be too muchare that the person is profoundly fa-tigued, or restless and overly ener-gized, both of which usually disappearwithin twenty-four hours.
c. Assessment of which offset frequencyfrom the dominant frequency is mostefficacious at which to present stimu-lation.
d. If the prospective client appears rea-sonably sturdy, an offset evaluation isperformed to assess these factors.
e. If the person appears from the evalua-tion to be vulnerable to over stimula-tion, a much shorter and less intenseevaluation is done, giving all the in-
10 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
formation above except a suggestionabout which offset to use. The offsetfrequency is then presumed to be 20Hz faster than the dominant frequencyfor themost sensitive-reactiveclients.
3. Mapping. Construction of a topographicmap of EEG activity, without necessarilyproviding any feedback, of amplitudesacross the 1-30 Hz spectrum across theentire scalp. Electrode site selection intreatment is determined by ranking EEGactivity from least to highest in each EEGband, in microvolts amplitude and stan-dard deviationsum for each sensor site. Asingle channel EEG is used, monitoringeach of the standard 10-20 electrode sitesin sequence. While amplitude and stan-dard deviation measurements appear tobe reliable enough and reasonably corre-lated with quantitative EEG (QEEG)patterns, measuring correlations amongmultiple sites is not currently possiblesince the sites are measured in sequence,and not simultaneously.
4. Treatment providing the feedback in thedose and at the offset frequency as sug-gested by the above evaluations, in a se-quence prescribed by the map.
5. Monitoring the subjective reactions ofthe patient through self report and the re-ports of others when available, and theobjective changes in the EEG (obtainedby periodic remapping) to continue ormodify the dosage and site sequencesused in the treatment.
6. Involving other tactics to evaluate in-ferred EEG comodulation (correlated ac-tivity in amplitude and/or standard devia-tion) across the scalp. Comodulationmaybe responsible for treatment complexity,as well as the duration and stubbornnessof their condition.
Most recipients of the LENS input stimula-tion will have no immediate reaction to the useof this procedure. Some will have relativelyshort courses of treatment. However, some ofthose with latent emotional conflicts andintergenerational genetic physiological prob-lems will require longer treatment processes.
Even though this type of stimulation hasbeen found to reduce seizures when they are
present, in somepatientswho havehadseizuresin thepastbutwhere theyarenotcurrentlypres-ent, they have been known to reappear for abrief period of time. Hence the pre-treatmentinterview is useful in anticipating a complex orproblematic treatment. This allows both thetherapist and client a chance to review whetherthe re-experiencing of seizures (or other prob-lems such as anger outbursts, tics, inconti-nence,ormigraines) is somethingthat theclientwill tolerate.
Reaction Patterns Observed During Treat-ment. An interesting complexity appears whensymptoms become worse during LENS treat-ment. Many of these patterns we are about todiscuss have been considered “side effects.” Infact, they may better be considered as stages intreatment that are sometimes experienced ingaining mastery over symptoms. These prob-lems are of five types.
First,vascular typereactionpatterns:whethertalking about vascular (throbbing pain), peri-ods of anger, rage, sadness, obstinacy, explo-siveness, bed wetting (below age six), tics, orconvulsions, these episodes become sharper,but shorter induration,andfartherapart in time.As they become increasingly brief, they are ex-perienced increasingly as a fraction of their for-mer intensity, and may not show at all on thesurface, in the behavior of the patient. It is oftensaid that as treatment proceeds, the reactionspass faster and have less of a grip on the patient.Finally, their intensity diminishes.
In the end, patients often reflect that circum-stances that would have evoked a symptom nolonger do. They are completely inarticulate asto what process is happening inside themselvestobringabout thischange.However, theyretro-spectivelydonotice thedifferenceandattributeit to the LENS treatment.
It has been mentioned that the resultsbrought about from the LENS may be either theresult of placebo or hypnosis. Yet many of therecipients of the LENS had numerous previoustreatments, and many novel ones. Each of theseindividuals had the opportunity to have hypno-sis or placebo work during prior treatment ex-perience. If placebo and hypnosis, either di-rectly or indirectly, have not occurred in thepast for these patients, it would seem implausi-ble that the LENS would finally bring them theplacebo results that prior attempts had failed to
Len Ochs 11
bring. They are involved in receiving the LENStreatment because previous placebos have notworked. Therefore, it is assumed that placeboplays very little part in their current improve-ment.
Treatment with LENS
It is most important to understand that juststarting the use of the LENS does not bring animmediate halt to patient symptoms; in fact,they may appear worse for a while. While thesesymptoms are ones the patient has had in vary-ing degrees previously and are not caused bythe treatment, the change in the way the prob-lem manifests itself and is now experienced isdirectly attributable to the LENS treatment.The increasing sharpness of these problems,predictable or not, is always of concern for pa-tients, care givers, and referral sources alike. Itis also important to know that we expect thetherapist to predict and discuss the anticipatedchanges in how the problems may shift in theirmanifestations in order to give the patient pre-dictability and confidence in both the treatmentprocess and therapist. A therapist who does notpredict thissequenceisdeprivinghimorherselfof theconfidenceof thepatient.Further, it is im-portant to be considerate of the patient, allow-inghimorher tochoosenot tobecomeinvolvedin this approach if the possible consequencesare not appealing.
Second, muscular type reactions: musclecontraction pain in non-spastic muscles, andthe terrible muscle contraction pain in thosewith spastic muscles, may occur in head injury,strokepatients,andwhenever there isparalysis.Muscle contraction pain of a non-spastic typesimply diminishes with time, in contrast to thevascular pattern cited above. There is also painfrom the LENS-evoked spasticity reductionthat isseeninconditionssuchasTBIandstroke.This has been in nearly every instance almostintolerable to the patient and those close to thepatient. Special care needs to be taken with pa-tients who are hypersensitive to pain medica-tion and are, therefore, unable to use it to allevi-ate this temporary pain. This intense painappears to be a function of the decreased brac-ingofferedbynon-spasticmuscle fibers,whichpermits the spastic muscles to contract with in-creasing vigor before they too begin to soften
and relax. When this reaction occurs, the intensepain experienced during spasticity reductiontypically lasts from three to five days. It is oftenaccompanied by the sequence of uncontrolledmuscle contractions, jumping limbs, increasesin sensation, and then the return of partial orcomplete movements. Note: This kind of paincan be reduced or often completely eliminatedwith the use of a modality called photonic stim-ulation.
The third type of reaction is the surprisere-appearance of convulsive or tic-related phe-nomena that may have long since disappeared.This is actually considered a sub-type of thefirst class of vascular reactions. These prob-lems re-appear after their long absence, to thenear-horror and fright of the parents, care giv-ers, and referral sources. Bed wetting, tics, sim-ple or generalized convulsions, and emotionalexplosions, may suddenly appear for a fewweeks before they subside and make way forhigher functioning levels not seen before.Anticonvulsantmedicationhas beenextremelyuseful as an adjunct when the severity of the be-havior warrants. The advent of more functionalbehavior after the cessation of these symptomshas led to the speculation that the untoward be-havior had been inhibited by the same mecha-nisms that kept the patient limited in other waysof functioning. When the behavior has reap-peared, and then once again remitted, it may bethat the brain found another mechanism to con-trol the aberrant behavior while permitting theflourishing of adaptive and useful skills. Nev-ertheless, everyone involved needs to providesupport, care,andsafety in thepresenceofdiffi-cult behavior. To date no one has been caughtforever ina trapof regressive,destructive,orbi-zarre behavior, although the behavior has onrare occasion been extreme and frightening tonearly everybody involved in the very unusualinstances when it has occurred.
The fourth type of reaction has been theemergence of adaptive but unvalued, or franklydisvalued, behavior in the patient. Examples ofthis have been: less fearfulness and greater in-dependence of autistic and Asperger’s chil-dren, which may be outside of the parents andschools value systems (i.e., children who ex-press anger at siblings when anger is felt to be“bad,” children and young adults that becomemore interested in theirown and others’ sexual-
12 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
ity, children who become more independent,adventurous, and exploratory, and, therefore,begin to take risks which frighten parents; chil-dren who voice their own points of view andneeds may be contrary to what the parents seeappropriate; and children who no longer feelcompelled to sit still within the constraints of arigid school system). All of these behaviorshave occurred as greater functioning, greaterindependence, and greater self-control becamemore prominent. Some parents who haveblanched at the changes in their children willusually keep struggling to be supportive, whileother parents have done little but glory at thechanges in their children. It is advised to avoidtreatment if, in discussions with the patient orfamily, theyareunwillingtorisk theoccurrenceof such behavior. In the approximately twodozen autistic or Pervasive DevelopmentalDisorderchildrenIhave treatedwith theLENS,only one has failed to respond at all, forunknown reasons, while all the rest havedelightedtheirparentswith theirachievements.
Another example of a positive reaction withuntoward effect occurred in the treatment of anolder man who had experienced a traumaticbrain injury more than a dozen years before heentered treatment. As someone from out oftown, he had allocated only a week for treat-ment before he needed to resume his travels.One of the major problems he had experiencedsincehisheadinjurywasrage,whichshowedit-self in verbal and physical violence. Otherproblems were chronic angina for which hetookmedication(andfrequentdrinksofalcoholfrom a flask always with him), and a loss ofthree-dimensional vision. After his first treat-ment he was freed from heart pain and an-nounced that he no longer needed to drink tocontrol the pain. Within 45 minutes after thetreatment he announced that his three-dimen-sional vision had returned. At first he walkeduncertainly as if he was wearing his first pair oftrifocals. The next day his wife accompaniedhim to therapy. He was visibly distressed. Shehad announced to him that she had suffered hisabuse long enough and that she was no longergoing to take it–since she no longer had to. Shecontinued to hurl invectives at him and he ac-cusedherof trying todestroy thegoodeffectsofthe treatment.She was offered treatment for thepost-traumatic stress which she most certainly
suffered, but she declined. He was asked to besupportiveofher inheranger,consideringwhatshe lived with for years. Over the next few daysunder her relentless attacks he regressed to hisformer state. At the end of treatment they left:him in pain, his three-dimensional vision againlost, and drinking again, and with her as hislong-suffering care taker. This illustrates theimportance sometimes of working with the en-tire social system, rather than narrowly focus-ing on a particular physiological problem inisolation. It also illustrates the inadvisability ofworking under fixed time limits.
A fifth type of reaction is the recapitulationof previous symptoms, from the most recent tothe oldest. Often patients will re-experiencefirst, recent symptoms, and in the last stages oftreatment, re-experience symptoms that theyexperienced as infants. They will often wonderwhy, for instance,as therapy isabout tobecom-pleted, they are experiencing abdominal pain.When questioned, they can often rememberhaving such pain or remembering stories ofhow they had such pain in childhood. These aretransient reactions and often pass in a week orso.
Diagnoses. The LENS is a non-specifictreatment approach; that is, treatment planningis not guided by diagnosis, which is seen bysome as a weakness of LENS treatment. Part ofthe problem with treating many conditions thathave been resistant to amelioration within con-ventional medical and psychological circles isthreefold. First, there is much misdiagnosis.Many of the diagnoses that are proffered arecatch basins and euphemisms, and are substi-tutes for professional ignorance. The problemsof diagnoses of many of these conditions, suchas Asperger’s, Parkinsonian variants, tuberoussclerosis, attention-deficit disorder, fibromy-algia, bipolar disorder, etc., are often beyondthe discriminative skills of many practitionersand the most fashionable diagnoses are oftenused. Second, many conditions are beyond thediscriminative capabilities of the diagnosticsystems themselves, or their existence as inde-pendent entities is controversial and at thewhim of what the medical-insurance systemwill accept given political (turf) and economicconsiderations. Third, the diagnostic name it-self can say little about the treatment when theindividual differences among people with the
Len Ochs 13
same diagnosis can demand major differencesin treatment strategies.
Considerable heterogeneity of brainwavepatterns has been found within the broadly de-fined diagnostic categories. Replacing treat-ment guided by diagnosis, LENS treatment ispredicated on the fact that many psychologicaland medical conditions involve various typesof abnormal EEG activity (Hughes & John,1999). LENS treatment is designed to reduceabnormal brainwave patterns and is individual-ized based on the distinctive amplitude andvariability patterns found through topographicbrain mapping, as well as the patient’s subjec-tive reactions to treatment. Finally, it may besaid, considering the vast responsibilities of thebrain, that the brain, itself, is a non-specific or-gan. This means that injuries to it may take thisshape or that, without any specific predictableoutcomes,associatedwithaparticular location,size, depth, or type of injury. Although someoutcomesarecertain inagross sense, thepartic-ularities of any injury are always some uniquecombination for the individual involved. Thepracticesof cliniciansusing the LENS are oftenfilled with almost nothing but patients who areexceptions tomedicalandpsychologicalpredic-tions of “no recovery possible.”
Differences between the LENS and Conven-tional Photic Stimulation Systems. The LENSdiffers from currently available consumer (orprofessional) AVS devices in the followingways. Most of these devices are considered en-trainmentdevices.They lock thebrainwaveac-tivity on the frequency used to stimulate. TheLENS disrupts the way the brain locks onto fre-quencies, or clusters of frequencies, hopefullyhelping to free the brain from rigid patterns sothat it canhave the flexibility topursue the tasksthat it and the person need it to pursue. Second,most of the AVS devices use light frequencies.The LENS uses various frequencies of electro-magnetic energy instead of photic stimulation,with is accompanying small risks of evoking aseizure. Light has not been use in most of ourapplications for the past seven years.
Third, with the LENS, the person’s EEG ac-tivitycontrols the frequencyof thepulsations inthe energy field. This customizes the pulse rateto the person’s own activity as it continuouslychanges. The stimulation frequency of con-sumer sound and light systems is both pre-pro-
grammed and set; a selection is made on the de-vice’s front panel, or programmed to change ina way unrelated to the person’s actual brain ac-tivity. Thus the input stimulation is not individ-ualized to the unique and ever changingbrainwave patterns.
Fourth, the LENS uses electromagnetic en-ergyfields infinitesimal instrength,whileotherdevices use much stronger signals. The LENSmay, despite the weakness of its energy fields,obtain its power through sustained resonancebetween the person’s EEG activity and the pul-sation frequency of the field returned, whichmay be receivedby the brain because of its abil-ity to detect patterns. While much of this isspeculation, it has been observed that when theresonant pattern of the feedback is broken(whenthe linkbetweenthedominantfrequencyand the feedback is broken) there are no longerany beneficial effects from our stimulation.That is,when thefeedbackresonance isbroken,bothnegativeas well as positiveeffects canstillappear, but, depending on the frequencies, in-tensities, and doses involved, they appear withmuch less consistency and predictability.
Anoteontheuseof thewordresonance:Res-onance tends to be used in two ways in currentmedicalparlance. In thephraseMagneticReso-nance Imaging, resonance is achieved by thepower of the magnetic field on the electronsadding energy to the electrons to move theminto higher order shells. Persinger (1974),Sandyk (1994), Rife (1953) and others use theword resonance to refer to a state in which astimulus intensity or frequency matches aknown or theorized fixed frequency in thebody. The word “resonance” is used here in anew way in the history of science: that of thechanges in the stimulus continuously matchingchanges in a physical variable (such as brainwaves or heart rate). In this sense the resonanceis a dynamic one, rather than a static one.Hence, this is a feedback system. However, un-like other biofeedback systems that feed backinformational stimuli, the LENS feeds backphysical stimuli, the physical properties ofwhich affects physiological changes.
The LENS Equipment Requirements. LENSrequires a brain wave measurement device; acomputer fitted with an EEG device that con-trols the emitted energy-field; software to linkthe brainwaves with the stimulation radio fre-
14 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
quency (RF) carrier wave and a system that candeliver levels of energy field feedback at lowbut precise levels of intensity. These levels arelower in intensity than the electrical field thatsurrounds digital wrist watches.
In order to provide feedback, the individualis first fitted with the EEG electrodes. In ourprevious systems, the patient used to wearglasses with components mounted on surfaceof the lenses, or sat with the glasses mounted ona stand at some distance in front him or her. Theoperator monitors the computer screen andcontrols and intensity and duration of feedbackso the person remains comfortable. The contin-ued presence of the equipment operator is nec-essary to watch the quality of the electrode con-tact,and todeterminethat thepatientpreferablyremains motionless for a few seconds beforethe stimulation is given.
While the final determination on how theLENS works must rest with a great deal of re-search, we believe that the LENS achieves itsresults by breaking up the rigid, self-protectiveway the brain has of responding after psycho-logical (stress)orphysical traumaandrestoringthe inhibitory capacity of the cortex.. There isevidence that during any kind of trauma thebrain protects itself from seizures and over-loads by releasing neurochemicals that protectit from these dangers. Unfortunately, the pro-tectionalsoreducesfunctionalcapacity,notun-like the effect of swelling on joint articulation.Long after the trauma is over and the danger ispast, the ‘protection’ may still remain. The per-son can, therefore, become stuck in variouskinds of disabilities due to the reduced neuralflexibility of functioning.
Technology Development of the LENS.There was something wrong with nearly all theLENS design elements and procedures fromthe point of view of those experienced in tradi-tional EEG recording and EEG neurofeedback.This is acutely evident in relation to:
• the established practical concerns regard-ingshaping reinforcementcontingencies
• using visual and/or auditory, or radio fre-quency feedback carriers for the feedbackof information to the brain
• managing high and low frequency EEGactivity
• thinking in terms of under- and over-arousal phenomena
• maximizing the amplitudes of some EEGfrequencies while inhibiting the ampli-tudes of other frequencies in relation toparticular problems
• locating electrode sites for training• using topographic maps to provide a treat-
ment plan• resisting micromanaging the inhibit and
reinforcement settings of the EEG in bio-feedback treatment
• deferring to subjective reports, rather thanquantitative measures of the EEG as ei-ther signs of pathology or progress.
Therewere no clues in the literature for guid-ance in the preliminary clinical work with theLENS or its predecessors, so the initial treat-ment guidelines became: Try it on oneself first,alwaysstrive tomaintainpatient’scomfort, andcut back if symptoms reflecting over stimula-tion follow a treatment–even if the post-sessiondiscomfort had nothing to do with the treat-ment.
EEG Site Location. Between 1990 and 1995the predecessors to the LENS most frequentlyfound success with consistent use of FPZ as theelectrode site for the active electrode (with thereference on an ear lobe, and ground at the backof the neck). Depression was typically dis-patched in six sessions. This raised the questionabout the efficacy of choosing any specific siteover another at the start of the treatment: onesite appeared to be as good as the next when us-ing the precursors to the LENS in the early1990s. An observation that had no meaning atthe time was that delta, primarily, and theta,secondarily, were predominant in the frontalEEG amplitude of nearly all of the patients. In1995 Ochs wrote a short piece titled ManyKinds of Depression Are Curable to spread thegood news.
No clear differences in either the way theoriginal light feedback was tolerated or thespeed of treatment were found when monitor-ing the EEG at the sites that were historicallypopularwith traditionalEEGbiofeedback ther-apists: occipital locations of O1 and O2, the topof the scalp at CZ, or the site of insult or its con-tra-coupdamage.Thecentral foreheadsiteFPZwas tried because the side effects were mini-
Len Ochs 15
mal, results were as good here as at the othersites, and because it was easier to avoid elec-trode paste in the hair of the patients during theinitial rapport-buildingsession. The frontal sitewas therefore selected as the point for use at thecommencement of treatment. The frontal sitehas indeed always been more prone to artifactfrom eye movement, jaw movement, facial ex-pression changes, swallowing, etc. However,since the artifact itself decreased as a functionof treatmentprogression, it seemed plausible toaccept the artifact decrease as one of the globalindicators of improvement. This suggested theselection of FPZ as an initial starting site. As aconsequence, the artifact component of theEEG records was and still is kept, rather thandiscarded, as is done in conventional neuro-feedback treatment.
Another consideration was related to thework of Davidson and Hydahl (1996) and theirobservation that the left frontalareawas lessac-tivated in depression. Moving the electrode lo-cated at the front-center of the forehead to theleft produced, again, no improvement in pa-tientswithdepressivefeatures.This isnot tosaythat lateralizing the traditional EEG biofeed-back might not make a difference in the suc-cessful treatment of depression. Using theLENS approach, however, the clinical efficacyof changing the electrode placement to the leftfrontal area and the practicality of using FPZoverrodeall theotherconsiderationspertainingto the selection and use of the more standardelectrode sites.
Interestingly, in 1995, with no changes inequipmentorsoftware, theselectionofFPZasasite no longer seemed efficacious. In contrast tothe delta and theta amplitudes that were pre-dominant in the frontal EEGs of previous pa-tients, alpha now seemed more predominant inthe frontal EEGs of those entering treatment.Instead of rapid resolution of depression, irrita-bility and moodiness often resulted from treat-ment. In contrast to the rapid resolution of de-pression that had previously been seen, and incontrast to any certainty about how to treat thatdepression and about placing the active elec-trodeatFPZ, therewasno longerany ideaaboutwhere to place the electrode, either on the basisof the literature or my own experience. This in-cluded experimenting with placing the activeelectrode at C3, C4, OZ, O1, O2, and at CZ. In
an unsystematic way the electrode was movedthroughout the standard 10-20 sites. At timesthere was a remarkable response from sites no-body had talked about; at other times there wasno response from any sites addressed.
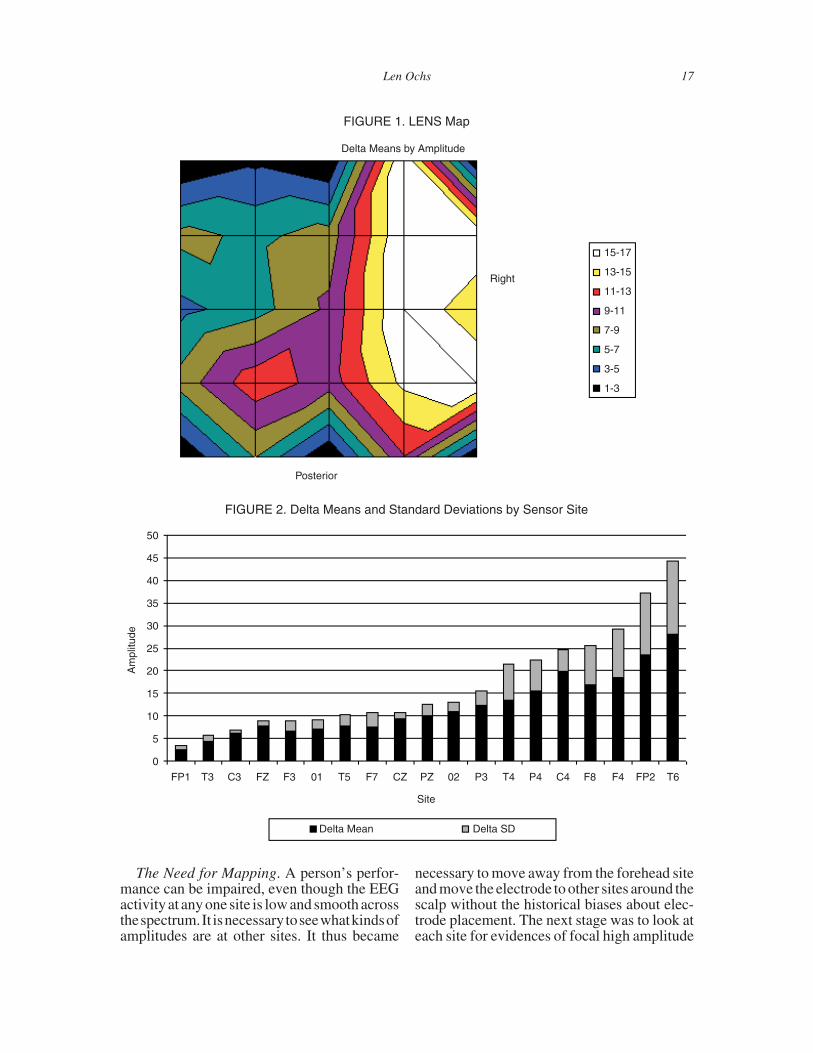
To better understand what was happening,less expensively than with quantitative EEGbrain mapping, single-channel data was col-lected from all the sites, one site at a time, andthis data was fed into Microsoft Excel’s surfacemap. An example of the resulting map is seen inFigure 1, which displays an example of a casewith high delta amplitudes throughout the righthemisphere.
A histogram (bar graph) was then created,one bar per electrode site. At first the data madenosensewhenitwassimplyorganizedin theor-der in which the data was collected. But, whenrank-ordered from lowest-to-highest ampli-tudes foreachEEGband, it thenappeared that itwas a picture of the functionality of the sites–that is, the lower the measured amplitude inmicrovolts, the more the cortex appeared to beinhibiting the subcortical activity from reach-ing the cortex so that it could be measured. Thegreater the inhibitory activity exerted by thecortex, the higher the level of functioning. Fig-ure2 illustrates thedata fromFigure1 in thisbargraph format, displaying the amplitudes andstandard deviations of the data, rank orderingthe electrode sites. The rank ordering becamethe clue about which sites to select for treat-ment, and in which sequence. A consistent, or-ganized way to select active electrode sitesmight be to proceed from those with lowest am-plitudes to those with the highest amplitudes.This might not have been the only way to selectsites, or necessarily the best way, but at least itwasempirical andnotbasedonstaticexperienceor research based on aggregated data.
Therationale for thiswas that instartingwiththe better-functioning (lower amplitude) sitesand proceeding to lower functioning (higheramplitude) sites, the better functioning sitesmight respond more rapidly and stimulate themore poorly functioning sites. By the time thesiteswith the loweramplitudeswereaddressed,the higher amplitudes at other sites would havealready decreased, lessening the work thatwouldneedtobedone.This turnedout tobetruewhentheamplitudeswereamongthehighest.
16 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
The Need for Mapping. A person’s perfor-mance can be impaired, even though the EEGactivity at any one site is low and smooth acrossthespectrum.It isnecessarytoseewhatkindsofamplitudes are at other sites. It thus became
necessary to move away from the forehead siteand move the electrode to other sites around thescalp without the historical biases about elec-trode placement. The next stage was to look ateach site for evidences of focal high amplitude
FIGURE 2. Delta Means and Standard Deviations by Sensor Site
andhighvariabilityactivity,andprovidestimu-lation at that site until the EEG activity was lowand stable. The activity at each site was as-sessed and worked with until ideally no high (>2.0 μV) amplitude/variability activity was ob-served.
Italsobecameclear that theinformationusedto make the surface maps could be used to gen-erate treatment plans, specifying the order ofsites to be used in treatment.This gives the ther-apist an empirical basis for starting treatmentwhere the cortex is most functional, and work-ing toward points of less functionality, therebybuilding upon the patient’s strengths in devel-oping their discriminatory capability.
The Beginnings of Mapping. Beginning in1996, performing inexpensive surface EEGmaps that showed the relative amplitude andvariability of the EEG at each electrode site (asseen in Figure 1) provided an unexpected treat-ment benefit, in addition to providing graphicpre and post measures. These maps were ac-quired by measuring the activityat each site in aspecified sequence, using a single-channelEEG instrument. Maps constructed in this waydonotallowaccuratemeasurementsof the rela-tionships among sites. The unexpected benefitof the sequentialmaps is that they do provide anexplicit plan of which sites to treat, and in whatsequence. Beginning at the sites of the lowestactivity, and working toward sites with thehighest activity, is the same as working fromwhere thecortexismost functional towhere it isleast functional.
Hyper-Reactivity: Alternating the Polarityof the Leading Frequency (Offset). One of thefirst clear reactions encountered in the use ofprecursors to the current LENS was hyper reac-tivity to the visual feedback stimuli. Initialwork began in 1990 with two individuals withpost-traumatic stress symptoms (PTSD). Nei-ther had been successfully treated with stan-dard psychotherapy, relaxation training, orwith biofeedback (including EEG biofeed-back). One of the individuals reacted stronglyto thevisualandauditoryfeedback.Shejumpedin her seat, and complained of a headache andbackache.
Later, patients complained about some as-pects of the feedback. Some expressed dislikeof the“flicker”of the lights.Others complainedabout the color; others, the brightness. Some
could not verbalize the quality they didn’t like,but reacted physically, or just said that theydidn’t like it. Others invoked a variety of verbaland non-verbal startle responses. One individ-ual became explosive and frightened staffmembers in other rooms with the volume of hisoutbursts.
In each of these cases, the therapist’s re-sponse was to change the direction of the lead-ing frequency or offset. If the lights were set toflash at +5 Hz faster than the dominant fre-quency, the polarity was changed to let themflash at �5 Hz (more slowly than the dominantfrequency). In nearly all instances of this prob-lem, changing the polarity of the leading fre-quency, or offset, decreased the immediate un-comfortable reactions. Further polarity changesat the occurrence of these reactions continuedto manage and minimize the reactions. Chang-ing the polarity of the feedback offset was thepreferred way to minimize these reactions be-cause the software permitted fast and easychanges of polarity. While a brightness controlwas available, it involved more time and com-plex manipulation of the controls.
Alternating polarities had so much impact inthe early 1990s that the old procedure, thencalled EEF (EEG Entrainment Feedback) wasmodified to allow for specific sequences ofpre-programmedpolarityalternation.Alternat-ingpolaritieswasoneof the importantelementsof the patent. The alternating polarities seemedto decrease the hyper reactivityof patients. Oneof the major differences between the ap-proaches in theearly1990sandnowis that thereare few, if any, immediate reactions of discom-fort for which the alternating polarities wouldbe needed. In contrast to the measures takenduring those early days, today’s strategies tendto be much more subtle.
What’s in a Name? The LENS process wasoriginally called EEG Entrainment Feedback(EEF), despite the urging of others, who per-sisted in theargument that thesystemseemedtobe freeing the brain from being locked up (en-training on itself). The ultimate inspiration forchanging the name from EEF to EDF (EEGDisentrainment Feedback) was found in Chaos:Making of a Science, by Gleick (1988, p. 293).Gleick used the word “disentrainment,” refer-ring to the unlocking of a system. This enabledthe precursors to LENS to be seen as disen-
18 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
trainment systems. The name of the processwas changed from EEF to EDF. After that, thename changed to Neurophotic Stimulation, toEEG-Driven Stimulation, and finally, to theFlexyx Neurofeedback System (FNS), termsthat were less theoretically encumbered andmore descriptive names.
It should be emphasized that the treatmenteffects observed were not due to training to in-creasesomecomponentsof theEEGbandor in-hibit others, even though the observablechanges in the EEG activity across the 0 - 40 Hzband appeared comparable to those obtainedfrom the traditional EEG biofeedback training.Experienced EEG clinicians and researchershave been observed attempting to truncate theEEG band activityat one end or the other, or at aselected frequency, either based on some theo-reticalbasis,orpreviousexperience.EarlyEEFwork was also done this way (i.e., attempting to“speed” the EEG by using positive leading fre-quencies). The system is now run by primarilycontrolling dosage: the duration of the sessionand the intensity of the feedback signal.
It is important to understand that in no way,as some people think, is the EEG ever “sped” or“slowed,” with the LENS. Under most condi-tions the amplitude and standard deviationacross the spectrum is reduced. Furthermore,this effect is accomplished from the biophysi-cal effects of the feedback signal and its reso-nance with the EEG of the person, rather thanfrom any reinforcement to elaborate or inhibitthe activity in certain bands or frequencies.
Subjects’ sensitivity to the brightness of theold visual feedback was recognized whileworking with Dr. Herbert Gross’ patients, aneuropsychiatrist who specialized in head in-jury. The patients’ brightness sensitivity be-came apparent when the brightness of the lightscould not be sufficiently reduced to permit pa-tient comfort. Although good results had beenachieved using red LEDs, among the most irri-tating colors one could employ, the protocolwaschanged tousegreenLEDswhen itwasob-served that the red LEDs annoyed the head in-jured population. This change worked well forthegroup of head injuredpatientswho hadbeenfunctioning extremely well prior to their headinjuries.
Hypersensitivity. An informal survey of“normal” people, in contrast to those with
symptoms, using light stimulation devicesavailable to consumers showed that they en-joyed lights at full brightness. At that time, theoperating presumption was the brighter thelights, the better the results. Once the idea wasgrasped that red lights were both too irritatingand too bright, the use of red lights gave way tothe more tolerable green ones. The desensitiza-tion process was developed gradually, slowlyintroducing the patients to increased lightbrightness. This desensitization process al-lowed them to maintain their comfort withlights of increasing brightness. After desensi-tizing them to the green lights, it was again pos-sible to use the glasses with the red light-emit-ting diodes (LEDs), and eventually withcontinued desensitization, at full brightness inthat generation of hardware and software, aswell.
While the green LEDs, with their decreasedbrightness, worked for those who had per-formed well prior to their head injuries, theywere inadequate to meet the sensitivities of asecond group of patients with heterogeneousdiagnoses prior to their exposure to the LENS,including diagnoses of borderline and variousanxiety problems. These patients requiredgreenLEDswith tissuepaper foldedover them,or with masking from manila folder material,andevenpartialcoveringfromvinylblackelec-trical tape. Only with such masking could theseultra-hypersensitive patients be comfortable,even with the lights at their lowest intensities.This ultra-hypersensitivity was observed evenwithout light.
As clinical work continued with both headinjury and non-head injury patients, it soonbecame apparent that greater incidence of be-havioral and physical pathology seemed to cor-respond with increasingly prominent hyper-sensitivity to the visual feedback. In otherwords, patients with depression, energy prob-lems, irritability, explosiveness, violence, dis-tractibility, short-term memory problems, dif-ficulty in organization, problems followingconversation, and difficulty reading, may haveall had irritable brains as evidenced by rela-tively large amplitude, low frequency activity,with relativelyhighstandarddeviations.This isanentirely testablehypothesis, and to theextentit isdetermined tobe true, is a rather remarkablestatement about human functioning and func-
Len Ochs 19
tional impairment. In fact, diagnosis of hyper-sensitivity might include much lower levellight than is usually used in the detection ofphoto-hypersensitivity, with more sensitivebehavioral observations than frank seizure orEEG spike and wave prominence. This discus-sion of photohypersensitivity refers to pre-1999 work with the antecedents to currentLENS work.
Historical note: The following discussionwas applicable when LENS feedback was ad-ministered for periods of up to 20 minutes persession. Since 1999, the feedback exposure istypically as brief as one second per electrodesite, with an average of four sites worked withduringanysession,which typicallyoccursonceaweek.Thusdesensitizationpre-1999wasquitedifferent from that which has occurred sincethenthroughthepresent. It isplacedhere, ratherthan inanappendix, togive the readera sense ofthe flowof theLENSdevelopment,aswell as tocontrast the current practice.
Desensitization. Desensitizationused to be acornerstoneofourearlywork linkingEEGwithphotic stimulation. There is no question that forsome patients, desensitization of some typemaystill be importantwhen theyappear to haveenergy and sudden-onset problems. However,as the mix of patient diagnoses and presentingproblems became more complex, and more pa-tients showed fatigue as a major complaint, de-sensitization began to play a smaller part. Atthis present time, because the feedback signals,even though not visible, evoke EEG changesmuch more rapidly than they used to be, it is of-ten not possible to expose patients for a briefenough time to the signals to start the desensiti-zationprocess. Thedifferencebetweenand oneand two seconds can be profound to a very sen-sitive patient.
With themore recent,briefer treatmentdura-tions characteristic of the LENS, there does notseemtobeenough timeor reason toconductde-sensitizationthewayweusedtodoit.However,desensitization can still be accomplished throughtheuseof theoffsetsettings.Heredityalsoplaysa part. When parents had a history of mood orenergy problems, problems were chronic, orslowinonset,desensitizationbecamelesshelp-ful and gave way to the application of feedbackwith only the gentlest touch, the briefest andleast frequent application. For this group, the
therapist using the old I-400 system might useonly green lights, masked glasses, and neverraise the brightness above “1” in brightness and1% in duty cycle during the entire course oftreatment. Work has been progressing since1998 using the profoundly low intensity feed-back, and while the electromagnetic stimuli arenot visible, this still produces changes in theEEG when the EEG is observed after the feed-back stimulus has been given.
Here is an example of how the need for de-sensitizationwasdiscoveredin theoriginalsys-tems. Ordinarily, the brightness of the lightswas varied frequently during a treatment ses-sion and over the course of treatment. Just dis-cussing the brightness of the lights, and none ofthe other treatment variables such as electrodesite, for example, an intensity of “1” may havebeen used during the first six sessions. As thesessions progressed, symptom intensity de-creased. In the seventh through the tenth ses-sion, intensity was increased to a brightness of“2.” In the eleventh through the thirteenth ses-sions the brightness was increased to “4.” Inother words, not only was the brightness in-creasing, but the pace of increase was comingmore and more rapidly as time progressed. Per-haps in the fourteenth session the brightnesswas increased three times, from “6” to “18” to“36.” The brightness ratings are in quotationmarks because they are arbitrary in value. Noluminosity values were ever formally evalu-ated for the numerals used to indicate bright-ness. Yet the brightness values were linearlycontrolled by current flow; so that relative toeach number, a brightness of “2” is half that of“4.” Whereas initially going from “1” to “2”would have been uncomfortable for this hypo-thetical patient, in the end leaping from “18” to“36” would have been quite comfortable. In themeantime, symptom intensities across theentire range would commonly have droppedprecipitously.
During one session, by accidentally usingnew software with a hidden defect, a protocolwas loaded that held the light frequency lowand constant during the feedback periods, re-vealing EEG activity which was initially seenwhen the patient’s complaints were prominent.A young woman in her thirties, otherwise highfunctioning, complained of a post-puberty his-tory of premenstrual fatigue, irritability, racing
20 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
thoughts and sleeping problems, leaving herwith severely restricted professional job func-tioning fifty per cent of the time each month.She left her job to avoid the continuous, ex-treme effort needed to fulfill her professionalduties two weeks of each month. For two men-strual cycles after desensitization had beencompleted, her sleep problems ceased, as didher racing thoughts, irritability, and diurnal fa-tigue. During her third premenstrual cycle,however, her fatigue returned and was everpresent. Examination of her EEG spectrum re-corded under moderately bright light showedrelatively largeamountsof high amplitude, lowfrequency activity when the brightness wasconsistent across all four feedbackperiods.Thesession was constructed using a one-minute,no-feedback pre-baseline, four 18-second peri-ods of feedback (during which feedback stimu-lationmayor maynot be given), and a one-min-ute no-feedback post-baseline, all repeated 17times. All recording was done eyes closed. TheelectrodesitewasCz,withaleft-earreference.
The high amplitude, low frequency activitywas not present when the light brightness wasreduced to 10% during the first and third18-second feedback-possible periods. The in-formal hypothesis that alternating brightnesswould have no effect in accelerating change inEEG amplitudes seemed patently wrong. Al-ternating flashes between the left and right eyesucceeded in lowering the amplitude of theEEG more than when we lowered the bright-ness of the feedback light stimulation, perhapsbecause there was only half as much stimula-tion being given.
At the current time, the intensity of the feed-back signals (which are no longer photic stimu-lation) are so weak, their effects so strong, andthe treatment times necessarily so short, that is-sues of desensitizationhave taken a back seat todosage. The exposures are now so short that ithasbeendifficult to seehow tomanageadesen-sitizationprogram.Ithasnotbeenuntil recentlythat six years of experience with the low powerelectromagnetic carrier wave feedback has al-lowed us to understand how to begin to inte-grate our prior experience with lights into cur-rent LENS work. Currently, increasing thenumber of electrode sites that we work withduring each session, decreasing the interval be-tween sessions, and decreasing the offset fre-
quency at which we provide the stimulation areall ways to increase the power of the feedbackstimulation and treatment dose.
Desensitization and Level of Functioning.Another past observation, equally testable, wasthat the levelof somepatients’ functioningcon-sistently increased as their comfort increasedwith progressively brighter light feedback.This means that depression, irritability, reac-tions to bright or interrupted light, impatienceand explosiveness lifted, non-focal pain de-creased, violence ceased, distractibility, anxi-ety reactions, organization, problems follow-ing conversation, and difficulty reading wereall markedly ameliorated–without any claimthat they were totally erased. The problemswere improved enough that friends, spouses,distant relatives, employers, and last, the pa-tients, themselves, were delighted and sur-prisedat the improvement.Academicgradeim-provements were noticed as well. Theseobservations were echoed by physicians andneuroscientists not involved in this treatment(although no attempt was made to keep themblind to who was involved in the treatment). Inretrospect, it may have been that the enhancedability of the cortex to inhibit electrophysi-ological reactions from the increased bright-ness of the feedback stimulation was the signthat the cortex had repaired itself. In contrast, ifsomeone’s brain had become re-traumatized, itwas very difficult to re-desensitize the personfor unknown reasons.
We learned that it was not always possible todesensitizesomeone.Desensitizationwas indi-cated especially when a person was energetic,and less useful when the person often felt fa-tigued. It is also possible that new techniqueswill permit successful partial desensitizationofthose people otherwise unable to tolerate thestandard process.
Paceof Desensitization. Therewas a charac-teristic desensitization curve, even though theentire desensitization process could take any-where from five minutes to five months. Theinitial pace of desensitization was always rela-tively slow, relative to its much higher rate ofchange at the end of the treatment process. Thedesensitization curve appeared to have been anaccelerating curvilinear function in which theslope of the rate of change of the light intensitywas often imperceptible initially, but its rate of
Len Ochs 21
change was geometric at the end. Put anotherway, the initial brightness changes may be 1%at a time, but increase in units to 20% at a clipoccurred in the final minutes of the process.
We found that during a long desensitizationprocess, lasting months, the final 80% of thebrightness changes may occur in one treatmentsession. This pattern was consistent across allpatients whenever the need for desensitizationwas present. The desensitization curve wasreminiscent of the logarithmic curves in theWeber-Fechner law of perception, in whichbrightness increases logarithmically with theabsolute value of the brightness of the stimulus.The observation of the adaptation of the brainmay cast light on the flip side of the brightnessestimation: that is, on the place that the rate ofreconnectivity of the cortex plays as it regainscompetence.
Decreasing Light Intensity After Desensiti-zation. One patient, early in the exploration ofthe LENS, suffered workplace abuse traumaand re-experienced symptoms formerly mini-mizedbytheLENS.Sheremainedfreefromherformer dislike of the brighter lights, however.There was the implication that she had not re-lapsed into photosensitivity and, therefore, didnot need a lowering of the light intensity. Con-tinued treatment with the LENS at high levelsof intensity, however, did not lead to a decreasein her new trauma symptoms, which showedthemselves prominently as depression, anxi-ety, and anger. High amplitude and variabilityin low EEG frequency bands again showed it-self in her record. It was hypothesized that theintensity might be re-stimulatingher pathology(i.e., perpetuating her re-traumatization). As atest of this hypothesis the intensity of the lightswas drastically lowered and almost immedi-ately she reported a decrease in her depression.During this same period, Russell was using theLENS with a few patients who had experiencedcerebral vascular accidents. He applied thischange in approach to the therapy he was doingand found that motoric and cognitive rehabili-tation progress was stimulated and acceleratedby lowering the intensity of the lights.
Interestingly,manyusersofpre-programmedfrequency, commercially-available sound andlight systems run their systems at full intensity.The colors and patterns are visually interestingat full intensity. The patients most often will
seek full intensity, partly for aesthetic reasons,and partly, upon questioning, because theythink that brighter is inherently better and thatall treatments inherently involve the struggle totolerate discomfort–which they feel they shoulddo if they really want to improve.
However, it is probably not legitimate toequate the stimulation from fixed or rampingfrequencies of the audio-visual stimulation(AVS) systems with that of the LENS and itspredecessors. The AVS systems’ stimulationintensity may be seen as ambient light, or“noise” stimulation, not nearly so tightly re-lated to the living, dynamic EEG. This may besupported by the observation that AVS usersneed to use much brighter light intensities thanwhat was ever used in the LENS predecessors.It seems to me that the inherent resonance of theLENS-type stimulation allows the LENS stim-ulation to remain at very low intensity and stillhave dramatic physiological and behavioral ef-fects. It is apparentlynot thecase thatbrighter isalways better, nor that tolerating increased dis-comfort will accelerate recovery. In fact, whencomfort is used as a cue for intensity settings,and the feedback LENS intensity is minimized,improvements in energy, mood, and cognitiveintegrity are often noted. This has been ourexperience with our older light stimulationsystemandwiththenewerversionsofLENS.
When the LENS treatment is completed, thecortex may be in a very different state than itwas at the start of treatment. Whether or not pa-tients had been desensitized, the patients were,in fact, more receptive to and discriminatingaboutexternalstimuli,butnothypersensitiveorhyper-reactive. Their responses were moreflexibleandappropriate to the levelof feedbackpresent in the moment. In view of the greatersensitivity, is it any wonder, then, that high in-tensity, strobic feedback would act as if it wasoverloading the cortex of these individuals andin a sense replicating the internally-producedpathology that once was there? Decreasing thefeedback stimulation after the desensitizationprocess might be more effective because thebrain has, through the course of treatment,become more responsive to feedback.
The pathology of some brains may require amajor change or reorganization at the start oftherapy, and trying to work locally at the site ofdamage may not be useful if the person is very
22 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
energetic. Once the brain has been globally re-organized by the desensitization process andthe patient is comfortable at full intensity, con-tinued feedback at the peak level of intensitymay now overwhelm the cortex. This repre-sents amethodby whichonemaysafelyexperi-ment with replicating trauma and recoveryfrom trauma. After desensitization, by lower-ing the intensity of the feedback, we may bemoreable to locallystimulate thecortex–some-thing that we were unable to do at the start oftreatment.At this stage in treatment,behavioralchanges may be more closely tied to what iscommonly thought of as local cortical neuro-psychological functions. In other words, localsite feedback and local site recovery may be ad-dressable only after global feedback and reor-ganization has taken place. This might alsomean that following LENS treatment, furtherlocalized treatment with traditional neuro-feedback might have more affect than it wouldhave had previously.
In an interesting side note, a highly func-tional scientist was put on an older LENS sys-tem,andnotonly feltnothing,butwas unable tobe overdosed by extremely high levels ofbrightness. It maybe thatone of thedefiningas-pects of functioning well is that the brain is ableto flexibly respond to high stimulation input, atleast in relatively short exposures.
Cortical Permeability. In the early days ofusing EEG-driven feedback, it was noticed thatthe EEGs of high-functioning individuals wererather quiet, low amplitude recordings. In con-trast, the EEGs of dysfunctional and physicallytraumatized individuals were typically filledwith high-amplitude, low frequency band ac-tivity. Recollect that the cortex is one of the lastorgans to develop both ontogenetically andphylogenetically. The ostensive purpose of thecortex is to provide the integration and inhibi-tion of subcortical brain center activity, whichresults in theappearanceofourhigher function-ing capabilities.
The appearance of this EEG slowing that isseen as high amplitude delta, theta, and alphaactivity, has been, in the view of traditionalEEG and neurofeedback circles, considered aproblem. Activity in these frequency bands isoften inhibited during neurofeedback. Discus-sion of delta, theta, and alpha excesses was andis often prominent in exchanges of ideas about
treatment. Yet delta, theta, and alpha activitymay not be the entire problem because activityin these bands is commonly present whenhigher functions are not engaged.
Occasional high amplitude activity in lowfrequencies (which is often seen as pathologi-cal) may be present in individuals who not onlyfunction well, but who are exceptionally cre-ative. These exceptions are not understood.Thus one needs to be careful about gliblypathologizing all EEG slowing, just as spinalanomalies were overly pathologized early inthe history of MRI.1
In individuals having problems, however,the presence of activity in these slower fre-quency bands may translate into sections of thecortex, by their impaired inhibitory function-ing, permit the delta, theta, and alpha activity toshow themselves and be recorded at the scalp.That is, these areas of the cortex no longer func-tion properly, and do not inhibit the low fre-quency activity. It is the poor functioning of thecortex that fails to inhibit the physiology thatgives rise to the excessive EEG activity, whichallowsthehighamplitudeEEGactivity tobere-corded; that is the problem–not the activity it-self. The task, then, of the treatment is to bringback the functioning of these impaired sectionsof the cortex. The sign that these areas are re-turning to normal function is twofold. First, theEEG amplitudes become inhibited and lower.Second, functional improvement results. Theobject is to reduce thepermeabilityof thecortexso that it regains its inhibitory and integrativefunctions. This, in turn, permits higher function-ing to return.
Decreases in the Amplitude and VariabilityofLowFrequencyActivity.Therewere,andare,decreases inEEGamplitudeandvariability thataccompany LENS feedback if the initial ampli-tudesarehighenough.Decreasesappearacrossthe entire 1-30 Hz spectrum, but especially inthe low frequency 1-12 Hz EEG range, includ-ing that activity which is clearly and even prob-ably attributable to artifact.
These decreases are sensitive to the level ofintensity of the feedback. There is a window atany time in which the feedback intensity willdecrease the amplitude and variability. If theintensity is too low or too high–a Yerkes-Dodgson curve–amplitude reduction will notoccur. In fact, if the intensity is (resonant and)
Len Ochs 23
too high, the amplitudesmay rise, as mentionedabove.
The range of intensity in which the ampli-tudesdropwillvarywith thephaseof treatment.For those with the energy and stamina, higherlevelsof feedbackwilldecreaseamplitudesandstandard deviations early in the treatment. Astreatment progresses and the patient becomesmore sensitive and less hyper reactive, the in-tensity will need to be reduced in order to con-tinue to reduce the levels of activity. Reducingthe level of intensity is necessary to reduce theamplitude and standard deviation, and toincrease the functioning the patients.
These evoked (by feedback) amplitude andvariability reductions may reflect, on a neur-onal level, organic events which parallel the re-covery of energy, mood, and cognitive capaci-ties. These alterations in functional reactivityappear torepresent thequietingof thebrain,andthe containing of emotional and attentional im-pulses in a state of ambient readiness. The re-covery of skill was apparent in both those whohad clear mechanical and physical trauma, andthose who suffered lifelong energy, emotional,anxiety, and cognitive functional problems.
This lowering of the EEG’s amplitude usingthe LENS stands in contrast to other attempts toincrease amplitudes of the same EEG bands us-ing traditional EEG biofeedback. Whether it isthe feedback itself, the desensitization process,alternate offset polarity, or some other elementof the procedure that automatically affects theamplitude and variability decrease, the keypoint is that these decreases occur in the LENSprocess without the treatment directing this,which is so characteristic of traditional EEGbiofeedback. The implication is that some ele-ment(s) in the LENS treatment process triggersa self-organizing/corrective mechanism in thebrain which optimizes functioning, and whichrequires no conscious involvement of theindividual receiving the feedback.
In addition to the frequent appearances ofEEG slowing, we encounter infrequent in-stances of patients with EEG suppression, orvery low amplitude and low standard deviationEEG activity. These have been most frequentlyseen in chronic fatigue and fibromyalgia, andusually interlaced with depression. Depres-sion, seen apart from occurrences of chronic fa-tigue, is most often accompanied by elevation
in EEG activity. Ordinarily we have screenedout those with unusually low amplitude EEGactivity (less than1 μV) because theyhavebeenparticularly refractory to our methods.2
One more type of EEG activity is importantto mention: normal or high amplitude EEG ac-tivity, accompanied by standard deviations ofbelow 1. The EEGs of those with these abnor-mally smooth EEG recordings are often seen toshow dramatic rises in elevation followingLENS treatment, often accompanied by in-creases in functioning. This appears to be a dueto a treatment-induced lifting of suppression ofthe EEG. The increase in functioning may bedue to the freeing of energy bound by theneurochemistry of suppression. Those withproblems functioning speak of the enormouseffort it takes to think,organize,plan–inshort tocompensate for both their symptoms and due tothe suppressive effects of neurochemical pro-tection.
Diagnostic Considerations. The LENS hasbeen successfully and reliably used with au-tism, Asperger’s syndrome, post-concussivedisorders, depressive disorders, post-traumaticstress disorders, attention deficit disorder withand without hyperactivity, chronic fatigue syn-drome, fibromyalgia, and spastic paresis fol-lowing cerebral vascular accidents. The im-provements have been significant enough tohave made noticeable differences in the lives ofpatients, both at home and at work. It may bemore useful to think about the above disordersas variations of a single disorder (cortical per-meability or insufficiency), in which the cortexis inadequate to the task of inhibiting thebioelectrical activity.
The Potential Central Locus of “Periph-eral” Problems. Most pathology is treated pe-ripherally, even when there are known centralnervous system mechanisms. To date, periph-eral treatment has been attempted though exer-cise, diet, etc., except where frank neurolepticor neurosurgical intervention has been in-volved. For instance, fibromyalgia is typicallyseen as a muscle problem, since the tenderpoints have been muscular, even though thebalance problems, mental fog, and fatigue aretypically seen as central problems.
The LENS provides a behavioral way to di-rectly influence central mechanisms versus theindirect means used in traditional EEG feed-
24 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
back. With the LENS, the signals picked upfrom the brain are ultimately fed back into thetissues of the brain. The information the LENSfeeds back to the brain has no graphic or sym-bolic meaning, as does the information fromtraditional EEG neurofeedback, so there isnothing to interpret. However, while the infor-mation is fed back directly into the brain, it isalso not targeted (i.e., certain frequencies arenot associated with particular functions) andthere is no selectivity of where the feedbacksignals go in the brain.
It is true, however, that only one site at anyone time establishes the resonance source forthe feedback and that is the site of the activeelectrode. So while the feedback is believed topermeate all of the brain tissues and is non-spe-cific in that sense, it remains resonant only withthe site of the active electrode, the site whosedominant frequency is generating the basis forthe feedback signal (feedback frequency =dominant frequency + offset).
The extent of the promise of this approachcan only be imagined. Emerging theories ofbrain function, specifically with regard to theself-organizingcapabilityof thebrain,will findthe LENS a significant intervention model forboth clinical treatment and pathology simula-tion studies.
The Corrected Technical Inadequacy Un-corrected: Alternating Hemispheric Feedback.One of the more interesting sides of exploringthe LENS has been the extent to which precon-ceptions about accuracy have been unneces-sarily attached to efficacy. There were clearinaccuracy problems in our first generationsoftware, causing the left and right lights tostrobe 180 degrees out of phase. It was assumedthat they had been flashing in phase synchrony.When the lights flashed at lower frequencies,however, they were observed to flash togetheronly inconsistently. The asynchronously flash-ing lights were called to the attention of the pro-grammer with the intention of emphasizinghow remarkable it was to obtain good resultswith phase dyssynchrony.
As the second generation software was de-veloped, left-right flash phase synchrony wasinitially looked at as an imprecise sloppiness,and not included. While the desensitizationprocess seemed identical in the second-genera-tion system, the results seemed to hold less
well–until the programmer was persuaded tosupply an option for permitting the lights tostrobe180degreesoutofphase.Additionally, itwas suggested that alternating hemisphereswere stimulated with the left-right alternatingfeedback. This strategy seemed to inhibit highvoltage activity relatively rapidly across thespectrum. The use of alternating light feedbackwas especially useful later in treatment. Usingalternating feedback as the first element oftreatment prevented treatment from having thecarry-over between sessions that it did when itwas used later in treatment, wherein it appearsto amplify treatment effects. The transfer oflearning value from alteration of phase later intreatment may correspond developmentallywith the acquisition of stereoptic vision.
Initially, it looked as if the work with alter-nating sides flashing might be an example, sub-ject to experimental verification, of the powerof accidental digressions from pre-planned de-signs. Initially it looked as if the left-right alter-nating stimulation was extremely significant ina number of ways. However, years later, thequestionchangedas towhether thiswas just an-other way of reducing the intensity of stimula-tion, only providing 50% of the intensity at anyone time. This question could be resolvablenowbydoingathoroughanalysisof theelectro-magnetic field emitted by any visual stimula-tion device so that the concurrent visual andelectromagnetic influences can be understoodfor their individual contribution to any observedphenomena.
Consciousness Is Optional. Psychologistsand traditional biofeedback therapists tend tohold to the model of treatment as a consciousprocess. Yet an unknown percent of patients re-ceive therapy that is primarily conversationalfor long periods of time with minimal concreteresults (even though they may report feelingbetter). Non-psychotherapeutic psychiatrists,on the other hand, tend to see medication as theprimary component in the recovery and symp-tom alleviation/management process, relegat-ing the patient’s conscious participation andlearning a secondary, if not functionally irrele-vant role.
The LENS appears to offer a behavioralnon-pharmacologic, non-surgical and non-psy-chotherapeutic way to influence behavior, cog-nitive function, and feeling states, especially
Len Ochs 25
with regard to symptoms that result from me-chanical and/or psychological trauma.LENS isbehavioral and not medical because the signalsare profoundly minimal in intensity. It seemslikely that functioning, and not structure is di-rectly influenced; the adaptability of the indi-vidual and subsystems of the individual are in-fluenced, and adaptability is learning.
Our subjects show significant decreases inEEG amplitude and standard deviation withoutspecific instructions to suppress this activity.LENS, therefore, complements both pharma-cologic and psychotherapeutic techniques.Conscious self-development associated withpsychotherapycanbevaluable,butcanproceedbetter when the patient’s consciousness isclearer and thereby more able to process infor-mation.
Is It Self-Regulation Even Though It Is Not aConscious, Deliberate Process? The use of theLENS has been criticized as inducing passivechange in the patient, which has little chance ofpromoting either a sense of empowerment orlong-term change in the patient’s psychologi-cal status. It is here hypothesized that theLENS, instead, shortens treatment by eliminat-ing a major portion of the time-consumingfeedbackprocess,clarifies thepatient’s tenden-cies tocontrol the inner flow of consciousexpe-rience, and still permits the chance to desensi-tize, drop defenses, and allow neurochemistryto return to productive homeostasis. Further,the EEG disentrainment supports, but does notforce, the patient to experience unfamiliarstates of consciousness that enhance thechances of recognizing these states with furthertreatment. While the person receiving theLENS treatment may feel as if they are “not do-ing anything” and are not involved in a con-scious learning process, they have nonethelessbrought themselves to a setting that is structuredtoallowtheirbrain toadaptand learnat aneuro-logical level.
Traditional neurofeedback therapy undoubt-edly contributes to the acquisition of self-regu-latory skills, as well as operantly conditioninghealthier brainwave patterns. However, theelimination of the lengthy and hard work infront of a computer screen with LENS treat-ment still seems to promote acute patientawareness of the operation of his or her defen-sive structure and process. The acquisition of a
state of passive-allowing of experience seemsfacilitated by the LENS as it increases the pa-tient’s awareness of being drawn into differentstates of consciousness.
Most of our self-regulatory processes arenon conscious, and not voluntary. To take on amission of micromanaging even a significantportionof these non conscious processes seemsto me to significantly reduce one’s availableconscious resources for tasks usually requiringlarge amounts of consciousness: learning newskills, and appreciating and enjoying life. Itseems ideal to me to find ways to maximize ournon conscious skills, so that we can find greaterease and clarity for our conscious lives.
Is the EEG Really Necessary to Drive theFeedback? This question is of central impor-tance. If the EEG is unnecessary to enhance theclarity and ease of our conscious experience,then ways can be found much less expensivelyto efficaciously use the fixed and/or pre-set fre-quency feedback in treatment.
There were several inadvertent triple blindstudies conducted during the history of theLENS.Tripleblindstudiesareoneswhereevenan experimenter does not know who gets whatprocedures. Not only were the subjects and ma-chine operators blind to the study, but I knewonly in retrospect exactly what happened. Un-beknownst to me or anybody else, during theuse of our earlier light feedback system, it wasdiscovered that the EEG had somehow beendisconnected from the lights and that the flashrate had remained at 4 Hz regardless of the in-strument readings to the contrary. After someinvestigation it became clear that there was abug in the program, installed by accident by theprogrammer after he “upgraded” the software.This bug prevented any change in the LENSprogramming without effectively disconnect-ing it from the EEG.
Reviewing the records of the half-dozen pa-tients seen during the time of the problem, allwere found to have regressed during the periodthat the EEG was disconnected from the visualfeedback. They were all either more hypersen-sitive, or more depressed. Patients were pro-vided with enough free treatment to correct theproblem and they began to progress again.
This experience yielded several differentconclusions.First, itappears thatusingtheEEGto influence the feedback stimulation rate is in-
26 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
deed necessary and useful. Second, programsthat were developed that intuitively compen-sated for the irritating fixed-frequency feed-back by dropping the intensity of the light feed-back that was originallyused further reinforcedthe utility of very low intensity levels. Third,thedefault fixed frequencywas changed from 4Hz to 20 Hz, to guard against inadvertent deltaand theta feedback occurring in the event of aprogramming error. Last, considering the ac-tual effects of over stimulation conditions inreplicating pathological states and functioning,it may be possible that we can better study cen-tral nervous system problems by using theproper kinds and levels of feedback stimulationto experimentally replicate and even tempo-rarily evoke problems in the brain to moreaccuratelystudybrain functioning, impairmentand recovery.
Frequency of Treatments. The optimal treat-ment schedule is one that leaves the individualrefreshed. There is no treatment schedule thataffects everybody the same way. Treatmentscan be effective when delivered on a daily basisif the patient can tolerate this level of feedback.On the other hand, it is possible to leave the pa-tient slightly disoriented, fatigued, and with aheadache from sessions which are too frequentor long in duration, or where the offset is toolow. While each patient is different, these fac-tors generally underlie clients’ reported post-session discomfort. With such patients, muchless frequent treatments may be the ones thatspeed the course of treatment the most. Treat-ment effects do appear to need a critical mass oftreatments to overcome the rigidity of thesystem that perpetuates the symptom systemsand pathology.
The therapist must be willing to rely on thesigns of subjective discomfort of the patient,such as fatigue, rigidity, obsessiveness, and de-pression that will not respond, and be willing totake the risk of giving too little feedback by re-ducing the stimulation even to such smallamounts that it seems ridiculous (i.e., one sec-ond per month) if need be. Thus while the rangeof feedback intensity dose can be enormous(e.g., ranging from three sessions/day to sixseconds per week) the primary cues for deci-sion making all come from the patient to thetherapist who is willing to risk anxiety and theappearance of being foolish, but who will, to
advance the welfare of the patient, reducefeedback intensity.
One of the seductive elements in the use ofthe LENS is that longer treatment sessions canappear to work well for some treatmentpopula-tions, such as autistic children. This may fit intopreconceived ideas that a therapist may haveabout the necessity of lengthier sessions. Theconsequence of longer sessions is that whilethey work in the short term, on a week-to-weekbasis theycontribute toaslower pace for theoc-currence of improvements. The therapistsmaintain that longer sessions do work for thispopulation. My response is “But have you triedbriefer . . . ?”
Duration of Treatment and Factors that De-termineTreatmentLength.Thedegreeofsensi-tivity to the LENS feedback, how rapid the rateof desensitization, and the pre-existing dura-tion of the symptoms and efforts to compensatefor them are the best determinants of the dura-tion of treatment. For example, the average du-rationof treatmentfora formerlyhighfunction-ing,multi-taskingpatientwhohadaheadinjury2.5 years prior to treatment, is approximately 6sessions with seven or fewer seconds of feed-back during each session. If the person had life-longproblemsprior to the trauma, the treatmenttime ranges from 40 to 70 sessions. If the prob-lemisseverepost-strokeorspinalcordbruisingparesis, the course of treatment may numberinto the hundreds of sessions. However, forthose with mild to moderate stroke, even withparalysis, shocking relief from paralysis maybe seen in between 6 and 14 sessions. An aver-age of three sessions has produced startling re-sultswithpeoplewhohavebeenoverlystressedby work and/or home conditions over severalyears. No matter if the patient is suicidal, if theywere high functioning before the protractedstress their treatment has averaged threesessions.
Reducing Treatment Time with Offsets. Theantecedent systems to the LENS were designedwith offsets from the start, originally to reducethe chance of elaborating a seizure that mighthave been triggeredby the originalbright flash-ing feedback lights. At that time offsets werecalled “leading frequencies,” because it wasthought that they led the dominant frequency torise or lower. The term “offset” was felt to bemore descriptive.
Len Ochs 27
If the feedback signal frequency could neverequal the peak, or dominant frequency, two ef-fects were anticipated. First, the feedback fre-quency might not elaborate seizure activity ifthere was a tendency toward seizing. Second,the offset feedback frequency might shift en-ergy away from the seizure frequency, whichwould be the peak EEG frequency at that time.In drawing energy away from the dominant fre-quency, the amplitude of the dominant fre-quencywouldbe lowered,corresponding to theeffect ordinarily seen.
Defining Frequency Offset. The offset eval-uation originated from examining patient datain a typical year-end review. Up to that time werotatedthrougheachof thestandardoffsetsof5,10, 15, and20 Hz ateachsitewe treated.Duringone particular year-end review of data it wasnoticed that patients considered more sensitiveshowed lower EEG amplitudes during the peri-ods when higher offsets (15 or 20 Hz) wereused; and patients considered more reactiveand less sensitive showed lower EEG ampli-tudes during the periods when the lower offsets(5 or 10 Hz) were used. If higher functioninglevels accompanied lower amplitudes, then itmight be wasting time to expose patients to off-sets that didn’t do much to lower their ampli-tudes. The task then became to design an evalu-ation that demonstrated the EEG response toeach of the standard offsets. It initially used abaseline of one minute, followed by each of theoffsets, structured as follows:
• One second of feedback with an offset of5, followed by one minuteof post baselinemonitoring
• One second of feedback with an offset of10, followed by one minute of post base-line monitoring
• One second of feedback with an offset of15, followed by one minute of post base-line monitoring
• One second of feedback with an offset of20, followed by one minute of post base-line monitoring
Toreduce thepossibility that relaxingduringthe 1-minute baseline would affect the EEGamplitudes during the stimulation, the baselinewas lengthened tosixminutes tobesure that thepatienthadstabilized in relaxationbeforebeing
exposed to the first offset. If the amplitudes ofdelta and alpha are measured after exposure tofeedback at different offsets from the measuredominant frequency, the amplitudes resultingfromeachoffsetcanbeassessed.Theoffset thatproduced the lowest band amplitude would bethe one to select during treatment to achievemaximum decrease in amplitude activity.
The problem with providing several differ-ent offsets in an evaluation, if the offsets arepresented in the same order, time after time, isthat order effects may be influencing the re-sults. In fact, it isprobably true thatordereffectsinfluence the observed responses of EEG am-plitudes to the offsets. To randomize the orderof presentation, however, brings its own prob-lems. In order to prevent the patient from beingover stimulated, there is limited opportunity topresent stimulation during any one session.Offset evaluations ordinarily provide a signifi-cantdoseoffoursecondsofstimulation,andarereserved for those patients who are sturdyenough to tolerate them. So it seems inadvis-able to do a comprehensive presentation ofstimulation with counterbalanced orders ofpresentation and hope to find the “real” or“right” offset. Rather, the offset evaluation isviewed as a starting place from which to derivethe offset.
Interestingly, it was found that the numbersdefined as offsets have face validity. A patientwho is reasonably insensitive and foggy at thestart of the treatment will often have an offsetcloser to 5 or 10 Hz. If the patient, in later treat-ment, declares that they are not much clearerand better functioning, one would expect that arepeat offset evaluation will show the offset re-defined at a higher number. The patient, then,will also seem more discriminant, less foggy,and more functional. And in fact, the repeat off-set evaluation often redefines the offset atcloser to 20.
Figure 3 displays an example of an offsetevaluation. It shows the response of the deltafrequency band amplitude and standard devia-tion to one second of feedback stimulation atthe fourdifferentoffset frequenciesof5,10,15,and 20 Hz. It can be seen that the most effectiveoffset frequency for reducing delta was 5 Hz.
Does the EEG Change with LENS Stimula-tion? There is usually a question in the minds ofboth the prospective patient as well as the pro-
28 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
spective therapist about whether the LENS ac-tually changes the EEG. After all, therapists us-ing traditional neurofeedback complained thatthey saw relatively little change in the EEGs ofsomeof theirpatients.Whilechangein theEEGitself may or may not be correlated with achiev-ing the kind of change that a patient wants, atleast it can serve as encouragement that some-thing positive may happen sooner rather thanlater. The offset evaluation has three purposes.First, as above, it empirically defines an offset.Second, it provides a chance for the non-sensi-tive patient to put a toe in the water and experi-ence a standardized dose of feedback. If the pa-tient is known to be very reactive (e.g., to light,sound, medications, weather changes, foods,odors, and other people), one can presume anoffset of 20, and use a less demanding proce-dure than the offset evaluation to provide an ex-perience. In either case we use a test dose offeedbackstimulationtobeassureaswecan thatthe experience leaves the patient comfortable.Finally, we can compare the baseline and feed-backsectionsof theevaluation tosee if theEEGhas changed in amplitude and standard devia-tion.
We have two choices in selecting an offsetfrequency to use in LENS sessions. One choiceis touse thegraphofdelta responses to thealter-native offset frequencies. The other choice is touse the alpha responses. Delta activity has al-waysseemedmore responsive thanalphaactiv-ity,perhapsbecausealphaactivitymaybemoregenetically determined. Therefore, we use thegraph of delta activity for selecting our offsetfrequency. This choice has proven more suc-
cessful than using alpha offset for reducingelevated amplitudes across the frequency spec-trum. In addition, delta offset responses are fa-vored over the reactions to offsets within thetheta band because clinical experience hasshown that using delta offset data was most ef-fective in reducing both delta and theta activity(in comparison with using theta offsets).
In Figure 4 it is clear that delta amplitude andstandard deviation dropped from the baselinefollowing feedback. In contrast to Figure 3, thisfigure presents the average of data from all fourof the offsets. However, it also shows that alphaamplitude and standard deviation slightly in-creased. This demonstrates that measurableEEG changes can be documented in a brief tenminute evaluation, with as little as four secondsof feedback being given during that time.
Reducing Treatment Time with Brain Map-ping. Quantitative EEG (QEEG) was discon-tinued in the early 1990s because it did not offerclear and reliable guidance in defining whichsites to work with and in what sequence. TheLENS practitioners were seeking treatmentplanning answers about patients who presentedmore complex problems. These problems cre-ated uncertainty about how best to bring aboutprogress, and especially in choosing electrodesites. A useful mapping system would graphi-cally specify the order and sequence of sites totreat. The operational definition of an “appro-priate” electrode site is one with reducedevoked EEG amplitude within five minutes.
It has been our clinical experience that bysimplymapping theamplitudeandstandardde-viation of the EEG at 19 or more electrode sites,we can specify electrode site sequencing andplacement. As a basis for treatment planningwith LENS this seems to speed the rate of EEGchange, wasted treatment time is avoided, anddiscomfort is minimized by choosing and treat-ingmultipleelectrodesitesduringeachsession,followinganorder fromlowest amplitude/vari-ability to greatest amplitude/variability.
EEG Coherence Issues. EEG coherence iscorrelated phase activity in a frequency bandbetween different EEG sites. Variability in theform of standard deviations can also be corre-lated, but is usually not talked about in relationto coherence across electrode sites. Interest-ingly a major EEG reference makes no mentionof coherence in its index (Niedermeyer & da
Len Ochs 29
14
12
10
8
6
4
2
05 10 15 20
Offset Frequency
Mic
roV
olts
Mean Standard Deviation
FIGURE 3. Delta Response to Different Offsets
Silva, 1999) making the following discussionhighly speculative.
The Clinical Side of Coherence. There arepatients who are easier to treat, and those whoare more complex. “Easier” means that ampli-tudes reduce and stay low at the sites treated.The easier patients do not suffer an exacerba-tion of their symptoms after initial treatments.“Complex” means that (a) frequency band am-plitude at any site may increase after it lowers,(b) another frequency band may increase in ac-tivity at the site monitored, (c) band amplitudesat the same site may see-saw (alpha and deltaamplitudes may see-saw), (d) band amplitudesat one site may fall while the same band ampli-tudes may rise at a different site, and (e) symp-toms may flare up after the session. Coherenceproblems may be recognized by any of theseitems. On the topographic maps, map areasshowing pools of the same color are, in fact,showing areas with the same amplitudes of ac-tivity within a frequency band. The sites, then,
have correlated amplitudes which may reflectthe probability of high coherence. A review of100 topographic maps, sorted into piles oflow-to-high areas of similar amplitude wasroughly correlated with patients who were, re-spectively easy-to-hard to treat. This evaluationwas crude and bears systematic and precise in-vestigation.
Hunches About Coherence and Systems.Correlated activity may mean that the activityoccurs in a system, an integrated pattern. Aswithanysystem, theactivityasawholebehavesdifferent than the behavior as the sum of theparts. Changes in the activity at specific sitesthatarepartof a systemwouldbeexpected tobemore resistant to change, and especially to last-ing change. Therefore, it is expected that a sys-tem would need to be worked with as a wholesystem, rather than at just at one or two sites.
Components of Systems. There are three ma-jor components of systems: (a) sites that are notinvolved in a system, (b) sites that react to the
30 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
9.008.007.006.005.004.003.002.001.000.00
9.008.007.006.005.004.003.002.001.000.00
Mic
roV
olts
Mic
roV
olts
PreBase
PreBase
Condition
Condition
Feedback
Feedback
Average Amplitude
Average Amplitude Delta
Average Amplitude Alpha
Average SDs Delta
Average SDs Alpha
Average Standard Deviations (SDs)
FIGURE 4. Offset Evaluation: Averaged Frequency and Standard Deviation Changes
activity in a system and either amplify the sys-tems activity or dampen the system’s activity,and (c) the generators of the system’s activity,influenced by the other components. When asite responds to treatment and remains affectedwithout reboundingafter thesession, itactsas ifit isunrelatedto thesystem.If therewerenosys-tem present, as is sometimes the case, the per-sonwouldexperiencea“miracle,”asuddenandnoticeable reduction in symptoms.
Ramifications of Coherence for the LENSTreatment Planning: A Story. As a metaphor,let’s say that there are three types of people in ariotous intersection. First, there are the by-standers. They are the ones who are easilymoved by those trying to reduce the noise in theintersection. They are not particularly involvedin the activity, and do not contribute to thenoise. But their presence does encourage theothers fomenting the noise.
Second, there are the collaborators. Theyhave varying degrees of interest and involve-ment in generating the noise in the intersection.They provide reinforcement and energy for theinstigators of the noise and they derive satisfac-tion from their involvement.The degree of easewith which the collaborators can be moved is afunction of their relationship with the instiga-tors, and with the amount of energy they have.Last, there are the instigators. They provide theenergy for the crowd.
In any system, there are the energeticsources, the other components that are influ-enced and in turn influence, and the uninvolvedparts. The trick for treatment is to discover howto move the less-involved parts, continue to re-duce the overall energy in the system, and tonudge the system toward lower noise andgreater flexibility.
It may be said that our job is to reduce thenoise in the above intersection: to increase theease with which messages are exchanged in thebrain. If we ask each person in the intersectiontomove, theones that firstmovewillbe theonesleast involved: the bystanders. With the by-standersabsent, there is less encouragement forthe collaborators and the instigators.
The next to move will be the least motivatedof the collaborators. Their absence providesstill less reinforcement for the more motivatedcollaborators and the instigators, making it eas-ier to move more collaborators. In a reiterative
fashion, the crowd thins, with more collabora-tors losing motivation as it does. In the end, theinstigators may or may not be moved. How-ever, there is now muchmore room for traffic toflow and the intersection can be more func-tional. It is the function of the LENS map toempirically define which of the sites are by-standers, collaborators, and perhaps, the insti-gator(s)–the generators. Of course this is some-thing of a conjecture and may to a large extentbe unnecessary. However, it does provide amethodology for approaching the complexclinicalpictures with which we deal. In fact, us-ing the LENS map the way we do may be one ofthe factors contributing to the relatively shorttreatment times. There may well be alternativeways of organizing the treatment approach thatcould result in further reduction in treatmentduration, more efficacious results, or both.
The Brain as a System. There are such thingsassimpleproblems.Thesecasesgenerallyhavea sudden onset of symptoms without aninter-generational or genetic basis to the symp-tom. The treatments are even simpler for thosepeople who were especially high functioningbefore their injury or trauma. Treatment ofthese individuals with acquired CNS problemsis often a joy. They may be the cases sharedamong colleagues, the ones which impress theaudiences, and propel the sales of EEG equip-ment. For these instances, it is quite plausible toapply traditional neurofeedback or the LENSmethodtooneor twoof thestandard10-20elec-trode sites and watch the miracles happen. Un-fortunately, informal surveys of therapists us-ing all of the current models of neurofeedbackequipment on the market evoke reports thatfrom 50 to 80 percent of the time the therapistsdo not feel like they know what they are doing.They feel lost about treatment direction anddisappointed at the results they are obtaining.
Achieving success with LENS at any oneelectrode site (i.e., reducing EEG amplitudeandvariability)canleadtobehavioral reboundsand reactions such as transient hyperactivity orfatigue.Whendoing topographicmapssequen-tially at different electrode sites, it is quite ap-parent when the problems that a person hasseem to be occurring within a system or multi-ple systems of activity as measured across thescalp. The complex cases invariably showmany kinds of EEG activity (i.e., unwanted
Len Ochs 31
rises in amplitudes and variability) that arecaused by isolated successes at the sites thatwere treated in isolation. If a site or a few sitesare treated without recognition of the extantsystems, then there are often untoward post-session problems.
This hypothesized activity occurring in sys-tems may be the same as hypercoherence: thesame frequency appearing at multiple sitesacross the scalp at the same time. If these sitesare linked together, and if the therapist is treat-ing one or a few of the sites, changes in thosefew sites will cause a reaction in the rest of thesystem which may both evoke strong concernor worry in the patient, and create managementproblems in treatment, as well as cause unnec-essarily long and uneconomical treatmentprocesses.
The topographic mapping process that weutilize holds promise to enable the therapist tounderstand how to approach the areas involvedin the pathology in a graded, elegant way, andwithout any biases based on “known facts”stemming from neuropsychology or literaturereports.Mappingreduces thechances thatasta-tistically unusual site plays a prominent part inthe functional pathology. It reduces the chancethat the unusual site or combinationof sites willbe missed, delaying the problem’s resolution.
Themapsshowthefrequencybands’evokedamplitude undulations shrinking spatially,dampening, and eventually stabilizing in am-plitude as treatment progresses. This translatesinto being able to observe the chaotic energysystems moving around and rearranging them-selves across the scalp surface as they becomeelectrically less noisy. The surface maps aretransformed into other graphs that specifywhich sites are to be worked with, and in whichsequence (see Figure 2).
Having these maps of evoked activity avail-able also permits the therapist to compare cur-rent versus previously measured values. Whenthere is too much of a discrepancy, the loss ofaccuracy indicates that the map is no longer afaithfulguide to treatmentand that another mapis needed to accurately predict the strategic sitesequences.
Sensitivity vs. Hypersensitivity.When pa-tients firstenter treatment theytendtosee them-selves as overly sensitive. In fact, they tend tobe quite reactive, but quite insensitive. An ex-
tremely reactive individual is so reactive tostimuli and caught up in the emotional, cogni-tive, glandular, vascular, immunological, and/ormotoricelementsof the reactions that there isliterallyno opening for being aware of the stim-uli.Hypersensitive individualsare rarelyawareof much about their situations or of their feel-ings. They are aware of their reactions to thesesituations and feelings, rather than of the situa-tions themselves. For example, they may beoverwhelmed by their reactions of discomfort,or overwhelmed by the difficulty of takingthings in.
The LENS ordinarily reduces the amplitudeand variability of the EEG across the spectrum.Inotherwords, theEEGbecomeslesshyper-re-active to the LENS feedback. This may be afunction of the enormous dynamic range of thefeedback intensity, which can potentially bevaried by 100,000 gradations from the weakestto most intense feedback intensity levels. Turn-ing the feedback on and off will at times showcorrelated amplitude and variability changes inthe EEG on the screen, even though patientscannot feel the feedback. As the patient’s hy-per-reactivitydrops, thepatient tends to experi-ence a subjective increase in ease, greater abil-ity to follow conversations, to understand whatis read, and to think more clearly. Clarity is a re-flection of greater perceptual acuity and a less-ening of mental fog. Often there are reports ofincreasing quiescence and decreases in rest-lessness. The intersection,as in theabovestory,has become quieter and more functional. An-otherway toput it is that thepatient isbecomingmore sensitive–but less hyper-reactive. The re-sult is that the patient is more aware of the envi-ronment and of inner feelings; more aware oflikes, dislikes, needs, and satisfactions of thoseneeds. The good and bad news is that while thepatient can be happier and unhappier, there ismore chance, because of decreased hyper-reac-tivity, to be more thoughtful about life.
Sensitivity: Its Acknowledgment, Manage-ment, and Benefits. The phenomenon of sensi-tivity to feedback intensity is one of the mostintriguing aspects of the LENS. There is an ap-parent relationship between dysfunction andreactivity to stimulation. Patients express thisverbally and/or motorically. This can also beobserved during treatment as increasing delta,theta, or alpha activity across a number of sites,
32 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
withouta return tobaselinewithinfiveminutes.These factors led me and my colleagues to con-sider alternative treatment models arising fromour new views regarding brain trauma and itsresolution.
The apparent plasticity of the dysfunctionunder thefeedbackof theLENSitselfcastscon-siderable doubt on the traditionally held viewthat much post-trauma dysfunction is attribut-able to the trauma; perhaps it is largely attribut-able to the brain’s own protective mechanisms.Rather than working with trauma-inducedbraindamage, in thecaseofbrain injurywemayneed to be working with the brain’s ownself-protective neurochemical systems.
What is most important is that we apparentlyare far more sensitive than we have ever ex-pected, at least when we become injured or inanywaydysfunctional.Muchof themedicales-tablishment, and to a certain extent the psycho-logical rehabilitation establishment, has takenup the “Jack LaLane” exercise, gain-through-pain approach to rehabilitation. This was thementality which was originally applied to theLENS work until it was recognized that the op-posite was the only approach that consistentlyproduced positive outcomes. It has turned outthat the more we take into account sensitivity,making treatment as gentle as possible in previ-ously unimaginable ways, the neuronal strengthof thepatientshasbeensupported,andrecoveryfollows far more often than not.
This shift in paradigm regarding the units ofanalysis, intervention and mechanism of actionoften means that the feedback intensity is keptto a minimum. During the early sessions thetherapist needs to know how to be content tomake very small interventions until the patient,with decreased symptoms, becomes ready formorepungencyinthefeedback.Ithasonlybeenwhen the patient’s sensitivity has been care-fully considered that maximum speed of treat-ment isachieved.Otherwisevaluabletreatmenttime is spent recovering from treatment-in-duced relapses.
Suppression. EEG activity suppression. Al-most without exception, all relatively high am-plitude EEG band activity drops (even withhigh beta) following LENS feedback. How-ever, low amplitude and standard deviationscan and do rise. When this occurs the low activ-ity is understood to have been suppressed. Pre-
scription medicationcan cause this kind of sup-pression. Internal automatic self-medicationwith perhaps inhibitory neurotransmitters mightalso cause this kind of suppression.
At first it was thought that the rises in ampli-tude that occur with the LENS treatments weresigns of over stimulation and signs of pathol-ogy. However, it has become apparent thatmost amplitude and standard deviation in-creases occur in the context of increasinglycompetent functioning–although not infre-quently in thecontextofsomenarrowlydefinedandextremelydisruptivesymptoms.Forexam-ple, while the patient is becoming more relaxedand less depressed, there may be an increase inseizures, tics, temper, muscular pain, toiletingaccidents, and perhaps substance abuse. Theseare not seen as side effects of treatment now. Incontrast, they are now seen as transition statesduringwhichshort-termcompensationsandin-hibitions have been released. They occur inthose with histories of the observed problems.It may be that the very problematic, potentiallydangerous, and most likely socially very em-barrassing symptoms were intuitively suppres-sed–and most likely forgotten, until the currenttreatment.
These symptoms, depending on their pathol-ogy and severity, typically last a week, and thenremit. They may also re-occur when a virus,other infection, or other body change is stillpre-clinical and unobserved. However, afterone or two infection or bodily change cycles,they no longer appear.
It is extremely important that each prospec-tive patient be interviewed for such previoushistorical symptoms. Their presence is not nec-essarily a contraindication for the LENS ap-proach. But if they were present at one point inhis or her life, it is a chance to ask the patientwhether the symptoms for which he or she isseeking relief are important enough to outweigh the risk of re-encountering for a shorttime the intensely problematic symptoms fromearlier life. It takes a relatively short while, dur-ing treatment, for the brain to integrate–ratherthan inhibit–problematic pathophysiology, andthus bring marked relief.
The What, Why, and How of the LENS. Thereare three considerations concerning the LENSand its mechanism: What is happening, why ithappens, and what treatment strategies bring
Len Ochs 33
about the effect. These can be labeled, respec-tively: permeability, inhibitory neurotransmit-ter activity alterations, and applied chaos the-ory. The statements addressing each area ofconcern are testable.
What. Changes in cortical permeability: Ithasbeenobserved that individualswithchroniccentral nervous system functioning problemshave higher levels of recordable low frequencyelectrical activity at scalp sites. It has furtherbeen observed that as the functioning of the in-dividual improves with treatment, the ampli-tudeof theEEGdiminishesacross thespectrumat each scalp site.
On a descriptive level, the most parsimoni-ous way to picture what happens as functioningimprovesandas themeasuredevokedEEGam-plitude drops, might be in terms of decreasingpermeability of the cortex: the higher ampli-tude activity probably remains present sub-cortically. It may be that it is simply not mea-surable at the scalp surface as the cortexre-assumes its integrative capacity and blocksthe appearance of the higher amplitude sub-cortical activity at the surface. The use of in-dwelling (needle) electrodes at various depthssimultaneously may help differentiate corticalfrom subcortical activity, and show with treat-ment, evidence of increased cortical activationas differentiated from subcortical activity.
Why. Inhibitory neurotransmitter activity al-ternations: Feeding back frequency informa-tion that is different from that which is mea-sured, but nevertheless still a function of thefrequency measured, may place differentneurochemicaldemandson thesynapseswhichfeed the measured activity. If there is post-trau-matic inhibitory neurotransmitter activity in-terferingwithcortical function(i.e.,makingthecortex more permeable) and if the mechanismperpetuating this activity is disturbed and is al-tered, then the synaptic neurotransmitter mixmightbe altered to once again permitdecreasedpermeability and proper cortical functioning.
How. Applied chaos therapy: Most neuro-feedback treatment focuses on the shaping ofactivity in one or two frequency bands throughvoluntarycontrolsatoneor twosites.Oneof thecomplaints about the duration of neurofeed-back treatment is that it takes too long and is tooexpensive. The sites commonly treated are, asoften as not, the ones showing the highest mea-
While treatment of acute patients with goodpremorbid histories may respond to a simplertreatment strategy, such a strategy may not suf-ficeforpatientswithcomplicated, life-longhis-tories and symptoms. In contrast, without try-ing tospeedor slowtheEEGactivity, theLENSaddresses all of the of the standard 10-20 sys-tem scalp sites as a method to control the feed-back in a sequence based on a ranking ofsite-permeability (irritability) from least tomost. By using this method, the activity at boththe sites that have problems in isolation, and atsites that act in coherence systems, can be de-creased in a predictable manner. This may re-duce treatment time and expense in compli-cated cases, and increase the longevity of apositive outcome.
CONCLUSION
The LENS has shown significant effects inthe treatment of a variety of CNS mediated dis-orders. Ongoing research will be required tofully understand the mechanisms of action andalgorithms for directing treatment (e.g., site se-lection, feedback intensity, duration, etc.). Thefollowing are some tentative conclusions re-garding the benefits and underlying principlesof the LENS.
Treatment benefits include: decreased feel-ings of irritability, anger, fatigue, anxiety, de-pression, anddecreasedanginawhencausedbycorticalproblems. Improvedmentalclarity(de-creased “mental fog”), sleep, energy, concen-tration,attention,short-termmemory, improvedvision and speech when due to cortical prob-lems, and increased ease of functioning. Tangi-ble clinical improvements are typically notedwithin three to six sessions. Reductions in EEGamplitude and variability will often be notedwithinthefirst fiveminutesof thefirstsession.
The LENS in the Current Social/Scientific/Clinical Context. The following are issues ofconcern expressed by non-The LENS profes-sionals.
Invasiveness
In contrast to traditional EEG feedback, theLENScouldbeconsideredminimallyinvasive.
34 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
The field strength of the stimulation is only10-18watts/cm2,which is far less invasive thanmedication or electroconvulsive therapy, andmicroscopic in comparison to transcranialmagnetic stimulation or even in comparison tothe stimulation received from holding a cellphone to one’s ear.
Two attitudes are interwoven in this contro-versy. One idea is that consciousness is a re-quirement for self-regulation. If the regulationthat occurs is not conscious and intentional, it isnot self-regulation. Yet the spinal cord andlower brain centers are not only responsible formany of our life-support systems, but they alsocan learn and adapt quite nicely without con-scious intervention. In other words, we may bejust as smart subcortically (and unconsciously)as we are consciously. So it seems wasteful todevalue non-conscious self-regulation and tothrow away resources that can be mobilized forlearning and life enhancement. Furthermore,although conscious effort and work is involvedwith traditional neurofeedback, it is not somuch teaching self-regulation as it is facilitat-ing the operant conditioning of healthierbrainwave patterns.
The second controversy is the locus of con-trol issue, or who is in control, therapist or pa-tient? This issue seems to be grounded in thenaïve belief that traditional biofeedback placesthe patient in charge, and that he or she is trulyengaged in self-regulation. There is, of course,the implicationthatwhena therapist isadminis-tering an energy field, the process is controlledby the therapist. In fact, the design of the treat-mentprotocolused in traditionalbiofeedbackisalso under therapist control (i.e., whether to en-hance a particular high frequency activity andinhibit low frequency activity). Further, the op-eration of the threshold, which determineswhich EEG activity gets which kinds of rein-forcement, is likewiseunder therapistcontrol intraditional EEG biofeedback.
Similarly, the therapist isclearlyincontrolofthe structure of the LENS session, but is guidedbythepatient’s subjectivesenseofwhat iscom-fortable and uncomfortable. In contrast, whenusing theLENSprotocols, thegoalof theLENS
treatment is flexibility of neural functioning,and there is no unilateral influence on the brainto either produce more fast-wave activity ormore slow-wave activity. The patient’s brain isleft free to do as it needs to, when it needs to, asthe amplitude and variability decrease acrossthe spectrum.
Hopefully, both LENS and general neuro-feedback procedures will maximize the abilityof the patient to be self-regulating. However, itisnaive tohold thepremise that traditionalEEGbiofeedback places the patient in charge of thestructure of the treatment, or that neuro-feedback is teaching self-regulation in thesense of learning a conscious skill. It seems thatthe more important scientific concern needs tobe: Under which clinical conditions is LENS ortraditional neurofeedback most effective andefficient? Each system may have its owndomains of applicability.
Physical or Psychological Harm
The Thalidomide tragedy has made every-one aware of the importance of looking atlong-term effects of a prospective treatment,and rightly so. It is always worth reviewing theprobability that wherever there is change, thereis disruption. And whether good or bad, therecan always be unpleasant as well as beneficialeffects, even if the treatment is “entirely natu-ral.”Oneissuehere isnotwhether thereare“un-pleasant side effects,” but to identify what theyare. Side effects or adverse reactions have beennoted with traditional neurofeedback technol-ogy (Hammond, Stockdale, Hoffman, Ayers,& Nash, 2001) and in fact, if misapplied tradi-tional neurofeedback has the potential to evokeiatrogenic effects, including seizures (Lubar etal., 1981; Lubar & Shouse, 1976, 1977). Onceidentified, theprospectiverecipientof the treat-ment can weigh the benefits against the risks oftreatment. The unpleasant side effects of treat-ment discovered to date echo the unpleasant ef-fects of any other kind of change process,whether it ishypnosis, psychotherapy,biofeed-back, yoga, etc. With the LENS system, no pa-tientover the last three years has ever reported anew symptom; that is, one thathad never beforebeenexperiencedby thatpatient.However, anycurrent symptom, physical or psychological,can be temporarily exacerbated.
Len Ochs 35
Another issue here is to differentiate un-pleasant “side-effects” from disruptive signs ofhealth and recovery. As people become clearerabout theirownreactions toadifficult,unpleas-ant, and even treacherous world, they are in-clined to become more angry, sad, or anxious,and appropriately so. They are apt to becomeless tolerant of what ought not to be tolerated.However, it is the amount of increased thought-fulness and productivity about the noxious ele-ments of life that makes these reactions differ-ent fromthehyper-reactive,blindreactions thatcharacterized their lives prior to the LENStreatment. These considerations need to bemade clear when individuals are consideringLENS treatment.
Dearth of Literature
It must be acknowledged that apart from thisvolume, there is only a limited scientific re-search (Donaldson, Sella, & Mueller, 1998;Mueller, Donaldson, Nelson & Layman, 2001;Schoenberger et al., 2001) on the use of LENS.We know littleabout the effects of variable-fre-quency feedback on EEG activity. However,we now have considerable clinical experienceinworkingwithanumberofdiagnoses.Aswithmost clinical areas of application of traditionalneurofeedback,adequatelycontrolledoutcomestudies with LENS are lacking. Therefore, theinformed consent process with patients mustacknowledge these facts to allow patients tomake an informed decision about using a moreinvestigational treatment.
Fear of LENS Treatment Being Too Rapid
Finally we should mention a frequently ex-pressed concern about the LENS producingtherapist unemployment because it is too rapidor effective. It is true that the LENS often re-duces treatment time, making for more rapidpatient turnover, and placing new demands ona’therapist’s marketing skills. However, it alsooften increases a’therapist’s effectiveness,opens up treatment as an option to new popula-tions,andmakes treatmentmoreaffordableandenjoyable. Further, it increases the number ofpatientsa therapistcanhelp inshorter lengthsoftime.
Summary
LENS is an innovative type of neuro-feedback that has evolved over the past 16years. It involves the use of very weak electro-magnetic energy fields which are fed back tothe brain based on the brain’s dominant fre-quency from moment-to-moment. This feed-back is usually effective in reducing high am-plitude activity, in many cases shortening thelength of treatment that is required in compari-son with traditional neurofeedback. Treatmentsessions are brief, and because of the minimaldemands it places on the patient it is very ap-pealingtosomepatientsandopensuptreatmentoptionsfornewpopulationsofpatients.Thena-ture of LENS technology will also facilitatedo-ing double-blind, placebo controlled studieswhich can advance our field.
NOTES
1. Some proportion of activity in the different fre-quency bands seems healthy, with either too much or toolittle being potentially problematic. Delta, for example,seems to have a functional role in facilitating inner con-centration by suppressing extraneous cortical inputs. Adelta deficit can correlate with reduced frontal corticalregulation or gating of maladaptive behavioral impulsesor extraneous cues, and can be found in conditions suchas cocaine addicts, alcoholics, ADD, subtypes of OCD,and schizophrenia (Alper, Prichep, Kowalek, Rosenthal,& John, 1998). Increased theta band activity may beseen in highly experienced mediators, and increaseddelta and theta EEG activity have also often been foundin association with various kinds of cognitive activity,such as performing calculations (e.g., Fernandez et al.,1995; Klimesch, Doppelmayer, Russegger, & Pachinger,1996).
2. Offsets were originally implemented to reduce thepossibility of exacerbating seizure activity and EEGslowing. When amplitudes are unusually low, an offsetof zero may help to stimulate the physiology to increaseamplitude. However, we have very little experience tostate this with any confidence.
REFERENCES
Alper, K. R., Prichep, L. S., Kowalek, S., Rosenthal, M.S., & John, E. R. (1998). Persistent QEEG abnormal-ity in crack cocaine users at 6 months of drug absti-nence. Neuropsychopharmacology, 19 (1), 1-9.
36 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
Carter, J. L., & Russell, H. L. (1981). Changes in verbalperformance of IQ discrepancy scores after left hemis-phere EEG frequency control training. AmericanJournal of Clinical Biofeedback, 4, 66-68.
Carter, J. L., & Russell, H. L. (1984). Application of bio-feedback relaxation procedures to handicapped chil-dren: Final resort. (Project No. 443CH00207, GrantNo. G008001608). Washington, DC: Bureau of Edu-cation for the Handicapped.
Carter, J. L., & Russell, H. L. (1993). A pilot investiga-tion of auditory and visual entrainment of brain waveactivity in learning disabled boys. Texas Researcher,4, 65-73.
Davidson, R J., & Hydahl, K. H. (Eds.) (1996). Brainasymmetry. Cambridge, MA: Bradford Books, MITPress.
Diamond, M. C. (1988). Enriching heredity: The impactof the environment on the anatomy of the brain. NewYork: The Free Press.
Donaldson, C. C. S., Sella, G. E., & Mueller, H. H.(1998). Fibromyalgia: A retrospective study of 252consecutive referrals. Canadian Journal of ClinicalMedicine, 5 (6), 116-127.
Fernandez, T., Harmony, T., Rodriguez, M., Bernal, J.,Silva, J., Reyes, A., et al. (1995). EEG activation pat-terns during the performance of tasks involvingdifferent components of mental calculation. Electro-encephalography & Clinical Neurophysiology, 94,175-182.
Gleick, J. (1988). Chaos: Making a new science. NewYork: Penguin
Hammond, D. C., Stockdale, S., Hoffman, D., Ayers, M.E., & Nash, J. (2001). Adverse reactions and poten-tial iatrogenic effects in neurofeedback training. Jour-nal of Neurotherapy, 4 (4), 57-69.
Hughes, J. R., & John, E. R. (1999). Conventional andquantitative electroencephalography in psychiatry.Journal of Neuropsychiatry and Clinical Neurosci-ence, 11, 190.
Klimesch, W., Doppelmayer, M., Russegger, H., &Pachinger, T. (1996). Theta band power in the hu-man scalp EEG and the encoding of new informa-tion. NeuroReport, 7, 1235-1240.
Lubar, J. L. (1985). Changing EEG activity through bio-feedback applications for the diagnosis and treatmentof learning disabled children. Theory into practice.Ohio State University, 24, 106-111.
Lubar, J. F., Shabsin, H. S., Natelson, S. E., Holder, G.S., Whitsett, S. F., Pamplin, W. E., et al. (1981). EEG
operant conditioning in intractable epileptics. Ar-chives of Neurology, 38, 700-704.
Lubar, J. F., & Shouse, M. N. (1976). EEG and behav-ioral changes in a hyperactive child concurrent withtraining of the sensorimotor rhythm (SMR): A pre-liminary report. Biofeedback & Self-Regulation, 1(3), 293-306.
Lubar, J. F., & Shouse, M. N. (1977). Use of biofeed-back in the treatment of seizure disorders and hyper-activity. Advances in Clinical Child Psychology, 1,204-251.
Mueller, H. H., Donaldson, C. C. S., Nelson, D. V., &Layman, M. (2001). Treatment of fibromyalgia in-corporating EEG-driven stimulation: A clinical out-comes study. Journal of Clinical Psychology, 57 (7),933-952.
Niedermeyer, E., & da Silva, F. H. L. (Eds.) (1999).Electroencephalography: Basic principles, clinicalapplications, and related fields. Philadelphia, PA:Lippincott, Williams & Wilkins.
Ochs, L. (1995). Many kinds of depression are curable.http://www.flexyx.com/articles/deprcure.html
Peniston, E. G., & Kulkosky, P. J. (1991). Alpha-thetabrainwave neurofeedback therapy for Vietnam vet-erans with combat-related posttraumatic stress disor-der. Medical Psychotherapy: An International Journal,4, 47-60.
Persinger, M. A. (Ed.) (1974). ELF and VLF electro-magnetic field effects. New York: Plenum Press.
Quirk, J. A., Fish, D. R., Smith, S. J., Sander, J. W.,Shorvon, S. D., & Allen, P. J. (1995). Incidence ofphotosensitive epilepsy: A prospective national study.Electroencephalography & Clinical Neurophysiol-ogy, 95 (4), 260-267.
Rife, R. R. (1953). History of the development of a suc-cessful treatment for cancer and other virus, bacteriaand fungi. San Diego: Rife Virus Microscope Insti-tute.
Sandyk, R. (1994). Improvement in word-fluency per-formance in Parkinson’s disease by administration ofelectromagnetic fields. International Journal of Neu-roscience, 77 (1-2), 23-46.
Schoenberger, N. E., Shiflett, S. C., Esty, M. L., Ochs,L., & Matheis, R. J. (2001). Flexyx neurotherapysystem in the treatment of traumatic brain injury: Aninitial evaluation. Journal of Head Trauma Rehabili-tation, 16 (3), 260-274.
This article seeks to offer some historical background, an outline of the theoretical basis for how theLow Energy Neurofeedback System (LENS) works, and the approach to treatment which is evolving fromthe applied clinical work and research being initiated by OchsLabs. The LENS is still evolving at a rapidpace. It is thus impractical to conceive of this overview as being up-to-date for any length of time. Thereader is cautioned to avoid any conclusion that this information reflects current practice. The reader isalso cautioned to avoid seeing any information presented herein as a claim for the LENS to be efficaciousfor any condition, medical or psychological. This is the most objective depiction possible of the evidenceon hand for its benefits and risks. No claims are being made.
The reader is cautioned that the purpose of this article is to enumerate some of the phenomena,issues, and concerns which were encountered, and not to provide a decision tree about which settings,options, conditions, and choices are to be made in any particular clinical instance. The information aboutsettings, conditions, and treatment options presented are to exemplify the concepts. The actual numberof options and considerations in the treatment planning process are outside the scope of this article.Further, there is still not enough concrete research-based information about the particular benefits ordrawbacks of any particular setting or settings, or whether such settings are useful or necessary. Compo-nent analyses are needed to determine which conditions (protocols) are necessary and useful.
The reader of this article may find more questions being raised than answered. This is the nature of theopening of a new arena of observation and study. In this case, this arena is the area of behavioral bio-physics: the interaction of resonant (feedback) physical stimuli on brain functioning. It is possible to ask ofmost of the statements in this article, “What is the evidence?” “Where are the data?” In fact, after 15 yearsof this exploration there is still a search for the fundamental questions. Furthermore, after 15 years, howto do research with the LENS is only beginning to clarify itself.
APPENDIX BCNS Functioning Assessment
Name ____________________________________ Date of Birth _______________ Age _________
Today’s Date ______________________ Time _______________ Diagnosis __________________
Are you able to drive a motor vehicle? Yes Partially No Are you able to work or study?Yes Partially No Are you able to sustain a close relationship with someone? Yes Partially No
How frequently do you have problems in the following areas? Please pick a number from0-to-10. “0” means Not at all, and “10” means All the time.
If one or more of your parents had this, or a similar problem, place a P in the column headed by“Parents?”
If the problem came on suddenly, put an S in the column head by “Suddenly?”
Sensory Frequency (0-10) Parents? Suddenly?Light, in general, or lights, bother youProblems with the sense of smellProblems with visionProblems with hearingProblems with the sense of touch
EmotionsProblems of sudden, unexplained changes in moodProblems of sudden, unexplained fearfulnessProblems of unexplained spells of depression
38 LENS: THE LOW ENERGY NEUROFEEDBACK SYSTEM
Problems of unexplained spells of elationProblems with explosivenessProblems with irritabilityProblems with suicidal thoughts or actions
ClarityFeel “foggy” and have problems with clarityProblems following conversations (with good hearing)Problems with confusionProblems following what you are readingRealize you have no idea what you have been readingProblems with concentrationProblems with attentionProblems with sequencingProblems with prioritizingProblems not finishing what you startProblems organizing your room, office, paperworkProblems with getting lost in daydreamingYou cover up that you don't know what was said or
asked of you
EnergyProblems with staminaFatigue during the dayTrouble sleeping at nightProblems awakening at nightProblems falling asleep again
MemoryForget what you have just heardForget what you are doing, what you need to doProblems with procrastination and lack of initiativeProblems not learning from experience
MovementProblems with paralysis of one or more limbsProblems focusing or converging the eyes
PainHead pain that is steadyHead pain that is throbbingShoulder and neck painWrist painKnee painAll-over painJoint painOther pain (specify)
Other ProblemsProblems with nauseaSkin problemsProblems with speech or articulationDizzinessNoise in ears (Tinnitus)