Dr. José Mª Miró Infectious Diseases Service Hospital Clinic - IDIBAPS University of Barcelona Barcelona (Spain) E-mail address: [email protected]6 th CME Update on COVID19 (SARS-CoV-2) March 17 th ; April 2 nd , May 10 th , July 5 th , December 14 th 2020 & May 25 th 2021 COVID-19 Second Year: SARS-CoV-2 Variants, Long COVID & Vaccines
6th CME Update on COVID19 (SARS-CoV-2)March 17th; April 2nd, May 10th, July 5th, December 14th 2020 & May 25th 2021
COVID-19 Second Year: SARS-CoV-2 Variants, Long COVID & Vaccines
COVID-19 Second Year: SARS-CoV-2 Variants, Long COVID-19 & Vaccines
Current epidemiological and mortality data New SARS-CoV-2 variants update Long COVID-19: where we are one year later Remdesivir, dexamethasone, heparin and … something else? Reinfections: state of the art Vaccines efficacy and impact of new SARS-CoV-2 variants Vaccines safety: TTS* Take-home messages
May 25th 2021*Thrombosis with Thrombocytopenia Syndrome (TTS)
COVID-19 Global Cases (May 25th 2021)
https://www.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6; accessed on May 25th 2021
Overall mortality 2.07%
https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-casesgift – May 24th 2021
Distribution of COVID-19 cases Worldwide: Almost 5 million weekly cases
Cases in Africa under reported!
https://www.ft.com/content/a2901ce8-5eb7-4633-b89c-cbdf5b386938?shareType=nongift – May 25th 2021
Global COVID-19: More than 12,000 daily deaths!
Europe≈ 16%
LatAm≈ 31%India≈ 33%
Roth GA et al. JAMA Netw Open. May 3 2021; 4(5):e218828. doi: 10.1001/jamanetworkopen.2021.8828.
Reduction of COVID-19 In-Hospital Mortality in the United States During the COVID-19 Pandemic
↓ 34-42%>50 yr.
in comparison
1st wave
https://www.ft.com/content/a2901ce8-5eb7-4633-b89c-cbdf5b386938?shareType=nongift – April 26th 2021
Global Coronavirus Death Toll Could Be 60% Higher Than Reported
COVID-19 Second Year: SARS-CoV-2 Variants, Long COVID-19 & Vaccines
Current epidemiological and mortality data New SARS-CoV-2 variants update Long COVID-19: where we are one year later Remdesivir, dexamethasone, heparin and … something else? Reinfections: state of the art Vaccines efficacy and impact of new SARS-CoV-2 variants Vaccines safety: TTS* Take-home messages
May 25th 2021*Thrombosis with Thrombocytopenia Syndrome (TTS)
Binding of the spike to an ACE2 receptor allows the virus to enter human cells
Lorenzo Casalino, Amaro Lab, U.C. San Diego.https://www.nytimes.com/interactive/2020/health/coronavirus-unveiled.html?campaign_id=154&emc=edit_cb_20201009&instance_id=23018&nl%E2%80%A6
ACE2 receptor
RBD=Receptor binding domain.
RBD RBD
RBD
RBD
RBDRBD
Spike
Mutations in SARS-CoV-2 Spike: First transition D614 to G614
Korber B et al. Cell. 2020 Aug 20; 182:812-827.e19. doi: 10.1016/j.cell.2020.06.043; Wesley-Long S et al. medRxiv September 29, 2020; doi: https://doi.org/10.1101/2020.09.22.20199125
A spike protein, at left, and a protective coating of sugars, at rightRBD=Receptor binding domain.
RBD RBD
Korber B et al. Cell. 2020 Aug 20; 182:812-827.e19. Baric RS. NEJM; 2020; 383,2684-2686.
Mutations in SARS-CoV-2 Spike: First transition D614 to G614 A SARS-CoV-2 variant with Spike G614 has replaced D614 as the dominant pandemic form
Exchange of an aspartic acid (D) for a glycine (G) in position 614
Korber B et al. Cell. 2020 Aug 20; 182:812-827.e19. doi: 10.1016/j.cell.2020.06.043; Wesley-Long S et al. medRxiv September 29, 2020; doi: https://doi.org/10.1101/2020.09.22.20199125 .
Mutations in SARS-CoV-2 Spike: Global Transition D614 to G614
Korber B et al. Cell. 2020 Aug 20; 182:812-827.e19. doi: 10.1016/j.cell.2020.06.043; Volz E et al. Cell. 2020 Nov 19;S0092-8674(20)31537-3. doi: 10.1016/j.cell.2020.11.020.Wesley-Long S et al. medRxiv September 29, 2020; doi: https://doi.org/10.1101/2020.09.22.20199125; Diez-Fuertes et al. J Virol. 2021 doi: 10.1128/JVI.01583-20
Mutations in SARS-CoV-2 Spike: G614 Increases Infectivity of the Virus but not the Severity of COVID-19 Disease
G614 is Associated with Higher Viral Load and Younger Age of Patients
Mechanisms for Generating SARS-CoV-2 VariabilitySARS CoV-2 virus• Low polymerase error rate (Nsp14, error correction exoribonuclease activity)• High-level replication• The population is the incubator → Global vaccination!
Quasispecies dynamics: Evolutionary advantages• Improves replicative capacity → Entry, infectivity, transmission• Improves ability to interact with cellular factors• Escape to class I interferon innate response• Escape to acquired response → Antibodies, CTLs• It may increase disease severity• Genetic "drift", founder effect
Alcami J, personal communication.
Selected SARS-CoV-2 Lineages
IndiaB.1.617B.1.618
Variant of Interest (VOI)→ Multiple mutations, rapid increase in incidence, spread in areas of high immunity. e.g. California, New York, India
Variant of Concern (VOC)→ Increased transmission, virulence, immune escape. e.g. UK, Brazil, South Africa
D614G → Increased transmission.
N501Y → Increased transmission.
E484K → Associated with “antibody resistance”.
K417 → Increased ACE2r affinity.
UK
Galloway SE et al. MMWR Morb Mortal Wkly Rep. Jan 15 2021
New SARS-CoV-2 VOC: B.1.1.7 (United Kingdom); B.1.351 (South Africa); P.1 (Brazil).
https://www.nytimes.com/interactive/2021/health/coronavirus-variant-tracker.html, May 24th 2021
New SARS-CoV-2 VOC: B.1.1.7 (United Kingdom)The variant was first detected in the United Kingdom in September 2020, and a look back at previous samples found it as early as September 20th 2020. It has now been detected in over 110 countries.
https://www.nytimes.com/interactive/2021/health/coronavirus-variant-tracker.html, May 24th 2021
New SARS-CoV-2 VOC: B.1.351 (South Africa)The variant spread from South Africa into neighboring countries in October 2020.
It has since spread to at least 68 countries.
https://www.nytimes.com/interactive/2021/health/coronavirus-variant-tracker.html, May 24th 2021
New SARS-CoV-2 VOC: P.1 (Brazil) P.1 was discovered in December 2020 and reached the United States in January, but it may have been
circulating as early as October 2020 in Manaus, Brazil. It has now spread to at least 37 countries.
New SARS-CoV-2 VOI: B.1.617.2 (India) In just a few weeks, the B.1.617 variant has become the dominant strain across India and has spread to
about 40 nations, including the United Kingdom, Fiji and Singapore.
Vaidyanathan G. Nature. 2021; 593: 321-322; https://www.ft.com/content/a2901ce8-5eb7-4633-b89c-cbdf5b386938
Almost 400,000 new infections on May 9 2021! Same growing rate as
B.1.1.7 (UK variant)
Tada T et al. bioRxiv May 16th 2021 preprint doi: https://doi.org/10.1101/2021.05.14.444076; https://www.nature.com/articles/d41586-021-01274-7
New SARS-CoV-2 VOI: B.1.617.2 (India) In just a few weeks, the B.1.617 variant has become the dominant strain across India and has spread to
about 40 nations, including the United Kingdom, Fiji and Singapore.
RBD=Receptor binding domain.
RBD
Tada T et al. bioRxiv May 16th 2021 preprint doi: https://doi.org/10.1101/2021.05.14.444076
B.1.617.2 (India): Increased Infectivity In just a few weeks, the B.1.617 variant has become the dominant strain across India and has spread to
about 40 nations, including the United Kingdom, Fiji and Singapore.
Infectivity in pseudotyped viruses
RLU=Luciferase activity was measured two days post-infection.
Tada T et al. bioRxiv May 16th 2021 preprint doi: https://doi.org/10.1101/2021.05.14.444076
B.1.617.2 (India): Lower Neutralization by Sera & VaccinesIn just a few weeks, the B.1.617 variant has become the dominant strain across India and has spread to
about 40 nations, including the United Kingdom, Fiji and Singapore.Neutralization of spike protein variants by convalescent sera and antibodies
elicited by BNT162b2 and mRNA1273 vaccines
UK variant = B.1.1.7; South Africa variant = B.1.1351
Tada T et al. bioRxiv May 16th 2021 preprint doi: https://doi.org/10.1101/2021.05.14.444076
B.1.617.2 (India): Lower Neutralization by monoclonal nAbsIn just a few weeks, the B.1.617 variant has become the dominant strain across India and has spread to
about 40 nations, including the United Kingdom, Fiji and Singapore.Neutralization of B.1.617 and B.1.618 spike protein variants by
neutralizing monoclonal REGN10933 and REGN10987 antibodies
(UK)(South Africa)
Remember these new variants of SARS-COV-2
UKSouth Africa
BrazilIndia
B1.1.7 (D614G, N501Y)
B.1.351(D614G, N501Y, K417N, E484R)
P.1(D614G, N501Y, K417T, E484R)
B.1.617.2 (D614G, L452R, P681R, E484R)
Potential clinical implications:- Loss of efficacy of monoclonal antibodies/convalescent plasma- Loss of efficacy of vaccines
→ N501Y (UK variant) → Vaccines and antibodies OK→ E484K (South Africa, Brazil, India variants) → Viral scape to vaccines and antibodies
COVID-19 Second Year: SARS-CoV-2 Variants, Long COVID-19 & Vaccines
Current epidemiological and mortality data New SARS-CoV-2 variants update Long COVID-19: where we are one year later Remdesivir, dexamethasone, heparin and … something else? Reinfections: state of the art Vaccines efficacy and impact of new SARS-CoV-2 variants Vaccines safety: TTS* Take-home messages
May 25th 2021*Thrombosis with Thrombocytopenia Syndrome (TTS)
Spain3,650,000 cases10% = 365,000 cases long COVID
Timeline of post-acute COVID-19
Nalbandian A et al. Post-acute COVID-19 syndrome. Nat Med. 2021 Apr;27(4):601-615.
Case Definition Post-Acute Covid-19 (≥4 weeks)• Long Covid Persistent symptoms beyond 4 weeks that may be present or not in
acute-COVID or appear later in asymptomatic subjects and are not the result of an apparent irreversible organ damageClinical phenotypes• Permanent • Relapsing/remitting• Progressive and slow improvement
Lledo G on behalf the Multidisciplinary Collaborative Group for the Scientific Monitoring of COVID-19 (GCMSC); https://www.isglobal.org/documents
• Sequelae Irreversible tissue damage after 12 weeks that could represent different degrees of permanent dysfunction and symptoms Clinical scenarios• Post-intensive care syndrome. • Post-thrombotic or hemorrhagic complications• Immunomediated phenomena in the acute phase. • MIS-C and MIS-A.
Long-COVID Pathogenesis
Lledo G on behalf the Multidisciplinary Collaborative Group for the Scientific Monitoring of COVID-19 (GCMSC); https://www.isglobal.org/documents; Nalbandian A et al. Nat Med. 2021 Apr;27(4):601-615; Wostyn P. Med Hypotheses. 2021 Jan;146:110469
• Direct viral toxicity• “Cytokine storm” Hyperinflammatory state• Immune system dysregulation complex interplay INN – ADAPT immune response• Microvascular injury: Thrombo-inflammation + Endothelitis• Neuro-psychiatric:
– Neuroinflammation/degeneration (neurofilament)– Dysfunctional lymphatic drainage (glymphatic system & CFS. Wostyn et el)– Astrogliosis
Phillips M. British Society of Rehabilitation Medicine, 2020; Greenhalgh T et al. BMJ. 2020 Aug 11;370:m3026. doi: 10.1136/bmj.m3026; Lledo G on behalf GCMSC. https://www.isglobal.org/documents
• No treatment data … but nowadays there
are treatment for specific symptoms
• Rule out other causes
• Individualize Not the same treatment for everyone
• Physical Rehabilitation
• Psychological support
• Multidisciplinary Team
• Best treatment… early diagnosis (screening)
• … Vaccines?Multidisciplinary Approach
Vaccines were safe and improved some symptoms in patients with long COVID in UK
Arnold DT et al. medRxiv March 14, 2021. https://doi.org/10.1101/2021.03.11.21253225; Lledo G on behalf GCMSC. https://www.isglobal.org/documents
Decrease in worsening symptoms (6% vaccinated vs 14% unvaccinated) and increase in symptom resolution (23% vaccinated vs 15% unvaccinated) (p=0.035).
COVID-19 Second Year: SARS-CoV-2 Variants, Long COVID-19 & Vaccines
Current epidemiological and mortality data New SARS-CoV-2 variants update Long COVID-19: where we are one year later Remdesivir, dexamethasone, heparin and … something else? Reinfections: state of the art Vaccines efficacy and impact of new SARS-CoV-2 variants Vaccines safety: TTS* Take-home messages
May 25th 2021*Thrombosis with Thrombocytopenia Syndrome (TTS)
Siddiqu HK, Mehra MR. J Heart Lung Transplant. 2020 doi: 10.1016/j.healun.2020.03.012; Pericas JM, Hernandez-Meneses M et al. Eur Heart J. June 8th 2020.
Remdesivir drug (FDA, EMA but not WHO)Convalescent plasma (FDA EUA)Monoclonal antibodies (FDA EUA)Dexamethasone and other corticosteroids (NIH, IDSA)IL-6 inhibitors: Tocilizumab
Remdesevir (GS-5734) RNA-dependent RNA polymerase inhibitor. Effective in vitro and in animal models against zoonotic and epidemic SARS-CoV, MERS-CoV and SARS-CoV-2 as both prophylactic and therapeutic agent. PK: Renal excretion. Not recommended eGFR ≤30 ml/min. Few DDI. Dosage: 200 mg IV, then 100 mg/24 h during 5-10 days. Safety: few side effects (hypotension during infusion).
Sheahan TP et al. Sci Transl Med, 2017; De Wit ET al. Proc Natl Acad Sci U S A, 2020; Sheahan TP et al. Nat Commun; 2020; Williamson BN et al. bioRxiv preprint doi: https://doi.org/10.1101/2020.04.15.043166.
• Double-blind, randomized, placebo-controlled trial involving 1,063 hospitalized patients with advanced COVID-19 disease• A total of 68 sites ultimately joined the study— 47 in the United States and 21 in countries in Europe and Asia.• Primary endpoint: time to recovery was defined as being well enough for hospital discharge or returning to normal activity level. • NIH showed preliminary data of interim analysis on April 29th 2020.
*Patients who received remdesivir had a 31% faster time to recovery than those who received placebo.
Remdesivir PlaceboNIAID trial- Median time to recovery, days*- Mortality
Beigel JH et al. N Engl J Med. 2020 May 22. doi: 10.1056/NEJMoa2007764.
• Double-blind, randomized, placebo-controlled trial involving 1,063 hospitalized patients with advanced COVID-19 disease• A total of 68 sites ultimately joined the study— 47 in the United States and 21 in countries in Europe and Asia.• Primary endpoint: time to recovery was defined as being well enough for hospital discharge or returning to normal activity level. • NIH showed preliminary data of interim analysis on April 29th 2020.
*Patients who received remdesivir had a 31% faster time to recovery than those who received placebo.
Remdesivir PlaceboNIAID trial- Median time to recovery, days*- Mortality
P-value118%
1511.6%
<0.0010.059
FDA Approval, May 1 2020EMA Approval, June 25 2020
Remdesivir – ACTT (NIH) vs. Solidarity (WHO)
Beigel JH et al. N Engl J Med. Nov 5 2020; Solidarity, medRxiv Oct 28 2020
ACTT (NIH)
SAEs: 21% REM vs. 27% PBO
Solidarity (WHO)
Remdesivir in Solidarity RCT: It does not analyze stages 5 and 6 separately
(Stage 5)(Stage 6)
(Stage 5 & 6)
Beigel JH et al. N Engl J Med. Nov 5 2020; Solidarity, medRxiv Oct 28 2020
Remdesivir Reduced the SARS-CoV-2 VL in BAL from Rhesus Macaques
Williamson BN et al. Nature. Sep 2020; 585: 273-276. doi: 10.1038/s41586-020-2423-5. Epub 2020 Jun 9.
SARS-CoV-2 VL and virus titers in BAL fluid and lung lobes collected from six Rhesus MacaquesVL in BAL (N=6) Infectious virus titers in
BAL (N=6)
VL = Viral load; BAL = Bronchoalveolar lavage
• Virus shedding from the upper respiratory tract was not reduced by remdesivir treatment. • At necropsy, remdesivir-treated animals had lower lung viral loads and reduced lung damage.
VL in tissues at necropsy (N=36)
Ivermectin in Adults with Mild COVID-19
Lopez-Medina E et al. JAMA. doi:10.1001/jama.2021.3071. Published online March 4, 2021.
• Double-blind RCT conducted at a single site in Cali, Colombia. A total of 476 adults with mild disease and symptoms for 7 days or fewer (at home or hospitalized) were enrolled between July and November 2020, and followed up through December 2020.
• Patients were randomized to receive ivermectin, 300 μg/kg of body weight per day for 5 days (n = 200) or placebo (n = 200).• Primary outcome was time to resolution of symptoms within a 21-day follow-up.
• The trial do not support the use of ivermectin for treatment of mild COVID-19.
Time to Resolution of Symptoms in the Primary Analysis Population.
• Symptoms resolution: 82% in the ivermectin group and 79% in the placebo group by day 21.
Molnupiravir – An Oral Drug for COVID-19 Treatment• Molnupiravir has potent in vitro activity against a broad range of coronaviruses, including SARS-COV-2 (including
remdesivir-resistant mutants).• Demonstrated activity in ferret and mouse models of SARS-CoV-2 disease, including prophylaxis, treatment, and
prevention of transmission• It is rapidly absorbed and distributed after oral administration and subsequently converted intracellularly to active form.• Inhibits SARS-COV-2 replication by inducing viral error catastrophe. It is not mutagenic or genotoxic in mammals.
Painter W, et al. CROI 2021 Poster #777.
• CROI 2021: Phase 2a RCT. 182 participants randomized 1:1 (200 mg) or 3:1 (400 mg, 800 mg) sequentially to receive molnupiravir or placebo twice-daily for 5 days.
• 78 cases (42.9%) had positive baseline cultures• Overall, there was a significant reduction in positive viral
culture at day 5 in molnupiravir-treated participants. Best activity reached with 800 mg BID. No infectious virus was recovered in any molnupiravir-treated participants.
• The drug was safe and well tolerated. Four cases experienced a serious AE (0 drug-related) and 7 discontinued study drug (3 due to an AE).
Molnupiravir – An Oral Drug for COVID-19 TreatmentUpdate on Progress of Clinical Development Program for Molnupiravir, an Investigational Oral Therapeutic for the Treatment of Mild-to-Moderate COVID-19
→ Phase 2/3 MOVe-IN Study in Hospitalized Patients Stopped.• Phase 2/3, randomized, placebo-controlled, double-blind, multi-site trial evaluating the efficacy, safety, and pharmacokinetics of orally administered
molnupiravir in hospitalized participants at least 18 years of age with laboratory confirmed. 304 participants randomized 1:1:1:1 to who received molnupiravir 200 mg, 400 mg, 800 mg or placebo twice daily for 5 days. The primary efficacy endpoint was to evaluate the rate of sustained recovery from randomization through Day 29.
→ Phase 3 MOVe-OUT Study in Outpatients is ongoing.• Phase 2/3, randomized, placebo-controlled, double-blind, multisite study evaluating the efficacy, safety and pharmacokinetics of orally administered
molnupiravir in non-hospitalized participants with COVID-19 confirmed using PCR. The primary efficacy objective is assessed by the percentage of patients who are hospitalized and/or die from the time of randomization through Day 29. Part 1 of MOVe-OUT enrolled a total of 302 participants, with symptom onset within seven days prior to randomization, who were assigned to receive molnupiravir 200 mg (75), 400 mg (77), or 800 mg (76), or placebo (74).
• Final data is estimated to be available in September/ October 2021
→ Molnupiravir for PEP in the second half of 2021Merck and Ridgeback Biotherapeutics press release. April 14th 2021.
Convalescent plasma transfusions do no work RCT performed in Argentina. 228 patients were assigned to receive convalescent plasma and 105 to receive placebo. Median time of symptoms was 8 days (IQR, 5 to 10). Hypoxemia was the most frequent severity criterion for enrollment. The infused convalescent plasma had a median titer of 1:3200 of total SARS-CoV-2 antibodies (IQR, 1:800 to1:3200).
Simonovich VA et al. NEJM Nov 24 2020 DOI: 10.1056/NEJMoa2031304
Time to Death or to Improvement after Treatment with Convalescent Plasma or Placebo
Convalescent plasma transfusions do not work
Janiaud P et al. JAMA. February 26, 2021. doi:10.1001/jama.2021.2747
Treatment with convalescent plasma compared with placebo or standard of care was not significantly associated with a decrease in all-cause mortality or with any benefit for other clinical outcomes ((length of hospital stay or mechanical ventilation use)
Early convalescent plasma transfusion works Randomized, double-blind, placebo-controlled trial of convalescent plasma with high IgG titers against SARS-CoV-2 in older adult patients (≥75 years or between 65-74 years with ≥1 comorbidity) ≤72 hours after the onset of mild Covid-19 symptoms. Primary end point was severe respiratory disease, defined as a respiratory rate of 30 breaths per minute or more, an oxygen saturation of less than 93% while the patient was breathing ambient air, or both.
Libster R et al. INFANT–COVID-19 Group. NEJM. Jan 6th 2021
Time to the Development of Severe Respiratory Disease (ITT) Primary End Point according to Donor SARS-CoV-2 S IgG Titer.
-73%-31%
The trial was stopped early at 76% of its projected sample size because cases of Covid-19 in the trial region decreased considerably and enrollment of trial patients became impossible.
Monoclonal Antibodies against the SARS-CoV-2 Spike Protein: Early Treatment (<10 d.) in Patients at High Risk of Progression
Chen P et al on behalf BLAZE-1 Investigators. NEJM Oct 28 2020; REGN-COV-2. REGENERON Press Release Nov 21 2020
Hospitalization rates at 28 days
mAb PBO
Bamlanivimab (iv single dose)- Chen P et al (N=552; 3:1)*
Casirivimab plus Imdevimab (iv single dose)- Regeneron mAb (N=799; 2:1)**
P-value
1.6%
3%
6.3%
9%
0.017
<0.001
* 452 patients were assigned to receive a single IV infusion of neutralizing antibody LY-CoV555 in one of three doses (700 mg, 2800 mg, or 7000 mg) or placebo** 266 patients received a single IV infusion of 2,400 milligrams casirivimab and imdevimab (1,200 mg of each), 267 received 8,000 mg casirivimab and imdevimab (4,000 mg of each), and 266 received a placebo, within three days of obtaining a positive SARS-CoV-2 viral test.The combination of casirivimab plus imdevimab is particularly effective in reducing VL in patients who are antibody-negative and those with high baseline VL.
Adapted from Ware LB et al. NEJM, 2000
SARS-CoV-2 (COVID19): Anti-inflammatory Treatment
ACE2
Cytokine Storm
→ ARDS
• Corticosteroids• IL-6 inhibitors
- Tocilizumab - Sarilumab no activity. - Siltuximab
• IL-1 inhibitors- Anakinra
• JAK inhibitors- Baricitinib (also entry inhibitor)
RECOVERY Trial: Low-dose Dexamethasone Reduced Death• RECOVERY was established as a randomized clinical trial to test a range of potential drugs for COVID-19, including dexamethasone.• The trial has proceeded at unprecedented speed, enrolling over 11,000 patients from 175 NHS hospitals in the UK.• The Independent Data Monitoring Committee (IDMC) has reviewed the emerging data about every two weeks to determine if there is
evidence that would be strong enough to affect national and global treatment of COVID-19.• Dexamethasone: 6 mg once per day (either by mouth or by intravenous injection) for 10 days vs. Standard of Care (SoC).• On June 8 IDMC concluded that dexamethasone reduced deaths in hospitalized patients with severe COVID-19.
Dexamethasone SoCRecovery trialNumber of patients28-day mortality- Mechanical ventilation*- Oxygen supply*- No respiratory intervention*
*Rate Ratio (95% confidence interval) RECOVERY Trial press release, June 16 2020; Horby PW et al. medRxiv. June 22, 2020; The
RECOVERY Collaborative Group. NEJM July 17 2020. DOI: 10.1056/NEJMoa2021436.
Tocilizumab plus Dexamethasone – RECOVERY Trial• Randomized, controlled, open-label, platform trial, including 4,116 patients.• Inclusion criteria: patients with hypoxia (oxygen saturation <92% on air or requiring oxygen therapy) and evidence of systemic inflammation
(C-reactive protein [CRP] ≥75 mg/L)• RCT: Standard of care alone (dexamethasone) vs. usual standard of care plus tocilizumab at a dose of 400 mg to 800 mg (depending
on weight) given intravenously. A second dose could be given 12-24 h. • The primary outcome was 28-day mortality, assessed in the intention-to-treat population.
RECOVERY Collaborative Group (Horby PW). Lancet 2021; 397: 1637–45.
28-day Mortality 28-day Discharge from hospital days
Tocilizumab plus Dexamethasone – RECOVERY Trial• Randomized, controlled, open-label, platform trial, including 4,116 patients.• Inclusion criteria: patients with hypoxia (oxygen saturation <92% on air or requiring oxygen therapy) and evidence of systemic inflammation
(C-reactive protein [CRP] ≥75 mg/L)• RCT: Standard of care alone (dexamethasone) vs. usual standard of care plus tocilizumab at a dose of 400 mg to 800 mg (depending
on weight) given intravenously. A second dose could be given 12-24 h. • The primary outcome was 28-day mortality, assessed in the intention-to-treat population.
*Rate Ratio (95% confidence interval) RECOVERY Collaborative Group (Horby PW). Lancet 2021; 397: 1637–45.
Tocilizumab: Meta-analysis of mortality in RCTs in hospitalized patients with COVID-19
*Rate Ratio (95% confidence interval) RECOVERY Collaborative Group (Horby PW). Lancet 2021; 397: 1637–45.
Baricitinib has antiviral and anti-inflammatory properties
Richardson P et al. Lancet, February 3, 2020; Stebbing J et al. Lancet, Feb 27 2020; *Cantini F et al. J infect. Jun 242020 . doi: 10.1016/j.jinf.2020.06.052; Pairo-
Castineira E. et al. Nature. 2020 Dec 11. doi: 10.1038/s41586-020-03065-y.
• There is a high expression of TYK2 gene in COVID-19 patients with poor outcome. JAK 1/2 inhibitors (baricitinib) could be useful to prevent inflammation.
• Baricitinib is indicated for the treatment of moderate to severe active rheumatoid arthritis in adult patients with an inadequate response or intolerance to one or more disease-modifying antirheumatic drugs. The recommended dose is 4 mg QD orally.
• The first pilot retrospective multicenter study showed that baricitinib 4 mg/day used for 2 weeks (together with LPV/rtv) was not associated with SAEs, reduced SARS-CoV-2 viral burden in nasopharyngeal swabs and ICU admissions of patients with COVID-19 pneumonia*
Remdesivir plus Baricitinib – ACTT-2 (NIH): Stage 6
Kalil AC et al. N Engl J Med. March 4, 2021. DOI: 10.1056/NEJMoa2031994
Positive results in patients:- Severe disease- Stage 6: high-flow oxygen & NIMV
Baseline Ordinal Scale 6 (Stage 6)
NIMV = Non-invasive mechanical ventilation
Baricitinib – Phase 3 RCT COV-BARRIER
Lilly and Incyte press release, April 8, 2021
• COV-BARRIER is a Phase 3 study evaluating baricitinib 4 mg once daily plus standard of care (SoC) vs. placebo plus SoC for 14 days.• The trial did not meet statistical significance on the primary endpoint, which was defined as a difference in the proportion of participants
progressing to the first occurrence of non-invasive ventilation including high flow oxygen or invasive mechanical ventilation (MV) including extracorporeal membrane oxygenation (ECMO) or death by Day 28.
• Baricitinib-treated patients were 2.7 percent less likely than those receiving standard of care to progress to ventilation (non-invasive or mechanical) or death, a difference that was not statistically significant (OR: 0.85; 95% CI 0.67, 1.08; p=0.1800).
Baricitinib PlaceboEnd-points by day 28- Number of patients- Combined (MV, ECMO, death)- 28-day mortality (secondary)
P-value764NA
8.1%
761NA
13.1%0.180
<0.001
• A reduction in mortality was also seen for the subgroups of patients being treated with or without corticosteroids at baseline.• Serious infections and venous thromboembolism (VTE) occurred in 8.5 percent and 2.7 percent of patients treated with
baricitinib, respectively, versus 9.8 percent and 2.5 percent of patients treated with placebo.• NA = Not available
Colchicine has antiviral and anti-inflammatory properties: the GRECCO Trial
Deftereos SG et al, JAMA Network Open. 2020;3(6):e2013136. doi:10.1001/jamanetworkopen.2020.13136
• Open-label, randomized clinical trial in Greece. 105 patients hospitalized with mild-moderate COVID-19 were included.• Colchicine (1.5-mg loading dose followed by 0.5mg after 60 min and maintenance doses of 0.5 mg BID) with SoC for 3 weeks• Primary end-point: increase hscTroponin/CRP or clinical deterioration by 2 points on a 7-grade clinical status scale.
AEs: Colchicine, 45% (GI) vs. Control,18%
D-Dimer: Colchicine, 0.76 vs. Control, 0.92 ug/mL
Colchicine in Non-Hospitalized Patients with COVID-19 (COLCORONA RCT)
Tardif JC et al. medRxiv preprint January 27, 2021; doi: https://doi.org/10.1101/2021.01.26.21250494.
• Double-blind RCT performed in Canada involving non-hospitalized patients with COVID-19 diagnosed by PCR testing or clinical criteria. • The patients were randomly assigned to receive colchicine (0.5 mg twice daily for 3 days and once daily thereafter) or placebo for 30 days. • The primary efficacy endpoint was the composite endpoint of death or hospitalization for COVID-19.
Colchicine PlaceboITT analysis- All patients (N=4,488)- Only PCR positive (N=4,159)
P-value
4.7%4.6%
5.8%6.0%
0.080.04
• There were no differences in total SAE. However, patients who took colchicine had more gastrointestinal side effects (diarrhea): 23.9% vs. 14.9% p = <0.001.
Colchicine in Hospitalized Patients with COVID-19 (RECOVERY RCT)
Statement from the RECOVERY trial chief investigators, 5 March 2021https://www.recoverytrial.net/news/recovery-trial-closes-recruitment-to-colchicine-treatment-for-patients-hospitalised-with-covid-19.
• The RECOVERY trial was established as a RCT to test a range of potential treatments for COVID-19. Since November 2020, the RECOVERY trial has included a randomized comparison of colchicine vs. usual care alone.
• The preliminary analysis is based on 2178 reported deaths among 11,162 randomized patients, 94% of whom were being treated with a corticosteroid such as dexamethasone. There is no significant difference in the primary endpoint of 28-day mortality (20% colchicine vs. 19% usual care alone; risk ratio 1.02 [95% confidence interval 0.94-1.11]; p=0.63).
• DSMB closed recruitment on March 4th 2021.
Colchicine SoCMortality at 28 days- All patients (N=11,162)
P-value
20% 19% 0.63
Virchow’s Triad and COVID-19 Associated Coagulopathy
Talasaz AH, et al. J Am Coll Cardiol. 2021 Apr 20;77(15):1903-1921.COVID-19, coronavirus disease-2019; DIC, disseminated intravascular coagulopathy; FDP, fibrin degradation products; GM-CSF, granulocyte-macrophage colony-stimulating factor; IL, interleukin; LV, left ventricular; PAI, plasminogen activator inhibitor; RNA, ribonucleic acid; SIC, sepsis-induced coagulopathy; TF, tissue factor; TNF, tumor necrosis factor; tPA, tissue type plasminogen activators; uPA, urokinase plasminogen activators; vWF, von Willebrand factor.
=
Effect of Intermediate-Dose vs. Standard-Dose Prophylactic Anticoagulation in ICU Patients with COVID-19: The INSPIRATION RCT
INSPIRATION investigators. JAMA. March 18, 2021. doi:10.1001/jama.2021.4152.
• Multicenter randomized trial with a 2 × 2 factorial design performed in 10 academic centers in Iran among 562 adult patients admitted to the ICU with COVID-19.
• Intermediate-dose (enoxaparin, 1mg/kg daily) (n = 276) vs. standard prophylactic anticoagulation (enoxaparin, 40mg daily) (n = 286), with modification according to body weight and creatinine clearance.
→ This RCT does not support the routine empirical use of intermediate-dose prophylactic anticoagulation in unselected patients admitted to the ICU with COVID-19.
• The primary outcome was a composite of adjudicated acute arterial thrombosis, venous thromboembolism, extracorporeal membrane oxygenation (ECMO), or all-cause mortality during 30 days from enrollment.
Ongoing Antithrombotic Therapy Trials in COVID-19 (N=83)
Talasaz AH, et al. J Am Coll Cardiol. 2021 Apr 20;77(15):1903-1921.
Symptomatic treatmentClose monitoring for early detection of progression.Potential use of plasma & IV monoclonal antibodiestherapy in high risk persons
Remdesivir, IV, 5-10 d.Stages 4 (no oxygen) & 5 (low-flow oxygen supply)Stage 6 plus baricitinib, oral, 14 days
Low molecular weight heparin, SCDuring the entire hospitalization period
- Randomized, double-blind, placebo-controlled trials for prevention of SARS-COV-2 infection in residents and staff of skilled nursing and assisted living facilities where at least 1 case of SARS-CoV-2 infection had been confirmed in the previous 7 days or in asymptomatic household contacts of people with COVID-19 documented within the previous 4 days and returning home.
- mABs can offer immediate protection for exposed or unvaccinated individuals in high risk settings (in contrast to vaccines that take 7-14 days to offer protection.
PEP trials with Monoclonal Antibodies (mABs)
Lilly press release, January 27, 2021; REGENERON press release, April 12, 2021
81% reduction symptomatic COVID-19 <0.001
*Nursing home residents; **Reduction of SARS-CoV-2 infection, shortened time of viral shedding and shortened time of high viral load (>104 copies/mL) shedding suggesting a benefit for reduced transmission.
COVID-19 Second Year: SARS-CoV-2 Variants, Long COVID-19 & Vaccines
Current epidemiological and mortality data New SARS-CoV-2 variants update Long COVID-19: where we are one year later Remdesivir, dexamethasone, heparin and … something else? Reinfections: state of the art Vaccines efficacy and impact of new SARS-CoV-2 variants Vaccines safety: TTS* Take-home messages
May 25th 2021*Thrombosis with Thrombocytopenia Syndrome (TTS)
COVID-19 Reinfections Occur, but Remain Rare
https://bnonews.com/index.php/2020/08/covid-19-reinfection-tracker/; ECDC; Ledford H. Nature. Sep 2020; 585:168-169. doi:10.1038/d41586-020-02506-y
• How common is reinfection? Reinfections are rare. Only 72 confirmed cases have been reported.• Are reinfections more or less severe than the first? Clinical picture is similar (88%). Mortality rates range: 0.1%-4.1%. • What implications do reinfections have for vaccine development? It is an important topic that is currently being studied.
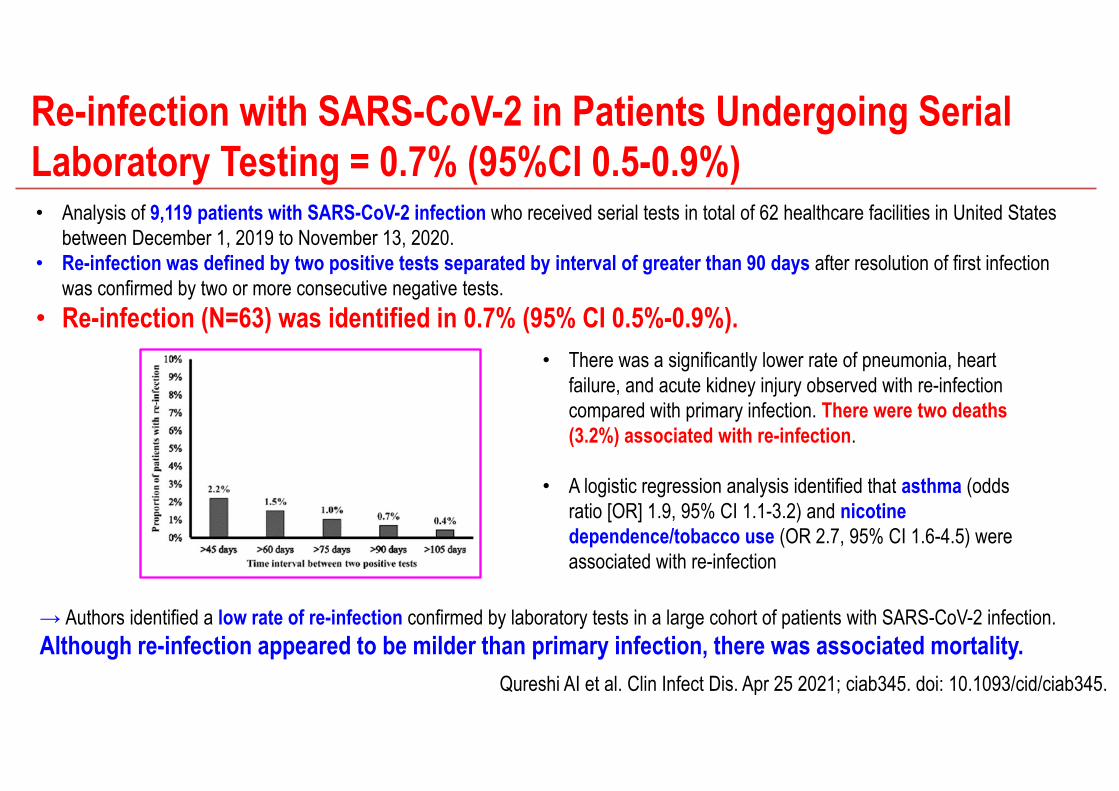
Re-infection with SARS-CoV-2 in Patients Undergoing Serial Laboratory Testing = 0.7% (95%CI 0.5-0.9%)
Qureshi AI et al. Clin Infect Dis. Apr 25 2021; ciab345. doi: 10.1093/cid/ciab345.
• Analysis of 9,119 patients with SARS-CoV-2 infection who received serial tests in total of 62 healthcare facilities in United States between December 1, 2019 to November 13, 2020.
• Re-infection was defined by two positive tests separated by interval of greater than 90 days after resolution of first infection was confirmed by two or more consecutive negative tests.
• Re-infection (N=63) was identified in 0.7% (95% CI 0.5%-0.9%).
→ Authors identified a low rate of re-infection confirmed by laboratory tests in a large cohort of patients with SARS-CoV-2 infection. Although re-infection appeared to be milder than primary infection, there was associated mortality.
• There was a significantly lower rate of pneumonia, heart failure, and acute kidney injury observed with re-infection compared with primary infection. There were two deaths (3.2%) associated with re-infection.
• A logistic regression analysis identified that asthma (odds ratio [OR] 1.9, 95% CI 1.1-3.2) and nicotine dependence/tobacco use (OR 2.7, 95% CI 1.6-4.5) were associated with re-infection
The Resurgence of COVID-19 in Manaus, Brazil, despite high SARS-CoV-2 seroprevalence was linked to a new P1 variant
Sabino EC et al. Lancet. 2021 Feb 6;397(10273):452-455. doi: 10.1016/S0140-6736(21)00183-5. Faria NR et al. Science. 2021 Apr 14;eabh2644. doi: 10.1126/science.abh2644.
→ Cases of SARS-CoV-2 infection in Manaus, Brazil, resurged in late 2020, despite previously high levels of infection. Genome sequencing of viruses sampled in Manaus between November 2020 and January 2021 revealed the emergence and circulation of a novel SARS-CoV-2 variant of concern: P1
• P.1 variant, acquired 17 mutations, including a trio in the spike protein (K417T, E484K and N501Y) associated with increased binding to the human ACE2 receptor.
• Molecular clock analysis shows that P.1 emergence occurred around mid-November 2020 and was preceded by a period of faster molecular evolution.
• P.1 may be 1.7-2.4-fold more transmissible, and that previous SARS-CoV-2 non-P.1 infection only provided 54-79% of the protection against infection with new P.1 variant.
P.1 variant
Protection against reinfection of natural immunity generated by past SARS-CoV-2 infection
>99% 50-80%Same Virus New P1 Variant
→ Implications for vaccine efficacy (immune escape)P.1 variant acquired 17 mutations, including a trio in the spike protein (K417T, E484K and N501Y)
COVID-19 Second Year: SARS-CoV-2 Variants, Long COVID-19 & Vaccines
Current epidemiological and mortality data New SARS-CoV-2 variants update Long COVID-19: where we are one year later Remdesivir, dexamethasone, heparin and … something else? Reinfections: state of the art Vaccines efficacy and impact of new SARS-CoV-2 variants Vaccines safety: TTS* Take-home messages
May 25th 2021*Thrombosis with Thrombocytopenia Syndrome (TTS)
Callaway Ewen. Nature 2020; 580, 576-577. IDSA COVID-19 Vaccines; https://www.nytimes.com/2020/12/25/health/turkey-brazil-sinovac-coronavirus-vaccine.html; https://www.nytimes.com/2020/12/30/business/china-vaccine.html; Abdool Karim SS et al. N Engl J Med; March 24 2021.
79%
51% Brazil 91% Turkey
Name Sponsor
CurrentTrial PhaseType of Vaccine
Adenovirus type 5 vector
Ad5-nCoVCanSino BiologicsChina
3
Adenovirus vector
rAdenovirustypes 26 & 5 vector
Gam-COVID-VacSputnik VGamaleya RIEM,Russia
2/3
Callaway Ewen. Nature 2020; 580, 576-577. doi: https://doi.org/10.1038/d41586-020-01221-y; IDSA COVID-19 Vaccines, Last updated: January 15, 2021
WeakenedAdenovirus
AZT1222Oxford - Astra Zeneca, UK
2/3
Vaccine Candidates: Viral-vector Vaccines
Vaccine Candidates: Viral-vector Vaccines
Name Sponsor
CurrentTrial PhaseType of Vaccine
Adenovirus type 26 recombinant vector
Ad26.COV2.S Janssen, Johnson & JohnsonBelgium, USA
3
Adenovirus
Callaway Ewen. Nature 2020; 580, 576-577. doi: https://doi.org/10.1038/d41586-020-01221-y; IDSA COVID-19 Vaccines, Last updated: January 15, 2021
*Single dose. Including patients with South Africa variant; Sadoff J et al. NEJM. April 21, 2021..Voysey M et al. Lancet Dec 8 2020; S0140-6736(20)32661-1. doi: 10.1016/S0140-6736(20)32661-1
Sputnik V phase 3 RCT data not published yet. Callaway E et al. Nature. Nov 11 2020. doi: 10.1038/d41586-020-03209-0https://www.nytimes.com/live/2020/12/11/world/covid-19-coronavirus?#british-and-russian-vaccine-makers-are-set-to-begin-clinical-trials-combining-two-vaccines
Efficacy of Adenovirus-vector Vaccines
70% 92%
AZD1222Oxford-Astra Zeneca
Sputnik VGamaleya
66%
Ad26.COV2.SJanssen*
Callaway Ewen. Nature 2020; 580, 576-577. doi: https://doi.org/10.1038/d41586-020-01221-y; IDSA COVID-19 Vaccines, Last updated: January 15, 2021
Vaccine Candidates: mRNA vaccinesName Sponsor
CurrentTrial PhaseType of Vaccine
mRNANanoparticles
BNT162Pfizer-BioNTechUSA-Germany
3
mRNANanoparticles
mRNA-1273ModernaUSA
3
mRNA → Spike
Polack FP et al. NEJM Dec.10 2020; DOI: 10.1056/NEJMoa2034577Callaway E. Nature. Nov. 16 2020; 587:337-338. doi: 10.1038/d41586-020-03248-7
Jackson LA et al. N Engl J Med. 2020 Nov 12;383(20):1920-1931. doi: 10.1056/NEJMoa2022483
Keech C et al. N Engl J Med 2020; 383: 2320-32. DOI: 10.1056/NEJMoa2026920
rSARS-CoV-2 nanoparticle vaccine*
NVX-CoV2373Novavax,USA
1/2b/3
SARS-CoV-2Spike Protein
89% UK
Where each vaccine is being used (I) The Oxford‐AstraZeneca vaccine is known as Covishield in India. Only countries that report doses administered are shown.
Other countries may have approved vaccines but have not administered them yet
https://www.nytimes.com/interactive/2021/world/covid-vaccinations-tracker.html May 8, 2021
https://www.nytimes.com/interactive/2021/world/covid-vaccinations-tracker.html May 8, 2021
Where each vaccine is being used (II) The Oxford‐AstraZeneca vaccine is known as Covishield in India. Only countries that report doses administered are shown.
Other countries may have approved vaccines but have not administered them yet
Polack FP et al. NEJM December 10 2020; DOI: 10.1056/NEJMoa2034577
Protection starts 12 days after 1st Vaccine Dose (Pfizer)!
Krammer F. Nature. 2020 Oct;586(7830):516-527. Levine-Tiefenbrun M et al. Nat Med. May 2021; 27:790-792.
• Avoid transmission• Disease severity
Mucosal and systemic immune responses to natural infection with respiratory viruses and to vaccination
Pfizer (BNT162b2) vaccine reduced viral load in breakthrough infections
occurring 12–37 days after the first dose of vaccine and thereby further suppress
onward transmission.
Decreased SARS-CoV-2 viral load after 12 d post-vaccination
Vaccination in persons with a history of SARS-CoV-2 infection
1 or 2 doses?
Krammer F et al. N Engl J Med. April 8 2021; 384:1372-1374. Anichiniet G. al. N Engl J Med. April 14 2021; doi: 10.1056/NEJMc2103825; Bradley T, et al. N Engl J Med. 2021 May 20; 384:1959-1961.
Krammer F et al. N Engl J Med. April 8 2021; 384:1372-1374.
Vaccination in persons with a history of SARS-CoV-2 infection: 1 dose is enough!
Immunogenicity of SARS-CoV-2 RNA Vaccines
A single dose of mRNA vaccine in seropositive participants ≥ seronegative participants who received two vaccinations.
Krammer F et al. N Engl J Med. April 8 2021; 384:1372-1374.
Vaccination in persons with a history of SARS-CoV-2 infection: 1 dose is enough!
Reactogenicity (Side Effects) of SARS-CoV-2 RNA Vaccines
Vaccine recipients with preexisting immunity had more systemic side effects than those without preexisting immunity (fatigue, headache, chills, muscle pain, fever, and joint pain, in order of decreasing frequency).
Vaccine efficacy against new SARS-CoV-2 variants
UKSouth Africa
BrazilIndia
B1.1.7B.1.351
P.1B.1.617.2
Mild/Moderate SeverePfizer-BioNTech (Qatar)- UK (B.1.1.7) 89.5% 100%- South Africa (B.1.351) 75% 100%
Abu-Raddad LJ et al. N Engl J Med. May 5 2021; Pfizer and BioNTech press release, April 1 2021. https://www .pfizer.com/ news/ press -release/ press -release -detail/ pfizer -and -biontech -confirm -high -efficacy -and -no -serious.
Pfizer (BNT162b2 mRNA) also did a trial in 800 individuals in South Africa, with no cases of Covid-19 in the vaccine group and nine cases in the placebo group.
Of the nine cases, six strains were confirmed to be of the B.1.351 lineage
Vaccine efficacy against UK (B.1.1.7) & South Africa (B.1.351) variants
Efficacy against symptomatic disease
Vaccine efficacy against South African variant (B.1.351)
Mild/Moderate SevereAstraZeneca- ChAdOx1 nCoV-19 (x2) 10% No casesJanssen- Ad26.COV2.S (x1) 64% 82%Novavax- NVX-CoV2373 (x2) 51% No cases
Madhi SA et al. N Engl J Med 2021;384:1885-98; Shinde V et al. N Engl J Med 2021;384:1899-909; Sadoff J et al. N Engl J Med. April 21 2021. doi: 10.1056/NEJMoa2101544.
Efficacy against symptomatic disease
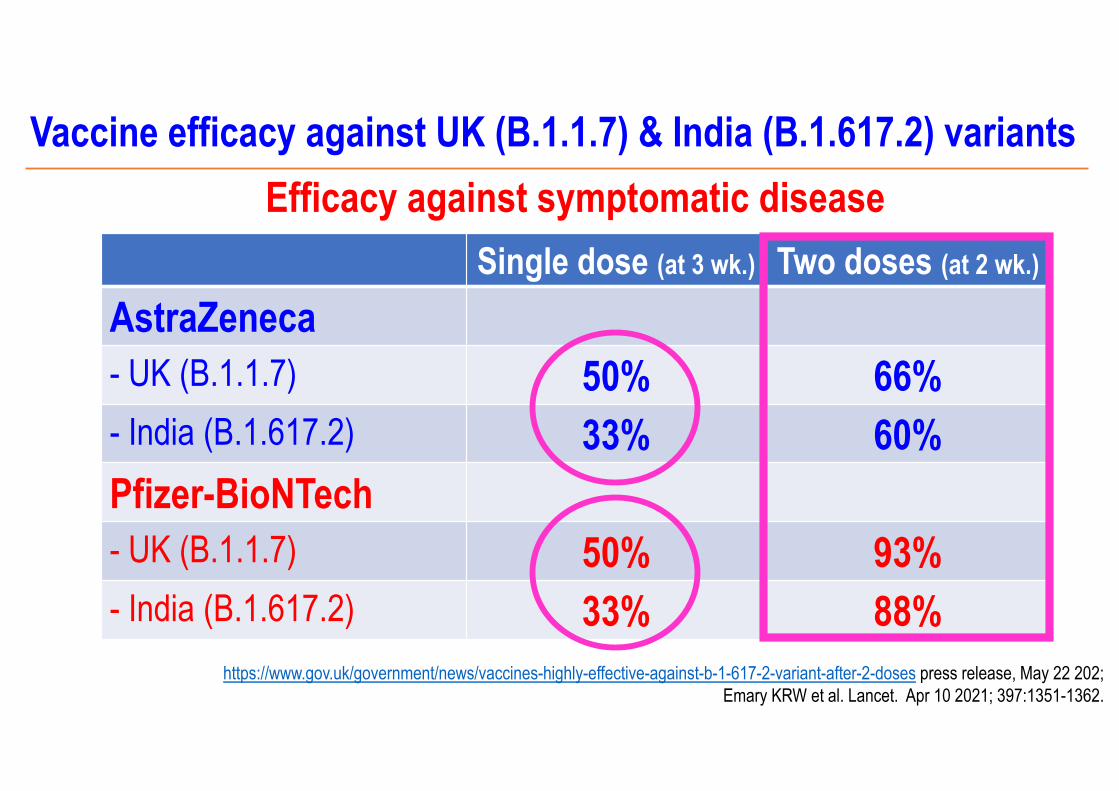
Vaccine efficacy against UK (B.1.1.7) & India (B.1.617.2) variants
Single dose (at 3 wk.) Two doses (at 2 wk.)
AstraZeneca- UK (B.1.1.7) 50% 66%- India (B.1.617.2) 33% 60%Pfizer-BioNTech- UK (B.1.1.7) 50% 93%- India (B.1.617.2) 33% 88%
Efficacy against symptomatic disease
https://www.gov.uk/government/news/vaccines-highly-effective-against-b-1-617-2-variant-after-2-doses press release, May 22 202; Emary KRW et al. Lancet. Apr 10 2021; 397:1351-1362.
Sumary of vaccine efficacy against new SARS-CoV-2 variants
• Good efficacy against UK (B.1.1.7) and India(B.1.617.2) variants.
• Poor efficacy against South Africa (B.1.351) variant. The good news are current vaccines protected individuals from severe disease.
• Few data against P.1 variant (Sinovac, 51%)
COVID-19 Second Year: SARS-CoV-2 Variants, Long COVID-19 & Vaccines
Current epidemiological and mortality data New SARS-CoV-2 variants update Long COVID-19: where we are one year later Remdesivir, dexamethasone, heparin and … something else? Reinfections: state of the art Vaccines efficacy and impact of new SARS-CoV-2 variants Vaccines safety: TTS* Take-home messages
May 25th 2021*Thrombosis with Thrombocytopenia Syndrome (TTS)
Menni C et al. Lancet Infect Dis April 27, 2021
Safety of COVID-19 Vaccines: 627,383 individuals in UK• Local side-effects after BNT162b2 (Pfizer) and ChAdOx1 nCoV-19 (Astra-Zeneca)
vaccination occur at frequencies lower than reported in phase 3 trials.Pfizer 1st dose Pfizer 2nd dose Astra-Zeneca 1st dose
72% 68% 59%
Menni C et al. Lancet Infect Dis April 27, 2021
Safety of COVID-19 Vaccines: 627,383 individuals in UK• Local adverse effects self-reported to the COVID Symptom Study app after COVID-19 vaccination,
stratified by sex, age, BMI, health status, and previous SARS-CoV-2 test status
Pfizer 2nd dose Astra-Zeneca 1st dose
Female gender, younger people, BMI<30 kg/m2, no comorbidities and previous SARS-CoV-2 test status were associated with local adverse effects
Menni C et al. Lancet Infect Dis April 27, 2021
• Systemic side-effects after BNT162b2 (Pfizer) and ChAdOx1 nCoV-19 (Astra-Zeneca) vaccination occur at frequencies lower than reported in phase 3 trials.
Safety of COVID-19 Vaccines: 627,383 individuals in UK
13% 22% 34%
Menni C et al. Lancet Infect Dis April 27, 2021
Safety of COVID-19 Vaccines: 627,383 individuals in UK• Systemic adverse effects self-reported to the COVID Symptom Study app after COVID-19
vaccination, stratified by sex, age, BMI, health status, and previous SARS-CoV-2 test status
Pfizer 2nd dose Astra_Zeneca 1st dose
Female gender, younger people, BMI<30 kg/m2, comorbidities and previous SARS-CoV-2 test status were associated with systemic adverse effects
Baden LR, et al. N Engl J Med 2021; 384:403-16; Blumenthal KG et al. N Engl J Med. April 1 2021.
Delayed Large Local Reactions to mRNA-1273 (Moderna) Vaccine• Injection-site reactions are common and observed in 84% of the participants after the first dose of mRNA-1273 vaccines. • Delayed injection-site reactions are rare events that occurred in 244 of the 30,420 participants (0.8%) after the first dose
and in 68 participants (0.2%) after the second dose.• Delayed-type or T-cell–mediated hypersensitivity was supported by skin-biopsy specimens.
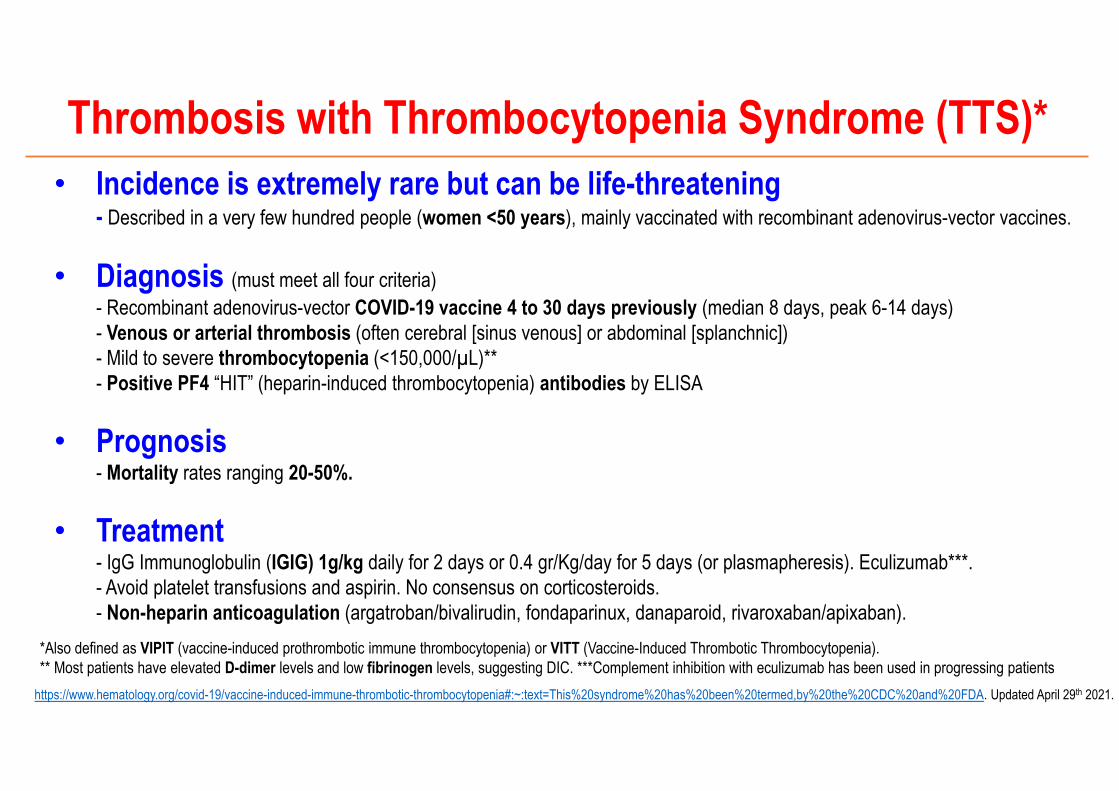
*Also defined as VIPIT (vaccine-induced prothrombotic immune thrombocytopenia) or VITT (Vaccine-Induced Thrombotic Thrombocytopenia).** Most patients have elevated D-dimer levels and low fibrinogen levels, suggesting DIC. ***Complement inhibition with eculizumab has been used in progressing patients
Thrombosis with Thrombocytopenia Syndrome (TTS)* • Incidence is extremely rare but can be life-threatening
- Described in a very few hundred people (women <50 years), mainly vaccinated with recombinant adenovirus-vector vaccines.
• Diagnosis (must meet all four criteria)- Recombinant adenovirus-vector COVID-19 vaccine 4 to 30 days previously (median 8 days, peak 6-14 days)- Venous or arterial thrombosis (often cerebral [sinus venous] or abdominal [splanchnic])- Mild to severe thrombocytopenia (<150,000/µL)**- Positive PF4 “HIT” (heparin-induced thrombocytopenia) antibodies by ELISA
• Prognosis- Mortality rates ranging 20-50%.
• Treatment- IgG Immunoglobulin (IGIG) 1g/kg daily for 2 days or 0.4 gr/Kg/day for 5 days (or plasmapheresis). Eculizumab***.- Avoid platelet transfusions and aspirin. No consensus on corticosteroids. - Non-heparin anticoagulation (argatroban/bivalirudin, fondaparinux, danaparoid, rivaroxaban/apixaban).
https://www.hematology.org/covid-19/vaccine-induced-immune-thrombotic-thrombocytopenia#:~:text=This%20syndrome%20has%20been%20termed,by%20the%20CDC%20and%20FDA. Updated April 29th 2021.
Second Dose Astra-Zeneca Vaccine
Yes or Not
Blanco J on behalf the Multidisciplinary Collaborative Group for the Scientific Monitoring of COVID-19 (GCMSC); https://www.isglobal.org/documents
• Administer a 2nd dose of the same Astra-Zeneca vaccine: an option with the potential risk of TTS.
Alternatives for individuals under 60 years of age having received the first dose of Astra-Zeneca vaccine
Blanco J on behalf the Multidisciplinary Collaborative Group for the Scientific Monitoring of COVID-19 (GCMSC); https://www.isglobal.org/documents
Adenovirus-vector vaccines• Oxford-Astra Zeneca
- After 1st dose: 10 cases per million→ After 2nd dose: 1 case per million
• Jansen: 2-4 cases per million• Sputnik V: no information
mRNA vaccines• Pfizer-BioNTech, 0.2 cases per million• Moderna, 0.4 cases per million
Thrombosis with Thrombocytopenia Syndrome (TTS) Rates
Blanco J on behalf the Multidisciplinary Collaborative Group for the Scientific Monitoring of COVID-19 (GCMSC); https://www.isglobal.org/documents
ICU admissions prevented with COVID-19 Vaccination and risk of TTS per age group
Blanco J on behalf the Multidisciplinary Collaborative Group for the Scientific Monitoring of COVID-19 (GCMSC); https://www.isglobal.org/documents
• Administer a 2nd dose of the same Astra-Zeneca vaccine: an option with the potential risk of TTS.
• Administer a 2nd dose of a different vaccine (mRNA Pfizer or Moderna): an option that lacks data.
Blanco J on behalf the Multidisciplinary Collaborative Group for the Scientific Monitoring of COVID-19 (GCMSC); https://www.isglobal.org/documents
Alternatives for individuals under 60 years of age having received the first dose of Astra-Zeneca vaccine
• Preclinical evidence in animal models.• Two studies in UK and one in Spain (ISCIII, Madrid) are on going.
Not powered to provide safety data.• Com-COV* provided initial reactogenicity data after 2nd dose
Administer a 2nd dose of a different Vaccine:mRNA Pfizer or Moderna vaccine
Blanco J on behalf the Multidisciplinary Collaborative Group for the Scientific Monitoring of COVID-19 (GCMSC); https://www.isglobal.org/documents*Shaw RH et al. Lancet. May 12, 2021
Prime/Boost Fever reported Paracematol use x AEs- AZ followed by AZ 10% 36%- AZ followed by Pfizer 34% 57%- Pfizer followed by Pfizer 21% 41%- Pfizer followed by AZ 41% 60%
• Administer a 2nd dose of the same Astra-Zeneca vaccine: an option with the potential risk of TTS.
• Administer a 2nd dose of a different vaccine (mRNA Pfizer or Moderna): an option that lacks data.
• Wait until evidence for one of the previous options is generated. This option relies on a still unknown parameter: the durability of immune response after a single dose.
Blanco J on behalf the Multidisciplinary Collaborative Group for the Scientific Monitoring of COVID-19 (GCMSC); https://www.isglobal.org/documents
Alternatives for individuals under 60 years of age having received the first dose of Astra-Zeneca vaccine
• There are no data (nor clinical trials) with Astra-Zeneca on how long the protection lasts beyond 3 months after the first dose.
• Antibody levels are not optimal after one dose of Astra Zeneca, and seem to be lower compared to Pfizer and Moderna’s vaccines.
• People could be more susceptible to infections by new SARS-CoV-2 variants, as suggested by several studies showing that people receiving one vaccine dose without prior infection showed reduced immunity against B1.1.7 (British), B1.351 (South African) and B.1.617 (India) variants.
Wait until evidence for previous options is generated: There is an important risk of leaving people with a single dose beyond 3 months!
Blanco J on behalf the Multidisciplinary Collaborative Group for the Scientific Monitoring of COVID-19 (GCMSC); https://www.isglobal.org/documents; https://www.gov.uk/government/news/vaccines-highly-effective-against-b-1-617-2-variant-after-2-doses press release, May 22 2021;
Emary KRW et al. Lancet. Apr 10 2021; 397:1351-1362.
• The safety/efficacy evidence for the administration of a second dose of mRNA vaccines to Astra-Zeneca vaccinated individuals is currently being studied.
• Meanwhile, a second dose of Astra-Zeneca should be offered no later than 3 months after 1st dose to individuals under age 60 given the strong evidence for efficacy and the very low risk of TTS.
Recommendations of the Multidisciplinary Collaborative Group for the Scientific Monitoring of COVID-19 (GCMSC)
Blanco J on behalf the Multidisciplinary Collaborative Group for the Scientific Monitoring of COVID-19 (GCMSC); https://www.isglobal.org/documents
• When millions of vaccines are administered, serious unexpected serious adverse reactions (SUSARs) can be detected.
• CDC investigating reports some young COVID-19 vaccine recipients have experienced myocarditis*
Pharmacovigilance!
*https://www.nytimes.com/2021/05/22/health/cdc-heart-teens-vaccination.html; May 22 2021
What plan do we have for 2021? Vaccination but still facial masks, hand washing, social distance!!!
Rail commuters wearing white protective masks, one with the additional message “wear a mask or go to jail,” during the 1918 influenza pandemic in California. Vintage Space/Alamy
https://www.nytimes.com/2020/08/03/us/mask-protests-1918.html; *Gandhi M et al. NEJM Oct 29 2020 https://www.nejm.org/doi/full/10.1056/NEJMp2026913
COVID-19 Second Year: SARS-CoV-2 Variants, Long COVID-19 & Vaccines
Current epidemiological and mortality data New SARS-CoV-2 variants update Long COVID-19: where we are one year later Remdesivir, dexamethasone, heparin and … something else? Reinfections: state of the art Vaccines efficacy and impact of new SARS-CoV-2 variants Vaccines safety: TTS* Take-home messages
May 25th 2021*Thrombosis with Thrombocytopenia Syndrome (TTS)
Take-home messages The SARS-COV-2 virus is continually evolving with new variants appearing (UK, South Africa, Brazil, India) that give it greater transmissibility and in some cases resistance to the antibodies generated by natural immunity or vaccines.
It is very important to distinguish the symptoms of long COVID from the sequelae of the infection. The prevalence is high and can persist for weeks or months. There is no specific treatment.
Remdesivir is effective against moderate and severe COVID-19 (stages 4-6), although it does not reduce mortality. Dexamethasone plus tocilizumab reduced mortality in severe and critical COVID-19.
Although there are already many millions of people vaccinated against COVID-19, implementation is uneven around the world. Some newer variants may escape vaccines, although the good news is vaccines still protect individuals against severe disease.
Acknowledgements
To all front-line health-care workersTo our patients and their families
A. MorenoR. ParedesC. PontesM. SansA. SarukhanJ. SellaresA. Vallano
J. BlancoC. BrotonsB. ClotetS. de San JoséO. CollG.M. LledóG. Mora
May 25th 2021
Acknowledgements
To all front-line health-care workersTo our patients and their families
A. MorenoR. ParedesC. PontesM. SansA. SarukhanJ. SellaresA. Vallano
J. BlancoC. BrotonsB. ClotetS. de San JoséO. CollG.M. LledóG. Mora
Thanks to the 1,500,000 people who have seen these CME videos!
May 25th 2021
ACTUALIZACIONESCONTENIDO COVID-19
Gracias al patrocinio de
#YoMeCorono
Ayuda a seguir investigando:yomecorono.com
Conversaciones COVID-19 con el Dr. Clotet: yomecorono.com/conversaciones