28
THE 3 D’S DEMENTIA, DELIRIUM, DEPRESSION Ida Shepherd 1
| Date post: | 22-Dec-2015 |
| Category: |
Documents |
| Upload: | della-harrell |
| View: | 217 times |
| Download: | 0 times |
1
THE 3 D’SDEMENTIA, DELIRIUM,
DEPRESSIONIda Shepherd
2
LEARNING OUTCOMESDistinguish between the functions of the left & right brain as well as the lobe functions.
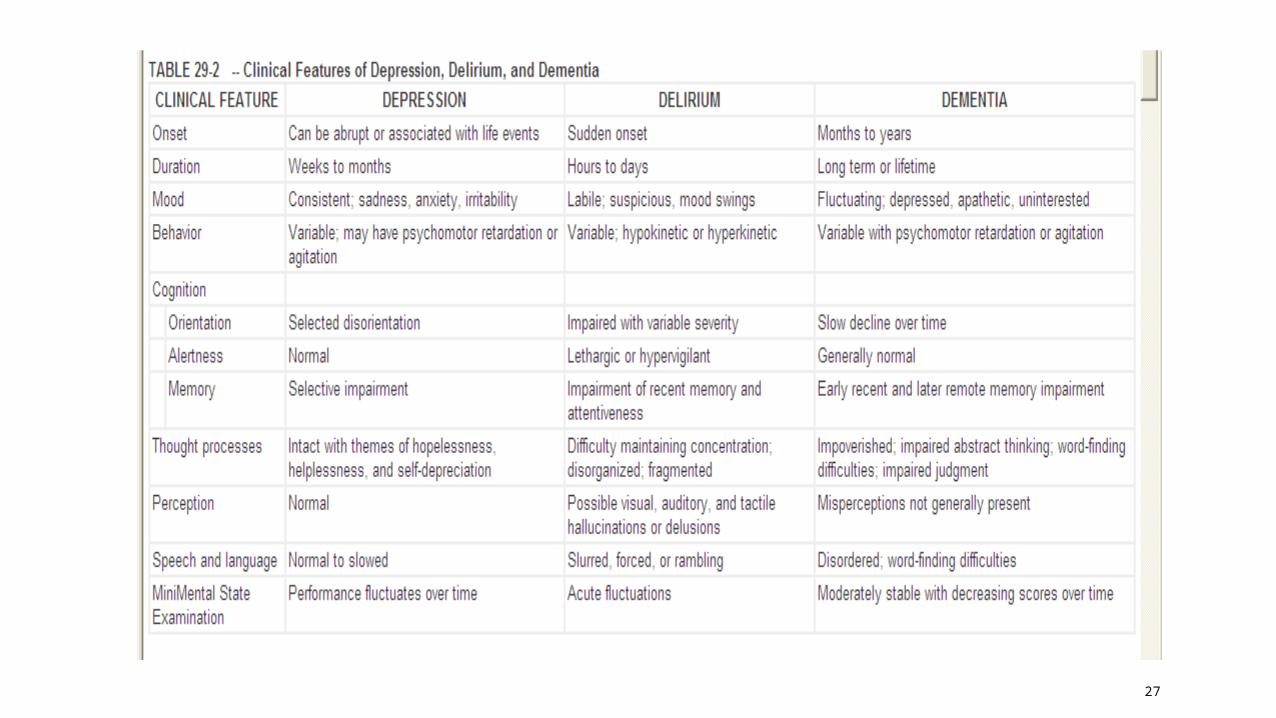
Define and discuss the differences between DDD.
Identify the causes of DDD.
Identify & define the behavioural & psychological Sx of dementia.
Identify the diagnostic interventions that aid diagnosis in dementia & delirium.
List medications useful in the Tx of DDD
Identify the Risk Factors for depression in the elderly.
Identify & discuss the clinical manifestations of depression in the elderly.
Discuss what Cognitive Behavioural Therapy is.
Identify & explain de-escalation strategies for personal & patient safety.
3
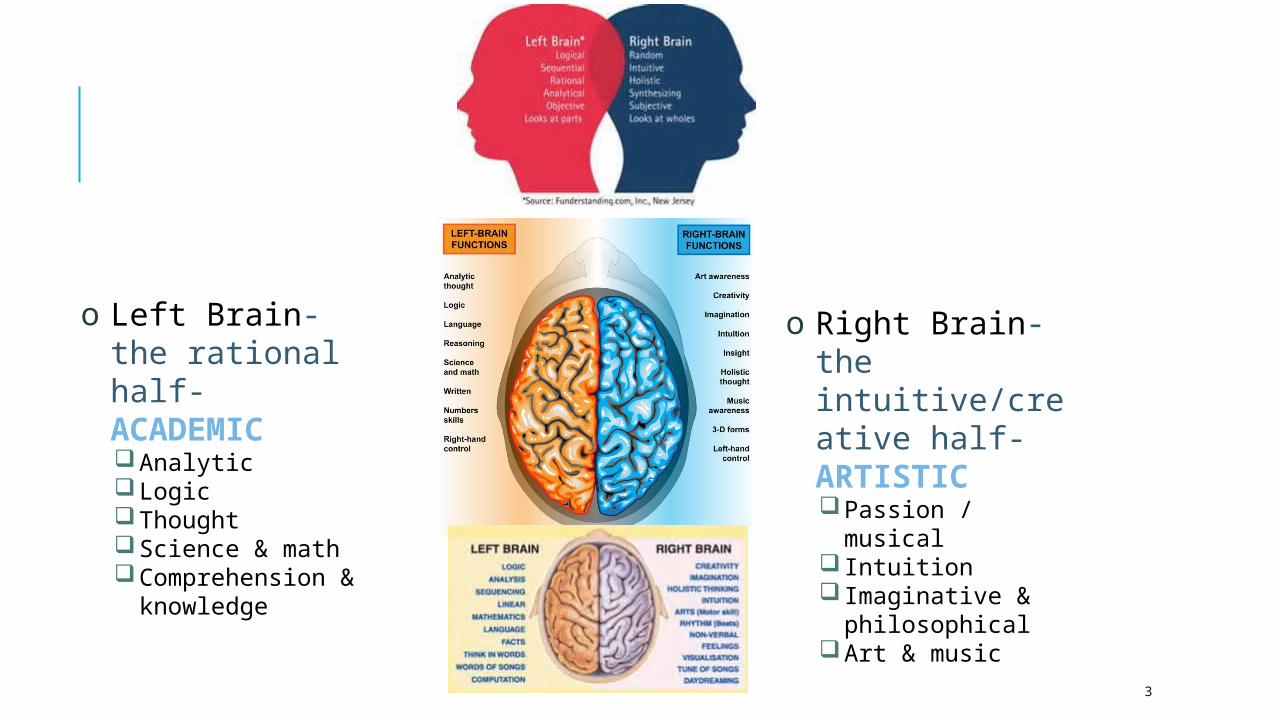
o Right Brain- the intuitive/creative half-ARTISTICPassion / musical Intuition Imaginative &
philosophicalArt & music
o Left Brain-the rational half-ACADEMICAnalyticLogicThoughtScience & mathComprehension &
knowledge
4
CRITICAL THINKINGMr K is a 75 year old retired engineer seen in the emergency room with his wife of 50 years who reports that her husband is confused, agitated, and has been seeing and hearing things that were not there. A major nursing intervention in caring for Mr K must include which of the following?
A. Assess duration of symptoms
B. Inquire about his current and over-the-counter medications, including if new medications hav3e been added recently
C. Inquire about substance abuse/dependence history
D. All of the above
5
DEMENTIA
• Multiple causes of dementia
• Is a syndrome associated with a range of diseases characterised by the progressive impairment of brain functions, which include loss of memory, cognitive skills, orientation, attention, language, judgment and reasoning, and personality.
• Manifestations can be mild – moderate – severe• See Table 56-6 “Causes of Dementia” Lewis Chapter 56.
• All dementias share a common symptom presentation but are differentiated based on etiology.
• The disorder may be progressive or static, permanent or reversible.
6
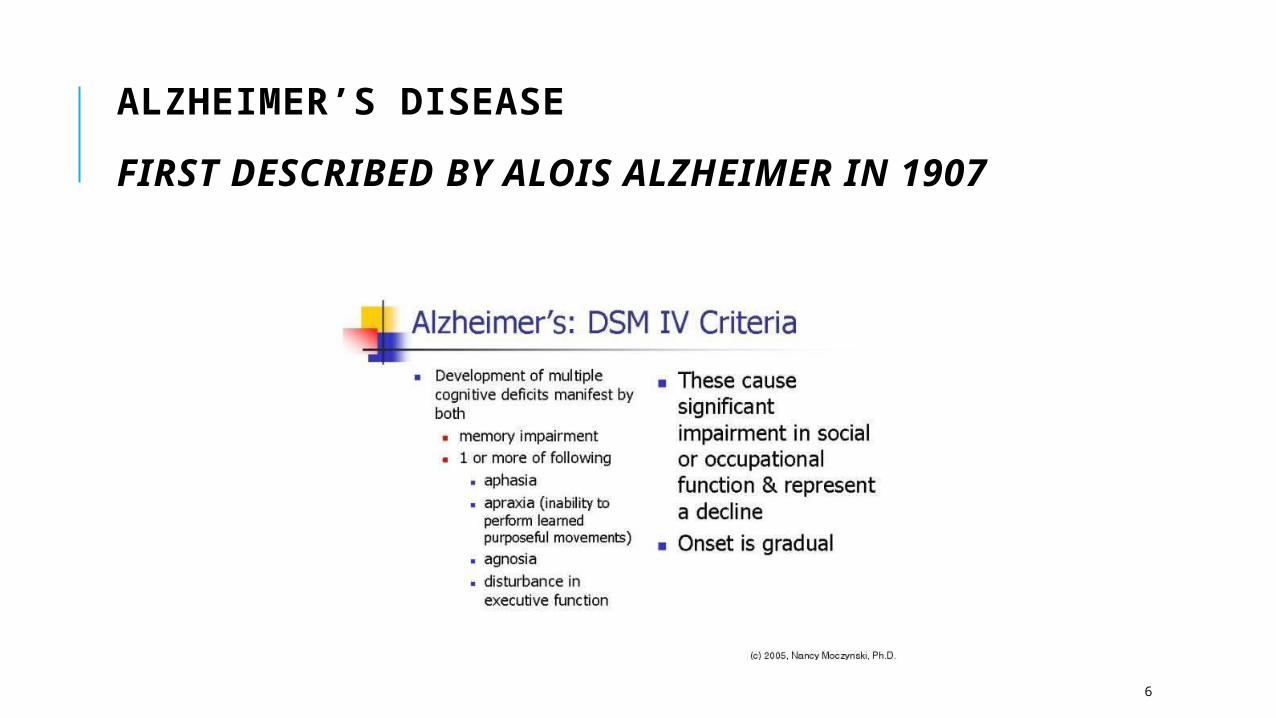
ALZHEIMER’S DISEASE
FIRST DESCRIBED BY ALOIS ALZHEIMER IN 1907
7
ALZHEIMER’S DISEASE IS THE DEGENERATION OF THE CEREBRAL CORTEX OF THE BRAIN RESULTING IN A CORTICAL DEMENTIA. IT IS CHARACTERIZED BY MULTIPLE IMPAIRMENTS IN COGNITIVE FUNCTION WITHOUT IMPAIRMENT OF CONSCIOUSNESS.” - DSM4
PathologyAlzheimer’s disease is the most common cause of dementia accounting for
more than 60% of diagnoses.
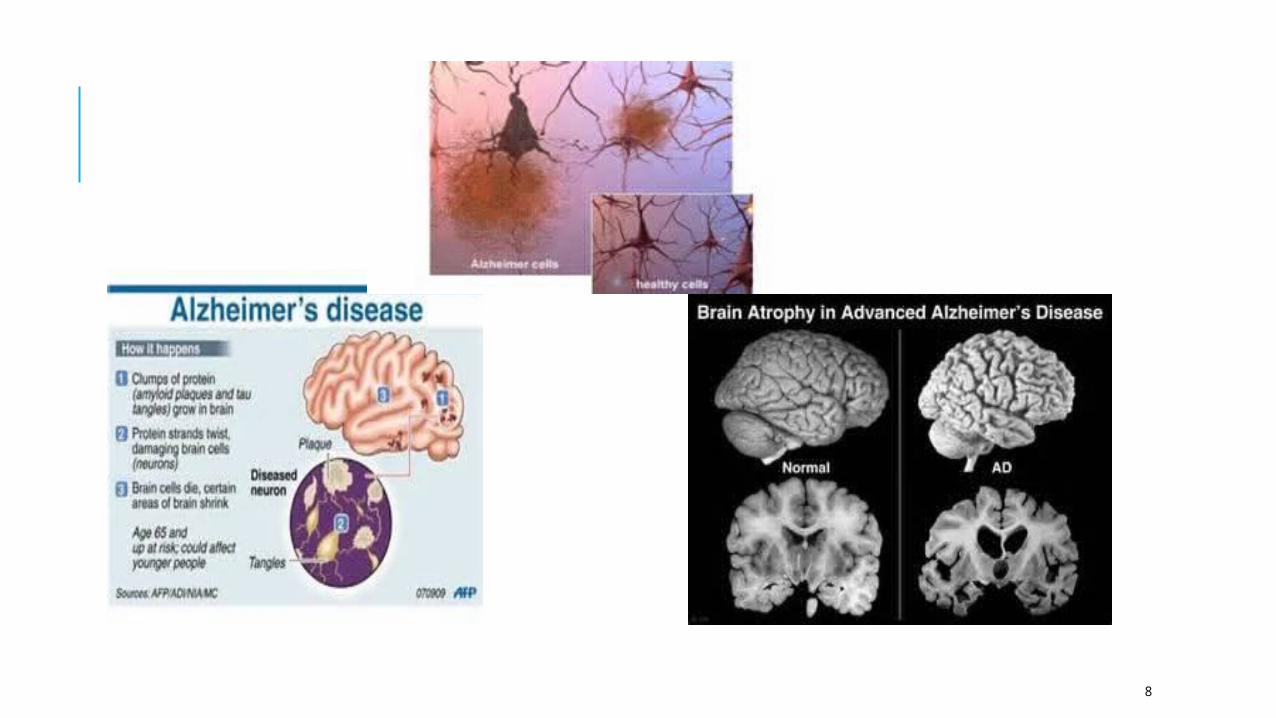
The pathology of Alzheimer’s disease includes diffuse, progressive atrophy of the cortex (resulting in smaller brain size) (& also in the parietal & temporal lobes), & with a loss of neurons, there is ventricular enlargement with a concomitant appearance of neuritic senile plaques ( secretion of amyloid β protein & degenerating axonal & dendritic nerve terminals) and neuro-fibrillary tangles (masses of non-functioning neurons composed of tau protein).
The number of plaques and tangles correlates to the severity of the dementia.
8
9
DEMENTIA WITH LEWY BODIES(DLB)
A neurodegenerative disease assoc with the formation & accumulation of round α-synuclein protein lumps called Lewy bodies inside affected neurons. They interfere with the actions of acetylcholine & dopamine.
Risk Factors: >60 yrs, male, family hx of DLB or a carrier of the apolipoprotein E46K allele.
May be the 2nd most prevalent type of dementia after AD.
Dx is challenging because some of the symptoms of DLB resemble those of AD or PD. Early course resembles AD, later course looks like PD.
DLB has distinct symptoms: behavioural problems, fluctuations in cognition, movement symptoms, extreme sensitivity to antipsychotics, sleep problems, & V/S changes
10
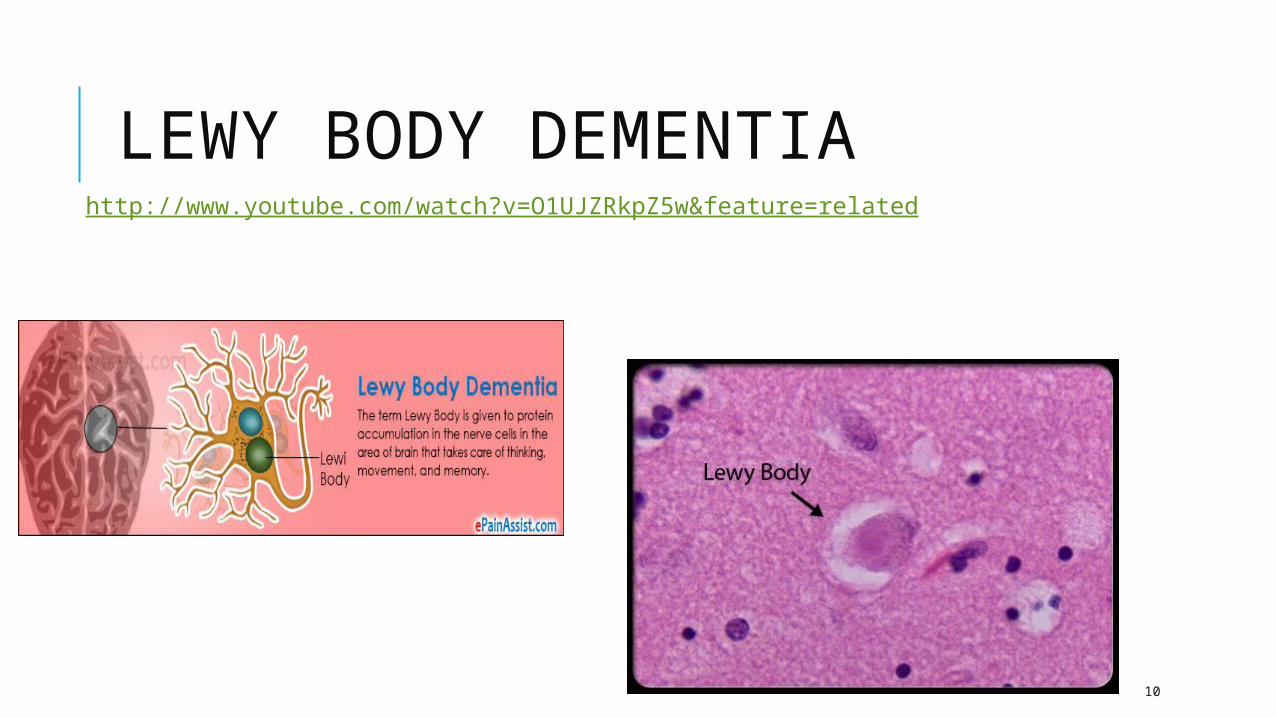
LEWY BODY DEMENTIAhttp://www.youtube.com/watch?v=O1UJZRkpZ5w&feature=related
11
CLINICAL MANIFESTATIONS
Depending on the cause of the dementia, symptoms can be insidious and gradual or more abrupt.
Neurological degeneration is gradual and progressive
Vascular dementia takes a stepwise deterioration.
12
BPSD - BEHAVIOURAL & PSYCHOLOGICAL SYMPTOMS OF DEMENTIA
BehaviouraloAggressionoWanderingoSleep disturbanceoShadowingoIntrusivenessoDisinhibitionoSocial withdrawaloPsycho-motor agitationoResistiveness
PsychologicaloDelusionsoHallucinationsoParanoiaoDepressionoAnxietyoMisidentificationoMisinterpretationoCatastrophic reactionsoAdjustment problems
13
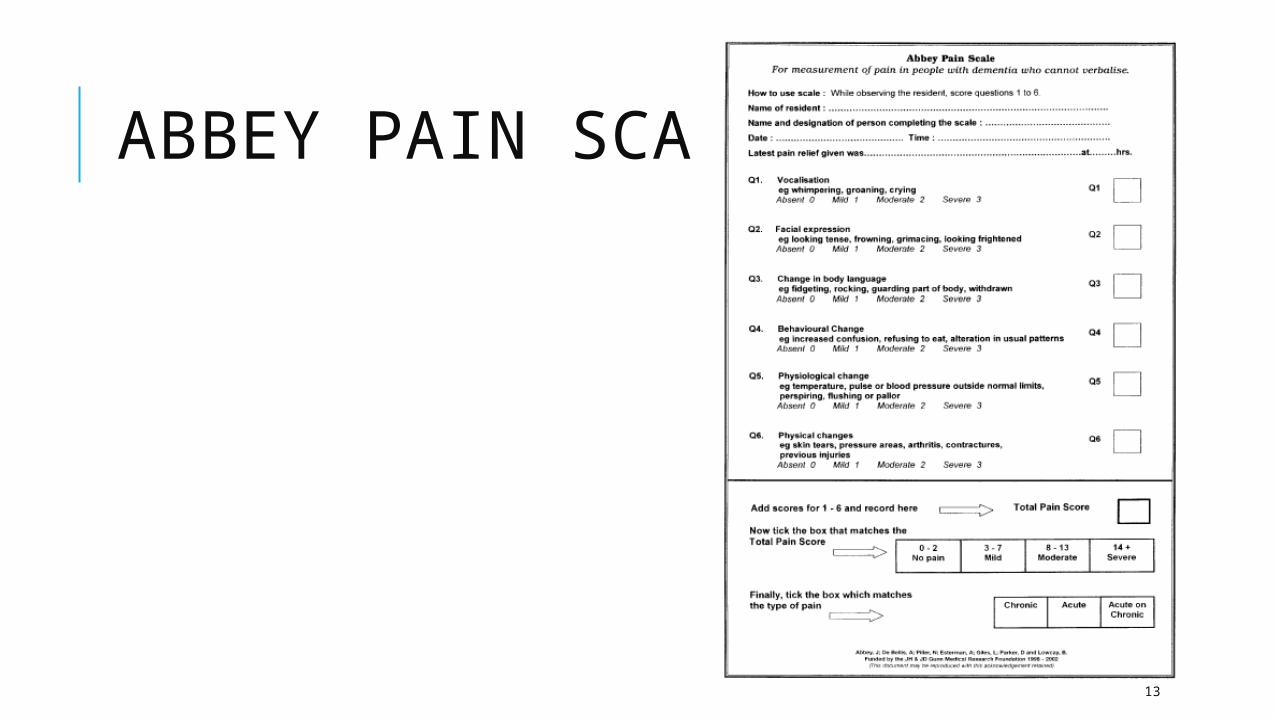
ABBEY PAIN SCALE
14
ALZHEIMER’S DISEASE
Diagnostic Primarily based on exclusion MRI & PET scans to identify
hippocampal atrophy CT or MRI may show brain atrophy,
enlarged ventricles in late stages (not definitive)
FBC, ECG, glucose, creatinine, urea, Vit B1-B6 & B12 levels, TFT, LFT
Neuropsychological testing, clock drawing and MMSE
Treatment Donepezil(acetylcholinesterase inhibitor) Galantamine(cholinomimetic) Rivastigmine(brain selective cholinesterase inhibitor) Risperidone(antipsychotic-neuroleptic) Nefazodone(anti-depressant) Memantine(noncompetitive N-methyl-D-aspartate [NMDA] antagonist
Gingko Biloba
15
PHARMACOLOGICAL INTERVENTIONS:THERE IS NO KNOWN DRUG TREATMENT THAT CAN REVERSE THE COURSE OF ALZHEIMER’S DISEASE.
Cholinesterase inhibitorso Initial brief improvement in cognitive ability
o Can help with behavioral and psychological symptoms
o Slows the progression of cognitive and non-cognitive loss
o Blocks cholinesterase which is an enzyme responsible for bkdwn of aceytylcholine
Antipsychotics – typical vs atypical Can help reduce BPSD Can cause cognitive impairment, sedation, and falls Multiple side-effects Same meds as in delirium
inhibitors
Benzodiazepines Anxiolytic effect Help with agitation and aggression Help reestablish sleep/wake cycle Cause motor & cognitive impairment Addiction & withdrawal Falls Paradoxical effects
AntidepressantsSSRIs help reduce distress and treat
SSRIs help reduce distress and treat depression
Occasionally help reduce BPSD
Can cause delirium
Fluoxetine, sertraline, CITALOPRAM (SSRI)
16
DELIRIUM AKA ACUTE CONFUSIONAL STATE
A transient, organic mental syndrome characterized by reduced level of consciousness, reduced ability to maintain attention, perceptual disturbances, and memory impairment (DSM4-TR in Meiner, 2006).
Delirium has a sudden onset, a usually brief, fluctuating course, and a rapid improvement once the causative factor is identified and treated.
Shows poor concentration, language disturbance, clouding of consciousness, misperceptions, illusions, or hallucinations, disorientation to PPT, memory problems, incr or decr physical activity, impaired judgment
17
POTENTIAL CAUSES OF DELIRIUM...
Absence of time and place cues
Change in environmentChronic illness (CHF)DehydrationElectrolyte imbalancesHospitalisation (ICU)Hypercarbia/capniaSensory deprivationSensory overloadStressTrauma
HyperthermiaHypoglycaemiaHypothermiaHypoxiaImmobilisationInfectionLiver diseaseMeds: sedative hypnotics, narcotics, benzosMetabolic disordersPain (untreated)Renal disease
18
DELIRIUM CONTINUED...
Can manifest as: hypoactivity or hyperactivity, and can be mixed at different times of the day.
Delirium will usually develop over 2-3 days
Diagnosis:
Med Hx
Physical exam
Medication scrutiny
MMSE
FBC, lytes, urea, creatinine, ECG, u/a, LFT, TFT’s, SP02, and if suspected - drug &/or ETOH levels, Ca, B12, ESR, CRP, glucose
19
DEPRESSION Common disorder throughout the lifespan
Most commonly diagnosed mental disorder in NZ & Australia
OA ‘s – diagnosis in relation to isolation, loss of partner, medical diagnoses that may require regular medical input e.g. MI or CA or functional/cognitive impairment
Increases the risk of suicide – very elderly most at risk of taking their own life
Australia has the highest rate for suicides among men in the 85+ age group compared to NZ where adults aged 65+ had the lowest suicide rate
A very uneven gender distribution as depression is about twice as common in women than in men. The reasons not entirely clear, but are thought to be partly biological, partly psychological, and partly sociocultural.
Using DSM-IV’s criteria for ‘major depressive disorder’an average person has about a one in seven (15 percent) chance of developing depression in the course of his or her lifetime
20
DEPRESSION CONT’D..........
MANIFESTATIONS Fatigue
Constipation
Psychomotor retardation
Depressed mood
Loss of interest
Decreased Energy
Failing to pay attention to pre-existing conditions
Decreased Libido or pleasure
Changes in appetite
Decreased Weight
Sleep patterns
Agitation
Anxiety
Crying
Increased somatic complaints
21
DEPRESSION CONT’D…
Risk assessment & suicide prevention
High rates of substance abuse being noticed in the OA population
Treatment is effective when there is a combination of psychological and medicinal therapies.
22
TREATMENT: Cognitive Behaviour Therapy & Interpersonal Psychotherapy
Drugs:
TCA’s (Tricyclic antidepressants) amitryptyline, imipramine, chlomipramine, nortriptyline.
MAOI’s: (Monoamine Oxidase inhibitors) Isocarboxzid (Marplan), Phenelzine (Nardil)
SSRI’s: (Selective Serotonin Receptive Inhibitors) Fluoxetine (Prozac) Sertraline, Fluvoxamine, Paroxetine
SNRI’s: (Serotonin and norepinephine reuptake inhibitors) Venalfaxine (Effexor XR), Duloxetine (Cymbalta), Desvenlafaxine (Pristia)
23
A CASE STUDY:
An 86-year-old man has just been admitted with dehydration. He is not a good historian because of acute confusion. However, his family indicates that he is an active, independent man who recently participated in the Senior Olympics. The nurse instructs him not to get out of bed by himself because he is old and frail. He has to void and calls for the nurse, but he cannot wait, so he walks to the bathroom and falls. To protect him from further falls, he is put in a vest restraint. He already has a reddened area over his sacrum. He then needs to void again but cannot, so he wets the bed. The patient is now restrained and has an incontinent brief in place.
Symptoms of depression and loss of appetite soon become evident. A feeding tube is inserted. The confusion gradually becomes more apparent; the patient pulls at his various tubes, prompting the nurse to apply wrist restraints. The patient's whole life has become a hospital bed. The cognitive impairments and the ever-changing environment prompt yelling out (from fear and anger). A chemical restraint is then applied in the form of a medication to reduce the agitation
24
DE-ESCALATION – SOME BASICS…
If you choose not to speak (up), see (what’s happening) or hear (what’s occurring), then all hell can break loose!!
25
HOW TO STAY CALM IN STRESSFUL SITUATIONS
Breathing
o as you initiate the event take a deep breath
consciously control your breathing
Self Talk
o Unconscious automatic thoughts generate emotions, emotions stimulate behaviour and physical responses, so . . . what we do is a result of what we feel and what we feel is a result of what we think
Body Language & Voice
o Relax – clench and unclench your fists
o check your body language
o check your voice
26
DE-ESCALATION STRATEGIESSAFETY – KEEP YOURSELF SAFE, THEN OTHERS, THEN THE PERSONIntervene early Be courteous
Inform others Express concern
Know your exits Acknowledge feelings
Know when to get help Avoid being judgmental
Stay calm Be willing to listen
Monitor your voice Provide reassurance
Monitor your body language Give the person a way out with dignity
Use open gestures Use humor
Remember KISS Be kind
Be assertive Permit verbal venting
Offer choice Set reasonable limits
Use open ended questions Use self talk
27
28
REFERENCES
Brown, D., & Edwards, H. (2008). Lewis’s medical-surgical nursing: Assessment and management of clinical problems. Sydney: Mosby Elsevier.
Meiner, S. E., & Lueckenotte, A. G. (2006).Gerontologic nursing (3rd ed.). St Louis: Mosby Elsevier.
Nay, R., & Garratt, S. (2009). Older people: Issues and innovations in care. (3rd ed.). Sydney: Churchill Livingstone Elsevier.
http://www.healthline.com/health/depression/medication-list

















