The administration of radiographic contrast media to patients with a history of a previous reaction Michael Schatz, M.D., Roy Putterson, M.D., John O’Rww~, M.D., James Nickelsen, M.D., and Cindy Nottkup, M.D. Chicnp, Ill. The occurrence of au immrtliatc, systemic reaction after the administra- tion of radiographic contrast media (RCM) constitutes a problem of initial and ~~Ot~Xtiilll~ l:ltt>r (‘Ollf’C1’11. Tllc immcdiatc problt~m rcqnircs trcatmmlt of the :W,UtC!, illli~~~ll~VlLl~~ti~ t,.VpP Of ma&m. 1 That later proldom that must bc considcrcd after the suhsitlcnrtt ol’ tlic initial reaction is whether or not, tllc patkiit call s;ti’cly reccivcx R(1JI 011any sihseq~~c!nt. oc*casion. Tllc g~cneral procedure that many pliyskians tlilVC f’ollowrtl for such IIiltiClltS was to inform then1 tht SUCll :I rc:ic!tion to I<(31 is an ;Iholutc ~ontriiintlic~ation to further use oi’ suds lllatcriill. Altliough this is appropriate adviw for most (1 rug reactions, the prYhleni wit11 li(‘Jl is soincwhrt SpCCiill. First, nnlikc inost tlrug I’CilCtiOllS, suitaldc noit-cross-reactil~~ suhtitutcs fol 1tCM arc not ;~vailatdc. S(~(+oiid, altl~ougl~ lY?il~thllS to ~oiitrast media arc im- From the Rrction of Allergy-lrnmuilology, Department of Medicine, Northxveatern IJniversity Mrtlkxl School. Supported by Ilnitrd Rtntrs Public Health Service Grant. No. Al 11403 and the Ernest 8. l~nzlcy Grant. Rrccivetl for pul~lkxtiou April 15, 1974. Reprint requests to: Dr. Roy Patterson, North~vestern IJniverCty Medical Bclmool, 303 XC. C’llic*ngo Ave., Chicago, 111. 60611. Vol. .55, No. 5, pp. 35X-366
Transcript
The administration of radiographic contrast media to patients with a history of a previous reaction Michael Schatz, M.D., Roy Putterson, M.D., John O’Rww~, M.D.,
James Nickelsen, M.D., and Cindy Nottkup, M.D. Chicnp, Ill.
The occurrence of au immrtliatc, systemic reaction after the administra- tion of radiographic contrast media (RCM) constitutes a problem of initial and ~~Ot~Xtiilll~ l:ltt>r (‘Ollf’C1’11. Tllc immcdiatc problt~m rcqnircs trcatmmlt of the :W,UtC!, illli~~~ll~VlLl~~ti~ t,.VpP Of ma&m. 1 That later proldom that must bc considcrcd after the suhsitlcnrtt ol’ tlic initial reaction is whether or not, tllc patkiit call s;ti’cly reccivcx R(1JI 011 any sihseq~~c!nt. oc*casion. Tllc g~cneral procedure that many pliyskians tlilVC f’ollowrtl for such IIiltiClltS was to inform then1 tht SUCll
:I rc:ic!tion to I<(31 is an ;Iholutc ~ontriiintlic~ation to further use oi’ suds lllatcriill. Altliough this is appropriate adviw for most (1 rug reactions, the prYhleni wit11 li(‘Jl is soincwhrt SpCCiill.
First, nnlikc inost tlrug I’CilCtiOllS, suitaldc noit-cross-reactil~~ suhtitutcs fol 1tCM arc not ;~vailatdc. S(~(+oiid, altl~ougl~ lY?il~thllS to ~oiitrast media arc im-
From the Rrction of Allergy-lrnmuilology, Department of Medicine, Northxveatern IJniversity Mrtlkxl School.
Supported by Ilnitrd Rtntrs Public Health Service Grant. No. Al 11403 and the Ernest 8. l~nzlcy Grant.
Rrccivetl for pul~lkxtiou April 15, 1974.
Reprint requests to: Dr. Roy Patterson, North~vestern IJniverCty Medical Bclmool, 303 XC. C’llic*ngo Ave., Chicago, 111. 60611.
Vol. .55, No. 5, pp. 35X-366
VOLUME 55 NUMBER 5
Administration of radiographic contrast media 359
mediate in onset and mimic IgE-mediated reactions, there is no evidence that these reactions are immunologic in mechanism, particularly in relation to IgE. Immediate-type cutaneous reactivity that is not an irritant reaction, as demon- strated by passive transfer with serum, does not, to our knowledge, occur. The reactions thus may be considered to result from the nonimmunologic release of vasoactive mediators, presumptively histamine, from mast cells and basophils.2-4 Finally, diagnostic indications for the use of RCM are such that they may be of
great importance to the individual patient. Preoperative diagnosis of vascular or neoplastic lesions may demonstrate the necessity for a lifesaving procedure, or, conversely, demonstrate that the procedure is unnecessary. The latter situation is of particular significance in high-risk surgical procedures or in patients who are at risk because of cardiovascular or other disease.
Recognizing these factors, in 3965 the Allergy-Immunology Section at this medical center accepted the task of attempting to evaluate, advise, and, where necessary, administer RCM to patients who gave a history of previous adverse reactions to RCM. This report describes the experience in 95 consecutive consultations requested for this problem, the majority of whom have been seen since .Julp, 1972. The clinical series includes patients who had histories that were not considered to constitute an additional risk; patients who, after careful consideration, did not need the readministration of RCM; and patients with a history of previous reactions who rrqnired and received RCM.
METHODS Patients and evaluation of previous reactions
Consultative opinions on 95 patients were requested from the Allergy-Immunology Section
of this medical center. The history of the previous reaction to RCM was evaluated in detail, and the previous reaction was classified as an immediate, generalized reaction (IGR) if the
patient described urticarin, generalized pruritus, nngioedema, syncope, definite hypotension recorded by a physician, or asthma, occurring within minutes of the previous test. A general
feeling of warmth was not accepted as an IGR when it was not accompanied by cutaneous
lesions or definite pruritus.
Evaluation of the indication for repeat administration of RCM
General medical history, physical examination, and laboratory data were evaluated in
relation to the presumptive diagnosis and the indication for the radiographic procedure. The
attending physician and, in most cases, a consultant were asked to define the necessity for the radiographic procedure. In the case of a patient with a history of an IGR to RCM, they
were further asked to state their opinions that the indication for the procedure justified the
readministration of RCM in view of the fact that there was an unknown degree of additional risk.
After establishment of the indication for the study, both the need for the study and the possible risks were discussed with the patient. Where indicated, the potential risk was discussed
with relatives of the patient.
Preparation for the procedure
Skin testilzg. It is our experience that the intracutaneous injection of undiluted RCM will produce primary irritant reactions in a high percentage of normal subjects. Although im-
360 Schatz et al. J. ALLERGY CLIN. IMMUNOL. MAY 1975
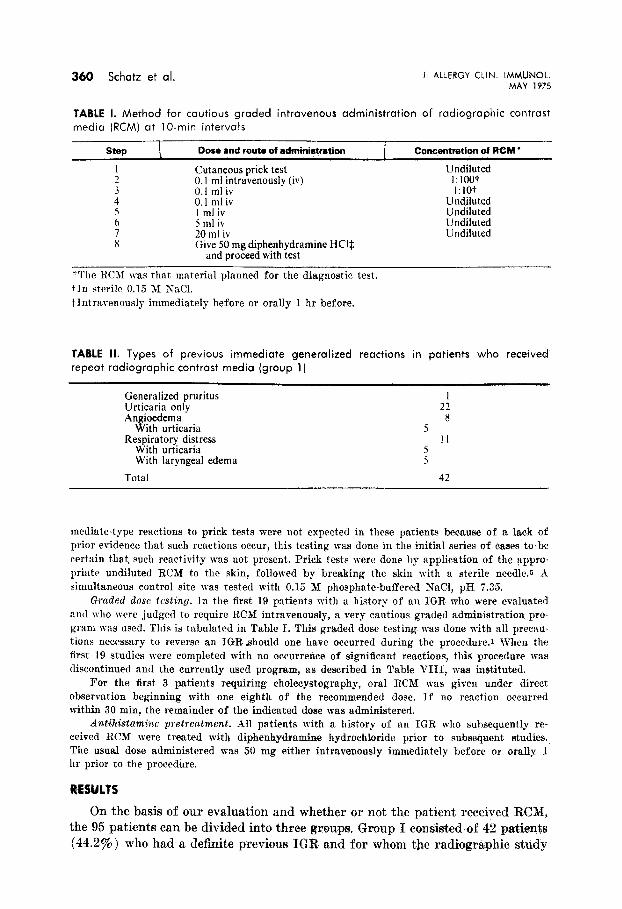
TABLE 1. Method for cautious graded intravenous administration of radiographic contrast
media (RCM) at IO-min intervals
step L Dose and routa of admih%atian CtorwerwMon of RCM l
: Cutaneous prick test Undiluted i:) rnf ;;travenously (iv) 1:100t
;: 1:10+
Undiluted 5
y.;;tiv Undiluted
6 5 ml iv Undiluted
ii 20 ml iv Undiluted Give 50 mg diphenhydramine HCQ
and proceed with test
“The RCM was that material planned for the diagnostic test. tin sterile 0.15 M SaCl. $ Intravenously immediately hefore or orally 1 hr before.
TABLE II. Types of previous immediate generalized reactions in patients who received
repeat radiographic contrast media (group 1)
Generalized pruritus Urticaria only Angioedema
With urticaria Respiratory distress
With urticaria With laryngeal edema
Total
2: 8
5 11
5 5
42
mediate-type reactions to prick tests were not expected in these patients because of a lack of prior evidence that such reactions occur, this testing was done in the initial series of eases to be certain that, such reactivity was not present. Prick tests were done by application of the xpyru- priate undiluted RCM to the skin, followed by breaking the skin with a sterile needle.5 A simultaneous control site was tested with 0.15 M phosphate-buffered SaCl, pH 7.35.
Graded dose testing. Jn the first 19 patients with a history of an IGR. who were evaluated and who were judged to require RCSI intravenously, a very cautious graded administration pro- gram was used. This is tabulated in Table I. This graded dose testing was done with all precau- tions necessary to reverse an TGRshould one have occurred during the proeedare.r When the first 19 studies were completed with no occurrence of significant reactions, this procedure wax discontinued and the currently used program, as described in Table VIII, was instituted.
For the first 3 patients requiring cholecystography, oral RCM was given under direct observation beginning with one eighth of the recommended dose. If no reaction occurred within 30 min, the remainder of the indicated dose was administered.
Antihistnmine pretreatment. dll patients with a history of an IGR who subsequently re- ceived RCM were treated with diphenhydramine hydrochloride prior to subsequent studies. The usual dose administered was 50 mg either intravenously immediately before or orally .l hr prior to the procedure.
RESULTS
On the basis of our evaluation and whether or not the patient received RCN, the 95 patients can be divided into three groups. Group I consisted of 42 patients (44.2%) who had a definite previous IGR and for wham the radiographic study
VOLUME 55 NUMBER 5
Administration of radiographic contrast media 361
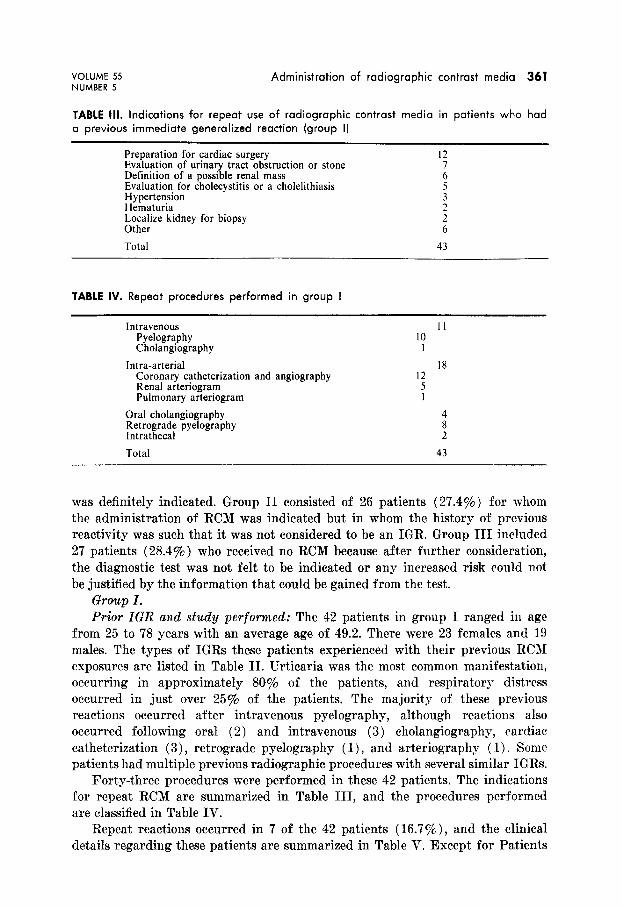
TABLE III. Indications for repeat use of radiographic contrast media in patients who had
a previous immediate generalized reaction (group I]
Preparation for cardiac surgery Evaluation of urinary tract obstruction or stone Definition of a possible renal mass Evaluation for cholecystitis or a cholelithiasis Hypertension Hematuria Localize kidney for biopsy Other
Total
I2
i
i
: 6
43
TABLE IV. Repeat procedures performed in group I
Intravenous Pyelography Cholangiography
Intra-arterial Coronary catheterization and angiography Renal arteriogram Pulmonary arteriogram
was definitely indicated. Group II consisted of 26 patients (27.4%) for whom the administration of RCM was indicated but in whom the history of previous reactivity was such that it was not considered to be an IGR. Group III included 27 patients (28.4%) who received no RCM because after further consideration, the diagnostic test was not felt to be indicated or any increased risk could not be justified by the information that could be gained from the test.
Grozcp I. Prior IGR and study performed: The 42 patients in group I ranged in age
from 25 to 78 years with an average age of 49.2. There mere 23 females and 19 males. The types of IGRs these patients experienced with their previous RCJI exposures arc listed in Table II. Erticaria was the most common manifestation, occurring in approximately 80% of the patients, and respiratory distress occurred in just over 25% of the patients. The majority of these previous reactions occurred after intravenous pyelography, although reactions also occurred following oral (2) and intravenous (3) cholangiography, cardiac catheterization (3)) retrograde pyelography ( 1) , and arteriography ( 1). Some patients had multiple previous radiographic procedures with several similar IGRs.
Forty-three procedures were performed in these 42 patients. The indications for repeat RCN arc summarized in Table III, and the procedures performed are classified in Table IV.
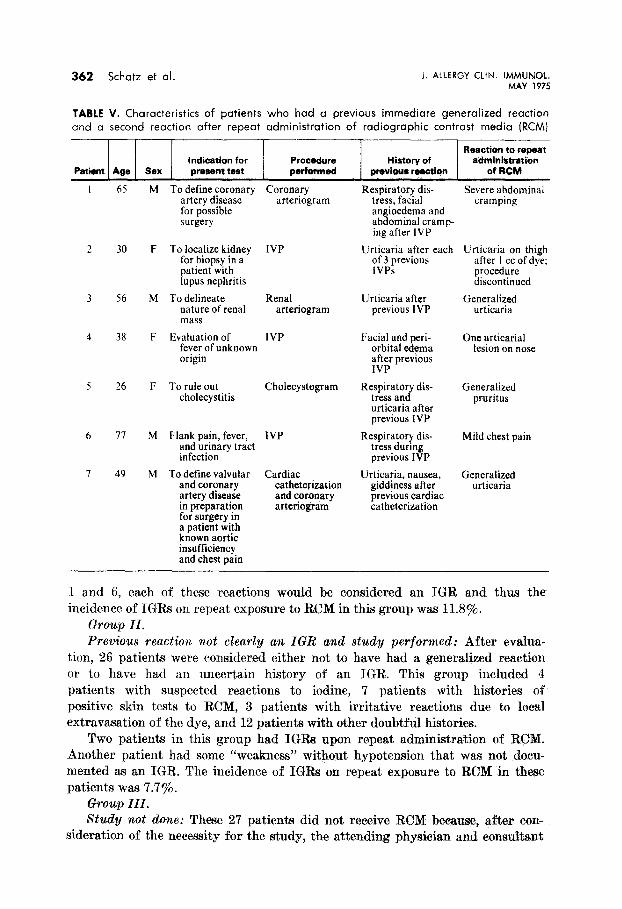
Repeat reactions occurred in 7 of the 42 patients (16.7%)) and the clinical details regarding these patients are summarized in Table V. Except for Patients
362 Schatz et al. J. ALLERGY CLIN. IMMUNOL. MAY 1975
TABLE V. Characteristics of patients who had a previous immediate generalized reaction
and a second reaction after repeat administration of radiographic contrast media (RCMJ
Reaction to repeat Indication for Procedure History of administration
Patient Age SBX present test Pa*msd previaue reaction of RCM
65
30
56
38
26
77
49
M To define coronary artery disease for possible surgery
F To localize kidney for biopsy in a patient with lupus nephritis
M To delineate nature of renal mass
F Evaluation of fever of unknown origin
F To rule out cholecystitis
M Flank pain, fever, and urinary tract infection
M To define valvular and coronary artery disease in preparation for surgery in a patient with known aortic insufficiency and chest pain
Coronary arteriogram
IVP
Renal Urticaria after Generalized arteriogram previous IVP urticaria
IVP Facial and peri- orbital edema after previous IVP
One urticarial tesion on nose
Cholecystogram
IVP
Cardiac catheterization and coronary arteriogram
Respiratory dis- tress, facial angioedema and abdominal cramp- ing after IVP
Urticaria after each of 3 previous lVPs
Respiratory dis- tress and urticaria after previous IVP
Respiratory dis- tress during previous IVP
Urticaria, nausea, giddiness after previous cardiac catheterization
Severe abdominal cramping
Urticaria on thigh after I cc of dye: procedure discontinued
Generalized pruritus
Mild chest pain
Generalized urticaria
1 and 6, each of these reactions would be considered an IGR and thus the incidence of IGRs on repeat exposure to RCM in this group was 11.8%.
Chup II. Yrevious react&m mt clearly an IGR a;nd study pwformed: After evalua-
tion, 26 patients were considered either not to have had a generalized reaction or to have had an uncertain history of an IGR. This group included 4 patients with suspected reactions to iodine, 7 patients with histories of positive skin tests to RCM, 3 patients with irritative reactions due to local extravasation of the dye, and 12 patients with other doubtful histories.
Two patients in this group had IGRs upon repeat administration of RCM. Another patient had some “weakness” without hypotension that was not docu- mented as an IGR. The incidence of ICI% on repeat exposure to RCM in these patients ~88 7.7%.
Group III. study not 0%~: These 2’7 patients did not receive RCM because, after cart-
sideration of the necessity for the study, the attending physician and consu%a~~t
VOLUME 55 NUMBER 5
Administration of radiographic contrast media 363
did not believe that the diagnostic test would justify the unknown risk associated with readministration of RCM. Four potential kidney donors warranted special consideration. abased on the experience to date, it was felt that the unpredictable additional risk to these patients was not justified, since the diagnostic test and possible attendant risk was not for the direct benefit of the patient.
DISCUSSION
Since the early 1920’s when contrast medium was introduced for the visualization of the urinary tract, adverse reactions have been known to occur following its administration. In a review of 10,000 consecutive intravenous urograms, Coleman, Ochsner, and Watson6 reported an overall incidence of 8:53y4 systemic reactions. Of these patients, 1.68% had “allergic-like” reactions that included shock, asthma, nasal congestion, or urticaria. Witten, Hirsch, and Hartman? reported an incidence of 6.8% side effects with 1.72% “acute reac- tions.” Pendergrass and associate@ estimated that there was an occurrence rate of 8.6 deaths per million intravenous pyelograms, or approximately one death in every 116,000. A recent survey3 reveals an incidence of one death in 50,000 studies.
Because a large number of tests involving RCM are performed and the incidence of severe adverse reactions is quite small, most attempts at prevention of “allergic” reactions following RCM administration have been related to identification and special treatment of the high-risk patient. There have been several techniques employed in an attempt to identify such patients. Because the reactions resemble allergic reactions, a variety of sensitivity tests have been recommended, the most common of which involves intracutaneous skin testing. It has been demonstrated, however, that the incidence of positive intracutaneous tests to RCM did not differ significantly between patients who subsequently had a reaction and those who did not. I” Furthermore, it is now well known that many reactions have been reported in patients who had negative preliminary sensitivity tests of any kind. These tests have thus not been able to adequately identify the high-risk patient.
A second approach has been the use of pretesting with small intravenous doses of RCM prior to the complete procedure. Both the incidence of serious reactions after the pretest and the incidence of significant reactions following a negative pretest have led several investigators recently to suggest abandonment of this procedure.7’ 9 One should note that the usual test dose is 1 cc of undiluted RCM” and contrast this to our graded dose program, which begins with 0.1 cc of a 1:lOO dilution or l/1,000 of this 1 cc standard test dose, which not infre- quently causes a reaction.
A third potential means of identifying the high-risk patient has been obtain- ing a personal history of allergy of any kind. There is conflicting evidence regarding whether a patient with a history of atopy in general has an increased risk of a reaction to the administration of RCM.ll Because these studies are equivocal and because of the lack of evidence that IGRs after contrast media are IgE-mediated, at this point in time we do not consider the atopic population,
364 Schatz et al. J. ALLERGY CLIN. IMMUNOL. MAY 1975
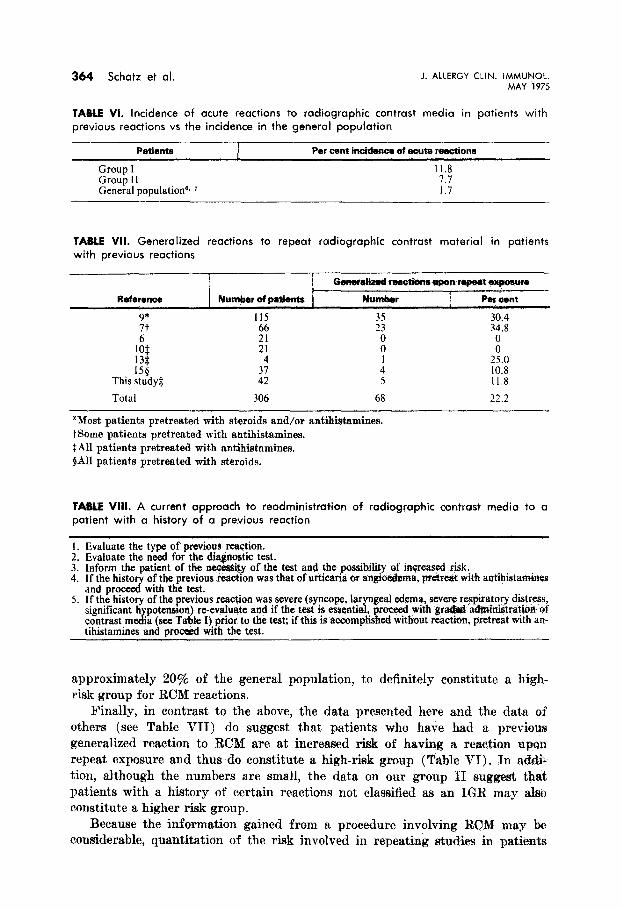
TABLE VI. Incidence of acute reactions to radiographic contrast media in patients with
previous reactions vs the incidence in the general population
Patients Par cent inoi&nce of aout Mtlctions
Group I 11.8 Group II 7.7 General populationa, ’ 1.7
TABLE VII. Generalized reactions to repeat radiographic contrast material in patients with previous reactions
Reference
9+ 7t
Numw of patients
115 ;:
21 4
Oanar*d rsm&tum upon rapaetexpowre
Nwnbsr I Per a4nt
30.4 :: 34.8
: : 1 25.0
158 This study$ ::
4 10.8 5 11.8
Total 306 68 22.2
“Xost patients pretreated with steroids and/or antihistamines. t Some patients pretreated with antihistamines. L%ll patients pretreated with antihistamines. $A11 patients pretreated with steroids.
TA6iE VIII. A current approach to readministration of radiographic contrast media to a patient with a history of a previous reaction
I. Evaluate the type of previous rea@ion. 2. Evaluate the need for the diagnostic test. 3. Inform the patient of the n$ces&y of the test and tfK possibility of inGreased risk. 4. I f the hi&or of the previous rca&on was that of utiicana or an&&ema, pretreat with antihistamines
and prdwith the test. 5. If the history of the previous reaction was severe (syncope, laryngeal edema, severe reqira!qry distress,
significant h contrast m fdi
potenston) re-evsluate and if the test is essential a (see Table I) prior to the test; if this is
,gwea$ accomp1
w&h gr+& ruknmtstr$io& ef ed without reaction. pretreat with an-
tihistamines and proceed with the test.
approximately 20% of the general population, to definitely constitute a high- risk group for RCM reactions.
Finally, in contrast to the above, the data presented here and the data of others (see Table VII) do suggest that patients who have had a previous generalized reaction to RCM are at increased risk of having a reaction upon repeat exposure and thus do constitute a high-risk group (Table VI). In addi- tion, although the numbers are small, the data on our group II suggest that patients with a history of certain reactions not classified as an IGR may also constitute a higher risk group.
Because the information gained from a procedure involving RCM may be considerable, quantitation of the risk involved in repeating studies in patielrts
VOLUME 55 NUMBER 5
Administration of radiographic contrast media 365
with a history of a generalized reaction would be important. Table VII shows the results in 306 patients in this study and in the literature who had repeat RCM after a previous generalized reaction. There were no fatalities in these patients and none of the repeat acute reactions was any worse than the original one. Ansell,’ however, commented on 2 eases with progressively more severe reactions.
An evaluation of the effect of pretreatment with antihistamines or steroids in these high-risk patients is difficult. Although pretreatment with antihistamines has been reported to decrease the incidence of “allergic reactions” to RCM in genera&l”* I4 the use of antihistamine pretreatment in Table VI varied from study to study and within a given study. Regarding steroids, the numbers in Table VI are too small and variable to determine definitely whether steroid pre- treatment had a significant protective effect. However, a comparison between our study and that of Zweiman and Hildreth’” suggests that there is no definite ad- vantage to steroid pretreatment.
This study and our evaluation of the experience of others have led to our current approach to the readministration of RCM to a patient with a history of a previous reaction (Table VIII). Although the safest approach would be to avoid repeat exposure to RCM, this may not always bc in the patient’s best interest. The risk of repeat reaction does appear to bc increasrd; it does not, however, appear to be prohibitive when a dcfinitc indication for repcat study exists. This is not intended to imply that such procedures should be done routinely, and this increased risk should be carefully discussed with the patient. In addition, if the procedure is to be done, we would recom- mend pretreatment with antihistamines. It is rceognixctl that an antihistamine is not a certain method of preventing an IGR; however, it is a benign medication and may modify a potcntiallp scvcrc reaction to a milder one. Although the graded dosing procedure may be unnecessary for most patients with a history of a mild to moderate reaction, it would appear to bc prudent in a patient with a history of a more severe reaction for whom the study appears essential.
REFERENCES
1 Weiszer, I.: Allergic emergencies, in Patterson, R., editor : Allergic diseases : Diagnosis and management, Philadelphia, 1972, J. B. Lippincott Co., 1’. 327.
2 Rockoff, H. D., Brasch, R. C., Kuhn, C., and Chraplyvy, M.: Contrast, media :IS histamine liberators. 1. Mast cell histamine release in vitro by sodium salts of contrast media, Invest. Radiol. 5: 503, 1970.
3 Bras&, R. C., Rockoff, S. D., Kuhn, C., and Chraplyvy, M.: Contrast media as histamine liberators. Il. Histamino release into venous plasma during intraveuous urography in man, Invest. Radiol. 5: 510, 1970.
4 Lasser, E. C., Walters, A., Reuter, 8. R., and Lang, .T. : Histamine relwse by contrast media, Radiology 100: 683, 1971.
5 Booth, B. J.: Diagnosis of immediate hypcrscnsitivity, in Patterson, R., editor: Allergic diseases: Diagnosis and management, Philadelphia, 1972, J. B. Lippincott Co., 1’. 63.
6 Coleman, W. P., Ochsner, S. F., and Watson, B. E.: Allergic reactions in 10,060 consceutive intravenous urographies, Southern Mrd. J. 57: 1401, 196-1.
7 Wittcn, D. M., Hirsch, F. D., and Hartman, 0. \V.: Acute reac+ions to urographic contrast medium: Incidence, clinical chnrarteristics, and relationship to history of hyper- sensitivity states, Am. J. Rocntgenol. 119: 832, 1973.
366 Schatz et al. J. ALLERGY CLIN. IMMLJNOL. MAY 1975
8 Pendergrass, II. P., Tondreau, R. L., Pendergrass, E. I’., Ritehie, D. J., Hildroth, E. A., and Askovitz, 5. I.: Reactions associated with intravenous urography : Histological and statistical review, Radiology 71: 1, 1958.
9 Fischer, H. W., and Doust, V. L.: An evaluation of pretesting in t,lro problem of serious and fatal reactions to excretory urography, Radiology 108: 497, 1972.
10 Mathov, E., Salmun, N., Grinstein, XT., Ferrari, A., Greiding, I+ Kaliman, ,M., Hzlazer, M., AXontangero, C., and Lemke, A.: Prevention of allergic shock produced by TV iodide in radiology, Prensa Med. Argent. 56: 1459, 1969.
11 DeSwarte, R. D.: Drug allergy, ia Patterson, R., editor: Allergic Diseases: Diagnosis and management, Philadelphia, 1972, J. R. Lippincott Co., p, 476.
12 Ansell, G. : Adverse reaction to contrast agents, Invest. Radiol. 8: 374, 1970. 13 Sanger, i\d. D.: Further observations with antihistamines in reducing reactions in
intravenous pyelography, Ann. Allergy 17: 762, 1959. 14 Gates, D. F., and Cecoarelli, F. E.: Renadyl and the IVP reaction, .J. Ural. 108: 627, 1972. 15 Zweiman, B., and Hildreth, E. A. ; An approach to contrast studies in reactive humans,