Charcot‐Marie‐Tooth The Role of Podiatric Medicine and Surgery in Treatment of the Charcot‐Marie‐Tooth Patient September 14, 2011 San Francisco, CA Hal Ornstein, DPM, FASPS Howell, New Jersey Reviewed and accepted by the 2011-2012 Neuromuscular Committee of the American Association of Neuromuscular & Electrodiagnostic Medicine Certified for CME credit 10/2011 – 05/2020 Reviewed 10/2017 by the 2017-2018 Neuromuscular Committee
Transcript
Charcot‐Marie‐Tooth
The Role of Podiatric Medicine and Surgery in Treatment of theCharcot‐Marie‐Tooth Patient
September 14, 2011San Francisco, CA
Hal Ornstein, DPM, FASPSHowell, New Jersey
Reviewed and accepted by the 2011-2012 Neuromuscular Committee ofthe American Association of Neuromuscular & Electrodiagnostic Medicine Certified for
CME credit 10/2011 – 05/2020Reviewed 10/2017 by the 2017-2018 Neuromuscular Committee
Dr. C. Everett Koop, former US Surgeon General, once said “The best prescription is knowledge.”
What is Podiatric Medicine?
• Medical and surgical care and treatment of the foot and ankle
• Sub‐specialties include sports medicine, wound care, podopediatrics, podogeriatrics, reconstructive foot and ankle surgery, trauma, and the diabetic foot
Education of a Podiatrist
• Four year undergraduate degree required• Four years of podiatric medical school
(nine schools in the US)*** two‐part National Board while in podiatric medical school and another part upon completion of the podiatric medical school program.
• Two to four year residency (most are three years)
• Additional fellowship training
What is the licensing and certification process for D.P.M.s?
Two Major Certifying Boards in Podiatry
The American Board of Podiatric Orthopedicsand Primary Podiatric Medicine
The American Board of Podiatric Surgery
What is a D.P.M. (Doctor of Podiatric Medicine)?
Comprehensive health practitioner of the lower extremity that specializes
in the diagnosis and treatment of conditions effecting the foot, ankle and lower leg in all age groups
• Conducts examinations• Prescribes medications• Performs surgery• Academic appointments at university hospitals• Conducts translational research • Approximately 15,000 podiatrists in the US
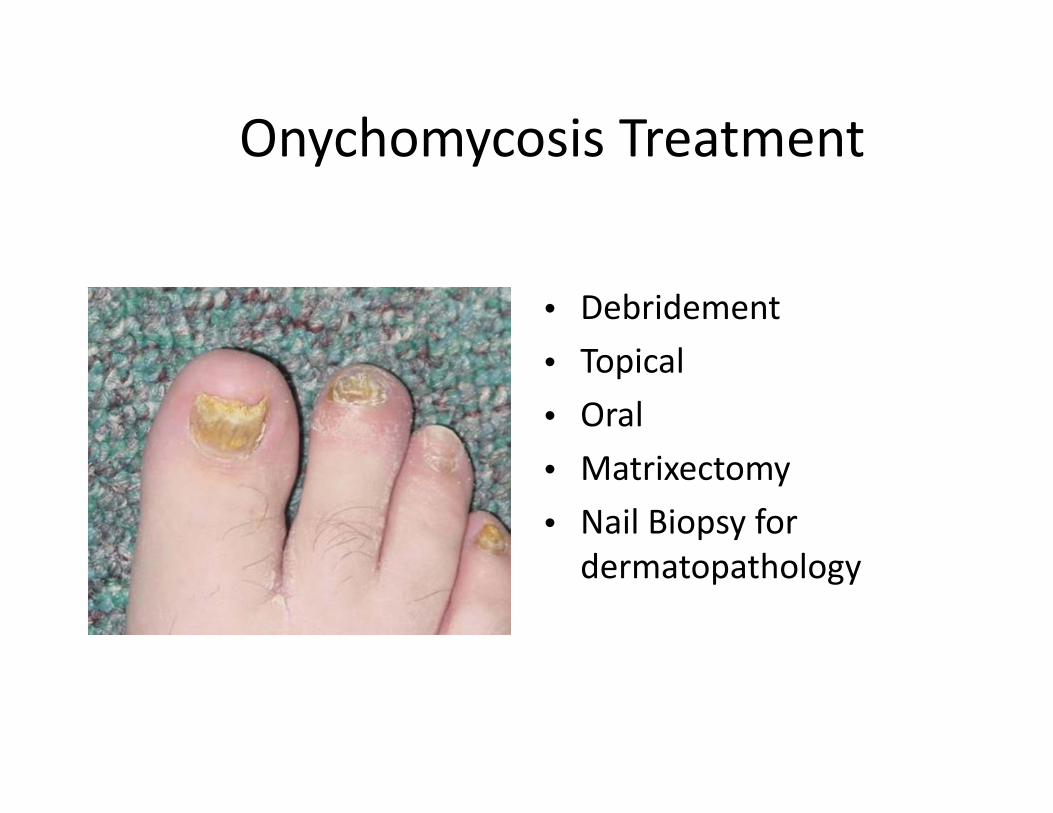
• Debridement• Topical• Oral• Matrixectomy• Nail Biopsy for dermatopathology
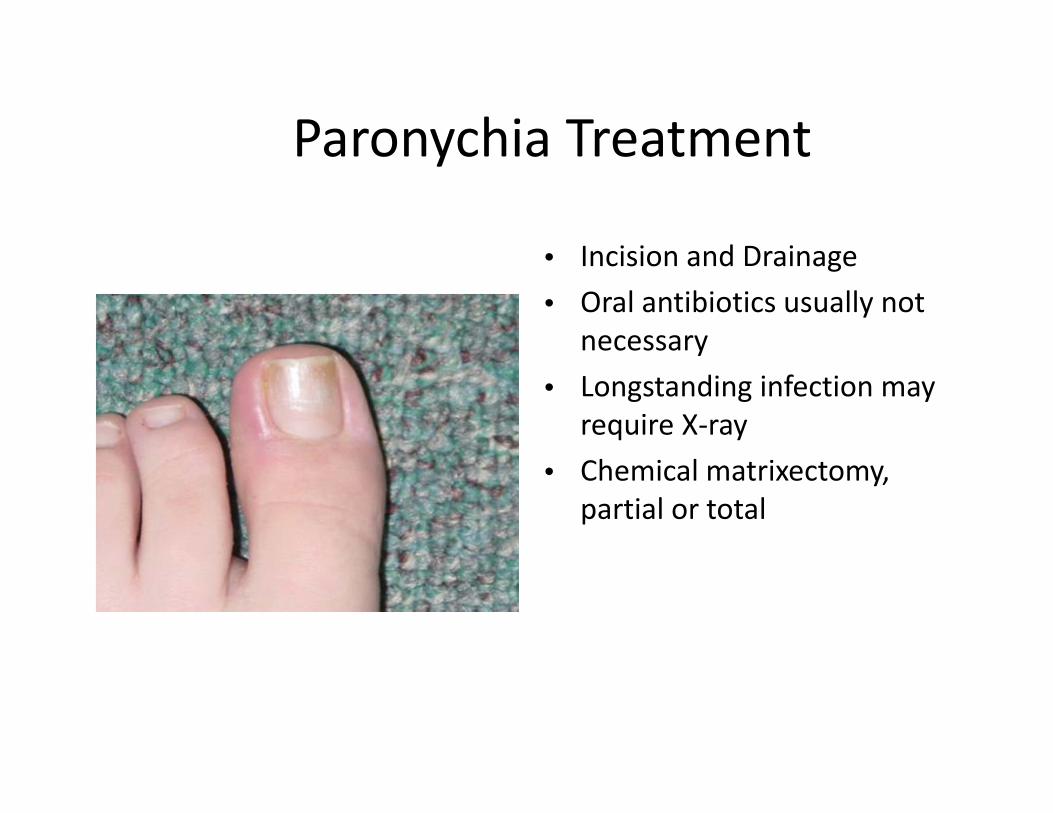
Paronychia
• Erythema and edema of the ungual labia
• Wide or incurvated nail plate
• May drain serous to purulent exudate
• Hallux most effected
Paronychia Treatment
• Incision and Drainage• Oral antibiotics usually not
necessary• Longstanding infection may
require X‐ray• Chemical matrixectomy,
partial or total
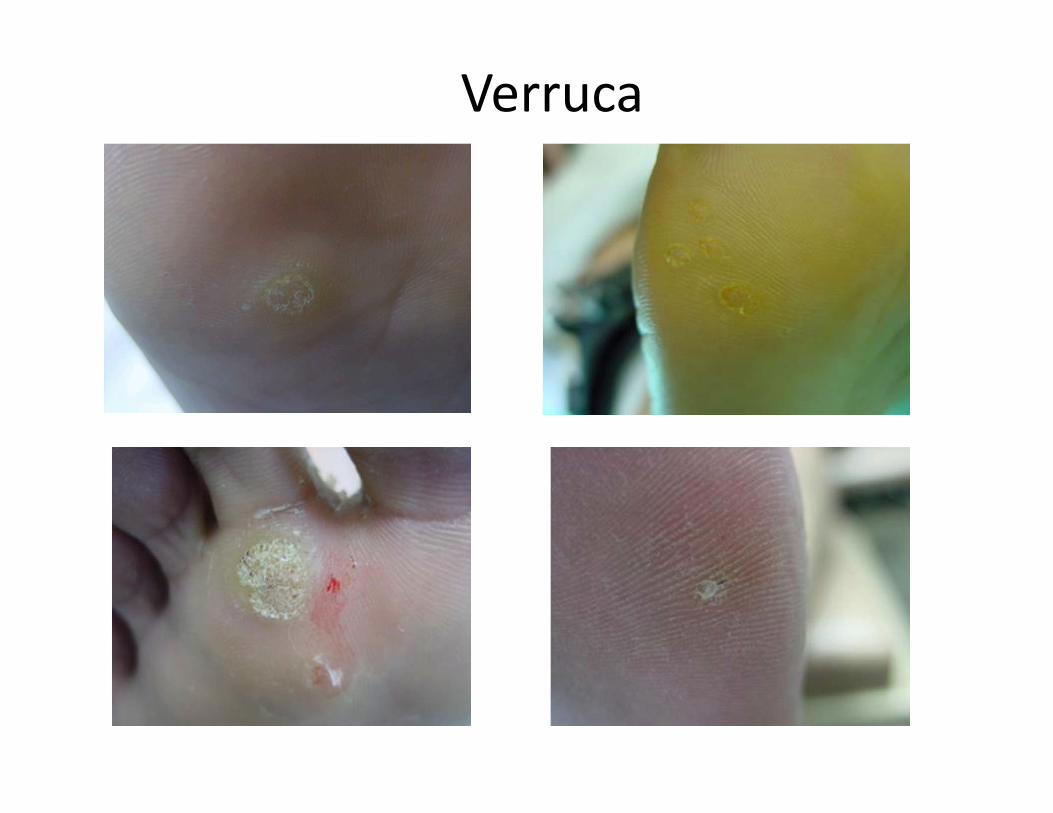
Verruca
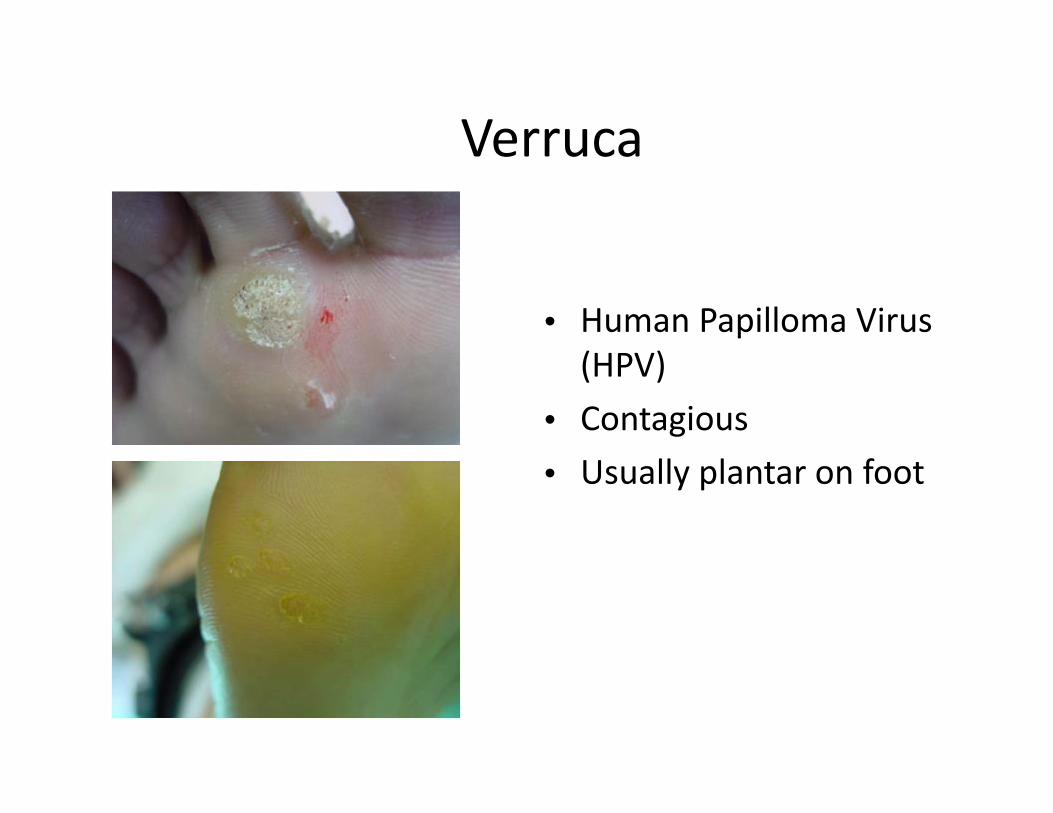
Verruca
• Human Papilloma Virus (HPV)
• Contagious• Usually plantar on foot
Verruca Treatment
• Debridement is diagnostic and therapeutic• Chemocautery• Various topical treatments available• Oral Cimetidine for pediatric usage (30‐40Mg/Kg in 3 divided doses)
• Curretage
Plantar Fasciitis• Inflammation and pain of
the plantar fascia, usually at its insertion at the plantar medial tubercle of the calcaneus
• Becomes chronic in 5‐10% of all patients
• Is not necessarily associated with a heel spur
• Over 90% resolve with conservative treatment
Plantar Fasciitis Symptoms
• Weight‐bearing pain on arising• Pain subsides, returns with activity• Footwear related to pain?
Plantar Fasciitis Treatment
• Stretching• RICE• Change shoes• OTC inserts
Plantar Fasciitis Treatment
• Nocturnal Anti‐contracture Devices
• Orthotics• NSAIDS• Cortisone shot(s)• Rarely surgery
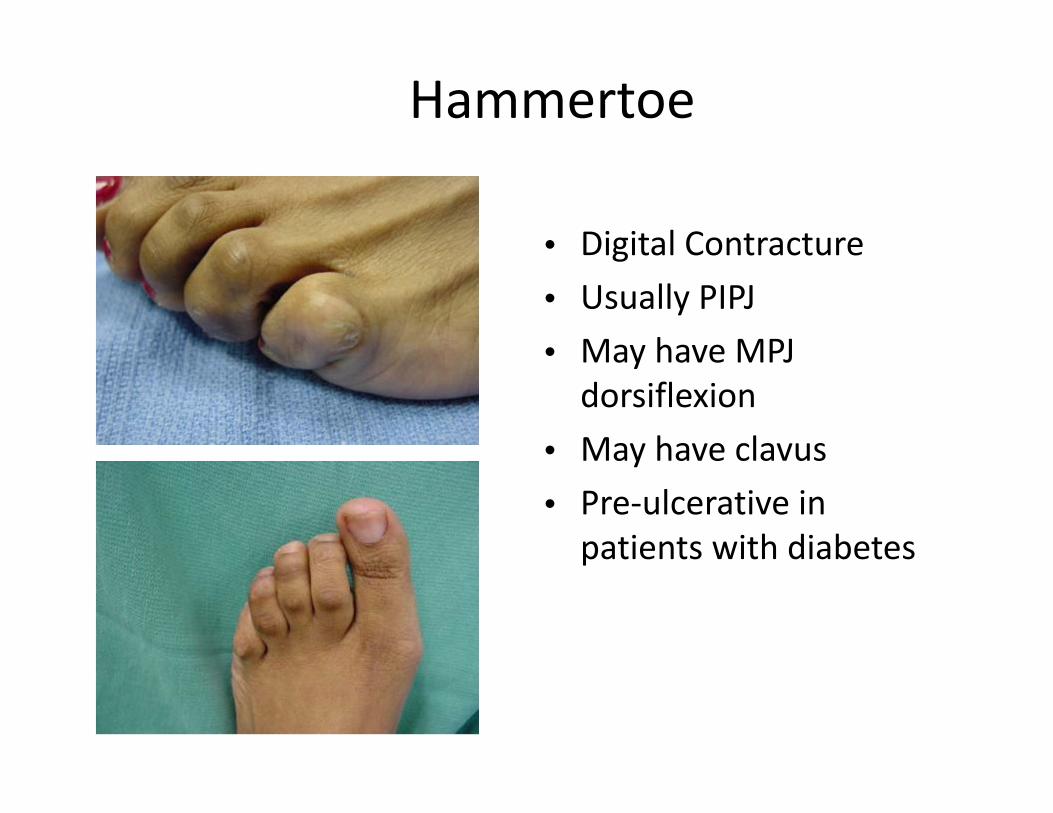
Hammertoe
• Digital Contracture• Usually PIPJ• May have MPJ dorsiflexion
• May have clavus• Pre‐ulcerative in patients with diabetes
Hammertoe Treatment
• Debridement• Padding• Shoe gear change• Surgery as a last option
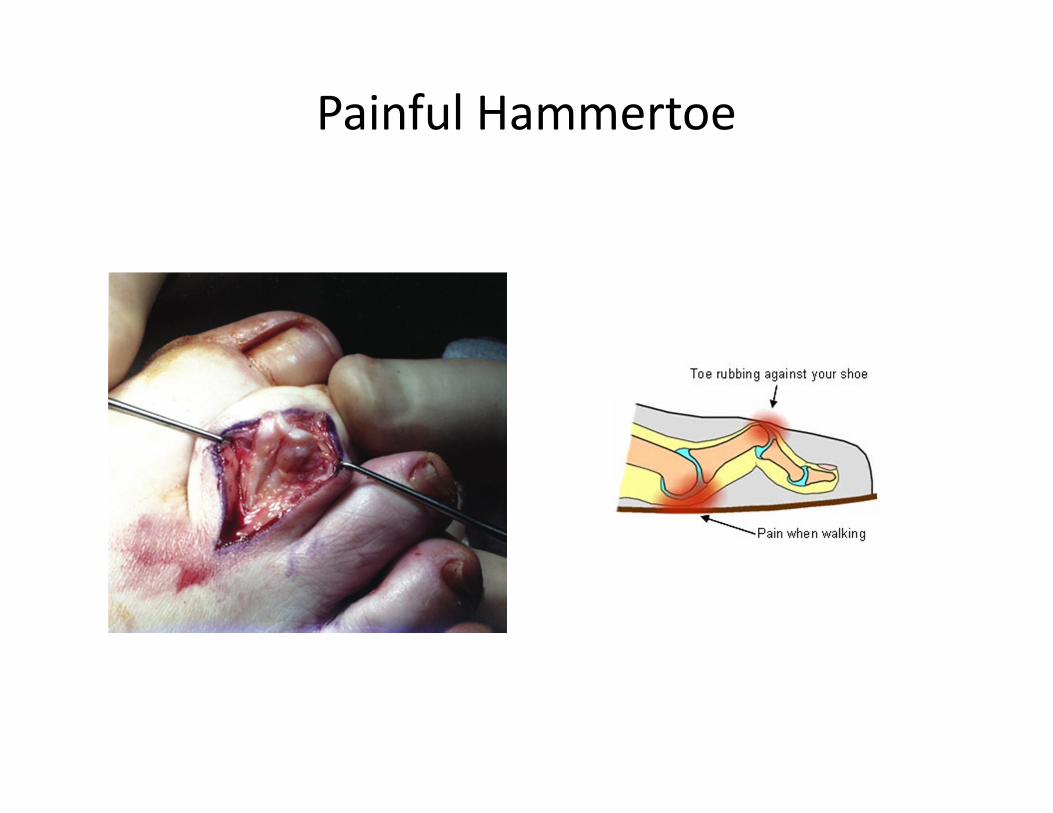
Painful Hammertoe
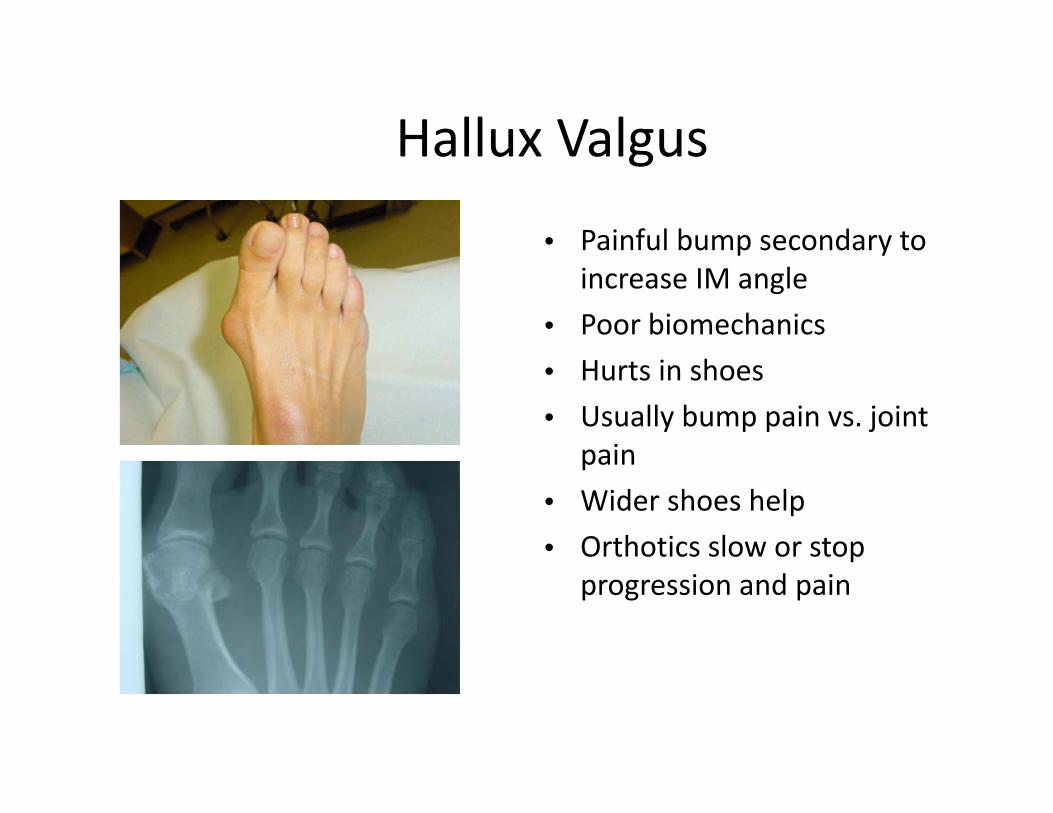
Hallux Valgus
• Painful bump secondary to increase IM angle
• Poor biomechanics• Hurts in shoes• Usually bump pain vs. joint
pain• Wider shoes help• Orthotics slow or stop
progression and pain
Hallux Abducto Valgus (Bunion Deformity)
Osteoarthritis
• Usually at first MPJ• Hallux limitus/rigidus• Poor biomechanics• Painful to walk
Osteoarthritis Treatment
• Cortisone injection• Physical therapy• NSAIDS• Orthotics• Surgery
Ankle ‐ Foot Orthosis
• Articulated hinge device• Used when functional orthotic fails or will fail
• For active patient that can tolerate motion
• Excellent for sports
Ankle – Foot Orthosis
• Gauntlet style for total control
• For patients that cannot tolerate motion
• Good for severe DJD and Charcot foot
Ankle Sprains and Fractures• Tear or stretching of the
ligaments of the ankle. Usually the ligaments on the outside of the ankle are involved.
• Caused by and twisting injury of the foot / ankle .
• Instability of the ankle can develop due to the ligament injury.
• Most often treated conservatively. Surgical repair can be performed to treat chronic ankle sprains.
Ankle Sprain Treatment
• Immobilize early • Consider Non‐Weight bearing
• RICE• NSAIDS
Ankle Sprain Rehabilitation
• CAM walker to Stirrup• Stirrup to gauntlet• Physical therapy
Morton’s Neuroma
• Painful swelling of the interdigital nerve
• Most commonly seen in third web space
• Patients can feel numbness of adjacent digits and plantar pain
• Bony prominence is usually involved (hammertoe, bunion, plantarflexed metatarsal, bone spur)
• Often start as a blister, corn or callous
Diabetic ulcer treatment• Always obtain serial X‐rays to rule
out osteomyelitis• Debride the wound to granular
bed• Remove hyperkeratosis• Gently probe wound for deep
sinus• Dress initially with Silvadene
cream• Consider other wound products• Consider offloading
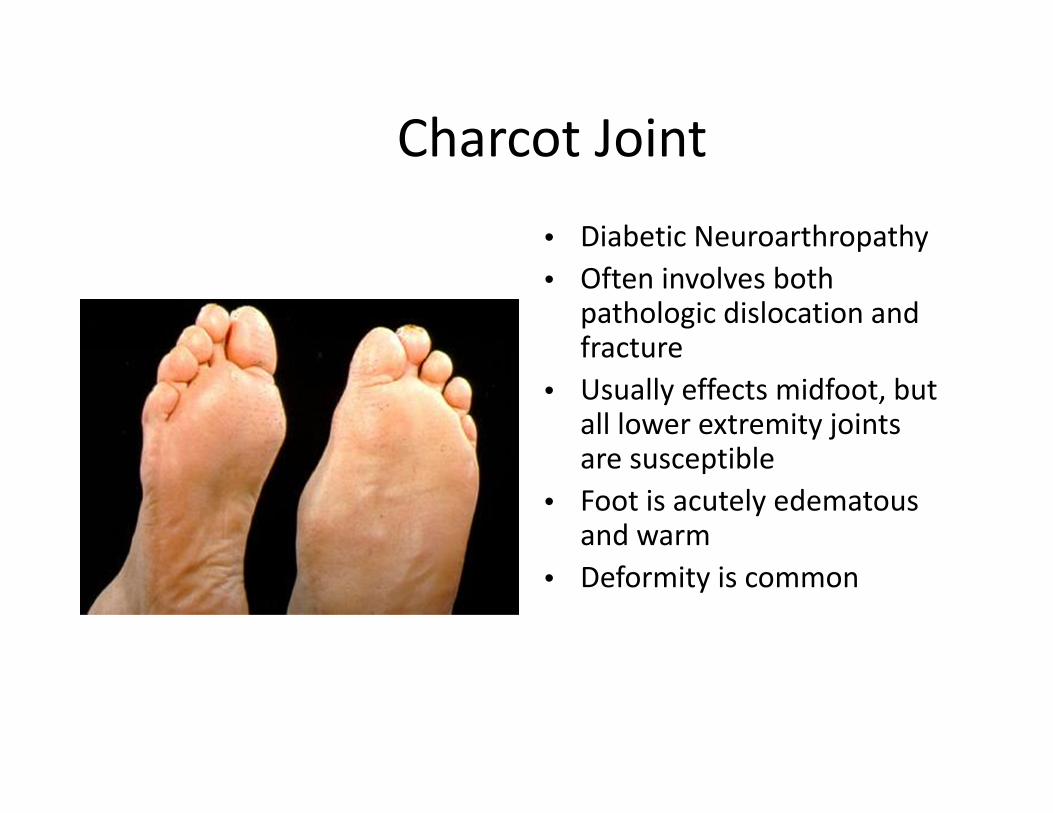
Charcot Joint• Diabetic Neuroarthropathy• Often involves both
pathologic dislocation and fracture
• Usually effects midfoot, but all lower extremity joints are susceptible
• Foot is acutely edematous and warm
• Deformity is common
Charcot Joint Treatment
• Non‐weight bearing for 12 weeks
• Patient education is critical to outcome
• Serial X‐rays to document deformity
• Molded shoe often needed after coalescence
• Surgical Treatment
Therapeutic Shoes
• Newly diagnosed + 33% 1990’s
• Amputations + 28% 2000 ‐2001
• Medicare has stated that 50% of amputations were preventable
Therapeutic Shoes
• Focal pressure keratosis with accompanying risk factors are the major cause of ulcer.
• Patients who have regular, frequent foot clinic visits that include risk evaluation, debridement of lesions, prescription of appropriate shoes and patient education are less likely to ulcerate. 1
• 1 Sage RA, Webster JK, Fisher SG: Outpatient Care and Morbidity Reduction in Diabetic Foot Ulcers Associated with Chronic Pressure Callus. JAPMA 91:275, 2001.
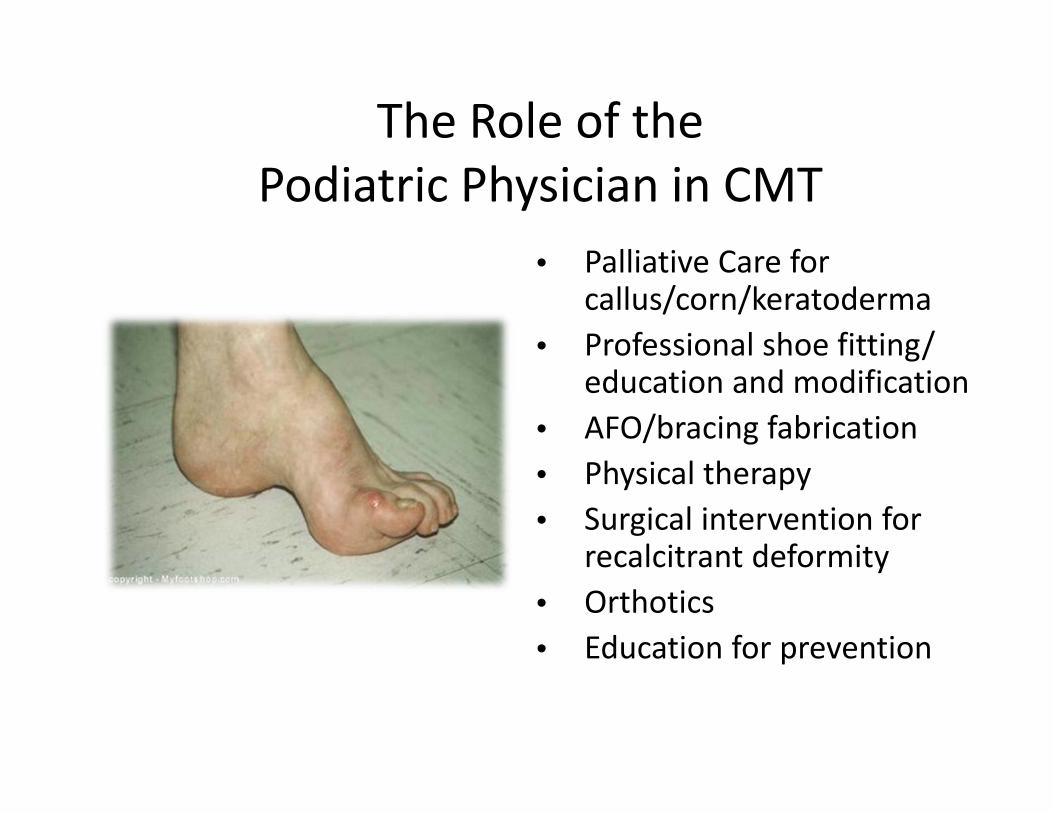
The Role of the Podiatric Physician in CMT
• Palliative Care for callus/corn/keratoderma
• Professional shoe fitting/ education and modification
• AFO/bracing fabrication• Physical therapy• Surgical intervention for
recalcitrant deformity• Orthotics• Education for prevention
References1. Berciano J, Gallardo E, Garcıa A, Pelayo‐Negro AL, Infante G, Combarros O. New insights into the pathophysiology of pes cavus in Charcot–Marie–
Tooth disease type 1A duplication. J Neurol 20112. Brewerton DA, Sandifer PH, Sweetnam DR. Br Med J. 1963 Sep 14;2(5358):659‐613. Burns J, Ouvrier RA, Yiu EM, et al. Effect of ascorbic acid in patients with Charcot‐Marie‐Tooth disease type 1A: a multicentre, randomized, double
blind, placebo‐controlled trial. Lancet Neurol 2009; 8: 1103. 4. Burns J, Ryan MM, Ouvrier RA. Evolution of Foot and Ankle Manifestations in Children with CMT1A. Muscle Nerve 39: 158 –166, 20095. Burns J, Scheinberg A, Ryan MM, Ouvrier RA. Randomized Trial of Botulinum Toxin to Prevent Pes Cavus Progression in Pediatric Charcot‐Marie‐
Tooth Type 1A. Muscle and Nerve. 262 ‐7, 20106. Chetlin R, Gutmann L, Tarnopolsky M, Ullrich I, Yeater, R. Resistance Training Effectiveness in Patients with Charcot‐Marie –Tooth Disease:
Recommendations for Exercise Prescription; Arch Phys Med Rehabil 2004; 85: 1217‐12227. Croban et al. CMT Facts IV. Treatment of Familial Neuropathies. Vol 4. 1998.8. Del Porto LA, Nicholson GA, Ketheswaren P. Correlation between muscle atrophy on MRI and manual strength testing in hereditary neuropathies.
Journal of Clinical Neuroscience 17 874–878, 20109. Duval A, Kalempokas K, Penicaud A, Guiochon A, Mantel E, Bachmeyer C. Neuropathic leg ulcer indicating late adult‐onset of Charcot‐Marie‐Tooth
disease. J Am Acad Dermatol (64); 1215‐1216, 2011. 10. Lupski et al. Finding CMT gene ends a quest and begins a new era. Science Med. March 2010.11. Guyton, G. Orthopaedic Aspects of Charcot‐Marie‐Tooth Disease. Foot and Ankle International. Vol 27. 2006; 1003‐10.12. Hewitt SM, Tagoe M. Surgical Management of Pes Cavus Deformity with an Underlying Neurological Disorder: A Case Presentation. JFAS (50) 235–
240, 2011 13. McGlamry’s Comprehensive Textbook of Foot and Ankle Surgery. Third Ed. Section 5: Chapter 34 Charcot‐Marie‐ Tooth Disease. 2001; 1071‐108914. Menotti F, Felici F, Damiani A, Mangiola F, Vannicelli R, Macaluso A. Charcot‐Marie Tooth 1A patients with a higher energy cost of walking than
healthy individuals; Neuromuscular Disorders 2011; 21:52‐57315. Micaleff J, Attarian S, Dubourg O, et al. Effect of ascorbic acid in patients with Charcot Marie Tooth disease type 1A: a multicentre, randomized,
double blind, placebo‐controlled trial. Lancet Neurol 2009; 8:110316. Mondelli M. Some considerations on atypical cases of Charcot‐Marie‐Tooth disease and use of genetic testing in idiopathic polyneuropathies.
Clinical Neurology and Neurosurgery 112 (2010) 745–74617. Oatis Carol. Charcot‐Marie Tooth Disorders: Pathophysiology, Molecular Genetics and Therapy. John Wiley & Sons, Inc. 199018. Ramcharitar SI: Lower Extremity Manifestations of Neuromuscular Diseases. Clinics of Podiatric Medicine & Surgery, 15: 722‐724, 1998.19. Reilly M, Murphy S, Laura M. Charcot‐Marie‐Tooth Disease. Journal of the Peripheral Nervous System 2011; 16:1‐1420. Sreda MW, Meyer zu Horste G, Suter U, et al. Therapeutic administration of progesterone antagonist in a model of Charcot‐Marie‐Tooth disease
(CMT‐1A). Nat Med 2003; 9:153321. Van der Linden MH, Van der Linden SC, A, Hendricks HT, Van Engelen BGM, Geurts ACH. Postural instability in Charcot‐Marie‐Tooth type 1A
patients is strongly associated with reducedsomatosensation. Gait & Posture 31 (2010) 483–48822. Walsh B, Fontera W. Brace modification improves aerobic performance in Charcot‐Marie Tooth disease: A single‐subject design. AM J Phys Med
Rehabil 2001;80:578‐582. 23. Ward et al. “Long‐Term Results of Reconstruction for Treatment of a Flexible Cavovarus Foot in CMT disease.” The Journal of Bone and Joint
Surgery. 90:2631‐42. 2008.24. Westmore et al. “Long‐Term Results of Triple Arthrodesis in CMT disease.” The Journal of Bone and Joint Surgery. 71‐A No 3. 1989.
Thank You! Life Just Gets Better
Hal Ornstein, DPM, FACFASAffiliated Foot and Ankle Center, LLP