The Clinical Application of the Biopsychosocial Model
BY GEORGE L. ENGEL, M.D.
Howphysicians approach patients and the problems
they present is much influenced by the conceptual
models around which their knowledge is organized. In
this paper the implications ofthe biopsychosocial
modelfor the study and care ofa patient with an acute
myocardial infarction are presented and contrasted
with approaches used by adherents ofthe more
traditional biomedical model. A medical rather than
psychiatric patient was selected to emphasize the
unity of medicine and to help define the place of
psychiatrists in the education of physicians of the
future.
T he Vestermark award acknowledges contributionsto psychiatric education. For the most part
awardees have taken the occasion to discuss issuespertaining to psychiatric education. This paper will doso only indirectly. In it I intend to elaborate on thebiopsychosocial model by demonstrating its practicalapplicability to the understanding and care of a pa-tient. For this purpose I have deliberately selected amedical rather than a psychiatric patient, a man whoexperienced a myocardial infarction complicated bycardiac arrest. I do so to emphasize the unity of medi-cine and the uniqueness of physicianhood, for psychia-try is a medical discipline and psychiatrists are physi-
The Seymour Vestermark Memorial Lecture, presented at the132nd annual meeting of the American Psychiatric Association, Chi-cago, Ill., May 12-18, 1979. Received July 16, 1979; accepted July27, 1979.
From the Departments of Psychiatry and Medicine, University ofRochester School of Medicine and Dentistry.
Address reprint requests to Dr. Engel, Strong Memorial Hospital,300 Crittenden Blvd., Rochester, N.Y. 14642.
Supported in part by a grant from the Henry Kaiser Family Foun-dation. Dr. Engel is the recipient of a Career Research Award fromthe U.S. Public Health Service.
cians. The biopsychosocial model is a scientific modelconstructed to take into account the missing dimen-sions of the biomedical model. To the extent that itsucceeds it also serves to define the educational tasksof medicine and particularly the tasks and roles of psy-chiatrists in the education ofphysicians ofthe future.
How physicians approach patients and the problemsthey present is very much influenced by the concep-tual models in relationship to which their knowledgeand experience are organized. Commonly, however,physicians are largely unaware of the power such mod-els exert on their thinking and behavior. This is be-cause the dominant models are not necessarily madeexplicit. Rather, they become that part of the fabric ofeducation which is taken for granted, the culturalbackground against which they learn to become physi-cians. Their teachers, their mentors, the texts they
use, the practices they are encouraged to follow, andeven the medical institutions and administrative organ-izations in which they work, all reflect the prevailingconceptual models of the era.
The dominant model in medicine today is called the“biomedical” model. The biomedical model repre-sents the application to medicine of the classical fac-tor-analytic approach that has characterized Westernscience for many centuries. Elsewhere (1-3), I haveconsidered the limitations of that model and presentedan alternative model, the biopsychosocial model. Thenew model is based on a systems approach, a develop-ment in biology hardly more than 50 years old, the ori-gin and elaboration of which may be credited chiefly tothe biologists Paul Weiss and Ludwig von Bertalanify.
In this paper I will consider how the biopsychosocialmodel enables the physician to extend application ofthe scientific method to aspects of everyday practiceand patient care heretofore not deemed accessible to ascientific approach. As a result the goal of the Flexnerreform to educate a truly scientific physician will comecloser to reality (4, 5).
The most obvious fact of medicine is that it is a hu-
536 THE BIOPSYCHOSOCIAL MODEL Am J Ps)�chi#{224}tr/ 137:5, May 1%O
man discipline, one involving role- and task-definedactivities of two or more people. Such roles and tasksare defined in a complementary fashion. Roles arebased on the linking of the need of one party, the pa-tient, with an expected set of responses (services)from the other party, the physician. Broadly speaking,the need of the patient is to be relieved of “distress”rightly or wrongly attributed to “illness,” howeverconceptualized. The expectation of the patient is thatthe other party, the physician, has the professionalcompetence and motivation to provide such relief. Inpractical terms the doctor’s tasks are, first, to find outhow and what the patient is or has been feeling andexperiencing; then to formulate explanations (hypoth-eses) for the patient’s feelings and experiences (the“why” and the “what for”); to engage the patient’sparticipation in further clinical and laboratory studiesto test such hypotheses; and, finally, to elicit the pa-tient’s cooperation in activities aimed to alleviate dis-tress and/or correct underlying derangements that maybe contributing to distress or disability. The patient’stasks and responsibilities complement those of thephysician.
In a broad sense this characterization of the corn-plemeritary roles and tasks ofphysician and patient ap-plies to all healing and health care systems, whetherprimitive folk medicine or modern scientific medicine.The former is based largely on authority, tradition, andan appeal to magical formulae, while the latter relieson scientific knowledge and the scientific method asthe best means to achieve the goals of health and well-being. Both the successes and the deficiencies of thecurrent scientific approach, predicated as it is on thebiomedical model, are currently the subject of livelycontroversy. Protagonists of the biomedical modelclaim that its achievements more than justify the ex-pectation that in time all major problems will succumbto further refinements in biomedical research. Criticsargue that such dependence on “science” in effect isat the expense of the humanity of the patient. This is afruitless controversy which cannot be resolved be-cause it is predicated, by advocate and critic alike, ona flawed premise, that the biomedical model is an ade-quate scientific model for medical research and prac-tice (2, 3).
The crippling flaw of the model is that it does notinclude the patient and his attributes as a person, a
human being. Yet in the everyday work of the physi-cian the prime object of study is a person, and many ofthe data necessary for hypothesis development andtesting are gathered within the framework of an ongo-ing human relationship and appear in behavioral andpsychological forms, namely, how the patient behavesand what he reports about himself and his life. Thebiomedical model can make provision neither for theperson as a whole nor for data of a psychological orsocial nature, for the reductionism and mind-bodydualism on which the model is predicated requires that
these must first be reduced to physico�chemica1 termsbefore they can have meaning (2, 3). Hence, the veryessence of medical practice perforce remains “art”and beyond the reach of science (6).
THE BIOPSYCHOSOCIAL MODEL
Focusing on what the physician does in con-tradistinction to what the bench scientist does high-
lights the appropriateness, indeed the necessity, of asystems approach, as exemplified in the proposedbiopsychosocial model. While the bench scientist canwith relative impunity single out and isolate for se-
quential study components of an organized whole, thephysician does so at the risk of neglect of, if not injuryto, the object of study, the patient. Proponents of thebiomedical model often cite this impossibility of deal-ing with a patient as one would an experimental animalin the laboratory to support their argument that medi-cine cannot ever be truly scientific. But such a con-tention assumes that the factor-analytic approach ofreductionism alone qualifies as scientific. Systems the-ory, by providing a conceptual framework withinwhich both organized wholes and component parts canbe studied, overcomes this centuries-old limitation.
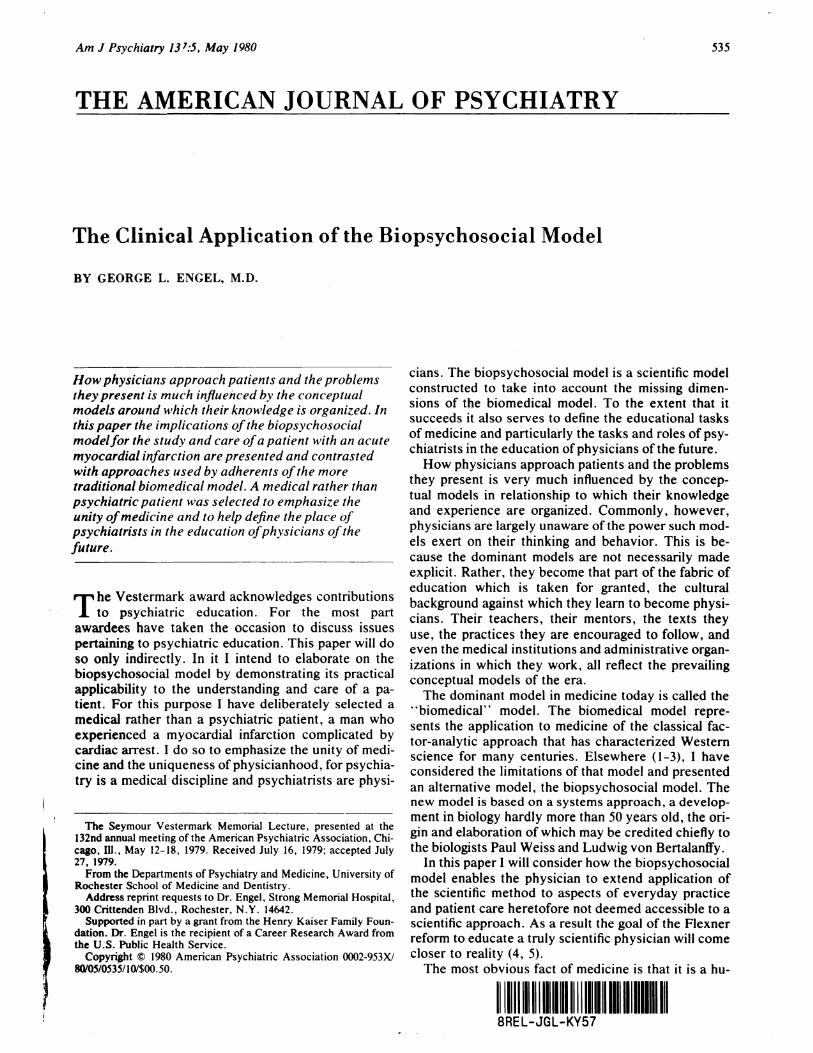
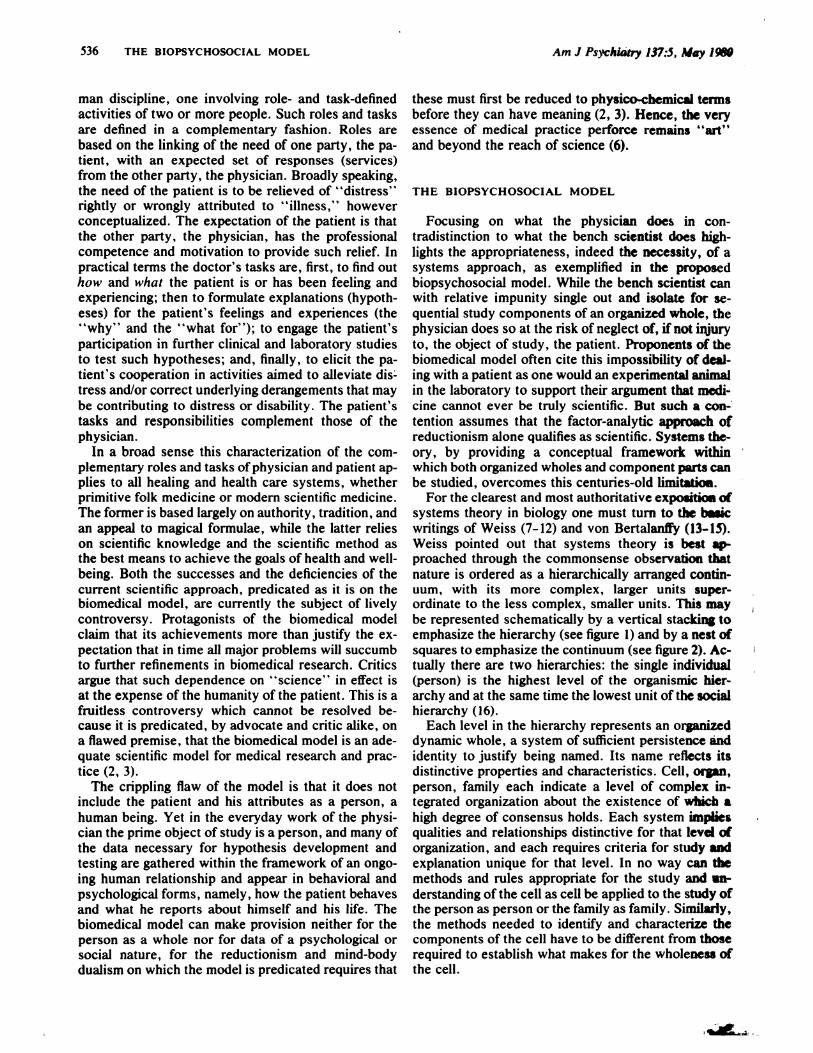
For the clearest and most authoritative exposition ofsystems theory in biology one must turn to the �icwritings of Weiss (7-12) and von Bertalanffy (13-45).Weiss pointed out that systems theory is best ap�proached through the commonsense observation thatnature is ordered as a hierarchically arranged contin-uum, with its more complex, larger units super-ordinate to the less complex, smaller units. This maybe represented schematically by a vertical stacking toemphasize the hierarchy (see figure 1) and by a nest ofsquares to emphasize the continuum (see figure 2). Ac-tually there are two hierarchies: the single individual(person) is the highest level of the organismic hier-archy and at the same time the lowest unit of the socialhierarchy (16).
Each level in the hierarchy represents an organizeddynamic whole, a system of sufficient persistence andidentity to justify being named. Its name reflects itsdistinctive properties and characteristics. Cell, organ,person, family each indicate a level of complex in-tegrated organization about the existence of which ahigh degree of consensus holds. Each system impliesqualities and relationships distinctive for that level oforganization, and each requires criteria for study andexplanation unique for that level. In no way can themethods and rules appropriate for the study and in-derstanding of the cell as cell be applied to the study ofthe person as person or the family as family. Similarly,the methods needed to identify and characterize thecomponents of the cell have to be different from thoserequired to establish what makes for the wholeness ofthe cell.
FIGURE 1Hierarchy of Natural Systems
FIGURE 2Continuum of Natural Systems
BIOSPHERE
SOCIETY-NATiON
CULTURE-SUBCULTURE
�MMUNfl�
FAMILY
TWO PERSONBIOSPHERE
SOCIETY-NATION
CULTURE-SUBCULTURE
COMMUNITY
FAMILY
ITWO-PERSON
PERSON
(experience & behavior)
NERVOUS SYSTEM
IORGANS/ORGANS SYSTEMS
ITiSSUES
ICELLS
IORGANELLES
IMOLECULES
IATOMS
ISUBATOMIC PARTiCLES
Am J Psychiatry 137:5, May 1980 GEORGE L. ENGEL 537
SYSTEMS HIERARCHY
(LEVELS OF ORGANIZATiON)
Consideration of the hierarchy as a continuum re-veals another obvious fact. Each system is at the same
time a component of higher systems (figure 2). Systemcell is a component of systems tissue and organ andperson. Person and two-person are components offamily and community. In the continuity of natural
systems every unit is at the very same time both awhole and a part. Person (or individual) represents atthe same time the highest level of the organismic hier-archy and the lowest level of the social hierarchy.Each system as a whole has its own unique character-istics and dynamics; as a part it is a component of ahigher-level system. The designation “system” be-speaks the existence of a stable configuration in timeand space, a configuration that is maintained not onlyby the coordination of component parts in some kindof internal dynamic network but also by the character-istics of the larger system of which it is a componentpart. Stable configuration also implies the existence of
�RSONNERVOUS SYSTEM
ORGAN/ORGAN SYSTEMS
boundaries between organized systems across whichmaterial and information flow.
Nothing exists in isolation. Whether a cell or a per-son, every system is influenced by the configuration ofthe systems of which each is a part, that is, by its envi-ronment. More precisely, neither the cell nor the per-son can be fully characterized as a dynamic systemwithout characterizing the larger system(s) (environ-ment) of which it is a part. This is implicit in the labelsused. The designation “red blood cell” identifies di-rectly and by implication the larger systems withoutwhich the red blood cell has no existence. The term“patient” characterizes an individual in terms of alarger social system. Identification of the patient byname, age, sex, marital status, occupation, and resi-dence identifies other systems of which that patient isa component and which in turn are part of his environ-ment.
In scientific work the investigator generally isobliged to select one system level on which to concen-trate, or at least at which to begin, his efforts. For thephysician that system level is always person, i.e., apatient. The systems-oriented scientist will be awarethat the task is always a dual and complementary one.On the one hand the constituent components of thesystem must be identified and characterized in detailand with precision. For this end the factor-analytic ap-proach has served well. Application of increasingly di-verse and refined techniques to the study of the cellhave almost endlessly extended knowledge of the con-stituent parts (systems) making up a cell. But the sys-tems characteristics of each component part of any
538 THE BIOPSYCHOSOCIAL MODEL Am J Psychiatry 137:5, May 1980
system must also be studied. Different approaches arerequired to gain understanding of the rules and forcesresponsible for the collective order of a system,whether an organelle, a cell, a person, or a commu-nity. These cannot be understood merely as an assem-blage (or reassemblage) of constituent parts (10).
The systems-oriented scientist, including the physi-cian, always has in mind this distinction and the com-plementarity inherent in it. This stands in contrast tothe orientation of the reductionist scientist, for whomconfidence in the ultimate explanatory power of thefactor-analytic approach in effect inhibits attention towhat characterizes the whole. For medicine in particu-lar the neglect of the whole inherent in the reduc-tionism of the biomedical model is largely responsiblefor the physician’s preoccupation with the body andwith disease and the corresponding neglect of the pa-tient as a person. This has contributed importantly tothe widespread public feeling that scientific medicineis impersonal, an attitude consistent with how the bio-medically trained physician views the place of sciencein his everyday work. For him “science” and the sci-entific method have to do with the understanding andtreatment of disease, not with the patient and patientcare. The reductionist scientific culture of the day islargely responsible for the public view of science andhumanism as antithetical.
APPLICATION OF THE BIOPSYCHOSOCIAL
MODEL
Let us examine how this antithesis between scienceand humanity might be attenuated, if not eliminated
altogether, were the physician to approach clinicalproblems from the more inclusive perspective of thesystems-oriented biopsychosocial model, free of theconstraints imposed by the exclusively reductionisticapproach of the biomedical model. The hierarchy andcontinuum of natural systems, as depicted in figures 1and 2, provide a guide to the systems that the physi-cian keeps in mind when undertaking the care of a pa-tient. How this works out in practice may be illus-trated by a particular clinical example, the case of Mr.Glover (a pseudonym); a 55-year-old married real es-tate salesman with two adult sons, who was brought tothe emergency department with symptoms similar towhat he had experienced six months earlier, when hehad had a myocardial infarction.
We begin consideration of the model by remindingourselves that in practice the physician’s first sourceof information is the patient himself (or some other in-formed person). Thus, clinical study begins at the per-son level and takes place within a two-person system,the doctor-patient relationship. The data consist of re-ported inner experience (e.g., feelings, sensations,thoughts, opinions, and memories) and reported and
observable behavior. In the instance of Mr. Glover,
his employer recognized that the patient was sickerthan he acknowledged himself to be, reported her ob-servations to the doctor, and persuaded the patient tolet her take him to the hospital.
How is the clinical approach of the physician influ-enced by the systems perspective of the biopsychoso-cial model? With the systems hierarchy as a guide, thephysician from the outset considers all information interms of systems levels and the possible relevance andusefulness of data from each level for the patient’s fur-ther study and care.
Even such minimal screening data as Mr. Glover’sage, gender, place of residence, marital and familystatus, occupation, and employment already indicatesystems characteristics useful for future judgmentsand decisions. The information that the patient resist-ed acknowledging illness, especially in the face of adocumented heart attack six months earlier, and hadto be persuaded to seek medical attention, tells some-thing of this man’s psychological style and conflicts.From this alone the systems-oriented physician is
alerted to the possibility, if not the probability, that thecourse of the illness and the care of the patient may beimportantly influenced by processes at the psychologi-cal and interpersonal levels of organization . Of course,the similarity of Mr. Glover’s current symptoms tothose of his recent myocardial infarction prepares thephysician to consider systems derangements at thecardiovascular level as well as at the symbolic level of“another heart attack.”
Such an inclusive approach, with consideration ofall the levels of organization that might possibly be im-portant for immediate and long-term care, may be con-trasted with the parsimonious approach of the biomed-ical model. In that mode the ideal is to find as quicklyas possible the simplest explanation, preferably the di-agnosis of a single disease, and to regard all else ascomplications, “overlay,” or just plain irrelevant tothe doctor’s task. For the reductionist physician a di-agnosis of “acute myocardial infarction” suffices tocharacterize Mr. Glover’s problem and to define thedoctor’s job. Indeed, once so categorized Mr. Gloveris likely to be referred to by the staff as “an MI.”
The Sequence of Events
Let us now reconstruct in systems terms the se-quence of events comprising the acute phase of Mr.
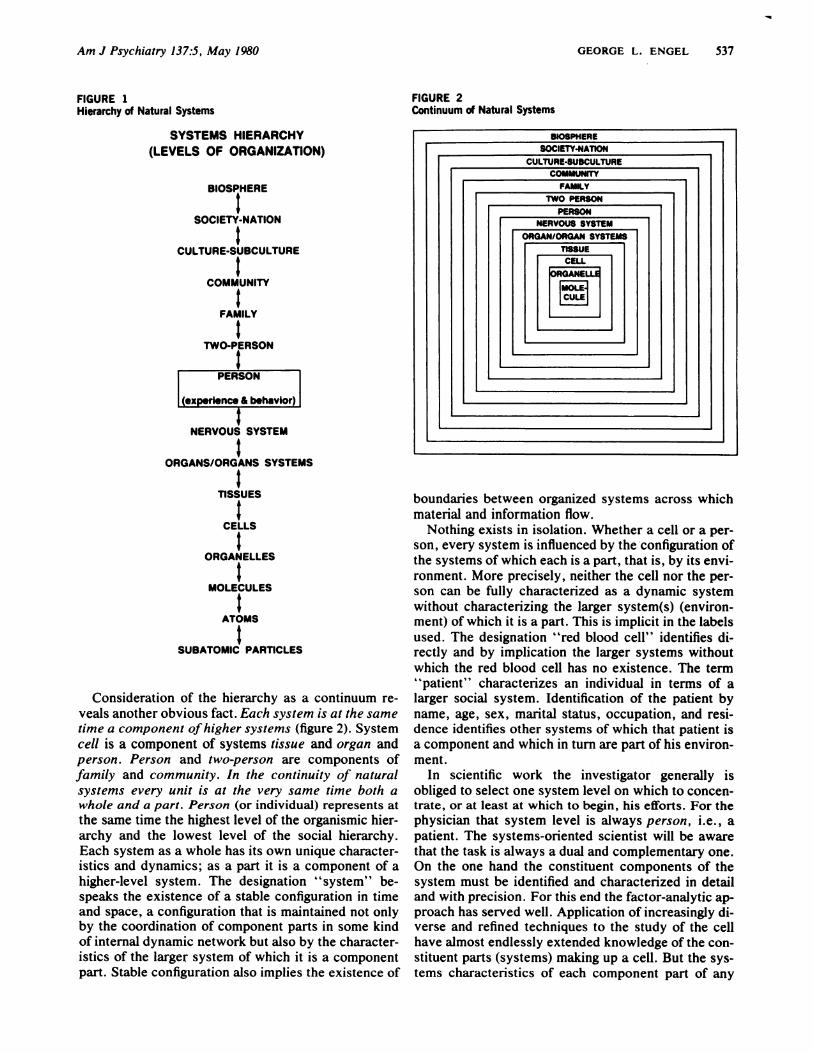
Glover’s illness. To simplify presentation we arbi-trarily take as the starting point for this analysis the 90-minute period during which the patient experiencedevolving myocardial ischemia in the form of symp-toms. This and subsequent critical events and theirconsequences for intra- and intersystemic harmonyare schematized in figures 3-9. Each diagram indi-cates the system level that the event in ques-tion affected as well as its reverberations up anddown the systems hierarchy. Appreciating the unity ofthe hierarchy, that each system is at the same time
ORGAN/ORGAN SYSTEM -�. cardiovascular reactionsand adjustments
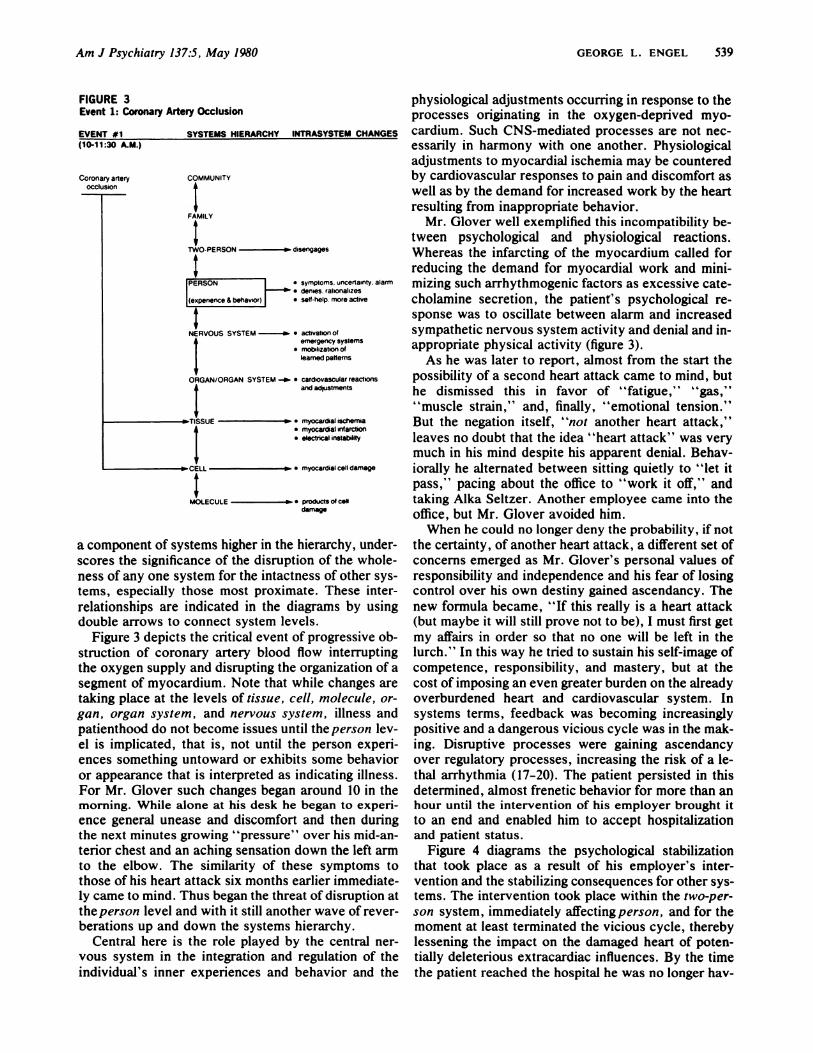
physiological adjustments occurring in response to theprocesses originating in the oxygen-deprived myo-
cardium. Such CNS-mediated processes are not nec-essarily in harmony with one another. Physiologicaladjustments to myocardial ischemia may be counteredby cardiovascular responses to pain and discomfort aswell as by the demand for increased work by the heartresulting from inappropriate behavior.
Mr. Glover well exemplified this incompatibility be-tween psychological and physiological reactions.Whereas the infarcting of the myocardium called forreducing the demand for myocardial work and mini-mizing such arrhythmogenic factors as excessive cate-cholamine secretion, the patient’s psychological re-sponse was to oscillate between alarm and increasedsympathetic nervous system activity and denial and in-appropriate physical activity (figure 3).
As he was later to report, almost from the start thepossibility of a second heart attack came to mind, buthe dismissed this in favor of “fatigue,” “gas,”‘ ‘muscle strain,’ ‘ and, finally, ‘ ‘emotional tension.”But the negation itself, “not another heart attack,”leaves no doubt that the idea “heart attack” was verymuch in his mind despite his apparent denial. Behav-iorally he alternated between sitting quietly to “let itpass,” pacing about the office to “work it off,” andtaking Alka Seltzer. Another employee came into theoffice, but Mr. Glover avoided him.
When he could no longer deny the probability , if notthe certainty, of another heart attack, a different set ofconcerns emerged as Mr. Glover’s personal values ofresponsibility and independence and his fear of losingcontrol over his own destiny gained ascendancy. Thenew formula became, “If this really is a heart attack(but maybe it will still prove not to be), I must first getmy affairs in order so that no one will be left in thelurch.” In this way he tried to sustain his self-image ofcompetence, responsibility, and mastery, but at thecost of imposing an even greater burden on the alreadyoverburdened heart and cardiovascular system. Insystems terms, feedback was becoming increasinglypositive and a dangerous vicious cycle was in the mak-ing. Disruptive processes were gaining ascendancyover regulatory processes, increasing the risk of a le-thal arrhythmia (17-20). The patient persisted in thisdetermined, almost frenetic behavior for more than anhour until the intervention of his employer brought it
to an end and enabled him to accept hospitalizationand patient status.
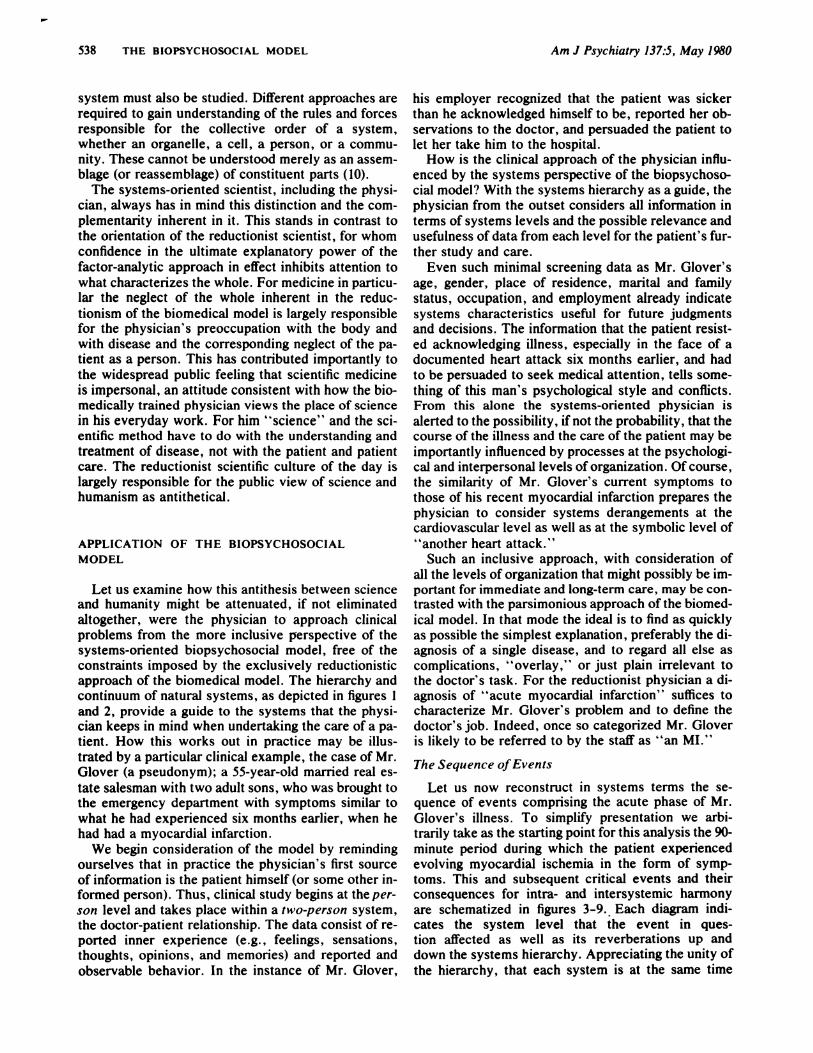
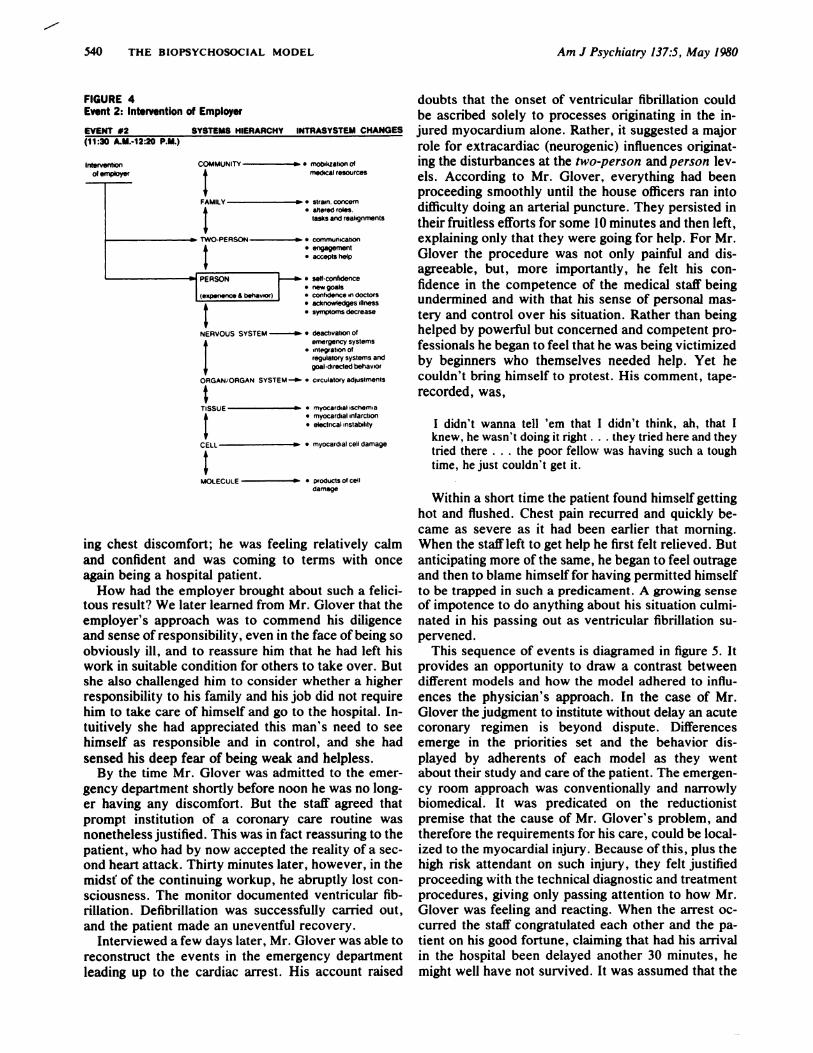
Figure 4 diagrams the psychological stabilizationthat took place as a result of his employer’s inter-vention and the stabilizing consequences for other sys-tems. The intervention took place within the two-per-
son system, immediately affectingperson, and for themoment at least terminated the vicious cycle, therebylessening the impact on the damaged heart of poten-tially deleterious extracardiac influences. By the timethe patient reached the hospital he was no longer hay-
CELL � #{149}myocardial cell damage
I _______________
MOLECULE � #{149}products of calf
a component of systems higher in the hierarchy, under-scores the significance of the disruption of the whole-ness of any one system for the intactness of other sys-tems, especially those most proximate. These inter-relationships are indicated in the diagrams by usingdouble arrows to connect system levels.
Figure 3 depicts the critical event of progressive ob-struction of coronary artery blood flow interruptingthe oxygen supply and disrupting the organization of asegment of myocardium. Note that while changes aretaking place at the levels of tissue, cell, molecule, or-
gan, organ system, and nervous system, illness andpatienthood do not become issues until the person lev-el is implicated, that is, not until the person experi-ences something untoward or exhibits some behavioror appearance that is interpreted as indicating illness.For Mr. Glover such changes began around 10 in themorning. While alone at his desk he began to experi-
ence general unease and discomfort and then duringthe next minutes growing “pressure” over his mid-an-terior chest and an aching sensation down the left armto the elbow. The similarity of these symptoms tothose of his heart attack six months earlier immediate-ly came to mind. Thus began the threat of disruption atthe person level and with it still another wave of rever-berations up and down the systems hierarchy.
Central here is the role played by the central ner-vous system in the integration and regulation of theindividual’s inner experiences and behavior and the
Am J Psychiatry 137:5, May 1980 GEORGE L. ENGEL 539
.. rnyocardsal ischem#{232}a
#{149}myocart�at infarction
#{149}electrical instabEldy
of employer
540 THE BIOPSYCHOSOCIAL MODEL Am J Psychiatry 137:5, May 1980
FIGURE 4Event 2: Intervention of Employer
EVENT #2 SYSTEMS HIERARCHY INTRASYSTEM CHANGES(11:30 A.M.-12:20 P.M.)
COMMUNITY � C motskzation of
I medical resourcesFAMILY w e strain, concern4 #{149}altered roles.
tasks and reahgnments
TWO-PERSON � #{149}communication4 e engagement
#{149}accepts help
� PERSON l-e’. #{149}a new goals#{149}confidence in doctorse acknowledges illnessa symptoms decrease
NERVOUS SYSTEM ‘ C deactivation Ofemergency systems
a infegration ofregulatory systems andgoal-directed behavior
ORGAN/ORGAN SYSTEM -� . circulatory adjustments
TISSUE � #{149}myocardial schemia4 e myocardial infarction
I #{149}electrical instab#{243}ltyCELL � #{149}myocardial cell damage
I ______________
MOLECULE ie #{149}products of celldamage
ing chest discomfort; he was feeling relatively calmand confident and was coming to terms with onceagain being a hospital patient.
How had the employer brought about such a felici-tous result? We later learned from Mr. Glover that theemployer’s approach was to commend his diligenceand sense of responsibility, even in the face of being soobviously ill, and to reassure him that he had left hiswork in suitable condition for others to take over. Butshe also challenged him to consider whether a higherresponsibility to his family and his job did not requirehim to take care of himself and go to the hospital. In-tuitively she had appreciated this man’s need to seehimself as responsible and in control, and she had
sensed his deep fear of being weak and helpless.By the time Mr. Glover was admitted to the emer-
gency department shortly before noon he was no long-er having any discomfort. But the staff agreed thatprompt institution of a coronary care routine wasnonetheless justified. This was in fact reassuring to thepatient, who had by now accepted the reality of a sec-ond heart attack. Thirty minutes later, however, in themids( of the continuing workup, he abruptly lost con-sciousness. The monitor documented ventricular fib-rillation. Defibrillation was successfully carried out,and the patient made an uneventful recovery.
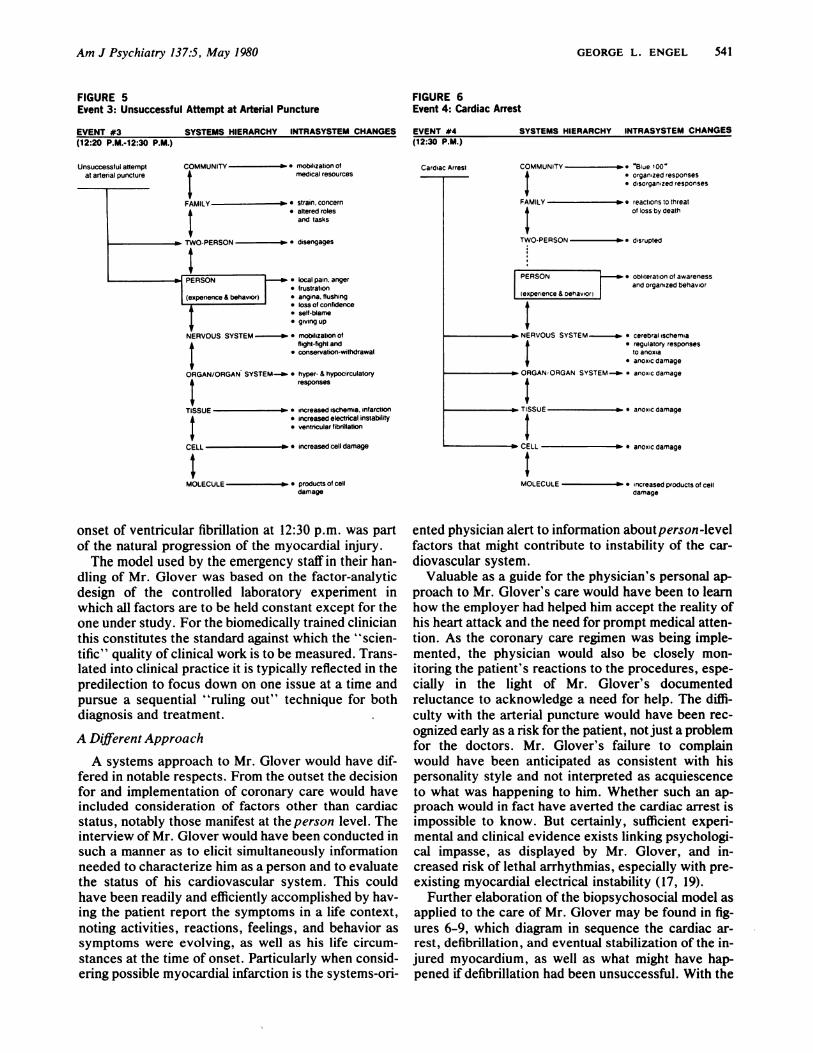
Interviewed a few days later, Mr. Glover was able toreconstruct the events in the emergency departmentleading up to the cardiac arrest. His account raised
doubts that the onset of ventricular fibrillation couldbe ascribed solely to processes originating in the in-jured myocardium alone. Rather, it suggested a majorrole for extracardiac (neurogenic) influences originat-ing the disturbances at the two-person and person 1ev-els. According to Mr. Glover, everything had beenproceeding smoothly until the house officers ran intodifficulty doing an arterial puncture. They persisted in
their fruitless efforts for some 10 minutes and then left,explaining only that they were going for help. For Mr.Glover the procedure was not only painful and dis-agreeable, but, more importantly, he felt his con-fidence in the competence of the medical staff beingundermined and with that his sense of personal mas-tery and control over his situation. Rather than beinghelped by powerful but concerned and competent pro-fessionals he began to feel that he was being victimizedby beginners who themselves needed help. Yet hecouldn’t bring himself to protest. His comment, tape-
recorded, was,
I didn’t wanna tell ‘em that I didn’t think, ah, that Iknew, he wasn’t doing it right . . . they tried here and theytried there . . . the poor fellow was having such a toughtime, he just couldn’t get it.
Within a short time the patient found himself gettinghot and flushed. Chest pain recurred and quickly be-
came as severe as it had been earlier that morning.When the staffleft to get help he first felt relieved. Butanticipating more of the same, he began to feel outrageand then to blame himselffor having permitted himselfto be trapped in such a predicament. A growing senseof impotence to do anything about his situation culmi-nated in his passing out as ventricular fibrillation su-pervened.
This sequence of events is diagramed in figure 5. Itprovides an opportunity to draw a contrast betweendifferent models and how the model adhered to influ-ences the physician’s approach. In the case of Mr.Glover the judgment to institute without delay an acutecoronary regimen is beyond dispute. Differencesemerge in the priorities set and the behavior dis-
played by adherents of each model as they wentabout their study and care of the patient. The emergen-
cy room approach was conventionally and narrowly
biomedical. It was predicated on the reductionistpremise that the cause of Mr. Glover’s problem, andtherefore the requirements for his care, could be local-ized to the myocardial injury. Because of this, plus thehigh risk attendant on such injury, they felt justifiedproceeding with the technical diagnostic and treatmentprocedures, giving only passing attention to how Mr.Glover was feeling and reacting. When the arrest oc-
curred the staff congratulated each other and the pa-
tient on his good fortune, claiming that had his arrival
in the hospital been delayed another 30 minutes, he
might well have not survived. It was assumed that the
Unsuccessful attemptat arterial puncture
COMMUNITY a- #{149}mobilization ofmedical resources
FAMILY -a- e strain, concern
#{149}altered rolesand tasks
TWO-PERSON a-. disengages
Cardiac Arrest COMMUNITY a’ Blue 1004 #{149}organized responses
#{149}disorganized responses
FAMILY a reactions to threatof loss by death
TWO-PERSON a disrupted
PERSON ]-,.- a Obliteration of awareness
and organized behaviorexperience & Dehavior)
a NERVOUS SYSTEM a #{149}cerebral ischemia4 #{149}regulatory responses
I toanoxia4 a anoxic damage
a ORGANORGAN SYSTEM-a- #{149}anoxic damage
___________________ I ___________________
a TISSUE a a anosic damage
____________________ I _____________________
a- CELL. a- e anoxic damage
I _______________
MOLECULE � a increased products of celldamage
Am J Psychiatry 137:5, May 1980 GEORGE L. ENGEL 541
FIGURE 5Event 3: Unsuccessful Attempt at Arterial Puncture
EVENT #3 SYSTEMS HIERARCHY INTRASYSTEM CHANGES(12:20 P.M.-12:30 P.M.)
FIGURE 6Event 4: Cardiac Arrest
EVENT #4 SYSTEMS HIERARCHY INTRASYSTEM CHANGES(12:30 P.M.)
#{149}local pain, anger#{149}frustration#{149}angina, flushing#{149}loss of confidence#{149}self-blame#{149}giving up
onset of ventricular fibrillation at 12:30 p.m. was partof the natural progression of the myocardial injury.
The model used by the emergency staff in their han-dling of Mr. Glover was based on the factor-analyticdesign of the controlled laboratory experiment inwhich all factors are to be held constant except for theone under study. For the biomedically trained clinicianthis constitutes the standard against which the ‘ ‘scien-tific” quality ofclinical work is to be measured. Trans-lated into clinical practice it is typically reflected in thepredilection to focus down on one issue at a time andpursue a sequential “ruling out” technique for bothdiagnosis and treatment. -
A Different Approach
A systems approach to Mr. Glover would have dif-fered in notable respects. From the outset the decisionfor and implementation of coronary care would haveincluded consideration of factors other than cardiacstatus, notably those manifest at the person level. Theinterview of Mr. Glover would have been conducted in
such a manner as to elicit simultaneously informationneeded to characterize him as a person and to evaluate
the status of his cardiovascular system. This couldhave been readily and efficiently accomplished by hav-ing the patient report the symptoms in a life context,
noting activities, reactions, feelings, and behavior assymptoms were evolving, as well as his life circum-stances at the time of onset. Particularly when consid-ering possible myocardial infarction is the systems-on-
ented physician alert to information aboutperson -levelfactors that might contribute to instability of the car-diovascular system.
Valuable as a guide for the physician’s personal ap-proach to Mr. Glover’s care would have been to learnhow the employer had helped him accept the reality of
his heart attack and the need for prompt medical atten-tion. As the coronary care regimen was being imple-mented, the physician would also be closely mon-itoring the patient’s reactions to the procedures, espe-cially in the light of Mr. Glover’s documentedreluctance to acknowledge a need for help. The diffi-
culty with the arterial puncture would have been rec-ognized early as a risk for the patient, notjust a problemfor the doctors. Mr. Glover’s failure to complainwould have been anticipated as consistent with his
personality style and not interpreted as acquiescenceto what was happening to him. Whether such an ap-proach would in fact have averted the cardiac arrest isimpossible to know. But certainly, sufficient experi-mental and clinical evidence exists linking psychologi-cal impasse, as displayed by Mr. Glover, and in-creased risk of lethal arrhythmias, especially with pre-existing myocardial electrical instability (17, 19).
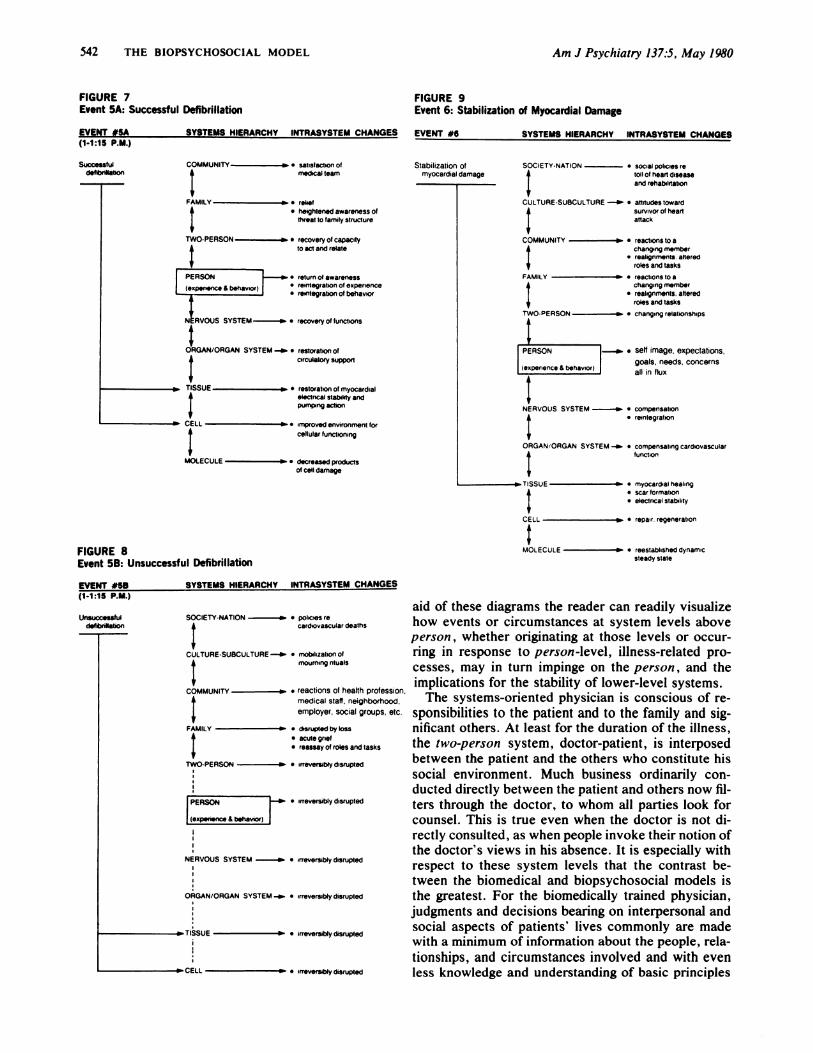
Further elaboration of the biopsychosocial model asapplied to the care of Mr. Glover may be found in fig-
ures 6-9, which diagram in sequence the cardiac ar-rest, defibrillation, and eventual stabilization of the in-
jured myocardium, as well as what might have hap-pened if defibrillation had been unsuccessful. With the
Successfulde�on
Am J Psychiatry 137:5, May 1980
EVENT #6 SYSTEMS HIERARCHY INTRASYSTEM CHANGES
Unsuccau�defibfllfaben
Stabilization of SOCIETY-NATION #{149}social policies remyocardial damage 4 toll of heart disease
� and rehabilitation
CULTURE-SUBCULTURE -a- . attitudes toward4 SurvivOr of heart
attack
COMMUNITY �a #{149}reactions to a4 changing member
I #{149}realignments. alteredt roles and tasks
FAMILY a a reactions to a
4 changing member� e realignments. altered4 roles and tasks
TWO-PERSON -a #{149}changing relationships
Ir PERSON -a- . self image, expectations,
goals. needs, concerns(experience & behaviorl all in flux
NERVOUS SYSTEM -a- a compensation
I a reintegrationORGAN/ORGAN SYSTEM -a- #{149}compensating cardiovascular� function
-a TISSUE a . myocardial healing4 . scar formation
#{149}electncal stability
CELL a- #{149}repair. regeneration
MOLECULE -a . reestablished dynamicsteady state
aid of these diagrams the reader can readily visualizehow events or circumstances at system levels above
person , whether originating at those levels or occur-ring in response to person-level, illness-related pro-cesses, may in turn impinge on the person , and the
implications for the stability of lower-level systems.The systems-oriented physician is conscious of re-
sponsibilities to the patient and to the family and sig-nificant others. At least for the duration of the illness,the two-person system, doctor-patient, is interposedbetween the patient and the others who constitute his
social environment. Much business ordinarily con-ducted directly between the patient and others now fil-ters through the doctor, to whom all parties look for
counsel. This is true even when the doctor is not di-rectly consulted, as when people invoke their notion ofthe doctor’s views in his absence. It is especially withrespect to these system levels that the contrast be-tween the biomedical and biopsychosocial models isthe greatest. For the biomedically trained physician,judgments and decisions bearing on interpersonal andsocial aspects of patients’ lives commonly are made
with a minimum of information about the people, rela-
tionships, and circumstances involved and with even
less knowledge and understanding of basic principles
COMMUNITY a- e reaclions of health profession,+ medical staff, neighborhood,
employer, social groups, etc.
FAMILY a #{149}disrupted by lOSS
+ #{149}acute grief#{149}reassay of roles and tasks
TWO-PERSON a #{149}irreversibly disrupted
Am J Psychiatry 137:5, May /980 GEORGE L. ENGEL 543
underlying interpersonal and social transactions. Byand large the physician reaches decisions on the basisof tradition, custom, prescribed rules, compassion, in-
tuition, “common sense,” and sometimes highly per-sonal self-reference. Such processes involving the per-son and supraperson levels, often of crucial impor-
tance for the patient and for the significant others,remain outside the realm of science and critical in-
quiry. Not so for the biopsychosocially oriented physi-cian, who recognizes that to best serve the patient,higher-system-level occurrences must be approachedwith the same rigor and critical scrutiny that are ap-plied to systems lower in the hierarchy. This meansthat the physician identifies and evaluates the stabiliz-ing and destabilizing potential of events and relation-ships in the patient’s social environment, not neglect-ing how the destabilizing effects of the patient’s illnesson others may feed back as a further destabilizing in-
fluence on the patient.
Consider the responsibilities that Mr. Glover’s phy-
sician would have had to face, for example, had Mrs.Glover fallen ill-or even died-under the strain of her
husband’s illness and near-death. Consider, too, how in-
formation about Mrs. Glover, readily available to thephysician skilled at observation and conscious of itsvalue, would enable him or her to recognize her vul-
nerabiities and hence avert her breakdown and ill-ness. The continuity of systems makes attention to
Mrs. Glover’s well-being a necessary element in Mr.
Glover’s care. For the biopsychosocially oriented phy-sician this is not merely a matter of compassion andhumanity, as some would have us believe, but one ofrigorous application of the principles and practices of
science, a human science (20).Some argue that the biopsychosocial model imposes
an impossible demand on the physician. This misses
the point. The model does not add anything to what is
not already involved in patient care. Rather, it pro-vides a conceptual framework and a way of thinkingthat enables the physician to act rationally in areas
now excluded from a rational approach. Further, itmotivates the physician to become more informed andskillful in the psychosocial areas, disciplines now seen
as alien and remote even by those who intuitively rec-ognize their importance. And finally, the model servesto counteract the often wasteful reductionist pursuit ofwhat often prove to be trivial rather than crucial de-terminants of illness. The biopsychosocial physician is
expected to have a working knowledge of the prin-ciples, language, and basic facts of each relevant dis-cipline; he is not expected to be an expert in all.
THE BIOPSYCHOSOCIAL MODEL AS A
SCIENTIFIC MODEL
I hope the example of Mr. Glover, with all of itsoversimplification, indicates how the working concep-
tual model used by the physician can influence the ap-proach to patient care. The biopsychosocial model is a
scientific model. So, too, was the biomedical model. Butas Fabrega (21) pointed out, by now it has becometransformed into a folk model, actually the dominantfolk model of the Western world. As such it has cometo constitute a dogma. The hallmark of a scientific
model is that it provides a framework within which the
scientific method may be applied. The value ofa scien-tific model is measured not by whether it is right orwrong but by how useful it is. It is modified or dis-carded when it no longer helps to generate and testnew knowledge. Dogmas, in contrast, maintain theirinfluence through authority and tradition. They resistchange and hence tend to promote opposition and thepromulgation of rival dogmas by dissident figures. The
counter dogmas being put forth these days in opposi-tion to biomedical dogma are called “holistic’ ‘ and‘ ‘ medicine. They qualify as dogmas to theextent that they eschew the scientific method and leaninstead on faith and belief systems handed down fromremote and obscure or charismatic authority figures.They tend to place science and humanism in opposi-tion. But as the history of the biomedical model itselfhas shown, progress is made only where the scientificmethod is applied. The triumphs of the biomedicalmodel all have been in the areas for which the modelhas provided a suitable framework for scientific study.The biopsychosocial model extends that framework to
heretofore neglected areas.
REFERENCES
I. Engel GL: A unified concept of health and disease. PerspectBiol Med 3:459-485, 1960
2. Engel GL: The need for a new medical model: a challenge forbiomedicine. Science 196: 129-136, 1977
3. Engel GL: The biopsychosocial model and the education ofhealth professionals. Ann NY Acad Sci 310:169-181, 1978
4. Flexner A: Medical Education in the United States and Canada:A Report of the Carnegie Foundation of the Advancement ofTeaching. Bulletin 4. Boston, Updyke, 1910
5. Engel GL: Biomedicine’s failure to achieve flexnerian standardsof education. J Med Educ 53:387-392, 1978
6. Engel GL: The care of the patient: art or science? Johns Hop-kins Med J 140:222-232, 1977
7. Weiss P: Animal behavior as system reaction: orientation to-ward light and gravity in the resting postures of butterflies(Vanessa) (1925). General Systems: Yearbook of the Society forGeneral Systems Research 4: 1-44, 1959
8. Weiss P: The problem of cell individuality in development.American Naturalist 74:34-46, 1940
9. Weiss P: The biological basis ofadaptation, in Adaptation. Edit-ed by Romano J. Ithaca, NY, Cornell University Press, 1949
10. Weiss P: 1 + 1 * 2: when one plus one does not equal two, inThe Neurosciences: A Study Program. Edited by Quarton OC,Melnechuk T, Schmidt FO. New York, Rockefeller UniversityPress, 1967
11. Weiss P: The living system: determinism stratified, in BeyondReductionism. Edited by Koestler A, Smythies JR. New York,Macmillan Publishing Co, 1969
12. Weiss P: The system of nature and the nature of systems: empir-ical holism and practical reductionism harmonized, in Toward aMan-Centered Medical Science. Edited by Schaefer KE, Hen-
544 THE BIOPSYCHOSOCIAL MODEL Am J Psychiatry 137:5, May 1980
Phenothiazine antipsychotics: Dr. Davis, (312) 996-1065
sd H, Brody R. Mt Kisco, NY, Futura Publishing Co, 197713. von Bertalanify L: Problems of Life. New York, John Wiley &
Sons, 195214. von Bertalanify L: General System Theory. New York, Brazil-
1cr, 196815. von Bertalanify L: Chance or law, in Beyond Reductionism. Ed-
ited by Koestler A, Smythies JR. New York, Macmillan Pub-lishing Co, 1969
16. Koestler A, Smythies JR (eds): Beyond Reductionism. NewYork, Macmillan Publishing Co, 1969
Notice to Clinical Investigators
17. Engel GL: Sudden and rapid death during psychological stress:folklore or folkwisdom? Ann Intern Med 74:771-782, 1971
18. Lown B, Verrier RL, Rabinowitz SH: Neural and psychologicmechanisms and the problem of sudden death. Am J Cardiol39:890-902, 1977
19. Engel GL: Psychologic stress, vasodepressor (vasovagal) syn-cope and sudden death. Ann Intern Med 89:403-412, 1978
20. Mead M: Towards a human science. Science 191:903-909, 197621. Fabrega H: The need for an ethnomedical science. Science
189:969-975, 1975
Under program support from the Foundations’ Fund for Research in Psychiatry, threeresearch laboratories have been designated as resource groups for clinical investigatorsdoing blood level research with antianxiety, antidepressant, and antipsychotic drugs. In-vestigators who seek to establish the reliability of their methods or those who wish toparticipate in a proficiency testing protocol should contact the appropriate group listedbelow.