ALLHAT. U.S. Department of Health and Human Services. National Institutes of Health. National Heart, Lung, and Blood Institute. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic. - PowerPoint PPT Presentation
1 U.S. Department of Health and Human Services National Institutes of Health National Heart, Lung, and Blood Institute Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) The ALLHAT Collaborative Research Group Sponsored by the National Heart, Lung, and Blood Institute (NHLBI) ALLHAT JAMA. 2002;288:2981-2997
Transcript
1
U.S. Department of Health and Human
Services
National Institutes of Health
National Heart, Lung, and Blood Institute
Major Outcomes in High Risk Hypertensive Patients Randomized to
Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT)
The ALLHAT Collaborative Research Group
Sponsored by the National Heart, Lung, and Blood Institute (NHLBI)
• Determine whether occurrence of fatal CHD or nonfatal MI is lower for high-risk hypertensive patients treated with newer agents (CCB, ACEI, alpha-blocker) compared with a diuretic
• 42,418 high-risk hypertensive patients ≥ 55 years
– Records from the Center for Medicare & Medicaid Services (CMS) database (participants age 65 or older)
ALLHAT
15
Decision to Dropan ALLHAT Arm
• January 24, 2000 – NHLBI Director accepts the recommendation of an independent review group to terminate doxazosin arm
– Futility of finding a significant difference for primary outcome
– Statistically significant 25 percent higher rate of major secondary endpoint, combined CVD outcomes
ALLHAT
16
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0 1 2 3 4
Cu
mu
lati
ve E
ven
t R
ate
Years of Follow-up
doxazosin
chlorthalidone
Cardiovascular Disease
C: 15,268D: 9,067
12,990 7,382
9,4435,285
4,8272,654
2,0101,083
Rel Risk 1.25
z = 6.77, p < 0.0001
95% CI1.17-1.33
ALLHAT
JAMA. 2000;283:1967-1975
17
0.00
0.02
0.04
0.06
0.08
0.10
0 1 2 3 4
Cu
mu
lati
ve E
ven
t R
ate
Years of Follow-up
doxazosinchlorthalidone
Heart Failure
C: 15,268D: 9,067
13,644 7,845
5,5313,089
2,4271,351
9,541 5,457
Rel Risk 2.04
z = 10.95, p < 0.0001
95% CI1.79-2.32
ALLHAT
JAMA. 2000;283:1967-1975
18
Comparison of Doxazosin with Chlorthalidone -
Conclusions
• Doxazosin is not recommended as first-line therapy in hypertension.
• ALLHAT does not allow an assessment of the effect of doxazosin compared with placebo on the incidence of CVD.
• The use of doxazosin as a step-up drug for treating hypertension was not tested in this trial.
• These findings are likely to apply to all alpha-blockers.
ALLHAT
JAMA. 2000;283:1967-1975
19
Baseline Characteristics
Chlorthalidone 15,255
Amlodipine 9,048
Lisinopril 9,054
Mean SBP/DBP 146 / 84 146 / 84 146 / 84
Treated (90%)
Untreated (10%)
145 / 83
156 / 89
145 / 83
157 / 90
145 / 84
156 / 89
Mean age, y 67 67 67
Black, % 35 36 36
Women, % 47 47 46
Current smoking % 22 22 22
History of CHD, % 26 24 25
Type 2 diabetes, % 36 37 36
ALLHAT
20
On Step 1 or Equivalent Treatment by Antihypertensive Treatment Group
0.0
20.0
40.0
60.0
80.0
100.0
%
Chlor 87.1 84.7 82.7 80.8 80.5
Aml 87.6 85.2 83.2 80.5 80.4
Lis 82.4 78.4 77.1 74.8 72.6
1 Year 2 Years 3 Years 4 Years 5 Years
ALLHAT
21
Full Crossovers by Antihypertensive Treatment Group
0.0
5.0
10.0
15.0
%
Chlor 5.1 6.7 7.7 8.2 9.0
Amlodipine 2.8 4.5 5.0 6.0 6.9
Lisinopril 3.5 5.1 6.0 7.0 8.5
1 Year 2 Years 3 Years 4 Years 5 Years
ALLHATChlorthalidone: not on assigned medicine or open-label diuretic, but on open-label calcium channel blocker or ACE-inhibitorAmlodipine: not on assigned medicine or open-label calcium channel blocker, but on open-label diureticLisinopril: not on assigned medicine or open-label ACE-inhibitor, but on open-label diuretic
22
On Step 2 or Step 3 Treatment by Antihypertensive Treatment Group
0.0
20.0
40.0
60.0
80.0
100.0
%
Chlor 26.7 32.2 35.6 38.0 40.7
Aml 25.9 32.0 35.2 36.9 39.5
Lis 32.6 36.3 38.8 40.7 43.0
1 Year 2 Years 3 Years 4 Years 5 Years
ALLHAT
23
BP Results by Treatment Group
Compared to chlorthalidone:
SBP significantly higher in the amlodipine group (~1 mm Hg) and the lisinopril group (~2 mm Hg).
Compared to chlorthalidone:
DBP significantly lower in the amlodipine group (~1 mm Hg).
ALLHAT
BL 6M 1Y 3Y 5Y
C 146.2 138.2 136.6 134.6 134.1
A 146.2 140.0 138.3 135.4 134.9
L 146.4 141.4 139.7 136.4 136.1
BL 6M 1Y 3Y 5Y
C 84.0 80.1 79.2 77.1 75.4
A 83.9 79.7 78.5 76.1 74.5
L 84.1 80.8 79.7 77.2 75.4
24
Biochemical Results
Chlorthalidone Amlodipine Lisinopril
Serum cholesterol- mg/dL, mean (SD)
Baseline 216.1 (43.8) 216.5 (44.1) 215.6 (42.4)
4 Years 197.2 (42.1) 195.6 (41.0)* 195.0 (40.6)*
Serum potassium – mmol/L, mean (SD)
Baseline 4.3 (0.7) 4.3 (0.7) 4.4 (0.7)*
4 Years 4.1 (0.7) 4.4 (0.7)* 4.5 (0.7)*
Estimated GFR† – mL/min/1.73m2 ,mean (SD)
Baseline 77.6 (19.7) 78.0 (19.7) 77.7 (19.9)
4 Years 70.0 (19.7) 75.1 (20.7)* 70.7 (20.1)*
* p<.05 compared to chlorthalidone† Ann Intern Med. 1999;130:461-470
ALLHAT
25
Biochemical Results – Fasting Glucose – mg/dL
Chlorthalidone Amlodipine Lisinopril
Total –mean (SD)
Baseline 123.5 (58.3) 123.1 (57.0) 122.9 (56.1)
4 Years 126.3 (55.6) 123.7 (52.0) 121.5 (51.3)*
Among baseline nondiabetics with baseline <126 mg/dL – mean (SD)
Because of the superiority of thiazide-type diuretics in preventing one or more major forms of CVD and their lower cost, they should be the drugs of choice for first-step antihypertensive drug therapy.
38
Other Conclusions
• Neither amlodipine (representing CCB) nor lisinopril (representing ACEI) was superior to chlorthalidone (representing thiazide-type diuretics) in preventing major coronary events or increasing overall survival.
• Although chlorthalidone did not differ from amlodipine in overall CVD event prevention, it was superior to amlodipine (by about one-fourth) in preventing heart failure, overall and for hospitalized or fatal cases.
ALLHAT
39
Other Conclusions
• Chlorthalidone was superior to lisinopril in preventing aggregate CV events, principally stroke, HF, angina, and coronary revascularization
• Chlorthalidone was superior to doxazosin (representing alpha-blockers) in preventing CV events, including both HF and other CVD.
ALLHAT
40
Other Conclusions
• Given the large sample size, almost all biochemical differences between treatment groups at 4 years were statistically significant.
• Total cholesterol 1-2 mg/dL higher in chlorthalidone compared to amlodipine and lisinopril.
• Serum potassium 0.3-0.4 mmol/L lower in chlorthalidone compared to amlodipine and lisinopril.
– Potassium <3.5 mmol/L 6-8% higher among those randomized to chlorthalidone
• Fasting glucose 3 mg/dL higher in chlorthalidone than amlodipine group, 5 mg/dL higher in chlorthalidone than lisinopril group.
ALLHAT
41
Other Conclusions
• Among nondiabetic participants, incidence of fasting glucose 126 mg/dL at 4 years was 1.8% higher in chlorthalidone vs amlodipine, and 3.5% higher in chlorthalidone vs lisinopril.
• Estimated GFR decreased by 7-8 units at 4 years in chlorthalidone and lisinopril arms, but decreased only by about 3 units in the amlodipine arm.
• Overall, metabolic differences did not translate into more adverse cardiovascular events, or into higher all-cause mortality, with chlorthalidone.
ALLHAT
42
Further Conclusions: Amlodipine versus
Chlorthalidone
Drug tolerance and blood pressure control were similar (and high):
• The percent of participants who remained on the assigned drug or another of the same class was essentially identical (80% of those attending the 5-year visit)
• Mean SBP averaged about 1 mm Hg higher, and mean DBP about 1 mm Hg lower, in the amlodipine group
• BP control averaged about 2% better in the chlorthalidone group, reaching 68% after 5 years
ALLHAT
43
Further Conclusions: Amlodipine versus Chlorthalidone
There were no differences for other secondary outcomes:
– Hospitalization for gastrointestinal bleeding (in a subset of the cohort)
– All-cause mortality
ALLHAT
44
Further Conclusions: Amlodipine versus Chlorthalidone
Results for all cited outcomes were consistent for major (pre-specified) subgroups:
– Men and women
– Black and nonblack participants
– Older and younger participants (<65 and 65+)
– Diabetic and non-diabetic participants
ALLHAT
45
Further Conclusions: Lisinopril versus Chlorthalidone
Drug tolerance and blood pressure control were better with chlorthalidone, especially for black patients:
• The percent of participants remaining on lisinopril or another ACEI averaged about 5-6% less than participants assigned to the diuretic
• About 6-8% more of the participants in the lisinopril group than those in the chlorthalidone group required additional antihypertensive drugs
ALLHAT
46
Further Conclusions: Lisinopril versus Chlorthalidone
• Mean SBP averaged about 2 mm Hg higher in the lisinopril than the chlorthalidone group (4 mm Hg for blacks); mean DBPs were equivalent
• BP control averaged about 4-7% better in the chlorthalidone group
• Of patients in the lisinopril group who remained on an ACEI, 19% were also on a diuretic at 5 years
ALLHAT
47
Further Conclusions: Lisinopril versus Chlorthalidone
There were no differences for other secondary outcomes
– peripheral arterial disease
– end stage renal disease
– cancer incidence and mortality
– all-cause mortality
ALLHAT
48
Further Conclusions: Lisinopril versus Chlorthalidone
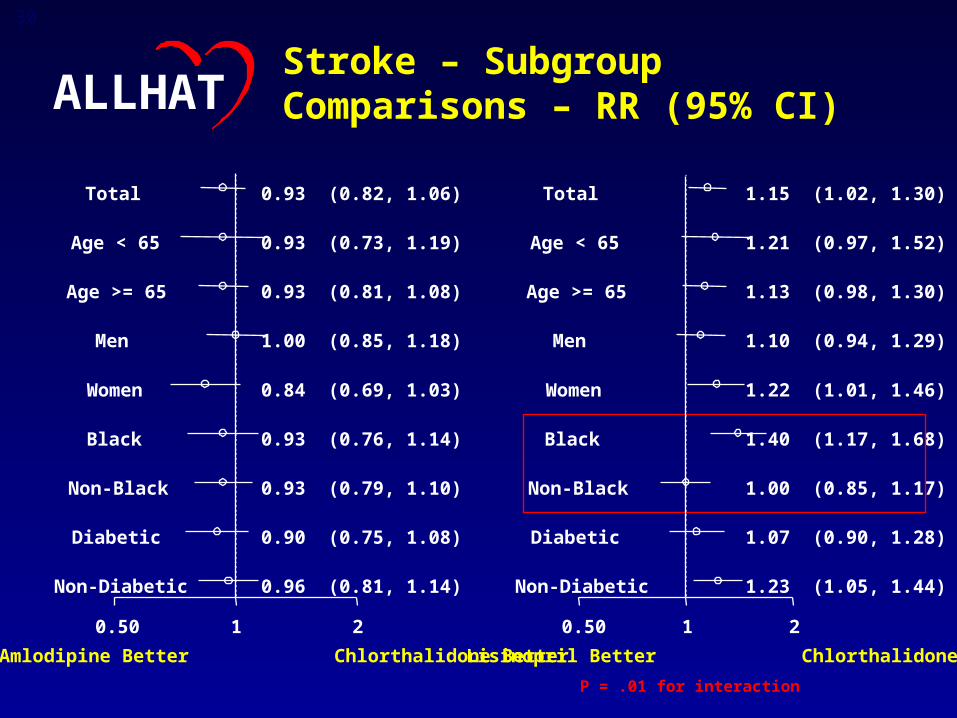
• Results were consistent for all outcomes by age, gender, race, and diabetic status, except for stroke and CVD, where there was significant heterogeneity by race (p=.01 and p=.04, respectively)
– Among black participants assigned to lisinopril, the stroke rate was increased 40% compared to the chlorthalidone group. (No difference among non-black participants.)
– The combined CVD rate was increased 19% in blacks and by 6% in whites.
• Angiodema, a rare adverse effect, was more frequent with lisinopril, especially in blacks
ALLHAT
49
Antihypertensive Trial:Implications
• Diuretics should be the drug of choice for first step therapy of hypertension
• For the patient who cannot take a diuretic (which should be an unusual circumstance), CCB’s and ACEI’s may be considered.
• Most hypertensive patients require more than one drug. Diuretics should generally be part of the antihypertensive regimen. Lifestyle advice should also be provided.
ALLHAT
50
Angioedema
Total BlacksNon-
blacks
Chlorthalidone 8 / 15,255
0.1%
2 / 5,369
<0.1%
6 / 9,886
0.1%
Lisinopril 38 / 9,054
0.4%
23 / 3,210
0.7%
15 / 5,844
0.3%p<.001 p<.001 p=.002
There were 3 cases (<0.1%) of angioedema in the amlodipine group (comparison to chlorthalidone not significant).