6/16/2015 1 The BCAT Approach: The Gold Standard in Rapid Assessment and Treatment of Cognitive Disorders in Older Adults Prepared by Dr. William Mansbach Founder & CEO, Mansbach Health Tools, LLC Home of the BCAT at www.thebcat.com Presented by Sarah Kneisler RMT/NHA at [email protected]Course Description Proficiency in the cognitive assessment of persons who have a subjective or objective memory or cognitive complaint is critically important to effective diagnosis, treatment, education, and support. This session will assist learners in understanding the three major cognitive stages: normal, mild cognitive impairment and dementia and understand why cognition should be assessed, understand the BCAT Gold Standard test systems and be able to apply test results to optimize care and promote the highest practicable functioning level. 2
Transcript
6/16/2015
1
The BCAT Approach: The Gold Standard in Rapid Assessment and Treatment of Cognitive Disorders in Older Adults
Proficiency in the cognitive assessment of persons who have a subjective or objective memory or cognitive complaint is critically important to effective diagnosis, treatment, education, and support. This session will assist learners in understanding the three major cognitive stages: normal, mild cognitive impairment and dementia and understand why cognition should be assessed, understand the BCAT Gold Standard test systems and be able to apply test results to optimize care and promote the highest practicable functioning level.
2
6/16/2015
2
Course Outline
• What is cognition and why should it be assessed?
• What is the BCAT Approach?
• The BCAT Interventions
• BCAT Science – Empirical Evidence
• Why is the BCAT Approach Important?
3
Section I
What is cognition and
why should it be assessed?
4
6/16/2015
3
• Over 5 million people have Alzheimer’s disease (AD), anticipated to be 13‐16 million by 2050
• Numbers are vastly greater if you include other dementias and people with Mild Cognitive Impairment (MCI)
• MCI dementia conversion rates (10‐15% annually)
• A majority of MCI patients will develop dementia within 3‐5 years.
Background5
The Assisted Living Resident of Today in Cognitive Terms
• In 2000, approximately 50% of ALF residents had a diagnosable cognitive impairment
• In 2010, 75‐80% of ALF residents have a diagnosable cognitive impairment
• 750,000 individuals currently residing in ALF communities
6
6/16/2015
4
Cognitive Functioning of ALF Residents: A Bird’s Eye View
• 20% of residents are cognitively “Normal”
• 30% of residents have Mild Cognitive Impairment
• 50% of residents have Dementia (at varying stages)
7
What is Cognition?
• Cognition is the sixth “vital sign”
• Cognition is at the center of our experience
• Cognition consists of multiple domains
• Cognition is a fluid process
• Cognitive Task Manager (Attention, Contextual Memory, and Executive Functions)
8
6/16/2015
5
Review of the Cognitive Continuum
The Three Cognitive Stages: “Bird’s Eye View”
• Normal: Inefficiencies but not pathology
• MCI: The four subtypesAmnestic (aMCI)
Executive (eMCI)
Multi‐domain (mMCI)
Undifferentiated (uMCI) or “pre‐MCI”
• MCI conversions to dementia
• Dementia: Mild, Moderate, & Severe
9
The Three Cognitive Stages (continued)
• Dementia: A matter of degree
Progressive
Cognitive, mood, behavior, function
Causes (multiple)
Background 10
6/16/2015
6
Working Memory
• Temporary storage and management of information
• Lasts <30 seconds (more like 10‐15 seconds)
• 4‐5 pieces of new information
11
Working Memory
• Critical for improving memory
• Critical for buffering against future declines
• Consists of two phases
Attention
Cognitive Manipulation
12
6/16/2015
7
Neuroplasticity
• Brain’s ability to re‐organize itself
• Brain forms new neural connections
• Life‐long process that occurs naturally
• Brain rehabilitation concentrates the process
13
Cognitive Reserve
• Brain’s ability to tolerate pathology and still function
• When the disease process has begun
• A method for buffering against cognitive decline
• Measures the major domains (“clusters”) of contextual memory, executive functions, attentional capacity
• Cognitive Task Manager
20
6/16/2015
11
The BCAT Short Form (BCAT – SF)
• Abbreviated version of the full BCAT
• Can be administered in about three (3) minutes
• Pulls from the three full BCAT clusters
Attention
Contextual memory
Executive functions
21
The BCAT Short Form (BCAT – SF)
• Has six items
• 21 points
• Can be scored online
• Has a test report
• “Cut” scores differentiating normal cognitive functioning, Mild Cognitive Impairment and dementia
22
6/16/2015
12
Use of The BCAT Short Form (BCAT – SF)
• When time is at very short
• When the patient can’t tolerate more than a few minutes
• A quick assessment once a full BCAT baseline has been established
• Often used in primary care offices
• Used by facility admissions staff
23
The Brief Cognitive Impairment Scale (BCIS)
• Assesses cognitive function with severe dementia
• 14 items
• 18 point scale
• Can track changes in severely demented residents and can provide information to manage behavior problems
• Use when the resident scores less than 50 on the BCAT
24
6/16/2015
13
The Kitchen Picture Test (KPT)
• Visually presented test of practical judgment
• Pictures a kitchen scene with 3 potentially dangerous situations unfolding
• The individual is asked to describe the scene as fully as he/she can and then rank the order of importance of each situation in terms of its dangerousness, and then offer solutions that would resolve the three problems
25
The Kitchen Picture Test (KPT) (cont.)
• Successfully measures the construct of judgment
• Can be used to differentiate between those who have dementia and those who don’t
26
6/16/2015
14
The Brief Anxiety and Depression Scale (BADS)
• “Process screening instrument” that can rapidly assess anxiety and depression status
• Has separate depression and anxiety scores
• Cannot make a mood diagnosis on the basis of the BADS alone, however, this measure is highly accurate in identifying individuals with a high likelihood of having a clinical anxiety and/or depression diagnosis
27
The Brief Anxiety and Depression Scale (BADS)
• 8 questions
• Takes less than 5 minutes
• Can track mood over time
• Can be administered by a clinician, proxy* or as a self‐report measure
• Provides useful real‐time information
• Can be used with the cognitively intact, or the cognitively impaired
28
6/16/2015
15
Section III
The BCAT Interventions
29
The BCAT Interventions
• The BCAT Working Memory Exercise Book
• The BCAT Online Brain Rehabilitation Modules
• New and coming in the next portion of slides: MemPicsTMMeaningful Engagement Books
30
6/16/2015
16
Key Tips and Guidelines
• Don’t let the perfect be the enemy of the good
• “Frustration minus 1”
• Successful exercise performance carry‐over is over‐rated
• Active versus passive therapist approach
• The three most important words: repetition, repetition, repetition
• Exercises can be modified to fit skills of your patient
• Can be used in a “restorative” model
32
6/16/2015
17
Structure of the BCAT Working Memory Exercise Book
• 15 exercise sections
• Basic versus Complex sub‐exercises
• Exercises introductions
– Background
– Procedure
– Tip
– BCAT insight
33
Application of BCAT Working Memory ExerciseBelow there are six objects. Sort them into two categories. Once this is done, attempt to memorize them. Onthe following page, list (or say) all objects by their identified category. You can try this multiple times. Aftereach attempt, you may go back and review the objects from the previous page. Then try again.
BASIC LEVEL:
34
6/16/2015
18
Application of BCAT Working Memory ExerciseCOMPLEX LEVEL:
35
Application of BCAT Working Memory ExerciseIn the box below there are 12 words. Sort them into four categories. Once this is done, attempt to memorizethem. On the following page, list (or say) all sixteen words by their category. You can try this three times.After each attempt, go back and review the words from the previous page. Then try again.
36
6/16/2015
19
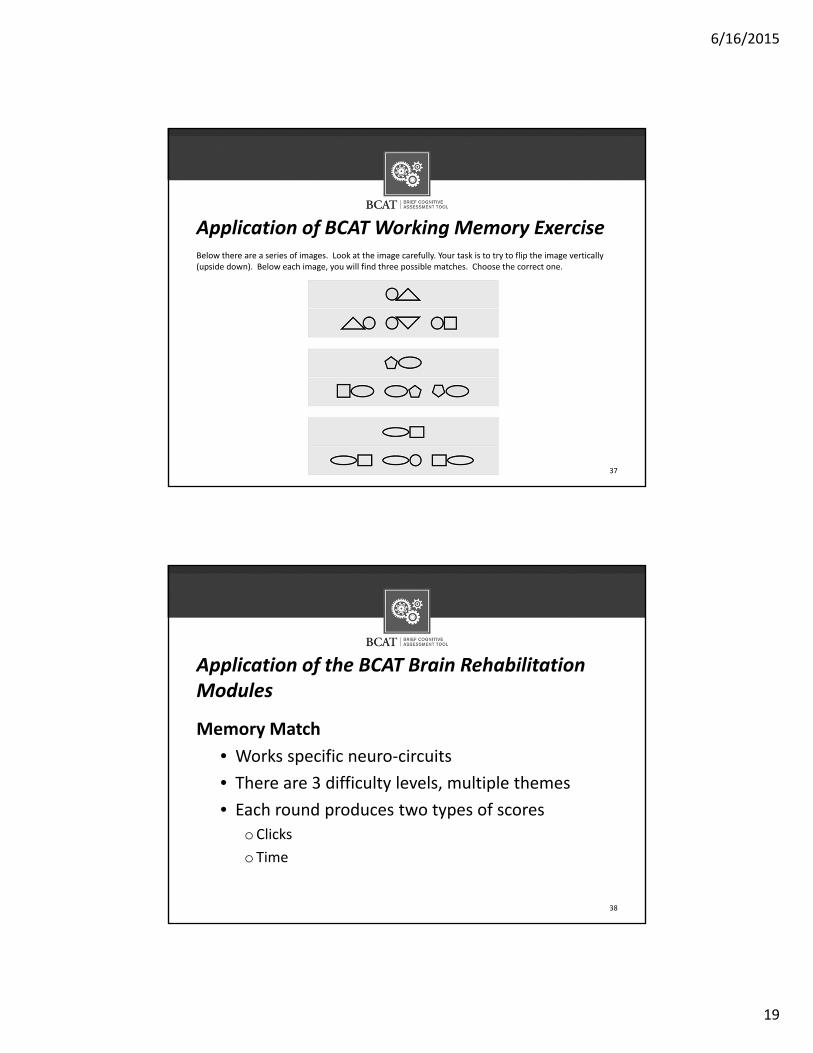
Application of BCAT Working Memory ExerciseBelow there are a series of images. Look at the image carefully. Your task is to try to flip the image vertically (upside down). Below each image, you will find three possible matches. Choose the correct one.
37
Application of the BCAT Brain Rehabilitation Modules
Memory Match
• Works specific neuro‐circuits
• There are 3 difficulty levels, multiple themes
• Each round produces two types of scores
oClicks
o Time
38
6/16/2015
20
Memory Match: Level 2, Animal Kingdom Theme
39
Memory Match: Level 2, Animal Kingdom Theme
40
6/16/2015
21
Application of 3 BCAT Brain Rehabilitation Modules
Sort the Set
• Focuses on attention and cognitive set‐shifting
• Set‐shifting is an essential executive function
• Requires the patient to change cognitive sets, through switching between specific categories
41
Application of 3 BCAT Brain Rehabilitation Modules
Sort the Set (continued)
• Works specific neuro‐circuits
• There are 3 difficulty levels
• Each round produces two types of scores (attempts, time)
42
6/16/2015
22
Sort the Set: Level 1
43
Sort the Set: Level 2
44
6/16/2015
23
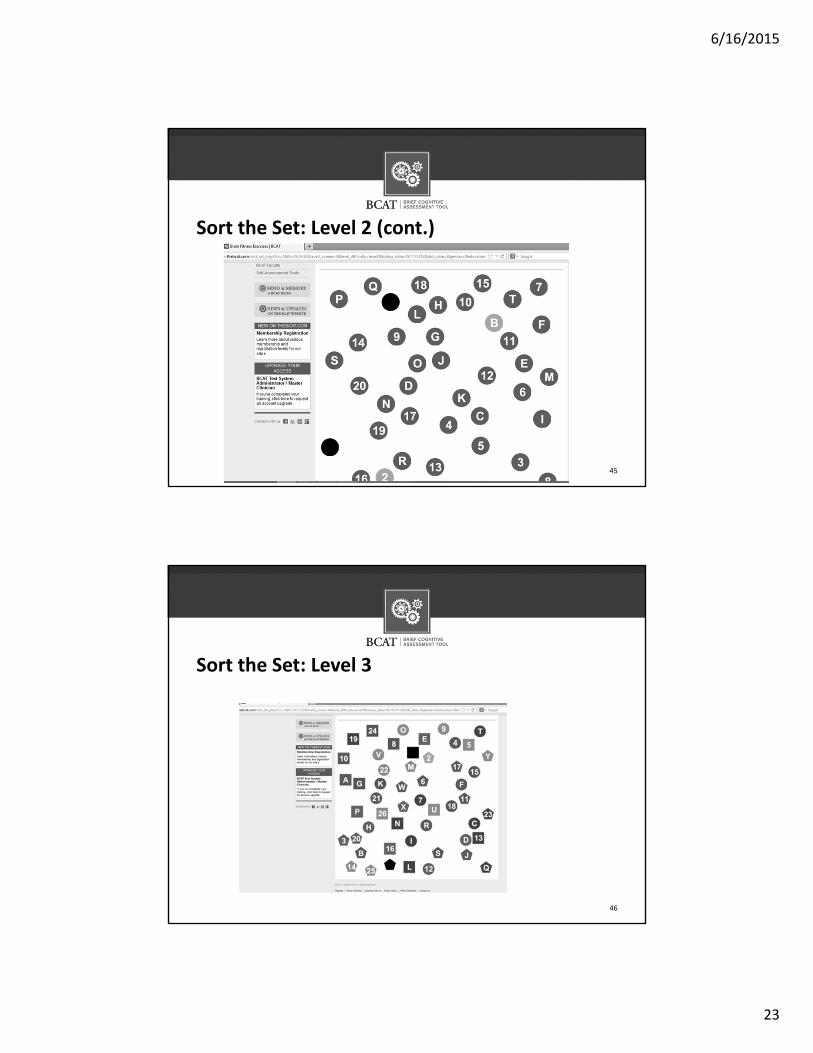
Sort the Set: Level 2 (cont.)
45
Sort the Set: Level 3
46
6/16/2015
24
Application of 3 BCAT Brain Rehabilitation Modules
Color Illusion• Focuses on “selective” attention
• Selective attention is closely associated with the executive functions
• Requires the patient to selectively attend to one task while not attending to a competing task
• Requires the patient to say words out loud
• The module is not automatically scored47
48
Color Illusion: Level 1
6/16/2015
25
Section IV
BCAT Science – Empirical Evidence
49
BCAT Science – Empirical Evidence
• Can be administered by paraprofessionals or clinicians in ~15 minutes
• Sensitive to the full range of cognitive functioning (normal, MCI, dementia)