71
THE BEDSIDE PHYSIOLOGIST Yogesh Apte Intensivist, Robina Hospital
| Date post: | 14-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | oliver-flower |
| View: | 362 times |
| Download: | 0 times |
THE BEDSIDE PHYSIOLOGISTYogesh Apte
Intensivist, Robina Hospital
CASE• 47 y male
• morbidly obese, non-smoker, 2 beers a day
• H/O 5/7 worsening cough, SOB walking bed
• GP visit 2/7 ago
• ED examination
• alert, febrile T = 38’C
• HR 100/min sinus, BP 120/50 (MAP 75), warm
• RR ~ 20, few crackles bilaterally, no wheeze
• SPO2 94% HM 6 lpm O2
• Laboratory results
• WCC 25000, neutrophilia
• mild LFT derangement
• Normal Coagulation profile and albumin
• Urea 11 Creatinine 150

MET CALL
MET CALL• respiratory distress
MET CALL• respiratory distress
• RR ~ 30/min, SPO2 ~ 92% on 10 lpm HM O2
MET CALL• respiratory distress
• RR ~ 30/min, SPO2 ~ 92% on 10 lpm HM O2
• HR 120/min sinus, BP 90/50 (MAP ~ 65)
MET CALL• respiratory distress
• RR ~ 30/min, SPO2 ~ 92% on 10 lpm HM O2
• HR 120/min sinus, BP 90/50 (MAP ~ 65)
• ABG -
MET CALL• respiratory distress
• RR ~ 30/min, SPO2 ~ 92% on 10 lpm HM O2
• HR 120/min sinus, BP 90/50 (MAP ~ 65)
• ABG -
• pH 7.29 PCO2 30 PO2 70 SaO2 92%
MET CALL• respiratory distress
• RR ~ 30/min, SPO2 ~ 92% on 10 lpm HM O2
• HR 120/min sinus, BP 90/50 (MAP ~ 65)
• ABG -
• pH 7.29 PCO2 30 PO2 70 SaO2 92%
• HCO3 18, Lactate 2, Na 136 K 4.6 Cl 98
MET CALL• respiratory distress
• RR ~ 30/min, SPO2 ~ 92% on 10 lpm HM O2
• HR 120/min sinus, BP 90/50 (MAP ~ 65)
• ABG -
• pH 7.29 PCO2 30 PO2 70 SaO2 92%
• HCO3 18, Lactate 2, Na 136 K 4.6 Cl 98
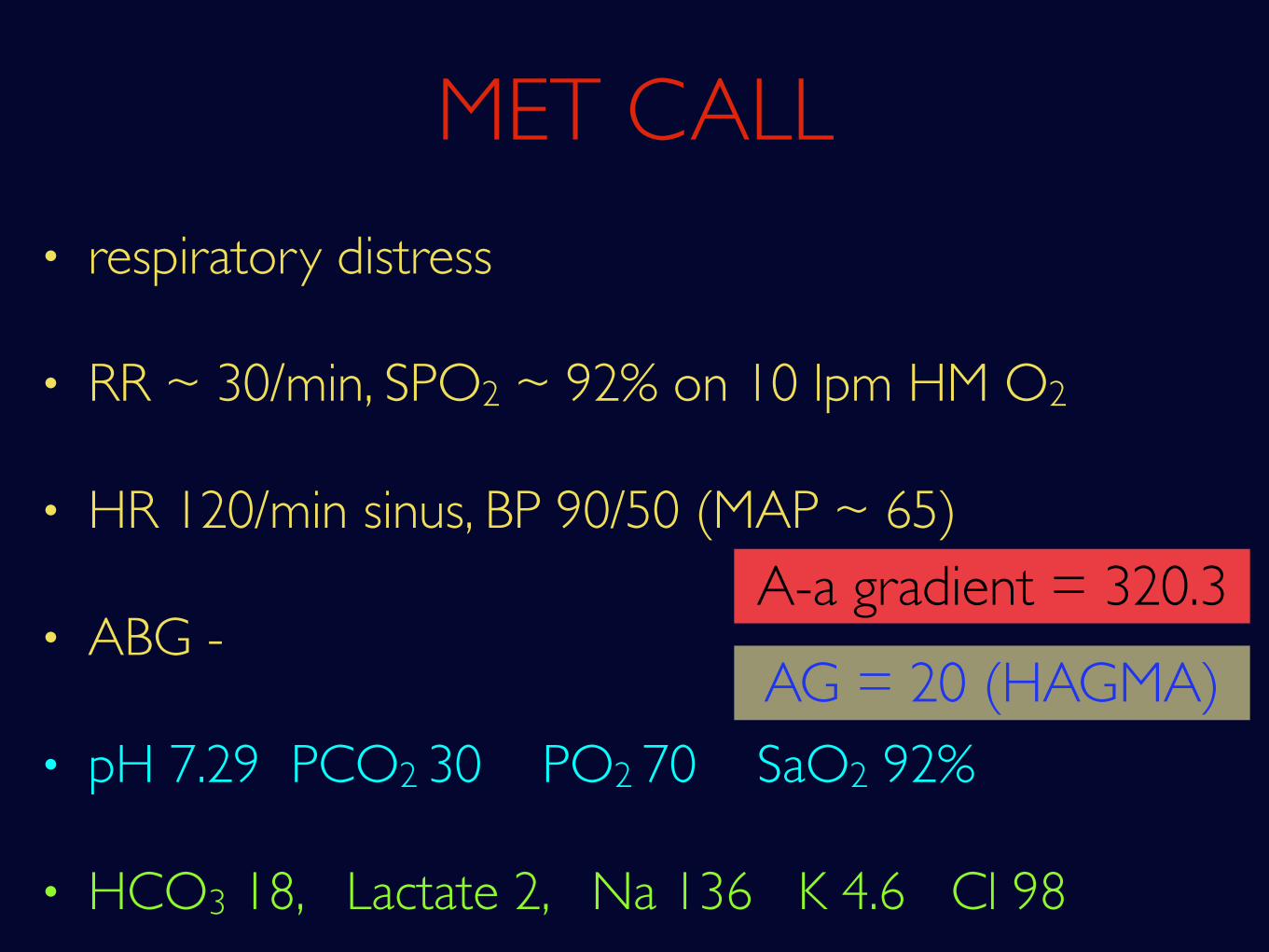
A-a gradient = 320.3
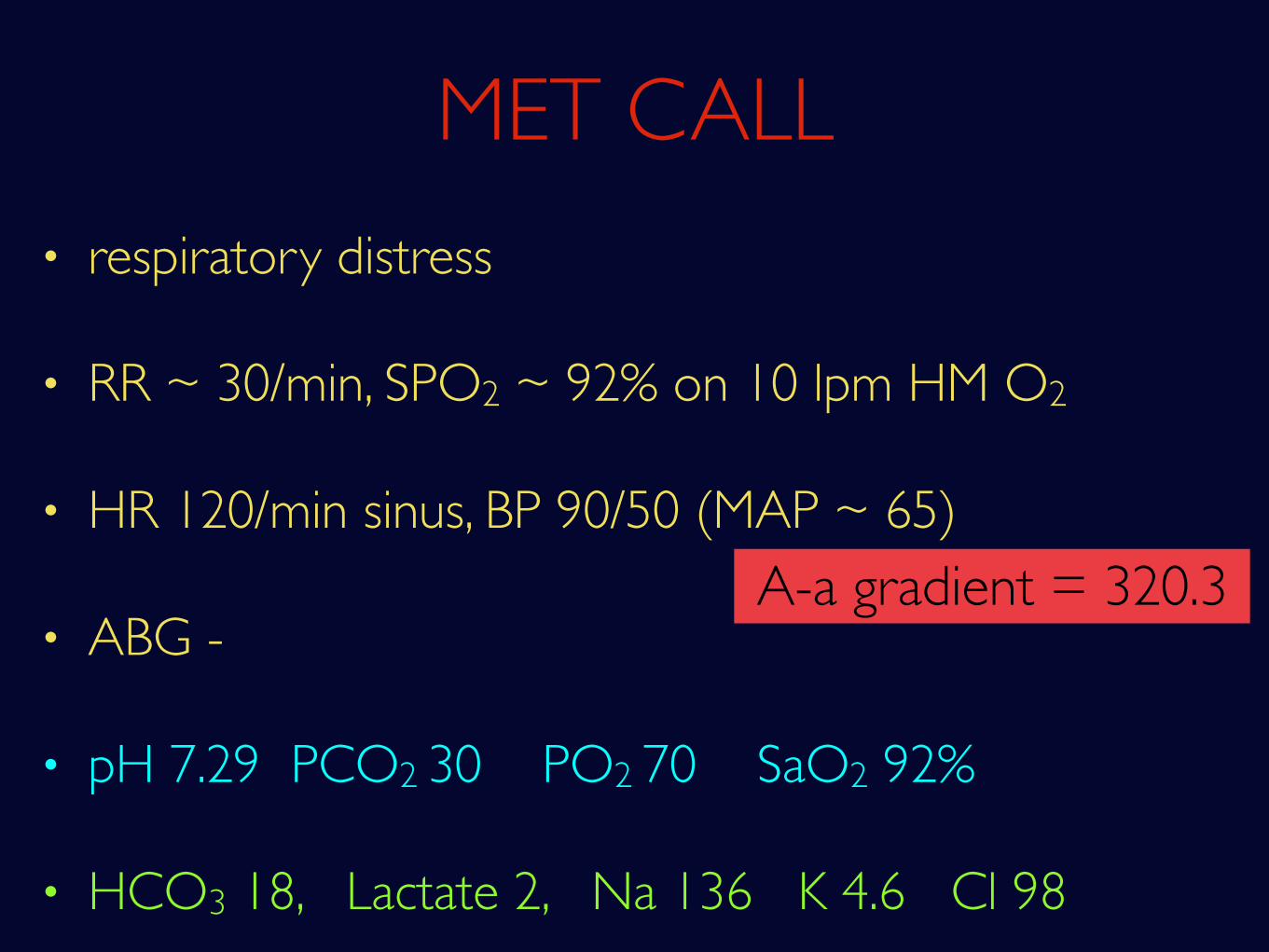
MET CALL• respiratory distress
• RR ~ 30/min, SPO2 ~ 92% on 10 lpm HM O2
• HR 120/min sinus, BP 90/50 (MAP ~ 65)
• ABG -
• pH 7.29 PCO2 30 PO2 70 SaO2 92%
• HCO3 18, Lactate 2, Na 136 K 4.6 Cl 98
AG = 20 (HAGMA)A-a gradient = 320.3
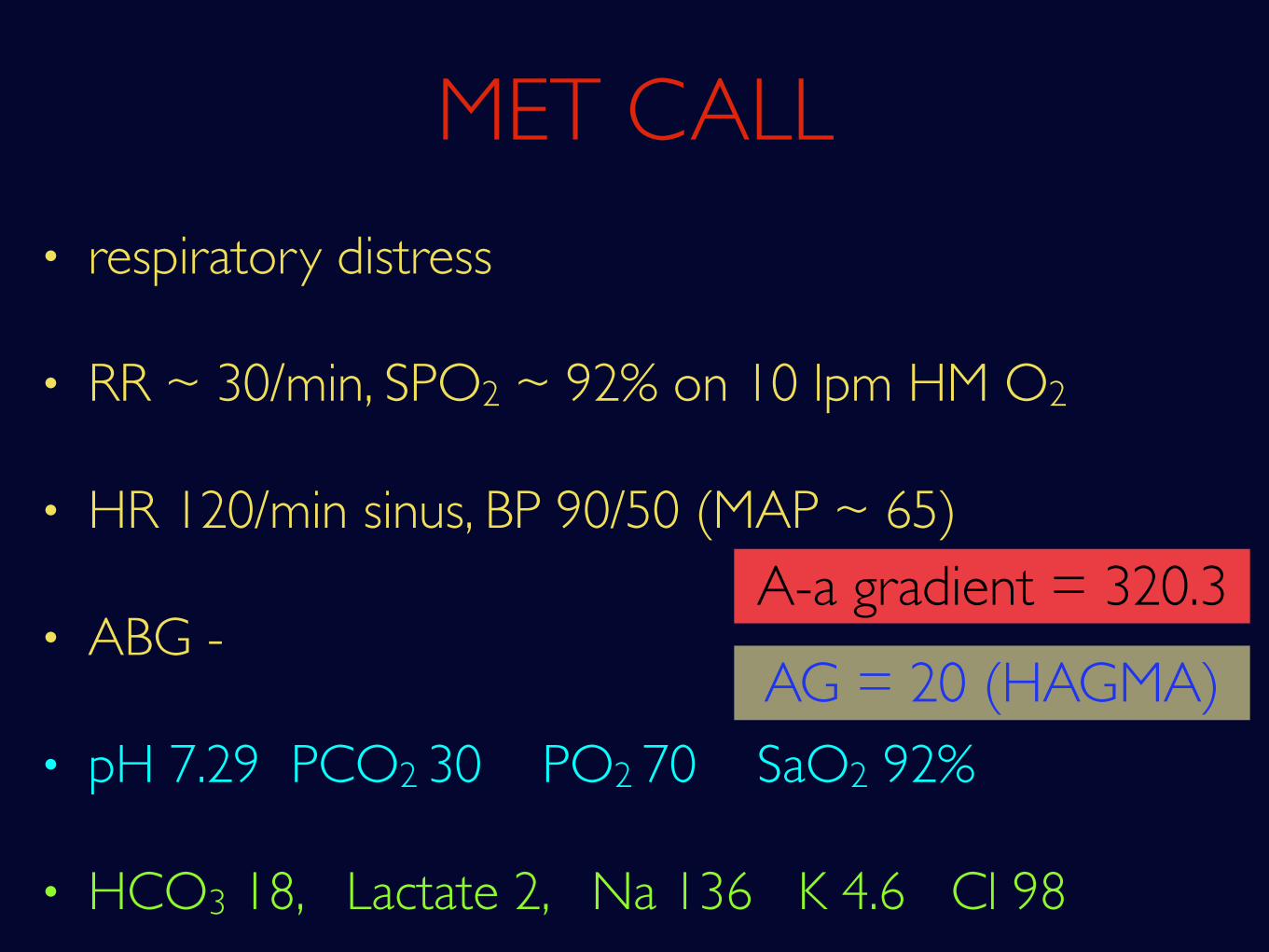
MET CALL• respiratory distress
• RR ~ 30/min, SPO2 ~ 92% on 10 lpm HM O2
• HR 120/min sinus, BP 90/50 (MAP ~ 65)
• ABG -
• pH 7.29 PCO2 30 PO2 70 SaO2 92%
• HCO3 18, Lactate 2, Na 136 K 4.6 Cl 98
AG = 20 (HAGMA)
High A-a gradient hypoxia
• Dead Space
High A-a gradient hypoxia
• Dead Space
• Shunt
High A-a gradient hypoxia
• Dead Space
• Shunt
• Diffusion defects
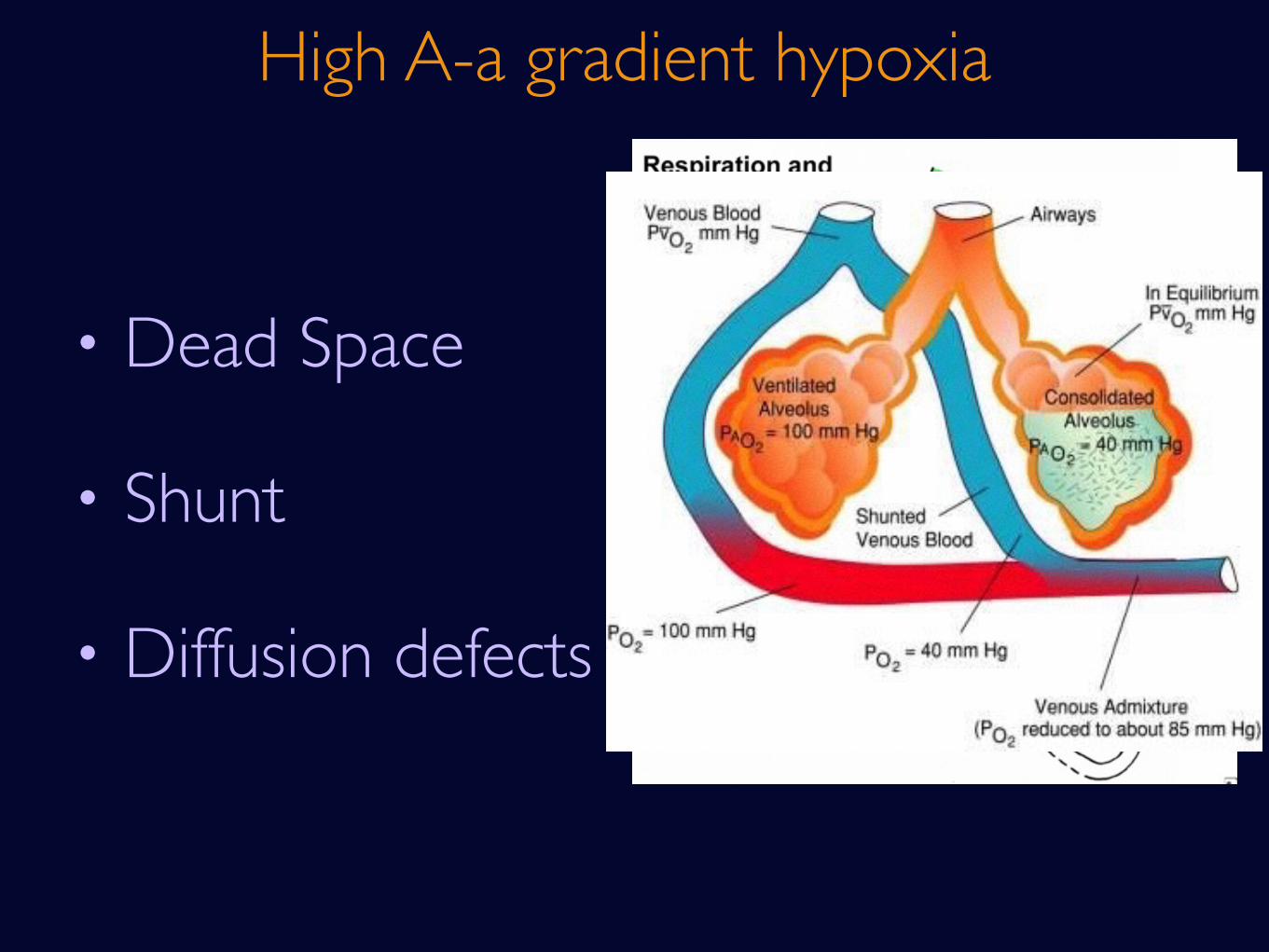
High A-a gradient hypoxia
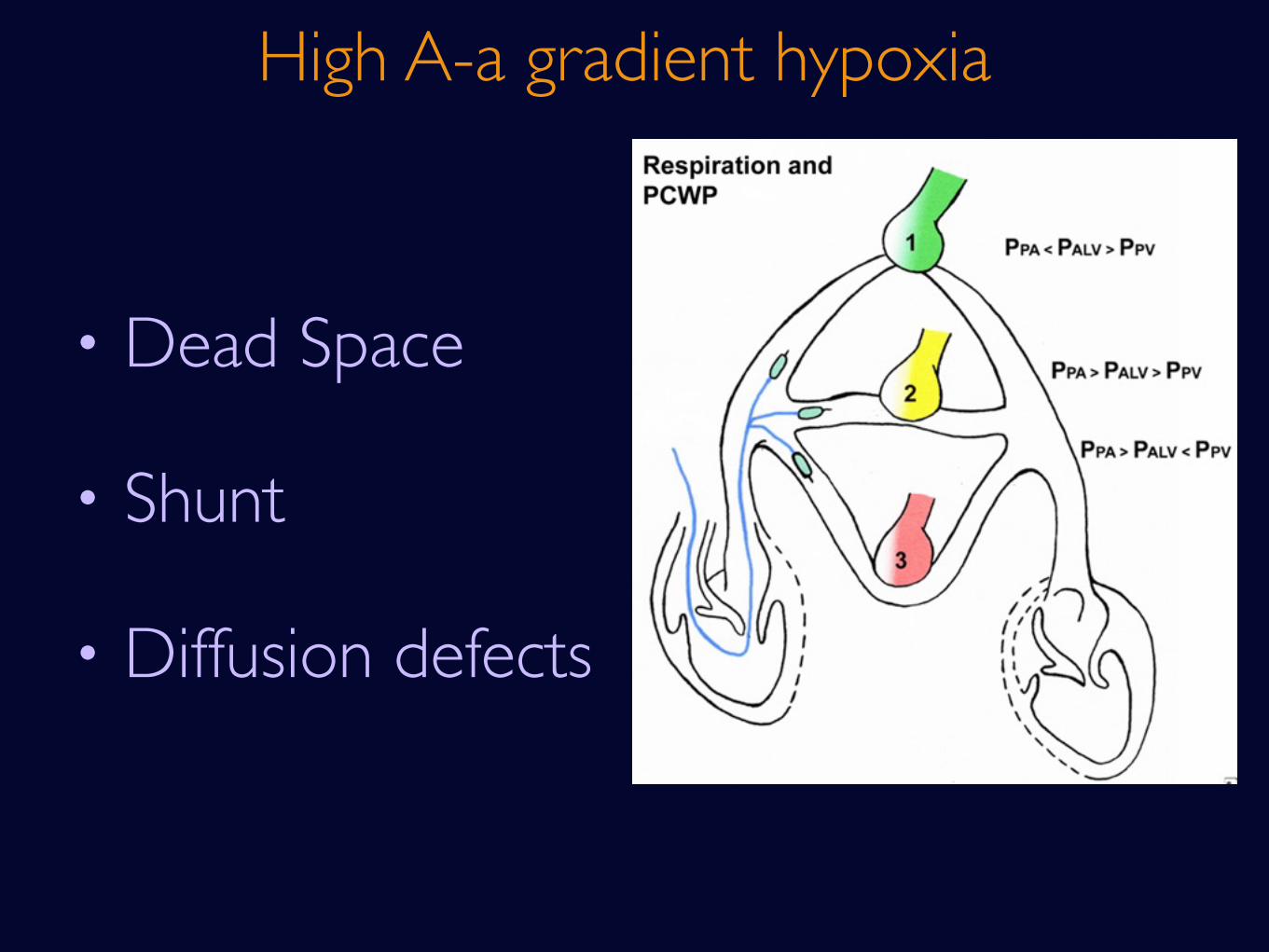
• Dead Space
• Shunt
• Diffusion defects
High A-a gradient hypoxia
• Dead Space
• Shunt
• Diffusion defects
High A-a gradient hypoxia
MET CALL• respiratory distress
• RR ~ 30/min, SPO2 ~ 92% on 10 lpm HM O2
• HR 120/min sinus, BP 90/50 (MAP ~ 65)
• ABG -
• pH 7.29 PCO2 30 PO2 70 SaO2 92%
• HCO3 18, Lactate 2, Na 136 K 4.6 Cl 98
AG = 20 (HAGMA)A-a gradient = 320.3
MET CALL• respiratory distress
• RR ~ 30/min, SPO2 ~ 92% on 10 lpm HM O2
• HR 120/min sinus, BP 90/50 (MAP ~ 65)
• ABG -
• pH 7.29 PCO2 30 PO2 70 SaO2 92%
• HCO3 18, Lactate 2, Na 136 K 4.6 Cl 98
A-a gradient = 320.3
HAGMA
M - methanol U - uremia (AKI)
HAGMA
M - methanol U - uremia (AKI)
D - DKA P - paraglutamic acid
HAGMA
M - methanol U - uremia (AKI)
D - DKA P - paraglutamic acid
I - INH, Iron L - lactic acidosis
HAGMA

M - methanol U - uremia (AKI)
D - DKA P - paraglutamic acid
I - INH, Iron L - lactic acidosis
E - ethylene glycol R - rhabdomyolysis
HAGMA
M - methanol U - uremia (AKI)
D - DKA P - paraglutamic acid
I - INH, Iron L - lactic acidosis
E - ethylene glycol R - rhabdomyolysis
S - salicylates, sepsis
HAGMA
MET CALL• respiratory distress
• RR ~ 30/min, SPO2 ~ 92% on 10 lpm HM O2
• HR 120/min sinus, BP 90/50 (MAP ~ 65)
• ABG -
• pH 7.29 PCO2 30 PO2 70 SaO2 92%
• HCO3 18, Lactate 2, Na 136 K 4.6 Cl 98
AG = 20 (HAGMA)A-a gradient = 320.3

• Hypoxic respiratory failure due to severe CAP and morbid obesity
• Septic shock with MODS
What we know
• Cardiac function
• Bug
• Respiratory mechanics-dynamics
Unknowns
• BiPAP 100% pre-oxygenation
• IAL inserted - MAP 50
• RIJ CVC inserted - CVP 12 cm H2O
• ScvO2 80%
• BiPAP 100% pre-oxygenation
• IAL inserted - MAP 50
• RIJ CVC inserted - CVP 12 cm H2O
• ScvO2 80%
CVP
• BiPAP 100% pre-oxygenation
• IAL inserted - MAP 50
• RIJ CVC inserted - CVP 12 cm H2O
• ScvO2 80%
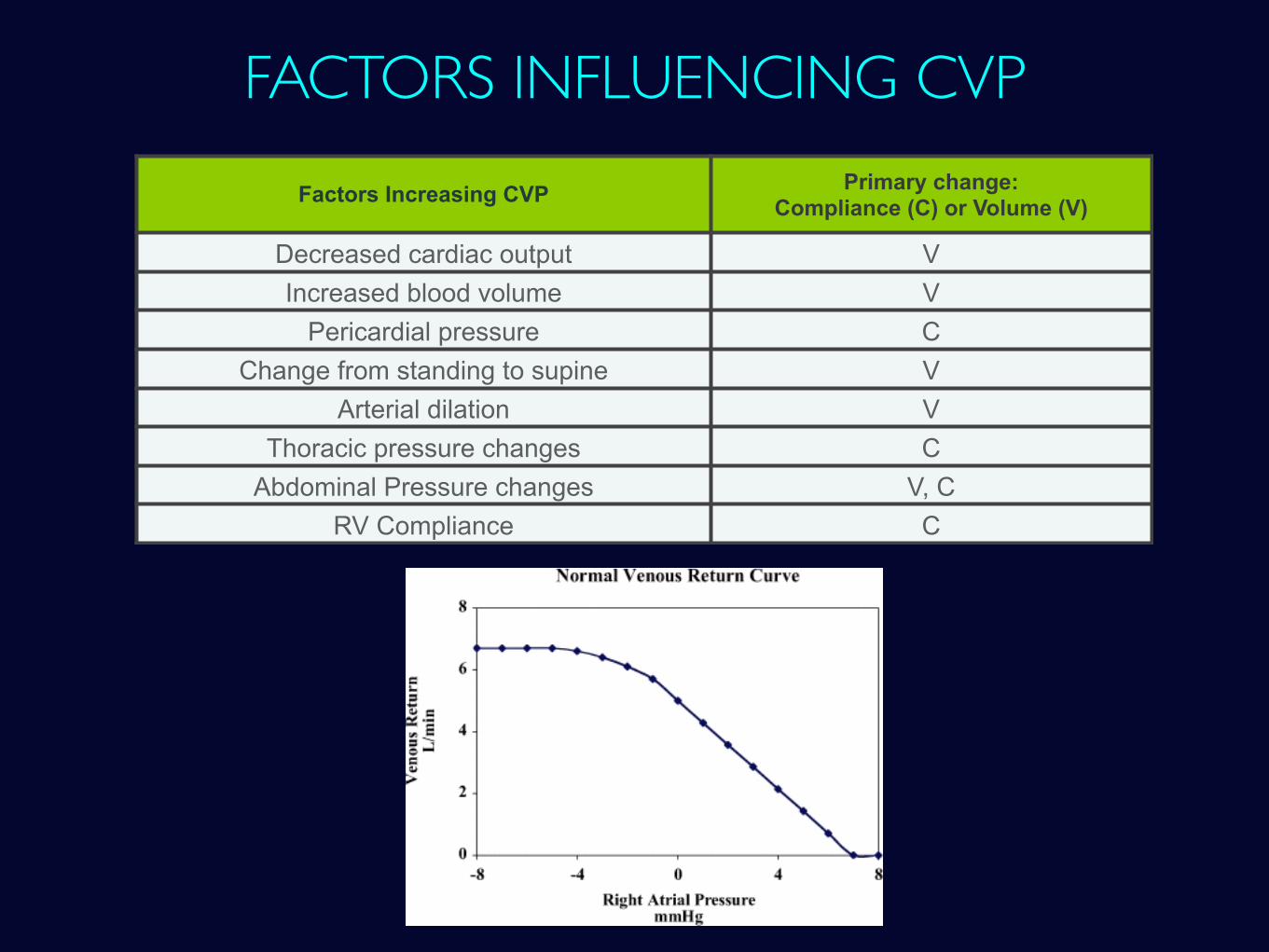
FACTORS INFLUENCING CVPFactors Increasing CVP Primary change:
Compliance (C) or Volume (V)
Decreased cardiac output VIncreased blood volume V
Pericardial pressure CChange from standing to supine V
Arterial dilation VThoracic pressure changes C
Abdominal Pressure changes V, CRV Compliance C
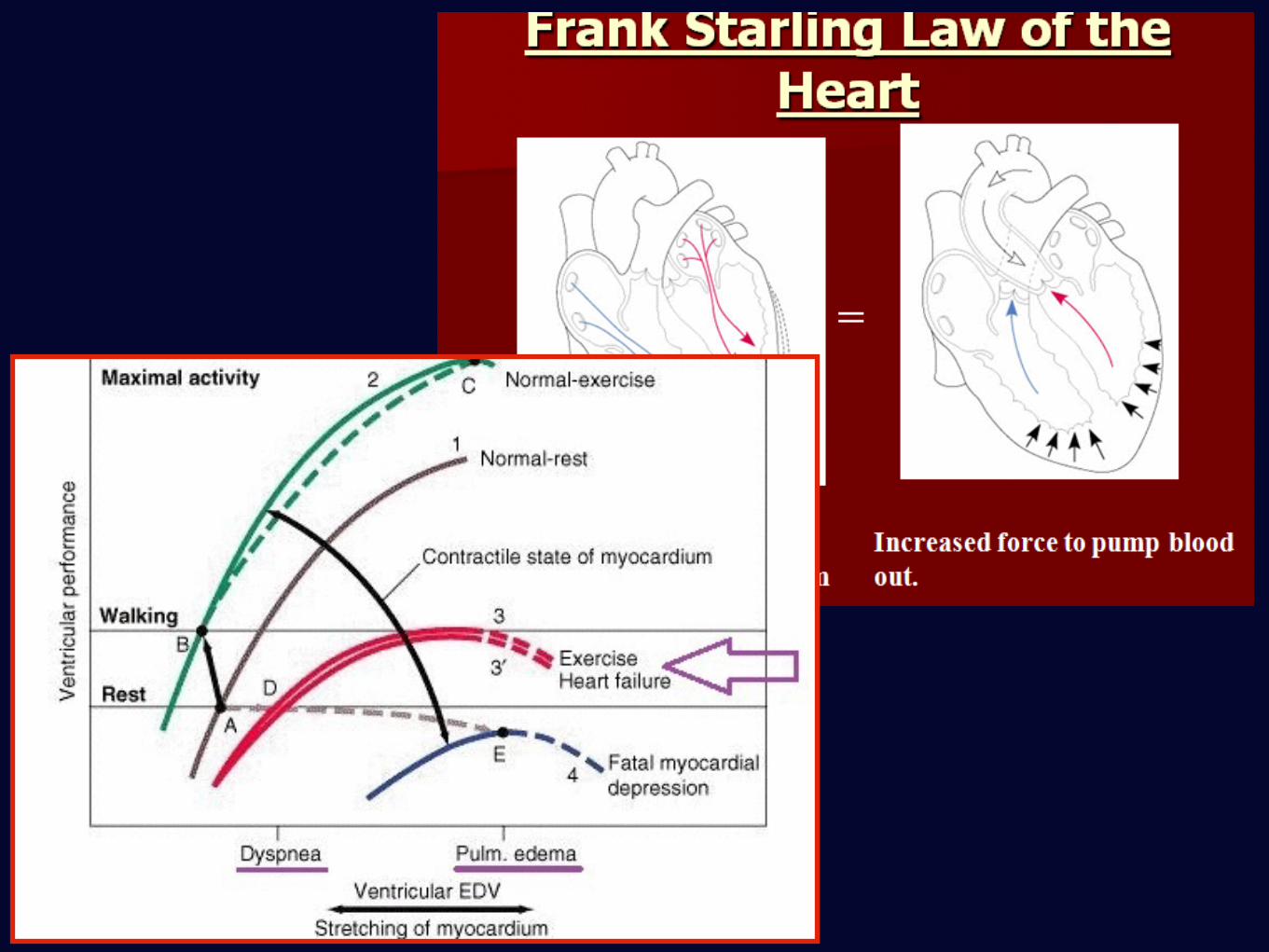
The only reason to give fluid challenge in critically ill patients should be to improve their
cardiac output.
“Filling up the tank” shows no understanding of human physiology.
SCVO2
• O2 consumption = O2 delivery x O2ER
SCVO2
• O2 consumption = O2 delivery x O2ER
• VO2 = DO2 x O2ER
SCVO2
• O2 consumption = O2 delivery x O2ER
• VO2 = DO2 x O2ER
• O2ER =VO2 / DO2
SCVO2
• O2 consumption = O2 delivery x O2ER
• VO2 = DO2 x O2ER
• O2ER =VO2 / DO2
• SVO2 = 1 - O2ER
SCVO2
• O2 consumption = O2 delivery x O2ER
• VO2 = DO2 x O2ER
• O2ER =VO2 / DO2
• SVO2 = 1 - O2ER
• Normal SVO2 = 75%
SCVO2
SCVO2
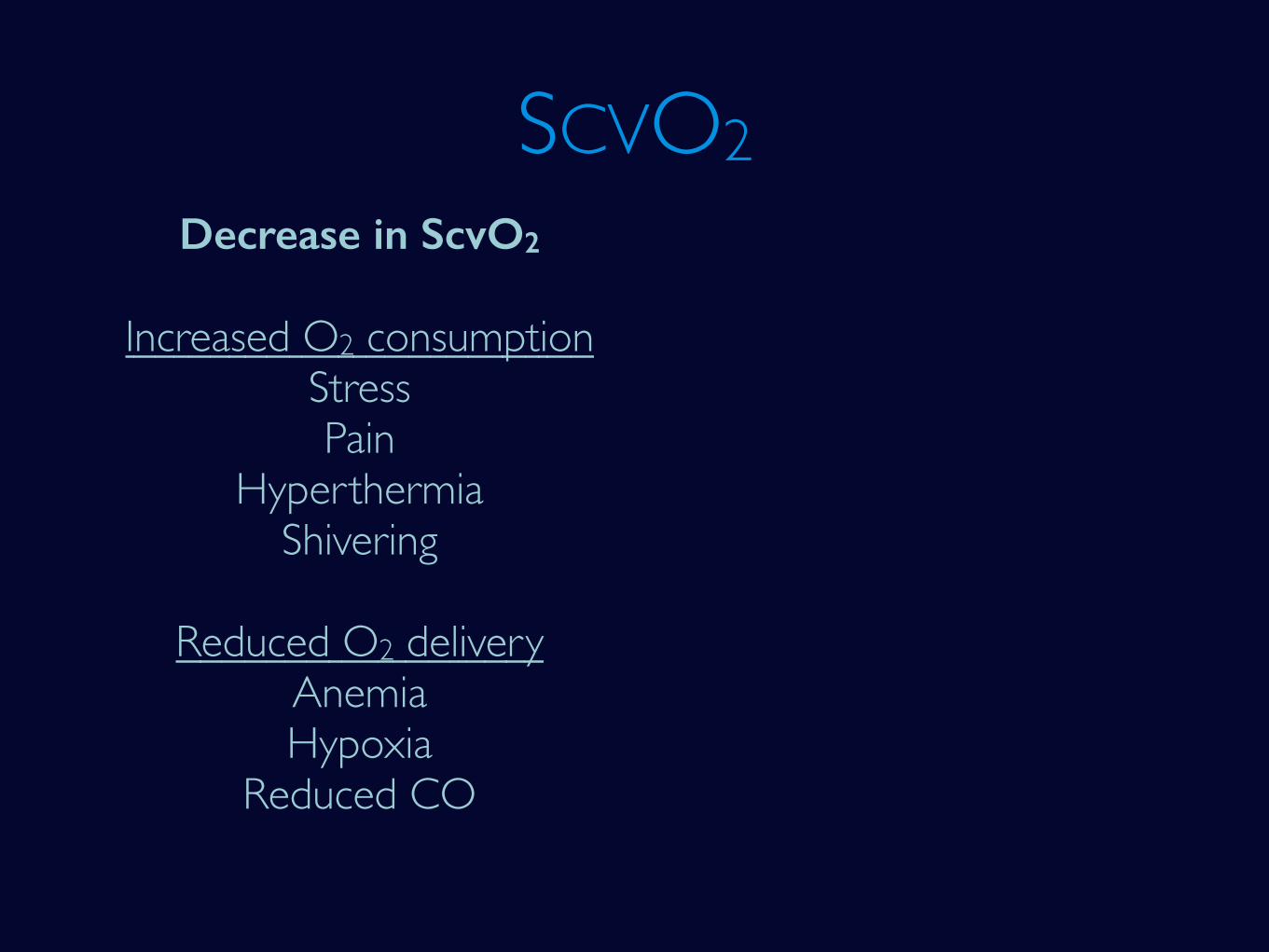
SCVO2Decrease in ScvO2
Increased O2 consumptionStressPain
HyperthermiaShivering
Reduced O2 deliveryAnemiaHypoxia
Reduced CO
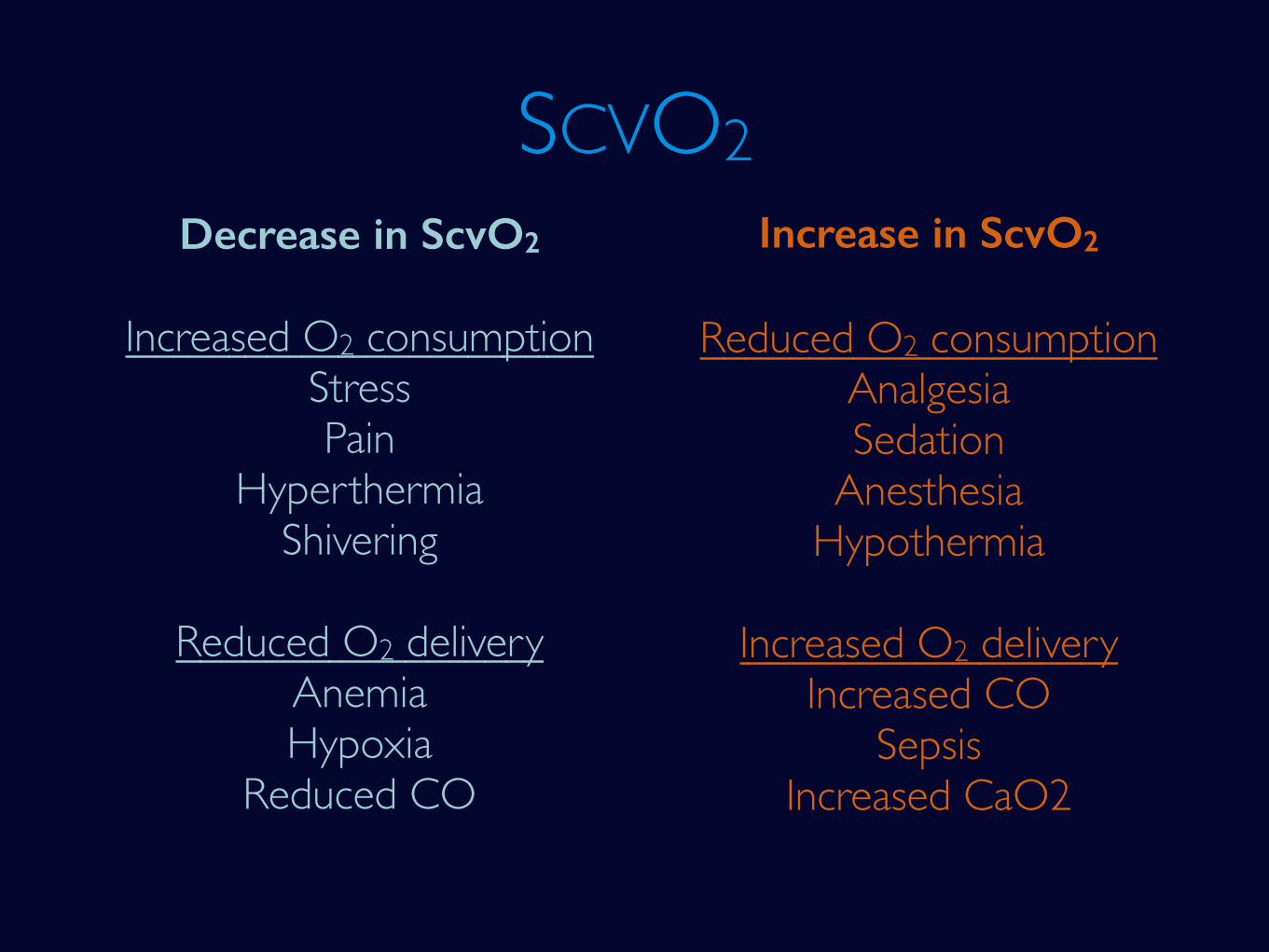
SCVO2Decrease in ScvO2
Increased O2 consumptionStressPain
HyperthermiaShivering
Reduced O2 deliveryAnemiaHypoxia
Reduced CO
Increase in ScvO2
Reduced O2 consumptionAnalgesiaSedation
AnesthesiaHypothermia
Increased O2 deliveryIncreased CO
SepsisIncreased CaO2
• No more fluids given
• Noradrenaline started
• RSI, intubated using C-Mac Grade II larynx

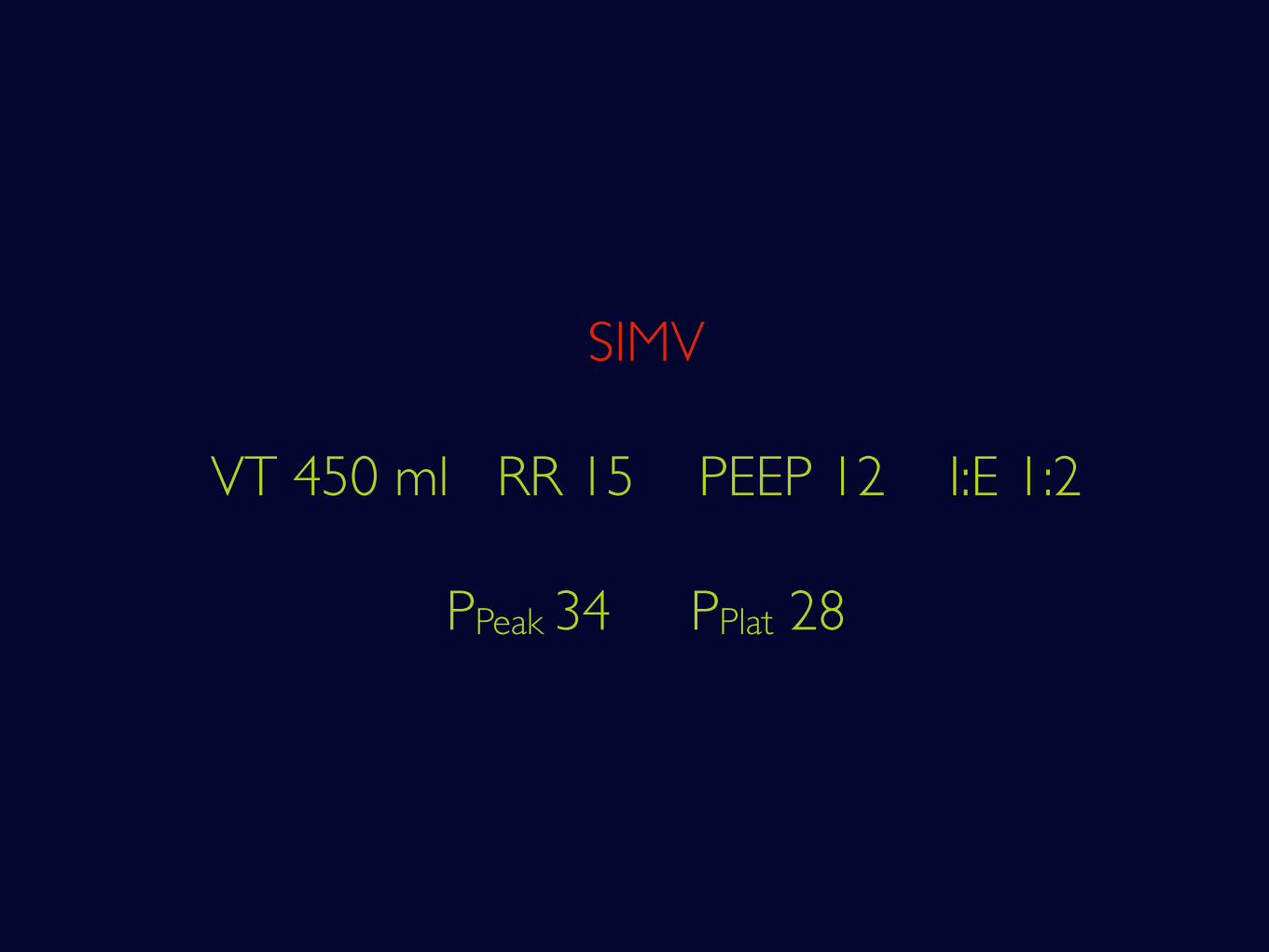
SIMV
VT 450 ml RR 15 PEEP 12 I:E 1:2
PPeak 34 PPlat 28
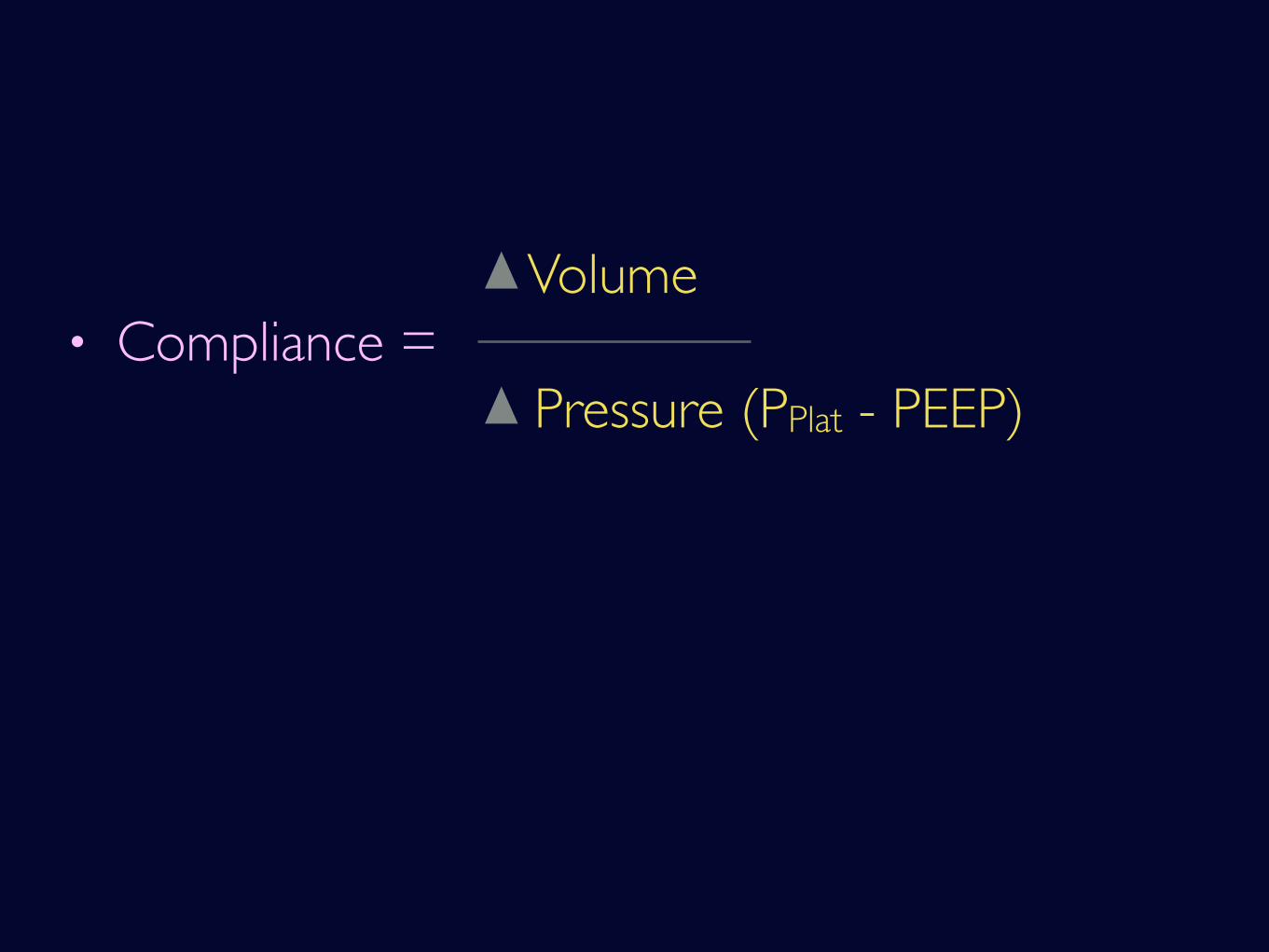
Volume
Pressure (PPlat - PEEP) • Compliance =
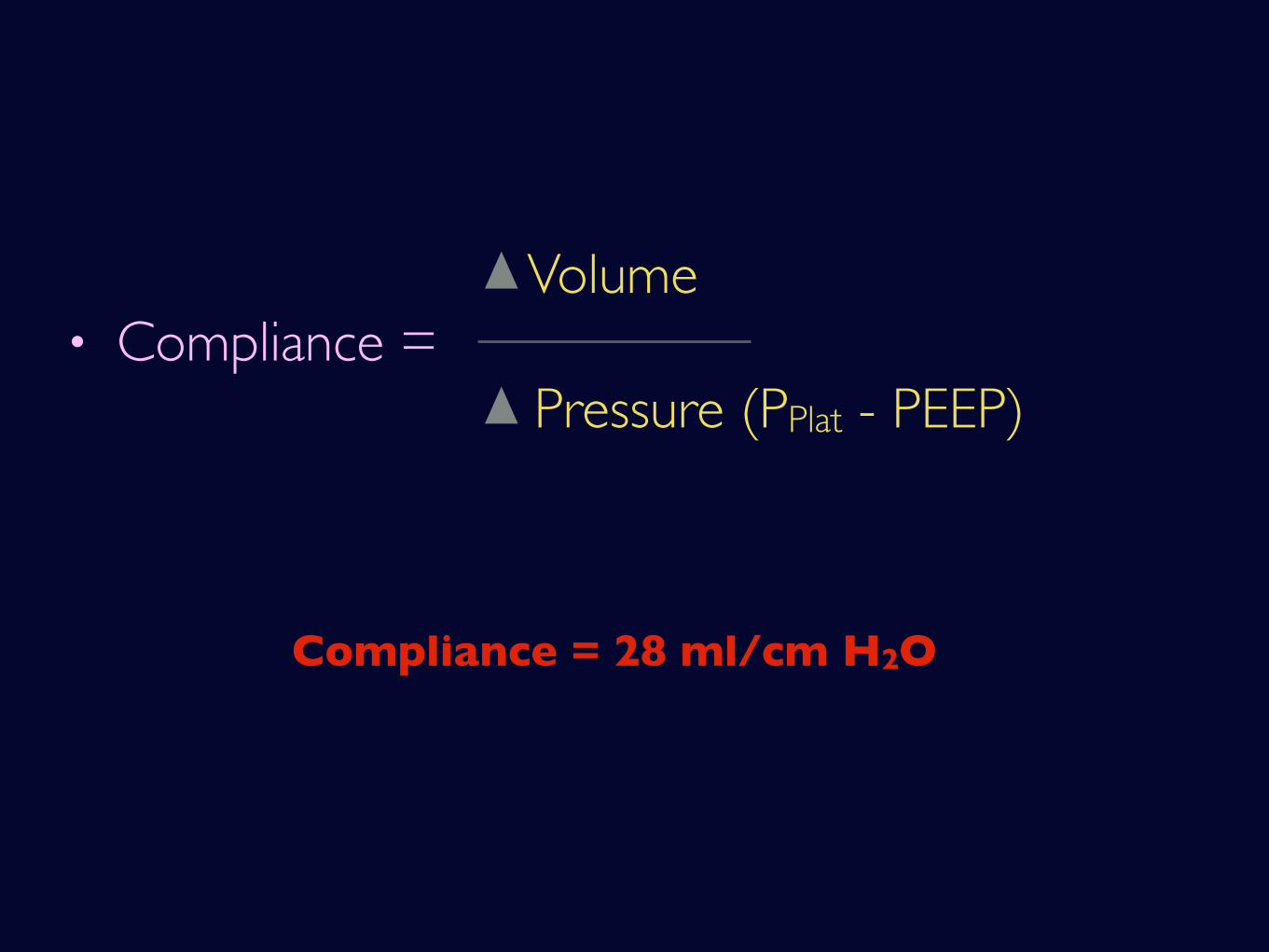
Volume
Pressure (PPlat - PEEP) • Compliance =
Compliance = 28 ml/cm H2O
Volume
Pressure (PPlat - PEEP) • Compliance =
Compliance = 28 ml/cm H2O
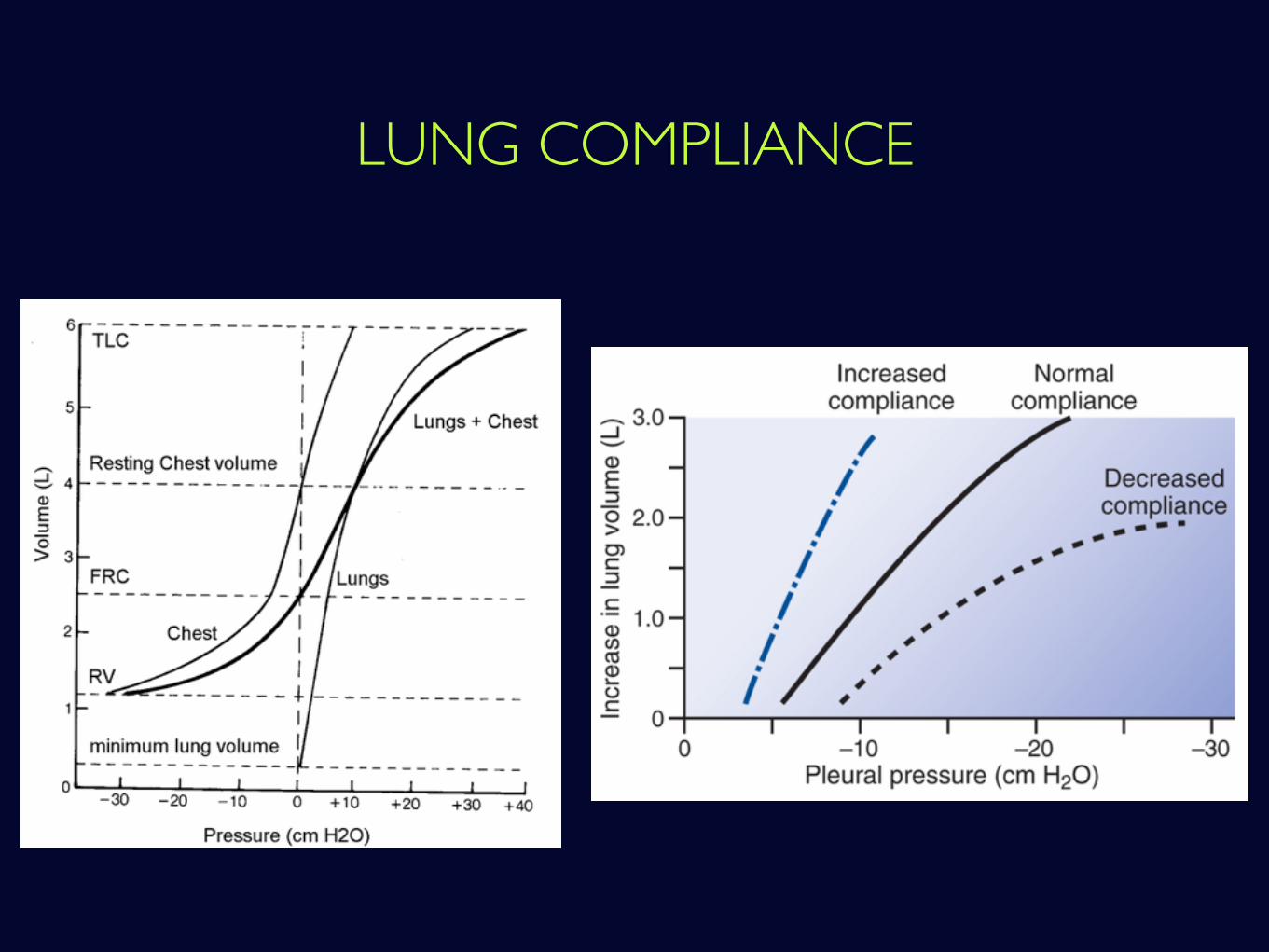
LUNG COMPLIANCE
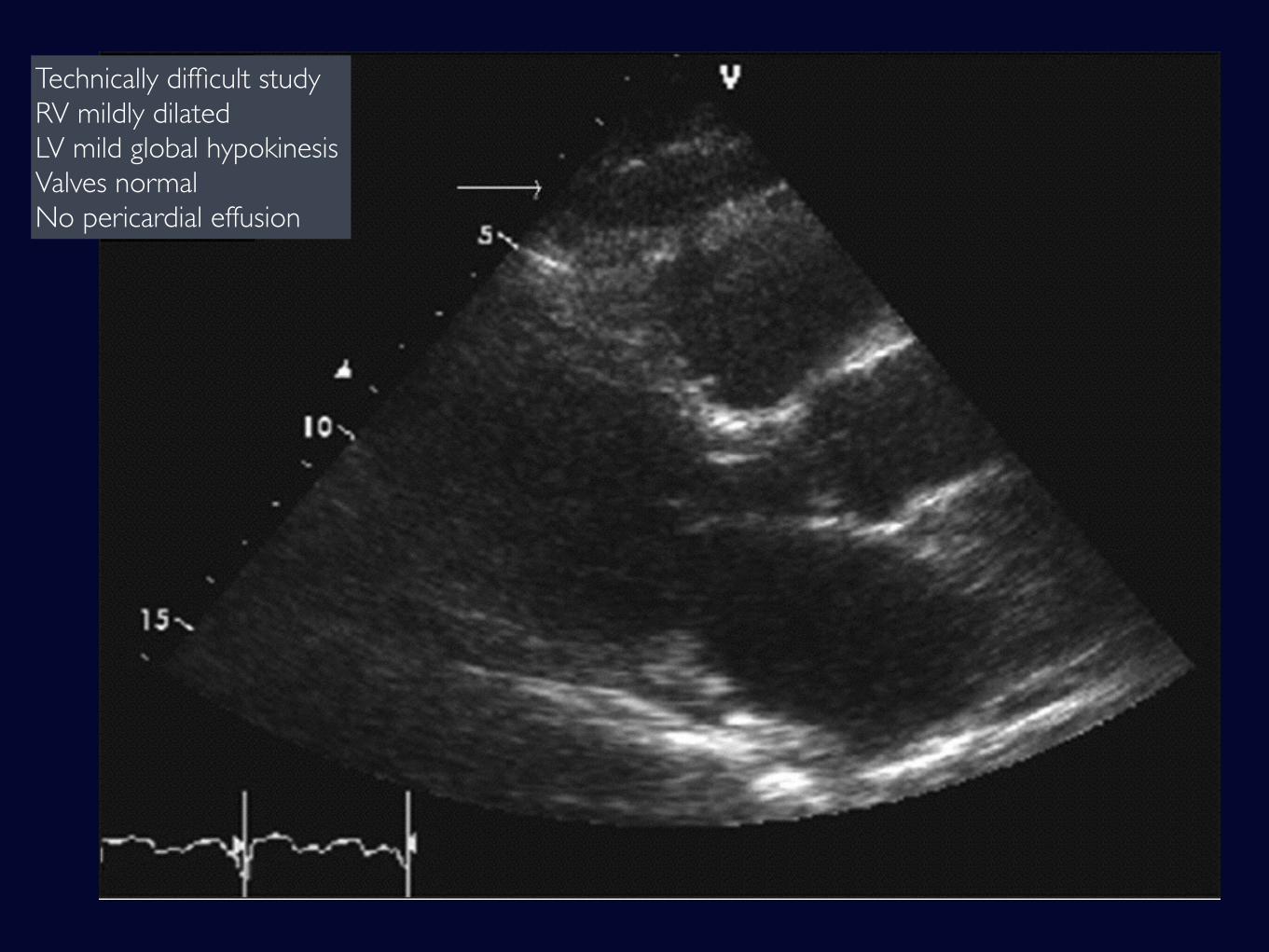
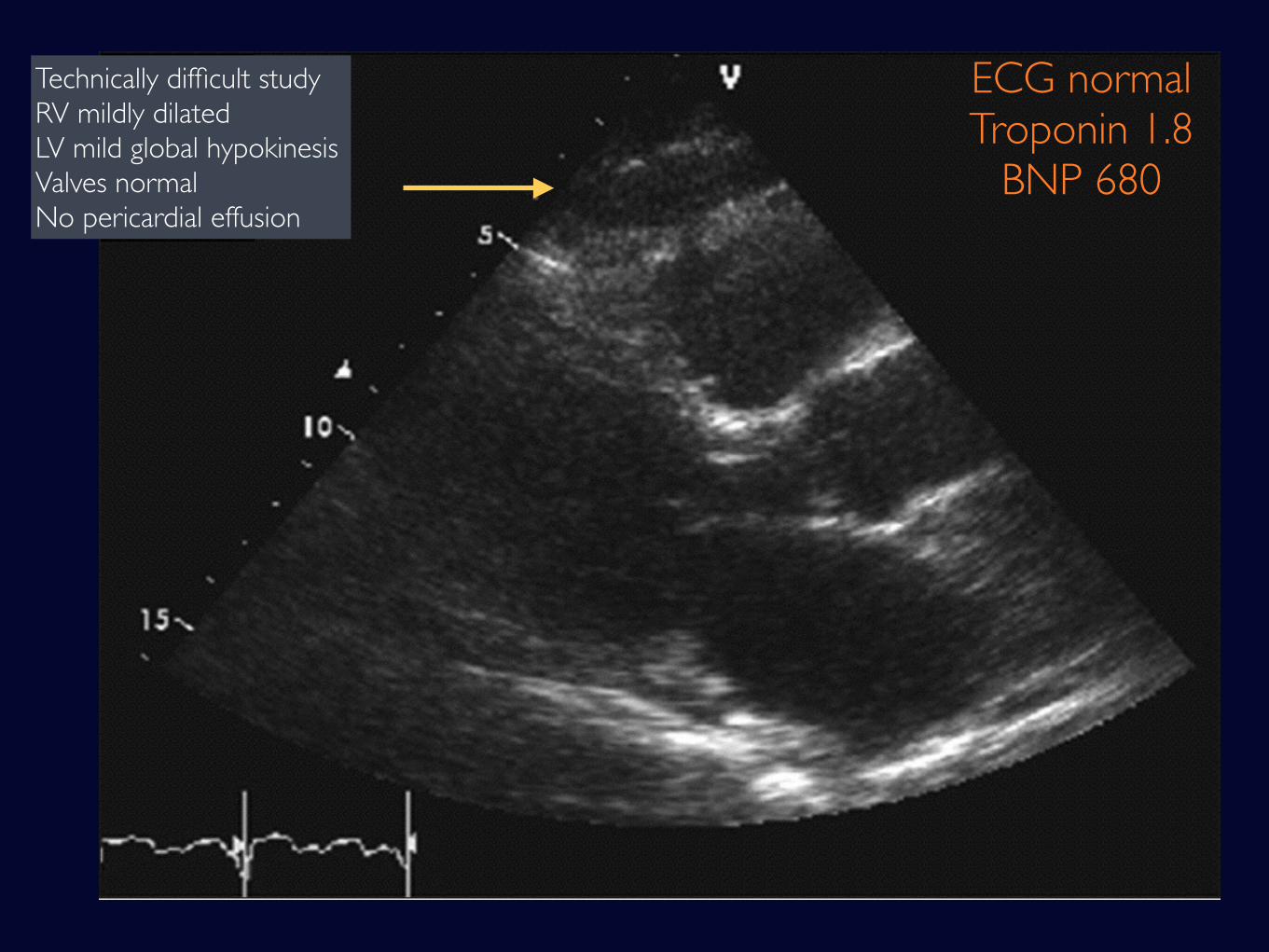
Technically difficult studyRV mildly dilatedLV mild global hypokinesisValves normalNo pericardial effusion
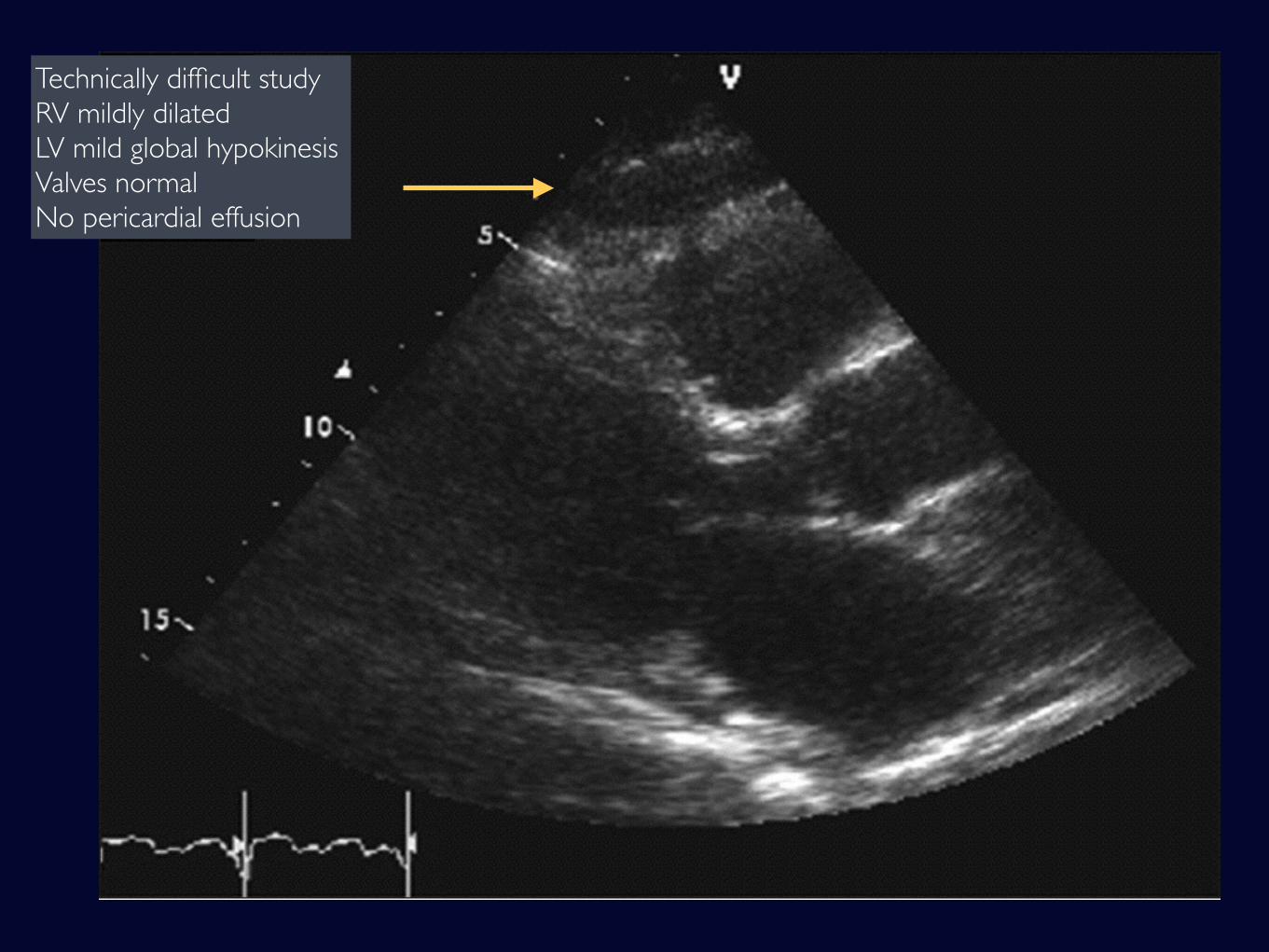
Technically difficult studyRV mildly dilatedLV mild global hypokinesisValves normalNo pericardial effusion
Technically difficult studyRV mildly dilatedLV mild global hypokinesisValves normalNo pericardial effusion
ECG normalTroponin 1.8
BNP 680
Further strategies
• Diuretics
• Recruitment
• Nitric Oxide
• Prostacyclin
• Proning
• ECMO
Further strategies
Progress
• Vasopressin added to NorAd
Progress
• Vasopressin added to NorAd
• Dialysed (SLEDD x 5 treatments)
Progress
• Vasopressin added to NorAd
• Dialysed (SLEDD x 5 treatments)
• Tracheostomy D6 ICU
Progress
• Vasopressin added to NorAd
• Dialysed (SLEDD x 5 treatments)
• Tracheostomy D6 ICU
• Sputum: Klebsiella Pneumoniae - sensitive toTazocin
Progress
• Vasopressin added to NorAd
• Dialysed (SLEDD x 5 treatments)
• Tracheostomy D6 ICU
• Sputum: Klebsiella Pneumoniae - sensitive toTazocin
• Discharged from ICU on D19 and to home D56
Progress
Eyes see what your brain knows.
Eyes see what your brain knows.
What our eyes can't see, the brain fills in.

















