SCIENTIFIC ARTICLES The Biometry of Mandibular Osteotomy Repair MONTY REITZIK, MB, CHB, FDSRCS* The healing of experimental mandibular osteotomies in monkeys was monitored by biometric testing. Results indicate that full strength returns to the osteotomy site in 20 weeks. The implications for the treatment of osteotomies and fractures of the mandible in humans are discussed. Relapse following the surgical correction of man- dibular malposition has been extensively docu- mented.lp4 A detailed cephalometric study of long- term “relapse” in both the distal and the proximal segments of the surgically corrected prognathic mandible has revealed a consistent pattern of spatial changes in both fragments following the removal of maxillomandibular fixation. These changes are al- most certainly due to muscle action upon a weak bone scar at the osteotomy site.5 Considerable attention has been directed toward modification of muscle activity in an attempt to re- duce or avoid relapse.l~“-s The use of neck braces,“,‘” suprahyoid myotomy,” and prolonged maxilloman- dibular fixation by elastic traction’ have all been reported with variable results. Hirose’ uses maxillo- mandibular elastics for six months following sur- gery to achieve a stable result. Pitkin collars and neck braces9 are also used for considerable periods. The length of time that muscle modification is re- quired to prevent relapse depends on the time that it takes for the osteotomy site to reach sufficient strength to withstand the resultant forces of the pterygomasseteric sling and the other muscles of mastication.” The question thus arises: How long does it take for a mandibular osteotomy site to heal completely? The healing of fractured bones has been exten- sively investigated. The long bone mode11L~‘5 has usually been used in the past, as it is easily accessi- ble in vivo, experimental fractures can be induced surgically, and healing can be readily monitored. Clinical evidence of healing as evidenced by manual * Associate Professor, Department of Oral and Maxillofacial Surnerv. Fact&v of Dentistry. The University of British Colum- bia,-Vancouver; B.C.; formerly Acting Chairman of the Depart- ment of Maxillofacial and Oral Surgery, University of the Wit- watersrand, Johannesburg, South Africa. Address correspondence and reprint requests to Dr. Reitzik. bending of bone is an indication of bone stiffness. As a test of healing, bending has many drawbacks. It is subjective to the clinician3 and bears little re- lationship to the breaking strength of bone,14 as much of the healing process postdates the time of “clinical” union. The lessening or absence of symptomatic pain is also used to monitor the prog- ress of healing for long bones. Again, this method is subjective and its limitations are obvious. Radio- logic evidence of healing is a very late feature and is dependent on the reconstitution of bone salts and the reorientation of the Haversian systems. In mandibular fractures it may be delayed 18 months or more.’ The passage of time is the commonest criterion used in planning the treatment of fractures. Arbi- trary periods are used for the splinting of long bones and mandibles. Two weeks is the shortest period advocated for maxillomandibular fixation of man- dibular fractures,‘” with an average of four to six weeks for normal healthy adults and eight weeks for the elderly. l7 Biomechanical testing of healing fractures adds considerably to our knowledge and has been exten- sively investigated in long bones.1”-14~‘s-2” How- ever, almost all experimental studies on the healing of fractures of the mandible have relied on subjec- tive clinical assessment of healing together with radiologic and histologic evidence.“‘-” Clarke and Hayes”” are perhaps the only investigators to have used biometric techniques in the study of healing in mandibular fractures. They compared healing when rigid and semirigid fixation was used. A fixed weight was attached to the anterior end of the man- dible to bend it at the fracture site. Quantitation was effected by measuring the changed angle of four previously implanted bone markers. This experi- ment measured the stiffness of the bone, but the results were of course influenced by the rigidity of the fixation itself. The only meaningful measure- 02782391/82/0400/0214 $01.00 Q American Association of Oral and Maxillofacial Surgeons 214
Transcript
SCIENTIFIC ARTICLES
The Biometry of Mandibular Osteotomy Repair
MONTY REITZIK, MB, CHB, FDSRCS*
The healing of experimental mandibular osteotomies in monkeys was monitored by biometric testing. Results indicate that full strength returns to the osteotomy site in 20 weeks. The implications for the treatment of osteotomies and fractures of the mandible in humans are discussed.
Relapse following the surgical correction of man- dibular malposition has been extensively docu- mented.lp4 A detailed cephalometric study of long- term “relapse” in both the distal and the proximal segments of the surgically corrected prognathic mandible has revealed a consistent pattern of spatial changes in both fragments following the removal of maxillomandibular fixation. These changes are al- most certainly due to muscle action upon a weak bone scar at the osteotomy site.5
Considerable attention has been directed toward modification of muscle activity in an attempt to re- duce or avoid relapse.l~“-s The use of neck braces,“,‘” suprahyoid myotomy,” and prolonged maxilloman- dibular fixation by elastic traction’ have all been reported with variable results. Hirose’ uses maxillo- mandibular elastics for six months following sur- gery to achieve a stable result. Pitkin collars and neck braces9 are also used for considerable periods. The length of time that muscle modification is re- quired to prevent relapse depends on the time that it takes for the osteotomy site to reach sufficient strength to withstand the resultant forces of the pterygomasseteric sling and the other muscles of mastication.” The question thus arises: How long does it take for a mandibular osteotomy site to heal completely?
The healing of fractured bones has been exten- sively investigated. The long bone mode11L~‘5 has usually been used in the past, as it is easily accessi- ble in vivo, experimental fractures can be induced surgically, and healing can be readily monitored. Clinical evidence of healing as evidenced by manual
* Associate Professor, Department of Oral and Maxillofacial Surnerv. Fact&v of Dentistry. The University of British Colum- bia,-Vancouver; B.C.; formerly Acting Chairman of the Depart- ment of Maxillofacial and Oral Surgery, University of the Wit- watersrand, Johannesburg, South Africa.
Address correspondence and reprint requests to Dr. Reitzik.
bending of bone is an indication of bone stiffness. As a test of healing, bending has many drawbacks. It is subjective to the clinician3 and bears little re- lationship to the breaking strength of bone,14 as much of the healing process postdates the time of “clinical” union. The lessening or absence of symptomatic pain is also used to monitor the prog- ress of healing for long bones. Again, this method is subjective and its limitations are obvious. Radio- logic evidence of healing is a very late feature and is dependent on the reconstitution of bone salts and the reorientation of the Haversian systems. In mandibular fractures it may be delayed 18 months or more.’
The passage of time is the commonest criterion used in planning the treatment of fractures. Arbi- trary periods are used for the splinting of long bones and mandibles. Two weeks is the shortest period advocated for maxillomandibular fixation of man- dibular fractures,‘” with an average of four to six weeks for normal healthy adults and eight weeks for the elderly. l7
Biomechanical testing of healing fractures adds considerably to our knowledge and has been exten- sively investigated in long bones.1”-14~‘s-2” How- ever, almost all experimental studies on the healing of fractures of the mandible have relied on subjec- tive clinical assessment of healing together with radiologic and histologic evidence.“‘-” Clarke and Hayes”” are perhaps the only investigators to have used biometric techniques in the study of healing in mandibular fractures. They compared healing when rigid and semirigid fixation was used. A fixed weight was attached to the anterior end of the man- dible to bend it at the fracture site. Quantitation was effected by measuring the changed angle of four previously implanted bone markers. This experi- ment measured the stiffness of the bone, but the results were of course influenced by the rigidity of the fixation itself. The only meaningful measure-
02782391/82/0400/0214 $01.00 Q American Association of Oral and Maxillofacial Surgeons
214
REITZIK 215
ment was the one performed after the removal of the wires and plates, which limited the value of the results.
In view of the paucity of experimental data on mandibular osteotomy and fracture healing, it was believed that construction of a timetable of healing based on time only would be of some value to clini- cians.
Methods and Materials
African green Vet-vet monkeys (Cercopithecus aethiops) were used in this study. Animals of both sexes, weighing 3 kg ? 0.5 kg were used, to stan- dardize the size of the mandibles tested. Almost all the animals had erupted third molars (over 42 months old). Four animals, however, had unerupted third molars, and to standardize the specimens the erupted or unerupted third molars of all animals were removed at least 12 weeks before experimen- tal osteotomy.
Each monkey was sedated with intramuscular phencyclidine HCl or ketamine and then anesthe- tized with intravenous phenobarbitone. The animal was intubated and the submandibular triangle shaved. A midline incision was made from the menton to the thyroid cartilage to expose each side of the mandi- ble. A Stryker reciprocating saw was used to trans- sect the mandible from the area of the retromolar pad superiorly to the antegonial notch inferiorly, care being taken not to compound the fracture into the oral cavity. This site was chosen because de- struction tests in the pilot series to determine the full strength of unfractured monkey mandibles consis- tently produced fractures in this region.“” The width of the defect was the width of the blade (0.75 mm). Rigid internal fixation with 0.25 Vitallium mesh and 5-mm screws (Fig. 1) obviated any need for maxillo- mandibular faation. The wound was closed in layers, and skin closure was effected with a continuous multifilament suture. Recovery from the procedure was rapid. All animals were eating their normal diet within 24 hours (monkey chow, fresh fruit and vege- tables, and vitamin supplements). Postoperative swelling in the submandibular region usually re- solved within five days.
BIOMETRIC TESTING
At least two animals were killed at four, six, eight, ten, 14. 18, 22, and 40 weeks after operation. Immediately after death, the mandibles were re- moved and cleaned of all soft tissues (Fig. 2). The mesh and screws were removed from both sides, and the mandible was hemisected through the sym- physis. Each side was radiographed. The half man- dible was embedded in a cyclindrical block of
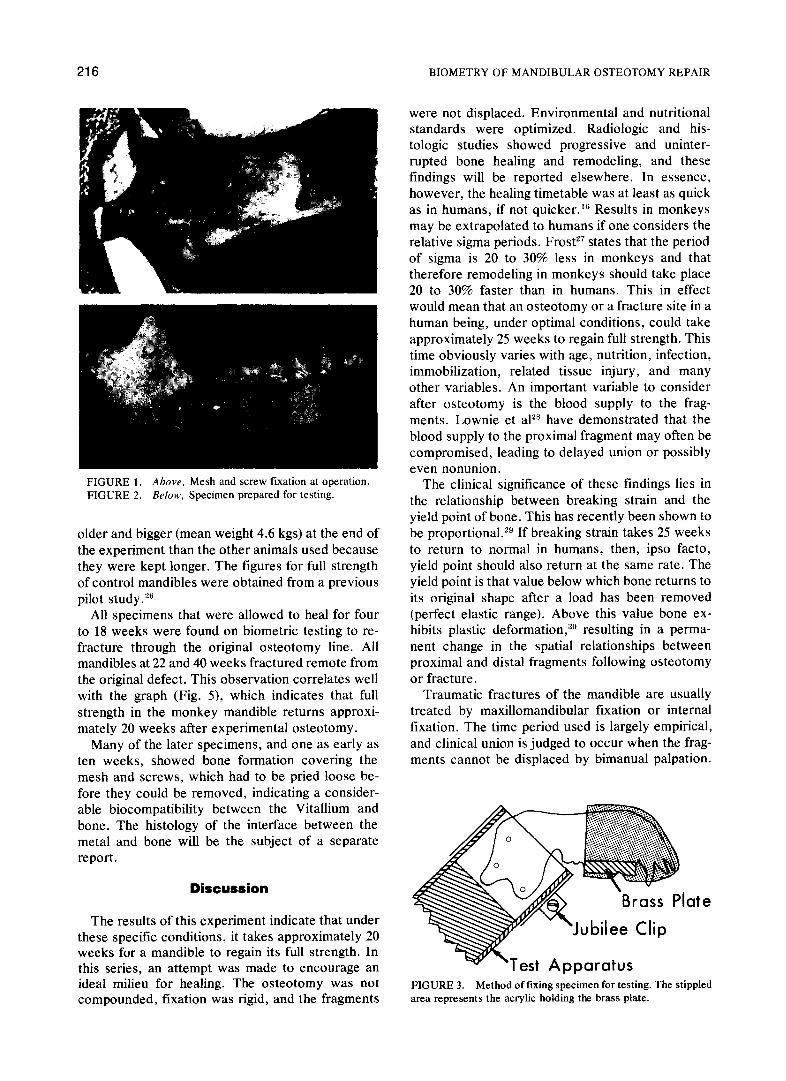
acrylic by positioning it in a metal ring mold so that the lower border of the body of the mandible was 45” to the horizontal plane. Three holes were drilled through the ascending ramus, and metal rods were inserted to act as drag anchors to obviate movement of the fragment within the acrylic block. As soon as the acrylic began to cure, the half mandible and mold were placed under running cold water to eliminate the effect of heat on bone. The acrylic block containing the half mandible was tapped out of its ring former when cured. A brass plate was fixed to the dentate surface of the anterior half of the body of mandible with acrylic, to provide a rigid point of application of tensile force (Fig. 3), and a groove was cut into the brass plate at a fixed dis- tance from the center of the fracture. The speci- mens were kept moist with tap water throughout the experiment.
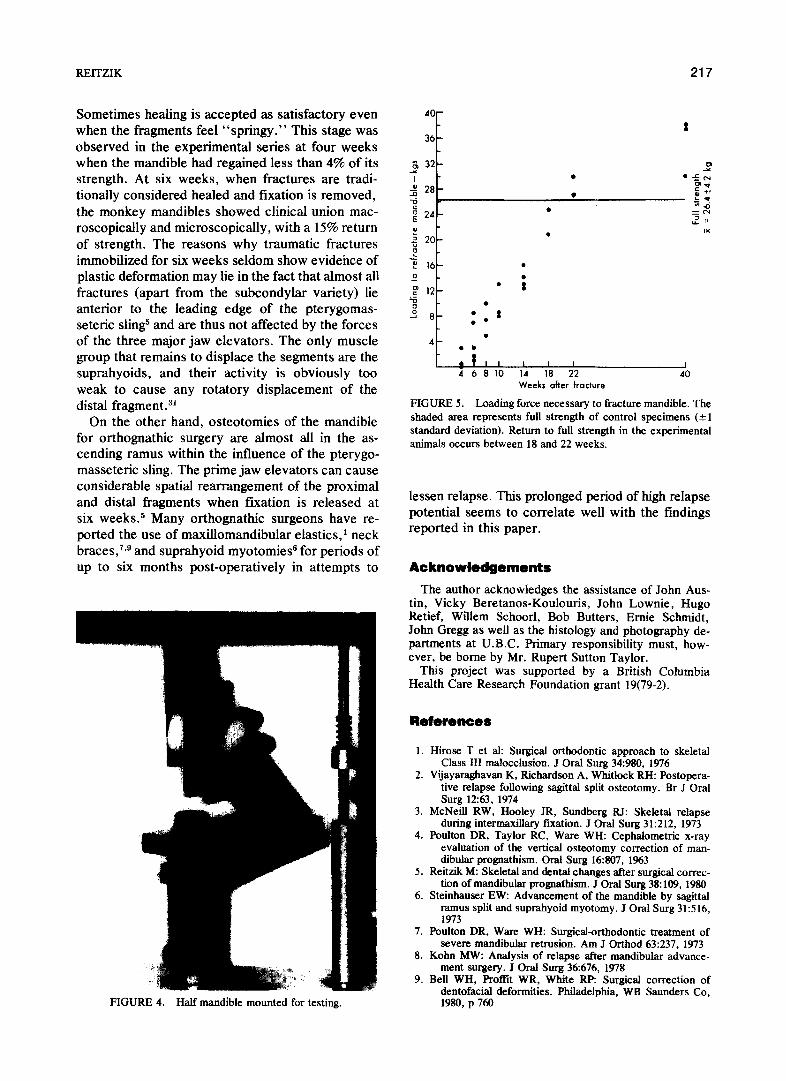
The specimen was then placed into a special- ly constructed holder (45” to the horizontal) and mounted into an Instron tensiometer (Fig. 4). The mandible was loaded with a tensile force applied to the groove in the brass plate at a right angle to the lower border of the body of the mandible. A con- stant crosshead speed was used, and the mandible was tested to destruction. A stress/strain curve was produced, and the site of refracture was noted (either through or distant from the surgical fracture site). Results were read to the nearest 0.1 kg.
At least one specimen from each time group was kept for histologic examination.
None of the animals showed any complications referable to the procedure, although three monkeys were lost due to intractable stress diarrhea, one on the tenth postoperative day and two during the con- ditioning period before operation. This is not un- common in feral animals. All monkeys that came to testing were healthy throughout, and no cases of nonunion or of infection in the fracture site were found.
Results
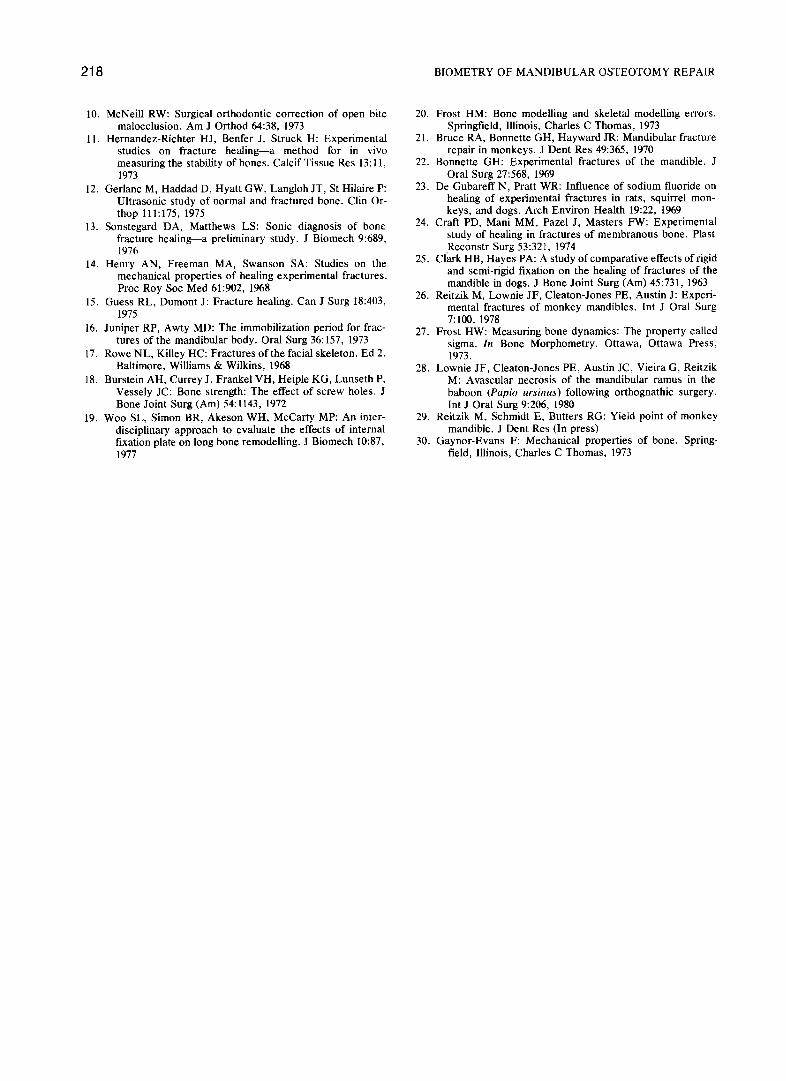
At four weeks, only one specimen was strong enough to test on the tensiometer, and that frac- tured at 3 kgs. None of these specimens exhibited “clinical union,” although macroscopic and micro- scopic examination showed good bony healing. At six weeks, there was a fairly wide scatter of results (R = 4.0 kgs ? 3.6 kgs). This scatter narrowed down with longer healing periods (at fourteen weeks R = 13.85 kgs +- 1.6 kg).
Three animals were kept for 40 weeks following experimental osteotomy, and biometric testing showed that these mandibles were stronger than those of control animals. These three animals were
216 BIOMETRY OF MANDIBULAR OSTEOTOMY REPAIR
FIGURE 1. Above, Mesh and screw fixation at operation. FIGURE 2. B&W, Specimen prepared for testing.
older and bigger (mean weight 4.6 kgs) at the end of the experiment than the other animals used because they were kept longer. The figures for full strength of control mandibles were obtained from a previous pilot study.‘”
All specimens that were allowed to heal for four to 18 weeks were found on biometric testing to re- fracture through the original osteotomy line. All mandibles at 22 and 40 weeks fractured remote from the original defect. This observation correlates well with the graph (Fig. S), which indicates that full strength in the monkey mandible returns approxi- mately 20 weeks after experimental osteotomy.
Many of the later specimens, and one as early as ten weeks, showed bone formation covering the mesh and screws, which had to be pried loose be- fore they could be removed, indicating a consider- able biocompatibility between the Vitallium and bone. The histology of the interface between the metal and bone will be the subject of a separate report.
Discussion
The results of this experiment indicate that under these specific conditions, it takes approximately 20 weeks for a mandible to regain its full strength. In this series, an attempt was made to encourage an ideal milieu for healing. The osteotomy was not compounded, fixation was rigid, and the fragments
were not displaced. Environmental and nutritional standards were optimized. Radiologic and his- tologic studies showed progressive and uninter- rupted bone healing and remodeling, and these findings will be reported elsewhere. In essence, however, the healing timetable was at least as quick as in humans, if not quicker.l” Results in monkeys may be extrapolated to humans if one considers the relative sigma periods. FrostZ7 states that the period of sigma is 20 to 30% less in monkeys and that therefore remodeling in monkeys should take place 20 to 30% faster than in humans. This in effect would mean that an osteotomy or a fracture site in a human being, under optimal conditions, could take approximately 25 weeks to regain full strength. This time obviously varies with age, nutrition, infection, immobilization, related tissue injury, and many other variables. An important variable to consider after osteotomy is the blood supply to the frag- ments. Lownie et aP have demonstrated that the blood supply to the proximal fragment may often be compromised, leading to delayed union or possibly even nonunion.
The clinical significance of these findings lies in the relationship between breaking strain and the yield point of bone. This has recently been shown to be proportional. 2y If breaking strain takes 25 weeks to return to normal in humans, then, ipso facto, yield point should also return at the same rate. The yield point is that value below which bone returns to its original shape after a load has been removed (perfect elastic range). Above this value bone ex- hibits plastic deformation,3” resulting in a perma- nent change in the spatial relationships between proximal and distal fragments following osteotomy or fracture.
Traumatic fractures of the mandible are usually treated by maxillomandibular fixation or internal fixation. The time period used is largely empirical, and clinical union is judged to occur when the frag- ments cannot be displaced by bimanual palpation.
FIGURE 3. Method of fixing specimen for testing. The stippled area represents the acrylic holding the brass plate.
REITZIK 217
Sometimes healing is accepted as satisfactory even when the fragments feel “springy.” This stage was observed in the experimental series at four weeks when the mandible had regained less than 4% of its strength. At six weeks, when fractures are tradi- tionally considered healed and fixation is removed, the monkey mandibles showed clinical union mac- roscopically and microscopically, with a 15% return of strength. The reasons why traumatic fractures immobilized for six weeks seldom show evidehce of plastic deformation may lie in the fact that almost all fractures (apart from the subcondylar variety) lie anterior to the ieading edge of the pterygomas- seteric sling5 and are thus not affected by the forces of the three major jaw elevators. The only muscle group that remains to displace the segments are the suprahyoids, and their activity is obviously too weak to cause any rotatory displacement of the distal fi-agment.31
On the other hand, osteotomies of the mandible for orthognathic surgery are almost all in the as- cending ramus within the influence of the pterygo- masseteric sling. The prime jaw elevators can cause considerable spatial rearrangement of the proximal and distal fragments when fixation is released at six weeks.s Many orthognathic surgeons have re- ported the use of maxillomandibular elastics,’ neck braces,7,g and suprahyoid myotomie9 for periods of up to six months post-operatively in attempts to
FIGURE 4. Half mandible mounted for testing.
40-
:
36-
16- .
1 .
12 ;
.
8 :.*
c . 4
. c
t $?I1 1 I I 4 6 0 10 14 18 22
weeks after fracture
I 40
FIGURE 5. Loading force necessary to fracture mandible. The shaded area represents full strength of control specimens (21 standard deviation). Return to full strength in the experimental animals occurs between 18 and 22 weeks.
lessen relapse. This prolonged period of high relapse potential seems to correlate well with the findings reported in this paper.
Acknowledgements The author acknowledges the assistance of John Aus-
tin, Vicky Beretanos-Koulouris, John Lownie, Hugo Retief, Willem Schoorl, Bob Butters, Ernie Schmidt, John Gregg as well as the histology and photography de- partments at U.B.C. Primary responsibility must, how- ever, be borne by Mr. Rupert Sutton Taylor.
This project was supported by a British Columbia Health Care Research Foundation grant 19(79-2).
References
1. Hirose T et al: Surgical orthodontic approach to skeletal Class III malocclusion. J Oral Surg 34980, 1976
2. Vijayaraghavan K, Richardson A, Whitlock RH: Postopera- tive relapse following sag&al split osteotomy. Br J Oral Surg 12:63, 1974
4. Poulton DR, Taylor RC, Ware WH: Cephalometric x-ray evaluation of the vertical osteotomy correction of man- dibular prognathism. Oral Surg l&807, 1963
5. Reitzik M: Skeletal and dental changes after surgical correc- tion of mandibular prognathism. J Oral Surg 38:109, 1980
6. Steinhauser EW: Advancement of the mandible by sag&al ramus split and suprahyoid myotomy. J Oral Surg 31516, 1973
7. Poulton DR, Ware WH: Surgical-orthodontic treatment of severe mandibular retrusion. Am J Orthod 63:237, 1973
8. Kohn MW: Analysis of relapse after mandibular advance- ment surgery. J Oral Surg 36676, 1978
9. Bell WH, Proffit WR, White Rp: Surgical correction of dentofacial deformities. Philadelphia, WB Saunders Co, 1980, p 760
218 BIOMETRY OF MANDIBULAR OSTEOTOMY REPAIR
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
McNeil1 RW: Surgical orthodontic correction of open bite 20. Frost HM: Bone modelling and skeletal modelling errors. malocclusion. Am J Orthod 64:38, 1973 Springfield, Illinois, Charles C Thomas, 1973
Hernandez-Richter HJ, Benfer J, Struck H: Experimental 21. Bruce RA, Bonnette GH, Hayward JR: Mandibular fracture studies on fracture healing-a method for in vivo repair in monkeys. J Dent Res 49:365, 1970 measuring the stability of bones. Calcif Tissue Res 13: 11, 22. Bonnette GH: Experimental fractures of the mandible. J 1973 Oral Surg 27:568, 1969
Gerlanc M, Haddad D, Hyatt GW, Langloh JT, St Hilaire P: Ultrasonic study of normal and fractured bone. Clin Or- thop 111:175, 1975
Sonstegard DA, Matthews LS: Sonic diagnosis of bone fracture healing-a preliminary study. J Biomech 9:689, 1976
Henry AN, Freeman MA, Swanson SA: Studies on the mechanical properties of healing experimental fractures. Proc Roy Sot Med 61:902, 1968
Juniper RP, Awty MD: The immobilization period for frac- tures of the mandibular body. Oral Surg 36: 157, 1973
Rowe NL, Killey HC: Fractures of the facial skeleton. Ed 2. Baltimore, Williams & Wilkins, 1968
Burstein AH, Currey J, Frankel VH, Heiple KG, Lunseth P, Vessely JC: Bone strength: The effect of screw holes. .I Bone Joint Surg (Am) 54: 1143, 1972
Woo SL, Simon BR, Akeson WH, McCarty MP: An inter- disciplinary approach to evaluate the effects of internal fixation plate on long bone remodelling. J Biomech 10:87, 1977
23. De Gubareff N, Pratt WR: Influence of sodium fluoride on healing of experimental fractures in rats, squirrel mon- keys, and dogs. Arch Environ Health 19:22, 1969
24. Craft PD, Mani MM, Pazel J, Masters FW: Experimental study of healing in fractures of membranous bone. Plast ,Reconstr Surg 53:321, 1974
25. Clark HB, Hayes PA: A study of comparative effects of rigid and semi-rigid fixation on the healing of fractures of the mandible in dogs. J Bone Joint Surg (Am) 45:731, 1963
26. Reitzik M, Lownie JF, Cleaton-Jones PE, Austin J: Experi- mental fractures of monkey mandibles. Int J Oral Surg 7:100, 1978
27. Frost HW: Measuring bone dynamics: The property called sigma. In Bone Morphometry. Ottawa, Ottawa Press, 1973.
28. Lownie JF, Cleaton-Jones PE, Austin JC, Vieira G, Reitzik M: Avascular necrosis of the mandibular ramus in the baboon (Papio ursinus) following orthognathic surgery. Int J Oral Surg 9:206, 1980
29. Reitzik M, Schmidt E, Butters RG: Yield point of monkey mandible. J Dent Res (In press)
30. Gaynor-Evans F: Mechanical properties of bone. Spring- field, Illinois, Charles C Thomas, 1973