38
The Case for Exercise in a Clinical Context Jonathan Myers, PhD VA Palo Alto Health Care System Stanford University
The Case for Exercise in a Clinical Context
Jonathan Myers, PhDVA Palo Alto Health Care System
Stanford University

The Veterans Exercise Testing Study (VETS)
◼ An ongoing, prospective evaluation of veteran subjects referred for exercise testing for clinical reasons, designed to address exercise test, clinical, and lifestyle factors and their association with health outcomes
◼ ≈25,000 subjects followed beginning in 1987
Minimal recommendations for physical activity – WHO, CDC, AHA, ACSM, US Surgeon General’s Report, USHHS, ESC Working Group*
“All individuals should attempt to accumulate 30 minutes of moderate activity on most, if not all, days of the week”
“Additional health benefits can be gained through greater amounts of physical activity…”
30 minutes daily activity ≈20 to 40% reductions in cardiovascular and all-cause morbidity/mortality
*Australia, Canada, Fiji, UK, New Zealand, Germany, Singapore, the Philippines, Switzerland; all are generally based on the United States Surgeon General’s recommendations for physical activity
Key messages:
◼ Cardiorespiratory fitness powerfully predicts risk for mortality, cardiovascular events, and other adverse outcomes
◼ Fitness should be viewed as a vital sign, similar to blood pressure
◼ We’re less physically active than we have been in human history
◼ Physical activity counseling should be part of every clinical encounter

Message #1:
Cardiorespiratory fitness powerfully predicts risk for mortality, cardiovascular events, and other adverse outcomes

Importance of Assessing Cardiorespiratory Fitnessin Clinical Practice: A Case for Fitness as a Clinical
Vital Sign. A Scientific Statement From the American Heart Association
Robert Ross, PhD, FAHA, Chair, Steven N. Blair, PED, FAHA, Co-Chair, Ross Arena, PhD, PT, FAHA,Timothy S. Church, MD, MPH, PhD, Jean-Pierre Després, PhD, FAHA, Barry A. Franklin, PhD, FAHA, William L. Haskell, PhD, Leonard A. Kaminsky, PhD, FAHA, Benjamin D. Levine, MD, FAHA,
Carl J. Lavie, Jr, MD, Jonathan Myers, PhD, FAHA, Josef Niebauer, MD, PhD, MBA, Robert Sallis, MD, Susumu S. Sawada, PhD,
Xuemei Sui, MD, MPH, PhD, Ulrik Wisløff, PhD
On behalf of the American Heart Association Physical Activity Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Clinical
Cardiology; Council on Epidemiology and Prevention; Council on Cardiovascular and Stroke Nursing; Council on Functional Genomics and
Translational Biology; and Stroke Council
Circulation 134:e653-e699, 2016

Call to Action on Making Physical Activity
Assessment and Prescription a Medical
Standard of Care Robert E. Sallis,MD, FACSM; Jason M. Matuszak,MD, FAAFP; Aaron L. Baggish,MD, FACC, FACSM;Barry A. Franklin, PhD, FACSM; Wojtek Chodzko-Zajko, PhD, FACSM; Barbara J. Fletcher, RN, MSN, FAAN, FPCNA; Andrew Gregory, MD, FAAP, FACSM; Elizabeth Joy, MD, MPH, FACSM; Gordon Matheson, MD, PhD, FACSM; Patrick McBride, MD, MPH, FACC; James C. Puffer, MD, FACSM; Jennifer Trilk, PhD; and Janet Williams, MA
Abstract The U.S. population is plagued by physical inactivity, lack of cardiorespiratory fitness, and sedentary lifestyles, all of which are strongly associated with the emerging epidemic of chronic disease. The time is right to incorporate physical activity assessment and promotion into health care in a manner that engages clinicians and patients. In April 2015, the American College of Sports Medicine and Kaiser Permanente convened a joint consensus meeting of subject matter experts from stakeholder organizations to discuss the development and implementation of a physical activity vital sign (PAVS) to be obtained and recorded at every medical visit for every patient. This statement represents a summary of the discussion, recommendations, and next steps developed during the consensus meeting. Foremost, it is a call to action for current and future clinicians and the health care community to implement a PAVS in daily practice with every patient. Introduction/Purpose Nearly 60 years ago, President Eisenhower established the President’s Council on Fitness and Sports (originally named the
President’s Council on Youth Fitness) in response to growing concern for the deteriorating level of American youth
physical fitness. Despite this and many other national health initiatives that emphasize physical activity in both children
and adults, the U.S. population is still plagued by physical inactivity, lack of cardiorespiratory fitness, and sedentary
lifestyles, all ofwhich are strongly associatedwith the emerging epidemic of chronic disease. In fact, at the annual meeting
of the AmericanCollege of Sports Medicine in 2014, then acting US Surgeon General, Dr. Boris Lushniak, echoed
research by Blair et al, stating, “Physical inactivity is the major public health issue in this country…”
Current Sports Medicine Reports 18;207-214

Population Attributable Risk
The incidence of disease in a population that would be eliminated if a given risk
factor were eliminated
02468
1012141618
Low CRF*
Obese
Smoker
Hypertension
High Chol
Diabetes
Men
Women
Cooper Aerobics Center Longitudinal Study, 1970-2004. In progress
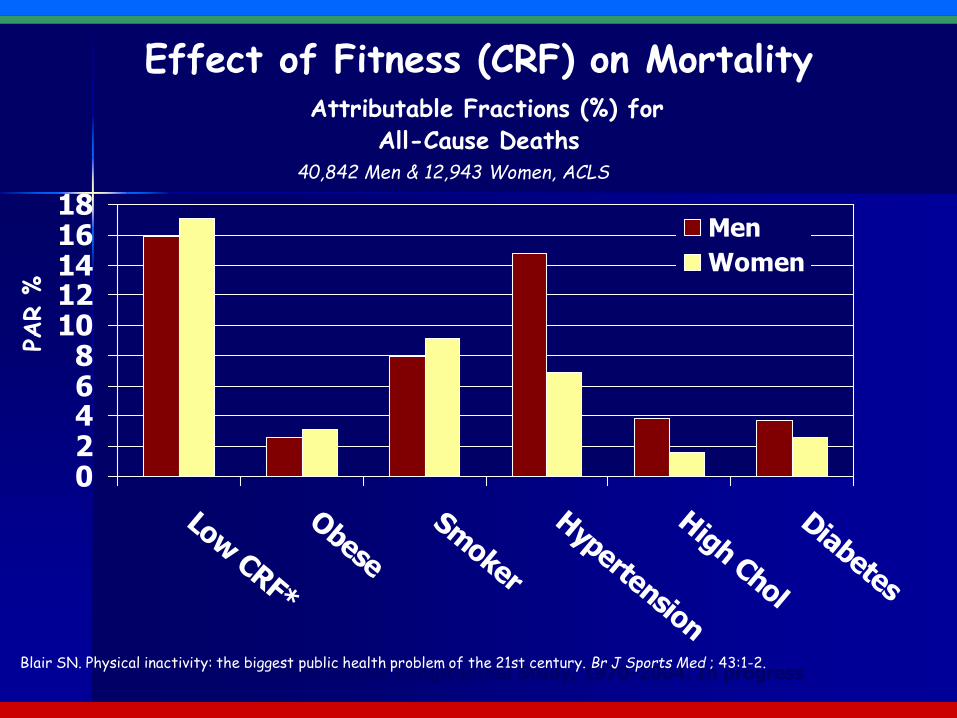
40,842 Men & 12,943 Women, ACLS
Effect of Fitness (CRF) on MortalityAttributable Fractions (%) for
All-Cause Deaths
Blair SN. Physical inactivity: the biggest public health problem of the 21st century. Br J Sports Med ; 43:1-2.
PAR %
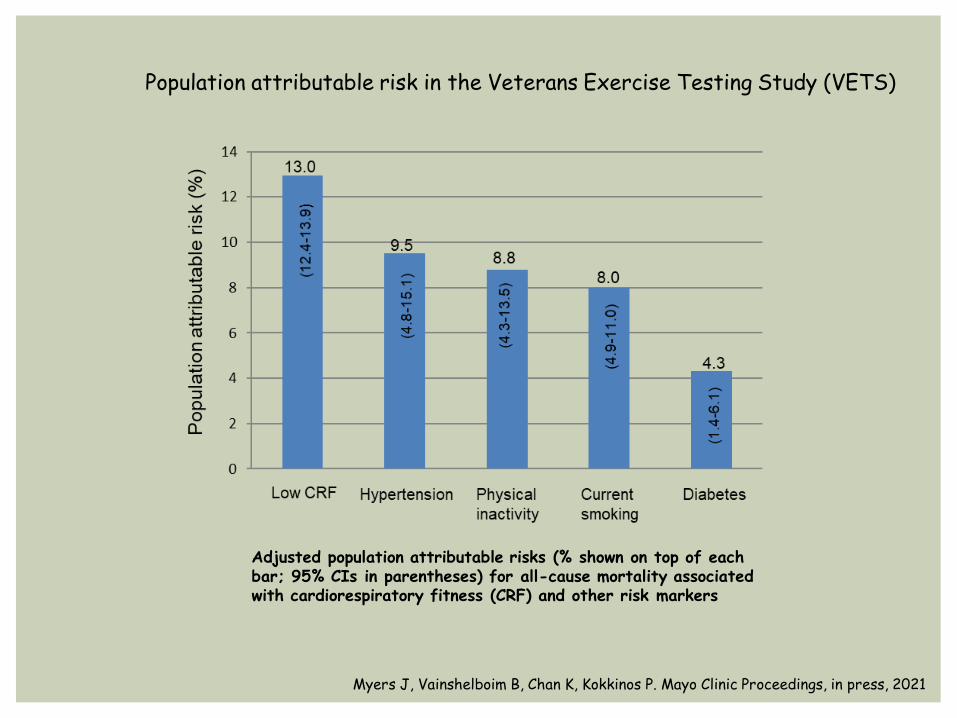
Adjusted population attributable risks (% shown on top of each bar; 95% CIs in parentheses) for all-cause mortality associated with cardiorespiratory fitness (CRF) and other risk markers
Myers J, Vainshelboim B, Chan K, Kokkinos P. Mayo Clinic Proceedings, in press, 2021
Population attributable risk in the Veterans Exercise Testing Study (VETS)

Comparison of global burden between smoking and physical inactivity. Prevalence of smoking, population attributable risk (PAR), and global deaths for smoking were obtained from WHO.
Chi Pang Wen , Xifeng Wu. Stressing harms of physical inactivity to promote exercise. The Lancet Volume 380, Issue 9838;192 - 193
MET and MET-Hour:
◼ 1 MET ≈ resting metabolic rate (3.5 ml O2/kg/min)
◼ Exercise capacity commonly expressed in multiples of the resting metabolic rate (mean peak METs at the VA ≈ 8)
◼ MET-Hour - Multiple of the resting metabolic rate (METs) x duration of activity (hours)
◼ Metric that considers exercise intensity and duration
◼ Minimal guidelines for activity ≈ 8-10 MET-hours/week
(walking [3 METs] x 30 minutes/day, 6 days/wk [3 hours] = [3x3 = 9 MET-hours]
Relative Risk
The probability of an event occurring in one group compared to the probability of
an event occurring in another group
What if we compare high fit subjects with other groups?

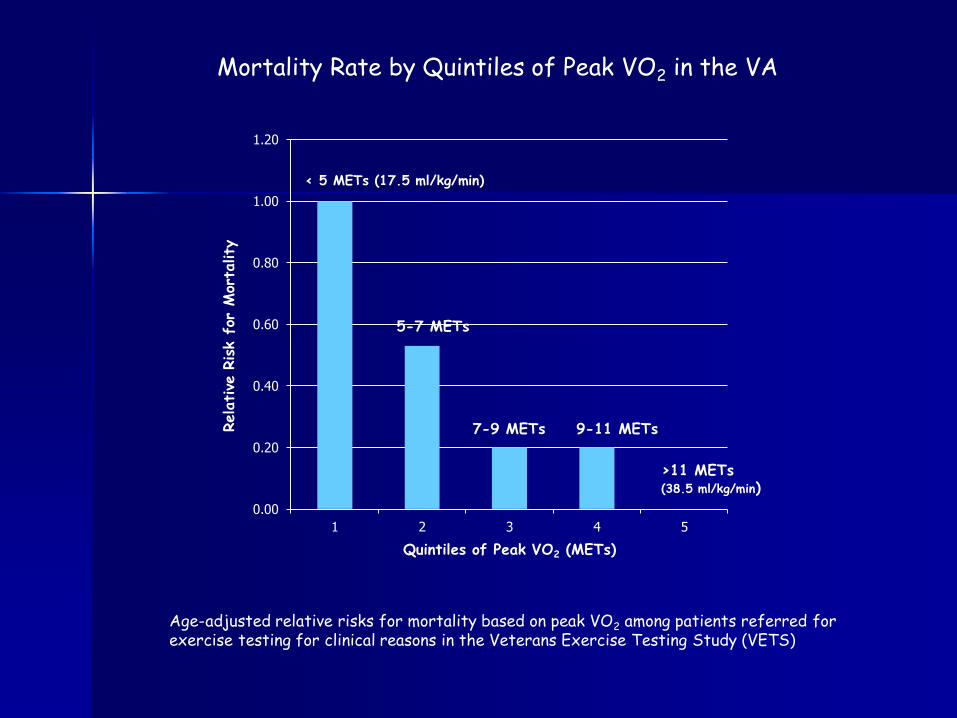
Myers J, et al. New Engl J Med 346: 793, 2002
➢Exercise capacity most powerful predictor of risk
➢ 12% lower mortality per higher MET
0.00
0.20
0.40
0.60
0.80
1.00
1.20
1 2 3 4 5
Relative
Risk f
or M
orta
lity
Quintiles of Peak VO2 (METs)
5-7 METs
7-9 METs 9-11 METs
>11 METs(38.5 ml/kg/min)
< 5 METs (17.5 ml/kg/min)
Age-adjusted relative risks for mortality based on peak VO2 among patients referred for exercise testing for clinical reasons in the Veterans Exercise Testing Study (VETS)
Mortality Rate by Quintiles of Peak VO2 in the VA
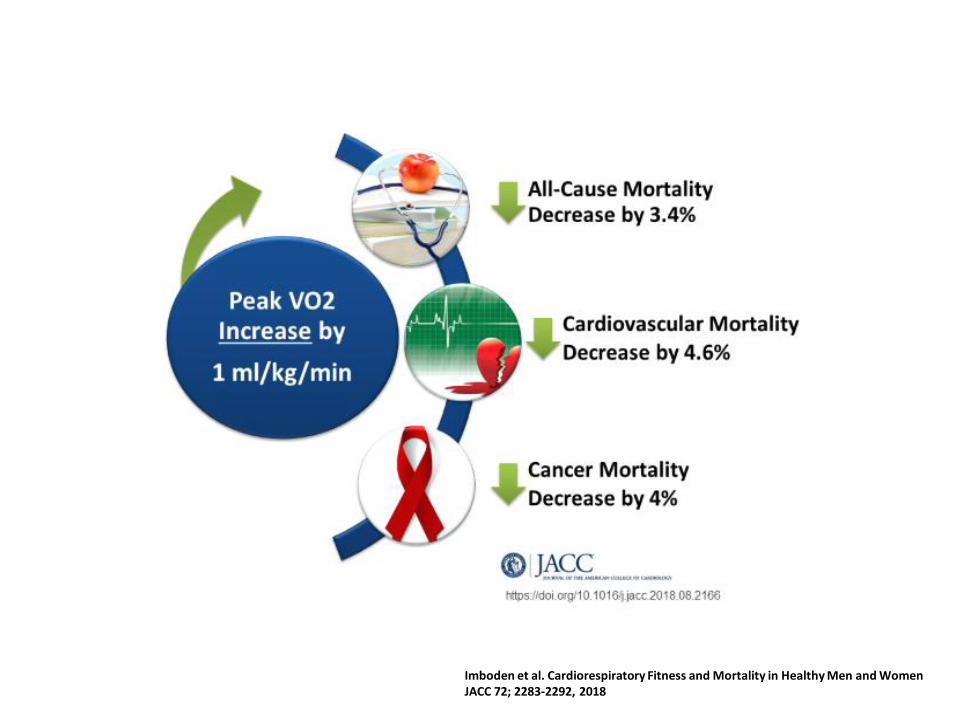
Imboden et al. Cardiorespiratory Fitness and Mortality in Healthy Men and WomenJACC 72; 2283-2292, 2018

Message #2:
We’re less physically active than we have been in human history

Temporal Trends in the Cardiorespiratory Fitness of 2,525,827 AdultsBetween 1967 and 2016: A Systematic Review
Lamoureux et al. Sports Medicine (2019) 49:41–55
There has been a moderate international decline in adult CRF since 1980………… Declines in CRF were reported across all included countries, with declines generally larger for men than for women, and for young adults than for middle-aged adults…………. Countries with the largest increases in adult obesity experienced the largest declines in CRF.

Wang et al. Lancet 378(9793): 815-825
Growth in World-Wide Prevalence of Overweight
More active individuals have lower risk for cardiovascular and all-cause mortality (2000-2020):◼ Framingham Heart Study◼ Aerobics Center Longitudinal
Study (ACLS)◼ Honolulu Heart Study◼ Canada Health Survey◼ Harvard Alumni Health Study◼ Copenhagen Male Study◼ Zutphen Elderly Study◼ Osteoporotic Fractures
Research Group◼ Caerphilly Wales Study◼ Puerto Rico Heart Health
Program ◼ Nordic Research Project on
Aging (NORA)◼ Swedish Annual Level of Living
Survey (SALLS)◼ NIH-AARP Diet and Health
Study◼ Copenhagen City Heart Study◼ Henry Ford Hospital (FIT) Study
◼ Finnish Twin Study◼ Lipid Research Clinics Follow-up
Study◼ Belgian Physical Fitness Study◼ Physicians Health Follow-up
Study◼ Nurses Health Study◼ Veterans Exercise Testing Study ◼ The Whitehall Study ◼ National Center for Chronic
Disease Prevention and Health Promotion, CDC
◼ The SENECA Study◼ Baltimore Longitudinal Study on
Aging◼ Women’s Health Initiative
Observational Study◼ Netherlands Elderly (FINE)
Study◼ HUNT Study (Norway)◼ STABILITY study

Key Physical Activity Guidelines for Adults from HHS (2018):
- Adults should move more and sit less throughout the day. Some physical activity is better than none
- For health benefits, adults should do at least 150 minutes of moderate activity per week.
(or 75 minutes of vigorous activity per week)
- Adults should also do muscle strengthening activities of moderate or greater intensity that involve all major muscle groups on 2 or more days a week, as these activities provide additional health benefits.
United States Health and Human Services November 2018

2018 US DHHS Physical Activity Guidelines
◼ 780 page document
◼ It is estimated that in the US, nearly $117 billion in annual healthcare costs and 10% of all premature mortality are associated with failure to meet the recommended levels of physical activity
◼ Only 26% of men, 19% of women, and 20% of adolescents meet the recommended guidelines, despite the fact that the recommendations are achievable by most individuals
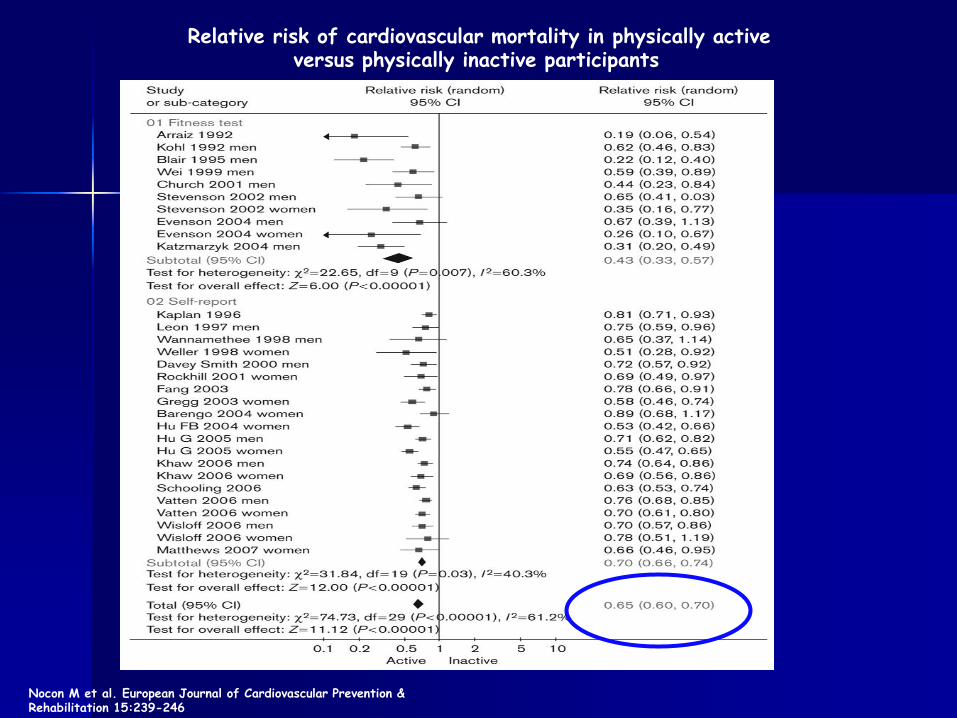
Relative risk of cardiovascular mortality in physically active versus physically inactive participants
Nocon M et al. European Journal of Cardiovascular Prevention & Rehabilitation 15:239-246

Relative risks for classification of activity at the time of a treadmill test among Veterans
p for trend <0.001
Myers et al. Am J Med 128: 396-402, 2015
Rela
tive
Ris
k
Sedentary Minimally Active Moderately Active Active

A few examples from the literature
Association of Step Volume and Intensity With All-Cause Mortality in Older WomenLee IM, Shiroma EJ, Kamada M, Bassett DR, Mathews CE, Buring JE JAMA Intern Med; JAMA Intern Med 179:1105-1112, 2019
◼ 16, 741 women, mean age of 72 years
◼ Steps per day and several measures of stepping intensity measured over 7 days
◼ Mean step count 5,499/day
◼ 504 deaths over mean follow-up of 4.3 years

➢ As few as approximately 4400 steps/d was significantly related to lower mortality rates
➢ With more steps per day, mortality rates progressively decreased before leveling at approximately 7500 steps/d.
4,000 Steps/day
13,000 Steps/day
Leisure time physical activity and mortality:A detailed pooled analysis of the dose-response relationshipArem et al. JAMA Intern Med 175:959-967, 2015
◼ Pooled data from 6 studies in the National Cancer Institute Cohort Consortium
◼ Self-reported physical activity
◼ Total of 661,137 men and women; 116,686 deaths
◼ Median follow-up 14.2 years
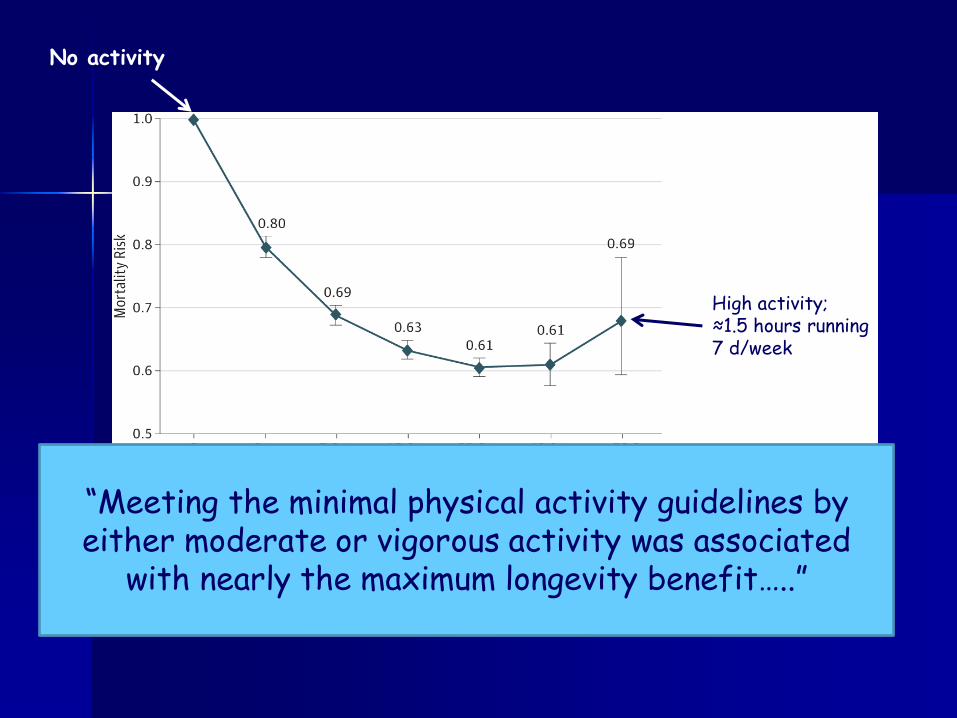
◼ Meeting the minimal physical activity guidelines associated with nearly the maximum longevity benefit
Arem et al. Leisure Time Physical Activity and Mortality: A Detailed Pooled Analysis of the Dose-Response Relationship. JAMA Intern Med 175:959-967, 2015
High activity;≈1.5 hours running7 d/week
No activity
“Meeting the minimal physical activity guidelines by either moderate or vigorous activity was associated
with nearly the maximum longevity benefit…..”
Sedentary Time
0
500
1000
1500
2000
2500
1980 1990 2000 2010 2020
# C
itation
s
Year
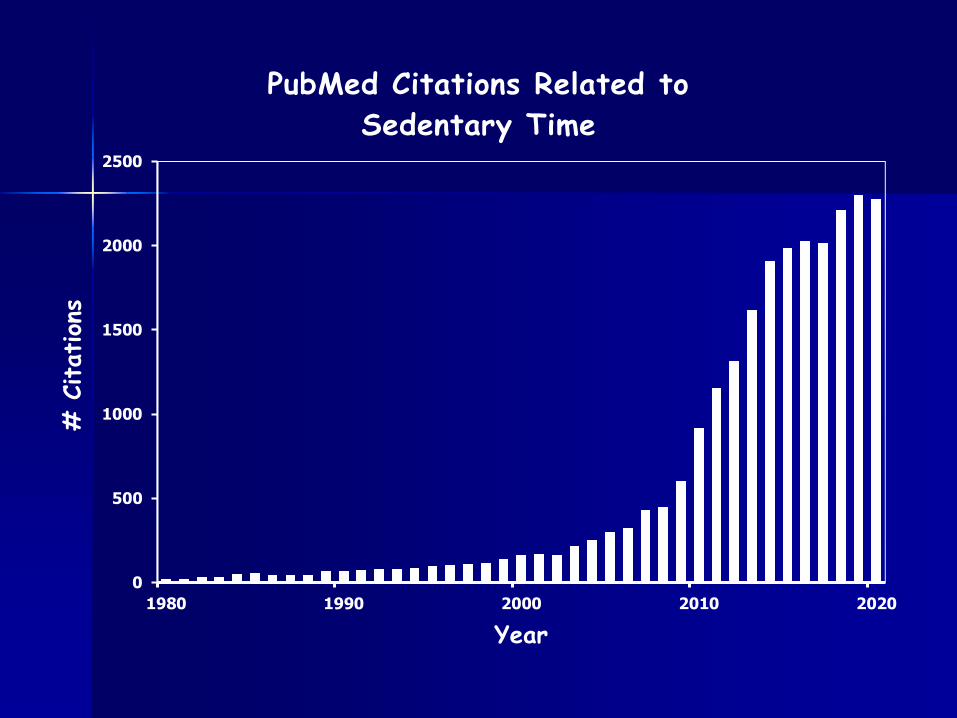
PubMed Citations Related to
Sedentary Time
Sedentary Behavior and Cardiovascular Morbidity and Mortality: A Scientific Advisory
from the American Heart Association
Young DR, Hivert MF, Alhassan S, Cahmi SM, Ferguson JF, Katzmarzyk PT, Lewis CE, Owen N,
Perry CK, Siddique J, Yong CM
On behalf of the Physical Activity Committee of the Council on Lifestyle and Cardiometaboic Health; Council on Clinical
Cardiology; Council on Epidemiology and Prevention; Council on Functional Genomics and Translational Biology; and Stroke Council
Circulation 2016;134:e262-79

2
Kaplan-Meier survival curve for all-cause mortality across categories of daily sitting time in 17,013 men and women 18-90 years of age, in the Canada Fitness Survey
Katzmarzyk P, Church T, Cora C, Bouchard C. Sitting Time and Mortality from All Causes, Cardiovascular Disease, and Cancer. Medicine & Science in Sports & Exercise. 41:998-1005.
Proportion of the day spent sitting (n=17,013)

Key Point:
Reducing sitting time by even a modest amount reduces mortality
Message #3:
Physical activity counseling should be part of every clinical encounter

Physical activity is rarely discussed during typical patient encounters:
➢ Gabrys et al. 2016 - 8.6% of patients between 18 and 64 years of age report having received PA counseling in the past 12 months in Germany
➢ Tarasenko et al. 2015. Less than half of the U.S. cancer survivors report receipt of exercise counseling.
➢ Ruhmann, L. 2014. None of the surveyed physicians in Berlin region provided exercise prescription
➢ Peek et al 2008 – Exercise counseling occurred during 18% of visits (n=6,852) in National Ambulatory Medical Care Survey
➢ Walsh et al 1999 - 12% of physicians familiar with ACSM recommendations for activity➢ Fontaine et al 2005 – 42% of patients “ever received advice about exercise”➢ Ma et al 2005 – 22% of adolescents provided exercise counseling during routine
physician visit➢ Mellen et al 2004 – Of 137 million physician visits, activity counseling provided during
26%; slightly higher with ≥2 risk factors➢ Ma et al 2004 – activity counseling provided <30% of physician visits➢ Tsui et al 2004 – activity discussed 16% of visits to residents or attending MD’s at
Emory➢ Honda 2004 – Of 26,158 physician visits, 24.5% discussed exercise; college educated
75% more like to receive exercise advice➢ Frank et al 2003 – 33% of female MD specialists counseled patients at least yearly➢ Kennedy et al 2003 – 11.8% of family practice MD’s counsel most patients in Canada➢ Glasgow et al 2001 – 28% of patients surveyed received physician advice to increase
activity level➢ Epel et al 2000 – 16% received activity advice from health care provider visit in Israel➢ Stafford et al 2000 – 32.8% of obese patients in NHANES study (≈56,000 office visits)
received exercise counseling during physician visit (weight loss counseling in 52%) ➢ Wee et al 1999 - Among 9,777 patients who had a medical check-up within the last year,
34% of physicians discussed physical activity
Between <10 and 40% of adults reported receiving activity counseling during typical clinic visits

Key messages:
◼ Both an individual’s fitness and physical activity pattern are strongly related to health outcomes
◼ Fitness should be considered a “vital sign” similar to blood pressure
◼ More work needs to be done to convince the public, patients, and health care providers that physical activity is important
“

















