The Catalytic Initiative to Save a Million Lives: Overview and latest update of the Catalytic Initiative Global Immunization Meeting: 19 February 2009, New York Dr. Mark W. Young Senior Health Specialist, Policy and Evidence Unit, Health Section, UNICEF New York
Transcript
The Catalytic Initiative to Save a
Million Lives: Overview and latest
update of the Catalytic Initiative
Global Immunization Meeting: 19 February 2009, New York
Dr. Mark W. YoungSenior Health Specialist, Policy and Evidence Unit,
Health Section, UNICEF New York
The Catalytic Initiative: Principles, Aims and Objectives
• Intensify efforts to achieve MDGs 4&5 by supporting country-led systems to deliver a package of proven, high-impact and cost-effective interventions and to demonstrate the level of impact that can be achieved
• Intervention package may vary by country and will depend on local context and epidemiological profile
• Focus on “Human Resources for Health”: training, equipping and supervision of front-line health workers
• “Program Monitoring and Results Tracking”, in order to demonstrate lessons learned - “Learning by Doing”
• Existing country-level processes should be followed -alignment with national plans and M&E framework
Initiating Partners
• Canadian International Development Agency (CIDA) – announcement of CDN $105 million in Nov. 2007
• UNICEF – matching CIDA contribution of $105M
• World Bank, WHO, UNFPA
• Bill and Melinda Gates Foundation (PMNCH)
• Norway, Australia, USAID, Doris Duke F. & others..
• Viewed within the context of the International Health Partnership (IHP+) as a concrete step for country-level scale-up
CI Countries
• Countries where new funding has so far been allocated: Afghanistan, Burkina Faso, Benin, Ghana, Ethiopia, Malawi, Mali, Mozambique, Niger, Pakistan and Tanzania;
• Approximately $350 million of new money out of a total goal of $500 million has been allocated to date for this initial list of countries
• Cost-effectiveness of child survival package estimated at $500/life saved; therefore aims to “save a million lives” over the course of the initiative
• Plan to implement over 5 year period: 2008 - 2012
Learning by Doing: Monitoring and Evaluation
• Major component of the CI activities is “learning by doing” to demonstrate impact that can be achieved: documentation of “what works” to expand the evidence base (build on lessons from ACSD Evaluation):
• Begin with solid evidence on causes of death and prioritize interventions that have greatest impact
• Rapid impact can be achieved through integrated package at community level and outreach (building on EPI and ANC platforms)
• Develop feasible and sustainable systems for monitoring inputs, outputs and outcomes, and use data to improve program performance
• Data will need to be collected frequently enough and quickly enough to modify plans based on analysis and results (“real-time monitoring”)
• Johns Hopkins University engaged to act as the focal agency for the CI to develop an overall comprehensive framework for CI Program Monitoring
Integrated Health System Strengthening (IHSS):
CIDA-UNICEF Collaboration under the
Catalytic Initiative
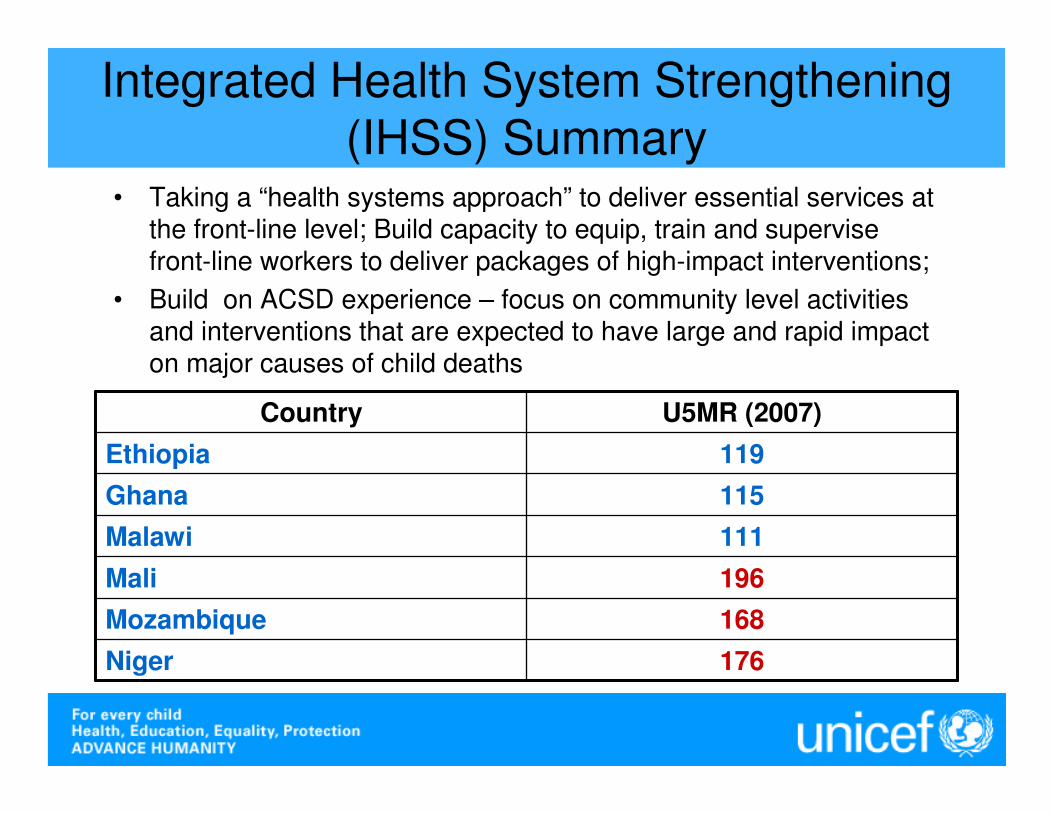
Integrated Health System Strengthening (IHSS) Summary
• Taking a “health systems approach” to deliver essential services at the front-line level; Build capacity to equip, train and supervise front-line workers to deliver packages of high-impact interventions;
• Build on ACSD experience – focus on community level activities and interventions that are expected to have large and rapid impact on major causes of child deaths
176Niger
168Mozambique
196Mali
111Malawi
115Ghana
119Ethiopia
U5MR (2007)Country
Intervention Packages include:
1. Treatment for diarrheal disease, pneumonia and malaria; 2. Immunizations (in order to fill gaps not met by current or
imminent efforts);3. Tetanus immunization for pregnant women; 4. Long lasting insecticide treated bednets (LLIN) for both
pregnant women and U5s; 5. Intermittent preventative treatment for malaria in
pregnancy (IPTp);6. Vitamin A supplementation; 7. Breastfeeding promotion and counselling; 8. Birth spacing and/or contraceptive provision; 9. PMTCT (where appropriate)
Country Implementation • Ethiopia – in context of Health Sector Development
Plan (HSDP III):– Training of Health Extension Workers (HEWs) to deliver health
extension package
• Malawi – in context of Malawi Poverty Reduction Strategy and Health SWAp:– Training of Health Surveillance Assistants (HSAs) to deliver
essential health package
• Ghana – in context of “High Impact, Rapid Delivery (HIRD)” component of 5-Yr POW:– Training of Community-Based Agents (CBAs) to deliver high
impact package of services
• Niger – in context of 5-Yr health sector plan (PDS):– Training of Community Health Agents for community case
management and essential services
Implementation of CI/IHSS in Malawi: Implementation of CI/IHSS in Malawi:
Which Interventions will have the Which Interventions will have the
greatest Impact?greatest Impact?
Nationwide CoverageNational baseline
Target
2006/7 2011
Antenatal care 57% 90%
IPTp 47% 81%
Skilled care at birth 54% 67%
Postnatal visit after delivery 21% 60%
Sleeping under insecticide treated net 23% 69%
Vitamin A supplementation 80% 80%
Exclusive breastfeeding 56% 70%
85%55%Treatment of diarrhoea
69%27%Treatment of malaria
67%29%Treatment of pneumonia
85%71%Immunization
The challenge: To prioritiseinterventions with greatest impact
Nationwide CoverageNational
baselineTarget
2006/7 2011
Sleeping under insecticide treated Net
23% 69%
Treatment of pneumonia 29% 67%
Treatment of malaria 27% 69%
Treatment of diarrhoea 55% 85%
How to get there…
� Focus initially on ten districts to ensure coverage targets are achieved
� Scale up of Village Clinics across all hard-to-reach areas
� Ensure quality IMNCI in first level facilities
� Community mobilisation for improved care seeking and ITN use
� Link with ongoing PMTCT and nutrition activities (complementary feeding; management of severe malnutrition) for maximum impact
� Consider additional interventions such as postnatal visits for newborn care, WASH etc . . .
Implementation of CI/IHSS in Mozambique: Use of
the “RED Approach”
Use of RED Approach: “Reaching Every District”
Building capacity at district, health facility and community level:
1. Planning and resource management
2. Supportive supervision
3. Re-establishing Outreach services
4. Linking services with communities
5. Monitoring for action
Improve access and utilization of immunization services and create a platform for the integration of maternal and child survival interventions with immunization services.
Implementation of RED in Mozambique in context of CI/IHSS (1)
• Initial implementation in 33 Districts (three in each of 11 Provinces) in 2007/08 (criteria est. by MOH and partners)
• Deliver expanded components of the Maternal and Child Survival Package with a strong involvement of the communities, through routine services and a bi-annual Integrated Child Survival catch up interventions
• Using the EPI package as an “entry point” (through fixed, outreach and mobile strategies) for all Maternal & Child Health Survival Interventions in the district (C-IMNCI, ANC+, Targeted home visits to deliver key family practices, home treatment for newborn, etc)
Implementation of RED in Mozambique in context of CI/IHSS (2)
• Data Collection and Analysis - Database for each district has been elaborated
• Microplanning - Action plans involving all 5 RED components developed for all districts and for 350 health zones (including mapping of hard to reach areas)
• Monitoring and Supervision – 69% of planned supervisions were implemented in 1st half of 2008
• Re-establishing Outreach – only 50% of planned outreach were implemented in 1st half of 2008 (resource limitation)
• Linking Services with communities – meetings with community leaders and CHWs (>80% completed)
• Integration - activities during vaccination sessions in the health centers and outreach services are integrated with other child survival interventions such as VitAsupplementation and Antenatal care etc.
Role of Catalytic Initiative and Next Steps in Mozambique
• Accelerate policy status related to community-based services to ease implementation of community case management (e.g. pneumonia), and population oriented interventions needing inputs from Community Health Workers
• Mobilize financial assistance for scale-up and roll-out, and accelerate administrative procedures for transfer of funds to districts
• Institutionalize integration of RED in annual work plans of provinces, districts and national level
• Strengthen support to supervision, monitoring and evaluation - use of data at district and health zone levels for improved program delivery